Embed Size (px)
Citation preview

Larry Collins, MPAS, PA-C, ATC, DFAAPA
Assistant Professor, Physician Assistant ProgramAssistant Professor, Department of Orthopaedics & Sports MedicineUSF Health, Morsani College of Medicine
General Considerations for
Intra-Articular Injections
and Joint Aspirations
So, this won’t hurt a bit, eh?

Disclosures
I have no real or apparent conflicts of interest to report

Guidelines
• Identify underlying etiology
• Advise patient of associated risks
• Aseptic technique
• Knowledge of local anatomy
• Avoid tracking steroid/anesthetic combo
• Avoid repeat injections

Indications
• Treatment of musculoskeletal conditions, injuries and pain
• Combined with activity modifications, other pharmacologic medications and rehabilitation

Indications
• Corticosteroids– Temporary relief of painful musculoskeletal
conditions
• Hyaluronic acid derivatives– Osteoarthritis
• Platelet-rich plasma (PRP)– Ligament tears, tendinopathies or tears and OA
• Stem Cells– Ligament tears, tendinopathies or tears and OA

Contraindications
ABSOLUTE
• Septic Joint
• Bacteremia
• Cellulitis
• Allergy
• Uncontrolled bleeding disorder
RELATIVE
• Diabetes
• Anticoagulant therapy
• Sickle cell anemia

Adverse effects
• Post-injection ‘flare’
• Steroid arthropathy
• Hemarthrosis
• Facial flushing
• Skin atrophy/depigmentation
• Iatrogenic infection
• Hypersensitivity reaction
• Elevation in blood sugar

Iatrogenic infection
• Hematogenous contamination of needle track
• Contamination of drug
• Introduction of bacteria from skin
• Activation of quiescent infection

Tips for success
• Identify inflammatory process• Discuss treatment options with patient• Obtain informed consent• Selection of appropriate medication(s)
in sufficient quantity• Patient positioning• Anatomic landmarks

Tips for success
• Sterile skin prep• Superficial anesthesia• Needle placement• Aspiration/injection at steady/constant
rate• Post-injection pressure• Post-injection instructions


NEVER TOUCH
Tip or Plunger
Aseptic Technique – Syringes

• Hub– Where needle attaches to
syringe tip
• Bevel– Tip of needle is slanted to a
point
– Bevel allows for smooth insertions through stoppers and ports with minimal coring
Aseptic Technique – Needles

• Coring – Development of a core
or hole in the rubber of a vial
– Prevent coring by inserting bevel tip first, then pressing downward and toward the bevel so bevel tip and heel enter at same point
Aseptic Technique – Needles

• Common needle sizes include• 18G 1 & 1½ inch
• 22G 1 & 1½ inch
• 25G 1 inch
• Proper disposal of all needles and syringes
Aseptic Technique – Needles

Vials Ampules
Aseptic Technique – Vials and Ampules

Anesthetic
Typical Concentration
Duration (hr) Maximum Dose (mg/kg)
Lidocaine 1%-2%10-20 mg/mL
0.5-3 3-5
Mepivacainehydrochloride
0.5%-1%5-10 mg/mL
1.5-3 4
Bupivacainehydrochloride
0.25%-0.5%2.5-5 mg/mL
4-24 1-2
Commonly Used Local Anesthetic Agents

Generic Name Trade Name Equivalent
Dose (mg)
Large Joint
(mg)
Small Joint
(mg)
Betamethasone sodium
phosphate
Celestone 0.6 12 6
Dexamethasone sodium
phosphate
Decadron 0.75 2 – 4 0.8 – 1
Triamcinolone diacetate Aristospan Forte 4 10 – 40 5 – 10
Methylprednisolone acetate Depo-Medrol 4 20 – 80 5 – 20
Hydrocortisone acetate Hydrocortisone 20 25 10 – 25
Dexamethasone acetate Decadron LA 0.75 5 – 15 4 – 5
Prednisolone acetate Predalone 5 10 – 25 5 – 10
Triamcinolone acetonide Kenalog 4 5 – 40 2.5 – 5
Triamcinolone hexacetonide Aristospan 4 10 – 20 2 – 6
Betamethasone sodium
phosphate – betamethasone
acetate
Celestone Soluspan 0.6 6 – 12 1.5 – 3
Most
Least
S
O
L
U
B
I
L
I
T
Y
Modified from Noerdlinger MA, Fadale PD. The Role of Injectable Corticosteroids in Orthopedics. Orthopedics. April, 2001.
Comparison of common corticosteroids

Surface anatomy of the shoulder
• Clavicle
• Acromion
– (anterior, lateral and posterior borders)
• A-C joint
• Coracoid process








Surface anatomy of the knee
• Patella
– (superior and inferior poles, medial and lateral borders)
• Patella tendon
– (medial and lateral borders)
• Tibial plateau
• Tibial tubercle







Surface anatomy – Lateral Elbow

Surface anatomy – Lateral Elbow
• Position patient prone or supine• Elbow flexed 45-90°• Mark landmarks of lateral triangle• Lateral olecranon• Lateral epicondyle• Radial head
• Insert at center of lateral triangle• Needle perpendicular angled towards
medial epicondyle• Aspirate prior to injection

Surface anatomy – Lateral Elbow
Pryor P, Mauck S and Adler K. Has This Laceration Compromised the Joint? http://epmonthly.com/article/has-this-laceration-
compromised-the-joint/. Accessed 7/28/2017.

De Quervain's
The Ultrasound Site. Obtained from https://theultrasoundsite.co.uk/de-quervains-tenosynovitis/. Accessed 8/1/2017.
• Maximally abduct thumb (accentuates abductor tendon)
• Inject at snuffbox near base of thumb in first dorsal wrist compartment
• Between Abductor pollicis longus and Extensor pollicis brevis

De Quervain's
Scott Moses - Family Practice Notebook - http://www.fpnotebook.com/_media/OrthoWristDequervains.jpg. Accessed 7/28/2017.

De Quervain's
• Angle needle 45° proximally toward radial styloid
• Insert needle between the 2 tendons• Move thumb
• Distal paresthesias with needle before steroid indicates needle at sensory branch of radial nerve Do not inject here! … withdraw and redirect needle 2-3 mm to either side

De Quervain's
Solomons, MW. (2015). Corticosteroid usage in hand and wrist surgery. SA Orthopaedic Journal, 14(2), 48-51.
https://dx.doi.org/10.17159/2309-8309

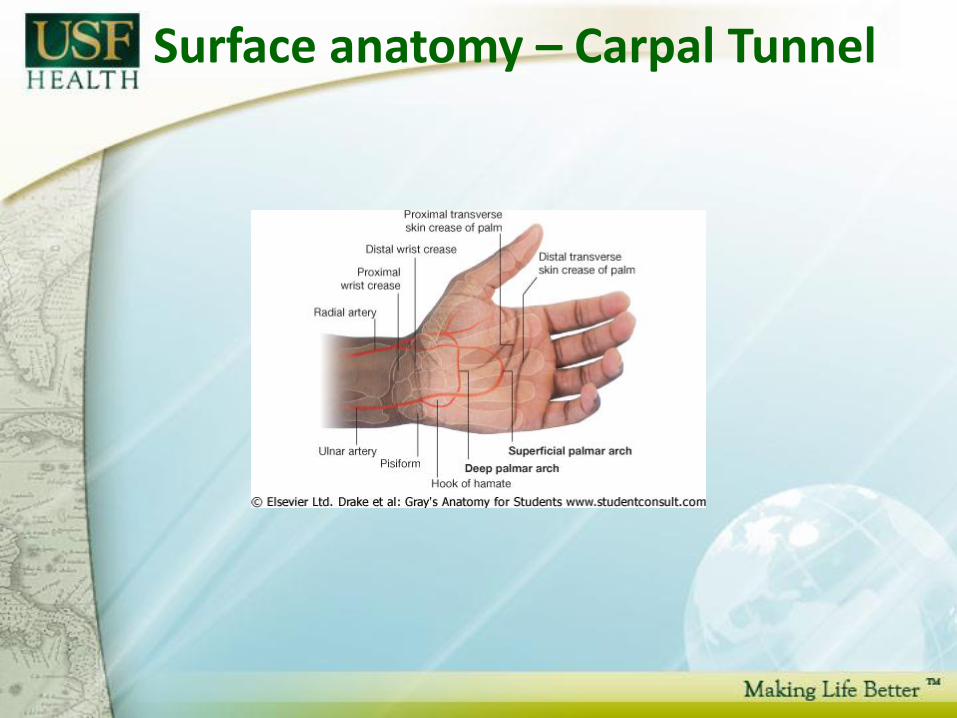
Surface anatomy – Carpal Tunnel
• Distal volar flexion crease• Crosses proximal end of the scaphoid &
pisiform• Identifies proximal edge of the
transverse carpal ligament• Pisiform palpable just laterally identifies
entry of ulnar nerve and artery into hand• Thenar & hypothenar muscles originate
from the transverse carpal ligament

Surface anatomy – Carpal Tunnel
Surface anatomy – Carpal Tunnel

Surface anatomy – Carpal Tunnel
• Dorsiflex wrist to 30°• Proximal wrist crease (or
1 cm proximal to most distal wrist crease)
• Ulnar side of Palmaris longus tendon (midline if palmaris longus absent)• Find by opposing
thumb with pinky

Surface anatomy – Carpal Tunnel
• Angle 30-45° distal – towards middle-ring finger
• Insert needle 1-2 cm until no resistance (nerve is very superficial)
• Distal paresthesias with needle before steroid indicates needle is at median nerve Do not inject here!
• Remove needle and replace further to the ulnar side

MCP
MCP
• Identify the joint line• Identify the extensor tendon passing over
the MCP joint• Extend the ray against resistance to help
identify the tendon• Mark entry site at the MCP joint, either
medial or lateral to the extensor tendon• Insert needle into joint• Distraction of thumb is helpful – assistant

MCP
Myers S. Hand Injection Techniques - Base of Thumb (Thumb CMC Joint) Osteoarthritis.
https://www.youtube.com/watch?v=wQfjVk7dM1k. Accessed 8/2/2017

Post-injection Instructions
• Avoid excessive activity for 24-48 hours
• Obtain full range of motion
• Apply ice regularly, 20-30 min/hr
• NSAID use for pain/inflammation
• Gradual return to activity after 48 hours
• Patient specific instructions
(i.e. diabetes, anti-coagulation therapy, etc)
Larry Collins, MPAS, PA-C, ATC, DFAAPA
Assistant Professor, Physician Assistant ProgramAssistant Professor, Department of Orthopaedics & Sports MedicineUSF Health, Morsani College of [email protected]
General Considerations for
Intra-Articular Injections
and Joint Aspirations
Questions?





























