Embed Size (px)
Citation preview

Some Observations on the Effects of ExperimentalDiets on Pulmonary Tuberculosis
By GEORGE DAY(Pkvsician, Mundesley Sanatorium)
To-day food rationing is providing us with a unique opportunity for performingmass-experiment~ in dietetics. In fact, it is performing some of the experimentsfor us: all we have to do is to make our observations and draw our conclusions.Unfortunately there are no simultaneous controls; so we have instead to dig backinto the archives of the past for our controls and discover how patients throvewhen all varieties of foodstuffs were more plentiful. Even so, comparison betweenthe progress rates of groups of patients at different epochs cannot be regarded asvalid unless it can be shown that the type of patients, the character of their diseaseand the lines of treatment, both general and special, remained fairly constantthroughout the years in question. As far as possible, evidence will be forthcomingto show that such was the case in these experiments.
~1ETHODS OF MEASURING PROGRESS.
For the purposes of this investigation, two and only two pieces of evidence willbe regarded when comparison is drawn between the effects of different diets uponpatients suffering from pulmonary tuberculosis; and they will be changes in bodyweight and changes in sedimentin index. According to these methods of assessment,a patient who has lost two stone in body weight is more 'ill' than one who has lostonly a few pounds; so is the patient with an index of 2'0 unit~ than one with 1'0
units. Similarly the patient showing an average improvement in his index of 0'06
units per month will be regarded as making progress three times as fast as one wholessens his index by 0'02 units.
Roth of these standards have their imperfections. Rarely does a patient on admi~
sion to the Sanatorium know what his normal (or optimum) body-weight should be:neither can he tell to within half-a-stone how much weight he has lost during theyear before his breakdown. If he has lost much weight, he naturally stands a greaterchance of gaining weight rapidly and over a prolonged period of time than anotherpatient does, who is already up to his normal weight. Similarly there is no means ofknowing in advance what the patient's 'normal' sedimentin index should be.There is no standard 'normal' index, any more than there is a standard 'normal'body temperature. In health the average index is found to be higher in women thanin men, in the elderly than in the young, and in the physically strenuous than in theparalysed. Again, both body-weight and sedimentin index are affected by a number of disease processes not specifically tuberculous.
Nevertheless, in spite of individual discrepancies in health and disease, the massbehaviour of body-weight and sedimentin index, if observed in a sufficiently largegroup of patients, gives us useful numerical assessments of the average rate of progress of that group for comparison with corresponding averages of similar groups.

216 TUBERCLE
THE ESTABLISHMENT OF CONTROLS
October 1942
During the three years ending Den'mber, 1939, before any rationing of foodstuffs came into action, the diet at ~Iundesley Sanatorium maintained a veryuniform level both in quantity and quality. During this period, too, the rate ~fprogress of the average patient as shown by the rate at which his body-weight increased and his sedimentin index diminished was remarkably constant. These rates,~xpressed respectively as (a) pounds of body-weight gained per month, and (b)units of sedimentin dropped per month, will be adopted as our controls. With themwill be contrasted the average rates of progress shown by groups of patients subjected to various experimental diets.
(a) Body-weight Control.-AII patients who are not too seriously ill to be movedfrom their beds are weighed weekly, and at the beginning of each month the weightgained or lost during the preceding month is noted. These gains and losses throughout the Sanatorium, added together and divided by the number of patients weighed. ,give the change in weight of the average patient for that month. During the controlyears 1937-8-9, this hypothetical average patient showed unfailingly a gain eachmonth. The variation in gain was from ~ to 3 lb. per month, due partly to seasonaland climatic influences but more largely to variations in the personnel. The averagepatient was found to gain weight faster during his first three months of treatmentthan he did later. The Group I Curve in fig. 5 shows that the total gain for the firstthree months was 5'75 lb. and for the second three months 4,'7 lb. After nine ortwelve months treatment very little increase in body-weight can be expected.Months therefore in which many new patients were admitted had high average;and at other times, when there was a preponderance of fit ambulant patients on theverge of departing, who were actually reducing their superfluous flesh by increasingexercise, the average gain for the months in question was lower. Bad cases, whobecame too ill to be weighed, were prevented thereby from contributing theirlosses to the aggregate, and so the observed average monthly gain is occasionallyhigher than a strictly accurate one would have been; but on the reasonable assumption of 'bad cases' developed during the course of the experimental diets, this discrepancy will cancel out.
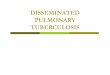
Fig. 1 shows the change in body-weight of the average patient month by monthfor the years 1937-8-9. It will be noticed that, although the yearly curves of summation diverge and converge, they run on the whole remarkably close togetherexcept for the last six months of 1939. During each of the years 1937 and 1938 theaverage patient gained about 16 lb., i.e. at the rate of 1'3 lb. per month, and thiswas maintained until the middle of 1939, after which it went ahead at about 2 lb.per month.
In parenthesis I must admit that I have never understood this sudden increase inrate which was so well sustained for the rest of that year. July and August were notparticularly happy months, and in September war was declared. Our patients werethereupon subjected to the tension of hourly news-bulletins, the irritation of unskilled black-out and consequent impairment of ventilation, and the growingconsciousness that (at that time) Mundesley was the nearest point on the Englishcoast to the enemy; all of which might have been expected to diminish appetitesand promote loss of weight. Instead, the increased rate of gain did not waver fromJuly to December 31St.

October 1942 TUB ERe L E 217
Without these 'bumper months' the average gain in weight was 1'3 per monthincluding them, it was 1 '47 lb. per month. The former figure will be Ilsed as 'control'for body-weight gain.
(b) Sedimentin Index Con/yol.-AII patients, except the completely moribund, havetheir sedimentin indices determined by a technique described elsewhere (Day, 1940)at the beginning of each month, when the number of units gained or lost during theprevious month is noted. The summation of all the gains and losses, divided by thenumber of patients tested, gives the change of index of the average patient for thatmonth. Unfortunately, systematic determination of indices throughout the Sanatorium was not practised before 1939; so the summation-curve for that year (fig. 4control) must stand a~ our control. It will be seen that it is subject to somewhatwider fluctuations from the straight line than is the weight-summation curve. The
22
20
/8
/6
14
Ibl.12- -
10
FIt;. I.
, ••01939
1 '30 lb. per month.0'053 units per month.
main reason for this is that certain transient conditions, e.g., acute pleurisy witheffusion, produce a much more violent effect upon the index than upon the bodyweight. In fact, if 4 or 5 per cent of the patients develop pleural effusions in anygiven month, their combined increase in index is more than enough to cancel thedecrease contributed by the remaining patients for that month, and the averagewill therefore show a deterioration. When the acute onset is over, these samepatients will lower their indices fairly quickly, but rather less than half as fast asthey increased them, so that for the next two or three months the average will showan exalted improvement. In spite of these kinks in the summation-curve, a monthlyaverage can be extl acted from it. It shows that the average patient improved hisindex at the rate of0'053 units per month.
Our average control figures will therefore be ;Increase in body-weightDecrease in sedimentin index

218 TUBERCLE October 194-2
THE EXPERntE~TS.
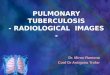
MAss EXPERIMENT No. I: SUDDEN CURTAILMENT OF SUGAR.-At the beginning ofJanuary, 1940, butter, bacon and sugar were rationed. Restriction of butter and baconscarcely affected the patients at all: ham, cold or grilled, replaced the hacon and margarine, which had frequently graced the table under another name (for experimentalreasons) merely flew under its true colours henceforward, and flew, it might be added,just as fast as the proverbial butter. But the restriction ofsugar \,'as felt i~mediately. Strangethough it may seem to us now, nearly three years later, the reductIOn of the allowancefrom It lb. per head per week for all purposes to i lb. was deeply felt and openly grieved.At the end of the first month of sugar-rationing, for the first time in the history of theSanatorium, the average patient showed a loss of weight. For the previous six months(the 'bumper months') he had been gaining at the rate of 2 lb. per month. He now lostllh. (see. fig. 2).
EXPECTED GAIN
/[AVERAGE/ Of 19J7·a,? J
II,,,
J
/,ACTUAL GAIN
.1940
./,
I
SUGAR CURTAILED
IIb,
o+--------..,.;,:::-----,i----------
l'DATE Of BROADCAST
• APPEAL' EAT MOR~ BREAD'
/ t---....:-fROST_1•
)939
BODY·WEIGHT GAIN OF AVERAGE PATIENT PLOTTED. TIME
SHOWING APPARENT SEQUELIt
TO SUDDEN CURTAILMENT Of SUGAR.19J9
0CT,
FIG. 2.
Now the weather was exceptionally hard that winter. Blizzards laged for weeks on (ndand we were snowbound on four ocasions. 1 he question aros:., 'Is this loss of bodyweight due to the hard winter, or to curtailed carbohydrate or to hath?' Over our 'InternalBroadcast System' to all patients' headphones was immediately broadcast a statementof the facts and an appeal for collaboration in a mass-experiment which might answer theabove question. The experiment simply consisted in eating more bread and potatoes,'An extra It lb. of bread is roughly equivalent to the curtailed i lh. of sugar. Alternatively

TUBERCLEOctober 1942 21 9
61b. of potatoes will do. Will you all kindly eat more bread or potatoes?'·-The responsewas magnificent. They chose bread, the daily order for which leapt up by 15 loaves'which meant that the average patient was consuming two extra loaves each week. Theyimmediately be~an to put on weight again, and by the end of the month the average gainwas I °'9 II). The frost continued-happily for the experiment-and did not break untilFebruary 26. But the patients-as one of them put it~'tired of eating themselves dizzyon bread'. More and more waste bread found its way into the swill-tubs, and by the endof March the consumption had dropped to a little over one extra loaf per patient perweek; and no tears, thrcats or entreaties, would induce them to repeat their violent Spurtof bread-gluttony. But a higher bread consumption has been maintained since the experiment than obtained before, and new patients have been drilled to eat a great deal morebread than they were accustomed to take at home.
MAss EXPERIMENT No.2: WARTIME RATIONING.-This experiment began, of course,on January 9, 1940, when the first sugar, butter and bacon coupons came into play, andit is still going on to this day. It would have been a much more conclusive experiment ifonly the conditions had remained constant for a few consecutive months. Unfortunatelythey did not. Before one had time to study the effect of curtailment of one particularfoodstuff, another foodstuff was curtailed, and the picture thereby confused. Our butter,sugar and bacon allowances were cut down in January 1940. In February there was alull. In March meat was rationed, but not offal, and the butter ration was doubled. Itwas halved again in June, when bacon and ham were docked further. Since July the fatration has remained constant, but margarine and butter have played Box and Cox severaltimes. And so it has gone on. Our rations have been cut so stealthily during the past twoyears that it is impossible to disentangle the different factors. Quite often, too, a substitutecould be found to replace a rationed commodity-temporarily, until the substitute wasrationed in its turn. Thus, as the available meat protein decreased, our consumption ofmilk increased, until it was supplying the patients with about a quarter of their proteinand fat, and a quarter of their calories. To some extent poultry and eggs replaced meat;but more noticeable was that with the fall of the consumption of meat and fats came acompensatory rise in the consumption of potatoes, green vegetables and bread. It is atruism that 'The less you eat of one thing the more you eat of another' (McCance); butthere appears to be a time-lag between curtailment and compensatory changes in thehabits of eating, with a corresponding lag in body-weight gain.
Further variations in the conditions of the experiment occured when on MidsummerDay, 1940, the Sanatorium transferred from Mundesley to Cheshire. From then onwardwe enjoyed milk twice as rich in cream, interesting changes in the quality of the meat andbread (the consumption of which showed another rise) and a deterioration in the qualityof the vegetables. The most noticeable change was the absence of bracing East Coast airand its replacement by something quite diflerenl. Our general feeling was that it was achange for the worse, but apart from a lag in the month ofJune itself, there was no noticeable change in the rate of our patients' progress.
By November, 1940, our ration of meat-protein was only a half, our fat a half, and oursugar a third of what it had been in June, 1939. Our average caloric intake per diem haddropped from 4,500 to 3,000.
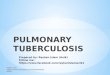
Fig. 3 shows what happened to the average body-weight since rationing began. Itshows the last few 'bumper months' of 1939, the loss in January, 1940, and the subsequentcurves for 1940 and 194t contrasted with the control curves. Similarly fig. 4 shows whathas happened to the S.I. since rationing bf gan. It is clear that in both respects the rateof progress of the average patient has been slowed. (It will be noticed that towards the endof 1941 both curves begin to gain a sleeper slope. This was after Experiment NO.3 hadbeen in operation some months, and an ever increasing number of the personnel weretaking the augmented diet.)

October 1942
[Eltpenmcn(No ) began
...•.
I 30 Ib per month~ 50 Ib100 Ib
.•...
SUGARRATIONING 8EGAN
J,n 9 1940
CONTROL A[1937.8.9J ./
,/./
./ .. '~~'./
./././
/ ....:.:..:.•., ..../' •.....•.•.....
TUBERCLE
BODY·WEIGHT
AVERAGE GAIN" CONTROL'19401941
12
·10
220
20
18
16
14
12
10Ibs.
8
14
FIG. 3·- Curves showing rate of increase in body-weight of avera!l'e patient.
CONTROL[l939J
070
060
050
040unlB
030
020
o 10
0
010
020/939
030
040
SUGARRATIONING 8EGAN
J.n 9. 1940
5EDIMENTIN INDEX-
AVERAGE IMPROVEMENT 19391940 "1941 .
(E Kpcrunent
No l "g.nl
0053 umt! per month00240043
MAYJUNEJUL YAUG.SEPT OCT. NOV DEC.
FIG 4-Curvcs showing rate of decrease in sedimentin index of a\'er~e patient.

October 1942 TUBERCLE 221
EXPERIMENT NO.3: THE RESULTS OF CARBOHYDRATE ExcEss.-By November, 1940,the situation appeared desperate. Patients were not doin~ at all well, and the evidence upto date seemed to suggest that deficiency of sugar might be at the root of the trouble.During'the three years before the war I had found that a group of patients on a highcarbohydrate diet with frequent and large doses of insulin fared better than the rest ofthe Sanatorium who received a normal diet, with no insulin (Day, 1940). Was the poorprogress at this juncture due to the general curtailment of food, or was it due in particularto too Iowa carbohydrate diet? This raised the question-'Supposing these patients couldreturn to the pre-war ration of sugar, i,e. It lb. per head per week, would they return totheir old rate of progress?' The Medical Research Council, approached with this problem,suggested that if patients were given not I t lb. but 5 lb. of sugar per week, not only wouldthe first question be answered, but the behaviour of a group of patients on a high carbohydrate diet without insulin would serve as a comparable control, hitherto lacking, to mypre-war group of 'insulin' patients: for they had had the very same quantity of sugarpluJ insulin. Accordingly it was decided that patients should receive 5 lb. of sugar perweek and a permit was granted to that effect.
Now it will be perfectly obvious to anyone who has worked in a Sanatorium that it isimpossible suddenly to get all patients, many of whom are real 'old lags,' deeply rootedin their habits, to co-operate willingly and reliably in an experimental scheme that entailstaking an extra four pounds of sugar per week for the rest of their sojourn. Some wouldhave struck, many would have tired of it after a week or two-as they did in the breadeating contest referred to earlier-and the experiment would have fizzled out.
Instead the sugar was introduced insidiously. Every new patient after November, 1940,had a fruit drink three times a day solemnly prescribed as part of his treatment. Eachfruit drink contained three ounces of sugar in flavouring of citric acid and syrup of lemon-a by no means unpalatable drink, as I found during the week I tried it on myself, and,what is more important still, one which can be drunk between meals without impairingthe appetite for the next meal. In this way each new patient automatically ingested 41b.(less an ounce) of sugar per week over and above what was cooked in his food and suppliedin his sugar basin, which is equivalent to an exira 1,000 calories a day. In all he receives5 Ih. of sugar per week.
In order to draw comparisons we need a new control curve for this experiment. Thecurve we have been using has shown the monthly variation in a cross-section of theSanatorium, and has dealt with patients new and old simultaneously. In the new controlcurve all patients admitted during the pre-rationing days have been shifted in time sothat they all start at zero-as if they had all been admitted on the same day. This curve islabelled Group I (figs. 5 and 6). Similarly all patients admitted between January andNovember, '940, who were subjected to unmitigated wartime rationing, are all broughtto their zero in Group 2. Finally, all patients admitted between November, 1940 andNovember, 1941, who have had the wartime diet and extra sugar, have been similarlygrouped and synchronized in Group 2+CH. Group I +Ins. is the curve shown by thepre-war group of patients who received Group I diet plus four pounds of sugar per week,and, of course, insulin.
The weight curves (fig. 5) and the S.l. curves (fig. 6) speak for themselves. GroupI +Ins. patients made the most rapid progress. Group I beats Group 2+CH by a shorthead; and Group 2 comes a poor last.
DISCUSSION.
Group 1+Ins. on a full pre-war diet plus four pounds of sugar per week, andhaving in addition an average dosage of 60 units of insulin per diem, showed themost rapid progress of all groups under consideration. But comparison betweenGroup I +Ins. and the other groups is perhaps hardly fair. It is a very small groupin the first place, and all its members were having insulin. They were also very muchmore ill than those of the other ~roups, being, without exception, patients whowere palpably below their normal body-weip;ht and who had been making little or

222 TUBERCLE October 1942
18
17
16
15
THE GROUPS COMPARED
[GAIN IN 80DY-WEIGHT '. TlH£)
AS IF ALL PATIENTS HAD
STARTED SIMULTANEOUSLY
14
Il,,
I
12 /I
II
'0
8lb.
7ShOWII'l! P.m:or loss o(
GROUP 1 In.before bCg,MIf'lt
Insulin ~nd
rllgh CH ~"~l
"
"I
I
II
(,ROl'P I{(''''''o') /'
P','?""'fRAGE GA''''5 PER HO"'TH
GROUP I [on. 500 ,,10".'](,ROlJP II ] 000GROUP II (H .. OCO
GROUP I, In, (on 5.500,)nd IMullAlJ
1Hlb.O'J IbI II Ib) 60 Ib
2m 1m ZERO 1m 2m I.. ''0 5'0 6m
FIG. 5.
060
THE GROUPS COMPARED(DECREA~E 1N 51 , TIME)AS If ALL PAlIENTS HADSTARTED SIMULTANEOUSLY
050.f GROUP I • lnhlhn J.nd high CH D,N
Pre: WH
A 'fRAGE fAll IN INDEX PER MONTH
0064 uniCSoOJI005)0150 "
4'03m2m111'1ZERO1m
...•.•.
ShO'f\lng Race orIncreJsc of S.J. InGROUP I In'lJdore begInningtn~uhn .lind
H'g" CH d,et
GROUP J Ion .. SOO (,\Iorlc~l
GROUP II J OJ()GROuP II CH .000 ..GROuP I ·lr>~ [00 S >00 <Jloru:'
r / Jnd IflHlhnl
,./GROUP II CH./. (, c SUl"ptcmcnury
./ 4 lbSug.vl--'. /'/'-' GROUP n
• Vnm..t'<td W., D,et:--- .e--'-'OL...--l---";~;';;;;~-~I--+---+---+--t------
2m
0)0
010
0'0
020
Flu. (i.

October 1942 TUBERCLE 223
no progress on an ordinary diet. The average S.1. when treatment began (see Table)was about 0'25 units higher than that of the other groups; and this means that theywere, so to speak nearly five months behindhand, reckoning that the average rateof improvement of the control group was 0'05 units per month. Finally, the averagepatient of this group had been losing weight and increasing his index for two monthsand sometimes longer, before this treatment was started (see figs. 5 and 6). It is truethat the likelihood of these patients doing well was poorer than it was of thosewithout these handicaps, but it is equally true that their scope for improvementfor covering emaciated frames and decreasing high indices-was much greater.
Insulin therapy has been used (as will be seen in the Table) in a larger percentageof cases since rationing began than ever before. The number of 'War ratiuned'patients so treated up to date is too small to be synthesized into a group ofany value,but my impression is that the results they show, although bettcr than those ofGroup r and very much better than those of Group 2+CH (which is havingexactly the same diet) are not so good as those shown by Group 1+ Ins. Myexperience convinces me more and more that Insulin remains the therapy of choicein cases where the nature and distribution of the disease preclude any immediateform of collapse therapy and when progress on routine diet is poor, absent or 'in thewrong direction'.
Groups r, 2 and 2 +CH (see Table) are far more comparable regarding age,male-female ratio, and their initial sedimentin indices. They differ to a greateror less extent as to the percentage of 'T.R. Positives', as to the percentage whichunderwent specialised lines of treatment (e.g. A. P., thoracoscopy, phrenic paralysis,gold, insulin, etc.), and as to the percentage which suffered from pleurisy witheffusion. Examination of these differences, however, reveals no reason why Group 2
should fare so much worse than Groups rand 2+CH. It would therefore appearthat the difference in caloric intake is responsible for the differences in rates of progress. Group r on 4,500 calories per diem beat Group 2 +CH on 4,000 calories.Group 2, receiving only 3,000 calories makes the slowest progress. Group 1+lns.,on the highest caloric diet, i.e. 5,500 per diem, makes the most rapid progress ofall. It may have no significance but it is perhaps worthy of note in passing that, bysubtracting 2,500 calories from each of these diets (as being a reasonable quantityto maintain health and hody-weight), the resultant figures over and above this areproportional to the wcight-gains shown by the three comparable groups: i.e.2,000 : 500 : 1,500 : : r '74 : 0'43 : I' r r.
If then calories be the motive force of progress, what is the best source of calories?Protein, carbohydrate or fat? It is highly improbable that one of these sources alonewould prove effective without the co-operation of the other two, not to mention thenumerous vitamins and mineral salts necessary for health: a certain balance in thediet is essential both for metabolic efficiency and for palatability. All the same it isworth examining our data to discover whether, given a basal foundation of all threeingredients, increase of one or other of them helps the body-tissues to triumph overtuberculosis. Should we prescribe an excess of protein, fat or carbohydrate?
The ration of meat-protein available from every source-meat, offal, eggs andcheese-dwindled steadily throughout the years of the experiments, so that to-daythe Mundesley patient gets between a third and a half of what he used to get beforethe War. And yet the average rate of progress has not become steadily worse.

224- TUB ERe L E October 1942
During the latter half of 1941, in spite of the growing restriction on tinned meatscaused by the 'points' system, there was a marked improvement in the progress-rate.Meat-protein we may therefore fairly conclude, is relatively inessential.
The importance of fats is rather harder to determine. Our patients suflered nocurtailment of their total fats until July 1940; so fat-deficiency cannot be blamedfor the poor progress during the first six months of that year. InJuly the combinedtotal for table fats (Le. butter and margarine) was limited to 6 oz. per week, andcooking fats to 2 oz. per week; but just about this time our milk doubled its creamcontent. Since July 194-0 the supplies of fats from these sources have continuedwithout further abatement; but, as a goodly proportion of the total daily fats beforethe War was derived from fat meat and bacon, which have since been more andmore restricted, the total fat-ration has undoubtedly dwindled since that date.Were fats of m~jor importance we should have expected their curtailment to leaveits mark on the curves 194-0 and 194I in figs. 3 and 4; but nothing of the sort isapparent.
Two observations suggest that carbohydrate is the most important foodstuff inthe treatment of tuberculosis. First is the sudden change in the rate of progressthroughout the Sanatorium as a whole when sugar was rationed, as shown in Massexperiment No. I (fig. 2), and the failure to recover anything like the old progreSsthroughout the rest of that year. Second is the way the Sanatorium's progress rateimproved as more and more patients received the extra sugar (see figs. 3 and 4-).Only newcomers, it will be remembered, were given it: five or six in December,1940; another half-dozen in January, 1941; and so on until by July, 1941, nearlyevery patient was having it. From that time onwards the progress-rate curvessteepen until they almost parallel those of the controls, in spite of the fact that otherfoodstuffs were continually heing curtailed.
We cannot, however, rule out the possibility that Group 2+CH might havefared equally well (or even better) had its extra calories been supplied as fat~ insteadof sugar. Personally I do not think it would. Before the War my experience withextra fats was disappointing. Very rarely was 1 convinced that any patient benefitedfrom extra cream and cod liver oil. The few who did had invariably suggested theseadditions to their diet themselves. They seemed to know instinctively that theyneeded them. To prescribe extra fats indiscriminately to all who were 'not gettingon' was to court disappointment. Many, probably already suffering from hypochlorhydria, would find it cloyed their appetite. Again, most of the patients whosubsequently formed Group I +- Ins. had a preliminary trial of these extra fats without any encouraging result. Then when they began insulin injections and the highcarbohydrate diet, all extra fats were cut right out of their diet-even milk drinks-and they responded at once by changing from a 'negative' to a 'positive' rate ofprogress.
Himsworth's (1938) researches showed that the tuberculous diabetic fared betteron a high-carbohydrate low-fat diet with massive doses of insulin than on a lowcarbohydrate high-fat diet with a mere adequacy of insulin. ~ly Group I +Ins.results confirmed the value of the high-carbohydrate diet with insulin for thenon-diabetic tuberculous patient; but the question as applied to the non-diabeticpatient not in receipt of insulin wiII remain open until a group of such patients havebeen subjected to wartime diet plus 1,000 calories per diem in fats. This experiment

October '942 TUB ERe L E 225
is in progress at the moment at Tor-Na-Dee Sanatorium, and results will be published in due course,
By definition 'consumption' upsets metabolism, i.e. causes wasting; but th~ resultsof the foregoing experiments remind us that wasting should be regarded merelyas a segment of a vicious circle. If, in spite of severe destructive disease with itsresultant toxa'mia, metabolism can be improved by enlightened dietary, the viciouscircle is broken, or rather reversed, and made benign. If a patient's metabolism canbe improved, even only temporarily, the circle may remain benign when he returnsto a more restricted diet, and he will certainly be in better fettle for any operativeprocedure that may be desirable than he was when going downhill.
In this connection it should be noted that improvement in body-weight appearsto precede improvement in sedimentin index. With the individual patient thi~ isnot always the case. For instance, an emaciated patient, on being suddenlyput to complete bed-rest and given a full diet, may start to regain his lost bodyweight at a most gratifying speed, while his lung lesions deteriorate both clinicallyand radiologically, and his index rises accordingly. In another case a selectiverelaxation of the diseased area of lung obtained by operative measures may inaugurate more rapid improvement in the index than in the weight, and toxa'miabeing lessened pari passu, the vicious circle is reversed in another segment. Withlessened toxremia metabolism improves and gains in body-weight follow. Usuallyhowever, other things being equal, changes in the index, good or bad, follow hardon the heels of similar changes in the body-weight. In Mass-Experiment No. " loss
10 6·6 ,8'7 32
24 35'3 37'4 932 '5 42 50 40
3'5 4'4 '4 99 9 II 9
'9 9 4'7 '46 " II ('00)
5'4 " 3'2 '98'4 " ,6
'3'7 22 '9 '9
, '7' , '70 ,,68 "95
4'500 3'000 4'000 5'500
1'74 0'43 /'3 3,6
0.064 0'°31 0'°55 0'15°
Number in GroupAverage AgePercentage of MalesPercentage of FemalesPercentage of T.n. PositivePercentage with 'A,P.' established
before admissionInduced within six monthsTotal 'A.P.s'
Percentage with Double 'A.P,s'Percentage with Phrenic Paralysis
Gold Injections ,.Insulin Therapy . ,
Percentage with Pleural Effusionpresent on admission ,.
Developed within six months "Total
Average Sedimentin Index onAdmission (Units)
TABLESHOWING THE OCCURRENCE OF DIFFERENT FACTORS WHICH MIGHTPOSSIBLY INFLUENCE RATE OF PROGRESS IN THE DIFFERENT GROUPS
Group, Group 2 Group 2+CH Group 1+Ins.166 45 63 22
36.8 36'5 35'9 32 '2
67 62 70 60
33 38 30 40
57 64 7' 73
Daily Caloric Contellt oj DietAverage mOllthly gaill ill Body-weight
(pounds)Average monthly decrease ill Sedimelltill
Index (units)

226 TUBERCLE October 1942
in body-weight in January was followed by deterioration in index in February.Group I +Ins. also showed its maximum improvement in index after three monthsof intensive gain in body-weight.
Finally, the experiments amply demonstrate that on an average the patient whogains body-weight most rapidly will also diminish his index most rapidly; thereforeif, inter alia, two of the objects in the treatment of pulmonary tuberculosis are tocause the patient to regain the lost stone or half-stone of body-weight, and to reducehis index from the neighbourhood of) '70 units to the neighbourhood of 1'00 units,it is going to take about twice as long to achieve these desiderata on Group 2 dietas it will on Group 2+CH diet.
Is it not possible too, in spite of all authoritative pronouncements to the contrary,that wartime rations may be inadequate to check the progress of the disease of thelightly-infected patient, which on a more ample diet would resolve without everemerging from the preclinical phase?
SUMMARY.Over different periods of time dUt ing the past five years different groups of
patients suffering from pulmonary tuberculosis have been subjected to differentdiets, and the rates at which they progressed towards health have been observedand compared.
The diets were:-(a) Unrestricted pre-war diet.(b) Unrestricted pre-war diet with extra sugar and injections of insulin.(c) Wartime-rationed diet.(d) Wartime-rationed diet with extra sugar.
The progress-rate of the average patient of each of these groups has been calculated from the rate at which his body-weight increased and the rate at which hissedimentin index decreased. These different rates have been compared and contrasted.
It is found that the third group of patients, subjected to unmitigated wartimediet, made considerably poorer progress than did the other groups on less restricteddiets, both in body-building and in index-lowering.
It appears too, within the limits of the experiments, that rate of progress is pro~ortional to the height of the diet's caloric value.
The question as to whether carbohydrate is the most effective ingredient of dietto be increased in order to achieve a high caloric content is discussed but left undecided on the evidence available at present.
My grateful thanks are due to my partners Dr. Wynne-Edwards and Dr. Vere Pearsonfor their unfailing collaboration; to Professor H. P. Himsworth, Dr. R. A. McCanceand Dr. A. Bradford Hill for pungent but helpful criticism; and to the Medical ResearchCouncil for enabling me to obtain the extra sugar necessary for the experiment.
REFERENCES.Day, G. (1940) Lancet, I, 1160.Day, G. (1940) Brit. Med. ]ourn., 2, 376.Himsworth, H. P. (1938) Q,uart.]. Med., n.s., 7, 373.McCance, R. A. and Widdowson, E. M. (1940) Chemical Composition of Foods,
Medical Research Council.