Embed Size (px)
Citation preview

Sonography of Diffuse Liver
Disease
Mitchell E. Tublin, M.D.
Professor of Radiology
Vice Chair of Clinical and Academic Affairs
Section Chief: Abdominal Imaging
University of Pittsburgh
School of Medicine

Diffuse Liver Disease
• Clinical manifestations often subtle…. or absent
• Patient history helpful….sometimes
• Pattern of LFT abnormality sometimes helpful….. but often not

Diffuse Liver Disease: Ultrasound
• US: premier modality for screening of diffuse liver disease, elevated LFTs
• Findings may be subtle, or nonspecific
• Clinical correlation, “second look sonography” improves sensitivity/specificity
• Look for changes in
– echotexture
– echogenicity
– contour

Diffuse Liver Disease: Ultrasound
• Our goals
• Discuss clinical manifestations, diagnostic clues of spectrum of diffuse liver diseases
– NAFLD (nonalcoholic fatty liver disease)
– Cirrhosis and mimics
– Hepatitis
• Describe innovative ultrasound techniques for identifying and quantifying disease
• Demonstrate practical tips…

Nonalcoholic fatty liver disease
• Fatty infiltration and inflammation common complication of ETOH abuse
• Nonalcoholic fatty liver disease (NAFLD) described in 1980
• Spectrum of metabolic fatty liver diseases
– Steatosis
– Nonalcoholic steatohepatitis (NASH)
– Cirrhosis
• Complex pathophysiology: “lipotoxicity” and oxidative stress

Nonalcoholic fatty liver disease
• Epidemiology/risk factors
– Obesity (central>>overall)
– DM type 2
– Dyslipidemia (↑ triglyc, cholesterol) → metabolic syndrome
– Surgical intervention/extensive SB resection
– Exogenous, endogenous steroids
– Medications (tamoxifen, methotrexate, HAART)
– TPN, starvation, rapid weight loss

Nonalcoholic fatty liver disease
• Obesity epidemic
• NAFLD prevalence in United States (sono, MR spectrometry, liver enzymes): 22-45%
• Histologic progression to cirrhosis: 32-37%
• Public health nightmare

NAFLD: initial assessment
• Scoring systems: clinical and biochemical markers (LFT ratios, DM, HTN, age…)
• Maybe CT, DECT, MR, MRS, MRE….
• Ultrasound still primary imaging screen
• In ideal world:
– Quantify fat
– Detect NASH
– Grade Fibrosis

Steatosis: Swollen, “ballooned” hepatocytes
NASH: steatosis and lobular inflammation. Perisinusoidal
collagen (trichrome)Brunt, Modern Pathology, 2007

NASH to Cirrhosis: 4 years

NASH to Cirrhosis:
Pre biopsy ultrasound

Fatty infiltration: ultrasound
• Grades
– “Mild”: ↑ liver echogenicity
– “Moderate”: ↑↑ echogenicity, “slightly” impaired visualization of vessels, diagphragm
– “Severe”: ↑↑↑ echogenicity, beam attenuation – obscured vessels, posterior liver, diaphragm

Mild Moderate
Severe

Fatty infiltration: ultrasound
• Issues
– Qualitative assessment, operator dependent Poor sensitivity
• Mild fatty infiltration (<30%)
• Morbid obesity
– Patchy fat
– Steatosis vs. NASH vs. early Cirrhosis
• Pearls
– Optimize TGC
– Look for sparing

Fatty infiltration: ultrasound
• Quantification attempts
– Traditional image-based analysis: hepatorenal index
– Raw radiofrequency data
• Speed of sound
• US backscatter, attenuation coefficients
• Controlled-attenuation parameter (Fibroscan)
• Shear wave dispersion
• Not ready for prime time
– Reproducibility, validation
– Fat vs. Fibrosis

Obesity
No fatty infiltration Fatty infiltration

Patchy fat
Minimal fat

62 female, HTN, dyslipidemia, obesity, ↑↑↑
AST, ALT. Sono: severe fat
BX: 80% macrovesicular steatosis, chronic
steatohepatitis, mild periportal fibrosis

Cirrhosis: Ultrasound
• End result of chronic liver injury: cell death, fibrosis, regeneration (nodules, nodules, nodules…)
• Micronodular vs macronodular: pattern often not helpful (or detected)
• Ultrasound used to screen for liver injury/fibrosis

Cirrhosis: Ultrasound features
• Volume distribution
–Early (or primary biliary) cirrhosis: large liver
–Advanced cirrhosis: small liver
–Relative enlargement of left lobe, caudate
–Posterior, medial segment atrophy
–Confluent fibrosis: capsular retraction

Small liver
Big caudatePost seg atrophy
Big lateral seg

Cirrhosis: Ultrasound features
• Coarse echotexture
– Subjective
– Beware of infiltrating tumor (HCC, metastases), bad technique, marginal equipment
• Nodular surface
– Easiest to assess when ascites present
– Lateral segment: linear probe (?)

Hepatic Kaposi sarcoma
Adenoca: unknown primary
Cirrhosis
Hepatic sarcoid

ETOH,
jaundice:
“R/O
cirrhosis”Pearl 1
• Refractive shadows
• Sound refracted by
tissues of different
acoustic impedance
• An indirect sign of
isoechoic tumor
PVP
FSE
+ PVT

Pearl 2: Capsular Nodularity in
Cirrhosis
• Present in more advanced cases
• Anterior surface: sagittal view of left
hepatic lobe
• Nodularity may be more apparent on
undersurface of the liver

PBC: Technique & Scanner Upgrade

Cirrhosis: Ultrasound features
• Secondary findings of portal HTN
–Splenomegaly
–Ascites
• Doppler
–Monophasic HV flow
–HA hypertrophy
–Hepatofugal PV flow
–Shunts

Enlarged hepatic artery &
hepatofugal left PV flowMonophasic HV flow

Cavernous
transformationGastric varices

What do these pts all have in common?
Answer: ‘4’
omental caking capsular thickening
implant omental caking
Ascites
1) Cirrhosis
2) Liver Mets
3) HCC
4) Carcinomatosis
Courtesy: Brooke Jeffrey, MD

Pearl 3: Perihepatic
Manifestations of Disease
• Don’t get tunnel vision: evaluate pleural
and perihepatic areas
• Look for causes of ascites: omental and
peritoneal implants
• Look for surface nodules or subtle capsular
thickening
• Remember long DDX of splenomegaly

Offsite imaging center tunnel vision
Prelim: “ascites”
Perfunctory cine loop

Normal: 10 cm
Cirrhosis: 18 cm
Mononucleosis: 19 cm

Sonography of fibrosis
• Traditional imaging doesn’t cut it
–We only identify end stage
fibrosis/cirrhosis
–Lesser degrees of fibrosis now
amenable for therapy (Hep C / NAFLD)
missed

The answer: stiffness assessment and
liver sonoelastography
• Validated, available, requested, reimburseable
• Dedicated SAR workshops on setting up an
elastography practice
• Straightforward, but several pearls (and
pitfalls) learned along the way
• No physics today

Transient elastography vs. ARFI
techniques
• TE (Fibroscan)
• Mechanical impulse
• M, XL probes
• Speed measurement of longitudinal shear
wave
• Not an imaging technique

transducer
explored volume
4 cm
1 cm
Transient Elastography

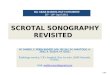
Point-SWE (pSWE)
• ARFI – Acoustic Radiation Force Impulse
• Transient shear waves
• ROI: 10 x 5 mm2
• Values in m/s or kPa
• QA: IQR/median < 30%
✓ Ultrasound image
✗ No elastography map

Two dimensional-SWE (2D-SWE)
• Multiple ARFI pulse pushes
• Larger ROI than in pSWE
• Values in m/s or kPa
• QA: IQR/median < 30%
✓ Ultrasound image
✓ Elastography map

Normal-mild fibrosis / Metavir F1NAFLD HCV

HCV: (F4) Cirrhosis

NAFLD- (F4) Cirrhosis

Pearl 4: Technique matters
SRU Consensus Statement (Barr et al., Radiology 2015)

Shallow Breath vs. Deep Inspiration

Pearl 5: Many reasons for variability
SRU Consensus Statement (Barr et al., Radiology 2015)

Congestive hepatopathy

ETOH, PVT,
osteomyelitis, possible
ascending cholangitis,
sepsis: “R/O cirrhosis”

Pearl 6: Lots of “In-betweener” Overlap
Two cutoff values (low vs. high risk for advanced fibrosis)
with likelihood ratios advocated (Barr, SRU consensus, Radiology 2015

Pearl 6: Lots of “In-betweener” Overlap
HCV, F2(?) at SWE, BX confirmed F2

Pearl 7: The tough ROI (fat, fibrosis ARFI attenuation)

Acute Hepatitis: Ultrasound
• Clinical diagnosis, but ultrasound may be
performed (pre-LFT evaluation) for eval of
RUQ pain, jaundice
• “Starry sky” liver: increased periportal
echogenicity Kurtz, Radiology, 1980
• Gallbladder wall thickening Juttner, Radiology, 1982
• Nonspecific….and often not present

RUQ pain
Hepatitis: “starry sky” liver

Periportal edema
OLTX Passive congestion

A final important case:
Tylenol overdose
ALT 5K, AST 4K
↓ Hepatic attenuation
but….normal ultrasound?
Fulminant hepatic necrosis

Conclusions
• Despite operator dependence, sono is still primary
imaging screen
• NAFLD is a public health nightmare – we’re often the
first to suggest the DX
• Conventional sonography performs well at extremes
(lots of fat, lots of fibrosis)
– Obesity doesn’t automatically imply steatosis: use internal
controls
– Beware of infiltrating tumor: don’t have tunnel vision

Conclusion
• Grading of steatosis is still subjective
– Validated, reproducible sono based fat quantification
methods needed
• SWE can differentiate between no/minimal and
advanced fibrosis
– Accepted, available, reimburseable
– Easily performed, but technique matters, and many
causes for variability