Embed Size (px)
Citation preview

GHeredia-2013 │Page 1
Should we PROmote PROMACTA®
for Thrombocytopenia in Patients with Hepatitis C?
Source: http://alpha-1foundation.org/wordpress/wp-content/uploads/2012/03/Retouched-Liver-300x225.jpg
Grecia Heredia, PharmD PGY1-Community Pharmacy Resident 2013-2014
Centro de Salud Familiar La Fe, Inc.-Federally Qualified Health Center UTEP/UT Austin Cooperative Pharmacy Program
November 8, 2013 Objectives:
1. Discuss chronic Hepatitis C disease, complications, and associated health-care costs 2. Apply current treatment guidelines to determine appropriate treatment options for Hepatitis C 3. Describe management considerations in Hepatitis C related thrombocytopenia 4. Evaluate clinical trials to assess the role of platelet activators in thrombocytopenia related to Hepatitis C

GHeredia-2013 │Page 2
Hepatitis C I. Introduction
A. Epidemiology1-4 1. Approximately 3.2-3.9 million people in the United States chronically infected with Hepatitis C
a. About 75% are Baby Boomers (people born between 1945-1965) 2. Increasing health care costs associated with Hepatitis C virus (HCV)
a. Total annual costs in the United States estimated to be $5.46 billion in 1997 b. Predicted to increase to $10.7 billion in 2010-2019 due to advanced disease
B. Etiology2, 3, 5
1. Hepatitis C is a single-stranded RNA virus from the Flaviviridae family 2. Six different genotypes around the world
Table 1. Hepatitis C Genotypes around the World2
Genotype Region 1 Worldwide: especially US, northern Europe 2 Worldwide; especially northern Europe, Japan, India 3 India 4 Middle East, Africa 5 South Africa 6 Hong Kong, Southeast Asia
C. Transmission1-3, 6
1. Transmitted through large or repeated percutaneous exposure to infected blood 2. Most common blood-borne pathogen
a. Injection drug users (most common) b. Blood transfusion or donated organ with infected blood c. Needle sticks (healthcare providers) d. Birth to an HCV infected mother e. Sexually (extremely rare)
II. Pathophysiology7, 8
A. Virus attacks hepatocytes and interferes with body’s ability to clear virus (does not directly damage) B. Activation of CD8 cells and natural killer (NK) cells cause most of the damage
1. CD4 and CD8 lymphocytes and interferon decrease viral replication a. Eradication of virus occurs by the CD8 lymphocytes or interferon inducing apoptosis of
infected hepatocytes C. Extent of liver damage correlates with the extent of hepatocytes that undergo apoptosis D. HCV does not usually cause disease until 10-20 years later
III. Complications7, 9, 10 A. Cirrhosis
1. Portal hypertension (HTN) 2. Esophageal varices 3. Ascites
GHeredia-2013 │Page 3
4. Hepatic encephalopathy 5. Coagulopathies 6. Portal vein thrombosis
B. Liver transplant C. Hepatocellular Carcinoma (HCC)
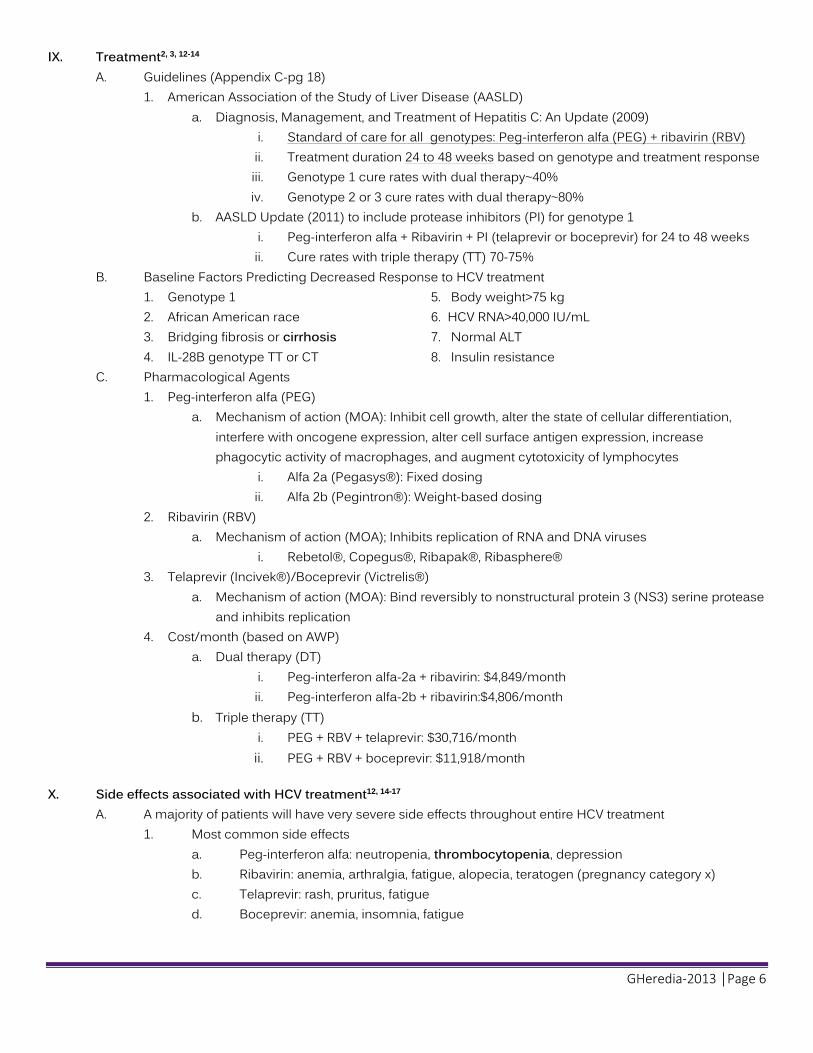
IV. Cost of hepatitis C4 A. Projected costs to increase to $10.7 billion for the 10-year period of 2010-2019
Table 2. Per Patient Per Year All Cause Health Care Costs for Patients with Hepatitis C Virus Overall and by Stage of Liver
Disease in a National and Pharmacy Claims Database: 2002-20104
All HCV HCV Without Liver Disease
HCV with Compensated
Cirrhosis
HCV with Decompensated Cirrhosis
HCV with HCC HCV with Liver
Transplant
Total ($) Mean $19,660 $14,915 $16,911 $41,943 $58,208 $113,282
Median $19,664 $14,916 $16,925 $41,832 $57,959 $113,710 Range $19,072-$20,195 $14,464-$15,686 $15,313-$18,806 $38,670-$44,936 $50,878-$66,116 $101,474-$125,998
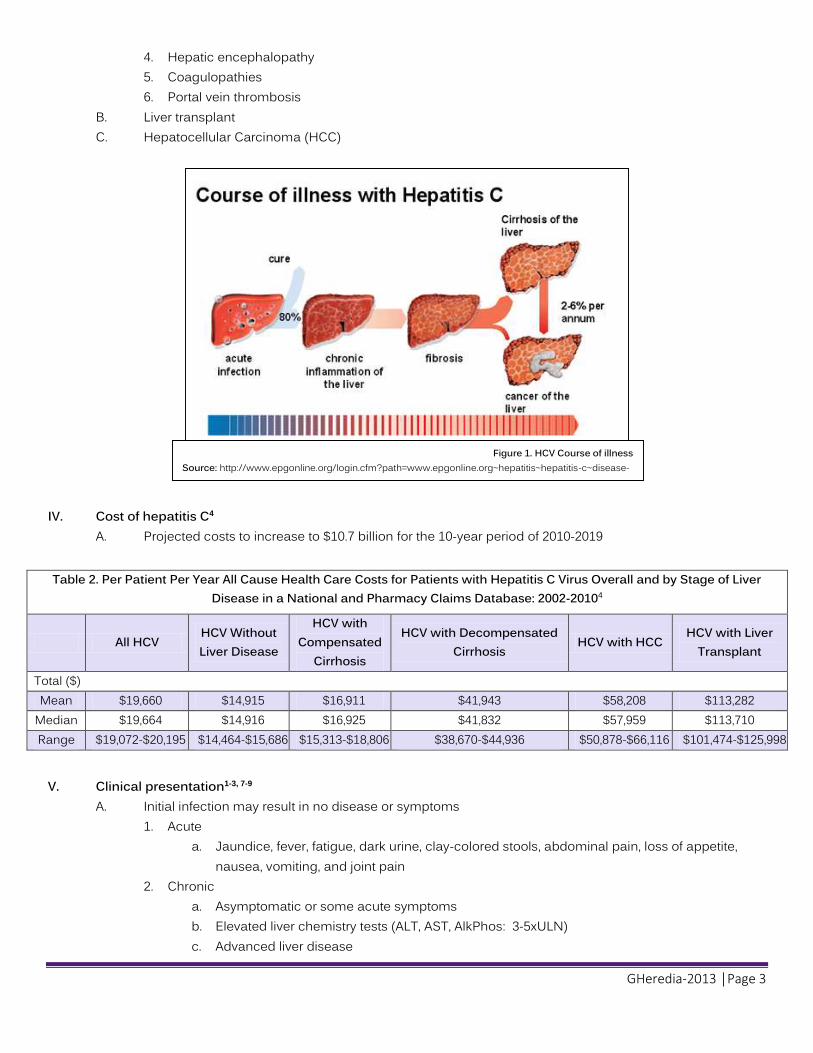
V. Clinical presentation1-3, 7-9 A. Initial infection may result in no disease or symptoms
1. Acute a. Jaundice, fever, fatigue, dark urine, clay-colored stools, abdominal pain, loss of appetite,
nausea, vomiting, and joint pain 2. Chronic
a. Asymptomatic or some acute symptoms b. Elevated liver chemistry tests (ALT, AST, AlkPhos: 3-5xULN) c. Advanced liver disease
Figure 1. HCV Course of illness Source: http://www.epgonline.org/login.cfm?path=www.epgonline.org~hepatitis~hepatitis-c~disease-progression-and-burden-of-hepatitis-c-virus.cfm

GHeredia-2013 │Page 4
VI. Diagnosis2 A. Blood test
1. Anti-HCV antibody a. Appears 4-10 weeks after infection
i. EIA: Enzyme immunoassay ii. CIA: Enhanced chemiluminescence immunoassay
2. Quantitative Hepatitis C virus RNA a. Appears 2-3 weeks after infection
i. By polymerase chain reaction (PCR) ii. How much virus in the blood
Table 3. Diagnosis of Hepatitis C Virus2
Anti-HCV HCV RNA INTERPRETATION
+ + Acute or chronic
+ - Resolution of HCV; Acute: low viremia
- + Early acute HCV infection; chronic if immunocompromised; false positive
- - No infection
VII. Response markers2
A. Major Definitions (most commonly used) (Other definitions in Appendix A and B-pg 17) 1. Rapid virologic response (RVR): HCV RNA negative at treatment week 4 2. Early virologic response (EVR):
a. Partial: ≥2 log reduction in HCV RNA level at week 12 b. Complete: HCV RNA negative at week 12
3. End-of-Treatment response (ETR): HCV RNA negative at end of week 24 or 48 4. Sustained virologic response (SVR): HCV RNA negative 24 weeks after end of treatment
VIII. Treatment candidacy2, 11 A. Liver biopsy to assess damage (gold standard)
1. Not necessary in genotype 2 or 3 2. Invasive procedure to quantify grade (inflammation) and stage (fibrosis) 3. Associated risks include bleeding & perforation of other organs 4. Cost: $1,500 to $2,000
B. Scoring systems 1. METAVIR (most common) 2. Batts-Ludwig 3. International Association for the Study of the Liver (IASL) 4. Ishak Scoring Systems

GHeredia-2013 │Page 5
Table 4. Comparison of Scoring Systems for Histological Stage2
Stage IASL Batts-Ludwig Metavir Ishak 0 No fibrosis No fibrosis No fibrosis No fibrosis
1 Mild fibrosis Fibrous portal
expansion Periportal fibrotic
expansion Fibrous expansion of some portal areas with or without
short fibrous septa
2 Moderate
fibrosis Rare bridges or
septae Periportal septae
Fibrous expansion of most portal areas with or without short fibrous septa
3 Severe fibrosis
Numerous bridges or septae
Porto-central septae
Fibrous expansion of most portal areas with occasional portal to portal bridging
4
Cirrhosis Cirrhosis Cirrhosis
Fibrous expansion of most portal areas with marked bridging (portal to portal and portal to central)
5 Marked bridging (portal to portal and portal to central)
with occasional nodules (incomplete cirrhosis 6 Cirrhosis
C. Non-invasive tests
1. Take into account other lab parameters/tests a. Fibroscan®
i. Transient ultrasound elastography ii. Ultrasound measures liver stiffness
b. Reliable method for diagnosis of fibrosis and cirrhosis 2. Direct biomarkers
a. FibroSure® i. Takes into account age, sex, haptoglobin, α2-macroglobulin, apolipoprotein A1, γ-
glutamyltransferase, and bilirubin analyses ii. Generates a score that is correlated with the degree of liver damage
Table 5. HCV-Treatment Candidacy2
Characteristic Acceptable range
Age Older than 18 yrs
HCV RNA Detectable Liver biopsy (if available)
Chronic hepatitis with bridging fibrosis or greater; moderate fibrosis (Europe)
Disease severity Compensated disease ( bilirubin<1.5 g/dl, INR<1.5, albumin>3.4, platelets>75,000/mm3, no encephalopathy or ascites)
Labs Hgb>13 g/dL for men or >12 g/dL for women, neutrophil count> 1500/mm3, SCr<1.5 mg/dL
GHeredia-2013 │Page 6
IX. Treatment2, 3, 12-14 A. Guidelines (Appendix C-pg 18)
1. American Association of the Study of Liver Disease (AASLD) a. Diagnosis, Management, and Treatment of Hepatitis C: An Update (2009)
i. Standard of care for all genotypes: Peg-interferon alfa (PEG) + ribavirin (RBV) ii. Treatment duration 24 to 48 weeks based on genotype and treatment response iii. Genotype 1 cure rates with dual therapy~40% iv. Genotype 2 or 3 cure rates with dual therapy~80%
b. AASLD Update (2011) to include protease inhibitors (PI) for genotype 1 i. Peg-interferon alfa + Ribavirin + PI (telaprevir or boceprevir) for 24 to 48 weeks ii. Cure rates with triple therapy (TT) 70-75%
B. Baseline Factors Predicting Decreased Response to HCV treatment 1. Genotype 1 5. Body weight>75 kg 2. African American race 6. HCV RNA>40,000 IU/mL 3. Bridging fibrosis or cirrhosis 7. Normal ALT 4. IL-28B genotype TT or CT 8. Insulin resistance
C. Pharmacological Agents 1. Peg-interferon alfa (PEG)
a. Mechanism of action (MOA): Inhibit cell growth, alter the state of cellular differentiation, interfere with oncogene expression, alter cell surface antigen expression, increase phagocytic activity of macrophages, and augment cytotoxicity of lymphocytes
i. Alfa 2a (Pegasys®): Fixed dosing ii. Alfa 2b (Pegintron®): Weight-based dosing
2. Ribavirin (RBV) a. Mechanism of action (MOA); Inhibits replication of RNA and DNA viruses
i. Rebetol®, Copegus®, Ribapak®, Ribasphere® 3. Telaprevir (Incivek®)/Boceprevir (Victrelis®)
a. Mechanism of action (MOA): Bind reversibly to nonstructural protein 3 (NS3) serine protease and inhibits replication
4. Cost/month (based on AWP) a. Dual therapy (DT)
i. Peg-interferon alfa-2a + ribavirin: $4,849/month ii. Peg-interferon alfa-2b + ribavirin:$4,806/month
b. Triple therapy (TT) i. PEG + RBV + telaprevir: $30,716/month ii. PEG + RBV + boceprevir: $11,918/month
X. Side effects associated with HCV treatment12, 14-17 A. A majority of patients will have very severe side effects throughout entire HCV treatment
1. Most common side effects a. Peg-interferon alfa: neutropenia, thrombocytopenia, depression b. Ribavirin: anemia, arthralgia, fatigue, alopecia, teratogen (pregnancy category x) c. Telaprevir: rash, pruritus, fatigue d. Boceprevir: anemia, insomnia, fatigue

GHeredia-2013 │Page 7
B. Side effect management15, 16, 18-20
1. Important to improve patient quality of life (QOL) and continue HCV treatment 2. Common side effects and management (Appendix D-pg 19)
a. Non-pharmacological recommendations i. Adequate hydration ii. Mild to moderate exercise iii. Smaller meals iv. Limit exposure to sunlight
3. Decreased doses of peg-interferon alfa and ribavirin or adjunct agents added 4. Hematologic side effects very common 5. Anemia management
a. Recommended if hemoglobin is below 10 g/dL or 3 g/dL drop in 4 weeks b. Ribavirin dose reduction made in 200 mg increments
i. Minimum effective ribavirin dose is 10.6 mg/kg/day c. Epoeitin alfa (Procrit®) 20,000-40,000 IU weekly subcutaneous injections
i. Discontinued once hemoblobin >12 g/dL ii. Cost/month (based on AWP)
(a) 40,000 units /mL (1 mL): $927.84 x 4 injections/month = $3,711 6. Neutropenia management
a. Filgrastim (Neupogen®) 150-300 mcg weekly subcutaneous injections, 2 days before PEG i. Cost/month (based on AWP)
(a) 300 mcg/mL (1 mL): $329.70 x 4 injections/month = $1,318 b. Recommended if absolute neutrophil count (ANC) falls below 500/mm3
7. Thrombocytopenia management a. Recommended if platelet count falls below 50,000 platelets/mm3 b. Eltrombopag (Promacta®) 25 mg by mouth once daily; titrated based on platelet response
i. Cost/month (based on AWP) (a) 12.5 mg tablets (#30): $3,056.29 (b) 25 mg tablets (#30): $3,056.29 (c) 50 mg tablets (#30): $6,112.57 (d) 75 mg tablets (#30): $9,168.86
Table 6. HCV-Medications Most Common Side Effects12
Hea
dach
e
Fatig
ue
Arth
ralg
ia
Inso
mni
a
Dep
ress
ion
Emot
iona
l lia
bilit
y
Anem
ia
Neu
trope
nia
Thro
mbo
cyto
peni
a
Rash
Dry
Ski
n
Prur
itus
Alop
ecia
Nau
sea
Vom
iting
Anor
exia
PEG 56-70% 52-94% 23-51% 23% 29-59% 28% 12-47% 6-70% 7-20% 6-36% 12% 22-34% 26-64% 11%
RBV 43-66% 60-70% 22-34% 26-41% 20-36% 7-12% 11-17% 8-42% 1-15% 5-28% 10-24% 13-29% 27-36% 25-47% 9-25% 21-32%
TEL 56% 36% 3% 56% 47% 39% 13%
BOC >10% 55-58% 19-23% 30-34% 25-26% 45-50% 14-31% 16-17% 18-22% 22-27% 43-46% 15-20% 25-26%
GHeredia-2013 │Page 8
HCV and Cirrhosis
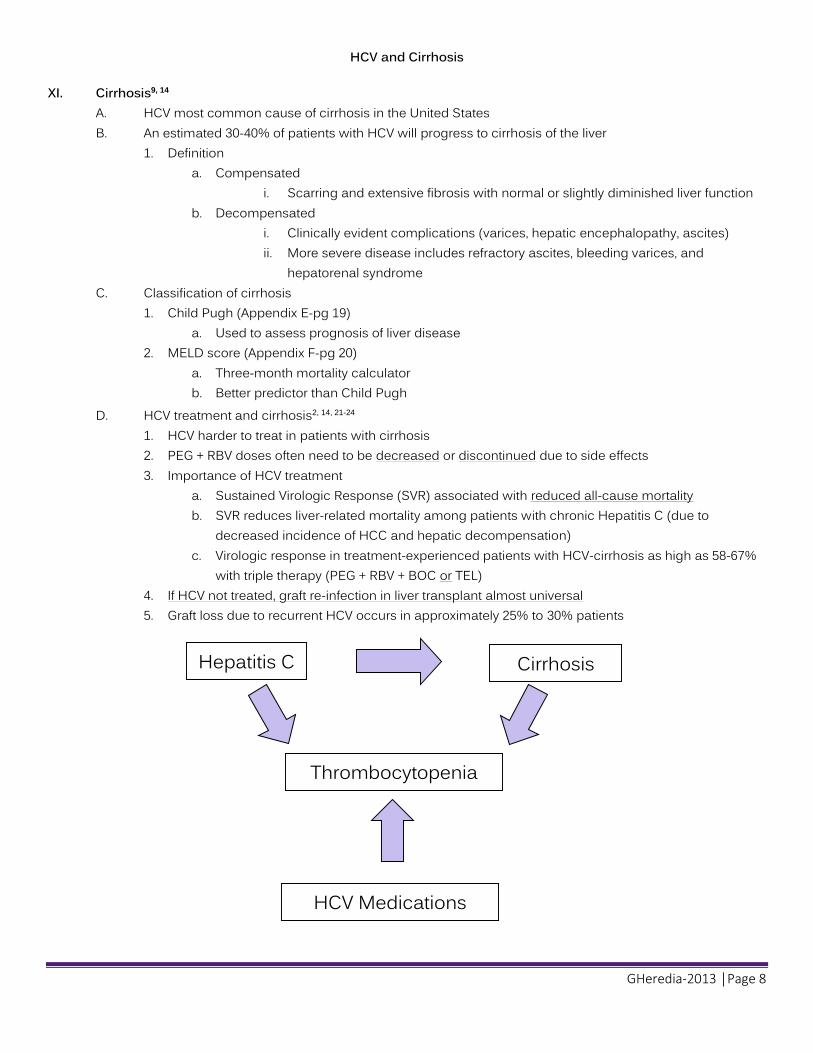
XI. Cirrhosis9, 14 A. HCV most common cause of cirrhosis in the United States B. An estimated 30-40% of patients with HCV will progress to cirrhosis of the liver
1. Definition a. Compensated
i. Scarring and extensive fibrosis with normal or slightly diminished liver function b. Decompensated
i. Clinically evident complications (varices, hepatic encephalopathy, ascites) ii. More severe disease includes refractory ascites, bleeding varices, and
hepatorenal syndrome C. Classification of cirrhosis
1. Child Pugh (Appendix E-pg 19) a. Used to assess prognosis of liver disease
2. MELD score (Appendix F-pg 20) a. Three-month mortality calculator b. Better predictor than Child Pugh
D. HCV treatment and cirrhosis2, 14, 21-24 1. HCV harder to treat in patients with cirrhosis 2. PEG + RBV doses often need to be decreased or discontinued due to side effects 3. Importance of HCV treatment
a. Sustained Virologic Response (SVR) associated with reduced all-cause mortality b. SVR reduces liver-related mortality among patients with chronic Hepatitis C (due to
decreased incidence of HCC and hepatic decompensation) c. Virologic response in treatment-experienced patients with HCV-cirrhosis as high as 58-67%
with triple therapy (PEG + RBV + BOC or TEL) 4. If HCV not treated, graft re-infection in liver transplant almost universal 5. Graft loss due to recurrent HCV occurs in approximately 25% to 30% patients
Thrombocytopenia
Hepatitis C
Cirrhosis
HCV Medications

GHeredia-2013 │Page 9
XII. Thrombocytopenia25-30 A. Associated with liver disease progression and HCV treatment
1. Thrombocytopenia is found in 15-70% of patients with cirrhosis a. Platelet counts correlates with degree of fibrosis
2. More than 24% reported rates of thrombocytopenia in patients with chronic HCV B. Definition
1. Platelet count <150,000 platelets/L a. Moderate: 50,000-75,000 platelets/L b. Severe: <50,000 platelets/L
C. Mechanism of action (MOA): 1. HCV-related (multi-factorial)25-29
a. Due to splenic platelet sequestration and hypersplenism secondary to portal HTN i. Platelets made in liver, but stored in spleen
b. Increased platelet breakdown c. Decreased platelet production
i. Due to decreased thrombopoeitin (TPO) production in liver ii. Serum TPO levels substantially lower in patients with HCV-related cirrhosis
d. Bone marrow suppression e. Immune associated platelet destruction (anti-GPIIb/IIIa antibody)
2. Interferon-related30 a. Inhibition of platelet production but not proliferation in megakaryocytes
D. Complications25 1. Bleeding 2. Need for decreased PEG/RBV doses or HCV treatment discontinuation
E. Management26, 31-33
1. Platelet transfusion indicated for platelet count <10,000 platelets/L 2. Thrombopoeitin (TPO) stimulating agents (eltrombopag recommended for platelet count<50,000/L)
a. Eltrombopag (Promacta®) (Appendix G-pg 20) i. Mechanism of action (MOA): Binds to TPO receptor (without competing with
TPO) and activates intracellular signal transduction pathways along with endogenous TPOleading to the increased proliferation and differentiation of human bone marrow progenitor cells into megakaryocytes and increased platelet production
Table 7. Recommended dose reduction for peg-interferon alfa12
Medication Dose reduction
Peg-interferon alfa 2a Platelet count<50,000/L: 90 mcg weekly Platelet count<25,000/L: Discontinue
Peg-interferon alfa 2b Platelet count 25,000/L to <50,000/L : 1 mcg/kg/week, may further decrease to 0.5 mcg/kg/week Platelet count<25,000/L: Discontinue

GHeredia-2013 │Page 10
F. Eltrombopag (Promacta®) monograph34
Table 8. Eltrombopag (Promacta®) Monograph34
Indication Immune thrombocytopenia (ITP) Chronic hepatitis C-associated thrombocytopenia
Dose Initial 25 mg once daily; dose titrated based on platelet response Maximum dose: 100 mg daily
Contraindications No contraindications
Black Box Warning May cause hepatotoxicity; obtain ALT, AST and bilirubin prior to treatment initiation, every 2 weeks during adjustment phase, then monthly Discontinue treatment for ALT 3 x ULN
Warnings Thromboembolism (venous or arterial) Use with caution in patients with known risk factors for thromboembolism Risk for portal vein thrombosis
Administration On an empty stomach, 1 hour before or 2 hours after a meal Do not take with antacids, calcium or minerals (separate by 4 hours)
Monitoring LFT’s, bilirubin
PK/PD
Onset of action (platelet count increase): within 1-2 weeks Peak: 14-16 days Duration (return to baseline): 1-2 weeks after last dose Protein binding: >99% Bioavailability: ~52% Half-life: ~21-32 hours Excretion: feces
Pregnancy category
C
G. Eltrombopag dose adjustments34
1. Based on platelet response 2. Check CBC with differential weekly until stable platelet count achieved, then monthly thereafter
Table 9. Dose Adjustments of eltrombopag (Promacta®)34
Platelet Count Dose adjustment <50,000/L after 2 weeks of eltrombopag Increase by 25 mg to a max dose of 100 mg/day
≥200,000/L to ≤400,000/L at any time Decrease daily dose by 25 mg Wait 2 weeks to asses effects
>400,000/L Stop eltrombopag Once platelet count <150,000/L, re-start at a daily dose reduced by 25 mg
>400,000/L after 2 weeks of lowest dose Discontinue eltrombopag

GHeredia-2013 │Page 11
XIII. Evaluation of literature A. Trial to assess if eltrombopag increases platelets in patients with HCV (Landmark trial)
McHutchinson JG, Dusheiko G, Shiffman ML, et al. Eltrombopag for thrombocytopenia in patients with cirrhosis associated with hepatitis c. N Engl J Med. 2007; 357(22)22: 2227-36.
Study objective Assess whether the use of eltrombopag can increase platelet counts in patients with thrombocytopenia associated with cirrhosis due to chronic HCV infection
Study design International, multi-center, double blind, placebo controlled, Phase 2 trial
Patient Population
Inclusion criteria Over the age of 18 Chronic HCV Compensated liver disease Thrombocytopenia (platelet count >20,000 to <70,000/mm3) Evidence of cirrhosis (confirmed by liver biopsy, radiographic evidence, or evidence of portal
hypertension)
Exclusion criteria Pregnancy History of
thrombosis HIV co-infected HBV co-infected
Interventions
N=74 Patients Patients randomly assigned to: 30 mg eltrombopag: 50 mg eltrombopag: 75 mg eltrombopag: placebo x 4 weeks
After 4 weeks, HCV treatment started for up to 12 weeks PEG+RBV started if platelet count>70,000 for peg-interferon alfa-2a and >100,000/ mm3 for peg-interferon alfa-2b
Statistics Multiple logistic regression analysis
Outcomes
Primary endpoint: Increase in platelet count from 20,000 to <70,000 platelets/mm3 to 100,000 platelets/mm3 or
more in 4 weeks of eltrombopag
Secondary endpoint: Safety Tolerability
Results
Variable Eltrombopag Placebo 30 mg
n=14 50 mg n=19
75 mg n=23
Placebo n=18
End of initial treatment phase Platelet count (platelets/mm3)
# patients with data 11 16 22 14 Median 125,000 212,000 204,000 53,000 Range 40,000 to 214,000 47,000 to 599,000 78,000 to 527,000 34,000 to 74,000
Change from baseline (platelets/mm3) # patients with data 12 16 22 14 Median 74,000 152,000 151,000 -3,000 Range 6,000 to 155,000 10,000 to 540,000 45,000 to 473,000 -22,000 to 13,000 ≥100,000/mm3 9/12 (75%) 15/19 (79%) 20/21 (95%) 0/17 ≥200,000/mm3 3/12 (25%) 9/19 (47%) 11/21 (52%) 0/17
P<0.001 for overall treatment effect 49 of 74 patients proceeded to antiviral treatment phase: 4/18 receiving placebo, 10/14 receiving 30 mg, 14/19 receiving 50 mg, 21/23 receiving 75 mg
Author’s conclusions
Increases in platelet counts in all active drug treatment arms were significant compared to placebo Primary efficacy endpoint reached in 75-95% of patients receiving eltrombopag in a dose-dependent manner
Reviewer’s conclusions
Eltrombopag effective to initiate HCV treatment Dose dependent effect, however, no added benefit after 50 mg of eltrombopag Strengths: Study population (HCV), compensated and decompensated cirrhosis Limitations: Power not reached

GHeredia-2013 │Page 12
B. Trial to assess safety and efficacy of lower doses of eltrombopag
Kawaguchi T, Komori A, Seike M, et al. Efficacy and safety of eltrombopag in Japanese patients with chronic liver disease and thrombocytopenia:
a randomized, open-label, phase II study. J Gastroenterol . 2012;47:1342-51. Study
objective Assess the efficacy and safety of eltrombopag in Japanese patients with chronic liver disease and thrombocytopenia using lower daily doses (12.5, 25, or 37.5 mg) than those typically used for Caucasian patients
Study design Multicenter, open-label, dose-ranging phase II study Two part study
Patient Population
Inclusion criteria: 20 years of age or older Thrombocytopenia (baseline platelet<50,000/uL) Child-Pugh score of 9 or less Hemoglobin>8 g/dL for at least 4 weeks before enrollment
Exclusion criteria: HIV infection Evidence of portal vein thrombosis History of arterial or venous thrombosis with 2 or more
thrombosis risk factors Platelet agglutination abnormalities World Health Organization (WHO) grade 3 or 4
bleeding Pregnant or breastfeeding women Patients who require use of polyvalent cation-
containing medicines Patients taking anti-platelet agents Patients taking HMG-CoA reductase inhibitors
Interventions First part: 12 subjects received 12.5 mg of eltrombopag once daily x 2
weeks
Second part: 26 new subjects randomly assigned 1:1 to 25 mg or
37.5 mg of eltrombopag once daily for 2 weeks
Statistics Point estimates and 2-sided 95% confidence intervals Changes from baseline using ANCOVA
Outcomes
Primary endpoint: Change from baseline platelet counts at end of week 2
Secondary endpoint: Response rate (achieving platelets >80,000/µL) Median platelet counts Safety
Results
Variable Eltrombopag 12.5 mg
n=12 25 mg n=14
37.5 mg n=12
Mean platelet increases from baseline at end of week 2 (platelets/L) 24,800
(95% CI-8,200-41,400) 54,000
(95% CI-28,200-79,800) 60,000
(95% CI-29,300-90,700) Response rate to platelet counts >80,000/µL at week 2
3 (25%) 6 (42.9%) 7 (58.3%) Drug-related AE’s
1/12 (8%) 4/14 (29%) 4/12 (33%)
Author’s conclusions
Significant increases in platelet counts can be achieved by 2 week administration of eltrombopag to Japanese patients with chronic liver disease and thrombocytopenia
Daily dose of 25 mg for 2 weeks recommended
Reviewer’s conclusions
Lower doses of eltrombopag effective in Japanese patients Strengths :Analysis included all patients who had received at least one dose of eltrombopag Limitations: Might not be able to extrapolate data to rest of the world, compensated cirrhosis

GHeredia-2013 │Page 13
C. Trial to assess safety and efficacy of eltrombopag with PEG + RBV (Landmark trials)
Afdhal NH. Dusheiko GM, Giannini EG, et al. Eltrombopag Increases Platelet Numbers in Thrombocytopenic Patients with HCV Infection and Cirrhosis,
Allowing for Effective Antiviral Therapy. Gastroenterology (2013), doi: 10.1053/j.gastro.2013.10.012
Study objective
Assess the ability of supportive eltrombopag therapy to increase platelets to levels sufficient to initiate and maintain PEG+RBV antiviral therapy
Study design
Two part study: Open-label eltrombopag & double-blind, multi-center, placebo-controlled trial (antiviral phase) ENABLE-1 (PEG alfa-2a)+RBV ENABLE-2 (PEG alfa-2b)+RBV
Patient Population
Inclusion Criteria: ≥18 years Confirmed HCV infection Baseline platelets<75,000/µL Adequate hepatic, renal and hematologic function
to receive antiviral therapy
Exclusion criteria: Non-responders to previous PEG+RBV Decompensated liver disease Serious cardiac, cerebrovascular or pulmonary disease History of thromboembolic events Hepatitis B virus HIV Active bleeding or need for anticoagulation History of clinically significant bleeding from esophageal or
gastric varices
Interventions
Two part study: Open-label eltrombopag (25 mg. 50 mg, 75 mg, or 100 mg) for 2-9 weeks Antiviral phase: Subjects who reached pre-determined platelet threshold were randomized 2:1 to eltrombopag + HCV
treatment or placebo + HCV treatment (treatment duration 24-48 weeks according to HCV genotype)
Statistics Stratified Cochran-Mantel-Haenszel chi square, adjusted for stratification
Outcomes
Primary endpoints: SVR Secondary endpoints: Platelets counts PEG and/or RBV dose reduction
or discontinuation RVR, EVR, cEVR, ETR
Safety: AE’s Treatment emergent AE’s
Results
Efficacy: ENABLE-1 n=681 (n=449 vs n=232 placebo) ENABLE-2 n=758 (n=506 vs. n=252 placebo) SVR rates: ENABLE-1: 23% vs. 14%, P=0.0064 ENABLE-2: 19% vs 13%, P=0.0202
Safety: Thromboembolic events 34 TEE in eltrombopag vs. 5 TEE in placebo: Portal vein thrombosis n=12 eltrombopag vs. n=2 placebo Hepatic decompensation: Eltrombopag 10% vs. 5% placebo
Author’s conclusion
Eltrombopag can be used safely in subjects with HCV related liver disease and thrombocytopenia to allow initiation and maintenance of HCV treatment
Reviewer’s conclusions
Eltrombopag effective to initiate and maintain HCV treatment Monitor patients closely for hepatic decompensation, hepatotoxicity, and thromboembolic events Strengths: Large trial, efficacy analyzed using intent-to-treat (ITT), power reached Limitations: No standard guideline to decrease PEG or RBV doses based on hematologic toxicity, compensated only

GHeredia-2013 │Page 14
XIV. Safety of eltrombopag (Promacta®)34 A. Adverse reactions
Table 10. Eltrombopag Adverse Reactions (>10%) from ENABLE-1 and ENABLE-2 Clinical Trials34
Adverse Reaction Eltrombopag + PEG + RBV
n=955 %
Placebo + PEG + RBV n=484
% Anemia 40 35 Pyrexia 30 24 Fatigue 28 23 Headache 21 20 Nausea 19 14 Diarrhea 19 11 Decreased appetite 18 14 Flu-like symptoms 18 16 Asthenia 18 13 Insomnia 16 15 Cough 16 12 Pruritus 15 13 Chills 14 9 Myalgia 12 10 Alopecia 10 6 Peripheral edema 10 5
B. Increased risk of portal vein thrombosis and other thromboembolic events33, 34
1. ENABLE-1 and ENABLE-2 clinical trials a. 31/955 (3%) in eltrombopag vs. 5/484 (1%) in placebo arm (majority were portal vein) b. Thromboembolic events observed at low and high platelet counts
2. Systematic review and meta-analysis of risk of thromboembolism (Appendix G)35 a. Thromboembolism risk increased in patients on TPOr agonists (not statistically significant) b. Overall number needed to harm 1/55 patients
C. Hepatic decompensation in patients with HCV in ENABLE-1 and ENABLE-2 clinical trials33, 34 1. Ascites and encephalopathy in 10% eltrombopag vs. 5% placebo
D. Hepatotoxicity (black box warning)12, 33, 34 1. ENABLE-1 and ENABLE-2 clinical trials
a. ALT and AST 3 x ULN reported in 34% eltrombopag vs. 38% placebo b. Total bilirubin >1.5 x ULN reported in 76% eltrombopag vs. 50% placebo
Should we PROmote PROMACTA® for Thrombocytopenia in Patients with Hepatitis C?

GHeredia-2013 │Page 15
XV. Conclusion A. Role in increasing platelet levels to initiate HCV treatment (should not be used to normalize platelets) B. Adjunct treatment can help avoid dose reductions/discontinuation of HCV treatment C. Safety
1. Thromboembolism risk a. Portal vein thrombosis already a complication with cirrhosis (20-25%) b. Careful monitoring for thromboembolic events c. Risk vs. benefit in patients with known risk factors for thromboembolism
(e.g., anti-phospholipid syndrome, Factor V Leiden) d. Eltrombopag (Promacta®) dose titration based on platelet response
2. Hepatic decompensation risk a. Rates of hepatic decompensation similar to placebo arm in ENABLE-1 and ENABLE-2 b. Increased risk in patients with albumin <3.5 g/dl and baseline MELD≥10
3. Hepatotoxicity a. Similar rates in eltrombopag treatment arm vs. placebo b. Monitor ALT, AST, and bilirubin before starting and every 2 weeks during dose adjustment c. Monitor monthly after stable dose established
D. Cost: Patient assistance program available36 E. Ongoing study: Promacta® to MAINTAIN triple therapy (BOC + RBV + PEG)-SQUELCH-C
XVI. Wave of the future37-39 A. New HCV medications in the pipeline
1. Interferon-free treatment with less hematological side effects (e.g., thrombocytopenia) a. Sofosbuvir-FDA advisory board voted to approve for genotype 2 and 3 in combination with
RBV and genotype 1 and 4 in combination with RBV and PEG i. Likely approved by December 2013 ii. NOT approved yet without peg-interferon for genotype 1 and 4
b. Simeprevir-FDA advisory board also voted to approve for genotype 1-4 with RBV and PEG c. Simeprevir + Sofosbuvir + RBV (COSMOS trial) - up to 90% SVR in patients with genotype 1
B. Thrombocytopenia STILL a complication of HCV and cirrhosis
Hepatitis C Cirrhosis
Thrombocytopenia
HCV Medications

GHeredia-2013 │Page 16
Resources: 1. Centers for Disease Control and Prevention. Hepatitis C information for healthcare providers. http://www.cdc.gov/hepatitis/HCV/HCVfaq.htm. Accessed 08/16, 2013. 2. Ghany MG, Strader DB, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C: An update. Hepatology. 2009;49(4):1335-1374. doi: 10.1002/hep.22759. 3. Ghany MG, Nelson DR, Strader DB, Thomas DL, Seeff LB. An update on treatment of genotype 1 chronic hepatitis C virus infection: 2011 practice guideline by the american
association for the study of liver diseases. Hepatology. 2011;54(4):1433-1444. doi: 10.1002/hep.24641. 4. McAdam-Marx C, McGarry LJ, Hane CA, Biskupiak J, Deniz B, Brixner DI. All-cause and incremental per patient per year cost associated with chronic hepatitis C virus and
associated liver complications in the united states: A managed care perspective. J Manag Care Pharm. 2011;17(7):531-546. 5. Strauss J, Straus E. Chapter 3-plus stranded RNA viruses. In: ; 2008:106. 6. Moyer VA. Screening for hepatitis C virus infection in adults: U.S. preventive services task force recommendation statement. Ann Intern Med. 2013. 7. Wells B, Dipiro J, Schwinghammer T, et al. Pharmacotherapy Handbook. 8th Edition ed. McGraw Hill; 2012. 8. Texas Department of State Health Services. Don't get stuck with hepatitis C. www.dshs.state.tx.us/idcu/disease/hepatitis/hepatitis_c/. Accessed 07/25, 2013. 9. Maasoumy B, Wedemeyer H. Natural history of acute and chronic hepatitis C. Best Pract Res Clin Gastroenterol. 2012;26(4):401-412. doi: 10.1016/j.bpg.2012.09.009. 10. Tsochatzis EA, Senzolo M, Germani G, Gatt A, Burroughs AK. Systematic review: Portal vein thrombosis in cirrhosis. Aliment Pharmacol Ther. 2010;31(3):366-374. doi:
10.1111/j.1365-2036.2009.04182.x. 11. Baranova A, Lal P, Birerdinc A, Younossi ZM. Non-invasive markers for hepatic fibrosis. BMC Gastroenterol. 2011;11:91-91. doi: 10.1186/1471-230X-11-91. 12. Lexi-Comp Online, Lexi-Drugs. Hudson, Ohio; Lexi-Comp, Inc. july 22, 2013. 13. Cooper C, Lester R, Thorlund K, et al. Direct-acting antiviral therapies for hepatitis C genotype 1 infection: A multiple treatment comparison meta-analysis. QJM.
2013;106(2):153-163. doi: 10.1093/qjmed/hcs214. 14. Yee HS, Chang MF, Pocha C, et al. Update on the management and treatment of hepatitis C virus infection: Recommendations from the department of veterans affairs
hepatitis C resource center program and the national hepatitis C program office. Am J Gastroenterol. 2012;107(5):669-689. doi: 10.1038/ajg.2012.48. 15. Gaetano JN, Reau N. Hepatitis C: Management of side effects in the era of direct-acting antivirals. Curr Gastroenterol Rep. 2013;15(1):305-305.doi: 10.1007/s11894-012-0305-1. 16. Kelleher TB, Afdhal NH. Management of the Side Effects of Peginterferon and Ribavirin being used for Treatment of Chronic Hepatitis C Virus Infection. in: UpToDate.
Waltham, MA: UpToDate; 2013. 17. Minami T, Kishikawa T, Sato M, Tateishi R, Yoshida H, Koike K. Meta-analysis: Mortality and serious adverse events of peginterferon plus ribavirin therapy for chronic hepatitis
C. J Gastroenterol. 2013;48(2):254-268. doi: 10.1007/s00535-012-0631-y. 18. Romero-Gómez M, Berenguer M, Molina E, Calleja JL. Management of anemia induced by triple therapy in patients with chronic hepatitis C: Challenges, opportunities and
recommendations. J Hepatol. 2013. 19. Sulkowski MS, Poordad F, Manns MP, et al. Anemia during treatment with peginterferon alfa-2b/ribavirin and boceprevir: Analysis from the serine protease inhibitor therapy 2
(SPRINT-2) trial. Hepatology. 2013;57(3):974-984. doi: 10.1002/hep.26096. 20. Talal AH, Liu R, Zeremski M, et al. Randomized trial comparing dose reduction and growth factor supplementation for management of hematological side effects in
HIV/hepatitis C virus patients receiving pegylated-interferon and ribavirin. J Acquir Immune Defic Syndr. 2011;58(3):261-268. 21. Hézode C, Fontaine H, Dorival C, et al. Triple therapy in treatment-experienced patients with HCV-cirrhosis in a multicentre cohort of the french early access programme
(ANRS CO20-CUPIC) - NCT01514890. J Hepatol. 2013;59(3):434-441. doi: 10.1016/j.jhep.2013.04.035. 22. Backus LI, Boothroyd DB, Phillips BR, Belperio P, Halloran J, Mole LA. A sustained virologic response reduces risk of all-cause mortality in patients with hepatitis C. Clin
Gastroenterol Hepatol. 2011;9(6):509-516.e1. doi: 10.1016/j.cgh.2011.03.004. 23. Iacobellis A, Siciliano M, Annicchiarico BE, et al. Sustained virological responses following standard anti-viral therapy in decompensated HCV-infected cirrhotic patients.
Aliment Pharmacol Ther. 2009;30(2):146-153. doi: 10.1111/j.1365-2036.2009.04025.x. 24. Ng V, Saab S. Effects of a sustained virologic response on outcomes of patients with chronic hepatitis C. Clin Gastroenterol Hepatol. 2011;9(11):923-930. doi:
10.1016/j.cgh.2011.05.028. 25. Afdhal N, McHutchison J, Brown R, et al. Thrombocytopenia associated with chronic liver disease. J Hepatol. 2008;48(6):1000-1007. doi: 10.1016/j.jhep.2008.03.009. 26. Dusheiko G. Thrombopoietin agonists for the treatment of thrombocytopenia in liver disease and hepatitis C. Clin Liver Dis. 2009;13(3):487-501. doi: 10.1016/j.cld.2009.05.012. 27. Lin K, Hsu P, Yu H, et al. Factors linked to severe thrombocytopenia during antiviral therapy in patients with chronic hepatitis c and pretreatment low platelet counts. BMC
Gastroenterol. 2012;12:7-7. doi: 10.1186/1471-230X-12-7. 28. Louie KS, Micallef JM, Pimenta JM, Forssen UM. Prevalence of thrombocytopenia among patients with chronic hepatitis C: A systematic review. J Viral Hepat. 2011;18(1):1-7.
doi: 10.1111/j.1365-2893.2010.01366.x. 29. Weksler BB. Review article: The pathophysiology of thrombocytopenia in hepatitis C virus infection and chronic liver disease. Aliment Pharmacol Ther. 2007;26 Suppl 1:13-19. 30. Yamane A, Nakamura T, Suzuki H, et al. Interferon-alpha 2b-induced thrombocytopenia is caused by inhibition of platelet production but not proliferation and endomitosis in
human megakaryocytes. Blood. 2008;112(3):542-550. doi: 10.1182/blood-2007-12-125906. 31. McHutchison JG, Dusheiko G, Shiffman ML, et al.Eltrombopag for thrombocytopenia in patients with cirrhosis associated with hepatitis C.N Engl J Med. 2007;357(22):2227-36. 32. Slichter SJ. Evidence-based platelet transfusion guidelines. Hematology Am Soc Hematol Educ Program. 2007:172-178. 33. Afdhal NH, Dusheiko GM, Giannini EG, et al. Eltrombopag increases platelet numbers in thrombocytopenic patients with HCV infection and cirrhosis, allowing for effective
antiviral therapy. Gastroenterology. 2013. 34. Promacta Prescribing Information. Research Triangle Park, NC: GlaxoSmithKline; 2012. 35. Catalá-López F, Corrales I, Martín-Serrano G, Tobías A, Calvo G. Risk of thromboembolism with thrombopoietin receptor agonists in adult patients with thrombocytopenia:
Systematic review and meta-analysis of randomized controlled trials. Med Clin (Barc). 2012;139(10):421-429. doi: 10.1016/j.medcli.2011.11.023. 36. GlaxoSmithKline. Promacta patient assistance. http://www.needymeds.org/drug_list.taf?_function=name&name=Promacta&gname=eltrombopag. Accessed October 30,
2013. 37. Janssen. FDA advisory committee recommends approval of simeprevir for combination treatment of genotype 1 chronic hepatitis C in adult patients.
http://www.refworks.com/refworks2/?r=references|MainLayout::init#Zt-pE9eyM9nh_OQxMP44|start. Accessed October 30, 2013. 38. Gilead. FDA advisory committee supports approval of gilead’s sofosbuvir for chronic hepatitis C infection. http://www.gilead.com/news/press-releases/2013/10/fda-advisory-
committee-supports-approval-of-gileads-sofosbuvir-for-chronic-hepatitis-c-infection. Accessed October 30, 2013. 39. Medivir. Medivir announces interim results from cohort 2 of the COSMOS study evaluating simeprevir and sofosbuvir in HCV patients with METAVIR scores F3-F4.
http://globenewswire.com/news-release/2013/08/28/569633/0/en/Medivir-announces-interim-results-from-Cohort-2-of-the-COSMOS-study-evaluating-Simeprevir-and-Sofosbuvir-in-HCV-patients-with-METAVIR-scores-F3-F4.html. Accessed October 30, 2013

GHeredia-2013 │Page 17
Acknowledgements Content Reviewer: Jenny Ngo, PharmD Style Reviewer: Jacquelyn Navarrete, PharmD Preceptor: Jeri Sias, PharmD, MPH Margie Padilla, PharmD, CDE Jackson Kelly, PharmD Jessica Gomez, PharmD Ogechika Alozie, MD, MPH
Appendices Appendix A Other Definitions2,3
1. Breakthrough: Re-appearance of HCV in serum while still on therapy 2. Relapse: Reappearance of HCV RNA in serum after therapy discontinued 3. Non-responder: Failure to clear HCV RNA from serum after 24 weeks of therapy 4. Null-responder: Failure to decrease HCV RNA by <2 log after 24 weeks of therapy 5. Partial responder: 2 log decrease in HCV RNA but still positive at week 24
Appendix B
Source: http://d2j7fjepcxuj0a.cloudfront.net/wp-content/uploads/2012/09/HepCUpdate_fig1.jpg
Virologic Response

GHeredia-2013 │Page 18
Appendix C Table 1. American Association of the Study of Liver Disease Guidelines for Hepatitis C2
Recommendations Evidence Level
HCV Genotype 1 and 4 For genotype 1 and 4, treatment should be 48 weeks 1A Peginterferon alfa-2a 180 mcg subcutaneously per week with ribavirin 1000 mg for patients ≤75 kg and 1200 mg for >75 kg 1A Peginterferon alfa-2b 1.5 mcg/kg subcutaneously per week with ribavirin 800 mg if <65 kg, 1000 mg for >65 to 85 kg, 1200 mg for >85 kg to 105 kg, and 1400 for >105 kg
1A
Treatment may be discontinued in patients who do not achieve an early virological response (EVR; ≥2 log reduction in HCV RNA at week 12 of treatment
1A
Patient who do not achieve a complete EVR (undetectable HCV RNA at week 12 of treatment should be re-tested at week 24, and if HCV RNA remains positive, treatment should be discontinued
1A
For patients with genotype 1 infection who have delayed virus clearance (HCV RNA test becomes negative between weeks 12 and 24), consideration should be given to extending therapy to 72 weeks
2B
HCV Genotype 2 or 3 Treatment with peginterferon plus ribavirin should be administered for 24 weeks, using a ribavirin dose of 800 mg 1A Patients whose treatment continues through 24 weeks and whose measurement of HCV RNA with a highly sensitive assay is negative should be re-testes for HCV RNA 24 weeks later to evaluate for an SVR
1A
Patients with HCV-related cirrhosis who achieve an SVR, regardless of the genotype, should continue to be monitored at 6 to 12 month intervals for the development of HCC
2C
HIV Co-infection Initial treatment of hepatitis C in most HIV-infected patients should be peg-interferon alfa plus ribavirin for 48 weeks at doses recommended for HCV mono-infected patients
1A
Patient with Cirrhosis Patients with HCV-related compensated cirrhosis can be treated with the standard regimen of pegylated interferon and ribavirin but will require close monitoring for adverse events
1A
Interferon-based therapy may be initiated at a lower dose in patients with decompensated cirrhosis as long as treatment is administered by experienced clinicians with vigilant monitoring for adverse events preferably in patients who have already been accepted as candidates for liver transplantation
2B
Growth factors can be used for treatment-associated anemia and leukopenia to improve quality of life and may limit the need for antiviral dose reductions in patients with decompensated cirrhosis
2C
Liver transplant patients Treatment of HCV-related disease following liver transplantation should be initiated in appropriate candidates after demonstration of recurrent histologic disease
2A
Table 2. American Association of the Study of Liver Disease Guidelines for Genotype 13
Recommendations Evidence Level
Use BOC or TEL in combination with PEG+RBV 1A BOC and TEL should not be used without PEG+RBV 1A For treatment naïve patients: BOC 800 mg with food TID with PEG+RBV for 24-44 weeks, preceded by 4 weeks of lead in treatment with PEG+RBV
1A
Patients without Cirrhosis: treated with BOC+PEG+RBV, whose HCV RNA levels at week 8 and 24 are undetectable, may consider shortened therapy: 28 weeks total
2B
Triple therapy should be stopped if HCV RNA level is >100 IU/ml at treatment week 12 or detectable at week 24 2B TEL 750 mg with food (not low fat) TID+PEG+RBV for 12 weeks, followed by additional 12-36 weeks of PEG+RBV 1A Patient without Cirrhosis: treated with TEL+PEG+RBV whose HCV RNA at weeks 4 and 12 undetectable should be considered for shortened therapy of 24 weeks
2A
Patients with Cirrhosis: 48 weeks triple therapy 2B Triple therapy should be stopped if HCV RNA level is >1,000 IU/ml at treatment week 4 and 12 and/or detectable at week 24 2B Abbreviations: BOC=Boceprevir, TEL=Telaprevir, PEG=Peg-interferon alfa, RBV=Weight-based Ribavirin, HCV=Hepatitis C virus

GHeredia-2013 │Page 19
Appendix D HCV Treatment Side Effect Management15-20
Side Effect Management
Anemia
RBV dose reduction(by 200 mg up to 600 mg daily, minimum effective dose 10.6 mg/kg/day) Peg-interferon Alfa-2b dose reduction: by 50% Or EPO 40,000 units every week
Neutropenia
Peg-interferon alfa-2a: ANC<750/mm3: 135 mcg weekly ANC<500/mm3: Suspend therapy until >1000/mm3, then restart at 90 mcg weekly
Peg-interferon alfa-2b: 1 mcg/kg/week, may further decrease to 0.5 mcg/kg/week
Neupogen® 150-300 mcg once weekly to 3/times a week Inject 2 days before interferon injection
Thrombocytopenia Peg-interferon Alfa-2a: Platelet count<50,000/mm3: 90 mcg weekly Platelet count<25,000/mm3: Discontinue
Peg-interferon Alfa-2b: 1 mcg/kg/week, may further decrease to 0.5 mcg/kg/week
Depression
Peg-interferon Alfa-2a: Mild depression: No adjustment necessary Moderate depression: 135 mcg once weekly Severe depression: DC interferon
Peg-interferon Alfa-2b: Mild depression: No adjustment necessary Moderate depression: 1 mcg/kg/week, may further reduce to 0.5 mcg/kg/week if necessary SSRI’s: escitalopram, citalopram, paroxetine, fluoxetine Other anti-depressants: Bupropion
Flu-like Symptoms Scheduled APAP or Ibuprofen after PEG injection Adequate fluid intake
Rash Over the counter Emollients/moisturizers Low potency topical corticosteroids Limit exposure to sunlight-wear sunscreen
Anorectal discomfort/pruritus
Over the counter topical corticosteroid + lidocaine Hydrocortisone suppositories Sitz baths Zinc Oxide cream
Nausea/Vomiting
Prescription anti-emetics: -Metoclopramide (PO, IV: 10-40 mg q4-6 hours as needed) -Ondansetron (PO, IV: 4-8 mg as needed) -Promethazine(PO,IM,IV: 12.5-25 mg q4-6 hours as needed) Smaller meals
Appendix E
Source: http://depts.washington.edu/hepstudy/images/mgmt/ascites_Rx-d01.png
Child-Pugh Score

GHeredia-2013 │Page 20
Appendix F Appendix G
Source: http://img.medscape.com/article/706/262/706262-fig1.jpg
Source: http://www.livercancergenomics.com/wp-content/uploads/2011/02/meld.jpg
Appendix H Meta-analysis and Systematic review: Thromboembolism in TPOr agonists controlled trials35
Study TPOr Agonist group Control group RR ARR NNH
# outcomes/total # of patients % # outcomes/total # of patients %
Bussel et al. 2006 0/17 0 1/4 25 0.1
(0-1.9) -25 -4
Kutel et al. 2008; Gernsheimer et al.2010
2/83 2.4 1/42 2.4 1
(0.1-10.8) 0 -
Kuter et al.2010 6/154 3.9 2/75 2.7 1.5
(0.3-7.1) 1.2 83
Manufacturer registry 5/134 3.7 1/46 2.2 1.7
(0.2-14.3) 1.6 63
Bussel et al.2007 1/88 1.1 0/29 0 1
(0.04-14.2) 1.1 91
Cheng et al. 2011, manufacturer registry
3/135 2.2 0/62 0 3.2
(0.2-61.8) 2.2 45
Manufacturer registry 1/15 6.7 0/8 0 1.7
(0.1-37.3) 6.7 15
Manufacturer registry; EPAR
6/143 4.2 2/145 1.4 3
(0.6-14.8) 2.8 36
Abbreviations: RR=relative risk, ARR=Absolute risk reduction, NNH=Number needed to harm
Eltrombopag
Eltrombopag MOA MELD Score