Embed Size (px)
Citation preview
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 3
SMOKE INHALATION &HYDROGEN CYANIDE POISONING
The Danger Posed to Firefighters & Victims in Structure Fires
CONTENTS
6Hydrogen cyanide poisoning proves increasinglycommon in smoke-inhalation victimsBY RICHARD ALCORTA, MD, FACEP
Smoke Inhalation & Acute Cyanide Poisoning
5Fire smoke’s silent killerBY KEN RIDDLE, DEPUTY CHIEF FIRE MARSHAL
18Meeting the needs of fire victimsBY JEAN-LUC FORTIN, MD, M. RUTTIMAN, MD,L. DOMANSKI, MD, & J.J. KOWALSKI, MD
Hydroxocobalamin:Treatment for Smoke
Inhalation-Associated Cyanide Poisoning
22BY MARC ECKSTEIN, MD, FACEP
Cyanide as a ChemicalTerrorism Weapon
SMOKE INHALATION & HYDROGEN CYANIDE POISONING
A Jems Communications SupplementSponsored by EMD Pharmaceuticals
Publisher/General Manager Jeff Berend
Senior Editor Keri Losavio
Supplement Editor Jennifer Doyle
Supplement Art Director Daniel DiPinto
Production Manager Tim Francis
Smoke Inhalation & Hydrogen Cyanide Poisoning is an edi-torial supplement sponsored by EMD Pharmaceuticals andpublished by Jems Communications, 525 B Street, Suite 1900,San Diego, CA 92101-4495; 800/266-5367 (fed. ID #13-935377).Copyright 2004 Elsevier Inc. No material may be reproducedor uploaded on computer network services without theexpressed permission of the publisher. Subscription infor-mation: To subscribe to a Jems Communications publication,visit www.jems.com. Advertising information: Rates areavailable on request. Contact Jems CommunicationsAdvertising Department at 525 B Street, Suite 1900, SanDiego, CA 92101-4495; 800/266-5367.
Hydrogen Cyanide

TREATMENT FOR SMOKEINHALATION in the United Stateshas not changed much during the pastseveral years: We remove the victimfrom the source, provide high-flow100% oxygen and assist with ventila-tion, if needed. Responding EMS per-sonnel and firefighters are primarilyconcerned with carbon monoxide poi-soning and hypoxia in smoke-inhala-tion patients. However, hydrogencyanide poisoning is an increasinglycommon byproduct of fire smoke instructure fires, threatening both firevictims and firefighters. Unfortunately,it is rarely treated in the United States,and when it is, the current U.S. drugtherapy for cyanide poisoning carries arisk of actually doing more harm thangood.
At the International Association ofFire Chiefs EMS Section’s Fire-RescueMed Conference in April, I served asthe moderator for a panel of expertswho addressed the topic of cyanidepoisoning in smoke inhalation andchemical terrorism. The presentations,compiled in this special issue, aredesigned to educate emergencyresponse professionals on the risks ofcyanide poisoning, as well as the treat-ment options.
In the first article, Richard Alcorta,MD, medical director at the MarylandInstitute for Emergency MedicalServices System, notes that smokeinhalation causes 5,000–10,000 deathsand more than 23,000 injuries—includ-ing 5,000 firefighters—in the UnitedStates annually. Dr. Alcorta presentsdata from several studies revealingelevated cyanide concentrations insmoke-inhalation victims, highlightingthe direct relationship between cyanideblood concentrations and probability ofdeath, and indicating that cyanide andcarbon monoxide enhance the toxiceffects of one another. He also reviewsthe current treatment for smoke inhala-tion, which some authorities do not rec-
ommend using, and discusses howimportant rapid treatment is to improv-ing chances for survival.
In the second presentation, Jean-LucFortin, MD, chief of medicine for theThird Division of the Paris (France) FireBrigade, provides data on an alternativecyanide antidote that is currently avail-able in Europe. Hydroxocobalamin isroutinely used in France to treatsmoke-inhalation victims at the sceneof fires. Dr. Fortin reviews data from aretrospective study of 81 smoke-inhala-tion victims treated with hydroxocobal-amin by the Paris Fire Brigade. Theresults are promising, with a 62.1% sur-vival rate following hydroxocobalaminadministration as part of treatment forcyanide poisoning and carbon monox-ide exposure.
The final presenter, Marc Eckstein,MD, medical director for the LosAngeles Fire Department and an asso-ciate professor of emergency medicineat the University of SouthernCalifornia School of Medicine, discuss-es the intentional use of cyanide as anagent of war and terror. He notes thatcyanide is plentiful, readily availableand does not require special expertiseto use. Dr. Eckstein also indicates thatif hydroxocobalamin becomes avail-able in the United States, cyanide poi-soning may be successfully treated in aprehospital setting.
Collectively, the presentations provide a broad overview of cyanidepoisoning and its treatment, both inconjunction with smoke-inhalationexposure and as an agent of chemicalterrorism. I believe you will find thearticles extremely informative andtimely. Armed with this knowledge, Iam optimistic that we can eventuallyreduce the significant number ofsmoke-inhalation deaths experiencedeach year in this country, as well asenhance our level of emergency pre-paredness for the potential use ofcyanide in chemical terrorism.
HYDROGEN CYANIDEFire Smoke’s Silent Killer
Deputy ChiefKen Riddlehas more than 30years’ experiencewith emergencyservices in boththe private andpublic sectors. A
member of the Las Vegas Department ofFire & Rescue for 25 years, Riddle cur-rently serves as the city’s fire marshal.As a chief officer for the past 10 years,he has been responsible for the opera-tions, administration and medical servicesdivisions. While serving in those positions,he designed and developed several major programs, including an ambulance transport program for the department.Riddle was certified as a paramedic forseveral years and also served as a flightmedic. An author and frequent speakeron fire-based EMS issues, he is theimmediate-past chair of the InternationalAssociation of Fire Chiefs EMS Sectionand the past president of the SouthernNevada Fire Chiefs Association. Riddlecontinues to serve as the conferencemanager for the EMS Section’s Fire-Rescue Med Conference, held annually inLas Vegas.
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 5

EMERGENCY medical and fire-rescue professionals tend toequate cyanide poisoning withaccidental or intentional inges-tion. However, cyanide toxicityfrom smoke inhalation in a struc-tural or an enclosed-space fire isthe most likely cause of cyanide
toxicity that EMS and fire profes-sionals will encounter.
Smoke inhalation is an impor-tant but often overlooked cause ofcyanide poisoning. A substantialbody of evidence reveals thatcyanide can be as great a threat ascarbon monoxide in fire smoke.
6 JEMS COMMUNICATIONS
SMOKEINHALATION & ACUTE CYANIDEPOISONING
SMOKEINHALATION & ACUTE CYANIDEPOISONING
Hydrogen cyanide poisoning proves increasingly common in smoke-inhalation victimsBY RICHARD ALCORTA, MD, FACEP
The family had gone to bed only two hours before the fire started.A space heater in the living room ignited a sofa cushion, which smoldered for a period of time, emitting toxic gases evenbefore the flames appeared. Within minutes after flames appeared, the fire spread upward from the burning sofa cush-ions and ignited first the draperies, then the ceiling. As the fire gained force, toxic smoke filled the room and entered thehallway. The smoke detector located down the hall finally activated and awakened the family. Meanwhile, a neighbor sawthe flames while he was walking his dog and called 9-1-1.
The fire’s heat and its dense black smoke prevented the family from exiting via the stairs. When firefighters arrivedwithin four minutes of the 9-1-1 call, they had to rescue the three victims through a second-story window. All were foundhuddled close to the window, disoriented or unconscious, with soot in their noses and mouths. The mother and four-year-old boy were given oxygen and transported to a hospital where they survived. The father, who had rushed into the halland into his son’s room in an attempt to rescue him, went into full respiratory arrest. He had only 10% burns on his faceand hands, but his condition, which initially appeared to stabilize, rapidly deteriorated en route to the hospital, despite100% oxygen and supportive care. He died without regaining consciousness.
The JEMS continuing education program is coordinated by theCenter for Emergency Medicine, Pittsburgh, and the University of Pittsburgh, School of Health and Rehabilitation Sciences.

SMOKE INHALATION & HYDROGEN CYANIDE POISONING 7
Pho
to G
len
E. E
llman

This article will discuss:• Why cyanide poisoning is a
growing concern in the fire andEMS communities;
• The role of cyanide in smokeinhalation-associated morbidi-ty and mortality as evidencedby two prospective studies— a 2002 meta-analysis of firevictim studies and animalresearch on cyanide-relatedincapacitation; and
• The factors involved in the man-agement of smoke inhalation-associated cyanide poisoning—its mechanism, manifestations,recognition and treatment.
SMOKE TOXICITYSmoke inhalation is a more com-mon source of fire-related mortalitythan burns. It causes 5,000–10,000deaths annually in the United Statesand more than 23,000 injuries,including approximately 5,000 fire-fighter injuries. In fact, the UnitedStates has one of the highest fire-death rates among industrializedcountries.1
Smoke toxicity is an increasingconcern, particularly in the fireservice, because the industrial prod-ucts used today are changing. Overthe past two decades, we’ve seen ashift away from woods and naturalmaterials toward lighter construc-tion materials, synthetics and petro-chemical-based materials. Thesematerials ignite and burn two tothree times hotter and faster thanconventional materials and, whenheated, emit a gas or smoke that willalso ignite two to three times fasterand burn two to three times hotterthan gas or smoke emitted from con-ventional materials.
These materials result in morefires reaching flashover and a short-er time per fire between ignition andflashover. Consequently, firefightershave less time to gain control of afire. Smoke-inhalation victims haveless time to escape and are morelikely to be incapacitated from thetoxic smoke, thereby increasing therisk of other injuries, such as thermalinjuries. More effective prehospitaltreatment will save lives.
Studies completed by theNational Institute of Standards andTechnology in conjunction with theFire Protection Research Foundationdocument a significant increase intoxic gases in smoke immediatelybefore flashover occurs, as well asafter flashover.2 Conditions of hightemperature and low oxygen pro-mote degradation of synthetics,which release hydrogen cyanide andother toxic gases.
FIRE SMOKESmoke is composed of particulatematter; heated gases, including irri-tants, such as hydrochloric acid,sulfur dioxide and ammonia;asphyxiates, such as carbon diox-ide; and toxins, such as hydrogensulfide and hydrogen cyanide.
The constituents of smoke varyfrom fire to fire and from one loca-tion to another in a given fire,depending on such factors as thecomposition of the burning material,the rate of burning, the absolute tem-perature and the ambient oxygenlevel. However, carbon monoxide andhydrogen cyanide are very likely tobe two of the most prevalent gases.3
Hydrogen cyanide, the gaseousform of cyanide, is generated by thecombustion of nitrogen- and carbon-containing substances, includingwool, silk, cotton and paper, as wellas synthetic substances, such asplastics and other polymers. Becauseof our extensive reliance on thepolymer industry’s nitrogen- andcarbon-containing products, thesehydrogen cyanide substrates areubiquitous in occupied structures.Hydrogen cyanide is likely to beproduced under burning conditions
8 JEMS COMMUNICATIONS
Objectives• List reasons for the increased
incidence of smoke inhalation-associated cyanide poisoning.
• Determine the role of cyanide in smoke inhalation-associatedmorbidity and mortality.
• Describe the management ofsmoke inhalation-associatedcyanide poisonings.
Cyanide toxicityfrom smokeinhalation in astructural orenclosed-spacefire is the mostlikely cause ofcyanide toxicitythat EMS & fire professionals will encounter.
Sources of Cyanide in Fire Smoke
Natural substances• Wool• Silk• Cotton • Paper
Synthetic substances• Plastics • Other
polymers

of high temperature and low oxygen,both of which are characteristic ofclosed-space fires. An enclosedspace serves as a container for thetoxic gases in smoke, such as hydro-gen cyanide.4,5
Our two greatest threats in firesmoke are carbon monoxide poison-ing, of which most of us are aware,and cyanide poisoning, of whichmany are not aware. Both carbonmonoxide and hydrogen cyanide aresilent killers. Both agents are color-less and odorless, dulling their victim’s cognitive function andimpairing the fight-or-flight responsewhile their victim is completelyunaware of their presence.
KEY CYANIDE STUDIESTwo prospective studies performedin Paris, France, and Dallas County,Texas, elucidate cyanide’s contribu-tion to smoke inhalation-associatedmortality.6,7 These studies weredesigned to assess cyanide’s role infire-related morbidity and mortality.The researchers overcame manyother studies’ limitations by collect-ing blood samples close to the timeof smoke exposure and measuringcyanide in survivors rather thanonly in fatalities.
In the Paris study, the first med-ical squads to arrive on scene at res-idential fires in Paris collected bloodin dry heparin over the span of ayear (1988–1989). The blood cyanidedata compared 109 fire victims (66survivors and 43 fatalities) with 114control individuals (40 with drugintoxication, 29 with carbon monox-ide poisoning [none fire-related]and 45 with major trauma).
The results show that mean bloodcyanide concentrations in both firevictims who survived (21.6 mol/L, or0.58 mg/L) and in those who died(116.4 mol/L, or 3.14 mg/L) were sig-nificantly (p<0.001) higher thanthose in control subjects (5.0 mol/L,or 0.01 mg/L), and levels in victimswho died were significantly higherthan those in victims who survived.Clearly, all those who died had avery high or lethal level of cyanide,perhaps due to the fact that cyanideaffects the heart and brain and caus-
es altered mental status and confu-sion, possibly preventing the victimsfrom escaping.
Several deaths occurred in victimswhose blood cyanide and carbonmonoxide levels were both in thenontoxic range.6 These deaths couldpossibly be attributed to causes otherthan the two toxins. However, thedeaths among individuals havingnontoxic cyanide and carbon monox-ide levels may also be explained bythe potentiation of either or bothcompounds’ toxic effects. This possi-bility is consistent with previousreports of fire victims having sub-lethal concentrations of carbonmonoxide and no other apparentcause of death.8,9 It is also consistentwith animal studies showing the syn-
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 9
PARIS FIRE Study Conclusions• Cyanide and carbon
monoxide were both impor-tant determinants of smokeinhalation-associated morbidity and mortality;
• Cyanide concentrations were directly related to theprobability of death;
• Cyanide poisoning may havepredominated over carbon monoxide poisoning as acause of death in some firevictims; and
• Cyanide and carbon monox-ide may have potentiated thetoxic effects of one another.
Treatment for hydrogen cyanide poisoning must be administeredas quickly as possible after exposure. Therefore, presumptivediagnosis and empiric treatment prove necessary to save lives.
Pho
to G
len
E. E
llman
ergistic lethality of cyanide and car-bon monoxide in the absence ofchanges in blood concentrations.10
The Dallas County study assessedtwo groups of smoke-inhalation vic-tims over the same two-year period.One group comprised 144 smoke-inhalation patients who were aliveat the time of initial evaluation inthe University of Texas HealthScience Center emergency depart-ment (ED). The second group com-prised 43 individuals who were deadon arrival at the Dallas County med-ical examiner’s office.
The results show that mean blood
cyanide concentrations in the 144smoke-inhalation victims whoarrived alive at the ED were lowerthan concentrations in the 43 vic-tims who were dead on arrival (0.65mg/L versus 2.15 mg/L). Of the 144patients who were alive when theyarrived at the ED, 12 had bloodcyanide concentrations exceeding 1mg/L, the lower limit of the rangedefined as potentially lethal in thisstudy. Of these 12 patients, eightdied. None of them had blood car-boxyhemoglobin (HbCO) concen-trations suggesting carbon monox-ide as the cause of death (e.g., ≥50%).Although some of the patients whodied had extensive burns that mayhave contributed to death, three ofthem had ≤4% total body surfacearea burn.6
These data are consistent withthe results of the Paris study inshowing pervasive elevated cyanideconcentrations and a direct relation-ship between blood cyanide concen-tration and probability of death andin suggesting that cyanide poisoningmay predominate over carbonmonoxide poisoning as a cause ofdeath in some fire victims. It is clearthat every victim metabolizescyanide differently—some betterthan others. For those who do notmetabolize it well, it remained intheir system and was apparentlycompounded by carbon monoxide,leading to their deaths. A limitedamount of cyanide is converted tobyproducts through the sulfur trans-ferase/rhodanese enzymes and theavailability of sulfur donor com-pounds. Patients with existing liverdisease or inherent limitation ofthese enzymes will have reducedclearance and increased toxicity.
2002 META-ANALYSIS OF FIRE DEATHSResults of a 2002 meta-analysis offire casualty databases suggest thatcyanide poisoning is a significant andindependent contributor to smoke-inhalation deaths.11 In the meta-analysis, data from seven publishedstudies in which blood cyanide con-centrations were reanalyzed in a uni-form manner to facilitate compar-
10 JEMS COMMUNICATIONS
• Asphyxiate: A gas that is non-toxic but will displace oxygenfrom the atmosphere, thus caus-ing a life-threatening environ-ment due to a lack of oxygen.
• Carboxyhemoglobin (HbCO):The laboratory measurablecomponent of blood that is thebound percent of hemoglobinwith carbon monoxide. Carbonmonoxide once attached tohemoglobin prevents oxygenfrom binding to those sites onthe hemoglobin.
• Flashover: In a compartmentfire there can come a stage inwhich the total thermal radia-tion from the fire plume, hotgases and hot compartmentboundaries causes the genera-tion of flammable products ofpyrolysis from all exposed com-bustible surfaces within thecompartment. Given a source ofignition, this will result in thesudden and sustained transition
of a growing fire to a fullydeveloped fire. The rapid transi-tion to a state of total surfaceinvolvement in a fire of combustible materials within acompartment.
• Histo-toxin: A cellular poison ora substance that has a direct poisonous effect at the cellular(histo) level. The substance caninhibit cellular respiration/metabolism.
• Pyrolysis: A form of incinera-tion that chemically decomposesorganic materials by heat in theabsence of oxygen or is thedecomposition/ transformationof a chemical compound caused by heat.
• Toxin: A poisonous substancethat can be produced during metabolism or growth of anorganism, or produced by thecombination/combustion ofmaterials.
DALLAS FIRE Study Conclusions• Elevated cyanide concentra-
tions were pervasive amongsmoke-inhalation victims;
• Cyanide concentrations weredirectly related to the proba-bility of death; and
• Cyanide poisoning may havepredominated over carbonmonoxide poisoning as acause of death in some firevictims.
Glossary

isons between studies. In most of thestudies measuring blood cyanide,HbCO (carboxyhemoglobin), which isformed by the union of carbonmonoxide with hemoglobin and is amarker of carbon monoxide poison-ing, was also measured.
The results of the meta-analysisshould be interpreted in the contextof its limitations, including the retro-spective data collection and analysisof many of the studies included inthe meta-analysis, inconsistenciesbetween studies in blood samplingmethods, and timing and significantdelays in some studies in analyzingblood samples. (Data from studies inwhich only carbon monoxide wasmeasured were also reported in themeta-analysis but are not describedhere. In addition, data from a 1966report that included blood cyanidemeasurements are not includedhere because no details about thestudy sample were described.)
The results show that, acrossstudies, significant proportions(33–87%) of fire victims had bloodcyanide levels of at least 1 mg/L, val-ues above which are potentiallylethal. Blood cyanide levels ≥3 mg/Lwere found in 5–46% of victimsacross studies. The percentage ofvictims with potentially lethal levelsof carbon monoxide ranged from5–98% across studies.
Cyanide perhaps played a greaterrole in mortality than carbonmonoxide in two particular firesconsidered in the meta-analysis: theManchester aircraft fire atManchester International Airport in1985 and the Dupont Plaza Hotelfire in San Juan, Puerto Rico, in1986. Victims of the Manchester firewere not severely burned and weredetermined to have died of smokeinhalation. The majority (87%) of the54 individuals who died had poten-tially lethal blood cyanide levels of≥1 mg/L (median=2.3 mg/L), where-as only 21% of victims had HbCOlevels exceeding 50% (medianHbCO=39%).
Similarly, in the Dupont PlazaHotel fire, approximately half (48%)of the 53 victims had potentiallylethal blood cyanide levels of ≥1 mg/L
(median=1 mg/L), whereas only 5% ofvictims had HbCO levels exceeding50% (median HbCO=33%). In this fire,unlike the Manchester aircraft fire,many of the victims were severelyburned, and the relative contribu-tions of smoke inhalation and burnsto their deaths are difficult to deter-mine. This caveat notwithstanding,the results considered in aggregateare consistent with the possibilitythat cyanide can sometimes be amore important determinant ofsmoke inhalation-associated mortali-ty than carbon monoxide, which isusually regarded as the primary toxicthreat in fire smoke.
The results of the 2002 meta-analysis show frequent exposure topotentially lethal concentrations ofcyanide, as well as coexposure to car-
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 11
2002 META-ANALYSIS Conclusions• Exposure to potentially
lethal cyanide concentrationswas frequent;
• Coexposure to carbonmonoxide and cyanide was frequent; and
• In some fire incidents,cyanide may have played a more important role incausing death than carbonmonoxide.
Hydrogen cyanideis generated bythe combustion of nitrogen- & carbon-containing substances,including wool,silk, cotton &paper, as well as synthetic substances, suchas plastics &other polymers.
Although poor tissue utilitization of oxygen in cyanide poisoningshould theoretically render supplemental oxygen useless,supportive care with administration of oxygen has proven effective in a number of poisonings.
Pho
to G
len
E. E
llman

bon monoxide and cyanide in smoke-inhalation victims. Consistent withthe prospective Paris and DallasCounty studies, the meta-analysisresults suggest that, in some fire inci-dents, cyanide may have played agreater role in causing death thancarbon monoxide.
SUBLETHAL CYANIDECONCENTRATIONSMost assessments of cyanide poi-soning in smoke-inhalation victimshave attempted to define the role ofcyanide exposure in fire-relateddeaths. The role of sublethal con-centrations of cyanide in smokeinhalation-associated morbidity andmortality has not been systematical-ly assessed in humans.
Data from research in whichmonkeys were exposed to fumesfrom the pyrolysis of polyacryloni-trile—a high-nitrogen polymerused in fiber form for fabrics,upholstery covers, infill paddingand clothing—suggest that sub-lethal levels of cyanide can causerapid incapacitation that preventsefforts to escape toxic fumes. Underthermal decomposition, approxi-mately half of the mass of polyacry-lonitrile becomes available as
hydrogen cyanide.Cyanide-exposed monkeys hyper-
ventilated and then rapidly lost con-sciousness at a rate dependent on theconcentration of exposure. A concen-tration of 200 parts per million (ppm)was associated with rapid incapacita-tion but not with elevated bloodcyanide concentrations measuredhours after exposure. The authorssuggest on the basis of these findingsthat cyanide in smoke can lead todeath indirectly via incapacitation,which immobilizes the smoke-inhala-tion victim and permits more pro-longed exposure to potentially fatalconcentrations of other toxins andasphyxiates identified as the primarycause of death.12
Considered in aggregate, theblood cyanide findings in fire vic-tims support an important role ofthis toxin in smoke inhalation-associated morbidity and mortality.Cyanide poisoning should be sus-pected in any fire victim and may beparticularly likely in individualsexposed to closed-space fires and inthose with soot in the mouth ornose, altered mental status orhypotension.11,13
SIGNS & SYMPTOMSSmoke inhalation-associated cyanidepoisoning manifestations vary. In vic-tims with low inhaled-cyanide con-centrations or very recent exposureto moderate or high concentrations,manifestations may include:
• Faintness;• Flushing;• Anxiety;• Excitement;• Perspiration;• Vertigo;• Headache;• Drowsiness;• Tachypnea;• Dyspnea; and• Tachycardia.
In victims with moderate or highconcentrations, manifestations mayinclude:
• Prostration;• Tremors;• Cardiac arrhythmia;• Convulsions;
12 JEMS COMMUNICATIONS
Firefighters who respond to enclosed-space fires are increasingly exposed to hydrogen cyanide, a byproduct of firesmoke from nitrogen- and carbon-containing materials used inconstruction and furniture today.
Pho
to G
len
E. E
llman
Cyanide poisoning shouldbe suspected inany fire victim & may be particularlylikely in individualsexposed toclosed-spacefires & in thosewith soot in themouth or nose,altered mentalstatus or hypotension.
• Stupor;• Paralysis;• Coma;• Respiratory depression;• Respiratory arrest; and• Cardiovascular collapse.
Cyanide is a histo-toxin. It caus-es toxicity by deactivating the mech-anism by which cells use oxygen.The heart and brain—organs thatrely on a substantial, continuoussupply of oxygen—are markedlyaffected by cyanide poisoning.Accordingly, most signs and symp-toms of acute cyanide poisoningreflect the nonspecific effects ofoxygen deprivation on the heart andbrain. Exposure to smaller concen-trations can initially cause respira-tory activation (manifested byhyperpnea and tachycardia) in anattempt to compensate for lack ofoxygen followed by respiratory andmyocardial depression.
Early neurologic manifestations,reflecting initial effects of brain oxy-gen deprivation, include headache,giddiness and anxiety. Later mani-festations of exposure to smallerconcentrations or early manifesta-tions of exposure to large concentra-tions include cardiac arrhythmias,stupor, coma and seizure that culmi-nate in respiratory depression anddeath.4,14,19
Successful intervention forcyanide poisoning depends primari-ly on the concentration of exposureand the time between exposure and treatment. Clearly, it is critical that treatment is administered as quickly as possible after exposure.Therefore, presumptive diagnosis ofcyanide poisoning and empirictreatment prove necessary.
PREHOSPITAL INTERVENTIONPrehospital management of acutecyanide poisoning in the smoke-inhalation victim involves movingthe victim from the source of expo-sure (while maintaining appropriateprovider respiratory protection,SCBA), restoring or maintaining air-way patency, administering 100%oxygen via non-rebreather mask orbag-valve mask technique, aggres-
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 13
PREHOSPITAL CareAggressive airway management with delivery of 100% oxygen can save lives:• Intubate if the patient is unconscious or the airway cannot
be protected.
• Establish an IV line, and provide cardiac monitoring.
• Administer sodium bicarbonate if the patient is unconsciousor hemodynamically unstable.
• Administer cyanide antidotes in prehospital care if diagnosisis relatively certain. Avoid the sodium nitrite portion of theTaylor cyanide antidote kit (also called the Lilly or Pasadenakit) in patients with smoke inhalation. Such treatment gener-ally should involve online medical control. Anticonvulsantsmay be needed for generalized seizures. Vasopressors (e.g.,epinephrine) are indicated for hypotension not responsive to a fluid challenge.
• Although poor tissue utilization of oxygen in cyanide poison-ing should theoretically render supplemental oxygen admin-istration useless, supportive care with administration of oxygen alone has proven effective in a number of poisonings.
Emergency Department Care: Initial ED care is identical to that provided in prehospital phase:• Consider antidotal therapy if diagnosis is strongly suspected.
• Begin antidotal therapy without waiting for laboratory confirmation.
• Avoid sodium nitrite portion of the Taylor cyanide antidote kit in patients with smoke inhalation unlesscarboxyhemoglobin concentration is very low (<10%).1
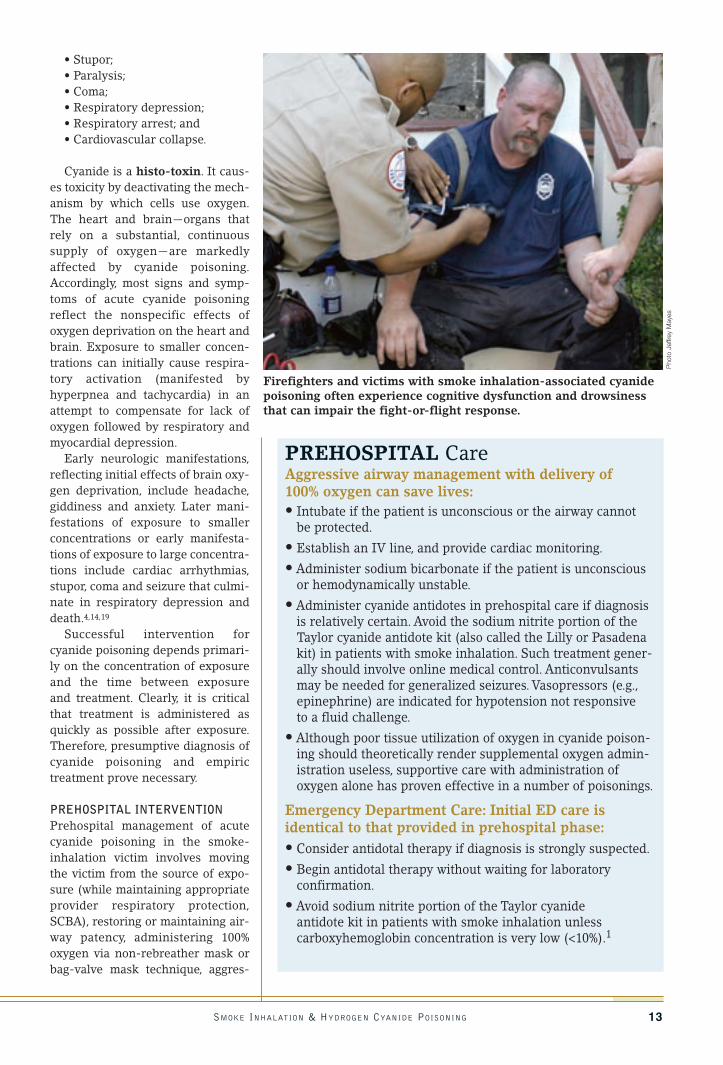
Firefighters and victims with smoke inhalation-associated cyanidepoisoning often experience cognitive dysfunction and drowsinessthat can impair the fight-or-flight response.
Pho
to J
effre
y M
ayes

sive advanced airway management,including early intubation, providingcardiopulmonary support and stabi-lizing vital signs, including the use oftrauma and burn management(Parkland formula). When clinicallyindicated, anticonvulsants (benzodi-azpines) should be given forseizures, epinephrine and antiar-rhythmics to stabilize cardiovascularfunction, and sodium bicarbonate to correct metabolic acidosis ifknown.4,5,13,15,19
Effective cyanide antidotes exist.However, a cyanide antidote appro-priate for use in smoke-inhalationvictims is not yet available in theUnited States, where the cyanideantidote kit (also called the Lilly kit,Taylor kit or Pasadena kit) is theonly antidote currently available.The kit consists of amyl nitrite, thio-sulfate and sodium nitrite.15
The cyanide antidote kit shouldnot be used outside of a hospital insmoke-inhalation victims. Thenitrites in the kit reduce the blood’soxygen-carrying capacity by bind-ing with hemoglobin to formmethemoglobin, which binds andneutralizes cyanide. Problematically,inducing methemoglobinemia canalso significantly reduce the blood’soxygen-carrying capacity. In smoke-
inhalation victims with cyanide poi-soning, concurrent carbon monoxidepoisoning almost always compro-mises the blood’s oxygen-carryingcapacity. Superimposing additionalreductions in oxygen-carryingcapacity of the blood from antidote-induced methemoglobinemia ispotentially dangerous and evenfatal. The currently availablecyanide antidote may also causesevere hypotension, an effect thatcounteracts efforts to achieve hemo-dynamic stability in fire victims.3,16,17
Hydroxocobalamin, a precursor ofvitamin B12, is being investigated forpossible introduction in the UnitedStates to meet the need for an anti-dote that can be used safely on anempiric basis. Hydroxocobalaminhas been available for nearly adecade in France, under the nameCyanokit™ (Merck-Santé s.a.s) andis the antidote used by the ParisFire Brigade.1 Hydroxocobalamindetoxifies cyanide by binding withit to form cyanocobalamin (vitaminB12), which in excess is excreted inthe urine.17,18 Should it becomeavailable in the United States,hydroxocobalamin potentially willenable prehospital antidotal treat-ment of cyanide poisoning in smoke-inhalation victims. The ability toadminister an antidote in the prehos-pital setting should increase thespeed of intervention and, arguably,its effectiveness.
For now, the best course of prehos-pital intervention is the provision ofrapid transport to a hospital ED orburn center where definitive treat-ment can be delivered.
FINAL WORDResearch suggests that cyanideshould be expected in fire victims’blood and is often as great a threat ascarbon monoxide. Morbidity andmortality from smoke inhalation-associated cyanide poisoning arepreventable if cyanide poisoning issuspected or promptly recognizedand antidotal therapy initiatedshortly after cyanide exposure.Hydroxocobalamin, currently underFDA evaluation, may offer a favor-able risk-benefit ratio that allows for
14 JEMS COMMUNICATIONS
Successfulintervention forcyanide poisoningdepends primarily on theconcentration ofexposure & thetime betweenexposure & treatment.
Prehospital management of acute hydrogen cyanide poisoningincludes moving the victim away from the source of exposure,restoring or maintaining airway patency, administering 100% oxygen via a non-rebreather mask or bag-valve technique,providing aggressive advanced airway management and cardiopulmonary support, and stabilizing vital signs.
Pho
to G
len
E. E
llman

its empirical use in the prehospitalsetting.
Richard Louis Alcorta, MD, FACEP,is the state EMS director for the MarylandInstitute for Emergency Medical ServicesSystems (MIEMSS). He is also theMaryland medical director of the ChemicalStockpile Emergency PreparednessProgram and an emergencyspecialist/physician. A former paramedicliaison at the Suburban Hospital inBethesda, Md., Alcorta is a fellow of theAmerican College of EmergencyPhysicians and is board-certified in emer-gency medicine by the American Board ofEmergency Medicine. He is also a certifiedMaryland state EMT-paramedic instructor,hospital hazardous material instructor andAdvanced Trauma Life Support instructor.Alcorta is a member of many professionalorganizations, including the Alpha OmegaAlpha Medical Honor Society, theAmerican Medical Association, theAmerican College of EmergencyPhysicians, the National Association ofEMS Physicians and the NationalAssociation of State EMS Directors.
Special thanks to Jane Saiers, PhD, whocompleted the background literatureresearch on cyanide presented in this article
This continuing education activity isapproved by the Center for EmergencyMedicine, an organization accredited by theContinuing Education Board for EmergencyMedical Services (CEBEMS), for 1.5 hourscredit for First Responder, Basic andAdvanced providers.
REFERENCES
1. Borron SW, Gaud FJ: “Toxicity, cyanide.”February 2003.www.emedicine.com/emerg/topic118.htm. Accessed Jan. 13, 2004.
2. Smoke Component Yields from Room-scale Fire Tests, Fire Research Division,Building and Fire Research Laboratory,National Institute of Standards andTechnology, Gaithersburg, Md., 20899-8664, 2002.
3. Kulig K: “Cyanide antidotes and firetoxicology.” New England Journal ofMedicine. 325:1801–1802, 1991.
4. Agency for Toxic Substances andDisease Registry. U.S. Department ofHealth and Human Services, PublicHealth Service. American Family
Physician. 48:107–114, 1993.
5. Lee-Chiong TL: “Smoke inhalationinjury.” Postgraduate Medical Journal.105:55–62, 1999.
6. Baud FJ, Barriot P, Toffis V, et al:“Elevated blood cyanide concentrationsin victims of smoke inhalation.” NewEngland Journal of Medicine.325:1761–1766, 1991.
7. Silverman SH, Purdue GF, Hunt JL, etal: “Cyanide toxicity in burned patients.”Journal of Trauma. 28(2):171–176, 1988.
8. Birky MM, Clarke FB: “Inhalation oftoxic products from fires.” Bulletin of theNew York Academy of Medicine.57(10):997–1013, 1981.
9.Teige B, Lundevall J, Fleiscer E:“Carboxyhemoglobin concentrations infire victims and in cases of fatal carbonmonoxide poisoning.” Zeitschrift furRechtsmedizin (Journal of LegalMedicine). 80(1):17–21, 1977.
10. Norris JC, Moore SJ, Hume AS:“Synergistic lethality induced by thecombination of carbon monoxide andcyanide.” Toxicology. 40:121–129, 1986.
11. Alarie Y: “Toxicity of fire smoke.”Critical Reviews in Toxicology.32:259–289, 2002.
12. Purser DA, Grimshaw P, Berrill KR:“Intoxication by cyanide in fires: astudy in monkeys using polyacryloni-trile” Archives of Environmental Health.39:394–400, 1984.
13. Koschel MJ: “Where there’s smoke,there may be cyanide.” AmericanJournal of Nursing. 102:39–42, 2002.
14. Chemical Casualty Care Division,Aberdeen Proving Ground, Md. UnitedStates Army Medical Research Instituteof Chemical Defense: MedicalManagement of Chemical CasualtiesHandbook, 3rd ed. The Virtual NavalHospital Project, 1997–2004.
15. Sauer SW, Keim ME:“Hydroxocobalamin: improved publichealth readiness for cyanide disas-ters.” Annals of Emergency Medicine.37: 635–641, 2001.
16. Hall AH, Rumack BH: “Clinical toxicol-ogy of cyanide.” Annals of EmergencyMedicine. 15:1067–1074, 1986.
17. Hall AH, Kulig KW, Rumack BH:“Suspected cyanide poisoning insmoke inhalation: complications ofsodium nitrite therapy.” Journal deToxicologie Clinique et Expérimentale.9:3–9, 1989.
18. Mégarbane B, Delahaye A, Goldgran-Toledano D, Baud FJ: “Antidotal treat-ment of cyanide poisoning.” Journal ofthe Chinese Medical Association.66:193–203, 2003.
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 15
(continued on next page)

16 JEMS COMMUNICATIONS
The JEMS CE program is coordinated by the Center for EmergencyMedicine and the University of Pittsburgh, School of Health andRehabilitation Sciences, which is accredited by the ContinuingEducation Coordinating Board for EMS to approve CE activities.
SMOKE INHALATION & ACUTE CYANIDE POISONING
1. EMS providers are most likely toencounter acute cyanide poisoning in patients:a. who intentionally overdose on cyanide in
a suicide attemptb. accidentally poisoned through improper
food storage c. poisoned through occupational exposuresd. with smoke inhalation from a closed-
space fire
2. Synthetics used in manufacturingtoday:a. are heavier than traditional building
materialsb. ignite slowly and burn with low intensityc. burn cleanly with little toxic chemical
emission d. burn hotter than traditional building
materials
3. Two of the most prevalent gases insmoke from most fires are:a. hydrogen cyanide and carbon monoxideb. carbon dioxide and hydrogen sulfidec. hydrogen sulfide and hydrogen chlorided. hydrogen chloride and carbon dioxide
4. Hydrogen cyanide is likely to be produced:a. in low temperature fire conditionsb. in fires with high oxygen contentc. by burning synthetic materials, never
natural materialsd. by the combustion of nitrogen-
containing products
5. Which of the following is true of hydrogen cyanide?a. Hydrogen cyanide has a distinctive smellb. Hydrogen cyanide is colorlessc. Hydrogen cyanide impairs muscular
ability but not cognitive functiond. Hydrogen cyanide plays no role in early
fire-related deaths
6. One of the findings from the Pariscyanide study was that:a. Cyanide may play a more important role
than CO as a cause of deathb. Cyanide levels at the scene were not close-
ly related to cyanide levels measured laterc. Cyanide played no role in determining the
probability of deathd. Carbon monoxide and cyanide appear to
function independently of one another
7. Cyanide in the body:a. is not metabolized—it must be removed
with blood filtrationb. is metabolized less efficiently by patients
with liver diseasec. remains active until an antidote is
deliveredd. only presents a problem if CO is present
8. HbCO is a measure of:a. the interaction between cyanide and
carbon monoxideb. cyanide levels in the bloodc. carbon monoxide poisoningd. cyanide levels in inhaled air
9. A conclusion from the 2002 meta analysis of fire deaths is that:a. patients rarely were exposed to both
cyanide and carbon monoxideb. patients frequently had lethal cyanide
exposuresc. carbon monoxide was a better
determinant of death than cyanided. carbon monoxide levels were not a
determining factor in patient deaths
10. Sub-lethal concentrations of cyanide can lead to:a. rapid incapacitationb. minor changes in alertnessc. changes in mental status, but are rarely
life-threateningd. few changes in patient condition unless
concentrations increase
11. Cyanide poisoning is especially likelyin those patients who:a. were in open-air firesb. have hypertension following exposure to
smokec. have a normal level of consciousness
following an enclosed space fired. have soot in their nose or mouth
12. Which of the following is typical oflow concentration cyanide poisoning:a. stuporb. headachec. tremorsd. respiratory depression
13. Organs most commonly affected bycyanide poisoning include the:a. lungs and heartb. liver and kidneysc. heart and braind. stomach and intestines
14. Cyanide antidote kits available in theUnited States:a. should be administered as soon as
possible to all smoke inhalation victimsb. should be administered if CO poisoning
is suspected in addition to cyanide poisoning
c. should be administered if the oxygen saturations in the blood are low
d. should not be administered outside of thehospital
15. Which of the following is true of cyanide antidotes?a. Currently, no effective antidote existsb. Effective antidotes for smoke-inhalation
patients are not available in the UnitedStates
c.The current cyanide antidote kit used inthe United States is an effective and safe treatment
d.The antidote kit available in the UnitedStates may not be effective, but it will do no harm
16. Hours after exposure, the cyanideblood level of monkeys exposed tosub-lethal cyanide doses showed:a. no elevationb. moderate elevationc. marked elevationd. extremely high levels
17. Cyanide causes toxicity by:a. blocking the release of neurotransmittersb. deactivating the mechanism by which cells
use oxygenc. releasing histamined. causing cells to rapidly use all
available oxygen
18. Patients with cyanide poisoning should be:a. intubated only if they are in cardiac arrestb. intubated if they cannot maintain their
own airwayc. managed without intubation due to poten-
tial damage to the trachead. managed with low-flow oxygen to slowly
restore oxygen levels
19. Known metabolic acidosis due tocyanide poisoning should be treated with:a. vasopressorsb. anticonvulsantsc. epinephrined. sodium bicarbonate
20. Which medication from the cyanide poisoning antidote kit should notbe administered in the prehospitalsetting?a. amyl nitriteb. thiosulfatec. sodium nitrited. atropine
CE TEST #199

SMOKE INHALATION & HYDROGEN CYANIDE POISONING 17
To be considered for credit, this testmust be postmarked by August 15, 2005.
Name __________________________________________
Address_________________________________________
City/State/ZIP ___________________________________
Organization_____________________________________
State Certification # ______________________________
Phone # ________________________________________
E-mail _________________________________________
S.S. # __________________________________________
National Registry #_______________________________
Skill Level: �� EMT �� EMT-I �� ParamedicArea of Service: �� Rural �� UrbanStatus: �� Volunteer �� Paid
Do you presently have a personal subscription to JEMS?�� Yes �� No
Are you using this test as part of your requirements for recertification? �� Yes �� No
Instructions for Obtaining CE Credit
1. Study the CE article in this supplement.2. Answer the test questions on this form that are
appropriate to your level of care. (Photocopies of theanswer strip are accepted if others wish to take thetest; for grading purposes; however, the strip shouldnot be enlarged or reduced.)
3. Mail completed answer strip with $10 testing fee or program coupon to:
JEMS COMMUNICATIONS525 B ST., STE. 1900
SAN DIEGO, CA 92101-4495ATTN: MYWEBCE
800/266-5367 TOLL-FREE PHONE
4. Within six weeks, you will receive your test score and,if you passed, a CE certificate.The passing score is 70%.
5. Please retain all course materials for future reference.
AnswersMark your answers in the appropriate box (1–20) (��)Paramedics graded on 1–20 (required),6 errors = fail. EMTs and others are graded on ques-tions 1–15 (16–20 corrected FYI), 4 errors = fail.
1. �� a. �� b. �� c. �� d. 11. �� a. �� b. �� c. �� d.
2. �� a. �� b. �� c. �� d. 12. �� a. �� b. �� c. �� d.
3. �� a. �� b. �� c. �� d. 13. �� a. �� b. �� c. �� d.
4. �� a. �� b. �� c. �� d. 14. �� a. �� b. �� c. �� d.
5. �� a. �� b. �� c. �� d. 15. �� a. �� b. �� c. �� d.
6. �� a. �� b. �� c. �� d. 16. �� a. �� b. �� c. �� d.
7. �� a. �� b. �� c. �� d. 17. �� a. �� b. �� c. �� d.
8. �� a. �� b. �� c. �� d. 18. �� a. �� b. �� c. �� d.
9. �� a. �� b. �� c. �� d. 19. �� a. �� b. �� c. �� d.
10. �� a. �� b. �� c. �� d. 20. �� a. �� b. �� c. �� d.
CE Answer Sheet #199Smoke Inhalation & Acute Cyanide Poisoning
MyWebCE.com is separate from, but related to, the print CE program.Thiscourse will be adapted for the Web and posted within 30 days. However, youcannot take this print CE test online or submit it via the myWebCE site.
ContinuingEducation That’sConvenient &AffordableCE CREDITS: EASY TO EARN—EASY TO AFFORD
Earn CE credits in the comfort of your own home. MyWebCE makes iteasy and affordable.Simply read the CE article,answer the accompanyingquestions and send in the answer sheet. The test is worth 1.5 hours ofcredit approved by the Continuing Education Coordinating Board forEMS.Take one test at a time for $10 each, or save and earn faster CE byvisiting myWebCE.com.
Send the completed test with your payment of $10,or one CE coupon,to:
Jems Communications,525 B St., Suite 1900, San Diego, CA 92101-4495
ATTN: myWebCE
Name
Title
Address
City State ZIP
Phone
Total payment ❏ Visa ❏ MasterCard ❏ Discover
Acct. # Exp. Date
Signature
❏ My check is enclosed, payable to Jems Communications
EMD 08/04
( )
$
For faster CEU, visit www.myWebCE.com.With real-time testing & grading,
your certificate is only a click away!

18 JEMS COMMUNICATIONS
THE PROBLEM IS THATthe Taylor kit has its limitations.The Taylor kit, a multicomponentkit consisting of inhaled amylnitrite, IV sodium nitrite and IVsodium thiosulfate, may be associ-ated with such effects as severehypotension, vomiting and methe-moglobinemia formation, whichresults in a reduction of the blood’soxygen-carrying capacity. The lattereffect, in particular, precludes theuse of the Taylor kit in most smoke-inhalation victims. In addition tobeing a source of cyanide poison-ing, smoke inhalation is almostalways associated with concomitantcarbon monoxide poisoning, a statecharacterized by deficient bloodoxygenation. Like carbon monox-ide, the amyl nitrite and sodiumnitrite found in the Taylor kit aremethemoglobin formers, whichreduce oxygenation of the blood.
When added to the blood oxygen-depriving effects of carbon monox-ide poisoning, antidote-inducedreductions in the oxygen-carryingcapacity of smoke-inhalation vic-tims’ blood can be dangerous andpossibly fatal.
Because of this potential toxicity,the Taylor kit is rarely used to treatsmoke-inhalation victims and isadministered only when cyanidepoisoning is confirmed by a labora-tory or very strongly suspected viadirect evidence of cyanide exposureor ingestion. Further, its use is oftenrestricted to hospital settingsbecause of the demands of manag-ing potentially dangerous antidote-associated side effects. The cyanideantidotes dicobalt-EDTA and 4-dimethylaminophenyl are availablein Europe; however, they, like theTaylor kit, are associated with somesignificant safety concerns.
HYDROXOCOBALAMIN:Treatment for SmokeInhalation-AssociatedCyanide Poisoning
HYDROXOCOBALAMIN:Treatment for SmokeInhalation-AssociatedCyanide Poisoning
Meeting the Needs of Fire VictimsBY J. L. FORTIN, MD, M. RUTTIMAN, MD, L. DOMANSKI, MD, & J. J. KOWALSKI, MD
The United States lacks a cyanide antidote useful for smoke-inhalation victims when cyanide toxicity is suspected on the basis of physical symptomsbut is unconfirmed by laboratory assay—arguably the most common occurrence ofacute cyanide poisoning. However, hydroxocobalamin, a cyanide antidote with a favor-able history of usage by the Paris (France) Fire Brigade, may offer a treatment optionsuperior to that which is currently available in the United States. The cyanide antidotekit made by Taylor Pharmaceuticals (also known as the Pasadena kit or the Lilly kit forthe company that originally made it) is the only currently available cyanide antidote inthe United States.

HYDROXOCOBALAMINThe cyanide antidote hydroxocobal-amin (Cyanokit™, Merck-Santés.a.s.) is being studied for possibleintroduction in the United States toaddress the unmet need for a safeand effective antidote that may beused empirically for victims ofsmoke inhalation as well as for othersources of cyanide poisoning.Hydroxocobalamin, a precursor ofvitamin B12 (see figure p. 20), neu-tralizes cyanide by fixing it to formcyanocobalamin (vitamin B12), anontoxic compound that is eliminat-ed in the urine.
Hydroxocobalamin has beenapproved for use in France sincemid 1996 and appears to be verywell tolerated, even at the highdoses necessary to treat cyanide poi-soning. To date, it has no knownmajor toxicities, and when adminis-tered acutely as a cyanide antidote, ithas not been associated with anyclinically relevant adverse events.However, it should be noted that theFDA has requested an additionalsafety study in human volunteers.
Because the molecule is red incolor, hydroxocobalamin turnsmucous membranes, skin and urinered, and it may interfere with somespecific colorimetric clinical labora-tory values, including aspartateaminotransferase, total bilirubin,creatinine and magnesium. No aller-gic reactions have been documentedto the antidote administration; how-ever, chronic use of small doses ofhydroxocobalamin for vitamin B12deficiency has been associated withrare allergic responses.
Hydroxocobalamin has a historyof clinical use for decades in coun-tries other than the United States.Merck-Santé s.a.s. commerciallyregistered hydroxocobalamin as anantidote for acute cyanide poisoningin France in 1996; however, it wasprepared and used by multiple hos-pital pharmacies in France for sev-eral years prior to that time. It hasalso been used and studied as acyanide antidote in other Europeancountries, such as Spain, where it isconsidered to be an effective anti-dote for cyanide toxicity from any
source or route. Other publishedtherapeutic uses of hydroxocobal-amin include its use in treatment ofpernicious anemia, hepatic insuffi-ciency, encephalopathy, neuropathy,amblyopia and various neuropsychi-atric syndromes.
Hydroxocobalamin is commer-cially available in Europe asCyanokit™. According to its label-ing, each kit includes two vials of 2.5g hydroxocobalamin lyophilizate forreconstitution with 100 mL salineper vial before use and two steriletransfer kits.The initial adult dose ofhydroxocobalamin is typically 5 gintravenously.Additional doses of upto 15 g can be given according to theclinical status of the patient per thelabeling. The dosing instructions forhydroxocobalamin in the UnitedStates (should the antidote beapproved as anticipated) have yet tobe established.
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 19
In addition to expected supportive care, victims of smoke-inhalation from structural fires in the United States may benefitfrom prehospital treatment with hydroxocobalamin, which is routinely administered in the field to smoke-inhalation victims of structural or enclosed-space fires in France.
Pho
to G
len
E. E
llman
Carbon Monoxide Hydrogen Cyanide• Neurological alteration• Normal respiration
• Neurological alteration• Respiratory frequency
disturbance or apnea
SYNERGISTIC EFFECTS
The Taylor kit may be associatedwith such effects assevere hypotension,vomiting & methemoglobinemiaformation, whichresult in a reduction of the blood’s oxygen-carryingcapacity.
PARIS FIRE BRIGADE USE OFHYDROXOCOBALAMINThe Paris Fire Brigade comprises7,020 firefighters divided among 77fire stations and responds to morethan 18,000 fire-related incidentsannually. The department serves 759square kilometers (roughly 450square miles) with a population ofmore than 6 million.To meet the pop-ulation’s needs, the Paris Fire Brigadeemploys 50 doctors who specialize inemergency medicine, 60 nurses and36 intensive-care ambulance driverswho operate seven intensive-careambulances. Each intensive-caremobile unit has one doctor, one nurseand one driver on board. Hydroxo-cobalamin is part of the Paris FireBrigade’s standard treatment protocolfor cyanide poisoning victims.
CIRCUMSTANCES OF ACUTEHYDROGEN CYANIDE POISONINGIN FIRESHydrogen cyanide is frequently asso-ciated and acts synergistically withcarbon monoxide in cases of smoketoxicity in structural or enclosed-space fires where degrading syntheticor natural substances release cyanide.The synergistic adverse interaction ofhydrogen cyanide with carbonmonoxide should not be underesti-mated.This interaction can result in areduction of respiratory frequency,even apnea, as well as hypotension
and possibly a state of shock. In addi-tion, hydrogen cyanide poisoning isresponsible for a deterioration of theneurological state. An increase in lac-tate, in particular, is related to hydro-gen cyanide poisoning associated withcarbon monoxide toxicity, because thebody makes a compensatory switch toanaerobic metabolism.
PARIS FIRE BRIGADE STUDY:PRELIMINARY DATAHydroxocobalamin is routinelyadministered in the field to smoke-inhalation victims of structural orenclosed-space fires in France. Theprehospital use of hydroxocobalaminby the Paris Fire Brigade over a five-year period from January 1998 toDecember 2002 was evaluated in aretrospective study. Some data fromthis study are available, and data col-lection and analysis are ongoing.
According to a preliminary reviewof the data, 70 of the 81 patients (41males and 40 females) treated withhydroxocobalamin (usually at a doseof 5 g or 70 mg/kg) recovered cardiacand/or respiratory function at the firescene, and 11 died. In a subset of 29patients in cardiac arrest beforehydroxocobalamin administration, 18patients spontaneously recoveredcardiac activity following hydroxo-cobalamin and adrenalin administra-tion (plus other supportive care) in anaverage time of 19.3 minutes. Elevenpatients receiving hydroxocobalaminand adrenalin died at the fire scene.No side effects attributed to hydroxo-cobalamin were reported.This result-ed in a 62.1% survival rate followinghydroxocobalamin administration inconjunction with the expected sup-portive care.
Of the subset of 15 hemodynami-cally unstable patients, 12 hadrecovery of systolic blood pressureto >90 mmHg in 29 minutes, on aver-age, after the end of hydroxocobal-amin infusion. Rapid recovery ofsystolic blood pressure wasobserved even in severely hypoten-sive patients. These data suggestthat hydroxocobalamin mayimprove hemodynamic stability insmoke-inhalation victims. Thispotential hemodynamic-stabilizing
20 JEMS COMMUNICATIONS
FIGURE. Hydroxocobalamin is the precursor of vitamin B12.
Conclusions Basedon PreliminaryDATA FROMPARIS FIREBRIGADE• Hydroxocobalamin appears
to be a safe, effectivecyanide antidote suitablefor prehospital use for acutecyanide poisoning causedby smoke inhalation.
• An effective dose is 5 g (70mg/kg) intravenously.
Hydroxocobalamin,a precursor of vitamin B12,neutralizescyanide by fixing it to formcyanocobalamin(vitamin B12), anontoxic compoundthat is eliminated in the urine.

SMOKE INHALATION & HYDROGEN CYANIDE POISONING 21
Hydroxocobalamin has been approved for use in France since mid1996 and appears to be very well tolerated, even at the high dosesnecessary to treat cyanide poisoning.
In a subset of 29patients in cardiacarrest beforehydroxocobalaminadministration,18 patients spontaneouslyrecovered cardiac activityfollowing hydroxocobalamin& adrenalinadministration(plus other supportive care) in an average timeof 19.3 minutes.
property of hydroxocobalamin dif-ferentiates it from the cyanide anti-dote kit currently available in theUnited States, which can causesevere hypotension. The hemody-namic-stabilizing property ofhydroxocobalamin may be particu-larly important in the prehospitalsetting, where rapid attainment ofhemodynamic stability is crucial forsaving lives and enabling timelytransport to the hospital.
CONCLUSIONSAccumulating data from an ongoingstudy on the prehospital use ofhydroxocobalamin for cyanide poi-soning suggest that it has a favorablerisk-benefit ratio and a reasonablesafety profile. Hydroxocobalamin at adose of 5 g appears to be effectiveand safe in smoke-inhalation vic-tims, as empiric treatment and asprehospital treatment.With this pro-file, hydroxocobalamin may be capa-ble of fulfilling the currently unmetneed in the United States for acyanide antidote that can be admin-istered safely in the prehospital set-ting as empiric therapy for smokeinhalation as well as the range ofcauses of cyanide poisoning.
Lead researcher Jean-Luc Fortin,MD, is the chief of medicine, third divi-sion, of the Paris Fire Brigade, one of thelargest urban fire-and-rescue depart-ments in the world. Fortin is also an aux-iliary physician in the intensive-care burnunit at the Army Teaching Hospital ofPercy in Clamart, France. Before joiningthe Brigade in 1999, Fortin was an emer-gency physician at the University HospitalCenter of Timone Emergency Medical AidService in Timone, France. He also servedas an emergency physician for the Frenchmilitary as Director of Medical Care in theNavy Battalion Fire Brigade of Marseille(ambulance, emergency and intensivecare service), and as an intensive-carephysician at the Renee Le Bas ArmyHospital Center in Cherbourg, France.Fortin received two inter-university diplo-mas—one in subaquatic and hyperbaricmedicine in 1993 and another in highereducation in emergency medicine in 1999.He received university diplomas in burncare and treatment, pediatric emergenciesand radiological evaluation of medical/surgical emergencies. He is licensed inemergency medical assistance, cata-strophic medicine, and aeronautical andspace medicine.
Additional researchers: M.Ruttiman,MD,L. Domanski, MD, and J.J. Kowalski, MD.

22 JEMS COMMUNICATIONS
OTHER RECENT INCIDENTS inwhich cyanide was used butreceived little press attentioninclude the 1995 Tokyo subwayattack, where the precursors ofcyanide were found in the subwaybathrooms;1 the foiled 2002 al-Qaeda attempt to use cyanide gas tokill commuters in the LondonUnderground;2 the 2002 arrests offour Moroccans (again with ties toal-Qaeda) who were plotting to usecyanide to poison water suppliesaround the U.S. embassy in Rome;3
the December 2002 recovery of acyanide store in Paris linked to threesuspected al-Qaeda operatives;4
and, most recently, the May 2003cyanide bomb found in the posses-sion of white supremacists in Texas.5
Although these events were thwart-ed, it’s not difficult to envision a suc-
cessful attack, particularly when wetake into account the variouscyanide delivery methods availableto terrorists.
Cyanide differs from many otherbiological or chemical agents forwhich little or no defense is available in that its individual andpublic-health effects are largelyremediable through appropriatepreparedness and response. Thisarticle discusses cyanide as a poten-tial chemical terrorism weapon,cyanide sources, the attributes that
CYANIDE ASA CHEMICALTERRORISMWEAPON
CYANIDE ASA CHEMICALTERRORISMWEAPON
“Chance favors the prepared mind.”—Louis Pasteur
BY MARC ECKSTEIN, MD, FACEP
Several recent incidents in which cyanide was intended for useas a weapon of terror should cause emergency services personnel to pause and careful-ly consider the potential consequences. For example, many are unaware that cyanide wasused during the 1993 World Trade Center bombing. In the aftermath, investigators foundtraces of cyanide in the vans in the parking garage that caused the explosion.Fortunately, the cyanide burned up in the explosion.1
Fire smoke is an often-overlookedsource of cyanide exposure in terrorist bombings. Following thefirst World Trade Center bombing in 1993, investigators found tracesof cyanide in the vans where theexplosion in the parking garageoriginated.
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 23
AP
/Wid
e W
orld
Pho
tos

make it an attractive terrorism tooland recent history of its use orplanned use as a terrorist weapon.In addition, strategies will be dis-cussed for enhancing preparednessfor a cyanide disaster. Current man-agement of acute cyanide poisoningis considered in the context ofCenters for Disease Control andPrevention (CDC) recommendationsfor preparedness for chemicalattacks.
U.S. governmental agencies,including the CDC and theDepartment of Homeland Security,consider cyanide among the mostlikely agents of chemical terror-ism.6,7 Other main categories ofchemical weapons include nerve,blister and pulmonary agents. Oneof the most rapidly acting poisons,cyanide shares several character-istics of other chemical agents,such as sarin and chlorine, thatrender it a useful and effective toolfor terrorists.8-12
Among many in the military,cyanide continues to be known as ablood agent. This term, which is out-dated and somewhat misleading,originated from the perception thatcyanide is carried in the blood andthat its primary site of action is thebloodstream. Although cyanide iscarried in the blood, so too are otherchemical weapons, includingabsorbed nerve agents. Therefore,the term does not differentiatecyanide from other categories of
chemical weapons. Also, cyanide’sprimary site of action is not neces-sarily the bloodstream.
CYANIDE SOURCESCyanide exists in several forms,including the gases hydrogen cyanideand cyanogen chloride, solublecyanide salts and insoluble cyanidesalts.13,14 Both gaseous and solidforms are used in industry. Cyanideis used in the recovery of gold andsilver from mineral ores and of sil-ver from photographic materials; inthe production of plastics, pigmentsand dyes; and as a pesticide.13,1
Moreover, hydrogen cyanide isreleased as a combustion productduring the combustion of plasticsand other polymers, silks, wood, cot-ton and many other nitrogen-con-taining substances.
Most literature on cyanide as aterrorist weapon focuses on the pos-sibility of the intentional release ofhydrogen cyanide gas into enclosedspaces, such as office buildings orstadiums.10-12 Exposure to hydrogencyanide via inhalation of fire smoke,the most common source of cyanidepoisoning in the United States, couldalso occur during a terrorist attack.Cyanide salts introduced into phar-maceuticals, the food supply and thewater supply also pose a terroristthreat.
Fire smoke is often overlooked asa source of cyanide exposure in aterrorist attack. Insofar as a terroristattack involves explosions and/orfire, cyanide is likely to be involved.In fact, given the frequency withwhich terrorist attacks involve fire,fire smoke is arguably the most like-ly source of cyanide in a terroristattack. Release of hydrogen cyanideas a combustion product in closed-space fires should be consideredamong the probable outcomes ofany terrorist attack involving fire inan enclosed structure or vehicle.
THE IDEAL WEAPONWhat makes cyanide an attractiveterrorist weapon? To be most usefulto a terrorist, a chemical agentshould be plentiful and readilyavailable and should not require
24 JEMS COMMUNICATIONS
Agents ofCHEMICALTERRORISMBlood agents
• Hydrogencyanide
• Cyanogenchloride
Nerve agents
• Tabun
• Sarin
• Soman
Blister agents
• Lewisite
• Nitrogen and sulfur mustards
Pulmonaryagents
• Phosgene
• Chlorine6,10
CYANIDE &INDUSTRYCyanide is commonly found inindustry settings, including:
• Fumigating, electroplatingand mining operations; and
• Synthetic fiber, plastic,polymer, dye and pesticide production.
Cyanide is also a common by-product from the combustion of:
• Carbon- and nitrogen-containing synthetic substances; and
• Natural substances,such as wood, silk and cotton.1,13-14
Cyanide is easilyobtainable byvirtue of itswidespread usein industry &researchlaboratories.

special knowledge to use. With theseattributes, the terrorist does notneed to spend significant time orresources in procuring or preparingto use the weapon and can procurethe weapon while arousing minimalnotice or suspicion. In addition, achemical agent should be capable ofaccomplishing terrorists’ primarygoals of causing mass incapacitationand casualties as well as causingmass confusion, panic and socialdisruption. Finally, the ideal terrorweapon would require large quanti-ties of specific resources to combatits effects—a feature associated withthe reduced likelihood of adequatedefense preparations.6,10
Cyanide possesses all of theseattributes. First, it is plentiful andreadily available. Each year, theUnited States produces approxi-mately three-quarters of a milliontons of cyanide. Cyanide is easilyobtainable by virtue of its wide-spread use in industry and researchlaboratories. It is transported bytruck and rail, both of which are sus-ceptible to theft, hijacking attemptsand other terrorist acts that couldculminate in use of cyanide as aweapon.
Second, cyanide does notrequire special knowledge to use.Unlike some biological or chemicalweapons that require specific tech-nological or scientific proficiencyfor effective use, cyanide incidentscan be planned and implementedsuccessfully by individuals withoutspecific expertise or training.
Third, cyanide is capable ofcausing mass incapacitation andcasualties.
Fourth, cyanide is capable ofcausing mass confusion, panic andsocial disruption.
Symptoms of cyanide poisoningare often dramatic and include stu-por, seizures and coma. In a terroristattack, these dramatic effects ofcyanide poisoning may occur in theabsence of an immediately localiz-able source of cyanide. The dramaticpresentation of cyanide poisoning,its lethality and the difficulty inlocalizing its source during an emer-gent terrorist incident contribute to
the potential use of cyanide to createpanic, confusion and social disrup-tion during a cyanide-related terror-ism event.
Finally, cyanide poisoning requireslarge quantities of specific resourcesto combat its effects. Moderate tohigh concentrations of cyanide canbe expected to cause death in themajority of victims unless a cyanideantidote is quickly administered.Public health readiness for a large-scale cyanide disaster would entailstockpiling sufficient quantities ofcyanide antidote. Correspondingly,effective use of cyanide as a terroristweapon is predicated on the lack ofavailability of large quantities ofantidote that can be rapidly dissemi-nated and administered to affectedindividuals.
HISTORICAL USESThe recent history of cyanide’s actu-al and intended use in intentionalpoisoning illustrates its utility as aweapon. Cyanide has been used as amurder weapon, as a poison in indi-vidual and mass suicides andattempted genocide, as a weapon ofwar and in recent attempted terror-ist incidents (described at the open-ing of this article). The range of set-tings in which cyanide has beenused and its various modes of deliv-ery illustrate its versatility as aweapon.The terrorist plots involvingcyanide also suggest that it’s animportant component of modernterrorists’ armamentarium.2-5,9,15-17
Cyanide was used as a murderweapon several times in the past twodecades in the United States. In themost notorious of these events,
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 25
Attributes of anIDEAL TERRORIST WEAPON
Cyanide possesses every one of these characteristics.6,10
• Plentiful;
• Readily available;
• Does not require a lot of
special knowledge to use;
• Capable of causing massincapacitation and casualties;
• Capable of causing mass confusion, panic and socialdisruption;
• Requires large quantities ofspecific resources to combatits effects.
Given the frequency withwhich terroristattacks involvefire, fire smoke is arguably the most likelysource of cyanide in a terrorist attack.

seven Chicagoans were killed in1982 when they took cyanide-taint-ed Extra Strength Tylenol® capsules.Other incidents of cyanide’s use as amurder weapon involved beverages(Vanilla Coke®) and food (LiptonCup-A-Soup®).
Cyanide was also used to commitmass suicide in Jonestown, Guyana,where 913 followers of the ReverendJim Jones died after drinkingcyanide-spiked Kool-Aid®. As anagent of genocide, cyanide (asZyklon B) was used to kill gas cham-ber victims in concentration campsduring World War II.
Cyanide has also been used as aweapon of war, although its militaryusefulness is limited by its highvolatility, which results in rapidevaporation and dispersion, and itsrelatively high lethal dose comparedwith that of such agents as sarin.Cyanide was used as a war weaponduring WWI and, allegedly, WWII.The Iraqis also allegedly usedcyanide against the Kurds in the1980s.9
Cyanide poisons cells by pre-venting them from using oxygen,an effect that causes them to relyon anaerobic metabolism (i.e., oxy-gen-independent metabolism, asopposed to the usual oxygen-dependent metabolism), whichcauses accumulation of toxicbyproducts. Accordingly, organsmost susceptible to cyanide toxicityinclude the heart and brain, whichnormally rely on a substantial anduninterrupted oxygen supply.
Clinical manifestations of cyanide
poisoning primarily reflect theeffects of oxygen deprivation on theheart and brain and are dependenton the route of exposure and severityof exposure. The onset of signs andsymptoms typically occurs seconds tominutes after exposure, and deathcan occur within minutes after mod-erate to high levels of exposure.13,20
MANAGEMENT OF ACUTECYANIDE POISONINGPrehospital management of acutecyanide poisoning involves movingthe victim from the source of expo-sure and providing supportive care,including administering 100% oxy-gen, providing cardiopulmonarysupport and stabilizing vital signs.When clinically indicated, anticon-vulsants are given for seizures, epi-nephrine and antiarrhythmics tostabilize cardiovascular function,and sodium bicarbonate to correctmetabolic acidosis.
Supportive care is necessary butusually insufficient to save the livesof cyanide poisoning victims; anantidote must also be given tocounter the cellular effects of thetoxin. Like supportive care, the anti-dote must be administered withinminutes of exposure to moderate tohigh concentrations of cyanide inorder to be effective.1,21-22
PREPARING FOR A CYANIDE ATTACKBy disabling the blood’s mechanismfor carrying oxygen, cyanide can killquickly. At moderate to high concen-trations of exposure, victims are
26 JEMS COMMUNICATIONS
SOURCES OFCYANIDEEXPOSURE in aTerrorist Attack• Hydrogen cyanide gas
released into an enclosedspace (e.g., a stadium or an office building);
• Fire smoke;
• Cyanide salts in the water supply;
• Cyanide salts in food;and/or
• Cyanide salts in pharmaceuticals.10-12
Recent History:Cyanide as a Murder Weapon
1982: Seven Chicagoans killed
1986: One person killed
1991: Two people killed
1992: One person killed
2003: One Maryland teenager killed
Cyanide as an Agent of Mass Suicide
1978: Jonestown, Guyana, 913followers of the Reverend JimJones committed suicide withcyanide-spiked Kool-Aid®.
Cyanide as an Agent of Genocide
World War II: Cyanide (as Zyklon B) was used in the gas chambers in concentrationcamps.
Cyanide as a Weapon of War
World War I: France usedapproximately 4,000 tons ofcyanide.
World War II: Japan allegedlyused cyanide against China.
World War II: United Statesmaintained cyanide munitions.
1980s Iraqi aggression: Iraqallegedly used cyanide againstthe Kurds.9

incapacitated within seconds tominutes, and death can occur withinminutes. Unlike illness or toxicitycaused by many other biological andchemical weapons, cyanide poison-ing can be effectively treated.Because it progresses so quickly andbecause no diagnostic test can con-firm cyanide poisoning in the timerequired for initiating intervention,cyanide poisoning must be diag-nosed presumptively by firstresponders on scene at a terroristattack. Rapid recognition andempiric intervention by first respon-ders are crucial to saving lives andreducing morbidity.18-19
In 2000, a CDC taskforce collabo-rated with other groups to publishstrategic recommendations for pre-paredness for and response to bio-logical and chemical terrorism. Thetaskforce concluded that prepared-ness for terrorist attacks constitutesa critical component of the U.S. pub-lic health surveillance and responsesystem, and they identified fiveactivities that local, state and federalpublic health organizations shouldundertake in order to enhance pre-paredness for chemical attacks. Forthe United States to be prepared fora chemical attack involving cyanide,public health organizations need todevelop action plans for and allocateresources to each of these prepared-ness activities.6
All of the activities outlined bythe CDC taskforce apply to enhanc-ing readiness for chemical terrorisminvolving cyanide. However, pre-paredness initiatives involvingcyanide antidotes warrant particu-lar attention because, at present, theavailability of cyanide antidotes iswholly inadequate to meet thenation’s needs. The United Statescurrently lacks an antidote with arisk-benefit ratio that favors empir-ic administration at the scene of adisaster.1
INADEQUACY OF CURRENTPREPAREDNESSWith appropriate preparedness, thepublic health threat posed by acyanide attack can be contained toan extent. Containment is possible
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 27
Cyanide was used to commit mass suicide in Jonestown, Guyana,where 913 followers of the Reverend Jim Jones died after drink-ing cyanide-spiked Kool-Aid®.
PLANNING PARAMETERS to ConsiderThere are several parameters emergency respondersshould consider when preparing for a cyanide attack:• Cyanide kills quickly by disabling the blood’s mechanism for
carrying oxygen;
• It can incapacitate victims within seconds to minutes;
• It causes death within minutes following moderate to high levels of exposure;
• Unlike illness or toxicity caused by many other biological orchemical agents, cyanide poisoning can be effectively treated; and
• Rapid recognition and empiric treatment by emergency responders are necessary to reduce a chemical attack’s impact on individuals and the public health system.18,19
AP
/Wid
e W
orld
Pho
tos

in part because signs and symptomsof poisoning manifest instanta-neously and dramatically afterexposure to moderate to high levelsof cyanide, and they elicit the imme-diate attention of medical personneland emergency responders trainedto recognize chemical poisoning.The absence of significant delaybetween cyanide exposure and theonset of obvious, attention-com-manding signs and symptomsenhances the probability thatcyanide poisoning will be recog-nized—a prerequisite for initiatingeffective intervention. Unlikecyanide, many other poisons andtoxins are associated with a delayedonset of illness and, corresponding-ly, a delay in diagnosis and interven-tion. The fact that an effective antidote exists differentiatescyanide from many other chemicaland biological weapons that have noknown effective countermeasure.1
THE CYANIDE ANTIDOTE KITOf several cyanide antidotes availablearound the world, only one, thecyanide antidote kit, is presently mar-keted in the United States. Thecyanide antidote kit includes threecomponents that are to be adminis-tered sequentially: amyl nitrite, sodi-um nitrite and sodium thiosulfate.The amyl nitrite (available as pearls)is administered via a mechanical ven-tilation device or by gauze sponge forinhalation to stabilize the victim dur-ing the time before an IV line can be
established. The sodium nitrite andthiosulfate are administered intra-venously. Sodium nitrite and amylnitrite neutralize cyanide by bindingwith it to form methemoglobin.Problematically, nitrite-inducedmethemoglobinemia reduces theblood’s ability to carry oxygen andthus constitutes a dangerous, poten-tially fatal toxic state. In addition tocausing methemoglobinemia, thecyanide antidote kit may cause severehypotension leading to shock. Theseliabilities contribute to a sub-optimalrisk-benefit ratio of the cyanide anti-dote kit in empiric prehospital treat-ment of cyanide poisoning.1
Methemoglobinemia is especial-ly dangerous for smoke-inhalationvictims, who often have concurrentcarboxyhemoglobinemia due tocarbon monoxide exposure. Bothcarboxyhemoglobinemia and methe-moglobinemia reduce the blood’soxygen-carrying capacity, and theadditive effects of the two condi-tions in smoke-inhalation victimscan be lethal. Some authorities,therefore, do not recommend thecyanide antidote kit for smoke-inhalation victims, who often haveconcurrent cyanide and carbon-monoxide poisoning, because of thepossibility of causing life-threaten-ing complications.23
IMPROVING PREPAREDNESS:HYDROXOCOBALAMINThe cyanide antidote kit’s potentialtoxicity and multiple-component
28 JEMS COMMUNICATIONS
CDC-RecommendedPREPAREDNESSMEASURES• Enhance epidemiologic
capacity for detecting andresponding to chemicalattacks;
• Enhance awareness ofchemical terrorism amongEMS personnel, police officers, firefighters,physicians and nurses;
• Stockpile chemical antidotes;
• Develop and provide bioassays for detection anddiagnosis of chemicalinjuries; and
• Prepare educational materials to inform the public during and after achemical attack.6
Cyanide ToxicitySmall amounts of cyanide aremetabolized in the liver andexcreted in the urine.Cyanide binds to iron (Fe+++)in the mitochondria, prevent-ing cells from using oxygen.Without oxygen, cells die. Theeffects are of progressive tis-sue hypoxia, and because theheart and brain are theorgans most sensitive tohypoxia, they are the firstorgans to be affected.
Acute Cyanide Poisoning Symptoms & SignsSymptoms• Nearly immediate loss of
consciousness;• Stupor;• Giddiness;• Palpitations;• Dizziness;• Nausea/vomiting;• Hyperventilation;• Drowsiness; and• Eye irritation.
Signs• Respiratory arrest;• Cardiac arrest;• Coma;• Seizures;• Pink or red skin color;• Elevated venous blood
oxygen concentration; and• Metabolic acidosis.13,20

administration renders it ill-suitedfor use in terrorist incident responseand other situations requiring rapidprehospital intervention. The Foodand Drug Administration is current-ly evaluating the cyanide antidotehydroxocobalamin for possibleintroduction in the United States. Aprecursor of vitamin B12, hydroxo-cobalamin is currently available inother countries, including France,where it is the cyanide antidote usedby the Paris Fire Brigade.
Hydroxocobalamin, which neu-tralizes cyanide by binding it to formvitamin B12, appears to be at least aseffective as the cyanide antidote kitin the treatment of cyanide poison-ing but does not appear to be associ-ated with the safety liabilities of the cyanide antidote kit.Hydroxocobalamin does not appearto induce methemoglobinemia orcause hemodynamic instability. Itsmost common side effects arethought to include discoloration ofurine and mucous membranes andabnormalities in specific laboratorytests. These effects are transient(lasting one to two days) and do notappear to reflect clinically meaning-ful changes.
From the literature, the safetyrisks of administering hydroxo-cobalamin appear to be negligible,and the antidote in France is admin-istered at disaster scenes so thatintervention is not delayed untilhospital care can be provided.Further, because of its favorablerisk-benefit ratio, as reported in theliterature, hydroxocobalamin neednot be reserved for cases of con-firmed cyanide poisoning but can beadministered in cases of suspectedpoisoning. Both of these attributescould lead to more rapid initiation oftreatment than is possible with thecurrently available cyanide antidotekit and, thereby, could improve out-comes in a cyanide disaster.1,13-14,23-25
In other countries, hydroxocobal-amin is recognized as an efficacious,safe and easily administeredcyanide antidote with an extremelylow adverse effect profile suitablefor prehospital use in suspectedcyanide intoxication. According to
expert opinion, in order to effectivelyprepare for a cyanide disaster, theUnited States should investigate,adopt, manufacture and stockpilehydroxocobalamin to prevent need-less morbidity and mortality.1
In a June 2001 paper assessingpublic health readiness for cyanidedisasters, authors Samual Sauer,MD, of the U.S. Army Medical Corpand The School of Public Health atthe University of Hawaii and MarkKeim, MD, of the CDC and theDepartment of Emergency Medicineat Emory University characterizedthe U.S. state of preparedness for acyanide disaster as abysmal. In thecontext of terrorists’ continuedinterest in the use of cyanide as aweapon, the need to implement
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 29
The United States currently lacksan antidotewith a risk-benefit ratio that favors empiric administration at the scene of a disaster.
Firefighters emerge after cleaning toxic gas-contaminated cars atTokyo's Kodemmacho subway station in March 1995. Although itreceived little press attention, the precursors of cyanide werefound in the subway bathrooms.
AP
/Wid
e W
orld
Pho
tos

the imperatives set forth by Sauerand Keim seems even more press-ing today than when their paperoriginally appeared.1
What would constitute adequatepreparedness for a chemical attack?First, antidotes that are effective andsafe for empiric prehospital useshould be made available in theUnited States. Progress has beenmade on that front since the time ofSauer and Keim’s paper in that reg-ulators are evaluating hydroxo-cobalamin for possible introductionin the United States.
To realize the potential benefitsof hydroxocobalamin, parallelprogress needs to occur in otheraspects of readiness, including butnot limited to developing plans forensuring local and regional avail-ability of antidote and educatingemergency responders and health-care professionals in the recogni-tion and management of cyanidepoisoning. Many U.S. hospitals cur-
rently stock one or fewer currentlyavailable cyanide antidote kits, andmany emergency responders andother health-care providers arepoorly informed in the use of theantidote and the recognition ofcyanide poisoning.
In conclusion, the recent history ofuse and planned use of cyanide sug-gests that a terrorist attack involvingcyanide is quite possible in the UnitedStates. Cyanide poisoning can betreated effectively if it is treatedquickly. The ability to manage acyanide attack’s effect on individualsand public health depends on thespeed of recognition and fast inter-vention. The potential introduction inthe United States of hydroxocobal-amin, an antidote with a promisingrisk-benefit ratio for empiric treat-ment, may help to enhance prepared-ness for a cyanide attack. However,progress is also necessary in otherareas, including educating emergencyresponders and health-care profes-sionals in the recognition and man-agement of cyanide poisoning, andraising public awareness of thepotential for a chemical weaponsattack and how to respond.
Marc Eckstein, MD, is the medicaldirector of the Los Angeles FireDepartment, an associate professor ofemergency medicine at the Keck School ofMedicine at the University of SouthernCalifornia and the director of prehospitalcare at Los Angeles County/University ofSouthern California Medical Center. A for-mer New York City paramedic, Ecksteinreceived his Doctor of Medicine from theMount Sinai School of Medicine in NewYork City. He holds numerous professionalcertifications, including an advanced oper-ations certification on weapons of massdestruction from FEMA, and serves as aninstructor in Chemical, Ordinance,Biological, Radiological Agent (COBRA)incident response with the Office ofDomestic Preparedness. He is a fellow ofthe American Board of EmergencyPhysicians and a member of several pro-fessional organizations, including theAmerican College of EmergencyPhysicians and the National Association ofEMS Physicians.
30 JEMS COMMUNICATIONS
The safety risks of administeringhydroxocobalaminare believed to benegligible, & theantidote is administered at disaster scenes so that intervention isnot delayeduntil hospital carecan be provided.
Any terrorist attack that involves explosions or fire in a structureor other enclosed space, such as a train, will likely involve therelease of hydrogen cyanide.
Pho
to G
len
E. E
llman
REFERENCES
1. Sauer SW, Keim ME:Hydroxocobalamin: improved publichealth readiness for cyanide disas-ters.” Annals of Emergency Medicine.37:635–641, 2001.
2. “M15 foils al-Qaeda’s London cyanideplot.” Sunday Herald. Nov. 17, 2002.www.sundayherald.com/print29314.Accessed Jan. 26, 2004.
3. “Cyanide plotters face terrorcharges.” 21 February 2002. BBC.http://news.bbc.co.uk/1/hi/world/europe/1833646.stm. Accessed Jan.26, 2004.
4. Cloud DS. “Long in US signs, a youngterrorist builds grim resume.” TheWall Street Journal. Feb. 10, 2004.
5. “Cyanide arsenal stirs domestic ter-ror fear.” Jan. 30, 2004. CNN.www.cnn.com/2004/US/Southwest/01/30/cyanide.probe.ap/index.html.Accessed Feb. 9, 2004.
6. Khan A, Levitt A, Sage M, et al:“Biological and Chemical Terrorism:Strategic Plan for Preparedness andResponse.” Morbidity and MortalityWeekly Report, Centers for DiseaseControl. 49(RR04):1–14, 2000.
7. “National terror alert: terrorism sur-vival guide-facts about cyanide.”National Terror Alert ResourceCenter. www.nationalterroralert.com/readyguide/cyanide.htm. AccessedJan. 26, 2004.
8. Agency for Toxic Substances andDisease Registry. US Department ofHealth and Human Services, PublicHealth Service. American FamilyPhysician. 48:107–114, 1993.
9. Chemical Casualty Care Division,Aberdeen Proving Ground, Md.“Cyanide AC, CK.” United States ArmyMedical Research Institute ofChemical Defense: MedicalManagement of Chemical CasualtiesHandbook, 3rd ed. The Virtual NavalHospital Project, 1997–2004.www.vnh.org/CHEMCASU/03Cyanide.html. Accessed Jan. 10, 2004.
10. Noeller TP. “Biological and chemicalterrorism: recognition and manage-ment.” Cleveland Clinic Journal ofMedicine. 68:1001–1016, 2001.
11. Martin CO, Adams HP Jr.:Neurological aspects of biologicaland chemical terrorism: a review forneurologists.” Archives of Neurology.60:21–25, 2003.
12. Greenfield RA, Brown BR, HutchinsJB, et al: “Microbiological, biological,and chemical weapons of warfareand terrorism.” American Journal ofMedical Science. 323:326–340, 2002.
13. Mégarbane B, Delahaye A,Goldgran-Toledano D, et al:“Antidotal treatment of cyanide poi-soning.” Journal of the ChineseMedical Association. 66:193–203,2003.
14. Borron SW, Baud FJ: “Toxicity,cyanide.” February 2003. www.emedicine.com/emerg/topic118.htm.Accessed Jan. 13, 2004.
15. Malkin M: “Borders, cyanide, andterrorism.” Creators Syndicate Inc.,2002. www.townhall.com/columnists/michellemalkin/mm20020529.shtml. Accessed Jan. 26, 2004.
16. “Cyanide poisonings associated withover-the-counter medication—Washington State, 1991.” Morbidityand Mortality Weekly Report.40(10):161,167–168, 1991.
17. Manning J: “The Tylenol murders.”The Eighties Club. http://eighti-esclub.tripod.com/id298.htm.Accessed Feb. 8, 2004.
18. Baskin SI, Brewer TH: In ZajtchukR, Bellamy RF (Ed.), Medical aspectsof chemical and biological warfare.Office of the Surgeon General,Department of Army, US, 1997. p.271–286.
19. Kales SN, Christiani DC. “Acutechemical emergencies.” NewEngland Journal of Medicine.350(8):800–808, 2004.
20. National Institute of OccupationalSafety and Health EmergencyResponse Card. www.bt.cdc.gov/agent/cyanide/erc74-90-8pr.asp.
21. Lee-Chiong TL: “Smoke inhalationinjury.” Postgraduate MedicalJournal. 105:55–62, 1999.
22. Koschel MJ. “Where there’s smoke,there may be cyanide.” AmericanJournal of Nursing. 102:39–42, 2002.
23. Hall AH, Kulig KW, Rumack BH:“Suspected cyanide poisoning insmoke inhalation: complications ofsodium nitrate therapy.” Journal deToxicologie Clinique etExpérimentale 9:3–9, 1989.
24. Baskin SI, Brewer TG: Zajtchuk R(ed). “Cyanide poisoning.” Textbookof Military Medicine: MedicalAspects of Chemical and BiologicalWarfare. Office of the SurgeonGeneral, United States Army,Washington, D.C., 1997.
25. Hall AH, Rumack BH: Annals ofEmergency Medicine. 15:1067–1074,1986.
SMOKE INHALATION & HYDROGEN CYANIDE POISONING 31





![Detecting Carbon Monoxide Poisoning Detecting Carbon ...2].pdf · Detecting Carbon Monoxide Poisoning Detecting Carbon Monoxide Poisoning. Detecting Carbon Monoxide Poisoning C arbon](https://img.pdfslide.net/doc/110x75/5f551747b859172cd56bb119/detecting-carbon-monoxide-poisoning-detecting-carbon-2pdf-detecting-carbon.jpg)