Embed Size (px)
Citation preview

1
Modern Approaches to Spinal Modern Approaches to Spinal Tumor SurgeryTumor Surgery
Christopher Ames MDChristopher Ames MDDirector Director
Spinal Tumor and Deformity ServiceSpinal Tumor and Deformity ServiceCoCo--Director Director NeurospinalNeurospinal DisordersDisordersUCSF Department of NeurosurgeryUCSF Department of Neurosurgery
OrganizationOrganization--TalkTalk
TranspedicularTranspedicular approach for ventral approach for ventral intraduralintradural tumorstumorsTranspedicularTranspedicular CorpectomyCorpectomyEn Bloc ResectionEn Bloc ResectionEn Bloc En Bloc SpondylectomySpondylectomyEn Bloc Complete En Bloc Complete SacrectomySacrectomyCombined Combined SacrectomySacrectomy/Pelvic Resection/Pelvic Resection
Skull Base Surgery for Skull Base Surgery for the Spinethe Spine
DefinitionDefinition
Minimize or eliminate neural element Minimize or eliminate neural element retraction retraction Accomplish this by maximizing Accomplish this by maximizing exposure through resection of boneexposure through resection of boneIntimate knowledge of local anatomy Intimate knowledge of local anatomy and tumor anatomy allows selection of and tumor anatomy allows selection of optimum approach corridor optimum approach corridor
Application to SpineApplication to Spine
Previous approach to ventral and Previous approach to ventral and ventral lateral ventral lateral intraduralintradural tumorstumors–– LaminectomyLaminectomy and and FacetectomyFacetectomy–– Cut nerve roots Cut nerve roots ––C1C1--C4, T2 and belowC4, T2 and below–– Dentate ligament section and cord Dentate ligament section and cord
rotation/retractionrotation/retraction–– NeuromonitoringNeuromonitoring SSEP/MEP/EMG to alert SSEP/MEP/EMG to alert
to potential problems to potential problems while problem is still while problem is still reversiblereversible
Direct Anterior ApproachDirect Anterior ApproachAccess corridor is deep and narrow for Access corridor is deep and narrow for cervical approachcervical approach——i.e. i.e. corpectomycorpectomyProblematic for multilevel casesProblematic for multilevel cases——sacrificing sacrificing significant anterior column bone to access significant anterior column bone to access lesionlesionCome right down on the tumorCome right down on the tumor——dondon’’t t visualize normal anatomy firstvisualize normal anatomy firstDifficult Difficult duraldural reconstructionreconstructionProbably best used only for single level, Probably best used only for single level, purely ventral lesions purely ventral lesions ––lateral component lateral component may be challenging to reachmay be challenging to reach

2
Limitations of Traditional Posterior Limitations of Traditional Posterior ApproachApproach
Poor visualization of tumorPoor visualization of tumorConstant cord retraction in order to Constant cord retraction in order to workworkBlood loss from internal tumor Blood loss from internal tumor debulkingdebulkingNo working roomNo working roomMEP changes may be sudden and MEP changes may be sudden and irreversibleirreversible
NeuromonitoringNeuromonitoring ChangesChanges
Cord already compromised and now Cord already compromised and now must be retracted and rotatedmust be retracted and rotatedBlood loss and hypotension during Blood loss and hypotension during resectionresectionNerve root EMG activity of unclear Nerve root EMG activity of unclear significancesignificance
New TechniqueNew Technique
Lateral Lateral ParamedianParamedian TranspedicularTranspedicularApproach for Approach for IntraduralIntradural TumorsTumors
Spine March 15 2007
Cervical Spine Presents Unique Cervical Spine Presents Unique ChallengesChallenges
Where is the lesion??
?
Necessity of Necessity of PediculectomyPediculectomy
Increased working roomImproved nerve root mobilization
3
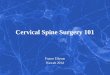
Vertebral Artery Mobilization/Dorsal Vertebral Artery Mobilization/Dorsal CorpectomyCorpectomy (working room)(working room)
Remove with Lempert or upbiting pituitary
Partial Partial CorpectomyCorpectomy TechniqueTechnique DuralDural H FlapH Flap
Downward Downward duraldural traction traction ““deliversdelivers””tumor en bloc away from cordtumor en bloc away from cord Table Rotation Improves ViewTable Rotation Improves View

4
Case 1Case 1
18 18 y.oy.o. female about to begin college . female about to begin college with mild LE weakness, right hand with mild LE weakness, right hand weaknessweakness
Case 2 –after bone and pedicle resection prior to table rotation
After table rotation and tumor After table rotation and tumor resectionresection Case 1 ReconstructionCase 1 Reconstruction
Case 2Case 2
38 38 y.oy.o. mother of 2 with progressive LE . mother of 2 with progressive LE weaknessweaknessPMH: NF1PMH: NF1

5
Visualization Visualization and Working and Working SpaceSpace
Case 3 Large but LateralizedCase 3 Large but Lateralized
Reconstruction TechniqueReconstruction Technique
Significant vertebral column resection Significant vertebral column resection results in instabilityresults in instabilityLoss of posterior fusion surface Loss of posterior fusion surface Loss of fixation points in lateral mass and Loss of fixation points in lateral mass and pediclespediclesNeed to engage anterior column for Need to engage anterior column for lordosislordosis restorationrestoration
Translational WorkTranslational Work--TechniquesTechniques ReconstructionReconstruction
Artificial pedicle screws Artificial pedicle screws –– Requires only vertebral bodyRequires only vertebral body–– Cortical Cortical –– Control of anterior column for reductionControl of anterior column for reduction–– Placed under direct vision, no danger toPlaced under direct vision, no danger to
vertebral arteryvertebral arteryMay also be used for fractured lateral May also be used for fractured lateral mass bailout for routine pathologymass bailout for routine pathology

6
Artificial Pedicle ScrewsArtificial Pedicle Screws VA APS
Construct ShorteningConstruct Shortening
LordosisLordosis Restoration with APSRestoration with APS Fusion SurfaceFusion Surface
BMP-2 Local autograft

7
TranspedicularTranspedicular CorpectomyCorpectomyfor for MetastaticMetastatic DiseaseDisease
TokuhashiTokuhashi Scoring systemScoring system(who we operate on)(who we operate on)
1. Who to operate on2. How much surgery to do
TokuhashiTokuhashi Scoring System for Scoring System for MetastaticMetastaticSpine Tumor Prognosis Spine 2005Spine Tumor Prognosis Spine 2005
TokuhashiTokuhashi score and survival score and survival validationvalidation •62F metastatic breast CA
•s/p T2-T3 laminectomy and tumor debulking 1 month ago at outside institution•1 week history of increasing pain and LE weakness•Disease otherwise controlled
T2, T3, T4
TranspedicularTranspedicular corpectomycorpectomy
Eliminates need to open sternum or Eliminates need to open sternum or thoracic cavitythoracic cavityAllows complete Allows complete vertebrectomyvertebrectomy over 1, 2, over 1, 2, 3 or more levels3 or more levelsSimultaneous anterior and posterior Simultaneous anterior and posterior column reconstructioncolumn reconstructionCan be used in cervical, thoracic and Can be used in cervical, thoracic and lumbar spinelumbar spineExpandable cages very beneficial hereExpandable cages very beneficial here

8
Posterior ApproachesPosterior Approaches
TranspedicularTranspedicular CorpectomyCorpectomy–– C7C7--L5 L5 –– C2C2--C6 with unilateral vertebral sacrificeC6 with unilateral vertebral sacrifice–– One approach reconstructs anterior and One approach reconstructs anterior and
posterior columnsposterior columns–– The most extensileThe most extensile–– No difficulty with instrumentation placement No difficulty with instrumentation placement
around great vesselsaround great vessels
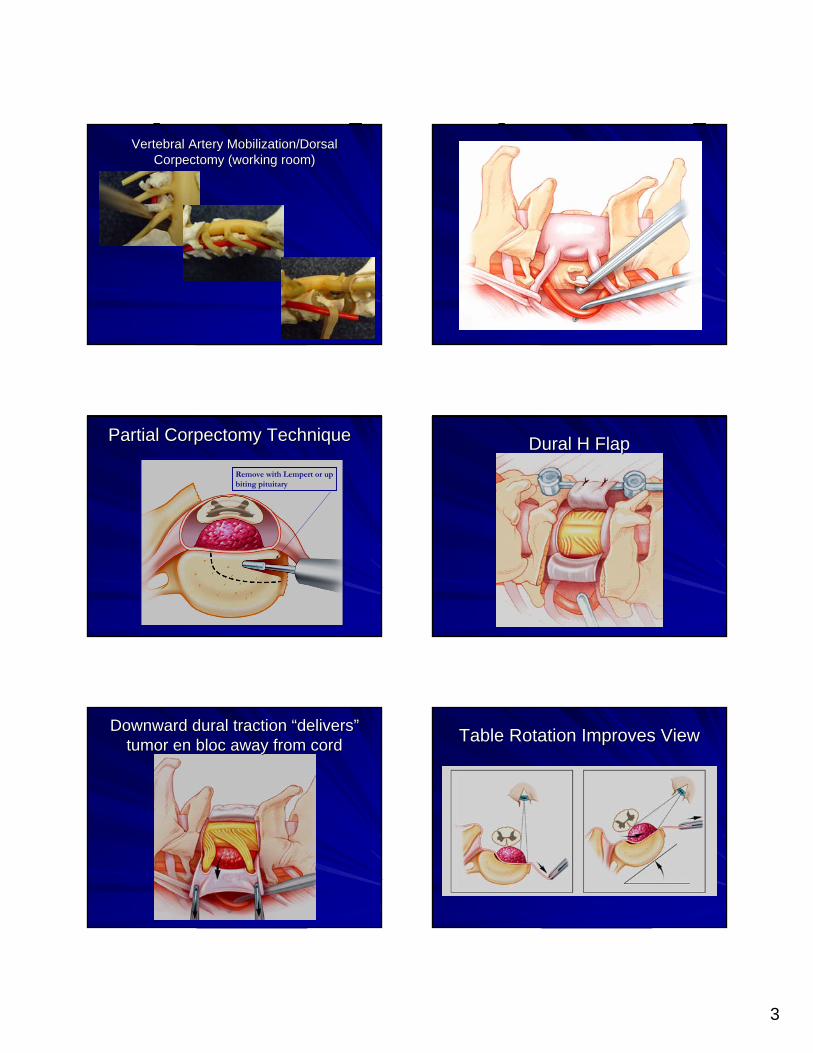
TechniqueTechnique
TechniqueTechnique TechniqueTechnique
TechniqueTechnique TechniqueTechnique
9
TechniqueTechnique TechniqueTechnique
TechniqueTechnique TechniqueTechnique
T2, T3, T4 T2
SternotomySternotomy
10
T2
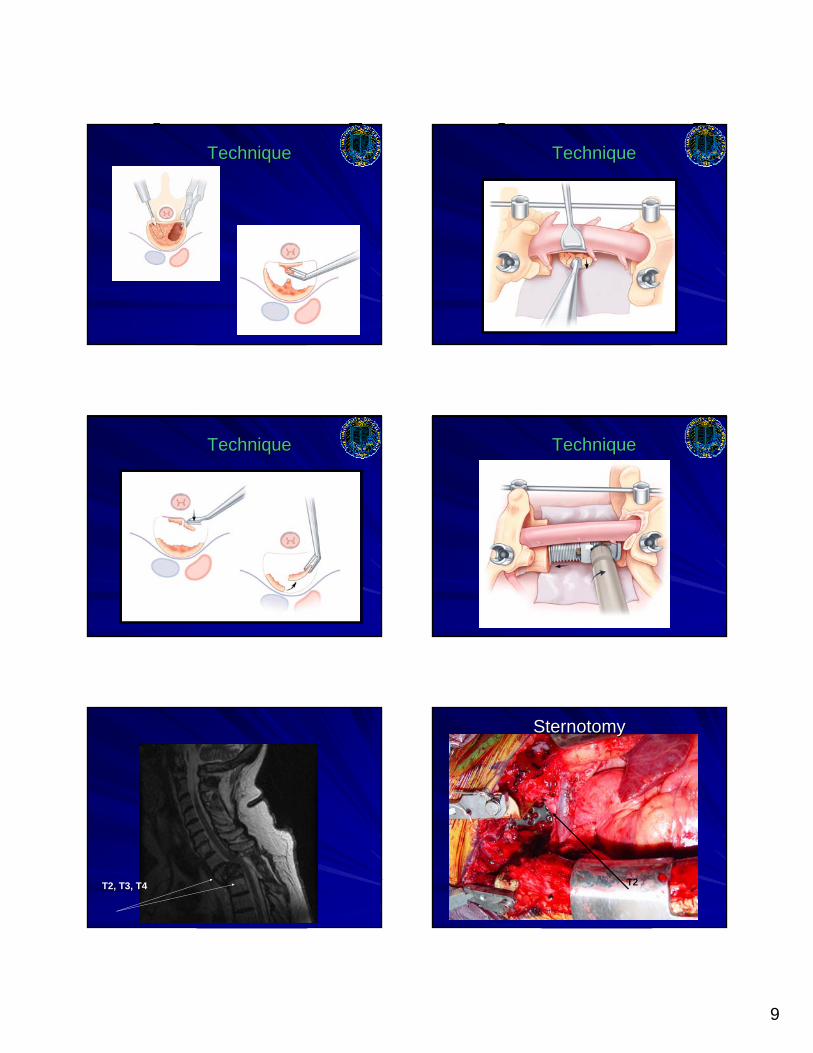
HemiHemi--clamshell/Trapdoorclamshell/Trapdoor
T2
T6
Trapdoor/Trapdoor/HemiclamshellHemiclamshell LimitsLimits
T1 corpectomy-low anteriorCervical/manubrectomy
T2-3 Sternal Split
T4 High Lateral Thoracotomy
TranspedicularCorpectomy
HemiClamshell/Trapdoor

11
OutcomeOutcome
Strength dramatically improvedStrength dramatically improvedNow ambulatingNow ambulatingDCDC’’dd to rehab POD #5to rehab POD #5
TPC Case Example 2TPC Case Example 2
63 63 yoyo male, LE male, LE weakness, renal CAweakness, renal CATPC @ L3? L2? L1?TPC @ L3? L2? L1?T1?T1?
S1

12
En Bloc ResectionEn Bloc Resection
Mayo 2005 Mayo 2005 ChordomaChordoma
Translational WorkTranslational Work--TechniqueTechnique
JCNS 2007
BorianiBoriani ClassificationClassification

13
H and PH and P
44 44 yoyo female with r le weakness female with r le weakness Q/TA/EHL 4/5Q/TA/EHL 4/5Referring DXReferring DX--benign nerve sheath tumor, benign nerve sheath tumor, neurofibromaneurofibroma
PlanPlan
Needle Needle bxbx––LeiomyosarcomaLeiomyosarcoma ––medium medium gradegrade
TXTX
En bloc posterior resection with L5 En bloc posterior resection with L5 hemicorpectomyhemicorpectomy via via sagittalsagittal osteotomyosteotomySacrifice of R L4, L5 rootsSacrifice of R L4, L5 rootsAnteriorAnterior--Ex Lap, Ex Lap, bxbx nodes, completion nodes, completion corpectomycorpectomy for reconstruction, IORTfor reconstruction, IORT

14

15
En Bloc En Bloc SpondylectomySpondylectomy
En Bloc En Bloc SpondylectomySpondylectomy
Complete removal of vertebral segment in Complete removal of vertebral segment in 2 pieces2 piecesMinimize violation of tumor to prevent Minimize violation of tumor to prevent seedingseedingApplication of surgical Application of surgical oncologicaloncologicalprincipals to spinal oncologyprincipals to spinal oncologyChordomaChordoma, , OsteosarcomaOsteosarcoma, , ChondrosarcomaChondrosarcoma, ? Isolated , ? Isolated metastaticmetastaticdiseasedisease
En Bloc En Bloc SpondylectomySpondylectomy
Boriani Spine 1997
Enneking Staging
En Bloc En Bloc SpondylectomySpondylectomy
WBB Surgical Staging
H and PH and P
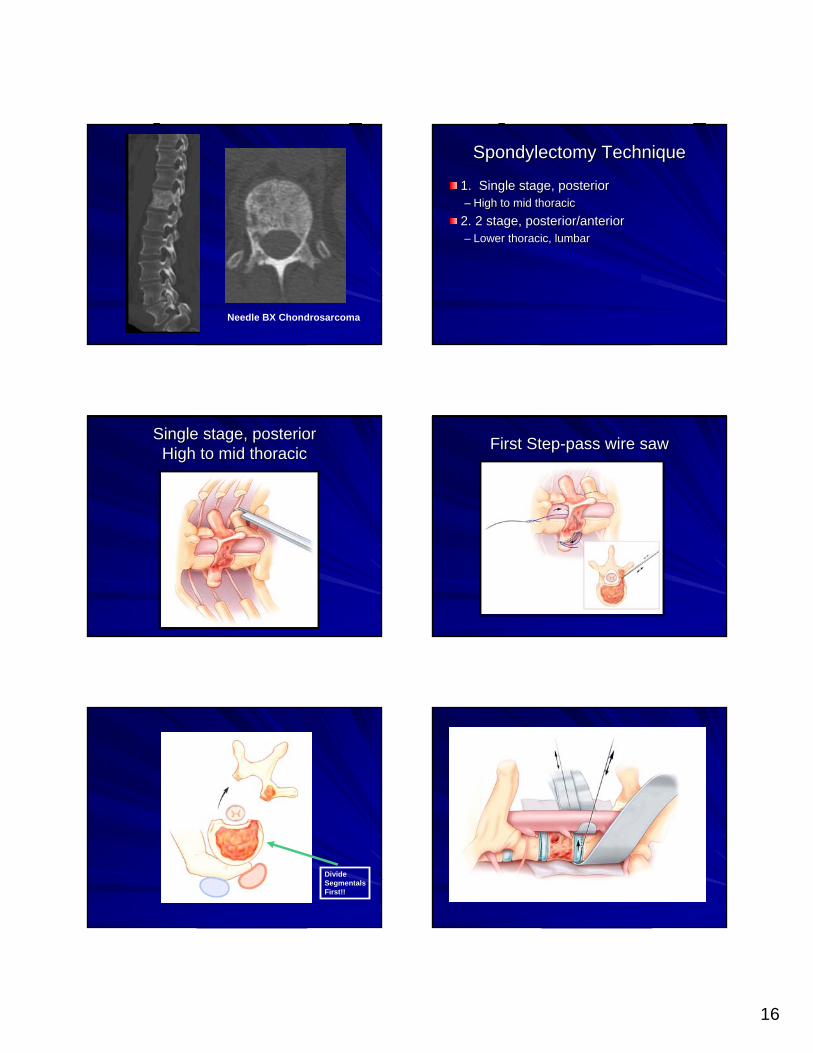
45 45 y.oy.o male presents with a 6 month male presents with a 6 month history of T/L junction painhistory of T/L junction painNeuroNeuro exam is normalexam is normal
16
Needle BX Chondrosarcoma
SpondylectomySpondylectomy TechniqueTechnique
1. Single stage, posterior1. Single stage, posterior–– High to mid thoracicHigh to mid thoracic
2. 2 stage, posterior/anterior2. 2 stage, posterior/anterior–– Lower thoracic, lumbarLower thoracic, lumbar
Single stage, posteriorSingle stage, posteriorHigh to mid thoracicHigh to mid thoracic First StepFirst Step--pass wire sawpass wire saw
Divide SegmentalsFirst!!

17
Single stage, posteriorSingle stage, posteriorHigh to mid thoracicHigh to mid thoracic
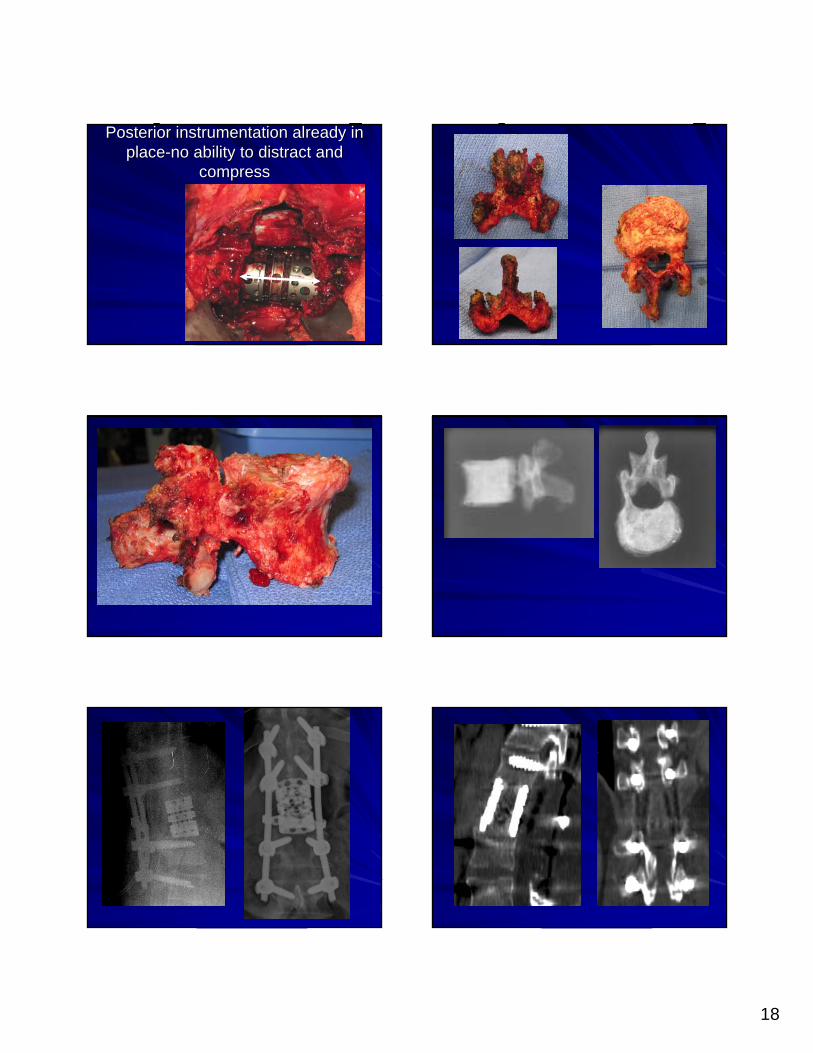
Back to our caseBack to our case2 stages since T122 stages since T12Larger bodyLarger bodyAny ? Of anterior Any ? Of anterior vessel attachmentsvessel attachments
18
Posterior instrumentation already in Posterior instrumentation already in placeplace--no ability to distract and no ability to distract and
compresscompress
19
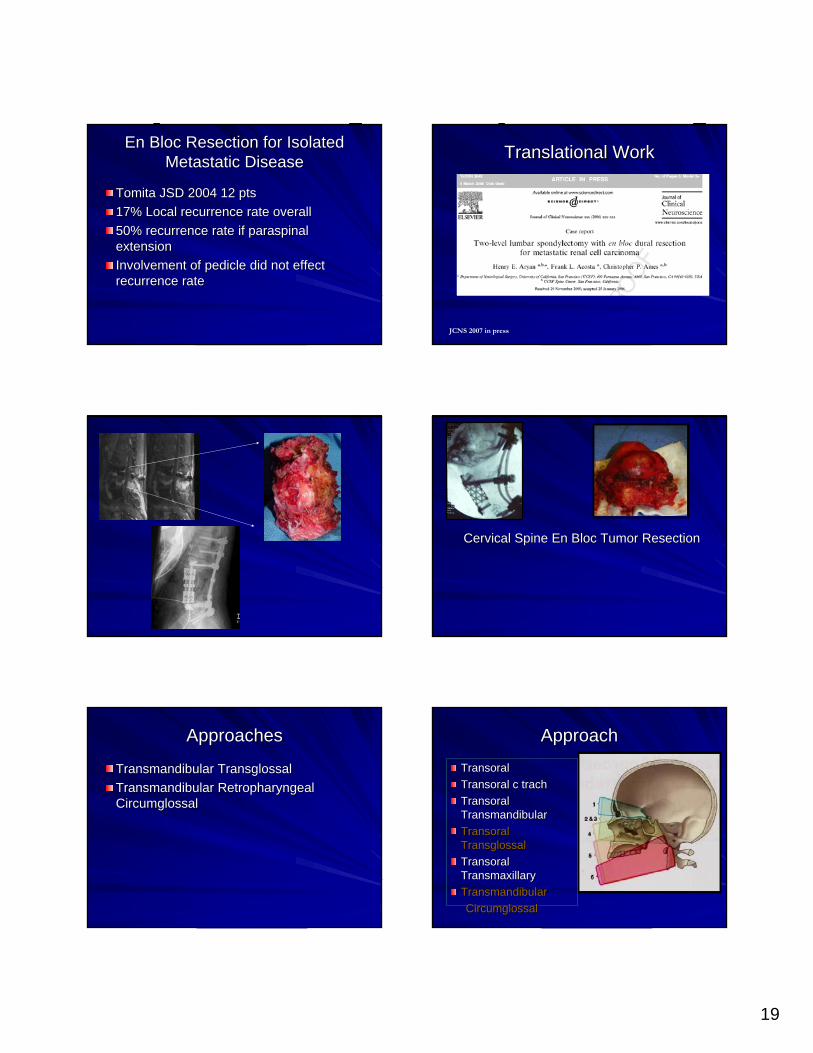
En Bloc Resection for Isolated En Bloc Resection for Isolated MetastaticMetastatic DiseaseDisease
Tomita JSD 2004 12 ptsTomita JSD 2004 12 pts17% Local recurrence rate overall17% Local recurrence rate overall50% recurrence rate if 50% recurrence rate if paraspinalparaspinalextensionextensionInvolvement of pedicle did not effect Involvement of pedicle did not effect recurrence raterecurrence rate
Translational WorkTranslational Work
JCNS 2007 in press
Cervical Spine En Bloc Tumor ResectionCervical Spine En Bloc Tumor Resection
ApproachesApproaches
TransmandibularTransmandibular TransglossalTransglossalTransmandibularTransmandibular Retropharyngeal Retropharyngeal CircumglossalCircumglossal
ApproachApproach
TransoralTransoralTransoralTransoral c c trachtrachTransoralTransoralTransmandibularTransmandibularTransoralTransoralTransglossalTransglossalTransoralTransoralTransmaxillaryTransmaxillaryTransmandibularTransmandibularCircumglossalCircumglossal
20
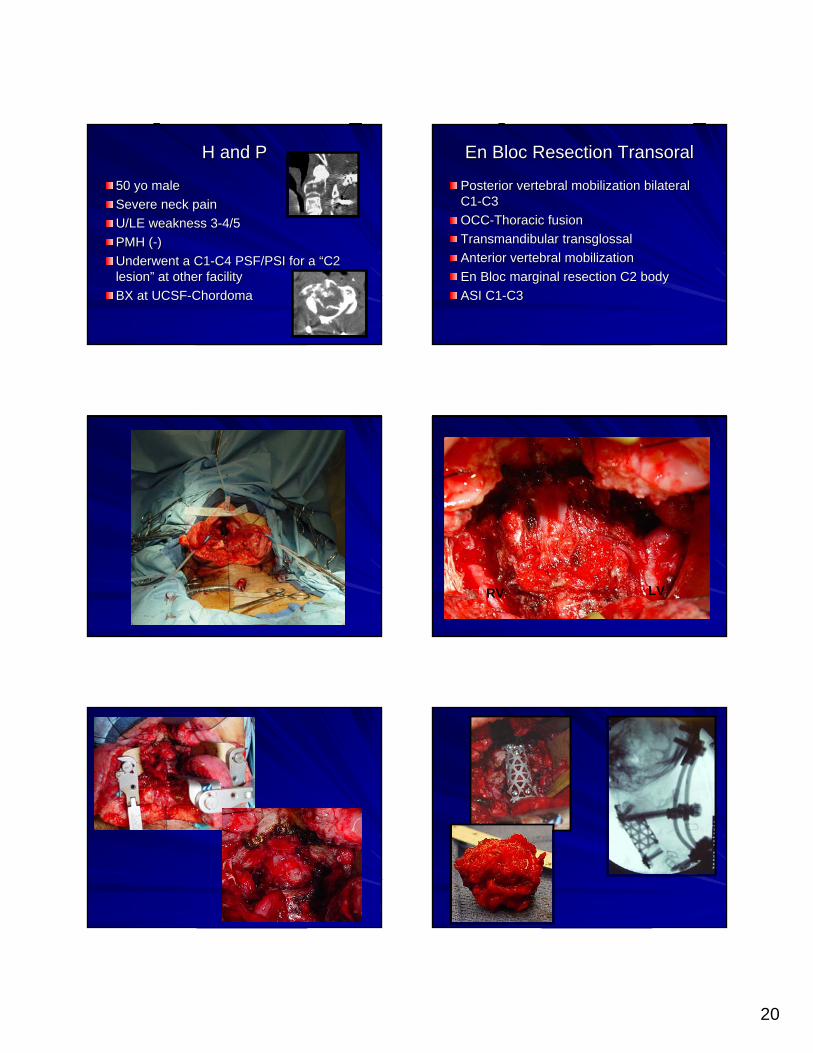
H and PH and P
50 50 yoyo malemaleSevere neck painSevere neck painU/LE weakness 3U/LE weakness 3--4/54/5PMH (PMH (--))Underwent a C1Underwent a C1--C4 PSF/PSI for a C4 PSF/PSI for a ““C2 C2 lesionlesion”” at other facilityat other facilityBX at UCSFBX at UCSF--ChordomaChordoma
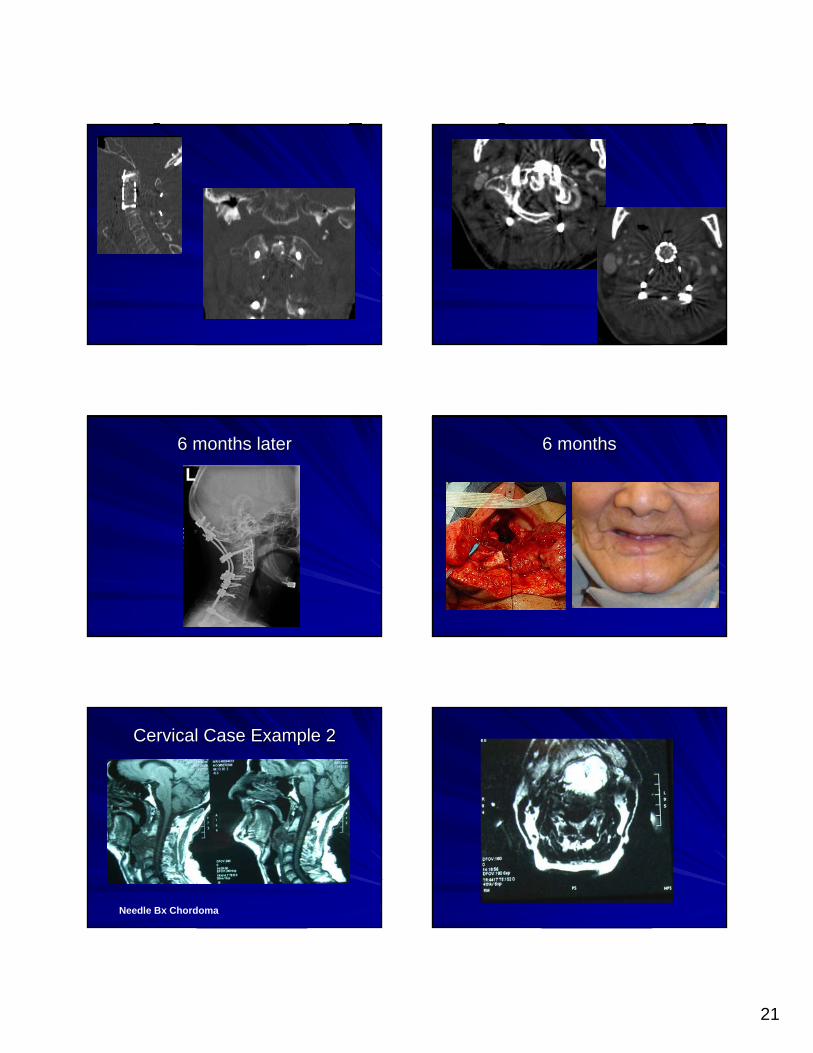
En Bloc Resection En Bloc Resection TransoralTransoral
Posterior vertebral mobilization bilateral Posterior vertebral mobilization bilateral C1C1--C3C3OCCOCC--Thoracic fusionThoracic fusionTransmandibularTransmandibular transglossaltransglossalAnterior vertebral mobilizationAnterior vertebral mobilizationEn Bloc marginal resection C2 bodyEn Bloc marginal resection C2 bodyASI C1ASI C1--C3C3
RV LV
21
6 months later6 months later 6 months6 months
Cervical Case Example 2Cervical Case Example 2
Needle Bx Chordoma

22
TransmandibularTransmandibular CircumglossalCircumglossal Posterior L Vertebral Artery Posterior L Vertebral Artery Occlusion/R Vertebral MobilizationOcclusion/R Vertebral Mobilization

23
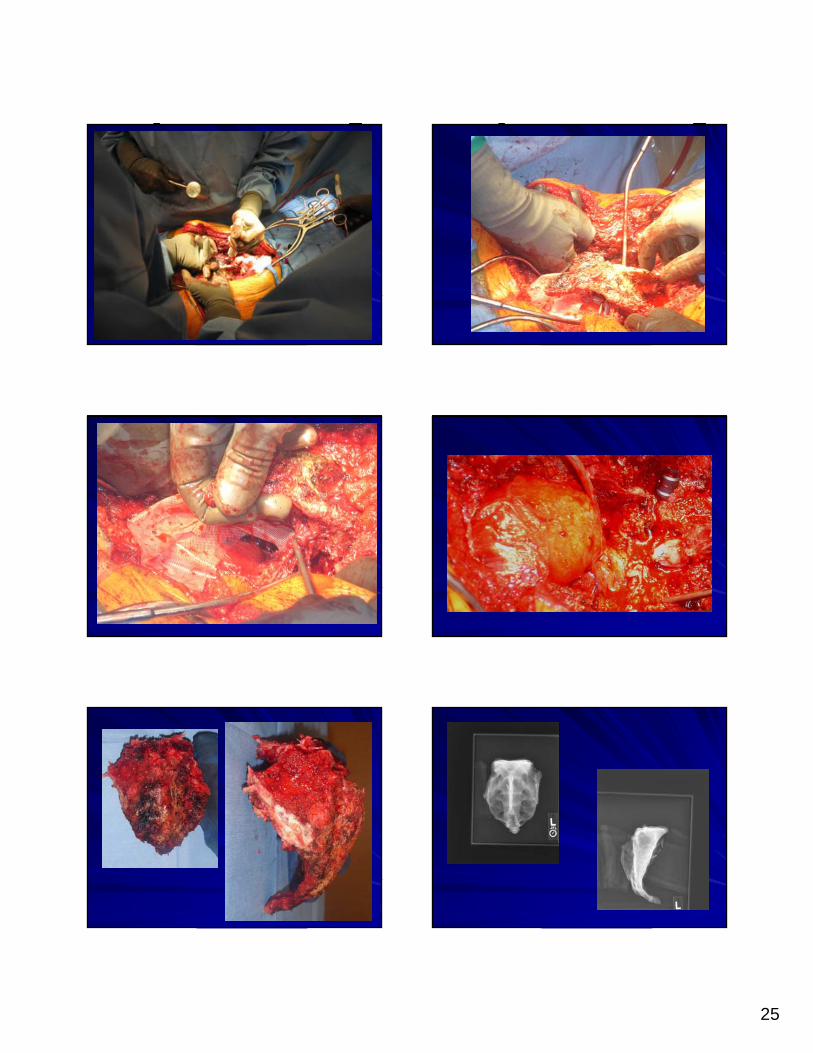
En Bloc En Bloc SacrectomySacrectomy--Technique Technique EvolutionEvolution
Anterior StageAnterior Stage--no no osteotomyosteotomy--just just DiscectomyDiscectomy L5L5--S1, nerve mobilization, S1, nerve mobilization, sacrifice and protection, sacrifice and protection, silasticsilastic sheetsheet
PosteriorPosterior--no no transiliactransiliac bar, anchoring of bar, anchoring of femur into pelvis with AO screws, BMPfemur into pelvis with AO screws, BMP--22
H and PH and P
63 63 yoyo male with sacral pain and left leg male with sacral pain and left leg painpainNeuroNeuro examexam–– Bilateral S1 4/5Bilateral S1 4/5–– Decreased Decreased perinealperineal sensationsensation
Sacral Sacral ChordomaChordoma

24
Original Resection TechniqueOriginal Resection Technique
25

26
ReconstructionReconstruction
GokaslanGokaslan TechniqueTechnique
ISSLS Prize 2005ISSLS Prize 2005
Radiated 14 days after surgery –BMP-2
Advances in challenging Advances in challenging reconstructionsreconstructions
6 level corpectomy
BMP-2
27
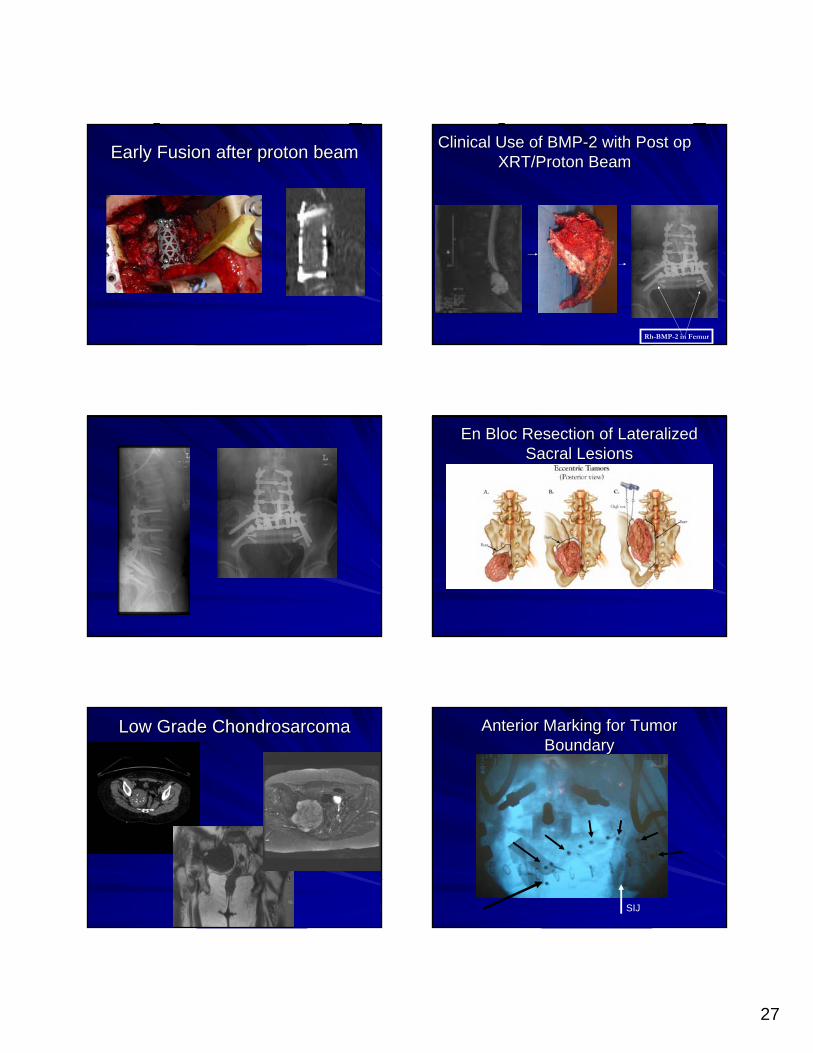
Early Fusion after proton beamEarly Fusion after proton beam Clinical Use of BMPClinical Use of BMP--2 with Post op 2 with Post op XRT/Proton BeamXRT/Proton Beam
Rh-BMP-2 in Femur
En Bloc Resection of Lateralized En Bloc Resection of Lateralized Sacral LesionsSacral Lesions
Low Grade Low Grade ChondrosarcomaChondrosarcoma Anterior Marking for Tumor Anterior Marking for Tumor BoundaryBoundary
SIJ
28
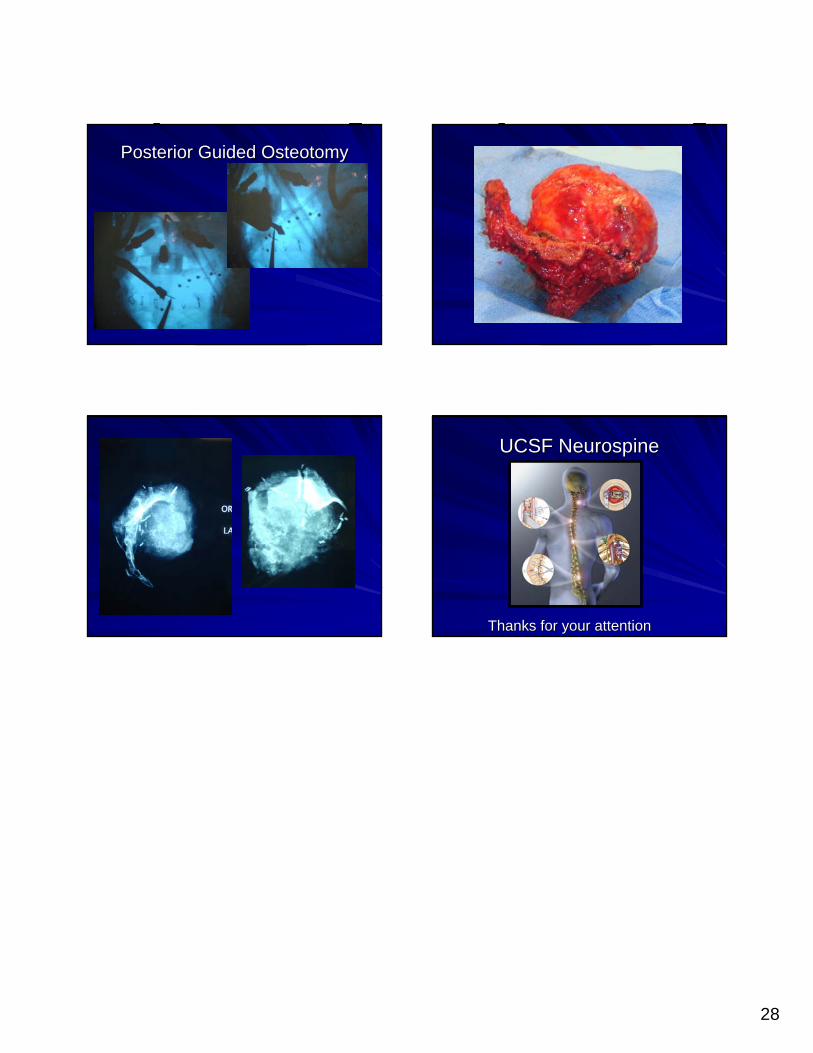
Posterior Guided Posterior Guided OsteotomyOsteotomy
UCSF UCSF NeurospineNeurospine
Thanks for your attentionThanks for your attention