-
British Journal of Ophthalmology, 1989, 73, 488-493
Simultaneous spontaneous and primary surgical repairof
eyelidsHEMANT K MEHTA
From the Department of Ophthalmology, Gwynedd District Hospital,
Bangor, Wales
SUMMARY Fifteen patients with suspected malignant lesions of the
lower eyelids or inner canthalregion, needing large excisions, were
managed as day cases with spontaneous repair andsimultaneous
subtotal primary surgical reconstruction under local anaesthesia.
For lesionsconfined to the lower eyelid, only those patients
requiring full-thickness margin-inclusive (FTMI)excisions of more
than half the horizontal extent of the eyelid are included in this
study - the largestexcision being 21 x 6 mm. For malignant lesions
of the inner canthus, only those patients needingmoderate to large
excision of inner canthal skin and orbicularis with simultaneous
FTMI excision ofthe medial one-third (8x5 mm) of the upper as well
as the lower eyelid are included. The 16thpatient had traumatic
loss of inner canthal tissue. The final cosmetic and functional
results in all 16patients were satisfactory and comparable with the
results of competent and in-toto primarysurgical reconstructions.
For large excisions at the inner canthus spontaneous with partial
primarysurgical repair allows the use of a less extensive and less
elaborate surgical procedure that is withinthe capabilities of most
ophthalmic surgeons.
The potential of the lower and upper eyelidsindividually-each on
its own-to yield a nearlynormal functional and cosmetic result
solely byspontaneous repair after a moderate sized full-thickness
margin-inclusive (FTMI) excision has beenestablished.'2 Before that
it had long been knownthat a competent primary and in-toto surgical
recon-struction after such FTMI excisions also producesnear normal
results. So far the combined manage-ment by primary surgical
reconstruction of part of theexcised area and simultaneous
spontaneous repair ofthe residual defect has not been reported.
This studydemonstrates the results of such combined manage-ment
after moderate to large FTMI excisions of thelower eyelid, and
large deep excisions of innercanthal skin and orbicularis with
contiguous FTMIexcisions of medial one-third of the upper as well
asthe lower eyelids.
Patients and methods
Fifteen consecutive patients with suspectedmalignant tumours
involving the lower eyelidmargin, or inner canthal skin, and
needing excisionsCorrespondence to H K Mehta, FRCS, Derwen Deg,
Bangor,Gwynedd LL57 2BN.
of 13 mm or more (that is, larger than ½/2 thehorizontal extent
of an eyelid) underwent combinedtreatment with spontaneous repair
and simultaneouspartial surgical reconstruction under local
anaes-thesia as day cases. One other patient involved in atraffic
accident had general anaesthesia. The ages ofthese 16 patients
ranged between 43 and 88 years,with five patients aged between 43
and 60, sevenbetween 61 and 80, and four between 81 and 88.Their
average age was 69 years. The average follow-up period was 17
months, ranging between 6 monthsand 3-8 years.These 16 patients can
be subdivided into three
groups: Group 1: Full-thickness margin-inclusive(FTMI) excision
of lower eyelid. Five patient hadFTMI excision of more than half
the horizontal and6 mm of vertical extent of the lower eyelid.
Thesmallest excision was 13x7 mm and the largest was21x6 mm. These
FTMI defects underwent partialsurgical reconstruction by one of the
following threemethods:
(i) For very large FTMI excision of the lower lid,subtotal
full-thickness surgical reconstruction of onlythe central area of
the defect was carded out in twolayers-posterior lamellar and
cutaneous-with atarsoconjunctival sliding flap from the
ipsilateral
488
on July 6, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.7.488 on 1 July 1989.
Dow
nloaded from
http://bjo.bmj.com/
-
489Simultaneous spontaneous andprimary surgical repair
ofeyelids
1H
IE IF
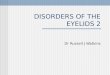
Fig. 1 (A) Rodent ulcer of 7years' duration, involving medial
two-thirds of left lower eyelid margin and palpebralconjunctiva in
a Caucasian male aged 64, treated under local anaesthesia as a day
case. (B) FTMI excision of26 x6 mm(including 5mm ofinner canthal
skin), with 4x5 mm FTMI excision ofupper eyelid. The extent of
excision is shown by thearea xabcfg in Fig. 2. (C, D) The central
cross hatched area dehk (Fig. 2) of13x6 mm was repaired in full
thickness with atarsoconjunctival slidingflap and a full-thickness
postauricular skin graft. The remaining defects xabcdk and efgh
(Fig. 2)were allowed to heal by spontaneous repair. (E) Appearance
at one week. (F) Final appearance at3 months. Note the
author'smodification ofDesmarres' retractor in Fig. C.
upper eyelid, and a full-thickness skin graft (FTSG)to cover the
sliding tarsoconjunctival flap. About3 mm of the FTMI defect on
either side of thiscentrally reconstructed defect was allowed to
heal byspontaneous repair. For the patient depicted in Fig.1A-F a
large FTMI excision of 26x6 mm was carriedout. Of this large defect
only the central area of 13 x6mm was reconstructed in
full-thickness (that is, intwo layers) with a tarsoconjunctival
sliding flap fromthe ipsilateral upper eyelid. The sliding flap
includeda 3 mm tarsal strip and Muller's muscle. This flap
wassutured to the horizontal edge of the remnant of thepalpebral
conjunctiva of the lower lid. The anteriorlamella was restructed
with a 13 x 6 mm full-thicknessskin graft tethered with marginal
and central sutures.The remaining FTMI defects xabcdk and efgh
(Fig. 2)were allowed to undergo spontaneous repair.
Thetarsoconjunctival flap was severed on the 7th day. Inretrospect
this division should have been postponedfor at least three more
weeks to avoid the formationof the small notch at the junction of
the lateralquarter of the lower lid.
(ii) For moderate to large (13-18x6 mm) FTMIdefects of the lower
eyelid only the posterior lamellar
defect was repaired with a tarsoconjunctival flapfrom the
ipsilateral upper eyelid. The anteriorlamellar defect superficial
to the tarsoconjunctivalflap was allowed to heal by spontaneous
repair. Thehorizontal extent of the tarsoconjunctival flap was6 mm
less than that of the FTMI excision, as it isusually possible to
pull together the sides of FTMIdefects by a quarter (that is, 6 mm)
of the full widthof an eyelid. Therefore the entire posterior
lamellawas made good without leaving any defect of theposterior
lamella. The anterior lamella was notreconstructed with an FTSG,
but was allowed to healspontaneously. The tarsoconjunctival flap
wassutured to the three sides of the posterior lamellardefect and
was divided, under local anaesthesia, as aday case, at a second
stage in about three weeks. (Fig.3A-F).
(iii) In two patients the tumour did not involve thelid margin
but came to within 3 mm of the margin. Inthese cases an
asymmetrical FTMI excision wascarried out. The cutaneous lamellar
excisionextended 8 mm downwards from the lid margin and13 mm
horizontally. The posterior lamellar excisionwas 3 mm in height
from the lid margin and a full
IA
ID
on July 6, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.7.488 on 1 July 1989.
Dow
nloaded from
http://bjo.bmj.com/
-
Hemant K Mehta
b
C aFig. 2 Diagramatic representation to simplify
descriptionsofthe surgical procedurefor Fig. 1. Vertically striped
areasxabcdk and efgh were allowed to heal by spontaneous
repair.
13 mm in horizontal extent. Therefore the FTMIexcision was 13 x3
mm, the remaining excision beingof the anterior lamella. In these
patients, only theentire anterior lamellar defect was made good
withskin graft (FTSG) of 13x 8 mm and the entireposterior lamellar
defect of 13 x 3 mm was allowed toheal by spontaneous repair (Fig.
4A-D).Group 2: Large excision of inner canthal skin and
orbicularis with simultaneous contiguous FTMIexcisions ofmedial
one-third ofthe upper as well as the
3A
lower eyelid. In 10 patients in this group such wideexcision was
mandatory because the rodent ulcerswere in theatening proximity to
the upper and lowereyelids. The average excision in this group was
30x25mm, including the FTMI excisions of the upper andlower
eyelids. The inner canthal skin and orbicularisdefect was made good
with a skin graft (FTSG) bytethering the skin graft to the
periosteum with centraland marginal sutures by the author's
technique,described previously.34IThe FTMI defects of themedial
one-third (8x5 mm) each of the upper andlower eyelid were allowed
to heal by spontaneousrepair (Figs. 5, 6A-E).Group 3: Traumatic
lacerations with loss of inner
canthal tissue. There was only one patient in this'group'. She
had severe bony injuries of limbs, FTMIlacerations of left upper
eyelid, caruncle, plica, andseverance of the medial canthal tendon,
as well asloss of an irregular patch of skin and orbicularis
about10 mm in diameter overlying the lacrimal sac.Primary surgical
repair only of the FTMI lacerationof the upper eyelid was carried
out. The remainingperipalpebral wounds were allowed to heal
byspontaneous repair.
SURGICAL TECHNIQUE AND MANAGEMENTThe 15 patients with eyelid
tumours were treated asday cases. The excision and partial surgical
recon-
iii
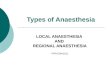
3D- 3E 3FFig. 3 (A) Rodent ulcer ofleft lower eyelid margin in a
Caucasian male aged 65. (B) FTMI excision 13x 7mm. Ipsilateralupper
eyelid is shown everted to obtain a tarsoconjunctival slidingflap
of8mm in horizontal extent and including 8x3 mmtarsal strip with
attached Muller's muscle. The sides ofthe FTMI excision of13 mm
were pulled together by about 6 mm tosuture the 8mm wide
tarsoconjunctivalflap to the remnant ofthe lower lid conjunctiva on
the three sides. The anterior lamellardefect was allowed to heal by
spontaneous repair. (C) Appearance ofthe tarsoconjunctivalflap on
the seventh postoperativeday. (D) Appearance at three weeks,
immediately after the severance ofthe tarsoconjunctivalflap. The
anterior lamellar defecthas healed by nearly 75%. (E, F) Final
appearance at three months.
490
on July 6, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.7.488 on 1 July 1989.
Dow
nloaded from
http://bjo.bmj.com/
-
491Simultaneous spontaneous andprimary surgical repair
ofeyelids
4B
41)
Fig. 4 (A) Keratoacanthoma oftwo years' duration, affecting the
right lower eyelid ofa Caucasian male aged 71. Theexcision was
asymmetrical in that the cutaneous lamellar excision extended 8mm
downwards from the lid margin and was 13mm in horizontal extent.
The posterior lamellar excision was 3mm in height and 13mm
horizontally. The FTMI defect wastherefore 13x3 mm. (B) The entire
anterior lamellar defect was restructured with a 13x8mm FTSG, while
the posteriorlamellar defect was allowed to heal by spontaneous
repair. (C, D) Final result at three months.
struction was carried out under local anaesthesia withlignocaine
2% and bupivacaine 05% (Marcain) withadrenaline. The patient with
traumatic lacerationhad numerous bony injuries for which she
hadgeneral anaesthesia. The partial surgical repair of herpalpebral
and surrounding injuries was carried out atthe same time. The
details of surgical procedures inthe remaining patients have been
given above andwith the captions of Figs. 1 to 6.At the end of the
partial surgical reconstruction
antibiotic eye ointment was instilled and a Cartellashield was
applied as the sole dressing. All patientswere given 2 tablets of
cotrimoxazole (Septrin) twicedaily for 5 days and antibiotic eye
ointment to beapplied twice daily to the eyelids, the skin graft,
and
*its donor site. The patients were seen for the firstdressing at
48 hours, and on the seventh postopera-tive day for removal of
sutures. Thereafter thefollow-up period was progressively increased
toattain six-monthly follow-up.
Results
The functional and cosmetic results were as normaland
satisfactory as the published results of totalsurgical
reconstructions of similar defectsimplemented by various competent
oculoplasticsurgeons."9 There were no palpebral or
ocularcomplications in any patient either during con-valescence or
subsequently. In four patients a
4A
4C
on July 6, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.7.488 on 1 July 1989.
Dow
nloaded from
http://bjo.bmj.com/
-
Hemant K Mehta
dFig. 5 Diagramatic representation of Fig. 6. Area abxcdwas
allowed to heal by spontaneous repair and included 6x5mm FTMI
defect each ofthe upper and lower eyelid. Thereniform cross hatched
area was reconstructed with skin graft(FTSG).
planned second stage minor procedure for severanceof the
tarsoconjunctival flap from the upper eyelidwas carried out under
local anaesthesia as day cases,between one and three weeks after
the initial surgery.The single patient in group 3, with traumatic
loss ofinner canthal skin, developed a pseudoepicanthic
6A
fold which improved to almost normal in about sixmonths. She
also needed minor secondary surgery tocorrect the stenosed everted
left lower lacrimalpunctum. A one-snip dilatation of the punctum
andits repositioning by excision of an ellipse of
palpebralconjunctiva of the lower eyelid at the inner canthuswas
carried out nearly a year after the initial injury.Of suspected
rodent ulcers in the 15 patientshistology confirmed the clinical
diagnosis in 14.Keratoacanthoma was reported in the
remainingpatient. In all the 15 patients complete excision withgood
histological clearance was reported. There hasbeen no recurrence of
tumour in any of these 15patients.
Discussion
The current teaching of oculoplastic surgery is basedon the
assumption that defects created by excision ofpalpebral or
peripalpebral lesions must be repairedimmediately by total primary
surgical reconstruction.Traditionally, FTMI defects of lower
eyelids arereconstituted in two layers-tarsoconjunctival
andcutaneous-at least one of which should be a flapwith it blood
supply intact. The second layer canthen be a free graft from a
remote or adjacent donorsite."" Large defects at either canthus are
usually
6B 6C
Fig. 6 (A) Multicentric rodent ulcer at inner canthus ofa
Caucasianfemale aged 65. The extent ofthe excision was 30 mm
indiameter and included FTMI excision of6 x5mm ofupper lid and
6x6mm ofthe lower lid. Surgery under local anaesthesia asa day case
included skin graft (FTSG) from inner arm sutured with the author's
technique ofcentral and marginal sutures, inthe cross hatched area
ofFig. 5. The FTMI defects (depicted by vertical striped area abxcd
in Fig. 5) and the residual defect ofthe adjoining inner canthal
area, were allowed to heal by spontaneous repair. (B, C) Healthy
appearance onfirst dressing at 48hours. (D, E) Final appearance at
three months and at 18 months.
492
on July 6, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.7.488 on 1 July 1989.
Dow
nloaded from
http://bjo.bmj.com/
-
Simultaneous spontaneous andprimary surgical repair
ofeyelids
repaired with a skin flap from near by.- There are noreports so
far of exploiting the combined manage-ment of spontaneous repair
simultaneously withprimary surgical reconstruction. Therefore,
inaddition to being the first report of such combinedmanagement,
this study highlights the followingpoints: (1) Such combined
management givessatisfactory cosmetic and functional results.
(2)Simultaneous FTMI defects of ipsilateral upper andlower eyelids
(8x 5 mm each) heal as effectively andnormally as does a similar
FTMI defect of each eyelidindividually as already reported.'2 (3)
As a conse-quence of this, large defects at the inner canthus canbe
treated simply with a skin graft (FTSG) underlocal anaesthesia on a
day basis, with the FTMIdefects of both eyelids being allowed to
reform byspontaneous repair. (4) With lesions confined only tothe
lower eyelid large FTMI defects yield satisfactoryresults from the
various methods of subtotal full-thickness or full-width lamellar
surgical reconstruc-tion in conjunction with spontaneous repair of
theresidual defect.The most crucial point to emerge from this study
is
that large excisions at the inner canthus with simul-taneous
FTMI excision of adjacent one-third ofupper and lower eyelids need
a less extensive, simplesurgical reconstruction with a skin graft
(FTSG),which if secured with the central suturing
techniquedescribed by the author34 12 allows consistently
goodresults. These central sutures act as a combinedpressing and
immobilising agent and thereby preventhaematoma formation under the
graft. The patientscan therefore be treated as day cases, without
anyrestrictions on their postoperative activity.
It is not possible to obtain such large skin graftsfrom the
postauricular region, but the supraclavicu-lar region is an
excellent donor site that providesgood colour match. The
conventional method ofsurgical repair of large defects at the inner
canthus isby a rotational skin flap from the forehead. The
maindisadvantage of such a flap is the distortion andscarring
produced on a readily visible part of the face.Moreover, such a
flap does not necessarily provide agood colour match as seen in
some postoperativeresults.""'5 It therefore has no advantage over a
largeskin graft (FTSG), especially if the graft is obtainedfrom the
supraclavicular region, where the skin ishairless and provides a
satisfactory colour match. Inaddition to the reconstruction of the
skin defect at theinner canthus conventional surgical
managementwould have entailed full-thickness reconstruction
inmucosal and cutaneous layers of any coexisting FTMIdefect of the
eyelids. Such reconstructions aredifficult and complex procedures
that demand theskill of a specialist oculoplastic surgeon, whereas,
thecombined spontaneous and partial surgical repair
shown here (Figs. 5, 6) can be carried out by anophthalmic
surgeon with an interest in plasticsurgery.The combined management
does not confer any
worthwhile advantage in the management ofmoderate or large FTMI
excisions confined only tothe lower eyelid, because any surgeon
capable ofinstituting a 12 mm wide tarsoconjunctival slidingflap
from the upper eyelid could almost as readilyobtain an 18 mm wide
flap and a skin graft (FTSG) toreconstruct the entire defect. The
same applies tofull-width but lamellar reconstructions. However,
forthese large FTMI defects confined to the lower lid,the study
documents the feasibility and the scope ofspontaneous repair if
only for its scientific interest.By conventional criteria all 16
patients in this studywould have been treated by primary and
solelysurgical reconstruction in toto to achieve
similarresults.
References
1 Mehta HK. Spontaneous reformation of lower eyelid.Br J
Ophthalmol 1981; 65: 202-8.
2 Mehta HK. Spontaneous reformation of upper eyelid.Br J
Ophthalmol in press.
3 Mehta HK. Assessment of major intraocular and
extraocularsurgery performed as day cases. Trans Ophthalmol Soc UK
1977;97:117-23.
4 Mehta HK. A new method of full thickness skin graft
fixation.Br J Ophthalmol 1979; 63: 125-8.
5 Mustard JC. Repair and reconstruction in the orbital
region.Edinburgh, London, New York: Churchill Livingstone,
1980:182, Fig. 11. 16.
6 Iliff CE, Iliff WJ, Iliff NT. Oculoplastic surgery.
Philadelphia:Saunders, 1979: 247-9, Figs. 9-66 to 9-80.
7 Hatt M. Ophthalmic plastic and reconstructive surgery.
Stuttgart,New York: Thieme, 1986: 120, Fig. 9.25.
8 Callahan A. Reconstructive surgery of the eyelids and
ocularadnexa. Birmingham, Alabama: Aesculapius, 1966: 279,
Figs.287-9.
9 Stasior OG, Callahan A, Korn E, Cerise DP, Kristan RW.Medial
canthal reconstruction. In: Smith Byron C, Della RoccaRC, Nesi FA,
Lisman RD, eds. Ophthalmic plastic and recon-structive surgery. St
Louis, Washington, Toronto: Mosby, 1987;2: 820, Figs. 40.40-45.
10 Mustard JC. Repair and reconstruction in the orbital
region.Edinburgh, London, New York: Churchill Livingstone, 1980:92,
Fig. 7.1.
11 Collin JRO. A manual of systematic eyelid surgery.
Edinburgh,London, Melbourne, New York: Churchill Livingstone,
1983:83-6.
12 Mehta HK. Surgical management of carcinoma of eyelids
andperiorbital skin. Br J Ophthalmol 1979; 63: 578-85, Fig. 4.
13 Mustard JC. Repair and reconstruction in the orbital
region.Edinburgh, London, New York: Churchill Livingstone,
1980:181-2, Fig. 11:16 A-J.
14 Hatt M. Ophthalmic plastic and reconstructive
surgery.Stuttgart, New York: Thieme, 1986: 117, Fig. 9:19.
15 Tenzel RR. Lid reconstruction. In: Smith Byron C, Della
RoccaRC, Nesi FA, Lisman RD, eds. Plastic and
reconstructivesurgery. St Louis, Washington, Toronto: Mosby, 1987;
2: 798-801, Fig. 39:27-30.
Accepted for publication 20 October 1988.
493
on July 6, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.73.7.488 on 1 July 1989.
Dow
nloaded from
http://bjo.bmj.com/