Embed Size (px)
Citation preview

Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
Sonographer Ergonomics: Assessment and workplace redesign
Anchal Patil
Mechanical Engineering Department
Indian Institute of Technology Delhi
Delhi India
P V M Rao
Mechanical Engineering Department
Indian Institute of Technology Delhi
Delhi India
Abstract— Work related risk associated with Medical personnel reported in previous studies several times. A large no of
sonographers were reported suffering work related musculoskeletal disorder (WRMSD). Awkward postures for performing scans,
High work load, less frequent relaxation times, ignorance and lack of initiatives from both management and individuals add in the
problems substantially. This paper provides a comprehensive study of sonographer’s ergonomics, first accessing the workplace using
Digital Human Modelling (DHM) then proposing a noble methodology to optimally redesign workplace, fusing qualitative and
quantitative ergonomic fitness criteria. Fusion of Microsoft Kinect and Inertial sensor performed for obtaining workplace
parameters and DHM simulation were utilized for determining the optimal value of workplace parameters.
Keywords— Sonographer ergonomics, DHM, Kinect, Optimization.
I. INTRODUCTION
Sonographers work related musculoskeletal disorder reported in previous studies considerably. A large no of questioner based work mapped the injury profile of sonographers, among these studies approximately 65% - 96% sonographers reported suffering from some form of work related injuries[1][2]. These injuries includes the mild pain in joints, discomforts in muscles and tendons, swelling, loss of sensation, clumsiness etc. Some body parts such as neck, shoulder, wrist, upper back and arm are more prone to injury due to long duration scanning[3]. Main cause of these injuries are unfavourable postures, pinch grip, repetitive motion, forceful exertion, sonographer rotation schedule etc.[4][5]. From economic perspective WRMSD in sonographers results in huge financially losses, increased absences and negative emotional impact [6] And must be eradicated with an easily adoptable solution.
To counter the hazardous ergonomics of sonographers three types of approaches are identified - engineering intervention, administrative intervention and personal/behavioural intervention. Few engineering intervention been identified in the literature mostly in trial period proposing arm support system[7], articulating arm [8], ultrasound system[9], probe supporting robot [10] and voice scan system [11]. These solutions are effective but market adoption will not likely to happen anytime soon. Administrative interventions constitute small modules of ergonomic training/workshops, optimal scheduling etc. which needs awareness and coordination among healthcare units, manufacturing industries and sonographers.
Third and most easily adaptable, behavioural intervention for sonographers presented in few studies. Workplace redesign for sonographers have been proposed in [12] for diagnosis animals. Most recommendation made on the positioning of animals and equipment subjectively, [13] described importance of proper adjustment between equipment’s, patient and sonographer and provides a set of guidelines to prevent WRMSD, [14] recommends the individual sonographer approach to be more effective, [15] organized a workshop sharing various sonographer practices to deals with WRMD supporting individually customized workplace practices, [16] Proposed alexander technique to make aware the individuals for better work practice, [17] Concluded prevention to be the best cure for WRMSD. Above mentioned studies mostly focussed towards individual awareness and weight the individual for a better work practices but lacks a systemic approach towards individual intervention. Individual intervention is a multifactorial approach and requires individually customized solutions.
Most ultrasound machines available in the markets are equipped with customization ability but customization performed by user based on gut feeling which could leads to comfortable but hazardous postures. A systematic quantitative approach is lacking where a user can customized the workplace considering patient size, types of diagnosis, user’s anthropometry and room layout.
Therefore, the aim of this study was to access the sonographer’s ergonomics and develop a methodology for individual intervention. Particularly this study aims to optimize the sonographer’s workplace using weighted product model with DHM in
3403© IEOM Society International
Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
order to decrease the rapid upper limb assessment (RULA) score and lower back (L4/L5) compression force. The advantage of proposed methodology is discussed in terms of adaptability and feasibility in later section.
II. METHODOLOGY
The proposed approach takes place in following order –
(1) Ergonomics assessment of sonographer’s workplace using DHM. Most commonly performed diagnosis are categorisedinto 4 types depends upon the targeting patient body parts since for different body parts different postures are required.
(2) A new approach to redesign the workplace is proposed here. Proposed algorithm is generic that can be applied to otherproblems as well. Quantitative and qualitative criteria are considered for a holistic approach.
(3) Abdominal and carotid diagnosis, two most severe and frequent diagnosis obtained is targeted using proposed algorithm.
A. Ergonomics assessment of sonographers
Three method of ergonomic assessment presents in most literatures – survey questioners, DHM simulation and sensor basedassessment. Sonographer’s assessment had been carried out using sensors (electromyography and joint angle meter, motion capture system and dynamometer) in [18] [19] [20] , deriving joint angles and stress data.
Only occurrence of DHM simulation applied on sonographers found in [21] assessing abdominal ultrasound.
We considered 4 types of diagnosis. Since diagnosis of different body parts needs adoption of particular types of postures, hence categorisation of diagnosis is necessary for an accurate and comprehensive assessment. DHM performed on following diagnosis-
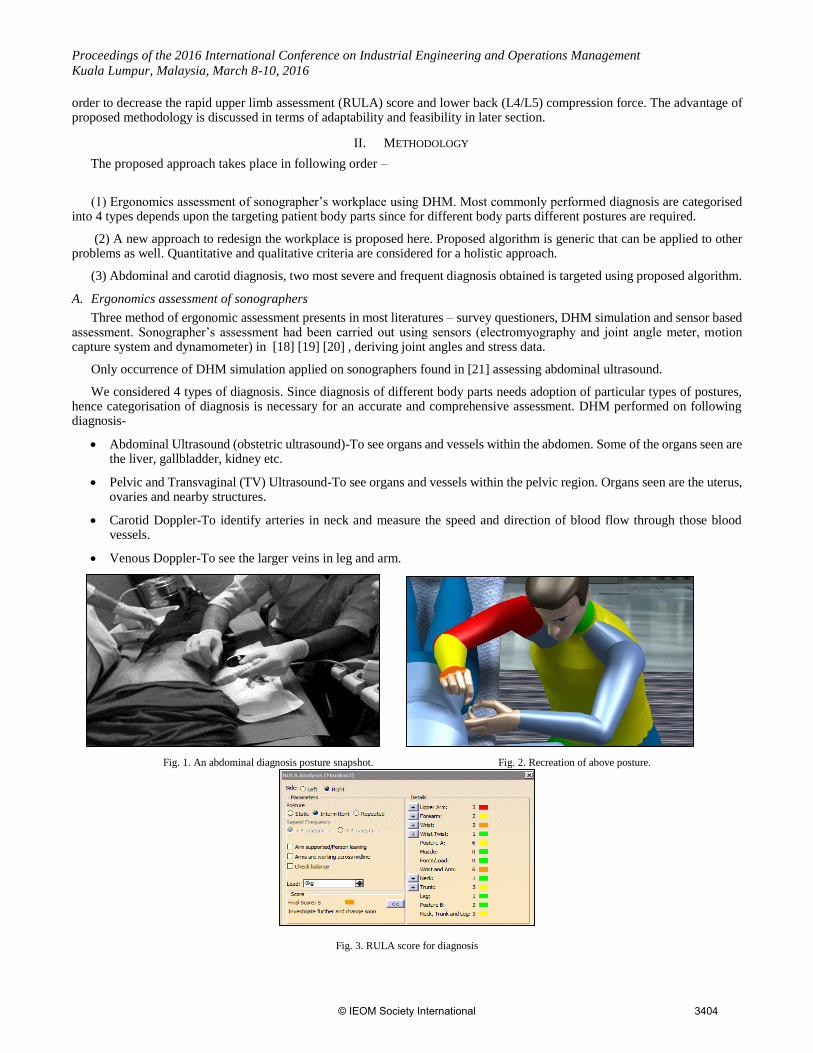
Abdominal Ultrasound (obstetric ultrasound)-To see organs and vessels within the abdomen. Some of the organs seen arethe liver, gallbladder, kidney etc.
Pelvic and Transvaginal (TV) Ultrasound-To see organs and vessels within the pelvic region. Organs seen are the uterus,ovaries and nearby structures.
Carotid Doppler-To identify arteries in neck and measure the speed and direction of blood flow through those bloodvessels.
Venous Doppler-To see the larger veins in leg and arm.
Fig. 1. An abdominal diagnosis posture snapshot. Fig. 2. Recreation of above posture.
Fig. 3. RULA score for diagnosis
3404© IEOM Society International

Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
A. 1. Results
RULA is a proven technique to evaluate the posture for neck, trunk and upper extremity. RULA results for current studies are summarized in table 2. Rating of 1 and 2 in RULA indicate accepted posture (green), 3 and 4 indicate further change(yellow), 5 and 6 indicate, the soon change required(orange) and 7 indicate immediate change. No one posture manages to score 1 or 2.
TABLE I. RULA Evaluation results (average and variance)
Types of Diagnosis Average Variance
Abdominal
Pelvic and TV
Carotid Venous
4.5
4.9
6.6 4.6
1.5
0.72 0.33
1.05
B. Ergonomics Redesign Methodology
This section describes an interactive optimization technique to optimize the sonographer workplace. Proposed methodology is inspired from [22] who used virtual manufacturing (VM) and Design of experiment (DOE) to optimized a fruit packing workstation and [23] proposing Interactive evolutionary computation (IEC) for ergonomic optimization.
We present a novel methodology to redesign the workstation. Proposed methodology uses fusion of Microsoft Kinect and inertial sensors to capture the motion and workplace information. Data is being imported into DHM. Weighted product model is applied to optimize the workstation design variables for DHM quantitative assessment (RULA analysis and Lower back analysis). Method incorporates Qualitative inputs from both designer & sonographer.
Fig. 4. Flow Chart for Proposed Redesign Methodology
Start with a real world solution
Modelling in Virtual world
Optimization DHM
Evaluation: Qualitative
Quantitative fitness
MS Kinect
Inertial Sensor
User
Designer
Stop Criteria
Yes
Validation: DHM
END
No
Real world
3405© IEOM Society International

Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
B. 1. Formulation
Formulation of proposed methodology is as follows –
Objective Functions:
Fitness function consists of the multiple objectives in terms of quantitative and qualitative criteria’s. Objective is to minimize
the fitness function. We considered only two DHM quantitative functions considering requirements of sonographer’s problem
however more function may be added for different cases.
Performance measures are –
DHM Quantitative assessments Qualitative assessments
min 𝐹 = [𝑓1
𝑓2]
𝐹4(𝑐, 𝑙) = 𝑓5(𝑐, 𝑙)
𝐹5(𝑟, 𝑣) = 𝑓5(𝑟, 𝑣)
𝒇𝟏 ∑ 𝑝𝑖 ∗ 𝑡𝑖/𝑇𝑡𝑎𝑠𝑘𝑚𝑖=1
This is the time weighted average of the postural score obtained from DHM. Objective is to minimize the hazardous postures
duration).
𝑝𝑖 = 𝑟𝑢𝑙𝑎 𝑠𝑐𝑜𝑟𝑒 , 𝑇𝑡𝑎𝑠𝑘 = 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑜𝑛 𝑡𝑖𝑚𝑒
𝑡𝑖 = 𝑡𝑖𝑚𝑒 𝑡𝑜 𝑝𝑒𝑟𝑓𝑜𝑟𝑚 𝑒𝑎𝑐ℎ 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑜𝑛
𝒇𝟐=(∑ 𝑒𝑖∗𝑡𝑖)/𝑇𝑡𝑎𝑠𝑘𝑚𝑖=1 (2)
This is the Lower back analysis results
𝑒𝑖 = 𝑐𝑜𝑚𝑝𝑟𝑒𝑠𝑠𝑖𝑜𝑛 𝑓𝑜𝑟𝑐𝑒
f4(𝑐, 𝑙) = User’s qualitative assessment rating (from 0-1 denoting comfort and liking) [23].
f5(𝑟, 𝑣) = User reachability and visibility assessment from DHM (from 0-1).
Normalization:
Each quantitative objective function is normalized using upper-lower bound transformation.
𝒇𝟏𝒏 =
𝑓1′−𝑓1
1(𝑓1ℎ−𝑓1
𝑙) (3)
𝒇𝟏′ = 𝑓1
ℎ + 0.1(𝑓1ℎ − 𝑓1
𝑙) (4)
𝑓1ℎ = 𝑢𝑝𝑝𝑒𝑟 𝑙𝑖𝑚𝑖𝑡 𝑎𝑛𝑑 𝑓1
𝑙 = 𝑙𝑜𝑤𝑒𝑟 𝑙𝑖𝑚𝑖𝑡
Fitness Function:
Fitness function is derived using weighted product of 4 objective functions. Consideration of relative importance of
objective function is insured by subjectively assignment.
𝑭𝒔 = (∏ 𝑑𝑠𝑝𝑟𝑣4
𝑝=1 )1/∑ 𝑟𝑣 (5)
Solution sets s=1………K.
𝑟𝑣 = 𝑟𝑒𝑙𝑎𝑡𝑖𝑣𝑒 𝑖𝑚𝑝𝑜𝑟𝑡𝑎𝑛𝑐𝑒 𝑜𝑓 𝑒𝑎𝑐ℎ 𝑝𝑒𝑟𝑓𝑜𝑟𝑚𝑎𝑛𝑐𝑒 𝑚𝑒𝑎𝑠𝑢𝑟𝑒
3406© IEOM Society International
Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
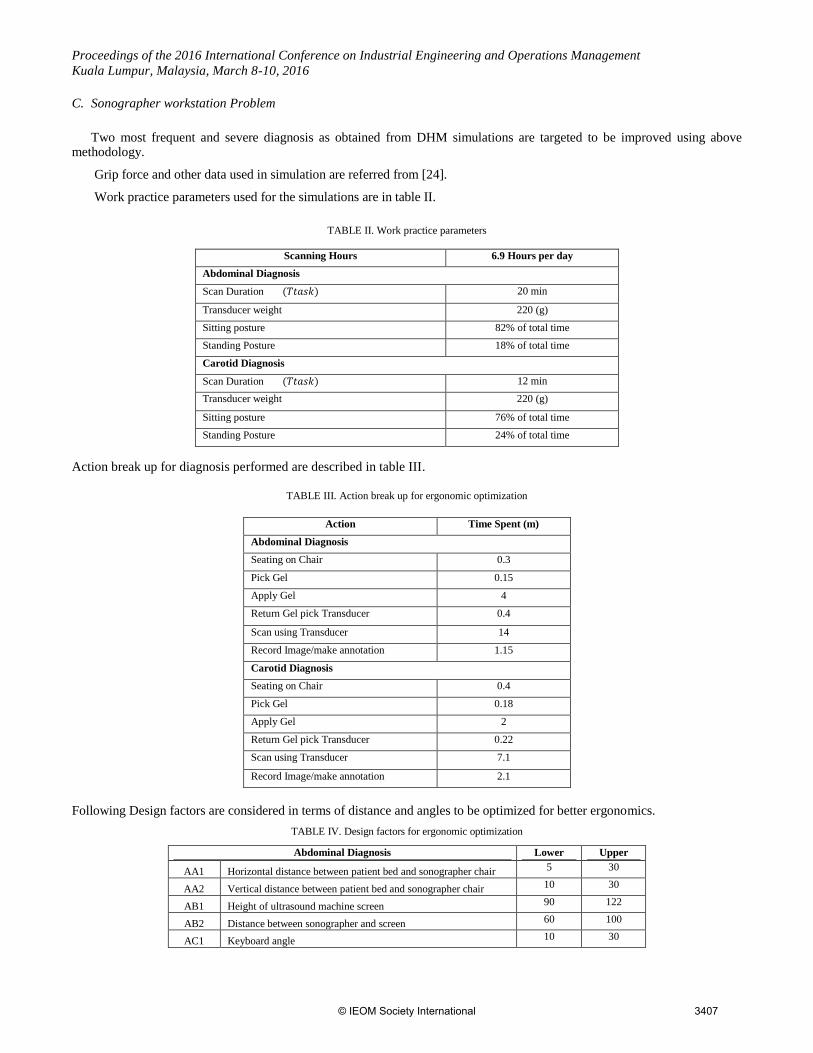
C. Sonographer workstation Problem
Two most frequent and severe diagnosis as obtained from DHM simulations are targeted to be improved using abovemethodology.
Grip force and other data used in simulation are referred from [24].
Work practice parameters used for the simulations are in table II.
TABLE II. Work practice parameters
Scanning Hours 6.9 Hours per day
Abdominal Diagnosis
Scan Duration (𝑇𝑡𝑎𝑠𝑘) 20 min
Transducer weight 220 (g)
Sitting posture 82% of total time
Standing Posture 18% of total time
Carotid Diagnosis
Scan Duration (𝑇𝑡𝑎𝑠𝑘) 12 min
Transducer weight 220 (g)
Sitting posture 76% of total time
Standing Posture 24% of total time
Action break up for diagnosis performed are described in table III.
TABLE III. Action break up for ergonomic optimization
Action Time Spent (m)
Abdominal Diagnosis
Seating on Chair 0.3
Pick Gel 0.15
Apply Gel 4
Return Gel pick Transducer 0.4
Scan using Transducer 14
Record Image/make annotation 1.15
Carotid Diagnosis
Seating on Chair 0.4
Pick Gel 0.18
Apply Gel 2
Return Gel pick Transducer 0.22
Scan using Transducer 7.1
Record Image/make annotation 2.1
Following Design factors are considered in terms of distance and angles to be optimized for better ergonomics.
TABLE IV. Design factors for ergonomic optimization
Abdominal Diagnosis Lower Upper
AA1 Horizontal distance between patient bed and sonographer chair 5 30
AA2 Vertical distance between patient bed and sonographer chair 10 30
AB1 Height of ultrasound machine screen 90 122
AB2 Distance between sonographer and screen 60 100
AC1 Keyboard angle 10 30
3407© IEOM Society International
Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
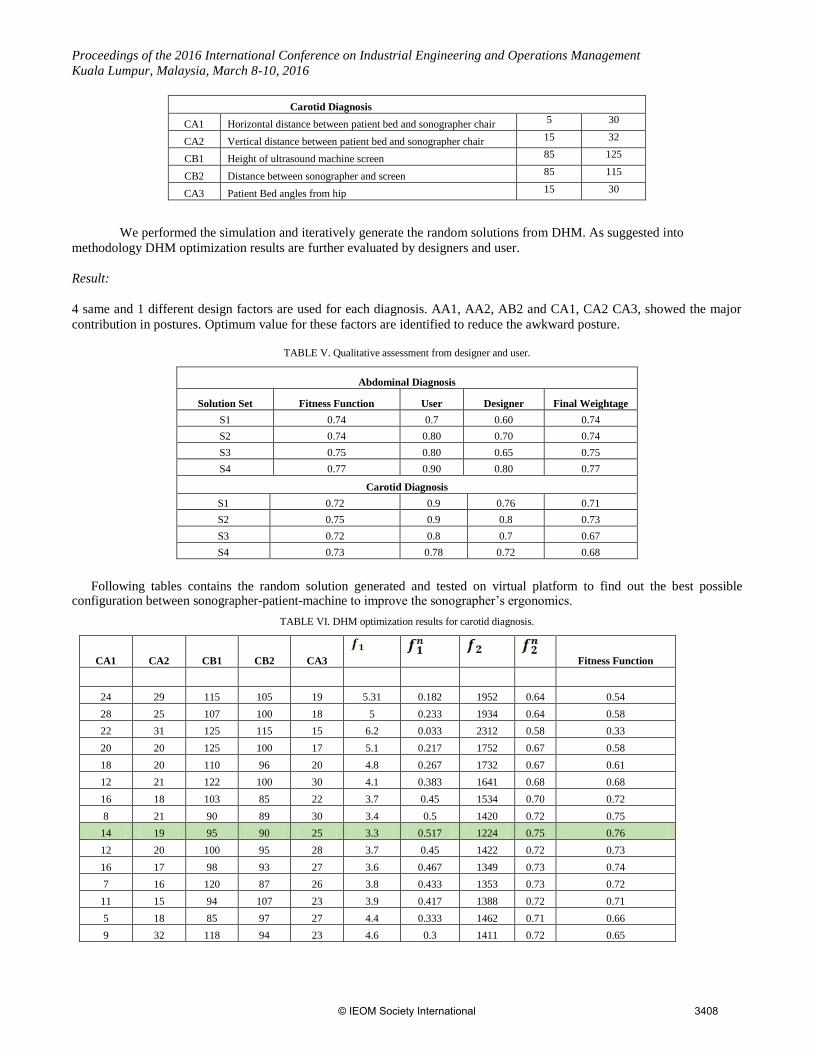
Carotid Diagnosis
CA1 Horizontal distance between patient bed and sonographer chair 5 30
CA2 Vertical distance between patient bed and sonographer chair 15 32
CB1 Height of ultrasound machine screen 85 125
CB2 Distance between sonographer and screen 85 115
CA3 Patient Bed angles from hip 15 30
We performed the simulation and iteratively generate the random solutions from DHM. As suggested into
methodology DHM optimization results are further evaluated by designers and user.
Result:
4 same and 1 different design factors are used for each diagnosis. AA1, AA2, AB2 and CA1, CA2 CA3, showed the major
contribution in postures. Optimum value for these factors are identified to reduce the awkward posture.
TABLE V. Qualitative assessment from designer and user.
Abdominal Diagnosis
Solution Set Fitness Function User Designer Final Weightage
S1 0.74 0.7 0.60 0.74
S2 0.74 0.80 0.70 0.74
S3 0.75 0.80 0.65 0.75
S4 0.77 0.90 0.80 0.77
Carotid Diagnosis
S1 0.72 0.9 0.76 0.71
S2 0.75 0.9 0.8 0.73
S3 0.72 0.8 0.7 0.67
S4 0.73 0.78 0.72 0.68
Following tables contains the random solution generated and tested on virtual platform to find out the best possible configuration between sonographer-patient-machine to improve the sonographer’s ergonomics.
TABLE VI. DHM optimization results for carotid diagnosis.
CA1 CA2 CB1 CB2 CA3
Fitness Function
24 29 115 105 19 5.31 0.182 1952 0.64 0.54
28 25 107 100 18 5 0.233 1934 0.64 0.58
22 31 125 115 15 6.2 0.033 2312 0.58 0.33
20 20 125 100 17 5.1 0.217 1752 0.67 0.58
18 20 110 96 20 4.8 0.267 1732 0.67 0.61
12 21 122 100 30 4.1 0.383 1641 0.68 0.68
16 18 103 85 22 3.7 0.45 1534 0.70 0.72
8 21 90 89 30 3.4 0.5 1420 0.72 0.75
14 19 95 90 25 3.3 0.517 1224 0.75 0.76
12 20 100 95 28 3.7 0.45 1422 0.72 0.73
16 17 98 93 27 3.6 0.467 1349 0.73 0.74
7 16 120 87 26 3.8 0.433 1353 0.73 0.72
11 15 94 107 23 3.9 0.417 1388 0.72 0.71
5 18 85 97 27 4.4 0.333 1462 0.71 0.66
9 32 118 94 23 4.6 0.3 1411 0.72 0.65
3408© IEOM Society International

Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
5 20 123 104 18 4.8 0.267 1480 0.71 0.62
10 21 98 86 16 4.3 0.35 1377 0.72 0.68
11 15 94 89 22 3.9 0.417 1458 0.71 0.71
9 16 88 98 19 4.2 0.367 1519 0.70 0.68
21 28 113 111 27 4.8 0.267 1674 0.68 0.62
30 32 125 115 30 6.3 0.017 2415 0.57 0.27
TABLE VI. DHM optimization results for abdominal diagnosis
AA1 AA2 AB1 AB2 AC1
Fitness Function
18 21 102 84 15 4.99 0.24 1569 0.69 0.60
28 25 120 84 15 4.5 0.32 1800 0.66 0.64
29 30 110 100 29 6 0.07 1753 0.67 0.41
18 21 118 84 30 5.3 0.18 1590 0.69 0.56
16 24 109 70 15 4.3 0.35 1676 0.68 0.66
13 21 118 100 24 3.9 0.42 1514 0.70 0.71
8 26 96 75 15 4.11 0.38 1591 0.69 0.68
11 21 11 75 30 3.58 0.47 1507 0.70 0.73
8 11 90 84 10 3.5 0.48 1504 0.70 0.74
8 21 99 84 18 3.8 0.43 1542 0.70 0.71
21 11 114 84 19 3.5 0.48 1431 0.72 0.74
18 21 121 60 15 3.4 0.50 1410 0.72 0.75
8 15 90 65 15 3.2 0.53 1320 0.73 0.77
8 10 97 75 30 4 0.40 1420 0.72 0.70
18 19 94 84 21 3.7 0.45 1435 0.71 0.72
24 11 103 60 10 4.1 0.38 1422 0.72 0.69
10 11 92 65 15 3.6 0.47 1503 0.70 0.73
17 11 116 75 28 4.2 0.37 1588 0.69 0.68
24 18 120 88 25 5.2 0.20 1632 0.69 0.57
30 30 122 100 30 6.2 0.03 1932 0.64 0.34
III. CONCLUSION
Ergonomic intervention strategies proposed had been tried for two cases and successfully provides a set of design variables to improve the sonographer ergonomics. A 50% percentile sonographer doing abdominal and carotid diagnosis can adopt these parameters to improve the ergonomics.
The work presented here is a small step towards integrating state of the art yet cheap motion capture system and virtual platform to cater the ergonomic issues and intervene at individual level.
IV. DISCUSSION
Used methodology successfully reduced the awkward posture to some extents however sometimes when grip force is too high, lower back objective function cannot be minimized. Also some awkward postures are still arriving for short durations. To overcome these shortcomings users mind propagate towards more innovative solutions. The method may be used as a systematic way to arrive towards product based solutions by exactly identifying the problematic behaviour.
Integration of DHM into Interactive evolutionary techniques could be a potential path for more optimal solutions. Interactive input from designers and sonographers can be reduced using neural networking. Also simulation time in DHM is fairly enough to prevent the quick adoption of method for every individual. However a database considering ergonomically optimized design variables for 5, 50, 95 percentile sonographer will be sufficient enough. Methodology needs to be followed for other diagnosis procedure as well with lesser no of assumptions.
A system comprising advanced artificial intelligence tools, motion capture hardware system such as Microsoft Kinect or Vicon and DHM tools such as Siemens Jack or Catia can comprehensively approve the ergonomics.
3409© IEOM Society International

Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
REFERENCES
[1] A. Schoenfeld, J. Goverman, D. M. Weiss, and I. Meizner, “Transducer user syndrome: an occupational hazard of the ultrasonographer.,”
Eur. J. Ultrasound, vol. 10, no. 1, pp. 41–5, Sep. 1999.
[2] E. Ransom, “THE CAUSES OF Musculoskeletal injury amongst sonographers,” no. June, 2002.
[3] J. P. Baker and C. T. Coffin, “The Importance of an Ergonomic Workstation to Practicing Sonographers,” J. Ultrasound Med., vol. 32,
no. 8, pp. 1363–1375, 2013.
[4] S. C. Roll, K. D. Evans, C. D. Hutmire, and J. P. Baker, “An analysis of occupational factors related to shoulder discomfort in diagnostic
medical sonographers and vascular technologists.,” Work, vol. 42, no. 3, pp. 355–65, Jan. 2012.
[5] C. T. Coffin, “Work-related musculoskeletal disorders in sonographers : a review of causes and types of injury and best practices for
reducing injury risk,” pp. 15–26, 2014.
[6] S. L. Murphey and C. T. Coffin, “Ergonomics and Sonographer Well-being in Practice,” Sound Ergon.
[7] C. T. Coffin, “The use of a vertical arm support device to reduce upper extremity muscle firing in sonographers.,” Work, vol. 42, no. 3,
pp. 367–71, Jan. 2012.
[8] R. Z. Radin Umar, C. Sommerich, K. Evans, S. Lavender, E. Sanders, W.-T. Yen, S. Joines, and S. Lamar, “Ergonomic Interventional
Design of an Articulating Arm for Echocardiography Application: Front-End Design and Pilot Study,” Proc. Hum. Factors Ergon. Soc.
Annu. Meet., vol. 55, no. 1, pp. 980–983, Sep. 2011.
[9] S. Park, J. Yim, and G. Lee, “Design of an ergonomic ultrasound system: accommodation of user anthropometrics.,” Work, vol. 41 Suppl
1, no. Supplement 1, pp. 2037–42, Jan. 2012.
[10] R. Nakadate, Y. Tokunaga, J. Solis, A. Takanishi, E. Minagawa, M. Sugawara, K. Niki, and A. Saito, “Development of robot assisted
measurement system for abdominal ultrasound diagnosis,” 2010 3rd IEEE RAS EMBS Int. Conf. Biomed. Robot. Biomechatronics,
BioRob 2010, pp. 367–372, 2010.
[11] K. L. Bravo, “The Potential Reduction in Musculoskeletal Injury in the Nonscanning Arm by Using VoiceScan Technology During
Sonographic Examinations,” J. Diagnostic Med. Sonogr., vol. 21, no. 4, pp. 304–308, 2005.
[12] K. Macdonald and P. Scott, “Scanning through the pain: ergonomic considerations for performing echocardiography of animals.,” J. Vet.
Cardiol., vol. 15, no. 1, pp. 57–63, Mar. 2013.
[13] O. Sonography, T. Rousseau, N. Mottet, G. Mace, C. Franceschini, and P. Sagot, “Practice Guidelines for Prevention of Musculoskeletal
Disorders in,” pp. 157–164, 2013.
[14] V. Gibbs and H. Edwards, “An investigation of sonographers unaffected by work-related musculoskeletal disorders,” Ultrasound, vol.
20, no. 3, pp. 149–154, Aug. 2012.
[15] V. Gibbs and P. Young, “A study of the experiences of participants following attendance at a workshop on methods to prevent or reduce
work-related musculoskeletal disorders amongst sonographers,” Radiography, vol. 17, no. 3, pp. 223–229, Aug. 2011.
[16] V. Gibbs and P. Young, “Work-related Musculoskeletal Disorders in Sonography and the Alexander Technique,” Ultrasound, vol. 16,
no. 4, pp. 213–219, Nov. 2008.
[17] B. Morton and P. Delf, “The prevalence and causes of MSI amongst sonographers,” Radiography, vol. 14, no. 3, pp. 195–200, Aug.
2008.
[18] J. Pocratsky, B. Ashby, and J. Beasley, “Upper Extremity Kinematics in Sonographers During Kidney Scanning,” J. Diagnostic Med.
Sonogr., vol. 30, no. 2, pp. 67–76, Dec. 2013.
[19] H. Suzuki, T. Saito, Y. Shimomura, and T. Katsuura, “Effects of horizontal console position on operator muscular stress during abdominal
ultrasonic diagnosis,” J. Med. Ultrason., vol. 41, no. 2, pp. 155–162, 2013.
[20] E. J. Bastian, J. K. Kits, J. D. Weaver, J. R. Stevenson, L. Carlton, S. A. Raaymakers, and J. Vanderpoel, “Effects of Work Experience,
Patient Size, and Hand Preference on the Performance of Sonography Studies,” J. Diagnostic Med. Sonogr., vol. 25, no. 1, pp. 25–37,
Jan. 2009.
[21] E. Bertoloni, M. Fenaroli, F. Marciano, D. Rossi, and P. Cabassa, “Sonographers ’ Workplace Improvement : Ergonomics Evaluation
using Modelling and Simulation Software,” pp. 603–612, 2012.
[22] I. Ben-Gal and J. Bukchin, “The ergonomic design of workstations using virtual manufacturing and response surface methodology,” IIE
Trans., vol. 34, pp. 375–391, 2002.
[23] A. M. Brintrup, J. Ramsden, H. Takagi, and A. Tiwari, “Ergonomic chair design by fusing qualitative and quantitative criteria using
interactive genetic algorithms,” IEEE Trans. Evol. Comput., vol. 12, no. 3, pp. 343–354, 2008.
[24] J. Village and C. Trask, “Ergonomic analysis of postural and muscular loads to diagnostic sonographers,” Int. J. Ind. Ergon., vol. 37, no.9–10, pp. 781–789, Sep. 2007.
BIOGRAPHY
Anchal Patil graduated from Indian Institute of Tecnology Delhi India. He earned Master of Technology in industrial engineering from IIT
Delhi and Bachelor of Technology in industrial engineering and management from National Institute of Technology Kuruskhetra. His area
of research interests are biomechnaics and motor control, ergonomics, Operation Research and advanced optimization techniques.
P V M Rao is an Professor in Mechanical Engineering Department at Indian Institute of Technology Delhi India. He earned B.E. from college
of engineering, Osmania University, M.Tech from Indian Institute of Technology BHU and Ph.D. from Indian Institute of Technology
3410© IEOM Society International
Proceedings of the 2016 International Conference on Industrial Engineering and Operations Management
Kuala Lumpur, Malaysia, March 8-10, 2016
Kanpur. He was visiting faculty at Stanford University USA and guest researcher for Nation Institue of Standards and Technology. He is
actively involoved in assitive technology and biomedical device development.
3411© IEOM Society International