Embed Size (px)
Citation preview

11/1/2019
1
Small Cell Lung CancerJoel Michalski MD PHD
Medical Oncology
Nebraska Cancer Specialists
Disclosures
• Grant/Research Support: NA
• Speaker’s Bureau: NA
• Consultant: NA
• Major Shareholder: NA
• Other: NA

11/1/2019
2
Outline
• Objectives
• Case
• Small cell lung cancer
• Presentation
• Risk factors
• Treatment
• Future
• Summary
• Comments and questions
Objectives
• By the end of this discussion, the audience will
• Be able to appreciate the major risk features for small cell lung cancer (SCLC)
• Understand the presentation of (SCLC)
• Appreciate the multi-speciality collaboration required to adequately treat SCLC
• Understand the current state of systemic therapy for SCLC

11/1/2019
3
Let’s start with a case…
• 60-ish white male
• Presented to urgent care 3 times with left arm weakness and pain
• Contact 1: MSK injury->symptomatic care
• Contact 2: 1 week later: referral to PT
• Contact 3: 1 week later: noticed pupil asymmetry -> ED
Let’s start with a case…
• 60-ish white male
• Presented to urgent care 3 times with left arm weakness and pain
• Contact 1: MSK injury->symptomatic care
• Contact 2; 1 week later: referral to PT
• Contact 3; 1 week later: noticed pupil asymmetry -> ED
• ED->concern for stroke->brain MRI and CTA head and neck
• No stroke, but large infiltrative mass invading the left brachial plexus
• Onc consult:

11/1/2019
4
Let’s start with a case…
• 60-ish white male
• Presented to urgent care 3 times with left arm weakness and pain
• Contact 1: MSK injury->symptomatic care
• Contact 2; 1 week later: referral to PT
• Contact 3; 1 week later: noticed pupil asymmetry -> ED
• ED->concern for stroke->brain MRI and CTA head and neck
• No stroke, but large infiltrative mass invading the left brachial plexus
• Onc consult: Exam: Large chest wall mass, nicotine patch
Let’s start with a case…
• 60-ish white male
• Presented to urgent care 3 times with left arm weakness and pain
• Contact 1: MSK injury->symptomatic care
• Contact 2; 1 week later: referral to PT
• Contact 3; 1 week later: noticed pupil asymmetry -> ED
• ED->concern for stroke->brain MRI and CTA head and neck
• No stroke, but large infiltrative mass invading the left brachial plexus
• Onc consult: Large chest wall mass, nicotine patch
• Biopsy->SCLC

11/1/2019
5
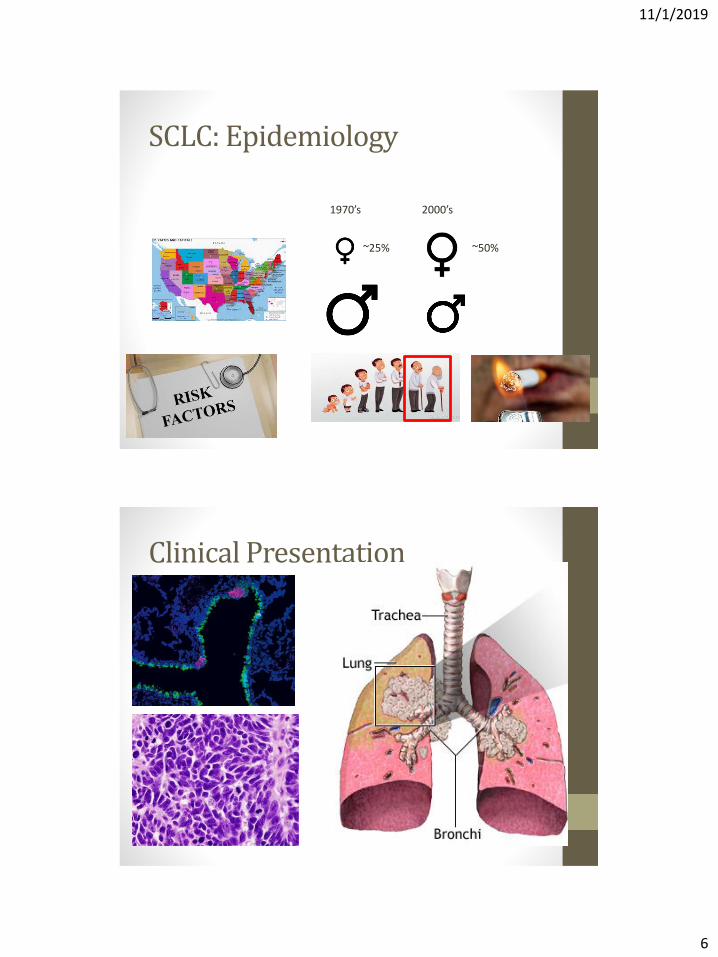
SCLC: Epidemiology
Incidence 200k/year New cases 2019: ~30,000
SCLC: Epidemiology
1970’s
~25%
2000’s
~50%
11/1/2019
6
SCLC: Epidemiology
1970’s 2000’s
~25% ~50%
Clinical Presentation

11/1/2019
7
Clinical Presentation

11/1/2019
8
Staging: body imaging
• Brain MRI
• Combined staging system
• AJCC TNM system
• VA Lung Study Groups 2-stage system:
Staging: body imaging
• Brain MRI
• Combined staging system
• AJCC TNM system
• VA Lung Study Groups 2-stage system:• Limited Stage

11/1/2019
9
Staging:
• Brain MRI
• Combined staging system
• AJCC TNM system
• VA Lung Study Groups 2-stage system:• Limited Stage
Staging:
• Brain MRI
• Combined staging system
• AJCC TNM system
• VA Lung Study Groups 2-stage system:• Limited Stage
• Extensive Stage

11/1/2019
10
Treatment
• Regardless of stage, systemic therapy plays a role
• Multi-speciality evaluation
• Limited stage: Mediastinal LN eval negative
• Surgery candidate: T1-2 with pN0->lobectomy
• pN0 confirmed->systemic therapy
• pN1/2->RT plus systemic therapy
• Poor surgical candidate:
• SABR->systemic therapy or,
• Concurrent systemic therapy and RT
Treatment
• Regardless of stage, systemic therapy plays a role
• Multispeciality evaluation
• Limited stage: Mediastinal LN eval Positive
• T3-T4, N0; or T1-4, N1-3: systemic therapy + RT

11/1/2019
11
Systemic therapy
CisplatinEtoposide
1980’s 2006-7 2018
Irinotecan/Cis?Topotecan
Immunotherapy
At least 40 phase III clinical trials, largely negative
Immunotherapy and SCLC
• Mixed results, in general…
• ES-SCLC, front line: IMPOWER-133 trial:
https://www.lungcancernews.org/2019/02/26/impower133-finally-moving-the-needle-in-sclc/

11/1/2019
12
NEJM 12/6/2018; 379:2220-2229
NEJM 12/6/2018; 379:2220-2229

11/1/2019
13
Immunotherapy and SCLC
• Mixed results, in general…
• ES-SCLC, front line: IMPOWER-133 trial: Positive
• ES-SCLC, frontline: NCT01450761
954 pts 1:1-Chemo-Chemo+Ipi
Immunotherapy and SCLC
• Mixed results, in general…
• ES-SCLC, front line: IMPOWER-133 trial: Positive
• ES-SCLC, frontline: NCT01450761: Negative

11/1/2019
14
Immunotherapy and SCLC
• Mixed results, in general…
• ES-SCLC, front line: IMPOWER-133 trial: Positive
• ES-SCLC, frontline: NCT01450761: Negative
• ES-SCLC, pembrolizumab maintenance: negative (phase II)
Immunotherapy and SCLC
• Mixed results, in general…
• ES-SCLC, front line: IMPOWER-133 trial: Positive
• ES-SCLC, frontline: NCT01450761: Negative
• ES-SCLC, pembrolizumab maintenance: negative (phase II)
• ES-SCLC, CASPIAN Trial: Positive
• EP
• EP+durvalumab followed by 1 year of durvalumab
• EP+durvalumab+tremelimumab+durvalumab followed by 1 year of durvalumab
• OS improved (mOS 13.0 months in DEP vs 10.3 mos in the EP)
• Tremelimumab data is not mature

11/1/2019
15
Immunotherapy and SCLC
• Mixed results, in general…
• ES-SCLC, front line: IMPOWER-133 trial: Positive
• ES-SCLC, frontline: NCT01450761: Negative
• ES-SCLC, pembrolizumab maintenance: negative (phase II)
• ES-SCLC, CASPIAN Trial: Positive
• ES-SCLC, ipi+nivo maintenance: CheckMate-451: Negative (phase III, unpublished)
On the horizon…
• Immunotherapy:
• PD-1 inhibitor: 12 trials
• PD-L1 inhibitor: 6 trials
• CTLA-4+PD-1/L1 inhibitors: 7 trials
• Other (CD47, JAK1, etc): 5 trials
• Cell cycle modulators/inhibitors: 6 trials
• Stem cell pathways: 6 trials
• Epigenetics: 3 trials
• DNA damage repair: 8 trials
• Others: 13 trials

11/1/2019
16
Case update
• Patient was staged
• T4: extensive soft tissue involvement, 8cm mass with mediastinal invasion
• M1a: separate pleural nodule in the same hemithorax
• AJCC=IVa
• VA-LSG=Extensive stage
• Started on Carboplatin, Etoposide, atezolizumab per IMPOWER 133
• Palliative RT to brachial plexus
• Presented for Cycle 2:
• Horner’s syndrome: stable
• Pain: improved
• Weakness: stable
• Chest wall mass: barely appreciable
• Constitutional: increasing wt, more active
Summary
• SCLC is
• Rare: 10-15% of lung cancers
• Aggressive:
• Two thirds of pts have extra-thoracic disease at diagnosis
• Median OS is ~10-12 months from diagnosis
• Associated with several paraneoplastic syndromes
• Heavily investigated, with frustrating resistance to many classes of therapeutics
• 40 years of research->5 new drugs approved (pembrolizumab, atezolizumab, nivolumab+/- ipilimumab, topotecan)
• Systemic therapy is indicated in all circumstances
• Chemotherapy is the backbone of systemic therapy; platinum+etoposide
• Immunotherapy has a role in relapse and upfront; marginal benefit

11/1/2019
17
Thanks for your attention!
• Questions?







![Establishment and Identification of Small Cell Lung Cancer Cell … · [CANCER RESEARCH 45, 2913-2923, June 1985] Establishment and Identification of Small Cell Lung Cancer Cell Lines](https://img.pdfslide.net/doc/110x75/60347fa5d25195593e3efdb8/establishment-and-identification-of-small-cell-lung-cancer-cell-cancer-research.jpg)