Embed Size (px)
Citation preview
Sonographic Diagnosis of a Medial TalarAvulsion Fracture
Chia-Yu Hsu, MD,1 Yi-Pin Chiang, MD,1 Cheng-Tsung Liao, MD,2 Yu-Chung Hong, MD3
1 Department of Rehabilitation Medicine, Mackay Memorial Hospital, Taipei, Taiwan2 Department of Rehabilitation Medicine, Chiuan-Shiang Rehabilitation Clinic, Sansia, New Taipei City, Taiwan3 Department of Radiology, Mackay Memorial Hospital, Taipei, Taiwan
Received 8 January 2012; accepted 13 July 2012
ABSTRACT: Occult talus fractures can be easily mis-
diagnosed as simple ankle sprains, resulting in pain-
ful nonunion, arthrosis, avascular necrosis, and long-
term disability. We present a case of ankle injury with
medial talar fracture that was negative on plain radi-
ography but was diagnosed with sonography. Sonog-
raphy is a valuable tool in screening ankle sprains
and may assist clinicians in diagnosing the nature of
ankle injury, thus guiding the most appropriate thera-
peutic strategy. VVC 2012 Wiley Periodicals, Inc. J Clin
Ultrasound 00:000–000, 2012; Published online in
Wiley Online Library (wileyonlinelibrary.com). DOI:
10.1002/jcu.21977
Keywords: talus; fracture; ultrasonography; musculo-
skeletal system; foot
The talus is the second largest bone of thefoot.1 Anatomically, the talus is divided into
the head, neck, and body. It articulates proxi-mally with the tibia and fibula (ankle joint), dis-tally with the navicular bone (talonavicularjoint), and inferiorly with the calcaneus (anterior,middle, and posterior talocalcaneal joints). Thesearticulations are responsible for over 90% of themotion that occurs in the foot and ankle.2
Fractures of the talus are the second mostcommon site of all tarsal bone fractures.2 Frac-tures of the talus may occur at the neck,2–5
body,6–8 lateral process,1,9 talar dome,10 and pos-terior process.11,12 Fractures of the medial tuber-cle of the posterior process are relatively rare.10
The proposed injury mechanism is a sudden forceapplied to the foot in a position of combined dorsi-flexion and pronation.13 This force may lead to
avulsion of the medial tubercle by increased ten-sion on the posterior talotibial component of thedeltoid ligament. Recognizing a fracture of the ta-lus is imperative, because a prolonged period ofnon-weight-bearing is necessary for healing.14
However, the clinical presentation of some subtlefractures can be misdiagnosed as ankle sprainson initial examination.10 Delays in treatment ofunrecognized fractures may result in long-termdisability, painful nonunion, arthrosis, or avascu-lar necrosis.11,15 Plain radiography, the mostcommon imaging tool for the initial evaluation ofacute or chronic ankle sprains, has shown vary-ing degrees of sensitivity in the detection of anklefractures in previous studies.8,16 Ultrasonogra-phy (US) may be a valuable tool in screening thesprains associated with tarsal bone fractures. Weherein present a case of a patient with a medialtalar fracture diagnosed with US.
CASE REPORT
A 26-year-old woman presented to our physiatryclinic 2 months after spraining her right ankle ina motor vehicle accident. Initially, diffused painand swelling without obvious ecchymoses orwound were noted at her right ankle. The radio-graphs (anterior-posterior and lateral views)obtained immediately after the injury were unre-markable. Under the impression of a right anklesprain, she received regular physiotherapy to herright ankle in a local clinic. Because the symp-toms persisted, she was referred to our physiatrydepartment for further evaluation.
On physical examination, moderate local swel-ling of the right ankle was noted, with no ecchy-moses or definite tender point. She was able to
Correspondence to: Y.-P. Chiang
' 2012 Wiley Periodicals, Inc.
VOL. 00, NO. 0, MONTH 2012 1
Case Report
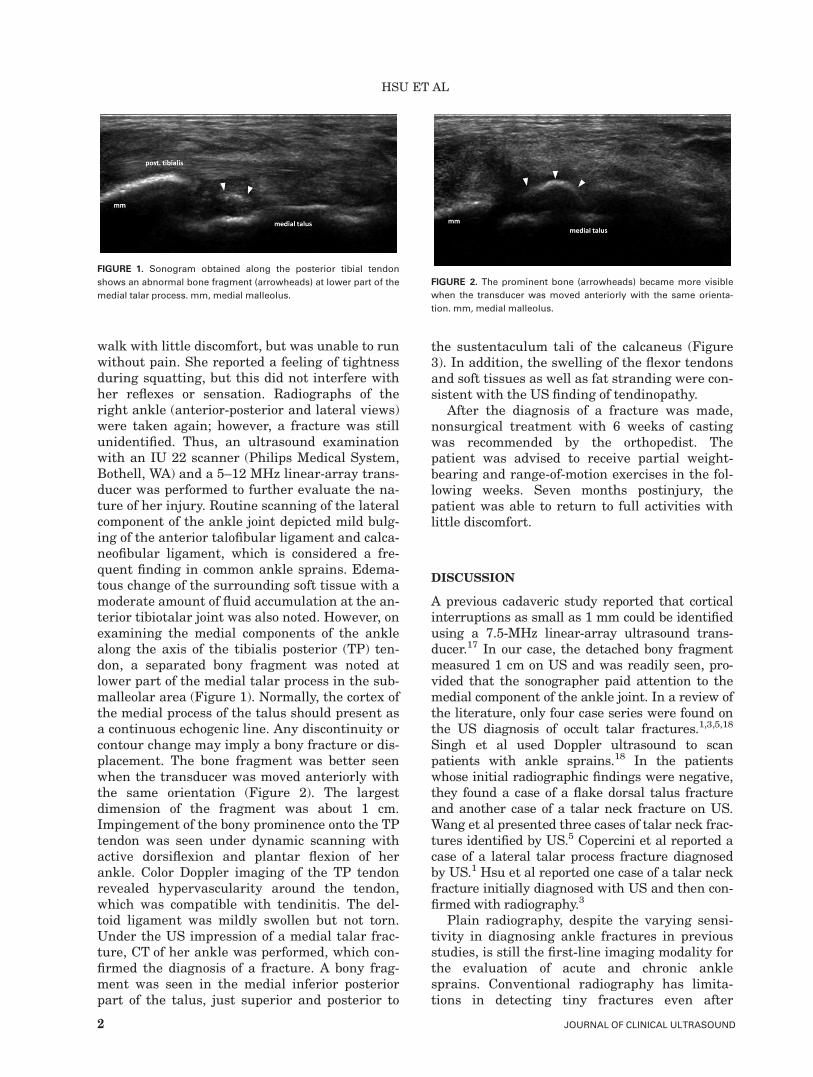
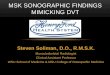
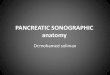
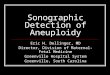
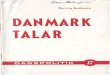
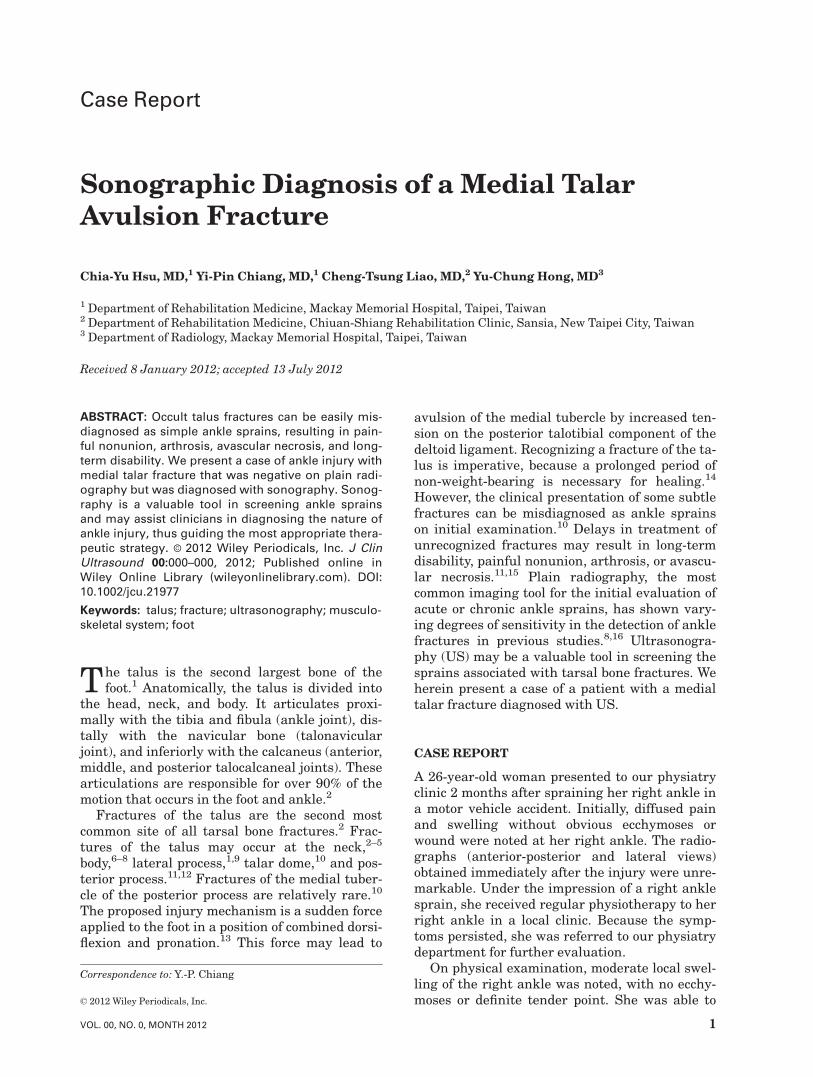
walk with little discomfort, but was unable to runwithout pain. She reported a feeling of tightnessduring squatting, but this did not interfere withher reflexes or sensation. Radiographs of theright ankle (anterior-posterior and lateral views)were taken again; however, a fracture was stillunidentified. Thus, an ultrasound examinationwith an IU 22 scanner (Philips Medical System,Bothell, WA) and a 5–12 MHz linear-array trans-ducer was performed to further evaluate the na-ture of her injury. Routine scanning of the lateralcomponent of the ankle joint depicted mild bulg-ing of the anterior talofibular ligament and calca-neofibular ligament, which is considered a fre-quent finding in common ankle sprains. Edema-tous change of the surrounding soft tissue with amoderate amount of fluid accumulation at the an-terior tibiotalar joint was also noted. However, onexamining the medial components of the anklealong the axis of the tibialis posterior (TP) ten-don, a separated bony fragment was noted atlower part of the medial talar process in the sub-malleolar area (Figure 1). Normally, the cortex ofthe medial process of the talus should present asa continuous echogenic line. Any discontinuity orcontour change may imply a bony fracture or dis-placement. The bone fragment was better seenwhen the transducer was moved anteriorly withthe same orientation (Figure 2). The largestdimension of the fragment was about 1 cm.Impingement of the bony prominence onto the TPtendon was seen under dynamic scanning withactive dorsiflexion and plantar flexion of herankle. Color Doppler imaging of the TP tendonrevealed hypervascularity around the tendon,which was compatible with tendinitis. The del-toid ligament was mildly swollen but not torn.Under the US impression of a medial talar frac-ture, CT of her ankle was performed, which con-firmed the diagnosis of a fracture. A bony frag-ment was seen in the medial inferior posteriorpart of the talus, just superior and posterior to
the sustentaculum tali of the calcaneus (Figure3). In addition, the swelling of the flexor tendonsand soft tissues as well as fat stranding were con-sistent with the US finding of tendinopathy.
After the diagnosis of a fracture was made,nonsurgical treatment with 6 weeks of castingwas recommended by the orthopedist. Thepatient was advised to receive partial weight-bearing and range-of-motion exercises in the fol-lowing weeks. Seven months postinjury, thepatient was able to return to full activities withlittle discomfort.
DISCUSSION
A previous cadaveric study reported that corticalinterruptions as small as 1 mm could be identifiedusing a 7.5-MHz linear-array ultrasound trans-ducer.17 In our case, the detached bony fragmentmeasured 1 cm on US and was readily seen, pro-vided that the sonographer paid attention to themedial component of the ankle joint. In a review ofthe literature, only four case series were found onthe US diagnosis of occult talar fractures.1,3,5,18
Singh et al used Doppler ultrasound to scanpatients with ankle sprains.18 In the patientswhose initial radiographic findings were negative,they found a case of a flake dorsal talus fractureand another case of a talar neck fracture on US.Wang et al presented three cases of talar neck frac-tures identified by US.5 Copercini et al reported acase of a lateral talar process fracture diagnosedby US.1 Hsu et al reported one case of a talar neckfracture initially diagnosed with US and then con-firmed with radiography.3
Plain radiography, despite the varying sensi-tivity in diagnosing ankle fractures in previousstudies, is still the first-line imaging modality forthe evaluation of acute and chronic anklesprains. Conventional radiography has limita-tions in detecting tiny fractures even after
FIGURE 1. Sonogram obtained along the posterior tibial tendon
shows an abnormal bone fragment (arrowheads) at lower part of the
medial talar process. mm, medial malleolus.
FIGURE 2. The prominent bone (arrowheads) became more visible
when the transducer was moved anteriorly with the same orienta-
tion. mm, medial malleolus.
HSU ET AL
2 JOURNAL OF CLINICAL ULTRASOUND

repeated examinations.8 Sujitkumar et alconducted a retrospective study of 2000 ankleinjuries and found that the sensitivity of routineradiography was very low in detecting ‘‘signifi-cant’’ or avulsion fractures.16 The American Col-lege of Radiology has suggested a three-viewplain radiology series (anterior-posterior, lateral,and mortise views) for patients meeting theOttawa rules for suspected ankle fractures.19 Inour case, the fracture involved the medial processof the talus. On the standard anterior-posteriorview the inferior-medial part of the talus wassuperimposed with the navicular and metatarsalbone and thus the fracture was missed. The bene-fit of US is to image in various planes. The trans-ducer was placed where the patient indicated herdiscomfort, and the bony fracture was easilydetected. In addition to the bony fracture,impingement of the TP tendon to the fracturedfragment was also noted, which provided valua-ble information to the clinician for treatment de-cision-making.
The differential diagnosis of a discontinuity orcontour change of bone on sonograms includes abony fracture, calcification deposits, heterotopicossification, and the presence of the accessorybone. A fracture could be diagnosed sonographi-cally by an abrupt discontinuity of the bone surfaceassociated with overlying soft tissue edema, withor without soft tissue injury.20 Because the surfaceof bony fragment of our case was smooth and thesize was as big as 1 cm, calcification was less likely.Other imaging studies may be needed to rule outheterotopic ossification or an accessory bone.20
Considering that persistent symptoms may bethe presentation of missed fractures in chronicankle sprains,21 the possibility of undiagnosedankle fractures should always be kept in mind andimaging tools including radiography,10,11,22 US,CT,11,23 or MRI1,8,11 may be required for an accu-rate diagnosis. CT has very good resolution for thedetection of bony abnormalities. However, it can-not be used to screen for occult bony lesions due toits cost and radiation exposure. US has severaladvantages over MRI in the evaluation of occultfractures including real-time imaging and good re-solution in detecting cortical abnormalities.20 Effi-cacy in detecting occult fractures had been estab-lished.24,25 US also provides valuable informationabout associated soft tissue lesions or the presenceof joint effusion in the injured ankle.26,27
Nonsurgical management should be consid-ered for small (<1 cm) or minimally displaced(<2 mm) fractures.10,11,28 Immobilization in abelow knee, non-weight-bearing cast can resultin a favorable outcome.28
In conclusion, occult fractures of the medialtalar process can be missed in ankle sprains. Themedial compartment, especially the bony struc-ture of the medial talus, should be carefullychecked during sonographic scanning of thepatients with ankle sprains.
REFERENCES
1. Copercini M, Bonvin F, Martinoli C, et al. Sono-graphic diagnosis of talar lateral process fracture.J Ultrasound Med 2003;22:635.
FIGURE 3. CT scans (A, axial; B, coronal) show the avulsed bony fragment (arrowheads) at medial inferior posterior part of the talus. Lm, lateral
malleolus.
MEDIAL TALAR FRACTURE
VOL. 00, NO. 0, MONTH 2012 3

2. Veerappa LA, Gopalkrishna C. Talar neck fracturewith talar head dislocation and intact ankle andsubtalar joints—a rare case report. Foot (Edinb)2010;20:39.
3. Hsu CC, Tsai WC, Chen CP, et al. Ultrasono-graphic examination for inversion ankle sprainsassociated with osseous injuries. Am J Phys MedRehabil 2006;85:785.
4. Valentine BC, 2nd, Buoye SF, Naples JJ. Talarfracture/dislocation in the adolescent patient. JFoot Ankle Surg 1995;34:379.
5. Wang CL, Shieh JY, Wang TG, et al. Sonographicdetection of occult fractures in the foot and ankle.J Clin Ultrasound 1999;27:421.
6. Sayegh FE, Nikolaides AP, Anagnostidis KS, et al.Simultaneous bilateral fracture-dislocation of thetalus: a case report. Foot (Edinb) 2009;19:125.
7. Verettas DA, Ververidis A, Drosos GI, et al. Talarbody fracture combined with bimalleolar fracture.Arch Orthop Trauma Surg 2008;128:731.
8. Rossi F, Dragoni S. Talar body fatigue stress frac-tures: three cases observed in elite female gym-nasts. Skeletal Radiol 2005;34:389.
9. Sanders TG, Ptaszek AJ, Morrison WB. Fractureof the lateral process of the talus: appearance atMR imaging and clinical significance. SkeletalRadiol 1999;28:236.
10. Judd DB, Kim DH. Foot fractures frequently mis-diagnosed as ankle sprains. Am Fam Physician2002;66:785.
11. Berkowitz MJ, Kim DH. Process and tubercle frac-tures of the hindfoot. J Am Acad Orthop Surg2005;13:492.
12. Rogosic S, Bojanic I, Boric I, et al. Unrecognizedfracture of the posteromedial process of the talus—a case report and review of literature. Acta ClinCroat 2010;49:315.
13. Cedell CA. Rupture of the posterior talotibial liga-ment with the avulsion of a bone fragment fromthe talus. Acta Orthop Scand 1974;45:454.
14. Dewar FP, Evans DC. Occult fracture-subluxationof the midtarsal joint. J Bone Joint Surg Br1968;50:386.
15. Babu N, Schuberth JM. Partial avascular necrosis af-ter talar neck fracture. Foot Ankle Int 2010;31:777.
16. Sujitkumar P, Hadfield JM, Yates DW. Sprain orfracture? An analysis of 2000 ankle injuries. ArchEmerg Med 1986;3:101.
17. Grechenig W, Clement HG, Fellinger M, et al.Scope and limitations of ultrasonography in thedocumentation of fractures—an experimentalstudy. Arch Orthop Trauma Surg 1998;117:368.
18. Singh AK, Malpass TS, Walker G. Ultrasonicassessment of injuries to the lateral complex of theankle. Arch Emerg Med 1990;7:90.
19. Dalinka MK, Alazraki N, Berquist TH, et al. Imag-ing evaluation of suspected ankle fractures. Amer-ican College of Radiology ACR AppropriatenessCriteria. Radiology 2000;215(Suppl):239.
20. Cho KH, Lee SM, Lee YH, et al. Ultrasound diag-nosis of either an occult or missed fracture of anextremity in pediatric-aged children. Korean JRadiol 2010;11:84.
21. DIGiovanni BF, Fraga CJ, Cohen BE, et al. Associ-ated injuries found in chronic lateral ankle insta-bility. Foot Ankle Int 2000;21:809.
22. Lucchesi GM, Jackson RE, Peacock WF, et al. Sen-sitivity of the Ottawa rules. Ann Emerg Med1995;26:1.
23. Bonvin F, Montet X, Copercini M, et al. Imagingof fractures of the lateral process of the talus, afrequently missed diagnosis. Eur J Radiol2003;47:64.
24. Simanovsky N, Lamdan R, Hiller N. Sonographicdetection of radiographically occult fractures in pe-diatric ankle and wrist injuries. J Pediatr Orthop2009;29:142.
25. Cho KH, Lee SM, Lee YH, et al. Ultrasound diag-nosis of either an occult or missed fracture of anextremity in pediatric-aged children. Korean JRadiol 2010;11:84.
26. Guillodo Y, Riban P, Guennoc X, et al. Usefulnessof ultrasonographic detection of talocruraleffusion in ankle sprains. J Ultrasound Med 2007;26:831.
27. Peetrons P, Creteur V, Bacq C. Sonography ofankle ligaments. J Clin Ultrasound 2004;32:491.
28. Mizel MS, Hecht PJ, Marymont JV, et al. Evalua-tion and treatment of chronic ankle pain. InstrCourse Lect 2004;53:311.
HSU ET AL
4 JOURNAL OF CLINICAL ULTRASOUND