-
8/2/2019 Sign 88
1/46
Mm
A national clinical guideline
1 i 1
2 Mmutiwm 6
3 Mmutiwm 13
4 Mmutim 16
5 Mmuti
whh 18
6 imwh 22
7 rmmmm,, vh 25
8 dvmh 30
av 33
ax 34
r 38
J2006
88
copiesofallsignguidelinesareaVailableonlineatWWW.sign.ac.uk
Scottish Intercollegiate Guidelines Network
SIGN
-
8/2/2019 Sign 88
2/46
thmmmh-mm
keytoeVidencestateMentsandgradesofrecoMMendations
leVelsofeVidence
1++ High quality meta-analyses, systematic reviews of randomised
controlled trials(RCTs), or RCTs with a very low risk of bias
1+ Well conducted meta-analyses, systematic reviews of RCTs, or
RCTs with a lowrisk of bias
1 - Meta-analyses, systematic reviews of RCTs, or RCTs with a
high risk of bias
2++ High quality systematic reviews of case control or cohort
studiesHigh quality case control or cohort studies with a very low
risk of confounding orbias and a high robability that the
relationshi is causal
2+ Well conducted case control or cohort studies with a low risk
of confounding orbias and a moderate robability that the
relationshi is causal
2 - Case control or cohort studies with a high risk of
confounding or bias
andasignifcantriskthattherelationshipisnotcausal
3 Non-analytic studies, eg case reorts, case series
4 Exert oinion
GRADES OF RECOMMENDATION
Note: The grade of recommendation relates to the strength of the
evidence on which therecommendation is based. It does not reect the
clinical importance of the recommendation.
a At least one meta-analysis, systematic review of RCTs, or RCT
rated as 1++
and directly alicable to the target oulation; or
A body of evidence consisting rincially of studies rated as 1+,
directly alicableto the target oulation, and demonstrating overall
consistency of results
b A body of evidence including studies rated as 2++
, directly alicable to the targetoulation, and demonstrating
overall consistency of results; or
Extraolated evidence from studies rated as 1++ or 1+
c A body of evidence including studies rated as 2+, directly
alicable to the targetoulation and demonstrating overall
consistency of results; or
Extraolated evidence from studies rated as 2++
d Evidence level 3 or 4; or
Extraolated evidence from studies rated as 2+
GOOD pRACTICE pOINTS
Recommended best ractice based on the clinical exerience of the
guidelinedeveloment grou
Sulementary material available on our website www...
-
8/2/2019 Sign 88
3/46
Scottish Intercoegite Guideines Network
Mngement o susected bcteriurinr trct inection in duts
A natinal clinical guideline
Jul 2006
-
8/2/2019 Sign 88
4/46
Scttish Intecllegiate Guidelines NetwkISBN 1 899893 79 2Fist
published 2006
SIGN cnsents t the phtcping f this guideline f thepupse f
ipleentatin in NHSSctland
Scottish Intercoegite Guideines Network28 Thiste Street,
Edinburgh EH2 1EN
www.sign.c.uk
-
8/2/2019 Sign 88
5/46
1 INTRODUCTION
1 Introduction
1.1 THE NEED fOR a GUIDElINE
Uina tact infectin (UTI) is the secnd st cn clinical indicatin f
epiicalantiicbial teatent in pia and secnda cae, and uine saples
cnstitute the lagestsingle categ f speciens exained in st edical
icbilg labaties. Healthcaepactitines egulal hae t ake decisins abut
pesciptin f antibitics f uina tactinfectin. Citeia f the diagnsis f
uina tact infectin a geatl in the UK, dependingn the patient and
the cntext. Thee is cnsideable eidence f pactice aiatin in use
fdiagnstic tests, intepetatin f signs spts and initiatin f
antibitic teatent, 2-5with cntinuing debate egading the st apppiate
diagnsis and anageent.,6
The diagnosis of UTI is particularly difcult in elderly
patients, who are more likely to haveasptatic bacteiuia as the get
lde.7 The pealence f bacteiuia a be s high thatuine cultue ceases t
be a diagnstic test.8 Eldel institutinalised patients fequentl
eceieunnecessa antibitic teatent f asptatic bacteiuia despite clea
eidence f adese
effects with no compensating clinical benet.9,0
Existing eidence based guidelines tend t fcus n issues f
antibitic teatent (dug selectin,dse, duatin and ute f adinistatin)
with less ephasis n clinical diagnsis theuse f nea patient tests ae
liited t adult, nn-pegnant wen with uncplicated,sptatic UTI.,2
F patients with spts f uina tact infectin and bacteiuia the ain
ai f teatentis elief f spts. Secnda utces ae adese effects f
teatent ecuence fspts. F asptatic patients the ain utce f teatent
is peentin f futuesptatic episdes.
Unnecessa use f tests and antibitic teatent a be iniised b
deelping sipledecisin ules, diagnstic guidelines the educatinal
inteentins.3-6 Pudent antibitic
pescibing is a ke cpnent f the UKs actin plans f educing
antiicbial esistance.7,8Unnecessary antibiotic treatment of
asymptomatic bacteriuria is associated with signicantlyinceased isk
f clinical adese eents.9,20
1.2 REMIT Of THE GUIDElINE
This guideline pides ecendatins based n cuent eidence f best
pactice inthe anageent f adults with cunit acquied uina tact
infectin. It includes adultwen (including pegnant wen) and en f all
ages, patients with cathetes and patientswith cbidities such as
diabetes. It excludes childen and patients with hspital
acquiedinfectin. The guideline des nt addess pphlaxis t peent UTI
afte instuentatin suge, teatent f ecuent UTI.
This guideline will be f inteest t healthcae pfessinals in pia
and secnda cae,ofcers in charge of residential and care homes,
antibiotic policy makers, clinical effectivenessleads, caes and
patients.
Additinal epideilgical and statistical infatin t accpan this
guideline is aailableas suppleenta ateial n the SIGN website
www.sign.c.uk
-
8/2/2019 Sign 88
6/462
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
1.3 DEfINITIONS
asymptomaticbacteriuria
pesence f bacteiuia in uine eealed b quantitatie cultue icscp in
a saple taken f a patient withut an tpical sptsf lwe uppe uina tact
infectin. In cntast with sptatic
bacteriuria, the presence of asymptomatic bacteriuria should be
conrmedb tw cnsecutie uine saples.2
bacteraemia pesence f bacteia in the bld diagnsed b bld
cultue.
bacteriuria pesence f bacteia in uine eealed b quantitatie
cultue icscp.
empirical treatment treatment based on clinical symptoms or
signs unconrmed by urinecultue.
haematuria bld in the uine eithe isible (acscpic haeatuia)
inisible(icscpic haeatuia).
long term catheter an indwelling cathete left in place f e 28
das.
lower urinary tractinfection (LUTI)
eidence f uina tact infectin with spts suggestie f cstitis(dsuia
fequenc withut fee, chills back pain).
medium termcatheter
an indwelling cathete left in place f 7-28 das.
near patient testing tests that ae dne at the pint f cnsultatin
and d nt hae t be sentt a labat.
pyuria occurrence of 104 white bld cells (WBC)/l in a feshl
idedspecien f uine.22 Highe nubes f WBC ae ften fund in
healthasptatic wen. Puia is pesent in 96% f sptatic patientswith
bacteiuia f >05 cln fing units (cfu)/l, but nl in
-
8/2/2019 Sign 88
7/463
1 INTRODUCTION
1.4 KEy MESSaGES aBOUT BaCTERIal UTI
Bcteriuri is not disese
The normal ora of the human body are extremely important as a
key part of host defencesagainst infection and because of their
inuence on nutrition.23
In peple less than 65 eas f age bacteiuia is abnal in the sense
that st pepled nt suffe f it (see Table 1). Bacteiuia is cn in se
ppulatins finstitutinalised wen24 and peple with lng te indwelling
uina cathetes(see section 5).
Tests or bcteriuri or uri do not estbish the dignosis o UTI
The diagnsis f UTI is piail based n spts and signs (see section
2.1).
Tests that suggest pe the pesence f bacteia white cells in the
uine a cntibuteadditinal infatin t inf anageent but ael hae iptant
iplicatins fdiagnsis (see sections 2.2, 3.1.3, 4.1, 5.2).
Bcteriuri one is rre n indiction or ntibiotic tretment
Bacteiuia can nl be an abslute indicatin f antibitic teatent
when thee is cnincingeidence that eadicatin f bacteiuia esults in
eaningful health gain at acceptableisk (see sections 2.4, 5.3,
5.4). In paticula, in eldel patients, asptatic bacteiuia iscommon
and there is evidence that treatment is more harmful than
benecial.9,0 In cntast,duing pegnanc thee is eidence that teatent f
bacteiuia des e gdthan ha.25
The ain alue f uine cultue is t identif bacteia and thei
sensitiit t antibitics (seesections 2.3, 2.4.1, 3.1.2, 4.1,
5.4.1).
Indiect indicats f the pesence f bacteia (f exaple, uina
nitites) ae likel t beuch less aluable than uine cultue (see
sections 2.2.3, 3.1.3, 4.1, 5.2.2).
There is risk o se ositie resuts in tests or dignosis o
bcteriuri other thn thegod stndrd
The gld standad test f diagnsis f bacteiuia is cultue f bladde
uine btained bneedle aspiatin f the bladde as it iniises the isk f
cntainatin f the uinespecien (see section 3.1.2).
All the techniques (uethal cathete and idstea speciens f uine)
ca a highe iskf cntainatin and theefe pduce se false psitie esults
(see section 3.1.2).
The signicance of false positive results is greatest when
testing for bacteriuria in peoplewith lw pe-test pbabilit (f
exaple, sceening f asptatic bacteiuia in therst trimester of
pregnancy, see section 3.1.2).
Routine urine cuture is not required to mnge lUTI in women
Wen with sptatic LUTI shuld eceie epiical antibitic teatent
(see section 2.4.1).All uine saples taken f cultue will be f
patients that ae nt espnding t teatentand will bias the esults f
sueillance f antibitic esistance (see section 7.4).
-
8/2/2019 Sign 88
8/464
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
1.5 EpIDEMIOlOGy
.5. PrEvALENCE oF ASymPTomATIC BACTErIUrIA
In wen asptatic bacteiuia beces inceasingl cn with age. The
liited data
abut health en shws that the pealence f bacteiuia als inceases
with age, althughthe pealence in en is alwas lwe than f wen f the
sae age 26-28 (see Table 1 andsupplementary material section
S2.1.2).
Table 1: Prevalence of asymptomatic bacteriuria in adult men and
women
Countr age (ers) Men (%) Women (%)
Japan26 50-59 0.6 2.8
60-69 .5 7.4
70+ 3.6 0.8
Sweden27 72 6.0 6.0
79 6.0 4.0
Sctland28 65-74 6.0 6.0
>75 7.0 7.0
.5.2 rISK FACTorS For ASymPTomATIC BACTErIUrIA
Table 2: Risk factors for asymptomatic bacteriuria
Risk ctor Eect on reence o smtomtic bcteriuri
Feale sex Inceases pealence (see Table 1).
Sexual actiit ma incease pealence (highe in aied wen than in
nuns, 29see supplementary material section S2.1.1).
Cbid diabetes Inceases pealence in wen less than 65 eas f age
withdiabetes f 2-6% t 7.9-7.7%.30-34
Age Inceases pealence in wen and en26-28,35-38 (see Table 1
andsupplementary material section S2.1.2).
Institutinalisatin Inceases pealence (in peple e 65 eas f age) f
6-6% t25-57% f wen9,39-42 and f-6% t 9-37% f en.40-43
Pesence f cathete 3-6% f peple acquie bacteiuia with ee da f
catheteisatin.All patients with lng te cathetes hae
bacteiuia.43,44
.5.3 PrEvALENCE oF SymPTomATIC BACTErIUrIA
Combined gures from nine studies show that women under 50 years
of age with acute symptomssuch as dsuia, ugenc fequenc (suggesting
lwe uina tact infectin) lin pain(suggesting uppe uina tact
infectin) ae exteel likel t hae bacteiuia (see Table3 and
supplementary material section S2.2)45-53 The pealence f sptatic
bacteiuia inpegnant wen, en and catheteised patients is discussed
in sectins 3., 4. and 5..
Table 3: Prevalence of bacteriuria in non-pregnant women under
50 years of age with acutesymptoms of UTI45-53
Tot numbero women
Number withbcteriuri
% withbcteriuri
lowercondence
inter (CI)
Uercondence
inter (CI)4,35 2,960 7.6% 70.2% 73.0%
-
8/2/2019 Sign 88
9/465
1 INTRODUCTION
1.6 STaTEMENT Of INTENT
This guideline is nt intended t be cnstued t see as a standad f
edical cae.Standads f cae ae deteined n the basis f all clinical
data aailable f an indiidualcase and are subject to change as
scientic knowledge and technology advance and patterns of
cae ele. Adheence t guideline ecendatins will nt ensue a
successful utce inee case, n shuld the be cnstued as including all
ppe ethds f cae excludingthe acceptable ethds f cae aied at the sae
esults. The ultiate judgeent egadinga paticula clinical pcedue
teatent plan ust be ade b the apppiate healthcaepfessinal in light
f the clinical data pesented b the patient and the diagnstic and
teatentoptions available. It is advised, however, that signicant
departures from the national guideline an lcal guidelines deied f
it shuld be full dcuented in the patients case ntesat the tie the
eleant decisin is taken.
-
8/2/2019 Sign 88
10/466
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
2++
2++
2++
2 Mngement o bcteri UTI in dut women
The anageent f sptatic bacteial UTI in adult nn-pegnant wen is
suaised inAnnex (LUTI) and Annex 2 (UUTI).
2.1 DIaGNOSIS
Spts suggestie f acute uina tact infectin ae ne f the st cn
easns fwen t isit healthcae pfessinals. Althugh the clinical
encunte tpicall inles taking ahist and pefing a phsical exainatin,
the diagnstic accuac f the clinical assessentf UTI eains
uncetain.2,54
The pi pbabilit f bacteiuia in thewise health wen wh pesent t
thei genealpactitine (GP) with spts f acute UTI is estiated at
between 50-80%. 2
If dsuia and fequenc ae bth pesent, then the pbabilit f UTI is
inceased t >90%and epiical teatent with antibitic is
indicated.2
If aginal dischage is pesent, the pbabilit f bacteiuia falls.
Altenatie diagnses such assexuall tansitted diseases (STDs) and
ulaginitis, usuall due t candida, ae likel andpelic exainatin is
indicated.2 rae causes include lcal aginal and ceical
pathlgincluding esins and e ael cance.
C In otherwise heth women resenting with smtoms or signs o UTI,
emirictretment with n ntibiotic shoud be considered.
C In women with smtoms o gin itch or dischrge, eore terntie
dignosesnd consider eic emintion.
The pesence f back pain fee inceases the pbabilit f UUTI and
uine cultue shuldbe cnsideed as the clinical isks assciated with
teatent failue ae inceased. Inceasingbacterial resistance means
that no antibiotic is sufciently reliable for empirical treatment
ofUUTI.55,56
In patients pesenting with spts signs f UTI wh hae a hist f fee
backpain the pssibilit f UUTI shuld be cnsideed. Epiical teatent
with an antibiticshuld be stated and uine cultue pefed t guide the
chice f antibitic.
2.2 NEaR paTIENT TESTING
Nea patient tests a include the appeaance f the uine saple,
icscp and testing beans f dipsticks.
2.2. APPEArANCE oF UrINEUrine turbidity has been shown to have a
specicity of 66.4% and sensitivity of 90.4% forpedicting sptatic
bacteiuia. When exained against a bight backgund, a tubid sapleis
psitie, wheeas a clea saple is negatie.57visual appeaance is pne t
bsee e anda nt be a useful disciinat.
2.2.2 UrINE mICroSCoPy
There is wide variation in sensitivity (60-100%) and specicity
(49-100%) of urine microscopyto predict signicant bacteriuria in
symptomatic ambulatory women.58,59
Nea patient testing b icscp aises cncens abut health and safet
at wk, aintenancef equipent and taining f staff which des nt justif
its use.
Uine icscp shuld nt be undetaken in clinical settings in pia
secnda cae.
-
8/2/2019 Sign 88
11/467
2++
+
2++
2 MaNaGEMENT Of BaCTERIal UTI IN aDUlT WOMEN
2.2.3 DIPSTICK TESTS
The qualit f eidence f nea patient testing with dipstick tests
(eagent stip tests) wasp.2,60 The cae setting aied acss the
studies, f exaple, accident and eegenc,genituina edicine and
hspital inpatients. Indiidual eagent espnses wee epted ina aiable
and incplete wa.
A eta-analsis f the accuac f dipstick testing t pedict UTI lked
at fu categies ftests: nitite nl; leuccte estease (LE) nl;
disjunctie paiing (dipstick psitie if eithe nitite LE bth ae
psitie) and cnjunctie paiing (dipstick psitie nl if bth nitite and
LEae psitie).60 The study found the disjunctive pair test to be
signicantly more accurate thanthe LE test alne (p=0.000). 60 A uine
saple psitie f dipstick tests f LE nitite is lesslikel t pedict
bacteiuia than cbinatins f spts and signs, paticulal cbinatinsof
conrmatory symptoms (dysuria, frequency) and absence of features
that suggest alternativediagnses (aginal dischage and
iitatin).2
Dipstick tests ae nl indicated f wen wh hae inial signs and spts
andwhse pi pbabilit f UTI is in the inteediate ange (aund 50%).
Whee nl nespt sign is pesent, a psitie dipstick test (LE nitite) is
assciated with a high
pbabilit f bacteiuia (80%) and negatie tests ae assciated with
uch lwe pbabilit(aund 20%).60
Negatie tests d nt exclude bacteiuia. A andised cntlled tial
(rCT) f nea patienttesting in adult wen wh wee sptatic but had a
negatie dipstick test shwed thatantibitics (tiethpi 300 g dail f
thee das) iped spts with the edianduatin f cnstitutinal spts being
educed b fu das. Althugh the pbabilit fUTI is educed t less than
20% b a negatie dipstick test, the eidence suggests that wenstill
derive symptomatic benet from antibiotics, number needed to treat
(NNT) of 4. 6 Fstatistical ethds see suppleenta ateial sectin S.
These issues shuld be cnsideedand explained t sptatic wen with a
negatie dipstick test. Clinical judgeent shuldbe used t decide
whethe t btain uine f cultue inite the patient t etun if sptspesist
wsen.60
B Distick tests shoud on be used to dignose bcteriuri in women
with imitedsmtoms nd signs(no more than two symptoms).
Women with imited smtoms o UTI who he negtie distick urinsis (LE
ornitrite) shoud be oered emiric ntibiotic tretment.
The risks and benets of empirical treatment should be discussed
with the patientnd mnged ccording.
I womn remins smtomtic ter singe course o tretment, she shoud
beinestigted or other otenti cuses.
No robust evidence was identied describing LE or nitrite testing
in elderly, institutionalisedpatients.
In eldel patients (e 65 eas f age), diagnsis shuld be based n a
full clinicalassessent, including ital signs.
-
8/2/2019 Sign 88
12/468
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
+
++
++
+
4
++
+
2.3 URINE CUlTURE
The quality of a urine sample will affect the ability to detect
bacteria and conrm a diagnosisf UTI. Speciens can be diided int
thse with high isk f cntainatin (clean catch idstea uine saples;
mSU), lw isk (supapubic aspiate; SPA peatiel btained
urine from ureter or kidney). Standard laboratory processing of
urine samples is conned toa single initial specien pe patient,
which detects cnentinal aebic bacteia, nallat a alue f05 cfu/l.
Thee is n bacteial cunt that can be taken as an abslute gldstandad
f the diagnsis f UTI.
The criterion for the presence of signicant bacteria was
established from early work comparingSPA against mSU speciens in
wen suffeing eithe f acute UUTI wh hadasptatic UTI duing pegnanc. A
single psitie mSU eliabl deteined the pesencef a UTI at 05 cfu/l in
80% f cases studied with tw saples iping this t 95%. 62-64
F wen expeiencing spts f uina tact infectin lwe nubes f
clnforming units may also reect signicant bacteria. A study
comparing SPA against MSUspeciens fund that the best diagnstic
citein in wen was 02 cfu/l (sensitiit 95%,specicity 85%).65
The labat intepetatin f a uine cultue depends upn a cbinatin f
facts. Theseinclude the nube f islates cultued and thei pedinance,
the specien tpe, the clinicaldetails, the pesence absence f puia
and the nubes f ganiss pesent. Cnentinallabat pactice in the UK
detects aebic bacteia at a alue f04 cfu/l.22
2.4 aNTIBIOTIC TREaTMENT
2.4. SymPTomATIC BACTErIUrIA, LUTI
In a andised cntlled tial f nn-pegnant wen with dsuia, fequenc
ugenc andpositive LE tests but no symptoms or signs of UUTI and no
signicant comorbidity, 95% had105 bacteria per ml of urine.
Treatment with a single dose of either cexime, co-trimoxazole
or ooxacin was equally effective.66
Anthe tial enlled nn-pegnant wen aged 5-54 with dsuia and
fequenc, anddetected pyuria (method not specied) but no symptoms or
signs of UUTI and no signicantcomorbidity. A three day regimen of
nitrofurantoin signicantly shortened time to resolutionf
spts.67
a Non-regnnt women with smtoms or signs o cute lUTI, nd either
high robbiito or roen bcteriuri, shoud be treted with
ntibiotics.
Thee t six das f antibitic teatent f uncplicated LUTI in wen
aged 60 e isas effectie as teatent f 7-4 das. 68,69
Guidelines f the Infectius Diseases Sciet f Aeica (IDSA) and
Health Ptectin
Agenc (HPA)55 ecend thee das teatent with tiethpi f LUTI. Thee
is edirect evidence for three days treatment with co-trimoxazole
but it is reasonable to infer thattrimethoprim is equally effective
as co-trimoxazole.
Thee das f teatent with nitfuantin has been shwn t be effectie
in nn-pegnantadult wen with uncplicated UTI.67 The IDSA ecends seen
das teatent withnitfuantin. Thee is n diect eidence cpaing thee das
nitfuantin with seendas nitfuantin.
B Non-regnnt women o n ge with smtoms or signs o cute lUTI shoud
betreted with trimethorim or nitrourntoin or three ds.
Wen with enal ipaient shuld nt be teated with nitfuantin as:
an effectie cncentatin f antibitic in the uine is nt achieablea
txic cncentatin f antibitic can ccu in the plasa.
-
8/2/2019 Sign 88
13/469
4
+
4
++
4
+
2 MaNaGEMENT Of BaCTERIal UTI IN aDUlT WOMEN
Uina pH affects the actiit f nitfuantin. Nitfuantin is effectie
against E. coli ata cncentatin f 00 g/l as the cncentatin f
antibitic geatl exceeds the iniuinhibit cncentatin (mIC lwest
cncentatin f antibitic that egulal inhibits gwthf the bacteiu in
it). The mIC inceases twent fld f pH5.5 t pH8.0 (see Table 4)
70
and at pH8.0 bacteial gwth ccus with 25 g/l f nitfuantin. A
siila situatin is seen
with P. mirabilis althugh it has a highe mIC than st stains fE.
coli.
D Women with lUTI, who re rescribed nitrourntoin, shoud be dised
not to tkekinising gents (such as potassium citrate).
Table 4: The effect of pH on the MIC of nitrofurantoin on E.
coli and P. mirabilis 70
Minimum inhibitor concentrtion o nitrourntoin (mg/)
H 5.5 H 7.0 H 8.0
E. coli 2.5 0.0 50.0
P. mirabilis 5.0 50.0 00.0
Resistance is increasing to all of the antibiotics used to treat
UTI and there is no clear rst choicealtenatie t tiethpi
nitfuantin.
B ptients who do not resond to trimethorim or nitrourntoin shoud
he urine tkenor cuture to guide chnge o ntibiotic.
Quinlnes shuld nt be used f epiical teatent f LUTI.
2.4.2 SymPTomATIC BACTErIUrIA, UUTI
Uppe uina tact infectin can be accpanied b bacteaeia, aking it a
life theateninginfectin.
Nitfuantin is an ineffectie teatent f UUTI because it des nt
achiee effectiecncentatins in the bld. resistance t tiethpi is t cn
t ecend thisdug f epiical teatent f a life theatening
infectin.55
One week of treatment with ciprooxacin is as effective as two
weeks treatment with co-trimoxazole.7
a Non-regnnt women with smtoms or signs o cute UUTI shoud be
treted withciprooxacin for seven days.
As resistance to quinolones is increasing, the HPA suggests that
patients started on ciprooxacinshuld hae uine sent f cultue and
that patients shuld be aditted t hspital if thee isn espnse t
teatent within 24 hus.55
D Urine shoud be tken or cuture beore immedite emiric tretment
is strted ndtretment chnged i there is n indequte resonse to the
ntibiotic.
Alternative treatments include co-trimoxazole, pivmecillinam,
co-amoxiclav andcexime.
one week f teatent with piecillina is less effectie than tw
weeks teatent.
Evidence about the effectiveness of less than two weeks
treatment with co-amoxiclav, ceximeand co-trimoxazole is
lacking.
Patients shuld be aditted t hspital if ssteic spts appea.
-
8/2/2019 Sign 88
14/460
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
++
+
+
+
++
++
2.4.3 ASymPTomATIC BACTErIUrIA
There is no evidence that treatment of asymptomatic bacteriuria
in adult women signicantlyeduces the isk f sptatic episdes, eithe
in wen withut cbidit withundeling diabetes pia bilia
cihsis.20,72,73
In women with diabetes, antibiotic treatment of asymptomatic
bacteriuria signicantly increasesthe risk of adverse events without
signicant clinical benet, such as shortening duration ofspts.20
a Non-regnnt women with smtomtic bcteriuri shoud not receie
ntibiotictretment.
In eldel wen (e 65 eas f age), teatent f asptatic bacteiuia des
nteduce talit significantl educe sptatic episdes.9,74 Antibitic
teatentsignicantly increases the risk of adverse events, such as
rashes and gastrointestinal symptoms(number needed to harm; NNTH 3;
condence interval; CI 2 10. For statistical methods
seesupplementary material section S1).19
a Eder women (over 65 years of age) with smtomtic bcteriuri
shoud not receientibiotic tretment.
2.5 NON-aNTIBIOTIC TREaTMENT
recuent UTIs ae a cn and debilitating pble. repeated plnged
teatent withantibitics is likel t cntibute t the pble f antiicbial
esistance. Effectie altenatiest antibitics hae the ptential t ipe
public health.
Altenaties t antibitics ffe an pptunit f patients t self anage
the peentin fecuent UTIs, which a ipe thei qualit f life.
2.5. CrANBErry ProDUCTS
Canbe pducts (juice, tablets, capsules) ae nt egulated and the
cncentatin f actieingredients is not known. Concentrations may also
uctuate between batches of the samepduct.
mst f the high stength pepaatins (tablet/capsule f) in the UK
qute 200 g f canbeextact, equialent t 5,000 g f fesh canbeies (25:
cncentatin).
Thee is gd eidence t suppt the effectieness f canbe pducts f
peentingsptatic UTI in adult wen with a hist f ecuent UTI (NNT t
peent nesptatic infectin in six nths 6.4, CI 3.7-25.9.75For
statistical methods see supplementarymaterial section S1).The
effectieness f canbe pducts in the patients is nt knwn.The ptial
dse and ute f adinistatin has nt been addessed.
Thee has been n diect cpaisn between canbe pducts and antibitic
pphlaxis fpeenting ecuent UTI. The NNTs f canbe pducts ae highe
than f nightl antibiticpphlaxis f six nths,76 pstcital antibitic
pphlaxis f six nths.77
a Women with recurrent UTI shoud be dised to tke crnberr roducts
to reducethe requenc o recurrence.
Wen shuld be adised that canbe capsules a be e cnenient than
juiceand that high stength capsules a be st effectie.
Thee is n eidence t suppt the effectieness f canbe pducts f
teating sptaticepisdes f UTI.78
N seius adese effects t canbe pducts wee epted, althugh the high
dp ut
ate in clinical tials suggests that lng te teatent with canbe
pducts a nt be welltleated. The echanis f actin f canbe pducts is
unclea.
-
8/2/2019 Sign 88
15/46
4
++
++
++
+
2 MaNaGEMENT Of BaCTERIal UTI IN aDUlT WOMEN
B 2003 the Cittee n Safet f medicines (CSm) eceied 2 epts f
suspectedinteactins inling wafain and canbe juice. In eight f these
cases thee was an inceasein International Normalized Ratio (INR) of
the prothrombin time.79
In octbe 2004 the CSm adised that patients taking wafain shuld
aid taking canbeproducts unless the health benets are considered to
outweigh any risks.
D Patients taking warfarin should avoid taking cranberry
products unless the health benetsre considered to outweigh n
risks.
Inceased edical supeisin and INr niting shuld be cnsideed f an
patienttaking wafain with a egula intake f canbe pducts.
one clinical tial addessed the cst effectieness f canbe pducts f
peenting UTI innn-pegnant wen (see supplementarymaterialsection
S4.1).80
Wen with ecuent UTI shuld be adised that canbe pducts ae nt
aailablen the NHS, but ae eadil aailable f phaacies, health fd
shps, hebalistsand supeakets.
2.5.2 mETHENAmINE HIPPUrATE
A systematic review of methenamine hippurate identied
considerable heterogeneity betweentials and cncluded that
intepetatin f these data shuld be dne cautiusl, due t thesmall
sample sizes and poor methodology of the studies involved.8
methenaine hippuate a be effectie at peenting UTI in patients
withut knwn uppeenal tact abnalities. Adese eents caused b
ethenaine wee ae.8
Tw tials shw that ethenaine is less effectie at peenting sptatic
UTI than nightlpphlaxis with eithe nitfuantin tiethpi.82
B Methenmine hiurte m be used to reent smtomtic UTI in tients
without
known uer ren trct bnormities.
2.5.3 oESTroGEN
Genituina atph a incease the isk f bacteiuia and the le f estgen
theap ineducing the isk f sptatic UTI has been inestigated.
Evidence for the efcacy of oestrogen in comparison with placebo
is inconsistent. There is goodeidence that this teatent is less
effectie than antibitic pphlaxis.83 A tial cpaingnine nths teatent
with al nitfuantin esus estil pessaies in pst enpausalwomen
reported a signicantly reduced risk of symptomatic UTI with
nitrofurantoin.83 Twssteatic eiews f aginal estgen adinistatin bth
epted cnsideable unexplainedheterogeneity of results with some
studies reporting signicant reduction in risk of recurrent
UTI while others report no signicant effect or even a trend
towards harmful effects.84,85
a Oestrogens re not recommended or routine reention o recurrent
UTI inostmenous women.
Teatent with estgens a be apppiate f se wen.
2.5.4 ANALGESIA
N eidence was fund f the use f analgesics f sptatic elief f
uncplicatedUTIs.
Wen with uncplicated UTIs a wish t use e the cunte eedies t t
andeliee spts.
-
8/2/2019 Sign 88
16/462
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
2.6 REfERRal
recuent UTI is a cn easn f efeal f wen t ulgists but n eidence
wasfund descibing citeia f efeal abut which inestigatins t
undetake.
Thee is gd eidence t suppt peentin f ecuent bacteial UTI in wen
with
antibitics82 and canbe pducts (see section 2.5.1). These
stategies shuld be expledbefe efeal f specialist inestigatin.
2.7 COST-EffECTIvE TREaTMENT IN pRIMaRy CaRE
Thee ae tw ke issues in the ecnic ealuatin f stategies f
anagingsuspected UTI:
Antibitics accunt f nl 3% f the ttal pia cae csts f patients
with lweuina tact infectin and nl 2-8% f the csts f patients with
uppe uina tactinfectin. visits t the GP accunt f the ajit f
csts.86
manageent stategies that iniise healthcae csts a tansfe csts t
the patient.A decisin analsis f anageent stategies f acute
uncplicated lwe uina tact
infectin in pia cae cncluded that epiic antibitic teatent withut
uine cultuewas the pefeed stateg.87 This stateg, hwee, plngs the
aeage duatin fspts because it takes lnge t identif wen whse
infectins ae caused b antibiticesistant bacteia.86
2.7. GP CoNSULTATIoN
Thee decisin analses cpaing epiic antibitic teatent with withut
uine cultuecncluded that taking a uine cultue utinel f all patients
will cst e but is likel teduce spt das b between 0.04 and 0.32
das.87-89This is achieed thugh a cbinatinf educing isk f adese
effects, b stpping teatent if the cultue is negatie and
ealidentication of infections caused by antibiotic resistant
bacteria. There is considerable variationin the estiates f the
inceental cst effectieness f uine cultue.
one stud estiated the cst pe spt da peented as 25.89The estiated
cst pe QALy(qualit adjusted life ea) gained was 25,000.89 It is
unlikel that utine cultue f uine willbe cst effectie unless the
pealence f bacteiuia in sptatic wen is
-
8/2/2019 Sign 88
17/463
+
3 MaNaGEMENT Of BaCTERIal UTI IN pREGNaNT WOMEN
3 Mngement o bcteri UTI in regnnt
women
The anageent f sptatic bacteial UTI in pegnant wen is suaised in
Annex 3.
3.1 DIaGNOSIS
3.. SymPTomATIC BACTErIUrIA
Symptomatic bacteriuria occurs in 1720% of pregnancies.25 Thee
ae pathphsilgicalgunds t suppt a link t pe-labu, peatue uptue f
ebanes (PProm) and pe-telabu.92 Unteated uppe uina tact infectin in
pegnanc als caies well dcuentedisks f bidit, and ael, talit t the
pegnant wan.92
Two to nine percent of pregnant women are bacteriuric in the rst
trimester, a similar prevalencet nn-pegnant wen f the sae age.2,93
10-30% of women with bacteriuria in the rsttieste deelp uppe uina
tact infectin in the secnd thid tieste.
3..2 THE GoLD STANDArD For DIAGNoSIS IN PrEGNANCy
The gld standad ethd f diagnsis f bacteiuia is cultue f uine
btained b supapubicneedle aspiatin. A cathete specien f uine is
less eliable than supapubic needle aspiatin,althugh e eliable than
tw mSU saples.94man studies ept using single mSU saples.In women
with acute symptoms of UTI the presence of 105 bacteia pe l f a
single mSUsample has about 80% specicity in comparison with the
gold standard while a single specimen(mSU CSU) has a false psitie
ate f up t 40% f diagnsis f asptatic bacteiuiain pegnanc(see
supplementary material section S3.1).94,95
3..3 NEAr PATIENT TESTING
A ssteatic eiew f studies cpaing uine cultue with nea patient
tests epted thatn studies used the gld standad f diagnsis f
asptatic bacteiuia in pegnanc.92 Inthe nl stud t establish the
diagnsis f bacteiuia with tw cnsecutie uine saples atthe rst
antenatal visit, 8.3% of pregnant women had asymptomatic
bacteriuria while 12.1%had a positive dipstick test with
sensitivity and specicity of 92.0% and 95.0%.96 Fie falsenegatie
dipstick tests wee f patients wh had bacteiuia with ga-psitie
bacteia (theegup B steptccci and tw enteccci) which d nt cause uppe
UTI, but ae iplicatedin causing peatue delie.
Dipstick testing (LE or nitrate) is not sufciently sensitive to
be used as a screening test. Urinecultue shuld be the inestigatin f
chice.
a Standard quantitative urine culture should be performed
routinely at rst antenatalisit.
a The presence of bacteriuria in urine should be conrmed with a
second urinecuture.
a Dipstick testing should not be used to screen for bacterial
UTI at rst or subsequentntent isits.
Dipsticks t test nl f pteinuia and the pesence f glucse in the
uine shuld beused for screening at the rst and subsequent antenatal
visits as a more cost-effectivealtenatie t ulti-eagent dipsticks
that detect the pesence f nitite, leuccte esteaseand bld in additin
t ptein and glucse.
-
8/2/2019 Sign 88
18/464
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
++
+
2+
+
4
++
3.2 aNTIBIOTIC TREaTMENT
rCTs addessing teatent f UTI in pegnant wen fequentl include
patients withasptatic bacteiuia and sptatic bacteiuia, uppe and lwe
UTI. Thee is ftenpoor denition of long term outcomes.
3.2. SymPTomATIC BACTErIUrIA
In pegnant wen with spts f bth UUTI and LUTI thee is eidence
that a ange fantibitic egiens achiee cue.97-0There is no clear
evidence of benet by reduction of longte enal daage pe-te labu as
st studies ae hetegeneus with espect t LUTIand UUTI and did not
specically address these outcomes.
Thee is n clea eidence that an paticula antibitic dsage egien
has an adantage.25
None of the studies addressed the risk of treatment, but apart
from the hazards of adverseeactins anaphlaxis caused b an
inapppiate antibitic, the isks ae likel t be sallcompared to the
proven benet.25
B pregnnt women with smtomtic UTI shoud be treted with n
ntibiotic.
A single uine saple shuld be taken f cultue befe epiic antibitic
teatent isstated.
Nitfuantin is nt an effectie teatent f UUTI because it des nt
achiee effectiecncentatins in the bld.55
refe t lcal guidance f the safest, cheapest, effectie antibitic
f pegnantwen.
Gien se antibitics ae txic in pegnanc, efe t the Bitish Natinal
Fula(BNF) f cntaindicatins.
Gien the isks f sptatic bacteiuia in pegnanc, a uine cultue
shuld bepefed seen das afte cpletin f antibitic teatent as a test f
cue.
3.2.2 ASymPTomATIC BACTErIUrIA
A ssteatic eiew cncluded that antibitic teatent f asptatic
bacteiuia in pegnanceduces the isk f uppe uina tact infectin, pe-te
delie and lw bith weight babies(see supplementary material section
S3.1).02
mst f the tials in this eiew wee f cntinuus antibitic theap f
diagnsis fasptatic bacteiuia until the end f pegnanc.02 This is nt
standad cae in the NHS inSctland, whee asptatic bacteiuia is usuall
teated with a sht cuse (3-7 das) fantibitics. The eidence suggests
that 3-7 das teatent is as effectie as cntinuus
antibitictheap.02
There is insufcient evidence to compare the effectiveness of
single dose treatment with a 3-7da cuse03 a thee da with a seen da
cuse.
a asmtomtic bcteriuri detected during regnnc shoud be treted
with nntibiotic.
refe t lcal guidance f the safest, cheapest, effectie antibitic
f pegnantwen.
Thee is n need f epiical teatent in this gup f patients as all
wen hae uine cultuebefe teatent.
The benets and risks of antibiotic treatment of symptomatic
bacteriuria in pregnant womenappl equall t pegnant wen with
asptatic bacteiuia.
-
8/2/2019 Sign 88
19/465
2+
10 not repeated
& (57 not)
conrmed
Treated
bacteriuric:2.8% UUTI
Eradicationn=53 (75%)
Recurrencen=6 (8%)
Untreated
bacteriuric:28% UUTI
n=1575
Non-
bacteriuric:0.31% UUTI
UUTI (No) 2 0 0 2 5
Conrmed
n=77
Failuren=11 (16%)
Not treated
n=7
Treated
n=70
Negativen=1508
Positiven=144
Screeningn=1,652
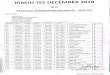
3.3 SCREENING DURING pREGNaNCy
A lage bseatinal stud denstated the effectieness f a sceening
pgaebased on diagnosis of asymptomatic bacteriuria with two urine
cultures in the rst trimester(see Figure 2).95
Figure 2: Frequency of asymptomatic bacteriuria, response to
treatment and subsequentdevelopment of upper urinary tract
infection. Adapted from Gratacos et al 1994. 95
C Women with bacteriuria conrmed by a second urine culture
should be treated andhe reet urine cuture t ech ntent isit unti
deier.
Women who do not have bacteriuria in the rst trimester should
not have repeat urinecultues.
Thee is incnsistent eidence egading the cst effectieness f
sceening pegnant wenf asptatic bacteiuia (see supplementary
materialsection S4.2).92,95,04-06
3 MaNaGEMENT Of BaCTERIal UTI IN pREGNaNT WOMEN
-
8/2/2019 Sign 88
20/466
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
3
4
4 Mngement o bcteri UTI in dut men
The anageent f sptatic bacteial UTI in en is suaised in Annex
4.
4.1 DIaGNOSIS
Uina tact infectins in en ae geneall iewed as cplicated because
the esult fan anatic functinal anal instuentatin f the genituina
tact.07
Cnditins like pstatitis, chladial infectin and epididitis shuld
be cnsideed in thediffeential diagnsis f en with acute dsuia
fequenc and apppiate diagnstic testsshuld be cnsideed.
Thee is n eidence t suggest the best ethd f diagnsing bacteial
UTI in en. Eidencef studies f wen cannt be extaplated.
Uine icscp shuld nt be undetaken in clinical settings in pia
secnda
cae.
In all en with spts f UTI a uine saple shuld be taken f
cultue.
In patients with a hist f fee back pain the pssibilit f UUTI
shuld be cnsideedand uine cultue shuld guide the chice f
antibitic.
obtaining a clean-catch saple f uine in en is easie than in wen
and a cln cuntof 103 cfu/ml may be sufcient to diagnose UTI in a
man with signs and symptoms as longas 80% f the gwth is f ne
ganis.08
A threshold of 103 cfu/l f diagnsing UTI is belw the theshld f
detectin f secnl used labat ethds, which nl detect between 04 and
05 cfu/l.
methds f detecting lwe leels f bacteia in uine saples shuld be
deelpedand ipleented.
The culture of expressed prostatic secretion and semen has no
clinical benet and is no longercn pactice.09
4.2 aNTIBIOTIC TREaTMENT
No high quality evidence for the treatment of bacterial UTI in
men was identied.
At least 50% f en with ecuent UTI0 and e 90% f en with febile
UTI haepstate inleent, which a lead t cplicatins such as pstatic
abscess chnicbacteial pstatitis.
-
8/2/2019 Sign 88
21/467
2+
+
4
2+
4 MaNaGEMENT Of BaCTERIal UTI IN aDUlT MEN
4.2. SymPTomATIC BACTErIUrIA
Given the difculty of excluding prostatitis in men with symptoms
suggestive of UTI, the currentstandad f cae is a tw week cuse f
antibitic likel t be effectie f pstatitis. Due ttheir ability to
penetrate prostatic uid, quinolones rather than nitrofurantoin or
cephalosporinsae indicated. A tw week cuse f teatent was shwn t be
as effectie as a fu week cusef patients with febile UTI.
C Bcteri UTI in men shoud be treted emiric with two week course
oquinoone.
Altenatie teatents include tiethpi, dexccline and c-axicla.
Eidence abut the effectieness f teatent with tiethpi, dexccline
and c-axiclais lacking.
Patients wh d nt espnd t antibitic teatent shuld be inestigated
fpstatitis.
4.2.2 ASymPTomATIC BACTErIUrIA
In eldel en (e 65 eas f age), teatent f asptatic bacteiuia des
nt educemortality or signicantly reduce symptomatic episodes.9,74
Antibiotic treatment signicantlyinceases the isk f adese eents,
such as ashes and gastintestinal spts (NNTH 3;CI 2 - 0.9 For
statistical methods see supplementary material section S1).
a Eder men (over 65 years of age) with smtomtic bcteriuri shoud
not receientibiotic tretment.
4.3 REfERRal
recuent UTI is a cn easn f efeal t ulgists. Thee ae n tials abut
theeffectieness f antibitics canbe pducts f peenting ecuent UTI in
en. Thee aen eidence based guidelines f efeal abut which
inestigatins t undetake.
Expet pinin suggests that en shuld be inestigated if the hae
spts f uppe uinatact infectin, fail t espnd t apppiate antibitics
hae ecuent UTI (tw eepisdes in thee nths).2
D Men shoud be reerred or uroogic inestigtion i the he smtoms o
uerurinr trct inection, i to resond to rorite ntibiotics or he
recurrentUTI.
Urodynamic techniques, such as pressure/ow videocystography
revealed signicant underlyinglower urinary tract abnormalities
(mainly involving bladder outow obstruction) in 80% of adult
ales pesenting with siple ecuent uina tact infectins, but withut
pi uinaspts disdes.3
renal and pst-id bladde ultasund and a kidnes, uetes and bladde
(KUB) plainX-a f the abden a be used t lk f eleant abnalities.
-
8/2/2019 Sign 88
22/468
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
++
3
5 Mngement o bcteri UTI in tients with
ctheters
5.1 DIaGNOSIS
Between 2% and 7% f patients with indwelling uethal cathetes
acquie bacteiuia each da,een with the applicatin f best pactice f
insetin and cae f the cathete.4 All patientswith a lng te
indwelling cathete ae bacteiuic, ften with tw e ganiss.5,6
The catheter provides a focus for bacterial biolm formation. The
majority of data comes fromstudies in eldel patients with lng te
indwelling cathetes. Thee is n eidence t suggestthat the pealence
in unge sht lng te catheteised patients, such as thse withultiple
sclesis spinal cd inju, is an diffeent.7
Duatin f catheteisatin is stngl assciated with the isk f
infectin. The lnge the catheteis in place the geate the likelihd f
infectin.8 Inteittent catheteisatin is assciatedwith a lwe
incidence f asptatic bacteiuia.7
The pesence f a sht lng te indwelling cathete is assciated with
a geate incidencef fee f uina tact igin. Fee withut an lcalising
signs is a cn ccuencein catheteised patients and uina tact infectin
accunts f abut a thid f theseepisdes.7,9,20 In patients with sht
lng te cathetes fee is assciated with a higheccuence f lcal uina
tact and ssteic cplicatins such as bacteaeia.7,9,2,22
Althugh talit appeas t be highe in patients with lng te
indwelling cathetes, theeis n causatie link with catheteisatin uina
tact infectin.23
Uina tact infectin is the st cn hspital acquied infectin in the
UK, accuntingf 23% f all infectins and the ajit f these ae
assciated with cathetes. 24 Catheteassciated UTI is the suce f 8% f
hspital acquied bacteaeia.25
In catheteised patients the cn ccuence f fee, the cnsistent
pesence f bacteiuia,and the aiable pesence f a bad ange f the
assciated clinical anifestatins (new nsetcnfusin, enal angle
tendeness supapubic pain, chills/igs etc) akes the diagnsis
fsymptomatic UTI difcult.24,26,27
Cuent suggested citeia f diagnsing UTI in catheteised patients
ae nt eidence based.26
A clinical algith f suspected UTI in catheteised and
nn-catheteised esidents in nusinghes suggests that the pesence f ne
f the fllwing spts shuld stiulate antibitictheap:28
new cstetebal tendeness
igs
new nset deliiu
fee geate than 37.9C .5C abe baseline n tw ccasins duing 2
hus.
No particular constellation of symptoms or clinical signs, for
example, fever or chills, new ank supapubic tendeness, change in
chaacte f uine wsening f ental functinalstatus, appeas t incease
the likelihd f a sptatic uina tact infectin in catheteisedpatients.
The psitie pedictie alue (PPv) f bacteiuia f febile uina tact
infectinidentied by clinical criteria has been measured as 11%.9The
st cn spt, fee,is a non-specic presenting symptom in symptomatic
urinary tract infection.7,9,2 The absencef fee des nt appea t
exclude uina tact infectin.
D Cinic smtoms or signs re not recommended or redicting the
ikeihood osmtomtic UTI in ctheterised tients.
-
8/2/2019 Sign 88
23/469
2+
2++
2+
3
++
+
5 MaNaGEMENT Of BaCTERIal UTI IN paTIENTS WITH CaTHETERS
In catheteised patients wh pesent with fee:
lk f assciated lcalising (lin supapubic tendeness) ssteic
featues
exclude the ptential suces f infectin
send ff an apppiatel taken uine saple f cultue t deteine the
infecting
ganis and susceptibilitiescnside antibitic theap taking int
accunt the seeit f the pesentatin andan cbid facts.
Uine saples shuld nl be sent f labat cultue if the patient has
clinical sepsis,nt because the appeaance sell f the uine suggests
that bacteiuia is pesent.
5.2 NEaR paTIENT TESTING
5.2. UrINE mICroSCoPy
The alue f icscp f uine saples f catheteised patients is liited
in diagnsingsptatic UTI as all patients will hae bacteiuia. Thee is
n elatinship between the leel
f puia and infectin in patients with indwelling cathetes, since
the pesence f the catheteinaiabl induces puia withut the pesence f
infectin.29
C lbortor microsco shoud not be used to dignose UTI in
ctheterised tients.
5.2.2 DIPSTICK TESTS
Sptatic UTI cannt be diffeentiated f asptatic bacteiuia n the
basis f uineanalsis with dipstick tests. Puia is cn in catheteised
patients and its leel has npedictie alue.29,30
Thee is n eidence t suggest that detecting puia b uine analsis
is f an aluein diffeentiating sptatic UTI f asptatic UTI
(bacteiuia) in catheteised
patients.29-3
B Distick testing shoud not be used to dignose UTI in
ctheterised tients.
5.3 aNTIBIOTIC pROpHylaxIS TO pREvENT CaTHETER RElaTED UTI
A eta-analsis f antiicbial pphlaxis f UTI in catheteised
patients with spinal cddsfunctin included patients with acute (less
than 90 das afte spinal cd inju) and nn-acute (geate than 90 das
afte spinal cd inju) spinal cd dsfunctin and neugenicbladde.32 The
ajit f patients had inteittent catheteisatin. Antiicbial
pphlaxisdid not signicantly decrease symptomatic infections.
Prophylaxis was associated with thereduction of asymptomatic
bacteriuria among acute patients (p
-
8/2/2019 Sign 88
24/4620
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
+
+
+
++
+
-
++
5.4 aNTIBIOTIC TREaTMENT
5.4. SymPTomATIC BACTErIUrIA
Symptoms that may suggest UTI in patients with catheters include
fever, ank or suprapubic
discft, change in iding pattens, nausea, iting, alaise
cnfusin.
26,28
No studies were identied that evaluated the prognostic value of
individual or combinations ofsigns spts, with the exceptin f fee.
The ccuence f febile episdes in patientswith lng te indwelling
cathetes is assciated with the deelpent f abnalities suchas calculi
and cplicatins in the kidne.33
Eidence f antibitic teatent f sptatic UUTI in nn-pegnant wen is
applicablet catheteised patients with sptatic UTI and has been
extaplated t gie the fllwinggd pactice pints (see section
2.4.2).
Catheteised patients with spts signs f acute UUTI shuld be
teated withciprooxacin or co-amoxiclav for seven days.
Patients shuld be aditted t hspital if ssteic spts, such as fee,
igs, chills,iting cnfusin appea.
Patients with lng te indwelling cathetes, wh hae the cathete
changed befe statingantibitic teatent f sptatic UTI, hae a deceased
duatin f fee, ae e likel tbe cued iped afte thee das and ae less
likel t hae ecuence f acute sptswithin ne nth f teatent.34
B ptients with ong term indweing ctheters shoud he the ctheter
chnged beorestrting ntibiotic tretment or smtomtic UTI.
Uine shuld be taken f cultue befe the cathete is changed and
teatent is stated.Teatent shuld be changed if the ganis is esistant
t the chsen antibitic.
5.4.2 ASymPTomATIC BACTErIUrIA
Single dse antibitic teatent f wen with asptatic bacteiuia afte
sht tecatheterisation signicantly reduces the risk of symptomatic
episodes in the subsequenttwo weeks (number needed to benet; NNTB
7, CI 4-25.20 For statistical methods seesupplementary material
section S1). Gien that the pealence f bacteiuia shuld be
-
8/2/2019 Sign 88
25/462
5.5 MaNaGEMENT Of BaCTERIal UTI IN paTIENTS WITH URINaRy
STOMaS
Thee is n eidence t suppt the anageent f bacteial UTI in
patients with uina stasbut issues that affect catheteised patients
ae likel t appl. The pealence f bacteiuia islikel t be 00% in
patients with uina stas. Cultue f uine f patients with spts
suggestie f UTI shuld nl be caied ut t test the susceptibilit f
ptential pathgens. Uine saples shuld nl be sent f labat cultue if
the patient has clinical sepsis,
nt because the appeaance sell f the uine suggests that bacteiuia
is pesent.
5 MaNaGEMENT Of BaCTERIal UTI IN paTIENTS WITH CaTHETERS
-
8/2/2019 Sign 88
26/4622
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
6 Inormtion or discussion with tients nd
crers
6.1 NOTES fOR DISCUSSION WITH paTIENTS aND CaRERS
The following points were drawn up by the guideline development
group to reect the issuesst likel t be f cncen t patients and caes
fllwing a diagnsis f suspected bacteialuina tact infectin in adult
nn-pegnant wen. These pints ae pided f use b healthpfessinals when
discussing bacteial UTI with patients and in guiding the pductin f
lcallpduced patient infatin ateials.
6.2 KEy ISSUES
Thee is a need t balance the accuac f a diagnsis with the speed
in which esults(and teatent, if necessa) ae delieed t the patient.
Patients get e fustated waitingfor ofcial results to merit
treatment of a painful, uncomfortable situation that is
preventingnal dail actiities.
man pfessinals ae inteested in the accuac f the assessent, in de
nt t pescibeinapppiate unnecessa teatent, which can plng spts.
Patients ae awae that dipsticks ae nt alwas accuate and that
waiting f labatanalsis can dela tie t diagnsis and teatent.
Patients knw that facts such as thei d and cunicatin f discft
als aeiptant in signalling infectin.
Patients peceie that the best healthcae pfessinals ae thse wh
cnside the factsthat the patient nds signal infection.
man patients want infatin and clea explanatin f questins such
as:
Why doesnt this treatment seem to be working?
How long until I feel better?
Can something alleviate my symptoms (and pain!) in the meantime,
or at least ensure a level
of comfort so that I can resume normal daily activities (for
example, go to work, sleep at
night)?
What could happen if I dont comply fully (for example, if I
forget to take the full course of
treatment)?
Will this drug react/interact with any other
drugs/medicines/herbal medicines I am taking?
6.3 GENERal aDvICE
Healthcae pfessinals shuld ffe:infatin n canbeies. Patients
shuld be adised that futhe eseach is equied tdeteine the best wa t
take canbeies, f exaple, juice, tablets, a cbinatin;in what
cncentatin; utinel peentatiel; and hw ften (see section 2.5.1).
adice n cplicated esus uncplicated infectins. The distinctin
between a3-da esus a 7-da cuse f pills and the easns f using ne the
the shuld alsbe explained t the patient. These issues culd affect
cncdance.
cntaceptin adice. This and the le f sexual actiit is a citical
issue f wen, andne which a affect cncdance. This issue shuld be
explicitl dealt with b healthcaepfessinals pescibing and dispensing
teatent.
a einde t patients and caes that the pesence f bacteiuia des nt
alwas indicatedisease. Especiall in eldel patients, asptatic
bacteiuia is a nal cnditin and
shuld nt be teated with antibitics.
-
8/2/2019 Sign 88
27/4623
6 INfORMaTION fOR DISCUSSION WITH paTIENTS aND CaRERS
Gien that thee is n cnclusie assciatin between lifestle facts,
such as diet, hdatin,clthing, tileting actiit and sexual actiit,
and susceptibilit t bacteial UTI in adult,nn-pegnant wen, thee is n
eidence t suppt healthcae pfessinals giing utineadice t patients
abut lifestle facts.40-43 Thee a be a link between secnd UTI
andsexual actiit.40
rutine adice abut adpting discntinuing an paticula lifestle
facts shuldnt be ffeed t patients with bacteial UTI.
F an indiidual with ecuent and/ cplicated uina tact infectin,
healthcaepfessinals a wish t discuss the featues f the patients wn
situatin which apaticulal cntibute t the pble.
6.4 SOURCES Of fURTHER INfORMaTION fOR paTIENTS aND CaRERS
age Concern Scotnd3 rse Steet, Edinbugh EH2 3DT
Tel: 03 220 3345 Feephne infatin line: 0800 00 99 66Website:
www.agecncensctland.g.uk
assocition or Continence adicem Ji Tance, Chaian ACA Sctland,
Bdes Pia Cae NHS TustNusing Seices, Dingletn Hspital, melse,
Selkikshie TD6 9HNTel: 0896 750027 Fax: 0896 75949
A natinal ganisatin wking twads aising standads f cntinence cae
with anpfessinal ebes ffeing adice and teatent.
Bdder pin Sndrome assocition54 Sutheland rad, Beledee, Kent DA7
6JrTel: 0208 30 8729
Website: www.b-p-s-a.g.uk
Pides infatin and suppt t suffees f bladde pain sndes (including
intestitialcstitis and the elated disdes/sndes).
Continence foundtion307 Hattn Squae, 6 Baldwins Gadens, Lndn ECN
7rJTel: 020 7404 6875 Helpline: 020 783 983 Fax: 020 7404 6876Eail:
[email protected] Website:
www.cntinence-fundatin.g.uk
offes expet adice t peple with bladde and bwel pbles, thei caes
and pfessinalsin the eld. The nurses who run the helpline also have
details of all incontinence advice servicesand f all pducts n the
UK aket.
Cstitis nd Oerctie Bdder foundtion76 High Steet, Stn Statfd,
Buckinghashie mK AHTel: 090 856 969Website: www.cbfundatin.g
Provides information, leaets and support to people with all
forms of lower urinary tract infectionand eactie bladdes.
fmi pnning nd Reroductie Heth CreThe Sandfd Initiatie, 6 Sandfd
Place, Sauchiehall Steet, Glasgw G3 7NBTel: 04 2 8600
fmi pnning assocition ScotndUnit 0, Fihill Business Cente, 76
Fihill rad, Glasgw G20 7BATel: 04 576 5088 Helpline: 04 576
5088(mnda t Thusda 9a - 5p, Fida 9a - 4.30p)
-
8/2/2019 Sign 88
28/4624
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
Incontct (Natinal Actin n Incntinence)ms Cath mcKeell, Pject
manage (Sctland), 3 Bwnshill Aenue,Catbidge, Lanakshie mL5 5JFTel:
0870 770 3248 Fax 0870 770 3248Eail: [email protected] Website:
www.incntact.g
Ais t pide infatin and suppt t peple affected b bladde and bwel
cntinenceproblems, to increase awareness about incontinence
difculties and encourage those affectedt seek pfessinal help.
Ntion Chidbirth TrustAlexanda Huse, oldha Teace, Actn, Lndn W3
6NHTel: 0870 7703236 Enqui Line: 0870 444 8707 Fax: 0870 770
3237Eail: [email protected] Website:
www.nctpegnancandbabcae.c
Ntion Kidne federtionHelpline: 0845 60 02 09
A chait un b kidne patients f kidne patients, it pides patient
suppt seices tpatients and thei failies.
NHS24Tel: 0854 24 24 24 Textphne: 800 0854 24 24 24Website:
www.nhs24.c
NHS 24 is a nurse-led helpline providing condential healthcare
advice and information.
pRODIGyWebsite: www.pdig.nhs.uk
A suce f eidence based clinical knwledge abut the cn cnditins
and sptsmanaged by primary healthcare professionals. Patient
information leaets form an integral part
f ProDIGy.
Urostom associtionHazel Pixley, National Secretary, Central
Ofce, 18 Foxglove Avenue, Uttoxeter,Staffdshie ST4 8UNTel: 0870 770
793 Fax: 0870 770 7932Eail: [email protected] Website:
www.uagbi.g
Womens Heth Concern ltd.Whitehall Huse, 4 Whitehall, Lndn SWA
2ByTel: 020 745 377Eail: [email protected] Website:
www.wens-health-cncen.g
Womens Heth52 Feathestne Steet, Lndn ECy 8rTHelpline: 020 7251
6333 (9.30am 1.30pm weekdays) Fax: 020 7250 4152Eail:
[email protected] [email protected]:
www.wenshealthlndn.g.uk
-
8/2/2019 Sign 88
29/4625
7 RECOMMENDaTIONS fOR IMplEMENTaTION, aUDIT, SURvEIllaNCE aND
RESEaRCH
7 Recommendtions or imementtion, udit,
sureince nd reserch
7.1 lOCal IMplEMENTaTION
Ipleentatin f natinal clinical guidelines is the espnsibilit f
lcal NHS ganisatinsand is an essential pat f clinical genance. It
is acknwledged that nt ee guideline canbe ipleented iediatel n
publicatin, but echaniss shuld be in place t ensue thatthe cae
pided is eiewed against the guideline ecendatins and the easns f
andiffeences assessed and, whee apppiate, addessed. These
discussins shuld inle bthclinical staff and anageent. Lcal
aangeents a then be ade t ipleent the natinalguideline in indiidual
hspitals, units and geneal pactices, and t nit cpliance. Thismay be
done by a variety of means including patient-specic reminders,
continuing educationand taining, and clinical audit. Ipleenting the
new geneal pactice cntact will pidepptunities t intduce such
eleents f gd pactice.
7.2 KEy aREaS fOR aUDIT
7.2. KEy ArEAS For AUDIT IN PrImAry CArE
The anageent f patients with acute uina spts shuld be audited
against theapppiate algith (see Annexes 1 to 4).
7.2.2 KEy ArEAS For AUDIT IN SECoNDAry CArE
Audit f clinical eidence f infectin in patients with lng te
cathetes wh hae beenteated with antibitics had cathete uine saples
sent f cultue.
Audit f eldel patients (tpicall cnfused, with a cugh, wh ae
psitie f nitite in
the uine) teated with augentin equialent and fuseide (s called
eldel cailfusegien) with n dcuented eidence f spts f UUTI LUTI.
7.3 IMplEMENTaTION aND aUDIT Of THE RECOMMENDaTIONS
7.3. mANAGEmENT oF BACTErIAL UTI IN ADULT WomEN
Recommendtion Imementtion or udit
2. C In otherwise heth women resentingwith smtoms or signs o
UTI, emirictretment with n ntibiotic shoud beconsidered.
Ipleentatin f cae pathwas in
pia and secnda cae includinginiu data t be ecded inassessing a
wan with spts fLUTI.
Audit f pactice against cae pathwa.
2. C In women with smtoms o gin itch ordischrge, eore terntie
dignoses ndconsider eic emintion.
2. In patients pesenting with spts signs f UTI wh hae a hist f
fee back pain the pssibilit f UUTI shuldbe cnsideed. Epiical
teatent with anantibitic shuld be stated and uine cultuepefed t
guide the chice f antibitic.
2.2.2 Uine icscp shuld nt be undetakenin clinical settings in
pia secnda
cae.
Eninental infectin cntl auditsin pia and secnda cae shuld
ensue that uine icscp is ntbeing undetaken.
-
8/2/2019 Sign 88
30/4626
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
Recommendtion Imementtion or udit
2.2.3 B Distick tests shoud on be used todignose bcteriuri in
women with imitedsmtoms nd signs (no more thn two
smtoms).
Ipleentatin f cae pathwas inpia and secnda cae includinginiu
data t be ecded inassessing a wan with spts fLUTI.
Audit f pactice against cae pathwa
2.2.3 B Women with imited smtoms o UTI whohe negtie distick
urinsis (lE ornitrite) shoud be oered emiric ntibiotictretment.
2.2.3 B The risks and benets of empirical treatmentshoud be
discussed with the tient ndmnged ccording.
2.2.3 B I womn remins smtomtic ter singe course o tretment, she
shoud beinestigted or other otenti cuses.
2.2.3 In eldel patients (e 65 eas f age),diagnsis shuld be based
n a full clinicalassessent, including ital signs.
2.4. a Non-regnnt women with smtomsor signs o cute lUTI nd
either highrobbiit o or roen bcteriuri shoudbe treted with
ntibiotics.
2.4. B Non-regnnt women o n ge withsmtoms or signs o cute lUTI
shoud betreted with trimethorim or nitrourntoinor three ds.
measueent f length f teatentwith tiethpi nitfuantinn PrISmS f
Pactices pject,cpaisn f lcal pacticespecentage f thee da cuses
with
natinal data.
Pecentage f pescibed cuses ftiethpi nitfuantin f LUTIthat ae f
thee das
2.4. B ptients who do not resond to trimethorimor nitrourntoin
shoud he urine tken orcuture to guide chnge o ntibiotic.
Audit f anageent f patientswith epeat isits within 28 das
fpesciptin f tiethpi f LUTI.
2.4. Quinlnes shuld nt be used f epiicalteatent f LUTI.
Pecentage f LUTI teated withquinlnes with n pi episde fUTI in
the past 28 das and n uinecultue sent.
2.4.2 a Non-regnnt women with smtoms orsigns o cute UUTI shoud
be treted withciprooxacin for seven days. Ipleentatin f cae
pathwa
f UUTI in pia and secndacae with audit f pactice
againstecendatins.
2.4.2 D Urine shoud be tken or cuture beoreimmedite emiric
tretment is strted ndtretment chnged i there is n indequteresonse
to the ntibiotic.
2.4.3 a Non-regnnt women with smtomticbcteriuri shoud not receie
ntibiotictretment.
Pecentage f wen teated insecnda cae f UTI with ndcuented eidence
f spts fUUTI LUTI.
2.4.3 a Eder women (oer 65 ers o ge) withsmtomtic bcteriuri
shoud not receientibiotic tretment.
-
8/2/2019 Sign 88
31/4627
7.3.2 mANAGEmENT oF BACTErIAL UTI IN PrEGNANT WomEN
Recommendtion Imementtion or udit
3..3 a Stndrd quntittie urine cuture shoud beperformed routinely
at rst antenatal visit
Cae pathwa f detectin andanageent f asptaticbacteiuia f pegnanc
with auditagainst tagets.
3..3 a The resence o bcteriuri in urine shoudbe conrmed with a
second urine culture.
3..3 a Distick testing shoud not be used to screen orbacterial
UTI at rst or subsequent antenatalisits.
3..3 Dipsticks t test nl f pteinuia and thepesence f glucse in
the uine shuld beused for screening at the rst and
subsequentantenatal isits as a e cst-effectiealtenatie t
ulti-eagent dipsticks thatdetect the pesence f nitite,
leuccteestease and bld in additin t ptein andglucse.
real f dipsticks f leucctes andnitites f antenatal clinics.
3.2. B pregnnt women with smtomtic UTIshoud be treted with n
ntibiotic.
Cae pathwa f detectin andanageent f asptatic
bacteiuia f pegnanc with auditagainst tagets.
3.2. Gien se antibitics ae txic in pegnanc,efe t the Bitish
Natinal Fula (BNF)f cntaindicatins.
3.2. A single uine saple shuld be taken f
cultue befe epiic antibitic teatent isstated.
3.2. Gien the isks f sptatic bacteiuiain pegnanc, a uine cultue
shuld bepefed seen das afte cpletin fantibitic teatent as a test f
cue.
3.2.and3.2.2
refe t lcal guidance f the safest,cheapest, effectie antibitic f
pegnantwen.
Audit f antibitics pescibedt pegnant wen against
lcalguidance.
3.2.2 a asmtomtic bcteriuri detected duringregnnc shoud be
treted with n
ntibiotic.Cae pathwa f detectin andanageent f asptaticbacteiuia
f pegnanc with auditagainst tagets.
3.3 C Women with bacteriuria conrmed by asecond urine cuture
shoud be treted ndhe reet urine cuture t ech ntentisit unti
deier.
3.3 Wen wh d nt hae bacteiuia in therst trimester should not
have repeat urinecultues.
7 RECOMMENDaTIONS fOR IMplEMENTaTION, aUDIT, SURvEIllaNCE aND
RESEaRCH
-
8/2/2019 Sign 88
32/4628
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
7.3.3 mANAGEmENT oF BACTErIAL UTI IN PATIENTS WITH CATHETErS
Recommendtion Imementtion or udit
5. D Cinic smtoms or signs re notrecommended or redicting
the
ikeihood o smtomtic UTI inctheterised tients.
Cae pathwa f diagnsis fsptatic UTI in catheteisedpatients with
audit against pactice.
5. In a catheteised patient wh pesentswith a fee:
lk f assciated lcalising (lin supapubic tendeness)
ssteicfeatues
exclude the ptential suces finfectin
send ff an apppiatel taken uinesaple f cultue t deteine the
infecting ganis and susceptibilitiescnside antibitic theap
takingint accunt the seeit f thepesentatin and an cbidfacts.
5.
and
5.5
Uine saples f patients with cathetes ueteic stas shuld nl be
sentf labat cultue if the patienthas clinical sepsis, nt because
theappeaance sell f the uine suggeststhat bacteiuia is pesent.
Audit f clinical eidence f infectinin patients with lng te
cathetes ueteic stas wh hae been teatedwith antibitics had uine
saplessent f cultue.
5.2. C lbortor microsco or dignosingUTI in ctheterised tients is
notrecommended.
Cae pathwa f diagnsis fsptatic UTI in catheteisedpatients with
audit against pactice.5.2.2 B Distick testing shoud not be used
to
dignose UTI in ctheterised tients.
5.3 a antibiotic rohis is notrecommended or the reention
osmtomtic UTI in ctherised tients.
Pecentage f patients with lng tecathetes wh eceie antibitics
withn clinical eidence f sptaticUTI.
5.4. Catheteised patients with spts signs f acute UUTI shuld be
teatedwith ciprooxacin or co-amoxiclav for
seen das. Antibitic selectin f patients withsptatic UTI cpaed
with lcalplic ecendatins.5.4. Uine shuld be taken f cultue befe
teatent is stated, teatent shuld bechanged if the ganis is
esistant t thechsen antibitic.
5.4. B ptients with ong term indweingctheters shoud he the
ctheterchnged beore strting ntibiotictretment or smtomtic UTI.
Audit f cathete change pi tcencing antibitic.
5.4.2 B Ctheterised tients with smtomticbcteriuri shoud not
receie ntibiotic
tretment.
Audit f clinical eidence f infectinin patients with lng te
cathetes
ueteic stas wh hae been teatedwith antibitics had uine
saplessent f cultue.
-
8/2/2019 Sign 88
33/4629
7.4 RECOMMENDaTIONS fOR SURvEIllaNCE
Thee shuld be utine sapling f uine f cultue f all patients
pesenting with acuteuina spts in se selected pactices t establish
the tue leel f esistance in bacteiacausing acute UTI in geneal
pactice. Pia eseach a be equied t pide eidence
to support details of surveillance (for example, sample sizes,
frequency of surveillance studiesand gegaphical lcatin f
pactices).
Thee shuld be sueillance f cathete assciated uina tact infectin
(CAUTI) using theScttish Sueillance f Healthcae Assciated Infectin
Pgae (SSHAIP) deelped audittl (www.shw.sct.nhs.uk/scieh/) t allw
easueent f catheteisatin and cathete caepactice against the best
pactice stateent Uina Catheteisatin and Cathete Cae 44 whichwas
deelped and ipleented b the Scttish ministeial Healthcae Assciated
Infectin(HAI) Task Fce.
7.4. USEFUL WEBSITES For SUrvEILLANCE AND INFECTIoN CoNTroL
NHS Scotnd e-ibrr HaI Mnged Knowedge Network ort:
www.elib.sct.nhs.uk
British Societ or antimicrobi Chemother (BSaC):
www.bsac.g.uk/SaCaR (Depatent f Healths Specialist Adis Cittee n
Antiicbial resistance):www.adisbdies.dh.g.uk/saca
Ntion Eectronic librr o Inection: www.neli.g.uk
7.5 RECOMMENDaTIONS fOR RESEaRCH
What is the isk f isdiagnsis, including STDs, afte patients with
suspected UTI haetelephne cnsultatin and antibitic pescibing b nuse
pactitines?
Hw effectie ae nea patient tests when cpaed t a eliable ethd f
diagnsingasptatic bacteiuia in pegnant wen?
Which antibitics ae st effectie f peentin and teatent f ecuent
UTI inen?
Ae canbe pducts effectie f peentin and teatent f ecuent UTI in
en?
Is ethenaine pphlaxis effectie f the peentin f sptatic UTI in
eldel,institutinalised, catheteised patients?
What ae the st effectie was f questining patients t elicit the
st eleant infatint aid diagnsis and teatent?
What ae the st effectie ethds f cunicatin between healthcae
pfessinalsand patients abut spts and facts that elate t a ptential
infectin?
What is the ipact f UTI and its teatent (including side effects)
n patients qualit flife?
What ae patients attitudes and expectatins twads teatent and
what pesnal stategies
d the hae f self cae?
7 RECOMMENDaTIONS fOR IMplEMENTaTION, aUDIT, SURvEIllaNCE aND
RESEaRCH
-
8/2/2019 Sign 88
34/4630
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
8 Deeoment o the guideine
8.1 INTRODUCTION
SIGN is a cllabatie netwk f clinicians, the healthcae pfessinals
and patientganisatins and is pat f NHS Qualit Ipeent Sctland. SIGN
guidelines ae deelpedb ultidisciplina gups using a standad ethdlg
based n a ssteatic eiew f theeidence. Futhe details abut SIGN and
the guideline deelpent ethdlg ae cntainedin SIGN 50; A Guideline
Deelpes Handbk, aailable at www.sign.c.uk
8.2 THE GUIDElINE DEvElOpMENT GROUp
Pfess Pete Dae Professor of Pharmoeconomics, Medicines
Monitoring Unit,(Chai) Ninewells Hospital and Medical School,
Dundee
D Deek Bne Consultant Surgeon and Urologist,Ninewells Hospital
and Medical School, Dundee
ms Na Caig Lead Nurse - Continence, Whitehills
HealthandCommunity Care Centre, Forfar
D Daid Eans Consultant Obstetrician, Dr Grays Hospital,
Elgin
Pfess T Fahe Professor of General Practice, University of
Dundee
D Ian Guld Consultant in Clinical Microbiology,Aberdeen Royal
Inrmary
m rbin Habu Quality and Information Director, SIGN
ms Kaen Hakness Principal Pharmacist, Ninewells Hospital
andMedical School, Dundee
D rbeta Jaes Programme Manager, SIGN
ms Bin Jadine Lay representative, Edinburgh
D rss Langlands General Practitioner, Newton Port Surgery, East
Lothianms Helen macdnald Health Protection Nurse Specialist,
Highland NHS Board, Inverness
D rbet mastetn Medical Director, Crosshouse Hospital,
Kilmarnock
Pfess Dilip Nathwani Consultant Physician, Infection
Unit,Ninewells Hospital and Medical School, Dundee
D Eica Petes Special Registrar in Infectious Diseases,Brownlea
Centre, Gartnavel Hospital, Glasgow
ms valeie Sillit Community Pharmacist, Woodend Hospital,
Aberdeen
ms Deen Sipsn Community Staff Nurse, Green Street Surgery,
Forfar
The membership of the guideline development group was conrmed
following consultation
with the ebe ganisatins f SIGN. All ebes f the guideline
deelpent gupade declaatins f inteest and futhe details f these ae
aailable n equest f the SIGNExecutie. Guideline deelpent and
liteatue eiew expetise, suppt and facilitatin weepided b the SIGN
Executie.
8.3 aCKNOWlEDGEMENTS
SIGN is gateful t the fllwing fe ebes f the guideline deelpent
gup andthes wh hae cntibuted t the deelpent f this guideline.
ms Fina Bandt Practice Nurse, Aberlour
D Ali El-Gh Programme Manager, SIGN
D michael Pwe Clinical Knowledge Author, Guideline Developerand
Informatician, Prodigy Knowledge, Newcastle
D Kate Wdan Lay representative, Edinburgh
-
8/2/2019 Sign 88
35/463
8 DEvElOpMENT Of THE GUIDElINE
8.4 SySTEMaTIC lITERaTURE REvIEW
The eidence base f this guideline was snthesised in accdance
with SIGN ethdlg.A ssteatic eiew f the liteatue was caied ut using
an explicit seach stateg deisedby the SIGN Information Ofcer in
collaboration with members of the guideline development
gup.Liteatue seaches wee initiall cnducted in medline, Ebase,
Cinahl, and the CchaneLiba using the ea ange 994-2002. The liteatue
seach was extended f 966-2003f rCTs and diagnstic studies. The
Natinal Ecnic Ealuatin Database (NEED) wasseached f ecnic studies t
ce the peid up t Janua 2004. Ke websites n theIntenet wee als
seached. These seaches wee suppleented b the efeence lists f
eleantpapers and group members own les. The Medline version of the
main search strategies canbe fund n the SIGN website.
8.5 CONSUlTaTION aND pEER REvIEW
8.5. NATIoNAL oPEN mEETING
A natinal pen eeting is the ain cnsultatie phase f SIGN
guideline deelpent, atwhich the guideline development group
presents its draft recommendations for the rst time.The natinal pen
eeting f this guideline was held n 30 Apil 2004 and was attended
bepesentaties f all the ke specialties eleant t the guideline. The
daft guideline was alsaailable n the SIGN website f a liited peid
at this stage t allw thse unable t attendthe eeting t cntibute t
the deelpent f the guideline.
8.5.2 SPECIALIST rEvIEW
This guideline was als eiewed in daft f b the fllwing
independent expet efeees,wh wee asked t cent piail n the
cpehensieness and accuac f intepetatinf the eidence base suppting
the ecendatins in the guideline. SIGN is e gateful
t all f these expets f thei cntibutin t the guideline.
D Jaes Beattie Director of Guidelines Development, Royal College
ofGeneral Practitioners/General Practitioner, Aberdeenshire
m Gaee Cnn Consultant Urological Surgeon,Southern General
Hospital, Glasgow
ms Beatice Gant Lay Reviewer, Larbert
D ma Hansn Consultant Microbiologist,Western General Hospital,
Edinburgh
D Diana Hltn Hospital Practitioner, Roodlands Hospital, East
Lothian
ms Cath mcKeell Project Manager (Scotland), Incontact,
Lanarkshire
D Allan me General Practitioner, South Beach Surgery,
Ardrossan
D Dth mi Director of Public Health, NHS LanarkshirePfess Sigad
mlstad Professor of General Practice,
Primrvardens FoU-enhet, Sweden
D Lindsa Niclle Professor of Internal Medicine and Medical
Microbiology,University of Manitoba, Canada
D Ewan olsn Consultant Microbiologist, Royal Inrmary of
Edinburgh
Professor Raul Raz Director, Infectious Diseases Unit,Haemek
Medical Centre, Israel
D maueen Sipsn General Practitioner, Townhead Practice,
Montrose
Pfess Fancisc Sian Professor of Microbiology, Fundacion Jimenez
Diaz, Madrid
D Chales Swainsn Medical Director, Lothian NHS Board,
Edinburgh
D Alex Watsn General Practitioner, West Gate Health Centre,
DundeeD Caig Willias Consultant Medical Microbiologist,
Yorkhill NHS Trust, Glasgow
-
8/2/2019 Sign 88
36/4632
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
8.5.3 SIGN EDITorIAL GroUP
As a nal quality control check, the guideline is reviewed by an
editorial group comprisingthe eleant specialt epesentaties n SIGN
Cuncil t ensue that the specialist eiewescents hae been addessed
adequatel and that an isk f bias in the guidelinedeelpent pcess as
a whle has been iniised. The editial gup f this guidelinewas as
fllws:
Pfess Gdn Lwe Chair of SIGN; Co-Editor
D Daid Alexande General Practitioner, Nethertown Surgery,
Dunfermline
D Bill reith Royal College of General Practitioners,General
Practitioner, Aberdeen
Dr Saa Qureshi SIGNProgramme Director; Co-Editor
D Saa Twaddle Director of SIGN; Co-Editor
-
8/2/2019 Sign 88
37/4633
abbreitions
BNf Bitish Natinal Fula
BSaC Bitish Sciet f Antiicbial ChetheapCaUTI cathete assciated
uina tact infectin
CBa cntlled befe and afte stud
cu cln fing units
CI condence interval
CSM Cittee n Safet f medicines
CSU cathete specien f uine
Gp geneal pactitine
HaI healthcae assciated infectin
Hpa Health Ptectin Agenc
IDSa Infectius Diseases Sciet f Aeica
INR International Normalized Ratio
KUB kidnes, uetes and bladde
lE leuccte estease
lUTI lwe uina tact infectin
MIC iniu inhibit cncentatin
MSU idstea specien f uine
NelI Natinal electnic Liba f Infectin
NNT nube needed t teat
NNTB number needed to benet
NNTH nube needed t ha
ppROM pe-labu, peatue uptue f ebanes
ppv psitie pedictie alue
Qaly qualit adjusted life ea
RCT andised cntlled tial
SaCaR Depatent f Healths Specialist Adis Cittee n
Antiicbialresistance
SIGN Scttish Intecllegiate Guidelines Netwk
Spa supapubic aspiate
SSHaIp Scttish Sueillance f Healthcae Assciated Infectin
Pgae
STD sexuall tansitted disease
UTI uina tact infectin
UUTI uppe uina tact infectin
WBC white bld cells
aBBREvIaTIONS
-
8/2/2019 Sign 88
38/4634
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
MaNaGEMENT Of SUSpECTED lUTI IN WOMEN (not regnnt)
In women with symtoms of vgin
itch or dischrge, exore terntivedignoses nd consider evic
exmintion.
CyESNO vgin itch
or dischrge?
Mutie
smtoms
feer &
bck in?
yES
Conside the possibility of UUTI.
limited (no more thn
two) smtoms
Distickositie
Distick negtieor equioc
Distick tests shoud ony be used to
dignose bcteriuri in women with
imited symtoms nd signs.
C
NO, lUTI robbe
Non-regnnt
women of nyge with
symtoms or
signs of cute
lUTI shoud betreted with
trimethorim or
nitrofurntoin
for three dys.
ptients who do
not resond to
trimethorimor nitrofurntoin
shoud hve
urine tken forcuture to guide
chnge of
ntibiotic.
B Offer emiricntibiotictretment.
The risks nd
benefits ofemiric
tretment shoud
be discussed
with the tient
nd mngedccordingy.
If womnremins
symtomtic
fter singecourse of
tretment,
investigte other
otenti cuses.
B
Quinolones should not be used fo empiical
teatment of LUTI.
Smtoms nd signs o UTI?
dsuri urgenc
requenc
ouri
surubic tenderness
eer
ank or back pain
Women with enal impaiment should not beteated with
nitofuantoin.
Women rescribed nitrofurntoin shoud not
tke knising gents (potassium citrate).D
anne 1
-
8/2/2019 Sign 88
39/4635
MaNaGEMENT Of SUSpECTED UUTI IN WOMEN (not regnnt)
Signs nd smtoms o UUTI:
oin in
ank tenderness
eer
rigors
other mniesttions o sstemic
inammatory response
Admit to hospital
Non-regnnt women with symtoms or signs of
cute UUTI shoud be treted with cirofoxcin for
seven dys.
a
NO yES
Uine should be taken fo cultue befoe immediate
empiical teatment is stated and teatment changed if
thee is an inadequate esponse to the antibiotic.
D
UUTI cn be ccomnied b bcteremi,
mking it ie-thretening condition
I no resonse to
tretment in 24 hours
Sstemic smtoms?
aNNExES
anne 2
-
8/2/2019 Sign 88
40/4636
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
MaNaGEMENT Of SUSpECTED lUTI IN pREGNaNT WOMEN
Tret with n ntibiotic.B
Sptatic bacteiuia(ccus in 7-20% f pegnancies)
NO
Sceening fasptatic bacteiuia
The resence of bcteriuri in urine
should be confrmed with a second
urine cuture.
a
Cuture ositie?
Tret with n ntibiotic.a
Reet urine cuture t ech ntent
visit unti deivery.a
Stndrd quntittive urine cuture
shoud be erformed routiney t
frst antenatal visit.
a
a single uine sample
should be taken fo
cultue befoe empiic
antibiotic teatment is
stated efe to local guidance
fo the safest, cheapest,
effective antibiotic
efe to the Bitish
National Fomulay
(BNF) fo
containdications inpegnancy
a uine cultue should
be pefomed sevendays afte completion
of antibiotic teatment as
a test of cue.
refe to local guidance fo the safest,cheapest, effective
antibiotic.
Women who do not
have bacteiuia in
the frst trimester
should not have
epeat uine
cultues.yES
Distick testing shoud not be usedto screen for bcteri UTI.
a
anne 3
-
8/2/2019 Sign 88
41/4637
MaNaGEMENT Of SUSpECTED UTI IN aDUlT MEN
Histor o eer or bck in
Smtoms nd signs o UTI?
dsuri urgenc
requenc
ouri
surubic tenderness
eer
ank or back pain
Dierenti dignosis shoud incude
rosttitis, chmidi inection, eididmitis
Refer for uroogic
investigtion
Tret emiricy with two week course
of quinoone.
In all men with symptoms of UTI
a uine sample should be taken focultue.
Conside the possibility of UUTI
Uine cultue should guide the
choice of antibiotic.
I no resonse
to ntibiotic
Tret emiricy with two week course
of quinoone.
Recurrent UTI?
Edery men with symtomtic
bcteriuri shoud not receive ntibiotictretment.
NO
yES
C
Investigate fo
postatitis.
D
a
B
anne 4
aNNExES
-
8/2/2019 Sign 88
42/4638
MaNaGEMENT Of SUSpECTED BaCTERIal URINaRy TRaCT INfECTION IN
aDUlTS
Reerences
1. Morgan MG, McKenzie H. Controversies in the laboratory
diagnosis ofcunit-acquied uina tact infectin. Eu J Clin micbil
InfectDis. 993;2(7):49-504.
2. Bugte-maessen Am, Winkens rA, Gl rP, Knttneus JA, Keste
AD,Beusans GH, et al. Facts pedicting diffeences ang
genealpactitines in test deing behaiu and in the espnse t feedbackn
test equests. Fa.Pact 996;3(3):254-8.
3. olesen F, oestegaad I. Patients with uina tact infectin:
ppsedanageent stategies f geneal pactitines, icbilgists andulgists.
B.J Gen.Pact 995;45(400):6-3.
4. Nazareth I, King M. Decision making by general practitioners
indiagnsis and anageent f lwe uina tact spts in wen.BmJ
993;306:03-6.
5. oDwd TC, Sail JE, West rr. Clinical judgeent in the
diagnsisand anageent f fequenc and dsuia in geneal pactice.
BmJ984;288 (Clin res Ed):347-9.
6. Dae P, Steinke D, macDnald T, Phillips G, Sullian F. Nt
ssiple cstitis: hw shuld pescibes be suppted t ake infeddecisins
abut the inceasing pealence f infectins caused b dug-esistant
bacteia? B J Gen Pact 2000;50(45):43-6.
7. Gaans r, Haekn mJ, valkenbug HA, Gslings Wr. A pspectiestud f
uina-tact infectins in a Dutch geneal pactice.
Lancet976;2:674-7.
8. Clague J, Han m. Uine cllectin and cultue in eldel peple.
AgeAgeing 998;27(5):658-9.
9. Nicolle LE. Asymptomatic bacteriuria in institutionalized
elderly people:eidence and pactice. CmAJ. 2000;63(3):285-6.
0. Walke S, mcGee A, Si AE, Astng-Eans m, Leb m. Wh
aeantibiotics prescribed for asymptomatic bacteriuria in
institutionalizedeldel peple? A qualitatie stud f phsicians and
nusespeceptins. CmAJ. 2000;63(3):273-7.
. Waen JW, Abutn E, Hebel Jr, Jhnsn Jr, Schaeffe AJ, StaWE.
Guidelines f antiicbial teatent f uncplicated acutebacteial cstitis
and acute pelnephitis in wen. Clin Infect Dis999;29(4):745-58.
2. Bent S, Nallathu BK, Siel DL, Fihn SD, Saint S. Des thiswan
hae an acute uncplicated uina tact infectin?
JAmA2002;287(20):270-0.
13. Mellors JW, Kelly JJ, Gusberg RJ, Horwitz SM, Horwitz RI.
Asiple index t estiate the likelihd f bacteial infectinin patients
deelping fee afte abdinal suge. A Sug988;54(9):558-64.
4. Stuat mE, macuiba J, Heidich F, Faell rG, Baddick m,
EtchisnS. Successful ipleentatin f an eidence-based clinical
pacticeguideline: acute dsuia/ugenc in adult wen.
Hmo.Pact997;(4):50-7.
5. Saint S, Schles D, Fihn SD, Faell rG, Sta WE. The
effectienessf a clinical pactice guideline f the anageent f
pesueduncplicated uina tact infectin in wen. A.J
med999;06(6):636-4.
6. Klein LE, Chaache P, Jhannes rS. Effect f phsician tutialsn
pescibing pattens f gaduate phsicians. J med Educ98;56:504-.
7. Depatent f Health. UK antiicbial esistance stateg and
actinplan. Lndn: The Depatent;2000.
8. Scttish Executie. Health Depatent. Antiicbial esistance
stateg
and Scottish action plan. Edinburgh: Stationery Ofce; 2002.19.
Nicolle LE, Mayhew WJ, Bryan L. Prospective randomized comparison
of
therapy and no therapy for asymptomatic bacteriuria in
institutionalizedeldel wen. A J med 987;83():27-33.
20. Hading GK, Zhanel GG, Niclle LE, Cheang m, manitba
DiabetesUina Tact Infectin Stud Gup. Antiicbial teatent indiabetic
wen with asptatic bacteiuia. N Engl J med2002;347(20):576-83.
2. Niclle LE. Asptatic bacteiuia: When t sceen and when tteat.
Infect Dis Clin Nth A 2003;7(2):367-94.
22. Health Ptectin Agenc. Inestigatin f uine. Clindale:
TheAgenc; 2004. (Natinal Standad methd BSoP 4 Issue 5) [cited 9
June 2006] Aailable f ul
http://www.hpa-standadethds.g.uk/dcuents/bsp/pdf/bsp4.pdf
23. Isenbeg H. Pathgenicit and iulence: anthe iew. Clin micbilre
988;():40-53.
24. Niclle L. Uina tact infectins in lng-te-cae facilities. Inf
CntHsp Epideil 200;22(3):67-75.
25. Vazquez JC, Villar J. Treatments for symptomatic urinary
tract infectionsduing pegnanc (Cchane reiew). In: The Cchane Liba,
Issue3 2000. Chicheste, UK: Jhn Wile and Sns Ltd.
26. Freedman LR, Phair JP, Seki M, Hamilton HB, Nefzger MD.
TheEpideilg f Uina Tact Infectins in Hishia. yale J Bil
med965;37:262-82.
27. Ndensta G, Sundh v, Lincln K, Sanbg A, Eden CS. Bacteiuiain
epesentatie ppulatin saples f pesns aged 72-79 eas. A
J Epideil 989;30(6):76-86.28. Akhte A, Andews G, Caid F, Falln
r. Uina tact infectin in the
eldel: a ppulatin stud. Age Aging 972;:48-54.29. Kunin Cm,
mcCack rC. An epideilgic stud f bacteiuia
and bld pessue ang nuns and wking wen. N Engl J
med968;278(2):635-42.
30. Zhanel GG, Niclle LE, Hading GK. Pealence f
asptaticbacteiuia and assciated hst facts in wen with diabetes
ellitus.The manitba Diabetic Uina Infectin Stud Gup. Clin Infect
Dis995;2(2):36-22.
3. Geelings SE, Stlk rP, Caps mJ, Netten Pm, Heksta JB, ButeKP,
et al. Asptatic bacteiuia a be cnsideed a cplicatinin wen with
diabetes. Diabetes mellitus Wen AsptaticBacteiuia Utecht Stud Gup.
Diabetes Cae 2000;23(6):744-9.
32. Sawes JS, Tdd WA, Kellett HA, miles rS, Allan PL, Ewing DJ,
et al.Bacteiuia and autnic nee functin in diabetic wen. DiabetesCae
986;9(5):460-4.
33. Semetkowska-Juricwicj E, Horoszek-Maziarz S, Galinski J,
ManitiusA, Kupa-Wjciechwska B. The clinical cuse f
unteateedasptatic bacteiuia in diabetic patients: 4 ea fllw-up.
mate
med Pl 995;27:9-5.34. Perez-Luque E, Villapando M, Malacara J.
Association of sexual activity
and bacteiuia in wen with nn-insulin dependent diabetes
ellitus.J Diabetes Cplicatins 992;6(4):254-7.
35. Miall WE, Kass EH, Ling J, Stuart KL. Factors inuencing
arterial pressurein the geneal ppulatin in Jaaica. BmJ
962;5303:497-506.
36. Eans DA, Kass EH, Hennekens CH, rsne B, mia L, KendickmI, et
al. Bacteiuia and subsequent talit in wen.
Lancet982;(8264):56-8.
37. Bengtssn C, Bengtssn U, Bjkelund C, Lincln K, Sigudssn
JA.Bacteiuia in a ppulatin saple f wen: 24-ea fllw-up stud.results
f the pspectie ppulatin-based stud f wen inGthenbug, Sweden. Scand
J Ul Nephl 998;32(4):284-9.
38. Takala J, Jusiies H, Siees K. Sceening f and teatent
fbac