Embed Size (px)
Citation preview
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
SHOULDER COMPLEX ANATOMY
Osseous Elements
The shoulder complex includes the articulations of the humerus, the clavicle, the scapula,
and the posterior surface of the ribs. The humerus is a long bone that forms the articulations of the
glenohumeral joint proximally (with the scapula), and the humeral ulnar joint and humeral radial joint
distally (with the ulna and radius respectively). The head of the humerus is semi-circular in shape
and is directed cephalically, medially, and slightly posteriorly, and is covered with smooth hyaline
cartilage. The head articulates with the glenoid cavity of the scapula, a fossa that is much smaller
than the diameter of the humeral head. The planar orientation of the head of the humerus and the
glenoid fossa, a ball-and-socket relationship, allows for substantial range of motion for the shoulder
specifically when compared to the ball-and-socket coxafemoral joint. The glenoid cavity is further
deepened by the contributions of the labrum, which is a fibrocartilaginous structure that consists of a
confluence of ligaments and capsular attachments (1).
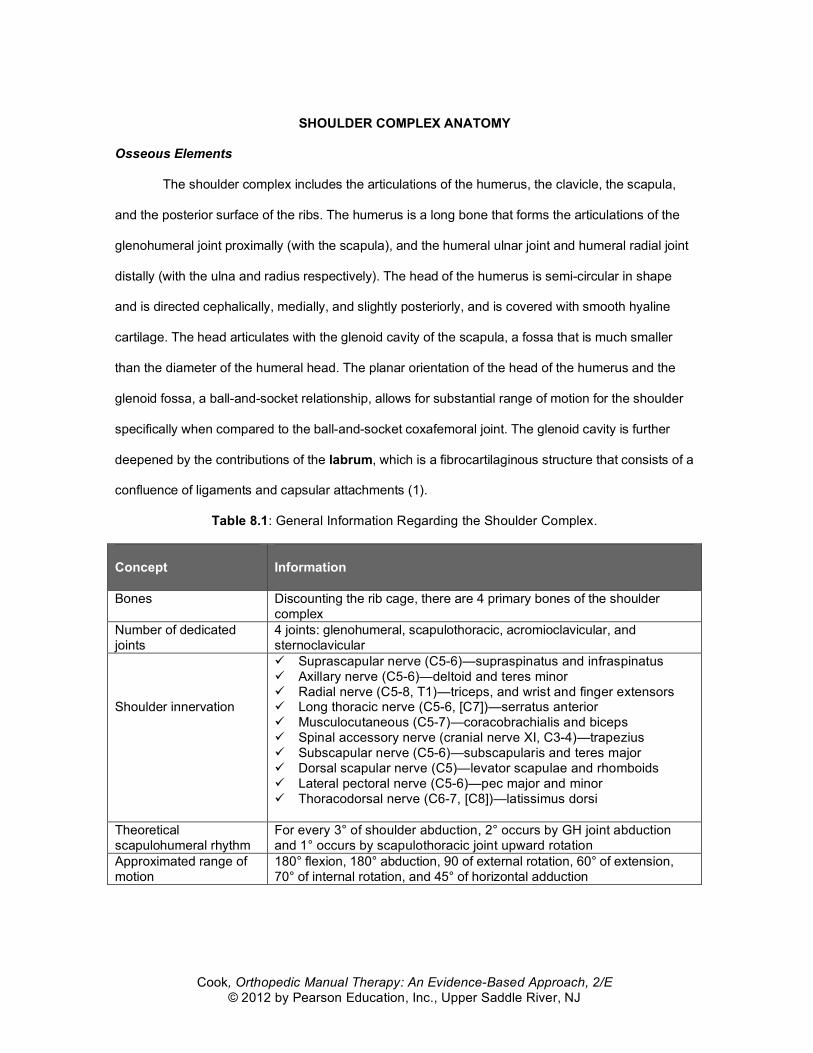
Table 8.1: General Information Regarding the Shoulder Complex. Concept
Information
Bones Discounting the rib cage, there are 4 primary bones of the shoulder complex
Number of dedicated joints
4 joints: glenohumeral, scapulothoracic, acromioclavicular, and sternoclavicular
Shoulder innervation
Suprascapular nerve (C5-6)—supraspinatus and infraspinatus Axillary nerve (C5-6)—deltoid and teres minor Radial nerve (C5-8, T1)—triceps, and wrist and finger extensors Long thoracic nerve (C5-6, [C7])—serratus anterior Musculocutaneous (C5-7)—coracobrachialis and biceps Spinal accessory nerve (cranial nerve XI, C3-4)—trapezius Subscapular nerve (C5-6)—subscapularis and teres major Dorsal scapular nerve (C5)—levator scapulae and rhomboids Lateral pectoral nerve (C5-6)—pec major and minor Thoracodorsal nerve (C6-7, [C8])—latissimus dorsi
Theoretical scapulohumeral rhythm
For every 3° of shoulder abduction, 2° occurs by GH joint abduction and 1° occurs by scapulothoracic joint upward rotation
Approximated range of motion
180° flexion, 180° abduction, 90 of external rotation, 60° of extension, 70° of internal rotation, and 45° of horizontal adduction

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
The anatomical neck of the humerus lies distal to the articulating head of the humerus. The
anatomical neck is obliquely directed and is represented by a narrow groove separating the head of
the humerus from the lesser and greater tubercles. The anatomical neck is the attachment site of the
articular capsule of the glenohumeral joint and the corresponding glenohumeral ligaments.
Two prominent features of the humerus are the greater and lesser tubercles. The greater
tubercle is positioned lateral to the head of the humerus and lesser tubercle. The greater tubercle
provides a site of insertion to the supraspinatus, infraspinatus, and the teres minor. The lesser
tubercle provides the insertion of the tendon of the subscapularis and lies medially and inferior to the
head of the humerus. The greater and lesser tubercles are separated by the bicipital groove, in
which the long head of the biceps brachii lies (2). The pectoral ridge extends from the greater
tubercle along the medial edge of the bone and is the insertion site of the pectoralis major. The
deltoid ridge extends from the greater tubercle along the lateral edge of the humerus and is the
broad insertion site for the deltoid muscle group. Caudal to the greater and lesser tubercle is the
surgical neck of the humerus. The surgical neck is narrower than the proximal humerus and is a
common site of fractures.
The clavicle contributes to the anterior and superior aspect of the glenohumeral articulation.
The clavicle lies horizontally on the anterior aspect of the chest wall and articulates medially with the
manubrium sterni and laterally with the acromion of the scapula. The clavicle has been compared to
a “crank” because it contains a double curve (3). Several muscles, including the deltoid, the
trapezius, and the pectoralis major have important attachments to the clavicle (3).
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
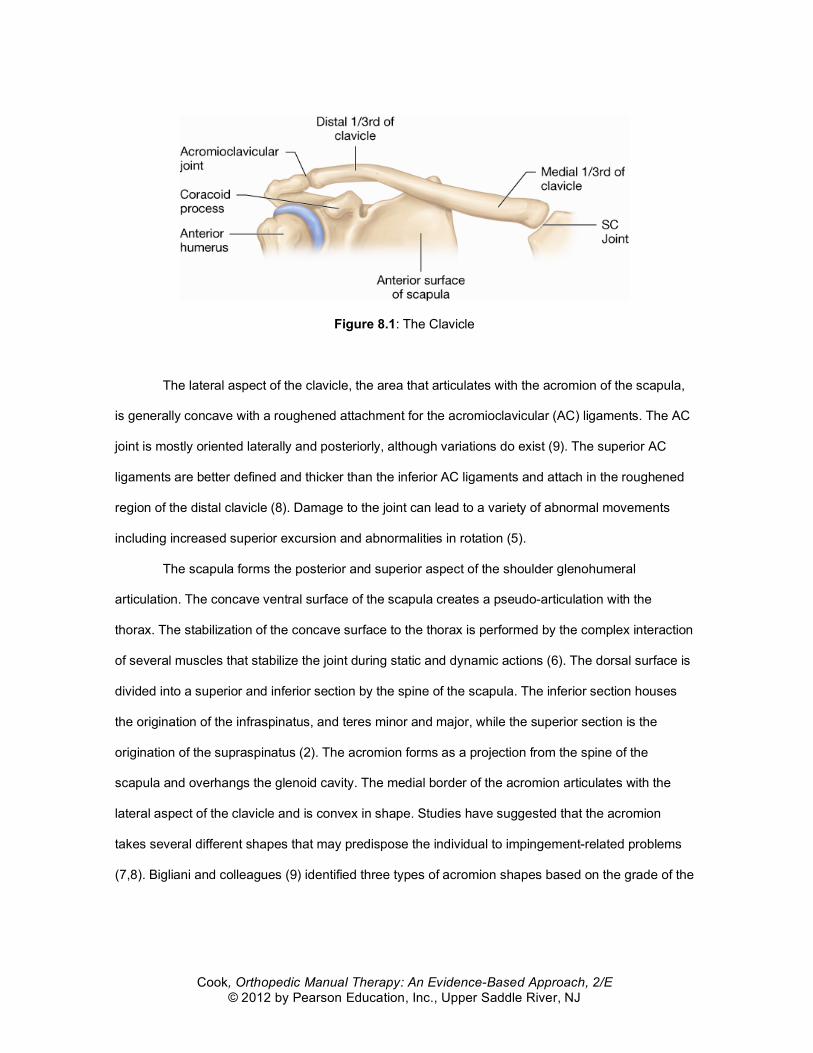
Figure 8.1: The Clavicle
The lateral aspect of the clavicle, the area that articulates with the acromion of the scapula,
is generally concave with a roughened attachment for the acromioclavicular (AC) ligaments. The AC
joint is mostly oriented laterally and posteriorly, although variations do exist (9). The superior AC
ligaments are better defined and thicker than the inferior AC ligaments and attach in the roughened
region of the distal clavicle (8). Damage to the joint can lead to a variety of abnormal movements
including increased superior excursion and abnormalities in rotation (5).
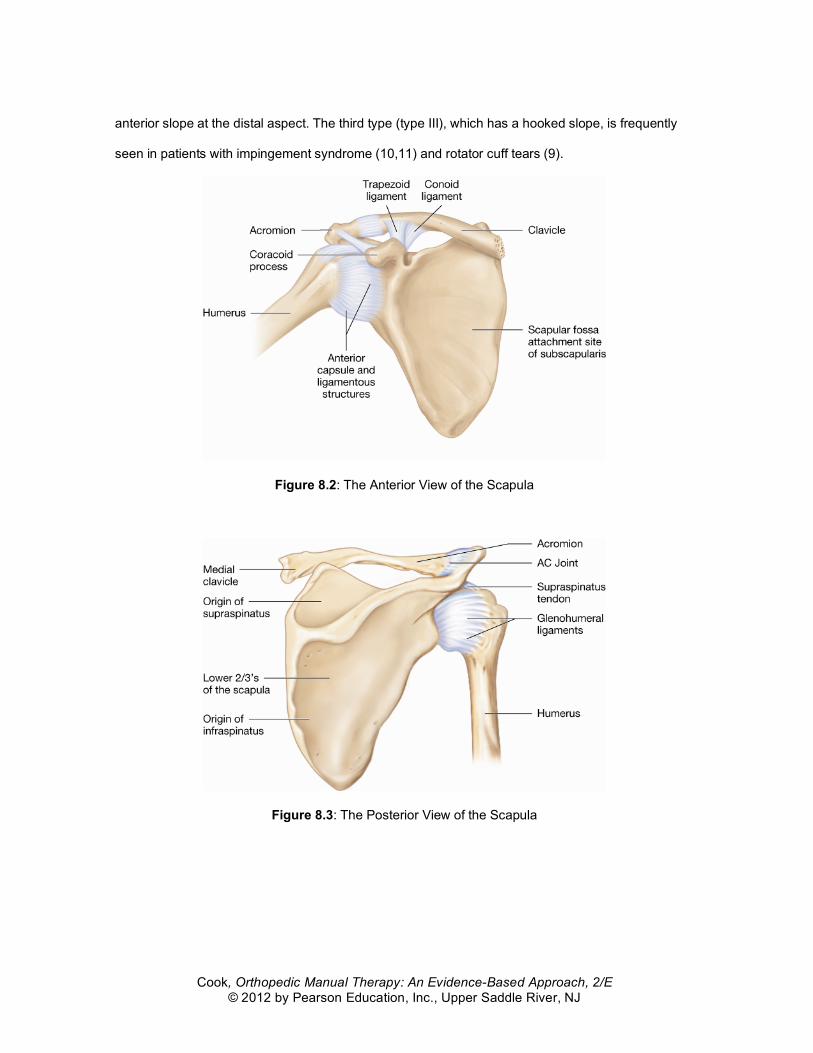
The scapula forms the posterior and superior aspect of the shoulder glenohumeral
articulation. The concave ventral surface of the scapula creates a pseudo-articulation with the
thorax. The stabilization of the concave surface to the thorax is performed by the complex interaction
of several muscles that stabilize the joint during static and dynamic actions (6). The dorsal surface is
divided into a superior and inferior section by the spine of the scapula. The inferior section houses
the origination of the infraspinatus, and teres minor and major, while the superior section is the
origination of the supraspinatus (2). The acromion forms as a projection from the spine of the
scapula and overhangs the glenoid cavity. The medial border of the acromion articulates with the
lateral aspect of the clavicle and is convex in shape. Studies have suggested that the acromion
takes several different shapes that may predispose the individual to impingement-related problems
(7,8). Bigliani and colleagues (9) identified three types of acromion shapes based on the grade of the
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
anterior slope at the distal aspect. The third type (type III), which has a hooked slope, is frequently
seen in patients with impingement syndrome (10,11) and rotator cuff tears (9).
Figure 8.2: The Anterior View of the Scapula
Figure 8.3: The Posterior View of the Scapula
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
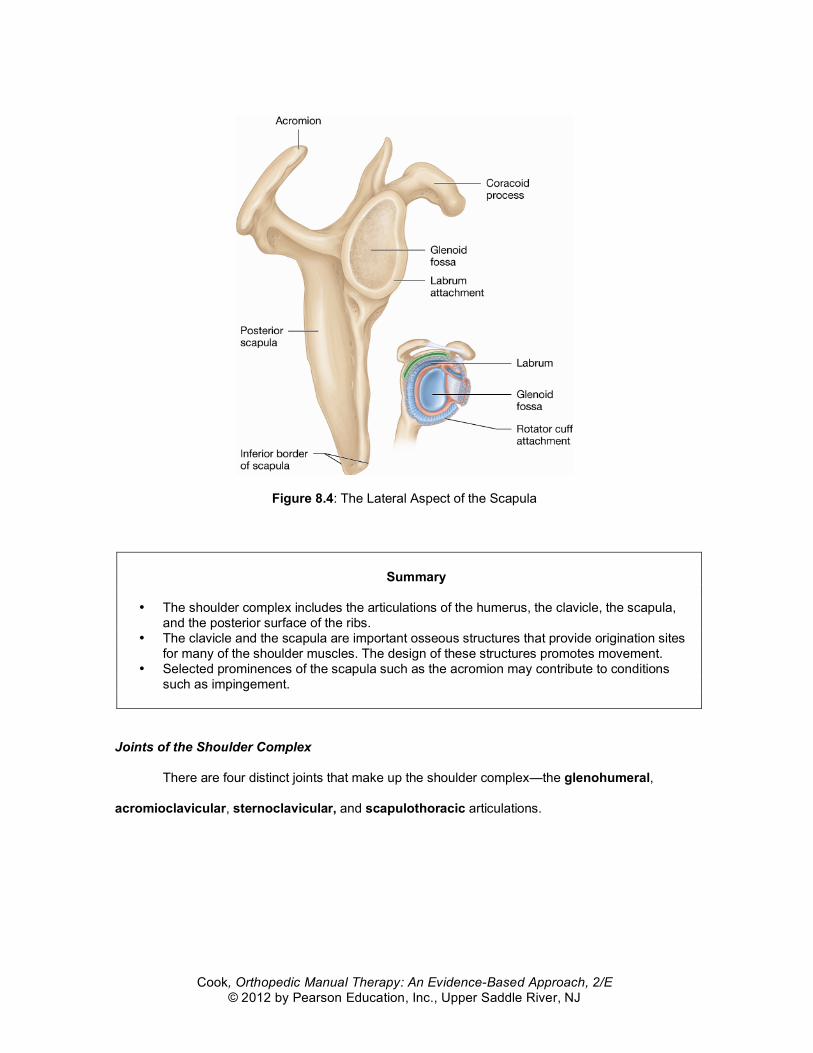
Figure 8.4: The Lateral Aspect of the Scapula
Summary
• The shoulder complex includes the articulations of the humerus, the clavicle, the scapula,
and the posterior surface of the ribs. • The clavicle and the scapula are important osseous structures that provide origination sites
for many of the shoulder muscles. The design of these structures promotes movement. • Selected prominences of the scapula such as the acromion may contribute to conditions
such as impingement.
Joints of the Shoulder Complex
There are four distinct joints that make up the shoulder complex—the glenohumeral,
acromioclavicular, sternoclavicular, and scapulothoracic articulations.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
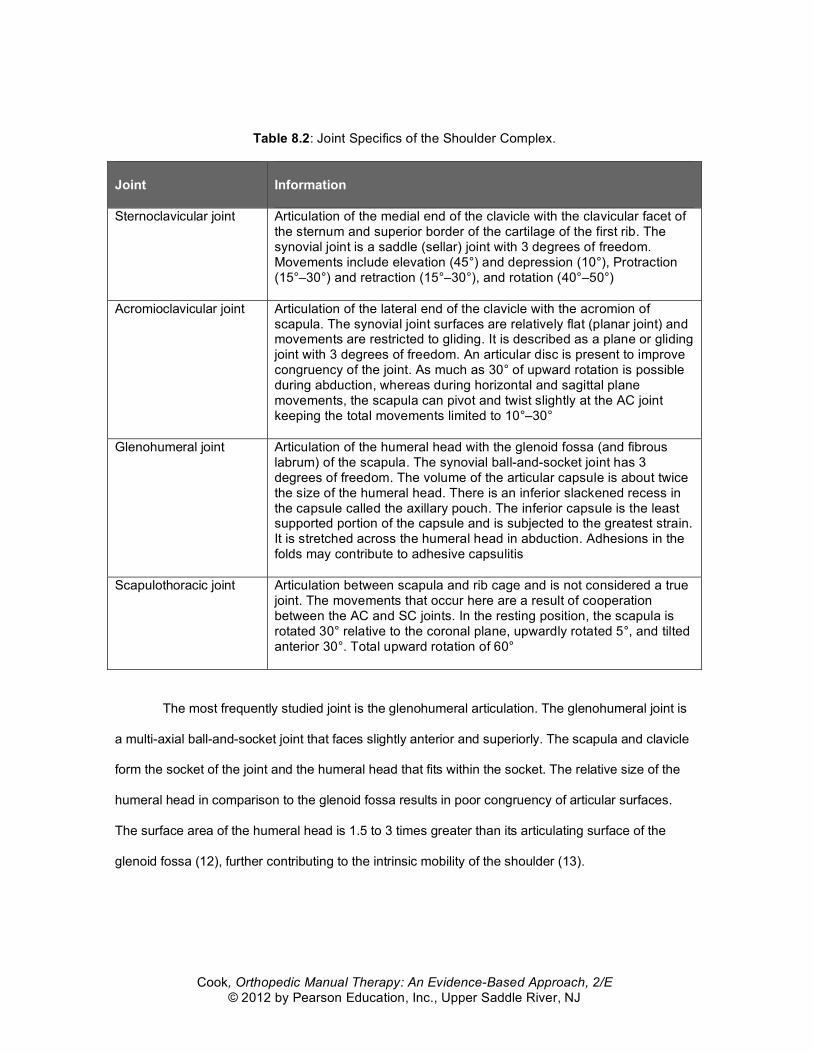
Table 8.2: Joint Specifics of the Shoulder Complex.
Joint
Information
Sternoclavicular joint Articulation of the medial end of the clavicle with the clavicular facet of the sternum and superior border of the cartilage of the first rib. The synovial joint is a saddle (sellar) joint with 3 degrees of freedom. Movements include elevation (45°) and depression (10°), Protraction (15°–30°) and retraction (15°–30°), and rotation (40°–50°)
Acromioclavicular joint Articulation of the lateral end of the clavicle with the acromion of scapula. The synovial joint surfaces are relatively flat (planar joint) and movements are restricted to gliding. It is described as a plane or gliding joint with 3 degrees of freedom. An articular disc is present to improve congruency of the joint. As much as 30° of upward rotation is possible during abduction, whereas during horizontal and sagittal plane movements, the scapula can pivot and twist slightly at the AC joint keeping the total movements limited to 10°–30°
Glenohumeral joint Articulation of the humeral head with the glenoid fossa (and fibrous labrum) of the scapula. The synovial ball-and-socket joint has 3 degrees of freedom. The volume of the articular capsule is about twice the size of the humeral head. There is an inferior slackened recess in the capsule called the axillary pouch. The inferior capsule is the least supported portion of the capsule and is subjected to the greatest strain. It is stretched across the humeral head in abduction. Adhesions in the folds may contribute to adhesive capsulitis
Scapulothoracic joint Articulation between scapula and rib cage and is not considered a true joint. The movements that occur here are a result of cooperation between the AC and SC joints. In the resting position, the scapula is rotated 30° relative to the coronal plane, upwardly rotated 5°, and tilted anterior 30°. Total upward rotation of 60°
The most frequently studied joint is the glenohumeral articulation. The glenohumeral joint is
a multi-axial ball-and-socket joint that faces slightly anterior and superiorly. The scapula and clavicle
form the socket of the joint and the humeral head that fits within the socket. The relative size of the
humeral head in comparison to the glenoid fossa results in poor congruency of articular surfaces.
The surface area of the humeral head is 1.5 to 3 times greater than its articulating surface of the
glenoid fossa (12), further contributing to the intrinsic mobility of the shoulder (13).
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
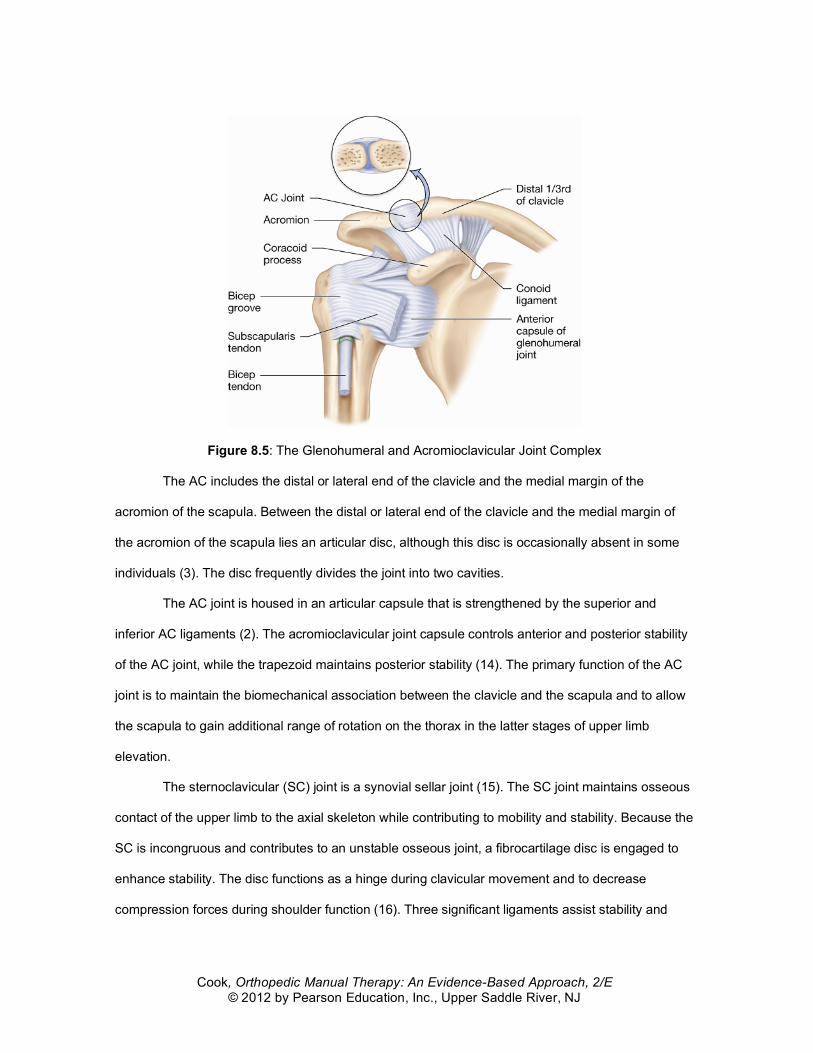
Figure 8.5: The Glenohumeral and Acromioclavicular Joint Complex
The AC includes the distal or lateral end of the clavicle and the medial margin of the
acromion of the scapula. Between the distal or lateral end of the clavicle and the medial margin of
the acromion of the scapula lies an articular disc, although this disc is occasionally absent in some
individuals (3). The disc frequently divides the joint into two cavities.
The AC joint is housed in an articular capsule that is strengthened by the superior and
inferior AC ligaments (2). The acromioclavicular joint capsule controls anterior and posterior stability
of the AC joint, while the trapezoid maintains posterior stability (14). The primary function of the AC
joint is to maintain the biomechanical association between the clavicle and the scapula and to allow
the scapula to gain additional range of rotation on the thorax in the latter stages of upper limb
elevation.
The sternoclavicular (SC) joint is a synovial sellar joint (15). The SC joint maintains osseous
contact of the upper limb to the axial skeleton while contributing to mobility and stability. Because the
SC is incongruous and contributes to an unstable osseous joint, a fibrocartilage disc is engaged to
enhance stability. The disc functions as a hinge during clavicular movement and to decrease
compression forces during shoulder function (16). Three significant ligaments assist stability and
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
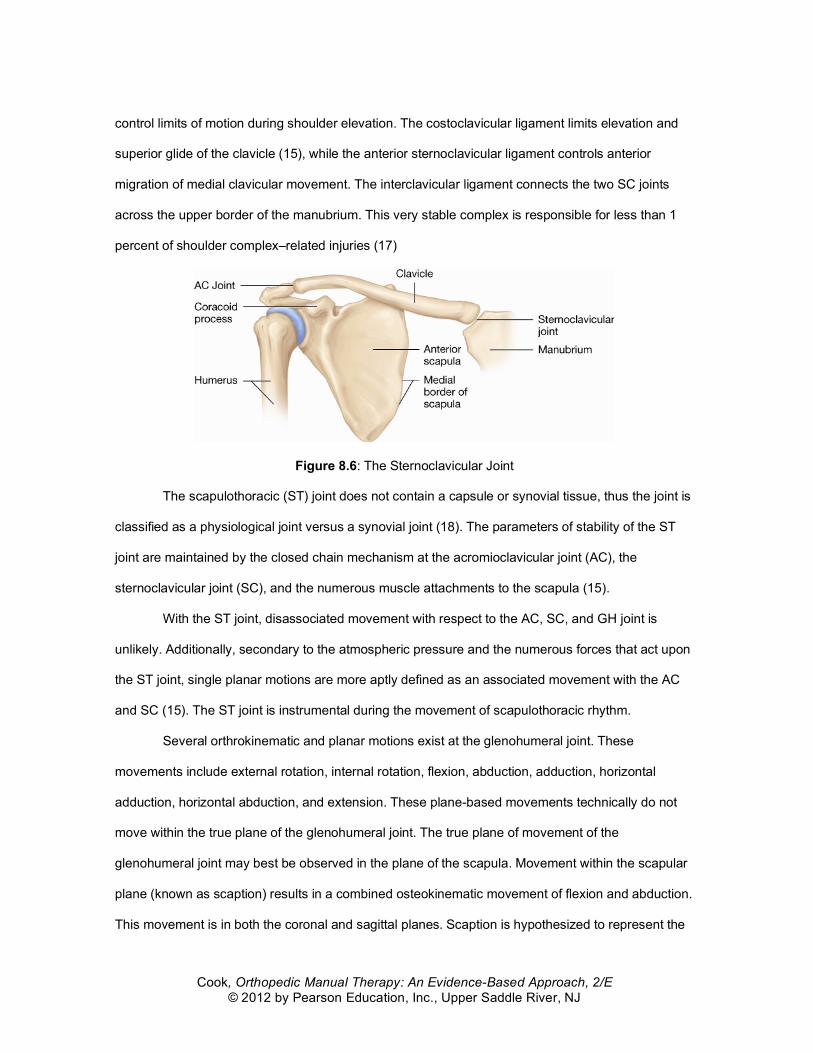
control limits of motion during shoulder elevation. The costoclavicular ligament limits elevation and
superior glide of the clavicle (15), while the anterior sternoclavicular ligament controls anterior
migration of medial clavicular movement. The interclavicular ligament connects the two SC joints
across the upper border of the manubrium. This very stable complex is responsible for less than 1
percent of shoulder complex–related injuries (17)
Figure 8.6: The Sternoclavicular Joint
The scapulothoracic (ST) joint does not contain a capsule or synovial tissue, thus the joint is
classified as a physiological joint versus a synovial joint (18). The parameters of stability of the ST
joint are maintained by the closed chain mechanism at the acromioclavicular joint (AC), the
sternoclavicular joint (SC), and the numerous muscle attachments to the scapula (15).
With the ST joint, disassociated movement with respect to the AC, SC, and GH joint is
unlikely. Additionally, secondary to the atmospheric pressure and the numerous forces that act upon
the ST joint, single planar motions are more aptly defined as an associated movement with the AC
and SC (15). The ST joint is instrumental during the movement of scapulothoracic rhythm.
Several orthrokinematic and planar motions exist at the glenohumeral joint. These
movements include external rotation, internal rotation, flexion, abduction, adduction, horizontal
adduction, horizontal abduction, and extension. These plane-based movements technically do not
move within the true plane of the glenohumeral joint. The true plane of movement of the
glenohumeral joint may best be observed in the plane of the scapula. Movement within the scapular
plane (known as scaption) results in a combined osteokinematic movement of flexion and abduction.
This movement is in both the coronal and sagittal planes. Scaption is hypothesized to represent the
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
most clinical significant length–tension relationship of the elevators and rotators of the shoulder (19).
However, selected studies demonstrate the external rotators are the only shoulder musculature that
benefits from greater torque when placed in the scaption plane (20–22).
Another notable component of scaption is the presence of greater joint congruency in the
scaption plane (19). This allows for capsular relaxation of fibers in a nonimpaired shoulder and less
potential for impingement of structures during movement (19).
Summary
• There are four distinct joints that make up the shoulder complex—the glenohumeral,
acromioclavicular, sternoclavicular, and scapulothoracic articulations. • The primary function of the glenohumeral joint is to allow mobility of the humerus by
providing a very precariously unstable connection. • The primary function of the AC joint is to maintain the biomechanical association between
the clavicle and the scapula and to allow the scapula to gain additional range of rotation on the thorax in the latter stages of upper limb elevation.
• The primary function of the SC joint is to maintain osseous contact of the upper limb to the axial skeleton while both contributing to mobility and stability.
• The clavicle and the scapula are important osseous structures that provide origination sites for many of the shoulder muscles. The design of these structures promotes movement.
• The scapulothoracic (ST) joint does not contain a capsule or synovial tissue but does supply a muscle contact with the thoracic region.
SHOULDER COMPLEX BIOMECHANICS
Glenohumeral Range of Motion
The glenohumeral joint has six degrees of freedom, which consist of three rotations and
three translations (23). Glenohumeral movement is significantly affected by the interaction of passive
and active structures that are further altered by pathology. Normal shoulder range of motion involves
the careful combination of the movements of glenohumeral, ST, AC, and SC and varies with age.

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
Table 8.3: Joint-Specific Biomechanics and Movement of the Shoulder Complex. Osteokinematics
Plane of Motion/Axis of Rotation
Arthrokinematics
Abduction/adduction Frontal plane/anterior-posterior axis of rotation
Roll and slide along joint’s longitudinal diameter
IR/ER Horizontal plane/vertical axis of rotation
Roll and slide along joint’s transverse diameter
Flexion/extension and IR/ER in 90° abduction
Sagittal plane/medial-lateral axis of rotation
Spin between humeral head and glenoid fossa
Historically, manual therapists have used two distinct biomechanical principles in the
examination and treatment of the shoulder complex: 1) the convex-concave rule and 2) Cyriax’s
capsular pattern. MacConail (24) first described the convex-concave theory of arthrokinematic
motion. This theory asserts that the joint surface geometry dictates the accessory movement pattern
during physiological movement (25). Examination and treatment is guided by the joint geometry, and
variations are considered either abnormal or inappropriate. In the shoulder, evidence to support this
theory is poor. Numerous studies indicate that the glenohumeral joint does not always move as a
ball-and-socket joint but occasionally displays translatory-only movements during pathology (25–27).
Because of this, it appears that the selection of a technique that focuses on a specific direction
based solely on the convex-concave rule may not yield values any better than the antagonistic
direction at the shoulder (28–30).
Cyriax initially proposed that pathology in the shoulder results in range-of-motion loss in
proportional patterns based on a ratio (31). He used this ratio to differentiate between losses of
motion secondary to bony, muscular, or capsular changes. His hierarchical-based capsular pattern
was external rotation limited more than abduction limited more than internal rotation, proportionally.
Several studies have identified variability of a capsular pattern of the shoulder (32–35); subsequently
the use of this biomechanical principle may yield little value.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
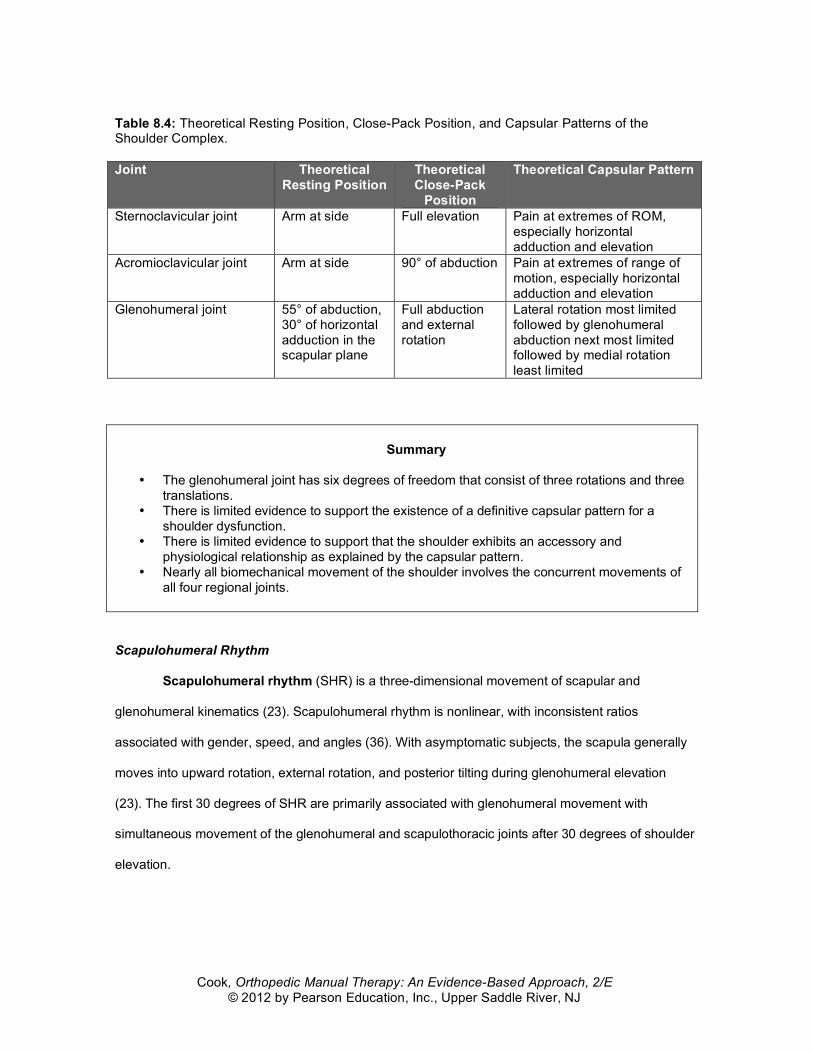
Table 8.4: Theoretical Resting Position, Close-Pack Position, and Capsular Patterns of the Shoulder Complex. Joint Theoretical
Resting Position Theoretical Close-Pack
Position
Theoretical Capsular Pattern
Sternoclavicular joint Arm at side
Full elevation Pain at extremes of ROM, especially horizontal adduction and elevation
Acromioclavicular joint Arm at side
90° of abduction Pain at extremes of range of motion, especially horizontal adduction and elevation
Glenohumeral joint 55° of abduction, 30° of horizontal adduction in the scapular plane
Full abduction and external rotation
Lateral rotation most limited followed by glenohumeral abduction next most limited followed by medial rotation least limited
Summary
• The glenohumeral joint has six degrees of freedom that consist of three rotations and three
translations. • There is limited evidence to support the existence of a definitive capsular pattern for a
shoulder dysfunction. • There is limited evidence to support that the shoulder exhibits an accessory and
physiological relationship as explained by the capsular pattern. • Nearly all biomechanical movement of the shoulder involves the concurrent movements of
all four regional joints.
Scapulohumeral Rhythm
Scapulohumeral rhythm (SHR) is a three-dimensional movement of scapular and
glenohumeral kinematics (23). Scapulohumeral rhythm is nonlinear, with inconsistent ratios
associated with gender, speed, and angles (36). With asymptomatic subjects, the scapula generally
moves into upward rotation, external rotation, and posterior tilting during glenohumeral elevation
(23). The first 30 degrees of SHR are primarily associated with glenohumeral movement with
simultaneous movement of the glenohumeral and scapulothoracic joints after 30 degrees of shoulder
elevation.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
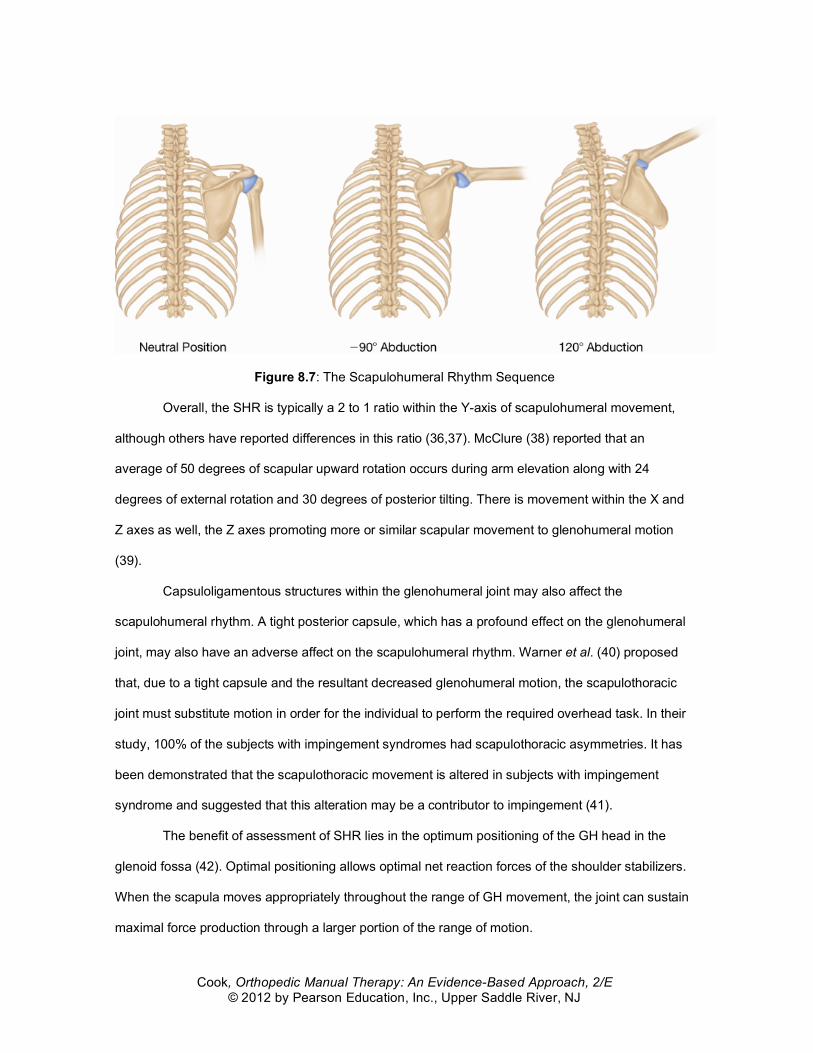
Figure 8.7: The Scapulohumeral Rhythm Sequence
Overall, the SHR is typically a 2 to 1 ratio within the Y-axis of scapulohumeral movement,
although others have reported differences in this ratio (36,37). McClure (38) reported that an
average of 50 degrees of scapular upward rotation occurs during arm elevation along with 24
degrees of external rotation and 30 degrees of posterior tilting. There is movement within the X and
Z axes as well, the Z axes promoting more or similar scapular movement to glenohumeral motion
(39).
Capsuloligamentous structures within the glenohumeral joint may also affect the
scapulohumeral rhythm. A tight posterior capsule, which has a profound effect on the glenohumeral
joint, may also have an adverse affect on the scapulohumeral rhythm. Warner et al. (40) proposed
that, due to a tight capsule and the resultant decreased glenohumeral motion, the scapulothoracic
joint must substitute motion in order for the individual to perform the required overhead task. In their
study, 100% of the subjects with impingement syndromes had scapulothoracic asymmetries. It has
been demonstrated that the scapulothoracic movement is altered in subjects with impingement
syndrome and suggested that this alteration may be a contributor to impingement (41).
The benefit of assessment of SHR lies in the optimum positioning of the GH head in the
glenoid fossa (42). Optimal positioning allows optimal net reaction forces of the shoulder stabilizers.
When the scapula moves appropriately throughout the range of GH movement, the joint can sustain
maximal force production through a larger portion of the range of motion.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
Summary
• Scapulohumeral rhythm (SHR) is a three-dimensional movement of scapular and
glenohumeral kinematics. • Although the SHR is variable across individuals, generally, the movement is associated with
two parts glenohumeral motion to one part scapular motion. • Abnormalities in SHR are commonly associated with impairments such as impingement
syndrome. • Scapulohumeral rhythm is designed to improve the position of the humeral head within the
glenoid fossa.
Acromioclavicular Range of Motion
Normal acromioclavicular motion works synergistically with scapulohumeral movement to
increase joint stability (5). Although nearly 40 to 50 degrees of clavicle rotation occurs during arm
elevation, only 5 to 8 degrees of movement occurs specifically at the AC because the clavicle moves
synergistically with the scapula (3).
Sternoclavicular Range of Motion
Like the AC, the SC is a synovial joint but has three degrees of freedom. The SC moves
with elevation depression and protraction retraction of the clavicle. During normal shoulder elevation,
the SC moves approximately 30 to 35 degrees. The majority of SC movement occurs in the first 90
degrees of arm movement with a ratio of 4 degrees of SC movement for every 10 degrees of
glenohumeral movement (3).
Summary
• Although nearly 40 to 50 degrees of rotation of the clavicle occurs during shoulder elevation,
only 5 to 8 degrees of motion is required at the AC joint. • During shoulder elevation, the SC moves approximately 30 to 35 degrees.
Passive Stabilization
Normally, the shoulder sacrifices passive stability for gains in mobility. The passive
stabilizers of the shoulder include the bony, cartilaginous, capsular, and ligamentous structures (42).
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
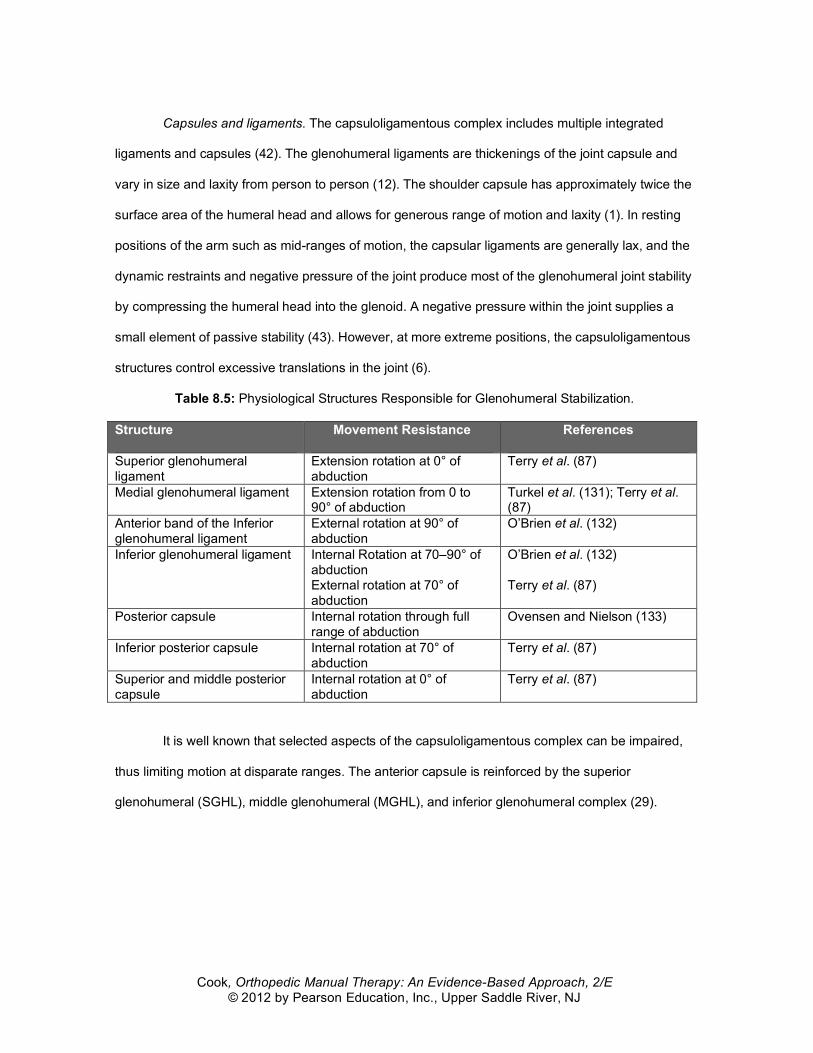
Capsules and ligaments. The capsuloligamentous complex includes multiple integrated
ligaments and capsules (42). The glenohumeral ligaments are thickenings of the joint capsule and
vary in size and laxity from person to person (12). The shoulder capsule has approximately twice the
surface area of the humeral head and allows for generous range of motion and laxity (1). In resting
positions of the arm such as mid-ranges of motion, the capsular ligaments are generally lax, and the
dynamic restraints and negative pressure of the joint produce most of the glenohumeral joint stability
by compressing the humeral head into the glenoid. A negative pressure within the joint supplies a
small element of passive stability (43). However, at more extreme positions, the capsuloligamentous
structures control excessive translations in the joint (6).
Table 8.5: Physiological Structures Responsible for Glenohumeral Stabilization.
Structure Movement Resistance References
Superior glenohumeral ligament
Extension rotation at 0° of abduction
Terry et al. (87)
Medial glenohumeral ligament Extension rotation from 0 to 90° of abduction
Turkel et al. (131); Terry et al. (87)
Anterior band of the Inferior glenohumeral ligament
External rotation at 90° of abduction
O’Brien et al. (132)
Inferior glenohumeral ligament Internal Rotation at 70–90° of abduction External rotation at 70° of abduction
O’Brien et al. (132) Terry et al. (87)
Posterior capsule Internal rotation through full range of abduction
Ovensen and Nielson (133)
Inferior posterior capsule Internal rotation at 70° of abduction
Terry et al. (87)
Superior and middle posterior capsule
Internal rotation at 0° of abduction
Terry et al. (87)
It is well known that selected aspects of the capsuloligamentous complex can be impaired,
thus limiting motion at disparate ranges. The anterior capsule is reinforced by the superior
glenohumeral (SGHL), middle glenohumeral (MGHL), and inferior glenohumeral complex (29).
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
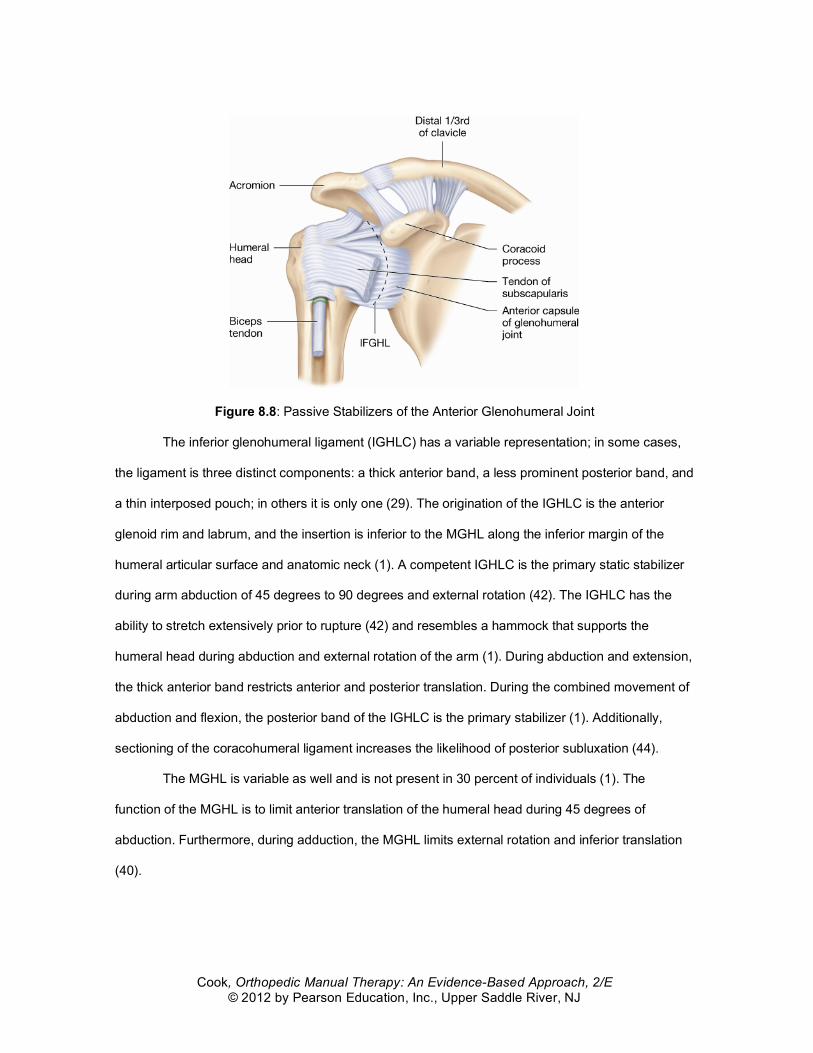
Figure 8.8: Passive Stabilizers of the Anterior Glenohumeral Joint
The inferior glenohumeral ligament (IGHLC) has a variable representation; in some cases,
the ligament is three distinct components: a thick anterior band, a less prominent posterior band, and
a thin interposed pouch; in others it is only one (29). The origination of the IGHLC is the anterior
glenoid rim and labrum, and the insertion is inferior to the MGHL along the inferior margin of the
humeral articular surface and anatomic neck (1). A competent IGHLC is the primary static stabilizer
during arm abduction of 45 degrees to 90 degrees and external rotation (42). The IGHLC has the
ability to stretch extensively prior to rupture (42) and resembles a hammock that supports the
humeral head during abduction and external rotation of the arm (1). During abduction and extension,
the thick anterior band restricts anterior and posterior translation. During the combined movement of
abduction and flexion, the posterior band of the IGHLC is the primary stabilizer (1). Additionally,
sectioning of the coracohumeral ligament increases the likelihood of posterior subluxation (44).
The MGHL is variable as well and is not present in 30 percent of individuals (1). The
function of the MGHL is to limit anterior translation of the humeral head during 45 degrees of
abduction. Furthermore, during adduction, the MGHL limits external rotation and inferior translation
(40).
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
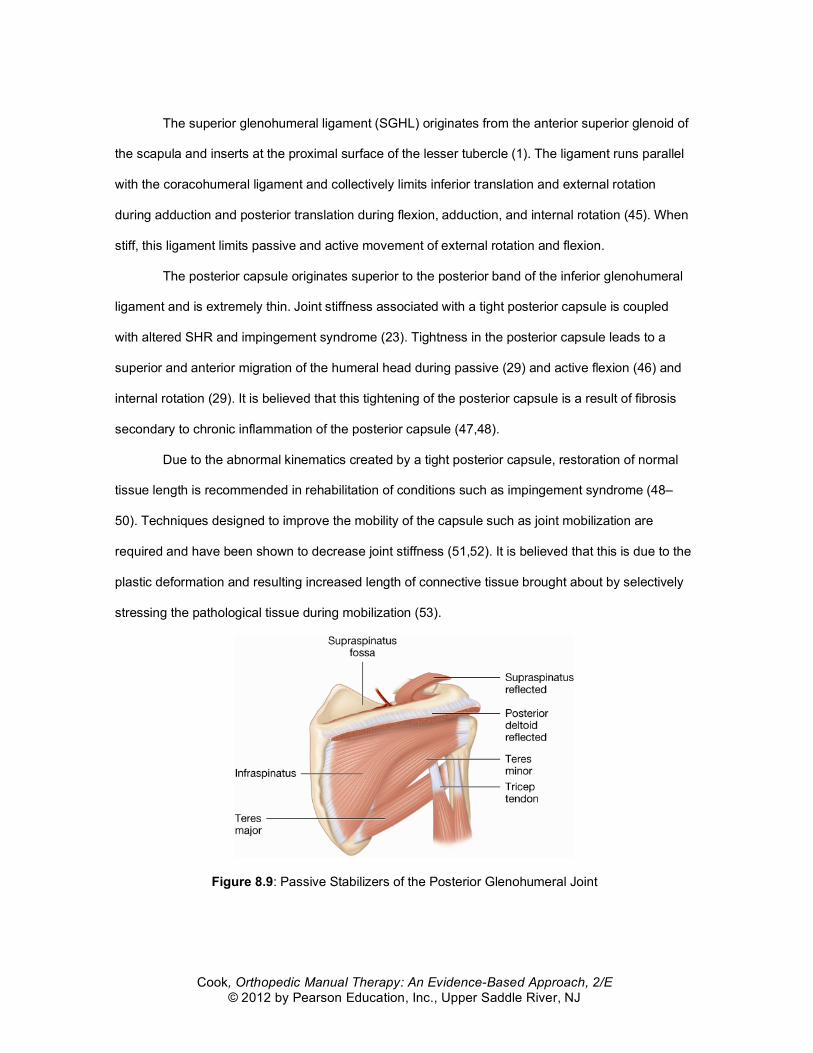
The superior glenohumeral ligament (SGHL) originates from the anterior superior glenoid of
the scapula and inserts at the proximal surface of the lesser tubercle (1). The ligament runs parallel
with the coracohumeral ligament and collectively limits inferior translation and external rotation
during adduction and posterior translation during flexion, adduction, and internal rotation (45). When
stiff, this ligament limits passive and active movement of external rotation and flexion.
The posterior capsule originates superior to the posterior band of the inferior glenohumeral
ligament and is extremely thin. Joint stiffness associated with a tight posterior capsule is coupled
with altered SHR and impingement syndrome (23). Tightness in the posterior capsule leads to a
superior and anterior migration of the humeral head during passive (29) and active flexion (46) and
internal rotation (29). It is believed that this tightening of the posterior capsule is a result of fibrosis
secondary to chronic inflammation of the posterior capsule (47,48).
Due to the abnormal kinematics created by a tight posterior capsule, restoration of normal
tissue length is recommended in rehabilitation of conditions such as impingement syndrome (48–
50). Techniques designed to improve the mobility of the capsule such as joint mobilization are
required and have been shown to decrease joint stiffness (51,52). It is believed that this is due to the
plastic deformation and resulting increased length of connective tissue brought about by selectively
stressing the pathological tissue during mobilization (53).
Figure 8.9: Passive Stabilizers of the Posterior Glenohumeral Joint
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
Passive structures responsible for stabilization of the AC include the joint capsule, the
trapezoid, and conoid ligaments. The joint capsule of the AC is very thin and is significantly
supported by ligaments (3). The superior AC ligament significantly effects the stabilization of the
distal clavicle during rotation (3). The inferior AC ligament is often indistinguishable from the capsule
and the contribution of this ligament to stability is not completely known (3). Fukuda et al. (14) noted
that the conoid ligament was the most significant contributor of stability during anterior and superior
translation. The conoid is often disrupted during marked superior translation of the clavicle with
respect to the scapula (3). Ironically, the conoid ligament inserts more medially on men than women,
potentially increasing the anterior and posterior movement of the clavicle to the scapula, though data
does not exist to support this (3). Additionally, soft tissue at the AC joint functions synergistically to
provide joint stability in all planes of movement (5).
Passive structures responsible for the SC include the costoclavicular ligament, which
stabilizes during elevation and rotation of the clavicle, and the interclavicular ligaments that stabilize
the clavicle with the SC capsule and sternum. Although the joint structure (diarthrodial, saddle-type
joint) is inherently flexible, the joint is one of the least dislocated in the body (3). The SC also has an
intra-articular disc that allows complex rotational motion similar to movement available in a ball-and-
socket joint. Passive stabilization of the joint through surgery is rarely successful because the
majority of surgeries result in a loosening of the hardware placed within the joint (3).
Summary
• The capsuloligamentous complex includes multiple integrated ligaments and capsule. • The inferior glenohumeral ligament (IGHLC) has a variable representation; in some cases,
the ligament is three distinct components: a thick anterior band, a less prominent posterior band, and a thin interposed pouch, in others it is only one.
• The middle glenohumeral ligament (MGHL) is variable as well and is not present in 30% of patients.
• The superior glenohumeral ligament (SGHL) limits inferior translation and external rotation during adduction and posterior translation during flexion, adduction, and internal rotation.
• Tightness in the posterior capsule leads to a superior and anterior migration of the humeral head during passive and active flexion and internal rotation.
• Passive structures responsible for stabilization of the AC include the joint capsule, and the trapezoid and conoid ligaments. The joint capsule of the AC is very thin and is significantly supported by ligaments.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
• Passive structures responsible for the SC include the costoclavicular ligament, which stabilizes during elevation and rotation of the clavicle, and the interclavicular ligaments, which stabilize the clavicle with the SC capsule and sternum.
Active Stabilization
The active stabilizers of the shoulder include all of the muscles of the shoulder (42). Poor
motor control leads to impairments in dynamic stability of the shoulder. Passively, the
capsuloligamentous structures contribute to glenohumeral stability, yet on their own, they are poor
stabilizers (54). Unlike other joint stabilizers, active muscle contraction of the glenohumeral joint
comprises the principal stabilization of the shoulder, specifically during dynamic motion (55,56).
Cocontraction of the rotator cuff musculature is designed to translate the humerus to the center of
the glenoid (57).
The supraspinatus is active during elevation of the arm, specifically at the early ranges of
motion and after 90 degrees of elevation (54). Rupture of the supraspinatus can cause anterior and
superior translation of the humeral head (42). Together with the deltoid, the majority of elevation of
the arm is associated with this muscle. Collectively, with all of the rotator cuff musculature, the head
of the humerus is compressed into the glenoid fossa and further stabilized during movement (42).
Active contraction of the infraspinatus and teres minor reduce anterior-superior translation
and produce active external range of motion (54). The infraspinatus assists in pulling the humeral
head inferiorly during elevation and works in a complementary fashion with the supraspinatus. The
combined contraction of the infraspinatus and the subscapularis increases the compression of the
head of the humerus during arm elevation and is an essential element of a force couple.
The subscapularis functions in a dual role, providing anterior stability (reducing anterior
translation of the humerus) and caudal depression of the humeral head (54). Uncontrolled humeral
translation increases dramatically during reduced rotator cuff activity (58). Normally, this uncontrolled
translation is countered by the subscapularis (57). Inflammation and constant pressure of the
humeral head on the anterior capsule may inhibit the action of the subscapularis muscle, leading to
further anterior laxity problems.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
When stability of the shoulder is compromised, the humeral head will typically migrate
anteriorly with rotator cuff activity, generally the opposite of the tightness of the capsule (usually
posterior) (29). In some cases, however, such as subacromial impingement, the humeral head may
translate superiorly rather than anteriorly or posteriorly (59).
Summary
• Active stabilizers of the shoulder include the rotator cuff muscles. They are the principle
structures associated with dynamic control of the shoulder. • The supraspinatus is active during elevation of the arm, specifically at the early ranges of
motion and after 90 degrees of elevation. Rupture of the supraspinatus can cause anterior and superior translation of the humeral head.
• The infraspinatus and teres minor reduce anterioinferior translation and produce active external range of motion.
• The subscapularis functions in a dual role, providing anterior stability (reducing anterior translation of the humerus) and caudal depression of the humeral head.
Online References
1. McCluskey G, Getz B. Pathophysiology of anterior shoulder instability. J Athletic Training. 2000;35:268–272.
2. Rockwood C, Matsen F. The shoulder. Philadelphia; W.B. Saunders Publishing: 1998. 3. Renfree K, Wright T. Anatomy and biomechanics of the acromioclavicular and
sternoclavicular joints. Clin Sports Med. 2003;22(2):219–237. 4. Urist UM. Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Am.
1963;45:1750–1753. 5. Debski R, Parsons IM, Woo SL, Fu FH. Effect of capsular injury on acromioclavicular
joint mechanics. J Bone Joint Surg Am. 2001;83-A(9):1344–1351. 6. Wang CH, McClure P, Pratt N, Nobilini N. Stretching and strengthening exercises: Their
effect on three-dimensional scapular kinematics. Arch Phys Med Rehabil. 1999;80:923–929.
7. Neer CS. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41–50.
8. Neer CS, Craing EV, Fukuda H. Cuff-tear arthropathy. J Bone Joint Surg Am. 1983;65:1232–1244.
9. Bigliani LU, Kelkar R, Flatow EL, Pollock RG, Mow VC. Glenohumeral instability: Biomechanical properties of passive and active stabilizers. Clin Orthop. 1996;330:13–30.
10. Bigliani LU, Ticker JB, Flatow EL, Soslowsky LJ, Mow VC. The relationship of acromial architecture to rotator cuff disease. Clin Sports Med. 1991;10(4):823–838.
11. Kim SJ, Lee JW, Kim BS. Arthroscopic decompression for subacromial impingement syndrome. J Korean Med Sci. 1997;12(2):123–127.
12. Tzannes A, Murrell GA. Clinical examination of the unstable shoulder. Sports Med. 2002;32(7):447–457.
13. Zatsiorsky V, Aktov A. Biomechanics of highly precise movements: Movement control: An interdisciplinary forum. VU University Press; Amsterdam: 1991.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
14. Fukuda K, Caring EV, An KN, Cofield RH, Chao EY. Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am. 1986;68:434–440. Warwick R, Williams P. Gray’s Anatomy, 35th ed. WB Saunders: Philadelphia. 1973.
15. Norkin CC, White JD. Measurement of joint motion: A guide to goniometry. 2nd ed. Philadelphia; FA Davis: 1995.
16. Sadr B, Swann M. Spontaneous dislocation of the sternoclavicular joint. Acta Orthop Scand. 1979;50:269.
17. Steindler A. Kinesiology of the human body under normal and pathological conditions. Charles C Thomas; Springfield, IL: 1955.
18. Poppen HK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg. 1976;58A:195–201.
19. Greenfield B, Johanson M, Donatelli R, Gonzalez Z. Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am. 1993;75(2):311–312.
20. Tata GE, Ng L, Kramer JF. Shoulder antagonistic strength ratios during concentric and eccentric muscle actions in the scapular plane. J Orthop Sports Phys Ther. 1993;18(6):654–660.
21. Helmig P, Sojbjerg JO, Kjaersgaard-Andersen P, Nielsen S, Ovesen J. Distal humeral migration as a component of multidirectional shoulder instability. An anatomical study in autopsy specimens. Clin Orthop Relat Res. 1990;252:139–143.
22. Michener L, McClure P, Karduna A. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech. 2003;18:369–379.
23. MacConail M. Joint Movement. Physiother. 1964;50:363–365. 24. McClure P, Flowers K. Treatment of limited should motion: a case study based on
biomechanical considerations. Phys Ther. 1992;72:929–936. 25. Baeyens J, Van Roy P, De Schepper A, Declercq G, Clarijs J. Glenohumeral joint
kinematics related to minor anterior instability of the shoulder at the end of the later preparatory phase of throwing. Clin Biomech. 2001;16:752–757.
26. Baeyens J, Van Roy P, Clarjjs J. Intra-articular kinematics of the normal glenohumeral joint in the late preparatory phase of throwing: Kaltenborn’s rule revisited. Ergonomics. 2000;10:1726–1737.
27. Hsu A, Ho L, Hedman T. Joint position during anterior-posterior glide mobilization: its effect on glenohumeral abduction range of motion. Arch Phys Med Rehabil. 2000;81:210–214.
28. Harryman DT, Sidles JA, Harris SL, Clark JM, McQuade KJ, Gibb TD, Matsen FA. Translation of the humeral head on the glenoid with passive glenohumeral motion. J Bone Jnt Surg. 1990;79A(9):1334–1343.
29. Brandt C, Sole G, Krause MW, Nel M. An evidence-based review on the validity of the Kaltenborn rule as applied to the glenohumeral joint. Man Ther. 2007;12(1):3–11.
30. Cyriax J. Illustrated manual of orthopedic medicine. 2nd ed. New York; Macmillan Publishing: 1978.
31. Mitsch J, Casey J, McKinnis R, Kegerreis S, Stikeleather J. Investigation of a consistent pattern of motion restriction in patients with adhesive capsulitis. J Man Manip Ther. 2004;12:153–159.
32. Winters JC, Groenier KH, Sobel JS, Arendzen HH, Meyboom-de Jongh B. Classification of shoulder complaints in general practice by means of cluster analysis. Arch Phys Med Rehabil. 1997;78:1369–1374.
33. Rundquist P, Ludewig P. Patterns of motion loss in subjects with idiopathic loss of shoulder range of motion. Clin Biomech. 2004;19:810–818.
34. Rundquist PJ, Anderson DD, Guanche CA, Ludewig PM. Shoulder kinematics in subjects with frozen shoulder. Arch Phys Med Rehabil. 2003;84:1473–1479.
35. Sugamoto K, Harada T, Machida A, et al. Scapulohumeral rhythm: relationship between motion velocity and rhythm Clin Orthop. 2002;401:119–124.
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
36. Doody SG, Feedman L, Waterland JC. Shoulder movements during abduction in the scapular plane. Arch Phys Med Rehabil. 1970;51(10):595–604.
37. McClure PW, Michener LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:269–277.
38. McQuade KJ, Wei SH, Smidt GL. Effects of local muscle fatigue on three-dimensional scapulohumeral rhythm. Clin Biomech.1995;10:114–148.
39. Warner JJ, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med. 1992;20:675–685.
40. Hebert LJ, Moffet H, McFadyen BJ, Dionne CE. Scapular behavior in shoulder impingement syndrome. Arch Phys Med Rehabil. 2002;83(1):60–69.
41. Abboud J, Soslowsky L. Interplay of the static and dynamic restraints in glenohumeral instability. Clin Orthop. 2002;400:48–57.
42. Silliman JF, Hawkins RJ. Current concepts and recent advances in the athlete’s shoulder. Clin Sports Med. 1991;10:693–705.
43. Blasier RB, Soslowsky LJ, Malicky DM. Posterior glenohumeral subluxation: active and passive stabilization in a biomechanical model. J Bone Joint Surg AM. 1997;79:433–440.
44. Prescher A. Anatomical basics, variations, and degenerative changes of the shoulder joint and shoulder girdle. Eur J Radiol. 2000;35:88–102.
45. Brossmann J, Preidler KW, Pedowitz RA, White LM, Trudell D, Resnick D. Shoulder impingement syndrome: influence of shoulder position on rotator cuff impingement—an anatomic study. AJR Am J Roentgenol. 1996;167(6):1511–1515.
46. Pappas A. Overuse Syndromes of the Shoulder and Arm. Adolesc Med. 1991;2(1):181–212.
47. Warner JP, Boardman ND. Anatomy, biomechanics and pathophysiology of glenohumeral instability. In: Warren et al. The unstable shoulder. Philadelphia; Lippincott Williams & Wilkins: 1998.
48. Kamkar A, Irrang J, Whitney S. Nonoperative management of secondary shoulder impingement syndrome. J Orthop Sports Phys Ther. 1993;17:212–223.
49. Tyler TF, Nicholas SJ, Roy T, Gleim GW. Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med. 2000;28(5):668–673.
50. Scheib JS. Diagnosis and rehabilitation of the shoulder impingement syndrome in the overhand and throwing athlete. Rheum Dis Clin North Am. 1990;16(4):971–988.
51. Hjelm R, Draper C, Spencer S. Anterior inferior capsule length insufficiency in the painful shoulder. J Orthop Sports Phys Ther. 1996;23:216–222.
52. Threlkeld A. The effects of manual therapy on connective tissue. Phys Ther. 1992;72(12):893–902.
53. Hess S. Functional stability of the glenohumeral joint. Man Ther. 2000;5(2):63–71. 54. Soslowsky LJ, Malicky DM, Blasier RB. Active and passive factors in inferior
glenohumeral stabilization: a biomechanical model. J Shoulder Elbow Surg. 1997;6(4):371–379.
55. Kronberg M, Brostrom LA, Soderlund V. Retroversion of the humeral head in the normal shoulder and its relationship to the normal range of motion. Clin Orthop Relat Res. 1990;253:113–117.
56. Lippitt S, Matsen F. Mechanisms of glenohumeral joint stability. Clin Orthop Relat Res. 1993;291:20–28.
57. Wuelker N, Korell M, Thren K. Dynamic glenohumeral joint stability. J Shoulder Elbow Surg. 1998;7(1):43–52.
58. Magarey ME, Jones MA. Specific evaluation of the function of force couples relevant for stabilization of the glenohumeral joint. Man Ther. 2003;8(4):247–253.