Embed Size (px)
Citation preview

University of New MexicoUNM Digital Repository
Sociology ETDs Electronic Theses and Dissertations
8-25-2016
Social network characteristics as they relate to themental health of refugeesRichard Greene
Follow this and additional works at: https://digitalrepository.unm.edu/soc_etds
This Thesis is brought to you for free and open access by the Electronic Theses and Dissertations at UNM Digital Repository. It has been accepted forinclusion in Sociology ETDs by an authorized administrator of UNM Digital Repository. For more information, please contact [email protected].
Recommended CitationGreene, Richard. "Social network characteristics as they relate to the mental health of refugees." (2016).https://digitalrepository.unm.edu/soc_etds/17

Richard Neil Greene Candidate Department of Sociology Department This thesis is approved, and it is acceptable in quality and form for publication: Approved by the Thesis Committee: Dr. Jessica Goodkind, Chairperson Dr. Brian Soller Dr. Kristin Barker
i

SOCIAL NETWORK CHARACTERISTICS AS THEY RELATE
TO THE MENTAL HEALTH OF REFUGEES
by
RICHARD NEIL GREENE
B.A. UNIVERSITY OF RHODE ISLAND, 2003 M.A. EMERSON COLLEGE, 2010
THESIS
Submitted in Partial Fulfillment of the Requirements for the Degree of
Master of Arts
Sociology
The University of New Mexico Albuquerque, New Mexico
July 2016
ii

Dedication
I would like to dedicate this work to my loving family and supportive friends, colleagues,
and mentors. Thank you for lending your perspective, guidance, and encouragement.
iii

Acknowledgements
This study uses data from a larger NIMHD-funded R01 (PI Goodkind). I wish to express
my gratitude for the opportunity and good fortune to use this data. I am indebted to the
entire refugee well-being team. I appreciate your early feedback on my thesis proposal
and comments on various drafts along the way.
Thank you, Jessica Goodkind for helping me think through the big picture and small
details essential to this project. Thanks to Brian Soller and Deborah Bybee for helping me
think through social network measurement, syntax, and findings. Thank you, Kristin
Barker, too, particularly for pushing me to informally talk about my thesis proposal with
sociologists at the Science Knowledge and Technology conference—even when I didn’t
feel ready yet.
Much thanks to all of the study team interpreters. I would particularly like to thank Suha
Amer, Eric Ndaaheba, and Martin Ndayisenga for conducting so many of the quantitative
interviews and interpreting many of our qualitative interviews. Last but not least, a very
large thank you to all of the study participants. Thank you for sharing so much about your
experience resettling in the United States. It is hoped that this paper can be used, in some
way, to make things better for both those who are here now and those who will come in
the future.
iv

Social network characteristics as they relate to the mental health of refugees
R. Neil Greene
B.A., Psychology, University of Rhode Island M.A., Health Communication, Emerson College
Abstract
This study (N=168) builds on a long lineage of scholarly work connecting social
networks to mental health by exploring relationships between refugee social network
compositions—network size, proportion of same sex ties, proportion of same community
ties, and role heterogeneity—and self-reported symptoms of PTSD, depression, and
anxiety.
This study finds that newly resettled refugee social networks are small and social
isolation is common; approximately 30% of participants reported having no local social
network ties. For refugees with local social network ties, the composition of social
networks does appear to matter. Having more same sex ties was negatively associated
with higher mental health symptoms while having more role heterogeneity was positively
associated with higher mental health symptoms. Refugees’ level of exposure to trauma
and income satisfaction were also significantly related to increased mental health
symptoms.
Qualitative interview data contextualizes and expands on quantitative findings and
suggests that refugees have important social relationships with distant family and friends
and begin to build relationships within their local communities that can address problems
with isolation and mental health disparities.
.
v

Table of Contents
List of Figures ----------------------------------------------------------------------- vii
List of Tables ------------------------------------------------------------------------ viii
Introduction -------------------------------------------------------------------------- 1
Research Questions ----------------------------------------------------------------- 7
Hypotheses --------------------------------------------------------------------------- 7
Data Sources ------------------------------------------------------------------------- 7
Measurement ------------------------------------------------------------------------ 9
Analysis ------------------------------------------------------------------------------ 14
Quantitative Findings --------------------------------------------------------------- 15
Qualitative Findings ---------------------------------------------------------------- 26
Discussion ---------------------------------------------------------------------------- 36
Study Limitations ------------------------------------------------------------------- 40
Conclusion --------------------------------------------------------------------------- 41
Appendices --------------------------------------------------------------------------- 43
References --------------------------------------------------------------------------- 47
vi

List of Figures
Figure 1 Case example of a male participant with a high proportion of same sex ties ---------------------------------------------------------------------- 11
Figure 2 Case example of an Iraqi participant with a high proportion of same cultural community ties ------------------------------------------------- 11
Figure 3 Case example of high role heterogeneity ----------------------------- 12
Figure 4 Total Social Networks --------------------------------------------------- 17
Figure 5 Interaction effect for Model 4 ------------------------------------------ 24
Figure 6 Interaction effect for Model 8 ------------------------------------------ 24
Figure 7 Interaction effect for Model 12 ----------------------------------------- 24
vii

List of Tables
Table 1 Social Network by question and cross tabs by Sample Characteristics --------------------------------------------------------- 17 Table 2 OLS Regression of PTSD Symptoms ---------------------------------- 21
Table 3 OLS Regression of Depression ------------------------------------------ 22
Table 4 OLS Regression of Anxiety ---------------------------------------------- 23
Appendix A Summary Statistics -------------------------------------------------- 43 Appendix B Proportion of same sex ties and cross tabs by nationality, gender, and age group -------------------------------------------- 44 Appendix C Proportion same cultural community and cross tabs by nationality, gender, and age group -------------------------------------------- 45 Appendix D Role heterogeneity and cross tabs by nationality, gender, and age group -------------------------------------------- 46
viii

“Whenever serious readjustments take place in the social order, whether or not due to a sudden
growth or to an unexpected catastrophe, men are more included to self-destruction” (Durkheim
[1897]1966:246).
Refugee-like situations can be viewed as anomic—as disruptions or “disturbances in the
collective order.” By resettling for safety, refugees leave behind loved ones and cultural
familiarity. In addition, their new living spaces may be drastically different from what they have
known; familiar sights, sounds, and smells are gone. In this new space, social connections have
great potential for enhancing refugees’ health and well-being.
Introduction
Social relationships have long been understood to be connected to health. Durkheim—the
founding father of modern sociology—introduced anomic conditions as predictors of suicide. He
revealed that there are unique social phenomena that affect our well-being. More recently,
Umberson and Montez (2010) have reminded us that “social relationships—both quantity and
quality—affect mental health, health behavior, physical health, and mortality risk” (S54).
Through this lens, social ties and networks have intrinsic value. Kadushin (2012) explains that
social networks are formed for psychological reasons like feelings of safety, comfort, and
support as well as reasons of productivity and efficiency—such as getting things done and status
seeking. In terms of benefits and supporters, Thoits (2011) suggests that social relationships
yield two types of support (emotional sustenance and active coping assistance) and two types of
supporters (significant others and experientially similar others). Further connecting social
relationships to health, Thoits (2011) describes seven possible interworking mechanisms: social
influence/social comparison, social control, role-based purpose and meaning (mattering), self-
esteem, sense of control, belonging and companionship, and perceived support availability.
1

Social capital—“the aggregate of the actual or potential resources which are linked to
possession of a durable network of more or less institutionalized relationships of mutual
acquaintance and recognition” (Bourdieu 1986:286)—may also explain how social networks are
linked to health. Kadushin (2012) describes social capital as a countervailing concept to
Durkheim’s anomie and suggests that social capital is one of ten master ideas of social networks.
Accordingly, social networks can be viewed as assets. To this end, Wellman and Wortley (1990)
argue that different types of support come from different network members, and at different
times, and in predictable ways. While friends are more likely to provide emotional support,
financial support is more likely to come from family (Wellman & Wortley 1990).
Social ties lend social support, but the characteristics of individuals and their ties are
important to consider. Certain structural characteristics of social networks have affected men and
women differently. Researchers have found that the protective effects of social networks are not
universal and that negative effects associated with more heterogeneous networks may be more
prominent among women (Kawachi & Berkman 2001), even though weak ties can have positive
effects (Granovetter 1973). Intuitively, those with access to more network ties and structural
networks might have access to more information and resources. While this access could be
associated with better health, Bearman and Moody (2004) have suggested that accessing
different types of networks can be related to being less embedded in any one network (and
having fewer stronger ties) and that this association negatively affects the well-being of females
compared to males. Further suggesting that the influence of social networks differs by gender,
Cornwell and Laumann (2011) contend that network position is related to traditional roles of
masculinity. The authors argue that having access to information from different ties and from
different network circles may have a unique psychological importance for males. In short, while
2

access to greater numbers of network ties and more diverse structural networks can be beneficial,
social network literature suggests that an overall benefit may be moderated by gender. Women
may not benefit from network size and heterogeneity as much as males do—and women may
even experience negative effects related to these social network characteristics.
The social networks of newly resettled refugees are important to explore for several
reasons. First, the very definition of a refugee suggests anomie: “refugees are of special
humanitarian concern…and have demonstrated that they were persecuted or have feared
persecution due to race, religion, nationality, political opinion, or membership in a particular
social group” (U.S. Citizenship and Immigration Services N.d.). In addition to forced migration,
many refugees have experienced extreme violence including war and torture. Accordingly,
refugees face mental health challenges that begin at home and continue in the United States.
Many suffer from post-traumatic stress disorder (PTSD), depression, and other forms of
psychological distress (Fazel, Wheeler & Danesh 2005; Porter & Haslam 2005). Secondly,
newly resettled refugees have nascent and developing social networks. Resettlement in the
United States often means being separated from family and friends and learning to navigate new
systems and cultures. Many must do so in a new language or one that they have not yet
developed confidence or proficiency.
Refugees must form new social ties in order to access new types of resources. Those that
are better equipped to access resources are more likely to regain footing on their path to a
meaningful and productive life faster than those who struggle to make similar connections.
Lastly, and perhaps most critically, the refugee experience is all too common. The United
Nations High Commission for Refugees (UNHCR 2015) has reported that there are
approximately 59.5 million people who have been displaced due to persecution, conflict, or
3

violence. This number includes refugees (19.5 million), internally displaced persons (38.3
million), and asylum seekers (1.8 million). In 2014 alone, 13.9 million people were newly
displaced.
Research on the physical and mental health of refugees is abundant, but it is limited in
several key ways. Fazel and colleagues (2005) have noted that more rigorous mental health
instruments and more robust study designs tend to yield lower rates of PTSD and that the
consequences of poor measurement can be dramatic. Underestimating mental health problems
could be neglectful and overestimating problems might be stigmatizing. Despite this caveat,
there is a vast amount of research on refugee mental health. In a meta-analysis of studies on
refugee mental health, Porter and Haslam (2005) extracted data from research published between
1959 and 2002 and utilized data from 67,294 individuals. The majority of these studies collected
data from Southeast Asians (Fazel and colleagues 2005). This is in striking contrast to current
trends where more refugees now come from the Middle East and Africa. As of 2014, the five
most common countries of origin for refugees are as follows: 1) Syrian Arab Republic (64,300);
2) Democratic Republic of the Congo (60,500); 3) Myanmar (57,400); 4) Afghanistan (49,000);
and 5) Iraq (45,700) (UNHCR 2015).
Although it might be assumed that refugees have few social ties when resettling in a new
country, characteristics about these nascent social networks are mostly unknown. What do these
networks look like, and how do they relate to health and mental health? Several studies have
touched on these issues, and while they present rich and useful information, a few limitations are
noteworthy. Smith (2013) conducted a case study analysis of the social networks of 17 female
refugees who resettled in the Midwestern United States. This study provides an in-depth look at
networks, but includes a relatively small sample that is all female. It also comprises refugees
4

who have had considerable time to adjust and rebuild social networks; the refugees in the study
had lived in the U.S for an average of six years. Lambda and Kralm (2003) conducted survey
research with 525 refugees who had resettled in Canada. The authors found that refugees
maintain and utilize familial ties as well as ties with sponsors, but note that there is missing
context that qualitative methods could elucidate. The authors state that “future research should
employ more qualitative methods to further document the complexity of refugees’ social
networks” (Lambda & Kralm 2003:356).
Several studies on people in refugee-like situations and their social networks are also
instructive. Harpviken (2009) applies social network theory to Afghan migration and uses data
from over 200 interviews to describe how war fragments relationships, but social networks that
remain intact can ameliorate the loss of structural protections. In an ethnographic study Monsutti
(2005) describes the social networks of the Hazaras of central Afghanistan as producing
solidarity and adaptive strategies of migration despite the country’s upheaval. While both of
these studies contribute to migration studies, neither of them directly address how social network
theory can also apply to newly resettled refugees. An ethnographic study conducted by Keown-
Bomar (2004) describes kinship networks among Hmong refugees in terms of both resilience and
adaptation. Primarily based on 19 interviews, the author describes the strong desire of families to
stay together and hold on to their culture despite large gaps in the experiences between
generations.
Scholars have connected social capital to immigrant populations in ways that might also
apply to refugees. Bankston (2014) suggests that immigrant networks and social capital go
beyond individual perspectives and account for how immigrants are connected to each other.
Likewise, Portes’ (1993) framework of segmented assimilation brings social structure into focus.
5

Following this framework, the likelihood of future success among refugees and immigrants is
associated with communities within which immigrants or refugees assimilate. Future success is
related to the federal, societal and co-ethnic-community receptions to new groups. These
frameworks can be applied to refugees, but it is important to note that refugees have unique
standpoints. Refugees have an official status that immigrants often do not. They receive benefits
such as cultural orientations, interest-free loans for airfare, and assistance with official
documents such as social security cards (U.S. Committee for Refugees and Immigrants N.d.), but
resources have dramatically declined in recent years (Zong & Batalova 2015). However,
refugees and immigrants have been linked together through xenophobic rhetoric by politicians at
multiple levels of government as well as by local extremist groups, particularly during recent
election cycles (Kaplan & Andrews 2015; Horn 2015; Holmes, Burrell & Casteneda 2015).
This study contributes to the existing body of knowledge on both social networks and
refugee mental health by examining the relationship that social networks have with refugee
mental health. By exploring the networks of newly resettled refugees from Afghanistan, Iraq, and
the Great Lakes region of Africa (Burundi, Democratic Republic of Congo, and Rwanda), this
study assesses current waves of refugees resettling in the United States using a unique local
community-based data set. Thus, it expands upon a body of literature that has been focused
primarily on Southeast Asian refugees.
Applying a mixed methods approach, quantitative social network characteristics and
mental health symptoms scores are contextualized by qualitative interview data. As such, refugee
voices are used to contextualize quantitative results in a way that has not been done to date. This
study takes a sociological approach to examine a new version of an age-old problem. It builds on
a long lineage of scholarly work suggesting that social integration and social networks affect
6

one’s health (Berkman et al. 2000; Kawachi 2010; Song 2010; Tsai & Papachristos 2015).
Refugees have faced much disruption and are working to rebuild their lives in a new social
space. This study examines what these newly formed social networks look like, how they are
related to refugees’ mental health, and how refugees talk about them.
Research Questions
1. How does social network size relate to refugee mental health status?
2. How does heterogeneity of social networks relate to refugee mental health status?
3. How do refugees’ descriptions of their social networks further elucidate the relationships
between refugees’ social networks and their mental health?
Hypotheses
1.1: Greater network size will be significantly and negatively related to PTSD, depression, and
anxiety symptoms scores.
1.2: The negative relationship between network size and PTSD, depression, and anxiety symptoms
scores will be weaker among refugee women.
2.1: Greater network heterogeneity will be significantly and negatively related to PTSD,
depression, and anxiety symptoms scores.
2.2: The negative relationship between network heterogeneity and PTSD, depression, and anxiety
symptoms scores will be weaker among refugee women.
Data Sources
Data analyzed in this study are from a larger study on refugee well-being funded by the
National Institute on Minority Health and Health Disparities (NIMHD R01MD007712). This
7

five-year study includes refugees from Afghanistan, Iraq, and the Great Lakes Region of Africa,
who have recently (within the previous 3 years) resettled in Albuquerque, New Mexico.
Participants are recruited with the help of local refugee assistance programs and native speaking
interpreters (e.g., speaking Dari, Pashtu, Arabic, French or Swahili) for four cohorts, with
participants in each cohort being interviewed at four time points over the course of 14 months.
After baseline interviews, participants are randomly assigned to either: 1) a six-month-long
intervention consisting of two main components (Learning Circles, which involve cultural
exchange and one-on-one learning for refugee adults, and Advocacy, which involves
undergraduate paraprofessionals mobilizing resources for refugee adults and transferring
advocacy skills to them); or 2) a control group that includes a one-time stress management
program. Further description of the intervention can be found elsewhere (Goodkind, Hang,
&Yang 2004; Goodkind 2005; Goodkind et al. 2014).
Participants in both the control and intervention groups with elevated PTSD symptoms,
are offered Narrative Exposure Therapy (NET), an evidence based treatment described as an
intervention that helps participants tell their stories until they are no longer traumatic
(Gwozdziewycz & Mehl-Madrona 2013). The authors report in a recent meta-analysis testing the
effectiveness of NET on refugee populations that most studies tend to have salutary results with
medium effect sizes. Any participant that indicates that he or she is at risk of harming his or
herself (e.g., talking about suicide) is immediately assessed by a study team member who is a
trained clinical psychologist.
At each data collection time point, participants complete a quantitative interview that
leverages computer assisted personal interviewing (CAPI). Interviews are programed to be
conducted in the participant’s first language and delivered by an interviewer/interpreter who
8

speaks their language. Quantitative interviews include questions about social networks, as well
as PTSD symptoms and depression symptoms. All participants complete qualitative interviews
with the assistance of interpreters at baseline. Semi-structured interviews lasting approximately
one hour include questions about one’s experience resettling in the United States. Questions that
often spark discussion about social ties are as follows: 1) “Are there any changes related to your
family back in [Iraq, Congo, Afghanistan or elsewhere in the world]?”; 2) “Have there been any
changes related to your social network (who you spend time with, visit, get advice or get help
from)?”; 3) “Have there been any changes (increases or decreases or level of difficulty) in your
access to social services or other resources in the community?”; 4) Are there any changes with
your comfort level in Albuquerque?” and; 5) “How are things going in terms of your health (by
health we mean physical health, emotional health, mental health and spiritual health)?”. This
study is approved by the University of New Mexico Human Research Protections Office.
Measurement
Control variables
Respondents were asked for their age in years, their sex (male or female), and for their
perceived level of English proficiency, highest level of education (less than high school to
graduate degree), marital status (single, married, widowed, divorced), how many people are in
their household, how many children they have, and their nationality. Participants were also asked
whether they have been employed within the last two months, their satisfaction with their income
(very dissatisfied to very satisfied), and the dollar amount of income they receive from wages or
benefits. English proficiency is based on the Perceived English Proficiency Scale (PEP; Wei et
al. 2012), which is a composite measure of how well participants rate their ability to read, write,
speak, and understand English, on a four-point scale from not at all to like a native English
9

speaker. Regarding nationality, the primary refugee subgroups are Afghans, Africans from the
Great Lakes Region (Burundi, Democratic Republic of Congo, and Rwanda), and Iraqis.
However, a wider range of nationalities were reported. As such, the following recoding was
performed based on geography and language: Tajik, Pakistani, and Iranian participants were
included with the Afghan group and Syrians were included in the Iraqi group.
Independent Variables
Using an ego network name generator system, network size was measured with the
following questions: 1) “Are there people (adults) in Albuquerque with whom you discuss
important matters?”; 2) “Are there people (adults) in Albuquerque who you have asked for
advice or help in getting things done in the United States?”; and 3) Are there people (adults) in
Albuquerque who you ask for advice or help when you are not feeling good about yourself or
your situation? Participants were asked to name up to six people for each question and provide
either a first name or initials for each person listed. An unduplicated total is calculated based on
the sum of these three questions with redundant ties left uncounted. Redundant ties are identified
by a question that follows the addition of each new tie that asks “is this a person you already
mentioned.” Any tie that has a yes response to this question is not counted.
Characteristics of network ties that measure heterogeneity include the following: 1) “Is this a
man or a woman?” 2) “Is this person from [Iraq/Afghanistan/the Great Lakes of Africa]?” 3)
“How do you know this person?” and 4) “Does this person speak your language?” Responses
choices for “How do you know this person?” are: family member not in household, friend,
coworker, doctor/medical provider, mental health care provider, social service provider, person
from Refugee Well-being Project (the intervention in the study), and other. Using these
10

characteristics of social ties, three indicators of heterogeneity or diversity of ties were calculated
as follows.
1) The proportion of ties that are of the same sex. For example, a male that has mostly male ties
has a high proportion of same sex ties. A female that has mostly female ties has a high
proportion of same sex ties. Conversely, a male that has mostly female ties has a low
proportion of same sex ties.
Figure 1 Case example of a male participant with a high proportion of same sex ties.
2) The proportion of ties that are from the same cultural community. For example, an Iraqi that
has mostly Iraqi ties has a high proportion of same cultural community ties. A refugee with a
lower proportion of ties from the same cultural community would have more ties outside
their cultural community, such as with Americans.
Figure 2 Case example of an Iraqi participant with a high proportion of same cultural
community ties.
Male
Fem
Male
Male
Male Male Ego
Iraqi
American
Iraqi
Iraqi
Iraqi Iraqi Ego
11

3) Role heterogeneity. A participant has higher role heterogeneity if they report more variety in
how they know their social ties. A participant with only family members as ties would have
no heterogeneity of social ties. With each additional type of tie reported, role heterogeneity
increases. An example of a participant with higher role heterogeneity is below in Figure 3.
As presented, this case has 5 ties, each with a different social role—a friend, coworker,
family member in their household, a family member outside their household, and a service
provider.
Figure 3 Case example of high role heterogeneity
Dependent Variables
Trauma exposure comprises items from three trauma measures (Foa et al. 1993; Mollica
1992; Weine et al.1995) that were selected based on the set of experiences that refugees are
likely to have, such as those related to combat and sexual assault. Higher scores indicate
exposure to more traumatic events. For each of 25 listed traumatic events, participants self-
reported whether yes they had experienced the event or no they had not. The trauma exposure
score is the sum of all events that a participant reported experiencing.
Post-Traumatic Stress Disorder symptoms are measured with the PTSD Checklist –
Civilian Version (PCL-C; Weathers et al. 2013) Ruggerio and colleagues (2003) have reported
very strong test-retest reliability (r = 0.96) as well as strong concurrent validity to other measures
Ego
Family outside household
Service Provider
Coworker
Family in household
Friend
12

of PTSD symptoms. The PCL-C has 17 items, asking respondents to report the frequency with
which they have been bothered by different key symptoms of PTSD in the last month. The items
are measured on a 5-point Likert-type scale, with response choices ranging from “not at all” to
“extremely.” Participants who have a total PTSD symptom score that is equal to or greater than
40 are considered to have clinically significant PTSD symptoms and are offered the opportunity
to meet with a study clinician to learn about Narrative Exposure Therapy and to determine
together whether it is appropriate for them. While some researchers and clinicians have
advocated a cutoff score of 50 (Arnetz et al. 2013), numerous studies with refugees use and
recommend 40 as the cutoff (Jordans et al. 2012; Pham et al. 2009; Rees et al. 2013).
Emotional Distress and Depression are measured from subscales of the Hopkins
Symptoms Checklist (HSCL) (Derogatis 1974). The original instrument included 58 questions on
a four- point Likert scale with 5 subscales (somatization, obsessive-compulsive, interpersonal
sensitivity, anxiety and depression) and is the precursor to the Hopkins Symptom Checklist 90.
The present study uses the anxiety and depression subscales in the form of the HSCL-25. This
measure has been utilized worldwide and with refugees in previous studies (Mollica et al. 2001).
Kaaya and colleagues (2002) reported good internal consistency using the HSCL-25 (alpha 0.93)
with HIV-positive pregnant women in Tanzania. Further, Bech and colleagues (2014) found the
depression and anxiety subscales of the Hopkins Symptoms Checklist to be psychometrically
valid. The anxiety subscale has 10 items and the depression scale has 15 items. Each item is
measured on a 4-point Likert-type scale, with response choices ranging from “not at all” to
“extremely.”
13

Analysis
Descriptive statistics and ordinary least squares (OLS) regressions were conducted using
Stata SE Version 14. In the models, theoretically informed control variables were run with social
network size, proportion of same sex ties, proportion of same cultural community ties, and role
heterogeneity as key independent variables. Dependent variables are PTSD symptoms,
depression and anxiety. For each dependent variable 4 models were run. First, all controls
variables were run with social network size as the key independent variables. Second, social
support was introduced to test whether it mediates the effect of social network size. The third
model introduces three variables describing social network characteristics: proportion of same
sex ties, proportion of same cultural community ties, and role heterogeneity of ties. The fourth
model introduces an interaction term testing whether female gender moderates the relationship of
role heterogeneity. Unstandardized coefficients with standard errors and standardized
coefficients are presented in tables 2-4. Interaction effects are plotted in figures 5-7. Qualitative
interview data was recorded, transcribed, and imported into NVivo Version 10. Data was coded
by a team of research assistants using a content analysis approach that included nodes on social
networks at home and in the United States as well as a node on social isolation. Results that were
coded within these categories were reviewed and synthesized into a memo on social networks
with emergent themes and salient quotations that was subsequently used to contextualize the
quantitative findings.
Sample Characteristics
After the first three waves of enrollment, the study includes 168 participants. Study
participants are 47% Iraqi, 32% Afghan, and 21% African. The mean number of months
participants have lived in the United States is 7.45 (SD 7.6) and the range was 0 to 27 months.
14

Fifty-two percent are female. The mean age is 36 (SD=12). Although 32% have less than a high
school education, 35% have an associate’s degree or more education. Fifty-nine percent of
participants are married, 31% single, 8% widowed and 2% divorced. Most participants resettled
with family members—72% have children and the mean number of children is 2.4 (SD 2.07).
The mean household size is 4.4 people (SD 1.88) with a range of 1 to 11. Just over a quarter of
participants (28.3%) are employed. The mean amount of income per month from salary or wages
is $642 (SD $661) with a range of $0 to $3,000. The mean amount of income from government
benefits per month is $731 (SD =$28) with a range of $0 to $2210. There were 7% who reported
not receiving any income from government benefits and 30% did not answer the question. The
mean level of satisfaction with one’s income was 2.01, which indicates that on average,
participants were “somewhat dissatisfied” with their level of income. Summary statistics are
presented in table form in Appendix A.
Results
The mean for trauma exposure was 8.5 (6.28 SD and range 0-25). This score indicates
that on average, refugees experienced about 9 types of traumatic events out of 25 possibilities
presented. While roughly 10% reported that they experienced none of the listed traumatic events,
almost 5% reported experiencing 20 or more of the listed traumatic events. The mean PTSD
symptom score was 33.60 (SD=16.23) with a range of 8-81. Twenty-eight percent of participants
had PTSD symptom scores above the cutoff of 40, which has been determined as a clinically
meaningful score, and were offered additional mental health services. The mean for emotional
distress (depression and anxiety symptoms combined) was 1.65 (SD=.636). Researchers have
used a mean rating of >1.75 as a convention to indicate need for treatment (Kayaa et al. 2002).
15

Two subscales of emotional distress had similar results: Depression (M=1.67, SD= .659) and
Anxiety (M=1.56, SD=.65).
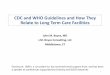
Comprising an unduplicated count of social network ties, the total social network sizes
reported ranged from 0 to 12 (M=2.11; SD=2.13), but, of importance, 30% of participants
reported having no network ties (this was the mode). A dot plot (Figure 4) presents the frequency
of total social network sizes. Summary statistics for each social network question and the total
social network size are presented in Table 1 with cross tabulations of total social network sizes
by nationality, gender, and age group. Cross tabulations indicate that most social network ties
were reported as ties that a participant discusses important matters with. Iraqi’s, males, and
participants aged 40-49 reported more social ties than other groups.
16

Figure 4 Total Social Networks
Table 1 Social Network by question and cross tabs by Sample Characteristics
Question Mean SD Range
Talk about important matters 1.61 1.59 0-6 Asked for advice or help in getting things done
0.58 1.15 0-6
Asked for advice or help when not feeling good
0.39 .92 0-6
Unduplicated total (overall total) 2.12 2.13 0-12 Total by nationality Afghan 1.41 2.31 0-12 African 2 2.29 0-10 Iraqi 2.64 1.78 0-7 Total by gender Male 2.40 2.40 0-12 Female 1.86 1.82 0-7 Total by age group 18-29 2.40 1.71 0-10 30-39 1.86 2.02 0-9 40-49 2.74 2.34 0-12 50-59 1.94 1.98 0-6 60-71 2.26 2.05 0-6
Source: Refugee Well-being Study (2012-2015)
17

The mean proportion of same sex ties was .603 (SD=.391). Here, a proportion of 0 would
indicate all opposite sex ties and a proportion of 1 would indicate all same sex ties. Accordingly,
the mean shows that on average, 60% of participants’ ties are with people of the same sex.
Africans had the highest proportion of same sex ties among the three nationality groups. Males
also had a higher proportion of same sex ties compared to females. The mean proportion of ties
coming from the same cultural community was .855 (SD=.284). As such, most ties are with
people from the same cultural community. The mean level of role heterogeneity is .175
(SD=.242). The most heterogeneity found was .67. Role heterogeneity was the highest among
Iraqis and people over the age of 60. This indicates that most refugees do not have much role
heterogeneity in their social networks. Cross tabs for proportion of same sex ties, same cultural
community ties, and heterogeneity of social roles of ties are presented in Appendices B-D.
PTSD Symptoms (Models 1-4)
Results show that previous trauma exposure is related to PTSD symptoms and is highly
statistically significant. For each traumatic event reported, participants have PTSD symptoms
scores that are 1.5 points higher. In model 4, this is statistically significant (p<.001). Income
satisfaction is also highly significant across models. In model 4, each level of increased
satisfaction with income is related to PTSD symptoms scores that are almost 2 points lower
(p<.01). On average, Iraqi’s tend to have higher PTSD symptoms scores than Afghans. In model
4, Iraqi’s have scores that are roughly 6 points higher than Afghans and this is statistically
significant (p<.05). While social network size does not approach statistical significance,
increases of role heterogeneity (having more different kinds of social ties, such as friends family,
and coworkers) is related to PTSD symptoms scores that are 10.5 points higher (p<.05) as
observed in model 3.
18

An interaction effect was also observed. For females, increases in heterogeneity are
associated with PTSD symptoms scores that are 21 points higher (p<.05). A graph of this effect
is presented in figure 5. Suggesting benefits of ties with similar characteristics (homophily),
higher proportions of same sex ties is related to PTSD symptoms scores that are 7 points lower
(p<.05) as observed in model 4. Having children approaches statistical significance in models 3
and 4, suggesting that having children may also be related to higher PTSD symptoms (p=.083).
Depression Symptoms (Models 5-8)
Previous trauma exposure is also highly related to depression scores. In model 8,
exposure to trauma is related to depression scores that are .05 points higher (p<.001). Increased
income satisfaction is also related to lower depression scores. Model 8 shows that each increase
of income satisfaction is related to a .09 lower depression score (p<.01). Iraqi’s have higher
depression scores than Afghans; in model 8 Iraqi’s have depression scores that are 0.3 points
higher than Afghans (p<.05). Social network size is marginally significant in model 5 (p=.097).
As such, one new social tie may be associated with depression scores that are .03 points lower.
Model 6 shows that the effect of social network size is weaker and no longer marginally
significant when social support is added to the model. Model 5 also shows that females tend to
have depression scores that are .2 points higher than males, (p<.05), but this effect is weaker and
only marginally significant in model 7 (after adding social support).
An increase in role heterogeneity is related to a depression score that is .5 points higher
as seen in model 7 (p<.05). For females, increases in heterogeneity are related to depression
scores that are .9 points higher in model 9 (p<.05). Model 9 also shows that an increase in
proportion of one’s same sex social ties is related to depression scores that are .36 points lower
(p<.05), thus suggesting a positive influence of predominantly same sex social networks.
19

Anxiety (Models 9-12)
Trauma exposure is also strongly related to anxiety scores. As shown in model 12, an
increase in trauma exposure is related to an anxiety score that is 0.5 points higher (p<.001). Also
in model 12, a one unit increase of income satisfaction is related to anxiety scores that are .06
points lower (p<.05). Both of these findings are consistent across models 9-12. Females are
observed to have anxiety scores that are .24 points higher than males in model 9 (p<.01) and this
is similarly observed in model 10 (p<.05), but not observed in models 11 and 12 once social
network characteristics are added into the models. In model 10, Iraqi’s are observed to have
anxiety scores that are .3 points higher than Afghans (p<.05) and Africans tend to have anxiety
scores that are .3 points lower than Afghans (p<.05). However, neither of these findings are
statistically significant once social network characteristics are added to models 11 and 12.
Neither social network size nor role heterogeneity were found to be related to anxiety scores. As
observed in model 12, an increase in the proportion of same sex ties is related to an anxiety score
that is .3 points lower (p=.044).
In sum, trauma exposure is strongly related to PTSD symptoms, depression, and anxiety.
Income satisfaction appears to be strongly related as well. Iraqi’s tend to report more distress
than Afghans. Africans tend to report less distress than Afghans. While social network size does
not appear to be related to distress, certain network characteristics were significantly related.
Role heterogeneity seems to be related to increased distress, particularly for females, while
higher proportions of same sex ties seems to be related to less distress.
20

Table 2 OLS Regression of PTSD Symptoms
Model 1 Model 2 Model 3 Model 4
b (se) b (se) b (se) b (se)
Nationality (compare to) Afghan
Iraqi 7.12(2.46)** 7.45(2.70)** 7.05 (3.01)* 6.20 (2.97)* African -7.85(3.12)* -6.68(3.38)+ -5.30 (4.05) -5.26 (3.96) Female 2.65(2.06) 2.56(2.17) -1.94 (2.79) -7.08 (3.54) Age 0.05(0.11) 0.02(0.12) -0.21(0.13) -0.23 (0.13)+ Marital status (compare to) single Married -3.73 (3.90) -3.34(4.16) -7.09 (5.59) -6.69 (5.47) Divorced 9.02 (7.84) 8.35(8.08) -1.80 (10.10) 0.55 (9.92) Widowed -0.85(5.62) -0.42(6.25) 4.33(7.23) 5.78 (7.09) Number in household -0.10 (0.61) -0.05(0.63) 0.68 (0.75) 0.70 (0.73) Children 5.20(3.93) 6.13(4.08) 9.43 (5.58)+ 9.58 (5.46)+ Education -0.84(0.56) -0.73(0.58) -0.30 (0.65) -0.19 (0.64) Perceived English proficiency 1.19(1.81) 0.73 (1.88) -2.05(2.10) -2.40 (2.06) Employed -2.75(2.25) -2.28(2.35) -0.80 (2.52) -0.14 (2.48) Income satisfaction -1.30(0.58)* -1.20(.61)* -1.90 (0.67)** -1.95 (0.66)** Trauma exposure 1.43 (0.18)*** 1.46(0.18)*** 1.50 (0.21)*** 1.51 (0.21)*** Total social network size -0.64(0.50) -0.50(0.55) -0.63 (.65) -0.64 (0.64) Social support -1.83(1.70) -3.34 (1.90)+ -2.69 (1.88) Proportion of same sex ties -5.50 (3.76) -7.68 (3.80)* Proportion of same community ties 2.81 (4.63) 4.84 (4.61) Role heterogeneity 10.57 (5.30)* 1.79 (6.46) Fem*Role heterogeneity 21.38 (9.41)* Constant 20.95(5.18)*** 23.45(5.65)*** 35.32 (8.85)*** 36.08 (9.41)*** N 149 141 110 110 R-Squared 0.55 0.55 0.60 0.62 Adjusted R-Squared 0.49 0.50 0.51 0.53
Source: Refugee Well-being Study (2012-2015); + p<.1, * p<.05, ** p<.01, ***p<.001 (two-tailed tests)
21

Table 3 OLS Regression of Depression
Model 5 Model 6 Model 7 Model 8
b (se) b (se) b (se) b (se)
Nationality (compare to) Afghan Iraqi 0.32(0.11)** 0.35(0.12)** 0.31(0.13)* 0.27(0.13)* African -0.29(0.14)* -0.23(0.15) -0.13(0.17) -0.14(0.16) Female 0.19(0.09)* 0.18(0.10)+ -0.02(0.12) -0.23(0.15) Age 0.00(0.01) 0.00(0.01) -0.01(0.01) -0.01(0.01) Marital status (compare to) single Married -0.24(0.17) -0.23(0.19) -0.32(0.24) -0.30(0.24) Divorced 0.33(0.35) 0.32 (0.36) -0.26(0.44) -0.16(0.43) Widowed -0.23(0.25) -0.18(0.28) 0.03(0.31) 0.09(0.31) Number in household -0.00(0.03) 0.00(0.03) 0.03(0.03) 0.03(0.03) Children 0.21(0.18) 0.25(0.18) 0.27(0.24) 0.28(0.23) Education -0.01(0.03) -0.01(0.03) 0.00(0.03) 0.01(0.03) Perceived English proficiency 0.05(0.08) 0.03(0.08) -0.09(0.09) -0.11(0.09) Employed -0.17(0.10)+ -0.15(0.10) -0.12(0.11) -0.09(0.11) Income satisfaction -0.07(0.03)** -0.07(0.03)* -0.09(0.03)** -0.09(0.03)** Trauma exposure 0.05(0.01)*** 0.05(0.01)*** 0.05(0.01)*** 0.05(0.01)*** Total social network size -0.04(0.02)+ -0.03(0.02) -0.04(0.03) -0.04(0.03) Social support -0.08(0.08) -0.16(0.08)+ -0.13 (0.08) Proportion of same sex ties -0.28(0.16)+ -0.36(0.16)* Proportion of same community ties 0.18(0.18) 0.23(0.18) Role heterogeneity 0.50(0.23)* 0.12(0.28) Fem*Role heterogeneity 0.90(0.40)* Constant 1.31(0.23)*** 1.41(0.25)*** 1.88(0.37)*** 1.96(0.36)*** N 150 142 111 111 R-Squared 0.47 0.47 0.53 0.56 Adjusted R-Squared 0.41 0.40 0.43 0.46
Source: Refugee Well-being Study (2012-2015); + p<.1, * p<.05, ** p<.01, ***p<.001 (two-tailed tests)
22

Table 4 OLS Regression of Anxiety
Model 9 Model 10 Model 11 Model 12
b (se) b (se) b (se) b (se)
Nationality (compare to) Afghan Iraqi 0.24(0.10)* 0.26(0.12)* 0.19(0.13) -0.15(0.13) African -0.34(0.13)* -0.29(0.14)* -0.29(0.17)+ -0.30(0.17) Female 0.24(0.09)** 0.24(0.09)* 0.07(0.12) -0.08(0.15) Age 0.00(0.00) 0.00(0.01) -0.00(0.01) -0.00(0.01) Marital status (compare to) single Married -0.17(0.17) -0.16(0.18) -0.25(0.25) -0.24(0.25) Divorced 0.42(0.34) 0.41(0.35) 0.02(0.45) 0.09(0.45) Widowed -0.31(0.24) -0.31(0.27) -0.26(0.32) -0.22(0.32) Number in household -0.00(0.03) -0.00(0.03) 0.03(0.03) 0.03(0.03) Children 0.23(0.17) 0.27(0.18) 0.32(0.25) 0.33(0.25) Education -0.02(0.02) -0.02(0.03) -0.00(0.03) 0.00(0.03) Perceived English proficiency 0.04(0.08) 0.02(0.08) -0.12(0.09) -0.13(0.09) Employed -0.09(0.10) -0.09(0.10) -0.07(0.11) -0.05(0.11) Income satisfaction -0.05(0.02)* -0.05(0.03)+ -0.06(0.03)+ -0.06(0.03)* Trauma exposure 0.05(0.01)*** 0.05(0.01)*** 0.05(0.01)*** 0.05(0.01)*** Total social network size -0.02 (0.02) -0.03(0.02) -0.02(0.03) -0.03(0.03) Social support -0.01(0.07) -0.09(0.08) -0.07(0.08) Proportion of same sex ties -0.28(0.16)+ -0.34(0.16)* Proportion of same community ties 0.03(0.19) 0.07(0.19) Role heterogeneity 0.25(0.23) -0.03(0.29) Fem*Role heterogeneity 0.66(0.42) Constant 1.00(0.22)*** 1.04(0.24)*** 1.54(0.38)*** 1.59(0.38) N 150 142 111 111 R-Squared 0.48 0.49 0.50 0.51 Adjusted R-Squared 0.43 0.43 0.39 0.40
Source: Refugee Well-being Study (2012-2015); + p<.1, * p<.05, ** p<.01, ***p<.001 (two-tailed tests)
23

Figure 5 Interaction effect for Model 4
Figures 6-7 Interaction effect for Model 8 and Model 12
24

Study hypotheses 1.1 and 1.2 must be rejected. Results do not show that social
network size is related to the mental health of newly resettled refugees, nor do they show
an interaction effect occurring between network size and gender. Study hypothesis 2.1
must also be rejected—statistical significance was found in a negative direction rather
than the hypothesized positive direction. Thus, increased heterogeneity of social ties
appears to be related to worse mental health. Hypothesis 2.2 should be rejected, but
heterogeneity does appear to be moderated by gender. Heterogeneity seems to depend on
gender—females with higher levels of role heterogeneity tend to have worse PTSD
symptom and depression scores.
1.1: Greater network size will be significantly and positively related to better indicators of
mental health: False
1.2: The positive relationship between network size and mental health will be weaker
among refugee women: False
2.1: Greater network heterogeneity will be significantly and positively related to better
indicators of mental health: False, a significantly and negatively related relationship was
found
2.2: The positive relationship between network heterogeneity and mental health will be
weaker among refugee women: False, but an interaction effect was found suggesting that
increased heterogeneity has a stronger negative effect for women.
Several key findings can be elucidated from the results and further contextualized by
the way that refugees talk about their social networks, thus addressing the third research
question in this paper. As Pierce (2012) contends, through mixed-methods research,
25

qualitative findings can add meaning to quantitative results. To this end, the following
four key findings have been derived: 1) although refugee network size does not appear to
be related to mental health, it can be noted that the social networks of newly resettled
refugees are small and that newly resettled refugees report feeling isolated; 2) role
heterogeneity has a negative relationship with mental health and this is moderated by
gender, but certain types of ties do seem particularly valuable; 3) local networks can
provide needed help, but distant networks are also valuable; and 4) current refugees are
building communities that can help future refugees, thus increasing the future availability
of beneficial local network ties. The first two findings contextualize quantitative results
and the third and fourth extend the quantitative findings by suggesting areas that were
unaddressed by quantitative analyses and results.
1) Refugee social networks are small and refugees report feeling isolated.
Thirty percent of refugees reported not having any local ties that they would discuss
important matters with, seek advice or help from when they need to get something done,
or seek advice or help from when they are not feeling well. The mean number of overall
ties was just over 2. Understanding that refugees have limited social support from family
and few local resources, it is worth considering the influence that this has on daily life
and what outstanding needs exist. Although, social network size does not appear to be
statistically related to mental health, refugees describe value and concern for familial ties.
They also suggest the loss of important ties from home: "This is the worst thing that I’m
feeling here. Because I am a stranger here and the loneliness, and I don’t know any
person here, and I don’t know the ways." Another participant portrayed this as being
foreign or, in other words, a stranger: "I’ve never been foreign before, so when I was
26

coming, I thought it would be easy and fun. When I got here, it’s totally different." Even
with improved familiarity with new surroundings, isolation often persists. One participant
stated this as follows:
"I’m comfortable regarding the city, but sometimes I feel annoyed or sad or depressed because I’m alone. I’m isolated. I’m a stranger. I don’t have my family here. I don’t have the one I love here with me.”
Forming new relationships can be distressing. Some participants described
wanting to move to a new area within the United States and others described wanting to
leave the U.S. entirely. As one participant stated: "Sometimes my husband will sit there
and cry, and he says, ‘We need to go back to Iraq, even if we are going die there, it is
better for us from here.’”
Another expressed similar sentiment as follows:
I prefer now to go back to where people kill us or [are] kidnapping or bumping, rather than to stay here in America, as a stranger, have no one to help me, have no one to take care of me. It’s really hard. Day after day, it’s become harder with the barrier of the language, of course.
The stress and strain of worry can influence one’s mental health. One participant
expressed this relationship as follows:
I’m not good at all. I suffer from depression and anxiety. I worry too much about members of my family. I kind of have thoughts all the time that I’m going lose them or one day I’m just going to Iraq and I’m going to experience the same thing I’ve been experiencing. Sometimes I would go at night and check whether my kids are still breathing, because I would be thinking that they are dead. All of these thoughts would occur to me on a regular basis in my mind and I would just explode and cry and cry and cry all the time and I would just feel that I want to go out of the house and just be out there. At night I cannot sleep at all. I have a lot of anxiety and my anxiety level is very high. Another participant described the striking difference between having family,
support, and resources nearby compared to far away: “That’s a big concern for all the
27

refugees. The family is like a body. If you lose a body part, you are disabled. Since 20 or
21 years, I’m away from my own family.”
Violence and turmoil in one’s home country clearly influences refugee status and
one’s networks. One participant described a horrendous scene:
They [the attackers] were there because my husband and brothers worked with an American and I was begging them not to shoot... but they just slapped me against the wall and shot my brother. They told me if you don’t leave the country we’re going to kill you all and we’re going to take your daughter. I was unable to walk for six months after this and still have back problems.
Another participant described losing his brother during an explosion and the
lasting impact of this experience. He stated that the explosion "happened [right] in front
of me, so, yeah...even if someone just mentions his name, I [would] just like slap myself
and cry and do weird stuff." The lasting effect of these experiences and their implied
influence on forming new social ties was succinctly stated: "When Iraqi refugees come to
the United States, the feelings, the old memories all—previous memories came with that."
Not only are family members separated during the resettlement process, but some are
permanently lost. These experiences plausibly affect the ability to form ties with people
of disparate backgrounds.
2. Role heterogeneity has a negative relationship with mental health and this is moderated by gender but certain types of ties do seem particularly valuable
Most refugees form social networks with people of the same sex and with people
of similar cultural backgrounds, with little role heterogeneity. Further explaining this
finding, refugees described real barriers to forming new ties. A nascent grasp of the
English language can be constraining. One participant described a lost opportunity to
make new relationships as follows:
28

As I told you before, I don’t have any social network or any people that I know in the U.S. The main obstacle for that is the language. Many times I take my daughter to the school and I would meet one of the American mothers, who would pass a compliment on how I dress. I would all the time want to reply and start a conversation, but I cannot do it most of the time. I just resort to “Thank you” because I don’t have the language. The language is the main problem. That’s the main obstacle for any social relationships.
Another participant described the process of learning English as more difficult
and isolating than expected:
The thing that really surprised me the most is the language. It’s so hard. I knew it. I didn’t know this language, but I didn’t think that I would be so surprised, because I’m here and I can’t talk to nobody.
Despite the difficulties with role heterogeneity, refugees indicated needing certain
pieces of information and implied the value of having social ties that could help them
navigate their new surroundings. Becoming familiar with a new area in terms of
directions and transportation can pose difficulties. One participant described missing a
healthcare appointment after not being able to find the location of the building:
I went by the bus, when the bus dropped me [off], I didn’t find it [the healthcare provider], so I just walked, walked and I didn’t find it. Then I called my husband. I told him, I’m lost. I don’t know where I am. He told me just go back to the bus station. Some refugees shared concern about not having any backup support for their
family in an emergency situation. Others mentioned having access to resources they
might need in an emergency, but not having the daily support that they need. For
example, one participant stated:
If I have a large problem from outside, I can call people. There are people that I can call. I can ask for help. Yeah, if I need a doctor or to go to the hospital or anything, yeah, there are people that I can call and they can help me. But concerning personal issues, no, I don’t. Emergency cases, there are people I can call on for that. But other problems, I have to solve them myself.
29

From a different perspective another shared the following:
If I get sick or happen something, nobody can—I cannot have anybody to take about my son, or maybe if I go out or going find job, then I should just stay home because nobody I have to take care about my son. Then I think just because my family [is] there and not with me then I don’t have anybody to help me here.
Another participant described the importance of having networks for applying for
a job:
Another challenge was that when we came to apply for a position or for a job, they always needed somebody—they always needed recommendation letters, and we do not know anyone to recommend us for the jobs here.
In sum, refugees have little network heterogeneity. Forming relationships with
people of the same sex and of the same ethnic community appears to be easier to do than
forming relationships with people in other settings such as with other parents from within
one’s children’s schools. One’s ability to speak English seems to contribute to this.
Although heterogeneity appears to be negatively related to mental health, gaps in
resources exist that theoretically could be ameliorated by new local social ties.
Different kinds of heterogeneity many be more or less beneficial. In the measure
of heterogeneity in this study, service providers were included as a type of tie alternative
to friends and family. Those without friends and family may have been more likely to
report service providers as ties. Friends and family members are also likely provide
different kinds of support not completely captured in the quantitative results. To this end,
the next two findings address qualitative results that extend beyond quantitative findings,
thus illuminating issues to be explored in future research endeavors.
3. Local networks are important, but distant networks are also valuable.
Quantitatively, local networks were assessed using a name generator in which
30% of refugees reported not having any local networks. However, when describing
30

social ties, refugees often spoke of distant family or friends. These distant networks are
clearly important to the health and well-being of refugees and were effectively missed in
quantitative calculations. Refugees recognized distant social ties in different ways. While
some spoke of the benefits of having social support from familiar ties, others mentioned a
change in their quality since leaving. Some described not wanting to talk to distant ties in
order to move on and turn a new page or get back on their feet.
Many participants spoke of regular online communication with family members
who are still in their home country. In addition to cell phones, tools such as Viber, Skype,
and Facebook are used. There are still challenges with maintaining communication,
however. Access to the internet on both sides is precarious. One participant reported, "I
don’t get to call them all the time. I don’t have Internet. Sometimes they would call me,
but they can’t really afford calling here because it’s expensive." Another substantiated
this by saying, "Because I don’t have a computer, I couldn’t do that, so I have to visit a
friend in order to open Facebook, to log in my Facebook in order to make a
communication.”
Communication with family provides a sense of comfort and normalcy for
refugees, but it can also introduce vicarious trauma and new stress. As one participant
shared: "absolutely, I feel good when I talk to them, but sometimes I feel depressed
because of the bad news." Family members share new and current traumatic experiences
and need help that newly resettled refugees cannot provide given their distance. One
participant stated:
The whole situation in Iraq is very unstable. My mother, her health is not that good. Whenever she talks to me about how the situation is in Iraq—she talks to me also about how she has problems with her daughters-in-law--I really get affected by that and I don’t know what to do.
31

Another participant described similar circumstances and further elaborated on the
strain of being far apart from family members:
When I speak to my family back home, I really get very worried about my mother especially because my mother is all the time telling me that she is sick because I am away from her and she is really worried about me. All the time, she would tell me that ‘You need to come back to Iraq no matter how difficult it is over here in Iraq’ I get really concerned about what she’s telling me, that I lose my focus. Even when I take my English classes, my mind is all the time with my family members back home.
Certainly some refugees are less tied to family, but this can also be stressful. One
participant described not maintaining regular contact by stating "I was hoping I would,
but we have this saying, ‘Far from the eyes is far from the heart.’” Another said:
One day, I went to that mountain, you know the one, the top of [it and then I] asked myself, ‘Oh, my god, why I am here?’ I can’t believe I am here. How many hours from here to Bagdad? Maybe, 23 hours by airplane.
Evoking the imagery of being lost, another participant described the reality of
intermittent and worrisome communication with loved ones as follows:
The way it is, he is in the forest. He is lost. Sometimes I call him and we’ll talk. Sometimes I call him and I can’t reach him. The last time I tried the phone and it went through, and I spoke to him. He was telling me the problems, and I cried because I can’t help him. I don’t have money. I told him I haven’t been successful yet but I’m just praying if he can get out and be able to get to the refugee camp. Maybe America will bring him or something and be able to get out that problem.
As previously described, refugees are often in contact with family networks from
afar. Reminders of the dangerous living conditions that loved ones continue to deal with
can strain these relationships, but there are other factors involved as well. As such,
support from these networks is diminished. In one key way, along with the change in
frequency of contact, transparency and openness about problems is also affected. As one
participant described:
32

I try to not contact them very much because I don't want to tell them the issue, the truth. They know America is very great place and all the people here are very happy and rich, but this is not the truth. Then I cannot call them and tell them [that this has not been true for me]. Then I wait 'til maybe after one year, or I don't know when, but just 'til I can find a good job, like my job as a teacher or teacher assistant. Maybe I can buy house. When I have all those issues and when I'm going to call them, I can tell what's going on with me. I cannot tell them now what's happening right now, that's difficult.
As depicted above, this participant was unable to share current difficulties with
distant family because a desire to present a positive reality. Accordingly, emotional
support that might have been previously available could not be obtained as easily. This
change in the qualitative value in distant relationships is further described by another
participant:
It's difficult to communicate with someone in another country. We talk on Facebook and stuff, but we used to spend days together, and so I basically lost my friend in Iraq. I lost my friend in Syria. I'm starting over.
In sum, local network name generators can miss many ties that newly resettled
refugees rely on. Further, communication with distant ties is possible and support can be
gained vis-à-vis advancements with internet and technology. This is noteworthy in
relation to the potential of family reunification and the development of new and vibrant
ethnic communities.
4. Current refugees are building communities that can help future refugees, thus increasing the availability of beneficial local network ties
Refugees report having learned what support was most needed and helpful for
them. They also describe how one or two cultural brokers—a family member who
resettled before them or friend in the community—helped them to navigate new systems.
These experiences are described as transformative; many have been encouraged to want
to open their doors and help newcomers. While these budding networks were not
33

captured through quantitative data, interviews revealed some potential for community
growth and improved support for future waves of refugees. Local ethnic communities
will likely grow as more refugees resettle in the United States. Some of these will involve
the reunification of family and friends. As such, refugees also expressed hopefulness
towards reuniting with their family members in the United States:
So yeah we still have and we wish we can, I mean when we support ourselves here maybe we’ll try to bring them here anyway like my dad and mom I think, her mom. So we are, we are in good relations still with them and hopefully we can give them a chance to come here. The value of having just one reliable person who can act as a cultural broker was
articulated by one participant whose brother lived nearby:
If I hadn't had my brother here, I would have had the worst time ever, like he did when he first got here. He didn't even have money to pay rent for a while. You talk to him, and he will explain all that to you, but he had a really, really tough time when he first got here, by his own. They didn't have a car. They had to walk in the rain till some stranger come and took them home.
Participants frequently described receiving help from English speakers who are
from their cultural community and understand their current challenges. As such, one
participant stated:
He’s doing great in helping me when I need support and especially with English language when I try to write letters or reports or emails or... getting advice sometimes for something complicated here. I can’t understand it so I call him and he gave me the advice ... good advice, he give us because he lived here like for 30 years, he came here like 1970 something, and he even Tony he came here like 1980.
Cultural brokers are also able to help refugees communicate with teachers and
other professionals whom refugee's children interact with. One participant described
receiving help from a friend who explained a holiday and time off from school to her
child's teacher in the following way:
34

The mother is a doctor and she knows Arabic. These past few days we had a feast and we wanted our daughter to take the day off from school, so we talked to our neighbors here, the Arabic family. She was able to call the school of our daughter and take a day off from school so that we could celebrate the feast together.
In return, many refugees make a commitment to helping newer refugees, as they
know the challenges that others might face so well. From this lens, the advice and help
that they provide is quite instructive. As one participant described:
I’ve told them, you have to take it easy; be patient. You can’t have everything at once, go step by step, and you’re—and about two weeks ago at Wal-Mart, I saw a person [in] the same situation. I told them you’re going to have to take it easy, be patient and everything. I told them about, just Arabic culture places such as Sahar or like restaurants and shops, that’s at least I can do for them.
Another participant reinforced the importance of helping others with the example of
transportation:
I teach my friend, he came after me, how he’s going [to] get his driver license, which test I do. I tell him what’s, on the street, how they are, people here, and I give him some information I already have as my own experience. If I know anything, I tell them, because they are just came after me. Then if I know already something, I tell them how they are should do [it]. In sum, qualitative interview data both elaborates on factors related to quantitative
findings and elucidates further nuance that is missing within these findings. Although
refugee networks are small, they are meaningful and growing. Challenges such as English
proficiency likely affect one’s formation of networks outside of one’s cultural
community. However, having cultural brokers from within one’s cultural community has
much value as described through the voices of refugees in terms of help communicating
with health providers, schools, and other services. While the local networks are
important, so are distant networks. The ability of refugees to connect with local and
culturally similar communities is of great value and as future waves of refugees resettle in
this community, network opportunities will likely grow and some families will hopefully
35

be reunited. Of those that have recently resettled, many will be influential in the success
of newcomers and future generations.
Discussion
Study results suggest that social isolation is common, social network
characteristics matter, and that trauma and income satisfaction are strongly related to
mental health symptoms. Although social network size was not statistically related to
PTSD, depression, or anxiety symptoms, refugees frequently discussed experiencing
social isolation. Secondly, the composition of social networks does appear to be
important. While role heterogeneity was related to increased distress, one’s proportion of
same sex ties was related to better mental health scores. Third, trauma exposure and
income satisfaction were consistently related to PTSD, depression, and anxiety
symptoms; as would be expected, more trauma exposure was related to worse mental
health scores and more income satisfaction was related to better mental health scores.
This finding highlights the impact of both pre- and post-migration factors on the mental
health and well-being of refugees.
Social isolation is common
A high proportion of refugees reported having small social networks and many
reported having no social ties (at least locally). This suggests isolation is a factor in
refugee mental health. While a relationship between social network size and PTSD,
depression, or anxiety symptoms was not found, refugees described social isolation in
numerous interviews. Similarly, scholars have linked social isolation to mental health
after refugee-like situations (Burnett & Peel 2001; Gorst-Unsworth & Goldenberg 1998).
The importance of social support is often evoked in this work (Schweitzer et al. 2006).
36

Miller and colleagues (2002) frame social isolation as a post-exile stressor and the
authors argue that interventions should focus on current stressors (including social
isolation). Social isolation appears to be common among newly resettled refugees. This
can be seen in the words refugees use such as being a stranger or being unable to talk to
potential social ties because of limited English skills.
I hypothesized that social network size would be associated with better mental
health because I thought that it would indicate social support and protection from social
isolation. Because networks were so small, it may be that there was not enough variance
in the data to detect such a finding. It may also be that social network size is not so
influential and that the real benefit comes from the value of certain ties—for example,
their particular characteristics.
Social network characteristics matter
A beneficial relationship was found for refugees with higher proportions of same
sex ties. Conversely, higher role heterogeneity was associated with worse mental health
scores. This finding supports the construct of homophily which follows the adage “birds
of a feather flock together.” McPherson and colleagues (2001) describe race and ethnicity
as the strongest examples of homophily in relationships followed by age, religion,
education, occupation, and gender. Role heterogeneity and its negative relationship to
mental health appears to be accentuated by gender as more role heterogeneity is related to
worse mental health scores for females. This finding evokes previous social network
research that suggests that females are less likely to find value in weak ties (Berman &
Moody 2004; Cornwell 2008; Kawachi & Berkman (2001).
37

While I hypothesized that more heterogeneity would be beneficial, akin to
Granovetter’s (1973) “strength of weak ties” premise, the opposite was found.
Granovetter (1973) found that access to different structural networks facilitates access to
more information. My hypotheses indirectly applied this idea by looking at different
types of ties within one’s social network and suggesting that different types of ties might
facilitate access to more information as well. This hypothesis does not address structural
dynamics inherent in the “strength of weak ties” because I was not able to assess whether
participants truly bridged gaps between different network groups. Findings may have
been further influenced by the broad range of options for identifying network ties, which
included service providers (mental and physical) as options for distinct types of network
ties. Accordingly, people who are receiving services would then logically have more
heterogeneity (assuming they also listed family members, friends, or other types of ties).
However, including service providers over additional friends, family members or
coworkers may also indicate that one has weaker ties in general and support the value of
strong ties. Strong ties may come from family and friends who are from the same cultural
community as well as those of the same sex. Overall, homophily is clearly important to
the social networks of refugees resettling in the United States. This may be most
important when refugees are new and learning English. As they become comfortable with
the English language they may form more ties with native English speakers.
Other types of heterogeneity are important as well, even if they were not
systematically measured. First it appears that relationships with cultural brokers who can
navigate multiple cultures are of much value. As such, the amount of time that one’s ties
have lived in the United States could be a useful metric. Additionally, network ties exist
38

beyond the local sphere; many refugees reported social support from family members and
friends who remain in their home country. Considering local and distant ties could be
another useful way to look at network heterogeneity.
Trauma and income satisfaction are highly significant
Exposure to trauma is common, but not universal. It should be noted that 10% of
refugees in this study reported no exposure to trauma. Previous research has found that
refugees have higher rates of PTSD compared to non-refugee populations. Fazel et al.
(2005) found that refugees are 10 times more likely to have PTSD compared to age-
matched general populations in each country. Numerous scholars have described
stressors and symptoms among refugee populations (Miller & Rasco 2004; Miller et al.
2008; Murray & Davidson 2010; Perara et al. 2013). In this study, PTSD exposure was
found to be related to PTSD symptoms, depression, and anxiety. This was the most
consistent finding across all 12 OLS regression models.
The relationship between income satisfaction and PTSD, depression, and anxiety
symptoms was the second most consistent finding. As such, access to benefits and to
meaningful employment opportunities is important. Local refugee resettlement agencies
justifiably place a premium on finding employment for refugees, but this should be done
cautiously and in such a way that sets refugees up for success both economically and
psychologically. Refugees sometimes describe having valuable skillsets that are
unrecognized. Along these lines, in a study exploring pre-displacement and post-
displacement factors associated with refugee mental health, Porter and Haslam (2005)
found that having a higher standard of living prior to resettling is related to worse mental
39

health once resettled. Unfortunately, in this study, many refugees have indicated income
dissatisfaction.
Study Limitations
Before continuing, several limitations to this study should be noted. Cross-
sectional data only points to correlation and not to causation. Additionally, while the
study uses data from three years in which virtually all known refugees in the study area
were recruited to participate and nearly all did, the sample consists of 168 participants.
Some models included fewer numbers of participants because listwise deletion was used
and many participants reported having no social networks. Social network characteristics
could not be computed for participants who did not report having social ties. As such,
these variables are not missing at random and multiple imputation could not be justified.
Lastly, with social network data collection, respondent error (from poor recall) and
fatigue can be at play as well. Accordingly, social network sizes are estimates and not
absolute. Finally, networks include only local ties, whereas it is clear from the qualitative
data that non-local networks matter as well. Despite these limitations, the study yields
several noteworthy implications.
Implications
Isolation is a concerning factor for refugees and refugees may need help and be
unable to access it. Study findings suggest that newly resettled refugees may benefit from
relationships with people with similar backgrounds. This knowledge can be advanced by
supporting programs that connect refugees with people within their cultural community
and broader communities. These relationships can help facilitate the navigation of
systems in the United States as well as help provide interpretation and advocacy, as
40

needed. Encouraging informal relationships can help augment the limitations of formal
refugee resettlement services (e.g., time, funding, and resources). Attention to meaningful
refugee employment opportunities is also important. These jobs sustain the economic and
psychological well-being of new families in local communities. As refugee communities
grow and take shape, opportunities for the formation of new social ties may increase.
Finding ways to support these opportunities and to encourage more established refugees
to act as cultural brokers for newcomers is essential.
Future research might examine how refugee networks take shape and grow over
time. Examining how this relates to mental health could be particularly useful. Ego
network studies might also add distant social networks to local network counts.
Particularly among newly resettled refugees, local networks are small and distant
networks are substantial. Studying the changing landscape of local communities that
embrace refugees may also be fruitful. As communities become more established, they
could become hubs facilitating access to resources and providing needed support.
Studying the diffusion of this knowledge could benefit other communities. The role of
new policies related to refugee resettlement could be particularly salient for future studies
as well.
Conclusion
Through employing a mixed-methods approach, findings related to social network
characteristics and the mental health of refugees have been observed, contextualized, and
extended. While some findings were easily contextualized, blind spots were also
revealed. Quantitative methods missed the support of distant networks as well as
resources provided by different types of friends (e.g., cultural brokers).
41

It is clear that the refugee experience is often traumatic, but resettlement offers
hope. Refugees seek to turn a new chapter in their lives, to rebuild, to reconnect, and to
start again. Throughout resettlement, new challenges replace old ones. Refugees must
learn how to thrive in a new home, with a new culture, language, and geography. New
social relationships and friendship ties are important to help connect refugees to
resources. Newly resettled refugees enter the United States with few local social network
ties, little variety in ties, and thus limited social capital. However, it seems a little social
capital can make a big difference. A few trusted ties can help newcomers adjust to their
new surroundings and develop a sense of security needed to ensure future success. As
Kawachi (2010) stated:
Social capital serves to remind us that population health is determined by more than access to health care, genetics, lifestyles, money, and schooling. The social world also matters a great deal, and our ties to familial, friends, coworkers, and neighbors constitute a credit bank—a form of capital—that we can rely upon to promote health (29).
This study suggests that newly resettled refugees obtain social capital through
people who are similar to them. Refugees described many needed resources—help with
English, transportation, learning where to shop, and with communication with schools,
healthcare organizations, and housing authorities. Cultural brokers who can provide this
social capital are limited, but encouraging these roles and supporting informal community
relationships is of the upmost importance.
42

Appendix A Summary Statistics Proportion Mean SD Range Independent Variables Afghan .32 African .21 Iraqi .47 Female .52 Age 36.01 12.09 18-71 Education 3.19 2.19 1-7 Number of Children 2.37 2.07 0-9 Household Size 4.44 1.89 1-11 Perceived English Proficiency
1.20 0.65 0-3
Satisfaction with Resources 3.35 0.94 1.25-5.38 Satisfaction with Income 2.01 1.85 0-6 Income from Salary or Wages
642.86 661.30 0-3000
Income from Benefits 731.26 428.32 0-2210 Social Support 1.94 0.66 0.54-4 Trauma Exposure 8.53 6.28 0-25 Total Social Networks 2.11 2.13 0-12 Proportion same sex 0.60 0.39 0-1 Proportion same cultural community
0.85 0.28 0-1
Heterogeneity of social roles
0.174 0.24 0- .66
Dependent Variables Emotional Distress 1.64 0.636 1-3.67 Depression 1.67 0.659 1-3.71 Anxiety 1.56 0.65 1-3.7 PTSD Symptoms 33.60 16.23 8-81 Source: Refugee Well-being Study (2012-2015)
43

Appendix B Proportion of same sex ties and cross tabs by nationality, gender, and age group Mean SD Range Overall total .603 .391 0-1 Nationality
Afghani 0.47 0.48 0-1 African 0.71 0.35 0-1 Iraqi 0.62 0.35 0-1 Gender
Male 0.83 0.27 0-1 Female 0.38 0.37 0-1 Age group
18-29 0.72 0.39 0-1 30-39 0.58 0.36 0-1 40-49 0.55 0.42 0-1 50-59 0.56 0.38 0-1 60-71 0.49 0.28 0-0.67 Source: Refugee Well-being Study (2012-2015)
44

Appendix C Proportion same cultural community and cross tabs by nationality, gender, and age group Mean SD Range Overall total 0.85 028 0-1 Nationality
Afghani 0.88 0.30 0-1 African 0.77 0.35 0-1 Iraqi 0.87 0.25 0-1 Gender
Male 0.85 0.27 0-1 Female 0.86 0.29 0-1 Age group
18-29 0.82 0.33 0-1 30-39 0.90 0.26 0-1 40-49 0.84 0.29 0-1 50-59 0.89 0.20 0.5-1 60-71 0.83 0.24 0.5-1 Source: Refugee Well-being Study (2012-2015)
45

Appendix D Role heterogeneity and cross tabs by nationality, gender, and age group Mean SD Range Overall total 0.17 0.24 0-0.67 Nationality
Afghani 0.12 0.21 0-0.67 African 0.11 0.21 0-0.64 Iraqi 0.22 0.26 0-0.67 Gender
Male 0.17 0.25 0-0.67 Female 0.18 0.24 0-0.67 Age group
18-29 0.18 0.25 0-.067 30-39 0.18 0.24 0-.067 40-49 0.15 0.23 0-.067 50-59 0.17 0.24 0-.05 60-71 0.36 0.34 0-.067 Source: Refugee Well-being Study (2012-2015)
46

References
Arnetz, Judith, Yoasif Rofa, Bengt Arnetz, Matthew Ventimiglia, and Hikmet Jamil. 2013. “Resilience as a Protective Factor against the Development of Psychopathology among Refugees.” The Journal of Nervous and Mental Disease 201(3):167–72.
Bankston III, Carl, L. 2014. Immigrant Networks and Social Capital. Cambridge: Polity Press.
Bech, P., Bille, J., Moller, S.B., Hellstrom, L.C., and Ostergaard, S.D. 2014. “Psychometric validation of the Hopkins Symptom Checklist (SCL-90) subscales for depression, anxiety, and interpersonal sensitivity.” Journal of Affective Disorders 160:98-103.
Bearman, Peter S. and James Moody. 2004. “Suicide and Friendships Among American Adolescents.” American Journal of Public Health 94:89–95.
Berkman, Lisa F., Thomas Glass, Ian Brissette, and Teresa E. Seeman. 2000. “From Social Integration to Health: Durkheim in the New Millennium.” Social Science & Medicine 51:843–57.
Blanchard, E.B., Jones-Alexander, J., Buckley, T.C., and Forneris, C.A. 1996. “Psychometric properties of the PTSD Checklist (PCL).” Behavior Research and Therapy 34:669–673.
Bourdieu, Pierre. 1986. “The Forms of Capital.” Pp. 241-58 in Handbook of Theory and Research for the Sociology of Education, edited by John G. Richardson. Westport, CT: Greenwood Press.
Burnett, A. and Michael Peel. 2001. “Health Needs of Asylum Seekers and Refugees.” BMJ (Clinical Research Ed.) 322 (7285): 544–47.
Cornwell, Benjamin. 2009. “Good Health and the Bridging of Structural Holes.” Social Networks 31:92–103.
Cornwell, Benjamin and Edward O. Laumann. 2011. “Network Position and Sexual Dysfunction: Implications of Partner Betweenness for Men.” American Journal of Sociology” 117 (1): 172-208.
Derogatis LR. 1974. “The Hopkins Symptom Checklist (HSCL): A self-report symptom
inventory”. Behavioral Science 19:1-15.
Durkheim, Emile. 1897:1966. Suicide. New York: Free Press Macmillan.
47

Fazel, Mina, Jeremy Wheeler, and John Danesh. 2005. “Prevalence of serious mental disorder in 7000 refugees resettled in western countries: A systematic review.” The Lancet 365:1309-1314.
Foa, Edna, B., David Riggs, Constance Dancu, and Barbara Rothbaum. 1993. “Reliability
and Validity of a Brief Instrument for Assessing Post-Traumatic Stress Disorder.” Journal of Traumatic Stress 6:459-473.
Goodkind Jessica R. 2005. “Effectiveness of a Community-Based Advocacy and
Learning Program for Hmong Refugees.” American Journal of Community Psychology 36:387-408.
Goodkind, Jessica R., Julia Hess, Brian Isakson, Marianna LaNoue, Ann Githinji, Natalie Roche, Kathryn Vadnais, and Danielle P. Parker. 2014. “Reducing Refugee Mental Health Disparities: A Community-Based Intervention to Address Postmigration Stressors With African Adults.” Psychological Services 11(3):333-346.
Goodkind, Jessica R., Panfua Hang, and Mee Yang. 2004. “Hmong Refugees in the United States: A Community-Based Advocacy and Learning Intervention.” Pp. 295-334 in The Mental Health of Refugees, edited by K.E. Miller and L.M. Rascoe. Mahwah, NJ: Lawrence Erlbaum Associates, Inc.
Gorst-Unsworth, C., and E. Goldenberg. 1998. "Psychological Sequelae of Torture and Organised Violence Suffered by Refugees from Iraq. Trauma-Related Factors Compared with Social Factors in Exile." The British Journal of Psychiatry 172(1):90-94.
Granovetter, Mark S. 1973. “The Strength of Weak Ties.” American Journal of Sociology
1360–80.
Gwozdziewycz, Nicolas, and Lewis Mehl-Madrona. 2013. “Meta-Analysis of the Use of Narrative Exposure Therapy for the Effects of Trauma Among Refugee Populations.” The Permanente Journal 17(1):70–76.
Harpviken, Kristian Berg. 2009. Social Networks and Migration in Wartime Afghanistan. Basingstoke: Palgrave Macmillan.
Holmes, Seth, Jennifer Burrell and Heide Castaneda. 2015. “American Politicians’ Reactions to Refugees Echo Past Xenophobia: Which Side of History Do We Want To Be On?” Huffington Post, November 20, Retrieved April 10, 2016 (http://www.huffingtonpost.com/american-anthropological-association/american-politicians-reac_b_8611446.html ).
Horn, Heather. 2015. “Is Eastern Europe Any More Xenophobic Than Western Europe?:
Investigating a stereotype of the refugee crisis” The Atlantic , October 16. Retrieved April 10, 2016
48

(http://www.theatlantic.com/international/archive/2015/10/xenophobia-eastern-europe-refugees/410800/).
Jordans, Mark J D, Ivan H Komproe, Wietse A Tol, Aline Ndayisaba, Theodora Nisabwe, and Brandon A Kohrt. 2012. “Reintegration of Child Soldiers in Burundi: A Tracer Study.” BMC Public Health 12(1):905.
Kaaya, S.F., Fawzi, M.C.S., Mbwambo, J.K., Lee, B., Msamanga, G.I., and Fawzi, W. 2002. “Validity of the Hopkins Symptom Checklist-25 amongst HIV-positive pregnant women in Tanzania”. Acta Psychiatrica Scandinavica 106:9-19.
Kadushin, Charles. 2012. Understanding Social Networks: Theories, Concepts, and
Findings. New York: Oxford University Press. Kaplan, Thomas and Wilson Andrews. 2015. “Presidential Candidates on Allowing
Syrian Refugees in the United States.” The New York Times, November 17. Retrieved April 10, 2016 (http://www.nytimes.com/interactive/2015/11/17/us/politics/presidential-candidates-on-syrian-refugees.html?_r=0).
Kawachi, Ichiro. 2010. “Social Capital and Health.” 2010. Pp. 18-32 in Handbook of Medical Sociology, edited by C.E. Bird, P. Conrad, A.M. Fremont, and S. Timmermans. Nashville: Vanderbilt University Press.
Kawachi, Ichiro, and Lisa F. Berkman. 2001. “Social Ties and Mental Health.” Journal of Urban Health 78(3):458–67.
Keown-Bomar, Julie. 2004. Kinship Networks among Hmong-American Refugees. New York: LFB Scholarly Publishing LLC.
Lamba, Navjot K., and Harvey Krahn. 2003. “Social Capital and Refugee Resettlement: The Social Networks of Refugees in Canada.” Journal of International Migration and Integration 4(3):335–60.
McPherson, Miller, Lynn Smith-Lovin, and James M. Cook. 2001. “Birds of a Feather: Homophily in Social Networks.” Annual Review of Sociology 27: 415–44.
Miller, Kenneth E., Stevan M. Weine, Alma Ramic, Nenad Brkic, Zvezdana Djuric Bjedic, Amer Smajkic, Esad Boskailo, and Greg Worthington. 2002. “The Relative Contribution of War Experiences and Exile-Related Stressors to Levels of Psychological Distress among Bosnian Refugees.” Journal of Traumatic Stress 15 (5): 377–87.
Miller, Kenneth E., Patricia Omidian, Andrew Rasmussen, Aziz Yaqubi, and Haqmal Daudzai. 2008. “Daily Stressors, War Experiences, and Mental Health in Afghanistan.” Transcultural Psychiatry 45(4):611-636.
49

Mollica, Richard F., Yael Caspi-Yavin, Paola Bollini, Toan Truong, Svang Tor, and James Lavelle. 1992. “The Harvard Trauma Questionnaire.” The Journal of Nervous and Mental Disease 180(2):111–16.
Mollica RF, Sarajlic N, Chernoff M, Lavelle J, Sarajlic Vukovic I, Massagli MP. 2001. “Longitudinal study of psychiatric symptoms, disability, mortality, and emigration among Bosnian refugees.” JAMA: Journal of the American Medical Association 286:546-54.
Monsutti, Alessandro. 2005. War and Migration: Social Networks and Economic
Strategies of the Hazaras of Afghanistan. Middle East studies: history, politics, and law; Middle East studies. New York: Routledge.
Murray, Kate E. and Graham R. Davidson. 2010. “Review of Refugee Mental Health Interventions Following Resettlement: Best Practices and Recommendations.” American Journal of Orthopsychiatry 80(4):576-585.
Perera, Sulani, Margaret Gavian, Patricia Frazier, David Johnson, Marline Spring, Joseph Westermeyer, James Butcher, Linda Halcon, Cheryl Robertson, Kay Savik, and James Jaranson. 2013. “A Longitudinal Study of Demographic Factors Associated With Stressors and Symptoms in African Refugees.” American Journal of Orthopsychiatry 83(4):472-482.
Pham, Phuong, N., Patrick Vinck, Didine, Kaba Kinkodi, and Harvey M. Weinstein. 2010. “Sense of Coherence and Its Association With Exposure to Traumatic Events, Posttraumatic Stress Disorder, and Depression in Eastern Democratic of Congo.” Journal of Traumatic Stress 23(3):313-321.
Pearce, Lisa, D. 2012. “Mixed Methods Inquiry in Sociology.” American Behavioral Scientist. 56(6):829-848.
Porter, Matthew and Nick Haslam. 2005. “Predisplacement and Postdisplacement Factors Associated With Mental Health of Refugees and Internally Displaced Persons.” Journal of the American Medical Association 294(5):602-612.
Portes, Alejandro and Min Zhou. 1993. “The New Second Generation: Segmented Assimilation and its Variants,” The Annals of the American Academy of Political and Social Science 530:74-96.
Rees, Brian, Fred Travis, David Sharpiro, and Ruth Chant. 2010. “Resilience and Crime Victimization.” Journal of Traumatic Stress 23(2):215–22.
Roberts, Bayard, Eliaba Yona Damundu, Olivia Lomoro, and Egbert Sondorp. 2009. “Post-Conflict Mental Health Needs: A Cross-Sectional Survey of Trauma, Depression and Associated Factors in Juba, Southern Sudan.” BMC Psychiatry 9(7):1–10.
50

Ruggiero, Kenneth J., Kevin Del Ben, Joseph R. Scotti, and Aline E. Rabalais. 2003. “Psychometric Properties of the PTSD Checklist - Civilian Version.” Journal of Traumatic Stress 16(5):495-502.
Schweitzer, Robert, Fritha Melville, Zachary Steel, and Philippe Lacherez. 2006. “Trauma, Post-Migration Living Difficulties, and Social Support as Predictors of Psychological Adjustment in Resettled Sudanese Refugees.” Australian and New Zealand Journal of Psychiatry 40(2):179–87.
Smith, L. Ripley. 2013. “Female Refugee Networks: Rebuilding Post-Conflict Identity.” International Journal of Intercultural Relations 37 (1):11–27.
Song, Lijun. 2010. “Social Capital and Psychological Distress.” Journal of Health and Social Behavior 52(4):478-492.
Thoits, Peggy A. 2011. “Mechanisms Linking Social Ties and Support to Physical and Mental Health.” Journal of Health and Social Behavior 52:145–61.
Tsai, Alexander C. and Andrew V. Papachristos. 2015. “From Social Networks to Health: Durkheim after the Turn of the Millennium.” Social Science & Medicine 125:1-7.
Umberson, Debra, and Jennifer Karas Montez. 2010. “Social Relationships and Health A Flashpoint for Health Policy.” Journal of Health and Social Behavior 51(Special Issue):S54–66.
United Nations High Commissioner For Refugees. 2015. “Statistics and Operational Data” Retrieved April 15, 2016 (http://www.unhcr.org/pages/49c3646c4d6.html).
United States Citizenship and Immigration Services. N.d. Refugees. Retrieved April 15, 2016 (https://www.uscis.gov/humanitarian/refugees-asylum/refugees).
United States Committee for Refugees and Immigrants. 2015. “Frequently Asked
Questions”, June 16. Retrieved April 15, 2016 (http://www.refugees.org/about-us/faqs.html#Difference).
Weathers, F.W., Litz, B.T., Keane, T.M., Palmieri, P.A., Marx, B.P., & Schnurr, P.P.
2013. “The PTSD Checklist for DSM-5 (PCL-5)”. National Center for PTSD Retrieved April 15, 2016 (http://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp).
Wei, Meifen, Pei-Chun Tsai, Ruth Chu-Lien Chao, Yi Du, and Shu-Ping Lin. (2012).
“Advisory Working Alliance, Perceived English Proficiency, and Acculturative Stress” Journal of Counseling Psychology 59(3)437-448.
Weine SM, Becker DF, McGlashan TH, Laub D., Lazrove S., Vojvoda D., and Hyman L.
1995. "Psychiatric Consequences of "ethnic Cleansing": Clinical Assessments and
51

Trauma Testimonies of Newly Resettled Bosnian Refugees." The American Journal of Psychiatry 152(4):536-42.
Wellman, Barry and Scot Wortley. 1990. “Different Strokes from Different Folks:
Community Ties and Social Support.” American Journal of Sociology: 96(3)558–88.
Zong, Jie and Jeanne Batalova. 2016. “Frequently Requested Statistics on Immigrants and Immigration in the United States.” Migration Policy Institute, April 14. Retrieved April 19, 2016 (http://www.migrationpolicy.org/article/frequently-requested-statistics-immigrants-and-immigration-united-states).
52









![Identify key features and characteristics of atmospheric, geological, hydrological, and biological systems as they relate to aquatic environments.[AQS.4A]](https://img.pdfslide.net/doc/110x75/56649e735503460f94b7228a/identify-key-features-and-characteristics-of-atmospheric-geological-hydrological.jpg)