Embed Size (px)
Citation preview
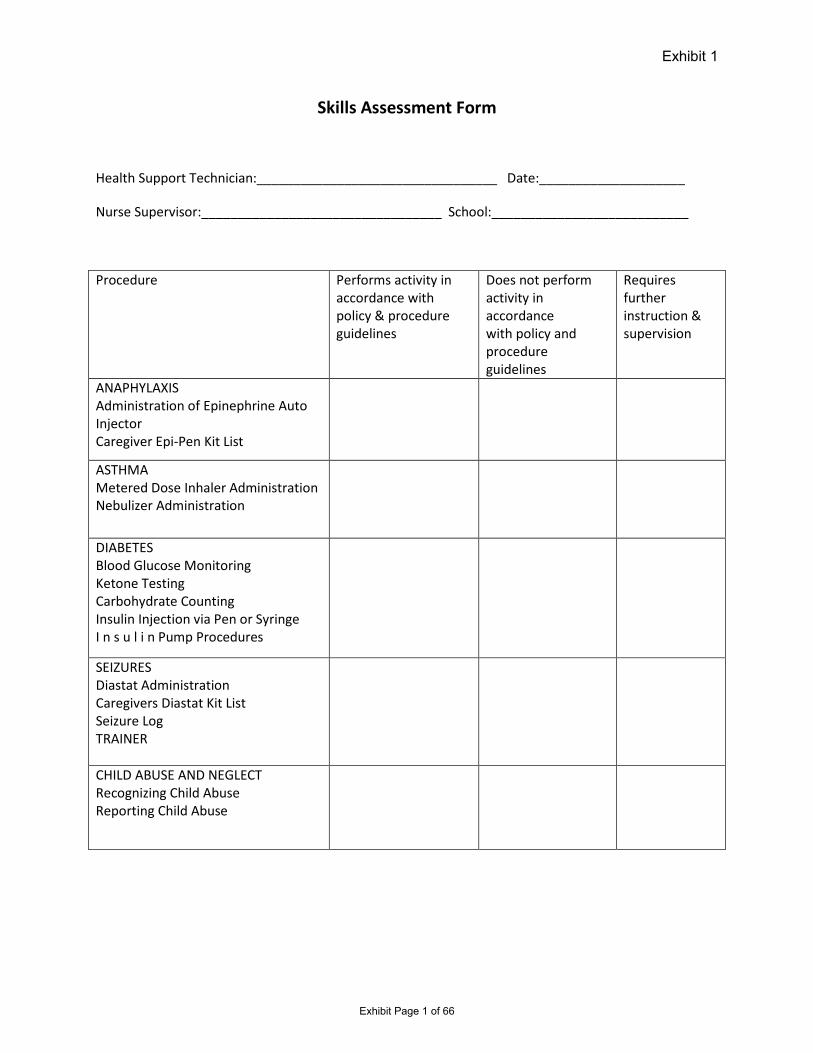
Exhibit 1
Skills Assessment Form
Health Support Technician:_________________________________ Date:____________________
Nurse Supervisor:_________________________________ School:___________________________
Procedure Performs activity in accordance with policy & procedure guidelines
Does not perform activity in accordance with policy and procedure guidelines
Requires further instruction & supervision
ANAPHYLAXIS Administration of Epinephrine Auto Injector Caregiver Epi-Pen Kit List
ASTHMA Metered Dose Inhaler Administration Nebulizer Administration
DIABETES Blood Glucose Monitoring Ketone Testing Carbohydrate Counting Insulin Injection via Pen or Syringe I n s u l i n Pump Procedures
SEIZURES Diastat Administration Caregivers Diastat Kit List Seizure Log TRAINER
CHILD ABUSE AND NEGLECT Recognizing Child Abuse Reporting Child Abuse
Exhibit Page 1 of 66
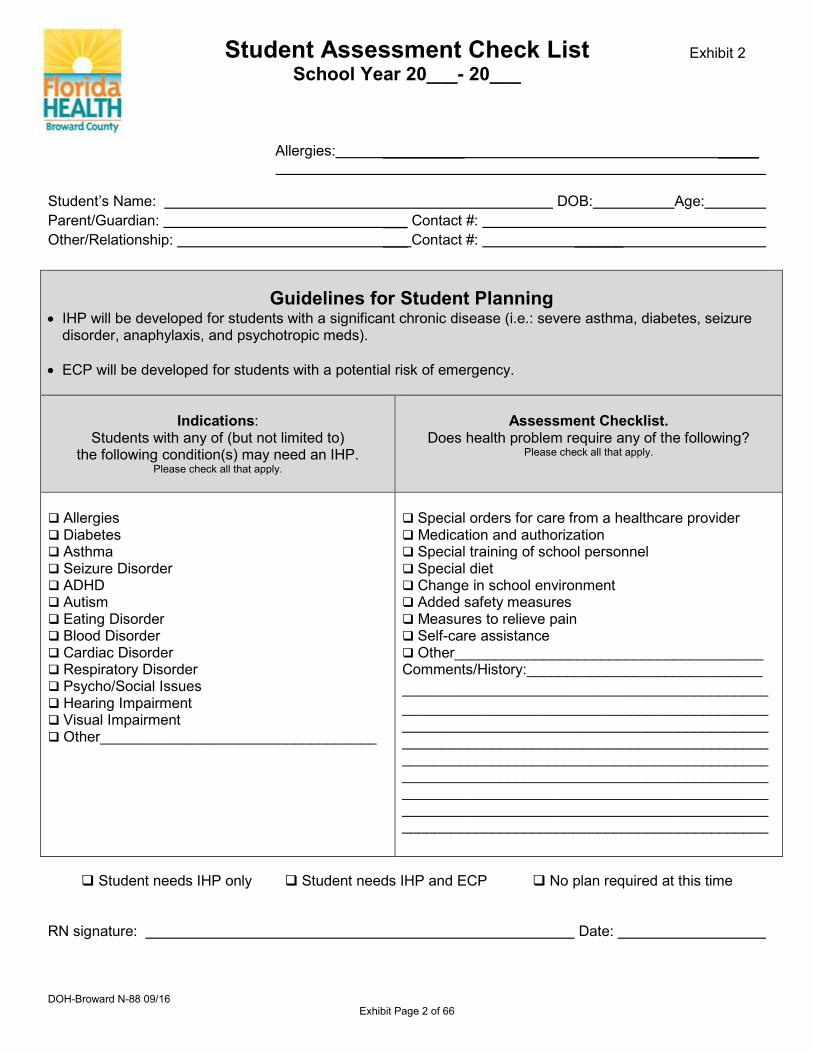
Student Assessment Check List School Year 20___- 20___
Allergies: __________ _____
Student’s Name: DOB: Age: Parent/Guardian: ___ Contact #: Other/Relationship: ___ Contact #: ______
Guidelines for Student Planning • IHP will be developed for students with a significant chronic disease (i.e.: severe asthma, diabetes, seizure
disorder, anaphylaxis, and psychotropic meds).
• ECP will be developed for students with a potential risk of emergency.
Indications: Students with any of (but not limited to)
the following condition(s) may need an IHP. Please check all that apply.
Assessment Checklist. Does health problem require any of the following?
Please check all that apply.
Allergies Diabetes Asthma Seizure Disorder ADHD Autism Eating Disorder Blood Disorder Cardiac Disorder Respiratory Disorder Psycho/Social Issues Hearing Impairment Visual Impairment Other__________________________________
Special orders for care from a healthcare provider Medication and authorization Special training of school personnel Special diet Change in school environment Added safety measures Measures to relieve pain Self-care assistance Other______________________________________Comments/History:_____________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________
Student needs IHP only Student needs IHP and ECP No plan required at this time
RN signature: Date:
Exhibit 2
DOH-Broward N-88 09/16 Exhibit Page 2 of 66
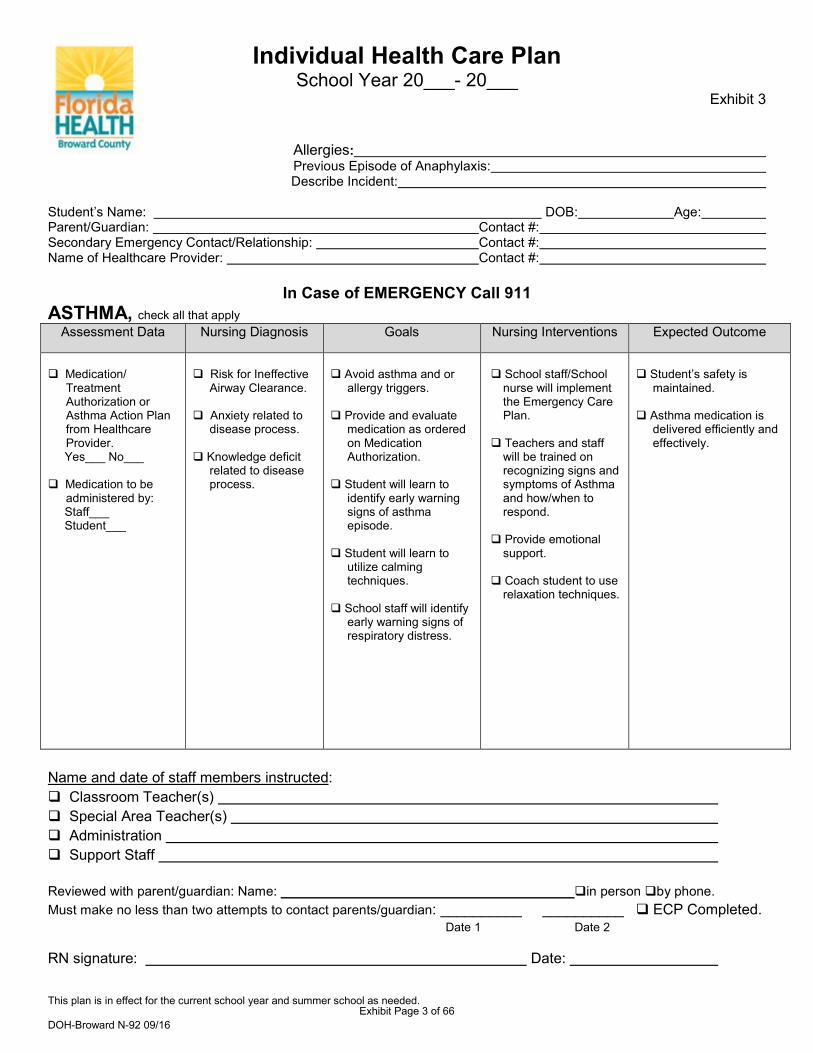
Individual Health Care Plan School Year 20___- 20___
Exhibit 3
Allergies: Previous Episode of Anaphylaxis:
Describe Incident:
Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #:
In Case of EMERGENCY Call 911 ASTHMA, check all that apply
Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome
Medication/TreatmentAuthorization orAsthma Action Planfrom HealthcareProvider.Yes___ No___
Medication to beadministered by:Staff___Student___
Risk for IneffectiveAirway Clearance.
Anxiety related todisease process.
Knowledge deficitrelated to diseaseprocess.
Avoid asthma and orallergy triggers.
Provide and evaluatemedication as orderedon MedicationAuthorization.
Student will learn toidentify early warningsigns of asthmaepisode.
Student will learn toutilize calmingtechniques.
School staff will identifyearly warning signs ofrespiratory distress.
School staff/Schoolnurse will implementthe Emergency CarePlan.
Teachers and staffwill be trained onrecognizing signs andsymptoms of Asthmaand how/when torespond.
Provide emotionalsupport.
Coach student to userelaxation techniques.
Student’s safety ismaintained.
Asthma medication isdelivered efficiently andeffectively.
Name and date of staff members instructed: Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff
Reviewed with parent/guardian: Name: in person by phone.Must make no less than two attempts to contact parents/guardian: __________ __________ ECP Completed.
Date 1 Date 2
RN signature: Date:
This plan is in effect for the current school year and summer school as needed.
DOH-Broward N-92 09/16 Exhibit Page 3 of 66
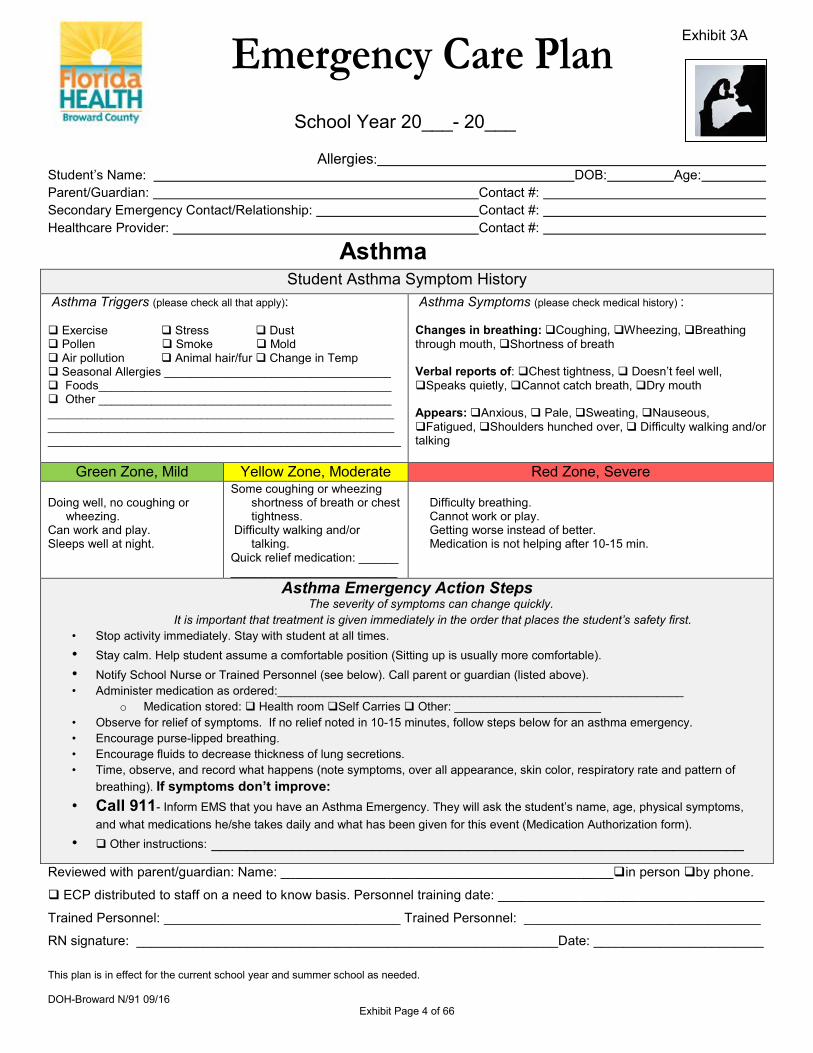
School Year 20___- 20___ Allergies: Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #:
Asthma
Student Asthma Symptom History Asthma Triggers (please check all that apply): Exercise Stress Dust Pollen Smoke Mold Air pollution Animal hair/fur Change in Temp Seasonal Allergies __________________________________ Foods____________________________________________ Other ____________________________________________ ____________________________________________________ ____________________________________________________ _____________________________________________________
Asthma Symptoms (please check medical history) : Changes in breathing: Coughing, Wheezing, Breathing through mouth, Shortness of breath Verbal reports of: Chest tightness, Doesn’t feel well, Speaks quietly, Cannot catch breath, Dry mouth Appears: Anxious, Pale, Sweating, Nauseous, Fatigued, Shoulders hunched over, Difficulty walking and/or talking
Green Zone, Mild Yellow Zone, Moderate Red Zone, Severe Doing well, no coughing or
wheezing. Can work and play. Sleeps well at night.
Some coughing or wheezing shortness of breath or chest tightness.
Difficulty walking and/or talking.
Quick relief medication: ______ _________________________
Difficulty breathing. Cannot work or play. Getting worse instead of better. Medication is not helping after 10-15 min.
Asthma Emergency Action Steps The severity of symptoms can change quickly.
It is important that treatment is given immediately in the order that places the student’s safety first. • Stop activity immediately. Stay with student at all times. • Stay calm. Help student assume a comfortable position (Sitting up is usually more comfortable). • Notify School Nurse or Trained Personnel (see below). Call parent or guardian (listed above). • Administer medication as ordered:_____________________________________________________________
o Medication stored: Health room Self Carries Other: ______________________ • Observe for relief of symptoms. If no relief noted in 10-15 minutes, follow steps below for an asthma emergency. • Encourage purse-lipped breathing. • Encourage fluids to decrease thickness of lung secretions. • Time, observe, and record what happens (note symptoms, over all appearance, skin color, respiratory rate and pattern of
breathing). If symptoms don’t improve: • Call 911- Inform EMS that you have an Asthma Emergency. They will ask the student’s name, age, physical symptoms,
and what medications he/she takes daily and what has been given for this event (Medication Authorization form). • Other instructions: ____________________________________________________________
Reviewed with parent/guardian: Name: _____________________________________________in person by phone.
ECP distributed to staff on a need to know basis. Personnel training date: ____________________________________
Trained Personnel: ________________________________ Trained Personnel: ________________________________
RN signature: _________________________________________________________Date: _______________________
Exhibit 3A
This plan is in effect for the current school year and summer school as needed. DOH-Broward N/91 09/16
Exhibit Page 4 of 66
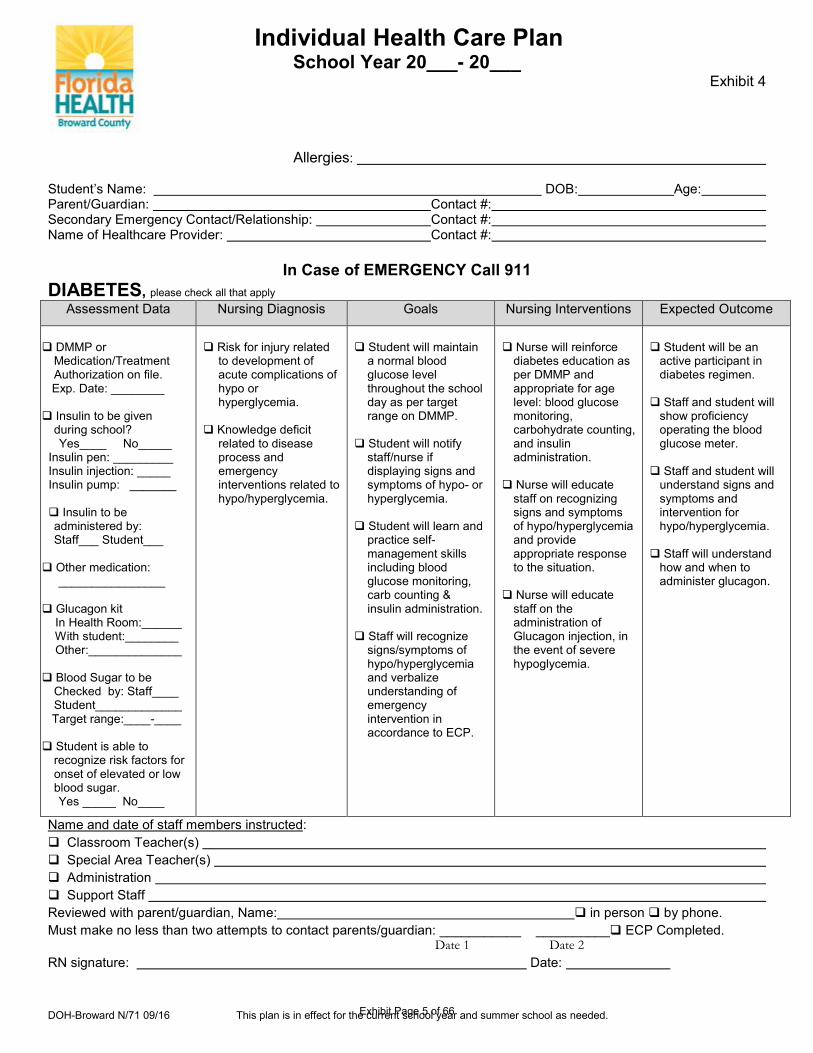
Individual Health Care Plan School Year 20___- 20___
Exhibit 4
Allergies:
Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #:
In Case of EMERGENCY Call 911
DIABETES, please check all that apply Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome
DMMP or
Medication/Treatment Authorization on file.
Exp. Date: ________ Insulin to be given
during school? Yes____ No_____
Insulin pen: _________ Insulin injection: _____ Insulin pump: _______ Insulin to be
administered by: Staff___ Student___
Other medication: ________________ Glucagon kit In Health Room:______ With student:________ Other:______________ Blood Sugar to be
Checked by: Staff____ Student_____________
Target range:____-____ Student is able to
recognize risk factors for onset of elevated or low blood sugar.
Yes _____ No____
Risk for injury related
to development of acute complications of hypo or hyperglycemia.
Knowledge deficit
related to disease process and emergency interventions related to hypo/hyperglycemia.
Student will maintain
a normal blood glucose level throughout the school day as per target range on DMMP.
Student will notify
staff/nurse if displaying signs and symptoms of hypo- or hyperglycemia.
Student will learn and
practice self-management skills including blood glucose monitoring, carb counting & insulin administration.
Staff will recognize
signs/symptoms of hypo/hyperglycemia and verbalize understanding of emergency intervention in accordance to ECP.
Nurse will reinforce
diabetes education as per DMMP and appropriate for age level: blood glucose monitoring, carbohydrate counting, and insulin administration.
Nurse will educate
staff on recognizing signs and symptoms of hypo/hyperglycemia and provide appropriate response to the situation.
Nurse will educate
staff on the administration of Glucagon injection, in the event of severe hypoglycemia.
Student will be an
active participant in diabetes regimen.
Staff and student will
show proficiency operating the blood glucose meter.
Staff and student will
understand signs and symptoms and intervention for hypo/hyperglycemia.
Staff will understand
how and when to administer glucagon.
Name and date of staff members instructed: Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff Reviewed with parent/guardian, Name: in person by phone. Must make no less than two attempts to contact parents/guardian: ___________ __________ ECP Completed. Date 1 Date 2 RN signature: Date:
DOH-Broward N/71 09/16 This plan is in effect for the current school year and summer school as needed.
Exhibit Page 5 of 66
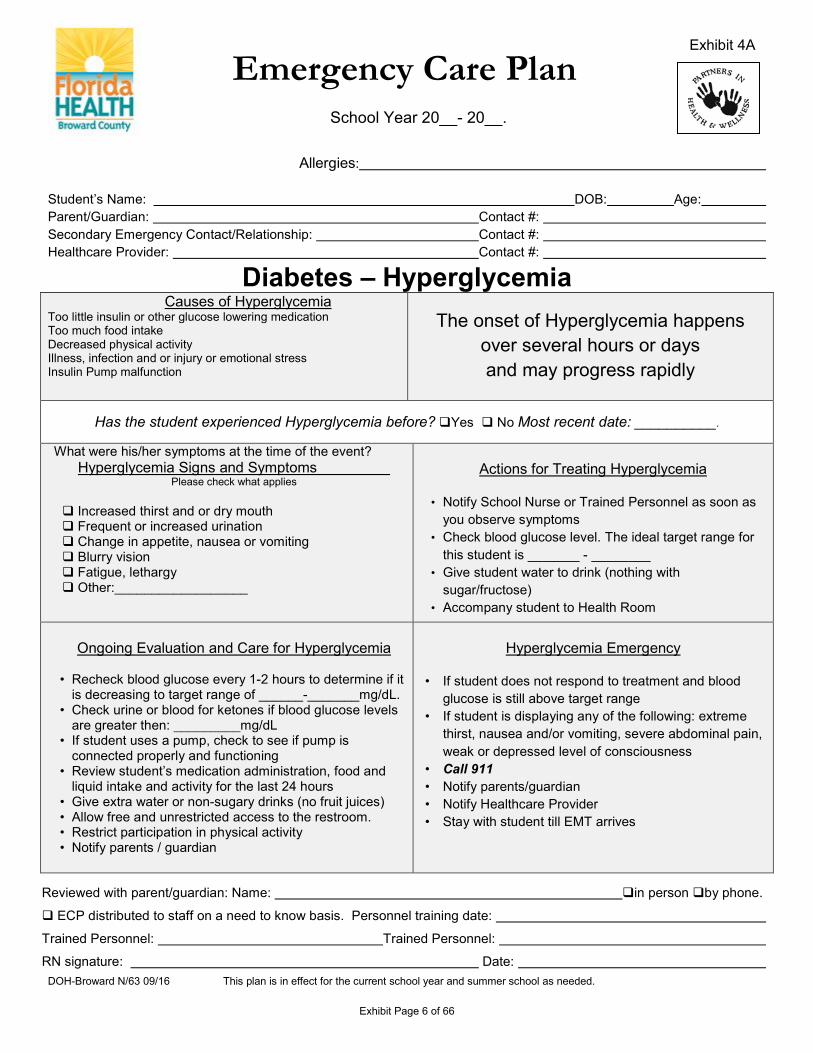
Emergency Care Plan
School Year 20__- 20__.
Allergies:
Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #:
Diabetes – Hyperglycemia Causes of Hyperglycemia
Too little insulin or other glucose lowering medication Too much food intake Decreased physical activity Illness, infection and or injury or emotional stress Insulin Pump malfunction
The onset of Hyperglycemia happens
over several hours or days and may progress rapidly
Has the student experienced Hyperglycemia before? Yes No Most recent date: __________.
What were his/her symptoms at the time of the event? Hyperglycemia Signs and Symptoms
Please check what applies Increased thirst and or dry mouth Frequent or increased urination Change in appetite, nausea or vomiting Blurry vision Fatigue, lethargy Other:__________________
Actions for Treating Hyperglycemia
• Notify School Nurse or Trained Personnel as soon as
you observe symptoms • Check blood glucose level. The ideal target range for
this student is _______ - ________ • Give student water to drink (nothing with
sugar/fructose) • Accompany student to Health Room
Ongoing Evaluation and Care for Hyperglycemia
• Recheck blood glucose every 1-2 hours to determine if it
is decreasing to target range of ______-_______mg/dL. • Check urine or blood for ketones if blood glucose levels
are greater then: _________mg/dL • If student uses a pump, check to see if pump is
connected properly and functioning • Review student’s medication administration, food and
liquid intake and activity for the last 24 hours • Give extra water or non-sugary drinks (no fruit juices) • Allow free and unrestricted access to the restroom. • Restrict participation in physical activity • Notify parents / guardian
Hyperglycemia Emergency
• If student does not respond to treatment and blood
glucose is still above target range • If student is displaying any of the following: extreme
thirst, nausea and/or vomiting, severe abdominal pain, weak or depressed level of consciousness
• Call 911 • Notify parents/guardian • Notify Healthcare Provider • Stay with student till EMT arrives
Reviewed with parent/guardian: Name: in person by phone.
ECP distributed to staff on a need to know basis. Personnel training date:
Trained Personnel: Trained Personnel:
RN signature: Date:
Exhibit 4A
DOH-Broward N/63 09/16 This plan is in effect for the current school year and summer school as needed.
Exhibit Page 6 of 66
Emergency Care Plan
School Year 20__- 20__.
Allergies: Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #:
Diabetes – Hypoglycemia
Causes of Hypoglycemia
• Too much insulin • Missing or delaying meals or snacks • Not eating enough foods (carbohydrates) • Getting intense or unplanned physical activity • Being ill, particularly with gastrointestinal illness
• Does the student have Glucagon ordered by
Healthcare Provider? Yes No, if yes, location of Glucagon: ________________________________
Trained personnel to administer Glucagon as ordered and Call 911
• CALL 911 • Special Instructions:
____________________________________ ________________________________________
Has the student experienced Hypoglycemia before? Yes No, most recent date:__________ What were his or her symptoms at the time? Please check below.
Hypoglycemia Signs and Symptoms
Shaky or jittery Pale or sweaty Thirsty and/or hungry Headache, blurry vision Dizzy, confused, or disoriented Change in behavior, irritable, nervous or combative Weak, sleepy or lethargic Other:__________________________________
Actions for Treating Hypoglycemia
• School Nurse or Trained Personnel should come to the classroom to assist student. Always stay with student.
• Check blood glucose level. Ideal blood glucose level for this student is _______-_______
• Give student a quick acting glucose product such as: ___________________________________________
• Contact the student’s parents/guardian • Other instructions: ___________________________ • ____________________________________________
Ongoing Evaluation and Care for Hypoglycemia
• Recheck blood glucose levels every 10-15 minutes • Repeat quick acting glucose product or fruit juice or soda
Treatment for Severe Hypoglycemia
• Position the student on his or her side • Do not attempt to give anything by mouth • If student is unable to eat or drink, unresponsive or
having convulsions: Administer Glucagon injection as ordered by the Healthcare Provider
• While treating, have another person CALL 911 • Notify parents / guardian of current situation • Call student’s Healthcare Provider • Stay with student until EMT arrives
The onset of Hypoglycemia happens quickly and may progress rapidly.
Reviewed with parent/guardian: Name: in person by phone.
ECP Distributed to staff on a need to know basis. Personnel training date: ______________________________
Trained Personnel: _________________________________ Trained Personnel:
RN signature: Date:
Exhibit 4B
DOH-Broward N/64 09/16 This plan is in effect for the current school year and summer school as needed. Exhibit Page 7 of 66
Individual Health Care Plan School Year 20___- 20___
Allergies: Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #:
In Case of EMERGENCY Call 911 SEIZURE DISORDER, Please check all that apply
Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome
Student has history of
seizure disorder. Last episode(date and duration), triggers and description of seizure: ___________________
___________________ ___________________
___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ Medication Orders from
Physician: Yes_____ No______
Based on seizure history: Risk of injury related to seizure activity. Yes No Potential for aspiration related to seizure activity. Yes No Importance of
compliance with meds.
Decreased
self-esteem related to chronic illness.
Train staff to identify
and respond to seizure.
Prevent injury during
seizure. Prevent aspiration
during seizure. Student receives
medication as ordered by Healthcare Provider to reduce risk of seizure activity.
Student will have
increased knowledge base of disease process regarding prevention of seizure with medication compliance and recognizing the onset of a seizure to prevent injury.
Train staff to protect,
support and prevent injury.
Position child on
his/her side to prevent aspiration. Call for help.
Maintain compliance
with medications as ordered by Healthcare Provider.
Increased self esteem
by providing education and support for student to talk about issues related to illness.
Student will not
experience seizure. Staff will be well
trained to provide care and support to the student.
Staff will identify
seizure and follow ECP and call for help.
If a seizure occurs
the student will not experience injury or aspirate during the seizure.
Name and date of staff members instructed:
Classroom Teacher(s)
Special Area Teacher(s)
Administration
Support Staff
Reviewed with parent/guardian: Name: in person by phone.
Must make no less than two attempts to contact parents/guardian: _________ __________ ECP Completed.
Date 1 Date 2
RN signature: Date:
Exhibit 5
DOH-Broward N/66 08/16 This plan is in effect for the current school year and summer school as needed Exhibit Page 8 of 66
Emergency Care Plan
School Year 20__- 20__.
Allergies: Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #:
Seizure Disorder
Basic Seizure First Aid
If you see this:
Symptoms of a seizure episode may include any or all of these. • Temporary confusion, staring spell • Convulsion lasting longer than ____ minutes • Uncontrollable jerking movements of the arms and legs • Loss of consciousness or awareness • Pale, clammy, nail beds pale/bluish gray in color • Rapid heart rate or changes in breathing patterns • Other symptoms:
____________________________________________________________________________________________________________________
__________________________________________________________
Do this:
• Stay calm. Remove bystanders • Keep airway clear, turn on side
if possible, nothing in mouth • Keep safe, remove objects, do
not restrain • Time, observe, record what
happens • Stay with student until
recovered from seizure
Seizure Emergency Action Steps
• Call 911 Inform EMS that you have a Seizure Emergency. They will ask the student’s name, age, physical symptoms and what medication he/she takes daily and what medication has been administered for this event.
• Notify School Nurse or Trained Personnel (see below). • Administer medication as ordered.
Location of medication: Clinic, Classroom, Self carries • Medication:_____________________ • Dose:___________________________ • Route:___________________________ • Time Administered: ________________ • Call parent or guardian (listed above)
Other instructions:_________________________________________________________________ _________________________________________________________________________________ _________________________________________________________________________________
Reviewed with parent/guardian: in person by phone. Name:
ECP Distributed to staff on a need to know basis. Personnel training date: _________________________
Trained Personnel: __________________________ Trained Personnel: ______________________________
RN signature: Date:
Exhibit 5A
DOH-Broward N/67 09/16 This plan is in effect for the current school year and summer school as needed Exhibit Page 9 of 66
Individual Health Care Plan School Year 20___- 20___
Exhibit 6
Allergies: Previous episode of Anaphylaxis: Describe Incident: Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Name of Healthcare Provider: Contact #:
In Case of EMERGENCY Call 911
Anaphylaxis / Allergy, Please check all that apply Assessment Data Nursing Diagnosis Goals Nursing Interventions Expected Outcome
Student has Medication/ Treatment Authorization. Yes_____ No______ Events which may trigger an allergic response: ______________________ ______________________ ______________________ Symptoms of student’s allergic response (check those that apply): Itching or swelling of the
mouth, lips, tongue, face, or extremities.
Cough, tightness in throat, difficulty swallowing, wheezing, shortness of breath, difficulty breathing.
Increased heart rate, weak pulse, dizziness, feeling faint.
Skin redness, itchy hives/rash, pain at site of exposure.
Nausea, vomiting, abdominal cramps, diarrhea.
Student is able to recognize risk factors for onset of anaphylaxis. Yes _____ No_____
Potential for severe
allergic reaction or life threatening episode.
Knowledge Deficit
related to disease process.
Student will maintain
optimum health and safety necessary for learning.
Student and staff will
understand the disease process of allergies/anaphylaxis and emergency interventions.
Staff will be educated
on the signs and symptoms of the early stages of anaphylaxis.
Staff will be educated
on emergency procedures for anaphylaxis.
Student will have an
Emergency Care Plan in place for severe allergy/anaphylaxis.
Staff will be educated
on use of Epinephrine.
Staff will be educated
on allergens and substances that can cause anaphylaxis and ways to avoid allergens.
All substances
causing anaphylaxis will be avoided and student will have an incident free learning experience.
Staff will understand
the emergency procedures and demonstrate competency regarding use of the Epinephrine.
Student will
participate in collaboration which facilitates optimum health and safety necessary for learning.
Staff will understand
the early stages of anaphylaxis and follow protocol to treat.
Name and date of staff members instructed:
Classroom Teacher(s) Special Area Teacher(s) Administration Support Staff Reviewed with parent/guardian: Name: in person by phone. Must make no less than two attempts to contact parents/guardian: ECP Completed Date 1 Date 2 RN signature: Date:
This plan is in effect for the current school year and summer school as needed. DOH-Broward N/62 09/16
Exhibit Page 10 of 66
School Year 20___- 20___
Allergies/triggers: nuts soy products wheat shellfish insects other: Date of previous episode of anaphylaxis: Describe Incident:
Student’s Name: DOB: Age: Parent/Guardian: Contact #: Secondary Emergency Contact/Relationship: Contact #: Healthcare Provider: Contact #:
Anaphylaxis
Does the student have Asthma? Yes (increased risk for severe reaction) No
Symptoms of an allergic reaction may include any/all of the following:
If you see this: (Circle those that apply)
Act Quickly! Follow the Medication / Treatment Authorization:
(Check all that apply)
• Itching or swelling of lips, tongue or mouth.
• Hoarse, coughing, tightness in throat, difficulty
swallowing, wheezing, shortness or difficulty breathing,
increased heart rate, weak pulse.
• Redness, itchy hives, itchy rash, swelling of face and
extremities.
• Nausea, vomiting, abdominal cramps, diarrhea.
• Dizziness, feeling faint, pain at site.
Comment: ___________________________________ ____________________________________________ ____________________________________________ ____________________________________________ ____________________________________________ ____________________________________________ ____________________________________________
Treatment should be initiated with symptoms Antihistamine ordered Epinephrine Auto Injector, follow instruction on devise Other:______________________________________ Medication in clinic Student self carries Other instructions:____________________________
• Call 911 after using Epinephrine Auto-Injector. • Call School Nurse or Trained Personnel. • Call parent/guardian (listed above). • Stay with student at all times. Stay calm. • Monitor student’s reaction, respiratory and heart rate • Special Instructions:_____________________________ _____________________________________________
Call 911- The severity of symptoms can change quickly It is important that treatment is given immediately in the order that places the student’s safety first.
Reviewed with parent/guardian: Name: in person by phone.
ECP distributed to staff on a need to know basis. Personnel training date: ___________________________
Trained Personnel: ______________________________ Trained Personnel: ___________________________________
RN signature: Date:
Exhibit 6A
DOH-Broward N/55 09/16 This plan is in effect for the current school year and summer school as needed. Exhibit Page 11 of 66
THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDACoordinated Student Health Services, 1400 NW 14 Court, Fort Lauderdale, FL 33311
AUTHORIZATION FOR MEDICATION: Prescription or Over-the-Counter Medication Student's Name: Date of Birth: Grade: School: _______________________________Phone #: Fax#: _______________ *********************************************************************************************************************************** Allergies: ___________________________________________________________________________ Diagnosis: ___________________________________________________________________________
MEDICATION DOSAGE & ROUTE
FREQUENCY SPECIFIC TIMES
SPECIAL INSTRUCTIONS/ SIDE EFFECTS
List any emergency precautions / health emergencies that should be anticipated for this student; e.g. allergy triggers, diabetic reactions, etc.) : _______________________________________________________________________________ _______________________________________________________________________________________There are no extraordinary emergency medical services available at school. Since only CPR and first aid are available until 911 arrive, is this adequate for student survival? YES NO, IF "NO", specifies: _______________________________________________________________________________________ *********************************************************************************************************************************** _________________________________________ _______________________________________ Physician’s Name (Printed) Physician’s Signature _________________________________________ _______________________________________
Physician’s Telephone & Fax Numbers _________________________________________ _______________________________________ Physician’s Office Address Date Completed *********************************************************************************************************************************** This information will be obtained by School Board District Personnel
PARENTAL PERMISSION FOR MEDICATION (TO BE COMPLETED BY THE STUDENT’S PARENT / GUARDIAN)
Student's Name: _______________________Date of Birth: ______________Grade:
I grant the principal or his / her designee the permission to assist or perform the administration of each medication to or for my child during the school day, including when he/she is away from school property for official school events. If my child has been authorized by his/her physician to self-administer their medication(s), I grant permission for my child to self-administer their medication at school and when they are away from school property for official school events. In the event that my child is unable to self-administer their medication, I give permission for the principal/designee to perform the administration of the prescribed medication.
NOTE: • Medications must be supplied in the original container. Ask the pharmacist to divide the medication into two completely
labeled containers, providing one for home and one for school. • School personnel may administer only medications authorized by a physician.• It is your responsibility to notify the school when there is a change in medication regimen.
___________________________________ _____________________________________________ Parent / Guardian Name (Printed) Signature of Parent / Guardian
___________________________________ _____________________________________________ Date Signed Home Phone Number
___________________________________________________________ Work/Cell Phone Number (Include Ext. if any)
Form #2240 Rev. 8/15
Exhibit 7
Page 1 of 2Exhibit Page 12 of 66
THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDACoordinated Student Health Services, 1400 NW 14 Court, Fort Lauderdale, FL 33311
AUTHORIZATION FOR TREATMENT Student's Name: Date of Birth: Grade: School: Phone #: Fax#: *********************************************************************************************************************************** Diagnosis: ________________________________________________ Allergies: _______________________________ TREATMENTS DURING SCHOOL HOURS Treatment Plan: _______________________________________________________________________________________
PROCEDURE TYPE MEDS / FEEDING
AMOUNT FREQUENCY
SPECIFIC TIMES RATE / FLOW
Catheterization Feedings G-Tube J-Tube
NG-Tube Special ________ Suctioning Oropharynx
Tracheostomy Deep Surface
Tracheostomy Tube Replacement Care (Cleaning)
CPT Oxygen /Misting Ventilator Nebulizer Tx Pulse Oximeter
Are any of the above procedures required for emergency care? YES NO, IF "YES", specify: _______________________________________________________________________________________List any procedures the student has been trained to perform __________________________________________ List any limitations / precautionary measures that should be considered; e.g. physical education, outdoor activities, transporting, lifting, moving, special devices / equipment: ___________________________________________ _______________________________________________________________________________________ List any emergency precautions / health emergencies that should be anticipated for this student; e.g. allergy triggers, diabetic reactions, etc.) : ____________________________________________________________________ _______________________________________________________________________________________There are no extraordinary emergency medical services available at school. Since only CPR and first aid are available until 911 arrive, is this adequate for student survival? YES NO, IF "NO", specifies: _______________________________________________________________________________________
_________________________________________ _______________________________________ Physician’s Name (Printed) Physician’s Signature
______________________________________________________ ____________________________________________________ Physician’s Telephone & Fax Numbers
_________________________________________ _______________________________________ Physician’s Office Address Date Completed *********************************************************************************************************************************** This information will be obtained by School Board District Personnel
PARENTAL PERMISSION FOR TREATMENT (TO BE COMPLETED BY THE STUDENT’S PARENT / GUARDIAN)
Student's Name: _______________________ Date of Birth: ______________Grade: _______________ I grant the principal or his / her designee the permission to assist or perform the administration of each treatment/procedure to or for my child during the school day, including when he/she is away from school property for official school events. If my child has been authorized by his/her physician to self-administer their medication(s), I grant permission for my child to self-administer their treatment at school and when they are away from school property for official school events. In the event that my child is unable to self-administer their treatment, I give permission for the principal/designee to perform the administration of the prescribed treatment. NOTE: school personnel may administer only treatments authorized by a physician. It is your responsibility to notify the school when there is a change in treatment regimen.
___________________________________ _____________________________________________ Parent / Guardian Name (Printed) Signature of Parent / Guardian _______________________________ __________________________ ____________________________________________ Date Signed Home Phone Number Work/Cell Phone Number (Include Ext. if any)
Exhibit 7
Page 2 of 2
Exhibit Page 13 of 66
STUDENT MEDICATION LOG Allergies
Student's Name: DOB: School: Hm Rm Teacher
Doctor: Phone # Fax #: Diagnosis :
Special Instructions: Side Effects: Month/Year:
MEDICATION
NAME DOSAGE
TIME TO BE GIVEN ROUTE
* Record the amount of Medication received (i.e. # of pills, amount of liquid) with each initial receipt in the“Notes” Section on the Reverse
* Record Time Medication was given (or Reason not given) and Initials in the appropriate boxes* If medication is not given, please use one of the following abbreviations to indicate the reason why:
A-absent O-out of medication F-field trip D-discontinued R-refused DW-dose wasted ER-early release day V-vacation/school closed S-Other and Provide explanation in the “Notes” Section on the Reverse side
Date AM
Initials PM
Initials AM
Initials PM
Initials AM
Initials PM
Initials AM
Initials PM
Initials
Signature/Initials/Date for each week.
Signature/Initials: Signature/Initials:
Exhibit 8
Exhibit Page 14 of 66
STUDENT MEDICATION LOG NOTES
DATE TIME DATE TIME
DOCUMENTATION OF RECEIPT OF MEDICATIONS
DATE RECEIVED
MEDICATION (Name and dosage)
AMOUNT (# of Tablets or amount
of Liquid)
PARENT/GUARDIAN SIGNATURE
RECEIVED BY (SIGNATURE)
. 9/27/10 OP 151-O-PHN 45 Attachment 32 2
Exhibit 8
Exhibit Page 15 of 66
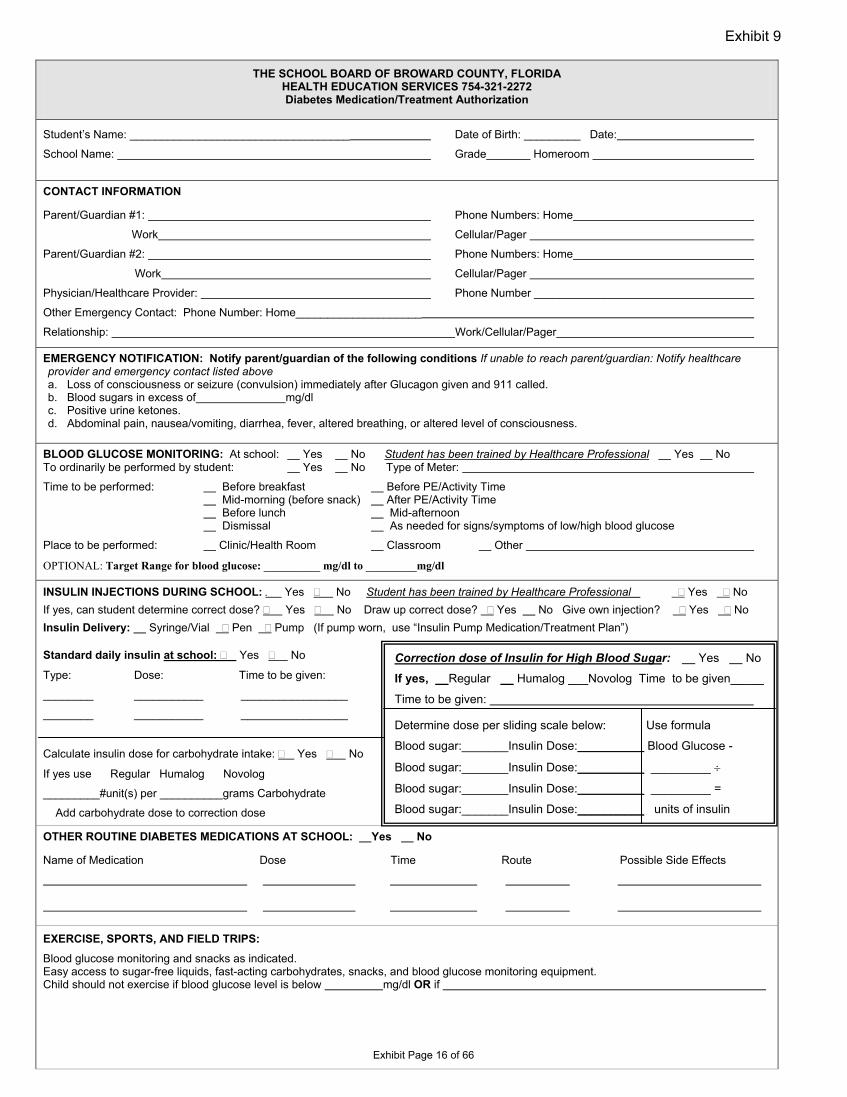
THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDA HEALTH EDUCATION SERVICES 754-321-2272 Diabetes Medication/Treatment Authorization
Student’s Name: ___________________________________ Date of Birth: _________ Date:
School Name: Grade_______ Homeroom
CONTACT INFORMATION
Parent/Guardian #1: Phone Numbers: Home
Work Cellular/Pager
Parent/Guardian #2: Phone Numbers: Home
Work Cellular/Pager
Physician/Healthcare Provider: Phone Number _________________
Other Emergency Contact: Phone Number: Home____________________
Relationship: Work/Cellular/Pager
EMERGENCY NOTIFICATION: Notify parent/guardian of the following conditions If unable to reach parent/guardian: Notify healthcare provider and emergency contact listed above a. Loss of consciousness or seizure (convulsion) immediately after Glucagon given and 911 called.b. Blood sugars in excess of mg/dl c. Positive urine ketones.d. Abdominal pain, nausea/vomiting, diarrhea, fever, altered breathing, or altered level of consciousness.
BLOOD GLUCOSE MONITORING: At school: Yes No Student has been trained by Healthcare Professional Yes No To ordinarily be performed by student: Yes No Type of Meter:
Time to be performed: Before breakfast Before PE/Activity Time Mid-morning (before snack) After PE/Activity Time Before lunch Mid-afternoon Dismissal As needed for signs/symptoms of low/high blood glucose
Place to be performed: Clinic/Health Room Classroom Other
OPTIONAL: Target Range for blood glucose: __________ mg/dl to _________mg/dl
INSULIN INJECTIONS DURING SCHOOL: . Yes � No Student has been trained by Healthcare Professional � Yes � No If yes, can student determine correct dose? � Yes � No Draw up correct dose? � Yes No Give own injection? � Yes � No Insulin Delivery: Syringe/Vial � Pen � Pump (If pump worn, use “Insulin Pump Medication/Treatment Plan”)
Standard daily insulin at school: � Yes � No
Type: Dose: Time to be given:
________ ___________ _________________
________ ___________ _________________
Calculate insulin dose for carbohydrate intake: � Yes � No
If yes use Regular Humalog Novolog
_________#unit(s) per __________grams Carbohydrate
Add carbohydrate dose to correction dose
OTHER ROUTINE DIABETES MEDICATIONS AT SCHOOL: Yes
Name of Medication Dose
EXERCISE, SPORTS, AND FIELD TRIPS: Blood glucose monitoring and snacks as indicated. Easy access to sugar-free liquids, fast-acting carbohydrates, snacks,Child should not exercise if blood glucose level is below m
Exhibit 9
Exh
Correction dose of Insulin for High Blood Sugar: Yes No
If yes, Regular Humalog ___Novolog Time to be given_____
Time to be given:
Determine dose per sliding scale below: Use formula
Blood sugar:_______Insulin Dose:__________ Blood Glucose -
Blood sugar:_______Insulin Dose:__________ _________ ÷
Blood sugar:_______Insulin Dose:__________ _________ =
Blood sugar:_______Insulin Dose:__________ units of insulin
No
Time Route Possible Side Effects
and blood glucose monitoring equipment. g/dl OR if
ibit Page 16 of 66
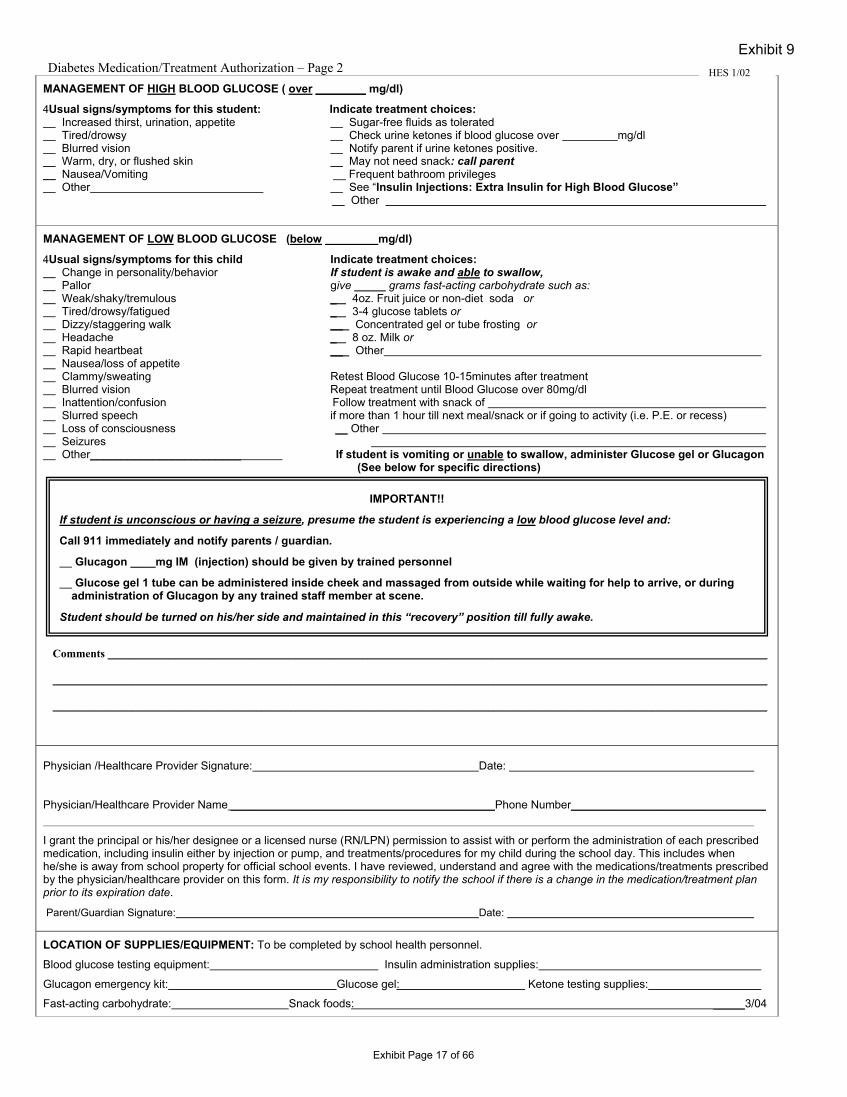
Diabetes Medication/Treatment Authorization – Page 2 MANAGEMENT OF HIGH BLOOD GLUCOSE ( over ________ mg/dl)
4Usual signs/symptoms for this student: Indicate treatment choices: Increased thirst, urination, appetite Sugar-free fluids as tolerated Tired/drowsy Check urine ketones if blood glucose over mg/dl Blurred vision Notify parent if urine ketones positive. Warm, dry, or flushed skin May not need snack: call parent
__ Nausea/Vomiting __ Frequent bathroom privileges Other See “Insulin Injections: Extra Insulin for High Blood Glucose”
Other
MANAGEMENT OF LOW BLOOD GLUCOSE (below mg/dl)
4Usual signs/symptoms for this child Indicate treatment choices: Change in personality/behavior If student is awake and able to swallow, Pallor give _____ grams fast-acting carbohydrate such as: Weak/shaky/tremulous _ 4oz. Fruit juice or non-diet soda or Tired/drowsy/fatigued _ 3-4 glucose tablets or Dizzy/staggering walk __ Concentrated gel or tube frosting or Headache _ 8 oz. Milk or Rapid heartbeat __ Other Nausea/loss of appetite Clammy/sweating Retest Blood Glucose 10-15minutes after treatment Blurred vision Repeat treatment until Blood Glucose over 80mg/dl Inattention/confusion Follow treatment with snack of Slurred speech if more than 1 hour till next meal/snack or if going to activity (i.e. P.E. or recess) Loss of consciousness Other Seizures Other________________________ If student is vomiting or unable to swallow, administer Glucose gel or Glucagon
(See below for specific directions)
Physician /Healthcare Provider Signature: Date:
Physician/Healthcare Provider Name __________________________________________Phone Number_______________________________
I grant the principal or his/her designee or a licensed nurse (RN/LPN) permission to assist with or perform the administration of each prescribed medication, including insulin either by injection or pump, and treatments/procedures for my child during the school day. This includes when he/she is away from school property for official school events. I have reviewed, understand and agree with the medications/treatments prescribed by the physician/healthcare provider on this form. It is my responsibility to notify the school if there is a change in the medication/treatment plan prior to its expiration date.
Parent/Guardian Signature: Date:
LOCATION OF SUPPLIES/EQUIPMENT: To be completed by school health personnel. Blood glucose testing equipment: Insulin administration supplies:
Glucagon emergency kit: Glucose gel: Ketone testing supplies:
Fast-acting carbohydrate: Snack foods: _____3/04
Exhibit 9 HES 1/02
IMPORTANT!! If student is unconscious or having a seizure, presume the student is experiencing a low blood glucose level and:
Call 911 immediately and notify parents / guardian.
Glucagon ____mg IM (injection) should be given by trained personnel
Glucose gel 1 tube can be administered inside cheek and massaged from outside while waiting for help to arrive, or during administration of Glucagon by any trained staff member at scene.
Student should be turned on his/her side and maintained in this “recovery” position till fully awake.
Comments _____________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________
Exhibit Page 17 of 66
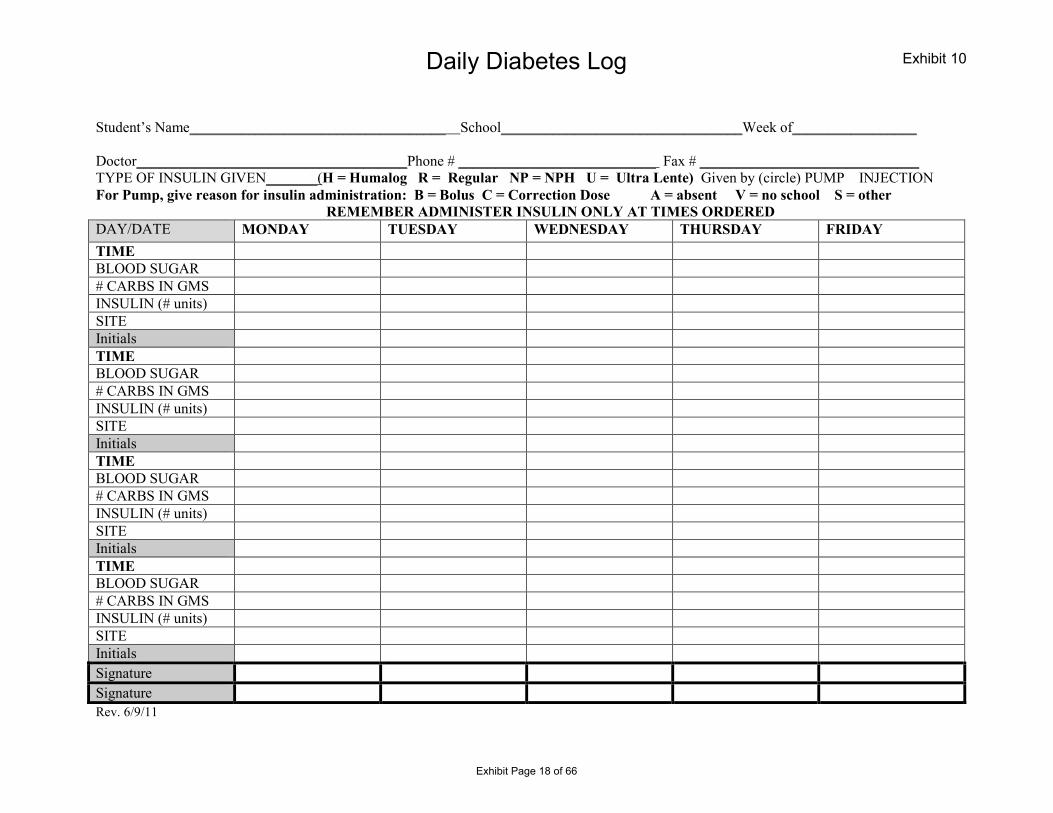
Daily Diabetes Log
Student’s Name___________________________________ School_________________________________Week of_________________
Doctor_____________________________________Phone # ___________________________ Fax # ______________________________ TYPE OF INSULIN GIVEN_______(H = Humalog R = Regular NP = NPH U = Ultra Lente) Given by (circle) PUMP INJECTION For Pump, give reason for insulin administration: B = Bolus C = Correction Dose A = absent V = no school S = other
REMEMBER ADMINISTER INSULIN ONLY AT TIMES ORDERED DAY/DATE MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials TIME BLOOD SUGAR # CARBS IN GMS INSULIN (# units) SITE Initials Signature Signature Rev. 6/9/11
Exhibit 10
Exhibit Page 18 of 66
Daily Diabetes Log
DATE TIME Initials
DATE RECEIVED
MEDICATION (Name and dosage)
AMOUNT PARENT/GUARDIAN SIGNATURE
RECEIVED BY (School designee signature)
HES 4/05 PAGE 2 Rev 6/9/11
Exhibit 10
Exhibit Page 19 of 66
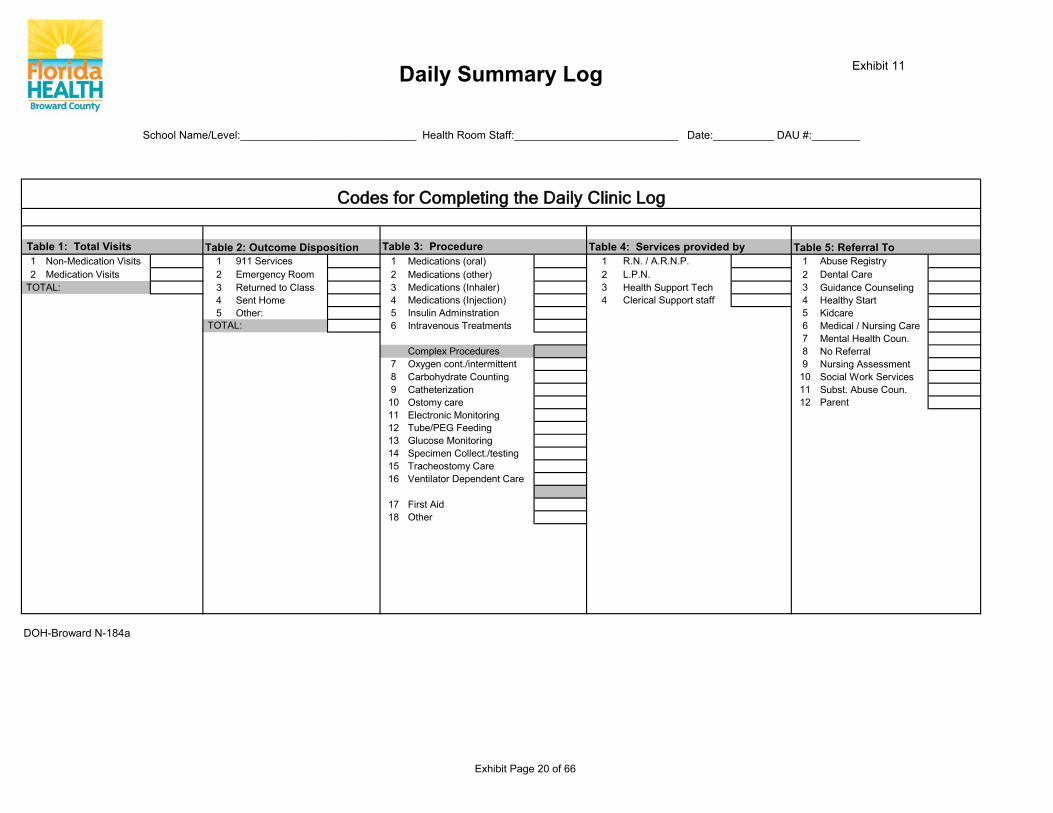
Table 4: Services provided by1 Non-Medication Visits 1 911 Services 1 Medications (oral) 1 R.N. / A.R.N.P. 1 Abuse Registry2 Medication Visits 2 Emergency Room 2 Medications (other) 2 L.P.N. 2 Dental Care
TOTAL: 3 Returned to Class 3 Medications (Inhaler) 3 Health Support Tech 3 Guidance Counseling4 Sent Home 4 Medications (Injection) 4 Clerical Support staff 4 Healthy Start5 Other: 5 Insulin Adminstration 5 Kidcare
TOTAL: 6 Intravenous Treatments 6 Medical / Nursing Care7 Mental Health Coun.
Complex Procedures 8 No Referral7 Oxygen cont./intermittent 9 Nursing Assessment8 Carbohydrate Counting 10 Social Work Services9 Catheterization 11 Subst. Abuse Coun.10 Ostomy care 12 Parent11 Electronic Monitoring12 Tube/PEG Feeding13 Glucose Monitoring14 Specimen Collect./testing 15 Tracheostomy Care16 Ventilator Dependent Care
17 First Aid18 Other
Table 1: Total Visits Table 5: Referral To Table 2: Outcome Disposition
Daily Summary Log
School Name/Level:_____________________________ Health Room Staff:___________________________ Date:__________ DAU #:________
Table 3: Procedure
Codes for Completing the Daily Clinic Log
DOH-Broward N-184a
Exhibit 11
Exhibit Page 20 of 66
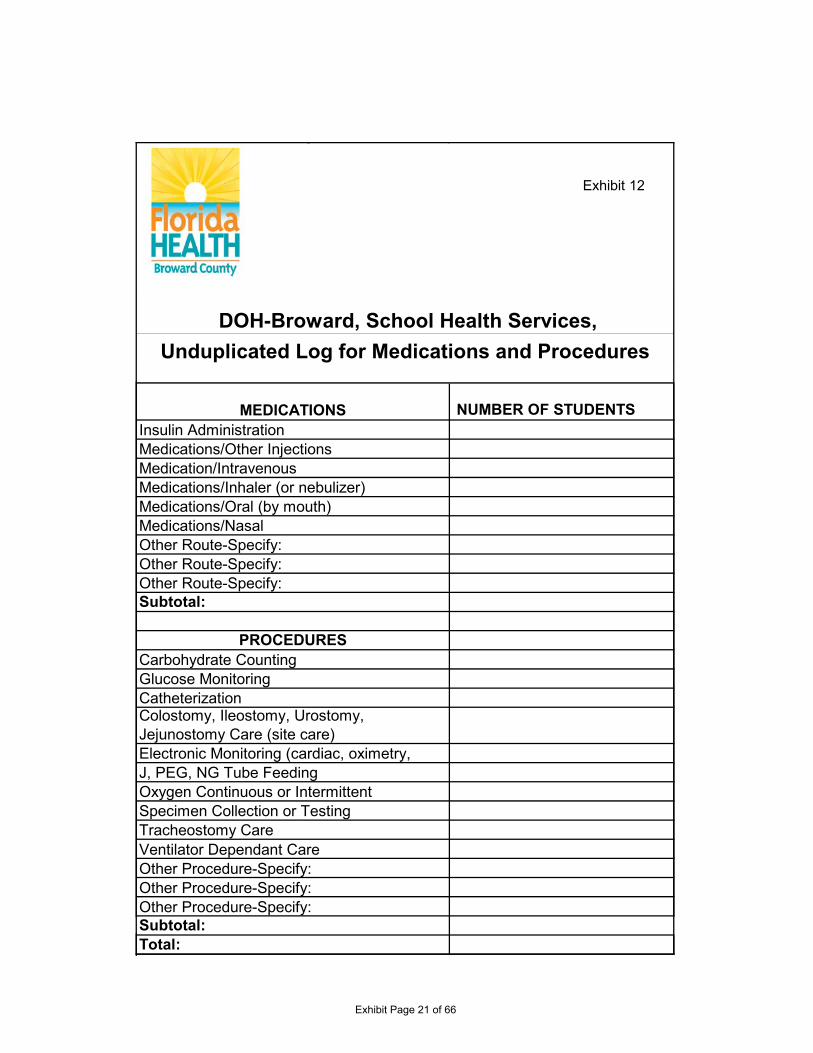
NUMBER OF STUDENTS
Ventilator Dependant CareOther Procedure-Specify:Other Procedure-Specify:Other Procedure-Specify:
MEDICATIONS
Medications/Other InjectionsMedication/IntravenousMedications/Inhaler (or nebulizer)
Colostomy, Ileostomy, Urostomy, Jejunostomy Care (site care)Electronic Monitoring (cardiac, oximetry,
DOH-Broward, School Health Services, Unduplicated Log for Medications and Procedures
Subtotal:
Oxygen Continuous or IntermittentJ, PEG, NG Tube Feeding
Specimen Collection or Testing
PROCEDURES
Insulin Administration
Medications/Oral (by mouth)
Carbohydrate Counting
Total:
Medications/NasalOther Route-Specify:Other Route-Specify:Other Route-Specify:
Glucose MonitoringCatheterization
Subtotal:
Tracheostomy Care
Exhibit 12
Exhibit Page 21 of 66
Revised 09.2013 Page 1 OP 151-O-PHN 45 Attachment 22
# STUDENTS NAME MEDICATION/PRODECURE1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
DOH-Broward, School Health Services · UNDUPLICATED LOGNumber of Students Needing Medications and/or Procedures During 20__ - 20___.
Exhibit 12
Exhibit Page 22 of 66
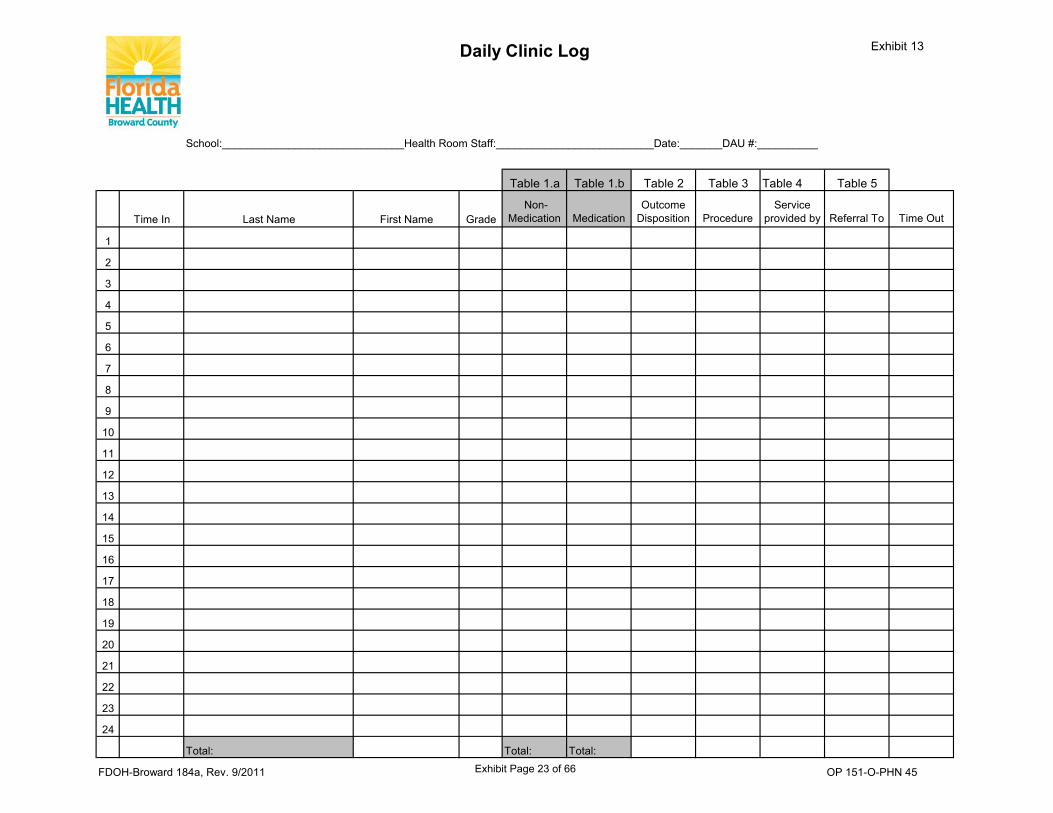
School:______________________________Health Room Staff:__________________________Date:_______DAU #:__________
Table 1.a Table 1.b Table 2 Table 3 Table 4 Table 5
Time In Last Name First Name Grade Non-
Medication MedicationOutcome
Disposition ProcedureService
provided by Referral To Time Out
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
Total: Total: Total:
OP 151-O-PHN 45FDOH-Broward 184a, Rev. 9/2011
Daily Clinic Log Exhibit 13
Exhibit Page 23 of 66
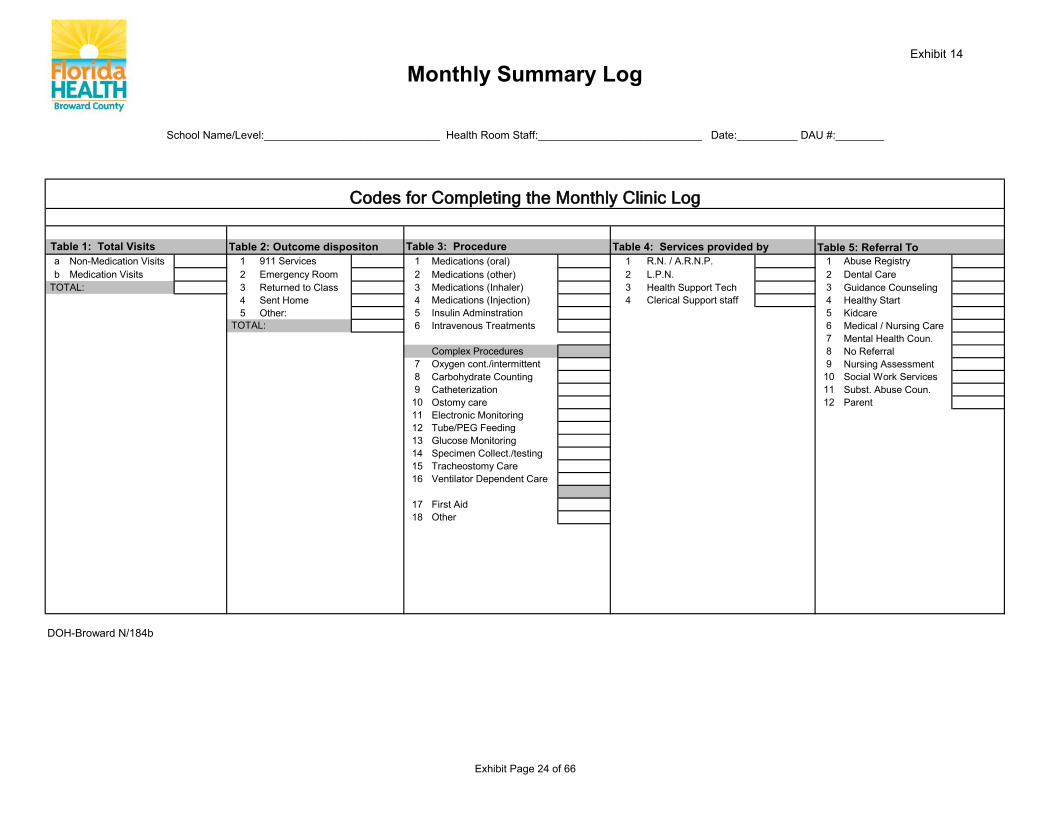
Table 2: Outcome dispositon Table 4: Services provided bya Non-Medication Visits 1 911 Services 1 Medications (oral) 1 R.N. / A.R.N.P. 1 Abuse Registryb Medication Visits 2 Emergency Room 2 Medications (other) 2 L.P.N. 2 Dental Care
TOTAL: 3 Returned to Class 3 Medications (Inhaler) 3 Health Support Tech 3 Guidance Counseling4 Sent Home 4 Medications (Injection) 4 Clerical Support staff 4 Healthy Start5 Other: 5 Insulin Adminstration 5 Kidcare
TOTAL: 6 Intravenous Treatments 6 Medical / Nursing Care7 Mental Health Coun.
Complex Procedures 8 No Referral7 Oxygen cont./intermittent 9 Nursing Assessment8 Carbohydrate Counting 10 Social Work Services9 Catheterization 11 Subst. Abuse Coun.10 Ostomy care 12 Parent11 Electronic Monitoring12 Tube/PEG Feeding13 Glucose Monitoring14 Specimen Collect./testing 15 Tracheostomy Care16 Ventilator Dependent Care
17 First Aid18 Other
DOH-Broward N/184b
Table 1: Total Visits Table 5: Referral To
Monthly Summary Log
School Name/Level:_____________________________ Health Room Staff:___________________________ Date:__________ DAU #:________
Table 3: Procedure
Codes for Completing the Monthly Clinic Log
Exhibit 14
Exhibit Page 24 of 66
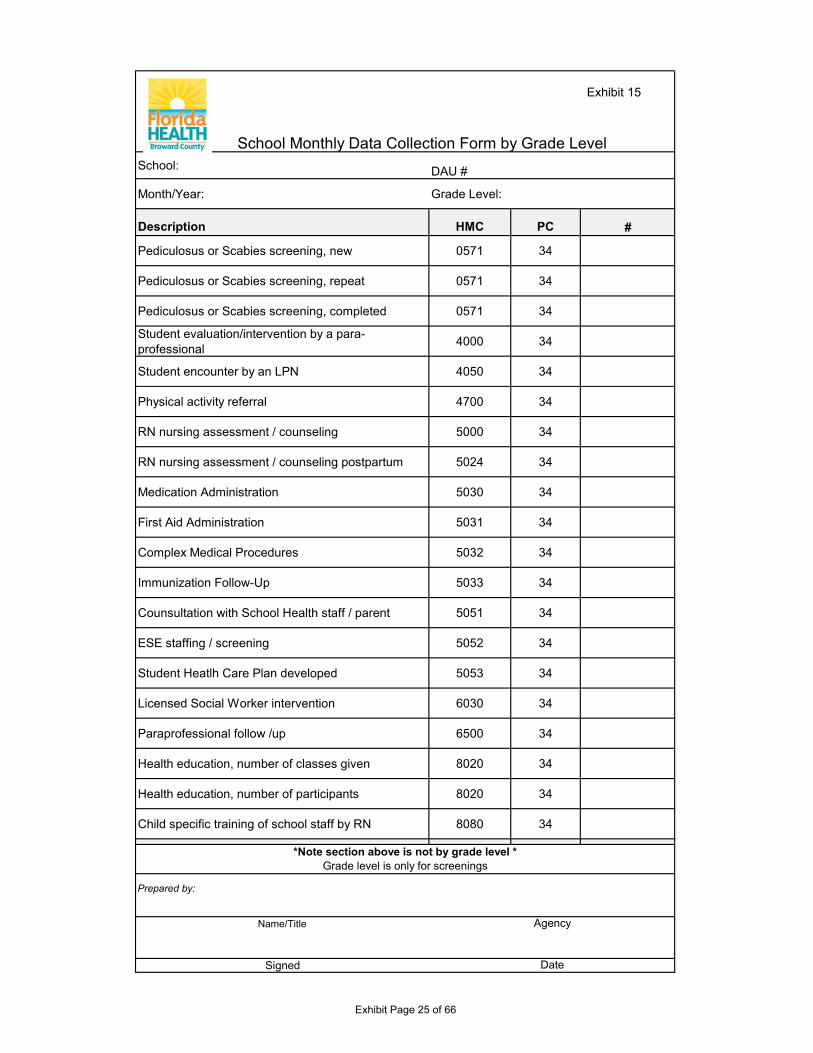
School Monthly Data Collection Form by Grade LevelSchool: DAU #
Month/Year: Grade Level:
Description HMC PC #
Pediculosus or Scabies screening, new 0571 34
Pediculosus or Scabies screening, repeat 0571 34
Pediculosus or Scabies screening, completed 0571 34
Student evaluation/intervention by a para-professional 4000 34
Student encounter by an LPN 4050 34
Physical activity referral 4700 34
RN nursing assessment / counseling 5000 34
RN nursing assessment / counseling postpartum 5024 34
Medication Administration 5030 34
First Aid Administration 5031 34
Complex Medical Procedures 5032 34
Immunization Follow-Up 5033 34
Counsultation with School Health staff / parent 5051 34
ESE staffing / screening 5052 34
Student Heatlh Care Plan developed 5053 34
Licensed Social Worker intervention 6030 34
Paraprofessional follow /up 6500 34
Health education, number of classes given 8020 34
Health education, number of participants 8020 34
Child specific training of school staff by RN 8080 34
Prepared by:
Name/Title
Signed Date
*Note section above is not by grade level *Grade level is only for screenings
Agency
Exhibit 15
Exhibit Page 25 of 66
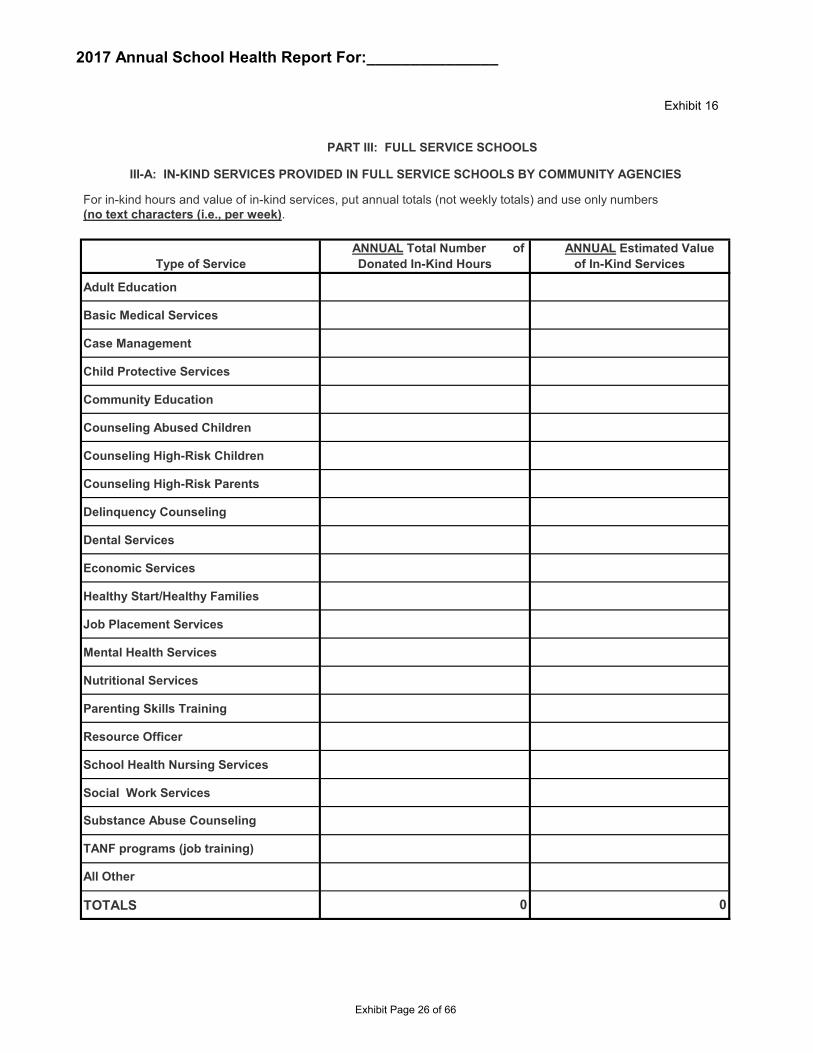
2017 Annual School Health Report For:_______________
For in-kind hours and value of in-kind services, put annual totals (not weekly totals) and use only numbers (no text characters (i.e., per week).
Adult Education
Basic Medical Services
Case Management
Child Protective Services
Community Education
Counseling Abused Children
Counseling High-Risk Children
Counseling High-Risk Parents
Delinquency Counseling
Dental Services
Economic Services
Healthy Start/Healthy Families
Job Placement Services
Mental Health Services
Nutritional Services
Parenting Skills Training
Resource Officer
School Health Nursing Services
Social Work Services
TOTALS 0 0
All Other
Substance Abuse Counseling
TANF programs (job training)
PART III: FULL SERVICE SCHOOLS
ANNUAL Total Number of Donated In-Kind Hours
ANNUAL Estimated Value of In-Kind ServicesType of Service
III-A: IN-KIND SERVICES PROVIDED IN FULL SERVICE SCHOOLS BY COMMUNITY AGENCIES
Exhibit 16
Exhibit Page 26 of 66
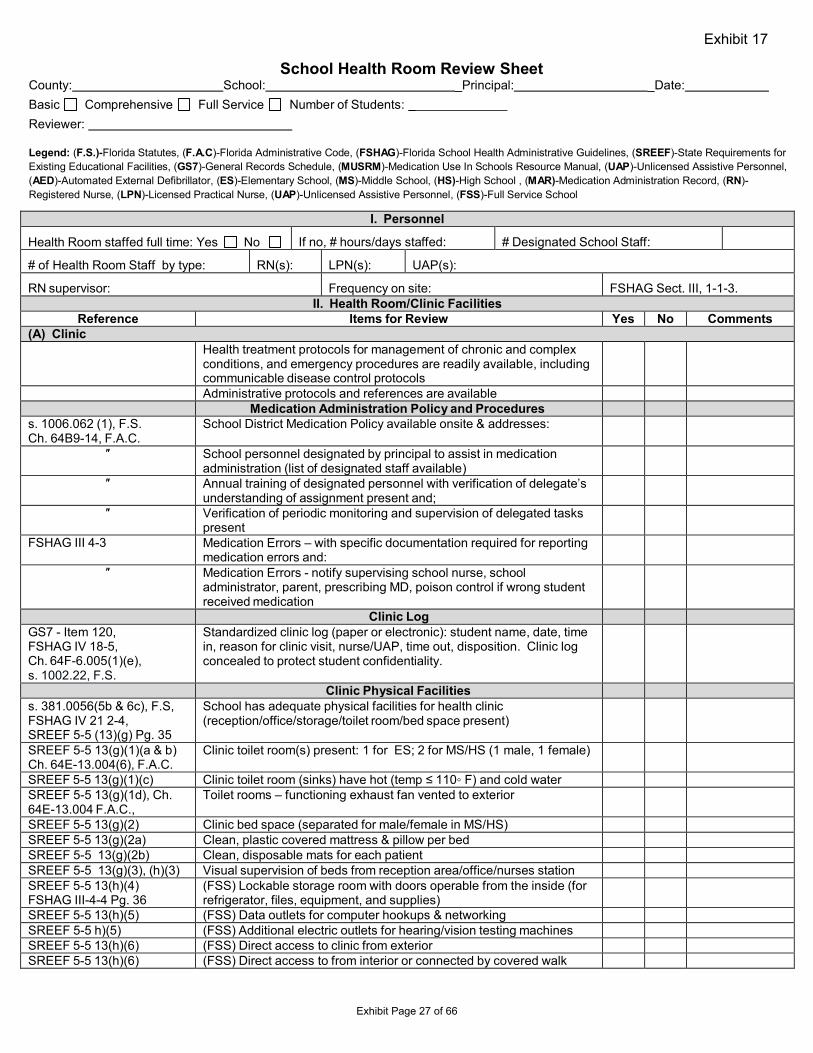
School Health Room Review Sheet County: School: _Principal: _Date: Basic Comprehensive Full Service Number of Students: Reviewer:
Legend: (F.S.)-Florida Statutes, (F.A.C)-Florida Administrative Code, (FSHAG)-Florida School Health Administrative Guidelines, (SREEF)-State Requirements for Existing Educational Facilities, (GS7)-General Records Schedule, (MUSRM)-Medication Use In Schools Resource Manual, (UAP)-Unlicensed Assistive Personnel, (AED)-Automated External Defibrillator, (ES)-Elementary School, (MS)-Middle School, (HS)-High School , (MAR)-Medication Administration Record, (RN)- Registered Nurse, (LPN)-Licensed Practical Nurse, (UAP)-Unlicensed Assistive Personnel, (FSS)-Full Service School
I. Personnel
Health Room staffed full time: Yes No If no, # hours/days staffed: # Designated School Staff:
# of Health Room Staff by type: RN(s): LPN(s): UAP(s):
RN supervisor: Frequency on site: FSHAG Sect. III, 1-1-3. II. Health Room/Clinic Facilities
Reference Items for Review Yes No Comments (A) Clinic
Health treatment protocols for management of chronic and complex conditions, and emergency procedures are readily available, including communicable disease control protocols Administrative protocols and references are available
Medication Administration Policy and Procedures s. 1006.062 (1), F.S.Ch. 64B9-14, F.A.C.
School District Medication Policy available onsite & addresses:
″ School personnel designated by principal to assist in medication administration (list of designated staff available)
″ Annual training of designated personnel with verification of delegate’s understanding of assignment present and;
″ Verification of periodic monitoring and supervision of delegated tasks present
FSHAG III 4-3 Medication Errors – with specific documentation required for reporting medication errors and:
″ Medication Errors - notify supervising school nurse, school administrator, parent, prescribing MD, poison control if wrong student received medication
Clinic Log GS7 - Item 120, FSHAG IV 18-5, Ch. 64F-6.005(1)(e), s. 1002.22, F.S.
Standardized clinic log (paper or electronic): student name, date, time in, reason for clinic visit, nurse/UAP, time out, disposition. Clinic log concealed to protect student confidentiality.
Clinic Physical Facilities s. 381.0056(5b & 6c), F.S,FSHAG IV 21 2-4, SREEF 5-5 (13)(g) Pg. 35
School has adequate physical facilities for health clinic (reception/office/storage/toilet room/bed space present)
SREEF 5-5 13(g)(1)(a & b) Ch. 64E-13.004(6), F.A.C.
Clinic toilet room(s) present: 1 for ES; 2 for MS/HS (1 male, 1 female)
SREEF 5-5 13(g)(1)(c) Clinic toilet room (sinks) have hot (temp ≤ 110◦ F) and cold water SREEF 5-5 13(g)(1d), Ch. 64E-13.004 F.A.C.,
Toilet rooms – functioning exhaust fan vented to exterior
SREEF 5-5 13(g)(2) Clinic bed space (separated for male/female in MS/HS) SREEF 5-5 13(g)(2a) Clean, plastic covered mattress & pillow per bed SREEF 5-5 13(g)(2b) Clean, disposable mats for each patient SREEF 5-5 13(g)(3), (h)(3) Visual supervision of beds from reception area/office/nurses station SREEF 5-5 13(h)(4) FSHAG III-4-4 Pg. 36
(FSS) Lockable storage room with doors operable from the inside (for refrigerator, files, equipment, and supplies)
SREEF 5-5 13(h)(5) (FSS) Data outlets for computer hookups & networking SREEF 5-5 h)(5) (FSS) Additional electric outlets for hearing/vision testing machines SREEF 5-5 13(h)(6) (FSS) Direct access to clinic from exterior SREEF 5-5 13(h)(6) (FSS) Direct access to from interior or connected by covered walk
Exhibit 17
Exhibit Page 27 of 66
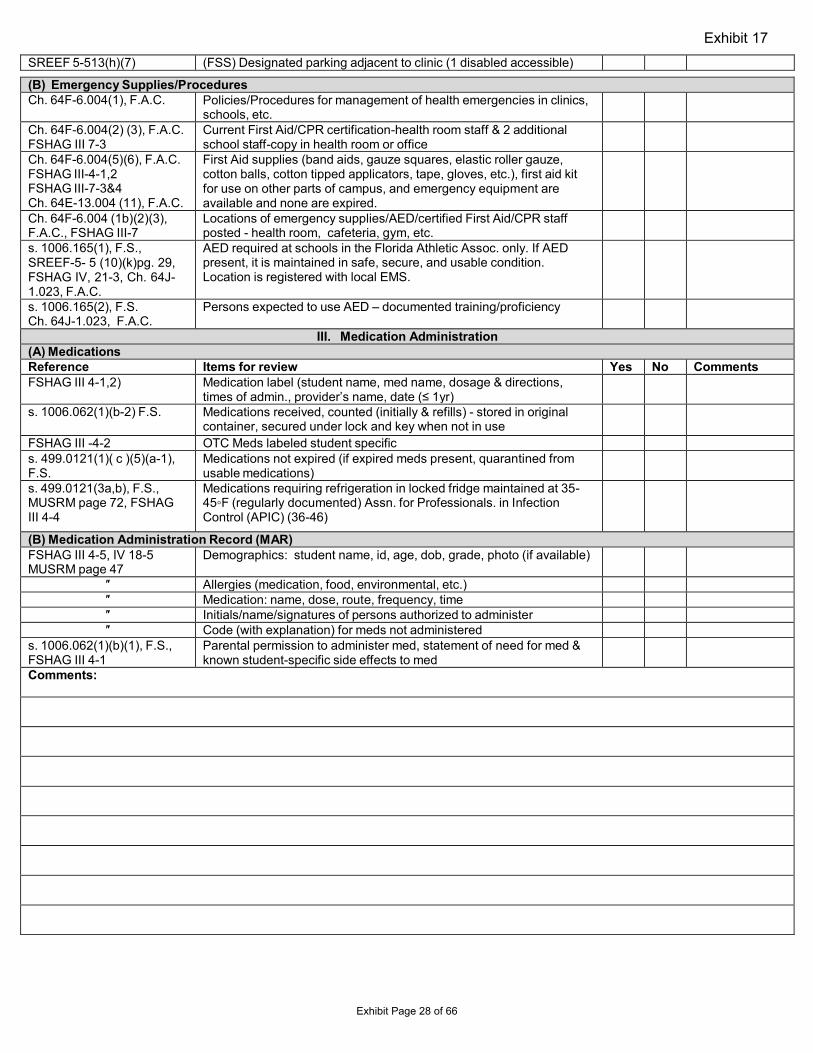
SREEF 5-513(h)(7) (FSS) Designated parking adjacent to clinic (1 disabled accessible)
(B) Emergency Supplies/Procedures Ch. 64F-6.004(1), F.A.C. Policies/Procedures for management of health emergencies in clinics,
schools, etc. Ch. 64F-6.004(2) (3), F.A.C. FSHAG III 7-3
Current First Aid/CPR certification-health room staff & 2 additional school staff-copy in health room or office
Ch. 64F-6.004(5)(6), F.A.C. FSHAG III-4-1,2 FSHAG III-7-3&4 Ch. 64E-13.004 (11), F.A.C.
First Aid supplies (band aids, gauze squares, elastic roller gauze, cotton balls, cotton tipped applicators, tape, gloves, etc.), first aid kit for use on other parts of campus, and emergency equipment are available and none are expired.
Ch. 64F-6.004 (1b)(2)(3), F.A.C., FSHAG III-7
Locations of emergency supplies/AED/certified First Aid/CPR staff posted - health room, cafeteria, gym, etc.
s. 1006.165(1), F.S.,SREEF-5- 5 (10)(k)pg. 29, FSHAG IV, 21-3, Ch. 64J- 1.023, F.A.C.
AED required at schools in the Florida Athletic Assoc. only. If AED present, it is maintained in safe, secure, and usable condition. Location is registered with local EMS.
s. 1006.165(2), F.S.Ch. 64J-1.023, F.A.C.
Persons expected to use AED – documented training/proficiency
III. Medication Administration(A) Medications Reference Items for review Yes No Comments FSHAG III 4-1,2) Medication label (student name, med name, dosage & directions,
times of admin., provider’s name, date (≤ 1yr) s. 1006.062(1)(b-2) F.S. Medications received, counted (initially & refills) - stored in original
container, secured under lock and key when not in use FSHAG III -4-2 OTC Meds labeled student specific s. 499.0121(1)( c )(5)(a-1),F.S.
Medications not expired (if expired meds present, quarantined from usable medications)
s. 499.0121(3a,b), F.S.,MUSRM page 72, FSHAG III 4-4
Medications requiring refrigeration in locked fridge maintained at 35- 45◦F (regularly documented) Assn. for Professionals. in Infection Control (APIC) (36-46)
(B) Medication Administration Record (MAR) FSHAG III 4-5, IV 18-5 MUSRM page 47
Demographics: student name, id, age, dob, grade, photo (if available)
″ Allergies (medication, food, environmental, etc.) ″ Medication: name, dose, route, frequency, time ″ Initials/name/signatures of persons authorized to administer ″ Code (with explanation) for meds not administered
s. 1006.062(1)(b)(1), F.S.,FSHAG III 4-1
Parental permission to administer med, statement of need for med & known student-specific side effects to med
Comments:
Exhibit 17
Exhibit Page 28 of 66
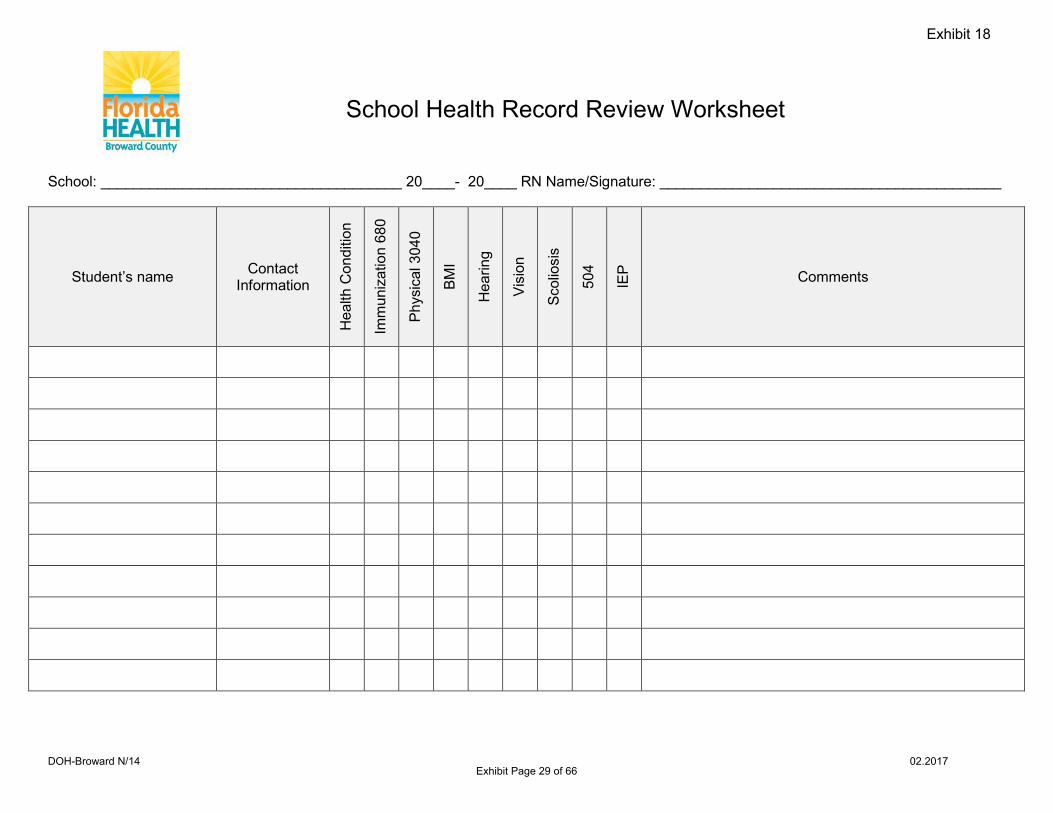
School: _____________________________________ 20____- 20____ RN Name/Signature: __________________________________________
Student’s name Contact Information
Hea
lth C
ondi
tion
Imm
uniz
atio
n 68
0
Phys
ical
304
0
BMI
Hea
ring
Visi
on
Scol
iosi
s
504
IEP Comments
School Health Record Review Worksheet
Exhibit 18
DOH-Broward N/14 02.2017 Exhibit Page 29 of 66
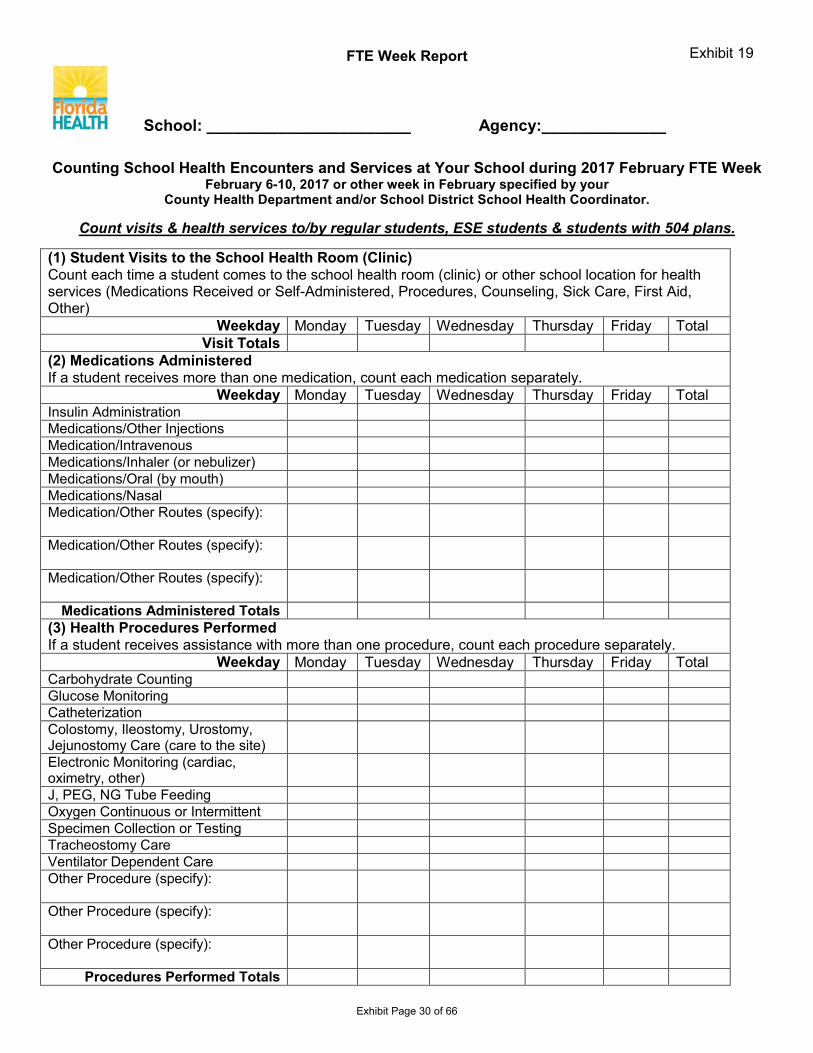
FTE Week Report
School: _______________________ Agency:______________
Counting School Health Encounters and Services at Your School during 2017 February FTE Week February 6-10, 2017 or other week in February specified by your
County Health Department and/or School District School Health Coordinator.
Count visits & health services to/by regular students, ESE students & students with 504 plans.
(1) Student Visits to the School Health Room (Clinic) Count each time a student comes to the school health room (clinic) or other school location for health services (Medications Received or Self-Administered, Procedures, Counseling, Sick Care, First Aid, Other)
Weekday Monday Tuesday Wednesday Thursday Friday Total Visit Totals
(2) Medications Administered If a student receives more than one medication, count each medication separately.
Weekday Monday Tuesday Wednesday Thursday Friday Total Insulin Administration Medications/Other Injections Medication/Intravenous Medications/Inhaler (or nebulizer) Medications/Oral (by mouth) Medications/Nasal Medication/Other Routes (specify):
Medication/Other Routes (specify):
Medication/Other Routes (specify):
Medications Administered Totals (3) Health Procedures Performed If a student receives assistance with more than one procedure, count each procedure separately.
Weekday Monday Tuesday Wednesday Thursday Friday Total Carbohydrate Counting Glucose Monitoring Catheterization Colostomy, Ileostomy, Urostomy, Jejunostomy Care (care to the site) Electronic Monitoring (cardiac, oximetry, other) J, PEG, NG Tube Feeding Oxygen Continuous or Intermittent Specimen Collection or Testing Tracheostomy Care Ventilator Dependent Care Other Procedure (specify):
Other Procedure (specify):
Other Procedure (specify):
Procedures Performed Totals
Exhibit 19
Exhibit Page 30 of 66
RN School Visit Log
RN Name: RN Signature: Dates: _____ - _____
Date School Visited Time In
Time out
Total Hours
School Personnel Signature
Exhibit 20
DOH-Broward 01.2017 Exhibit Page 31 of 66