Embed Size (px)
Citation preview

Social Workers Respond – International Workshop
June 19, 2019
Venue: 6 Ifjúság Street, Building A, Faculty of Humanities (Kari Tanácsterem)
Organizer:
UP, Department of Community and Social Studies
Editor: József Madácsy
ISBN: 978-963-429-432-0
© University of Pécs, Department of Community and Social Studies
2
Guests:
Participants of the program called
Xenophobia, Migration, Human Rights & Community Impact
Hungary, Austria, Czech Republic, June 13-30, 2019
Organizer:
Council of International Programs USA (CIPUSA)
Leader:
Stacy Moreno, MSW
Adjunct Faculty, Social Work
Council of International Programs, Phoenix Branch Director
Lecturers & workshop leaders:
Dr. Habil. Márta B. Erdős, PhD, Associate Professor
Dr. Habil. Gábor Szöllősi, PhD, Associate Professor
Dr. József Madácsy, PhD, Assistant Professor
Viktória Borda, Lecturer
Éva Vojtek, Lecturer

3
Contents
Márta B. Erdős: Social workers in Hungary 4
Viktória Borda & Éva Vojtek: Give kids a chance: How far we got, who we abandoned 18
József Madácsy: Substance use disorder 32
Gábor Szöllősi: Basic features of the Hungarian child welfare and protection system 40
4 5
Social Workers in Hungary
MÁRTA B. ERDŐS
A profession with core values (IASSW resources) but with
many different faces
Social work changes according to the local history of the
profession, local needs, and actual sociocultural and political
contexts.
Social work or social works?
- clinical social work in the United States
- social assistance/social care within the context of welfare
services in the European welfare states
- social pedagogy with a strong focus on education in some
European states, mainly with a German background
- social development/economic development in Africa and
Asia (Payne, 2014; Szöllősi, 2015)
History of Social Work in Hungary
Before WW2
A similar developmental path to those in the Western
countries.
Forms of “social care” (such as the protection of orphans and
widows) appearing in the Hungarian legislation as early as in
the 11th century. Church-based institutionalized care.
Modern, 19th century precedents: charity organizations
whose main mission was to serve the deserving and grateful
poor; and perhaps educate and control the undeserving poor
in the hope that they would finally meet upper class
expectations. (Pik, 1998)
At the turn of the 20th century, committed professionals
were about to introduce the settlement model: an early
experiment in Kolozsvár in 1905 and a Social Settlement in
Budapest in 1912, followed a number of other settlements in
the 1930s. (Giczey, 2015)
Parallel, former institutionalized care was exchanged for
“open care” provided in poor persons’ or families’ own
homes.
In the 1930’s fascist ideologies have gained grounds that
spread easily in a milieu of deep despair over the significant
losses brought about by the Trianon Treaty. Contrary to
Germany, where fascist dictatorship terminated social work
practice, Hungary has continued to develop new models for
assisting vulnerable families, though their activities had to be
justified as serving national interests, and representing
Christian values.
6 7
The communist era
Open dictatorship
Under the rule of the Soviets, social sciences and humanities
were replaced by mere ideologies.
Marxist theory (essentially a critical theory) was frozen into
a set of dogmas.
Social theorists who deviated from this route were
prosecuted, imprisoned or killed, utilizing the power of
conceptionist trials (showcase trials).
Poverty was extreme and universal.
The system of open dictatorship did not tolerate the
existence of social work. According to a central dogma: state
socialism, and subsequent communism are inherently free of
exploitation, and every single political act by the communists
serves people’s equality, social welfare and wellbeing… (Pik,
1998; B. Erdős & Kelemen, 2011)
Soft dictatorship after the 1956 Revolution
The pragmatism of the Kádár system did tolerate, and even
introduced certain forms of care to manage the problems that
might have been a menace to the system:
- the establishment of school social work/child protection
in the frameworks of “Educational Centers” in the 1960s
- “rehabilitation” (punishment) centers for alcoholics
- suicide prevention hotlines in the 1970s
- Social work was done by “social carers” who did not
necessarily have a university degree. The first university-
level training was organized by an institution of higher
education responsible for the training of special
pedagogues. These professionals were named social
organizers. (Pik, 1998)
- a peculiar form of community work was also present with
the aim of adult education and spreading the socialist
ideology (mirror translation: people cultivators,
népművelők)
Both terms suggest a readiness to control and direct people’s
lives.
Rebirth of the profession in the process of system change
(1989)
Reintroduction of sociology into the system of higher
education.
Social psychiatry: Hungarian psychotherapists had a deep
interest in the personal and family consequences of lasting
anomie in the Hungarian society.
A state-level research on social integration disturbances
(social and mental problems) in the 1980s.
Zsuzsa Ferge’s research on poverty. (Pik, 1998)
8 9
The first social workers in Hungary
Persons who wanted to preserve their power and status that
they could consolidate in the communist era. (Former party
secretaries & their assistants.) Short courses were provided
to offer them a wide road to obtain a leading position in a
social service institution.
Critical intelligentsia showing solidarity for the rapidly
emerging vulnerable groups within the Hungarian society.
Their core value is social justice. Problem: lack of education
or experiences on critical thinking – the contrary is not
necessarily the critical…
Fellow professionals, mainly sociologists, psychologists and
psychotherapists: new opportunities for collaboration – or
conquest. (Németh, 2014)
Welfare state?
Hungarian social workers mainly relied on European
traditions.
A strong emphasis on welfare state ideologies and the
related practices (e.g., the concept of social citizenship,
social workers’ mediating role between the citizen and the
state, adherence to social safety and the accompanying
social services and institutions).
These traditions developed in Europe after World War 2:
experiences on the positive impact of strong state
interventions into economic life. A relatively strong middle
class, whose interests temporarily coincided with those of
the less privileged. Hoping for protection against the
formation of Nazi and communist regimes.
A deep crisis of the welfare state coincided with the rebirth
of social work in Hungary.
Mission impossible: successfully combat all the social ills
brought about by the crisis of the system change.
(Kozma, n.d.; Darvas & Hegyesi, 2003)
State socialist legacy
State socialist attitudes and cognitions are coded in the
communicative memories of people.
An increased susceptibility for manipulation: lack of
autonomous thinking; impairments in critical thinking, such
as the dominance of ideologies over balanced reasoning.
Missing skills to negotiate social problems and possible
solutions until a stable and sustainable consensus is reached.
Lack of social solidarity: the idea that the state should and
does provide is rather widespread; consequently, anyone
suffering from some social ills must be an undeserving
person.
10 11
Fiscal issues prevail over welfare and wellbeing. This is
supported by the well-known Marxist idea of base and
superstructure. A “materialist” approach suggests that
relational, social and cultural issues are just the “surface”,
and as such, are not really important.
Public perception and misnomers
Public perceptions neither reflect the reality of social
problems nor that of social work as a profession.
The term “social” has a number of different translations in
the Hungarian language. “Társas”, refers to human
relations/communities in general; but “szociális” is related to
all types of human miseries. In another sense it might even
be associated with communist ideologies.
For quite a while, social workers were mistaken with
“socialist workers”, i.e., low prestige blue-collar workers in
state-owned factories. (Szoboszlai, 2014)
Worker translates as munkás, which, as a term, never refers
to professionals. The word munkás, as a member of the
working class (leading class in the communist era) lost all its
positive connotations.
Today, most would confuse a social worker with a person
employed for purposes of public utility, low-paid unskilled
labour force in government programs to integrate
unemployed persons into the labour market.
The 1990s: the social-mental „war” for professional
monopolies. Argument: psychosocial counselling is to be
separated from providing financial assistance and two
distinct professions (mental health counselling and social
work) should be introduced. (Bagdy, 1996)
2009: József Pálinkás, former President of the Hungarian
Academy of Sciences. (The Hungarian Flexner: an MA degree
is not necessary…)
Social challenges
Poverty, with an exceptionally high rate of material
deprivation
- in 2015, 44% (Gábos et al., 2016)
- in 2018, 38.5%. (Eurostat) Accompanying problems:
regional inequality and employment issues. „Working
poor” in Hungary (the subsistence level is higher than
net minimum wages).
Ageing society.
Substance use (alcohol, novel psychoactive substances).
Roma integration: numerous projects but with varied results.
Poverty is higher among the Roma groups, due to the loss of
their traditional employment areas, segregation in
education, and to discrimination in the labour market.
(Boros, 2017)
12 13
Homelessness as a salient problem.
Migration?
Challenges of the profession: SW education
Weak and diminishing monopolies. Competitors: Social
Pedagogy, Mental Health Counselling, Community
Development and Community Organization, Pastoral
Counselling and Organization Development – in Hungary,
these are not recognized today as study areas belonging to
Social Work, though the contents are strongly related to
social work.
Postgraduate non-degree programmes (specializations): in
certain positions, these may make a person a social
professional, provided they have a bachelor degree (e.g.,
School Social Work).
Special and centralized leadership courses since 2018
(previously, an MA degree was necessary to fulfill a leading
post in a social institution; leadership courses are indeed
important; but the advantage of a masters degree
decreased).
Education and practice. (Help or control?)
Craftsman, technical or managerial expertise or the
reflective practitioner? (Jones and Joss, 1995) Emphasizing
„practical” skills without reflective skills.
Critical thinking & innovations?
Praxis problems
Societal problems and psychosocial responses (Darvas &
Hegyesi, 2003): in some cases, underdeveloped counselling
skills are a barrier to change and empowerment. (Szabó,
2014)
Poor traditions of empowerment.
Casework, traditional or intensive case management?
(Szabó, 2014) Control vs. help.
The debated, recent introduction of social diagnosis.
High level care? Or a social Cerberus (letting in and letting
out, inclusion/exclusion)?
Increasing bureaucracy and internal contradictions of the
registration system.
Danger of Dickensian out-of-door relief.
The three sectors (state, NGO, church) – strong supports for
the church sector and charity work.

14 15
Challenges in SW research
Research is dominated by sociologists. No differentiation
between social and social work research. Result: use of
inadequate methods.
The peculiar role of evaluation research in Hungary
(monitoring or evaluating?). (B. Erdős, 2016)
Not any doctoral school or programme specifically for social
workers in the country.
Traditionally, poor representation of interests within the
Hungarian Academy of Sciences. (A Soviet tradition of strictly
separating disciplinary areas; inter- or transdisciplinarity and
applied areas were not considered “scientific” enough.)
2018: birth of the Social Work Sub-Committee within the
Hungarian Academy of Sciences.
Myth of STEM.
Lack of resources for social/social work research.
Conclusions
Social work is vulnerable to changes in the economic, societal
and political environment.
In the US, citizens’ solidarity actions and expectations
contributed to the development of social work. In Hungary,
social work was considered as a possible means of managing
the risks of the system change and was reintroduced in a top-
down process.
Currently, public perceptions on social work are distorted
and public supports are largely missing.
Professionalization – relying mostly on international literature
resources, international and domestic innovations – is in
progress; but this is not evident for the fellow professionals.
References
B. Erdős, M. & Kelemen, G. (2011). The Finite Universe:
Discursive Double Bind and Parrhesia in State Socialism. History
of Communism in Europe 2, pp. 281-309.
Bagdy, E. (1996). A Klinikai Pszichológiai Szakkollégium
állásfoglalása a mentálhigiéné, a segítő szakmák és a klinikai
pszichológiai és viszonyának kérdésében. Család, Gyermek,
Ifjúság 4(3-7).
Darvas, Á. & Hegyesi, G. (2003). Hungary, pp. 125-141. In: Weiss,
I., Gal, J. & Dixon, J. (eds.) Professional ideologies and
preferences in social work: a global study. Westport (CT), USA:
Praeger Publishers.
Gábos, A., Tátrai, A., B. Kis A. & Szivós, P. (2016). Anyagi
depriváció Magyarországon, 2009–2015.
http://old.tarki.hu/hu/publications/SR/2016/07gabos.pdf
16 17
Giczey, P. (2015). A settlementek esélyei Magyarországon.
http://www.kka.hu//_Kozossegi_Adattar/parolaar.nsf/nyomtat
/20323E5ED16D8656C1257F13005AC5DB?OpenDocument
Jones, S. & Joss, R. (1995). Models of Professionalism. In: Yelloly,
M. & Henkel, M. (eds.): Learning and Teaching in Social Work.
Towards Reflective Practice. London and Bristol, Pennsylvania:
Jessica Kingsley Publishers, pp. 15-33.
Kozma, J. (n.d.). A szociális munka professzionalizációja a jóléti
államokban. http://www.ncsszi.hu/files/1147.file
Material deprivation. Eurostat.
https://ec.europa.eu/eurostat/statistics-
explained/index.php?title=Archive:Material_deprivation_and_l
ow_work_intensity_statistics#Material_deprivation_and_sever
e_material_deprivation
Németh, L. (2014). Hová jutott a szociális szakma a
rendszerváltástól napjainkig? Esély, 3, pp. 95-99.
Payne, M. (2014). European social works and their identities.
ERIS Web Journal, 5(2).
Pik, K. (1998). A szociális munka története Magyarországon. A
pesti és budai Jóltévő asszonyi egyesület. Esély, 10(2), pp. 80-90.
Szabó, L. (2016). Az esetmenedzseri tevékenység jelenléte és
dilemmái a hazai szociális munkában. Párbeszéd, 3(2).
Szabó, L. (2017). Szociális munkások a terápiák világában.
Párbeszéd, 4(2).
Szoboszlai, K. (2014). A szociális munka a változások tükrében:
kik vagyunk, hol tartunk és mit kellene tennünk?
http://www.esely.org/kiadvanyok/2014_3/2014-3_3-
4_Szoboszlai_szocialis_munka.pdf
Szöllősi, G. (2015). A szociális munka új, 2014-es globális
definíciója. Párbeszéd, 2(1).
http://parbeszed.lib.unideb.hu/megjelent/html/55192b603fed
c
18 19
Give kids a chance: How far we got, who we
abandoned
VIKTÓRIA BORDA & ÉVA VOJTEK
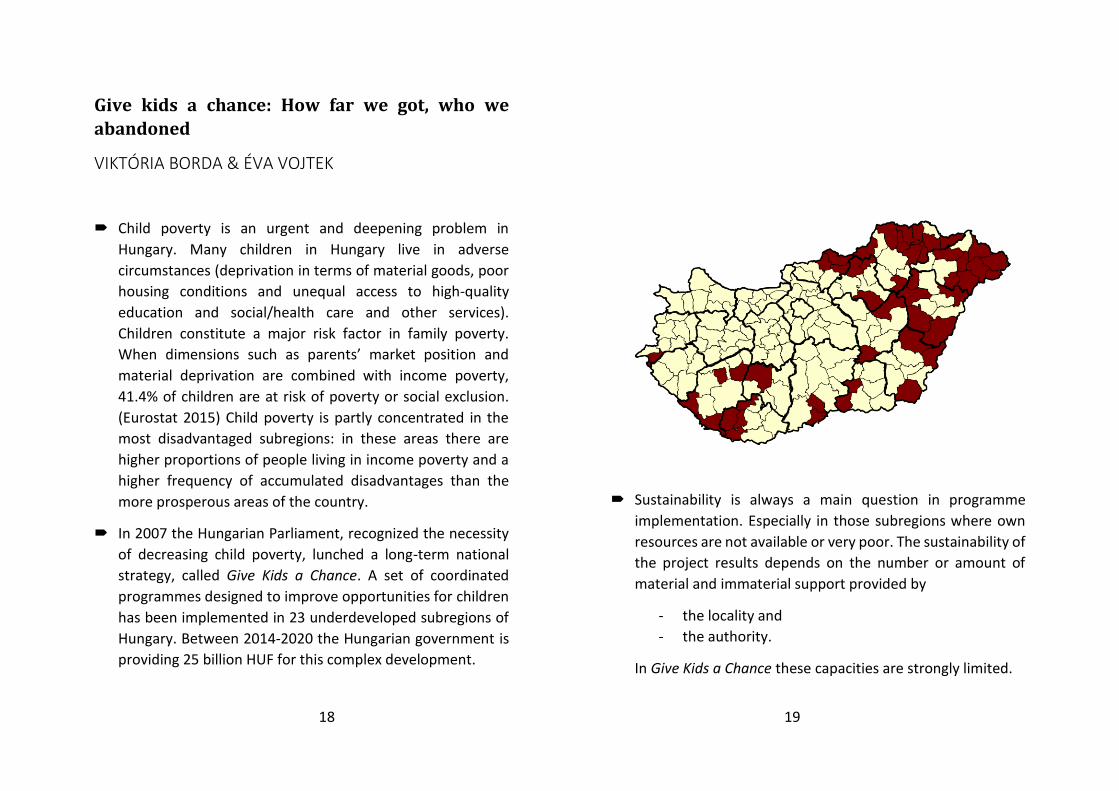
Child poverty is an urgent and deepening problem in
Hungary. Many children in Hungary live in adverse
circumstances (deprivation in terms of material goods, poor
housing conditions and unequal access to high-quality
education and social/health care and other services).
Children constitute a major risk factor in family poverty.
When dimensions such as parents’ market position and
material deprivation are combined with income poverty,
41.4% of children are at risk of poverty or social exclusion.
(Eurostat 2015) Child poverty is partly concentrated in the
most disadvantaged subregions: in these areas there are
higher proportions of people living in income poverty and a
higher frequency of accumulated disadvantages than the
more prosperous areas of the country.
In 2007 the Hungarian Parliament, recognized the necessity
of decreasing child poverty, lunched a long-term national
strategy, called Give Kids a Chance. A set of coordinated
programmes designed to improve opportunities for children
has been implemented in 23 underdeveloped subregions of
Hungary. Between 2014-2020 the Hungarian government is
providing 25 billion HUF for this complex development.
Sustainability is always a main question in programme
implementation. Especially in those subregions where own
resources are not available or very poor. The sustainability of
the project results depends on the number or amount of
material and immaterial support provided by
- the locality and
- the authority.
In Give Kids a Chance these capacities are strongly limited.
20 21
Quantitative research in Sellye in April, 2018
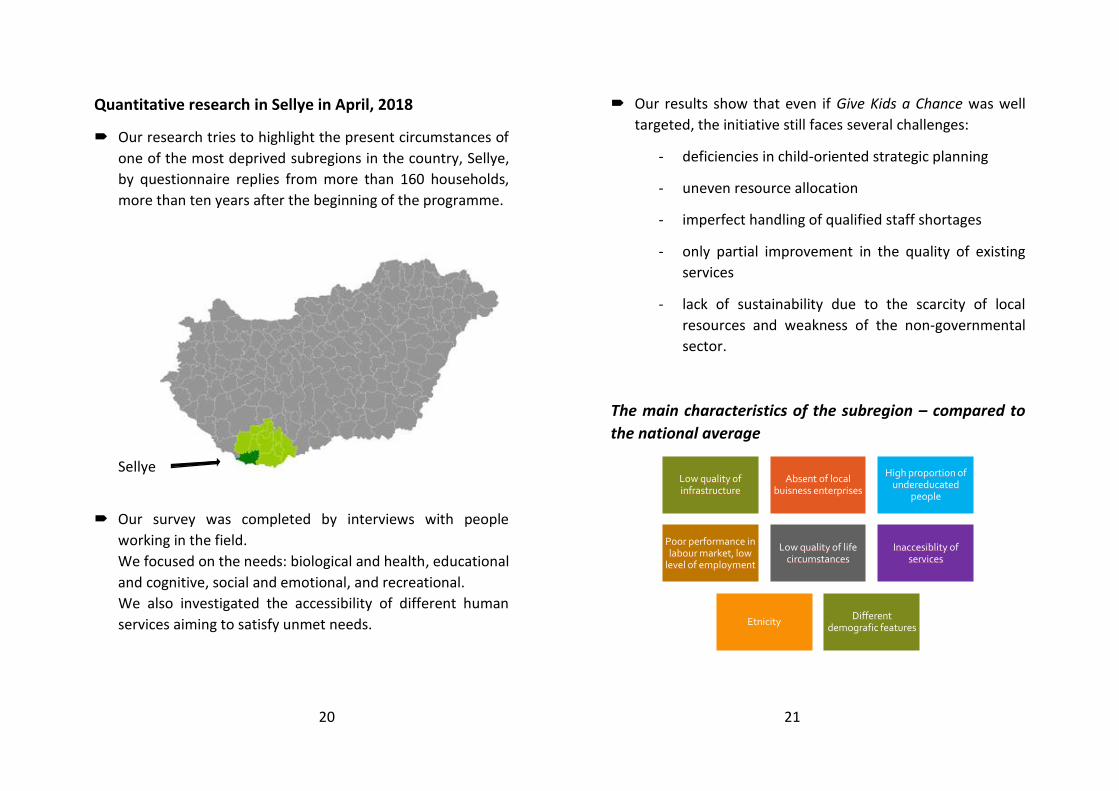
Our research tries to highlight the present circumstances of
one of the most deprived subregions in the country, Sellye,
by questionnaire replies from more than 160 households,
more than ten years after the beginning of the programme.
Sellye
Our survey was completed by interviews with people
working in the field.
We focused on the needs: biological and health, educational
and cognitive, social and emotional, and recreational.
We also investigated the accessibility of different human
services aiming to satisfy unmet needs.
Our results show that even if Give Kids a Chance was well
targeted, the initiative still faces several challenges:
- deficiencies in child-oriented strategic planning
- uneven resource allocation
- imperfect handling of qualified staff shortages
- only partial improvement in the quality of existing
services
- lack of sustainability due to the scarcity of local
resources and weakness of the non-governmental
sector.
The main characteristics of the subregion – compared to
the national average
Low quality of infrastructure
Absent of local buisness enterprises
High proportion of undereducated
people
Poor performance in labour market, low
level of employment
Low quality of life circumstances
Inaccesiblity of services
EtnicityDifferent
demografic features

22 23
Level of education
Sellye subregion
National
(KSH, 2017)
Employment
National public employment program:
Local councils use the program as a kind of recruiting tool, so
that they can reach reliable and proven public employed
people, whom they try to ’park’ at supported jobs.
Even so the intervention is required due to the insufficient
market demand, but in its present form it is a rather costly
and inefficient system.
Deprivation
Deprivation is a consequence of lack of income and other
resources, which cumulatively can be seen for people living in
poverty.

24 25
The indicators were built up from items covering:
clothing
fuel and light
housing and housing facilities
the general conditions and security of work
family support
recreation
education
health
social relations
(In 2017 10,2% of the Hungarian households lived in
deprivation.)
Can the household afford a family holiday?

26 27
Debts and arrears
37 households have some arrears in different kind of debts,
some of them can’t measure the level of their debts and
backlogs, but the answers of the responders present that the
amount of remainder is between 12.000 HUF and 9.000.000
HUF
Responding housholds have difficulties in the last 12
months in some type of expenses.
Subjective poverty
In most of the cases, however, poverty is defined by some
objective measures. Income level is the most widely used
measure of it. Besides, the number of children, age, education
attainment, labor market position, or level of comfort can also
be applied as a basis for defining objective poverty.

28 29
Subjective poverty is the subjective perception of deprivation.
Two approaches can be distinguished in defining subjective
poverty.
On the one hand, poverty can be defined by examining who
is considered to be poor in general.
On the other hand, it can also be defined by collecting their
beliefs about their own position in a system of inequalities.
Subjective well-being
Subjective well-being is a self-reported measure of well-being.
A person who has a high level of satisfaction with their life, and
who experiences a greater positive affect and little or less
negative affect, may be deemed to have a high level of SWB.

30 31
What was 3 years ago
What the future holds
32 33
Substance use disorder
JÓZSEF MADÁCSY
Substance use in Hungary
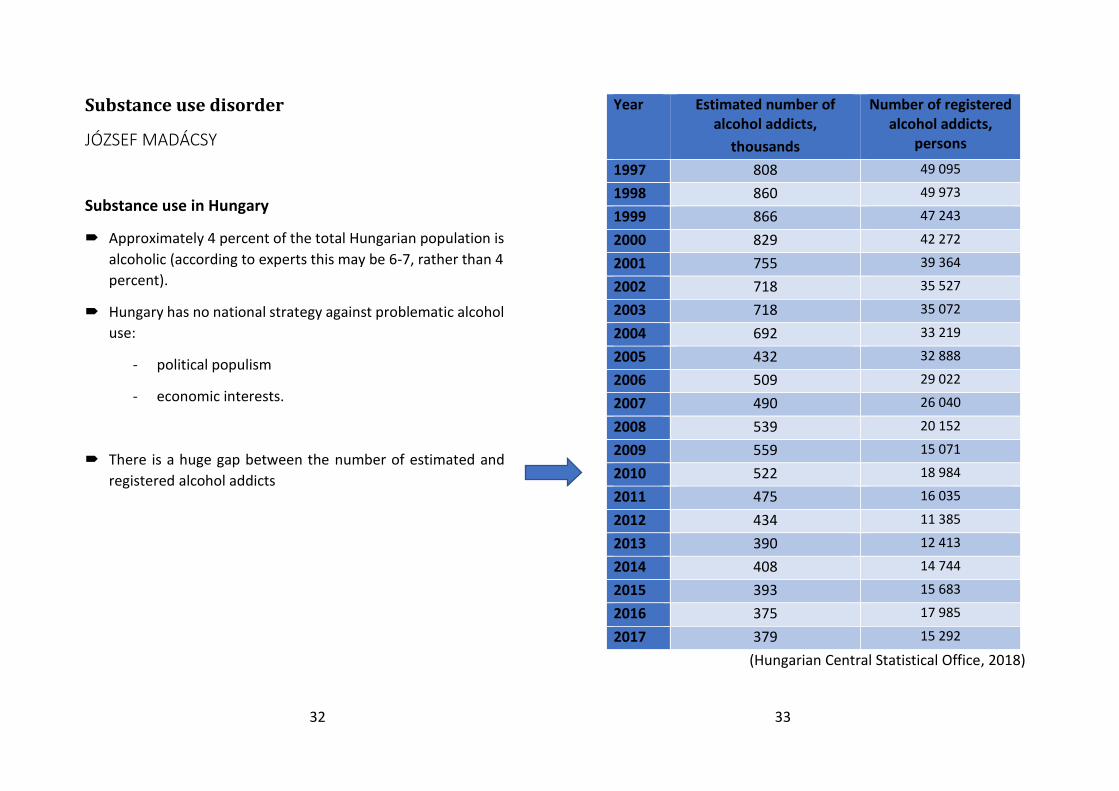
Approximately 4 percent of the total Hungarian population is
alcoholic (according to experts this may be 6-7, rather than 4
percent).
Hungary has no national strategy against problematic alcohol
use:
- political populism
- economic interests.
There is a huge gap between the number of estimated and
registered alcohol addicts
Year Estimated number of alcohol addicts,
thousands
Number of registered alcohol addicts,
persons
1997 808 49 095
1998 860 49 973
1999 866 47 243
2000 829 42 272
2001 755 39 364
2002 718 35 527
2003 718 35 072
2004 692 33 219
2005 432 32 888
2006 509 29 022
2007 490 26 040
2008 539 20 152
2009 559 15 071
2010 522 18 984
2011 475 16 035
2012 434 11 385
2013 390 12 413
2014 408 14 744
2015 393 15 683
2016 375 17 985
2017 379 15 292
(Hungarian Central Statistical Office, 2018)

34 35
Year Number of drug consumers treated first
time,
persons
Drug consumers at the treatment,
persons
1997 4 368 8 494
1998 5 275 9 458
1999 5 770 12 765
2000 4 701 12 789
2001 4 342 12 049
2002 4 717 12 777
2003 5 958 14 993
2004 5 655 14 165
2005 6 319 14 793
2006 5 673 15 480
2007 4 050 13 597
2008 4 635 14 353
2009 3 802 13 140
2010 5 337 16 923
2011 5 781 16 150
2012 5 883 16 016
2013 4 864 12 114
2014 6 866 14 268
2015 5 566 12 350
2016 3 988 13 592
2017 n.d. n.d.
(Hungarian Central Statistical Office, 2018)
The number of the registered drug consumers was 13.592 in
2016, but the estimated number of high-risk drug users
(HRDU) may be significantly higher.
Lifetime prevalence rates by substance types in the adult
population between 18-64 years and 18-34 years, in 2015 (%):
(2018 National Report, p. 19)
36 37
Injecting drug use: the size of the IDU population was 6707
persons in 2015. (2018 National Report, p. 47)
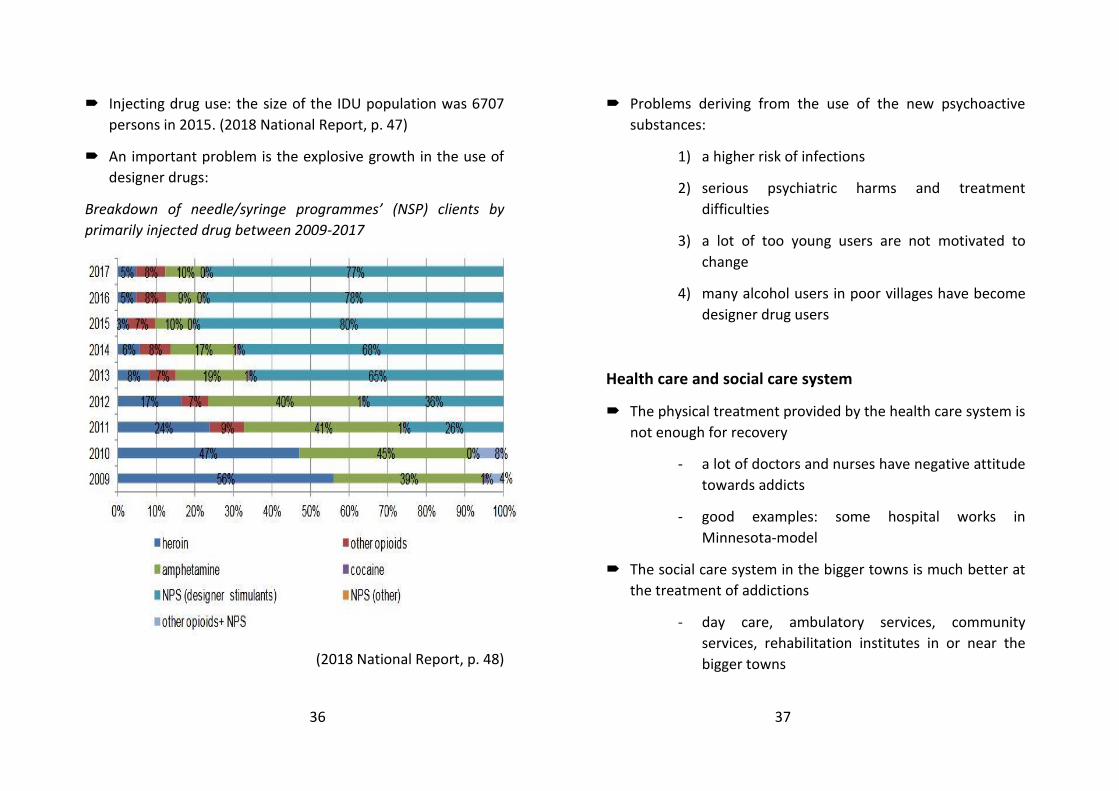
An important problem is the explosive growth in the use of
designer drugs:
Breakdown of needle/syringe programmes’ (NSP) clients by
primarily injected drug between 2009-2017
(2018 National Report, p. 48)
Problems deriving from the use of the new psychoactive
substances:
1) a higher risk of infections
2) serious psychiatric harms and treatment
difficulties
3) a lot of too young users are not motivated to
change
4) many alcohol users in poor villages have become
designer drug users
Health care and social care system
The physical treatment provided by the health care system is
not enough for recovery
- a lot of doctors and nurses have negative attitude
towards addicts
- good examples: some hospital works in
Minnesota-model
The social care system in the bigger towns is much better at
the treatment of addictions
- day care, ambulatory services, community
services, rehabilitation institutes in or near the
bigger towns

38 39
- self-help groups: there are approximately 150 AA
meetings and 30 NA meetings in the country
The weaknesses of the social care system:
1) no access to services in the poor country areas
2) underfunded system (e.g. harm reduction
programs)
3) no adequate treatment for special groups like
gypsies
4) cultural and legal difficulties in asking help
Drug policy
Conservative drug policy
- one of the toughest drug laws in Europe from 2013
Recovery-centered National Drug Strategy
- this conservative drug policy is not compatible with harm
reduction programs
References
2018 National Report to the EMCDDA.
http://drogfokuszpont.hu/wp-
content/uploads/HU_EMCDDA_jelentes_HUNGARY_2018_EN.p
df
Hungarian Central Statistical Office (2018). Care of drug
consumers and alcohol addicts (1997–)
https://www.ksh.hu/docs/eng/xstadat/xstadat_annual/i_fek005
.html

40 41
Basic features of the Hungarian child welfare and
protection system
SZÖLLŐSI GÁBOR
History
In discovering any child protection system, it is necessary to
examine the historical path of its development. The Hungarian
statutory child protection system, following the paths of
municipal, church, and charity predecessors, was created in 1901.
In the next more than one hundred years different processes of
development and some major ruptures had their impact on the
system. The most recent reform took place in 1997, according to
which a comprehensive child welfare and child protection system
came to existence. The latest amendments to the child welfare
law took place in 2015.
Issue (1): What mixture of forces can be optimal to develop a child
protection system: to follow the paths, or to implement reforms?
What are the experiences in different countries?
Welfare and/or protection?
Even the terms ’child protection’ and ’child welfare’ can have
different meanings in different parts of the world.
Usually ’child protection’ has a narrower meaning, for example in
this definition: ’Child protection systems comprise certain
structures, functions and capacities that have been assembled to
prevent and respond to violence, abuse, neglect and exploitation
of children’. (UNICEF, UNHCR Save the Children & World Vision,
2013)
On the other side ’child welfare’ denotes a system working for
the welfare of children (and not only against the ’ills’). But in
many discourses the term ’child protection’ cover both measures
against child maltreatment and measures for the welfare of
children.
The Hungarian system’s official title is ’child protection’, but in
detailed descriptions the law acknowledges its child welfare
goals. So, the Hungarian system is a complex child welfare and
child protection system, with welfare and protective subsystems
(tasks, provisions, organizations).
Issue (2): Whether the different wording can impact the
understanding of a national system for foreigners?
Orientations
The child protection / child welfare systems are unique in every
country; but typologies have been developed based on main
characteristics of the systems. Comparative descriptions of child
protection systems are based on these typologies.

42 43
According to Gilbert et al. (2011) the main orientations are:
- child protection
- family support
- child focused
In this typology the Hungarian system’s orientation can be
characterised as:
- family support (main, decisive)
- child protection (secondary)
- child focus (virtual)
Issue (3): Whether the goals stipulated in legal documents, or the
principles accomplished in the practice are best characterising a
child protection system?
Problem categories
Child protection systems are organized for handling specific
problems, and the most characteristic feature is the type of the
problems designated to this system.
In Hungary
- the general problem category is: ’child-at-risk’
- an additional problem category: ’child abuse’ and ’child
neglect’ (as special forms of child-at risk)
In the everyday practice only the smaller part of cases is labelled
as ‘child abuse’ or ‘child neglect’.
Issue (4): Whether the wording of the problem of the child can
generate prejudices about the nature of the situation?
Main provisions
The main categories of the provisions in child welfare and child
protection are:
- different income-tested benefits
- different welfare services (e.g. day-care of children)
- child and family social work (’basic care’)
- safeguarded child (in more direct translation: ’child under
protection’, which contains a) administrative measures,
and b) social work)
- out-of-home care (in more direct translation:
’professional child protection’, which contains a)
administrative measures, b) out-of-home care, and c)
permanency planning)
Issue (5): Whether we can find ‘protection’ and ‘welfare’ goals in
every categories of provisions (e.g. preventative functions of the
day care services)?

44 45
Main issues of child welfare and child protection in
Hungary
And finally, a list of the most essential issues of the Hungarian
child protection system:
- inconsistent relationship between handling child poverty
and measures of child protection
- strong control function of child and family social work
- in sufficient supply of organizational resources (e.g.
workload of social workers, shortage of foster parents.
etc.)
- adaptation demands to systemic changes
- issues around division of labour
Most recent adaptational tasks:
Since 2016 the child and family social work is divided between
two organizational levels:
- Family Helping and Child Welfare Service (in every
municipality, general level)
- Family Helping and Child Welfare Centre (in district
centres, special services and services connected to
administrative measures)
Since 2018 School Social Work (’School Social Assistance’) has
been introduced, as a new form of child welfare activities.
These developments have brought new issues around
division of labour, mainly between school social workers, the
Family Helping and Child Welfare Service, the Family Helping
and Child Welfare Centre, and teachers of the schools.
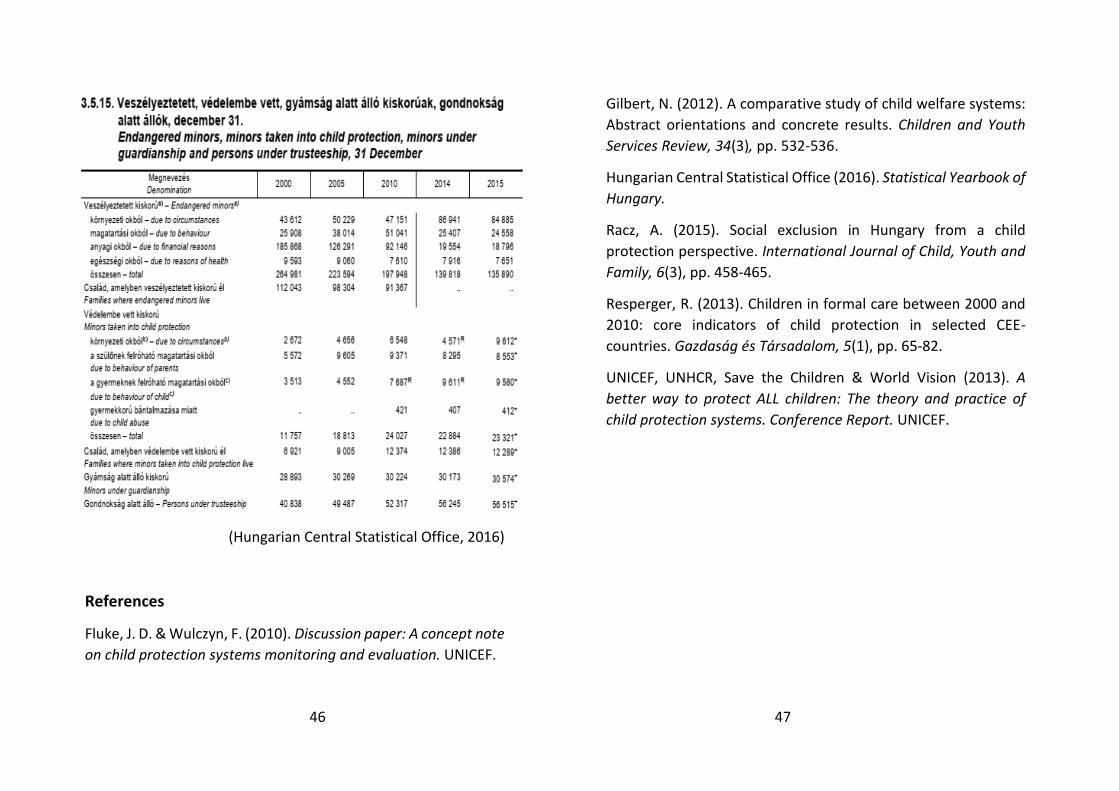
Statistics
46 47
(Hungarian Central Statistical Office, 2016)
References
Fluke, J. D. & Wulczyn, F. (2010). Discussion paper: A concept note
on child protection systems monitoring and evaluation. UNICEF.
Gilbert, N. (2012). A comparative study of child welfare systems:
Abstract orientations and concrete results. Children and Youth
Services Review, 34(3), pp. 532-536.
Hungarian Central Statistical Office (2016). Statistical Yearbook of
Hungary.
Racz, A. (2015). Social exclusion in Hungary from a child
protection perspective. International Journal of Child, Youth and
Family, 6(3), pp. 458-465.
Resperger, R. (2013). Children in formal care between 2000 and
2010: core indicators of child protection in selected CEE-
countries. Gazdaság és Társadalom, 5(1), pp. 65-82.
UNICEF, UNHCR, Save the Children & World Vision (2013). A
better way to protect ALL children: The theory and practice of
child protection systems. Conference Report. UNICEF.