Embed Size (px)
Citation preview
Sleeve En YDoes Changing the Name Change the Perception?
Mitchell Roslin, MD FACS
Chief of Bariatric Surgery
Lenox Hill Hospital
Northern Westchester Hospital Center
Disclosures
• Consultant J&J, Covidien, CR Bard• Research Grant Covidien• Patent License J&J, CR Bard, Allergan• SAB ValenTx, Scientific Intake• Founder VentralFix

• Gastric bypass has been most popular stapling procedure
• Best balance between outcome and complications?
• Preferable for sweet eaters because of dumping?• Dumping is an important component for weight
loss surgery as it deters carbohydrate intake?• Tremendous amount of long term data?
“A person with a new idea is a crank until the idea succeeds.”
Mark Twain • Described RYGB• Abandoned anemia, bone
loss, micronutrient deficiencies
• 1971 VBG• Lesser curvature• 2005 International
Registry• RYGB 67 vs 59 %EBL• VBG 0 mortality vs .5%
Edward E Mason MD, PHD

Harvey SUGERman• Compared VBG to
RYGB in sweet eaters• Big difference in
outcome 37% EBL VBG• What is a sweet eater?• 69% vs 67% wt loss in
sweet eaters vs non in rygb
• Dumping caused sweet aversion?
Ann Surg 1987
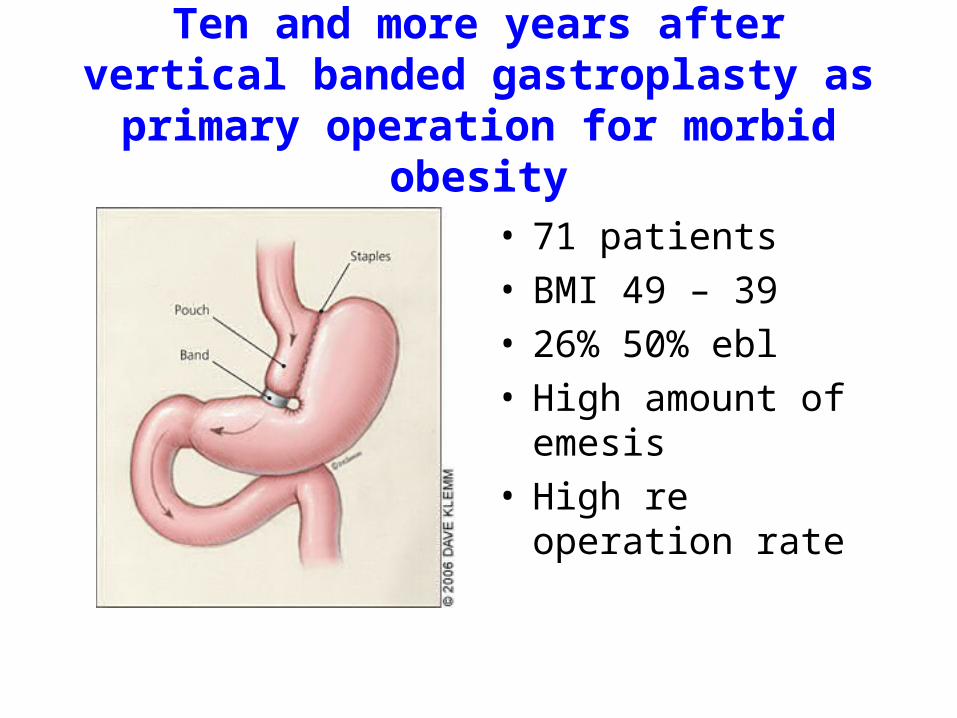
Ten and more years after vertical banded gastroplasty as primary operation for
morbid obesity
• 71 patients• BMI 49 – 39• 26% 50% ebl• High amount of
emesis• High re operation rate
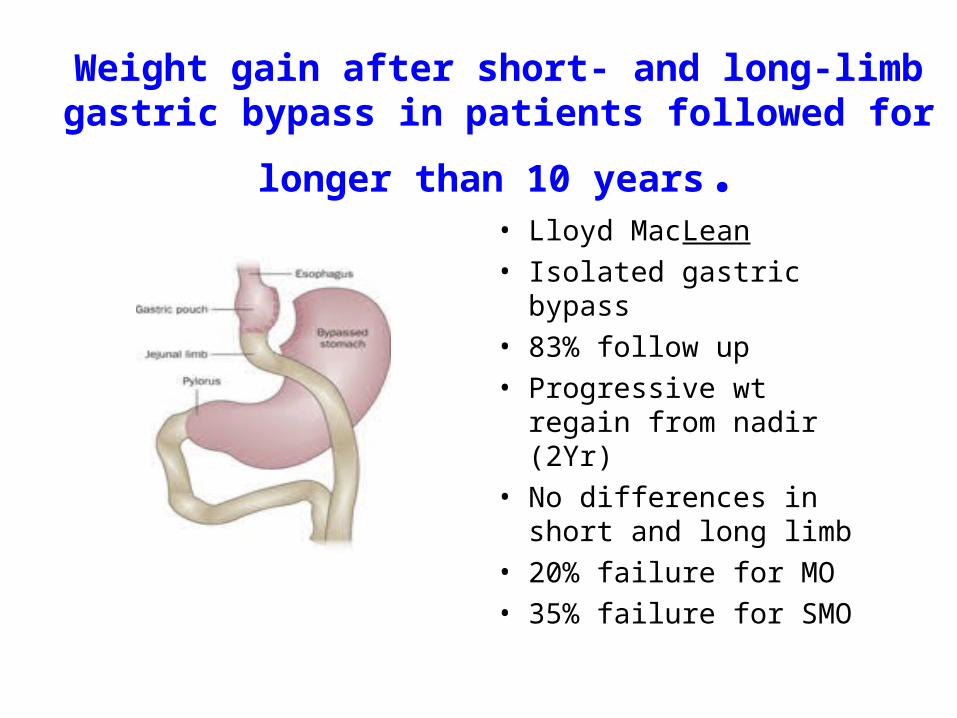
Weight gain after short- and long-limb gastric bypass in
patients followed for longer than 10 years.• Lloyd MacLean
• Isolated gastric bypass
• 83% follow up
• Progressive wt regain from nadir (2Yr)
• No differences in short and long limb
• 20% failure for MO
• 35% failure for SMO
Dumping?
• Literature contains numerous articles about hyperinsulinemic hypoglycemia
• None showing relationship between dumping and weight loss
• Mallory et al: No relationship between wt loss and dumping
OBESITY IS A CHRONIC DISEASE
• 70% of excess weight loss after one year• Much higher rate of recidivism than noted


Size does not Matter?
• In cohort that had dgj>2cm, no difference with increasing size
• Time matters• Will be difficult to
identify clinical target that is reproducible
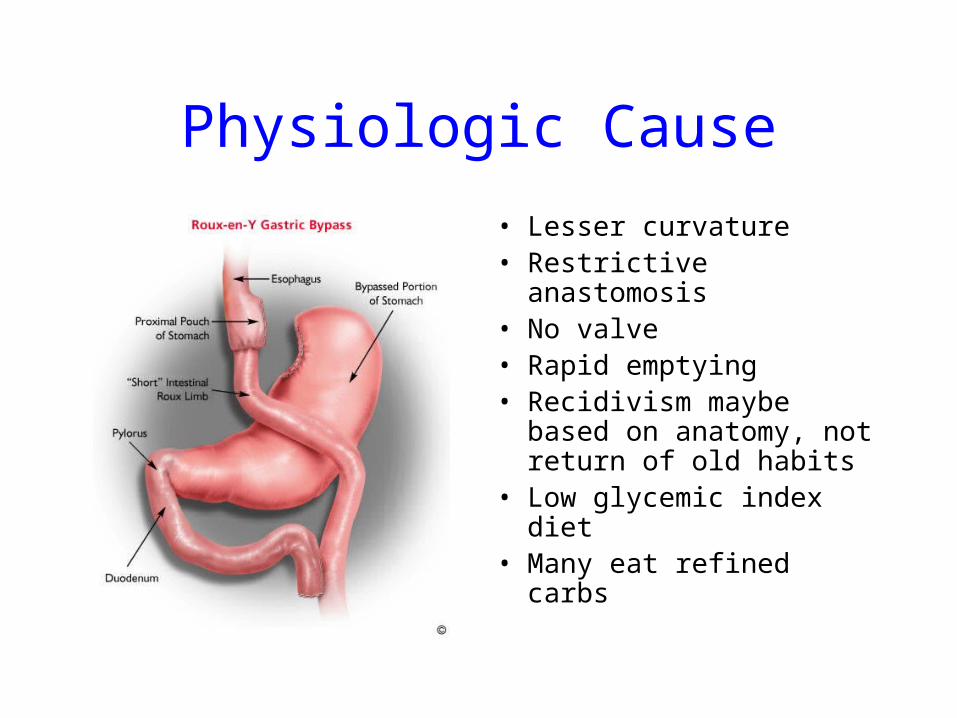
Physiologic Cause
• Lesser curvature• Restrictive anastomosis• No valve• Rapid emptying• Recidivism maybe based
on anatomy, not return of old habits
• Low glycemic index diet• Many eat refined carbs
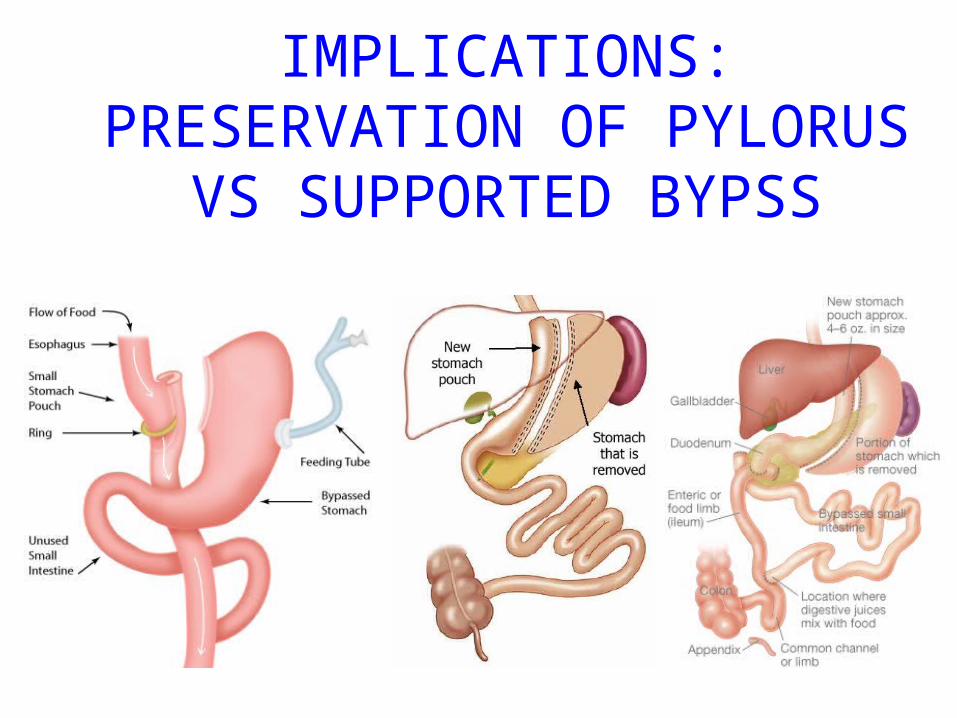
IMPLICATIONS:PRESERVATION OF PYLORUS
VS SUPPORTED BYPSS
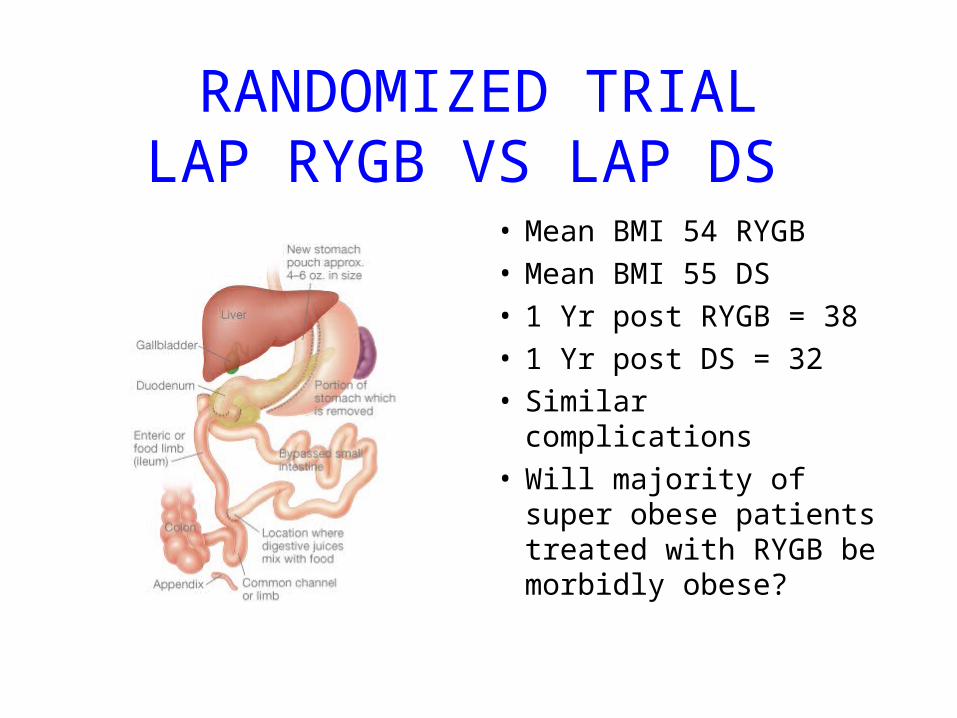
RANDOMIZED TRIALLAP RYGB VS LAP DS
• Mean BMI 54 RYGB• Mean BMI 55 DS• 1 Yr post RYGB = 38• 1 Yr post DS = 32• Similar complications• Will majority of super
obese patients treated with RYGB be morbidly obese?
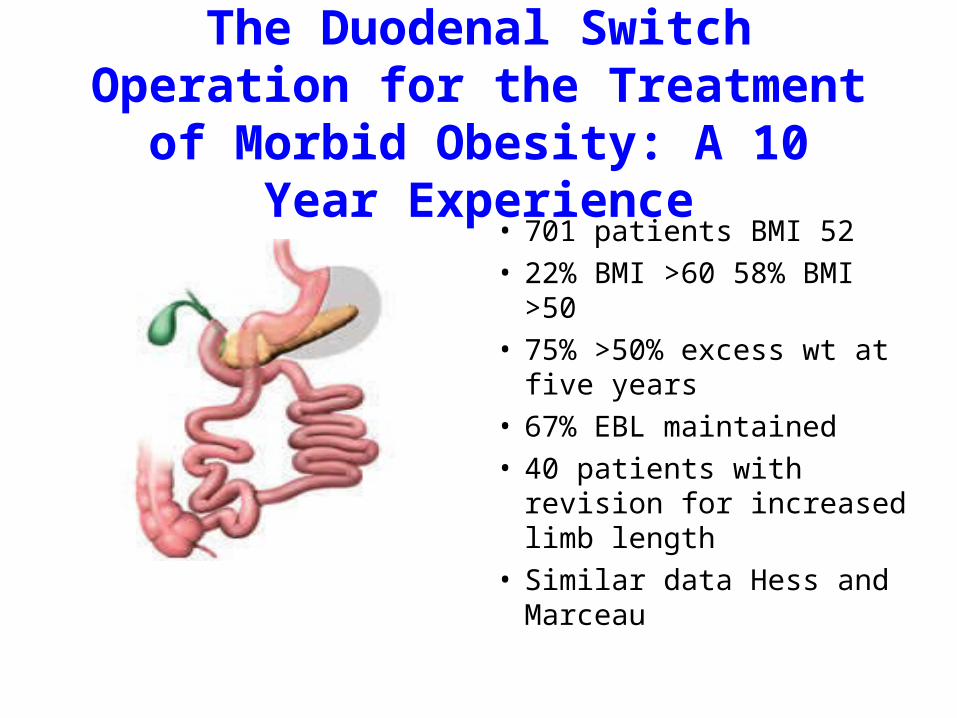
The Duodenal Switch Operation for the Treatment of Morbid Obesity: A
10 Year Experience• 701 patients BMI 52• 22% BMI >60 58% BMI >50• 75% >50% excess wt at five
years• 67% EBL maintained• 40 patients with revision for
increased limb length• Similar data Hess and
Marceau
Pyloric Preservation?
• Bypass with rapid emptying causing inter meal hunger
• Instead of artificial fixed valve use biologic smart valve
• Duodenal Switch has most weight loss
• Sleeve preserves options
Introducing the Sleeve En Y
• Effectiveness of sleeve shows the value of long narrow pouch with pylorus intact
• Combination of narrow pouch and pylorus limit intake and diarrhea
• Intestinal bypass plays metabolic role
• Can lengthen common channel to avoid oily stools and frequent bowel movements
Responder Analysis• BMI > 50 Nadir response > 1 year
• 50% EWL, BMI < 40, BMI < 35, BMI <30
• 13/120 Bands less than 40
• 270 of 346 RYGB less than 40
• 10 of 30 VSG
• 22 of 23 lap DS (majority have not reached nadir
• Lowest variability in response
• Does treatment of super morbid obesity require intestinal bypass?



![Essay: Roslin, M & Mme de Fries · Alexander Roslin, M. & Mme de Fries. NEIL JEFFARES . Alexander Roslin. ... writing the same day: 4 “toute la noblesse est portée pour [Roslin]](https://img.pdfslide.net/doc/110x75/5e6dfe6691c4c251d85ad7fa/essay-roslin-m-mme-de-alexander-roslin-m-mme-de-fries-neil-jeffares.jpg)