Embed Size (px)
Citation preview

Solving the Compliance Riddle with Compression Garments
Jeffrey D. Lehrman, DPM, FASPS, MAPWCA, CPC
Advisor, APMA Coding Committee
Advisor, APMA MACRA Task Force
Expert Panelist, Codingline
Fellow, American Academy of Podiatric Practice Management
Board of Directors, American Society of Podiatric Surgeons
Board of Directors, American Professional Wound Care Association
Editorial Advisory Board, WOUNDS
Twitter: @DrLehrman

FACTS: CHRONIC VENOUS ULCERS
Venous Ulcers account for 60-90% of leg ulcers
More common in women: 3X
Difficult to heal: 50% > 9 months/20% > 2 years
High rate of reccurrence: Up to 69%
Advances in Skin & Wound Care: August 2009 - Volume 22 - Issue 8 - p 384

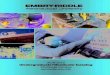
VASCULAR MECHANICS
DEEP VEINS
SUPERFICIAL VEINS
COMMUNICATING VEINS (PERFORATORS)
VALVES
CALF PUMP
Hegarty M,: Am Overview of Compression Therapy. Today’s Wound Clinic vol 4 issue
10-Oct 2010.

NORMAL ANATOMY
VENOUS SYSTEM
DEEP VEINS SUPERFICIAL VEINS PERFORATORS
Semin Intervent Radiol. Sep 2005; 22(3): 147–156.

http://konstati.co/venous-anatomy-of-the-arm/venous-anatomy-of-the-arm-and-figure-1-anatomy-of-the-venous-system-of-the-

ARTERY
PROVIDES OXYGENATED
BLOOD TO THE LIMB
IS A FACTOR IN VENOUS
DISEASE 20% OF THE
TIME
http://legacy.owensboro.kctcs.edu/gcaplan/anat2/notes/APIINotes5%20Circulatory%20Anatomy.htm

•Hypoxia in areas of venous congestion
•Growth factors get trapped

ANATOMICAL FAILURE
Venous Wall Physical Properties: Reduced Strength
Venous Valves
Primary Venous Disease: degenerative damage
Secondary Venous Disease: DVT
Calf Pump
90% of venous return is through these 3
Fletcher, Moffatt, Partsch, Vowden, Vowden: Principles of Compression in venous disease, a practitioner's guide to treatment andprevention of venous leg ulcers; Wounds International: 2013

LYMPHEDEMA
An abnormal collection of excessive tissue proteins, edema, chronic inflammation and fibrosis in the interstitial space.
Blockage in the lymphatic system
CHRONIC PROBLEM

EDEMA AND WOUND HEALING
Inflammation
Fibrosis
Induration
Elevated Proteases
Ischemia

ORGANIZED APPROACH TO WOUND CARE
1. Is there adequate perfusion
and/or oxygenation?
2. Is non-viable tissue present?
3. Are signs/symptoms of infection and/or inflammation present?
4. Is offloading or pressure relief appropriate?
5. Is edema controlled?
6. Is tissue growth optimized?
7. Is the wound microenvironment
conducive to healing?
8. Is pain controlled?
9. Are host factors optimized?
Disease Process
Controlled
Advanced ModalBalance
ities
Patient Centered Pain
Wound Moisture
Edema
Offloading
BioBurden
Debridement
Blood Flow

TREATMENTS
COUNTERACT GRAVITY EXERCISE
COMPRESSION
THERAPY
SURGERY

COMPRESSION THERAPY
• Application of pressure to the lower extremities.
• Recognized treatment of choice for venous leg ulcers.
• Systems include hose, tubular bandages, bungee systems, and bandage systems of two or morecomponents.
• These systems aim to provide graduated compression to the lower limb in order to improve venous return and to reduce edema.
http://wwundsinternational.com/pdf/content_10802.pdfw.wo

HOW DO WE DEFINE THIS IN PRACTICE??????
TYPES OF COMPRESSION
ELASTIC
INELASTIC
STATIC
DYNAMIC
WRAPS
HOSE

TYPES
COMPRESSION WRAPS
COMRESSION HOSIERY
INTERMITTENT PNEUMATIC
COMPRESSION (IPC)
BUNGEE + ZIPPER

WHAT TO DO BEFORE COMPRESSION
VASCULAR SCREENING

Venous studies
• Duplex ultrasound

Arterial Doppler

PURPOSE OF COMPRESSION
1. Counteract the force of gravity and promote
the normal flow of venous blood up the leg
2. Acts on the venous and lymphatic systems to
improve venous and lymph return and reduce
edema
3. Causes narrowing of the superficial veins
Meissner,M, Lower Extremity Venous Anatomy, Interventional Radiology, Sept. 2005, ; 22(3): 147-158

WHAT IS ADAQUATE COMPRESSION
Overcomes intravenous pressure
Exerts a sub-bandage resting pressure that is well tolerated in a resting position
Provides a pressure increase when the patient
rises to a standing position: (50-70mmHG)
Provides external compression improving venousreflux during walking
Fletcher, Moffatt, Partsch, Vowden, Vowden: Principles of Compression in venous disease, a practitioner's guide to treatment and prevention of venous leg ulcers; Wounds International: 2013
Partsch, H; compression therapy of venous ulcers;, Hemodynamic effects depend on interface pressure and stiffness; EWMA Journal 2006, vol 6 NO2.

TYPES OF BANDAGES
Non-Stretch
Short –Stretch
Long -Stretch

NON-STRETCH
ZINC PASTE BANDAGES

SHORT STRETCH
Bandages that stretch to less than 100% of
their original length: minimal extensibility
High Working Pressure/Low Resting Pressure


LONG STRETCH

LONG STRETCH
Expands over 100% of its original length
Low Working Pressure/High Resting
Pressure
Contains Elastomeric Fibers: fibers that are able
to stretch and return to almost their original size.
World Union of Wound Healing societies (WUWHS). Principles of best practice: Compression in venous leg ulcers. A consensus document. London: MEP Ltd,2008

• Assess whether home care nurses achieve adequate subbandage pressure when treating patients with venous leg ulcers
• 13 months• 68 nurses
Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers

Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers
• Participant-masked measurements of subbandage pressure
• Three bandage types:
1. an elastic, long-stretch,
single-component bandage
2. an inelastic, short-stretch, single-component bandage
3. a multilayer, 2-component bandage

Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers
• Association between achievement of optimal pressure and
– Years in the profession
– Attendance at wound care
educational programs
– Previous work experience
– Confidence in bandaging ability

Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers
• A substantial variation in exerted pressures was found
11mm Hg exerted by an inelastic bandage80mm Hg exerted by a 2-component bandage

Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers
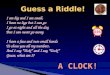
• The optimal subbandage pressure range, defined as 30 to 50 mm– 39 of 62 nurses (63%) applying the 2-
component bandage
– 28 of 68 nurses (41%) applying the
elastic bandage
– 27 of 68 nurses (40%) applying the
inelastic bandage

Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers
Pressures less than 30 mmHg
• Inelastic – 56%
• Elastic – 53%
• 2 component – 27%

Delivery of compression therapy for venous leg ulcers AMA Dermatol. 2014 doi: 10.10010amadermatol.2013.7962 Zarchi Kl, Jemec GBI
Delivery of Compression Therapy for Venous Leg Ulcers
• None of the investigated factors was associated with the ability to apply a bandage with optimal pressure.



Compliant Compression!
• Instead of Velcro, Bungee system to adjust compression
• No neoprene = no stretching out
• Breathable

Compliant Compression!
• 10 DIFFERENT SIZES
• 30-50 mmHg
• Garment, Liner, Bag
• Different Lengths

• 15mmHg just from zipping

• Must have a venous stasis ulcer
• A6545

Recurrence
60% - 70%

• Below-knee graduated compression stockings or hosiery likely to prevent recurrence of venous leg ulcers
• Application of external pressure with compression to calf muscle raises interstitial pressure resulting in improved venous return and reduction in the venous hypertension
Compression for preventing recurrence of venous ulcers. Nelson EA, Bell-Syer SE, Cullum NACochrane Database Syst Rev. 2000; (4):CD002303.

Options

THINGS TO CONSIDERWHEN CHOOSING COMPRESSION
ETIOLOGY OF WOUND
PATIENT’S MOBILITY
PATIENT’S ACCESS TO CARE
ULCER SITE
PATIENT’S TOLERANCE
CLINICIANS LEVEL OF EXPERIENCE
COSTSullivan V: Compression Pitfalls: improving patient Adherence with Compression Therapy.
Today’s Wound Clinic. Vol 4 Issue 12-Dec 2010

HOSE/SUPPORT STOCKINGS
Made of elasticated textile
Styles: knee, thigh, pantyhose lengths
Custom or off-the-shelf
Can be used as first line treatment in
patients with small ulcers
2-component systems

LEVELS OF COMPRESSION
Class I: 14-18 mmHg: Anti-Embolism hose
Not a therapeutic level of compression
Class II: 18-24 mmHg: dependent edema,
non-ambulatory, CHF
Class III: 25-35mmHg: Venous Insufficiency
Class IV: Lymphedema, need to have active
muscle movement

EXERCISE!!
CALF RAISES CALF STRETCHES
MARCHES
DAILY WALKING
UP AND DOWN STAIRS
SWIMMING

Compliance
• Can’t get them on
• Uncomfortable
• Cannot tolerate level of compression required

Not using compression = High degree of recurrence
Compression for preventing recurrence of venous ulcers. Nelson EA, Bell-Syer SE, Cullum NA Cochrane Database Syst Rev. 2000; (4):CD002303.

•58% non-compliance failure in Class 3 stockings
Prevention of recurrence of venous ulceration: randomized controlled trial of class 2 and class 3 elastic compression. Nelson EA, Harper DR, Prescott RJ, Gibson B, Brown D, Ruckley CVJ Vasc Surg. 2006 Oct; 44(4):803-8

• Recurrence is common
• Recurrence is more common in patients who are noncompliant with compression therapy
Healing of venous ulcers in an ambulatory care program: the roles of chronic venous insufficiency and patient compliance JOURNAL OF VASCULAR SURGERY November[1995 Curtis A. Erickson, MD, Debbie J. Lanza, BSN, RVT, Donna L. Karp, BSN, RVT, Janice W. Edwards, RN, RVT, Gary R. Seabrook, MD, Robert A. Cambria, MD, Julie A. Freischlag, MD, and Jonathan B. Towne, MD, Milwaukee, Wis.

Healing of venous ulcers in an ambulatory care program: the roles of chronic venous insufficiency and patient compliance JOURNAL OF VASCULAR SURGERY November[1995 Curtis A. Erickson, MD, Debbie J. Lanza, BSN, RVT, Donna L. Karp, BSN, RVT, Janice W. Edwards, RN, RVT, Gary R. Seabrook, MD, Robert A. Cambria, MD, Julie A. Freischlag, MD, and Jonathan B. Towne, MD, Milwaukee, Wis.
• Compliance is dependent on compression garment




Compliant Compression!
• Instead of Velcro, Bungee system to adjust compression
• No neoprene = no stretching out
• Breathable

Compliant Compression!
• 10 DIFFERENT SIZES
• 30-50 mmHg
• Garment, Liner, Bag
• Different Lengths


Liner

• 15mmHg just from zipping

• Must have a venous stasis ulcer
• A6545

Conclusion

Solving the Compliance Riddle with Compression Garments
Jeffrey D. Lehrman, DPM, FASPS, MAPWCA, CPC
Advisor, APMA Coding Committee
Advisor, APMA MACRA Task Force
Expert Panelist, Codingline
Fellow, American Academy of Podiatric Practice Management
Board of Directors, American Society of Podiatric Surgeons
Board of Directors, American Professional Wound Care Association
Editorial Advisory Board, WOUNDS
Twitter: @DrLehrman