Embed Size (px)
DESCRIPTION
schematic diagram
Citation preview

Sickle cell anemia

.

-

s
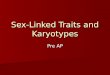
POLYCYTEMIA VERA
Polycythemia vera is a bone marrow disease that leads to an abnormal increase in the number of blood cells (primarily red blood cells).
Nursing Management:
Advised patients with a history of significant bleeding to avoid aspirin and aspirin containing medications.
Minimizing alcohol intake should be also emphasized to further diminished the risk of bleeding.
Instruct the patients that he must avoid iron supplements, including those within multivitamins supplements
Explain to avoid vigorous toweling after bathing.
Risk Factors:o Thromboseso Smokingo Obesityo Poorly controlled
hypertension
Pathophysiology:
Erythrocyte elevation predominates
Hematocrit elevation can exceed to 60%
Spleen resumes its embryonic function of hematopoises & enlarges
Lab. & Diagnostic Exams:
Bone marrow biopsy Complete blood
count with differential Comprehensive metabolic
panel Erythropoietin level Genetic test for the
JAK2V617F mutation Oxygen saturation of the
blood Red blood cell mass Vitamin B12 level
Manifestations:
Breathing difficulty when lying downDizzinessExcessive bleedingHeadacheItchinessShortness of breathFatigue
Bone marrow become fibrotic

Risk Factors:
Pathophysiology:
Nursing Management:
POLYCYTEMIA VERA
Polycythemia vera is a bone marrow disease that leads to an abnormal increase in the number of blood cells (primarily red blood cells).
Manifestations:
Breathing difficulty when lying downDizzinessExcessive bleedingHeadacheItchinessShortness of breathFatigue


.

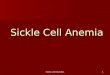
Hemophilia is a group of hereditary bleeding disorder characterized by a deficiency in a blood-clotting factor.
HEMOPHILIA A
This is a classic hemophilia and is the most common type;the missing clotting factor VIII
HEMOPHILIA B: ”Christmas disease’;the missing
clotting factor is factor IXHEMOPHILIA C:
The missing clotting factor is factor IX
1.Newborn bleeding signs:2.Nose bleeding (epistaxis)3.Skin sign: ecchymotic patches4.Spontaneous hematuria5.Anemia6.Hemarthrosis (hemorrhages in the
joints causing pain, swelling and limited movement)
Antifibrinolytic medicines tranexamic acid aminocaproic
acid Desmopressin Prophylactic
Defect in the intrinsic hemostatic mechanism and fibrin thread formation.
Gene deletions and point mutations.
Cascade of interactions involving clotting proteins, phosphor-lipids, and
Explain how to care for, administer, store and reconstitute the replacement factor.
Inform the child and family that superficial injuries are treated with ice and pressure.
Teach parents how to immobilize the joint, pack it in ice, and administer replacement factor.
Explain the possible side effects of therapy . Demonstrate passive ROM exercises. Emphasize avoidance of aspirin and aspirin-
containing compounds. Provide diet information because weight increase
can impose further stress on joints.
1. Monitor bleeding and maintain bleeding precautions.2. Prepare to administer replacement factor as prescribed.3. Monitor for joint pain, immobilize the affected extremity if joint pain occurs.4. Assess neurological status.5. Monitor urine for hematuria.6. Control joint bleeding by immobilization, elevation and the application of ice, in addition apply pressure for superficial bleeding.
low factor VIII in hemophilia A
, low factor IX in hemophilia B,
prolonged partial thromboplastin time
impaired prothrombin consumption
NURSING INTERVENTIONS
MEDICATIONSDIAGNOSTIC FINDINGS
HEALTH TEACHINGSBlood coagulation
HEMOPHILIA
PATHOPHYSIOLOGY
SIGNS AND SYMPTOMSTYPES OF HEMOPHILIA
HEMOPHILIA

new cells to replenish blood cells.[1] The condition, per its name, involves both aplasia and anemia. Typically, anemia refers to low red blood cell counts, but aplastic anemia patients have lower counts of all three blood cell types: red blood cells, white blood cells, and platelets, termed pancytopenia.
Exams and Tests
1. Bone marrow aspirate and biopsy2. History of iatrogenic exposure to cytotoxic chemotherapy3. X-rays, computed tomography (CT) scans, or ultrasound
imaging tests: enlarged lymph nodes (sign of lymphoma), kidneys and bones in arms and hands (abnormal in Fanconi anemia)
4. Chest X-ray: infections5. Liver tests: liver diseases6. Viral studies: viral infections7. Vitamin B12 and folate levels: vitamin deficiency8. Blood tests for paroxysmal nocturnal hemoglobinuria9. Test for antibodies: immune competence
Signs and Symptoms
malaise, pallor and associated symptoms such as palpitations, Thrombocytopenia (low platelet counts), leading to increased risk of hemorrhage, bruising and petechiae, Leukopenia (low white blood cell count), leading to increased risk of infection and Reticulocytopenia (low reticulocyte counts).
Nursing Interventions
1. Maintain established rapport
2. Monitor vital signs, especially temp.
3. Stress proper hand washing techniques by all caregivers between therapies
4. Monitor visitors/ caregivers of the client. Instruct SO to limit visitors especially those with known contagious illnesses.
5. Maintain aseptic/sterile techniques as much as possible
6.Advise the use of facial mask when going outside the client’s room
7. Encouraged early ambulation, deep breathing and turning exercises as indicated.

Severe pain:abdomen, joints, flank,legs

Pathophysiology
one of many types of the larger family of megaloblastic anemias. It is caused by loss of gastric parietal cells, and subsequent inability to absorb vitamin B12. The loss of ability to absorb vitamin B12 is the most common cause of adult vitamin B12 deficiency.
Medication
Vitamin B-12 is available for therapeutic use parenterally as either cyanocobalamin or hydroxocobalamin.[4] Both are equally useful in the treatment of vitamin B-12 deficiency, and they are nontoxic (except for rare allergic reactions). Theoretical advantages exist to using hydroxocobalamin because it is retained better in the body and is more available to cells; both chemical forms of cobalamine provide prompt correction.
Manifestations:
Fatigue, low blood pressure, rapid heart rate, high blood pressure, pallor, depression, muscle weakness, and shortness of breath
Neuropathic pain Frequent diarrhea Paresthesias Jaundice Glossitis Personality or memory changes]
Health Teachings
Compliance in obtaining adequate vitamin B-12 for a lifetime by injection (or possibly orally) is necessary to avoid relapse of pernicious anemia.
Explain the need to increase fluid intake to prevent dehydration that results from impaired ability to properly concentrate urine.
Teach the patient the potential for bleeding and hemorrhage, and instruction to prevent bleeding and discuss the need for regular dental examinations and explain the importance of maintaining regular bowel movements to prevent straining.
Exams and Tests
CBC Reticulocyte count Schilling test (if pernicious anemia is suspected) Serum LDH Serum vitamin B12 level and serum folate levels Esophagogastroduodenoscopy (EGD) to examine the
stomach, or enteroscopy to examine the small intestine may be done.
Bone marrow biopsy Physical exam
Pernicious anemia
(also known as Biermer's anemia, Addison's anemia, or Addison–Biermer anemia)
Nursing Interventions
Assess patient ability to perform ADLs Instruct client to stop activity if palpitations, chest pain, shortness of
breath, weakness, or dizziness occur Monitor vital sign (Blood Pressure, pulse, and respirations) during
and after activity Suggest client change position slowly; monitor for dizziness. Provide or recommend assistance with activities and ambulation as
necessary, allowing client to be an active participant as much as possible.
Identify and implement energy-saving techniques

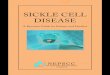
Severe hemolytic anemia occurring that results from inheritance of the sickle hemoglobin gene
Severe pain:abdomen,joints,flank legs
Severe chronic anemia Irritability,lethargy,
listlessness High fever Anorexia,vomiting Jaundice from red blood
cells destruction Enlargement of the liver
and spleen(hepatosplenomega-ly)
Analgesic-Morphine-Acetaminophen
Hydroxyurea Arginine
DIAGNOSTIC EXAMINATIONS
Hemoglobin electrophoresis-shows the presence of sickle hemoglobins
1. Institute bed rest to decrease the need for oxygen.
2. Maintain adequate hydration.3. Administer oxygen as ordered.4. Admister blood transfusion as ordered,for
hemoglobin levels lower than 4 g/dl.5. Assist the child to assume a comfortable
position so that child keeps the extremeties extended to promote venous return.
6. Encourage consumption of a high calorie ,high protein diet, with folic acid supplementation.
7. Keep warm.8. Administer antibiotics as prescribed to
prevent infection.
Erythrocyte containing HBs loses its round, pliable, biconcave disk shaped and becomes deformed, rigid and
sickle shaped
Low oxygen to venous blood
Sickle cell hemoglobin acquires a crystal like formation when exposed
to low oxygen tension
Inheritance o the sickle cell hemoglobin gene
PATHOPHYSIOLOGY
HEALTH TEACHING Genetic counseling Prenatal screening Screening of children Prevent sickle cell crisis by preventing hypoxia, infection, and dehydration Avoidance of activities that decrease oxygenation of the blood:
-smoking-flying in unpressured airplanes-living in high altitudes-living in high altitudes
Families should be encouraged to contact community sickle cell agencies for follow-up information, new drug protocols, and psychosocial support. Families should also follow the advances of gene therapy, bone marrow transplantation, and the usage of cord blood stem cells.
MEDICATIONS
NURSING INTERVENTIONS
SIGNS AND SYMPTOMS
SICKLE CELL ANEMIA