Embed Size (px)
Citation preview

Site of Heart Block in AcuteMyocardial Infarction
By KENNETH M. ROSEN, M.D., HENRY S. LOEB, M.D., RUBEN CHUQUIMIA, M.D.,
M. ZIAD SINNO, M.D., SHAHBUDIN H. RAHIMITOOLA) M.B., M.R.C.P.E.,
AND Roit M. GUNNAR, M.D.
SUMMARYBundle of His electrograms were recorded in eight patients with acute myocardial
infarction and heart block. Three patients with diaphragmatic myocardial infarction(DMI) and one with subendocardial infarction were characterized by slowing or blockabove the bundle of His and A-V junctional escape rhythms during periods of ad-vanced or complete block. An additional patient with DMI had block in the His bundleitself. Intraventricular conduction in the above patients was characterized by normalH-Q intervals (35 to 60 msec) and absence of widened QRS. In contrast, three pa-
tients with anterior infarction (AMI) manifested complete block below the bundle ofHis and idioventricular escape. P-H intervals were normal (80 to 140 msec) and A-Vconduction was considered unaffected. Our electrophysiologic observations coupledwith previous clinical, anatomic, and pathologic findings suggest that the heart blockin DMI is usually due to an ischemic lesion of the A-V node, while heart block inAMI is due to necrosis involvi-ig both bundle branches.
Additional Indexing Words:Wenckebach periods A-V node
IN MYOCARDIAL infarction with heartblock, the site of infarction may determine
the nature of block.1-3 It is suggested thatdiaphragmatic infarction (DMI) producesblock by virtue of reversible ischemia to theA-V node.4'5 In addition, DMI has beencharacterized by periods of type I block(Wenckebach), junctional rhythms, and abenign course.'-3
In contrast, anterior infarction (AMI) withblock is associated with massive septalinvolvement with necrosis of the bundle
From the Department of Adult Cardiology of theHektoen Institute for Medical Research and CookCounty Hospital and the Department of Medicine ofthe University of Illinois College of Medicine,Chicago, Illinois.
Supported in part by Grant HE-08834-06S1 fromthe National Heart and Lung Institute, U. S. PublicHealth Service.
Received June 16, 1970; revision accepted forpublication July 29, 1970.
Circulation, Volume XLII, November 1970
Mobitz block His bundle electrogram
branches.4 5 AMI with block has also beencharacterized by the occurrence of type IIblock, idioventricular rhythms, and highmortality." 2
In the present study, we have attempted tolocalize the physiologic site of block inpatients with acute myocardial infarction byrecording His bundle electrograms during theperiod of conduction disturbance.
MethodsClinical Material
Eight patients with acute myocardial infarctionand heart block were studied. All patients wereadmitted to the Intensive Coronary Care Unit ofCook County Hospital. Clinical data on thepatients are summarized in table 1. Pathologic Qwaves were present in six patients, with patternsdiagnostic of DMI in four and AMI in two. Onepatient was considered to have subendocardialinfarction because of widespread ST depressionsand T-wave inversions without Q waves. Onepatient had complete heart block (CHB) with anidioventricular rhythm on admission, and the
925
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

Table I
Clinical Data and Electrocardiograms
ElectrocardiogramLeads with
Age pathologic ST-segmentPatient (yr) Sex History Q waves changes Other
1 A.Jon 70 F Chest pain II, III, aVF Elev. in II, IIIand aVF
2 A.Joh 53 F Chest pain; III, III, aVF Elev. in II, IIIdyspnea and aVF
3 L.B. 55 F Chest pain; II, III, aVF Elev. in II, IIIsyncope and aVF
4 G.S. 70 M Chest pain; II, III, aVF Elev. in II, IIIdyspnea and aVF
5 F.K. 82 M Abdominal pain; Idioventricularsyncope rhythm
6 I.W. 62 F Chest pain; V1-V3 Elev. in V1-V5 RBBB with LADdyspnea
7 A.M. 48 M Chest pain; V1-V3 Elev. in VI-V4 RBBB with RADdyspnea
8 B.D. 52 M Chest pain None Dep. in II, III,aVF and VI-V6
Abbreviations: Elev. = elevation; Dep. = depression; RBBB = right bundle-branch block; LAD = left axis deviation;RAD = right axis deviation; AVB = A-V block; NSR = normal sinus rhythm; PM = postmortem examination.
diagnosis of acute AMI was made at autopsy.Elevations of serum glutamic oxalacetic transami-nase, serum lactic dehydrogenase, and creatininephosphokinase were noted in all patients.
ArrhythmiasA diagnosis of first degree A-V block was made
when the P-R interval was greater than 0.20 sec.Second degree A-V block was defined as
incomplete A-V block with sinus rhythm anddropped ventricular beats. Second degree blockwas classified into Mobitz type I (Wenckebach)block characterized by increasing prolongation ofP-R interval preceding the dropped beat andMobitz type II block, characterized by droppedbeats without change in the preceding P-Rintervals. Advanced A-V block was defined as
incomplete A-V block with a 2:1 or greaterdegree of block. Complete heart block wasdefined as periods of complete A-V dissociationwith atrial rates faster than ventricular rate.The arrhythmias observed are summarized in
table 1. The patients-with DMI as well as thepatient with subendocardial infarction had seconddegree or advanced A-V block on admission.Three of the patients with DMI and the patientvith subendocardial infarction all manifested
Wenckebach periods at some time during theirhospital stay. Three patients with DMI and thepatient with subendocardial infarction survived.One of the patients with AMI had CHB at the
time of admission. The other two were admittedwith normal sinus rhythm and right bundle-branch block, one with left (-300) and the otherwith right (+120°) axis deviation. In the lattertwo, sudden CHB developed on hospital day 5and 7, respectively, without preceding periods ofsecond degree block. CHB was permanent in twoof the patients with AMI (patients 5 and 6) andintermittent in one (patient 7) who had shortperiods of normal sinus rhythm. All patients withAMI and block died with either congestive failureor shock.
Electrophysiologic StudiesStudies were undertaken at the time of
transvenous pacemaker insertion in all patientsexcept patient 3 who was studied electivelyduring first degree A-V block. His bundleelectrograms were recorded by previouslydescribed technic.6' 7 A 6 or 7F tripolar catheterwas percutaneously passed via the right femoralvein and positioned across the tricuspid valve.Bipolar leads from the catheter were led into
Circulation, Volume XLII, November 1970
926 ROSEN ET AL.
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEART BLOCK IN MYOCARDIAL INFARCTION
Rhythms andconduction defects
observed
2°AVB (type 1);advanced AVB;
CHB20 AVB (type 1);advanced AVB;
CHB10 AVB; NSR
2°AVB (type 1);10AVB; NSR
Advanced AVB (2:1);NSRCHB
NSR; CHB
NSR; CHB
20 AVB (type 1);advanced AVB;CHB; 10 AVB;
NSR
Subendocardial
Outcome
Died in shock;PM: acute diaphragmatic infarction
Alive; return to NSR
Alive; return to NSR
Alive; recurrence of 2:1 block
Died in shock;PM; massive anteroseptal
infarctionDied in shock
Died in congestive heart failure
Alive; discharged in NSR
separate a-c inputs of the ECG preamplifiers of a
multichannel oscilloscopic photographic record-er.* Filter frequencies were set at 40 to 500 Hz.The catheter was then slowly withdrawn untilposition was optimal for recording of His bundlepotentials. ECG was recorded simultaneously.Recordings were made at paper speeds of 100and 200 mm/sec.The following intervals were measured in
milliseconds.1. P-H interval: the interval between the P
wave and the His bundle potential (normal80 to 140 msec).8
2. H-Q interval: the interval between the Hisbundle spike and the initial deflection ofthe QRS complex (normal 30 to 60msec) .8
The site of block was above or below thebundle of His, depending on the relation of theHis bundle spike to the atrial and ventricularelectrograms.9
ResultsThe results of the electrophysiologic studies
are summarized in table 2.
Diaphragmatic Infarction
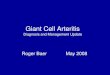
The predominant rhythms in patient 1noted during the study were 2:1 A-V blockand CHB. Atrial rate was about 100/min.During 2:1 block (fig. 1), conducted P waves
alternated with blocked P waves which were
not followed by His bundle deflections.During CHB (fig. 2), there was a regularventricular rhythm unrelated to atrial activity.Ventricular complexes were supraventricularin configuration and were all preceded by Hisbundle spikes, with H-Q intervals of 35 msec.
Thus, block occurred above the bundle of His,with junctional escape.
In patient 2, both advanced A-V block andCHB were noted. In advanced block, thepredominant rhythm was 2:1 A-V block withjunctional escape following the blocked Pwave and causing interference with conduc-tion of the third P wave of the sequence (fig.3A). The blocked P waves were not followedby conducted His bundle spikes. The resultsduring CHB were similar to those in patient 1
except that the junctional rhythm was faster
Site of infarction
DMI
DMI
DMI
DMI
AMI
AMI
AMI
*Electronics for Medicine, DR8 or Hewlett Packard(with modified frequency response).Circulation, Volume XLII, November 1970
927
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

Table 2
Results of Electrophysiologic Studies
Rate duringadvanced or complete heart block P-H H-Q
Patient Site of Rhythms At. Vent. interval intervalno. infarction during study (rate/min) (rate/min) (msec) (msec) Site of block
1 DMI Advanced AVB; 100 48 35 Above H-CHB
2 DMI Advanced AVB; 120 66 34 Above HCHB
3 DMI 10 AVB 180 40 Above H4 DMI Advanced AVB; 96 48 100* 60 In H
NSR5 AMI CHB 109 36 104 Below H6 AMI CHB 80 <40 140 Below H7 AMI CHB 120 <40 100 Below H8 Subendo- 3:2 W; 100 53 45 Above H
cardial advanced AVB;CHB
*During 2:1 A-V block.Abbreviations: W = Wenckebach conduction; H = bundle of His.
(66/min) (fig. 3B). H-Q interval was 34msec.
Patient 3 was studied while in normal sinusrhythm with first degree A-V block (fig. 4A).The P-R interval was 0.22 sec. P-H was 180msec, and H-Q was 40 msec. P-R prolongationwas duel to prolongation of P-H. With atrialpacing at 100 beats/min, typical Wenckebachperiods occurred (fig. 4B). His bundlepotentials did not follow the blocked Pwaves.
Patient 4 was in fixed 2:1 A-V block duringthe study. Conducted P waves with a P-Hinterval of 100 msec alternated with noncon-ducted P waves. Initially, a His bundle spikewas seen after all P waves (fig. 5A). However,moving the catheter approximately 5 mmdistally eliminateld the His bundle spikeassociated with the blocked P. Instead of thesharp H spike associated with the blocked P, ablunted low voltage complex was seen (fig.5B). The H-Q interval of the conducted beatswas 60 msec, and the QRS was notwidened.The above findings may be explained by
locating the site of block in the His bundleitself. With the recording poles placedproximal to the block, all P waves wereassociated with His bundle spikes. With the
poles at or distal to the block, only theconducted P waves had His bundle spikes.The low voltage complex probably represent-ed a decrementally blocked impulse in the Hisbundle. In the absence of bundle-branchblock pattern in the conducted beats, onemust postulate either block in the commonbundle or simultaneous 2:1 block in bothbundle branches. The latter seems unlikely.
In summary, recording of His bundlepotentials in three patients with DMI and
ECG k R
AR 100VR 50HQ 35
HBE-W p F. RJ55'
Figure 1
Simultaneously recorded ECG and His bundle elec-trogram (HBE) showing 2:1 A-V block above thebundle of His in diaphragmatic infarction in patient 1.P waves and atrial electrograms are labeled P, Hisbundle spikes are labeled H, and QRS and ventricularelectrograms are labeled R. Atrial rate (AR) is 100/min. and ventricular rate (VR) is 50/min. Paper speedis 200 mm/sec., and time lines are at 1 sec. The firstand third P waves are conducted with a P-H intervalof 155 msec while the second P wave is blockedabove the bundle oj His. Same labeling is used inall of the figur-s.
COrculation, Volume XLII, November 1970
ROSEN ET AL.928
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEART BLOCK IN MYOCARDIAL INFARCTION
F?HBEH P
AT RATE 100VT RATE 48
Figure 2Cotitinuous recording showing complete heart block above H in diaphragmatic infarction inpatient 1. Paper speed is 200 mm/sec, and time lines are at 1 sec.
A.
P
ECG
HIHBE pe'
215",
B.
ECG
HBE_ I
AR 1o
~~~~~~~~~PIF
RI
P
II.F,v .~~21e
-,VR 86
Figure 3
;4'
HQ 34
Diaphragmatic infarction with advanced and complete heart block in patient 2. (A) AdvancedA-V block. The first P wave is conducted with a P-H interval of 215 msec. The second Pwave is blocked above H and is followed by a junctional escape with preceding H spike. Thethird P wave is nonconducted and occurs during the escape beat. An alternate and less likelyexplarnation for this arrhythmia would be type I block with the first and second P waves be-ing conducted with increasing P-H intervals and the third P wave being blocked above H.
(B) Complete heart block above H in diaphragmatic infarction. Paper speed 100 mm/sec,and time lines are at 1 sec.
block revealed slowing or block above thebundle of His, most likely in the A-V node.One patient with DMI had block in thecommon bundle. All patients with DMI hadnormal H-Q intervals and supraventricularQRS complexes. Intraventricular conductionwas unaffected.Circulation, Volume XLII, November 1970
Subendocardial Infarction
Studies in patient 8 revealed an atrial rateof 100/min with periods of 3:2 type I block,advanced heart block, and complete heartblock. With both type I (fig. 6) and advancedblock, the blocked P was not followed by aHis bundle potential. During CHB, all
igru s- rF-- i-
I
-j
T
929
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROSEN ET AL.
P~.'.,:
-Q 40HQ 40
p a: i'st~ 1- .P
Figure 4
(A) First degree block in diaphragmatic infarction with prolongation of P-H interval duringnormal sinus rhythm (NSR) in patient 3. (B) Development of type I block with atrial (at.)pacing. The first atrial pacing spike is labeled Pi and subsequent spikes are labeled with ar-rows. The first and second P waves are conducted with P-H of 184 and 335 msec. The thirdP wave is blocked above H. Paper speed is 200 mm/sec; time lines are at 1 sec.
ventricular complexes were supraventricularin contour and were preceded by a His bundlepotential with a normal H-Q interval (45msec).
In this patient with subendocardial infarc-tion, type I block, advanced heart block, andCHB all occurred above the bundle of His.Intraventricular conduction was normal.Anterior Myocardial Infarction
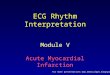
Patients 5, 6, and 7 were studied duringCHB. Atrial rates varied between 80 and 120.All atrial complexes were followed by Hisbundle spikes (figs. 7 and 8) with P-Hintervals of 104, 140, and 100 msec,respectively.A slow, unrelated, idioventricular rhythm
was present characterized by a wide QRSwithout preceding His bundle potential.Asystolic episodes occurred in patients 6 and7, necessitating control by ventricular pacing(fig. 8).In summary, the three patients with AMI
and CHB had block below the bundle of His,probably in the bundle branches. A-Vconduction appeared unaffected, with P-Hintervals remaining normal.
DiscussionA knowledge of the blood supply of the
cardiac conduction system is helpful inunderstanding the site of heart block inmyocardial infarction. In about 90% ofpatients, the A-V node and His bundle aresupplied by a branch of the right coronaryartery given off at the crux of the heart.0"11The ventricular septum and the bundlebranches are predominantly supplied bypenetrating branches from the left anteriordescending coronary artery.'0' 11
Pathologic studies in DMI with heart blockhave usually shown occlusion of the rightcoronary artery proximal to the take-off of theA-V node artery without major structuraldamage to the conduction system.4' 5 11 Thus,heart block has been felt to represent ischemiato the A-V node or His bundle, or both.4'5 InAMI, the pathologic lesion has usually beenmassive septal infarction with necrosisinvolving both bundle branches.4 5The results of this study are consistent with
the pathologic findings. Three of the fourpatients with DMI and the one patient withsubendocardial infarction had either prolonga-tion of P-H interval or block proximal to thebundle of His. Escape rhythms, when present,were characterized by a narrow QRSpreceded by a His bundle spike with normalH-Q interval, indicating normal conduction in
Circulation, Volume XLII, November 1970
-I.-
930
B. AT. PACE /minFr-A --)\- Z-1-d.,. -K -,
fll
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEART BLOCK IN MYOCARDIAL INFARCTION9
DMI.1C... 2:1 BLOCK
HR-96 PH-100 HQ-60Figure 5
(A and B) 2:1 block in diaphragmatic infarction (patient 4). The first and third P waves areconducted, and the second P wave is blocked in the bundle of His. (See text for discussion.)Paper speed is 200 mm/sec, and time lines are at 40 msec.
AR 1XoE C 3 HQ 45 p j
Figure 6
Subendocardial infarction with type I block in patient 8. Typical 3:2 Wenckebach period withP-H of 220, 310, and then block above H. Paper speed is 100 mm/sec, and times lines areat 1 sec.
the distal bundle of His and the bundlebranches. Thus, the usual site of block in DMIwould appear to be in the A-V node, althoughblock high in the His bundle cannot beexcluded by the technic of His bundlerecording. This site would explain thefrequency of Wenckebach periods as well asthe occurrence of pharmacologic reversibilityof block in DMI1, 2, 12, 13 since these areCirculation, Volume XLII, November 1970
characteristic of conduction delay at the A-Vnode.2 9 '4 The patient with subendocardialinfarction appeared to have a similar lesion.
In one patient with DMI and 2:1 block withnarrow QRS, a His bundle spike was initiallyseen following the blocked P wave. However,when the catheter was positioned a fewmillimeters distally into the right ventricle,only a low voltage deflection could be seen
931
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROSEN ET AL.
ECG
mBE , R
ECG
PH RH
ECG-
AR109 VR 36 PH 104
Figure 7
Continuous recordings from patient 5 showing com-plete heart block below the bundle of His in a pa-tient with anterior infarction. Note H spikes folowingevery P wave with normal P-H interval. Paper speedis 200 mm/sec. and time lines are at 1 sec.
after the blocked Ps where the sharp H spikeswere previously noted, and the H spikes of theconducted Ps remained well-recorded. Thislow voltage spike probably represented adecrementally blocked potential low in theHis bundle. Narula and co-workers'5 havedescribed a patient without infarction, whohad chronic block in the His bundlecharacterized by block distal to the bundle ofHis recording site with narrow QRS. The
HBE
ECG F Fi__
recordings obtained in our patient are similarto those obtained by Narula and associates,with the addition of the decremental spike.The findings in AMI with heart block were
also consistent with previously reportedpathologic findings. P-H intervals were notprolonged, suggesting normal function of theA-V node. Block occurred below the bundle ofHis recording site, and escape rhythms wereidioventricular, characterized by wide QRScomplexes without preceding His bundlespikes. Two of the three patients with AMIhad evidence of bilateral bundle-branchdisease prior to the developme.nt of CHB,both having right bundle-branch block, onewith left anterior, and the other with leftposterior hemiblock.16-18 These ECG findings,together with the results of the His bundlerecordings, suggest complete bilateral bundle-branch block as the site of block in AMI. Thissite would explain the occurrence of type IIblock in AMI, a type of block often signifyingdisease in the His-Purkinje system.2 14 Stokes-Adams attacks occur frequently in AMIwith CHB, reflecting the slow heart rate andunreliability of the idioventricular pace-maker.1 2, 12
In summary, DMIblock proximal to thewas characterized bybundle. Difference
was characterized byHis bundle while AMIblock distal to the Hisin clinical behavior
IAR 120 V Pace 90
Figure 8Complete block below H in anterior infarction during ventricular pacing. Pacing spikes arelabeled Pi and are followed by paced ventricular beats (R). All P waves have associated Hspikes with P-H interval of 140 msec. None of these are conducted with block occurring be-low H. Time lines are at 40 msec, and paper speed is 200 mm/sec.
Circulation, Volume XLII, November 1970
dko:I
l/
932
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEART BLOCK IN MYOCARDIAL INFARCTION
between these two conditions can be partiallyexplained by differing sites! of block.
AcknowledgmentWe would like to thank Miss B. Lake for her
secretarial help and Mrs. D. Gore for thephotographic work.
References1. McNALLY EM, BENCHIMOL A: Medical and
physiological considerations in the use ofartificial cardiac pacing: Part 1. Amer Heart J75: 380, 1968
2. LANGENDORF R, PICK A: Atrioventricular block,Type II (Mobitz): Its nature and clinicalsignificance. Circulation 38: 819, 1968
3. CHAMBERLAIN D, LEINBACH R: Electricalpacing in heart block complicating acutemyocardial infarction. Brit Heart J 32: 2,1970
4. BLONDEAU M, RizzoN M, LENEGRE J: Les troublesde la conduction auriculo-ventriculaire dansl'infarctus myocardique recent: II. Etudeanatomique. Arch Mal Coeur 54: 1104,1961
5. SUTTON R, DAVES M: The conduction system inacute myocardial infarction complicated byheart block. Circulation 38: 987, 1968
6. SCHERLAG BJ, LAU SH, HELFANT RH, ET AL:Catheter technique for recording His bundleactivity in man. Circulation 39: 13, 1969
7. RosEN KM, LAU SH, WEiss MB, ET AL: Theeffect of lidocaine on atrioventricular andintraventricular conduction in man. Amer JCardiol 25: 1, 1970
8. ROSEN KM, RAHIMTOOLA SH: Unpublisheddata
9. DAMATO AN, LAU SH, HELFANT RH, ET AL: Astudy of heart block in man using His bundlerecordings. Circulation 39: 297, 1969
10. JAMES TN, BURCH GE: Blood supply of thehuman interventricular septum. Circulation17: 391, 1958
11. JAMES TN: Anatomy of the coronary arteries inhealth and disease. Circulation 32: 1020,1965
12. NoRms RM: Heart block in posterior andanterior myocardial infarction. Brit Heart J31: 352, 1968
13. COURTER SR, MOFFAT J, FOWLER NO: Advancedatrioventricular block in acute myocardialinfarction. Circulation 27: 1034, 1963
14. WATANABE Y, DREniFus LS: Second degreeatrioventricular block. Cardiovasc Res 1: 150,1967
15. NARULA OS, SCHERLAG BJ, JAVIER RP, ET AL:
Analysis of the A-V conduction defect incomplete heart block utilizing His bundleelectrograms. Circulation 41: 437, 1970
16. ROSENBAUM MB, ELIZARI MV, LAzZARI JO, ETAL: Intraventricular trifasicular blocks: Reviewof the literature and classification. Amer HeartJ 78: 450, 1969
17. CASTELLANOS A, MAYTIN 0, ARCEBAL AG, ET
AL: Altemating and co-existing block in thedivisions of the left bundle branch. Dis Chest56: 103, 1969
18. GODMAN MJ, LASSERs BW, JULIAN DG:Complete bundle-branch block complicatingacute myocardial infarction. New Eng J Med282: 237, 1970
Circulation, Volume XLII, November 1970
933
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

SINNO, SHAHBUDIN H. RAHIMTOOLA and ROLF M. GUNNARKENNETH M. ROSEN, HENRY S. LOEB, RUBEN CHUQUIMIA, M. ZIAD
Site of Heart Block in Acute Myocardial Infarction
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1970 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.42.5.925
1970;42:925-933Circulation.
http://circ.ahajournals.org/content/42/5/925located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from




















](https://img.pdfslide.net/doc/110x75/5556ced7d8b42abb428b5615/acute-myocardial-infarction-final2.jpg)