Embed Size (px)
Citation preview

RESEARCH Open Access
Significance of incident reports by medicaldoctors for organizational transparency anddriving forces for patient safetyTatsuya Fukami*, Masakazu Uemura and Yoshimasa Nagao
Abstract
Background: Incident reporting is an effective strategy used to enhance patient safety and quality improvement inhealthcare. An incident is an event that could eventually result in harm to a patient. The aim of this study is to re-evaluate the importance of reporting by medical doctors to improve quality in healthcare and patient safety.
Methods: We conducted a retrospective analysis of the reported incidents registered in our institutional databasefrom April 1st 2015 to March 31st 2019, classified according to eight variables proposed by the National UniversityHospital Council of Japan, to determine the type of incidents and their potential harm to patients.
Results: Registered reports totalled 43,775, approximately 8% of which arise annually from medical doctors inclinical departments. Incidents with higher impact on patients have significantly increased the rate of reporting bymedical doctors. The most frequent types of report overall concerned medication incidents, followed by infusionlines, drainage-tube devices, cure, examination, and treatment outside the operating room. The most frequentreports by medical doctors involved operation-related incidents, followed by cure, examination, treatment outsidethe operation room, and medications.
Conclusion: Reporting by medical doctors reflects the organizational transparency and the driving forces behindpatient safety and quality improvement in healthcare. Efforts toward seamless improvement in patient safety andquality at our hospital continue apace.
BackgroundA reporting culture means cultivation of the atmospherewhereby workers in a hospital are able to report patientsafety concerns with fairness and without fear of blame[1]. Confidentiality will be guaranteed and the reportssubmitted by the employee will be acted upon for im-provement. Moreover, the report will be recognized as aworthy act. An incident-reporting system is an organizedapproach to reporting near misses or adverse events toenable improvement [2]. An incident-reporting system isa voluntary, anonymous, confidential electronic systemthat allows the reporting of incidents and adverse events
for analysis by experts in quality improvement and pa-tient safety [3–5]. Although this system might well im-prove patient safety by reducing the risk of adverseevents, it has many obvious limitations: reports aresometimes entirely subjective and therefore unfair, arenot comparable between hospitals, and carry unacknow-ledged bias [6, 7].This is a result of a third party reviewing medical re-
cords at hospitals nationwide and picking up adverseevents according to certain criteria. Figure 2 shows theestimates based on the results of this study and thenumbers reported by our hospital last year.The purpose of this study is to re-evaluate the import-
ance and submitting activity of incident reports by
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] of Patient Safety, Nagoya University Hospital, Nagoya, Japan
Fukami et al. Patient Safety in Surgery (2020) 14:13 https://doi.org/10.1186/s13037-020-00240-y

medical doctors to grasp the critical events in hospitaland ensure organizational transparency.
MethodsOur centre is a 1000-bed academic hospital with a clin-ical patient safety and quality management departmentthat oversees patient safety affairs and is responsible forthe incident-reporting system. Patient safety incidentreporting is mandatory for all staff in our hospital, in-cluding contracted workers, when they confront an inci-dent. We surveyed the incident reports submitted fromApril 1st 2015 to March 31st 2019, selected from all in-cidents reported by all hospital workers, and collectedinformation from the corresponding original electronicincident reports. We compared the reports by medicaldoctors and other workers in the hospital. The collecteddata included: the date of the incident; ward/departmentwhere the incident occurred; healthcare profession, yearsof experience, and affiliated department of the reporterand person involved in the incident; information regard-ing the patient; incident details; incident classification;and incident severity classification. Incident severity andcontinuity classification is widely used in Japanese hospi-tals to evaluate the impact on the patient conveyed bythe incident, and is based on a classification system de-veloped by the National University Hospital Council ofJapan [8]. The system classifies eight ranks by incidentseverity and continuity impact for patients (Table 1).Levels from 0 to 1 are defined as near miss, whereby anunexpected event has the potential to cause, but doesnot actually harm the patient or interrupt the normalsituation. A near miss is often an error prevented byother circumstances. Levels from 2 to 5 are defined asadverse event, which represents any unintentional or un-favourable clinical sign or symptom, including complica-tions, any new illness or disease or the deterioration ofexisting disease or illness, and any clinically significant
deterioration in any laboratory assessments or clinicaltests. The most commonly used tool in quality monitor-ing is the Pareto chart. In this chart, the values are pre-sented in decreasing order and the cumulative functionis a concave shape. A Pareto chart is deemed appropriatefor the first three steps in the problem-solving process(i.e., clarifying and breaking down the problem, then set-ting the target) because a Pareto chart aims to highlightthe most important causal factors. The electronic inci-dent reporting system used by our hospital is IncidentReport System version 1.0 (Safe Master, Fukuoka, Japan).We extracted only necessary incident information itemsfor this study, and processed information concerning in-dividuals (e.g., the reporter and target patient) anonym-ously. People who notice the event will report. It can bereported by multiple people in the same occupation, bymultiple occupations, or by only one person. All analyseswere performed using SPSS version 25 (IBM, Armonk,NY, USA). About patient and public involvement state-ment, this study was approved by the Institutional Re-view Board of the study hospital.
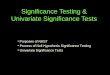
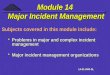
ResultsWhen patient safety incidents and accidents occur in thehospital, they are submitted to general risk and safetymanagers from various occupations via an electronicreporting system; over 10,000 cases are reported each year,and the total number of incident reports hospital-wide is43,775 (Fig. 1). A review of the incidents reported by med-ical doctors each year revealed that approximately 8%arose from all clinical departments (Fig. 1). The incidentswith higher impact on patients significantly increased thenumber of reports by medical doctors (Fig. 2).We classified incident reports using a Pareto chart.
The incident reports from nurses totalled 30,392, fromdoctors 2943, and from others 6488 for this 4-year ana-lysis. The most frequent type of report was medication
Table 1 Incident severity classification system recommended by the National University Hospital Council of Japan
Level Continuity ofinjury
Severity of injury Outcome/Treatment of injury
Level 0 – – Error or trouble with a pharmaceutical or medical device was found, but did not affect the patient
Level 1 None – There was no harm to the patient (but there was a possibility of some influence)
Level 2 Transient Mild Treatment was not necessary (mild change in vital signs, need for increased patient observation,examination for confirmation of safety, etc.)
Level 3a Transient Moderate Simple treatment was required (disinfection, poultice, skin suture, administration of analgesics, etc.)
Level 3b Transient Severe Substantial treatment was required (significant change in vital signs, use of artificial respirator, surgery,prolongation of hospitalization, hospitalization, fracture, etc.)
Level 4a Permanent Mild to moderate Permanent disability or subsequent complication remained, but was not accompanied by significantdysfunction or an aesthetic problem
Level 4b Permanent Moderate to severe Permanent disability or subsequent complication remained, accompanied with significant dysfunctionor an aesthetic problem
Level 5 Death – Death (excluding those due to the natural course of the underlying disease)
Fukami et al. Patient Safety in Surgery (2020) 14:13 Page 2 of 7

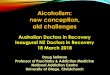
incidents, followed by infusion lines and drainage-tubedevices, and cure, examination and treatment outsidethe operating room (Fig. 3a). The most frequent reportsby medical doctors concerned operation-related inci-dents, followed by cure, examination and treatment out-side the operating room, and medications (Fig. 3b).Nurses most frequently reported incidents related tomedication, followed by infusion lines and drainage-tube
devices, and cure, examination and treatment outsidethe operating room (Fig. 3c).The clinical department in which the incidents oc-
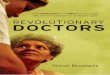
curred were reported by all workers. The departmentwith the largest number of reports was Paediatrics,followed by Gastroenterological Surgery 1 and Neuro-surgery (Fig. 4a). Based on reporting solely by doctors,reports came most frequently from Anaesthesiology,
Fig. 1 Total number of incident reports and percentage reported by medical doctors in each fiscal year
Fig. 2 Distribution of incidents reported by medical doctors and non-medical doctors
Fukami et al. Patient Safety in Surgery (2020) 14:13 Page 3 of 7

A
B
C
Fig. 3 Pareto chart showing incident-reporting frequency and severity for each event: (a) overall, (b) medical doctors, (c) nurses
Fukami et al. Patient Safety in Surgery (2020) 14:13 Page 4 of 7

followed by the Perinatal Centre and Emergency andCritical Care Medicine (Fig. 4b).
DiscussionThis study covers identification of the high-risk areas inthe hospital and the importance of incident reportingfrom medical doctors. The most frequently reported de-partments are not “dangerous departments”, but “acci-dent extraction power and transparency”, which shouldbe highly evaluated.Although the incident reporting system does not re-
flect the actual hospital-wide events in our centre, it is aworthwhile source of information from which to dis-cover potential risks and attributable factors of a repre-sentative patient safety issue [3, 9]. In this system, events
whose potential consequences are difficult to measure inpatient prognosis and which have been caused by exter-nal events or inappropriate or defective internal pro-cesses, systems, and/or systemic improvement activityare also indicated as risks [10]. Accumulation of near-miss incidents of the same type and with a small impactas a one-off event also carries the risk of potential ad-verse events. There is a positive correlation between thenumber of incident reports and improved safety cul-ture within the organization [11]. Our hospital is aleading centre in regard to the number of incident re-ports (Fig. 1) in Japan. Adverse events reported bymedical doctors helps to coordinate the treatment ofsevere and chronic injury and is important for contin-ued transparency and active reporting in the hospital.
A
B
Fig. 4 Pareto chart showing incident reporting frequency and severity. a Cases reported according to clinical department. b Cases reported bydoctors according to their clinical department
Fukami et al. Patient Safety in Surgery (2020) 14:13 Page 5 of 7

Certain specialties have reported more near missesthan others, and doctors have reported more harm in-cidents than near misses [11], in line with our presentresults (Fig. 2). According to another study, eventswith no harm to the patient represented a high per-centage of all incident reports from nurses, otherhealthcare providers, and other workers [12]. Weassessed the various factors involved using a Paretochart, the purpose of which is to highlight the mostimportant among a large set of factors. The major issuehospital-wide (Fig. 3a) and among nurses (Fig. 3c) is medi-cation errors, while for doctor operation-related matters areof greatest concern (Fig. 3b). Our aim is to target the out-standing issues and consider appropriate countermeasuresfor each incident, which can be complicated by many fac-tors. The countermeasures should be comprehensive andpractical. Furthermore, we investigated which departmenthas risks with or without errors. Paediatrics and surgicaldepartments are major sources of reported incidents(Fig. 4a). Paediatric patients are of varying age and carrya wide disease spectrum that can easily deteriorate.Healthcare providers should thus customize treatment foreach patient with detailed assessment of the individual’scondition. Surgical departments obviously are sensitive tovarious risks during preoperative diagnosis, surgical proce-dures, and postoperative treatments. Our reporting stan-dards include the occurrence of complications so that wecan pick up on potential risks when there is a recurrentcomplication. As well as surgeons, anaesthesiologists facemany challenging tasks and risks (Fig. 4b). Once again,bold and honourable reporting of incidents drives thesafety culture and leads to organizational transparency inanaesthesiology. Overseeing measures to assess the reduc-tion or increase in near misses or adverse events is a usefulapproach to improve the effectiveness of an incident-reporting system. Incident-reporting analyses demonstratetwo influential factors, systemic issues and human errors.To reduce the hospital-wide risk, prompt, correct, and fairincident reporting is mandatory for improvement inhealthcare [13, 14].
ConclusionIn conclusion, reporting of incidents by medical doctorsreflects the organizational transparency and the drive to-ward patient safety and quality improvement in health-care. In addition, the reporting of near-miss eventshospital-wide also assumes importance because they arethe sentinel for future adverse events. After identifyingthe high-risk areas in various clinical departments, thenext step should be to analyse the root cause of inci-dents, especially those reported by doctors, and inter-vene appropriately to improve the quality of healthcare.This should contribute directly to safer care and theoverall drive toward the enforcement of a culture of
patient safety in the hospital. We can say that reportsfrom doctors are overwhelmingly more severe than re-ports from other occupations. This means that hospitalscannot accurately ascertain adverse events unless thereare few reports from doctors. As a safety manager, wewant to clear adverse events as much as possible, and torespond to particularly serious adverse events by collect-ing the best of the hospital. Nurses can report manyattempted and harmless cases, minor cases such as abra-sions and bruises, but that alone is not enough. Our hos-pital is grasping the overall picture of adverse events dueto the increase in reports from doctors, and feels that wecan finally stand at the starting point of medical safety.Reporting by medical doctors reflects the organizational
transparency and dynamic efforts required for patientsafety and quality improvement in healthcare. Efforts toachieve seamless improvement in patient safety and careat our hospital will continue.
AcknowledgmentsWe thank staff of Department of Patient Safety, Nagoya University Hospitaland Hugh McGonigle, from Edanz Group (www.edanzediting.com/ac), forediting a draft of the manuscript.
Authors’ contributionsTF initiated the idea, carried out the study, and involved in drafting themanuscript. MU contributed to the statistical analysis and in preparing themanuscript. YN edits starting from the proposal development up to the finalmanuscript writing and critically reviewed the manuscript for intellectualcontent. All authors read and approved the final manuscript.
FundingThe author disclosed receipt of the following financial support for theresearch, authorship, and/or publication of this article: This work wassupported by Terumo Life Science Foundation (Kanagawa, Japan).
Availability of data and materialsAll data generated or analysed during this study are included in thispublished article.
Ethics approval and consent to participateIn order to keep the ethical soundness of the research, an ethical approvalletter was obtained from the Institutional Review Board (IRB) of NagoyaUniversity Hospital. Comprehensive consent was also secured before datacollection.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Received: 8 February 2020 Accepted: 8 April 2020
References1. Reason J. Safety paradoxes and safety culture. Int J Inj Control Saf Promot.
2000;7:3–14.2. Kohn LT, Corrigan JM, Donaldson MS. Eds. To err is human: building a safer
health system. Washington, DC: National Academies Press, Committee onQuality of Health Care in America, Institute of Medicine; 2000.
3. Ramírez E, Martín A, Villán Y, et al; SINOIRES Working Group. Effectivenessand limitations of an incident-reporting system analyzed by local clinicalsafety leaders in a tertiary hospital: Prospective evaluation through real-timeobservations of patient safety incidents. Medicine (Baltimore). 2018; 97(38):e12509.
Fukami et al. Patient Safety in Surgery (2020) 14:13 Page 6 of 7

4. Brunsveld-Reinders AH, Arbous MS, De Vos R, et al. Incident and errorreporting systems in intensive care: a systematic review of the literature. IntJ Qual Health Care. 2016;28:2–13.
5. Fukami T, Uemura M, Terai M, et al. Eliminating patient misidentificationusing step-by-step problem-solving procedures to improve patient safety.Nagoya J Med Sci. 2020; [Epub ahead of print].
6. Müller BS, Beyer M, Blazejewski T, Gruber D, Müller H, Gerlach FM. Improvingcritical incident reporting in primary care through education andinvolvement. BMJ Open Qual. 2019;8:e000556.
7. Niemeier M, Hamsen U, Yilmaz E, Schildhauer TA, Waydhas C. Criticalincident reporting systems (CIRS) in trauma patients may identify commonquality problems. Eur J Trauma Emerg Surg. 2019; [Epub ahead of print].
8. Guidelines for the public announcement of medical accidents at nationaluniversity hospitals (revised edition). National University Hospital Council ofJapan, Tokyo. 2012. http://www.univ-hosp.net/guide_cat_04_15.pdf.Accessed July 5, 2019. In Japanese.
9. Baba-Akbari A, Sheldon TA, Cracknell A, et al. Sensitivity of routine systemfor reporting patient safety incidents in an NHS hospital: retrospectivepatient case note review. BMJ. 2007;334(7584):79.
10. Spangler D, Edmark L, Winblad U, Colldén-Benneck J, Borg H, Blomberg H.Using trigger tools to identify triage errors by ambulance dispatch nurses inSweden: an observational study. BMJ Open. 2020;10:e035004.
11. Howell A-M, Burns EM, Bouras G, et al. Can patient safety incident reportsbe used to compare hospital safety? Results from a quantitative analysis ofthe English National Reporting and Learning System Data PLoS One. 2015;10:e0144107.
12. Griffith R. Duty of candour requires better protection for nurses. Br J Nurs.2013;22(6):350–1.
13. Mitchell I, Schuster A, Smith K, Pronovost P, Wu A. Patient safety incidentreporting: a qualitative study of thoughts and perceptions of experts 15years after 'To err is Human'. BMJ Qual Saf. 2016;25:92–9.
14. Anderson JE, Watt AJ. Using safety-II and resilient healthcare principles tolearn from never events. Int J Qual Health Care. 2020; [Epub ahead of print].
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Fukami et al. Patient Safety in Surgery (2020) 14:13 Page 7 of 7