Embed Size (px)
Citation preview
Short Term Central Venous Catheter
Policy Statement
The purpose of this policy is to provide clear guidance and instruction to staff with regard to the Trust’s approach to the insertion and management of short term central venous catheters
Key Points
The policy applies to all staff required to undertake insertion and management of short term central venous catheters (CVC’s) at Heart of England NHS Foundation Trust. The policy applies to all staff employed on a substantive or temporary contract by the Trust, including bank and agency The purpose of this policy is to ensure that complications associated with Short term CVC insertion are minimised.
Paper copies of this document
If you are reading a printed copy of this document you should check the Trust’s Policy
website (http://sharepoint/policies) to ensure that you are using the most current version.
Ratified Date: Feb 2012-01-25
Ratified By: TIPC
Review Date: Feb 2012
Accountable Directorate: Critical Care / Infection Control
Corresponding Author: Sarah Quinton & Andrew Simmons
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 1 of 25
This policy is applicable to services provided by Heartlands, Good Hope and Solihull Hospitals Divisions.
Meta Data
Document Title: Short Term Central Venous Catheter Policy
Status Final
Document Author: Sarah Quinton, Lead Nurse Andrew Simmons, Critical Care Practitioner
Source Directorate: Critical Care & Infection Control
Date Of Release: January 2012
Approval Date: Feb 2012
Approved by: TIPC
Ratification Date: Feb 2012
Ratified by: Feb 2012
Review Date: Feb 2014
Related documents • Hand Hygiene Policy 2011 • Consent to Examination & Treatment Policy 2010 • Sharps injury splash policy 2011Safe handling of sharps policy
2011 • The Health and Social care Act Code of Practice for Infection
Control 2008 • Standard Precautions Policy 2009 • Aseptic Non Touch Technique Policy V2 • Clinical Guideline for the management of suspected catheter
related blood stream infection in patients receiving parenteral nutrition (version 1)
Superseded documents
Short Term CVC policy Version 1.0 2007
Relevant External Standards/ Legislation
DH (2007) Saving Lives: Reducing Infection, delivering clean & safe care
Pratt RJ et al (2007) epic2: National Evidence-Based Guidelines for preventing healthcare –associated Infections in NHS Hospitals in England
NICE (2002) TA 49: Guidance on the use of ultrasound locating devices foe placing central venous catheters
Key Words Central Venous Catheter Vascular Access
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 2 of 25
Revision History
Version
Status
Date
Consultee
Comments Action from Comment
1.0 approved 2007 Sarah Quinton Anne Mutlow Darren Daniels
2.0 Draft 2011 Sarah Quinton Andy Simmons Carol Drugan
Policy due for review , minor amendments
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 3 of 25
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 4 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 4 of 25
Table of Contents
Policy Template .............................................................................. Error! Bookmark not defined.
(1)Circulation .................................................................................................................................. 5
(2)Scope......................................................................................................................................... 5
(3)Definitions .................................................................................................................................. 5
(4)Reason for development ............................................................................................................ 5
(5)Aims and Objectives .................................................................................................................. 5
(6)Standards (for Policies) / Process (for Procedure) (delete as applicable) ................................... 6
(7)Responsibilities .......................................................................................................................... 8
Individual Responsibilities............................................................... Error! Bookmark not defined.
Chief Executive .......................................................................... Error! Bookmark not defined.
Executive Directors.................................................................................................................... 8
Individual Staff Responsibilities ................................................................................................. 9
Other Staff/ Contractors/Patients ................................................ Error! Bookmark not defined.
Board and Committee Responsibilities ........................................... Error! Bookmark not defined.
Ratifying Board and Committee Responsibilities........................................................................ 9
Operational Committees ............................................................. Error! Bookmark not defined.
(8)Training Requirements ............................................................................................................. 10
(9)Monitoring and Compliance...................................................................................................... 10
See Core Training Policy (currently under development) ................. Error! Bookmark not defined.
Attachment 1: Equality and Diversity - Policy Screening Checklist............................................... 20
Attachment 2: Approval/Ratification Checklist.............................................................................. 23
Attachment 3: Launch and Implementation Plan.......................................................................... 25

©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 5 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 5 of 25
1 Circulation
This policy applies to all staff required to insert or manage patients who require a Short Term Central Venous Catheter (CVC) at Heart of England NHS Foundation Trust, employed on a substantive or temporary contract by the Trust including bank , agency & locum staff.
2. Scope
2.1 Includes:
This Policy applies to all staff required to undertake insertion and management of short term CVC’s by or on behalf of HEFT
2.2 Excludes:
This policy does not apply to Neonatal or Paediatric patients
Hickman Lines: Please see HEFT Policy
Renal Vascular Access : Please see HEFT Policy
PICC (Peripherally Inserted Central Catheter) Lines : Please see HEFT Policy
3. Definitions
Short term Central Venous Catheters (CVC): A short term CVC is any vascular access device sited in large vein of the neck or trunk with the purpose of accessing a central vein, which is intended to stay in situ for 28 days or less.
4. Reason for development
The use of CVC’s are associated with complications at any point from insertion through to removal.
National Evidence Based Guidelines for Preventing Healthcare Associated Infections in NHS Hospitals in England (ePIC2, 2007) endorsed by the Department of Health describe the precautions that healthcare workers should take and standard principles for preventing HCAI. EPIC 2 (2007) guidelines are based on the best currently available evidence and should be integrated into routine daily clinical practice at HEFT.
5. Aims and Objectives
The aim of this policy is to:
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 6 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 6 of 25
• ensure safe insertion, appropriate review and effective management of all inpatients requiring a short term CVC
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 7 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 7 of 25
The Objectives of this policy are to:
• Provide staff with an evidence based policy to enable them to carry out clinical procedures in
a manner that maintains and promotes principles of asepsis.
• Provide standardised education training and assessment to all staff undertaking such procedures
• Promote a standardised approach across the organisation
• Ensure that the Trust complies with National Statutory requirements in relation to the core
policies and follows current best evidence based practice
• NB: All staff have a responsibility to ensure that they develop and maintain the knowledge and skills to undertake the duties and responsibilities of their post.
6. Process
6.1 Assessing Patients for CVC Insertion
Prior to the insertion of a central venous catheter a full assessment must be performed of the patient’s clinical status
• All patients in a non Critical Care area must be referred to the Critical Care Outreach Team
to assess need for insertion. It is the responsibility of the ward nurse caring for the patient to ensure the referral has been made. However, if the line is required for the delivery of Total Parenteral Nutrition then the referral should be made to the Nutrition Team.
• If CVC insertion is required due to poor peripheral access, it should only be after all possible
attempts at peripheral cannulation have failed.
• Peripheral venous cannulae (venflon), PICC or Midline should be considered instead of short-term CVC
• Assessment should be undertaken to determine the best site for CVC insertion. The
Femoral site should be avoided unless absolutely necessary.
• Coagulation status should be checked prior to insertion - thrombocytopenia (low platelets <30) or INR >2, high risk factors for haemorrhage
• Respiratory function and ability to lie flat or head down should be considered
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 8 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 8 of 25
• Assess allergy status: dressings, cleaning solution, silver in CVC prior to procedure
• Consent must be obtained if patient has capacity. If patient does not have capacity then decision to insert line should be made in patients best interests.
6.2 Insertion of Central Venous Catheter
Where to insert
• Non emergency insertion of CVC should be performed only in a Critical Care area or operating theatres, or a designated clean clinical area.
• Critical Care Outreach should be contacted for advice to facilitate the process.
• If line inserted during a surgical procedure, then contact CCOT so appropriate follow up can
be arranged. This is the responsibility of the ward nurse to make the referral when the patient returns to the ward postoperatively. However, if line for parenteral feeding then the nutritional team must be contacted.
Who can insert
• Only Practitioners who have received training in the insertion of CVC’s can insert CVCs and supervise non-experienced clinicians
• Insertion techniques literature – NICE 2002 states that two-dimensional imaging ultrasound guidance is recommended as the preferred method for insertion of CVC in the internal jugular vein in adults
• HEFT recommends the use of ultrasound guidance when inserting CVC’s • CVC Insertion Observer Checklist should be completed at insertion (Appendix 2)
Equipment
• CVC insertion packs must be used. These packs contain most of the equipment required for
insertion • Other equipment required : Sterile gloves, hat, mask, Chlorhexidine impregnated
(chloraprep) sponge and lidocaine 1%, chlorhexidine impregnated patch (biopatch) Documentation
• CVC Insertion Observer Checklist should be completed at insertion (Appendix 2) • CVC insertion label must be completed and placed in patient notes (Label inside CVC pack)
Patient Decolonisation Prior to Insertion
• All patients should be washed in Chlorhexidine prior to insertion of the line. If this is omitted
then the reason should be clearly documented in patient multidisciplinary record.
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 9 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 9 of 25
Patients should then be washed daily in chlorhexidine until MRSA status is confirmed.
• Patients who are MRSA +ve should be washed daily using Chlorhexidine while the CVC remains in situ and continued until patient discharge.
6.3 Review & Removal of Central Venous Catheter
• All adult inpatients will be reviewed by CCOT every 24 - 48 hours for surveillance and monitoring
• CVC care bundle should be implemented • All reviews by the CCOT will be documented in the multidisciplinary notes • CVC’s should be removed as soon as no longer required
Any patients requiring a CVC for Total Parenteral nutrition will be handed over to the Nutrition team for continued daily review. It is the responsibility of the Critical Care Outreach Team to refer the patient to the Nutrition Team
If Total Parenteral nutrition is discontinued and the CVC is still required the nutrition team will refer the patient back to the Critical Care Outreach Team for ongoing monitoring and review, until line is removed. It is the responsibility of the Nutrition Team to make the referral back to the Critical Care Outreach Team
7. Responsibilities
7.1 Chief Executive
The Chief Executive has overall responsibility for the implementation, monitoring and
renewal of this Policy. This responsibility is delegated to the medical Director and Chief
Nurse .
7.2 Medical Directors It is the responsibility of the Group Medical Directors to oversee the monitoring and
application of this Policy and to report as necessary to the Trust Board via the
Operations Committee.
7.3 Chief Nurse
The Chief Nurse is responsible for monitoring compliance with the Short term CVC Policy
The Chief Nurse will delegate this operational responsibility to the Heads of Nursing
Team.
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 10 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 10 of 25
7.4 Heads of Nursing
The Heads of Nursing are responsible for monitoring compliance with the Policy on
behalf of the sites.
7.5 Clinical Directors
Clinical Directors are responsible for ensuring that Consultants within their Directorates
understand the Policy and ensure that it is applied within their practice.
7.6 Directorate Management Team
The Directorate Management Team is responsible for implementing and communicating the Short Term CVC Policy in their Directorate areas.
7.7 Matrons
Matrons are responsible for ensuring that all nursing staff within their remit comply with
the Short Term CVC policy. They are also responsible for ensuring that nursing staff are
competent to undertake care of a CVC in a manner which is appropriate to their roles
and responsibilities. Matrons may delegate day to day responsibility of training &
assessment to the line manager of the individual healthcare worker. This includes
student nurses, bank & agency staff in their area.
7.9 Individual Responsibility
• Individuals have a responsibility for their own development. All staff are required to demonstrate that they possess the knowledge, skills and abilities required for lawful, safe and effective practice without direct supervision.
• Medical staff should ensure they are familiar with and adhere to the Short Term CVC Policy.
• Undergraduates, Health Care Assistants and Support Workers should only undertake
procedures related to Short Term Central venous Catheters that have been deemed
appropriate to their duties and have been deemed competent to perform.
8. Board and Committee Responsibilities
Ratifying Board and Committee Responsibilities
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 11 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 11 of 25
Policy ratified by Trust Infection prevention and control committee. The purpose of the Trust Infection Prevention Committee is to ensure continuous improvement and reduction in rates of healthcare associated infection while proving a Trust wide operations facilitation forum for control of infection. The group consists of a membership including Management, Nursing, Infection Control and Hotel Services.
8. Training Requirements
All medical and nursing staff required to insert CVC’s as part of their role should have
received appropriate competency based education / training
The training & education provided on management of Short Term Central Venous Catheter may be delivered in a variety of formats eg:
Mandatory Infection Control Updates One off sessions/refresher training ISkills Video E- learning material Teaching in the clinical area and supervised practice Training within individual directorates or departments
9. Monitoring and Compliance
All staff required to insert and manage short term CVC’s are expected to comply with the
Trust Short Term CVC policy.
CCOT will monitor local compliance against Trust policy and reflect any poor compliance
through individual directorate teams.
9.1 Non Compliance Incidents of failure to comply with the Short term CVC policy should be reported in accordance with the Trust’s incident reporting policy.
It is the responsibility of all health care providers/professionals to report via the Trust’s incident reporting system failures to comply with policy.
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 12 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 12 of 25
10. References
Centres for Disease Control and Prevention (CCDSC) (2002) Guidelines for the prevention of intravascular catheter-related infections. Morbidity and Mortality weekly Report 51, 1-29.
Department of Health (DOH) (2001) Guidelines for preventing infections associated with insertion and maintenance of central venous catheters. Journal of Hospital Infection 47 (supplement), S47-S67.
Department of Health (2004),The NHS Knowledge and Skills Framework (NHS KSF) and the Development Review Process. Department of Health Publications, London.
Department of Health (DOH) (2005) Saving Lives: a delivery programme to reduce healthcare associated infection, including MRSA. London
Department of Health (2006) The Health Act: Code of Practice for the Prevention and Control of Health Care Associated Infections. London DH, 2006.
Drewett S. (2000) Complications of central venous catheters: nursing care. British Journal of Nursing, 9(8) 466-478.
Fletcher S.J. and Bodenham A.R. (1999a) Catheter-related sepsis: an overview – part 1. British Journal of Intensive Care 9, 46-53.
Maki, D. Ringer, M. & Alvardo, C.J. (1991) Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for the prevention of infection associated with central venous and arterial catheters. Lancet 338(10), 339-343.
Maki, D.G. Stolz, S.M. Wheeler, S. et al. (1997) Prevention of central venous catheter-related bloodstream infection by use of an antiseptic-impregnated catheter. Annals of Internal Medicine 127(4), 257-266
National Institute for Clinical Excellence (2002) Guidance on the use of ultrasound locating devices for placing central venous catheters. London.
National Institute for Clinical Excellence (2003) Infection Control: Prevention of Health Care Associated Infection in Primary and Community Care. London.
Pratt RJ, Pellowe CM, Wilson JA, Loveday HP, Harper PJ, Jones SRLJ, McDougall C,Wilcox MH (2007). Epic 2: National Evidence-Based Guidelines for Preventing Healthcare Associated Infections in NHS Hospitals in England. Journal of Hospital Infection 2007; 65 (Supplement): S1- S31.
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 13 of 25 ©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 13 of 25
Public Health Laboratory Service (PHLS) (1998) Protocol for surveillance of hospital-acquired bacteraemia: version 1, 1 internal policy document. London: Nosocomial Infection National Surveillance Scheme, Central Public Health Laboratory, March 1998, 45.
Royal Marsden Hospital (2004) Manual of Clinical Nursing Procedures. 6th Ed Blackwell Publishing, London.
Sitges-Serra, A. Linares, J. & Garau, J. (1985) Catheter sepsis: the clue is the hub. Surgery 97, 356-357.
Timsit, JF et al (2009) Chlorhexidine – impregnated sponges and less frequent dressing changes for prevention of catheter related infections in critically ill adults. JAMA, Vol 301, No. 12, 1231- 1244.
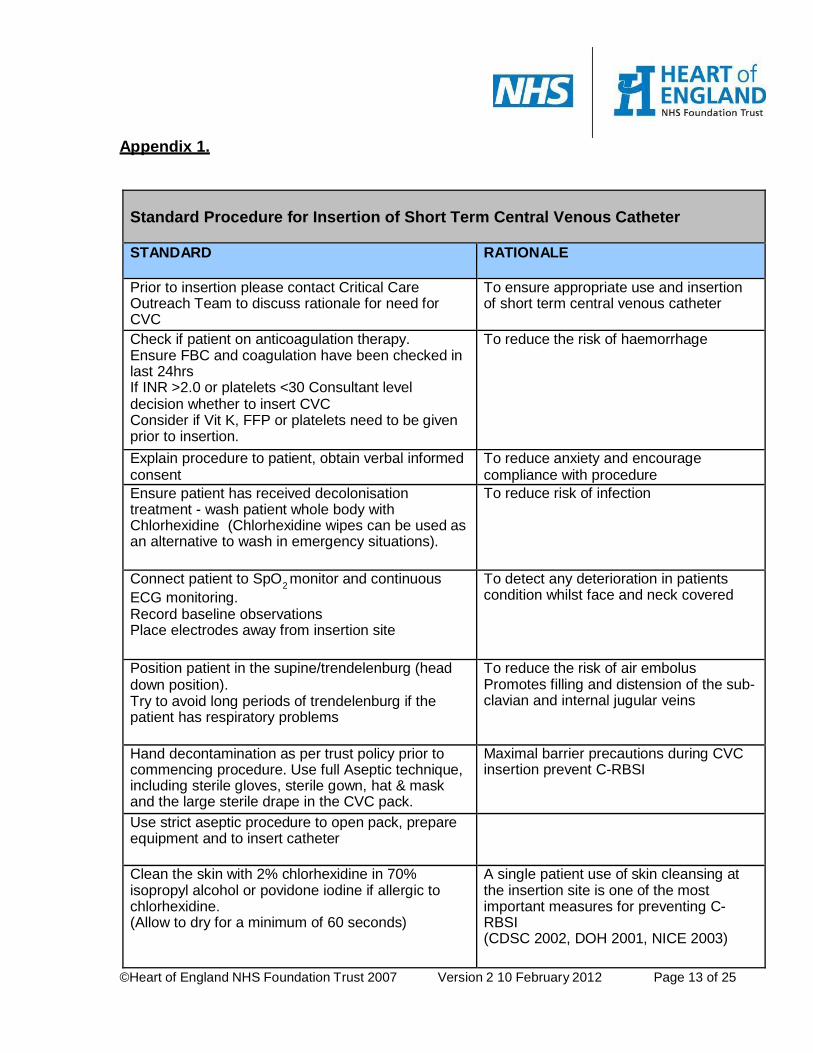
Appendix 1.
Standard Procedure for Insertion of Short Term Central Venous Catheter
STANDARD RATIONALE
Prior to insertion please contact Critical Care Outreach Team to discuss rationale for need for CVC
To ensure appropriate use and insertion of short term central venous catheter
Check if patient on anticoagulation therapy. Ensure FBC and coagulation have been checked in last 24hrs If INR >2.0 or platelets <30 Consultant level decision whether to insert CVC Consider if Vit K, FFP or platelets need to be given prior to insertion.
To reduce the risk of haemorrhage
Explain procedure to patient, obtain verbal informed consent
To reduce anxiety and encourage compliance with procedure
Ensure patient has received decolonisation treatment - wash patient whole body with Chlorhexidine (Chlorhexidine wipes can be used as an alternative to wash in emergency situations).
To reduce risk of infection
Connect patient to SpO monitor and continuous 2
ECG monitoring. Record baseline observations Place electrodes away from insertion site
To detect any deterioration in patients condition whilst face and neck covered
Position patient in the supine/trendelenburg (head down position). Try to avoid long periods of trendelenburg if the patient has respiratory problems
To reduce the risk of air embolus Promotes filling and distension of the sub- clavian and internal jugular veins
Hand decontamination as per trust policy prior to commencing procedure. Use full Aseptic technique, including sterile gloves, sterile gown, hat & mask and the large sterile drape in the CVC pack.
Maximal barrier precautions during CVC insertion prevent C-RBSI
Use strict aseptic procedure to open pack, prepare equipment and to insert catheter
Clean the skin with 2% chlorhexidine in 70% isopropyl alcohol or povidone iodine if allergic to chlorhexidine. (Allow to dry for a minimum of 60 seconds)
A single patient use of skin cleansing at the insertion site is one of the most important measures for preventing C- RBSI (CDSC 2002, DOH 2001, NICE 2003)
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 13 of 25
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 14 of 25
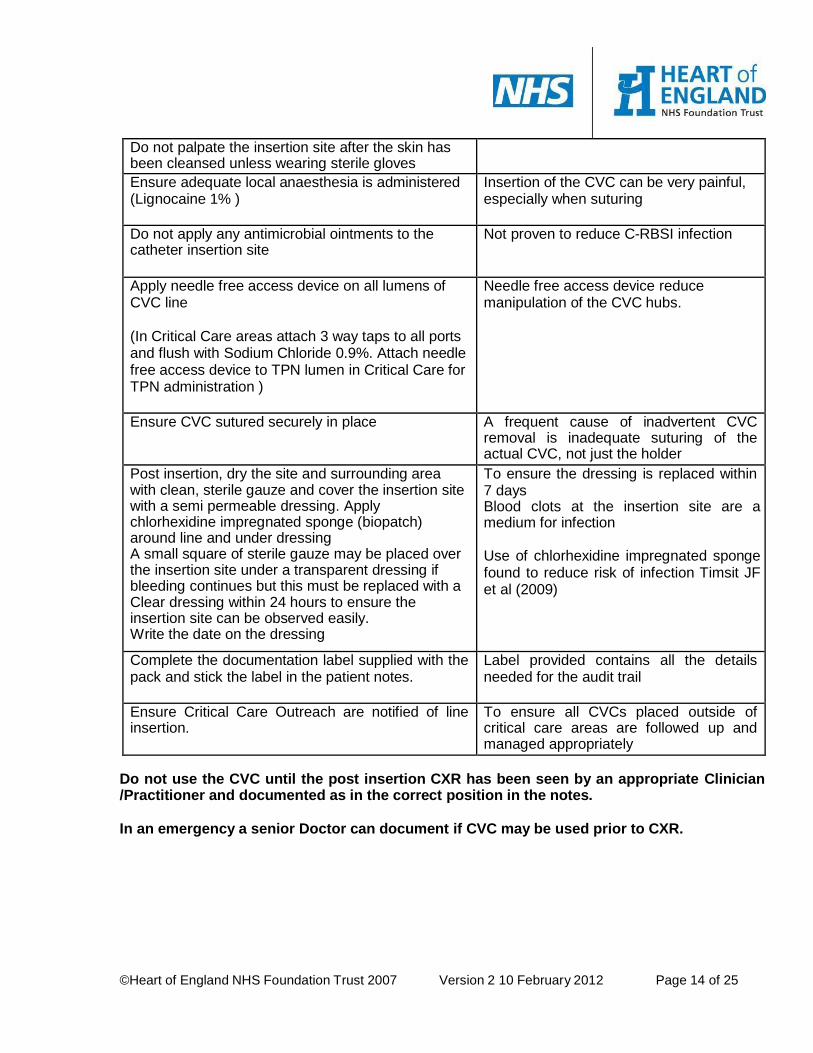
Do not palpate the insertion site after the skin has been cleansed unless wearing sterile gloves
Ensure adequate local anaesthesia is administered (Lignocaine 1% )
Insertion of the CVC can be very painful, especially when suturing
Do not apply any antimicrobial ointments to the catheter insertion site
Not proven to reduce C-RBSI infection
Apply needle free access device on all lumens of CVC line
(In Critical Care areas attach 3 way taps to all ports and flush with Sodium Chloride 0.9%. Attach needle free access device to TPN lumen in Critical Care for TPN administration )
Needle free access device reduce manipulation of the CVC hubs.
Ensure CVC sutured securely in place A frequent cause of inadvertent CVC removal is inadequate suturing of the actual CVC, not just the holder
Post insertion, dry the site and surrounding area with clean, sterile gauze and cover the insertion site with a semi permeable dressing. Apply chlorhexidine impregnated sponge (biopatch) around line and under dressing A small square of sterile gauze may be placed over the insertion site under a transparent dressing if bleeding continues but this must be replaced with a Clear dressing within 24 hours to ensure the insertion site can be observed easily. Write the date on the dressing
To ensure the dressing is replaced within 7 days Blood clots at the insertion site are a medium for infection
Use of chlorhexidine impregnated sponge found to reduce risk of infection Timsit JF et al (2009)
Complete the documentation label supplied with the pack and stick the label in the patient notes.
Label provided contains all the details needed for the audit trail
Ensure Critical Care Outreach are notified of line insertion.
To ensure all CVCs placed outside of critical care areas are followed up and managed appropriately
Do not use the CVC until the post insertion CXR has been seen by an appropriate Clinician /Practitioner and documented as in the correct position in the notes.
In an emergency a senior Doctor can document if CVC may be used prior to CXR.
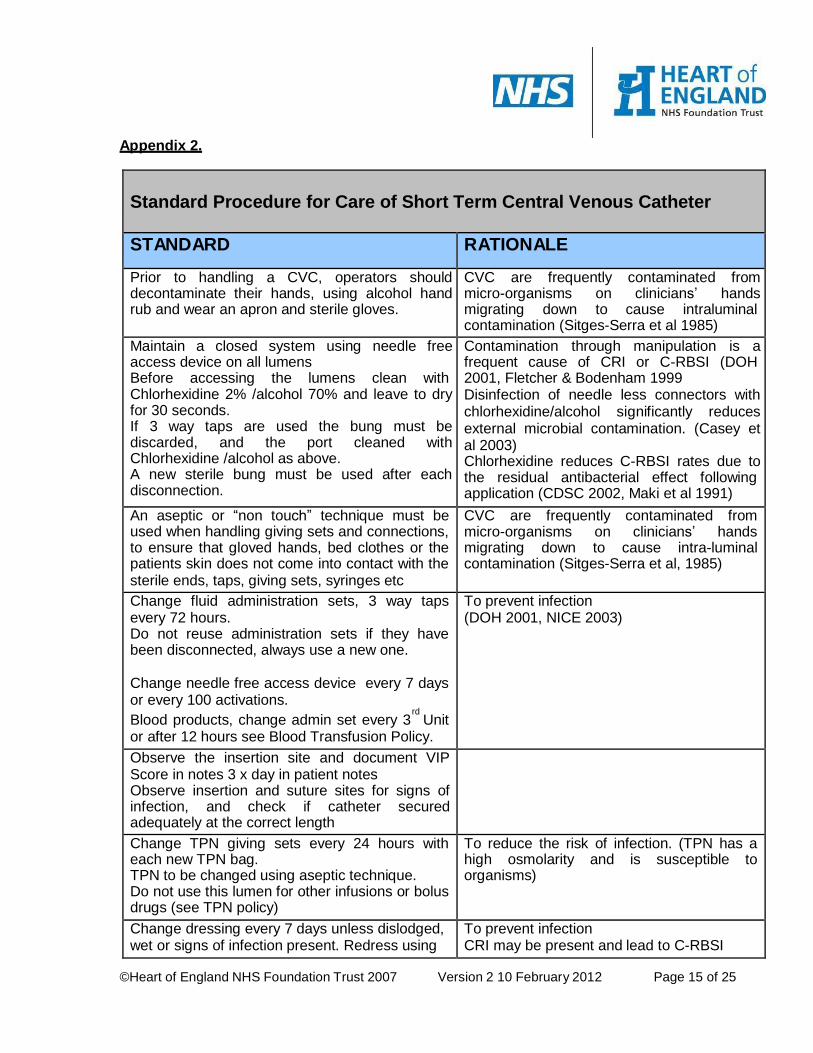
Appendix 2.
Standard Procedure for Care of Short Term Central Venous Catheter
STANDARD RATIONALE
Prior to handling a CVC, operators should decontaminate their hands, using alcohol hand rub and wear an apron and sterile gloves.
CVC are frequently contaminated from micro-organisms on clinicians’ hands migrating down to cause intraluminal contamination (Sitges-Serra et al 1985)
Maintain a closed system using needle free access device on all lumens Before accessing the lumens clean with Chlorhexidine 2% /alcohol 70% and leave to dry for 30 seconds. If 3 way taps are used the bung must be discarded, and the port cleaned with Chlorhexidine /alcohol as above. A new sterile bung must be used after each disconnection.
Contamination through manipulation is a frequent cause of CRI or C-RBSI (DOH 2001, Fletcher & Bodenham 1999 Disinfection of needle less connectors with chlorhexidine/alcohol significantly reduces external microbial contamination. (Casey et al 2003) Chlorhexidine reduces C-RBSI rates due to the residual antibacterial effect following application (CDSC 2002, Maki et al 1991)
An aseptic or “non touch” technique must be used when handling giving sets and connections, to ensure that gloved hands, bed clothes or the patients skin does not come into contact with the sterile ends, taps, giving sets, syringes etc
CVC are frequently contaminated from micro-organisms on clinicians’ hands migrating down to cause intra-luminal contamination (Sitges-Serra et al, 1985)
Change fluid administration sets, 3 way taps every 72 hours. Do not reuse administration sets if they have been disconnected, always use a new one.
Change needle free access device every 7 days or every 100 activations.
rd
Blood products, change admin set every 3 Unit or after 12 hours see Blood Transfusion Policy.
To prevent infection (DOH 2001, NICE 2003)
Observe the insertion site and document VIP Score in notes 3 x day in patient notes Observe insertion and suture sites for signs of infection, and check if catheter secured adequately at the correct length
Change TPN giving sets every 24 hours with each new TPN bag. TPN to be changed using aseptic technique. Do not use this lumen for other infusions or bolus drugs (see TPN policy)
To reduce the risk of infection. (TPN has a high osmolarity and is susceptible to organisms)
Change dressing every 7 days unless dislodged, wet or signs of infection present. Redress using
To prevent infection CRI may be present and lead to C-RBSI
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 15 of 25
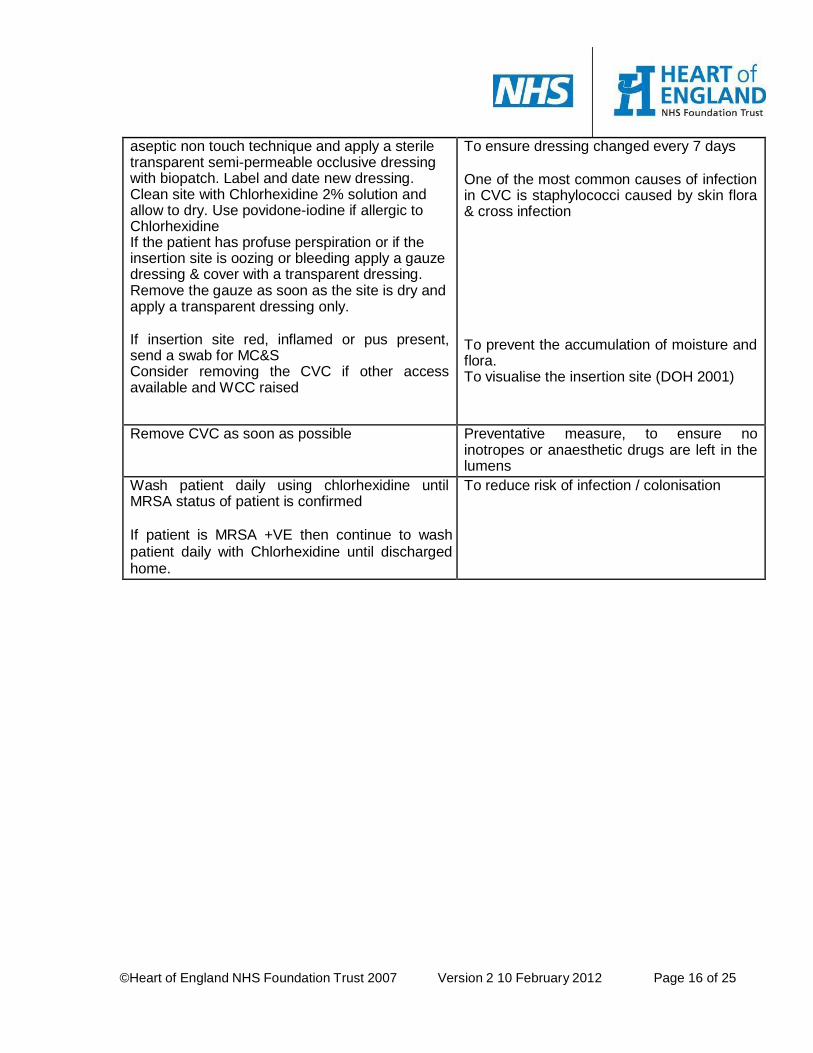
aseptic non touch technique and apply a sterile transparent semi-permeable occlusive dressing with biopatch. Label and date new dressing. Clean site with Chlorhexidine 2% solution and allow to dry. Use povidone-iodine if allergic to Chlorhexidine If the patient has profuse perspiration or if the insertion site is oozing or bleeding apply a gauze dressing & cover with a transparent dressing. Remove the gauze as soon as the site is dry and apply a transparent dressing only.
If insertion site red, inflamed or pus present, send a swab for MC&S Consider removing the CVC if other access available and WCC raised
To ensure dressing changed every 7 days One of the most common causes of infection in CVC is staphylococci caused by skin flora & cross infection
To prevent the accumulation of moisture and flora. To visualise the insertion site (DOH 2001)
Remove CVC as soon as possible Preventative measure, to ensure no inotropes or anaesthetic drugs are left in the lumens
Wash patient daily using chlorhexidine until MRSA status of patient is confirmed
If patient is MRSA +VE then continue to wash patient daily with Chlorhexidine until discharged home.
To reduce risk of infection / colonisation
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 16 of 25

Appendix 3
Standard Procedure for Administration of Dugs / Fluids via Short Term Central Venous Catheter
STANDARD RATIONALE
Explain and discuss procedure with the patient
Ensure clean technique (hand washing). Put on apron and sterile gloves
Reduce the risk of infection
Using aseptic technique - swab with Chlorhexidine 2% & Alcohol 70% leave to dry for 30 seconds, or remove bung and discard, then swab with prep pad as above.
Clamp line with attached plastic clip before any bungs, syringes or infusions are removed.
Flush line with 10ml Sodium Chloride 0.9% IV solution to ensure patency. Do not force. If resistance felt discontinue the procedure, cap off the lumen and inform medical staff or outreach team.
Inject drug as per hospital guidelines.
Replace with new sterile bung
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 17 of 25
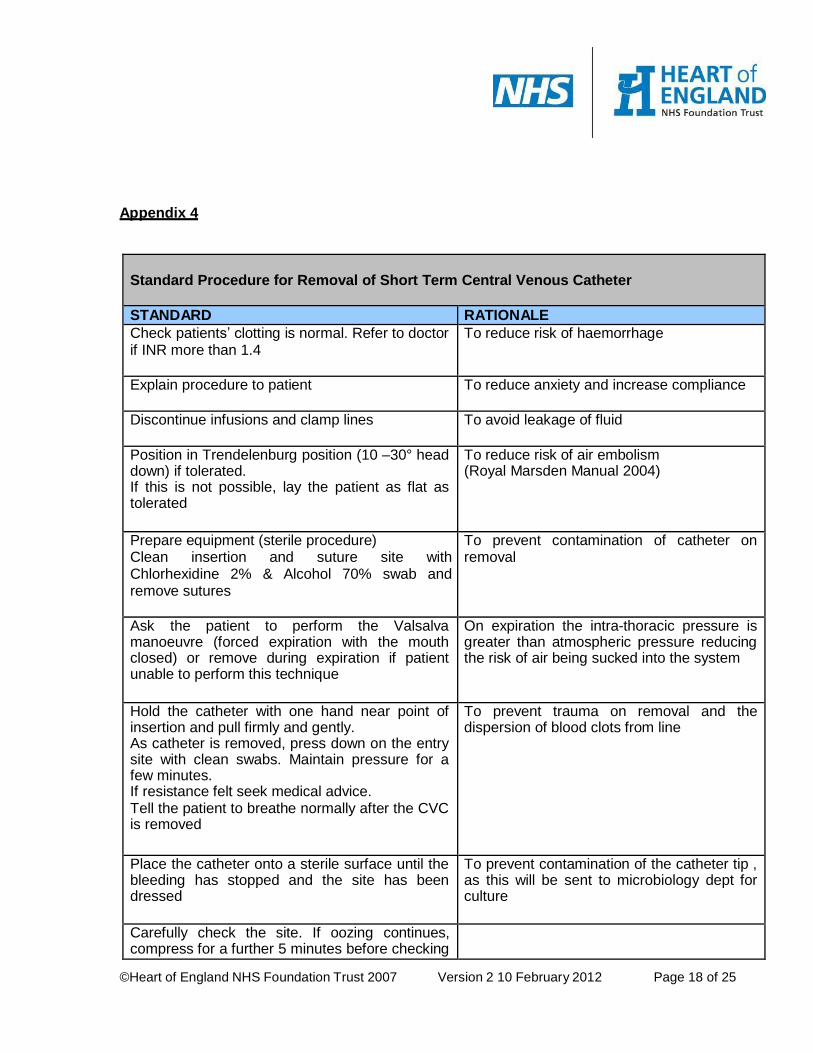
Appendix 4
Standard Procedure for Removal of Short Term Central Venous Catheter
STANDARD RATIONALE
Check patients’ clotting is normal. Refer to doctor if INR more than 1.4
To reduce risk of haemorrhage
Explain procedure to patient To reduce anxiety and increase compliance
Discontinue infusions and clamp lines To avoid leakage of fluid
Position in Trendelenburg position (10 –30° head down) if tolerated. If this is not possible, lay the patient as flat as tolerated
To reduce risk of air embolism (Royal Marsden Manual 2004)
Prepare equipment (sterile procedure) Clean insertion and suture site with Chlorhexidine 2% & Alcohol 70% swab and remove sutures
To prevent contamination of catheter on removal
Ask the patient to perform the Valsalva manoeuvre (forced expiration with the mouth closed) or remove during expiration if patient unable to perform this technique
On expiration the intra-thoracic pressure is greater than atmospheric pressure reducing the risk of air being sucked into the system
Hold the catheter with one hand near point of insertion and pull firmly and gently. As catheter is removed, press down on the entry site with clean swabs. Maintain pressure for a few minutes. If resistance felt seek medical advice. Tell the patient to breathe normally after the CVC is removed
To prevent trauma on removal and the dispersion of blood clots from line
Place the catheter onto a sterile surface until the bleeding has stopped and the site has been dressed
To prevent contamination of the catheter tip , as this will be sent to microbiology dept for culture
Carefully check the site. If oozing continues, compress for a further 5 minutes before checking
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 18 of 25
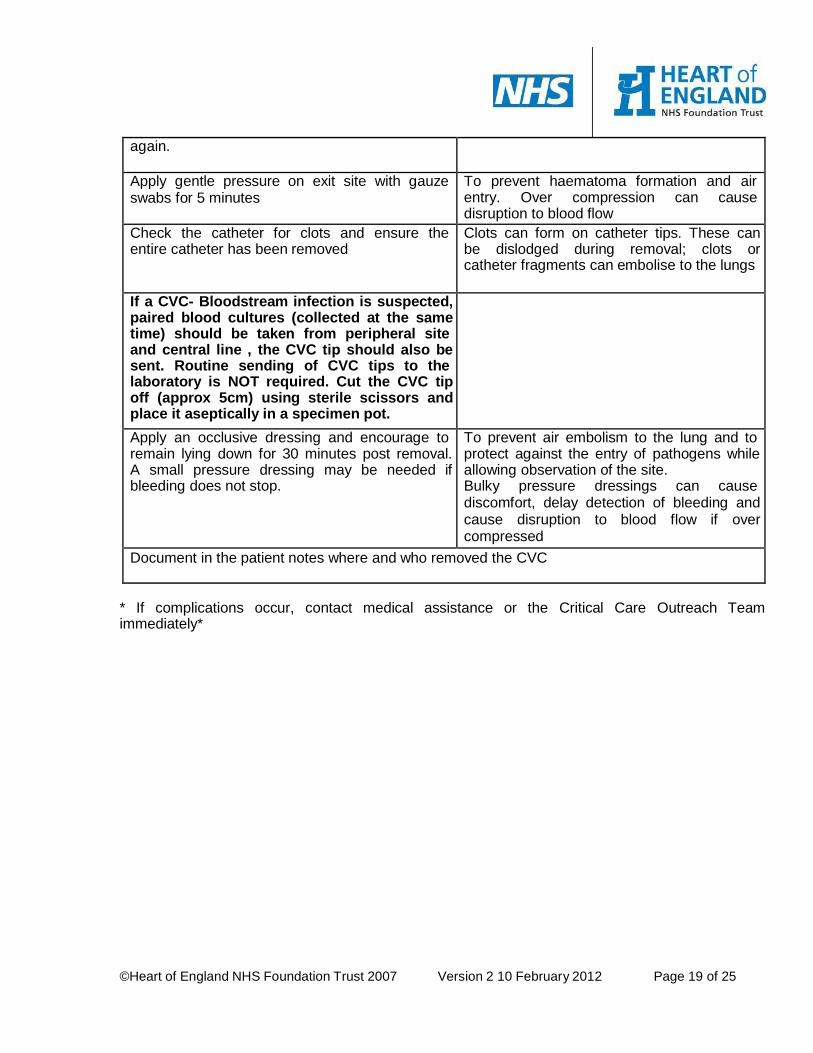
again.
Apply gentle pressure on exit site with gauze swabs for 5 minutes
To prevent haematoma formation and air entry. Over compression can cause disruption to blood flow
Check the catheter for clots and ensure the entire catheter has been removed
Clots can form on catheter tips. These can be dislodged during removal; clots or catheter fragments can embolise to the lungs
If a CVC- Bloodstream infection is suspected, paired blood cultures (collected at the same time) should be taken from peripheral site and central line , the CVC tip should also be sent. Routine sending of CVC tips to the laboratory is NOT required. Cut the CVC tip off (approx 5cm) using sterile scissors and place it aseptically in a specimen pot.
Apply an occlusive dressing and encourage to remain lying down for 30 minutes post removal. A small pressure dressing may be needed if bleeding does not stop.
To prevent air embolism to the lung and to protect against the entry of pathogens while allowing observation of the site. Bulky pressure dressings can cause discomfort, delay detection of bleeding and cause disruption to blood flow if over compressed
Document in the patient notes where and who removed the CVC
* If complications occur, contact medical assistance or the Critical Care Outreach Team immediately*
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 19 of 25
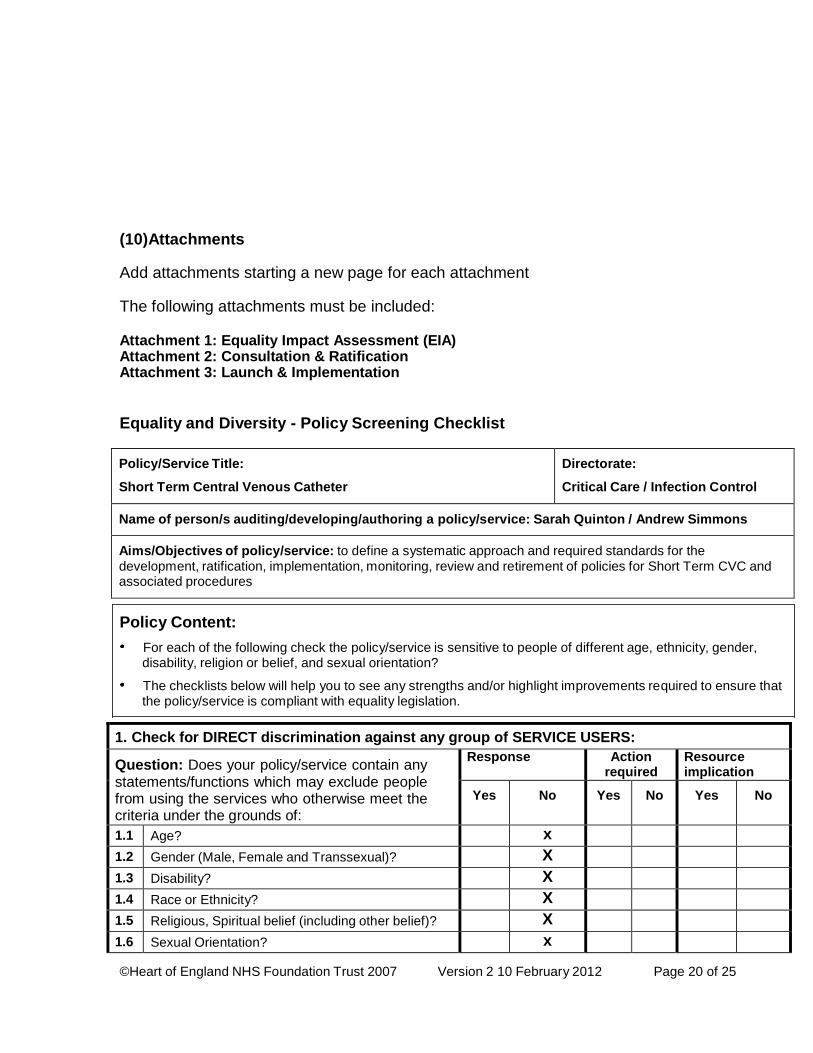
(10)Attachments
Add attachments starting a new page for each attachment
The following attachments must be included:
Attachment 1: Equality Impact Assessment (EIA) Attachment 2: Consultation & Ratification Attachment 3: Launch & Implementation
Equality and Diversity - Policy Screening Checklist
Policy/Service Title:
Short Term Central Venous Catheter
Directorate:
Critical Care / Infection Control
Name of person/s auditing/developing/authoring a policy/service: Sarah Quinton / Andrew Simmons
Aims/Objectives of policy/service: to define a systematic approach and required standards for the development, ratification, implementation, monitoring, review and retirement of policies for Short Term CVC and associated procedures
Policy Content:
For each of the following check the policy/service is sensitive to people of different age, ethnicity, gender, disability, religion or belief, and sexual orientation?
The checklists below will help you to see any strengths and/or highlight improvements required to ensure that the policy/service is compliant with equality legislation.
1. Check for DIRECT discrimination against any group of SERVICE USERS:
Question: Does your policy/service contain any statements/functions which may exclude people from using the services who otherwise meet the criteria under the grounds of:
Response Action required
Resource implication
Yes
No
Yes
No
Yes
No
1.1 Age? x
1.2 Gender (Male, Female and Transsexual)? X
1.3 Disability? X
1.4 Race or Ethnicity? X
1.5 Religious, Spiritual belief (including other belief)? X
1.6 Sexual Orientation? x
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 20 of 25
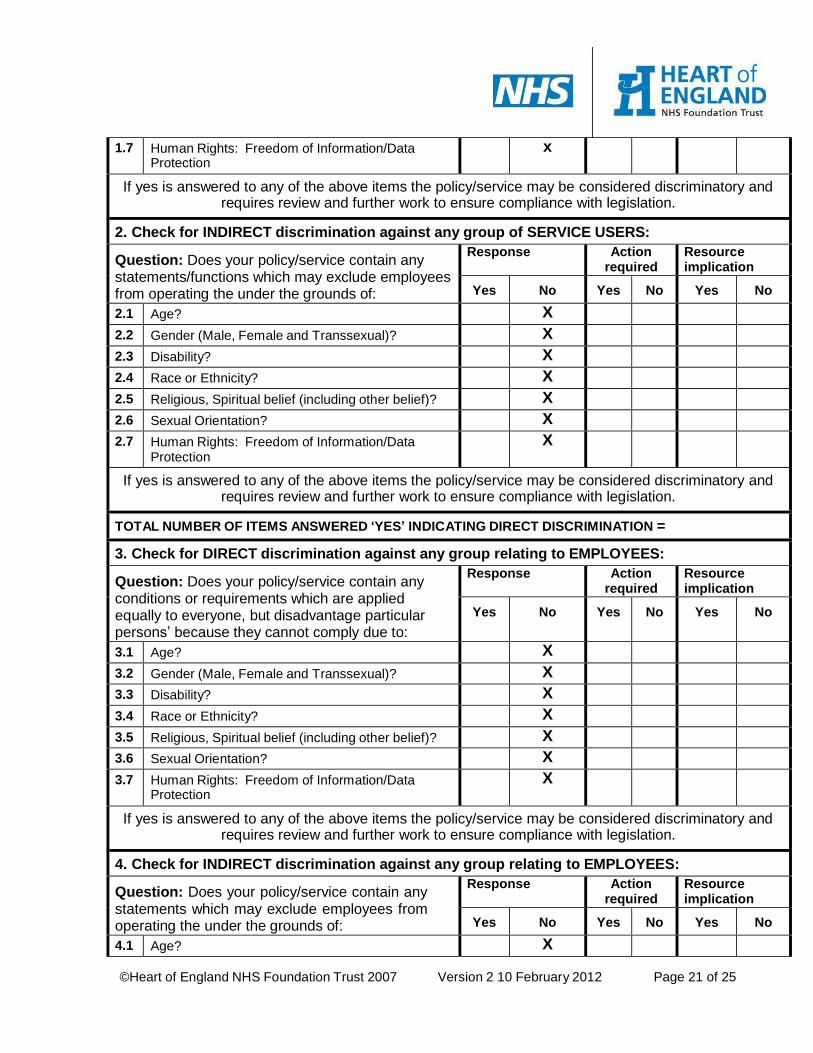
1.7 Human Rights: Freedom of Information/Data
Protection
x
If yes is answered to any of the above items the policy/service may be considered discriminatory and requires review and further work to ensure compliance with legislation.
2. Check for INDIRECT discrimination against any group of SERVICE USERS:
Question: Does your policy/service contain any statements/functions which may exclude employees from operating the under the grounds of:
Response Action required
Resource implication
Yes
No
Yes
No
Yes
No
2.1 Age? X
2.2 Gender (Male, Female and Transsexual)? X
2.3 Disability? X
2.4 Race or Ethnicity? X
2.5 Religious, Spiritual belief (including other belief)? X
2.6 Sexual Orientation? X
2.7 Human Rights: Freedom of Information/Data Protection
X
If yes is answered to any of the above items the policy/service may be considered discriminatory and requires review and further work to ensure compliance with legislation.
TOTAL NUMBER OF ITEMS ANSWERED ‘YES’ INDICATING DIRECT DISCRIMINATION =
3. Check for DIRECT discrimination against any group relating to EMPLOYEES:
Question: Does your policy/service contain any conditions or requirements which are applied equally to everyone, but disadvantage particular persons’ because they cannot comply due to:
Response Action required
Resource implication
Yes
No
Yes
No
Yes
No
3.1 Age? X
3.2 Gender (Male, Female and Transsexual)? X
3.3 Disability? X
3.4 Race or Ethnicity? X
3.5 Religious, Spiritual belief (including other belief)? X
3.6 Sexual Orientation? X
3.7 Human Rights: Freedom of Information/Data Protection
X
If yes is answered to any of the above items the policy/service may be considered discriminatory and requires review and further work to ensure compliance with legislation.
4. Check for INDIRECT discrimination against any group relating to EMPLOYEES:
Question: Does your policy/service contain any statements which may exclude employees from operating the under the grounds of:
Response Action required
Resource implication
Yes
No
Yes
No
Yes
No
4.1 Age? X
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 21 of 25
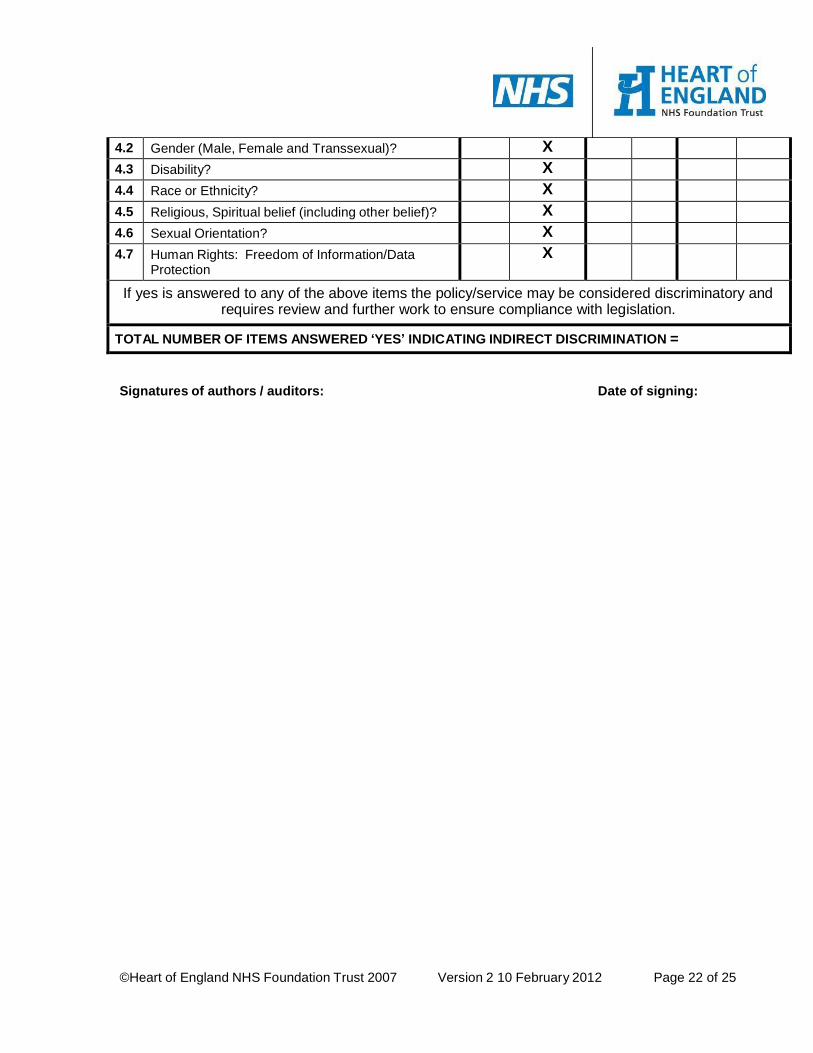
4.2 Gender (Male, Female and Transsexual)? X
4.3 Disability? X
4.4 Race or Ethnicity? X
4.5 Religious, Spiritual belief (including other belief)? X
4.6 Sexual Orientation? X
4.7 Human Rights: Freedom of Information/Data Protection
X
If yes is answered to any of the above items the policy/service may be considered discriminatory and requires review and further work to ensure compliance with legislation.
TOTAL NUMBER OF ITEMS ANSWERED ‘YES’ INDICATING INDIRECT DISCRIMINATION =
Signatures of authors / auditors: Date of signing:
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 22 of 25

Approval/Ratification Checklist
Title Short Term Central Venous Catheter Policy
Ratification checklist Details
1 Is this a: Combined Policy & Procedure
2 Is this: Revised
3* Format matches Policies and Procedures Template (Organisation-wide)
Yes
4* Consultation with range of internal /external groups/ individuals
Infection Control Team Consultant Intensivist – Dr R Daniels Consultant Microbiologist – Dr I Gupta
5* Equality Impact Assessment completed Yes
6 Are there any governance or risk implications? (e.g. patient safety, clinical effectiveness, compliance with or deviation from National guidance or legislation etc)
No
7 Are there any operational implications?
8 Are there any educational or training implications?
Yes Ongoing training required for medical & nursing staff
9 Are there any clinical implications? If yes, which clinical committee / personnel (including names and role) have assessed risks and approved the document
10 Are there any nursing implications? If yes, which nursing committee / personnel (including names and role) have assessed risks and approved the document
11 Does the document have financial implications?
No
12 Does the document have HR implications? No
13* Is there a launch/communication/implementation plan within the document?
Yes See attached plan
14* Is there a monitoring plan within the document?
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 23 of 25

15* Does the document have a review date in line with the Policies and Procedures Framework?
Yes
16* Is there a named Director responsible for review of the document?
No
17* Is there a named committee with clearly stated responsibility for approval monitoring and review of the document?
Trust Infection Prevention and control committee
Document Author / Sponsor
Signed ……………………… ………….…………
Title…………………………………………………
Date…………………….………….………….……
Approved by (Chair of Trust Committee or Executive Lead)
Signed ……………………… ………….…………
Title…………………………………………………
Date…………………….………….………….……
Ratified by (Chair of Trust Committee or Executive Lead)
Signed ……………………… ………….…………
Title…………………………………………………
Date…………………….………….………….……
©Heart of England NHS Foundation Trust 2007 Version 2 10 February 2012 Page 24 of 25
Policies and Procedures: HEFT Framework and Template v2
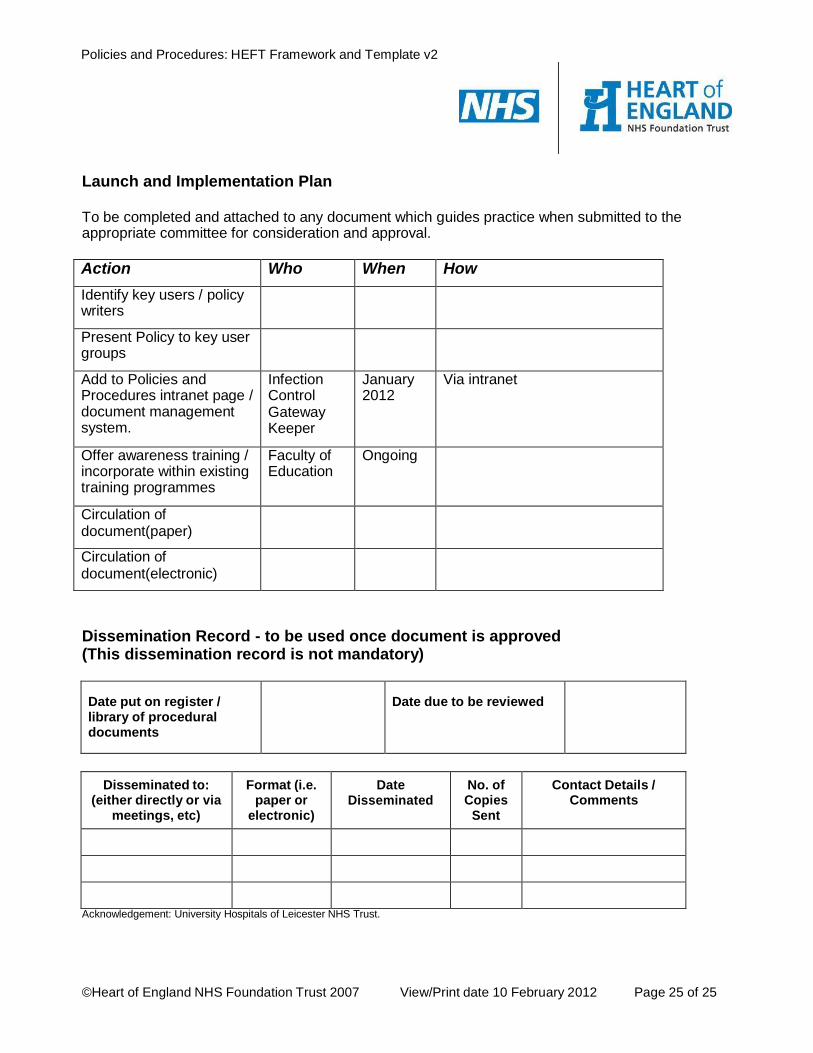
Launch and Implementation Plan
To be completed and attached to any document which guides practice when submitted to the appropriate committee for consideration and approval.
Action Who When How
Identify key users / policy writers
Present Policy to key user groups
Add to Policies and Procedures intranet page / document management system.
Infection Control Gateway Keeper
January 2012
Via intranet
Offer awareness training / incorporate within existing training programmes
Faculty of Education
Ongoing
Circulation of document(paper)
Circulation of document(electronic)
Dissemination Record - to be used once document is approved (This dissemination record is not mandatory)
Date put on register / library of procedural documents
Date due to be reviewed
Disseminated to: (either directly or via
meetings, etc)
Format (i.e. paper or
electronic)
Date Disseminated
No. of Copies
Sent
Contact Details / Comments
Acknowledgement: University Hospitals of Leicester NHS Trust.
©Heart of England NHS Foundation Trust 2007 View/Print date 10 February 2012 Page 25 of 25