Embed Size (px)
Citation preview

Sleep:The Golden Chain That Ties
Health and Our Bodies Together(A Review of Sleep Disorders)
Academy Of Medicine Clinical Day, February 24, 2012Elliott K. Lee MD, FRCP(C), D. ABPN, D. ABPN Addiction Psychiatry, D. ABSM
Assistant Professor, University of Ottawa Faculty of MedicineSleep Specialist, Royal Ottawa Mental Health Center Sleep
Disorders Clinic

Objectives
Describe the importance of sleep and impact of sleep disorders in the community.
Understand common sleep disorders and how they can be assessed and treated.

Outline
Review sleep architecture, and how sleep is controlled.
Review insomnia and excessive daytime sleepiness, and their causes

SLEEP
NREM Sleep
Stage N1, N2 (“Light sleep”)
procedural memory (skills, motor learning)
Stage N3 Deep or “Slow Wave
Sleep” (SWS)
CNS restorationDeclarative memory
REM Sleep
DreamingMood Regulatory Role?
Memory?

Sleep Hypnogram

Insomnia Excessive Daytime Sleepiness

Insomnia
Affects 3.3 million Canadians (1/7) according to Statistics Canada (2002)
Especially:- Middle aged (45-64)- Widowed- Minimal education- Obese- Women > men

Treating Insomnia:Personal Sleep Hygiene
Maintain a regular wake/sleep schedule, possibly add mild sleep restriction.
Refrain from taking naps. Exercise - but not within 3 hours of bedtime. Establish a relaxing routine before bedtime. Use the bedroom only for sleep activities. Avoid clock watching Set environment (light, noise, temperature)
at comfortable levels. Avoid caffeine after mid-afternoon.

Medication options
Zopiclone (Imovane)Trazodone (Desyrel)Other options:
- Melatonin- Tricyclic Antidepressants- Benzodiazepines- Mirtazapine (Remeron)- Atypical Antipsychotics

Eszopiclone
Sleep latency from ave = 70 minPlacebo = 45 minEszopiclone = 27.3 min
Total Sleep TimePlacebo = 330 minEszopiclone = 390 min
Eszopiclone users had improved quality of life, and no reported incidence of tolerance or withdrawal
Sleep Latency
Total Sleep Time
Walsh et al, Sleep, 2007

Obstructive Sleep Apnea (OSA) Pauses in breathing > 10 seconds in length Respiratory Disturbance Index (RDI): >5 hr =
significant Prevalence – up to 25% of men, and 9% of women Key diagnostic questions:
- Do you feel satisfied with the quality of your sleep?- Does your partner complain that you snore?

Obstructive Sleep Apnea Syndrome Symptoms
Snoring >80%*up to ½ of pts may sleep separately from partners
Apneic episodes (partner) 75%AM Dry Mouth 74%Restless Sleep/ AM H/A 50%Sensation of choking 18-
31%Nighttime bathroom visits 28%Kryger, Roth and Dement, Principles and
Practice of Sleep Medicine, 2005 p. 1043

OBSTRUCTIVE SLEEP APNEA (OSA)
Causes ▪ Narrow Upper Airway ▪ Elevated BMI ▪ Family Hx
Exacerbated by: ▪ Medications – muscle relaxants,
sedatives ▪ Alcohol Consumption
▪ Supine sleep ▪ REM sleep ▪ **Supine + REM sleep


Consequences of OSA

Odds Ratio – AHI to Hypertension
Peppard PE et al. N Eng J Med, 2000; 342(19): 1378-84

Odds Ratio – AHI to Hypertension
Peppard PE et al. N Eng J Med, 2000; 342(19): 1378-84
Change in BP with use of CPAP (9 weeks)
Becker HF et al. Circulation, 2003; 107(1):68-73

Traditional View
Obesity
Insulin Resistance
Low Grade Inflammation
↑ Oxidative Stress
Endothelial Dysfunction
Hypertension
Ischemic heart diseases
Arrhythmias
CV stroke/TIA
CardiovascularDisease

Atherosclerosis and Hypoxemia?Savransky and colleagues studied mice
– divided into 4 groups:
Intermittent Air (Control)
10
10
Chronic Intermittent Hypoxemia
10
10
Regular diet
High Cholesterol
diet
*Savransky V et al Am J Respir Crit Care Med, 2007

Atherosclerosis and Hypoxemia?Which ones developed atherosclerosis?
Intermittent Air (Control)
Chronic Intermittent Hypoxemia
Regular diet
High Cholesterol
diet
0
0
0
9
*Savransky V et al Am J Respir Crit Care Med, 2007

Atherosclerosis and Hypoxemia?Sections of aorta from the mice:
Intermittent Air (Control)
Chronic Intermittent Hypoxemia
Regular diet
High Cholesterol
diet
*Savransky V et al Am J Respir Crit Care Med, 2007
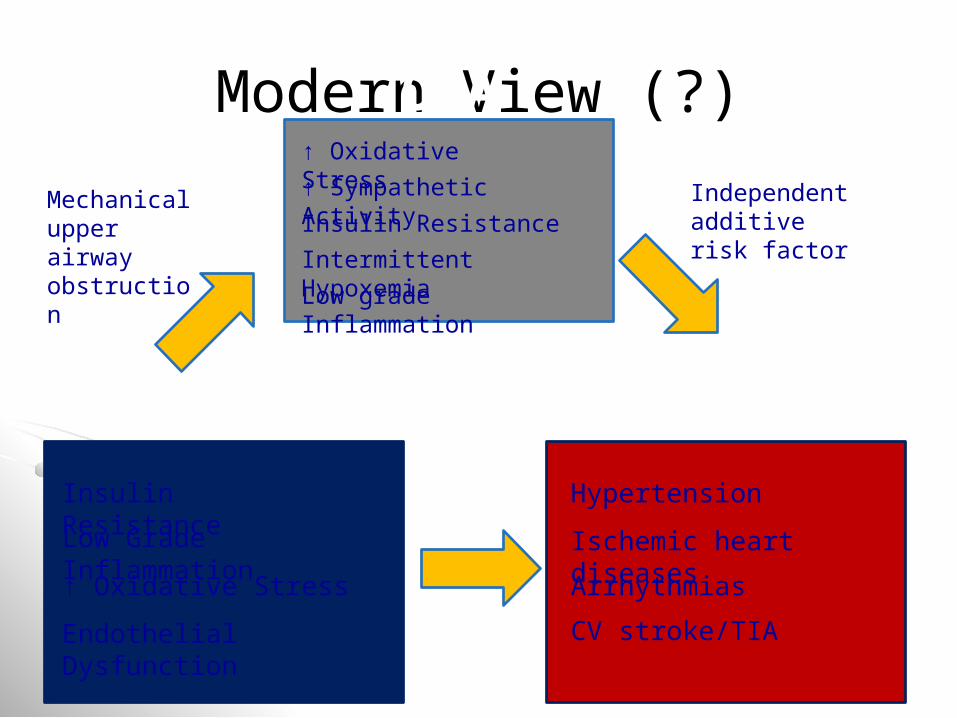
Modern View (?)
Obesity
Insulin Resistance
Low Grade Inflammation
↑ Oxidative Stress
Endothelial Dysfunction
Hypertension
Ischemic heart diseases
Arrhythmias
CV stroke/TIA
CardiovascularDisease
Mechanical upper airway obstruction
↑ Oxidative Stress
↑ Sympathetic Activity
Insulin Resistance
Intermittent Hypoxemia
Low grade Inflammation
Independent additive risk factor
OSA

MonthsMarin JM et al. Lancet, 2005
Fatal CV events and OSA

Nonfatal CV events and OSAMarin JM et al. Lancet, 2005
Sleep and Mental Illness
OSA can exacerbate mental illness:- Aggression /cognition in schizophrenia- Depression- Nightmares in PTSD- Cognitive dysfunction in dementias- Relapse to substance abuse
Sleep Psychiatricillness
Lee EK and Douglass AB. Can J Psychiatry, 2010; 55(7): 403-12

TREATMENTS FOR OSA
**CPAP – Continuous Positive Airway Pressure **Weight Loss - ↓ BMI = ↓ RDI Avoid Alcohol Consumption Avoid Sedative Medications “Snoreball” Technique / Positional Therapy Oral Appliance Upper Airway Surgery
Tonsillectomy (pediatrics) Uvulopalatopharyngoplasty (UPPP) Maxillomandibular advancement Tracheostomy

CPAP for OSA

Stage 4Stage 3Stage 2Stage 1
REMWake
Movement
23:00 00:00 01:00 02:00 03:00 04:00 05:00 06:00
STAG
ING
60
80
100
23:00 00:00 01:00 02:00 03:00 04:00 05:00 06:00
OXI
MET
RY
0
10
20
23:00 00:00 01:00 02:00 03:00 04:00 05:00 06:00
CPAP

Alcohol on Breathing
Issa and Sullivan, J Neurol Neurosurg Psychiatr, 1982; 45:353-9
Snoring (baseline)
Snoring, 2nd night, drank EtOH 6-9 PM, about 8-10 drinks
53 yr old male, “social drinker”

Oral Appliances
Silencer-
Johns Dental Labs
Klearway-
Great Lakes Orthodontics

Surgery (UPPP)

Restless Legs Syndrome

Restless Legs Syndrome
NB- symptoms WHILE AWAKE“URGE”
U – rge to move legs
R – est – symptoms worsened at rest
G – ets better with movement
E – vening – symptoms worse in evening
Often associated with periodic limb movements (PLMs), WHILE ASLEEP
Epidemiology – RLS
Affects 5-15% of the population Mean age – 27- 41 years old
- prevalence increases with age- age of onset varies widely
(children – elderly)Up to 2.5X more common in women

Restless Leg Syndrome + PLMD
Thought to be related to same problem – dopamine deficiency in the brain
May be exacerbated by caffeine, nicotine, alcohol, or iron deficiency
Mainstay of treatment- Dopamine replacement therapy
- levodopa, pramipexole, ropinirole- Other meds may also help
- neurontin, benzodiazepines, opioids

Narcolepsy
A pathologic disorder of sleepiness during the day – key symptom – sleepiness
May have insomnia at nighttimeAffects about 1/2000 peopleVery underdiagnosed; difficult to recognize80% may have cataplexy, a REM sleep
intrusion phenomenon on wakefulnessRelated to cerebrospinal fluid deficiency of
hypocretin (orexin)
Narcolepsy Treatment
SLEEPINESS: – Stimulants
d-amphetamine (Dexedrine), methylphenidate (Ritalin)
Novel - modafinil (Alertec / Provigil).- armodafinil
CATAPLEXY:– Antidepressants – e.g. venlafaxine– Sodium oxybate (Xyrem)

Summary
Sleep has a distinct architecture and is normally regulated by a complex set of environmental, biological and social influences
Insomnia and excessive daytime sleepiness are common issues among patients
If sleep is problematic, assessment for an underlying sleep disorder such as obstructive sleep apnea, restless legs syndrome, narcolepsy or others is important, as effective treatments are available for these conditions

Screening Questions For Symptoms Of Poor Sleep
Do you feel satisfied with the quality of your sleep?
Does you partner complain about your sleep?
Do you have difficulties falling or staying asleep?
Do you have problems with sleepiness during the day?
![Sleep and Sleep Disorders by RaeAnnon Fairlie [Sleep is] the golden chain that ties health and our bodies together. Thomas Dekker Thomas Dekker English](https://img.pdfslide.net/doc/110x75/55181dff55034684678b476e/sleep-and-sleep-disorders-by-raeannon-fairlie-sleep-is-the-golden-chain-that-ties-health-and-our-bodies-together-thomas-dekker-thomas-dekker-english.jpg)











![ROBERT JAMES ELLIOTT CURRICULUM VITAE CITIZENSHIP ...haskayne.ucalgary.ca/.../robert-elliott-cv.pdf · R.J. Elliott – CV [September, 2006 - Page 1] ROBERT JAMES ELLIOTT CURRICULUM](https://img.pdfslide.net/doc/110x75/5fdc51cfa239fb15507e657b/robert-james-elliott-curriculum-vitae-citizenship-rj-elliott-a-cv-september.jpg)
















