Embed Size (px)
Citation preview

1
Social Protection and Food Assistance for Vulnerable Groups in Lesotho
Country: LESOTHO
Project No: PRRO 10599.0
Duration: 32 months (1 May 2008 – 31 December 2010)
Number of beneficiaries: 150,000 (annual average)
WFP food tonnage: 36,047 mt
WFP food cost: US$18,752,245
Total cost to WFP: US$31,900,844
Executive Summary
Food insecurity, poverty and HIV are profoundly interrelated in Lesotho. The past decade has seen a decline of nearly all human index indicators due to this negative synergy. Food security largely depends on households’ purchasing power as fewer than 5 percent of households produce enough food for their families1 even in normal times. The current situation of food insecurity has been caused by three shocks to real incomes: unemployment, an increase in the price of staple foods, and the HIV and AIDS pandemic. As labour opportunities in South Africa have declined, unemployment has risen in Lesotho, and households’ incomes have concomitantly decreased. Recent droughts have also increased unemployment as agricultural labour opportunities have become much scarcer. Secondly, the price of maize on the local markets has doubled over 2005 prices2, creating severe food access problems for the poor. Lesotho’s high HIV prevalence of 23.2 percent has resulted in chronically ill people leaving the labour market to seek care at home. This not only decreases households’ income but also aggravates the drain on household resources. In this PRRO, WFP seeks to help households mitigate the impact of this destructive cycle through a social protection approach that combines relief and recovery activities. The PRRO will not only address the short-term food needs of vulnerable groups, such as HIV and AIDS, and TB patients undergoing treatment, mothers in Mother and Child Health (MCH) treatment programmes, malnourished children under five and Orphans and Vulnerable Children (OVC), but will also their promote livelihood recovery through food for work/assets programmes and sustainable livelihoods projects. Building the capacity of key government ministries to design, manage, and implement food security-related national social safety-net programmes constitutes a key aspect of WFP’s exit strategy. Consequently, a nutrition education and capacity-building component is also included in the PRRO. The focus will be on ensuring that food and nutrition programming
1 Lesotho Poverty Reduction Strategy 2 Ministry of Trade and Industry (May 2007 CPI)

2
form an integral part of national HIV-AIDS and social safety-net policies, with the prospect of WFP-assisted target groups benefiting from these schemes beyond 2010. The proposed PRRO is consistent with priorities outlined in the Government of Lesotho’s (GoL) Poverty Reduction Strategy (PRS); the National AIDS Strategic Plan (NASP) and the Food Security Policy Action Plan. The PRRO supports WFP’s Strategic Objective 2: Protect livelihoods in crisis situations and enhance resilience to shocks and Millennium Development Goals (MDGs) 1 & 7; Strategic Objective 3: Support the improved nutrition and health status of children, mothers and other vulnerable people and MDGs 4, 5 and 6; Strategic Objective 4: Support access to education and reduce gender disparity in access to education and skills training and MDGs 2 and 3; and Strategic Objective 5: Strengthen the capacities of countries and regions to establish and manage food assistance and hunger reduction programmes and MDGs 1 – 6.
1. SITUATION ANALYSIS AND SCENARIO(S) (a) The overall context 1. The Kingdom of Lesotho is home to 1.88 million Basotho people. The country is
entirely surrounded by the Republic of South Africa, causing Lesotho’s economy to be very sensitive to trends in that country. Lesotho is also mountainous, ranging in altitude from 1500m to 3500m, which results in ongoing challenges in infrastructure such as rural roads, electrification and communication. Lesotho’s topography also results in a fragile agro-ecology that is very sensitive to climate changes.
2. Lesotho suffers from highly variable and extreme weather conditions. The 2003/2004
and 2004/2005 agricultural seasons were affected by below-normal rainfall and the 2006/07 season suffered one of Lesotho’s worst droughts in over 30 years. Weather patterns also include the opposite extreme: the 2005/2006 season was plagued by above-normal rainfall, which delayed planting because of water-logged fields. Early frosts and erratic hailstorms were also experienced, causing the extensive destruction of crops and property. The 2007/2008 season is forecast to be similar, as above-average rainfall has been predicted by the Eleventh Southern Africa Regional Climate Outlook Forum, and two violent hailstorms have already been experienced on 4 December 2007 and 4 January 2008.
3. Lesotho is a food-deficit country, importing around 50 percent of its staple grain needs,
of which 30 percent is covered by informal cross-border trade and food aid. Maize is the country’s staple food, and it imports at least 220,000 mt annually.
4. The combination of poverty, increasing food insecurity, and the effects of the HIV
pandemic have caused human development indicators to deteriorate over the last decade. Life expectancy has dropped from 57 years in 1997 to 35.2 years in 20043. The country’s Human Development Index (HDI) ranking fell steadily from 127 out of 174 countries in 1998 to 149 out of 177 countries in 2006. In 2003, 56.6 percent of the
3 UNDP, HDR 2006

3
HIV Prevalence in Adults 15-49 Years (Source 2004 LDHS)
0
10
20
30
40
50
15-19 20-24 25-29 30-34 35-39 40-44 45-49
Age Group
Prev
alen
ce(%
)
Women
Men
population fell below the poverty line, a negligible improvement from 58 percent in 19954. The Gini coefficient has also worsened, from 0.52 in 1995 to 0.57 in 2003 and 0.67 in 2008.
5. The current HIV prevalence is 23.2 percent, the third highest rate in the world, and TB prevalence is the second highest. According to GoL/UNAIDS estimates, approximately 254,000 adults and 16,000 children are infected by HIV. Antiretroviral treatment for HIV has only been available in Lesotho in limited areas since 2005 but access is now rapidly expanding, including Prevention of Mother-to-Child Transmission (PMTCT) programmes for HIV-positive pregnant and nursing women. The HIV prevalence in bordering South African provinces is: Free State (31.1 percent), Kwazulu Natal (39.1 percent) and Eastern Cape (29 percent)5.
Figure 1: 6. The pandemic has already resulted in a crisis of orphans, with over 180,000 orphans
and vulnerable children in Lesotho. At least 100,000 are attributed to parental deaths due to AIDS. This has resulted in an increase of elderly, single-parent and child-headed households, which are more likely to suffer from poverty and food insecurity.
7. Poor households depend on agricultural or casual labour as their most important source
of cash income, making up to 45 percent of their total annual income. In the rural mountains, the poorest geographical area, income from agricultural labour contributes 35-40 percent of annual food consumed.6
(b) The food security and nutrition situation 8. In 2006, the Lesotho Vulnerability Assessment Committee (LVAC) determined that
245,739 people (about 14 percent of the population) were experiencing household food deficits. By June 2007, as indicated in the LVAC report, the level of food insecurity had nearly doubled to 553,300 people or over 30 percent of the population.7
4 2002/3 Household Budget Survey Report, Lesotho 5 South African Department of Health, “National HIV and Syphilis Sero-prevalence Survey in South Africa 2006”, published in 2007 6 Lesotho Vulnerability Assessment Committee, June 2007 7 Lesotho Vulnerability Assessment Committee, June 2007
4
Child Malnutrition Prevalence( LVAC 2006)
05
1015202530354045
2002 2004 2006
Per
cent
age
ofch
ildre
n
WastingUnderweightStunting
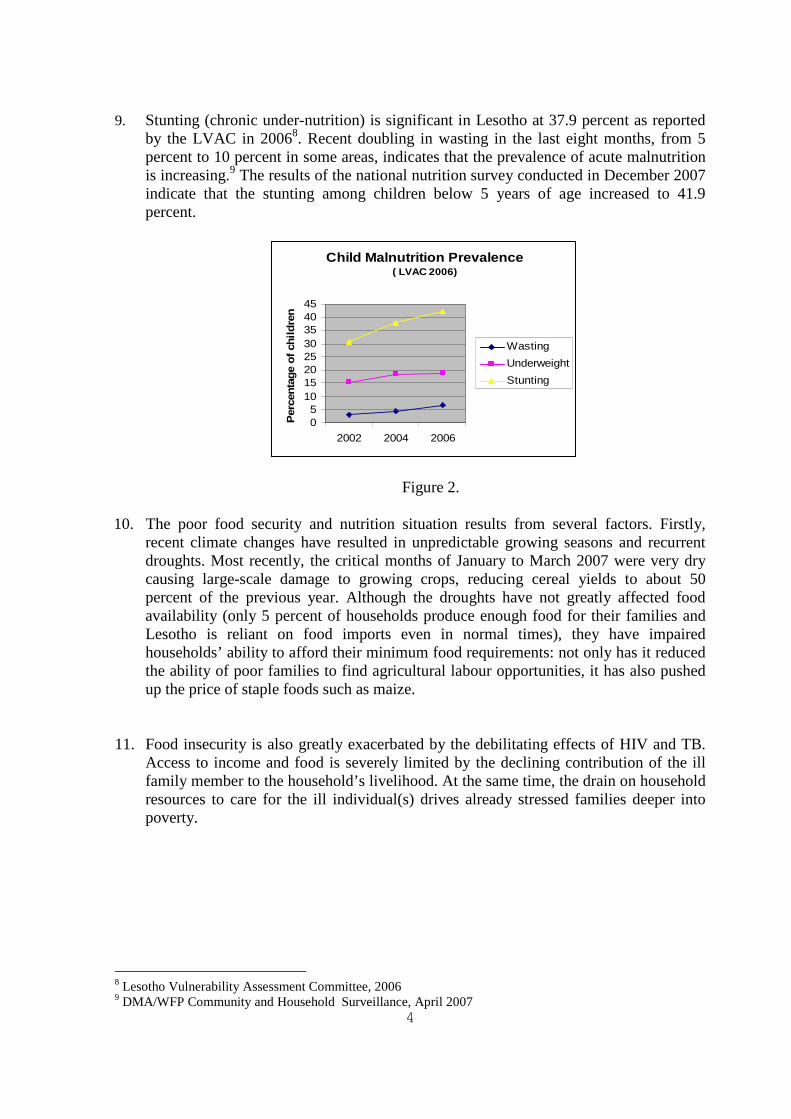
9. Stunting (chronic under-nutrition) is significant in Lesotho at 37.9 percent as reported by the LVAC in 20068. Recent doubling in wasting in the last eight months, from 5 percent to 10 percent in some areas, indicates that the prevalence of acute malnutrition is increasing.9 The results of the national nutrition survey conducted in December 2007 indicate that the stunting among children below 5 years of age increased to 41.9 percent.
Figure 2.
10. The poor food security and nutrition situation results from several factors. Firstly, recent climate changes have resulted in unpredictable growing seasons and recurrent droughts. Most recently, the critical months of January to March 2007 were very dry causing large-scale damage to growing crops, reducing cereal yields to about 50 percent of the previous year. Although the droughts have not greatly affected food availability (only 5 percent of households produce enough food for their families and Lesotho is reliant on food imports even in normal times), they have impaired households’ ability to afford their minimum food requirements: not only has it reduced the ability of poor families to find agricultural labour opportunities, it has also pushed up the price of staple foods such as maize.
11. Food insecurity is also greatly exacerbated by the debilitating effects of HIV and TB. Access to income and food is severely limited by the declining contribution of the ill family member to the household’s livelihood. At the same time, the drain on household resources to care for the ill individual(s) drives already stressed families deeper into poverty.
8 Lesotho Vulnerability Assessment Committee, 2006 9 DMA/WFP Community and Household Surveillance, April 2007

5
Table 1: National Health Indicators10
Index Rate Infant mortality 91 deaths /1000 live births Under 5 mortality 113 deaths/1000 live births Maternal mortality 762/100,000 live births Deaths due to AIDS 63 percent
12. Finally, food insecurity has been aggravated by the massive retrenchments in South African mines. Domestic opportunities have not filled the gap as the unemployment rate in Lesotho currently stands at 30 percent.
(c) Scenarios 13. Lesotho is suffering the consequences of one of its worst droughts in three decades.
Considering the impact that this has had on poverty, compounded by the negative impact of the HIV and AIDS pandemic on the country’s socio-economic development, there is little doubt that a significant proportion of the poor will continue to experience household food insecurity in the coming years.
14. Furthermore, future weather-based shocks and the lasting impact of HIV in the coming
years, compounded by the absence of any sound early warning mechanism, will most likely result in a future food emergency requiring intervention by WFP.
15. Although food insecurity has many negative consequences, one of these is especially
pernicious: The number of people needing ART in 2008 has increased to 80,000 although it is projected that by 2010 it might go down to 70,000 patients. Although the National AIDS Strategic Plan aims to cover 80 percent of this need and 100 percent of the HIV-positive women needing Prevention of Mother to Child Transmission (PMTCT) treatment to prevent transmission, ARV and TB treatments require proper and adequate nutrition in order to be fully effective. Pervasive food insecurity, by making it difficult for patients to meet their nutritional requirements, will therefore aggravate the impact of AIDS on Lesotho’s socio-economic development.
2. POLICIES, CAPACITIES AND ACTIONS OF THE GOVERNMENT AND OTHERS (a) Policies, capacities and actions of the government 16. In 2004, the Government of Lesotho launched its Poverty Reduction Strategy (PRS)
2004-2007, which emphasised eight priorities and three cross-cutting issues to focus on reducing poverty. The PRRO activities are directly aligned with three of these PRS concerns, namely food security, HIV and AIDS, and job creation. The next PRS for the period of five years (2008-12), which is under preparation, is expected to maintain the focus on these areas.
10 Demographic and Household Survey, 2004
6
17. The National Action Plan for Food Security outlines specific policies aiming to promote sustainable food production, address the micronutrient requirements for HIV and AIDS-affected households, and offer training in nutrition, crop production, and input supply to vulnerable households. The Ministry of Agriculture and Food Security (MoAFS) has undertaken many of these projects and will be a vital partner in the implementation of this PRRO.
18. The National AIDS Strategic Plan specifies targets for ART and PMTCT roll-out and
coverage that will directly impact on the implementation of this PRRO. 19. The LVAC, under the Disaster Management Authority (DMA), conducts annual
assessments of food security status providing data that is used for planning and targeting.
(b) Policies, capacities and actions of other major actors 20. The Government, in collaboration with other major actors, has been involved in
addressing the HIV and AIDS pandemic, but the focus has been on treatment, with very little attention given to food and nutrition support. However a concerted effort to address HIV-related food insecurity is now being made by WFP as well as other major food security stakeholders, such as FAO, UNICEF, Partners In Health, World Vision, CRS and The Clinton Foundation.
(c) Coordination 21. Within the United Nations system, all United Nations HIV-related activities are
coordinated through the Joint UN Team on AIDS. WFP serves as the technical lead for the team’s Nutrition Thematic Group, providing leadership in developing activities in support of the National HIV and AIDS Strategic Plan and the Joint Programmes of Support.
22. WFP is one of the core team members of the UN Food Security and Nutrition Task Force. This group, along with other UN agencies including, FAO, UNICEF, WHO and
PRS Priorities1. Job Creation 2. Food Security 3. Infrastructure 4. Governance 5. Health Care Quality and
Access 6. Education Quality and
Access 7. Environment 8. Public Service Delivery
PRS Cross-cutting Issues
1. HIV and AIDS 2. Gender 3. Children and Youth

7
UNDP, coordinates food security-related issues and provides advice to government counterparts. The UN Task Force collaborates with the National Task Force on Food Security to discuss food security-related topical issues and advise on appropriate responses to any food security crisis.
3. OBJECTIVES OF WFP ASSISTANCE 23. The PRRO aims to increase the food access of vulnerable households in areas of high
food insecurity and HIV prevalence.
The specific objectives of this PRRO (and related WFP Strategic Objectives/Millennium Development Goals) are to:
1. Increase the ability of food insecure households to protect their livelihoods and withstand external shocks.
(Strategic Objective 2: Protect livelihoods in crisis situations and enhance resilience to shocks - MDGs 1 & 7)
2. Safeguard health, nutrition and well-being of food insecure HIV and TB patients on antiretroviral, MCH and TB treatment programmes.
(Strategic Objective 3: Support the improved nutrition and health status of children, mothers and other vulnerable people - MDGs 4, 5 and 6)
3. Improve the nutrition and education status of orphans, vulnerable and malnourished children in food insecure households.
(Strategic Objective 3: Support the improved nutrition and health status of children, mothers and other vulnerable people - MDGs 4, 5 and 6, and Strategic Objective 4: Support access to education and reduce gender disparity in access to education and skills training - MDGs 2 and 3)
4. Enhance national capacity for the implementation of food-based social safety-net programming, including vulnerability assessment, monitoring of food security and nutrition surveillance.
(Strategic Objective 5: Strengthen the capacities of countries and regions to establish and manage food assistance and hunger reduction programmes – MDGs 1 – 6)
4. WFP RESPONSE STRATEGY (a) Nature and effectiveness of food-security related assistance to date.
24. Over the last decade, WFP has responded to recurrent large-scale emergencies in Lesotho in 1992, 1995 and 2002. Under EMOP 10290, WFP assisted 345,000 people from 2002 to 2004.
25. The regional PRRO 10310 followed from January 2005 to the end of April 2008. At its peak in 2005, this PRRO assisted some 450,000 vulnerable people in Lesotho. According to the 2006 mid-term evaluation of the PRRO, WFP’s food support notably contributed to increasing food access and averting a further deterioration of food insecurity in the region.

8
26. During this regional PRRO, food support for 7,000 TB patients was initiated. Sixty to sixty-five percent of those TB patients were also HIV-positive, and in some cases were on ARVs. The result of providing food support to these patients was highly encouraging.
27. WFP has supported school feeding in Lesotho for four decades. This year, the current
4-year programme, which expires on 31 December 2007, is supporting 115,000 children in 585 primary schools. The last 3-year school feeding project has been approved until 31 December 2010, at which time WFP expects to hand over the school feeding programme to the Government.
(b) Strategy outline 28. The PRRO will adopt a social protection approach that combines relief and recovery
activities. Short-term food assistance will be provided through an initial phase of targeted food relief, followed by livelihood recovery activities with partial food support.
29. The PRRO is designed to cover a period of 32 months, with a decreasing beneficiary caseload over time as intended outcomes are realized and food access and livelihoods are restored in the high food deficit communities. The rationale behind this duration is to coincide with the completion date of the school feeding project on 31 December 2010, so as to support a review of WFP’s future strategy in the country.
30. The capacity building of local government partners is also an integral part of the PRRO’s strategy, in order to ensure the project’s future sustainability.
Relief Component 31. During the relief phase, the PRRO will focus relief efforts on providing food and
nutritional support to the following vulnerable segments of the population:
• Food insecure people on ART: initial 9 months of the treatment programme.
• Food insecure patients on Directly Observed TB Treatment Short Courses (DOTS) Treatment: 7 months.
• Food insecure mothers on MCH treatment programmes: from 28 weeks into their pregnancy until the crucial first nine months of breastfeeding.
• Malnourished children under five years of age.
• Orphans and vulnerable children (OVC) in food insecure households, particularly those under the age of 15; they will receive a take-home ration. This support complements the WFP-assisted school feeding programme. Implementation of this intervention will be done by cooperating partners in
9
conjunction with the Ministry of Health and Social Welfare (MoHSW), the Ministry of Education and Training (MoET) and UNICEF.
• A family ration will also be provided to beneficiary households in order to protect the ration of chronically ill persons or the malnourished child and contribute to the family’s access to food during the illness.
32. As part of WFP’s 2007/8 drought response, free food distributions/vulnerable group feeding (FFD/VGF) are being provided to vulnerable households under the ongoing regional PRRO 10310, which will cover vulnerable households until the termination of the operation in April 2008. In view of the prospect of further droughts and corresponding relief requirements, additional relief needs have been considered in the contingency plan for 2009 and 2010 and would be covered under the relief component of this PRRO through a budget revision.
Recovery Component 33. In the social protection approach, which this PRRO follows, food aid is not a stand
alone support but part of a comprehensive package, which includes nutrition training, homestead gardening, skills transfer, HIV and AIDS education, etc. This PRRO particularly focuses on nutrition education and livelihood recovery activities.
34. Nutrition education is vital for four groups in particular: patients on ARVs and TB
medication, mothers, Village Health Workers and health professionals, including clinicians and MoHSW policy-makers. WFP will work with MoHSW and MoAFS to coordinate with district-level nutritionists and community extension workers on nutrition education and outreach. WFP will also emphasise this component in developing the country’s Joint UN Programme of Support for HIV-AIDS.
35. Livelihood recovery activities will be developed through programmes like Food for
Work (FFW)/Food for Assets (FFA). FFW/FFA will aim at the creation of gardens and the production of a wider variety of vegetables and other unconventional crops for small farmers, as well as the adoption of conservation farming techniques and key hole gardening production.
WFP will provide a family ration as a transitional support while households are engaged in these livelihood programmes.
Capacity-building Component 36. Capacity-building support will be provided specifically to the MoHSW and DMA,
WFP’s main partners for this PRRO.
37. Technical assistance will be provided to the MoHSW through the provision of a UNV to support the development of food and nutrition programmes in conjunction with national HIV-AIDS response strategies. A strong focus will be the improved use of data and information for planning (an internal goal expressed by the Ministry).

10
38. Ongoing technical support to LVAC will continue under this PRRO through the secondment of a UNV Specialist. The objective is to strengthen the institutionalisation of the LVAC and its capacity to conduct vulnerability assessments and food security monitoring to integrate the WFP Community and Household Surveillance (CHS) into the LVAC analytical framework, and to strengthen nutrition surveillance that is coordinated by the Food and Nutrition Coordination Office (FNCO).
39. WFP, jointly with FAO, will also provide assistance in specific areas of agronomy to
the Ministry of Agriculture and Food Security. Assistance will focus on recovery projects, such as, conservation farming and irrigation projects at the village level.
Cash transfer or vouchers pilot 40. This PRRO will also support a pilot programme to explore the potential use of cash
transfers or vouchers in conjunction with food-based relief and/or recovery, if and where possible. There is growing evidence that cash assistance is viable and effective in Lesotho in certain circumstances. The Ministry of Forestry has already begun a cash-for-work programme to support small farmers affected by the drought, and the MoHSW will be using a cash transfer system over the next four years in its OVC support programme, funded by the EC through UNICEF.
(c) Handover strategy 41. WFP will strongly encourage the MoHSW to include food and nutrition programming
as an integral part of its HIV-AIDS strategy, particularly in coordination with its ART roll-out plan. The MoHSW has already been increasing allocations of funds in its budget for food and nutrition programming through the Partners in Health (PIH). A national social safety-net programme is also being formulated to deal with vulnerable segments of the population, and WFP foresees its beneficiaries benefiting from these government schemes beyond 2010. Furthermore, WFP has already been successful in transferring activities to the Government, as witnessed in the school feeding project.
5. BENEFICIARIES AND TARGETING
42. Based on the analysis provided by the LVAC, the PRRO will employ a combination of geographic and individual vulnerability targeting by focusing on areas of high food insecurity and/or high HIV prevalence and targeting vulnerable individuals within these areas.
43. Lesotho’s rural population is spread across six livelihood zones, namely mountains, southern lowlands, northern lowlands, foothills, peri-urban and the Senqu river valley. According to the June 2007 LVAC report, the northern lowland areas do not face a food security problem; these areas have only 2 percent ‘very poor’ households. In rural areas, household’s food consumption is derived from their own crop production (40-45 percent of annual food consumption), from in-kind payment for agricultural labour (20-25 percent) and from food purchases on the market (15-20 percent). Casual labour

11
contributes 35-40 percent and pig sales contribute about 25-30 percent of annual cash income. The main coping strategies during crisis are to seek more casual labour opportunities and to increase pig sales.
44. Areas with higher food and expenditure deficits are as follows (from worst to better off) 11:
In peri-urban areas, individuals in “very poor” households are likely to face a per capita food deficit of 61 percent (i.e. they would normally be able to consume only 39 percent of the 2,100 kcal/person/day required to live a healthy and active life); in the mountains and Senqu river valley, individuals in “very poor” households are likely to face a per capita food deficit of 47 percent; in the southern lowlands, individuals in “very poor” households are likely to face a per capita food deficit of 43 percent; and in the foothills, individuals in “very poor” households are likely to suffer from a 38 percent food deficit. The livelihood profiles of the “poor”12 and “very poor”13 are common to most livelihood zones as all rely to some extent on own crop production and livestock rearing and depend heavily on casual labour.
45. Within the most food insecure livelihood zones, the PRRO will target the following individuals:
i) Food insecure individuals on ART, TB, and MCH programmes: These individuals will be identified through health facilities’ (hospitals/clinics) registers and will be referred for possible food assistance. Following this initial referral by social workers/local counsellors at the health clinics, a vulnerability questionnaire will be administered by social workers and/or cooperating partners to determine if the household is food insecure. The targeting of patients on these programmes is important as the ability to tolerate antiretroviral therapeutic toxicities used in PMTCT and ART programmes is closely linked to nutritional status.
ii) Malnourished children from 6 to 59 months: they will be identified through health centres and/or outpatient sites for malnourished children established by UNICEF and the MoHSW using the following criteria: WHZ between -2 and -3 or WHM < 80 percent without oedema, MUAC ≥ 110mm and ≤ 125mm.
iii) OVC (under age 15) from food insecure households and those who are still in primary school: they will receive a take-home ration, which will help support families hosting orphans, while promoting attendance and a continuation of schooling by the OVC. Initial lists of orphans will be provided by the MoHSW and the MoET and will be subjected to a vulnerability and food insecurity validation process by WFP and/or
11 Lesotho Food Security and Vulnerability Monitoring Report May-June 2007, LVAC, p.6-7; NB: some of the deficit could be made up through other sources, such as remittances, etc. 12 ‘Poor’ households engage in limited crop production, which contributes 15-25 percent of their annual food requirement; they also have limited livestock, a few chickens and/or a pig and depend heavily on casual labour for their food needs. 13 ‘Very poor’ households engage in very limited crop production, which contributes to less than 15 percent of their annual food requirement; they also normally have no livestock and depend heavily on casual labour for their food needs.

12
cooperating partners. In order to have a greater impact of food assistance on the OVC, the PRRO will be implemented in close collaboration with the upcoming OVC project, which is funded by the EC through UNICEF and implemented by MoHSW.
46. Livelihood recovery activities will primarily target those on ART and/or recovering from TB. Older OVC (over age 15 or having finished primary school) and household members of malnourished children, young OVC, or incapacitated patients, will also be eligible to participate in these activities.
47. The calculations of the target groups in Table 2 is based on the geographical
distribution of food insecurity (the level of food insecurity in the country during the 2007/2008 marketing year is estimated at 21 percent of the population14) and the current and projected levels of enrolment in HIV/TB/PMTCT treatment programmes. Targets for malnourished children are based on wasting levels, which result in the coverage of 10 percent of the children under five in target areas. The OVC targets are designed to link with and support the upcoming OVC project; thus the same number beneficiaries are covered as in the UNICEF-supported OVC project.
Table 2: Planned Beneficiaries by Type of Intervention
Type of Intervention 2008 (8 months, May – December)
2009 (12 months)
2010 (12 months)
RELIEF ACTIVITIES
Support to food insecure ART/TB and PMTCT clients (Individual Ration)
8,000 9,000 10,000
Support to corresponding ART/TB/PMTCT households (Family Ration)
24,000 27,000 30,000
Support to young OVC (Take-Home Rations) 60,000 60,000 50,000
Support to malnourished children (MCH) (Supplementary Feeding) 7,000 5,000 2,000
Support to corresponding MCH households (Family Ration) 21,000 15,000 6,000
RECOVERY ACTIVITIES
Sustainable Livelihoods (Individual Ration) (Food for Work/Assets, agriculture activities)
30,000 42,000 40,000
Yearly Totals (Main Activities) 150,000 158,000 138,000
14 CFSAM 2007: 401,200 vulnerable people facing food insecurity in the 2007/2008 marketing year, out of a total estimated population of 1,872,721.

13
6. NUTRITIONAL CONSIDERATIONS AND RATIONS 48. Shrubs and dry cow manure are the main sources of cooking fuel in rural Lesotho.
Though firewood is used by some households, its availability is extremely limited. Water collection points are generally accessible in the villages. Hand and foot pumps are available, including gravitational water delivery in some of the mountain areas. Rural water and sanitation conditions have improved substantially over the last ten years.
49. In rural areas, diet diversification is limited with a high proportion of carbohydrates (maize and sorghum) and a low proportion of protein, fats and micronutrients. Infant and young children feeding practices are generally inadequate. Only 36 percent15 of children under 6 months are exclusively breastfed. Vitamin A intake amongst young children and women is insufficient.
50. The WFP food basket will consist of fortified maize meal, pulses, vitamin-enriched vegetable oil and CSB. CSB, in particular, will be provided to the most nutritionally vulnerable beneficiaries – patients on ARVs or TB medication, women in PMTCT programmes, and malnourished children - to provide them with highly needed protein, micronutrients and an increased caloric intake. Family rations will not include CSB, nor will the OVC take-home ration since the ration for these groups is not intended to be the main source of food but a complementary one.
Table 3: Food Basket by Activity
(grams per person per day)
Type of Intervention Maize Meal
Pulses Oil CSB
(kcal/day)
Support to ART/TB/PMTCT treatment programmes (Individual Rations) 200
60
25
250
2,095
Support households with HIV and/or TB patient (Family Ration) 200
60
20
0 1,100
Support to MCH (Supplementary Feeding) 0 0 25
250
1,175
Support to MCH Households (Family Ration) 200
60
20
0 1,100
Support to OVC (Take-Home Rations) 200
60
20
0 1,100
Agriculture-Based Livelihoods Recovery 200
60
20
0 1,100
15 Lesotho Demographic and Health Survey (DHS) 2004
14
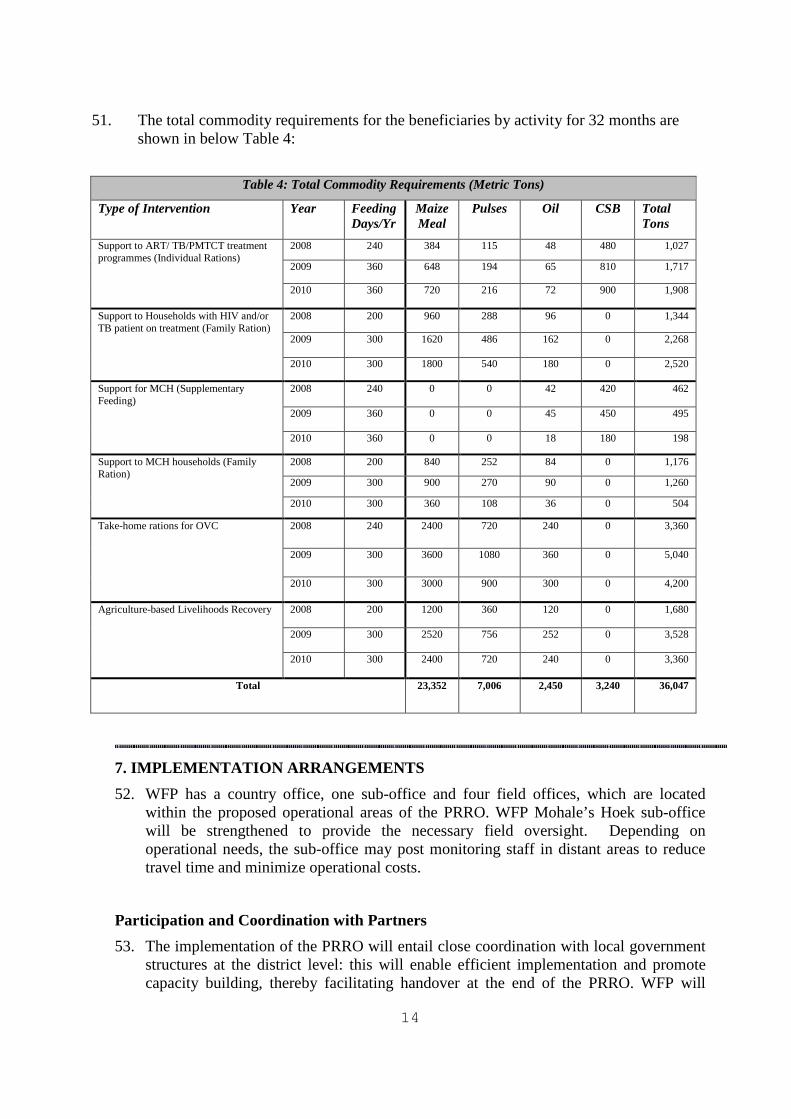
51. The total commodity requirements for the beneficiaries by activity for 32 months are shown in below Table 4:
Table 4: Total Commodity Requirements (Metric Tons)
Type of Intervention Year Feeding Days/Yr
Maize Meal
Pulses Oil CSB Total Tons
2008 240 384 115 48 480 1,027
2009 360 648 194 65 810 1,717
Support to ART/ TB/PMTCT treatment programmes (Individual Rations)
2010 360 720 216 72 900 1,908
2008 200 960 288 96 0 1,344
2009 300 1620 486 162 0 2,268
Support to Households with HIV and/or TB patient on treatment (Family Ration)
2010 300 1800 540 180 0 2,520
2008 240 0 0 42 420 462
2009 360 0 0 45 450 495
Support for MCH (Supplementary Feeding)
2010 360 0 0 18 180 198
2008 200 840 252 84 0 1,176
2009 300 900 270 90 0 1,260
Support to MCH households (Family Ration)
2010 300 360 108 36 0 504
2008 240 2400 720 240 0 3,360
2009 300 3600 1080 360 0 5,040
Take-home rations for OVC
2010 300 3000 900 300 0 4,200
2008 200 1200 360 120 0 1,680
2009 300 2520 756 252 0 3,528
Agriculture-based Livelihoods Recovery
2010 300 2400 720 240 0 3,360
Total 23,352 7,006 2,450 3,240 36,047
7. IMPLEMENTATION ARRANGEMENTS 52. WFP has a country office, one sub-office and four field offices, which are located
within the proposed operational areas of the PRRO. WFP Mohale’s Hoek sub-office will be strengthened to provide the necessary field oversight. Depending on operational needs, the sub-office may post monitoring staff in distant areas to reduce travel time and minimize operational costs.
Participation and Coordination with Partners 53. The implementation of the PRRO will entail close coordination with local government
structures at the district level: this will enable efficient implementation and promote capacity building, thereby facilitating handover at the end of the PRRO. WFP will

15
work with the District Administrator, Community Council and district-level offices in order to continue to utilise links with the Village Councils. The Village Councils will themselves facilitate the involvement of local groups, such as, Village Health Workers (VHWs), Village Disaster Management Teams and Village Relief Committees, thereby promoting community involvement.
54. For the implementation of the relief component, clinics and VHWs will be involved, working with partners to identify beneficiaries, monitor food distribution and usage, and prepare beneficiaries for the transition to recovery. Such activities will be facilitated by the coordination of monthly medical check-ups and food distribution schedules.
55. Recovery activities will be closely coordinated with the clinics to ensure that patients are integrated into livelihood recovery activities. Partners will work collaboratively with local village groups and beneficiaries in initiating livelihood activities that meet the needs and capabilities of the beneficiaries and their households. Extension agents of the Ministry of Agriculture and Food Security will continue to be involved as they can offer other food security enhancing training, such as food preservation techniques, homestead gardening and conservation farming projects, implemented by NGO partners and the Ministry of Agriculture and Food Security itself.
Commitments to Women 56. Food production, management, and consumption are typically the women’s domain in
Lesotho. The formulation of projects and their specific design characteristics (activities that ensure women’s participation and their access to assets) will ensure that women are actively involved and that their interests and preferences are given particular attention.
57. The packaging of cereals will be done in 25 kg bags to reduce the weight and transport
burden on women. Moreover, WFP will ensure that food distribution points are jointly agreed with local authorities, community leaders and women, in line with WFP’s Enhanced Commitments to Women (ECW) IV.5 to take into account travel distances and risks for women and girls from the distribution points to their respective homes. Food ration cards will continue to be issued in the name of women as much as possible.
58. Furthermore, gender targets will be formulated in agreement with cooperating partners to ensure that women constitute at least 50 percent or more of food management/local relief committees and that they continue serving in leadership positions. In addition, given that 68 percent of village council members and 90 percent of village health workers are women, women will naturally be an integral part of the planning and implementation processes on the ground.

16
59. Women will also make up the majority of beneficiaries. Taking into consideration the higher HIV and ARV prevalence among women16 as well as the women involved in PMTCT, 70 percent of adult beneficiaries on treatment will be women. Furthermore, the provision of household support to the families of patients or malnourished children will serve approximately 56 percent women due to an increasing number of female-headed households and the fact that these families are often at greater risk of food insecurity. Within the recovery component, at least 70 percent of the participants in food-assisted training, income-generating skills training, micro-enterprise and community leadership will be women.
Non-Food Inputs 60. The PRRO will provide a limited number of hand tools and materials for asset
creation/livelihood projects. Cooperating partners are expected to provide complementary training, tools, health/nutrition/HIV education, and limited agricultural inputs.
61. Technical assistance and supervision from relevant government ministries and departments will be provided to ensure that projects are sustainable and comply with standard specifications.
Logistics Arrangements 62. International food purchases will be shipped through the port of Durban, South Africa,
and trucked to Lesotho using Maseru Bridge as an entry point. Local and regional purchases will be transported directly to designated warehouses within the country.
63. District warehouses under the Food Management Unit (FMU) will continue to be used as Extended Delivery Points (EDPs) in the proposed operational areas. The total cumulative storage capacity of these warehouses is approximately 17,000 mt. These facilities will also be used for commodities earmarked for other purposes. In addition, the existing WFP transit warehouse in Maseru will be maintained, although its use will be reviewed after the first year, with a view to its possible closure and a transfer of the function to the FMU. The movement of food commodities from EDPs to Final Delivery Points (FDPs) will continue to be undertaken by the FMU.
64. The Commodity Tracking System (COMPAS) has been installed in three locations namely, Maseru, Mohale’s Hoek and Taba-sheka, and will track all commodity movements. COMPAS clerks attached to designated WFP sub- and field offices will provide assistance and support the FMU warehouse staff during the execution of this project.
65. There is a good local/regional cereals market. Though the local market prices of maize have increased significantly, prices in the region are still competitive. Emphasis will be
16 HIV prevalence for men aged 15-49 is 19.5 percent while for women it is 26.9 percent. The current ratio of female to male patients on ARVs is nearly 2 to 1.

17
placed on local cereal purchases where this is cost effective and does not adversely impact the market. It is estimated that donors would contribute about 33 percent of the total commodity requirements in-kind.
8. PERFORMANCE MONITORING 66. Community household surveillance (CHS) and Post Distribution Monitoring (PDM)
will be conducted on a quarterly basis to measure outputs and other results. The monthly food security data collection and analysis by VAM will be strengthened. Clinics will monitor the nutritional status of beneficiaries based on clinical assessment.
67. A monitoring and evaluation calendar will be prepared for the PRRO and will be updated quarterly to ensure that objectives are being met. Monitoring plans will be produced at field and country office levels and consolidated into the CO plan. Periodic joint monitoring visits will be organized by the WFP offices along with cooperating partners’ representatives to assess the level and quality of programme implementation. Random on-site monitoring will be carried out at food distribution points by WFP and/or the cooperating partners’ monitors.
9. RISK ASSESSMENT AND CONTINGENCY PLANNING (a) Risk assessment 68. The major risks envisaged for this PRRO are the limited resources of government
counterparts and NGO partners, and unpredictable donor contributions. These constraints could make procurement of food and NFIs difficult, thus impeding implementation of programme activities, especially recovery projects. In the event that partner resources are too limited for a comprehensive application of recovery activities, the CO will attempt to maximize the impact of available resources by scaling down projects to focus on areas where both relief and recovery can be fully implemented.
(b) Contingency Planning 69. The existing WFP Contingency Plan will be updated on an annual basis, using the
latest information generated from the Lesotho Meteorological Service, the Ministry of Agriculture, the Disaster Management Authority and other internal monitoring reports.
70. WFP will closely monitor and analyse periodic reports of the LVAC, CHS, weather forecasts, agro-meteorological quarterly bulletins and monthly food security monitoring reports to determine possible triggers for actions, such as, extreme weather situations or natural disasters.
71. In the event of a major food crisis requiring WFP intervention, the country office will request a budget revision to this PRRO to meet the increased food aid and operational requirements. The most likely scenario for a drought relief intervention would be the provision of assistance to 150,000 people.
18
10. SECURITY CONSIDERATIONS
72. There are no major security concerns within the country, which is in United Nations Security Phase One. The Security Management Team (SMT) meets regularly to review potential threats. While the political situation is stable (general election was held peacefully in February 2007) the potential security risk in the country is of a medium scale. Periodic security briefings are provided to all staff through the office of the resident UN Security Adviser. A security assessment of the WFP Lesotho Country Office was conducted in September 2007.
73. The WFP country office and Mohale’s Hoek sub-office are MOSS compliant, and these standards will be maintained and improved during the implementation of this project.
11. RECOMMENDATION
The Executive Director is requested to approve the proposed Protracted Relief and Recovery Operation for Lesotho No.10599.0, ‘Social Protection and Food Assistance for Vulnerable Groups in Lesotho’.
APPROVAL
………………………………. ……………………………….
Josette Sheeran Date:
Executive Director

19
Acronyms
AIDS Acquired Immune Deficiency Syndrome ART Antiretroviral Therapy ARV Antiretrovirals C-SAFE Consortium for the Southern Africa Food Security Emergency CHS Community Household Surveillance COMPAS Commodity Movement Processing and Analysis System CRS Catholic Relief Services CSB Corn Soya Blend CTS Commodity Tracking System DMA Disaster Management Authority ECW Enhanced Commitments to Women EDP Extended Delivery Point FDP Final Delivery Point FMU Food Management Unit FNCO Food and Nutrition Coordination Office HDI Human Development Index HIV Human Immunodeficiency Virus IGA Income Generating Activities LDHS Lesotho Demographic and Health Survey LENEPWHA Lesotho Network of People Living with HIV/AIDS LVAC Lesotho Vulnerability Assessment Committee MCH Mother and Child Health MIST Minimum Security Telecommunications Standards MoAFS Ministry of Agriculture and Food Security MoHSW Ministry of Health and Social Welfare MUAC Mid-upper arm circumference MOSS Minimum Operating Security Standards NASP National AIDS Strategic Plan NFI Non Food Items NGO Non Governmental Organisation OVC Orphans and Vulnerable Children PDM Post-Distribution Monitoring PMTCT Prevention of Mother to Child Transmission PRRO Protracted Relief and Recovery Operation PRS Poverty Reduction Strategy SMT Security Management Team UNV United Nations Volunteer VAM Vulnerability Analysis and Mapping WHM Weight for height as a percentage of the median WHZ Weight for height reference in z scores VHW Village Health Worker

20
ANNEX IA
WFP PROJECT COST BREAKDOWN
Quantity
(mt) Average cost (US$) per mt
Value
(US$)
COSTS
A. Direct operational costs
Maize Meal17 23,352 375.15 8,760,503
Pulses 7,005 815.92 5,715,520
Vegetable Oil 2,450 1144.82 2,804,809
Corn Soya Blend 3,240 454.14 1,471,414
Total commodities 36,047 520.22 18,752,245
External transport 2,186,251
Landside transport 1,413,618
ITSH 3,411,488
Total LTSH 4,825,106
Other direct operational costs 1,519,038
Total direct operational costs 27,282,640
B. Direct support costs (see table below for details) 2,531,233
C. Indirect support costs (7 percent of total direct costs) 2,086,971
TOTAL WFP COSTS 31,900,844
17 This is a notional food basket used for budgeting and approval purposes. The precise mix and actual quantities of commodities to be supplied to the project, as in all WFP-assisted projects, may vary over time depending on the availability of commodities to WFP and domestically within the recipient country.
21
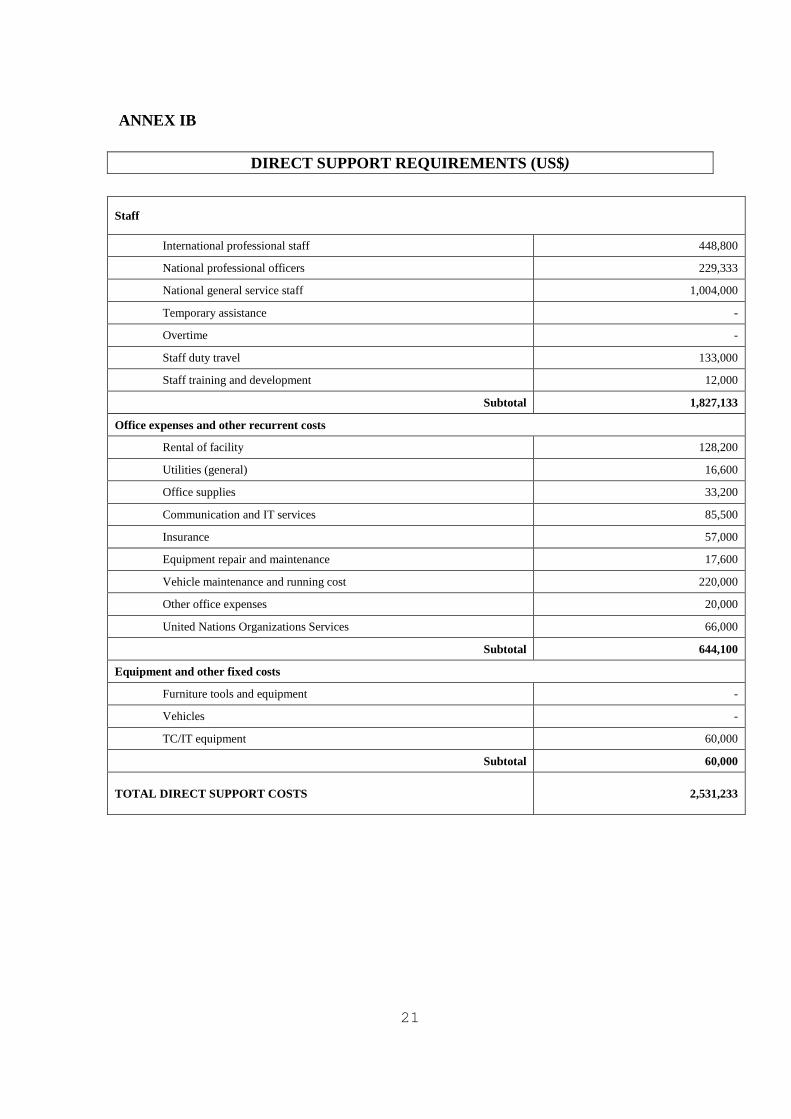
ANNEX IB
DIRECT SUPPORT REQUIREMENTS (US$)
Staff
International professional staff 448,800
National professional officers 229,333
National general service staff 1,004,000
Temporary assistance -
Overtime -
Staff duty travel 133,000
Staff training and development 12,000
Subtotal 1,827,133
Office expenses and other recurrent costs
Rental of facility 128,200
Utilities (general) 16,600
Office supplies 33,200
Communication and IT services 85,500
Insurance 57,000
Equipment repair and maintenance 17,600
Vehicle maintenance and running cost 220,000
Other office expenses 20,000
United Nations Organizations Services 66,000
Subtotal 644,100
Equipment and other fixed costs
Furniture tools and equipment -
Vehicles -
TC/IT equipment 60,000
Subtotal 60,000
TOTAL DIRECT SUPPORT COSTS 2,531,233
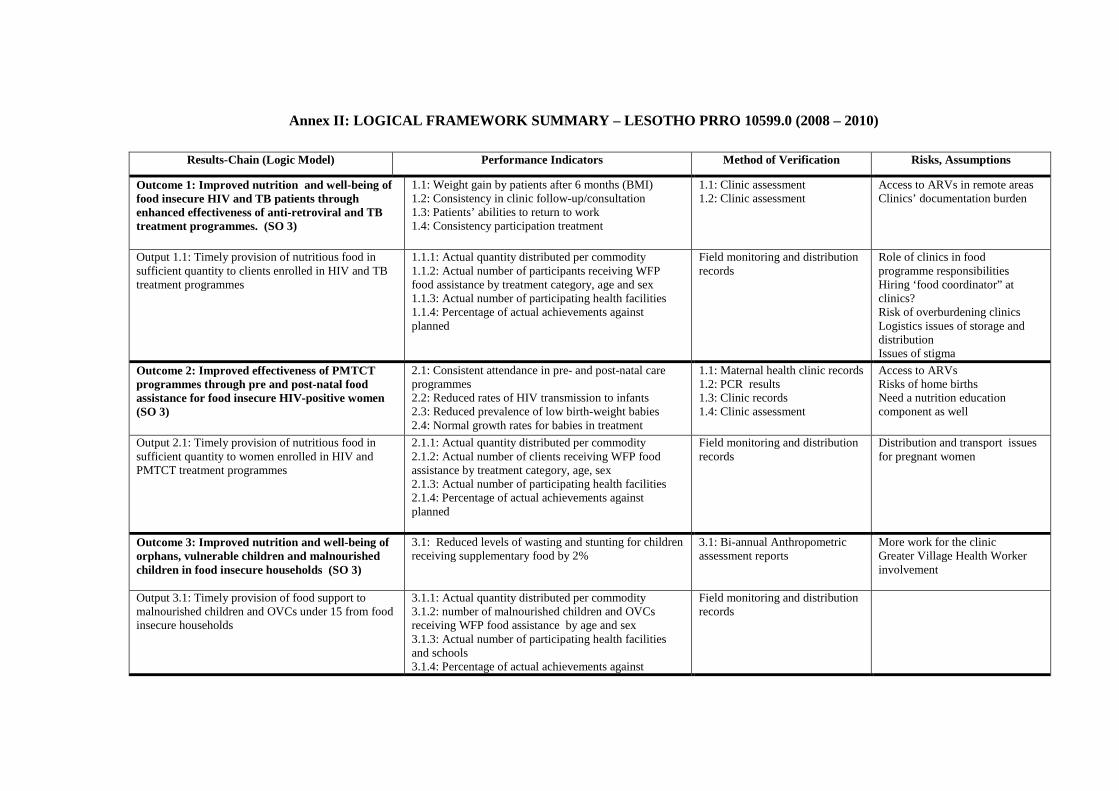
Annex II: LOGICAL FRAMEWORK SUMMARY – LESOTHO PRRO 10599.0 (2008 – 2010)
Results-Chain (Logic Model) Performance Indicators Method of Verification Risks, Assumptions
Outcome 1: Improved nutrition and well-being offood insecure HIV and TB patients throughenhanced effectiveness of anti-retroviral and TBtreatment programmes. (SO 3)
1.1: Weight gain by patients after 6 months (BMI)1.2: Consistency in clinic follow-up/consultation1.3: Patients’ abilities to return to work1.4: Consistency participation treatment
1.1: Clinic assessment1.2: Clinic assessment
Access to ARVs in remote areasClinics’ documentation burden
Output 1.1: Timely provision of nutritious food insufficient quantity to clients enrolled in HIV and TBtreatment programmes
1.1.1: Actual quantity distributed per commodity1.1.2: Actual number of participants receiving WFPfood assistance by treatment category, age and sex1.1.3: Actual number of participating health facilities1.1.4: Percentage of actual achievements againstplanned
Field monitoring and distributionrecords
Role of clinics in foodprogramme responsibilitiesHiring ‘food coordinator” atclinics?Risk of overburdening clinicsLogistics issues of storage anddistributionIssues of stigma
Outcome 2: Improved effectiveness of PMTCTprogrammes through pre and post-natal foodassistance for food insecure HIV-positive women(SO 3)
2.1: Consistent attendance in pre- and post-natal careprogrammes2.2: Reduced rates of HIV transmission to infants2.3: Reduced prevalence of low birth-weight babies2.4: Normal growth rates for babies in treatment
1.1: Maternal health clinic records1.2: PCR results1.3: Clinic records1.4: Clinic assessment
Access to ARVsRisks of home birthsNeed a nutrition educationcomponent as well
Output 2.1: Timely provision of nutritious food insufficient quantity to women enrolled in HIV andPMTCT treatment programmes
2.1.1: Actual quantity distributed per commodity2.1.2: Actual number of clients receiving WFP foodassistance by treatment category, age, sex2.1.3: Actual number of participating health facilities2.1.4: Percentage of actual achievements againstplanned
Field monitoring and distributionrecords
Distribution and transport issuesfor pregnant women
Outcome 3: Improved nutrition and well-being oforphans, vulnerable children and malnourishedchildren in food insecure households (SO 3)
3.1: Reduced levels of wasting and stunting for childrenreceiving supplementary food by 2%
3.1: Bi-annual Anthropometricassessment reports
More work for the clinicGreater Village Health Workerinvolvement
Output 3.1: Timely provision of food support tomalnourished children and OVCs under 15 from foodinsecure households
3.1.1: Actual quantity distributed per commodity3.1.2: number of malnourished children and OVCsreceiving WFP food assistance by age and sex3.1.3: Actual number of participating health facilitiesand schools3.1.4: Percentage of actual achievements against
Field monitoring and distributionrecords

planned
Outcome 4: Improved attendance of OVC boysand girls in WFP assisted schools (SO 4)
4.1 Attendance Rate: percentage of OVC children fromhouseholds receiving take home rations attendingclasses in WFP assisted school
Monthly school reports
Output 4.1 Timely provision of food in sufficientquantity to vulnerable OVCs selected WFP assistedschools
4.1.1 Actual beneficiaries receiving WFP take homerations by age group and sex4.1.2 Actual metric tons of food distributed as takehome rations to OVCs by commodity
Monitoring and distributionreports
Outcome 5: Increased ability of vulnerable foodinsecure households affected by HIV and or TB tomeet their food needs, becoming more good secureand able to withstand shocks. (SO 2)
5.1: Changes in Coping Strategies Index (CSI) belownational average5.2: Changes in Food Consumption Score (FCS) > 25
5.1.: Community HouseholdSurveys (CHS) – CSI and FCSdata5.1.2: Longer-term monitoring
Output 5.1: Provision of viable asset creation andlivelihood development activities, including FFW andFFA
5.1.1: Availability of activities that match beneficiaries’abilities and needs and community resources5.1.2: Consistent participation by beneficiaries inactivities
5.1.1: Partners’ processes andplanning of projects5.1.2: Data from project partners
Adequate number and reach ofpartners?Issues of stigmaInvolvement of communities indesigning projects, support oflocal government
Outcome 6: Contribute to improved nationalcapacity to develop and manage food-based andsocial safety net programmes, includingvulnerability assessment, monitoring of foodsecurity and nutrition tracking. (SO 5)
6.1: Increased level of government responsibility andinvolvement in food programmes6.2: Increased level of national funds allocated to foodand nutrition6.3: Integration of food and nutrition policy into nationalAIDS strategy6.4: Quality of assessments and reports
6.1: Level of coordination withMoH 3-year plan6.2: MoH budget allocations
Maintaining linkages withgovernment at central and locallevels.
Output 6.1: Provision of capacity-building assistanceto Disaster Management authority, Ministry of Healthand Social Welfare, and Food and NutritionCoordination Office
6.1.1: Assignment of government counterparts to workwith WFP, including at clinics6.1.2: Number of UNVs seconded to counterparts6.1.3: Actual amount spent on capacity-building againstamount planned
6.1.1: Staffing at clinics
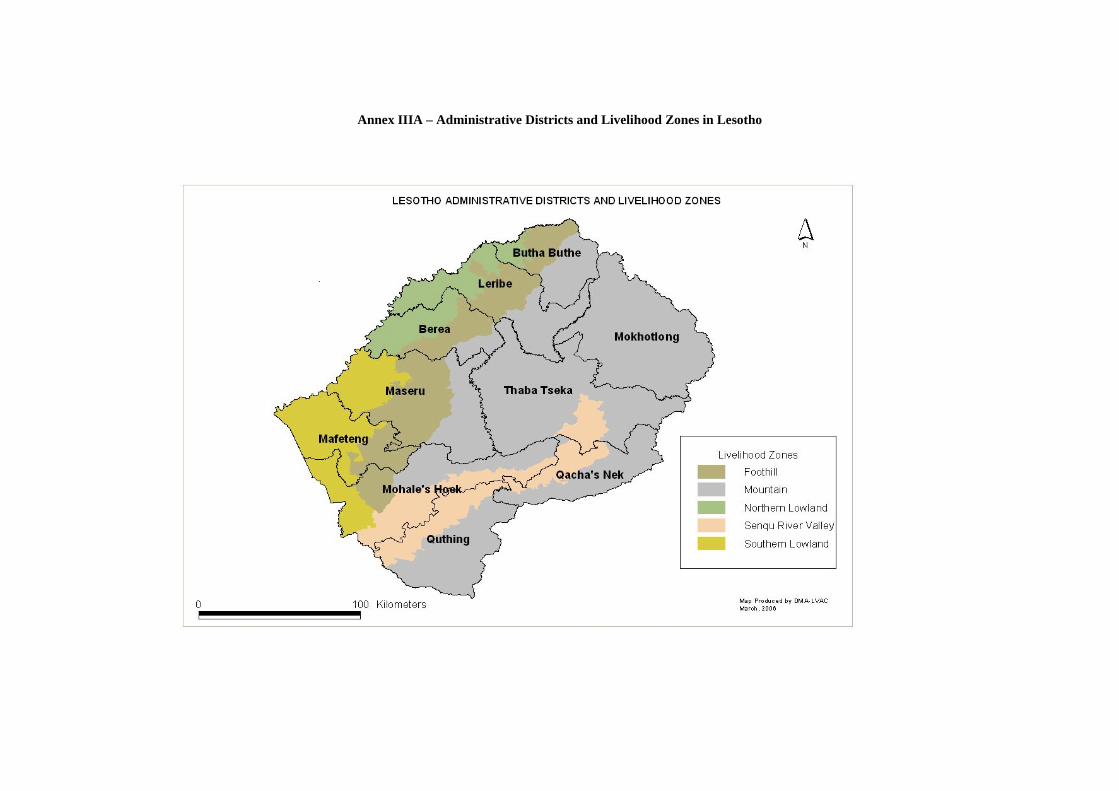
Annex IIIA – Administrative Districts and Livelihood Zones in Lesotho

Annex IIIB – Food and Expenditure Deficit by Livelihood Zone

Annex III - HIV Prevalence by District in Lesotho

ANNEX IV – LTSH Matrix
ANNEX V - Project Budget Plan
ANNEX VI - Project Statistics