Embed Size (px)
Citation preview

Case Reports
Journal of Clinical Neuroscience 20 (2013) 602–604
Contents lists available at SciVerse ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Simultaneous presentation in the neck and abdomen of malignant peripheralnerve sheath tumors involving two different nerve tracts
Panagiotis A. Sideras ⇑, Felipe Castorena, Jaswinder SinghDepartment of Internal Medicine, Mount Sinai School of Medicine/Queens Hospital Center, 62–86 164th Street, Jamaica, NY 11432, USA
a r t i c l e i n f o
Article history:Received 19 February 2012Accepted 24 February 2012
Keywords:Malignant peripheral nerve sheath tumorNeurofibromatosisSpindle cell
a b s t r a c t
Neurofibromatosis-1 (NF-1) is a relatively common autosomal dominant disease and it is caused bymutation of the NF-1 tumor suppressor gene; hence, the individuals affected have increased risk fordeveloping familial cancer. Abdominal cavity neurofibromas are common but the simultaneous occur-rence of a malignant peripheral nerve sheath tumor (MPNST) in the chest and in the abdomen is rare.
Here, we present a patient with MPNST (spindle cell sarcoma) affecting simultaneously the vagus nervein the head and neck region, mediastinum, pleura as well as celiac plexus branches near the stomach.
Published by Elsevier Ltd.
1. Introduction
Neurofibromatoses is a group of genetic disorders that primar-ily affect the growth of neural tissues. Neurofibromatosis-1 (NF-1)is the most common type and accounts for 90% of patients. Itsprevalence is 1 in 4000 live births.1 The lifetime risk of developingan MPNST in patients with NF-1 has varied among reports withestimates ranging from 5% to 13%.2,3 Most MPNST occur in thehead, neck or limbs, but simultaneous occurrence in the mediasti-num and retroperitoneal space is very rare.4,5
2. Case report
An Hispanic 31-year-old male with no significant medical his-tory presented to our hospital complaining of left-sided abdominalpain. At the onset of the symptoms 1 month prior to his presenta-tion, the patient had presented to his private doctor for symptomsof dyspepsia and was sent home with antacids but the symptomsdid not improve.
General examination revealed a cachectic young man in noapparent distress. Skin examination revealed multiple cutaneousnodules of varying sizes distributed diffusely but mainly in theupper trunk, several café au lait spots > 15 mm in diameter and ax-illary freckling. On examination of the abdomen, a tender masscould be palpated from the left rib cage to the level just belowthe umbilicus in the right lower quadrant. The patient underwenta CT scan of the abdomen, which revealed a left upper quadrantmass, measuring 19.36 cm � 15.42 cm � 14.5 cm (Fig. 1) givingthe impression that it was arising either from the gastric wall orwas a retroperitoneal mass that was compressing the stomach. ACT scan of the neck and chest also revealed a mass lesion arisingposteriorly to the carotid artery and jugular vein (Fig. 2), extending
⇑ Corresponding author. Tel.: +1 631 522 6094; fax: +1 718 883 6336.E-mail address: [email protected] (P.A. Sideras).
as far as the mediastinum anteriorly to the aortic arch and an addi-tional mass abutting the left parietal pleura (Fig. 3).
The patient was diagnosed with neurofibromatosis-1 based onthe clinical findings of the cutaneous nodules, the café au lait spotsand axillary freckling. In addition, based on the clinical and imag-ing findings, a provisional diagnosis of a gastric malignancy, suchas leiomyosarcoma versus a retroperitoneal mesenchymal tumor,was considered.
The patient subsequently underwent an exploratory laparot-omy with abdominal mass debulking by the surgical oncologyteam. The mass was partially resected into two masses: one mea-sured 20 cm � 14 cm � 12 cm and weighed 1480 g; and the othermeasured 9 cm � 8 cm � 4.5 cm and weighed 95 g. A pathologicaland immunohistochemical study of both masses revealed neoplas-tic cells diffusely positive for vimentin, S-100 protein, cytokeratin(CK) AE1/AE3 and CK5/6, suggestive of a spindle cell MPNST.
After receiving two cycles of doxorubicin, ifosfamide and etopo-side, the patient again returned to our hospital with the complaintof severe abdominal pain. He had a partial small bowel obstructionand was admitted for medical management. After taking carefulconsideration of the poor prognosis, and as per the patient’s choice,he was discharged to a hospice care facility.
3. Discussion
Neurofibromatosis, is an autosomal dominant disease of variedclinical manifestation. There are two clinically and genetically dis-tinct subtypes, designated as NF-1 and NF-2.6
NF-1 comprises the most common single gene defect. Clinically itis characterized by multiple peripheral nerve tumors, optic gliomas,sphenoid wing dysplasias, pigmented iris nodules and hyperpig-mented macular skin lesions known as café au lait spots.7 All mani-festations may not be present and the diagnostic criteria are met ifthe patient has two or more of the above-mentioned features.8

Fig. 1. Sagittal abdominal CT scan of a patient with malignant peripheral nervesheath tumors showing (arrows) a large antero-posterior intra-abdominal mass.The mass is compressing the stomach and, as found later, it arose from the celiacnerve axis.
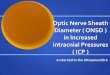
Fig. 2. Cervico-thoracic axial CT scan showing the mass lesion (arrows) of a patientwith malignant peripheral nerve sheath tumors arising posteriorly to the carotidartery and jugular vein, and involving the vagus nerve.
Fig. 3. Coronal thoracic CT scan of a patient with malignant peripheral nerve sheathtumors showing the mass producing a dumbbell shaped nerve swelling extendingas far as the mediastinum anteriorly to the aortic arch and an additional massabutting the left parietal pleura arising from the intercostal nerve (arrows).
Case Reports / Journal of Clinical Neuroscience 20 (2013) 602–604 603
There are no standardized criteria to diagnose MPNST; thus, fora definite diagnosis, the clinical findings need to be supplementedby the findings of a fusiform tumor in relation to a nerve, and to beassociated with the histopathological and immunocytochemicalfeatures.12 The reliability of S-100 protein as the universal markerof MPNST is questionable, as in 30% of patients the tumor may notshow reactivity; however, this did not occur in our report.
MPNST may appear similar to other spindle cell sarcomas;hence, certain histological features may help differentiate betweenthem.13
MPNST are locally invasive lesions, frequently leading to multi-ple recurrences and metastatic spread.14 They can disseminatethrough direct, hematogenous and perineural spread, whereasspread through the lymph nodes is rare.10 The most common met-astatic sites are the lungs followed by soft tissue and bone.
Prognosis of MPNST is poor and survival is influenced by tumorlocation and size. Survival is worse in patients with NF-1.15
4. Conclusion
MPNST constitutes a significant proportion of soft tissue sarco-mas. A combination of clinical history and examination, pathology,and immunohistochemistry helps in diagnosing these tumors. Theoverall treatment approach should be similar to that of other highgrade sarcomas. Patients with NF-1 need to be assessed periodi-cally to rule out any malignant change. Although multimodalitytherapy, including surgical resection and adjuvant radiotherapy,is available, the prognosis remains dismal.
References
1. Evans DG, Baser ME, McGaughran J, et al. Malignant peripheral nerve sheathtumours in neurofibromatosis 1. J Med Genet 2002;39:311–4.
2. McGaughran JM, Harris DI, Donnai D, et al. A clinical study of type 1neurofibromatosis in north west England. J Med Genet 1999;36:197–203.
3. Zoller ME, Rembeck B, Odén A, et al. Malignant and benign tumors in patientswith neurofibromatosis type 1 in a defined Swedish population. Cancer1997;79:2125–31.
The peripheral nerve sheath tumors are tumors arising outsidethe brain and spinal cord. MPNST is a term given to all spindle cellsarcomas arising from the peripheral nerves or existing neurofibro-mas or showing nerve sheath differentiation. Previously, variousterminologies were used to describe sarcomas arising from thenerve sheath, which included neurogenic sarcoma, neurolemmo-sarcoma, malignant fibrosarcoma and neurilemmoma but theWorld Health Organization (WHO) has denoted all such tumorsas MPNST.9
The association of MPNST with NF-1 is well established. Around40% of MPNST cases are found to be associated with neurofibroma-tosis, although among patients with NF-1, the risk of developingMPNST is only about 7%.10 NF-1 is associated with a mutation inthe NF-1 gene, a tumor suppressor gene located on chromosome17q11.2. This gene encodes a protein known as neurofibromin,which is important in the control of neural cell growth throughdownregulation of a ras gene product. The mechanism of malig-nant transformation is not well understood but the two-hithypothesis with loss of heterozygosity may explain malignanttransformation.11

604 Case Reports / Journal of Clinical Neuroscience 20 (2013) 604–606
4. Strauss DC, Qureshi YA, Hayes AJ, et al. Management of benign retroperitonealschwannomas: a single-center experience. Am J Surg 2011;202:194–8.
5. Turitto G, Di Bisceglie M, Moraca L, et al. Retroperitoneal schwannoma: a casereport. Recenti Prog Med 2011;102:307–9.
6. Hope DG, Mulvihill JJ. Malignancy in neurofibromatosis. Adv Neurol1981;29:33–56.
7. Lott IT, Richardson Jr EP. Neuropathological findings and the biology ofneurofibromatosis. Adv Neurol 1981;29:23–32.
8. Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin2002;52:195–215.
9. Friedrich RE, Hartmann M, Mautner VF. Malignant peripheral nerve sheathtumors (MPNST) in NF1-affected children. Anticancer Res 2007;27:1957–60.
10. Patil K, Mahima VG, Ambika L. Malignant peripheral nerve sheath tumour: anelusive diagnosis. Indian J Dent Res 2007;18:19–22.
11. Menon AG, Anderson KM, Riccardi VM, et al. Chromosome 17p deletions andp53 gene mutations associated with the formation of malignant
doi:http://dx.doi.org/10.1016/j.jocn.2012.02.040
Lambert-Eaton myasthenic syndrome in madenocarcinoma of extrapulmonary origin
Anna Chang a, Han-Cheng Wang a, Wei-Chih Hsu a,b,⇑a Department of Neurology, Shin-Kong WHS Memorial Hospital, 95 Wen-Chang Road, Shin-Lb Department of Medicine, College of Medicine, Fu-Jen Catholic University, Xinzhuang District
a r t i c l e i n f o
Article history:Received 22 February 2012Accepted 26 February 2012
Keywords:Extrapulmonary small cell carcinomaLambert-Eaton myasthenic syndromeLEMS
a b s t r a c t
A patient with typical Lambertimal muscle weaknesses, a largrate stimulation electrophysiollung. Here, we present a patienant muscle involvement, a boquencies, and a paraneoplaadenocarcinoma. The purposethe examination of a patient w
1. Introduction
Lambert–Eaton myasthenic syndrome (LEMS) is a paraneoplasticsyndrome involving disordered pre-synaptic neuromuscular trans-mission, with characteristics of easily fatigability, proximal muscleweakness, and mildly affected oculobular muscles.1 The typical elec-trophysiological test includes a reduced resting compound muscleaction potential (CMAP) amplitude, a decremental change of CMAPat low-rate repetitive nerve stimulation (RNS), and a larger-than-100% incremental change of CMAP at high-rate RNS.2 Among theparaneoplastic origins of LEMS, small cell carcinoma of lung (SCLC)is the most common.3 Here we present a patient with LEMS withan atypical clinical manifestation of oculobulbar-predominant mus-cle involvement, a borderline incremental change on high-rate RNS,and a paraneoplastic origin of extrapulmonary mixed small cell car-cinoma (SCC) and adenocarcinoma.
2. Case report
A 73-year-old man presented at the beginning of August 2009with progressive proximal limb weakness, which had initiatedsymmetrically from the lower to the upper body and led subse-
⇑ Corresponding author. Tel.: +886 2 28332211x2598; fax: +886 2 8344906.E-mail address: [email protected] (W.-C. Hsu).
neurofibrosarcomas in von Recklinghausen neurofibromatosis. Proc Nat AcadSci U S A 1990;87:5435–9.
12. Ducatman BS, Scheithauer BW, Piepgras DG, et al. Malignant peripheral nervesheath tumors. A clinicopathologic study of 120 cases. Cancer 1986;57:2006–21.
13. O’Sullivan MJ, Kyriakos M, Zhu X, et al. Malignant peripheral nerve sheathtumors with t(X;18). A pathologic and molecular genetic study. Mod Pathol2000;13:1253–63.
14. Coindre JM, Terrier P, Guillou L, et al. Predictive value of grade for metastasisdevelopment in the main histologic types of adult soft tissue sarcomas: a studyof 1240 patients from the French Federation of Cancer Centers Sarcoma Group.Cancer 2001;91:1914–26.
15. Sordillo PP, Helson L, Hajdu SI, et al. Malignant schwannoma–clinicalcharacteristics, survival, and response to therapy. Cancer 1981;47:2503–9.
ixed small cell carcinoma and
in District, Taipei, Taiwan, New Taipei City, Taiwan
–Eaton myasthenic syndrome (LEMS) has a clinical manifestation of prox-er-than-100% incremental change in repetitive nerve stimulation on high-ogical testing, and a paraneoplastic origin from small cell carcinoma of thent with an atypical myasthenic syndrome with an oculobulbar-predomi-rderline incremental change in repetitive nerve stimulation at high fre-
stic origin from extrapulmonary mixed small cell carcinoma andof this report is to emphasize the importance of painstaking scrutiny inith a less-common presentation of LEMS.
� 2012 Elsevier Ltd. All rights reserved.
quently to ambulatory dependence within 2 weeks. Moreover, asimultaneous oculobulbar involvement with bilateral ptosis, dys-arthria, and dysphagia were also noted, however neither sensorysymptoms nor consciousness disturbance was apparent. Furtherweakness forced him to become bedridden within 2 weeks; thus,he sought medical help at the local hospital.
The patient was in semi-comatose state on arrival because ofcarbon dioxide retention. Neurological examination showed sym-metrical, predominantly lower and proximal muscle weaknesses(Medical Research Council, grade 2 in lower limbs and grade 3 inupper limbs) with severe bulbar palsy, bilateral ptosis, and hypoac-tive tendon reflexes. Brain and cervical spine MRI were normal. Adecremental response at 3-Hz-RNS (11% in left trapezius muscle)was found. Myasthenia gravis (MG) was suspected, and he had a5-course plasma exchange. His oculobulbar symptoms hadimproved slightly with a longer duration of eye opening and lessdysarthria, yet he still remained bedridden. He was referred toour hospital for a second opinion 6 weeks later.
On assessment at admission, the patient’s clinical manifesta-tions were similar to previous records, except for a relatively alertconsciousness. Electrophysiological studies showed normal nerveconduction, including CMAP (4.0 mV in the median nerve, 6.6 mVin the ulnar nerve) and sensory nerve action potential amplitudes(34 lV in the median nerve, 25 lV in the ulnar nerve). RNS testsshowed a decremental change at 3 Hz (14% in left abductor