Embed Size (px)
Citation preview
Something Has To Change

1.Looking In
2. Looking Out
3. Looking At Theory
A Three-Strand Approach
Stress, burnout, depression, anxiety, compassion fatigue, secondary PTSD...
It is important to safeguard the health of those facing aggressive
outbursts on a daily basis.
The Psychology bit….
What is Attachment Theory?
Attachment/Trust/Resilience Cycle
Risk Factors
Patterns of Insecure Attachment
Associated Behaviours

'Evidence is accumulating that human beings
of all ages are happiest and able to deploy
their talents to best advantage when they are
confident that, standing behind them, there
are one or more trusted persons who will
come to their aid should difficulties arise. The
person trusted, also known as an attachment
figure, can be considered as providing his or
her companion with a secure base from which
to operate.' (Bowlby, 1979)
ATTACHMENT THEORY
John Bowlby ‘The Father of Attachment Theory’
Secure Base

The cumulative impact of events in the child’s life
may have led him to:
feel, ‘not free to focus his attention on
things other than survival,’
(Van Gulden and Bartels-Rabb, 1993).
feel safest when he exercises control over every
situation
feel unable to trust adults to provide for his needs,
even at the most basic level (Maslow, 1970)
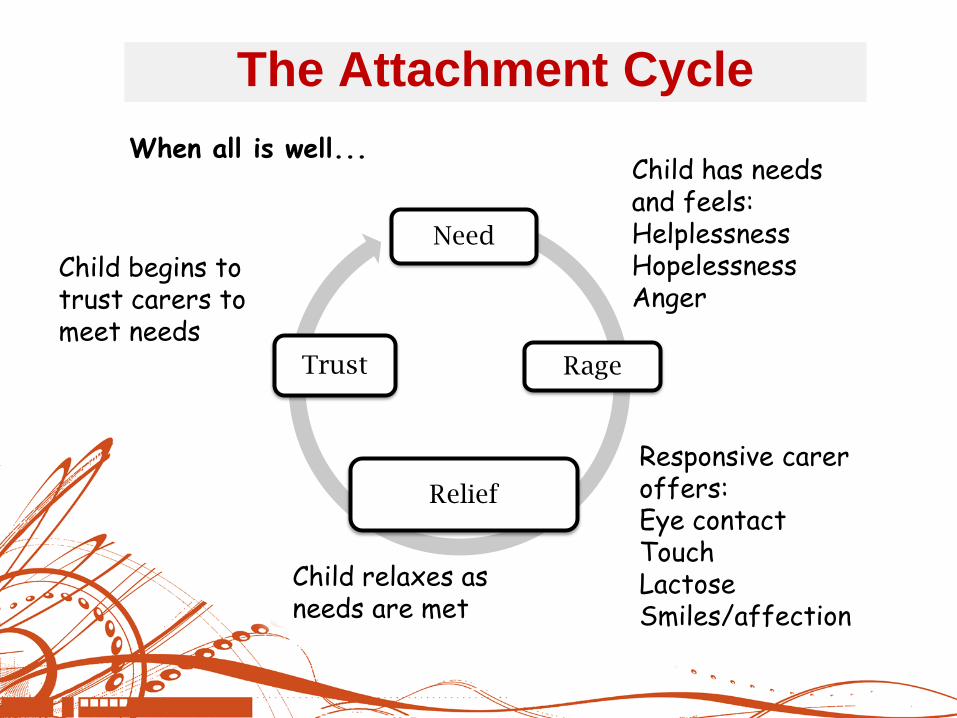
The Attachment Cycle
Child begins to trust carers to meet needs
Child has needs and feels: Helplessness
Hopelessness
Anger
Responsive carer offers: Eye contact Touch Lactose Smiles/affection
Child relaxes as needs are met
When all is well...
Need
Rage
Relief
Trust

Child has needs and feels: Helplessness
Hopelessness
Anger
Need
Rage
No Relief/unreliable relief
Unable to trust
Unresponsive or unreliable carer offers: Poor eye contact Touch without affection Anger/irritation
Child either... Withdraws becomes over compliant or increases rage ...as needs are not met
Child develops unhealthy survival strategies in attempt to make carer meet his needs
INTERRUPTION OF THE ATTACHMENT
CYCLE - 1
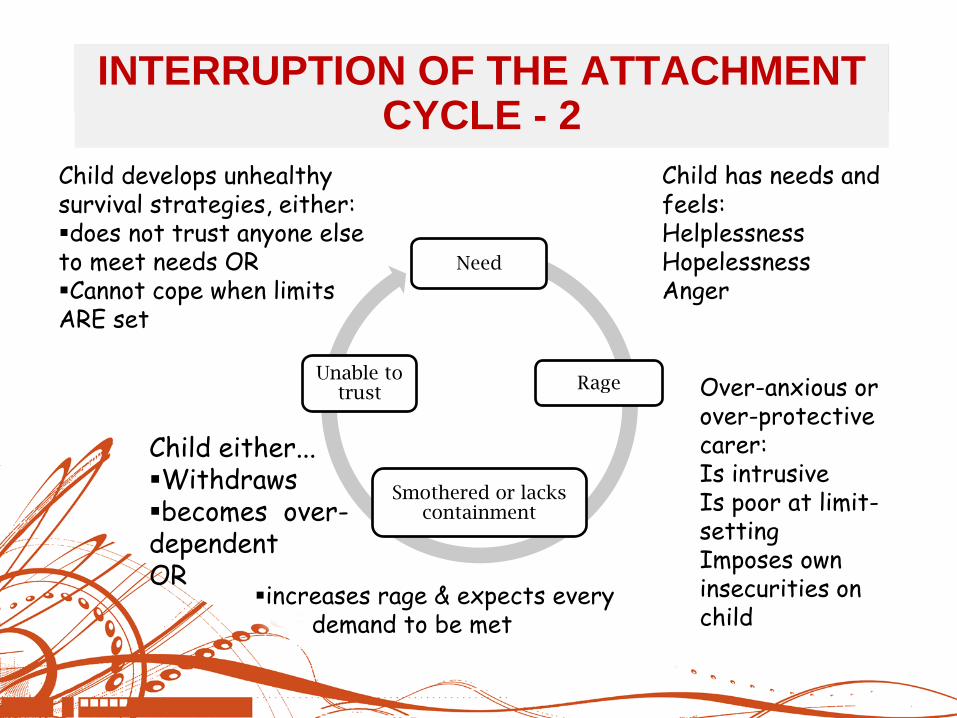
Child has needs and feels: Helplessness
Hopelessness
Anger
Need
Rage
Smothered or lacks containment
Unable to trust Over-anxious or
over-protective carer: Is intrusive Is poor at limit-setting Imposes own insecurities on child
Child either... Withdraws becomes over-dependent OR
Child develops unhealthy survival strategies, either: does not trust anyone else to meet needs OR Cannot cope when limits ARE set
INTERRUPTION OF THE ATTACHMENT CYCLE INTERRUPTION OF THE ATTACHMENT CYCLE - 2
increases rage & expects every demand to be met
Pre-birth stress, eg. mother’s self-harm or
domestic violence
Alcohol and/or drug taking during pregnancy
Parental illness before/after birth
Ante- or post-natal depression
Being a premature baby – separation in incubator
Medical complications - in the womb, at birth,
during the early years
Illness/Bereavements in the family
When things go wrong...Risk Factors
DON’T GET SUCKED INTO A BLAME GAME!
The baby having a disability
Neglect and/or abandonment
Emotional, sexual and physical abuse, domestic
violence
Home and family instability/breakdown
Poverty
Mental health difficulties in caregivers
Multiple home and school placements during the
child’s early years (based on Bomber, 2007)
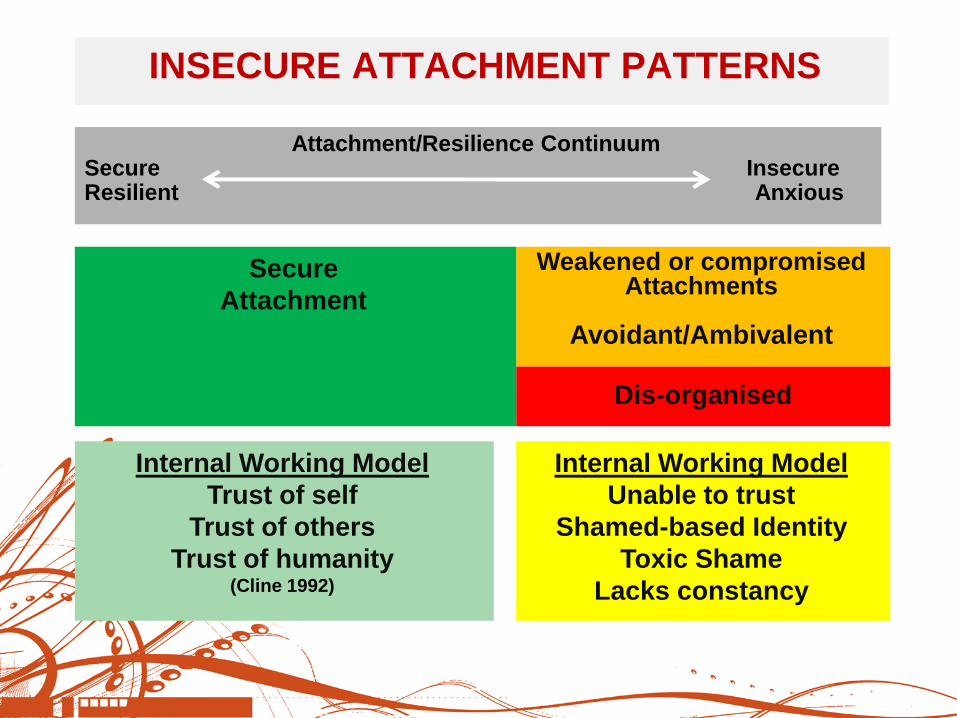
INSECURE ATTACHMENT PATTERNS
Dis-organised
Attachment/Resilience Continuum Secure Insecure Resilient Anxious
Weakened or compromised Attachments
Avoidant/Ambivalent
Secure
Attachment
Internal Working Model
Trust of self
Trust of others
Trust of humanity (Cline 1992)
Internal Working Model
Unable to trust
Shamed-based Identity
Toxic Shame
Lacks constancy
‘The fifth edition of the Diagnostic and Statistical Manual
of Mental Disorders (DSM-5) updates disorder criteria to
more precisely capture the experiences and symptoms
of children:’ (2013, American Psychiatric Association)
CHANGES IN DSM-5
Reactive Attachment Disorder is now
divided into:
Reactive Attachment Disorder (RAD)
Disinhibited Social Engagement Disorder
(DSED)
‘Clinicians and families often were frustrated that DSM-
IV did not define or describe some of the clinically
significant behaviours and symptoms they observed in
children.’ (2013, DSM-5 and Diagnoses for Children, American Psychiatric Association)
Social Communication Disorder (SCD)
Disruptive Mood Dysregulation Disorder (DMDD)
Post Traumatic Stress Disorder (PTSD) Pre-School Subtype
Separation Anxiety Disorder
Oppositional Defiant Disorder (ODD)
Conduct disorder
Intermittent Explosive Disorder
Attention Deficit/Hyperactivity Disorder (ADHD)
etc, etc, etc….
DIAGNOSIS – LEAVE IT TO THE PROFESSIONALS!
The Brain Science Bit….
The Brain in 3 Parts
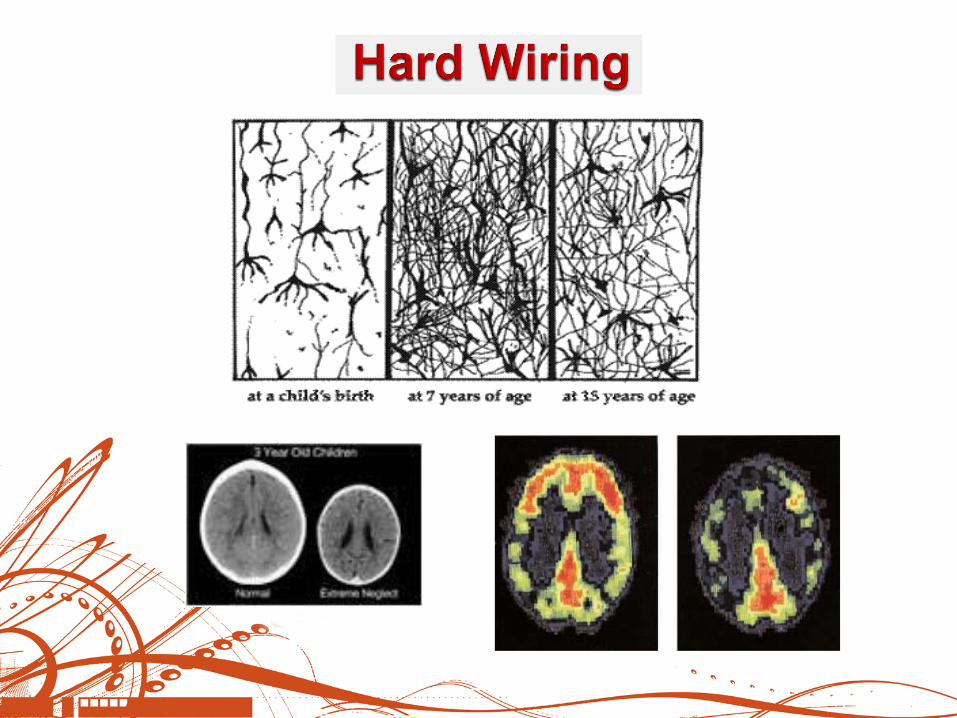
Hardwiring
Startle Reaction
New Neural Pathways = Change in
Behaviour
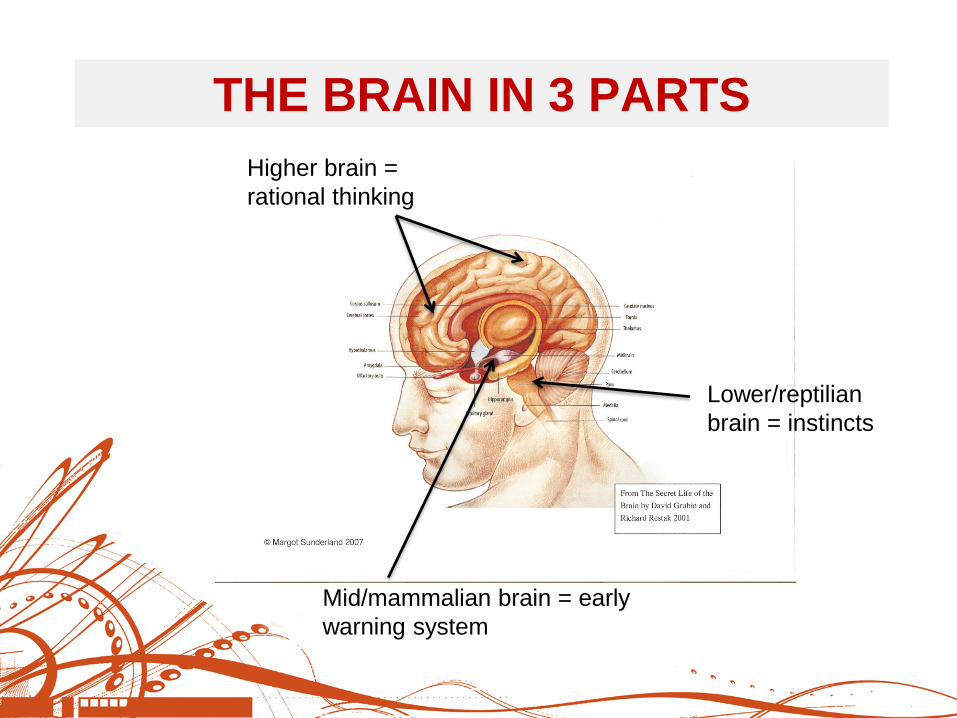
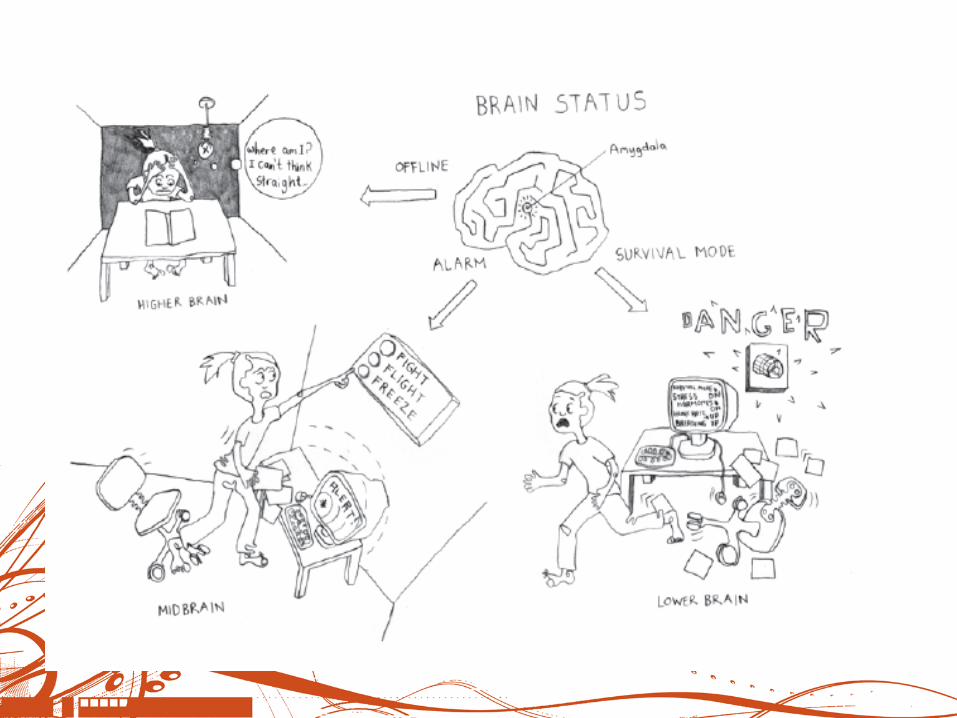
THE BRAIN IN 3 PARTS
Higher brain =
rational thinking
Lower/reptilian
brain = instincts
Mid/mammalian brain = early
warning system
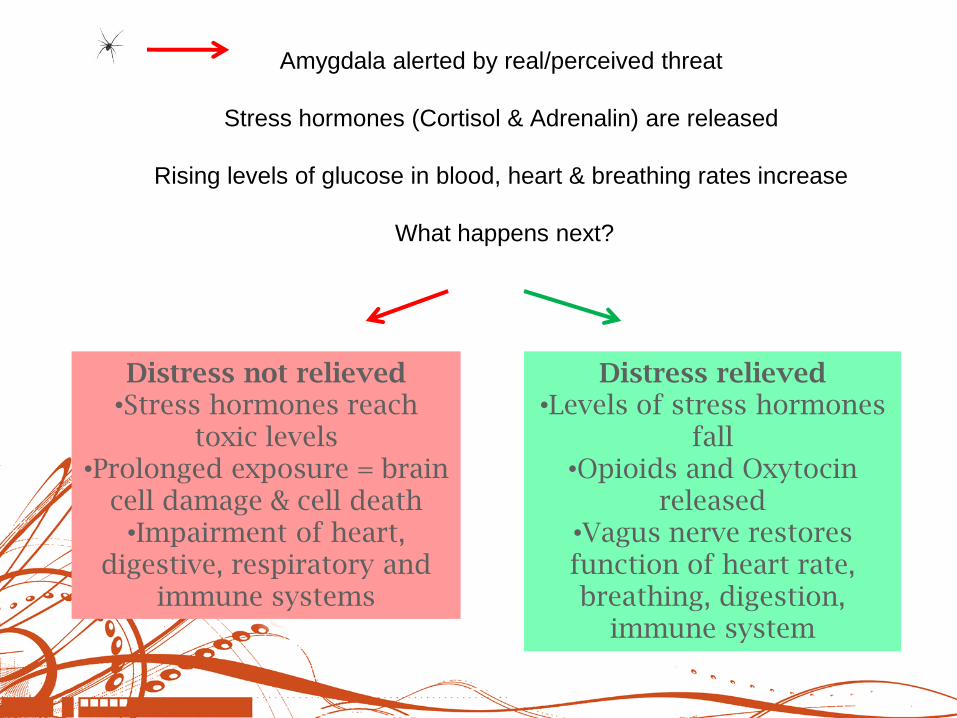
Amygdala alerted by real/perceived threat
Stress hormones (Cortisol & Adrenalin) are released
Rising levels of glucose in blood, heart & breathing rates increase
What happens next?
Distress not relieved •Stress hormones reach
toxic levels •Prolonged exposure = brain
cell damage & cell death •Impairment of heart,
digestive, respiratory and immune systems
Distress relieved •Levels of stress hormones
fall •Opioids and Oxytocin
released •Vagus nerve restores function of heart rate, breathing, digestion,
immune system
The Cornfield Model
The Staircase Model
‘Think Toddler’
First, Calm the Body
Behaviour ‘Management’ Cycles
New
neural
pathways
=
changes
in
behaviour
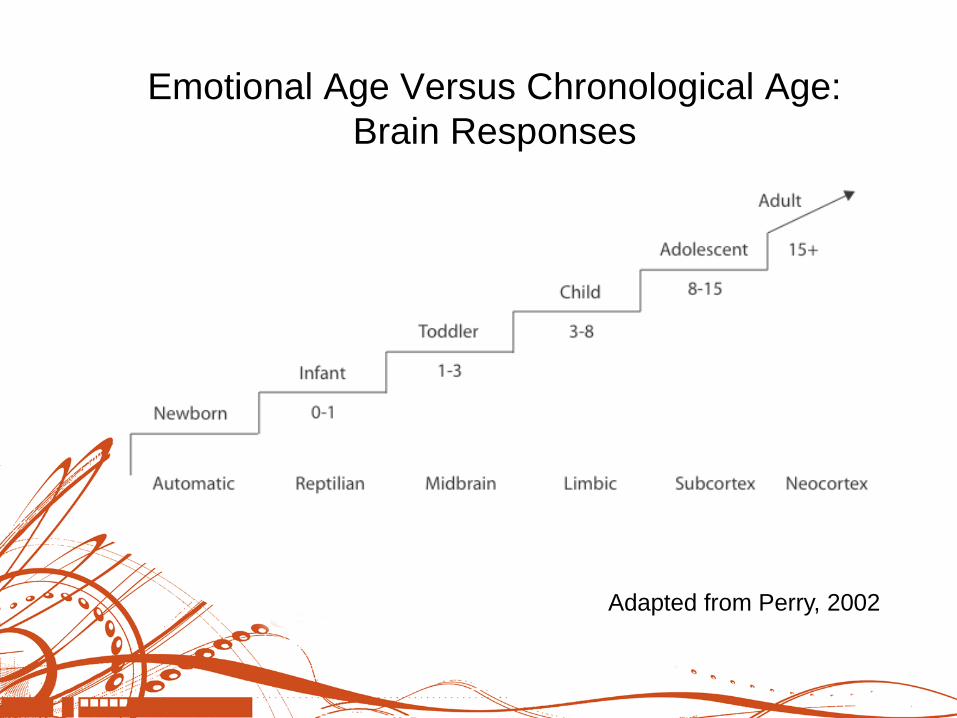
Emotional Age Versus Chronological Age:
Brain Responses
Adapted from Perry, 2002
‘Think Toddler’
(Based on Archer: 2002)
First, calm the body
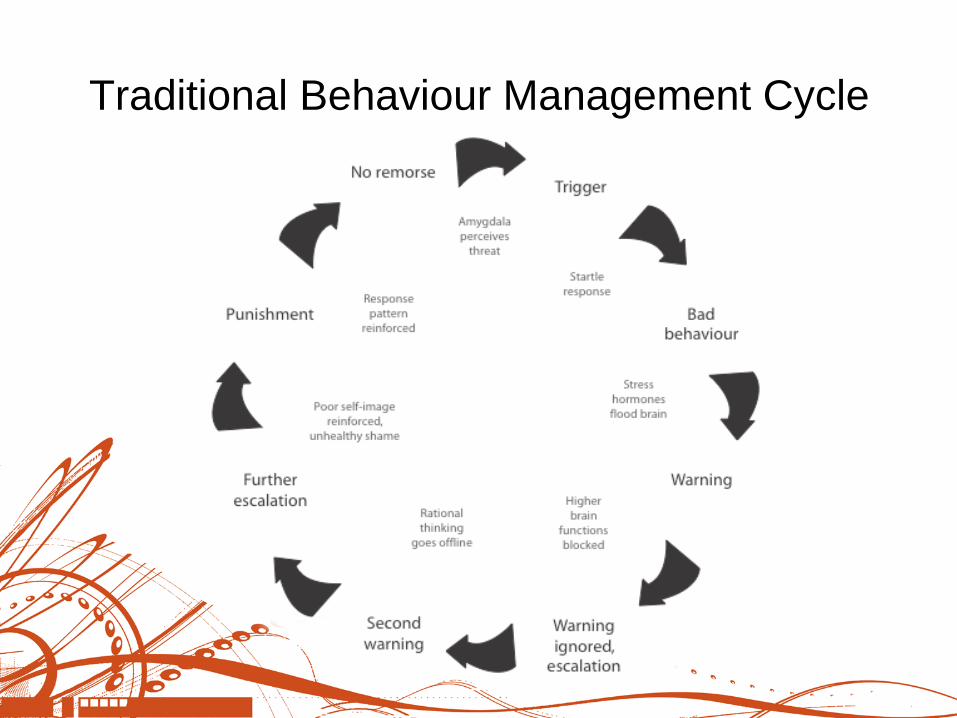
Traditional Behaviour Management Cycle
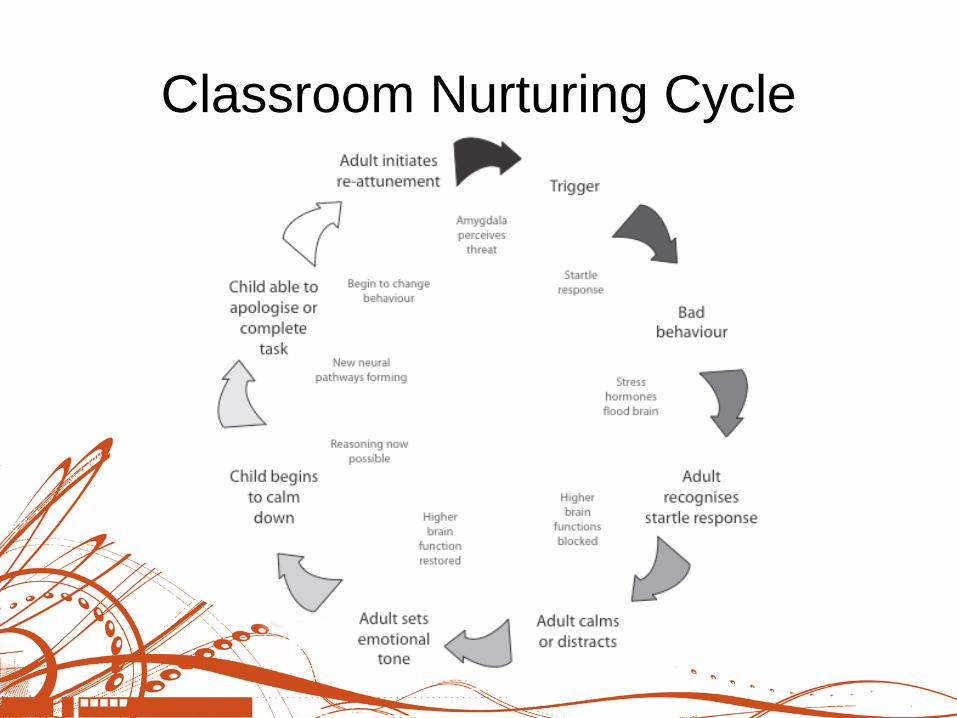
Classroom Nurturing Cycle
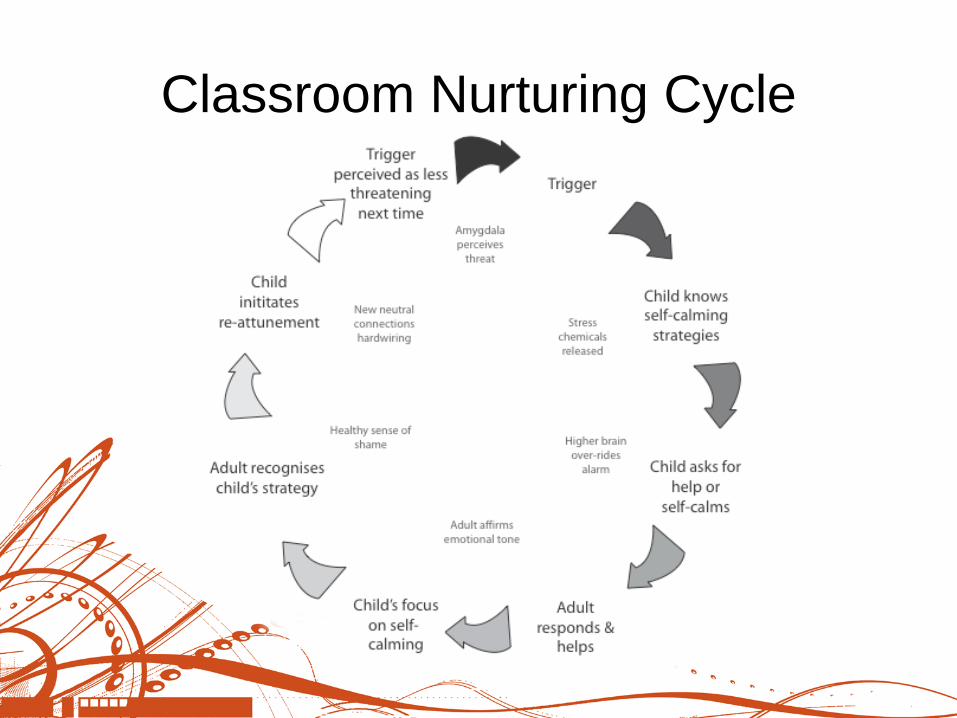
Classroom Nurturing Cycle

Held in Mind
Routines and Relaxation
Permission to Fail
Rewards & Sanctions
Behaviour ‘Management’ Cycles
Observing: ABC & the three strand
approach

Held in Mind
‘The child exists for the teacher when
he is not immediately with her. The
teacher conveys this sense... by
perceiving a need and offering
something to him before he had
directly indicated that he wanted it.’
(Pawl, 2006)
Change and uncertainty cause
anxiety.
‘Uncertainty can be felt as
overwhelming anxiety, and
tolerating the uncertainty of not
knowing becomes an unbearable
threat.’
(Geddes, 2007)
Routines and Relaxation
Permission to Fail
‘The emotion of shame plays an important
role in healthy identity formation. In its
healthiest form, shame teaches the child
that he is human, with limitations and
fallibility. Taken to an extreme, however,
shame can lead a child to feel flawed as a
human being, even to the point of being
somehow less than human.’
(Van Gulden & Bartels-Rabb, 1993)
‘Empathy will support the child to
experience discipline for its intended
purpose rather than as abuse or
rejection.’ (Bombèr, 2007)
‘We may feel that praising a child will help
to make him feel more positive about
himself, while the child may view praise
as a threat to his sense of self.’
(Family Futures, 2008)
Rewards & Sanctions
Stress, burnout, depression, anxiety, compassion fatigue, secondary PTSD...
It is important to safeguard the health of those facing aggressive
outbursts on a daily basis.