Embed Size (px)
Citation preview

SICKLE CELL DISEASE
Dr. M. SOFI MD;FRCP (London); FRCPEdin; FRCSEdin

Sickle cell disease (SCD)Sickle cell disease (SCD) and its variants are genetic disorders resulting from the presence of a mutated form of hemoglobin, hemoglobin S (HbS). The most common form of SCD is homozygous HbS disease (HbSS), an autosomal recessive disorder first described by Herrick in 1910. SCD causes significant morbidity and mortality, particularly in people of African and Mediterranean ancestry. Morbidity, frequency of crisis, degree of anemia, and the organ systems involved vary considerably from individual to individual.

SCD denotes all genotypes containing at least one sickle gene, in which HbS makes up at least half the hemoglobin present. Major sickle genotypes described so far include the following:
• HbSS disease or sickle cell anemia (the most common) - Homozygote for the S globin with usually a severe or moderately severe phenotype and with the shortest survival
• HbS/b-0 thalassemia - Double heterozygote for HbS and b-0 thalassemia; clinically indistinguishable from sickle cell anemia (SCA)
• HbS/b+ thalassemia - Mild-to-moderate severity with variability in different ethnicities
Genetics

• HbSC disease - Double heterozygote for HbS and HbC characterized by moderate clinical severity
• HbS/hereditary persistence of fetal Hb (S/HPHP) - Very mild or asymptomatic phenotype
• HbS/HbE syndrome - Very rare with a phenotype usually similar to HbS/b+ thalassemia
• Rare combinations of HbS with other abnormal hemoglobins such as HbD Los Angeles, G-Philadelphia, HbO Arab, and others
• Sickle cell trait or the carrier state is the heterozygous form characterized by the presence of around 40% HbS, absence of anemia, inability to concentrate urine (isosthenuria), and hematuria.
Genetics

• Heterozygotes; there is typically 60% HbA and 40% HbS.
• Sickle cell trait protects against malaria.
• Sickle cell trait occurs in approximately 300 million people worldwide, with the highest prevalence of approximately 30% to 40% in sub-Saharan Africa.
• Patients with sickle cell trait are generally asymptomatic
Sickle cell trait is occasionally associated with significant morbidity - e.g.,
• Haematuria, • Renal papillary necrosis• Splenic infarction, • Exertion
rhabdomyolysis • Exercise-related
sudden death. • Sickle cell trait is also
associated with rare but often fatal renal medullary cancer.
Sickle cell trait:

• Average lifespan of individuals with sickle cell trait is similar to general population.
• Laboratory tests are normal: No anemia, No hemolysis Only presence of
hemoglobin AS on hemoglobin electrophoresis.
• Severe hypoxia during: general anesthesia Severe dehydration severe physical exertion
Adequate hydration:• Avoiding excessive fluid
loss and severe heat• People with sickle cell
trait should be advised to build up slowly in training with paced progressions, allowing longer periods of rest and recovery between repetitions.
• Pre-season strength and sports-specific conditioning programmes should be encouraged
Sickle cell trait

• SCD is the most common severe genetic disease.
• The prevalence of SCD is highest in sub-Saharan Africa.
• The sickle beta globin gene is spread widely throughout Africa, the Middle East, the Mediterranean and India
• Sickle genes are present in 1 in every 50 Asians and 1 in every 100 Northern Greeks.
• The frequency of sickle cell carriers is up to 1 in 4 in West Africans and 1 in 10 in Afro-Caribbeans.
• There is evidence for partial resistance of carriers to all forms of Plasmodium falciparum malaria in many populations.
Sickle cell disease

Presentation• Symptoms of SCD can
begin between 3 months and 6 months of age when HbF levels are falling.
• Anemia, jaundice, pallor, lethargy, growth restriction and general weakness
Common causes of anemia are:
• Acute splenic sequestration,
• Transient red cell aplasia,
• Hyperhemolysis in patients with severe infection.
• Susceptibility to encapsulated bacteria such as pneumococcus
• Risk of overwhelming infection is highest before the age of 3 years.
• Splenomegaly may be present in infancy and childhood but recurrent splenic infarcts then cause autosplenectomy.
• Delayed puberty.
Sickle cell disease

• Acute and chronic pain in any body part: The most common clinical manifestation of SCD is vaso-occlusive crisis; pain crises are the most distinguishing clinical feature of SCD
• Bone pain: The long bones of the extremities are often involved, often due to bone marrow infarction
• Anemia: Universally present, chronic, and hemolytic in nature
• Aplastic crisis: Serious complication due to infection with B19V
• Growth retardation, delayed sexual maturation, being underweight
• Splenic sequestration: Characterized by the onset of life-threatening anemia with rapid enlargement of the spleen and high reticulocyte count
• Infection: Organisms that pose the greatest danger include encapsulated respiratory bacteria, particularly Streptococcus pneumonia; adult infections are predominately with gram-negative organisms, especially Salmonella
• Hand-foot syndrome: This is a dactylitis presenting as bilateral painful and swollen hands and/or feet in children
Signs and symptomsSickle cell disease (SCD) usually manifests early in childhood. Complaints may include the following:

• Acute chest syndrome: Young children present with chest pain, fever, cough, tachypnea, leukocytosis, and pulmonary infiltrates in the upper lobes; adults are usually afebrile, dyspneic with severe chest pain, with multilobar/lower lobe disease
• Pulmonary hypertension: Increasingly recognized as a serious complication of SCD
• Avascular necrosis of the femoral or humeral head: This is due to vascular occlusion
• CNS involvement: Most severe manifestation is stroke
• Ophthalmologic involvement: Ptosis, retinal vascular changes, proliferative retinitis
• Cardiac involvement: Dilation of both ventricles and the left atrium
• GI involvement: Cholelithiasis is common in children; liver may become involved
• GU involvement: Kidneys lose concentrating capacity; priapism is a well-recognized complication of SCD
• Dermatologic involvement: Leg ulcers are a chronic painful problem
Signs and symptomsSickle cell disease (SCD) usually manifests early in childhood. Complaints may include the following:

Triggers of vaso-occlusive crisis include the following:
Hypoxemia: May be due to acute chest syndrome or respiratory complications
Dehydration: Acidosis results in a shift of the oxygen dissociation curve
Changes in body temperature (eg, an increase due to fever or a decrease due to environmental temperature change)

Laboratory tests used in patients with SCD include the following:
• Mandatory screening for HbS at birth; prenatal testing can be obtained via chorionic villus sampling
• Hemoglobin electrophoresis • CBC count with differential and
reticulocyte count • Serum electrolytes • Hemoglobin solubility testing • Peripheral blood smear
• Pulmonary function tests (transcutaneous O 2 saturation)
• Renal function (creatine, BUN, urinalysis)
• Hepatobiliary function tests, (ALT, fractionated bilirubin)
• CSF examination: Consider LP in febrile children who appear toxic and in those with neurologic findings (eg, neck stiffness, + Brudzinski/Kernig signs, focal deficits); consider CT scanning before performing LP
• Blood cultures • ABGs • Secretory phospholipase A2 (sPLA2)
DiagnosisSCD is suggested by the typical clinical picture of chronic hemolytic anemia and vaso-occlusive crisis. Electrophoresis confirms the diagnosis with the presence of homozygous HbS and can also document other hemoglobinopathies (eg, HbSC, HbS-beta+ thalassemia).

• Radiography: Chest x-rays should be performed in patients with respiratory symptoms
• MRI: Useful for early detection of bone marrow changes due to acute and chronic bone marrow infarction, marrow hyperplasia, osteomyelitis, and osteonecrosis
• CT scanning: May demonstrate subtle regions of osteonecrosis not apparent on plain radiographs in patients who are unable to have an MRI and to exclude renal medullary carcinoma in patients presenting with hematuria
• Nuclear medicine scanning: 99m Tc bone scanning detects early stages of osteonecrosis; In WBC scanning is used for diagnosing osteomyelitis
• Transcranial Doppler ultrasonography: Can identify children with SCD at high risk for stroke
• Abdominal ultrasonography: Can be used to rule out cholecystitis, cholelithiasis, or an ectopic pregnancy and to measure spleen and liver size
• Echocardiography: Identifies patients with pulmonary hypertension
DiagnosisImaging studiesImaging studies that aid in the diagnosis of sickle cell anemia in patients in whom the disease is suggested clinically include the following:

Vaso-occlusive crises (obstruction of the microcirculation by sickled red blood cells, causing ischemia):
• It may be precipitated by cold, infection, dehydration, exertion or ischemia.
• Often no cause can be found.
• Occlusion of small vessels by sickled erythrocytes causes pain which is variable from mild to severe.
• May present with swollen painful joints
• Tachypnea or other signs of lung involvement
• Acute abdominal distension and pain (mesenteric sickling and bowel ischemia)
Sickle cell Crisis

• Loin pain (renal papillary necrosis may cause renal colic or severe hematuria)
• Priapism • Hyphaema • Retinal occlusion.• Large vessels may also
be involved, causing thrombotic strokes
• Acute sickle chest syndrome
Stroke:• Variable presentation,
including fits and focal neurological signs.
• Cerebral infarction is more common in children.
• Hemorrhage from microaneurysms which develop around infarctions
• “Moyamoya” is more common in adults.
Sickle cell Crisis

Sequestration crisis:• Acute splenic
sequestration has been defined as an acute fall of haemoglobin and markedly elevated reticulocyte count, together with an acute increase in spleen size.
• Mainly in babies and young children.
• Recurrent splenic sequestration is an indication for splenectomy.
• Severity is variable but can present with hypovolemic shock and anemia.
• Sequestration causes significant mortality.
• Mortality rates can be reduced substantially by parental education, regular palpation of the abdomen at home to detect early signs of splenic enlargement, and prompt transfusion.
Sickle cell Crisis

Aplastic crisis (temporary cessation of erythropoiesis, causing severe anemia):
• Usually precipitated by infection with parvovirus B19.
• There is usually a drop in hemoglobin over about one week.
• Recovery may be spontaneous but a transfusion is usually required.
• With the severe anemia associated with an aplastic crisis, patients may present with high-output congestive heart failure.
Sickle cell Crisis

Acute chest syndrome (vaso-occlusive crisis affecting the lungs):
• Defined as a new pulmonary infiltrate on the chest radiograph combined with one or more manifestations such as fever, cough, sputum production, tachypnoea, dyspnoea, or new-onset hypoxia.
Lung infections tend to predominate in children, and infarcts predominate in adults.
Hyperhemolytic crisis (excessive hemolysis):
• Uncommon; during painful crises there may be a marked increase in the rate of hemolysis with a fall in the hemoglobin level.
Sickle cell Crisis

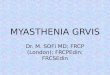
Skeletal sickle cell anemia. Bone-within-bone appearance. Following multiple infarctions of the long bones, sclerosis may assume the appearance of a bone within a bone, reflecting the old cortex within the new cortex.
Sickle cell anemia

Splenic sequestration is an acute emergency and can be fatal in 1-2 hours secondary to circulatory hypovolemia. Treatment is with volume resuscitation and blood transfusion. The CT image shown demonstrates splenomegaly with a mass-like process (arrows) from splenic sequestration.
Sickle cell anemia

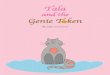
In renal papillary necrosis, repeated vascular occlusion infarcts the renal medullary pyramids and papillae. This causes sloughing of papillae, which obstructs the urinary tract.
The intravenous pyelogram demonstrates the "egg-in-a-cup" appearance of sloughed renal papillae (arrows) secondary to renal papillary necrosis.
Sickle cell anemia

Skeletal sickle cell anemia. Advanced dactylitis. Lytic processes are present at the first and fifth metacarpals, along with periostitis, which is most prominent in the third metacarpal.
Sickle cell anemia

Sickle cell retinopathy is believed to be vaso-occlusion of peripheral arterioles of the retina leading to: • Retinal hypoxia, ischemia,
and infarction. • New vessels then form at
the junction of the vascular and avascular areas of retina.
• Another common ocular manifestation is hyphema.
• Anterior chamber bleeding occurs spontaneously leading to glaucomatous changes
• Optic nerve damage from even mildly elevated intraocular pressures.
Sickle cell anemia
Hyphema
Retinal neovasculrization

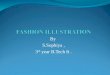
A 12-year-old boy with HgbSS disease presents to the pediatric emergency department with altered mental status, left-sided gaze paralysis with his head tilted to the left, and flaccid paralysis of the right arm and leg. A CT scan of the brain was obtained immediately.
Sickle cell anemia

Management
The goals of treatment in SCD are symptom control and management of disease complications. Treatment strategies include the following 7 goals:
1. Management of vaso-occlusive crisis 2. Management of chronic pain syndromes 3. Management of chronic hemolytic anemia 4. Prevention and treatment of infections 5. Management of the complications and the various organ damage
syndromes associated with the disease 6. Prevention of stroke 7. Detection and treatment of pulmonary hypertension

PharmacotherapySCD may be treated with the following medications:Antimetabolites: Hydroxyurea Opioid analgesics (eg, oxycodone/ASA, methadone, morphine sulfate, oxycodone/APAP, fentanyl, nalbuphine, codeine, APAP/codeine) Nonsteroidal analgesics (eg, ketorolac, ASA, APAP, ibuprofen) Antibiotics (eg, cefuroxime, amoxicillin/clavulanate, penicillin VK, ceftriaxone, azithromycin, cefaclor) Vaccines (eg, PCV7, PPV23, meningococcal, influenza, recommended scheduled childhood/adult vaccinations) Vitamins (eg, folic acid)

Nonpharmacologic therapy• Other approaches to managing
SCD include the following:• Stem cell transplantation: Can
be curative • Transfusions: For sudden,
severe anemia due to acute splenic sequestration, parvovirus B19 infection, or hyperhemolytic crises
• Physical therapy • Heat and cold application • Acupuncture and acupressure • TENS
Combination pharmacotherapy and nonpharmacotherapy
• Vigorous hydration (plus analgesics): For vaso-occlusive crisis
• Oxygen, antibiotics, analgesics, incentive spirometry, simple transfusion, and bronchodilators: For treatment of acute chest syndrome
Treatment

• Pre-operative screening for sickle cell disease should be carried out in patients from ethnic groups in which there is a significant prevalence of the condition.
• Emergency screening with sickle solubility tests must always be followed by definitive analysis.
• Prenatal diagnosis: sickle cell disease can also be diagnosed in a fetus through from amniocentesis, chorionic villus sampling and fetal blood sampling
Screening

• It is very important that people with sickle cell disease are reviewed regularly by a specialist
• Patients should be monitored regularly in specialist clinics for their growth, development and organ function so that active management may be considered before organ failure develops.
Parental and patient education:
• Avoiding situations that can precipitate crises (e.g., cold, dehydration, and exhaustion) and early recognition and treatment of infection.
Management

• Palpation for splenic size to ensure early detection of splenic sequestration can significantly reduce deaths.
• All patients should be advised to avoid alcohol because of its dehydrating effects and smoking because it may cause the acute sickle chest syndrome.
• Folic acid supplements may be required.
• Zinc supplementation should also be considered if growth is restricted.
• Vitamin D deficiency is very prevalent and may co-exist with sickle cell disease, so advice should be given regarding vitamin supplementation
Management

Psychological:• Good support of
patients, families and other careers is essential.
• Cognitive behavioural therapy may be indicated.
Infection:• Oral penicillin
prophylaxis is started at diagnosis.
• The risk of pneumoccocal infection remains high but decreases with age.
• Penicillin prophylaxis is continued throughout life in some countries but is stopped at age 5 years in other countries.
Management

• Routine childhood vaccinations include protection against Haemophilus influenzae type B and conjugated vaccines against Streptococcus pneumoniae in most high-income countries.
• Children should also receive unconjugated pneumococcal vaccine from 2 years of age, repeated every three to five years
• Immunisation against meningococcus, influenza, and hepatitis B.
• Because malaria is a significant cause of morbidity and mortality in patients with sickle cell disease, malaria chemoprophylaxis is often recommended
Management

Blood transfusions:• Transfusion therapy is a
key intervention in decreasing morbidity and mortality.
• Transfusion may be required for severe anemia or to reduce the proportion of HbS if there are lung or central nervous system complications.
• Partial exchange transfusion is in acute life-threatening complications, such as severe acute chest syndrome, acute stroke, multi-organ failure or urgent preparation for major surgery
• Iron overload is a possible complication of regular transfusions and iron chelation should be started in all children receiving regular blood transfusions
Management

Hydroxycarbamide (hydroxyurea):
• Many cytotoxic drugs increase fetal haemoglobin concentrations, which is potentially beneficial for patients with sickle cell disease.
• Benefits include increasing haemoglobin concentrations, and decreasing platelet and white cell counts.
• Concerns remain about its myelosuppressive and teratogenic effects and its possible long-term toxicity. Hydroxycarbamide (hydroxyurea) should be stopped at least three months before conception
Management

Hydroxyurea can reduce:
• The frequency of crises in SCD.
• The episodes of acute chest sydnrome
• The need for blood transfusions.
• It should still be used only on a named patient basis with close haematological supervision.
Bone marrow transplantation:
• Haematopoietic stem cell transplantation is potentially curative but is currently used only in patients with a severe clinical course and a matched sibling donor.
• Its use is limited by the toxicity and the availability of suitable donors.
Management

Treatment of acute chest syndrome:
• Treatment includes• Inspired oxygen,• Incentive spirometry
(also used for pain crises with back or chest pain)
• Continuous positive airways pressure and exchange transfusion.
• Occasionally ventilation may be necessary.
• Antibiotics are given using a combination of a macrolide with I/V cephalosporin.
• Hydroxycarbamide decreased the episodes of acute chest syndrome in one multicentre study.
• Periodic transfusion is also effective in preventing recurrences.
Management

Treatment of priapism:
• Priapism is an emergency requiring hydration and analgesia.
• In minor episodes, bladder emptying, exercise such as jogging, warm baths and analgesia may help abort an attack.
• Oral etilefrine may reduce the frequency of stuttering priapism.
• In a prolonged episode, aspiration and irrigation of the corpora cavernosa with adrenaline (epinephrine) or etilefrine is now the treatment of choice.
Management

Treatment of priapism :
• Children and their carers should be advised to seek treatment early and should attend hospital as an emergency if priapism persists for more than two hours.
Contraception:• Hormone and barrier
methods are all acceptable choices but intrauterine devices are not recommended, as they may be associated with uterine bleeding and infection.
• Depot contraceptive is safe and has been found to improve the blood picture and reduce pain crises.
Management

Painful crises• Many episodes of
uncomplicated acute pain can be managed at home with simple analgesia.
• Pain experienced in a vaso-occlusive crisis results from oxygen deprivation of tissues and avascular necrosis of the bone marrow.
• Dactylitis is a common early manifestation that may occur before the age of 6 months.
• It is uncommon after 2 years of age.
• The risk of vaso-occlusive episodes is increased by exposure to cold, fever, and dehydration.
• Over 90% of hospital admissions for patients with sickle cell disease are for painful crises.
Management

Painful crises:• Hydroxycarbamide can reduce the frequency of
painful crises in SCD.• Avoid exposure to cold, fever, dehydration and
stress.• A simple analgesic ladder starting with paracetamol
and/or ibuprofen.• Weak opioids (e.g., codeine or dextropropoxyphene)
for patients with mild pain.• Admit patients if pain does not subside promptly, if
there is a need for strong opioid treatment, or if fever, pallor or signs of respiratory compromise are noted.
• Benzodiazepines may be helpful to reduce anxiety
Management

Prognosis• Clinical severity and
prognosis are very variable, ranging from survival into the 60s and 70s to a severe disease with substantial organ damage and early death.
• Median life expectancy is currently 40-60 years in high-income countries but much less in low-income areas.
• The most common cause of death in the first two years of life is infection, with or without splenic sequestration.
• In adults, common causes of death are cerebrovascular accidents, sepsis, acute chest syndrome and pulmonary hypertension
Complications