Embed Size (px)
Citation preview

Amit A. Desai*, Dnyanesh M. Belekar**, V. V. Dewoolkar***
Single Dose Antimicrobial Use in Clean and Clean Contaminated Surgical Wounds Prospective Open Control Trial (Of 100 patients)
Abstract
Introduction : Whenever antibiotics are given empirically, in a surgery, they should
be used when local wound defenses are not established. Ideally, maximal blood and
tissue levels of antibiotic should be present at the time, incision is made and also
before contamination occurs.
Continuation of antibiotics beyond the operative day increases the cost of treatment
and may not be useful in reducing site infections.
Many surgical units in various centres have their own protocols regarding use of
antimicrobial drugs in the peri-operative period depending on their unit chief’s
personal experience over years. These protocols may be very effective, although at
times there is excessive use of ‘extra’ drugs. Sadly, many of these effective protocols
are not documented. We now need unbiased evidence based proof of a particular
drug protocol in surgical practice that is actually ‘useful’ for every centre.
We have conducted a prospective and double blind open control trial in a tertiary
care private hospital (single centre) over a period of six months.
Aims and Objectives
1. To Compare the efficacy of peri-operative single dose antimicrobials against the
extended antimicrobials in preventing surgical site infections.
2. To study the effect of factors, that influence surgical site infections, on these
protocols.
3. To study the cost effectiveness of peri-operative single dose antimicrobials
versus the extended dose antimicrobials.
Introduction
he ancient Egyptians were the first civilization to have trained physicians
to treat physical ailments. Way back in 1510, the concept of wound healing appeared as a mystical craft and long associated with religious overtones which was highlighted in the famous saying by a
T
*Assi. Prof., **Asso. Prof., ***Dean and Prof., Dept. of Gen. Surgery, K. J. Somaiya Medical College, Hospital and Research Center, Sion, Mumbai-22.
French military surgeon.
In the days before Joseph Lister, an
English surgeon (1827-1912) said,
surgical patient commonly developed
postoperative “irritative fever,” followed by
purulent drainage from their incisions,
overwhelming sepsis, and often death.
Without antisepsis and asepsis major
surgical operation had been ending in
death, making surgeons helpless in
dealing with wound infection. Lister
41Bombay Hospital Journal, Vol. 53, Special Issue, 2011370

introduced the principles of antisepsis
that decreased postoperative infectious
morbidity substantially. His work
radically changed surgery from an activity
associated with infection and death to a
discipline that could eliminate suffering
and prolong life.
Any infection that occurs at the site of a
surgical incision is called surgical site
infection. The New CDC-definitions for
surveillance of surgical site infections
(1992) take into account 3 classes of
surgical site infections (SSI) :
1. Superficial incisional SSI
2. Deep incisional SSI
3. Organ/space SSI
The most important host-related risk
factors for development of SSI are
advanced age, morbid obesity, disease
severity, an ASA (American Society of
Anaesthesiologist) score > 2, prolonged
preoperative hospital stay, and infection at
distal sites. Microbial contamination of the
surgical site occurs mainly during the
surgical intervention. Although exogenous
contamination may be of concern,
especially in clean operations, most
surgical site infections are caused by
endogenous microorganisms of the
patient’s own commensal flora. SSI rates
vary according to the type and duration of
the surgical procedure and the skill of the
surgeon. Aseptic surgical technique is the
most important factor in the prevention of
SSI. Modification of host risk factors
should be attempted whenever possible. In
addition, adequate protocols for
an t im i c r ob i a l p r ophy lax i s w i th
appropriate antibiotics should be followed.
Surveillance of surgical site infections is
probably beneficial for SSI prevention.
The basic principle of antibiotic
prophylaxis in surgery is to achieve
adequate serum and tissue drug levels
that exceed, for the duration of operation,
t h e M E C s ( m i n i m u m e f f e c t i v e
concentration) or the organism that are
likely to be encountered during the
operation.
The selection of an appropriate
antimicrobial agent depends on the
identification of the most likely pathogens
that are associated with a specific surgical
operation. The prolonged use of
prophylactic antimicrobials is associated
with the emergence of resistant bacterial
strains.
Surgical site infections are the second
most common cause of nosocomial
infections. In hospitals, patients who
develop surgical site infections are up to
60% more likely to spend time in an ICU, 5
times more likely to be readmitted to the
hospital and 2 times more likely to die than
are patients without any SSI. Prophylactic
antibiotics are effective in a wide range of
surgical procedures and have contributed
substantially in reducing post operative
wound infection rates. It has been
estimated that 33% to 50% of antibiotics
used in hospital is for surgical prophylaxis
rather than for treatment. Although
properly administered antibiotics can
reduce post operative SSIs secondary to
preoperative bacterial contamination, use
of broad spectrum antibiotics has
d i sadvantages o f emergence o f
multiresistant organisms. Therefore it is
essential to ensure the quality use of
surgical antibiotic prophylaxis, not only to
improve the drug therapy outcome but
a l s o t o p r e v e n t e m e r g e n c e o f
multiresistant organism strains.
Total 100 patients in each arm were
selected in the study group and control
group who had clean wounds. Patients
with contaminated wounds were excluded
Material and Methods
Bombay Hospital Journal, Vol. 53, Special Issue, 2011 371

from the study.
Patients in the study group received a
single dose of intravenous injection of
amoxycillin, in the operation theatre, just
prior to taking an incision.
The control group patients were given
injection ceftriaxone with sulbactum and
injection metronidazole intravenously
eight hourly for three days followed by
tablet cefixime eight hourly till removal of
sutures.
Anti-diabetic medications were
omitted on the day of surgery and an
insulin drip was started during surgery.
Antihypertensive drugs were given with
sips of water on the morning of surgery.
Immuno-compromised and Australia
antigen positive patients were operated
only on Saturdays in a separate operation
theatre and the operation theatre was
fumigated after the surgery. Shaving at the
operation site was done one hour prior to
surgery using a hair trimmer.
Pre-operative preparation of skin was
done by povidone iodine scrub, spirit and
5% povidone iodine solution.
Skin was sutured with No. 2/0 or 3/0
p o l y a m i d e ( n o n - a b s o r b a b l e ,
monofilament) sutures. Povidone iodine
dressing was given.
In case of discharge from the wound or
induration, the pus was drained and sent
for culture sensitivity.
Age of the patients
The youngest patient was 8 year old
and the eldest 89 year.
Serial Order of the surgery
Following were the serial orders of the
Results
surgeries performed in the study group :
Following were the serial orders of the
surgeries performed in the control group :
Average Cost of Treatment
The average cost of treatment for the
Co-morbid conditions : 1
Parameter
15
2
2
0
1
47
1
Study group
Obesity
HBsAg
HIV
Hypertensive
Alcoholic
Mesh
Drain
2
0
0
0
0
2
2
Infec-tion
16
0
1
3
0
29
13
Controlgroup
2
0
0
0
0
2
2
Infec-tion
Experience of the surgeon
32
46
14
9
Study group
QualifiedSeniors
QualifiedJuniors
UnqualifiedSeniors
UnqualifiedJuniors
3
1
0
0
Infec-tion
35
57
9
3
Controlgroup
0
3
0
0
Infec-tion
Experience
(> 5 yrs, postM.S)
(< 5 yrs, postM.S)
rd(3 yearResidents)
st nd (1 , 2 yearResidents)
Development of wound infection :
Total Number
Study Group
Control Group
100
100
4
3
Cases Wound Infection
Bombay Hospital Journal, Vol. 53, Special Issue, 2011372
Serial order on list
32
27
19
12
3
6
1
st1nd2rd3th4th5th6th7
Study group
1
2
0
0
0
1
0
Infec-tion
35
24
12
16
9
4
1
Controlgroup
1
0
1
1
0
0
0
Infection

study group, was Rs. 150/-, however for
control group was Rs. 1050/-
Statistics
Using Chi-Square Test
Since the observed value (0.1478) is
much lower, we conclude that the null
hypothesis is true and that there is not
much difference between the two protocols
of peri-operative antimicrobial drug
administration.
Discussion
Until the middle of the 19th century,
when Ignaz Semmelweis and Joseph Lister
became the pioneers of infection control by
introducing antiseptic surgery, most
wounds became infected. In cases of deep
or extensive infection this resulted in a 1mortality rate of 70-80%. Since then a
number of significant developments,
particularly in the field of microbiology,
have made surgery safer. However, the
overall incidence of healthcare associated
infections (HAIs) still remains high and
represents a substantial burden of
disease.
In 1992, the US Centers for Disease
Control (CDC) revised its definition of
‘wound infection’, creating the definition 2‘surgical site infection’ (SSI) to prevent
confusion between the infection of a
surgical incision and the infection of a
traumatic wound. Most SSIs are
superficial, but even so they contribute
greatly to the morbidity and mortality
3,4associated with surgery. Estimating the
cost of SSIs has proved to be difficult but
many studies agree that additional bed
occupancy is the most significant factor.
Surgical site infections are classified
into three groups -
• superficial and
• deep incisional SSIs and
• Organ-space SSIs - depending on
the site and the extent of infection.
The CDC definition states that only
infections occurring within 30 days of
surgery (or within a year in the case of
implants) should be classified as SSIs.
Incisional surgical site infections 2must meet the following two criteria :
• occur within 30 days of procedure
• Involve only the skin or
subcutaneous tissue around the
incision.
Superficial incisional SSI
Criteria as per Definition + at least
one of the following must be present :
• Purulent drainage, with or
without laboratory confirmation,
from the superficial incision.
• Organisms isolated from an
aseptically obtained culture of
fluid or tissue from the superficial
incision.
• At least one of the following signs
or symptoms of infection : Pain or
tenderness, localized swelling,
redness or heat.
• Diagnosis of superficial incisional
SSI by the surgeon or attending
physician.
Deep incisional SSI
Criteria as per definition + at least one
Culture of Wound Swab
S. aureus
Study Group
Control Group
2
2
Organism E. coli
1
0
Negative Culture
1
1
Bombay Hospital Journal, Vol. 53, Special Issue, 2011 373

of the following :
• Purulent drainage from deep
incision.
• A deep incision spontaneously
dehisces or is deliberately opened
by a surgeon when the patient has 0either – Fever (> 38 C), localised
pain or tenderness. An abscess or
other evidence of infection involving the deep incision is
found on direct examination,
during reoperation, or radiologic
examination.
• Diagnosis of deep incisional SSI
by a surgeon or attending
physician.
Note : Report infection that involoves both
superficial and deep incision sites
and an organ/space SSI that drains
through the incision as deep
incisional SSI.
Organ/space SSI
Criteria as per definition + at least one
of the following :
• Purulent discharge from a drain
that is placed through a stab
wound into the organ/space.
• Organisms isolated from an
aseptically obtained culture of
fluid or tissue in the organ/space.
• An abscess or other evidence of
i n f e c t i o n i n v o l v i n g t h e
organ/space that is found on
direct examination, during
reoperation, or by histopathology
or radiological examination.
• Diagnosis of an organ/space SSI
by a surgeon or attending
physician.
Aetiology : In a primary infection, the
wound is the primary site of infection,
whereas a secondary infection arises
following a complication that is not directly
related to the wound.
Time : An early infection presented
within 30 days of a surgical procedure,
whereas an infection is described as
intermediate if it occurs between one and
three months afterwards and late if it
presents more than three months after
surgery.
Severity : A wound infection is
described as minor if there is discharge
without cellulitis or deep tissue
destruction, and major if the discharge of
pus is associated with tissue breakdown,
partial or total dehiscence of the deep
fascial layers of the wound, or if systemic
illness is present.
Causes and Risk factors
• Bacterial factors : In our study 2
infections in the study group and
2 infections in the control group
were caused by staphylococcus
aureus (sensitive to Linezolid) and
one infection in the study group
was caused by E. coli (sensitive to
ciprofloxacin and ofloxacin). One
infection in each of the groups was
caused by organisms which could
not be cultured.
• Local wound factors : No
significant difference was noted in
our study, by drain or mesh
insertion on the incidence of local
wound infection in both groups.
• Patient factors : Obesity (B.M.I.
Bombay Hospital Journal, Vol. 53, Special Issue, 2011374

more than 30) predisposed the
patient to an increased risk of
wound infection in our study, but
a significant difference was not
seen between the study and
control group as far as prevention
of wound infection in the obese
patient is concerned.
Bacterial factors
vBacterial no., Virulence,
antimicrobial resistance.
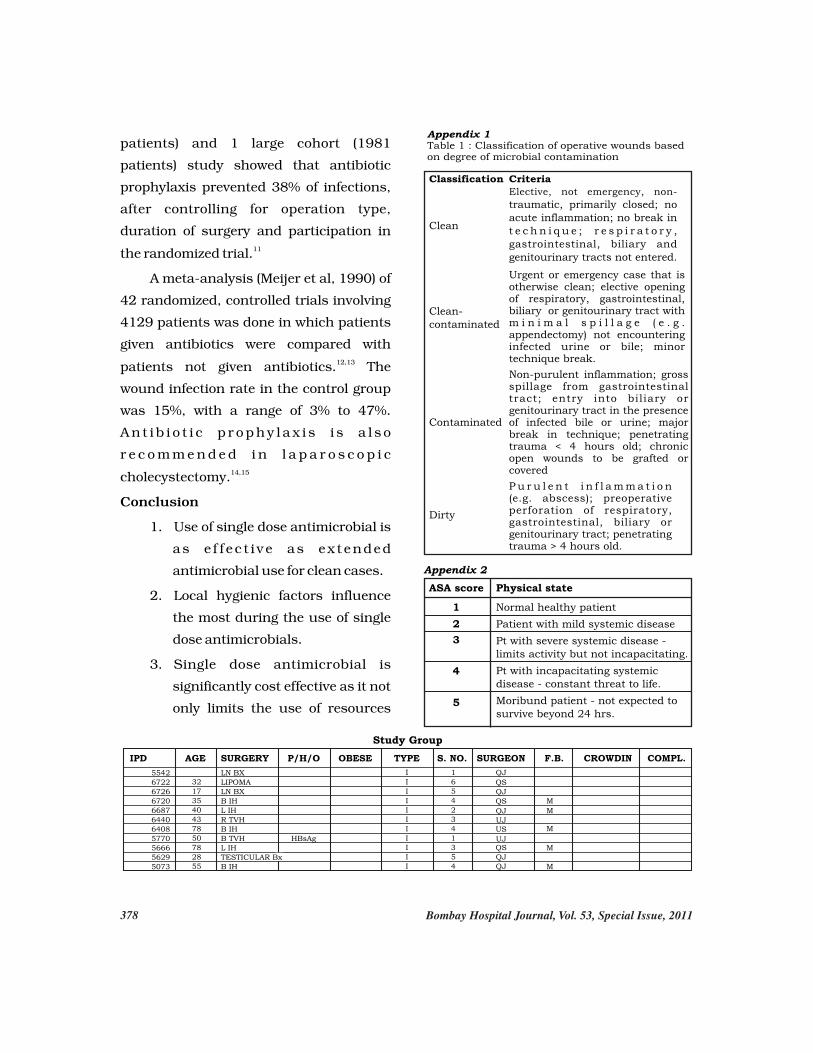
vWound classification : A
system of classification for
operative wounds that is
based on the degree of
microbial contamination was
developed by the US National
Research Council group in 51964. Four wound classes
with an increasing risk of
SSIs were described : clean,
c l e a n - c o n t a m i n a t e d ,
contaminated and dirty. The
simplicity of this system of
classification has resulted in
it being widely used to predict
the rate of infection after
surgery.
vLength of preoperative
hospital stay : The average
length of stay in hospital was
shorter for patients in the
study group. Patients in the
study group stayed for an
average of about 3 days in the
hospital. Patients in the
control group stayed for an
average of 7 days in the
hospital. Most of these
patients were discharged
after suture removal.
However, the length of hospital
stay did not have any significant
impact on the number of post-
operative wound infections.
vRemote site infection at the
time of surgery.
vDuration of the procedure :
Most of the procedures
included in this study lasted
for about 60 minutes. Some
of the difficult procedures
were performed by senior
surgeons and this was
probably the cause for
increased incidence of post-
operative wound infection in
the study groups in the
patients operated by senior
surgeons. On an average,
time taken for a procedure by
s e n i o r s u r g e o n s w a s
considerably less than the
time taken by junior resident
surgeons.
vPre operative shaving : In our
study, we had used clippers
for pre-operative shaving
which was done just one hour
prior to surgery.
vIntensive care unit patient :
Our patients belonged to ASA
grade I, II, III and none of
them were shifted to the
intensive care unit.
vPrior antibiotic therapy :
None of our patients had
received any prior antibiotic
therapy prior to admission.
• Bac te r i a l no . , V i ru l ence ,
antimicrobial resistance.
vT ox ins , r e s i s t ance t o
Bombay Hospital Journal, Vol. 53, Special Issue, 2011 375
phagocytosis, intracellular
destruction.
vS u r f a c e c o m p o n e n t s
( c a p s u l e s ,
lipopolysaccharides)
vBacterial load more than 5 10.
• Duration of the procedure : thProlonged surgeries : > 75
percentile for that procedure.
• Preoperative shaving :
vIncreases risk by 100%.
vExtensive shaving not
needed. Removal by clippers
before procedure preferred.
vPrior antibiotic therapy :
I n c r e a s e s c h a n c e s o f
antibiotic resistance
Local wound factors
vSeroma/Haematoma
vPressure necrosis
vIncorrect sutures
vDrains
vForeign bodies
• All these factors increase the risk
of SSIs.
• Good surgical technique - best
way to avoid SSIs.
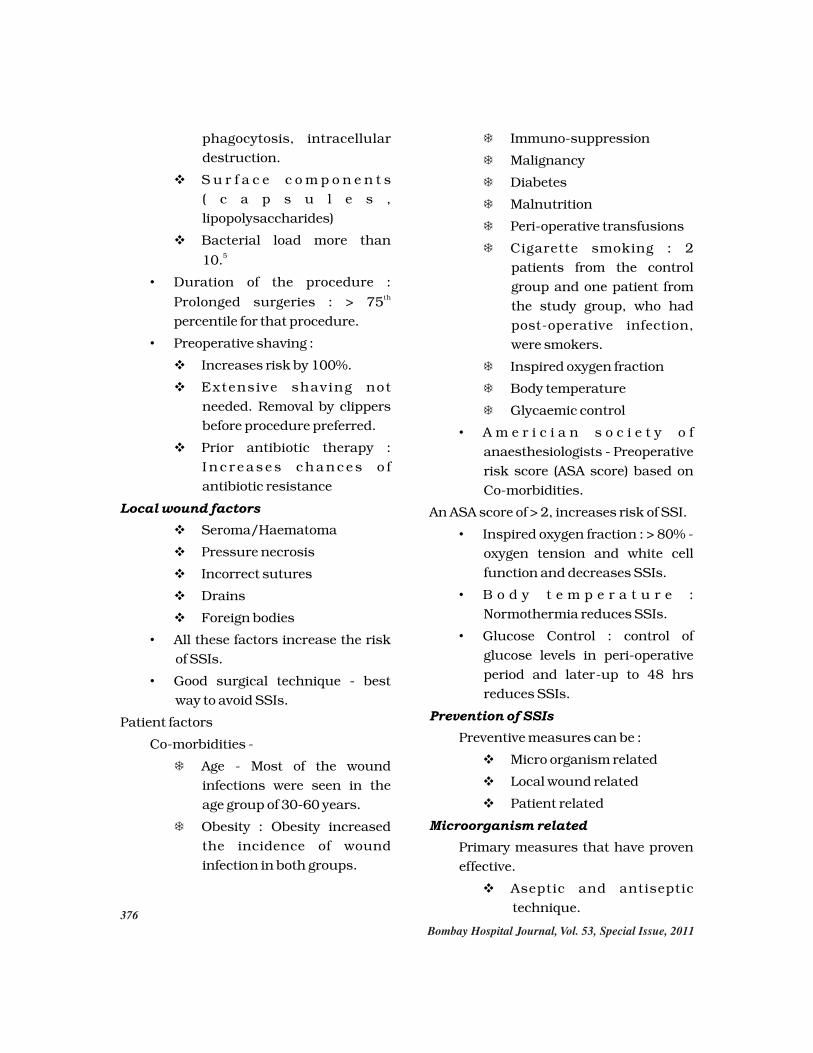
Patient factors
Co-morbidities -
TAge - Most of the wound
infections were seen in the
age group of 30-60 years.
TObesity : Obesity increased
the incidence of wound
infection in both groups.
TImmuno-suppression
TMalignancy
TDiabetes
TMalnutrition
TPeri-operative transfusions
TCigarette smoking : 2
patients from the control
group and one patient from
the study group, who had
post-operative infection,
were smokers.
TInspired oxygen fraction
TBody temperature
TGlycaemic control
• A m e r i c i a n s o c i e t y o f
anaesthesiologists - Preoperative
risk score (ASA score) based on
Co-morbidities.
An ASA score of > 2, increases risk of SSI.
• Inspired oxygen fraction : > 80% -
oxygen tension and white cell
function and decreases SSIs.
• B o d y t e m p e r a t u r e :
Normothermia reduces SSIs.
• Glucose Control : control of
glucose levels in peri-operative
period and later-up to 48 hrs
reduces SSIs.
Prevention of SSIs
Preventive measures can be :
vMicro organism related
vLocal wound related
vPatient related
Microorganism related
Primary measures that have proven
effective.
vAseptic and antiseptic
technique.
Bombay Hospital Journal, Vol. 53, Special Issue, 2011376

vP r o p e r a n t i m i c r o b i a l
prophylaxis.
vI m p l e m e n t a t i o n o f
surveillance programmes.
Aseptic and antiseptic techniques.
Environmental and architectural
character of OT
• Size
• Air management
• Equipment handling
• Traffic rules
• Operating room personnel asepsis
and clothing
Our hospital is a tertiary care centre
as well as teaching institute for
undergraduate and postgraduate
students. It is designed with a reception
area, sterile area and the operation room
(two in number). Surgical equipments are
maintained and autoclaved by trained
personnel and staff nurses. Daily cross
checking of the autoclave procedure is
done by the surgeons of the concerned
surgical unit.
Five undergraduate students are
allowed on any day and they are allowed
entry only after changing into operating
room changes and cap and masks.
Surgical site preparation
• Antiseptic preoperative showers
• Skin preparation of the surgical
site (germicidal antiseptic, incise
drapes)
• Scrubbing (1st time - 5 minutes,
consecutively 3 minutes)
• Alcoholic hand scrub solution
• Sterile drapes and gowns
• Double gloving
To be ef fective, prophylactic
antibiotics must be present in the relevant
tissues at the time the incision is made
and for the duration of the surgical 6procedure. The studies by Burke and a
recent follow-up study have shown for
preoperative antibiotics, those given 2
hours before the incision had the greatest
reduction on wound infection rates. Peri-
operative and postoperative antibiotics
were much less useful in reducing
infections than those given before 7surgery.
In most elective surgical procedures,
single dose antibiotic prophylaxis is
recommended.
3. If a procedure lasts longer than the
half-life of the prophylactic antibiotic
given, a second dose of the antibiotic
is recommended. Subsequent doses,
if necessary should be given at
intervals not longer than twice the
half-life of the drug.
4. The choice of the antibiotic should be
based on the following parameters :
TEfficacy
TSafety and adverse reactions
TEpidemio logy o f expected
pathogen
TLocal resistance pattern
TCost
A meta-analysis of 3 randomized
controlled trials (Codamos, 1999)
concluded that the use of antibiotic
prophylaxis in breast surgery resulted to
a decrease in surgical site infections from 8,9,109.5% to 5.5%. Another meta-analysis
(Platt, 1993) of 1 randomized (606
Bombay Hospital Journal, Vol. 53, Special Issue, 2011 377
Bombay Hospital Journal, Vol. 53, Special Issue, 2011
patients) and 1 large cohort (1981
patients) study showed that antibiotic
prophylaxis prevented 38% of infections,
after controlling for operation type,
duration of surgery and participation in 11the randomized trial.
A meta-analysis (Meijer et al, 1990) of
42 randomized, controlled trials involving
4129 patients was done in which patients
given antibiotics were compared with 12,13patients not given antibiotics. The
wound infection rate in the control group
was 15%, with a range of 3% to 47%.
A n t i b i o t i c p r o p h y l a x i s i s a l s o
r e c o m m e n d e d i n l a p a r o s c o p i c 14,15cholecystectomy.
Conclusion
1. Use of single dose antimicrobial is
as e f f e c t i v e as ex t ended
antimicrobial use for clean cases.
2. Local hygienic factors influence
the most during the use of single
dose antimicrobials.
3. Single dose antimicrobial is
significantly cost effective as it not
only limits the use of resources
IPD AGE SURGERY P/H/O OBESE TYPE S. NO. SURGEON F.B. CROWDIN COMPL.
Study Group
55426722672667206687644064085770566656295073
32173540437850782855
LN BXLIPOMALN BXB IHL IHR TVHB IHB TVHL IHTESTICULAR BxB IH
HBsAg
IIIIIIIIIII
16542341354
QJ
QSQJQS
QJUJUS
UJQSQJQJ
M
M
M
M
M
Appendix 2
ASA score Physical state
Normal healthy patient
Patient with mild systemic disease
Pt with severe systemic disease -limits activity but not incapacitating.
Pt with incapacitating systemicdisease - constant threat to life.
Moribund patient - not expected tosurvive beyond 24 hrs.
1
2
3
4
5
Elective, not emergency, non-
traumatic, primarily closed; no acute inflammation; no break in t e c h n i q u e ; r e s p i r a t o r y , gastrointestinal, biliary and genitourinary tracts not entered.
Clean
Urgent or emergency case that isotherwise clean; elective opening of respiratory, gastrointestinal, biliary or genitourinary tract with m i n i m a l s p i l l a g e ( e . g . appendectomy) not encountering infected urine or bile; minor technique break.
Clean-contaminated
Non-purulent inflammation; grossspillage from gastrointestinal tract; entry into biliary or genitourinary tract in the presenceof infected bile or urine; majorbreak in technique; penetratingtrauma < 4 hours old; chronic open wounds to be grafted or covered
Contaminated
P u r u l e n t i n f l a m m a t i o n (e.g. abscess); preoperative perforation of respiratory,gastrointestinal, biliary or genitourinary tract; penetratingtrauma > 4 hours old.
Dirty
Appendix 1Table 1 : Classification of operative wounds based on degree of microbial contamination
Classification Criteria
378

Bombay Hospital Journal, Vol. 53, Special Issue, 2011
IPD AGE SURGERY P/H/O OBESE TYPE S. NO. SURGEON F.B. CROWDIN COMPL.
Study Group
6072
5801
6327
6465
6512
6395
6412
6648
6787
6840
7818
6
30
28
46
1.5
65
22
49
50
45
40 HIV
YI
I
I
I
I
I
I
I
I
I
I
2
1
4
2
1
2
2
3
3
4
1
QS
US
QS
QS
QJ
QJ
QJ
QJ
QJ
QJ
QJ
M
M
M
M
D
M
L IH
TVH
SSG
B IH
CIRCUMCISION
L IH
R FIBROAD.
L IH
R IH
AX. LIPOMA
R IH
[9] 809/1459/152[9] 729/3839/755
9/628[9]689/9009/9029/1030
[9]3972
[9]3801
[9]4253
[9]3759
[9]44264
489848474434441739693723736276497818
40454036422548485120555460536995
3490351659236722506756817548
4494
4495
4575
4623
4876
5000
5172
5193
5182
5181
5208
5195
5478
5809
5747
5409
5366
59001
5903
5909
60608
5954
5963
5850
28
30452840
55405041
32
5218326225262817
55
65
16
43
64
58
5
1.5
25
42
6
70
35
2.5
65
35
60
60
1.5
39
39
38
32
84
55
65
2
59
25
46687532321465
3075212226
PAROTIDR TVHLIPOMAR IHR IHIHSCC EXCISIONPAROTIDINC. HERNIATUMORAL CAL.FIBROAD.FIBROAD.LIPOMAFIBROAD.
R IH
INC. HERN
LABIAL CYST
FEM. HERINA
R TVHCIRCUMCB IHSEB CYSTB IHLIHR IHR IHR IH
LIPOMASEB. CYSTFIBROAD.FIBROAD.FIBROAD.B TVHCIRCUMCISIONORCHIECTOMYLIPOMABR. BIOPSYFIBROAD.INC. HERINA
LIH
L ORCHIDECTOMY
RIH
RIH
BURSAB TVH
INC. HERNIA
L FIBROAD.
INC. HERNIA
BIH
LIH
CIRCUMCISION
LIH
SSG
L FIBROAD.
UMB. HERNIALIPOMA
L MRM
FRENULOPLASTY
RIH
BIH
INC. HERINA
LIVER BIO CIRR.
FRENULOPLASTY
R IH
n
n
HIV
nn
n
n
IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII
I
I
I
I
I
I
II
I
II
I
I
I
I
I
I
I
I
II
I
II
I
II
I
I
1111114214123122621124353211
1376311
2322
6
13242111
631631234112314
2
USQJUSQSQJQJQJQJQJQS
USUJQJQJ
USQSQSQSQJ
USUJQSQSUJUJUSQJ
QJUJUS
QSQS
USUJQJ
QJ
QSQSQJ
QJ
QJ
QSUSQJQSUJQJQJ
QS
USQSUSQSQJQS
QJQSQJQJQJQSQJ
QJ
QS
M
MMMMM
D
M
MM
DM.D
M.D
M
M
M
M
M
M
D
M
M
D.M
M
M
M
M
COMPL.
COMPL.
>>>
COMPL.
379
Y

Bombay Hospital Journal, Vol. 53, Special Issue, 2011
123
383
432
168
540
418
715
979
1353
1563
1537
1812
1666
1895
18109
27
32
66
77
24
58
40
54
80
5
19
60
60
1.5
29
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
2
3
1
2
2
3
3
4
1
2
2
3
2
2
2
QJ
QS
QJ
QJ
QJ
QJ
QS
QS
QJ
QS
QJ
US
QJ
QS
QS
M
M
M
M
M
M
M
M
M
M
M
M
M
L IH
R IH
L IH
R IH
R IH
B IH
R IH
L IH
R IH
R IH
R IH
L IH
R IH
R IH
L IH
Y
but also decreases the overall
hospital stay.
1. Altemeier WA. Sepsis in surgery. Presidential
address. Arch Surg 1982; 117(2):107-12.
2. Horan TC, Gaynes RP, Martone WJ, Jarvis WR,
Emori TG. CDC definitions of nosocomial
surgical site infections, 1992; a modification of
CDC definitions of surgical wound infections.
Infect Control Hosp Epidemiol 1992;
13(10):606-8.
3. Leaper DJ, van Goor H, Reilly J, et al. Surgical
site infection - a European perspective of
incidence and economical burden. Int Wound
Journal 2004; 1(4):247-273.
4. Dipiro JT, Martindale RG, Bakst A, et al.
Infection in surgical patients : effects on
mortality, hospitalization, and postdischarge
care. Am J Health Syst Pharm 1998; 55(8):777-
81.
5. Berard F, Gandon J. Postoperative wound
infections : the influence of ultraviolet
irradiation of the operating room and of various
other factors. Ann Surg 1964; 160 (Suppl 1) : 1-
192.
6. Classen DC, Evana Rs. et al. The Timing of
prophylactic administration of antibiotic of
antibiotics and the risk of surgical wound
infection. N. Engl. Med. 1992; 326:281-286.
7. Di Piro JT, Bowden Jr, TA, Hooks Ii VH.
Prophylaxis parenteral cephalosporins in
surgery. Are the newer ones better? JAMA
1984; 252:3277-3279.
8. Platt R. Zucker JR, Zaleznik DF, Hopkins CC, et
al. Perioperative antibiotic prophylaxis and
wound infection following breast surgery.
Journal of Antimicrobial Chemotherapy 1993;
References
31; Supplement B:43-48.
9. Codamos LJ, Catungal MM, Coronel RF.
Antibiotic prophylaxis for breast surgery : a
meta-analysis of randomized placebo-
controlled trials. Phillippine Journal of
Surgical Specialties 2000; 55(1):30-32.
10. Platt R, Zaleznik DF, Hopkins CC, et al.
Perioperative antibiotic prophylaxis for
herniorrhaphy and breast surgery. The New
England Journal of Medicine, 1990; 322:153-
60.
11. Platt R, Zucker JR, Zaleznik DF, et al.
Prophylaxis against wound infection following
herniorhaphy or breast surgery. The Journal of
Infectious Disease, 1992; 166:556-60.
12. Meijer, WS, Schmitz PI. Prophylactic use of
cefuroxime in biliary tract surgery :
Randomized controlled trial of single va
multiple doses in high risk patients. Galant
trial study group. Br J Surg., 1993 July;
80(7):917-21.
13. Meijer WS, Schmitz PIM, Jeekel J. Metaanalysis
of randomized controlled antibiotic prophylaxis
in biliary tract surgery. Br. J. Surg., 1990,
March; 77:283-290.
14. Higgins A, London J. et al. Prophylactic
antibiotics for elective laparoscopic
cholecystectomy : Are they necessary? Arch
Surg, 1999; Jun; 134(6):611-3; discussion
614. National library of medicine. Medline.
15. Illig K.A., et al. Are prophylactic antibiotics
r equ i r ed f o r e l e c t i v e l apa r oscop i c
cholecystectomy? J Am Coll of Surg., 1997;
184(4):353-6.
380