Embed Size (px)
Citation preview

STATISTICS IN MEDICINEStatist. Med. 2000; 19:3389–3400
Some practical issues in the design, monitoring and analysisof a sequential randomized trial in pressure sore prevention‡
Julia Brown1;∗;†, Damien McElvenny1, Jane Nixon2, Jackie Bainbridge1
and Su Mason1
1Northern and Yorkshire Clinical Trials and Research Unit; University of Leeds; U.K.2Nursing Research and Development Unit; St James’s University Hospital; Leeds; U.K.
SUMMARY
A sequential double blind (assessor and patient) triangular design was used to compare the incidenceof pressure sores following elective major surgery among patients lying on a standard foam mattresswith those on a dry visco-elastic polymer pad during their operation. A total of 446 patients wererecruited into the trial between 1994 and 1996. Interim analyses were carried out after 181 patientswere entered into the trial and then subsequently after approximately every 100 patients recruited. Thetrial unexpectedly reached a stopping boundary at the �rst interim analysis, however the IndependentData Monitoring Committee recommended continuation of the trial. They were concerned that there wasa need for a larger de�nitive trial and about an apparent treatment by centre interaction. They requireda substudy to be undertaken to further validate the subjective endpoint, and that further sensitivityanalyses of the main trail endpoint should be carried out in the second interim analysis. The trial wasstopped at the third interim analysis when again a stopping boundary was crossed indicating that thegel pad was associated with signi�cantly fewer pressure sores than the standard mattress (log odds ratio−0:7, (95 per cent con�dence interval (CI), −1:28;−0:11), p=0:02) (estimate CI, p-value adjustedfor group sequential conduct). The design, monitoring and analysis of this trial will be presented as anexample of the practical problems or non-problems encountered for the local hospitals, for the trialsunit, for the data monitoring committee and for the funding committee. Copyright ? 2000 John Wiley& Sons, Ltd.
INTRODUCTION
Pressure sores on patients cause major di�culties both for the patients and health authorities.Pressure sores cause discomfort and pain for patients and in severe cases may even inhibit
∗Correspondence to: Julia Brown, Head of Unit (Joint), Northern and Yorkshire Clinical Trials and ResearchUnit, University of Leeds, 17 Spring�eld Mount, Leeds LS2 9NG, U.K.
† E-mail: [email protected]‡ Presented at the International Society for Clinical Biostatistics, Eighteenth International Meeting, Boston, U.S.A.,July 1997.
Contract=grant sponsor: Northern and Yorkshire Regional Research Committee
Received June 1998Copyright ? 2000 John Wiley & Sons, Ltd. Accepted August 2000

3390 J. BROWN ET AL.
Table I. Site-speci�c outcome classi�cation according to combination of skin assessment scores.
Assessment timeImmediate Immediate (up to 1=2 hour) 1=2–1 hour following Day 1 post-operation Site speci�cpre-operation post-operation previous assessment (8a.m.–8p.m.) outcome
0 0 any value any value success0 ¿1 ¿1 ¿1 failure0 ¿1 ¿1 0 success0 ¿1 0 any value success1 0 any value any value success1 1 any value any value success1 ¿2a ¿2a ¿2a failure1 ¿2a ¿2a 1=0 success1 ¿2a 0=1 any value success
rehabilitation and cause death. They may cause prolongation of hospital stay so reducingavailability of hospital beds and hence the throughput of patients.The critical determinants of a pressure sore development are the intensity and duration of
pressure and tolerance of skin to pressure. A literature review of intra-operative pressure soredevelopment has suggested a causal relationship between events during surgery and subsequentdevelopment of pressure sores [1]. Although many hospitals in the U.K. have pressure soreprevention strategies, prior to 1994 none of the products available for use in theatres had beensubject to rigorous evaluation [2]. Evidence was available mainly from measuring the pressureof operating theatre equipment on the skin, although the importance of these measurements inrelation to skin damage has not yet been determined. In addition, small observational studieshad been carried out [3].Products for use in the operating theatre were being marketed on their ability to reduce
interface pressure but their role in reducing pressure sores originating in the theatre hadnot been determined. We were therefore interested in comparing such an interface pressure-relieving mattress, the dry visco-elastic polymer pad, with a standard operating mattress inrelation to the post-operative pressure sore incidence.
DESIGN
To answer this question, a trial was set up to be run in two centres in the North of England.The trial protocol was approved by the Local Research Ethics Committee in each of thesehospitals. The primary endpoint for the trial was determined as a success (no pressure sore) orfailure (pressure sore) (Table I) at one or more of the �ve skin sites most likely to incur skindamage (sacrum, left and right buttocks, and left and right heels) [4]. The primary endpointwas established using the de�nition of a pressure sore as ‘persistent discolouration of the sameskin site on two or more successive days’ [5]. Skin was assessed using a scale previouslydeveloped by Torrance [6] (see Table II). A particular feature of the endpoint de�nition wasthe speci�city of persistent worsening of the skin condition from its pre-operative conditionto that post-operatively.
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

SEQUENTIAL RANDOMIZED TRIAL IN PRESSURE SORE PREVENTION 3391
Table II. Skin assessment scale.
Grade Description of skin
0 No discolouration of skin1 Redness to skin – blanching occurs2a Redness to skin – non-blanching area2b Super�cial damage to epidermis – broken or blistered3 Ulceration progressed through the dermis4 Ulceration extends into subcutaneous fat5 Necrosis penetrates the deep fascia and extends to muscle
The skin was assessed at four stages for the purposes of determining the endpoint: atbaseline in the anaesthetic room before surgery by the local data manager; immediately afterthe operation in the recovery room by the recovery room sta�; one hour after the operation,and on the ward the day after the operation by ward sta�. Success or failure for a particular sitewas determined as set out in Table I. Secondary questions included the identi�cation of riskfactors for subsequent pressure sore development and the prevalence of pre-operative pressuredamage to the skin. This paper will concentrate on the design, monitoring and analysis issuesassociated with the primary endpoint. The full trial results are presented elsewhere [5].Patients were included in the trial if they were scheduled for elective major (that is, planned
surgery with an average surgical time of 90 minutes or more), general, gynaecological orvascular surgery, were aged 55 or over, and were to be in a supine or lithotomy positionduring surgery. Essentially these were the patients considered to be more likely to developa pressure sore than a general population of surgical patients. Patients with existing damageor skin pigmentation=conditions which precluded reliable identi�cation of skin discolourationwere excluded.The double triangular sequential design was used in this trial [7]. The sequential design
was chosen because a priori a large di�erence in the e�ect of the two mattresses was ex-pected, based on the results from the small scale studies. However there was relatively poorinformation about the incidences that might be expected, in particular on the standard arm[8–11]. In a sequential trial with a binary primary outcome the power is preserved as longas the di�erence to be observed remains the same regardless of the true value on the con-trol arm. In this particular study, ‘di�erence’ is referred to on the log-odds ratio scale. Itwas also important to determine the e�cacy or lack of e�cacy of the gel pad as quickly aspossible since the dry visco-elastic polymer pads were in use on an ad hoc basis in one ofthe hospitals. The sequential design would allow a valid analysis of the results at the timeof stopping, regardless of when this was, and possibly allow a reduction in the number ofpatients required to answer the question over a �xed sample design, therefore reducing costs.The double triangular version of the sequential design was chosen because it was importantthat inferiority of the gel pad could be distinguished from a lack of di�erence, and that earlystopping would be possible even if there was no di�erence between the mattresses, enablinghospitals already using the gel pads to make policy decisions.Based on the previous small studies, the trial was designed to detect a reduction from 10
per cent pressure sores on the standard mattress to 5 per cent pressure sores on the gel pad,with 90 per cent power at a 5 per cent signi�cance level, that is, to be able to detect a
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

3392 J. BROWN ET AL.
Table III. Properties of the proposed double triangular design.
� PS PG c+(�) c−(�) E(n∗) p90(n∗)−1:12 0.1 0.254 0.000 0.998 228 312−0:75 0.1 0.19 0.000 0.900 394 5880 0.1 0.1 0.025 0.025 583 7700:75 0.1 0.05 0.900 0.000 685 10501.12 0.1 0.035 0.998 0.000 494 723
E(n∗) is the expected total number of patients.p90(n∗) shows the total number of patients which is exceeded with probability 0.10.c+(�) is the probability of concluding that the gel pad is better at the 5 per cent signi�cance level when the e�ectsize is �.c−(�) is the probability of concluding that the gel pad is worse at the 5 per cent signi�cance level when the e�ectsize is �.
log-odds ratio of gel pad to standard mattress of −0:75. A decision was made at this stageto perform interim analyses after the trial had been recruiting for six months and thereafterat three-monthly intervals. The projected accrual �gures suggested that this schedule wouldentail analysis after approximately 200 patients and then after each 100 subsequent patients.It was felt that this would be a practical approach given that two centres were involved inthe trial. Although stopping after 200 patients was thought to be unlikely, this analysis wouldallow assessment of accrual, data ow and safety issues. The choice of the interim analysisschedule was a balance between practicality and bene�t from sequential design; obviouslymore frequent examination would allow the full bene�t of sequential analysis to be exploited,with maximum bene�t from early stopping. However the logistics of arranging data monitoringcommittee meetings and the need to have collected enough data to be ‘convincing’ led thechoice of the interim analysis schedule. Table III shows the power of the study, assuming theinterim analysis schedule as detailed above, for various potential values of the log-odds ratioand the expected number of patients who would be required to be entered before stopping thetrial. A �xed sample design would have required 1085 patients. For this sequential design,randomization was to occur until a stopping boundary was crossed which was almost certainto occur by the time 1700 patients had been recruited and very likely to occur considerablysooner.The sequential plan is given in Figure 1.The di�erence between the gel pad and the standard mattress is given by the log-odds ratio
�= log(PG(1− PS)=PS(1− PG))
where PS is the proportion of patients allocated a standard mattress developing a pressure soreand PG is the proportion of patients allocated a dry visco-elastic polymer pad developing apressure sore. Thus �¡0 if the gel pad is superior, �=0 if they are equivalent, and �¿0 ifthe gel pad is inferior.At each interim analysis Z , the e�cient score for the log-odds ratio �, and V , the Fisher’s
information for �, were plotted to see if any of the boundaries for acceptance or rejectionof H0 had been crossed. The statistic Z is approximately normally distributed with mean �V ,variance V: Z measures cumulative evidence of treatment e�ect, and V measures amount of
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

SEQUENTIAL RANDOMIZED TRIAL IN PRESSURE SORE PREVENTION 3393
Figure 1. Illustration of the double triangular sequential design.
information contained in the data about the treatment e�ect:
Z = (nGFS − nSFG)=nV = nGnSSF=n3
where nS is the number of patients with an endpoint recorded on the standard mattress, nG isthe number of patients with an endpoint recorded on the gel pad, FS is the number of patientsdeveloping a pressure sore on the standard mattress, FG is the number of patients developinga pressure sore on the gel pad and
F = FS + FG
n = nS + nG
S = n− F
If Z lies above the upper boundary or below the lower boundary then the trial shouldbe stopped since there is evidence of a di�erence between the mattresses; if Z crosses themiddle boundary then the trial should be stopped and no di�erence between the mattressesdeclared. Alternatively, if Z lies within the boundaries then the trial should be continued tothe next interim analysis. The continuous boundaries shown in Figure 1 were adjusted at each
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

3394 J. BROWN ET AL.
interim analysis for the fact that the sample path was only inspected at discrete times and notcontinuously. The continuous boundaries assume continuous monitoring of the sample path,whereas in fact inspections took place at discrete times. This adjustment, the ‘Christmas tree’adjustment, contracts the boundaries by 0:583
√(Vi − Vi−1) where Vi − Vi−1 is the increase in
information at the ith inspection [12]. The longer the gap between data inspections, the greaterthe magnitude of this adjustment.Randomization was strati�ed by centre and age (55–69, 70 years plus). A telephone ran-
domization service was used, based on permuted blocks of size 6. All pre-operative data wererecorded by a data manager assigned to the trial in each centre. All post-operative data wererecorded by local hospital sta� who had received training in the pressure sore assessment tooland were blind to the randomization mattress allocation.A Data Monitoring Committee (DMC) was set up to oversee the monitoring of the trial,
consisting of a statistician, a representative of an NHS purchasing organization who was alsoa member of the funding committee, and a nurse researcher. The statistician analysing thetrial and the DMC were blind to the mattress allocation.All statistical analyses were carried out on an ‘intention to treat’ basis using the PEST3 [13]
and SAS software packages. The analysis was carried out using the log-odds ratio formulationof the design. All analyses were adjusted for the strati�cation factors used in the treatmentallocation (centre and age of patient) and the covariates identi�ed as important in the protocol(that is, type of surgery and length of operation). The second and �nal interim analyses and theanalysis on termination were adjusted for strati�cation factors, covariates in the protocol andcovariates identi�ed by the Data Monitoring Committee at the �rst interim analyses meeting(that is, length of pre-operative stay and percentage of time the patient was in a hypoten-sive state during surgery). Recent work by Jennison and Turnbull [14], and also Scharfsteinet al. [15], has provided con�rmation that in the presence of covariates the joint distributionof this series of the score (Z) statistics is multivariate normal with an independent incrementscovariance structure, and that the joint distribution depends only on the statistical informationavailable at each interim analysis.The covariate adjustment analysis was carried out using the logistic regression and inter-
active matrix language procedures in SAS. The strati�ed and covariate adjusted analysis oftreatment e�ect on termination was carried out using the overrunning analysis option in PEST3[16]. The overrunning analysis incorporates data from the 47 patients who had already beenrandomized by the time the DMC recommended stopping the trial. Essentially the overrunninganalysis adjusts for all interim analyses except for the one which called for stopping (andwas in a sense temporarily disobeyed). All interim analyses were carried out on the primaryendpoint only.
MONITORING=INTERIM ANALYSIS
A total of three interim analyses were undertaken. The �rst interim analysis was carried outafter 181 patients had been randomized. At this �rst analysis the overall rate of pressure sores(20 per cent) was much higher than had been expected based on previous literature. Theinterim analysis is shown by the �rst cross in Figure 2, with the appropriate Z and V valuesgiven in Table IV. The results had crossed a stopping boundary suggesting that there wasa statistically signi�cant di�erence between the mattresses. At this stage the blind was not
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

SEQUENTIAL RANDOMIZED TRIAL IN PRESSURE SORE PREVENTION 3395
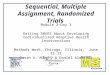
Figure 2. The di�erence in pressure sore incidence for the two mattress types.
Table IV. Interim analysis record.
Interim analysis Date V Z
1 27=6=95 6.6 7.62 22=1=96 8.1 6.73 30=5=96 11.6 9.94 5=6=96 12.9 10.2
broken; the signi�cant di�erence was subsequently found to be in favour of the gel pad. Thisinterim analysis was presented to the DMC which, despite a stopping boundary being crossed,decided to continue the trial. Contrary to initial beliefs of the trial investigators and the datamonitoring committee when designing the study, members felt there was an overwhelmingneed for a larger de�nitive trial, were concerned that there was a major di�erence in the rateof pressure sores between the two centres involved which needed investigation (4 per centversus 27 per cent) and that the endpoint chosen for the study was subjective. They decidedthat, in order for the results to be taken seriously, a sub-study within the trial to validate theendpoint should be undertaken. In addition there was felt to be no major risk to patients incontinuing recruitment. As the de facto rule was stricter about stopping to show treatmentdi�erence than the one adjusted for, the analysis shown is (very slightly) more conservativeand, in particular, the reported p-value is (very slightly) larger than for the de facto rule.
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

3396 J. BROWN ET AL.
There was also a need to recruit more patients in order to be able to assess risk factorsfor pressure sore development, one of the secondary aims of the trial. DMC members alsosuggested that additional variables (length of pre-operative stay and percentage of time patientwas in a hypotensive state during surgery) be used as covariates to adjust the treatment e�ectin future interim analyses. Work was therefore initiated to investigate di�erences in pressuresore management policy at the two centres and a co-assessment system was set up such thatpost-operative assessments of skin were undertaken by two independent assessors.The second interim analysis was undertaken when 293 patients had been randomized, and
is shown by the second cross in Figure 2 and Table IV. The trial had moved back into thecontinuation region. The DMC now had to balance statistical considerations against practicalissues. Statistically the trial should continue; however, the rate of pressure sores recorded haddropped dramatically since the �rst interim analysis, there was some evidence of unreliabilityof the endpoint, the co-assessment study was showing there was disagreement about theskin assessment grade in 10–20 per cent of the assessments and the number of pressuresores in one centre was still extremely low. In favour of continuing the trial was the factthat there was a danger of overinterpreting the ‘subgroup’ of patients recruited since the�rst interim analysis; the co-assessment data were still only available on a small sample ofpatients, and the treatment estimates indicated that there was a potential di�erence betweenthe mattresses which would be worthy of investigation. The DMC recommended continuationof the trial.The third interim analysis was undertaken when 399 patients had been randomized and
is shown by the third cross in Figure 2 and Table IV. There was a statistically signi�cantdi�erence in incidence of pressure sores such that the stopping boundary had again beencrossed. The co-assessment discrepancy rate had levelled o� at around 7 per cent. The DMCdecided that patient randomization should be suspended and the data for all patients shouldbe analysed. This overrunning analysis or ‘analysis on termination’ was outside the stoppingboundary, as shown by the fourth cross on Figure 2 and in Table IV, so the trial was stoppedafter 446 patients had been randomized.
ANALYSIS ON TERMINATION
The analysis on termination of the trial included calculating the median unbiased e�ect of thelog-odds of developing a pressure sore on the gel pad compared with the standard mattress.The gel pad signi�cantly reduced the log-odds of a pressure sore as compared with standardmattress by −0:7 with 95 per cent CI (−1:28;−0:11); p=0:02. (Estimate, con�dence interval,p-value all adjusted for the group sequential design, strata in the randomization allocationand covariates of interest.) Using a conventional �xed sample analysis would have obtaineda log-odds of −0:77 with 95 per cent CI (−1:36;−0:18); p=0:01. Adjusted point estimatesof the probability of developing a pressure sore on gel pad compared with standard mattresswere 0.11 and 0.2, respectively. Sensitivity analyses were carried out whereby all missingendpoints were counted as failures and, where endpoints were showing discrepancies fromthe co-assessments, these were substituted into the analysis instead. These analyses made nodi�erence to the direction of the treatment e�ect and the treatment e�ect remained statisticallysigni�cant.
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

SEQUENTIAL RANDOMIZED TRIAL IN PRESSURE SORE PREVENTION 3397
ENDPOINT DETERMINATION
The inclusion of reactive hyperaemia (skin redness) within the endpoint de�nition of this studyand others is a source of debate [17]. Central to this are questions regarding the relationshipbetween the observation of reactive hyperaemia and subsequent skin=tissue loss, which hasbeen the subject of little research, and the validity of the use of a skin response whichis reversible or transient. However, when assessing the immediate e�ect of a single pressureassault, hyperaemia provides sensitive clinical evidence of capillary occlusion and the endpointcriteria used in this study clearly distinguishes between transient and persistent skin changesproviding an outcome which enables di�erentiation between the two support surfaces. Thevalidity of the outcome criteria is further supported by the large percentage (69 per cent)of endpoint failure patients whose skin was observed to have changes persistent beyond theendpoint period of day 1 post-operatively.The trial also included a large number of post-operative assessors which may have a�ected
the validity of the results. However the co-assessment study quanti�ed this level of disagree-ment between assessors at 7 per cent and, as these disagreements were all one point di�erenton the skin scale, this only a�ected classi�cation of �ve endpoints and did not impact on theoverall di�erence between the mattresses.Of the 446 patients randomized into the trial, the endpoint was not determinable on 16
patients due to missing post-operative assessments. Skin assessments were not possible dueto patients leaving theatre with bandages or being bandaged on the ward over one or more ofthe key sites, patients having to return to theatre within a day, patient emergency in recovery,or patients too ill to be moved for assessment. Sensitivity analysis to try and estimate thepotential impact of the missing data did not alter the conclusions of the trial. For three patientsthe endpoint was determined on only four sites since it was not possible to undertake pre-or post-operative assessments on one site due to bandaging (as above) or, in one case, thepatient having previously had the right leg amputated.
DATA COLLECTION
Di�culties were encountered in trial management resulting in a 30 per cent loss of the eligiblepatients. For example, there was a tendency for more than one patient to arrive at one time inthe anaesthetic room, causing problems for the data manager in carrying out the pre-operativeskin assessments; pre-medication had sometimes been administered before the data managerscould obtain informed consent; patients were very anxious about the impending operation andtherefore felt unable to consent to the trial; patients were too ill to be approached; operationswere rescheduled, necessitating pre-operative assessments to be repeated. Recovery room sta�were also very busy, so there was the danger of missing some of the post-operative skinassessments unless they were constantly reminded. A further issue not anticipated was thatpatients undergoing general, vascular or gynaecological operations could be having more thanone operation within the recruitment period; six patients were entered twice into the trialbefore the eligibility criteria were altered appropriately. The data for these six patients fortheir second entry were excluded from the �nal analysis. In addition the operative positionof some of the patients was changed from lithotomy or supine to another position during theoperation. The data from these patients were still included in the intention to treat analysis.
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

3398 J. BROWN ET AL.
SEQUENTIAL TRIAL – PRACTICAL ISSUES
In practice the sequential design for this two-centre trial did not cause a lot of di�culties forthe Trials Unit. The data collection, data input and analysis required a disciplined approachso that the interim analyses could be undertaken as planned. Speedy data collection wasfacilitated by local data managers on each site who were contactable on a daily basis and bythe fact that data collection was kept to a minimum, thus data validation, entry and checkingcould be kept up to date.There were problems with funding for the trial. Neither the Trials Unit, the lead clinician
nor the funding committee had previous experience of sequential trial design. In the fundingapplication, although the committee was aware of the potential variability in sample size, theyinsisted that a sample size should be given in order to agree an initial budget for the trial.The trials team costed the trial for a sample size of 600 patients, the 90th percentile forthe terminal sample size if the log-odds ratio of gel pad to standard was −0:75. Luckily thesample did not go beyond this estimate. The funding committee also felt uneasy about thetrial and insisted they should be represented on the Data Monitoring Committee. This couldhave raised problems with con icts of interest for that member; however, in practice this didnot seem to be an issue. The trial team also calculated funding for posts to recruit the requirednumber of patients to be randomized; in practice 70 per cent of the eligible patients wererandomized but all were processed to some extent. Recruitment of the local data managersor central Trials Unit sta� could have posed problems because of the uncertain length of thetrial. In practice this was achieved by sta� at the participating hospitals being seconded tothe trial is an open-ended arrangement. The Trials Unit was able to use experienced sta�who were funded from other trials in addition to this one, thus providing some security ofemployment. With hindsight the �rst interim analysis could have been undertaken later than itwas, since it was clear that the DMC felt reluctant to stop the trial at the �rst interim analysis,that is, after 200 patients. However they were aware that overriding the formal indication forstopping in this way should have little e�ect on the �nal analysis. Moreover this interimanalysis did provide the DMC with an opportunity to make suggestions on the trial conductwhich ultimately improved the trial design.A further limitation of the methodology at the time of the analysis of this trial was that
there was no reliably accurate approach to the calculation of the con�dence intervals for theproportions of patients with success on each treatment group. Recent work published by Toddand Whitehead provides such a method [18].Finally the estimate of the log-odds ratio with the triangular design will always be less
precise than with the �xed sample design, even if the �xed sample size is exceeded (refer-ence [7], p. 145). It can be demonstrated by analogy or by the use of PEST that the samerelationship holds for the double triangular test.
GENERAL ISSUES
The most striking result was the major di�erence in the rate of sores between centres: 3 percent versus 20 per cent. The di�erences observed are not mirrored in the continued follow-upto day 8 where the number of pressure sores is the same in each of the centres. A detaileddata collection procedure was required to be able to investigate which factors in uenced the
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

SEQUENTIAL RANDOMIZED TRIAL IN PRESSURE SORE PREVENTION 3399
centres’ rates. A review of pressure management procedures at the two centres was carriedout but this did not reveal any di�erences. Time and �nancial constraints meant that it wasnot possible to collect further detailed data at the centres. It must be noted however that aretrospective review would have had limited usefulness.This does mean that more work is required to identify which factors in uence the develop-
ment of a post-operative pressure sore and that these factors might have the potential to havemore impact on pressure sore rates than the use of the di�erent mattresses in the operatingtheatre.
CONCLUSION
This trial represents a considerable improvement over the previous trials of pressure soreequipment. It is larger than most of the preceding studies, the endpoints are measured blindand the eligibility criteria are clearly speci�ed. Generally the sequential methodology hasworked well and enabled us to obtain a quicker answer to the question with a valid methodof analysis than if we had used a �xed design. Overall the trial has established the principlethat the use of a gel pad in the operating theatre can reduce the risk of subsequent pressure soredevelopment. This result is consistent with the broader conclusions derived from a systematicreview of pressure sore prevention equipment [19]. Further work is now required on theidenti�cation of risk factors for pressure sore development in order that the design of futurestudies can be improved.The use of a sequential design in nursing research is feasible, although not entirely without
some practical di�culties.
ACKNOWLEDGEMENTS
We would like to acknowledge the input of the local data managers: Suzanne Coleman; Lisa Hope;Darren McVitie, Alison Briscoe, and senior trial co-ordinator Angela Phillips. Further we are indebtedto John Whitehead for his invaluable statistical advice throughout all stages of this trial, and to PatriciaShevlin for her thorough comments on earlier drafts of this paper. We are also grateful to Alice Hamarfor her administrative support throughout. This trial was funded by a grant from the Northern andYorkshire Regional Research Committee.
REFERENCES
1. Bridel J. Pressure sores and intra-operative risk. Nursing Standard 1992; 7(5):28–31.2. Bridel J. Assessing trolley and table products. Nursing Standard 1993; 7(21):11.3. Neander KD, Birken�eld R. Decubitus prophylaxis in the operating theatre? Journal of Tissue Viability 1991;1(3):71–74.
4. Bridel J. The epidemiology of pressure sores. Nursing Standard 1993; 7(42):25–30.5. Nixon J, McElvenny D, Mason S, et al. A sequential randomised controlled trial comparing a dry visco-elasticpolymer gel pad and standard operating table mattresses in the prevention of post-operative pressure sores.International Journal of Nursing Studies 1998; 35:193–203.
6. Torrance C. Pressure Sore: Aetiology; Treatment and Prevention. Croom Helm: London, 1983.7. Whitehead J. The Design and Analysis of Sequential Clinical Trials (revised 2nd edn). Ellis Horwood:Chichester, 1997.
8. Gendron F. Burns occurring during lengthy surgical procedures. Journal of Clinical Engineering 1980; 51(1):19–26.
9. Stotts NA. Predicting pressure ulcer development in surgical patients. Heart Lung 1988; 17(6) Part 1:641–647.
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400

3400 J. BROWN ET AL.
10. Kemp MG, Keighley JK, Smith DW et al. Factors which contribute to pressure sores in surgical patients.Research in Nursing and Health 1990; 13(5):293–301.
11. Bridel J. Pressure sore risk in operating theatres. Nursing Standard 1993; 7(32):4–10.12. Stallard N, Facy KM. Comparison of the spending function method and the Christmas tree correction for group
sequential trials. Journal of Biopharmaceutical Statistics 1996; 6(3):361–373.13. Brunier H, Whitehead J. Pest 3.0 Operating Manual. The University of Reading: Reading, 1993.14. Jennison C, Turnbull BW. Group-sequential analysis incorporating covariate information. Journal of the
American Statistical Association 1997; 92(440):1330–1341.15. Scharfstein DO, Tsiatis AA, Robins JM. Semiparametric e�ciency and its implication on the design and analysis
of group-sequential studies. Journal of the American Statistical Association 1997; 92(440):1342–1350.16. Whitehead J. Overrunning and underrunning in sequential clinical trials. Controlled Clinical Trials 1992; 13:
106–121.17. Hitch S. NHS Executive Nursing Directorate—Strategy for Major Clinical Guidelines—Prevention and
management of pressure sores: a literate review. Journal of Tissue Viability 1995; 5(1):3–24.18. Todd S, Whitehead J. Con�dence interval calculation for a sequential clinical trial of binary responses.
Biometrika 1997; 84(3):737–743.19. Cullum N, Deeks J, Fletcher A et al. The prevention and management of pressure sores. How e�ective are
pressure relieving interventions and risk assessment for the prevention and treatment of pressure sores? E�ectiveHealth Care 1995; 2(1):1–15.
Copyright ? 2000 John Wiley & Sons, Ltd. Statist. Med. 2000; 19:3389–3400