Embed Size (px)
Citation preview

Southern Regional Program Abstracts
Cardiovascular Club I11:00 AMThursday, February 21, 20131
EFFECT OF LOW DOSE DOPAMINE INFUSION ON RENALFUNCTION IN ACUTE DECOMPENSATED HEART FAILUREPATIENTS TREATED WITH INTRAVENOUS FUROSEMIDE
Peters MN1, Alkadri ME2, Katz MJ1, Ventura HO2. 1Tulane UniversityHealth Sciences Center, New Orleans, LA and 2Ochsner Medical Center,Jefferson, LA.Purpose of Study: Worsening renal function (WRF) is common in patientshospitalized with acute decompensated heart failure (ADHF) and is associ-ated with intravenous (IV) furosemide diuresis. Recently it has been shownthat addition of low dose dopamine to low-dose furosemide decreased theincidence of WRF while the diuresis remained clinically effective. The effectof dopamine on renal function in patients with ADHF and chronic kidneydisease (CKD) is unknown.Methods Used: Consecutive patients with a history of congestive heartfailure, baseline ejection fraction e 35% and glomerular filtration rateG60 mL min-1 presenting with ADHF were retrospectively assessed. Allpatients received Q120mg IV furosemide/24 hours for Q48 hours. Threecohorts were established based on physician-initiated therapy: (1) low dosedopamine (2-5Kg kg-1 min-1) initiated G 6 hours after presentation (Jan 2010-Jan 2012), (2) low dose dopamine initiated 9 24 hours after presentation(Jan 2010- Jan 2012) and (3) no dopamine (Jan 2010-July 2010).Summary of Results: Patients who received dopamine during hospitaliza-tion for ADHF had a significantly decreased incidence of WRF and durationof hospitalization and a non-significant increase in 30 day rehospitalizationand 6 month mortality (Table). Timing of dopamine administration did nothave a significant effect.Conclusions: Among patients with CKD admitted for ADHF the additionof low dose dopamine to intravenous furosemide significantly decreased oc-currence of WRF and length of hospitalization.
2
MYOFIBROBLAST SECRETOME AND PATHOLOGICREMODELING IN HYPERTENSIVE HEART DISEASE
Al Darazi F, Zhao T, Zhao W, Sun Y, Weber KT. University of TennesseeHealth Science Center, Memphis, TN.
Purpose of Study: Chronic aldosteronism (inappropriate for dietary Na+)is accompanied by hypertensive heart disease (HHD). Its pathophysiologicorigins and tissue heterogeneity are rooted in fibrosis produced by myofi-broblasts (myoFb), phenotypically transformed fibroblast-like cells, whosehigh turnover of type I collagen is driven by angiotensin(Ang) II produced denovo through angiotensin converting enzyme (ACE) activity and AT1 recep-tor binding. This profibrogenic ACE/AngII/AT1R signaling axis representsa myoFb secretome. It is opposed by ACE2 and Ang1-7 formed by the localhydrolysis of AngII and its binding to Mas receptors (MasR). We hypothe-sized this counterregulatory ACE2/Ang1-7/MasR axis, which could preventfibrosis, is downregulated in chronic aldosteronism, where circulating AngIIis suppressed.Methods Used: Eight-wk-old uninephrectomized male Sprague-Dawleyrats received a minipump implanted subcutaneously and releasing aldoste-rone (0.75 Kg/h) to raise its plasma levels to those found with human aldo-steronism; drinking water was fortified with 1% NaCl (ALDOST) and 0.4%KCl to prevent hypokalemia. A separate group received ALDOST plusvalsartan (Val, 10 mg/kg/day by gavage), an AT1 receptor blocker, and age-/sex-matched untreated rats served as controls. In heart tissue harvested at4 wks we determined: ACE2 mRNA expression; density of autoradio-graphic ACE and AT1 receptor binding; MasR expression by Western blot;myoFb >-smooth muscle actin (>-SMA) immunolabeling; and fibrosis bymRNA expression of type I collagen and histochemical assessment of col-lagen volume fraction.Summary of Results: Compared to controls, at 4 wks ALDOSTwe founddownregulation (pG0.05) of ACE2 mRNA expression and MasR protein.Contrariwise, high density ACE and AT1 receptor binding were anatomicallycoincident with >-SMA positive myoFb at sites of type I collagen accumu-lation and tissue fibrosis (pG0.05), which were prevented by Val cotreatment(pG0.05).Conclusions: The pathologic remodeling of myocardium in the HHD as-sociated with ALDOST is based on an activated myoFb fibrogenic phenotypeand its secretomeVthe ACE/AngII/AT1 receptor pathway and signature offibrosisVwhile the antifibrogenic ACE-2/MasR axis is downregulated.
3
SPECIFIC INACTIVATION OF INSULIN-LIKE GROWTHFACTOR-1 RECEPTOR IN ENDOTHELIUM OF APOEKNOCKOUT MICE INCREASES ATHEROSCLEROTICPLAQUE BURDEN
Shai S, Sukhanov S, Kim CD, Delafontaine P, Higashi Y. Tulane UniversitySchool of Medicine, New Orleans, LA.Purpose of Study: Although IGF-1 infusion in ApoE-/- mice reduces ath-erosclerotic plaque burden via a nitric oxide-independent pathway, the role ofendothelial IGF-1 receptor (IGF-1R) signaling in atherogenesis is unknownMethods Used: Mice with an endothelial-specific IGF-1R null mutation(VFIRKO mice) were generated by crossing mice overexpressing cadherin5 promoter-driven Cre recombinase with floxed IGF-1R/Apoe-/- mice. 7 wold VFIRKO and FIR/Apoe-/- (FIR, control, CTL) mice (n=20) were fed withWestern-type diet for 12 weeks. Serum IGF-1 level were measured by Elisa.Aortic plaques were quantified by Oil-red O en face analysis. Cultured hu-man aortic endothelial cells were used to study the mechanisms wherebyIGF-1/IGF-1R signaling altered OxLDL-induced oxidative stressSummary of Results: Endothelial-specific IGF-1R deletion did not altercirculating IGF-1 levels (VFIRKO/FIR, 307.6+15.0 vs. 300.7+12.6 ng/ml),mouse body weight (VFIRKO/FIR, 26.3+0.8 vs. 26.0+0.8 g), spleen weight(VFIRKO/FIR, 130.5+13.3 vs. 25.2+32.2 mg), plasma nitrate/nitrite levels(index of nitric oxide bioavailability, VFIRKO/FIR, 8.6+0.4 vs. 7.3+0.9 umol/L)and systolic blood pressure (VFIRKO/FIR, 112.8+4.1 vs. 113.0+3.9 mm Hg).However, VFIRKO mice had increased atherosclerotic lesion surface area as
SOUTHERN REGIONAL PROGRAM ABSTRACTS
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 373
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

assessed by Oil Red O staining of en face aortas (VFIRKO/FIR, 7.7+0.5% vs.5.1+0.4%, pG0.005), indicating that endothelial IGF-1R signaling is anti-atherogenic. To determine mechanisms we assessed potential anti-oxidanteffects of IGF-1 on vascular endothelium. IGF-1 (100 ng/ml, 24h) markedlyreduced oxidized LDL-induced ROS generation in human aortic endothelialcells (EC, 67T9% decrease vs. OxLDL alone, PG0.01, DCF assay). IGF-1 didnot alter expression or activity of superoxide dismutase-1, 2 or catalase butmarkedly increased expression (2.6-fold at 24h, Western blot, PG0.01) andactivity (IGF-1 24h, 21.2 T 2.1 U/mg protein vs. control, 4.4T1.2 U/mg protein,PG0.01) of glutathione peroxidase (GPX-1), a crucial anti-oxidant enzyme.Conclusions: In summary, inhibition of endothelial IGF-1R signaling ispro-atherogenic. Our data suggest that GPX-dependent endothelial ROS sup-pression might mediate IGF-1-induced atheroprotection.
4
RACE AND SEX DIFFERENCES IN CENTRAL TOPERIPHERAL HEMODYNAMIC PATTERNS IN ADULTS:BOGALUSA HEART STUDY
Clark R, Fernandez C, Berenson G, Giles T, Sander G. Tulane UniversitySchool of Medicine, New Orleans, LA.Purpose of Study: Measurements of aortic compliance are important pre-dictors of cardiovascular mortality; however, the relationship between cen-tral parameters and peripheral parameters has not been fully described,especially in different race and sex groups. This study sought to describewhite-black and male-female differences in the relationship between centralsystolic blood pressure (cSBP) and peripheral pulse pressure (pPP) in theBogalusa study adult population.Methods Used: Arterial pressure was measured with a standard cuff andan Omron applanation tonometer. A linear regression model was used to de-scribe the relationship between cSBP and pPP and an Altman Bland test ofinteraction was used to compare the strength of correlation between race andsex groups. Data from 906 participants were available.Summary of Results: Participants were 31.6% black, 68.4% white and41.9% were male (mean age of 43.3 years T 4.4). Overall, linear regressionshowed strong correlation between pPP and cSBP (r=0.694; pG0.001). Cor-relation remained strong when the cohort was divided by only race (blacks:r=0.67; pG.001, whites: r=0.51; pG.001), only sex (males: r=0.58; pG.001,females: r=0.65; pG.01) and by race-sex specific groups (white males:r=0.44; pG.001, black males: r=0.61; pG.001, white females: r=0.59; pG.001,black females: r=0.69; pG.01). There was significant difference in strength ofcorrelation between overall males and females (pG0.01) as well as betweenother race-sex groups (Table 1).Conclusions: Peripheral PP and cSBP were strongly correlated, suggestingincreased aortic stiffening is associated with predictable increases in pPP. Ourdata suggest there are significant differences in central versus peripheral he-modynamic patterns between men, women, blacks and whites. This is con-sistent with previous analysis showing hemodynamic differences in blacksand whites while further suggesting differences between men and women.
Adult Clinical Case Symposium
1:00 PMThursday, February 21, 20135
AN UNUSUAL CAUSE OF SPLENOMEGALY IN ANADULT - CAROLI’S SYNDROME
Panikkath R, Lado J. TTUHSC, Lubbock, TX.
Case Report:Introduction: Caroli’s disease is a rare inherited disorder characterized bydilatation of intrahepatic biliary tree, whereas Caroli’s syndrome is a complexof hepatic fibrosis, intrahepatic biliary dilatation and portal hypertension. Itis unusual to present in young Caucasians and with isolated splenomegaly.It is usually seen in Asia. Caroli’s disease is inherited as autosomal dominantpattern whereas Caroli’s syndrome is inherited as an autosomal recessive pattern.Methods: This is a case report of a patient with Caroli’s syndrome whopresented with splenomegaly.Results: A 22 year old healthy adult Caucasian male presented to us forevaluation of massive splenomegaly. Detailed investigations for the work upof splenomegaly including infectious, hematologic and neoplastic causeswere negative. His karyotype, cytogenetics and osmotic fragility tests werealso normal. Ultrasound and MRI abdomen showed dilated portal vein andcollaterals suggestive of portal hypertension. MRI showed significant intra-hepatic biliary dilatation as well. He denied history of gastrointestinal bleed.Liver function tests were normal including total bilirubin and alkaline phos-phatase. He denied drinking alcohol and his hepatitis panel was negative.Serum ferritin and ceruloplasmin were normal. He underwent a liver biopsywhich showed features suggestive of intrahepatic biliary dilatation and he-patic fibrosis suggestive of Caroli’s disease. His aunt had a history of liverproblems and splenomegaly due to unclear reasons. Since he had features ofhepatic fibrosis, portal hypertension and intrahepatic biliary dilatation (withoutany significant obstruction of the extra or intra hepatic biliary system), CarolisSyndrome was diagnosed.Conclusion: Caroli’s Syndrome is a rare inherited cause of liver diseaseusually seen in Asians. This syndrome, presenting in young Caucasian malewith isolated splenomegaly without other symptoms is extremely rare.
6
GASTROINTESTINAL SARCOIDOSIS ASSOCIATED WITHPNEUMATOSIS CYSTOIDES INTESTINALIS
Rahim H, Amorosa L. UMDNJ-RWJMS, New Brunswick, NJ.Case Report: A 39 year old male reported fevers, weight loss, loose wa-tery stools, and decreased visual acuity in his right eye over the previousfive years. He was pancytopenic, had an elevated ACE level, total bilirubin,and alkaline phosphatase. CT of the abdomen and pelvis revealed massivehepatosplenomegaly and emphysematous lung changes. Liver biopsy showednon caseating granulomas. The patient was diagnosed with extrapulmonarysarcoidosis and was treated with prednisone. The patient symptomaticallyimproved but five months later presented with abdominal pain caused byperforation of the cecum. He underwent a cecectomy and pathology revealedpneumatosis cystoides intestinalis.
The 5 year interval between symptom onset and treatment allowed thedisease to follow its natural history presumably resulting in the atypicalpresentations and rare complications that may be avoided with earlier treat-ment. This case represents the first reported association between pneumatosiscystoides intestinalis and sarcoidosis. Furthermore, emphysematous lungchanges and pancytopenia are extraordinarily uncommon with sarcoidosis.
7
LARGE CORONARY ARTERY FISTULA IN ANASYMPTOMATIC PATIENT
Perez RE, Martinez Ojeda J, Martinez Toro J, Figueroa R. University of PuertoRico, San Juan, Puerto Rico.Case Report: We present the case of a 55-year-old asymptomatic Hispanicfemale with a large coronary to pulmonary artery fistula in association tomultiple aneurysms and an abnormal coronary artery system, diagnosed aftera routine evaluation. Patient was referred to our institution due to abnormalfindings on chest imaging studies. On evaluation patient referred no relevantsymptoms. Physical examination and past history was unremarkable.
Coronary angiography revealed a coronary to pulmonary artery fistulaand three large saccular aneurysms in the left anterior descending coronaryartery (LAD). A high pulmonary-systemic blood flow ratio was confirmed byechocardiography. Curiously, the LAD continued an abnormal path awayfrom the myocardium distal to the bifurcation with the first diagonal artery.
Closure by percutaneous intervention was considered optimal due to ab-normal coronary anatomy and its association to three large saccular aneurysms
Differences in Strength of Correlation between Race-Sexgroups, Altman Bland test of Interaction
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
374 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

proximal to the fistula. Patient underwent transcatheter embolization with acoil devise without any complications.
Coronary artery fistula accounts for 50% of pediatric coronary vascula-ture anomalies and 56% are diagnosed after 20 years of age. Early closureis highly recommended due to the natural progression of large sized fistula.Transcatheter and surgical closure have comparable early effectiveness, mor-bidity and mortality. Still, a percutaneous intervention is considered preferablein case of an abnormal coronary system.
8
SYNDROME OF INAPPROPRIATE ANTIDIURETICHORMONE SECRETION ASSOCIATED WITH NSAIDS
Lim S, Panikkath R, Prabhakar S. Texas Tech University Health SciencesCenter, LUBBOCK, TX.Case Report: Nonsteroidal anti-inflammatory drugs (NSAIDs) are com-monly used analgesic drugs. Although rare, clinicians need to keep in mindthat their use may precipitate hyponatremia and syndrome of inappropriateantidiuretic hormone secretion (SIADH).
A 65 year old male with past medical history of chronic alcohol abuse,chronic obstructive lung disease on steroid maintenance therapy presentedwith acute severe back pain. He was admitted to the hospital for furtherworkup and control of his pain. Computed tomography scan with intravenouscontrast was negative for dissection of the aorta. Myoview was negative forischemic heart disease. Subsequent MRI of the back showed vertebral frac-ture in T6. He was started on keterolac intravenously initially for pain control.Subsequently tramadol, hydrocodone and morphine were added because hispain was poorly controlled. He developed worsening hyponatremia, 135 meq/L(day 1 of admission) to 118 meq/L (day 5 of admission). He was clinicallyeuvolemic. He was increasingly agitated and confused. Other pertinent labsinclude serum osmolality 267 mOsm/kg, urine osmolality 517 mOsm/kg,urine sodium 34 meq/L. Kidney, thyroid function and morning serum cortisollevels were normal. He was transferred to the intensive care unit. Keterolacwas stopped along with other pain medications. He was treated with waterrestriction, and was given benzodiazepines for alcohol withdrawal. His so-dium subsequently normalized to baseline.
The risk of development of hyponatremia and SIADH is increased inpatients with NSAID use because the effect of antidiuretic hormone (ADH) inthe kidneys are potentiated by NSAIDs. NSAIDs inhibit the synthesis ofrenal prostaglandin, an inhibitor of ADH. Development of hyponatremia ex-clusively due to NSAIDs is uncommon, as NSAIDs seem to have antagonis-tic effects on ADH release from the nervous system. However, NSAIDs mayprecipitate the development of SIADH and hyponatremia in high risk pa-tients. One case series found that extremes of age was a risk factor for de-velopment of hyponatremia from NSAIDs. Caution is required when usingNSAIDs. Patients who are at risk need to be monitored for development ofhyponatremia and SIADH.
9
A NEW CONSIDERATION WHEN ANGIOEDEMA STRIKES ADIABETIC: LIRAGLUTIDE
Vandiver L, Smalligan RD. Texas Tech Univ Health Sciences Center, Amarillo, TX.Case Report: A 64-year-old African American female with diabetes andhypertension presented to the emergency room with swelling on the right sideof her upper lip, spreading to both upper and lower lips while waiting to beseen. The patient was short of breath with difficulty speaking. Her diet androutine had not changed recently. PMH: atrial fibrillation, GERD, osteoporo-sis, chronic kidney disease, gout, depression and hyperlipidemia. Medications:rivaroxaban, furosemide, lisinopril, simvastatin, amlodipine, metoprolol, cal-citriol, raloxifene, insulin, liraglutide, citalopram and allopurinol. Physical exam:T 98.7, BP 131/75, HR 69, RR 20, O2 sat 94% on RA. The patient was inmoderate distress with circumoral swelling. Tongue and pharynx were with-out swelling. Breath sounds were clear to auscultation without stridor. Cardiac,abdominal, and neurological systems were normal. Labs were normal exceptfor Cr 1.42. The patient was admitted for observation and possible airwayprotection. Lisinopril was discontinued and methylprednisolone and diphen-hydramine administered. Overnight she still complained of shortness of breathand was transferred to the ICU. After careful retaking of the history it wasdiscovered that liraglutide was started 2 weeks prior to admission. Liraglutidewas discontinued in the ICU and within one day the patient’s swelling andshortness of breath markedly improved. She was discharged on steroids andinstructed to avoid liraglutide and ACE inhibitors.Discussion: As of 2011, 25.8 million people in the US suffer from diabetes.New agents such as glucagon-like peptide-1 (GLP-1) analogues are an optionfor those with difficulty optimizing glycemic control. Liraglutide is a relativelynewGLP-1 analogue used for treatment of T2DM. Post marketing reports showhypersensitivity reactions like anaphylaxis and angioedema can occur whenusing GLP-1 analogues. Although our patient was also taking lisinopril, thetiming of the onset makes liraglutide the more suspicious agent. As the use ofnew diabetic medications, like liraglutide, is certain to continue to increase inpopularity, it is important for physicians to be aware of possible severe ad-verse side effects in order to improve patient care and avoid complications byquickly discontinuing offending medications.
10
SHOULD WE ALWAYS BLAME HER-MONES? AN INSIDELOOK AT CEREBRALVENOUS THROMBOSIS
Subash M, Walker JW. Texas Tech University Health Sciences Center Schoolof Medicine, Amarillo, TX.Case Report: A 29 year-old Caucasian female presents with sudden, sharppain in the front and back of her head that escalated from 6 weeks prior. Shereports diplopia, vomiting, and digital paresthesias. Social history includes12 year history of OCP use and being a non-smoker. She had one normalpregnancy 12 years ago. Her family history includes no history of coagulop-athy. MRI reveals transverse sinus thromboses and right-sided mastoiditis withno parenchymal abnormalities. She screened negative for Factor V, Antipho-spholipid and ANA antibodies and positive for heterozygous MTHFR genevariants (C677T and A1298C). Homocysteine levels were not elevated. Shediscontinued OCPs and began warfarin anticoagulation. Although contra-ception was offered, she returned to clinic later with a positive pregnancy test.She was switched to LMWH and monitored closely.Discussion: Although OCP users are 22.1 times more likely to develop ce-rebral venous thromboses (CVT) as compared to non-users, the event-free lengthof OCP use in our patient diminishes her risk of venous thromboembolism(VTE) up to 50%. Her previously normal pregnancy supports that estrogenfluctuation was not the major mediator of her CVT. The most frequent pre-disposing conditions to CVT include prothrombotic conditions, recent onsetof OCP usage, pregnancy, and infection. Though absent in our patient, pa-renchymal lesions and decreased cerebrospinal fluid absorption are oftencaused by cerebral venous thrombosis. Occlusions lead to elevated intra-cranial pressure, resulting in headaches, vomiting, and visual deficits. Focalheadaches are the most frequent symptom of CVT. Reversing potentiat-ing factors and anticoagulation are the mainstays of treatment for CVT. Ourpatient inherited heterozygous mutations of the MTHFR gene, generally notassociated with hyperhomocysteinemia. She had normal homocysteine levels
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 375
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of 5.9 umol/L. Historically, hyperhomocysteinemia associated with C677Thomozygous states often increases CVT risk by favoring a prothromboticstate. Our patient didn’t fit the ‘traditional’ risk factors for CVT. She main-tained a long event-free history of OCP use, no gross abnormalities on MRI,and normal homocysteine levels. Her case underscores the need for a closerlook at the screening for and etiology of CVT.
11
COMBINED THROMBOSIS AND BLEEDING IN A PATIENTWITH SLE
Aly M, Nusrat M, Nugent K, El-Bakush A, Mazek H. Texas Tech Lubbock,Lubbock, TX.Purpose of Study: This case highlights a rare coexisting thrombophilia andbleeding tendency in a patient with SLE without the antiphospholipid syn-drome. We report a case with newly diagnosed SLE with extensive clottingwho subsequently had a clinically significant bleeding, a subarachnoid hem-orrhage, while patient was in the therapeutic range of anticoagulation. Thismight indicate the possibility that other unknown factors in patients with SLEcontribute to both clotting tendency and a higher than average risk for bleeding.Methods Used: Case report and literature review.Summary of Results: A 23-y-o Hispanic woman was admitted with a newdiagnosis of SLE with proteinuria and worsening renal function. Renal du-plex of the left kidney shows no Doppler signal in the mid renal vein. MRIshowed extensive thrombus in the left renal vein extending into the infra andintrahepatic IVC. Work up for thrombophilia was within normal limits: INR,PTT, PT, PLT, BETA2-Glycoprotein I Ab IgA, BETA2-Glycoprotein I AbIgG, BETA2-Glycoprotein I Ab IgM, Phosphoserine IgA, PhosphoserineIgG, Phosphoserine IgM, Cardiolipin IgA, Cardiolipin IgG, Cardiolipin IgM,and negative Antiphospholipid Ab. The patient developed subarachnoidhemorrhage while in therapeutic range of anticoagulation and her MRA andCT angiogram were negative for aneurysm and vascular malformation.Conclusions: Systemic lupus erythematosus (SLE) is an autoimmune sys-temic inflammatory disease associated with premature vasculitis, and coa-gulopathy. Subarachnoid hemorrhage has been described in case reports inpatients with SLE. In the case we are presenting, the patient had a mixture ofboth thrombophilia and a bleeding tendency while anticoagulated. She didnot have the antiphospholipid syndrome and no apparent explanation for herbleeding event on her lab and radiographic studies. The coexistence of bothconditions in such cases is rare and has not been reported before.
12
RECURRENT ASEPTIC MENINGITIS: A CASE OFMOLLARET’S MENINGITIS
Sotello D1, Temple B1,2, Rivas M1, Patel G1,3. 1Texas Tech University HealthSciences Center, Lubbock, TX; 2Texas Tech University Health SciencesCenter, Lubbock, TX and 3Texas Tech University Health Sciences Center,Lubbock, TX.Case Report: Recurrent Aseptic Meningitis (RAM) is a medical conditionwith multiple possible etiologies that presents a challenging clinical dilemma.The main differential diagnoses include: drug hypersensitivity, infections,neoplasms, Systemic Lupus Erythematosus, Behcet syndrome, sarcoidosis.We present a case of RAM, produced by a chronic infection of HerpexSimplex Virus type 2 (HSV-2) also known as Mollaret’s Meningitis (MM).
This is a 34 year old male, with a history of 3 episodes of aseptic men-ingitis of unknown etiology in the last 8 years, fully recovering after eachepisode. He presented to the emergency center with a 2 day history of severefrontal and retroorbital pain with radiation to the nape of the neck, associ-ated with fever, photophobia and neck stiffness. On physical examination thepatient was afebrile with stable vital signs. His exam was negative for Kernigand Brudzinski signs and laboratory exams were within normal limits. Alumbar puncture was performed, Cerebrospinal fluid (CSF) findings: color-less, clear, RBC: 93/mm3, WBC: 52/mm3, neutrophil: 49%, lymphocytes: 47%,monocytes: 4%, glucose: 49 mg/dl, protein: 80 mg/dl with negative gramstain and culture. HIV, ANA, Head CTandMRI were negative. CSF PCR wasnegative for enterovirus but positive for HSV-2 (437 copies/ml). The patientwas treated with IV acyclovir for 14 days, without any complications.
Pierre Mollaret first described MM in 1944. MM is a benign RAMcharacterized by episodes of fever and signs of meningeal irritation lastingbetween 2 and 5 days. It is also associated with spontaneous recovery and alymphocytic pleocytosis in the CSF. The most common etiology found inMM is HSV-2, and less commonly: Echovirus, Coxsackie, Epstein BarrVirus. Various authors recommend checking for HSV-2 PCR in CSF betweenthe 2nd and 5th day of symptom onset. Treatment is with intravenous acy-clovir (10 mg/kg/q8h for 10-21 days). Suppressive treatment for frequentrelapses has been described, with oral acyclovir, valacyclovir or famciclovir;due to the rarity of the disease no randomized controlled trials have beenperformed.
13
SEIZED BY A DESIRE TO GET HIGH BY SNORTING(BUPROPION INSUFFLATION LEADS TO SEIZURES)
Klaus B, Mahnoor R, Smalligan RD. Texas Tech Univ Health Sciences Center,Amarillo, TX.Case Report:Case: A 38yo man with a history of depression presented to the ED afterbeing found seizing. The patient denied fever, headache, blurred vision, nau-sea, vomiting or urinary symptoms leading up to the event. The patient reporteda similar episode 1 month prior. Both episodes of seizure occurred after hecrushed and insufflated (‘‘snorted’’) Wellbutrin XL tablets in an attempt to gethigh. On this date, the patient crushed and insufflated eleven 300mg pills. Hedenied any other recent medications, alcohol or illicit drug use. His pastmedical history was otherwise negative. Physical exam: T98.7 F, BP 120/72,pulse 120, RR 18, and O2 saturation 97% onRA. Patient was alert and oriented,had multiple tattoos and piercings, atraumatic head, PERRLA and dry mouth.Cardiac, pulmonary, neurologic and abdominal exams were normal. Lab: CBC,CMP, and hepatitis panel were normal except for AST 79 and ALT 72. Urinetoxicology screen, salicylate, acetaminophen and alcohol levels were nega-tive. CT of the head and EEG were normal. The patient was admitted, hy-drated and observed for seizures. He was discharged after 24 hours withoutfurther events.Discussion: Among antidepressants, bupropion is often used as an adjunctwhen further treatment beyond a serotonin reuptake inhibitor (SSRI) is re-quired. Bupropion has been associated with seizures in oral overdose and attherapeutic doses. This case demonstrates that the risk of seizures is also presentwhen the drug is insufflated. Our patient learned the practice of bupropioninsufflation while in prison. A search of PubMed revealed another case reportof bupropion insufflation by a prisoner, though without seizures. Anotherstudy reported oral bupropion as the third leading cause of new-onset drugrelated seizures. Bupropion undergoes 95% hepatic first pass metabolismwhen taken orally. The drug likely achieves greater bioavailability wheninsufflated by preventing the effect of first pass metabolism. It should alsobe noted that bupropion is a small and lipophilic molecule. The seizure riskof bupropion is dose dependent, hence insufflating even a therapeutic dosemay be dangerous. This case report reminds physicians to consider the abuseof bupropion by insufflation and its seizure risk despite the belief that themedication is of low abuse potential.
14WITHDREW
15
VANCOMYCIN/ ZOSYN INDUCED DIHS WITH BILATERALPLEURAL EFFUSIONS
Farooq S1, Childress D2. 1Univ of Tenessee health Science center, Memphis,TN and 2VA Medical Center, Memphis, TN.Case Report: We describe a case of DIHS (Drug Induced HypersensitivitySyndrome) induced by vancomycin and Zosyn with peripheral lymhocytosis,severe lung involvement but no eosinophillia. DIHS with bilateral pleuraleffusions is a rare presentation that we are reporting here.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
376 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

78 yo male came to ED with a rash for 5 days and shortness of breath for2 weeks. He was started on vancomycin and Zosyn 3 weeks earlier forosteomylitis. On exam he was febrile with bilateral decreased breath sounds.Skin exam showed a maculopapular, morbiliform, palpable rash that startedfrom trunk and involved the whole body. Biopsy from skin showed peri-vascular, spongiotic dermatitis consistent with drug eruption. Pleural fluidanalysis showed exudative effusion with monocytosis. Vancomycin and Zosynwere stopped. His rash, pleural effusions, fever, and SOB resolved within aweek after stopping antibiotics and pt was discharged with new regimen fortreatment of osteomyelitis.Discussion/ Conclusion: DIHS is a type IV drug allergy reaction and ischaracterized by the presence of at least three of the following findings:rash, fever, eosinophilia, atypical lymphocytosis, lymphadenopathy and multiorgan failure (1, 2, 3, ). Rarely DIHS can present without eosinophilia as inour case. The liver and kidneys are most often affected and anti-epileptics arethe most common drugs causing DIHS (1, 2). We are reporting Vancomycin/Zosyn causing DIHS with lung involvement in form of bilateral pleural ef-fusions which is a rare presentation.
Vancomycin and Zosyn can induce DIHS with lymphocytic predomi-nance, bilateral pleural effusions, and without eosinophilia. We cannot becertain which of the antibiotics caused the DIHS, as both antibiotics werestarted and stopped at the same time. Recognition of vancomycin/ Zosynas a cause of DIHS is important as many life threating cases have beenreported.
References:
1. Dauby N, Fink W, Seyler L, Luce S, Nouwynck C, Tas S, Jacobs F. ActaClin Belg. 2012 May-Jun;67(3):226-8.
2. Blumenthal KG, Patil SU, Long AA Allergy Asthma Proc. 2012Mar-Apr;33(2):165-71.
3. Pharmacotherapy. 2011 Mar;31(3):332. The DRESS syndrome:Fleming P, Marik PE. Source: Department of Medicine, Eastern VirginiaMeCriado PR, Criado RF, Avancini Jde M, Santi CG.
Pediatric Clinical Case Symposium
1:00 PMThursday, February 21, 201316
RECURRENT INTUSSUSCEPTION DUE TO NON HODGKIN’SLYMPHOMA IN A 6-YEAR-OLD BOY
Sankararaman S, Comeau J, Herbst J, Jeroudi M. Louisiana State UniversityHealth Sciences Center, Shreveport, LA.Case Report: A 6-year-old boy with no significant past medical historypresented to the emergency room with intermittent abdominal pain and nobowel movements for one week. Patient reported no recent illness or changein diet or intake of any medications. He was diagnosed with acute consti-pation and a Fleet enema was given. He was discharged home with a pre-scription of polyethylene glycol and advised to increase fluids and fiberintake. As the symptoms persisted, he returned to the pediatric clinic two dayslater. Abdominal examination did not reveal any tenderness, mass or dis-tension. Rectal examination revealed small amount of stool admixed withblood in the rectum. Abdominal radiograph was not contributory. The pres-ence of blood in the stools warranted further investigations. On colonoscopy,a pedunculated solid mass in the region of splenic flexure (Figure 1) wasfound. Biopsy from the tumor showed an unclassifiable high grade non-Hodgkin’s B-cell tumor. Computer tomogram of the abdomen showed a 3x2cm homogenous ovoid mass in the region of splenic flexure (Figure 2, in-dicated by white arrows). With persistent recurrence of symptoms, abdominalultrasound was done which revealed intussusception with the tumor as thelead point. Left hemicolectomy was done and the patient was started onchemotherapy. As constipation and functional abdominal pain are over-whelmingly common in children, diagnosis of relatively rare serious diseasessuch as malignancies is often significantly delayed. Hence high index ofsuspicion is required; thorough history and physical examination should bealways focused on ruling out these conditions.
17
HYPOCALCEMIA - A REVERSIBLE CAUSE OFDILATED CARDIOMYOPATHY
Velayuthan S, Gungor N, McVie R. Louisiana State University Health SciencesCenter, Shreveport, LA.Case Report: A five week old African-American male was brought to theemergency room (ER) with respiratory failure and severe dehydration. Healso had history of irritability and refusal of feeds for one day. He was born atfull term and had smooth transition. He was breast fed since birth. His par-ents and 8 year old half brother are healthy. Vital signs at presentation weretemperature of 97 F, pulse rate of 146/ minute, respiratory rate of 47/minuteand blood pressure of 74/41 mm of mercury. Physical exam revealed a le-thargic, dehydrated baby in severe respiratory distress. A grade 3 holosys-tolic murmur at the mirtal area and a third heart sound were heard. His liverwas palpable 3 cms below the right costal margin. The patient was intubatedand given 3 fluid boluses with 20cc of normal saline/kg each. The initiallaboratory work was significant for calcium of 3.9mg/dl, ionised calcium of0.55 mmol/L phosphorus of 15.2mg/dl, magnesium of 1.9 mg/dl and alkalinephosphotase of 239units/L. The parathyroid hormone level was very low (lessthan 2 pg/ml). Carnitine and 1, 25 dihydroxy vitamin D levels were normal.Chest Xray showed enlarged cardiac silhoutte. Electrocardiogram (ECHO)showed biventricular hypertrophy. ECHO demonstrated severely dilated leftatrium and left ventricle with poor contractility. The shortening fraction (SF)was 12% and ejection fraction (EF) was 28%. Based on these findings, di-agnosis of primary hypoparathyroidism and dilated cardiomyopathy second-ary to hypocalcemia was made.
After the initial stabilization with dobutamine and calcium chloride in-fusions, he was treated with calcium glubionate, dihydrotachysterol, digoxin,spiranolactone, hydrochlorthiazide and low phosphorus formula. ECHO per-formed 2 weeks later showed an improvement in SF and EF to 24% and 44%respectively. Our patient is now 9 years old and is on calcium supplements,calcitriol, enalapril and low phosphate diet. His growth is at the 25th per-centile for weight and 50th percentile for height. The causes of dilated car-diomyopathy are numerous and few reversible causes such as hypocalcemiashould be kept in mind. Therefore, we emphasize the need of awareness aboutthe potential reversible causes of cardiac failure among pediatricians whichcould be life saving.
18
CHEST PAIN WITH A TWIST
Brennard M, Monroe K. University of Alabama, Bham, AL.Case Report: A 16 yo African-American female presented with one dayshortness of breath and chest pain, worsened by walking up stairs, deepbreathing and coughing. Pain was sharp and achy in her central chest. She felttired for the past month with intermittent nausea, constipation, and headache.She reported weight loss, menorrhagia, and right leg cramps, with no fever,trauma, rash, or travel. She denied tobacco, alcohol, or drug use, but admittedto sexual activity. Injections for contraception had been used, then contra-ceptive pills and patch were prescribed for menorrahgia. PMH includedtonsillectomy last year and wisdom teeth extraction 3 weeks ago. FH waspositive for breast cancer (grandmother) and SLE (a distant cousin). Vitalsigns were weight 72.5kg, HR 99, RR 30, BP 128/82, and oxygen saturationof 99% on 1 L of oxygen. She was cooperative and non-toxic,with mild in-creased work of breathing, no wheezing, and unable to speak in full sentences.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 377
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Chest pain was not reproducible. She had tachycardia with a regular rhythm,no murmur, good perfusion, and normal pulses. CXR reported no cardio-megaly with low lung volume and EKG had normal sinus rhythm and bor-derline QTc. Chest CT showed evidence of pulmonary thromboembolism(PTE). Venous blood gas had pH 7.31, pCO2 33, pO2 38, and HCO3 16.6.Other blood tests reveal WBC 8.8, Hgb 15, Hct 44, plts 288, normal elec-trolytes, though calculated bicarbonate 17, glucose 385, and normal renalfunction. Urine studies show 3+ glucose and 3+ ketones, 3+ blood, and nosign of infection. These findings suggested her tachypnea was due to PTE,but also complicated by diabetic ketoacidosis (DKA). Her HgbA1C was13.6%. Upon further questioning, she admitted to polydipsia and polyuria.Enoxaparin was given for 4 weeks and ultrasound revealed no distal venousthromboses. Insulin treatment and diabetes education was initiated. Literaturereview found no report of DKA presenting with PTE, however, it is knownthat DKA promotes a hypercoaguable state. Changes in hemodynamic fac-tors, plts, and vascular endothelium during DKA may explain the increasedrisk of clotting. Several authors report increased risk of venous thrombosiswhen central lines are placed in DKA patients. The additional use of contra-ceptive medicines in this patient likely contributed to a hypercoaguable statecausing chest pain with a twist.
19
EMERGENCY DEPARTMENT DIAGNOSIS OF DIETL’SCRISIS IN A 7 YEAR-OLD WITH ABDOMINAL PAIN
Burhop J, Clingenpeel J, Poirier MP. Children’s Hospital of the King’sDaughters, Eastern Virginia Medical School, Norfolk, VA.Case Report: A 7 year-old female was diagnosed with Dietl’s Crisis aftershe was evaluated for abdominal pain and vomiting. The previously healthypatient presented to our pediatric emergency department at a tertiary chil-dren’s hospital with a 12-day history of abdominal pain accompanied by3-days of uncontrolled nausea, vomiting and subjective fever. She had beenevaluated 5-days prior at an outside hospital and sent home with Miralax forconstipation. On assessment in our pediatric emergency room, vital signswere within normal limits for age. Physical examination was significant forgeneralized somnolence, anorexia, LUQ fullness, pain and tenderness exac-erbated by soft palpation without guarding. Urine studies obtained, along withelectrolytes, BUN and creatinine were all within normal parameters. A com-puted tomography scan of the abdomen and kidneys was performed showingleft kidney cortical thinning, with a renal pelvis measuring 8.6 cm along withureteropelvic junction obstruction and a crossing vessel suggesting the di-agnosis of Dietl’s Crisis.
Teaching PointsY Children with Dietl’s Crisis often suffer a delay in diagnosis, with the
clinical entity being under-diagnosed.Y Pain is caused by compression of aberrant artery crossing dilated kidney.Y There is not a clear criteria for evaluating UPJO in childhood abdominal
pain in the ED setting.Y It has been suggested that ultrasound may aid in the diagnosis.Y As renal parenchyma is typically preserved, and there is a pauacity of
associated urological complaints, once properly diagnosed, most patients arewell served by a pyeloplasty.
20
CASE OF SACROILIITIS
Sidhu N. Arkansas Childrens Hospital, Little Rock, AR.Case Report: A 23 month old female was admitted with a history of re-fusing to bear weight on her right leg. She had presented with a 1 day historyof pain in the right hip, limping, fever, and fussiness. Significant findings onexamination included a temperature of 38.1 C, tachycardia, pain on palpationof the posterior right hip and buttock. Plain radiographs of the pelvis andultrasonography of the hips were normal. Laboratory findings showed awhiteblood cell of 12200/KL with 60% segs and no bands, erythrocyte sedimen-tation rate of 61, and a normal C reactive protein. Patient was admitted forobservation and IV hydration.
By the 2nd day of hospitalization patients temperature spiked to 38.5 C,and she continued to refuse to bear weight on the right leg. Her CRP hadelevated to 79 mg/L and blood cultures were obtained. By the 3rd day ofhospitalization the patient was refusing to sit up and had developed tender-
ness with passive range of motion on her right side. A nuclear bone scandemonstrated increased three-phase activity in the right sacroiliac joint com-patible with sacroiliitis. Patient was started on Clindamycin (40mg/kg/day),with daily blood cultures. A MRI of the pelvis was obtained and demon-strated right sacroiliitis with extensive myositis involving the right iliacus,obturator internus, and the gluteal musculature at the sacroiliac joint.
Sacroiliitis is a rare disease in children representing only 1-2% of os-teoarticular infections. Typical features include limping gait, fever, and but-tock pain but these can be difficult to differentiate from other conditions suchas trauma, septic arthritis, or osteomyelitis. Considerable delay is recognizedbetween presentation and diagnosis. Delay in diagnosis can lead to compli-cations such as sepsis, abscess or sequestration formation, and long term jointdeformity. Plain radiographs and ultrasound are often negative. Isotope bonescanning is helpful for early diagnosis andMRI has the highest sensitivity andspecificity. Medical management includes early diagnosis, antibiotic ther-apy with coverage against Staphylococcus aureus, and bed rest.
By the 4th day on parenteral antibiotic therapy patient was afebrile,crawling in bed and bearing some weight on her right lower extremity. HerCRP was decreasing and all blood cultures were negative. Patient was dis-charged home on Clindamycin for 4 weeks.
21
ADDISON’S DISEASE: AN UNUSUAL CAUSE OFHYPONATREMIA
Malpani N, Eltaha C, Hasan R, Kaulfers A. University of South AlabamaChildren’s and Women’s Hospital, Mobile, AL.Case Report:BACKGROUND: Addison’s disease is an autoimmune destruction of theadrenal glands leading to cortisol and aldosterone deficiency. It is a chal-lenging diagnosis to make due to its vague symptoms of abdominal pain,vomiting, and mood changes. Furthermore, its rarity with a prevalence ofonly 90-140 cases/ million often leads clinicians to ignore the possibility ofthis disease.OBJECTIVE: To make clinician’s aware of a rare yet serious disease thatcan present with hyponatremia.CASE DESCRIPTION: 11 year old Caucasian previously healthy malewas found to have a sodium level of 112 mmol/L (normal 9136). Three weeksago, his parents divorced. Since then, he had daily crying spells/ emotionallability and progressive abdominal pain with anorexia, followed by recurrentepisodes of emesis. For the past three days, he consumed only water. On theday of admission, he had an episode of syncope.
During his course in the PICU, we attempted to correct his sodium withaggressive rehydration using 3% normal saline and oral salt tablets, with onlymodest improvement in the sodium level to 130 mmol/L after one week.Psychiatry was consulted and diagnosed the patient with mood disorder,and he was put on an antidepressant.
Once he had been rehydrated, his sodium levels remained low, so En-docrine was consulted. He was still reporting extreme weakness, dizziness onattempt to stand, and emotional lability. Physical exam revealed diffusebronzing of the skin. Cosyntropin stimulation test results: baseline ACTHlevel was elevated at 2,919 pg/ml (range 9-55) and aldosterone level wasundetectable. Cortisol at baseline was 3 mcg/dl, and at 60 minutes was stilllow at 3.4 mcg/dl. 21-hydroxylase antibody was elevated at 8.2 unit/ml,confirming Addison’s disease.RESULTS: The patient was started on 30 mg/m2/day of hydrocortisoneand 0.1 mg twice daily of fludrocortisone. His sodium level returned to nor-mal in three days and all of his symptoms resolved. He was taken off theantidepressant one week later and continues to do well as an outpatient.CONCLUSION: Addison’s disease is rare with symptoms mimickinggastrointestinal and psychiatric disorders. As a result, a high degree of sus-picion is needed to make the diagnosis.
22
ARE ALL PURPURIC RASHES WORRISOME?
Anderson T. UAB, Birmingham, AL.Case Report: 14 month-old previously healthy female presents with feverand rash. She had had 4 days of fever to 104 as well as rhinorrhea. She wasseen at her pediatrician’s office on the day prior to presentation where she
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
378 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

received a dose of IM ceftriaxone and was started on azithromycin. That nightshe developed a rash, so parents returned to the pediatrician’s office thefollowing day. He was concerned by the appearance of her rash and sent herto the hospital.
PE: Temp 98.9, HR 173, RR 40, BP 128/70. In general she appeareduncomfortable but nontoxic. ENT exam showed bilateral otitis media andrhinorrhea. No lesions on oral mucosa. CVexam showed tachycardia but goodperfusion. Lungs were clear. Abdomen was soft and nontender. Multiple tar-getoid purpuric plaques were seen on arms and legs. Ears, hands, and feet wereerythematous and edematous.
CBC, renal panel, UA, and ESR were wnl. CRP was 2.24. Admissionblood cultures remained negative. At admission she was given a 2nd doseof ceftriaxone as empiric treatment as well as to treat her otitis media. Shewas also started on IVFs because of tachycardia and poor po intake. Overthe next 24 hours, her rash progressed further to involve her face. Her trunkwas generally spared. The purpuric plaques remained fixed, rather thanwaxing and waning. Edema of hands and feet spread to arms and legs. Sheremained febrile, but never appeared toxic. After consulting with dermatologyand reviewing her clinical course, the diagnosis of acute hemorrhagic edemaof infancy (AHEI) was made. She was started on scheduled diphenhydramineand ranitidine. Within 48 hours, she began acting well.Discussion: AHEI is a rare, benign condition that can be mistaken for moreserious conditions if it goes unrecognized. It is a leukocytoclastic vasculi-tis thought to be triggered by infections, medications, or vaccinations. It isusually seen in children aged 4-24 months. It is characterized by fever, rash,and edema. Rash develops rapidly and is characterized by urticarial plaquesthat enlarge and become purpuric. The hallmark feature is edema of ears,hands, and feet that progresses to involve arms and legs. Rash resolves slowlyover 1-3 weeks. Use of antihistamines and steroids have been proposed to has-ten recovery. Recognition of this benign condition can prevent unnecessaryhospitalization and antibiotic treatment.
23
SUDDEN PURPURIC LESIONS IN A HEALTHY INFANT
Jethwa S, Sankararaman S, Mandava M, Raman V, Bocchini J. LSU HealthSciences Center, Shreveport, LA.Case Report: A 12-month-old previously healthy African-American femalepresented to the Emergency Department with a one day history of painlessbilateral swelling of the ears and urticaria-like lesions on her face and upperextremities. She did not have fever or recent illness, appetite and behaviorwere normal. A diagnosis of insect bites with cellulitis was made. She wassent home with diphenhydramine and clindamycin. She returned 8 hours laterwith new lesions and enlargement of the original lesions which had devel-oped a purplish discoloration. On re-examination, her vital signs were nor-mal. The ear swelling had worsened, the cutaneous lesions were larger,purpuric and palpable (Figure 1). She did not have mucosal involvement.After completing a work up for sepsis, antibiotic therapy was initiated and thepatient was admitted. Laboratory evaluations were within normal limits. Bloodand cerebrospinal fluid cultures were negative. A biopsy of one of the lesionsrevealed leucocytoclastic vasculitis of small vessels confirming the diagno-sis of acute hemorrhagic edema of infancy (AHEI). The following day herlesions and swelling of the ears began to improve. She was discharged andwithin 1 week all symptoms resolved.Discussion: AHEI or infantile Henoch-Schonlein purpura is a rare selflimited benign disorder of young children characterized by painless edema of
the face and/or extremities with typical purpuric lesions. In view of the ex-treme rarity of this condition, the diagnosis is usually delayed. Awareness ofthis condition is important because prompt differentiation from the otherserious diseases presenting with palpable purpura, such as meningococcemiaand rickettsial infections, is required.
24
HEREDITARY ANGIOEDEMA PRESENTING ASCOLOCOLONIC INTUSSUSCEPTION
Mitchell H. Univeristy of Alabama at Birmingham, Birmingham, AL.Case Report: This was a 10year old female with a history of mild autismwho presented to the emergency department with a chief complaint of ab-dominal pain. She had had 48 hours of nonbloody loose stools three daysprior to presentation which resolved. The day of presentation she had 2 to 3episodes of nonbloody, nonbilious emesis with severe abdominal pain in herperiumbilical region. While obtaining the history, the father noted that thepatient’s mother carried a diagnosis of hereditary angioedema and had simi-lar episodes to the patient’s symptoms of abdominal pain with flares of herangioedema. The patient had never been tested or diagnosed with this dis-order so a full work up was done in the emergency department. Physical examwas significant for a soft, nondistended abdomen that was moderately tenderin the periumbilical region with voluntary guarding present. Labs were sig-nificant for a white blood cell count of 24K with 87% neutrophils but other-wise other labs including a CMP, ESR, CRP, lipase were normal. An abdominalCT with contrast was obtained that showed extensive bowel wall edema in-volving both the large and small bowel, mucosal hyperenhancement and muralstratification. In addition, a small area of colocolonic intussusception wasseen in the transverse colon. Surgery was consulted and after their reviewof the CT they requested an air enema to reduce the intussusception. Therewas a detailed discussion between the surgeon and the radiologist about therisks and benefits of this procedure given the significant findings of bowelwall edema on the CTand the decision wasmade to proceed with the air enema.The air enema successfully reduced the intussusception and there were nocomplications. Given the CT findings the most likely diagnosis at this pointseemed to be a new diagnosis of hereditary angioedema so the on call allergy/immunology fellow was consulted who recommended checking a C4 leveland C-1 inhibitor level. The patient was admitted to the surgery service. Shehad resolution of her pain in the hospital and was discharged home after48 hours. Labs came back showing a C4 level of G2 (normal range 8-44) andC1 inhibitor level of 20 (normal is 968 and abnormal is G40) which wereconsistent with a diagnosis of hereditary angioedema. Patient is currentlybeing followed in our immunology clinic.
25
4 Y.O. WITH ATAXIA LAURA A. WRIGHT MD, LADONNACREWS MD, GRACE HUNDLEY MD
Wright L1, Crews L1, Hundley G2. 1USA, Mobile, AL and 2Universityof South Alabama, Mobile, AL.Case Report: Sydenham’s chorea (SC) is the neurological manifestationfollowing an untreated streptococcal infection. This disorder is characterizedby the stereotypical choreiform movements, emotional lability and muscleweakness.
This case report highlights an unusual neurological manifestation and thechallenge of diagnosing Sydenham’s chorea.
A 4 year old female presented with a two day history of seizure likeactivity with head bobbing and arm and leg shaking. There was no loss ofconsciousness or incontinence and she gradually lost the ability to walk.There was no indication of recent infection. Fever, sore throat and joint painwere denied. Mom reported emotional lability for the last 2 months whichworsened with the presenting symptoms. She had stable vital signs and thecardiopulmonary exam was normal. There was head bobbing with continual,irregular, uncontrolled movements of her arms and legs. She was ataxic andwas unable to sit or walk unassisted. While assisted, she had a wide based gaitwith irregular, unsteady steps. Her ataxia did not improve whether her eyeswere open or closed. She was unable to do the finger nose test.
A complete blood cell count and differential, CRP and ESR were nor-mal. A continuous EEG, lumbar puncture with cerebrospinal fluid studies
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 379
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

and MRI with and without contrast were unremarkable. Anti DNAse andASO titers were 447 and 379 respectively.
SC is the sequela of untreated streptococcal infections. Ten to fifteenpercent of children present with emotional lability and uncontrolled move-ments alone. With a presumed autoimmune etiology, treatment now focuseson immune regulation. IVIG, 1g/kg per day for two days was begun. Withintwo days the head bobbing had resolved. She was able to walk unassisted andher emotional lability had improved.
When a child presents to a physician with chief complaint of abnormalmovements and the common etiologies have been ruled out, it is important toremember atypical presentations of SC. In patients with debilitating neuro-logical symptoms, the use of intravenous immunoglobulins should be considered.
26
ABDOMINAL PAIN TO HEART FAILURE: PURULENTPERICARDITIS IN A HEALTHY CHILD
Rowe RK, Rajan D, Gaviria C, Garcia C. University of Texas Southwestern,Dallas, TX.Case Report: A 13 month old previously healthy male, except for a his-tory of recurrent otitis media, presented with 1 day of fever, decreased activityand appetite, and difficulty breathing. Parents also described symptoms oforthopnea the night prior to admission. The day of admission he presented tohis pediatrician, and was referred to the emergency department with concernfor acute abdominal process. On exam, he was fussy, tachycardic, tachypneic,grunting, and liver was palpable 3cm below the right costal margin. Labo-ratory evaluation was significant for elevated white blood cells (18k/mm3)with prominent left shift (60% neutrophils, 11% bands) and a CRP of 19.6,all indicative of an infectious or inflammatory process. Evaluation for ab-dominal causes including ultrasound and CT abdomen revealed a normalabdomen but was notable for pericardial effusion. He was transferred to theICU where pulse oximeter tracing was consistent with pulsus paradoxus, EKGshowed diffuse ST elevation, and echocardiogram was consistent with tampo-nade physiology. Bedside pericardiocentesis was productive of purulent fluid(69k nucleated cells/mm3, 78% neutrophils, 20% bands), and was positive formethicillin-resistant Staphylococcus aureus (MRSA) (susceptible to genta-micin, trimethoprim/sulfamethoxazole, vancomycin, and clindamycin). Heultimately had pericardial window placement and received a 7 week courseof antibiotics, including 2 weeks of parenteral and 5 weeks of oral therapy.
MRSA infection most commonly presents as skin and soft tissue infec-tions, often easy to recognize and treat with oral antibiotics. However, in-vasive infections are frequently seen in the pediatric population, includingosteomyelitis, pyomyositis, pneumonia/empyema, or deep abscesses. Whilepathogenesis is not clear, invasive infections are thought to begin with asuperficial infection such as an abscess or cellulitis, which seeds deeper tissuesby contiguous spread or transient bacteremia. MRSA infection rarely presentsas an isolated pericarditis, most commonly found in children with underlyinglung or cardiac pathologies, or post-operatively. However in this case, pu-rulent pericarditis in a healthy child is even more unusual and often requires ahigh level of suspicion for diagnosis and timely management.
27
CRESCENTIC GLOMERULONEPHRITIS IN PEDIATRICPATIENT
McLaughlin N1, Hirsh S2, El-Dahr S1, Meleg-Smith S2, Yosypiv I1. 1TulaneSOM, New Orleans, LA and 2Tulane, New Orleans, LA.Case Report: A 6 year-old multi-racial female presented to local ER withpainless gross hematuria. Based on presence of numerous WBCs and RBCsin the urine, patient was treated for presumptive UTI. Persistence of grosshematuria and onset of emesis required repeat evaluation at local ER. Ele-vated serum creatinine of 1.4 mg/dL and low albumin of 2.0 mg/dL promptednephrology consultation with admission to tertiary care center. Physical ex-amination revealed mild periorbital and lower extremity edema, blood pres-sure of 120/83 mmHg. Urinalysis showed numerous RBCs, WBCs, cellular castsand protein/creatinine ratio of 12. Blood tests showed depressed C3 com-plement (30 mg/dL), normal C4 (40 mg/dL), elevated total/LDL cholesteroland triglycerides, normal ANA and ASO titers, elevated atypical p-ANCA(1:320), and negative HepB and C serologies. A diagnosis of acute glomer-ulonephritis (GN) with nephrotic syndrome was established and therapy with
high-dose oral prednisone, diuretics and a calcium channel blocker waspromptly initiated. Light microscopy of the renal biopsy specimen revealedpresence of cellular crescents in 25% of glomeruli, abundant neutrophils incapillary loops and dilated tubules. IF showed scarce granular deposits ofIgG in the capillary loops and abundant mesangial C3. Acute postinfectious(APIGN) and membranoproliferative (MPGN) GN were considered initially.EM demonstrated subepithelial ‘‘lump’’-type electron dense deposits (EDD),focal podocyte foot process effacement and occasional subendothelial EDD.Gradual normalization of renal function and C3 complement levels promptedavoidance of more aggressive immunosuppressive treatment with pulsesteroids/cyclophosphamide or in-depth evaluation of the alternative pathwayof complement cascade to exclude C3 glomerulopathy (C3G). Nephrologistsshould consider C3G in a child with acute GN, evidence of dysregulation ofthe alternative and terminal pathway of complement cascade, and suben-dothelial EDD. The presence of atypical p-ANCA does not indicate a poorprognosis in APIGN.
28
ERYTHEMA MULTIFORME PRESENTING AS KAWASAKIDISEASE
Korah-Sedgwick M1,2, Dimitriades V1,3. 1LSU Health Sciences Center, NewOrleans, LA; 2LSU Health Sciences Center, New Orleans, LA and 3LSU HealthSciences Center, New Orleans, LA.Case Report: A 10yo previously healthy female presented with a history offever, malaise, and dry cough for approximately one week. A three day his-tory of facial edema and conjunctivitis was accompanied by a diffusely pruritic,papular rash on her face and trunk, now spreading to her palms and soles,with new-onset oral excoriations. Initial treatment of symptoms prior to onsetof rash included Dextromethorphan and Ibuprofen, both of which the patienthad previously tolerated without incident. Physical exam revealed vaginaland oral ulcerations, significant exudative conjunctivitis, and diffuse macu-lopapular crusting lesions. Laboratory evaluation showed a leukocytosis withelevated ESR and CRP and a chest X-ray showed bilateral interstitial infil-trates indicative of lower respiratory viral infection.With five diagnostic criteriamet for Kawasaki disease, the patient was admitted and IVIG with aspirintherapy was initiated. 2D Echocardiogram at that time was within normallimits. Despite treatment, the patient continued to have fever, conjunctivitis,and increasing oral lesions. Her rash became violaceous and targetoid withcentral clearing and a presumptive diagnosis of Erythema Multiforme (EM)Major was made. Given her history of cough prior to onset of the rash,Mycoplasma was assumed to be a likely cause and a course of Azithromycinwas initiated empirically. Biopsy confirmed necrotic keratinocytes and dermalpapillary edema consistent with EM, and serology later confirmed positiv-ity for Mycoplasma IgM antibodies. Management included ophthalmologicmonitoring for keratitis and ulcerations, pain management for the oral le-sions, and topical antimicrobials to prevent mucosal superinfection. Afterseveral days of supportive care, the patient was discharged home to com-plete her antibiotic course with no further issues.Discussion: Erythema Multiforme Major is an acute immune-mediatedprocess with cutaneous target-like lesions and mucosal involvement. Infectionis the cause in up to 90% of cases and the clinical course is often self-limitedwith treatment based on the degree of mucosal membrane involvement andthe necessity for pain management.
29
GASTROINTESTINAL OBSTRUCTION AND SMASYNDROME SECONDARY TO THYROTOXICOSIS
Malhotra S1, Felipe D2. 1Tulane University, New Orleans, LA and 2OchsnerMedical Center, New Orleans, LA.Case Report: A 14 year old girl with previous history of prematurity pre-sented with multiple bouts of nausea, vomiting, diffuse abdominal pain, anddistension. Pancreatic enzymes were elevated with otherwise normal liverfunction tests. CT Scan of the abdomen showed gastrointestinal obstructionwith findings consistent with Superior Mesenteric Artery Syndrome. Place-ment of nasogastric tube and return of greater than 1,000 mL of bilious fluidinitially relieved her abdominal pain, distension, and nausea. Incidental thy-roid function tests performed on an outpatient basis secondary to goiter onphysical exam revealed Grave’s Disease. Repeat thyroid function tests showed
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
380 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

similar TSH and free T4 levels as well as significantly elevated total T3 levels.Further history and growth chart review showed weight loss over severalmonths. Patient was started on IV Steroids, Propylthiouracil, and Atenolol.Liver function tests demonstrated acute elevation post Propylthiouracil ad-ministration which was promptly switched to Methimazole. Over the courseof five days, lab values showed decreased free T4 and total T3 Levels. Patientrequired total parenteral nutrition and intralipids while feeds were increasedsecondary to persistent abdominal distension and elevated pancreatic en-zymes. Superior mesenteric artery (SMA) syndrome is an uncommon butwell recognized entity characterized by compression of either the third ortransverse portion of the duodenum between the aorta and the superiormesenteric artery. Profound weight loss with reduced omental fat is the mostcommon cause for this phenomenon which has been described in childrenwith anorexia nervosa, spinal cord and burn injuries, malabsorption syn-dromes, and trauma. Our patient’s case is one of the few reported cases todemonstrate an association between rapid weight loss due to hyperthyroidismand SMA Syndrome. Our patient’s gastrointestinal symptoms were the prom-inent presenting feature of the thyrotoxicosis. Alleviation of symptoms oc-curred with the initiation of antithyroid medications, steroids, and a course ofparenteral nutrition. Although rare, hyperthyroidism should be considered inthe differential diagnosis of SMA Syndrome in the pediatric population.
30
CAT SCRATCH FEVER: A CASE OF DISSEMINATEDBARTONELLA INFECTION MIMICKING MALIGNANCY
Moll C, Huckabee M. UAMS, Little Rock, AR.Case Report: A previously healthy 3-year-old girl presented with 4-weekhistory of fever and back pain. Fever was present most days and ranged from102-104F with back pain starting after fever onset. She also had episodesof leg pain and would refuse to bear weight. During this illness, she receivedamoxicillin-clavulanate, clindamycin and azithromycin without improvement.At admission, she had no bony tenderness and full range of motion of alljoints without pain. She had a 1.5 cm nontender right axillary lymph node butno other lymphadenopathy. Admission labs showed CRP 85mg/L, ESR 973mm/hr, WBC 12,300/uL with benign differential, hematocrit 24.6%, plate-lets 555,000/uL, and negative blood culture. MRI showed enhancement at theL3 vertebral body, erector spinae muscles, posterior epidural tissue, iliacbones, right acetabulum, and left proximal femur and also identified lesionsin the liver and spleen. This was read as concerning for Langerhans cellhistiocytosis. The Hematology/Oncology and Infectious Diseases teams wereconsulted and recommended further imaging, tissue biopsy, and additionalserological studies. Labs drawn included uric acid, LDH, Bartonella serology,HIV, CPK, retic, and LFTs. Symptoms persisted throughout hospitalization.Then on day 6, her Bartonella serology returned with IgG titer 1:512 and IgMtiter 1:32 leading to a diagnosis of disseminated Bartonella. The family didnote exposure to adult cats; no bites or scratches were reported. She wasdischarged with a 6-week course of rifampin and azithromycin. She was seen inID Clinic for follow-up with complete resolution of symptoms.
Bartonella henselae is known to cause cat scratch disease, typicallymanifested as self-limited fever and lymphadenopathy. Atypical presentationsinclude prolonged fever, pseudomalignancy, and diffuse organ system in-volvement. This patient presented a diagnostic challenge because her pre-sentation and MRI were consistent with malignancy, specifically Langerhanscell histiocytosis. Although this patient’s symptoms were alarming for ma-lignancy, infectious causes remained in the differential given her presentation.While most cases of Bartonella require no treatment, this patient’s diffusedisease and duration of symptoms required treatment.
Case Reports in Cardiovascular Medicine
2:00 PMThursday, February 21, 201331
ACUTE MYOCARDIAL INFARCTION IN A YOUNG FEMALEBODYBUILDER WITH ULCERATIVE COLITIS ANDCHRONIC ANABOLIC STEROID USE
Garcia Gordo PO, Martinez Toro J, Martinez Ojeda J, Figueroa Navarro R.University of Puerto Rico School of Medicine, San Juan, Puerto Rico.
Case Report: 23 year-old female bodybuilder with history of chronic an-abolic steroid use and a recent diagnosis of ulcerative colitis who was ad-mitted to our institution with an acute anterior myocardial infarction due toocclusion of the medial left anterior descending coronary artery. She had noother cardiovascular risk factors. She had been using stanozolol, growth hor-mone, drostanolone propionate, and anastrozole for period of 7 years.
The physical examination revealed no abnormalities. The ECG showedSTelevation in the anterior leads. Laboratories were unremarkable except forelevated cardiac markers. She underwent successful primary percutaneouscoronary intervention and bare metal stenting for a total occlusion of themedial left anterior descending coronary artery. Echocardiogram showed alarge apical thrombus. She was discharged home 5 days after admission onwarfarin and secondary prevention medications. Four weeks later a cardiacMRI showed decrease in size of apical thrombus.
Anabolic androgenic steroids abuse has been linked to a variety of car-diovascular side effects. Myocardial infarction has been the most commonevent. Ulcerative colitis has also been associated with an increase risk forarterial and venous thrombosis. To our knowledge this is the first report ofa young female patient with ulcerative colitis and chronic anabolic steroid useassociated with an acute myocardial infarction in the absence of cardiovas-cular risk factors.
32
TETRALOGY OF FALLOT FEIGNING INFLAMMATORYBOWEL DISEASE
Al Janabi M, Ismaael T, Smalligan RD. Texas Tech University Health SciencesCenter, Amarillo, TX.Case Report: A 50yo male presented with worsening abdominal pain andbloody diarrhea. He had recently arrived from Mexico where he worked on afarm. He denied fever, sweats, chills, N/V. PMH negative; meds: none. Famhistory: neg for IBD. P/S history: neg for EtOH, drugs and smoking. PE: BP130/80, HR 90, RR 20, O2 sats 88% on RA, lips cyanotic, JVP elevated,lungs clear, heart: 3/6 systolic murmur, abd distended and tender, clubbing/cyanosis in fingers/toes and 2+ edema. WBC 4.4, Hgb 19.8, Cr 0.8, elec-trolytes, LFTs normal, alb 2.7, BNP 90, stool O&P neg, occult blood pos, C.diff neg, ESR 2. EKG: NSR with RVH. CXR: nl heart, prominent left hilumread as ‘‘worrisome for mass or adenopathy,’’ o/w nl lungs. Abd CT - severebowel wall thickening from prox sigmoid to rectum. TTE: EF 55%, enlarged RV,elevated RV pressures, no valvular abnormalities. Colonoscopy: colitis fromrectum to proximal sigmoid; biopsy: ischemia. PFTs: decreased DLCO c/wCV process, V/Q scan: low prob for PE. Right heart cath combined withcareful review of the TTE showed findings c/w Tetralogy of Fallot.Discussion: This case was a diagnostic challenge because the patient’s moststriking features on H&P were abd pain and bloody stools. His recent ar-rival from Mexico also raised suspicion of infectious colitis. The contiguousthickened bowel on the CT from the rectum to the sigmoid was suggestive ofulcerative colitis (inflammatory markers were not immediately available).Clinical findings pointing to the CV system including the low O2 sats,
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 381
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.
cyanosis, clubbing, and murmur prompted simultaneous workup of what wasfelt to be a separate issue. The CXR being ‘‘suspicious’’ was also distractingat the outset. The almost simultaneous return of the right heart cath, the re-examined TTE, the negative inflammatory and infectious lab results, and thecolon biopsy results with ischemia brought the case to a satisfying conclu-sion: previously undiagnosed Tetralogy of Fallot in a 50yo man from Mexicowith acute ischemic colitis. On more detailed questioning in Spanish thepatient admitted to what sounded like mild ‘‘tet’’spells as a child and decreasedexercise tolerance in the fields of Mexico in recent years. This case remindsphysicians to make every effort to seek a unifying diagnosis despite seem-ingly disparate features early on.
33
NEW-ONSET BRADYCARDIA IN RELAPSING-REMITTINGMULTIPLE SCLEROSIS
Elamin MB, Omer A, Islam AM, Ahmed M. Texas Tech University HealthSciences Center, Amarillo, TX.Case Report: Cardiovascular (CV) dysfunction in acute multiple sclerosis(MS) is a rare finding. The exact mechanism related to CValteration in MS isnot clearly defined. In this report, we are present a case of acute onset brady-cardia in a young female with relapsing-remitting MS without the pres-ence of any other factors affecting CV function.Case: A 29yo female with relapsing-remitting MS presented with slurredspeech and difficulty swallowing. Her heart rate was 83 per minute initiallywith a regular rhythm. Neurological exam revealed mild right upper motorneuron facial weakness and upper limb weakness. Magnetic resonance im-aging of the brain revealed white matter lesions bilaterally including the righthemisphere of the cerebellum. She was started on high doses of steroids.During her hospitalization she acutely became diaphoretic and light-headedwhile lying down. Her heart rate was 35-40 per minute without orthostatic hy-potension or syncope. Multiple EKGs showed sinus bradycardia and troponin-Iresults were negative.The patient recovered gradually without any intervention.Discussion: Symptoms related to alterations of the autonomic nervous sys-tem are frequent in MS. The frequency of abnormal findings in tests for theCV autonomic system varies due to the lack of standardized test perfor-mance and different cut-off values used. Pentland et al. showed nearly 19%of patients with MS had abnormalities in CV reflexes. Flachenecker et al.found abnormal responses in 40% of MS patients with a statistically signif-icant involvement of the sympathetic vasomotor system. Moreover, para-sympathetic dysfunction was closely related to the progression of disabilityin patients with MS. In a study by Anema et al, the blood pressure responseto standing was abnormal in 13% of MS patients and heart rate responseto standing was abnormal in 28%. On deep breathing, 36% of MS patientsshowed abnormal heart rate changes. Vita et al. showed in his study that therewas a significant association between the presence of autonomic dysfunctionand clinical (P G 0.02) and MRI (P G 0.005) evidence of brainstem lesions.Our case reminds internists to be alert for CVautonomic dysfunction in theirpatients with MS, especially during times of progression or flare ups of theirunderlying disease process.
34
LATE-ONSET PRESENTATION OF COARCTATION OFTHE AORTA
Mabry C, Yandle G, Erbil J, Engel LS, Happel K. LSU Health SciencesCenter, New Orleans, LA.Case Report:Introduction: Coarctation of the aorta (coarctation) is most commonly acongenital abnormality that involves stenosis of the proximal descendingthoracic aorta. This process accounts for about 7% of all congenital heartdiseases and occurs twice as frequently in men. It should always be ruled outif other rare conditions like bicuspid aortic valve, Turner’s syndrome, ven-tricular septal defect, or aneurysms of the circle of Willis are present. Di-agnosis of the disease is critical as the mortality rate is high in poorlymanaged patients. The average survival is approximately 35 years with75% mortality by age 46 without surgical intervention. The major mani-festation is a difference in systolic blood pressure between the upper and
lower extremities (usually upper extremity hypertension) with little differ-ence in the diastolic pressures. In addition to this, renal hypoperfusionmay increase renin secretion resulting in volume expansion and furtherhypertension.Case: A 61-year-old man with a past medical history of chronic, uncon-trolled hypertension received a non-contrasted Computed Tomography (CT)of the chest and abdomen to investigate for possible Conn’s Syndrome. Thisnoncontrast study showed some areas of nodularity around the vertebralbodies bilaterally with extension into the posterior mediastinal region. A CTof the chest with intravenous contrast showed a narrowing in the region ofthe aortic isthmus consistent with aortic coarctation. The extent of collateralvessel dilation inferred a hemodynamically significant finding.Discussion: With the advancements in imaging techniques in recent years,radiologic assessments have become the predominant tool to diagnose an aor-tic coarctation. The gold standard for diagnosing aortic coarctation usingimaging is with either magnetic resonance imaging (MRI) or computed to-mography (CT). As with our patient, these modalities allow for clear visu-alization of the severity of the coarctation as well as any collateral vesselsthat have developed. From our experience, a CT with intravenous contrastshould always be performed if this abnormality is suspected.
35
A STRIKING CASE OF CONSTRICTIVE PERICARDITIS
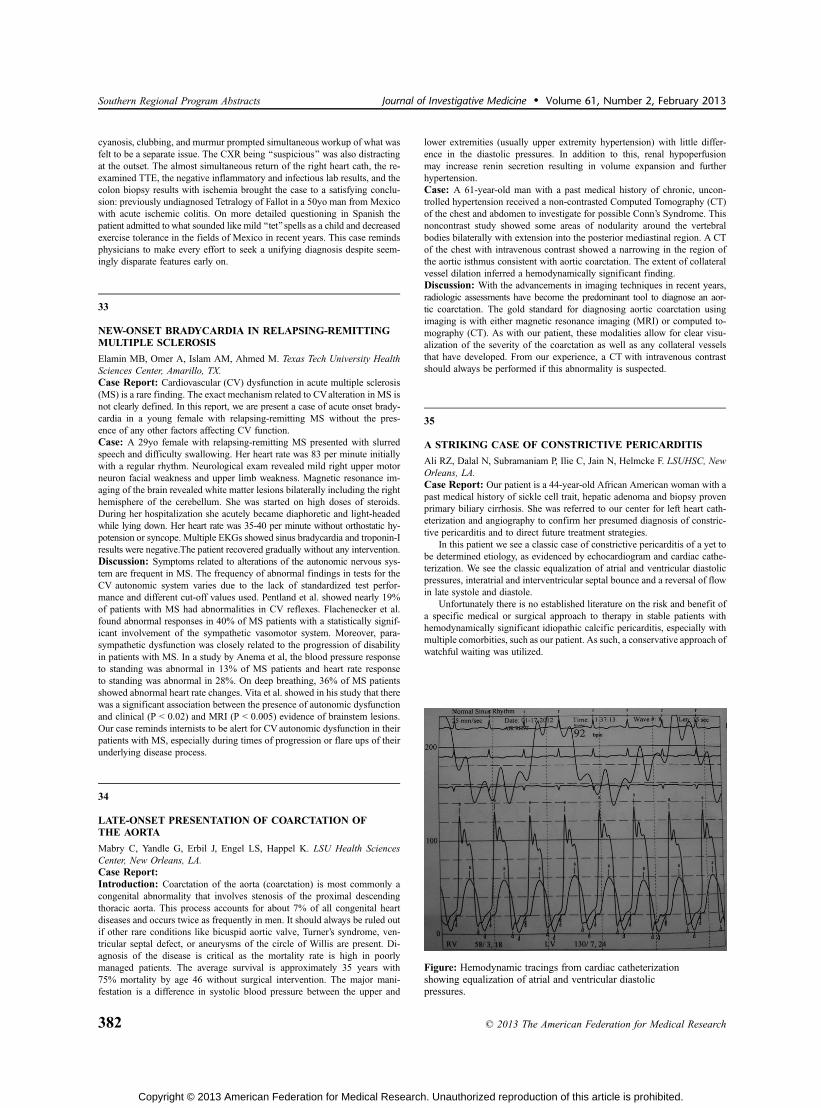
Ali RZ, Dalal N, Subramaniam P, Ilie C, Jain N, Helmcke F. LSUHSC, NewOrleans, LA.Case Report: Our patient is a 44-year-old African American woman with apast medical history of sickle cell trait, hepatic adenoma and biopsy provenprimary biliary cirrhosis. She was referred to our center for left heart cath-eterization and angiography to confirm her presumed diagnosis of constric-tive pericarditis and to direct future treatment strategies.
In this patient we see a classic case of constrictive pericarditis of a yet tobe determined etiology, as evidenced by echocardiogram and cardiac cathe-terization. We see the classic equalization of atrial and ventricular diastolicpressures, interatrial and interventricular septal bounce and a reversal of flowin late systole and diastole.
Unfortunately there is no established literature on the risk and benefit ofa specific medical or surgical approach to therapy in stable patients withhemodynamically significant idiopathic calcific pericarditis, especially withmultiple comorbities, such as our patient. As such, a conservative approach ofwatchful waiting was utilized.
Figure: Hemodynamic tracings from cardiac catheterizationshowing equalization of atrial and ventricular diastolicpressures.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
382 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

36
ACUTE OR CHRONIC HYPERKALEMIA AND THEAPPEARANCE OF SYMPTOMATIC BRADYCARDIAWITHJUNCTIONAL RHYTHM
Seawell MR, Alsafwah S, Weber KT. University of Tennessee Health ScienceCenter, Memphis, TN.Case Report: Purpose: Irrespective of its etiologic origins, hyperkalemiais a serious pathophysiologic disorder whose adverse outcomes are mostclosely related to disturbances in cardiac conduction and rhythm. The elec-trocardiogram (ECG) provides sentinel information on cardiac toxicity. Itsinitial manifestations, which appear when serum K+ ranges between 5.5-8.0 mmol/L, include tall, narrow peaked Twaves. Other less well-appreciatedcardiac manifestations for this level of hyperkalemia include lost P waves,based on the suppression of the atrial myocyte activity, with emergence ofa junctional rhythm. Herein, we present two cases wherein the cardiologyservice was consulted for patients having symptomatic bradycardia with ajunctional rhythm and which were presenting features of acute and chronichyperkalemia.Case Reports: Case 1. A 54-year-old woman with known hypertension,treated with a thiazide diuretic and atenolol, was hospitalized because of aurinary tract infection and started on intravenous antibiotics. She was notedto have hypokalemia (3.4 mmol/L) and was given supplemental intravenousKCl. Inadvertent iatrogenic hyperkalemia (7.9 mmol/L) occurred and was ac-companied by hypotension, bradycardia and junctional rhythm on her ECG.Hyperkalemia was promptly corrected and normal sinus rhythm restored withhemodynamic stability.
Case 2. A 67-year-old woman with end-stage renal disease on hemodi-alysis presented to the Emergency Department with dizziness and fatigueof several days’ duration. She was found to be hypotensive with a pulse of36 bpm and to have hyperkalemia (7.7 mmol/L). Temporary pacemaker place-ment with incremental, regulated heart rate and stabilization in blood pressurepermitted hemodialysis with correction of her hyperkalemia. Once corrected,her heart rate improved to 80 bpm with restoration of normal sinus rhythmand resolution of the junctional rhythm to permit pacemaker removal.Conclusions: Hyperkalemia, whether acute or gradual in onset, can lead tosuppression of atrial activity with lost electrocardiographic P waves andemergence of a junctional rhythm with consequent symptomatic bradycardiaand hypotension.
37
SYNCOPE AS A PRESENTATION OF INTRAVENOUSLEIOMYOMAWITH RIGHT VENTRICULAR OUTFLOWTRACT OBSTRUCTION
Jimenez L1, Calderon R1, Osterman A2, Quintana C3. 1University of PuertoRico School of Medicine, San Juan, Puerto Rico; 2University of Puerto RicoSchool of Medicine, San Juan, Puerto Rico and 3Cardiovascular Center ofPuerto Rico, San Juan, Puerto Rico.Case Report: A 40-year-old female with history of arterial hypertensionpresented with an episode of syncope during sexual intercourse. She referredseven months history of progressive dyspnea on exertion, palpitations andbilateral leg swelling. On physical examination, systolic murmur 3/6 andtumor plop were heard on the left lower sternal border.
An echocardiogram revealed a right atrial mass that prolapsed throughthe tricuspid valve into the right ventricle during diastole and into the inferiorvena cava during systole. A cardiac MRI revealed an elongated intravasculartubular mass extending from the inferior vena cava into the right atrium, rightventricle and pulmonary arteries. A computed tomography of the abdomenand pelvis revealed a complex multicystic left pelvic mass. Surgical excisionof the intracardiac mass was done with subsequent pathological identifica-tion of intravascular leiomyomatosis.
Benign leiomyomas are extremely common uterine tumors but on veryrare occasions may exhibit an unusual growth pattern characterized by in-travascular proliferation with extension into the right cardiac chambers viathe inferior vena cava. Less than one hundred cases have been reported in theliterature and only ten percent of these have intracardiac extension. Potentialcomplications like right ventricular outflow tract obstruction may causesyncopal episodes, as in this case.
Joint Plenary Poster SessionAdolescent Medicine and Pediatrics
5:00 PMThursday, February 21, 201338
A GANG OF VICIOUS ULCERS
Adimora-Nweke DE. Tulane University Health Science Center, New Orleans, LA.Case Report: A 16 year old obese girl with presented to the emergencydepartment with two-week history of recurrent and rapidly developing skinulcers. She described tender red pustules scattered mostly in her upper thigh/groin, left axilla, and abdomen. The pustules erupted within days of ap-pearing, expressing foul smelling discharge and thereafter leaving painfululcers. She also complained of bloody diarrhea with diffuse abdominal painand occasional subjective fevers for two weeks. She reported no previoushistory of ulcers, preceding trauma, spider bite, recent antibiotic or immu-nosuppressive treatment.
Admission sedimentation rate was elevated at 40 mm/hr. HIV was neg-ative along with ulcer wound cultures and stool studies. After dermatologi-cal consultation, the patient was diagnosed with pyoderma gangrenosum. Inpatient colonoscopy confirmed pancolitis consistent with ulcerative colitis.She was aggressively treated with high dose Prednisone, Mesalamine, andInfliximab. Two weeks later, the ulcers had epithelialized.
Inflammatory bowel disease is a diagnosis familiar to the pediatric hos-pitalist with 20% of cases presenting in pediatric years.1 Conversely, pyo-derma gangrenosum is an uncommon cutaneous manifestation occurring inless than 1% of IBD patients.2 This neutrophilic dermatosis, once thought tobe pathognomic of ulcerative colitis, is now seen with various systemic andlocalized conditions.
PG was first described as pustular lesions that progress to ulceration. Itis diagnosed based on clinical history, presentation and by excluding othercauses of cutaneous ulcerations such as infection, insect bite, self-inflictedulceration, vasculitis, malignancy, and vascular insufficiency. When associ-ated with IBD, PG may or may not parallel flares in bowel disease.
Treatment of new onset skin ulcers in the setting of a new inflammatorybowel disease diagnosis is a complex issue as exclusion of infectious causesof ulcers remains a major initial goal. Detailed history and laboratory work
Figure: Calcifications seen under fluorscopy
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 383
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

are needed to exclude other concerning differential diagnosis for new onsetcutaneous ulcers; Nevertheless, corticosteroid therapy must be initiated to ad-dress IBD and such corticosteroid treatment could then worsen skin ulcers ofinfectious etiology. Once other diagnosis have been excluded, PG can thenbe treated with high dose corticosteroids.
39
CHANGING PERCEPTIONS OF CHILDHOOD OBESITY IN AMEMPHIS RESIDENT CLINIC
Beeman G, Hare M. University of Tennessee Health Science Center,Memphis, TN.Purpose of Study: To assess differences in parental and provider percep-tions of childhood obesity in Memphis, TN, before and after community-wide efforts to educate and intervene in the obesity epidemic.Methods Used: This is cross-sectional study using rater judgment and an-thropometric data collected in August of 2003 and August of 2011. In theUniversity of Tennessee Health Science Center resident practice at LeBonheurChildren’s Hospital, children ages 2 - 17 who were scheduled for a healthmaintenance visit were weighed and measured in the usual manner. Beforethe anthropometric data were graphed and body mass index (BMI) calculated,parents and providers (nurses and resident physicians) were asked to rateperceptions of the child’s weight category percentiles - underweight (G5),normal (95 and G85), overweight (985 and G95), obese (995). Lay termi-nology was provided for the parents.Summary of Results: Participants included 185 African American (AA)children, 95 boys (51%) and 90 girls (49%) in 2003, and 180 AA children,91 boys (51%) and 88 girls (49%) in 2011. Age distribution and socioeco-nomic status were similar in both groups. The percentage of children with aBMI 985 percentile was 30% in 2003 and increased to 46% in 2011.Conclusions: In this small sample of AA children, the rate of childhoodobesity increased from 2003 to 2011. Despite broad community efforts, obe-sity in individual children is not recognized consistently by parents and healthcareprofessionals. Since awareness is often the first step to successful interven-tion, a different community approach is needed.
40
SCREENING FOR ASYMPTOMATIC CHLAMYDIA INPATIENTS WITH SICKLE CELL DISEASE
Bluett-Mills GM, Kanter-Washko J. Tulane University, New Orleans, LA.Purpose of Study: Louisiana has one of the highest rates of chlamydia, aneasily identifiable and treatable STI, in the United States. Chlamydia rates aredisproportionately higher among older teenagers, young adults and AfricanAmerican patients. The CDC and Louisiana state department of health recom-mend annual screening for asymptomatic disease in at risk patients.
We hypothesize that patients with a chronic disease, such as sickle celldisease (SCD), are not undergoing necessary age-based screening as a resultof forgoing primary care visits due frequent specialist visits with physicianswho may be unaware of primary screening recommendations.
Methods Used: Over a twelve-month period, patients with SCD betweenthe ages of 15-30 were screened for asymptomatic chlamydia by urine PCRduring visits to the pediatric or adult sickle cell clinic, sickle cell day hospital, oremergency department. Sickle cell disease patients of all genotypes (HbSS,HbSC, HBS-thalassemia) presenting for routine, comprehensive care or vaso-occlusive crisis were eligible for evaluation. Pregnant women and cognitivelyimpaired patients were excluded. Screening data from primary care clinicswas excluded from analysis.Summary of Results: Of 96 patients eligible patients who were identified,34 patients successfully underwent chlamydia testing during the study period.4/34 patients(11.8%) tested positive for chlamydia. Only one patient with apositive test had symptoms at the time of testing. Of the 3 asymptomaticpatients with a positive test, 2 presented because of vaso-occlusive pain.State-published data shows a chlamydia rate of 1,403/100,000(1.4%) amonga comparative cohort of African American patients.Conclusions: In a small sample, patients with SCD had a larger percentageof asymptomatic chlamydia compared to a demographically matched his-torical control population. This may reflect a higher prevalence of chlamydiabased on inadequate screening in this population. While there may also be anunknown susceptibility to chlamydial infection in this population, prelimi-nary findings suggest that patients with a chronic disease such as sickle celldisease may not be getting the recommended age-based screening evalua-tions (unrelated to their SCD). All at-risk patients should be screened byspecialist physicians in addition to ensuring patients undergo routine primarycare evaluations.
41
GEOGRAPHIC CLUSTER OF KAWASAKI DISEASE VS. ACONTROL POPULATION FOR FLORIDA PANHANDLEREGIONAL CHILDREN’S HOSPITAL
Burns JJ1, Broge T1, River-Diaz G1, Taylor S1, Hommeida S1, Onuegbu P1,Amin R2. 1FSU, Pensacola, FL and 2University of West Florida, Pensacola, FL.Purpose of Study: This study will determine if a geographic cluster ofKD found in the Florida panhandle will persist when compared to a matchedcontrol group.Methods Used: After mapping home addresses for KD patients and acontrol group (matched for age, gender and date of KD disease patient ad-mission) for a regional Children’s Hospital, SATSCANi was used to test forstatistically significant spatial clusters. SATSCANi was developed throughsupport of the National Cancer Institute and Center for Disease Control todetect geographical, time or space-time clusters in mapped data and has thecapability of making spatial comparison of cases to a control group. The basepopulation used in SATSCANi for rate calculations of cases/controls wasthe number of children residing in Census tracts. First Poisson spatial analysiswas applied to KD and control separately. Then using a Bernoulli model thespatial distribution of KD patients was compared to the control group.Summary of Results: There were statistically significant spatial clustersfound for KD cases using the discrete Poisson model (observed cases 47,expected 30.5; p = 0.011). This was also true for the control group (observedcases 47, expected 24.9; p=0.000). However on Bernoulli model analy-sis, comparing the spatial distribution of KD cases to control group cases,no statistically significant KD cluster was found (observed 7, expected 3.5;p = 0.242).Conclusions: The spatial distribution of KD cases admitted to a Floridapanhandle regional Children’s Hospital did not differ from matched controls.It is likely that the KD cluster found was due to factors that were not uniquelyrelated to having KD. Use of a control group is important to validate epi-demiologic studies investigating regional geographic patterns of disease.
42
HYPERTENSION IN HIV-INFECTED CHILDREN ANDADOLESCENTS
Chatterton-Kirchmeier S1, Chakraborty R3, Camacho-Gonzalez A3, Batisky D2.1Emory University School of Medicine, Atlanta, GA; 2Emory University, Atlanta,GA and 3Emory University, Atlanta, GA.Purpose of Study: HIV infection increases cardiovascular disease risk,and chronic administration of antiretrovirals (ARVs) exacerbates this. The
Mis-categorization of BMI
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
384 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

prevalence of hypertension (HTN) in adult HIV-infected populations hasbeen previously described; however, there is a paucity of similar data inchildren and adolescents. In order to better assess this long-term cardiovas-cular disease risk we characterized the prevalence of and risk factors for HTNin one of the largest cohorts of HIV-infected pediatric and adolescent sub-jects in the U.S.Methods Used: A retrospective chart review identified 266 patients fol-lowed in the Grady Pediatric Infectious Diseases Program, ages 2 to 25 years,with blood pressure readings at a recent clinic visit. HTN was defined as asingle systolic or diastolic reading 995th percentile for ages 2-17 and Q140/90 for patients 18-25. Characteristics known to contribute to elevated BPwere also reported including BMI, comorbidities, ARV administration, useof medications known to elevate BP, length of HIV infection, dyslipidemia,ethnicity and family history.Summary of Results: 47 subjects (17.7%) were considered to have HTNin the absence of underlying renal disease. Among children ages 2-17, 21/107(19.6%) were considered to have HTN. HTN was more common in subjectswith BMI 925 (24.6%) than with BMI e25 (15.7%) (p = 0.042). Having co-morbidities known to elevate BP, such as obesity, PCOS or cocaine use, was asignificant risk factor for HTN, with 34.9% of subjects with these comor-bidities found to have HTN, compared to 16.2% of subjects without (p =0.010). In the perinatally-infected subset of this cohort, duration of HIVinfection was positively correlated with HTN, with 4.0% of subjects hyper-tensive in 6-10 years, 16.7% in 11-15 years, and 23.1% 915 years (p = 0.001).Conclusions: Pediatric HTN prevalence in the U.S. has been reported be-tween 3-5% by NHANES data and other sources. The finding of 19.6%prevalence in a cohort of HIV-infected children and adolescents representsa significant disparity. Even if this finding is explained by BMI and comor-bid conditions, the life-long cardiovascular risks associated with HIV in-fection mandate the need for closer monitoring and management of BP inthese subjects.
43
IS THE HISTORY AND PHYSICAL EXAMINATIONOBSOLETE FOR MAKING THE DIAGNOSIS OF INFANTILEHYPERTROPHIC PYLORIC STENOSIS?
Chu EK1, Edwards C1, Lewis K2,1, Waller JL3, White C1. 1Medical College ofGeorgia at Georgia Health Sciences University, Augusta, GA; 2Medical Collegeof Georgia at Georgia Health Sciences University, Augusta, GA and 3MedicalCollege of Georgia at Georgia Health Sciences University, Augusta, GA.Purpose of Study: In recent years, abdominal ultrasonography has sup-planted clinical features such as the abdominal peristaltic wave or the pal-pable hypertrophic pyloric muscle (‘‘olive’’) in the diagnosis of infantilehypertrophic pyloric stenosis (IHPS). A recent patient in our hospital whosehistory and physical exam findings (including a gastric peristaltic wave)strongly suggested the diagnosis of IHPS had his surgery delayed nearly twoweeks because he failed to meet ultrasound diagnostic criteria for IHPS. Wewanted to see if there was a subset of infants with clinical findings of IHPSwho experienced delayed surgery because they failed to meet ultrasoundcriteria for IHPS on initial presentation. We also wanted to determine howoften a peristaltic wave or an olivewas mentioned in the physical examinationof these patients.Methods Used: We performed a 5-year retrospective chart review of allpatients at our academic medical center who underwent pyloromyotomy forIHPS, looking at their clinical and laboratory findings, and the ultrasound mea-surements of pyloric muscle thickness and pyloric muscle length.Summary of Results: 193 infants underwent pyloromyotomy for IHPS. Apalpable olive was not sought nor mentioned in 40.4% of patients, and aperistaltic wave was not sought nor mentioned in 96.4% of patients. Al-though vomiting was assessed in 97% of patients, bilious vomiting andprojectile vomiting were not sought or documented in 52.3% and 34.2%of patients respectively. Thirteen (6.7%) patients had a delay in surgery be-cause they failed to meet ultrasound criteria on initial evaluation.Conclusions: When ultrasound criteria were used exclusively for the di-agnosis of IHPS, a significant number of patients experienced a delay in theirsurgery despite strong clinical criteria supporting this diagnosis. In manycases classic physical findings associated with IHPS were not sought ormentioned in the initial hospital evaluation of these infants. We hope thatthese results will refocus efforts on using the history and physical exam todiagnose IHPS.
44
TRAINING PEDIATRICIANS IN EARLY CHILDHOODHEALTH PROMOTION IN HISPANIC COMMUNITIES
Faulconer E, Dunlap M, Gillaspy S, Weedn A. University of OklahomaHealth Sciences Center, Oklahoma City, OK.Purpose of Study: A significant gap exists in primary care pediatrics be-tween pediatricians reporting an overall awareness of and concern for child-hood obesity but lacking the training and resources to address it. In response, agrant was received by the OKAAP and the OUHSC Pediatrics ResidencyProgram to implement resident training in obesity prevention in communitysettings. The goal of this advocacy project is to report on the process ofincorporating community-based advocacy training in obesity prevention intoour residency program.Methods Used:We have partnered with the YMCA to train pediatric internson age-appropriate physical activity in preschool-aged children through theearly childhood CATCH curriculum. After training, residents will participatein training childcare staff on the CATCH curriculum at 2 community child-care centers. In addition, residents will lead parenting classes offered by thechildcare centers to educate parents on healthy active living through dem-onstration of age-appropriate activities for their pre-school aged children.These activities occur during the intern’s advocacy rotation. Additionally, allresidents receive training in obesity prevention and management throughdidactic lectures.Summary of Results: Evaluation of this advocacy project will be based onpre- and post-surveys of resident knowledge on obesity and communityresources for obesity prevention. Pre-surveys were administered to pediatricinterns at the beginning of their intern year. Post-surveys will be obtained atthe end of their advocacy rotation. Pre-survey data has shown that pediatricinterns have limited knowledge on community resources for obesity preven-tion and age-appropriate activities in preschool aged children. Post-survey datais currently being collected.Conclusions: Training in community-based obesity prevention through anadvocacy rotation may offer an opportunity to increase provider knowledgeof community resources for obesity management and engage pediatric resi-dents to advocate for healthy active living at the community level. Additionally,developing collaborations among pediatric trainees and community organiza-tions allows for unified obesity prevention messages in the community setting.
45
DEVELOPMENTAL FUNCTIONING AND MEDICALCO-MORBIDITY PROFILE OF CHILDREN WITH COMPLEXAND ESSENTIAL AUTISM
Flor J, Bellando J, Lopez M. University of Arkansas for Medical Sciences,Little Rock, AR.Purpose of Study: Children with Autism Spectrum Disorders (ASD) maybe categorized as ‘‘complex’’ (those with microcephaly and/or dysmorphol-ogy) or ‘‘essential’’ (those with neither of these two). The objective of thisstudy is to determine if there are differences in complex vs. essential subjectsbased on developmental profile (cognitive level, adaptive behavior, autismseverity, quality of life, and behavioral ratings) and medical comorbidities(GI symptomatology, sleep problems and medication usage) in a large co-hort of subjects with well-defined ASD.Methods Used: This study utilizes data from 1,347 individuals (2-17 yearsold) enrolled in Autism Treatment Network (ATN) Registry. ASD diagnosiswas established based on DSM-IV criteria and a standardized battery of as-sessments, including an Autism Diagnostic Observation Schedule (ADOS) anda medical evaluation. The ADM (Autism Dysmorphology Measure) was usedby trained physicians to classify subjects as complex or essential. Compar-isons between complex vs. essential subjects for the specified developmentaland medical markers were assessed.Summary of Results: The sample was homogenous in age and gen-der. 5.6% of the sample were classified as complex, with complex subjectsmore likely to have an Autistic Disorder diagnosis vs. Asperger ( pG.021).Significantly lower scores are seen for complex subjects in cognitive level(pG .025), adaptive behavior (pG.001), and quality of life (pG.050). No sig-nificant differences in behavioral ratings or ADOS calibrated autism severityscores were found. Complex subjects showed significantly increased physician-documented GI symptoms (pG.003), and are on higher number of medications
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 385
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

(pG.001). No significant differences were found in parent-reported sleepproblems.Conclusions: Using a large ASD sample, this study shows that complex andessential autism have distinct developmental and medical correlates, and thusunderlines the importance of looking for dysmorphology, even minor features,in the evaluation of a child with autism. Determining this distinction in autismmay have implications in prognosis, identifying medical co-morbidities, di-recting diagnostic evaluations, recommending treatment interventions, andfuture research participation.
46
MESENTERIC LYMPHANGIOMA PRESENTING AS SEPSISAND BILIOUS EMESIS IN A NEONATE
Hines L, DeLeon S. University of Oklahoma Health Sciences Center, OklahomaCity, OK.Case Report: The differential for pediatric abdominal masses is wide andoften dependent on the age of the patient. Specifically in neonates the dif-ferential must include congenital malformations and their complications, butbecause of their age the presenting symptoms may not be as obvious asthose found in older patients. This is demonstrated in the following casepresentation in which a neonate presenting with sepsis and bilious emesiswith a distended abdomen was found to have a rare but benign mesentericcyst known as a mesenteric lymphangioma.
DT was a 10-day-old male who presented initially with increased irri-tability, bilious emesis and fever for 2 days. He received a full sepsis workup for fever, which was ultimately negative. He tolerated some PO feedingsbut would have bilious emesis intermittently. On physical exam, the patientappeared uncomfortable and irritable but consolable. Serial abdominal examsrevealed a progressively distended abdomen with visible veins and tender-ness to palpation. The right abdomen was found to be firm without a palpableliver edge, while the left side was distended but soft with bowel soundspresent. Abdominal radiographs were significant for air throughout the bowelto the rectum in left abdomen and a paucity of gas in the right abdomen butwere read as essentially normal; an upper GI showed no evidence of malrota-tion. The right-sided paucity of gas was unchanged on subsequent abdominalfilms and raised concern for a space-occupying lesion. After an ultrasoundconfirmed a large mass, pediatric surgery performed an exploratory laparo-tomy. A largemesenteric cystic mass and portion of non-viable small bowelwasremoved. Pathology report showed the mass was a mesenteric lymphangioma.
Mesenteric lymphangiomas are rare benign cystic tumors with widelyvarying presentations including everything from incidental discovery to anacute abdomen as was found in our patient. There are few case reports in theliterature discussing this type of abdominal mass; however, it should be onthe differential for any neonate with exam findings consistent with a massbut otherwise normal bowel imaging. This case also reinforces the need torely on history and exam findings and not be falsely reassured by ‘normal’imaging studies.
47
AN INFANT WITH FAILURE TO THRIVE AND POORAPPETITE TREATED SUCCESSFULLY WITH PERIACTIN
Hines L, Hart N, Yates A, DeLeon S. University of Oklahoma HealthSciences Center, Oklahoma City, OK.Case Report: Failure to thrive (FTT) is a large concern in the pediatricpopulation due to the potential for adverse effects on future growth and de-velopment. If no etiology can be identified other than poor appetite or oralaversion, enteral supplementation is often provided via nasogastric tube tomaintain adequate caloric intake. This case report presents an 8-month-oldfemale with oral aversion, poor appetite, and FTT who achieved and main-tained appropriate weight gain while on Periactin.
An 8-month-old female with history of poor weight gain and feedingdifficulties was admitted for FTT. Her outpatient growth chart documentedthe patient at the 75th percentile from birth to 4 months with a drop to the 5thpercentile by 8 months of age. The patient would only breastfeed; she refusedbaby and table foods, bottles and sippy cups with multiple nipple types, sy-ringe feedings, and pacifiers. She also generally seemed to have a poor appe-tite as she once went 48 hours happily with only minimal intake when motherwas unavailable for feedings.
While hospitalized, bolus feeds via nasogastric tube in addition to ad libbreastfeeding were given. No organic etiology was identified. A speech con-sult identified no mechanical feeding problems but recommended an appetitestimulant.
Periactin was started at 0.25mg/kg/day. At discharge, the patient wasstill G5th percentile weight-for-age but demonstrated an average weight gainof 30g/day. She continued daily Periactin and NG supplemental feeds. Fiveweeks after discharge, the patient had gained approximately 40g/day and re-gained the 10th percentile weight-for-age. NG feeds were discontinued at thistime, and Periactin continued. After three months of treatment with Periactin,the patient continued to maintain the 10-15th percentile weight-for-age, dem-onstrating expected growth for age. The patient’s mother felt Periactin hadgreatly increased her daughter’s appetite.
Minimal literature exists concerning the use of Periactin in FTT, partic-ularly in infancy. Periactin has been used as an appetite stimulant in anore-xia nervosa and oncology patients. This case illustrates the successful use ofPeriactin as an appetite stimulant in an infant with FTT and oral aversion andhighlights the need for further studies in this area.
48
IDIOPATHIC COLLAPSING FOCAL SEGMENTALGLOMERULOSCLEROSIS (FSGS) IN PEDIATRIC PATIENTWITH ATTENTION DEFICIT HYPERACTIVITY (ADHD)AND OPPOSITIONAL DEFIANT (ODD) DISORDERS
Kaleemullah R2, Hirsh S2, Yosypiv I1. 1Tulane HSC, Metairie, LA and2Tulane HSC, New Orleans, LA.Purpose of Study: This case illustrates a rare case of primary collapsingFSGS, a chronic progressive disease potentially leading to end-stage renaldisease, in conjunction with ADHD and ODD. Physicians should be aware ofthe adverse effect of severe chronic disease and potent immunosuppressivemedications on exacerbation of mental diseases in children.Methods Used: Retrospective review of medical records. A 16 year oldAfrican American female with history of ADHD and ODD presented withdifficulty breathing and generalized edema. Psychosocial history consisted ofneglect, physical and sexual abuse, and foster family care. Physical examinationrevealed a blood pressure of 140/85 mmHg, periorbital edema, lung cracklesand 3+ pitting edema of the lower extremities.Summary of Results: Laboratory findings demonstrated (mg/dL): serumalbumin of 0.3, creatinine of 1.4, cholesterol 256, complement C3 118, C418, negative hepatitis B, C and HIV serologies, and spot urine protein tocreatinine ratio of 10.0. Her urinalysis was remarkable for proteinuria of600 mg/dl with 5-10 RBC’s. Renal ultrasound revealed presence of 2 struc-turally normal kidneys.Molecular diagnostic testing conducted to rule outgenetic causes of FSGS displayed variants of the NPHS2, LAMB2, and WTIof unknown clinical significance.Conclusions: Subsequent development of diuretic-resistant severe anasarcarequired intitiation of CRRT and high-dose intravenous administration ofsolumedrol (SM) combined with cyclophosphamide according to Mendozaprotocol. Complete remission of nephritic syndrome was achieved after6 months of SM infusions. ADHD and ODD were treated with methylphe-nidate and risperidone. Treatment with high dose SM and prednisone exac-erbated the patient’s mood symptoms which lead to increased non-adherencewith dietary restrictions and medications. Effective management of FSGS,ADHD and ODD required care by a multidisciplinary team which includedpediatric nephrologist and psychiatrist, general pediatrician and social worker.
49
AN ATYPICAL CAUSE OF CHEST PAIN IN AN ADOLESCENT
Malhotra S, Wells A. Tulane University, New Orleans, LA.Case Report: A 17 yr old boy with Hemoglobin SS Disease presented withseveral days of stabbing chest pain consistent with previous sickle cell crises.He reported vomiting but no fever or palpitations.He was afebrile but hy-pertensive and tachycardic with a systolic murmur along the left sternalborder that did not change with inspiration.Labs and radiologic studies in-cluding a complete blood count, electrolytes, liver profile, and chest x-raywere normal.Electrocardiogram revealed left ventricular hypertrophy andprolonged QT.He was admitted for a sickle cell pain crisis but had minimalpain relief with fluids and narcotics.His height was noted to be abnormal and
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
386 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

when plotted was at the 3rd percentile.Examination of his genitals placedhim at Tanner stage three.As a result, thyroid function tests were performedand showed depressed TSH and elevated T4 levels.He was started on pro-pylthiouracil and atenolol which subsequently resolved his chest pain andstabilized his thyroid levels.Although sickle cell crises and acute chest causemore than ninety percent of chest pain in sickle cell patients, ten percent ofthe population present with alternative diagnoses that must be explored.Hyperthyroidism commonly presents with symptoms such as heat intolerance,palpitations, and tremor. The presence of EKG abnormalities and growth fail-ure, although atypical as an initial presentation, make thyroid disease a strongconsideration of chest pain.In our patient’s case, his chest pain was initiallyattributed to sickle cell disease and treated accordingly. However, we foundthat his chest pain was the result of cardiac manifestations of hyperthy-roidism.Untreated endocrine disease can be missed when in the setting ofa concurrent chronic disease.Additionally, a complete physical examinationincluding sexual maturity rating and tools such as growth charts can revealclues to underlying disease entities. The use of these tools is especially im-portant in the transition of adolescent patients with chronic disease from pe-diatric to adult providers.It is important for clinicians to keep a high index ofsuspicion when evaluating adolescent patients with chronic disease so thatatypical disease presentations do not get dismissed as being ‘‘typical.’’
50
RUMINATION SYNDROME AND DENTAL EROSIONS INCHILDREN
Monagas JJ1,2, Ritwik P3,2, Clendaniel L2,1, Kolomensky A1,2, Kay D4, HymanPE1,2. 1Louisiana State University Health Sciences Center, New Orleans,LA; 2Children’s Hospital, New Orleans, LA; 3Louisiana State UniversityHealth Sciences Center, New Orleans, LA and 4Tulane, New Orleans, LA.Purpose of Study: Rumination syndrome is the effortless regurgitation ofrecently ingested food into the mouth with subsequent rechewing and re-swallowing or spitting out. The regurgitation is unassociated with discomfort,heartburn, or nausea. Rumination occurs as a self-stimulating, presumablypleasurable activity in some children with mental retardation. Ruminationalso occurs in children and adults of normal intelligence, but is often misdi-agnosed. Dental erosions (DE) affect 2% to 5% of the population. DE aredefined as loss of tooth enamel by a chemical process that does not involvebacteria, compared to caries which involve tooth damage due to bacteria. DEare caused by acid that can be from either an intrinsic or extrinsic source, or acombination of them. Vomiting, regurgitation, gastroesophageal reflux dis-ease (GERD), and rumination are all intrinsic sources of oral acid. We in-vestigated whether rumination in children is associated with dental erosions.Methods Used: Subjects 4 to 21 years of age diagnosed by their clinicianto have rumination syndrome, as well as age and sex-matched healthy con-trol subjects were enrolled in this study. Subjects were evaluated by a pedi-atric dentist for presence and severity of dental erosions as measured by theTaji et al. dental erosion grading system.Summary of Results: Of 12 subjects (6 male, mean age 10 yr) determinedto have rumination syndrome, 9 (75%) had dental erosions. Nine (75%) ofthese subjects suffered from additional functional disorders based on ROMEIII diagnostic criteria, with functional dyspepsia (25%) and functional ab-dominal pain (25%) being the most common comorbidities. For controlsubjects (10 male, mean age 10 yr), only 1 of 14 (7%) had dental erosions.Subjects with rumination are more likely to have dental erosions than healthycontrols (p = 0.0019).Conclusions: There was a strong statistical correlation between ruminationand dental erosions. However, more data are needed to determine if daily fre-quency and duration of rumination might predict erosion severity, and numberof involved teeth.
51
CLINICAL CHARACTERIZATION OF A COHORT OFCHILDREN WITH MULTICYSTIC DYSPLASTIC KIDNEY(MCDK)
Monlezun DJ, Song R, Yosypiv I. Tulane University School of Medicine,Lake Arthur, LA.Purpose of Study: MCDK is one of the most commonly identifiable formsof congenital anomalies of the kidney and urinary tract (CAKUT). The in-
cidence of MCDK is 0.3-1 in 1000 live births. Although Pax2, Six1 and Eya1mutations have been linked to MCDK in a subset of patients, the causeand clinical spectrum of MCDK in the majority of cases remains unknown.This study is thus meant to clinically characterize a pediatric MCDK cohort.Methods Used: Patients (six females and four males) were diagnosed withMCDK by renal ultrasonography during clinic encounters. eGFR was esti-mated with the Scwartz formula from serum creatinine measured by the Jaffemethod. VCUG was performed when indicated by history of UTIs or pres-ence of hydronephrosis in the contralateral kidney. Pedigree analysis wasperformed by interviewing caregivers.Summary of Results: The mean age of patients was 8.3T2.1 years. 2/10patients were Caucasian and 8/10 were African American. All cases wereunilateral MCDK with 6/10 involving the left kidney. Two patients hadTurner syndrome and one had Asperger syndrome, with the cystic kidneyregressing in one of the Turner patients and the Asperger patient. One patienthad contralateral kidney hydronephrosis and another had elevated bloodpressure. There were no UTIs or proteinuria cases. None of the first-degreerelatives reported during patient encounters the presence of known renalanomalies, including MCDK. Estimated GFR was decreased in one patient.Conclusions: Most MCDK cases were in isolated non-syndromic patients.3/10 cases were associated with Asperger and Turner syndromes, thoughthe association of both conditions with MCDK is not well documented in themedical literature. Most cases in this study were in females and involved theleft kidney. Associated renal anomalies were identified in 2/10 patients.These results do not support routine surgical removal of MCDK, but rathermedical monitoring throughout life. Medical monitoring should include as-sessment of growth, blood pressure, proteinuria, renal function, and urinarytract imaging. Further research is required to determine the mechanisms un-derlying isolated and syndromic cases of MCDK in children.
52
VARIATIONS IN ADOLESCENT VACCINATION RATES BYPRACTICE IN SOUTH CAROLINA & OKLAHOMA
Naifeh M1, Roberts J2, Hale J1, O’Brien E2, Darden P1. 1University ofOklahoma Health Sciences Center, Oklahoma City, OK and 2MedicalUniversity of South Carolina, Charleston, SC.Purpose of Study: In 2005 the Advisory Committee on ImmunizationPractices began recommending 3 new vaccines for adolescents: TetanusDiptheria & acellular Pertussis (TDaP), Meningococcal Conjugate Vaccine(MCV4) & Human Papillomavirus Vaccine (HPV). National immunizationrates have increased though they still remain below Healthy People 2020goals. This study examined variations in immunization rates between 6 pe-diatric practices in South Carolina & Oklahoma.Methods Used: Six Pediatric practices were included; 3 from OklahomaCity-the Latino Clinic (LC), the General Pediatrics Clinic (GPC) & theContinuity Clinic (CC), & 3 from South Carolina-Charleston Pediatrics (CP),Georgetown Pediatrics (GP) & Pediatric Primary Care (PPC). A conveniencesample of 384 teens (at least 60 per site) & parents were surveyed. Thesurveys collected basic demographic information including age, gender, race/ethnicity & reason for visit. Immunization status was determined using med-ical records. Data were analyzed using chi-square & logistic regression.Summary of Results: In total, 384 surveys were completed. Morerespondents from Oklahoma reported less than a high-school education (29%vs. 8% p=.0001). Patients seen in Oklahomawere more likely to receive HPVvaccine (49% vs. 38%, p=.0271). There was no significant difference be-tween states for TDaP & MCV4 immunization rates. Practice demographicsvaried considerably. Parents surveyed in CP were mostly white (95%) &college educated (83%) while those from LC were nearly all Hispanic (97%)& most had less than a high school education (67%). Immunization ratesdiffered by clinic site for all three vaccines (PG.05 for each vaccine): LC (HPV65%, TDaP 93%, MCV4 78%); PPC (57%, 90%, 88%); GPC (46%, 74%,59%); CC (37%, 75%, 66%); GP (31%, 85%, 72%); CP (23%, 73%, 55%).Practice site remained a significant predictor of immunization rates for allthree vaccines after including other significant factors & interactions.Conclusions: While patient characteristics are associated with variations inimmunization rates, the practice a patient attends is a powerful predictor ofpatient immunization rates independently of patient factors. Interventions toimprove immunization need to target practices as well as patients.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 387
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

53
NECROBIOSIS LIPOIDICA DIABETICORUM: THE CLUE TOA DIAGNOSIS OF DIABETES MELLITUS IN YOUTH
Nye SE, Dasari PS, Copeland KC. University of Oklahoma Health SciencesCenter, Oklahoma City, OK.Case Report:Introduction: Necrobiosis lipoidica diabeticorum (NLD) is an idiopathicskin finding often associated with, but not limited to, diabetes mellitus. Thedevelopment of this condition is more commonly manifested in adults and ismuch less common in children. We present the case of an obese, 13-year-oldfemale who sought medical attention for persistent and unusual skin lesions,NLD, leading to testing for and a diagnosis of type 2 diabetes mellitus.Case Description: AP, a 13-year-old female, presented to an emergencydepartment (ED) with concerns of a 2-month history of skin lesions on herlegs that would not heal. The lesions initially began as red circles on her legsthat grew larger over time, and one of the lesions later ulcerated. The patientinitially treated the lesions with sea salt, peroxide and antibiotic ointmentat home without improvement. In the ED, AP was found to have an elevatedblood pressure of 200/118 and was transferred to our facility. Upon arrivalshe was hypertensive, tachycardic, and morbidly obese. Physical exam re-vealed acanthosis nigricans on the neck and axilla, and multiple bilateral, yellow,2-5 cm pre-tibial plaques with erythematous borders. Laboratory workup re-vealed hyperglycemia, hyperlipidemia with hypertriglyceridemia, and a he-moglobin A1c of 11.5%. The physical exam and laboratory findings confirmedthe diagnosis of metabolic syndrome and type 2 diabetes mellitus. Derma-tology confirmed the diagnosis of classic NLD by physical exam, but de-clined to biopsy due to anticipated poor wound healing at the site. The patientwas placed on topical corticosteroid cream.Discussion: Few cases of NLD in children have been described, includingonly one in which NLD was noted to be an early feature of diabetes mellitustype 2. This case is unique because NLD is rare in children and is even morerarely found as a presenting symptom of diabetes mellitus. In the context ofthe new epidemic of obesity and type 2 diabetes in youth, this case demon-strates that skin lesions associated with diabetes may become a more commonpresenting symptom in children. The role of other potential contributing factorsin its pathogenesis, including hypertension and dyslipidemia, remains unclear.
54
THE PHEOCHROMOCYTOMA DOESN’T FALL FAR FROMTHE TREE: PEDIATRIC PHEOCHROMOCYTOMASIN MOTHER AND DAUGHTER
Patel J1,2, Leong K1,2, Conlin E1,2, Baez-Irizarry E1,2, Craver R1,2,Straatmann C1,2, Valerie E2, Marble M1,2, Vargas A1,2, Beatty K1,2. 1LSUHealth Sciences Center, New Orleans, LA and 2Children’s Hospital, NewOrleans, LA.Case Report: Pheochromocytomas are rare. The incidence is 1 to 2 million/year, mostly occurring in adults with only 10-23% of pheochromocytomasdiagnosed during childhood. Pheochromocytoma may be sporadic or associ-ated with a genetic mutation and age of onset varies with mutation. We presentthe case of an AA family where both mother and daughter were diagnosedwith pheochromocytomas at 12 years of age. The previously healthy daugh-ter presented with acute onset of anxiety & leg weakness without neurologi-cal deficit. Initially she was admitted for conversion disorder but was found tohave intermittent hypertension. Abdominal CT scan showed a 3.3 cm massin the left perihilar region. Normetanephrines were significantly elevated inplasma (4.56 nmol/L; NG0.89) and 24-h urine (1187 Kg/g Cr; NG287).Chromogranin Awas 381 ng/mL (N 0-95). Plasma calcitonin and aldosteronewere normal. In preparation for surgery hypertension was controlled with dox-azosin and labetalol. Laparoscopic tumor resection was performed afterwhich her blood pressure returned to normal. Pathology confirmed an extraadrenal pheochromocytoma. Interestingly, the patient’s mother was diagnosedwith right-sided adrenal pheochromocytoma at 12 years old after sufferingwith severe diaphoresis, palpitations, and hypertension. After tumor resectionher symptoms resolved. The mother is now 32 and remains tumor free.
Based on our patient’s family history, we suspect the tumors are secondaryto a genetic mutation. Compared to adults, pediatric pheochromocytomas aremore likely associated with a germ line mutation rather than sporadic in origin.
Several genetic mutations have been associated with pheochromocytomasand paragangliomas, including SDH, VHL, and RETmutations. Deletion andduplication analysis of SDH genes in our patient was negative and se-quencing is pending. If a genetic mutation is identified, genetic testing of thefamily members would be necessary. Clinical characterizations of familieslike this may lead to the discovery of new genetic mutations associated withparaganglioma syndromes.
55
ASSOCIATION BETWEEN HEMOGLOBIN A1C AND PULSEWAVE VELOCITY IN HEALTHY OVERWEIGHT/OBESEAFRICAN AMERICANS
Pham M, Bhagatawala J, Parikh S, Kotak I, Havens R, Huang Y, Zhu H,Dong Y. GHSU, Augusta, GA.Purpose of Study: In the present study, we aim to explore the relation-ship between hemoglobin A1C (HbA1C) and pulse wave velocity (PWV), amarker of arterial stiffness, in apparently healthy overweight/obese youngAfrican Americans.Methods Used: We recruited a total of 66 apparently healthy overweight/obese African American participants (age 13-45 years, 82 % females) fromthe local communities in Augusta, Georgia and surrounding areas. Carotidfemoral PWV (CF-PWV) was derived from radial applanation tonometry usingSphygmoCor device. HbA1C was derived quantitatively using ion exchangechromatography.Summary of Results: Mean (T standard deviation) for HbA1C and CF-PWV were 5.4 T 0.4 %, and 6.8 T 1.7 meter/second, respectively. Pearson’sbivariate correlation analysis showed that HbA1C was positively correlatedwith CF-PWV (r=0.35, p= 0.02). However, the relationship between HbA1Cand CF-PWV did not remain statistically significant after adjusting for knownconfounders such as age, sex, body mass index, and systolic blood pressure.Conclusions: Higher HbA1C seemed to be associated with increased PWVin apparently healthy young African Americans. However, studies with largersample size are needed to further establish this relationship in this group.
56
ACCESS TO A MEDICAL HOME FOR THE TODDLERS OFTEEN MOTHERS: DATA FROM THE OKLAHOMA PRAMS &TOTS SURVEYS, 2006-2010
Stewart K1, Kunnel B2, Lincoln A2, Gillaspy S1. 1University of OklahomaHealth Sciences Center, Oklahoma City, OK and 2Oklahoma State Departmentof Health, Oklahoma City, OK.
Baseline Characteristics of subjects
Bivariate correlations of HbA1C and PWV
Partial correlations of HbA1C and PWV adjusted for age, sex, BMI and SBP
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
388 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Purpose of Study: To determine whether Oklahoma teen mothers are lesslikely to report having access to a medical home for their toddlers. Also, todetermine whether there is an association between decreased medical homeaccess for toddlers of teen mothers and the rate and intention of subsequentpregnancies of those mothers within two years.Methods Used: The Pregnancy Risk Assessment Monitoring System(PRAMS) is a surveillance project of the Centers for Disease Control andPrevention (CDC) and state health departments which collects state-specific,population-based data on maternal attitudes and experiences before, during,and after pregnancy. The Oklahoma Toddler Survey (TOTS) is a two-yearfollow-back survey for Oklahoma PRAMS respondents. PRAMS and TOTSlinked data from 2006-2010 were used (n=6652). TOTS questions regard-ing access and utilization of a medical home for the two year-old were as-sessed and then compared TOTS questions on repeat pregnancy rate andpregnancy intention of the mother. Descriptive statistics and the Cochran-Mantel-Haenszel chi-square test were run to test associations (p G .05).Summary of Results: Teen mothers report significantly decreased accessto a medical home for their children. Mothers aged 19 and younger, 20-24,and 25+ reported access at 67.3%, 76.4%, and 83.6%. Adolescent motherswere significantly more likely to become pregnant again within two yearsthan older mothers (46.8 %, 33.5%, and 20.5%) and less likely to have anintended birth (13.2%, 26.4%, and 38.1%). Preliminary results suggest thataccess to a medical home for their toddlers was not associated with anychange in repeat pregnancy rate and possibly even negatively associated withintended pregnancy rate.Conclusions: Oklahoma teen mothers have reduced access to a medical homefor their toddlers. When accessed, medical homes for toddlers may be miss-ing opportunities to address the reproductive health needs of teen mothers. Thisdata will guide repeat teen pregnancy prevention efforts in Oklahoma, in-cluding the design of a teen-tot clinic model in Oklahoma City.
57
DO SEPTIC WORKUPS IN THE EMERGENCY DEPARTMENT(ED) DIFFER FOR INFANTS WITH FEVER LESS THAN90 DAYS DURING THE WINTER SEASON INCLUDING THENOVEL H1N1 PANDEMIC?
Thompson TM1, Cole CC2, Dick RM1. 1Univ of Arkansas for MedicalSciences, Little Rock, AR and 2Univ of Arknasas for Medical Sciences, LittleRock, AR.Purpose of Study: Febrile neonates less than 31 days without source,typically undergo a full septic work-up in the ED. This is often applied tofebrile infants between 31 and 90 days. In winter months, EDs are frequentlyovercrowded with respiratory illnesses and concomitant fever which in somestudies has lead to abbreviated work-ups. ED overcrowding was especiallysignificant during the H1N1 pandemic of 2009-10. The purpose of the studywas to determine if septic work-ups in the ED differed among infants lessthan 90 days during Influenza or RSV season, and secondarily to determineif those differences increased during the novel H1N1 influenza outbreak.Methods Used: To date chart review identified 237 infants less than3 months of age who were seen and admitted through the ED at a PediatricChildren’s Hospital from July 2005 to June 2008. Comparisons of septicwork-ups done during the In (influenza and RSV) and Out seasons wereperformed. Bacterial infections found via additional work-up obtained onceadmitted were also examined. Ongoing data collection focuses on dates duringthe pandemic influenza season of 2009-10.Summary of Results: Previous pilot data demonstrated that neonates (lessthan 31 days) comprised 91.1% of patients and were more likely to receive afull septic work-up than older infants (70.7% vs. 29.6%, pG0.001). Patientswere less likely to receive a full septic work-up if they tested positive foreither influenza or RSV (33.3% vs. 71.3%, pG0.001), but seasonality itselfdid not affect work-up (62.8% during In season vs. 71.1% Out of season,p=0.15). 24.2% of patients received subsequent work-up after admission,all less than 30 days of age. This data is currently being compared with datafrom the H1N1 season to see if there are any further work-up differences intimes of overwhelming ED census.Conclusions: Seasonality did not affect the work-up of infants in the ED,but age and the presence of a positive RSV or Influenza culture did. Ongo-ing data analysis will determine if this also holds true during the H1N1Pandemic.
58
PEDIATRIC SKULL FRACTURES: RISK FACTORS FORADMISSION AND PROLONGED LENGTH OF STAY
Williams DC, Selassie A, Russell S, Basco W. Medical University of SouthCarolina, Charleston, SC.Purpose of Study: Despite published guidelines, management of child-ren with isolated skull fracture (ISF) remains highly variable. We sought todescribe risk factors associated with the decision to admit patients with ISFfor overnight observation compared to those that require prolonged hospitali-zation and those discharged directly from the emergency department (ED).Methods Used: We evaluated children G 5 years of age who presented withISF using South Carolina Traumatic Brain Injury Surveillance and RegistrySystem data from 2001 through 2011. ICD9 codes 800.00 and 800.01 identi-fied patients with skull fractures of the cranial vault without other intracranialinjuries. Outcomes included: discharged from ED, admitted G24 hours (over-night observation), and admitted924 hours (prolonged hospitalization). Con-tingency tables and a multinomial logistic regression model compared groupsusing variables that included age, gender, race, poverty level, hospital traumastatus, injury severity, concomitant injuries (non-head), medical center prox-imity, pre-existing conditions, and mechanism of injury.Summary of Results: 527 patients met study criteria (ED discharge=283;inpatient G24 hours=156; inpatient 924 hours=88). Variables associated withhospitalization status included poverty level, pre-existing conditions, injuryseverity, concomitant injuries, mechanism of injury, and hospital trauma status(PG0.05). In the regression model, patients originating from counties withoutmajor medical centers (OR 0.34, 95% CI 0.18-0.63) and counties classifiedas having moderate to high poverty (OR 0.44, 95% CI 0.24-0.81 and OR0.39, 95% CI 0.16-0.95 respectively) were less likely to be discharged fromthe ED compared to admitted overnight. Conversely, unclassified and level 3trauma centers were more likely to discharge directly from the ED (OR 58.30,95% CI 18.55-183.26 and OR 11.82, 95% CI 5.98-23.33 respectively) com-pared to level 1 trauma centers. Only the presence of a concomitant injurypredicted prolonged hospitalization (OR 2.18, 95% CI 1.02-4.68).Conclusions: Access to care and available resources are important in thedisposition decision for children with ISF. Further work is needed to distin-guish medical necessity of overnight admissions versus concern regardingfollow-up care.
Joint Plenary Poster SessionAdult Clinical Case
5:00 PMThursday, February 21, 201359
A DIAGNOSIS MIMICS GUILLIAN-BARRE SYNDROME
Aly M, Nusrat M, Sherif K, El-Bakush A, Mazek H, Edriss H. Texas TechLubbock, Lubbock, TX.Purpose of Study: Here we report West Nile Virus that presented in apicture mimics Guillain-Barre syndrome, a differential diagnosis that shouldbe considered in such clinical picture. First appearance in United States wasin 1999 when it caused 62 cases of encephalitis and seven deaths in NewYork. This year, there was 1520 reported cases of West Nile infection in Texas700 of these cases were neuro-invasive and it caused 54 deaths in state ofTexas alone.Methods Used: Case presentation and a review of literature.Summary of Results: A 69 years old male presented with rapidly pro-gressing weakness of upper and lower extremities, initially in his lower ex-tremities then it progressed to his arms as well, weakness is more in the leftarm, and the Right leg, his weakness was associated with generalized head-ache, nausea, vomiting, and fever for about 3 days with possible mosquito bite2 weeks prior to onset of symptoms, denied any recent travel or ill contact.On Examination he was alert and oriented. No skin rash, pupils were equaland reacting to light and accommodation, other systems exams were unre-markable. Cranial nerves were intact. DTRs 2+, and symmetrical in all fourextremities. Sensory: Intact to pinprick, temperature, vibration, and proprio-ception. Muscle Strength: 3-4/5 , symmetric in the lower extremities. Flaccidmonoplegia in left arm. Labs were normal except WBC of 19.0. MRI of thespine, CT and MRI of the brain were all negative. Lumber puncture showed
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 389
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

clear CSF with WBC count of 460; 51% lymphocytes and 38 % neutrophilsand the protein of 164, blood and CSF culture was negative but blood andCSF tested positive for West Nile IgM antibodies, patient was treated withsupported measures including physiotherapy and recovered with some re-sidual deficit.Conclusions: West Nile Virus Infection can present with wide variety ofsymptoms. Common symptoms include fever, headache, nausea, meningis-mus, myalgias, rash, and tremor, yet it can present with features of an acute,asymmetric, flaccid paralysis that can resemble Guillain-Barre syndrome orother inflammatory neuropathies. In this case, WNV was presenting as my-elitis with correlation of anterior horn cell inflammation, with subjectiverather objective sensory manifestation. This should increase the awarenessand alertness of WNV infection in patients presenting with Guillain-Barresyndrome picture.
60
‘‘CIPROCLONUS’’: CIPROFLOXACIN INDUCEDMYOCLONUS
Anderson RM, Chowdhury N, Ahmed J, Smalligan RD. Texas Tech UnivHealth Sciences Center, Amarillo, TX.Case Report: A 63-year-old man with a history of schizophrenia was ad-mitted with generalized myoclonus for two days. He had no history of headtrauma, tumor or seizure disorder. Two days prior, before the myoclonus began,ciprofloxacin was initiated for UTI treatment. Other meds included quetiapine,benztropine, lorazepam, omeprazole, duloxetine, and hydrocodone. Neuro-logic exam revealed myoclonus especially involving the face and extremities.His vitals and other system exams were normal. CBC, chemistry, CPK andinflammatory markers were normal except for a BUN of 30 and Cr of 1.35,consistent with acute kidney injury. Head CT was unremarkable. Initiallyquetiapine was thought to be responsible for his myoclonus, however, symp-toms did not resolve after it was discontinued. Ciprofloxacin was then dis-continued, and the myoclonus resolved in less than 24 hours.
Discussion: Ciprofloxacin is one of the most widely utilized antibioticscurrently in medicine. Reported CNS side effects, though rare, include diz-ziness, headache, restlessness, delirium, hallucinations, and seizures. Casereports of myoclonus in addition to ours include an 85-year-old male whodeveloped myoclonus twice after rechallenge with ciprofloxacin. Although themechanism remains speculative, a proposed pathway is that ciprofloxacinacts as a GABA antagonist. By blocking inhibitory receptors, the neuron isexcited, which leads to stimulatory and possibly convulsatory effects. Thesesymptoms arise especially with advancing age, underlying renal failure, andin conjunction with NSAIDs. The elderly have a decreased plasma volumecausing ciprofloxacin to have a longer half-life causing excessive drug ac-cumulation. NSAIDs are thought to enhance the blockade of inhibitory recep-tors, increasing the epileptogenic potential of ciprofloxacin. Renal diseaseresults in impaired clearance of ciprofloxacin, which leads to higher overallplasma drug levels. Considering our patient’s age and kidney disease, he wasvulnerable to neurological complications of cipro. With an aging populationand the widespread use of quinolones, it is imperative for physicians to rec-ognize that rare side effects may occur and that discontinuation of the of-fending agent can bring prompt resolution of the problem.
61
RAPIDLY REVERSIBLE CARDIOMYOPATHY
Gaye BS, Giddings S, Darlington A, Cury J. University of Florida, Jacksonville,Jacksonville, FL.Case Report: This is a 27 year old Caucasian male with no significant pastmedical history who presented with a 3 week history of worsening lowerextremity edema, orthopnea and dyspnea on exertion. He denied any chestpain or palpitations. He also denied tobacco, alcohol or drug use. His familyhistory was negative for premature CAD or heart failure.
Physical examination revealed a cachectic male with exophthalmos. Hewas afebrile and normotensive. His JVP was elevated and there was nothyromegaly. He had an irregularly irregular rhythm but normal heart soundsand no murmurs. Lung auscultation revealed bibasilar crackles. He had bi-lateral pitting edema up to his thighs.
EKG showed atrial fibrillation with rapid ventricular rate of 220 beatsper minute. Chest x-ray findings were consistent with pulmonary edema butno cardiomegaly. His TSH was low with an accompanying elevated free T4and TSI antibodies. CBC and BMP were unremarkable. A bedside echocar-diogram showed global hypokinesis with normal ventricular chamber size.His ejection fraction was 5-10% and there was no evidence of valvular heartdisease.
His hospital course included a PEA arrest with return of spontaneouscirculation after 2 minutes of CPR. Synchronized cardioversion was performedwith achievement of sinus rhythm. He received medical treatment for thy-roid storm with methimazole, propranolol, potassium iodide and steroids. Hisclinical course improved and a repeat echocardiogram 1 week later showedejection fraction 45-50%.
Graves’s disease is a common cause of hyperthyroidism in clinical prac-tice. Its wide array of symptoms usually prompts patients to seek medicalattention. Congestive heart failure (CHF) as a presentation of hyperthyroidismand thyroid storm is considered rare. Few reports have described CHF andhyperthyroidism in patients less than 65 years. The pathophysiology of CHFin these patients could be due to tachycardia induced systolic dysfunctionor direct and prolonged myocardial exposure to thyroid hormones. Treat-ment of this patient’s thyroid storm resulted in marked improvement of hissevere systolic dysfunction within a week. The time course for improvementis not well known. In conclusion, hyperthyroidism can cause severe systolicdysfunction in young patients but this can be rapidly reversed with treatmentof the hyperthyroidism.
62
NO ORDINARY PNEUMONIA
Joseph Z, Miller M. University of Tennessee, MEMPHIS, TN.Case Report:Case History: A 64 year old male with a history of C.O.P.D., hyperten-sion, Type 2 Diabetes Mellitus presents with a 3 day history of fever, coughand increased work of breathing. He also reports a history of left sidedpleuritic chest pain. Vital signs : T:101.6F, HR 115, BP:160/85 RR: 24/minOn physical exam he is noted to have crackles in the left lung base. CXRdone in the ER reveals a left lower lobe pneumonia. He is admitted to themedicine floor for a 23 hr observation to treat for community acquiredpneumonia. In the interim, on reassessment of his clinical and laboratorydata, he was noted to have a Well’s score criteria for pulmonary embolism. ACT scan of the chest per PE protocol was done which revealed no pulmonaryembolus but an incidental finding of an aortic dissection. Aggressive bloodpressure control was initiated and he was transferred to the ICU. Vascularsurgery was consulted. The patient suffered no neurologic sequelae.Discussion: This case stresses the importance of good history taking andfrequent re-assessments on patients admitted overnight from the ER to thefloor. Many a times, in transition of care between physicians and services,assumptions of the clinical status are made based on the ‘‘sign out’’ obtainedor the last evaluation in the ER. Re-assessment of the patient after transferto the floor or unit is of utmost importance as patients can deteriorate withtime and in transport. The uncharacteristic presentation and coincident oc-currence of the pneumonia made the clinical recognition of the dissectiondifficult. However, the disciplined approach to management of his respiratorydistress and pneumonia enabled the timely diagnosis and management of hisdissection. Aggressive control of his blood pressure ensured prevention offurther progression of the dissection whilst vascular surgical intervention wasarranged. This is important in the overall prognosis where neurologic com-plications and death can be the catastrophic sequelae.
63
URINOTHORAX; AN UNUSUAL CAUSE OF PLEURALEFFUSION IN A PATIENT WITH LYMPHOMA
Malik S, Chaudary N. UMMC, Jackson, MS.Case Report:Introduction: Urinothorax is a rare cause of transudative pleural effusionsecondary to obstructive uropathy. We present a case of urinothorax in a
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
390 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

patient with B-cell lymphoma who underwent successful placement ofureteric stent with resolution of symptoms.Case presentation: A 60-year-old female with B-cell lymphoma receiv-ing chemotherapy was admitted with shortness of breath, abdominal pain andnausea. She gave a history of left ureteric stent two months ago for obstruc-tive uropathy from bulky pelvic lymphadenopathy. Physical exam revealedlymphadenopathy, dullness with decreased air entry at left lung base anddistended abdomen with left flank tenderness.
Chest x ray showed left pleural effusion. Renal ultrasound revealeded leftureteric stent with mild hydronephrosis. A CT scan chest and abdomendemonstrated moderate left sided pleural effusion and a hypodense collec-tion in left renal pelvis. Echocardiogram showed ejection fraction of 60%.Thoracentesis revealed transudative pleural effusion with pleural fluid toserum creatinine ratio more than one confirming the diagnosis of urino-thorax. A retrograde ureterocystogram showed filling defect in left kidney.The obstructed stent was replaced followed by successful resolution of pleuraleffusion.Discussion: Urinothorax occurs due to leakage of urine collection, knownas urinoma, from peritoneum and retroperitoneal space into the pleural spacethrough either diaphragmatic lymphatics or an anatomical defect in the dia-phragm. Confirmation is by a pleural fluid to serum creatinine ratio morethan one. Retroperitoneal fibrosis, shock wave lithotripsy, and removal/blockage of nephrostomy tubes may result in the formation of an urioma.Relief of urinary obstruction and drainage of urinoma is therapeutic.
This case supports the concept that urinothorax should be consideredwhenever transudative pleural effusion occurs in setting of urinary tract ob-struction or urologic intervention.
References:Current Opinion Pulmonary Med 12:259-263
63A
BOERHAAVE SYNDROME AS A COMPLICATION OFDELIRIUM TREMENS MANAGED WITHOUTTHORACOTOMY
Chaudary N, Malik S. UMMC, Jackson, MS.Case Report:Introduction: Boerhaave syndrome is a life threatening condition whichrequires prompt diagnosis and surgical repair. We report successful man-agement of Boerhaave syndrome in a patient with delirium tremens and chestpain without surgical intervention.Case presentation: A 65 year old male with a history of alcohol abusewas admitted with a twelve hour history of chest pain and vomiting. Hereported alcohol abuse and hallucinations. On physical exam, he had atemperature of 100.6, heart rate of 146, and respiratory rate of 22. Hehad decreased air entry with crackles in his left lung with guarding inright upper quadrant. Serum troponin and amylase were within normallimits. A chest xray showed pleural effusion. A CT scan of chest andabdomen showed a left-sided hydro pneumothorax a thickened, irregularesophagus pneumo mediastinum; and gallbladder wall thickening, all sus-picious for esophageal perforation. A Gastrograffin and thin barium eso-phogram was done to evaluate the esophagus and showed no obviousesophageal leak. Right upper quadrant ultrasound ruled out cholecystitis. Aleft sided chest tube was placed, and pleural fluid studies confirmedBoerhaave syndrome with a very high pleural fluid amylase to serumamylase ratio. Esophagoscopy showed red inflamed mucosa close to thegastric junction without obvious perforation. Patient was successfully re-suscitated with intravenous fluids, antibiotics, and stomach decompressionwithout thoracotomy.Discussion: Esophageal rupture often presents as the triad of chest pain,vomiting, and subcutaneous emphysema or pneumomediastinum. There is aclear association between time lapse from perforation to the onset of treat-ment and rate of survival. Patients may have a pleural effusion with highamylase concentration (from saliva), low pH, and particles of food. Its treatmentincludes immediate antibiotic therapy to prevent mediastinitis and sepsis,surgical repair of the perforation, and intravenous fluid therapy since oralrehydration is not possible. Our patient was treated medically, yet had a suc-cessful outcome.
References:Cases journal 2009,2:800 PMID: 12653057, 2762634 Indexed for medline
64
SEVERE LEG PAIN AND PROFOUND REVERSIBLEACIDEMIA
Nantsupawat T, Mankongpaisarnrung C, Soontrapa S, Limsuwat C, Nugent K.Texas Tech University Health Sciences Center, Lubbock, TX.Case Report: Lactic acidosis implies tissue hypoxia or impaired aerobicmetabolism in mitochondria. It can be dramatically reversed if the incitingfactor is halted. Grand mal seizures, strenuous exercise, propofol infusionsyndrome, alcoholic intoxication with thiamine deficiency, high dose met-formin, and repeated intravenous infusions of sorbitol and ethanol have beenreported as causes of transient or reversible lactic acidosis. Here we report anuncommon cause of reversible lactic acidosis.
A 57-year-old man presented with sudden severe right leg pain. Initial labstudies revealed lactic acid of 15mmol/L with a pH of 6.6. Extremities hadnormal pulses bilaterally, no weakness, numbness, or tenderness. Lactic acidlevels fell spontaneously to 2.5mmol/L 14 hours after pain onset. He wasclinically improved and extubated. Five hours after extubation, he developedsevere left leg pain with poikilothermic, pale, pulseless, and prominent livedoreticularis throughout his left leg. Lactate level rebounded to 8.13mmol/Lwith a pH of 7.29. ACT pulmonary and aorta angiogram revealed acute arterialocclusion of infrarenal abdominal aorta extending to bilateral common iliacarteries, external iliac arteries, and common femoral arteries. The patient hadcardiac arrest and died.
Acute arterial occlusion is typically presents with six ‘‘Ps’’: pain, pallor,pulselessness, poikilothermia, paresthesia, and paralysis. A patient we de-scribed here presented with transient right leg pain and profound reversiblesevere lactic acidosis which is an uncommon presentation of acute arterialocclusion. This delay in recognition and revascularization led to mortality inthis patient. Acute arterial occlusion should be included in the differentialdiagnosis of reversible lactic acidosis and requires urgent investigation.
65
SEVERE HYPONATREMIA: A CASE OF BEER POTOMANIA
Paccione R1, Engel LS1, DeBlieux P2. 1LSU Health Sciences Center, NewOrleans, LA and 2LSU Health Sciences Center, New Orleans, LA.Case Report:Introduction: Beer potomania presents as seizures, alterations in mentalstatus and is associated with a classic laboratory value of hyponatremia. Herewe describe a case that exhibited this triad of findings secondary to excessiveintake of beer.Case: A 62-year-old Caucasian man with a history of hypertension andalcohol abuse presented to the emergency department following a syncopalevent. He subsequently had seizure activity in the emergency department andwas intubated for airway protection. The patient drank 6 to 8 beers per dayand had poor nutritional intake. Triage vital signs included a temperature36.8 oC, heart rate 75 bpm, blood pressure 143/82 mmHg, respiratory rate20/min and, oxygen saturation 100% on room air. Serum chemistries in-cluded: Sodium 111 mmol/L, potassium 3.5 mmol/L, chloride 73 mmol/L,bicarb 26 mmol/L, BUN 11 mg/dL, creatinine 0.7 mg/dL, glucose 114 mg/dL,calcium 9.1 mg/dL. Tylenol and aspirin levels were undetectable. Urine so-dium was 20 mmol/L, urine osmolality was 120 mOsm/kg and his urine Toxscreen was negative. Following a two liters normal saline bolus, repeat serumsodium was 112 mmol/L. He was then bolused 50 mL of 3% saline and placedon a hypertonic saline drip. He was slowly corrected 10 mEq in the first24 hours and another 10 mEq over the next 48 hours. Upon discharge,sodium had normalized to 137 mmol/L. The diagnosis of beer potomania wasmade based on history, clinical presentation and laboratory findings.Discussion: Beer potomania is traditionally defined as the ingestion of largequantities of beer that can lead to severe hyponatremia, mental status changes,seizures and dilute urine. These patients typically have a history of excessivebeer drinking and poor dietary intake. The combination of minimal intake ofsolute and large amounts of hypoosmolar beer will lead to the inability toexcrete adequate amounts of freewater to keep up with the ingestion. Treatmentis dependent upon the severity of hyponatremia. Treatment with isotonic
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 391
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

sodium chloride should result in clearance of the free water. However, hy-pertonic saline is often used to aid in this process when isotonic saline aloneis not effective.
66
KERNOHANS NOTCH - AN UNUSUAL CAUSE OFHEMIPLEGIA
Panikkath R, Panikkath D, Lik Lim S, Nusrat M, Nugent K. TTUHSC,Lubbock, TX.Case Report:Introduction: The presence of hemiparesis ipsilateral to the site of a ce-rebral lesion has been called Kernohan’s notch. This sign has been reported incerebral tumors, subdural hematomas (SDH), and extradural hematomas withmidline shift. This sign was originally described after autopsy. Recently MRIhas been used to make diagnosis. However, computerized tomography (CT)of the head has not been used for the diagnosis of this syndrome.Methods: This is a case report of a patient with an unusual cause forhemiplegia.Results: A 69 year old woman with Alzheimer disease was referred to ourhospital in a comatose state. Detailed history from relatives indicated that shehad a history of recurrent falls. A CT head showed a large right subduralhematoma with midline shift of 18mm. She underwent urgent neurosurgicalevacuation of subdural hematoma. Her consciousness gradually recovered,but it was noted that she was unable to move the right arm and leg. An MRIdid not show any left-sided infarcts, which could explain this. Since herhemiplegia was ipsilateral to the side of subdural hematoma, the possibility ofKernohan’s notch was considered. Gross deviation of the crura of midbrainto the left side was noted on detailed review of CT head done prior to theevacuation of hematoma. The MRI pictures also showed evidence of shiftof midbrain to the left. A clinical picture of ipsilateral weakness in a patientwith subdural hematoma, evidence of compression of midbrain in CTand MRIbrain and absence of any infarcts on the contralateral side in diffusion weighted,T1 and T2 sequences of MRI confirmed our suspicion of Kernohans notch.Conclusion: Paralysis ipsilateral to the site of lesion in the brain could bedue to compression of the contralateral cerebral peduncles against the toughdural reflections causing damage to the pyramidal tract fibers in the brainstem. This false localizing sign needs to be recognized to prevent inappropri-ate surgery and medical management, including thrombolytics in patients withhemiplegia.
67
SWEET SEIZURES - EPILEPSIA PARTIALIS CONTINUA
Panikkath R, Lado J. TTUHSC, Lubbock, TX.Case Report:Introduction: Epilepsia partialis continua (EPC) refers to recurrent focalseizures that are focal and recurring every few seconds or minutes for ex-tended periods of time. Causes of this include stroke, neoplasia, viral in-fections, vascular malformations and Rasmussens encephalitis. Metabolicdisorders can rarely cause this disorder.Methods: This is a case report of a patient with epilpesia partialis continua.Results: A 65 year old female presented with recurrent involuntary move-ments of both upper extremities. This was disregarded as involuntary move-ments by the emergency room physician. However the recurrent focalmovements were suggestive of focal seizures (shown in video). She was con-scious, oriented and was conversing coherently during the episodes. Some ofthe episodes were followed by short lasting paralysis affecting the upperlimbs. She had diabetes mellitus type 2 with a plasma glucose level of814 mg/dl. Serum acetone was negative and measured serum osmolality was350 mOsm/L, indicating hyperglycemic hyperosmolar state (HHS). The in-voluntary movements stopped when euglycemia was reestablished. She hadsimilar movements two days before this episode, when she was treated atthe emergency department for hyperglycemia (plasma glucose 800 mg/dl),which again had subsided after reestablishment of euglycemia. An EEG(when euglycemic) and brain MRI were unremarkable. Recurrent focal sei-zures with short interictal periods, associated with Todds paralysis, suggestthat the patient had EPC precipitated by HHS.Conclusion: Although hyperglycemic hyperosmolar state is the most com-mon cause of reversible epilepsia partialis continua in adults, this cause may
often be overlooked. Correction of underlying metabolic abnormality is thetreatment for this condition rather than antiepileptic drugs.
68
GASTROESOPHEGIAL FISTULA, UNCOMMONCOMPLICATION FOR COMMON SURGERICALPROCEDURE
Sherif KA, Nusrat M, Aly M, Phy M. TTUHSC- Lubbock, Lubbock, TX.Case Report:Intoduction: Gastropericardial fistula is an acquired disorder with an abnor-mal communication between the stomach and the pericardium. It is associ-ated with high mortality rate. It is a rare complication of laparoscopic surgeryfor reflux disease and thoracic procedures. The hiatal hernia repair can causesubstantial life-threatening morbidity like gastropericardial fistula.Case: This is 74 year old lady with history of GERD and hiatal herniathat was surgically corrected 6 years ago, presented with chest pain anddyspnea. Physical examination was normal apart of cardiac examination thatshowed pericardial rub. Laboratory data showed leukocytosis. Chest X-rayshowed left side mass. Transthoracic echocardiography showed pericar-dial effusion with physiological temponade. Chest and abdominal CT scanshowed pericardial effusion with hiatal hernia and gastroperocardial connection(figures will be shown in presentation). Patient had hiatal hernia repair, eso-phagectomy, subtotal gastrectomy, and pericardial window and she improvedeventually.Discussion: Laparoscopic repair of hiatal hernia and GERD is known to beas a safe procedure. More than 90% of patients have had long-term positiveoutcome. Gastropericardial fistula is an uncommon complication for that pro-cedure but it has very high mortality rate which was estimated around 50%.Among conditions that result in gastropericardial fistula, peptic ulcer, hiatalhernia and esophagogastric surgery has been the most frequently reported.The occurrence of post-operative gastropericardial fistula is induced by theperihiatal scarring. In addition, recurrence of hiatal hernia or migration ofthe surgical wrap may also favor occurrence of fistula. Clinical features ofgastropericardial fistula are variable, ranging from dyspnea, precordial tym-pany, and pericardial friction rub to severe chest pain. For the gastropericardialfistula, contrast media-enhanced traditional examinations are the cornerstoneof diagnosis. Abdominal CT may reveal the fistula. Our patient did not receivea conventional barium exam because residual barium may produce artifact onsubsequent CT. Surgical correction is the most effective way for treatment.Conservative treatment is reserved for those with severe illness and carries ahigher mortality rate.
Joint Plenary Poster SessionCardiovascular Case Report
5:00 PMThursday, February 21, 201369
SINUS OF VALSALVA ANEURYSM RUPTURE: AN UNUSUALPRESENTATION OF CHROMOSOME 22q11.2 DELETION
Abuchaibe E. 1Miami Children’s Hospital, Miami, FL and 2Miami Children’sHospital, Miami, FL.Case Report: Sinus of Valsalva aneurysm (SVA) is defined as aweakness inthe aortic valve wall, immediately above the attachments of each of the aorticcusps. This weakness can rupture and create an aorto-cardiac fistula. Thereare many congenital heart defects associated with chromosome 22q11 de-letion, especially involving the aortic arch and its branches. SVA is not ananomaly usually associated with chromosome 22 deletion.
We report the case of a 19 year old female who presented to our insti-tution with SVA rupture. She was subsequently diagnosed with chromosome22q11 deletion syndrome. Despite dysmorphic facial features and a learn-ing disability, our patient had not been diagnosed with the chromosomeabnormality.
SVA is a rare congenital heart defect and has only once previously beenreported in a child with a chromosome 22q11 deletion. We report thefirst case where aneurysm rupture preceded the chromosomal findings.Chromosome 22q11 deletion could be missed due to either the unfamiliarity
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
392 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of physicians with the syndrome or the variability and subtlety of the phe-notype. This was demonstrated by our patient who, at age 19 after presentingwith an SVA rupture, prompted physicians to find an explanation for her co-existing dysmorphic features and her learning disability.
70
A FLOATING THROMBUS IN THE ASCENDING AORTA
Modica M1, Lathia V1, Subramaniam P1, Weaver M2. 1LSUHSC - NewOrleans, New Orleans, LA and 2Oschner Medical Center, Kenner, LA.Case Report: A 51-year-old African American male with a history of re-current pancreatitis and alcohol abuse presented to the emergency room forepigastric abdominal pain, which was similar to his previous pancreatitispain. The patient does not smoke and quit drinking about a year ago. Physi-cal exam was unremarkable for epigastric tenderness at the time of admis-sion, although during hospital course, he developed transient left arm weaknesswithout headache or any other focal neurological deficit. MRI of the brainrevealed acute infarct of the right corona radiata and subacute infarct of theleft occipital lobe. Embolic events were suspected and a transesophagealechocardiogram was ordered, which showed no valvular abnormality or ev-idence of intracardiac thrombus, although visualization of the ascendingaorta showed a mobile thrombus. Suprasternal view of transthoracic echo-cardiogram was performed, revealing a large, mobile, serpiginous thrombusin the ascending aorta. He underwent surgery for an ascending aorta thrombusremoval. Surgery was uneventful and a 4x1 cm long thrombus was removed.Histopathology of the thrombus confirmed that it was an organizing throm-bus. His workup for hypercoaguable state was negative.
Ascending aortic arch thrombus is a very rare finding. Patients gener-ally present with embolic events such as stroke, mesenteric ischemia, or limbischemia. Occasionally, it can be seen incidentally on echocardiography. Theyare associated with aortic dissection, aortic atherosclerotic disease, coagu-lopathy, prior aortic graft, or surgery. Echocardiogram is the preferred imagingbut CT or MRI can also help in evaluation of thrombi. Workup for coagulo-pathy, including lupus anticoagulant, anticardiolipin antibody, and Protein Cand S deficiency, should be performed when thrombus arises de novo.
Management of aortic arch thrombus is controversial. Medical manage-ment such as thrombolytics or heparin and warfarin are effective but thereis increased risk of embolization in mobile, serpiginous thrombi. Surgery ispreferred in these patients. Surgery involves aortic arch exploration and re-moval of thrombus after achieving circulatory arrest and femoral bypass.Patients with atherosclerotic plaques should be placed on antiplatelet ther-apy to prevent recurrence of thrombi.
71
MASSIVE CARDIAC HEMANGIOMA
Marcial JM1, Altieri PI1, Defendini E2, Maldonado J1, Gurrea CM2.1University of Puerto Rico, San Juan, Puerto Rico and 2CardiovascularCenter of Puerto Rico and the Caribbean, San Juan, Puerto Rico.Case Report: A 67-year-old woman presented to our institution after hav-ing 3 months of fatigability upon exertion. After initial work-up, contrast ChestCT through the heart demonstrated a lobulated, 9.8cm long x 6.2cm antero-posterior x 4.4cm transverse, pericardial mass located in the right cardiacborder with soft-tissue density and a few punctate interspersed calcifications.The patient was taken to the operating room for excision of the cardiac mass.The final report from pathology confirmed the cardiac mass to be a caver-nous hemangioma. Cardiac hemangiomas are extremely rare, representingless than 2% of all primary cardiac tumors. Depending on the size and lo-
cation of the mass, symptoms, if any, can include, arrhythmias, congestive heartfailure, pericardial effusion, syncope and sudden death. To our knowledge, lessthan 30 cases of cardiac hemangiomas have been described in the Englishliterature worldwide.
72
A TUBERCULOMA PRESENTING AS A LEFT ATRIAL MASS
Askari R, Ahmad KA, Das PA. University of Tennessee Health ScienceCenter, Memphis, TN.Case Report:Purpose: Tuberculosis (TB) has protean manifestations and can infect anyorgan. Herein, we describe a case in which it presented as a space-occupyingmass, or tuberculoma, of the left atrium.Case Report: A 25-yr-old African-American woman presented to theEmergency Department at Methodist University Hospital in Memphis withmultiple complaints of several months’ duration: nausea and vomiting; confu-sion and short-term memory loss; blurred vision; subjective fever with nightsweats; and unintentional weight loss. Past medical history was significant forpericardial effusion and pericardiocentesis at age 9. Her father had been di-agnosed with active TB when she was 6 yrs old, but neither he nor familymembers were treated. She denied travel outside of Memphis or the US.
On examination, the patient was found to have elevated temperature100.5-F and a rapid pulse 100 bpm. Jugular veins were not distended, apicalimpulse was not displaced, and no gallops, murmurs or rub were appreciated.She was only oriented to person while neurologic exam was noncontributory.No skin rash was appreciated.
Pertinent laboratory: hematocrit 26.9% with schistocytes on peripheralsmear; platelet count 20,000 hpf; serum creatinine 1.4 mg/dL; elevated lactatedehydrogenase 682 IU/L; and undetectable haptoglobin.
Plasmapheresis for 10 days led to stabilization and resolution of herputative thrombocytopenic purpura/hemolytic uremic syndrome. A persistentfever, however, prompted interrogation for possible endocarditis. A trans-thoracic echocardiogram identified a large calcified vegetation presumptivelyinvolving the posterior mitral valve leaflet. Subsequent transesophageal andcontrast CT imaging identified a calcified mass in the left atriumwhich surgicalresection and histologic examination revealed to be a 2�3 cm mass havingacute and chronic granulomatous inflammation with necrosis and areas ofcentral caseation. It was diagnosed as a tuberculoma and patient was placedon anti-TB therapy with rifampin, isoniazid, pyrazinamide and ethambutolfor 2 months and INH and rifampin for a total of 9 months. She was followedfor 18 months and has done well with no recurrence of symptoms.Conclusions: The protean and unusual manifestations of TB require ahigh index of suspicion for its diagnosis and management.
73
EARLY RECURRENCE OF LEFT ATRIAL MYXOMA
Figueroa R1, Banchs H1, Altieri P1, Gonzalez I2. 1University of Puerto RicoSchool of Medicine, San Juan, Puerto Rico and 2Cardiovascular Center ofPuerto Rico, San Juan, Puerto Rico.Case Report: A 50-years-old woman with history of hypothyroidism, di-abetes mellitus type II, fibromyalgia and a left atrial myxoma resected atage 47. Patient was admitted to our institution after an episode of syncope.
Physical examination was unremarkable except for a diastolic murmurwith a classical tumor plop. Echocardiogram showed a large mobile masson the left atrium with mitral regurgitation. Transesophageal echocardiogramconfirmed the finding of a large 4 x 2.2 cm pedunculated mass attached to theanterior leaflet of the mitral valve causing moderate valve regurgitation.
She underwent left atrial myxoma excision and mitral valve replacement.Hospitalization was complicated by deep vein thrombosis of the right sub-clavian and cephalic vein. Five days after procedure she was discharge homeon warfarin anticoagulation.
Atrial myxomas are the most common primary heart tumors, despite thistheir incidence is as low as 0.5 - 1 per million population per year. Sporadicrecurrence is reported in 4-7% of cases with interval formation taking usuallyover 4 years. The tumor may be asymptomatic and found incidentally or maypresent as symptoms of heart failure, dizziness, syncope, or findings relatedto embolization. We present a case of early recurrence of a large left atrialmyxoma presenting as a syncope in female patient.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 393
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

74
SYMPTOMATIC DOUBLE AORTIC ARCH IN AN ADULT
Choksy P1, Zaidi SS2, Arora V2, Kamath V2. 1Georgia Health SciencesUniversity, Augusta, GA and 2Georgia Health Sciences University, Augusta, GA.Case Report: The vascular ring anomaly of aortic arch accounts for 1-2% ofcongenital heart diseases of heart and aorta. Double aortic arch (DAA) andits management have been abundantly described in childhood. We report a rarecase of symptomatic adult presented with dysphagia associated with DAA.
52 year old white male was seen in clinic for dysphagia and weight lossof 40 lb. over period of 6 months. He had extensive workup which was negativeformalignancy.Multidetector computer tomographyof the chest was performedwhich revealed a double aortic arch with predominant right arch forming avascular ring and thus compressing the esophagus. Barium esophagogramrevealed pulsatile extrinsic compression of esophagus from the vascular ringformed by DAA. Left heart catheterization was also performed which con-firmed double aortic arch with non obstructive coronaries. He then underwentleft thoracotomy with division and repair of left aberrant arch and alsoesophageal dilatation without any complications. He continued to show clinicalimprovement with appropriate gain in weight during follow up clinic visits.
During embryogenesis, failure of the normal regression of one or moresegments of the six pairs of the aortic arches that arise from the truncusarteriosus leads to the formation of multiple anomalies of the aortic archwhich can result in complete or incomplete vascular ring depending on theencirclement of trachea and esophagus. Vascular rings can result in com-pression of tracheobronchial tree and/or esophagus, leading to respiratoryand gastrointestinal symptoms. Respiratory symptoms are common in thecase of vascular rings in infancy or early childhood. On the other hand, adultpatients complain of difficulties in swallowing rather than respiratory diffi-culties because of tracheal development. The above patient had a completevascular ring formed by the right-sided aortic arch and compressive left com-ponent, both of which rejoined posteriorly to form a single descending thoracicaorta. CT and MRI are important diagnostic modalities and provide great an-atomical details for surgical intervention. Surgical intervention involvingdivision of minor arch is indicated for adult patients who are symptomaticand have excellent clinical outcomes.
75
TAKOTSUBO CARDIOMYOPATHY WITH LEFTVENTRICULAR OUTFLOW TRACT OBSTRUCTION
Choksy P1, Zaidi S2, Kapoor D2, Robinson V2, Litwin S2. 1Georgia HealthSciences University, Augusta, GA and 2Georgia Health Sciences University,Augusta, GA.Case Report: Takotsubo cardiomyopathy also known as transient leftventricular apical ballooning syndrome or broken heart syndrome is a clinicalentity mimicking an acute coronary syndrome (ACS). It is characterized byreversible left ventricular dysfunction that is frequently precipitated by a stress-ful event either emotional or physical stress. We present a case of 57 year oldfemale with an atypical variant of Takotsubo cardiomyopathy with concom-itant Left ventricular outflow tract (LVOT) obstruction who presented as ACS.
57 year old white female presented with acute onset chest pain. She washypotensive and tachycardic on presentation. Electrocardiogram (EKG) showedright bundle branch block and ST-T wave changes. Troponin was elevated(0.33 ng/ml). Patient underwent urgent Left heart catheterization which showed
non obstructive coronaries with low ejection fraction (EF) (30%), apical bal-looning, basal hyperkinesis and severe LVOT obstruction. Transthoracic echo-cardiogram revealed EF of 45% with hyperdynamic base, apical ballooning,systolic anterior motion (SAM) and LVOT gradient 9100mm Hg. She wasresuscitated with intravenous fluids and metoprolol. Hemodynamics improvedwith resolution of tachycardia and hypotension. She was later found to havediffuse metastatic small cell cancer of lung. She died during the hospital course.
Underlying etiology for Takotsubo cardiomyopathy is not well knownand various mechanisms have been proposed but most likely is related to cat-echolamine excess.Takotsubo cardiomyopathy with concomitant LVOT ob-struction is an atypical variant found in 25% of cases. It can result in fatalcomplications like cardiogenic shock and arrhythmias. Orthodox managementof cardiogenic shock with inotropes and intra-aortic balloon pump is contra-indicated in this atypical variant as it can worsen the gradient and hypotension.Mainstay treatment includes beta blockers and intravenous fluid resuscitationdespite presence of cardiogenic shock. Alpha-1 agonists also have some role byincreasing afterload with subsequent reduction of the intraventricular gradient.Early detection of this variant of takotsubo syndrome is vital to avoid standardmanagement of cardiogenic shock which can lead to fatal outcomes.
76
UPPER EXTREMITIES VEIN THROMBOSIS: ANUNCOMMON COMPLICATION AFTER PERMANENTPACEMAKER PLACEMENT
Dumrongmongcolgul N, Mankongpaisarnrung C, Limsuwat C,Sutamtewagul G, Nugent K. Texas Tech University Health Sciences Center,Lubbock, TX.Case Report:Introduction: Upper extremities vein thrombosis (UEVT) is an uncommoncondition. The etiology includes primary thrombosis, Paget-Schorettersyndrome which is less common than secondary causes such as hyperco-agulable states, and complications from procedures such as central venouscatheter (CVC) or pacemaker placement (PP). Risk factors include historyof cancer, subclavian vein puncture, and left side catheter placement.Case presentation: A 66-year-old woman with history of hypertensionpresented with dizziness and fatigue. She has been taking hydrochlorothaizideand nifidipine for BP control. She was found to have bradycardia with heartrate of 34 bpm. Her exam was within normal limit. 12-lead ECG revealedthird degree AV block; therefore, she was hospitalized for pacemaker place-ment via axillary vein access. Her hospital course was uneventful and she wasdischarged home in 2 days. She returned to the clinic because of pain andswelling in her left arm without history of trauma. Physical examination re-vealed swelling and cold left upper extremity. Chest x-ray showed normalpacemaker lead placement without lead fractures. Venous duplex ultrasoundrevealed deep venous thrombosis (DVT) of subclavian, axillary, brachial, andproximal radial vein. Enoxaparin followed by warfarin were initiated. Her leftarm swelling was resolved, and repeat venous duplex ultrasound did notreveal evidence of DVT one month after discharge.Discussion: Approximately 4 to 10 % of DVT occurs in upper extremities.Axillary and subclavian veins are most affected veins. The incidence rate isincreasing because of an increase of CVC use, PP, and defibrillator devices.Complications of DVT which include pulmonary embolism and post-thrombotic syndrome are lower in UEVT than in lower extremities DVT.Those with UEVT can manifest with upper extremities edema, venous en-gorgement, and pain. Investigations include venous Doppler, CT venography,and venogram. Anticoagulant for 3-6 months is the mainstay of treatment ofUEVT. Common complications from PP include bleeding, infection. UEVTeven though is uncommon entity, should still be considered in isolated upperextremities edema after PP.
77
ISCHEMIC CEREBROVASCULAR ACCIDENT ASPRESENTATION FOR ISOLATED NON-COMPACTIONCARDIOMYOPATHY
Ricci Gorbea F1, Banchs H1, Altieri P1, Pabon A2, Maldonado J2. 1Universityof Puerto Rico School of Medicine, San Juan, Puerto Rico and 2University ofPuerto Rico School of Medicine, San Juan, Puerto Rico.Case Report: A 51-year-old man with a presumptive diagnosis of dilatedcardiomyopathy of unknown etiology and left atrial appendage thrombus, on
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
394 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

warfarin therapy was admitted with decompensated heart failure. Duringhospitalization, he suffered a right midbrain cerebrovascular accident con-firmed by brain MRI.
A transthoracic echocardiogram demonstrated a hypokinetic, markedlydilated left ventricle with systolic dysfunction (30% ejection fraction). Prom-inent trabeculations protruding toward the cavity were noted. Color flowDoppler and intravenous contrast-enhanced echocardiography demonstratedblood flow in between the trabeculae, compatible with left ventricular noncompaction (LVNC). Cardiac MRI confirmed that diagnosis. The ratio ofnoncompacted myocardium with respect to the compacted myocardium wasgreater than 2.3.
Non-compaction of the left ventricle is an extremely rare form of car-diomyopathy caused by arrest of normal embryogenesis of the endomyo-cardium. It is characterized by a thickened myocardial wall with prominenttrabeculae and deep intertrabecular recesses with two layers consisting of non-compacted and compacted myocardium. Diagnosis is usually made by echo-cardiography and other imaging modalities like cardiac MRI.The most commonmanifestations of LVNC are arrhythmias, heart failure and cardioembolicevents, as in this case. This is the third case of LVNC seen at our institution,and the second one complicated with a stroke.
78
A PROLONGED, REFRACTORY CASE OF ASTHMA?MAYBE NOT
Jordan M, Korah-Sedgwick M, Engel LS. LSU Health Sciences Center, NewOrleans, LA.Case Report:Introduction: Subaortic stenosis may present with dyspnea worsened withexertion and symptomatic systolic murmurs should warrant a thorough car-diac evaluation.Case: A 47-year-old woman with asthma, recurrent bronchitis, and a benignchildhood cardiac murmur developed weakness, cough, and fatigue. She wasseen by her PCP who diagnosed her with bronchitis and prescribed herantibiotics. However, her symptoms were not alleviated, and she presented toher PCP 3 months later with the same complaints and new onset dyspnea onexertion with any ambulation over 50 feet. She was diagnosed with an asthmaexacerbation and given long-acting beta agonists and inhaled corticosteroids.She continued to clinically deteriorate, with constant weakness and dyspneawith any activities of daily living. After failing two trials of outpatient glu-cocorticoids, she was admitted for further evaluation and treatment of herpersistent weakness and dyspnea. Further history on admission revealed anunintentional 50-pound weight loss, and an inability to sleep due to herdyspnea, all despite using her albuterol inhaler 6 to 7 times per day. Physicalexamination was notable for hypotension, a grade III/VI midsystolic cre-scendo-decrescendo murmur located at the right 2nd intercostal space at thesternal border without radiation to the carotids which did not change withvalsalva or clenching of the fists, rales at the bilateral lung bases with poorinspiratory effort but no wheezing, and diminished peripheral pulses com-pared to systolic auscultation. Laboratory studies were normal and chest
radiography revealed cardiomegaly. Transthoracic echocardiography revealeda thick, circumferential subaortic membrane approximately 8mm below theaortic valve. During cardiothoracic surgery she was found to have a fibroussubaortic membrane with muscular asymmetry of the septum. She success-fully underwent resection of the subvalvular aortic ring with myectomy ofventricular septum. She tolerated the post-operative period well and was dis-charged to home 4 days following the procedure.Discussion: Subaortic stenosis is the second most common form of aor-tic stenosis and is presumed to be due to a left ventricular outflow tractobstruction, in which turbulent flow leads to progressive fibrosis and wors-ening symptoms.
79
APICAL BALLOONING SYNDROME
Su J, Habib S, Yalamanchili K. Texas Tech University Health Sciences Center,Amarillo, TX.Case Report: A 55-year-old woman presented with 2 week history ofgradually worsening nausea, vomiting, and epigastric pain. Esophagogas-troduodenoscopy revealed a large pyloric ulcer with severe gastric outletobstruction. An uneventful partial gastrectomy was performed. Postopera-tively patient developed sudden onset of palpitations and tachycardia fol-lowed by hypotension and apnea. She was intubated, mechanically ventilated,and vasopressors initiated. CT angiogram showed pulmonary embolism, forwhich heparin drip was initiated. EKG was normal but Troponin I was ele-vated with peak value of 2.25 ng/mL. Echocardiogram revealed generalizedakinesis of the left ventricle with ejection fraction of 10%. Ventriculogramdemonstrated ballooning of a majority of the left ventricle. Coronary vesselswere patent. Her condition improved gradually, vasopressors were weaned offand mechanical ventilation was discontinued. Repeated echocardiogram 8and 14 days later revealed significantly improved cardiac function with LVEFof 45% and 75%, respectively.Discussion: Apical Ballooning Syndrome, also known as Takotsubo Car-diomyopathy, or Broken Heart Syndrome, is an acute cardiac condition causedby emotional or physical stress. It occurs mostly in postmenopausal women.Etiology is unknown, but might be related to coronary vasospasm or abnormalresponse to catecholamines. Temporary weakening of the myocardium oc-curs, usually at the apex. Patients typically present with chest pain, dyspneaas well as EKG changes similar to that of acute anterior wall myocardialinfarction. Cardiac enzymes can be mildly elevated. Diagnosis is made by thepathognomonic wall motion abnormalities in which the base of the left ven-tricle is contracting normally while the remainder of the LV is akinetic. Thisfinding on ventriculogram is accompanied by the lack of significant coro-nary artery disease that would explain the wall motion abnormalities. Treatmentis generally supportive with fluids, ACE inhibitors, A-blockers or calciumchannel blockers. Inotropes can be used cautiously in patients without LVoutflow obstruction. Intra-aortic balloon pump is the preferred therapy whenthere is marked LV dysfunction. Prognosis is excellent with rapid improve-ment of LV systolic function within several days to a few weeks. Recurrenceor relapse may occur.
80
FATALVASODEPRESSOR SYNCOPE IN A PATIENT WITHREFRACTORY IDIOPATHIC THROMBOCYTOPENICPURPURA
Eubanks J, Waespe CK, Geraci SA. University of Mississippi Medical Center,Jackson, MS.Case Report: Vasodepressor syncope may develop from a number ofpathologic conditions and can be accentuated by hypovolemia. There are noreports of deaths due to vasodepressor orthostasis. An 81 year old man withchronic atrial fibrillation/flutter, diabetes, hypertension, chronic kidney dis-ease, and chronic lymphocytic leukemia (CLL) underwent splenectomy forrefractory idiopathic thrombocytopenic purpura (ITP). Preoperatively, plate-lets were 3000/mm3; bone marrow was consistent with ITP and CLL. ECGrevealed atrial flutter/fibrillation, right bundle branch and left axis deviation.Left ventricular function was normal. Splenectomy was uncomplicated, withG100 mL blood loss; platelets improved to 214,000/mm3. On postop days 2and 3, he suffered three syncopal episodes, initially upon standing, then uponsitting; no rhythm changes occurred on telemetry. He was treated with IV
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 395
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

fluids. During further evaluation, another syncopal episode occurred uponmoving to a sitting position. Despite immediate supine positioning, he rapidlybecame pulseless and apneic. Throughout resuscitative efforts, he displayedan irregular rhythm at È90 bpm or a regular rhythm at È150 bpm, with awide QRS complex Y unchanged from pre-arrest rhythms. Despite hydrationand vasopressors, he remained pulseless. Echocardiogram confirmed cardiacstandstill despite a continued survivable rhythm. Autopsy was declined. Theetiology of our patient’s fatal vasodepressor syncope is uncertain. A similarepisode occurred a year earlier; he had no detailed evaluation or intercedingorthostatic symptoms. Despite underlying conduction disease, cardiac rhythmduring resuscitative efforts was unchanged from his prior perfused rhythm.No evidence of autonomic dysfunction or adrenal insufficiency was present,and his anemia had only mildly worsened. Though his platelet count hadrecovered, recurrent episodes precipitated only orthostatically, with recoveryto baseline shortly after multiple preterminal events, made recurrent pulmonaryemboli highly unlikely. Some degree of dehydration was likely present, butlack of response to hydration and vasopressors makes hypovolemia alone un-likely to be causative. Vasodepression has not been associated with any med-ications he received.
81
WHERE DO BROKEN HEARTS GOILOUISIANA
Laura S, Jordan M, Mabry C, Gendusa P, Abide W, Engel LS, Jain N. LSUHealth Sciences Center, New Orleans, LA.Case Report:Introduction: We present series of cases of Broken Heart Syndromerecently seen at our facility.Case 1: A 53-year-old man with a long history of alcohol abuse presentedwith weakness in his knees and difficulty standing. He was given painmedications and a benzodiazepine taper. He then returned two days later afterbeing found incoherent and tremulous. He was diagnosed with non-ST-elevation myocardial infarction. EKG revealed diffuse T-wave inversions andhis cardiac enzymes remained elevated. Left heart catheterization showed noevidence of obstructive coronary artery disease with an estimated left ven-tricular systolic ejection fraction of 20-25%, and a ventriculogram illustratedapical ballooning and dyskinesis without evidence of mitral regurgitation.Case 2: A 77 year old woman with a history of stage IV lung cancer wasadmitted to the ICU with shortness of breath and a pleural effusion. An echo-cardiogram at admission showed normal LV function. Following transfer tothe floor, she experienced a sudden onset of chest pain and worseningshortness of breath requiring intubation. Her EKG showed ST-elevation in9 leads concerning for an acute infarct. Her left ventriculogram showed ahypercontractile base with apical ballooning.Case 3: A 57-year-old woman with a history of hypertension and diver-ticulitis presented after a sigmoid colectomy with dyspnea and sudden onsetsubsternal chest pain. The patient admitted to severe stressors in her life thatwere only compounded by her recent hospitalization. There was a mild in-crease in her cardiac enzymes with nonspecific T-wave changes in her lateralleads on EKG. An echocardiography showed an ejection fraction of 25%. Acardiac catheterization as an outpatient a few weeks after discharge revealednon-obstructive coronary artery disease and improved left ventricular function.Discussion: Stress-induced cardiomyopathy also known as Takutsubo car-diomyopathy or Broken Heart Syndrome commonly mimics the acute cor-onary syndrome Factors such as acute emotional stress, acute withdrawalfrom alcohol and other sedative hypnotics may precipitate such a crisis. Thissyndrome is characterized by a transient decrease in systolic function withreversible left ventricular apical ballooning in the absence of significantcoronary disease.
82
CARDIAC TAMPONADE AS THE PRESENTING FEATURE OFSYSTEMIC LUPUS ERYTHEMATOSUS
Singh M1, Grewal G2, Jain N1. 1LSU, New Orleans, LA and 2Leonard JChabert Medical Center, Houma, LA.Case Report: Systemic Lupus Erythematosus (SLE) is a collagen vasculardisease that often involves the heart, with the pericardium most commonlyaffected. This results in pericarditis or pericardial effusion that is usually mildin intensity. In a few patients, pericardial involvement may be the initial
presentation of SLE. Cardiac tamponade is a rare clinical manifestation, andrarely the first manifestation, almost always reported in females. Our patient,a 32 year old African American male, presented complaining of nocturnalcyclic fevers occurring for the past two weeks. During his workup an echo-cardiogram was performed to evaluate exertional dyspnea. It showed a largepericardial effusion worrisome for cardiac tamponade. He was transferred toour facility for further evaluation and treatment of his active cardiac issues.Upon arrival he presented with tachycardia, tachypnea and in mild distress.Physical exam was significant for the absence of rales and the presence ofmuffled heart sounds. A malar rash was evident. A repeat echocardiogramrevealed a large circumferential pericardial effusion with features of cardiactamponade including right ventricular diastolic collapse, right atrial systoliccollapse and excessive transmitral Doppler flow respiratory variation. Thepatient consequently underwent therapeutic pericardiocentesis followed bycorticosteroid therapy. Laboratory data confirmed the diagnosis of SLE, withcardiac tamponade as its initial clinical manifestation. Given the annual in-cidence of cardiac tamponade in SLE patients of only 1-2.5%Yoccurringalmost exclusively in womenVthis case highlights the need to be vigilant forpericardial disease in male patients with SLE.
83
AMLODIPINE-INDUCED REVERSIBLE COMPLETE HEARTBLOCK IN A PATIENT WITH PRIOR MOBITZ TYPE ISECOND DEGREE BLOCK
Broyles MG, Askari R, Weber KT. University of Tennessee Health ScienceCenter, Memphis, TN.Purpose of Study: Dihydropyridine calcium channel blockers have limitedeffects on the normal cardiac conduction system. However, these effects maybe intensified in patients with preexisting cardiac conduction abnormalities.Methods Used: A 58-year-old male was referred to the cardiology clinic atthe Regional Medical Center in Memphis for worsening dyspnea on exertionover several months. He was known to have Mobitz type I (Wenckebach)second degree heart block. Five months ago his primary care physician (PCP)had placed him on lisinopril, metformin, glipizide and simvastatin for dia-betes mellitus and lipid disorder, and amlodipine for the control of his hyper-tension. Vital signs: blood pressure 122/66 mmHg; pulse 50 beats/min andregular; and respiratory rate 14 breaths/min. Cardiopulmonary exam revealedcannon Awaves in the jugular veins; apical impulse was not displaced and therewere no gallops, murmurs, or rubs; and lung fields were clear. A presumptiveclinical diagnosis of complete heart block of uncertain etiology was made.Summary of Results: ECG confirmed the presence of complete heartblock, which was contrary to previous ECG findings. Hence, etiologic factorscontributing to the progression of complete heart block were investigated.Myocardial perfusion scan was noncontributory. Echocardiogram revealed anEF 965% without segmental wall motion abnormality. Workup for sarcoid-osis (serum ACE) and amyloidosis (A-2 microglobulin) were each negative.We therefore hypothesized that amlodipine might have played a role in theappearance of complete heart block and that it would be reversible upondiscontinuation of amlodipine. At follow-up one week later the patient statedhis dyspnea on exertion had improved, cannon Awaves disappeared from hisjugular veins, and repeat ECG revealed a reversal from complete heart blockback to Mobitz type I secondary heart block. Amlodipine was therefore per-manently withheld and his PCP was notified of our findings.Conclusions: Dihydropyridine calcium channel blockers, such as amlodi-pine, may have minimal effects on normal atrioventricular nodal conduction,but should be used judiciously in patients with preexisting nodal diseasebecause they can impair conduction leading to symptomatic heart failure.
84
VITAMIN D LEVELS IN STATIN INTOLERANT PATIENTSAND EFFECT OF VITAMIN D REPLETION ON SUCCESSFULSTATIN RECHALLENGE
Birg A1,2, Hwang I1,2, Miseracki A1,2, Heimberg M2,1, Childress R2,1, ElamM2,1. 1University of Tennessee Health Science Center, Memphis, TN and2Memphis Veterans Affairs Medical Center, Memphis, TN.Purpose of Study: Intolerance to statins, primarily myalgia, occurs in up to10% of statin-treated patients and poses a significant barrier to effectivetreatment of lipids. The underlying causes of statin intolerance are unknown,
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
396 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

however, vitamin D deficiency has been proposed as a causal factor. Thisstudy sought to determine if vitamin D levels are lower in statin-intolerantpatients and correspondingly if vitamin D repletion increases the probabil-ity of a successful statin rechallenge.Methods Used: This study was a retrospective chart review looking atstatin-intolerant (SI) cases referred to the lipid clinic at a governmental HMO.Controls (statin-tolerant (ST) and statin-naBve (SN)) were randomly selectedfrom lists of statin-treated patients and patients with recent vitamin D levels.Cases and controls were blindly chosen without prior knowledge of theirVitamin D levels. Among statin-intolerant cases, Vitamin D levels prior toand following statin rechallenge were determined; as well as, if there was anyVitamin D repletion during the time of the rechallenge.Summary of Results: LDL-C levels were significantly higher among SIcases compared to ST controls (154T3 mg/dl versus 98T4 mg/dl, respectively).Vitamin D levels varied between the three groups (P=0.0223) and were signifi-cantly lower in SI cases (22.4T1.6 ng/ml) versus SN controls (30.3T2.4 ng/ml).Vitamin D levels did not differ between ST (25.3T1.5 ng/ml) and SI cases.Among SI patients, 74.6% treated with Vitamin D were successfully re-challenged; 47.5% of those not treated with Vitamin D had a successfulrechallenge. This shows statistically significant increase in rechallenge suc-cess rate with Vitamin D treatment with a p-value of 0.0002.Conclusions: Vitamin D levels are decreased in statin-intolerant patientscompared to statin-naBve controls. Repletion with vitamin D increases thelikelihood of successful rechallenge with statin. These findings suggest thatvitamin D deficiency may be an important factor in statin intolerance. Thefinding that 25% of SI cases remained intolerant despite vitamin D repletion,on the other hand, suggests that additional as yet unidentified factors may beresponsible for statin intolerance.
Joint Plenary Poster SessionEndocrinology and Metabolism
5:00 PMThursday, February 21, 201385
DESIGNING MYDIABETESCONNECT.COM: A MIXEDMETHODS APPROACH TO THE DEVELOPMENT OF ACOMMUNITY RESOURCE WEBSITE FRO TYPE 2 DIABETES
Cotter AP, Agne A, Guzman A, Cherrington A. University of Alabama atBirmingham, Birmingham, AL.Purpose of Study: Type 2 Diabetes (DM) prevalence continues to growin the United States. The internet is an important tool for facilitating edu-cation and self-management behaviors in patients with Type 2 DM. Theobjective of this project was to design a community resource website to helppatients with Type 2 DM locate resources in their local community to aid inlifestyle modification.Methods Used: A mixed methods approach was used, including a sys-tematic literature review and a series of 8 semi-structured interviews withkey members of local community based organizations and the local safetynet hospital. The review examined internet-based DM interventions promot-ing lifestyle modification. The PubMed Search Engine was used to identifyprograms; a backwards search technique was used to obtain additional ref-erences. Inclusion criteria were: focused on adults with Type 2 DM, describedweb-based interventions for lifestyle modification and patient education, andincluded program evaluation. Semi-structured interviews were conductedwith 8 directors of community based programs and focused on understand-ing local resources and barriers to their utilization. Interviews were coded by2 reviewers for major themes and findings.Summary of Results: Nine studies met inclusion criteria; they used acombination of static education and interactive components to effect life-style modifications. Studies including interactive components had betteroutcomes for targeted measures; no study improved all possible targeted areasof lifestyle modification. Interviews highlighted a need for a local communityresource database, desire for up-to-date information, and interactive compo-nents. Key barriers for the local community included: transportation, af-fordability, internet access, and a need for basic diabetes education.Conclusions: With the information gathered we designed MyDiabe-tesConnect.com. The site is specific for the Birmingham area, allowing usersto locate resources and events as well as facilitating user communication withothers in their community.
86
OBESITY IN EARLY CHILDHOOD DIABETES
Draffin S, Nashatker K, Lewis K, Paulo R, Bowlby D.MUSC, Charleston, SC.Purpose of Study: Type I diabetes (T1DM) is traditionally seen in slimyoung children in comparison to Type 2 diabetes (T2DM) in older overweightchildren. Weight loss is a symptom at diagnosis and resolves with treatment.Body mass index (BMI) is a factor used in the classification of childhooddiabetes. With the increase in childhood obesity this dictum may not be true.The obesogenic theory suggests the increase in childhood obesity may beleading to the increase in T1DM in young children.Methods Used: This is a retrospective study of patients ages 3-9 yrs, di-agnosed with diabetes at MUSC in 2009. Clinical data was analyzed at timeof diagnosis and at follow-up visit (3-6 mo).Summary of Results: In 2009, 27 patients (48% male; 74% Caucasian,22% Black, 4% Biracial) average age 7.8 + 2.0 yr (3.2-9.9) were diagnosedwith diabetes (89% T1DM; 11% T2DM). Patient BMI distribution was 33%obese (995%tile); 4% overweight (85-94%tile ); 30% normal (50-84%tile )and 33% underweight (G 50%tile ). Initial average BMI Z-score was 0.77 +1.5 (-2.02-3.08) with females having a higher score (1.09 + 1.49) than males(0.43 + 1.48). A1C was 11.5% + 2.3 (6-17.5%). The T2DM patients (N=3)were older (9-9.3 yrs), obese, female and Black. At follow-up (N=26) BMIdistribution was 31% obese; 15% overweight; 35% normal and 19% un-derweight. The average BMI Z-score increased to 0.99 + 1.2 (-1.94-3.85) andthe gender disparity persisted (female 1.26 + 1.31; male 0.71 + 1.11). A1Cimproved to 7.7% + 0.01 (4.9-11.7%).Conclusions: Young T1DM patients, especially females, can be obese/overweight at diagnosis. BMI worsens with initial treatment. Young obesechildren can develop T2DM. Improved medical nutrition therapy (MNT) atdiagnosis may improve BMI of young diabetes patients.
87
THE EFFECT OF MODIFIED SHAM FEEDING WITHORLISTAT IN OVERWEIGHT AND OBESE SUBJECTS: APILOT STUDY
Dubin RL, Fusiler K, Greenway F. Louisiana State University HealthSciences Center/ Pennington Biomedical Research Center, Baton Rouge, LA.Purpose of Study: Patients with obesity crave and consume more fatversus their lean counterparts. Emerging evidence suggests that a fat sensingmechanism is present in the oral cavity. The hydrolysis of dietary triglycer-ides into fatty acids via lingual lipase appears to initiate this process. Thelipase inhibitor, orlistat may affect fat perception and thus energy intake. Wepostulate that using orlistat mouthwash (i.e., modified sham feeding), may bebeneficial for manipulating dietary fat intake in humans.Methods Used: Ten overweight/obese subjects were randomized to eitherorlistat mouthwash treatments or placebo and then allowed to eat a high-fat mealad libitum. Fat and total energy intakes were determined, and appetite/satietywas assessed before and after the meal using Visual Analogue Scales (VAS).Summary of Results: The cohort consisted of 90% males and 90% cau-casians; mean age: 26.9 +/- 5.9 years; mean body mass index (BMI) was27.0 +/- 1.8 kg/m2. There was a small numerical decrease in total energy andtotal fat consumption (-20.1 kcal +/- 279.6 total energy and -15.5 +/- 217.9 kcaltotal fat) following the orlistat mouthwash versus placebo. Differences werenot statistically significant (p=0.45 for both comparisons). No correlation wasfound between BMI and total caloric intakes (r2=0.102, p=0.37).Conclusions: No significant differences were found in total energy intakeor fat intake using the orlistat mouthwash versus placebo. Oral lipase manip-ulation using this agent does not appear to be an effective treatment to alterfood intake in humans.
88
STIFF LEGS AND SEVERE MUSCLE CRAMPS IN TWOADOLESCENT BOYS
Hasan R, Kaulfers A, Bhowmick SK. University of south Alabama, Mobile, AL.Case Report: Case 1:A 14 year old AAM was brought to the emergencyroom after falling at school when his legs became very stiff. He reported severe
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 397
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

muscle cramps of both upper extremities. He was having circumoral numbnessand intermittent muscle cramps for about 6 months. Severe carpopedal spasmwas elicited with simple touch. He had a positive chvostek sign and trousseausign. He had a very low ionized calcium of 0.7 mmol/L, and normal thyroid andhepatic function tests. X-ray of the hand did not reveal any shortening ofmetacarpal bones. EKG showed prolonged QT interval.He was admitted tothe PICU for intravenous calcium infusion. He became asymptomatic within12 hours of IV calcium infusion. Case 2: A 14.5 year old AAMcame to ERwiththe complaint of severe generalized muscle cramps, tightness of legs, difficultyin walking, and carpopedal spasms. He was having circumoral tingling andnumbness for 4-6 months. Light touching of his hand elicited carpopedalspam and tetany. He had both positive chvostek and trousseau signs. Deeptendon reflexes were brisk. Ionized calcium was also low. He had normalthyroid and hepatic function tests. X-ray did not reveal any lytic lesions orshortening of metacarpal bones. Head Ct was negative for brain calcifica-tions. EKG showed prolonged QT interval. He was admitted to PICU forintravenous 10% calcium gluconate. Discussion: Diagnosis: Pseudohypo-parathyrodisim Type 1b. Pseudohypoparathyroidism is more common thanprimary hypoparathyroidism in pediatrics. The laboratory values are exactlythe same as hypoparathyroidism except for an inappropriately high or veryhigh PTH level. PHP is a heterogeneous group of disorders namely PHPType 1a, PHP Type 1b, PHP Type 1c and PHP Type 2. The most commonforms are PHP Type 1a and Type 1b.PHP 1b is a genetic defect. Hormoneproblems are usually limited to an inability of the kidney to respond fully toPTH. These conditions may not manifest until the later part of childhoodand during pubertal growth and development. Since PTH responsivenessis usually preserved in the bones, affected individuals are therefore func-tionally hypoparathyroidism but show normal skeletal architecture anddevelopment.
89
HYPERCALCEMIA AFTER SUBCUTANEOUS FAT NECROSISIN A NEWBORN
Hasan R, Kaulfers A. University of south Alabama, Mobile, AL.Case Report: A male 37+6 EGA infant was born after an emergency C/S.The infant was found to be in fetal distress. The infant needed continuousventilatory support due to poor respiratory effort. Cord blood gases reflectedsevere combined respiratory and metabolic acidosis. Whole-body coolingwas initiated to minimize the morbidity associated with hypoxic-ischemicencephalopathy in NICU. On day 4 of life, the infant developed an ery-thematous rash over the back and the forehead. Then progressed to a scler-ematous appearance by day 6. The lesions became more nodular and involvedthe back of the neck and part of the forehead. The patient was dischargedon day 42 of life. 5 days later, he was presented with poor oral intake. Bloodwork revealed hypercalcaemia, serum calcium 15.7mg/dL and ionized Cawas 1.99 mmol/L. PTH level was G1 pg/mL, vitamin D was 12 ng/mL, and1,25 hydroxy vitamin D was 75 ng/ml. The patient was treated with IVfurosemide, prednisolone and hyperhydration for 4 days. On the 47th dayof life, the calcium level was 9.7 mg/dl. The patient was discharged homeon oral steroids to follow up in the endocrinology clinic. Discussion: Sub-cutaneous fat necrosis (SCFN) of the newborn is an uncommon condition,occurring to term or post-term infants within the first few weeks afterbirth. We report a term infant developing extensive subcutaneous fat ne-crosis within the first five weeks of life after significant perinatal hypoxicinjury which was managed by a hypothermia protocol. After discharge, theinfant developed hypercalcemia and required re-admission with a pro-longed medical treatment. Although hypercalcemia is a rare complicationof subcutaneous fat necrosis, it can be life-threatening. Pediatricians shouldbe aware of this phenomenon and schedule frequent calcium monitoringafter discharge.
90
REAL-TIME TELE-MONITORING OF GLUCOSE ASADJUNCT TO THE MANAGEMENT OF TYPE 2 DIABETESIN PRIMARY CARE
Heudebert A3, Eichold B1,3, Arrieta MI2,3, Roach D4,3, Brown S1,Hansberry S2, Brye W2, Steigler S1, Mitchell F1, Oliver B4, Foreman R2,Moody K2, Crook E2,3. 1Mobile County Health Department, Mobile, AL;2University of South Alabama, Mobile, AL; 3University of South Alabama,Mobile, AL and 4University of South Alabama, Mobile, AL.Purpose of Study: Type 2 diabetes mellitus (T2DM) is a chronic conditionthat disproportionally affects ethnic minorities. Long term glycemic controlprevents complications of T2DM but is often difficult to achieve, particu-larly in patients with poor access to care. In this study we evaluate the roleof telemedicine in management of T2DM in a predominantly poor AfricanAmerican cohort.Methods Used: This randomized, controlled study measured the potentialimpact of tele-monitoring on glycemic control in T2DM patients. We hy-pothesized that our intervention arm would achieve better long-term glycemiccontrol than our control arm or those analyzed in our internal retrospectivecomparison group (IRC).Participants were recruited from the Mobile CountyHealth Department clinics, randomized, and followed for 9 months. The IRCgroup was derived from the medical records using patients outside of theenrollment period. T-test analysis of both primary endpoint Hemoglobin A1C(HgbA1C) as well as compliance of self monitored blood glucose (SMBG)data was conducted.Summary of Results: There was no difference (p=.8191) in mean changeof HgbA1C between intervention (N=69, $=-1.95%) and comparator group(N=65, $=-2.06%) at study end. Both control and intervention arms achievedsignificant reduction in HgbA1C from baseline to study end (p=G.0001).Both intervention and control group showed statistically significant differ-ence (p=.0380 and .0255 respectively) in mean change of HgbA1C levelscompared to the IRC group ($=-0.95%). Participants in the interventiongroup were more compliant with SMBG regimen (p=.0093).Conclusions: Use of a tele-monitoring system to monitor glucose levels inT2DM patients had no discernible effect on glycemic control between con-trols and intervention in our study. However, patients in both study armsachieved statistically significant improved glycemic control both within groupand relative to patients subject to usual care. Further analysis is warranted toexplain these findings.
91
METABOLIC SYNDROME AFTER HEART TRANSPLANT:THE POSSIBLE ROLE OF STEROIDS
Iravedra D1, Gonzalez W1, Altieri PI1,2, Sotolongo A1, Banchs HL1,2,Calderon R1, Gonzalez-Cancel IF2, Escobales N1, Crespo M1. 1University ofPuerto Rico, San Juan, Puerto Rico and 2Cardiovascular Center of PuertoRico and the Caribbean, San Juan, Puerto Rico.Purpose of Study: Study the metabolic syndrome changes in patients (P)after heart transplant.Methods Used: Review the records of 101 P. who had heart transplants.Summary of Results: 101 (P) had heart transplants due to multiple causes,including idiopathic, ischemic cardiomyopathy or other causes. There were
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
398 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

36 females and 65 males with a mean age of 51 years old. The metabolicchanges pre and post transplant respectively were:
1. BMI: (25 T 4 - 28 T 5 kg/m2) P G 0.052. Systolic BP: (107 T 17 - 131 T 20 mmHg) P G0.053. Diastolic BP: (70 T 13 - 81 T 10 mmHg) P G0.054. FBS: (107 T 37 - 117 T 55 mg%) N.S.5. Cholesterol: (170 T 55 - 189 T 32 mg/dl) P G0.056. HDL: (38 T 16 - 52 T 17 mg/dl) P G0.057. LDL: (99 T 20 - 83 T 15 mg/dl) N.S.8. Triglycerides: (163 T 10 - 188 T 12 mg/dl) N.S.All P. were in the anti-rejection protocol which included prednisone per-
manently. 16 P. died with rejection, mostly they were females.Conclusions: In conclusion, P. after heart transplant develops Mets. Wethink an important factor inducing this abnormality is the use of steroids. Achange in the rejection protocol is under discussion, because this complica-tion will reduce the survival of these P.
92
EFFECT OF DIET COMPOSITION ON HDL AND URINARYMICROALBUMIN IN OBESE NON-METABOLIC SYNDROMEFEMALES
Jacovino CA1, Stentz FB1, Kitabchi AE1, McDaniels K1, Tylavskym F2,Nyenwe E1, Wan J2, Sands C.1 1University of Tennessee Health ScienceCenter, Memphis, TN and 2University of Tennessee, Memphis, TN.Purpose of Study: While some studies have reported reduction in trigly-cerides in subjects eating low-carb diets, trials evaluating HDL and urinarymicroalbumin in subjects eating moderately high-protein diets are still pre-liminary. This study compares HDL and microalbumin outcomes after a 24-weekintensive intervention consisting of different weight loss diets; the traditionaldiet (HC) (55% carbs, 15% protein and 30% fat), and a high-protein diet (HP)(40% carbs, 30% protein and 30% fat).Methods Used: Using a randomized parallel-group trial, 24 pre-menopausal obese, non-diabetic women with a mean age of 36 yrs andmean BMI of 39 kg/m2 were placed on calorie restricted HP (12) or HC (12)diets over a 24 week period as calculated by their Resting Energy Expendi-ture. Participants on both diets received all of the food they were required toeat in weekly pickups and adherence to the diet and weight was measured.HDL at 4, 8, 12, and 24 weeks was the primary outcome. Secondary measuresincluded 24-hour urine microalbumin.Summary of Results: Over 24 weeks, the HP group was found to have a3.33 mg/dL increase in HDL as compared with a 4.9 mg/dL decrease in HDLin the HC group (pG.001). The HP group had a reduction in 24-hour urinarymicroalbumin of 8.3 mg/24hr and the HC group had an increase of 1.6 mg/24hr from baseline, however, that was not statistically different (p=.316).Conclusions: While both HC and HP diets caused weight loss, the HP groupcaused a statistically significant increase in HDL-C and a non-significantdecrease in urinary microalbumin, while the HC diet actually showed a furtherreduction of HDL-C despite similar weight loss to the HP group. In a previousstudy of patients with metabolic syndrome, reduction in HDL has been foundto precede micrcroalbuminuria, elevation in plasma glucose, and increase inblood pressure. Therefore, this study showing reductions in HDL in obese, non-metabolic syndrome females that improves significantly with low-carbohydrateis novel. While others studies have previously shown small increases in HDLwith low-carb diets, no studies have been comprehensive in providing daily food.
93
RECURRENT METASTATIC PHEOCHROMOCYTOMA NINEYEARS FOLLOWING BILATERAL ADRENALECTOMY
Jacovino CA, Rehman RA, Gosmonov AR. University of Tennessee HealthScience Center, Memphis, TN.Case Report: Pheochromocytoma is a catecholamine-secreting tumor thatrarely recurs after adrenalectomy. We report a case of recurrent pheochromo-cytomawith liver metastasis diagnosed nine years after bilateral adrenalectomy.
A 46-year-old African American female with past medical history ofbilateral pheochromocytoma followed by bilateral near-complete adrenalec-tomy in 2003 and primary hyperparathyroidism presented with headache,chest pain, and altered mental status. The patient’s B/P on admission was 193/127 and pulse of 127. Her medications included Amlodipine 10 mg. On
examination, she was well-developed and had no tongue or skin lesions. CTof the chest revealed incidental left adrenal mass. Further imaging studiesrevealed a 4.6x3.3 cm hypervascular left adrenal mass suspicious for pheo-chromocytoma and multiple hypervascular lesions in the liver. Recurrenceof pheochromocytoma seemed very likely. Serum free metanephrines were88 (G57 pg/mL) and normetanephrines were markedly elevated at 3942(G148 pg/mL). Urine total metanephrines were 486 (58-203 mcg/24hr) andnormetaneprhines were 9695 (88-649 mcg/24hr). Serum and urine dopaminelevels and serum aldosterone, DHEA-S, cortisol, and androstenedione levelswere normal. Chromogranin A was at 346.0 (1.9-15 ng/mL). Meta-Iodo-Benzyl-Guanidine scan showed increased activity in the left adrenal mass,liver, and retroperitoneal lymph nodes consistent with metastatic neuroen-docrine disease. Further work up revealed calcitonin of G2 (G5), PTH 78.2(14-72) and calcium 10.5 (8.5-10.1 mg/dL). Patient was started on phenoxy-benzamine followed by metoprolol before surgical resection.
Surgical resection is the definitive treatment for patients with pheochro-mocytoma. Organ preserving surgery avoids steroid supplementation in a ma-jority of cases, however in familial diseases there is a relevant risk of recurrentdisease. The rate of ipsilateral recurrence in familial pheochromocytoma isapproximately 20% during a follow-up of 20 years. In one meta-analysis, themedian time to recurrence was 4.6 years from the time of surgery in thosewith familial pheochromocytoma syndromes. Our patient did not have ge-netic testing done at the time of the initial diagnosis to assess whether she hadfamilial or sporadic pheochromocytoma.
94
COGNITIVE FEATURES OF HYPOTHYROIDISM WITHSYMPTOMS
Mabry C, Engel LS. LSU Health Sciences Center, New Orleans, LA.Case Report:Introduction: The thyroid gland produces many hormones including tri-iodothyronine (T3) and thyroxine (T4) which are regulated by thyroid-stim-ulating-hormone (TSH). With decreased function or serum concentration ofT3 and T4, the regulation of energy is affected and clinical manifestationssuch as fatigue, slowed speech and movements, cool skin, bradycardia, andneurologic changes develop.Case: A 43-year-old woman with a past medical history of thyroid cancer(unknown type), status post complete thyroidectomy and a history of myo-cardial infarction with stent placement presented to the emergency depart-ment because of 1 week of sinus pressure and generalized fatigue. Becauseof her thyroidectomy, the patient had been prescribed Levothyroxine in thepast, which she had not taken in 6 months. The patient had visited an urgentcare center 1 week before for the sinus pressure and was prescribed a corti-costeroid. She only took this for one day. Throughout the interval week, shedeveloped intermittent double and blurry vision. The most alarming changeoccurred when she suddenly awoke from sleep and had a strong urge to runout in the middle of traffic. She had never had any thoughts of suicide before.When she presented to our hospital, a TSH was ordered and found to be153KIU/mL. Her Free T4 was G0.15ng/dL at that same time. High-doses ofLevothyroxine were immediately given. She clinically improved after 3 dayswith no more thoughts of suicide or visual changes. She was sent home withthyroid replacement therapy and close endocrinology follow-up.Discussion: The exact pathophysiology causing the cognitive changes is notcompletely understood. Poor cerebral blood flow and thus poor glucose de-livery to the brain have been hypothesized; however no studies have been ableto confirm this. When delirium due to hypothyroidism is recognized, the stan-dard therapy is immediate hormone replacement to a euthyroid state. Althoughthe laboratory values might lag behind, there is generally quick clinical res-olution of the symptoms once the replacement therapy gets to therapeuticlevels. Some patients present with severe symptoms despite mild hormonedisturbances while others have mild symptoms in the face of high TSH levels.
95
UNEXPLAINED TACHYCARDIA
Musa F, Engel LS, De Silva T. LSU Health Sciences Center, New Orleans, LA.Case Report:Case: A 32 year old otherwise healthy man was admitted with multi-ple fractures following a car accident. On admission vital signs were blood
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 399
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

pressure 110/65 mmHg, heart rate 130 beats/minute, temperature 99 oF, andrespiratory rate 20 breaths/minute. He was alert and oriented to name andplace but not to time and event, heart rate was rapid but regular. Initiallaboratory work was remarkable for low hemoglobin of 10.6 gm/dL, elevatedbilirubin, AST, ALT and Alkaline phosphatase levels of 1.6 mg/dL, 47 u/L,54 u/L, 470 u/L respectively, and a normal TSH of 0.54 uIU/mL. As partof initial evaluation he underwent a CT of the abdomen with contrast. Onhospital day 27, TSH was repeated and found to be low at 0.13 uIU/ML, andfree T4 elevated at 5.59 of ng/dL. The Endocrinology service felt he metclinical criteria for thyroid storm possibly due to multifactorial precipitantsincluding trauma, stress, and the recent iodine load from CT scan. He wasstarted on propylthiouracil (PTU), propranolol and hydrocortisone. Potassiumiodine was subsequently added. A thyroid ultrasound revealed a prominentechogenic thyroid with increased vascularity without discrete nodules.Thyroid peroxidase antibody levels of greater than 500 IU/ML and thyroidstimulating immunoglobulin level of 280% were consistent with Graves’disease. Due to the worsening transaminitis, PTU was discontinued and cho-lestyramine was added. Too unstable for emergent thyroidectomy, the patientunderwent 5 cycles of plasmapheresis. Tachycardia, mental status, and trans-aminits improved, free T4 normalized.Discussion: Thyroid storm is a rare disorder with high mortality rate. It maybe precipitated by infection, trauma, surgery, acute iodine load, or physicalstress. Therapeutic plasma exchange may be considered in cases with severesymptoms, rapid clinical decline, poor response to treatment or contraindi-cation (agranulocytosis, renal insufficiency, asthma, heart failure) to conven-tional therapies. Plasmapheresis can result in an improvement through a directremoval of free thyroid hormones, replacement of bound carrier proteins withunsaturated carrier proteins, and reduction of T4 to T3 conversion. Plasmaexchange is a viable and valuable option to bridge patients to definitivetherapy, but it has never been studied in a randomized clinical trial.
96
FOLLICULAR THYROID CARCINOMA PRESENTING WITHENDOBRONCHIAL METASTASES
Onyeaso NC, Gosmanov A. University of Tennessee Health Science Center,Memphis, TN.Purpose of Study: Endobronchial metastases from follicular thyroid car-cinoma are rare. We report a patient with distant metastases to endobronchialtissue of lungs from follicular thyroid carcinoma.Methods Used: A 79-year old male presented with dyspnea, chest painand weight loss. Physical examination revealed an emaciated patient with aBMI of 16.7 kg/m2. Vital signs were within normal limits. CT chest revealedmultiple lung nodules. Subsequently, bronchoscopy demonstrated an endo-bronchial nodule in the right upper lobe. Pathological evaluation of thenodule revealed neoplastic cells that stained positive for thyroglobulin (TG),thyroid transcription factor-1 (TTF-1) and cytokeratin-7, consistent with met-astatic follicular thyroid carcinoma. Endocrine consultation was requestedand further evaluation revealed a firm fixed right thyroid nodule with ir-regular borders. His thyroid function tests were normal. Thyroid ultrasoundrevealed a 2.3x2.2x1.8 cm right thyroid solid nodule. Fine needle aspira-tion of the nodule revealed follicular cells. The patient subsequently had totalthyroidectomy and neck exploration. Thyroid gland pathology revealed anodule with features of high-grade follicular thyroid carcinoma. Nuclearimaging scans 5 days after the radioactive iodine therapy demonstratedmultiple foci of activity in lungs and neck consistent with metastatic thyroidcancer.Summary of Results: We report a rare case of follicular thyroid carcinomathat presented with endobronchial metastases. Follicular thyroid carcinoma(FTC) metastasizes primarily by hematogenous route. Distant metastasesoccur in 15% of FTCs, typically to bones, brain and lungs (usually as nodularlesions in lung parenchyma). Endobronchial metastases as in our patientare extremely rare and usually imply a poor prognosis. Pathogenesis ofendobronchial lesions formation may involve direct invasion from pa-renchymal lesion, direct extension of mediastinal lesions, transbronchialaspiration, direct lymphatic spread and/or direct metastasis via the bron-chial artery.Conclusions: We suggest that patients with signs and symptoms of malig-nancy and diagnosis of pulmonary nodules of unknown etiology shouldundergo examination of the thyroid gland to identify those subjects who maybe at risk for metastatic thyroid cancer.
97
A NOVEL CASE OF ENDOGEOUSHYPERTESTOSTERONEMIA
Panchal GB, Amin P, Peiris A. East Tennessee State University,Jonesborough, TN.Case Report: A 64 year hypertensive male, former heavy weightlifter wasevaluated for sexual dysfunction. Patient was asymptomatic apart from de-creased sexual satisfaction. He denied loss of libido or erectile dysfunction,recent use of anabolic steroids or any drugs to boost muscle mass. He wasa cooperative muscular male, with normal secondary sexual characteristicsand without acne or gynecomastia. He had no evidence of testicular atro-phy. His rest of the physical examination was normal. Serum testosteronewas 1320 ng/dl (193-740). His LH was 7.1 mU/ml (1.7-8.6), FSH 6.8mU/ml(1.5-12.4). Serum estrone, estradiol and urine cortisol were normal. Repeattestosterone panel showed total testosterone 1745 ng/dl (250-1100), free tes-tosterone 108.2 pg/ml (35-155), sex hormone binding globulin(SHBG) wasmarkedly elevated at 173.7 nmol/L (14.5-48.4). Urine drug screen includ-ing testing for anabolic steroids was negative. His liver enzymes showed ALT86 U/L (7-56) and AST 90 U/L (15-46). Bilirubin, complete blood count,renal and thyroid function tests were normal. Ultrasound of liver was con-sistent with fatty infiltration. Workup for acute hepatitis was negative and adiagnosis of nonalcoholic steatohepatitis was made.
***DISCUSSION***Elevated testosterone levels are encountered veryrarely in the absence of exogenous administration. Circulating testosteroneis bound to SHBG, with the unbound testosterone acting as the bioactivecomponent. Given the normal free testosterone and elevated total testoster-one, it is likely that the marked elevation of SHBG was responsible for histestosterone elevation. While we considered exogenous testosterone admin-istration given his prior history, one would expect a decrease of SHBG in thissetting. SHBG concentration is decreased by androgens, insulin, nephroticsyndrome and obesity; it is increased by estrogen administration, hyper-thyroidism. We believe that the acute liver damage from nonalcoholic stea-tohepatitis resulted in an increase in SHBG and thereby elevated totaltestosterone levels. We believe this is the first reported case of elevated SHBGassociated with steatohepatitis. Given the increase in obesity and steatohe-patitis along with enhanced testing for testosterone, clinicians should be awareof this potential cause for increase in testosterone values.
98
HOT FLASHES AS INITIAL PRESENTATION OF PITUITARYMASS IN A YOUNG MAN
Rehman R, Dagogo-Jack S. UTHSC, Memphis, TN.Case Report:Introduction: Hot flashes in males are not only rare but an unusual clinicalpresentation of an underlying sellar mass. We here in report the case of amale patient with a pituitary mass and hypogonadism who presented withhot flashes.History: A 41-year-old African American male presented with complaintsof recent onset of frequent hot flashes accompanied by profuse perspiration.Few months later, he experienced decreased libido and erectile dysfunction.He did not report any previous major health problems except chronic si-nusitis. He did report progressively worsening headaches, which he attributedto the long-standing chronic sinusitis.Examination: The patient looked healthy and well-androgenized; the bloodpressure was 102/66 mmHg, heart rate was 66 beats/min, and weight was192.2 kg. There were no Cushingoid or acromegalic features, and the patientwas clinically euthyroid. The extraocular movements were intact, and visualfields were full to confrontation. The remainder of the examination, includinggenitalia, was unremarkable.Labs: The total testosterone was 24ng/dl (241-827), repeated value was51ng/dl; 8 AM cortisol 8.2 ug/dl (4.3-22.4), FT4 0.46 ng/dl (.58-1.64), TSH0.439 uIU/ml (0.34-5.6), LH 0.9 mIU/ml (1.3-10.5), FSH 1.6 mIU/ml (1.6-9.7). The prolactin was 14ng/ml (2.1-17.7), IGF-1 141ng/ml (101-267),ACTH 37 pg/ml (6-50) and alpha-subunit was 0.24 ng/ml (0.05-0.53). HeadMRI showed a cystic sellar mass (1.7�1.7cm) with suprasellar extension.Diagnosis and Management: A diagnosis of non-functioning cystic sellarmass with secondary hypogonadism and hypothyroidism was made. Tes-tosterone and thyroid hormone replacement was started, resulting abatement
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
400 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of hot flashes and erectile dysfunction, but the headaches persisted. Thepatient was referred to Neurosurgery for excision of cystic sellar mass.Conclusion: Hot flashes are a common menopausal symptom in females,but rare in men. In males, hot flashes may accompany androgen deprivationtherapy for prostate cancer. In addition to the classic presentations of pituitarymasses (endocrine, neurological and visual perturbations), endocrinologistsshould be alert to atypical presentations such as hot flashes, as occurred in ourpatient.
Joint Plenary Poster SessionGastroenterology
5:00 PMThursday, February 21, 201399
UNUSUAL PRESENTATION OF HEPATOCELLULARCARCINOMA
Fenire M, Nusrat M, Ghaleb M, Nugent K. TTUHSC. Lubbock, Lubbock, TX.Case Report:Background: Hepatocellular Carcinoma (HCC) is one of the most com-mon tumors in the world. HCC usually metastasize to the lung, lymph nodeand bone. Metastasis to the spinal cord is uncommon. Spinal cord com-pression (SCC) signs in a patient with risk factors for HCC should promptHCC in the differential diagnosis.Observation: A 66 year-old man with no significant past medical historypresented with 6 week history of back pain. It started first at lumbar spine.The pain was described by the patient as a sharp, persistent unrelated tomovement. Aweek later, the patient started to have left leg weakness. On thesubsequent weeks, he developed right leg weakness. He visited medical fa-cility where he lives and was prescribed analgesic medication which did nothelp his symptoms. Patient denied any associated sphincter incontinence, head-ache or similar illness in the past. He had no previous history of trauma. MRIof the spine revealed destructive soft tissue metastasis involving T1 vertebralbody, protruding into the spinal canal and compressing the upper thoraciccord. CT scan of the chest showed large osteolytic lesions involving the T1and T12 vertebral bodies consistent with metastatic disease. CT abdomenreported 10 cm mass in the inferior right lobe of the liver suspicious for HCC,liver cirrhosis with portal hypertension, 2 cm right adrenal mass suspiciousfor metastatic lesion, and T12 osteolytic bone lesion. The patient testedpositive for HCVAb IgG and alpha feto protein was 33,203 IU/ml. Patientis scheduled to receive radiotherapy. The poor prognosis for the patient wasdiscussed with family and decided to discontinue the radiotherapy and takehim home with hospice care.Discussion: The presentation of the HCC includes spinal cord compression.The fact that the clinicians in the USA do not recognize SCC as result ofmetastatic HCC is not uncommon because few cases have been reported. Thepresent case may raise the suspicion for this presentation. SCC caused byHCC metastasis tends to have short time from the onset of bone pain to thedevelopment of neurological signs. In this patient it was only 6 weeks. Thiswindow of time is of critical importance when it comes to improving patient’squality of life. It is the opportunity that we can start early treatment andprevent severe neurological deficit.
100
ANATYPICAL CASE OF INTUSSUSCEPTION INA 4-YEAROLD
Stephenson LR, Thomas W, Herbst J, Sicard C, Bocchini J. LSU HealthShreveport, Shreveport, LA.Case Report: A 4 year old girl with no significant past medical historypresents to an outside ED complaining of diffuse crampy abdominal painof one day’s duration. While in the ED, she had four loose bowel movementsthat reportedly were bloody per mom and the doctor in the ED. These weretested, and found to be hemoccult negative. The patient had an abdominalultrasound that was reported to be negative. The other hospital attempted toobtain a CT, but the patient would not drink oral contrast. On initial exam atour facility, the patient had constant, writhing abdominal pain with voluntaryguarding. Exam was hemoccult negative, with a small external hemorrhoidnoted. An abdominal x-ray at our facility showed a paucity of bowel gas in theleft upper quadrant, concerning for a mass. A repeat ultrasound at our facility
showed a prominent colo-colic intussusception. The patient was immediatelytaken for gastrograffin reduction under fluoroscopy. The intussusception wasreduced successfully, but a filling defect was noted in the splenic flexure,suspicious for a polyp. Subsequently, the patient underwent a colonoscopy,where a small pedunculated polyp was found and removed. The pathologywas significant for a benign juvenile polyp.
This typical presentation for intussusception is occuring at an atypicalage. Patients greater than two years old with intussusception are more likelyto have pathologic lead points. Classically, these lead points are not detectedon primary radiographic studies.
Joint Plenary Poster SessionGeriatrics and Gerontology
5:00 PMThursday, February 21, 2013101
AN ATYPICAL CLINICAL PRESENTATION OF AN ELDERLYPATIENT
Cleinman A, Windham B, Meeks W. University of Mississippi MedicalCenter, Jackson, MS.Case Report:Introduction: While peptic ulcer disease (PUD) and its associated com-plications are on the decline in the general population, they are increasing inthe elderly, particularly among older women. Patients with perforated pepticulcers typically present with sudden, acute, sharp pain in the epigastrium. Thepresentation of PUD in the geriatric patient may be atypical, delaying itsidentification. While overall mortality associated with perforations is esti-mated at 23.5 to 30%, there is an increased mortality (30 to 41%) in thoseover 70 years old.Case Description: A 79 year-old white female presented to the emergencyroom complaining of abdominal, back, and chest pain. One week prior, shehad developed exertional shortness of breath, anorexia, and weight loss. Shedescribed her chest pain as retrosternal, dull, and radiating to her right armwith associated diaphoresis and nausea. Her abdominal pain was diffuse withno alleviating or aggravating factors. Her back pain was similar to her chronicarthritic pain, but of greater intensity. Home medications included 1 to 2 BCpowders daily for her arthritis; she denied tobacco or alcohol use. Abdominalexamination revealed a soft abdomen with mild tenderness to deep palpa-tion diffusely, but no guarding or rebound tenderness. Initial studies includeda white blood cell count 3.3, hematocrit 32.2, troponin G0.012; and chestx-ray with no acute findings. A CT Abdomen/Pelvis was performed, re-vealing pneumoperitoneum. The patient was volume resuscitated, antibioticswere given, and an exploratory laporatomy was performed. Intraoperativefindings included a 3cm perforation of the lesser gastric curvature; the gastric
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 401
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

ulcer was resected, and pyloroplasty was performed. Pathology of the gas-tric ulcer specimen showed ‘‘benign chronic gastric ulcer’’ and Helicobacterpylori was negative.Discussion: We present here a case of a peptic ulcer perforation in an elderlypatient, with a misleading history and atypical abdominal exam. This casehighlights the notion that geriatric patients frequently present in an atypicalfashion; leading to delay in diagnosis, which along with advanced age,greatly increases mortality in this patient population. This patient was diag-nosed and treated in a timely manner with a positive outcome.
Joint Plenary Poster SessionHealth Services Research
5:00 PMThursday, February 21, 2013102
BARRIERS TO ESTABLISHING SUSTAINABLEHEALTHCARE INITIATIVES IDENTIFIED FROMCOMPARISON OF THREE AFRICAN HEALTHCARESYSTEMS
San Miguel KB, Ruth N, Kamen DL. Medical University of SC, Charleston, SC.Purpose of Study: There is enormous disease burden and lack of publichealth initiatives in poor and remote African communities. Despite culturaldifferences, the underlying health problems are the same; such as high infantand maternal mortality, poor access to care, and tropical diseases. The purposeof this study was to compare healthcare systems between Eastern, Westernand Southern Africa to identify common barriers to public health initiatives.Methods Used: Regions of Africa included in the study were Nairobi,Kenya; Embangweni, Malawi; and Bo, Sierra Leone. Identification of health-care characteristics and barriers were measured by a student volunteer (KBSM)between 2006-12. Observations were based on: poverty, access to healthcarefacilities, government limitations, and availability of resources.Summary of Results: Two hospitals were urban, one of which was privately-funded (Nairobi) and the other was government-funded with some privatedonations (Bo). The 3rd was rural and government-funded (Embangweni).
Differences between the 3 regions included local tourism which impactedeconomic inequality and resource accessibility and utilization. Additionally,slow recovery from war resulted in varying government support of health-care. Scarce resource accessibility contributed to poor basic infrastructure,such as clean water, food, sanitation, and transportation.
Common threads to successful public health initiatives included sensi-tivity to local cultural norms and language, involvement of local people tosustain programs, and provide ongoing support.
Based on these observations, recommendations are: 1-Increase outreachto rural villages for checkups, vaccinations and education in their own lan-guage, 2-Encourage women with high risk deliveries to seek prenatal care,3-Educate women who received treatment to go back to their communitiesand teach others, 4-Offer leadership seminars for medical staff, 5-Furtheraddress poverty and its impact on healthcare and 6-Provide reliable consistenthealthcare data collection.Conclusions: Despite pervasive poverty and poor healthcare access, therewere lessons learned from comparing 3 regions of Africa. In conclusion, themost productive and sustainable efforts were those that incorporated the localculture and focused on the needs and priorities of each unique community.
Joint Plenary Poster SessionHematology and Oncology
5:00 PMThursday, February 21, 2013103
LEYDIG CELL TUMOR: A CASE OF MISTAKEN IDENTITY
Allee L, Cassell M. UMC, Jackson, MS.Case Report: Testicular cancer, although rare, is the most common solidmalignancy in young men. The American Cancer Society’s estimates 8,590new cases and 360 deaths from testicular cancer for 2012. Testicular cancer isone of the most curable forms of cancer with a 95% 5 year survival withproper management. Each different testicular tumor type is unique with re-
spect to biology and treatment options. Germ cell tumors account for morethan 95% of all testicular malignancies and respond to chemotherapy +/-radiation depending on type. In contrast, malignant sex cord-stromal tumors(SCST) are resistant to both chemotherapy and radiation and are generallytreated with orchiectomy and retroperitoneal lymphadenectomy. A significantchallenge in testicular pathology is the differential diagnosis. Many pathol-ogists have limited experience with testicular cancer as it accounts for only1% of malignancies. Most SCSTs are benign but 10-20% of these tumors inadults can metastasize and result in death. Staging of these tumors includespathologic diagnosis of surgical specimen after orchiectomy, CT of the chest,abdomen and pelvis, and often retroperitoneal lymph node dissection. Factorsindicating a SCST is more likely to be malignant include local or vascularinvasion, large size (95cm), increased mitotic activity, cytologic atypia andnecrosis. Stage I disease is usually successfully managed with excision ofthe primary tumor alone. Prognosis for patients with metastatic SCSTs ispoor and in patients with limited stage metastatic disease, metastectomy shouldbe considered when possible. We describe a 48 year old man with a historyof diagnosed Sertoli cell tumor status post orchiectomy who presented 8 yearslater with massive hemoptysis requiring intubation. He was discovered tohave lung and liver lesions. Pathology of bronchus mass and liver biopsy di-agnosed metastatic malignant leydig cell tumor. Laboratory studies revealeda hematocrit of 58% and testosterone level of 1500ng/dL. Further pathologicreview of initial orchiectomy diagnosed pT2NxMx malignant leydig cell stro-mal tumor with necrosis and lymphovascular invasion. This case emphasizesthe importance of accurate pathologic diagnosis, complete staging, associ-ated treatment in early stage, and good follow up in testicular cancer.
104
NOT SO CLEAR: A RARE CASE OF CLEAR CELL CARCINOMA
Anderson SD, Chowdhury N, Anderson R, Smalligan RD. Texas Tech UnivHealth Sciences Center, Amarillo, TX.Case Report: A 33yo man presented with a left neck mass that was firstnoted as he was shaving. He denied voice changes or dysphagia but did notesome orthopnea. The mass increased in size over the next month before a fineneedle aspirate was performed which was inconclusive. An incisional biopsythen showed spindle cells with malignant potential. Two months later, he wasevaluated at a cancer institute where CT showed a 6 x 4 x 6cm mass in the leftinferior neck extending to the thoracic inlet, along with several enlargedlymph nodes. On follow-up two weeks later, the mass had grown to 8cm indiameter. Given the size and rapid growth of the mass, it was decided re-section was indicated. Pathology showed a 9 x 5 x 7cm mass that had ex-tended from the left thyroid laterally to the esophagus. Pathology was read asclear cell carcinoma with sarcomatoid changes of parathyroid origin.Discussion: In general, clear cell neoplasms of the head and neck are ex-ceedingly rare; however, clear cell changes may be observed in almost anytumor. The differential diagnosis includes parathyroid adenoma, metastaticclear cell carcinoma, and thyroid or thymic carcinomawith clear cell features.Clear cell metastases to the neck may include malignancy from the lung,kidney or female genital tract. Classically, clear cell carcinoma is character-ized by epithelial cells with a well-defined cell membrane and clear cyto-plasm due to glycogens, phospholipids, and cholesterol esters. Pathologyreports in our case state that morphologically, the clear cell areas contain acentrally located small hyperchromatic nucleus and markedly hyperplasticvessels, favoring a parathyroid origin. Similarly, immunostains were per-formed on the sample that returned positive for pan-CK, vimentin and CD56,again consistent with parathyroid origin. Sarcomatoid changes indicate amore aggressive course of a tumor typically. Chemotherapy with temsir-olimus has been studied for renal cell carcinoma with sarcomatoid changesand may be useful in addition to radiation therapy. It is important for theinternist to remember in patients presenting with a neck mass, aggressive andrare tumors should always be considered in the differential and biopsy per-formed promptly if there is any doubt regarding the etiology.
105
SPONTANEOUS RECOVERY OF EPSTEIN-BARR VIRUSASSOCIATED HEMOPHAGOCYTICLYMPHOHISTIOCYTOSIS
Arora A, Imran H, Siddiqui A. University of South Alabama, Mobile, AL.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
402 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Case Report:BACKGROUND: Hemophagocytic Lymphohistiocytosis (HLH) is a rarebut life threatening complication of Epstein-Barr virus (EBV) infection.Immunochemotherapy according to the HLH-94 protocol can be success-ful if initiated within first 4 weeks. The treatment of HLH is associated withhigh morbidity including hypersensitivity reactions, infection relateddeaths and malignancies. We report a case of spontaneous resolution of EBVassociated HLH in a teenager who later was found to have a variant allele forMUNC13-4 gene.CASE REPORT: A 14 year old Caucasian female presented to an emer-gency room with one week history of persistent high grade fevers, diffusemaculopapular rash, jaundice, abdominal distension, hepatosplenomegalyand cervical lymphadenopathy. She was found to have pancytopenia, hypo-fibrinogenemia, hyperferritenemia, transaminitis and an elevated soluble in-terleukin 2 receptor level. Quantitative polymerase chain reaction (PCR) forEpstein Barr virus detected 800,000 genomic copies. The natural killer (NK)cell function was decreased but granzyme-B, perforin and CD107a levelswere normal. Bone marrow examination did not reveal hemophagocytosis.Two weeks into her illness the diagnosis of HLH was established. Beforeinitiating HLH specific therapy, she became afebrile and began recoveringher blood counts. Based on spontaneous improvement it was decided to holdoff HLH specific therapy. Over the next 4 weeks all her symptoms resolvedwith complete normalization of her laboratory data. The genetic testing forfamilial HLH revealed a normal and a variant allele (1772 C9T) for theMUNC13-4 gene. She is now 6 months into remission with undetectable EBVDNA via PCR methodology but her NK cell function remains decreased.DISCUSSION: Spontaneous resolution of EBV associated HLH has onlybeen reported once in the literature by Belyea et al. A potentially harmful andleukemogenic therapy may be avoided in certain patients based on an indi-vidual response. Our patient is also unique in having continued decreased NKcell function, possibly secondary to the abnormal allele for the MUNC13-4gene. This gene has been described to have a role in normal NK cell functionand CD107a activity but clinical significance of this allele remains uncertain.
106
T-CELL ACUTE LYMPHOBLASTIC LEUKEMIACOMPLICATED BY A HEMORRHAGIC STROKE ANDHEMOPHAGOCYTIC LYMPHOHISTIOCYTOSIS
Arora A1, Imran H1, Wilson F1, Polski J2, Siddiqui A1. 1University of SouthAlabama, Mobile, AL and 2University of South Alabama, Mobile, AL.Case Report:Background: T-cell acute lymphoblastic leukemia (ALL)with centralnervous system involvement has a poor outcome and requires aggressivetherapy. Hemophagocytic lymphohistiocytosis (HLH) is a rare but lifethreatening syndrome characterized by fever, rash, cytopenia and hepatosple-nomegaly and specific laboratory findings. It can be familial or secondary toinfections, malignancy or rheumatologic conditions. The current standardtreatment of HLH consists of immunochemotherapy with or without HSCT.We report a teenager with T-ALL who recovered from secondary HLH withimmunochemotherapy alone.Case Report: A 14 year old Caucasian girl presented with a left hemiparesisdue to a large intracerebral hemorrhage requiring emergency drainage in thecontext of hyperleukocytosis (WBC 600,000/cmm). The immunophenotyp-ing upon flowcytometry analysis of peripheral blood confirmed T-cell ALL.At the end of induction therapy, she developed high grade fever, diffuseerythematous macular rash, hepatosplenomegaly and pancytopenia, pleuraleffusion and respiratory failure. Laboratory data showed high ferritin,hypofibrinogenemia and an elevated soluble Interleukin-2 receptor (sIL2) level.Bone marrow examination revealed aplasia and hemophagocytoses. Naturalkiller cell function, perforin and granzyme-B levels were within normal limits.Mutation analyses for familial HLH were negative. Treatment with steroidsand etoposide according to HLH-94 protocol was started. She responded witha downwards trend in sIL2 and ferritin levels and resolution of her organo-megaly and pancytopenia. Therapy for ALL was resumed after 8 weeks ofHLH therapy upon resolution of pancytopenia. After receiving cranial radi-ation, she had a marrow relapse at the beginning of maintenance therapy. Sheis currently receiving re-induction therapy.Consclusion: Secondary HLH can be difficult to control especially in thecontext of a malignancy. There is no published report about the resolutionof HLH without HSCT in T-cell disease. This is likely due to early
diagnosis and initiation of HLH specific therapy. Our patient is now beingconsidered for a matched sibling donor HSCT as a definite treatment for arelapsed T-cell disease.
107
A CASE OF HEMOPHAGOCYTIC LYMPHOHISTIOCYTOSISIN A JEHOVAH’S WITNESS WITH SYSTEMIC LUPUS
Badillo R1,2, Tessema J1, Burton M1,2. 1UT Southwestern Medical Center,Dallas, TX and 2Parkland Health & Hospital System, Dallas, TX.Case Report: Learning Objectives:
1. Recognize clinical features of Hemophagocytic Lymphohistiocytosis(HLH).
2. Discuss barriers to early diagnosis and management of HLH in aJehovah’s Witness.
Case: A 30 year old Hispanic female with systemic lupus erythematosus (SLE)on azathioprine and hydroxychloroquine presented with one week of jaun-dice, nausea, fever and a malar rash. She was tachycardic, febrile and mildlyjaundiced without organomegaly. Aspartate aminotransferase was 311, bili-rubin was 5.2, INR was 915 and she was pancytopenic. Ferritin was 11,111.Cytomegalovirus (CMV) PCR was positive and ganciclovir was started.Secondary HLH was high on the differential; however, because she was aJehovah’sWitness, vitamin K was used to correct her coagulopathy over severaldays prior to biopsy. Eventually, both bone marrow biopsy and liver biopsyconfirmed active hemophagocytosis. She received high dose steroids and in-travenous immunoglobulin. Her clinical course deteriorated and she was ad-mitted to the ICU with confusion, followed by acute necrotizing pancreatitisand disseminated intravascular coagulopathy. On hospital day 14, her familyagreed to administration of blood products. She later developed ischemicbowel requiring subtotal colectomy. Extensive peritoneal hemorrhage wasfound during subsequent ostomy placement and surgeons were unable toachieve hemostasis. The family decided against further blood products andthe patient expired on hospital day 25.Discussion: HLH is an uncommon but often fatal disorder if not detectedand treated in a timely fashion. Patients with fever, cytopenia, coagulopathyand especially marked hyperferritinemia should be suspected to have HLH. Ahigh index of suspicion is required and bone marrow evaluation is confir-matory. In this patient with secondary HLH, both CMV and SLE are twopotential triggers; further research is needed to modify HLH diagnostic cri-teria to improve their sensitivity and specificity in adults with rheumaticconditions. A significant challenge to diagnosis and treatment of HLH andits complications in this case was religious objection to blood products.Clinicians should anticipate complications and know alternatives availableat their hospitals for patients who are Jehovah’s Witnesses.
108
KNOT ON THE HEAD: THE RARE OCCURRENCE OFMETASTATIC COLON CANCER PRESENTING ASTEMPORAL SWELLING AND HEADACHE
Bennett B, Williams JC, Frost J. University of Mississippi, Jackson, MS.Case Report: Brain metastasis occurs in 1.2% of patients with colorectalcancer, and bony destruction as the result of brain metastasis in these patientsis even rarer. This case presents exactly this complication in a patient whopresented to the emergency department (ED) with complaints of a headacheand right temporal swelling.
A 66 year old African-American male presented to the ED with a chiefcomplaint of headache and right temporal swelling. The headache was lo-calized to the right temporal region and described as sharp. It has beenpresent for one month, coinciding with the onset of the right temporalswelling. The patient also reported night sweats and a 20 pound uninten-tional weight loss over the past 8 months. He denied visual changes, hearingchanges, seizures or other neurological deficits. The patient had a history ofwell differentiated invasive adenocarcinoma of the ascending colon (AJCCtumor stage: T2pN0) treated with partial colectomy two years prior to thispresentation. The patient declined adjuvant chemotherapy after the partialcolectomy, and CEA at that time was 2.2.
CT evaluation in the ED revealed multiple masses involving the rightcerebral hemisphere and temporalis muscle, with associated destruction of
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 403
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

the squamous portion of the right temporal bone. Effacement of the rightlateral ventricle with midline shift was also noted, and the patient was startedon dexamethasone. Further contrasted CTevaluation revealed a pleural basedleft upper lobe mass, left infrahilar mass with satellite nodules and hepaticmetastasis. Subsequent biopsy of both the right temporal brain mass and alarge liver mass, and tissue from both biopsies revealed metastatic adenocar-cinoma similar to the previous primary colonic adenocarcinoma which wasremoved two years prior. CEA level at this time was found to be 638.8.Shortly after admission, the patient was initiated with capecitabine and re-ferred for whole brain irradiation.
This patient presents a very rare manifestation of metastatic colon cancerpresenting as brain metastasis with calvarium destruction. This case under-scores the importance of close clinic follow up and continual health careprovider initiated discussions offering adjuvant chemotherapy for potentiallycurable lower staged malignancies.
109
A CASE OF SARCOMATOID MESOTHELIOMA OF THEPLEURAWITH EXTENSIVE METASTATIC LESIONS
Bradley C1,2, Chowdhury N2, Walker WW2. 1Texas Tech University HealthSciences Center School of Medicine, Amarillo, TX and 2Texas Tech HealthSciences Center School of Medicine, Amarillo, TX.Case Report: A 73yo white male patient presented with atypical chest pain.He denied pulmonary symptoms and weight loss. Past medical history -HTN, rectal cancer 10 years prior (treated with surgery, chemotherapy andradiation therapy). Family history negative for cancer. Personal/Social -smokes a pipe daily, no alcohol or drug use. Patient worked on a military shipmany years earlier where he was exposed to asbestos. Physical exam: vitalsigns normal, heart regular, lungs: decreased breath sounds on the right, re-mainder of exam normal. CXR showed a mass in the right side of his chest.CT showed mass attached to the chest wall, 14x12x8 cm in dimension.Hospital course: Patient underwent wide excision of the mass and pathologycame positive for undifferentiated carcinoma consistent with metastatic can-cer of unknown primary. Palliative chemotherapy was begun with early positiveresponse. Eight months later, further testing found the tumor was a sarcoma-toid mesothelioma. Despite new chemotherapy regimen, the patient died fromprogression of the cancer.
General internists see patients with atypical chest pain frequently and inthis case the CXR immediately revealed the cause: an extensive chest wallcancer. Sarcomatoid neoplasms of the pleura are rare tumors that present acomplex differential diagnosis for surgical pathologists. Eighty percent ofpatients with this disease have been exposed to asbestos as had our patientand smoking is known to be a significant additional risk factor. The averageage at presentation is 60 and prognosis is poor with a median survival of 6-18 months. Our patient presented with a right sided mass which occurs in60% of patients with mesothelioma; only 5% present with bilateral disease.Diagnosis of mesothelioma is difficult as it can be difficult to distinguishfrom metastatic disease from such primaries as lung, breast, stomach, kidney,thymus, and prostate neoplasms. Combination chemotherapy with cisplatinand pemetrexed has been shown to improve quality of life and prolong sur-vival marginally.
110
PRIMARY PLASMA CELL LEUKEMIA
Castilllo E, Dhillon N, Puligothrampuligothram S, Ramirez R. LSU HealthSciences Center, New Orleans, LA.Case Report:Case: A 61-year-old woman with history of HTN presented to the emer-gency room with complaints of 35 pounds weight loss over past 3 monthsand progressive weakness over 3-4 months. Her initial physical exam wassignificant for a fixed 3 cm lymphadenopathy in the right axilla. Labsshowed a leucocyte count of 109800, hemoglobin 8.0, hematocrit 24.4% andplatelets 112000. Automated differential identified 91% of leukocytes asneutrophils. Peripheral blood smear reviewed by pathology was read aspossible chronic lymphocytic leukemia. However, a preliminary diagnosisof plasma cell leukemia was made based on flow cytometry on peripheralblood that identified most cells as plasma cells, and not lymphocytes as
thought initially. Bone marrow biopsy showed hypercellularity, with 70%atypical plasma cells, confirming the diagnosis.
Once the diagnosis was established, treatment with Bortezomib, Lenali-domide, and Dexamethasone was initiated. Shortly after receiving the firstdose of Dexamethasone, our patient developed severe hypertension (systolicblood pressure 190). She received intravenous hydralazine with transient im-provement but was later found unresponsive in her room. An emergent headCT showed an acute hemorrhage in the right cerebellar hemisphere. This ra-diological appearance was suggestive of hypertensive hemorrhage or hemor-rhagic metastasis. The patient was transferred to the MICU and Neurosurgerywas consulted. She was deemed a non surgical candidate. Family membersdecided to withdraw care and patient died within few hours.Discussion: Primary plasma cell leukemia is a rare disorder. Clinical pre-sentation is similar to that of multiple myeloma. Prognosis is extremely poor,despite chosen treatment with a median survival of 6-11 months. There are noprospective randomized trials for treatment and most recommendations areextrapolated from multiple myeloma data, thus regimen choice is challeng-ing. Even though, the cause of death in this patient was not clear, we feel theneed to stress the bad prognosis of primary cell leukemia and the need to starttreatment as soon as diagnosis is made.
111
‘‘DOUBLE-HIT’’ LYMPHOMA
Cheema FN1,2, Hildebrandt G1,2. 1Louisiana State University, Shreveport, LAand 2Feist Weiller Cancer Center, Shreveport, LA.Purpose of Study: Diffuse Large Cell Lymphomas (DLBCL) with trans-locations of both MYC and BCL2; ‘‘Double-Hit’’ Lymphomas, are highlyaggressive tumors, with a high treatment failure rate and limited data avail-able to guide therapeutic decisions. Recent literature suggests poor responseto aggressive measures including auto-transplant. We report a patient with anexcellent response to treatment with Rituxan, Ifosphamide, Carboplatin, Eto-poside (RICE) followed by autologous stem cell transplant.Methods Used: 55 year old male with stage IIA, International prognosticindex score 1, DLBCL with t(14,18)(q32,:q21) bcl2 and t(8;22)(q24;q11.2)myc translocations, diagnosed in November 2010. PET/CT revealed rightcervical, supraclavicular and axillary lymphadenopathy.Summary of Results: Hyper-CVAD cycle 1a and 1b administered betweenJuly to August 2011. Therapy switched to RICE after cycle 1b due to renalfailure. RICE administered for one cycle in August 2011 followed by twocycles of Rituxan alone, due to RICE associated prolonged thrombocyto-penia. He continued to receive CNS prophylaxis with intrathecal Metho-trexate and Cytarabine till October 2011. PET/CT prior to auto-transplant inOctober 2011 revealed no evidence of active disease. Auto-transplant with7 Million CD34+/Kg using R-BEAM conditioning was performed in No-vember 2011. He remains in complete remission one year post transplant.Conclusions: Impressive response with RICE followed by auto-transplantin ‘‘Double- Hit’’ lymphoma, underlines the importance of this modality forthis usually treatment resistant malignancy. Further prospective studies areessential.
112
A CASE OF CARDIAC INVOLVEMENT BY DIRECT INVASIONOF NON-SMALL CELL LUNG CANCER
DiSalvo NJ, Caruthers C, Ramirez RA. LSU Health Sciences Center, NewOrleans, LA.Case Report:Introduction: Lung cancer is the most lethal cancer in the world. Non-smallcell lung cancer (NSCLC) accounts for approximately 85% of cases. Meta-static spread of malignancies to the heart may be considered rare; however,autopsy studies demonstrate a 10% incidence. In addition, NSCLC can causecardiac manifestations due to direct extension and invasion. We report on acase of cardiac sequelae in a patient with NSCLC.Case: A 65 year old Lebanese male with a 50 pack year history of smok-ing presented with a two week history of cough and blood tinged sputum.CT scan revealed a heterogeneous 5 x 6.8 x 5.6 cm left lower lobe mass withleft hilar adenopathy. A PET/CT confirmed hypermetabolism in the massand hilum but did not reveal any mediastinal involvement. A bronchoscopyrevealed an endobronchial lesion in the left lower lobe. Histology from this
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
404 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

lesion showed adenocarcinoma. Mediastinal lymph node biopsies were nega-tive. He was staged as T2b, N1, M0. He was evaluated for possible resection.A pre-operative stress echo was done which revealed normal sinus rhythm,good systolic function and no evidence of ischemia. A thoracotomy wasattempted but due to extensive tumor involvement including the diaphragmand posterior chest wall he was deemed unresectable. He was seen by medicaland radiation oncology for concurrent therapy. Prior to initiation of treatmenthe developed worsening shortness of breath and was found to be in atrialfibrillation with rapid ventricular response. CT showed marked extensionof the tumor causing complete occlusion of the left bronchus, extension intothe entire left bronchial tree, invasion of the left pulmonary venous system,and the posterior wall of the left atrium. His heart rate was refractory tomedical therapy. The patient was offered palliative radiation therapy but had acardiac event prior to receiving this and died.Conclusions: Cardiac manifestations of NSCLC are infrequent but shouldbe recognized in patients with suspected or diagnosed NSCLC. Options fortreatment may include surgical resection, radiation, chemotherapy or a com-bination. Overall, most patients are advanced at the time of diagnosis andhave a poor prognosis.
113
YOU GET THE GIST
Englert D, Engel LS, McKay M. LSU Health Sciences Center, New Orleans, LA.Case Report:Introduction: Gastrointestinal Stromal Tumors (GISTs) are the mostcommon type of mesenchymal tumors in the GI tract. We present a case ofmetastatic GIST, a relatively uncommon entity, which can mimic other intra-abdominal malignancies.Case: A 49 year-old woman with iron-deficiency anemia, atrial fibrilla-tion, hypertension, and diabetes presented with complaints of weight loss forsix months, abdominal bloating, distension, and constipation progressingover two weeks, and abdominal pain beginning the morning of presenta-tion. She had been diagnosed with iron-deficiency anemia one year ago, butmissed her appointment for colonoscopy. Pertinent findings on physical examincluded abdominal distension and a large anterior pelvic mass that was pal-pable on both rectal exam and vaginal exam. Therewas no gross or occult bloodon rectal exam, and the vaginal vault was clear. Pertinent labs include a he-moglobin and hematocrit of 10.7 g/L and 35.3%, respectively an MCVof 71,and platelets of 580,000/KL. A CT scan with contrast of her abdomenrevealed numerous enhancing soft tissue nodules and masses of varying sizethroughout the mesentery, and along the course of the omentum in the ab-domen and pelvis, suggestive of metastatic disease. A transvaginal ultrasoundshowed a 12.0 x 16.1 x 21.4 centimeter mass of undetermined origin occu-pying the entire bony pelvis. The pathology specimen obtained by CT-guidedbiopsy showed collagenous tissue heavily infiltrated by spindle cells in astoriform pattern, with a single focus of coagulative necrosis within the le-sion. Immunohistochemical staining was positive for CD117 and vimentin;and negative for ER, PR, desmin, smooth muscle, and S100. These findingswere all consistent with a diagnosis of gastrointestinal stromal tumor. Thepatient was discharged, seen in oncology clinic, and started on treatment withimatinib mesylate.Discussion: The clinical presentation of GIST can vary from an incidenta-loma to widely metastatic disease at first presentation. Metastatic GIST isoften initially misdiagnosed as another intraabdominal malignancy, such ascolon cancer or ovarian cancer. Advancements in the field of immunohis-tochemistry have made the diagnosis of GIST much less complicated. Thiscase highlights the need to consider GIST in the differential diagnosis for anintraabdominal malignancy.
114
CHRONIC NEUTROPHILIC LEUKEMIA: A CASE REPORT
Herrington E, Buck T, and Lam J. University of MS Medical Center,Brandon, MS.Case Report: Chronic neutrophilic leukemia is a rare chronic myelopro-liferative neoplasm and is characterized by mature neutrophilic leukocyto-
sis with few or no circulating immature granulocytes, monocytosis, orbasophilia. We present a case of chronic neutrophilic leukemia.
A 79 year old white man with a history of asthma and liver cirrhosisdue to heavy alcohol use was referred to hematology from his primary carephysician for chronic leukocytosis and anemia. He initially presented withweight loss as well as generalized fatigue. Molecular testing for BCR/ABLand JAK2 V617F were negative. FISH for FIP1L1 and PDGFRA fusion andFISH for PDGFRB/TEL were negative. Bone marrow biopsy showed amarkedly hypercellular with marked granulocytic hyperplasia, likely repre-senting chronic neutrophilic leukemia. CT showed liver cirrhosis and evidenceof esophageal varices as well as splenomegaly. EGD showed esophagealvarices and a hiatus hernia in the esophagus. Colonoscopy showed internalgrade I hemorrhoids and mild diverticulosis in the sigmoid colon.
Our patient was diagnosed with chronic neutrophilic leukemia after othermyeloproliferative disorders and secondary causes had been excluded.
115
CHOROID PLEXUS PAPILLOMA COMPLICATING ACUTET CELL LYMPHOBLASTIC LEUKEMIA THERAPY
Joseph S, Siddiqui AH, Wilson F, Imran H. University of South Alabama,Mobile, AL.Case Report: Choroid plexus papilloma is a rare benign childhood tu-mor that frequently presents during infancy with signs of raised intracranialpressure due to CSFoutflow obstruction.This is the case of an older child whodeveloped T-acute lymphoblastic leukemia (ALL) and during the work up wasfound to have a ventricular mass that complicated therapy related decisions.Case Report: An 8-year-old Caucasian female presented with hyperleu-kocytosis in the context of a fever and abdominal pain. Immunophenotyp-ing upon flowcytometry on peripheral blood specimen was consistent withT-ALL. She was started on standard 4 drug induction chemotherapy. Followup imaging incidentally revealed a well circumscribed 1.2 cm lesion in the4th ventricle with no ventricular enlargement. Although CSF was negative formalignant cells, multidisciplinary team recommended additional intrathecalchemotherapy, considering the mass to be a leukemic deposit. Once she wasin remission, pros and cons of higher dose cranial radiation (assuming CNSpositive) vs. surgical morbidity were re-discussed and the decision was madeto resect the mass which turned out to be a choroid plexus papilloma. Sevenmonths into her diagnosis, the child remains in remission from leukemiawithout recurrence of the papilloma.Discussion: One case was reported previously of a patient with B-ALL withco-occurrence of choroid plexus carcinoma, but not a papilloma, whichoutnumber carcinoma by a ratio of 5:1 in general population. Even thoughmajority of the cases of choroid plexus tumors present early on, there havebeen reports of late onset presentation. Total surgical excision is curative incases of papillomas. T-ALL with hyperleukocytosis is considered a high riskdisease and entails possibility of CNS involvement. Our patient could haveended up receiving higher dose cranial radiation had we not attempted re-section. The decision to resect the mass was a difficult one, especially for achild undergoing induction/consolidation chemotherapy when blood countsand overall performance are suboptimal for any kind of invasive procedure. Ahigh index of suspicion is needed to make a diagnosis of choroid plexustumor in a patient with a pre-existing cancer especially a leukemia.
116
UNCOMMON CAUSE OF PANCYTOPENIAWITHHEPATOSPLENOMEGALY IN A YOUNG MAN
Mankongpaisarnrung C, Dumrongmongcolgul N, Sutamtewagul G, Tijani L,Nugent K. Texas Tech University Health Sciences Center (TTUHSC), Lubbock, TX.Case Report:Background: Pernicious anemia (PA) is an autoimmune disorder charac-terized by gastric parietal cell destruction and anti-intrinsic factor antibody(anti-IF Ab), resulting in B12 deficiency which can cause pancytopenia andneuropsychiatric symptoms. Alcohol intake can also reduce B12 absorptionand suppress bone marrow function. B12 deficiency may also occur with
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 405
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

dietary restriction, malabsorption, and congenital disorders of transcobala-min and IF.Case: A 36-year-old non-vegan, blood-type A man with a history of chronicalcohol use presented with fatigue, weight loss, and hematemesis for 2 months.His abdominal exam revealed massive hepatosplenomegaly (HSM), confirmedby abdominal CT scan (maximal diameters of liver and spleen- 24.4 cm and21 cm, respectively). His CBC showed WBC 3.2, Hb/Hct 4.4/12.7, Plt 23,MCV 100.9, RDW 29.6, N 24%, and L 74%. The peripheral blood smearrevealed hypersegmented neutrophils, nucleated RBCs with dysmaturation,decreased plt, and giant plt. Other labs included B12 56.4 pg/ml (low), homo-cysteine 180.4 Kmol/L (high), methylmalonic acid 12550 nmol/L (high), reti-culocyte index 0.5, negative Coomb’s test, and low haptoglobin (G8). Anti-IFAb was positive. LFT and iron studies revealed normal values except forindirect bilirubin (1mg/dl). EGD showed portal hypertensive gastropathy.Therefore, B12 deficiency from PA was diagnosed. He received 1-mg IMB12 daily for 7 days and then monthly. One month later, he had recoveredand no longer had HSM. His CBC returned to normal with Hb/Hct 12.4/36,WBC 9.1, N 66 %, Plt 346, and MCV 92.Discussion: This case had pancytopenia with megaloblastic anemia withnon-immune hemolysis (low haptoglobin and indirect hyperbilirubine-mia) due to ineffective erythropoiesis from severe B12 deficiency secondaryto PA and alcohol ingestion. Pancytopenia with HSM suggests hematologicmalignancy, but we would like to underscore the importance of peripheralblood smear in the diagnosis of B12 deficiency. In cases with pancytopeniaand HSM, PA should remain in the differential diagnoses even in low riskpatients. PA patients infrequently have transient HSM, and complete disap-pearance of HSM occurred in this patient within one month after startingtreatment.
117
INFANT ALL PRESENTING AS HYPERBILIRUBINEMIA
McClain JA, Pokala H. OU Children’s Hospital, Oklahoma City, OK.Case Report: Acute Lymphoblastic Leukemia (ALL) is the most commonmalignancy of childhood. Typical presentation includes fever, pallor, fatigue,petechiae and bone pain. Infant ALL (age G12 months at diagnosis) fre-quently presents with severe leukocytosis associated with renal insufficiencyand life threatening electrolyte imbalances. Leukemia can also expand be-yond the bone marrow and result in hepato-splenomegaly and lymphade-nopathy. At diagnosis children with ALL usually have an abnormal completeblood count (CBC) demonstrating leukocytosis or leukopenia with anemiaand thrombocytopenia. Circulating blasts may also be present.
An 11 week old previously healthy male presented to his primary carephysician with a two week history of scleral icterus with no other symptoms.Physical exam was otherwise normal. Lab work demonstrated hyperbiliru-binemia (total bilirubin 2.3 mg/dL, direct bilirubin 1.4 mg/dL). CBC withoutdifferential was reported as normal.
One week later at a follow up appointment labs demonstrated worseninghyperbilirubinemia (total bilirubin 5.4 mg/dL, direct bilirubin 3.3 mg/dL).CBC showed a white cell count of 16,500 cells/mm3 with differential in-cluding 54% blasts, as well as anemia (hemoglobin 8.6 g/dL) and thrombo-cytopenia (platelet count 109,000 cells/mm3). Flow cytometry identifiedblasts expressing CD34, HLA-DR, and CD19, but negative for CD10,TdT, T-cell and myeloid markers. This immunophenotype was consistentwith B precursor ALL. Renal function and electrolyte studies were normal.Abdominal ultrasound demonstrated hepato-splenomegaly with gallbladdersludge.
After 7 days of Induction Therapy his bilirubin markedly improved(total bilirubin 1.9 mg/dL, direct bilirubin 1.0 mg/dL) and has remainednormal.
This case reinforces the need to thoroughly evaluate late-onset jaundicein infants. While liver dysfunction can cause jaundice, checking a CBC withdifferential is also important, and in this case it was the CBC differentialthat incidentally identified leukemia as the cause of jaundice. As mentionedabove, infants with ALL most often have symptoms related to a high whitecount, and therefore leukemia involving the liver and resulting in directhyperbilirubinemia is an unusual presentation. If a CBC with differential hadnot been obtained diagnosis could have been delayed with potentially seriousconsequences.
118
IT’S ALL ABOUT THE BITE: A CASE OF BABESIOSISPRESENTING AS HEMOLYSIS
Milner CP, Elkins S. University of Mississippi Medical Center, Jackson, MS.Case Report: Babesiosis, a tick borne zoonosis, classically presents as aninfectious process characterized by acute hemolytic intravascular hemolysis.
An 82 year old Caucasian man with a past medical history significant forasthma presented to his pulmonologist with progressive fatigue and dyspneawith associated generalized weakness, fevers, subjective night sweats, and adecreased appetite for 3 weeks. He first noted the dyspnea while traveling tothe Western United States to an area of higher elevation. Several weeks priorhe had traveled to the Northeastern United States and had subsequently noteda rash consistent with erythema migrans. He was empirically treated for Lymedisease with a 5 week course of Amoxicillin.
Patient’s initial work up included a chest radiograph and EKG, whichrevealed no explanation for his new onset shortness of breath. The patient’sblood work displayed evidence of anemia and thrombocytopenia. He wasreferred to a hematologist for further evaluation. Upon further work-up, thelaboratory findings were consistent with a presence of hemolytic anemia dueto the collective presence of anemia, thrombocytopenia, an elevated reticu-locyte count, an elevated LDH, and decreased haptoglobin. In addition, thepatient had a mild transaminitis without an elevation in his indirect bilirubin.Blood smear revealed no shistocytes, but the presence of normal white bloodcell morphology, teardrop cells, a few enlarged platelets, and ‘‘sticky’’ RBCs.Given travel history with evidence of hemolysis, a thick and thin blood smeartest was ordered, but was negative for organisms. Babesiosis was suspected,and confirmed by IgG Ab of 91:2048 and a positive Babesia Microti PCR.Lyme titers returned as negative. Patient was started on Azithromycin andAtovaquone, and his hemolytic anemia has slowly resolved and his dyspneaimproved as a result.
This case highlights the importance of taking a thorough travel history ona patient with a very common complaint. As babesosis is concentrated pri-marily in the Northeastern areas of the United States, this is a disease that isnot commonly encountered in the Southern United States. Hemolytic anemiahas a broad differential diagnosis, and babesiosis must be considered inpatients whose travel history warrants further evaluation.
119
IgG4 RELATED TESTICULAR PSEUDOTUMOR
Nagireddy S, Herrin VE. University of Mississippi Medical Center, Jackson, MS.Case Report: 42 Year old African-American male noticed a left scrotalmass slowly growing for one year which was not associated with pain orweight loss. Physical examination showed a 2-3 cm firm, non-tender massin the left scrotum. Ultrasound of his scrotum showed a 2.5 x 2.4 x 2.0 cmmass superior to left epididymis. It also showed dilated vasculature of bi-lateral epididymis concerning for an obstructive lesion in the abdomen. A CTshowed a 3.3 x 1.8 cm retroperitoneal nodular mass; malignancy could not beruled out. He was scheduled for excision of left epididymal mass with possibleleft orchiectomy. Frozen section revealed a fibro-vascular lesion with a plasmacell infiltrate; no malignancy was noted, so no orchiectomy was performed.
Immunohistological stains confirmed a polyclonal plasma cell infiltratewith increased numbers of IgG4 positive cells; the IgG4/IgG ratio was 40-50%.He was diagnosed with PARATESTICULAR FIBROUS PSEUDOTUMOR,a new entity of IgG4-related disease (IgG4-RD). He was not treated withsteroids as he was asymptomatic. Repeat imaging of his abdomen after6 months showed a slight decrease in the size of the right paracaval retro-peritoneal mass. He continues to be asymptomatic
IgG4-RD’s are a group of disorders associated with multi-organ involve-ment mimicking an inflammatory or neoplastic process. They are characterizedby mass-forming lesions with pathology showing lymphoplasmacytic infil-trates and sclerosis. Multiple organs may be affected and share similarpathological and clinical features. Lymphadenopathy is common and re-sponds well to steroids. Proposed diagnostic criteria include increase in theIgG4 serum levels, more than 45 IgG4 positive cells per high power fieldand ratio of IgG4/IgG ration930% (Zen et al). An increase in the number ofT-regulatory cells with the production of IL-10 and transforming growthfactor (TGF) was also proposed in the pathogenesis of IgG4-RD (Tsuboi et al).
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
406 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Paratesticular Fibrous Pseudotumor is a rare benign tumor of unknownetiology possibly related to IgG4-related disease (Bosmuller et al). In our casethe patient presented with testicular mass and retroperitoneal lymphadenop-athy concerning for malignancy; fortunately, pathology confirmed IgG4-RD.Awareness of the spectrum of IgG4-RD diagnosis will decrease confusionand misdiagnosis.
120
BREAST IMPLANT ASSOCIATED ALK NEGATIVEANAPLASTIC LARGE T CELL LYMPHOMA
Neppalli AK, Koshy NV. LSU Health, Shreveport, LA.Case Report: A 45 year old female with history of ductal carcinoma in situ(DCIS) underwent bilateral mastectomy and breast reconstruction with salineimplants 10 years prior, presented to our facility with worsening discomfortand swelling in left breast. Physical examination was significant for asym-metrically enlarged left breast and imaging study with ultrasound showedfluid collection (seroma) around left breast implant. The fluid was subse-quently evacuated along with removal ofimplant. The pathology from the inneraspect of fibrous capsule and fluid was consistent with ALK-ve anaplastic largeT cell lymphoma. PET-CT scan did not show convincing evidence of FDG avidneoplastic process anywhere else. Patient was treated with systemic chemo-therapy with 4 cycles of CHOP followed by localized radiation.
Breast implant related anaplastic large T cell lymphoma is a rare lym-phoma with less than 50 cases described so far. The natural history, biologicbehavior and therapeutic strategy for this rare variant is not well defined.
121
DUODENAL DIFFUSE LARGE B CELL LYMPHOMA
Nusrat M, Tijani L, Aly M, Pannikkath R, Elbakush A, Umyarova E. TexasTech University Health science Center, Lubbock, TX.Purpose of Study: The duodenal involvement of the Lymphoma is a rarecondition and in this report we present a recent case of primary large B celllymphoma that was admitted to our Medical Center.Methods Used: Case reportSummary of Results: The patient is a 59 year old man who was admittedto the hospital with a four days history of nausea, vomiting and epigastricpain. Pain increased two hours after eating. He also had intermittent melenaand had lost about 12 lbs over 2 months. He had no fever or night sweats.
Physical examination showed normal vital signs. There was no significantlymphadenopathy. The only abnormal sign on examination was epigastrictenderness. Laboratory studies showed normal CBC, basic metabolic panel,and coagulation profiles but elevated liver enzymes (ALT 188, AST 101,alkaline phosphatase 220). Bilirubin was normal. CT abdomen showed a largesmoothly rounded mass in the descending part of the duodenum which wasconfirmed by MRI. Upper GI endoscopy revealed fungating bleeding mass inthe duodenum. A biopsy established the diagnosis of diffuse large B celllymphoma. Patient was started on R-CHOP chemotherapy and dischargedwith follow up at the Cancer Center.Conclusions: The diagnosis of a primary GI lymphoma requires that thereis no peripheral or mediastinal lymphadenopathy, a normal white bloodcell count and differentials on the peripheral blood smear, and tumor in-volvement predominantly in the GI tract with no evidence of liver or spleeninvolvement.
In a study of 371 patients registered in a German multicenter treatmentstudy for GI lymphomas, the stomach was most common site for involvement(75%), followed by small bowel (including duodenum- 9%), ileocecal region(7%), rectum (2%), and diffuse colonic involvement (1%) (2,3). In the UnitedStates, small bowel lymphoma occurs predominantly in adults, peaking in theseventh decade, and 60 percent of patients are male (4). Some of the pre-disposing conditions include autoimmune diseases, immunosuppression,Crohn’s disease, radiation therapy and nodular lymphoid hyperplasia. In ourpatient, the lymphoma was discovered in the second part of the duodenum.The patient had none of the previously mentioned predisposing factors exceptgender. Since this kind of tumor is rare, we present this case to remind cli-nicians about this type of primary GIT lymphoma.
122
BRAIN METASTASIS IN A CHILDWITH HEPATOBLASTOMAAND BECKWITH WIEDEMANN SYNDROME
Nwankwor I, Siddiqui AH, Wilson F, Imran H. University of South Alabama,Mobile, AL.Case Report: Background Hepatoblastoma is the most common childhoodliver tumor and mostly occurs in children G 5 years of age. Its incidence inBeckwith-Wiedemann syndrome (BWS) is 2,280 times that of the US chil-dren. Although hepatoblastoma commonly metastasizes to the lungs, brainmetastases are very rare. We report a 2 year old African American female withBWS and hepatoblastoma recurrence in the brain. Case Report A 33 weekpremature baby had omphalocele, macroglossia and hemi-hypertrophy ofthe right side. Genetic testing confirmed BWS. At 9 months of age an un-resectable right lobe liver tumor (9cm x 6cm) mass was found on routineultrasound. Serum alpha fetoprotein (AFP) level was 241,831. A liver biopsyconfirmed a mixed type hepatoblastoma with teratoid features. Metastaticwork up was negative. She was treated with vincristine, cisplatin and 5-flourouracil and a right hepatic lobectomy. She remained in remission for3 months until serum AFP level started to rise again. Imaging studies showeda subpleural 0.9 x 0.9 cm left lower lobe pulmonary nodule which was foundto be metastatic hepatoblastoma upon resection. The family refused chemo-therapy at that time. She remained relatively asymptomatic till 2 years ofage when she experienced new onset seizures the context of a viral illness.Brain imaging demonstrated 3 hyper dense parenchymal masses (largestmeasured 3.5 x 2.8cm). A biopsy confirmed metastatic hepatoblastoma. Sheunderwent cyberKnife stereotactic radiosurgery and received vincristine andirinotecan that were stopped after 3 cycles due to continued worsening ofthe brain and pulmonary lesions on imaging studies. The family refusedfurther chemotherapy options and she remained on hospice care until herdeath due to cardiopulmonary arrest at an age of 32 months. Discussion Theprognosis of children with hepatoblastoma with distant metastases is poor. Achild with cancer who presents with any central nervous system symptomor sign requires a high index of suspicion and urgent imaging studies. Thefinding of the brain metastases was unexpected given the rarity of such apresentation. Multiple metastases to the brain excluded a complete resectionwhile other comorbid conditions (BWS) prevented the family to opt for a thirdline more toxic chemotherapeutic agents.
123
A 36-YEAR-OLD MAN WITH LEFT UPPER QUADRANT PAIN,ANEMIA AND THROMBOCYTOPENIA
Paccione R, Spera M, Narmala SK, Boulmay B, Jetly-Shridhar R. LSUHealth Sciences Center, New Orleans, LA.Case Report:Case: A 36 year old African American man with past medical history ofhypertension and morbid obesity initially presented to a local hospital withleft upper quadrant pain, decreased appetite, and a thirty pound weight lossof two months duration. Four weeks later the patient returned with epistaxisand bilateral subconjuctival hemorrhage and he was transferred to our facility.Vital signs were blood pressure 140/69 mm Hg, pulse 108 bpm, respiratoryrate 20/min, and temperature 100.2-F. Physical examination revealed bilat-eral subconjuctival hemorrhage and splenomegaly with the spleen extending10-20 cm below the left costal margin. Pertinent laboratory values includeAST 67u/L, alkaline phosphatase 72 u/L, ALT 24 u/L. WBC 23,900 uL (33%segmented neutrophils, 6% bands, 21% lymphocytes, 9% monocytes, 29%immature mononuclear cells, and 13% nucleated RBC’s), hemoglobin 6.1 g/dL,hematocrit 17.2%, and platelet count 10,000 uL. Uric acid was elevated at8.7 mg/dL and LDH was elevated at 2,460 u/L. Abdominal ultrasoundrevealed severe splenomegaly with the spleen measuring 26.5 cm and he-patomegaly with the liver measuring 26.3 cm. A diagnosis of hepatosplenicT-cell lymphoma based on the clinical presentation and was supported byfindings on the liver biopsy. The patient was started on hyperCVAD fol-lowed by a course of pralatrexate. Unfortunately, both of these interventionsfailed and a course of gemcitabine with cisplatin was a final attempt. Arepeat bone marrow aspirate revealed persistence of hepatosplenic T celllymphoma despite multiple failed treatment modalities and the patient wasdischarged to hospice where he died two weeks later.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 407
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Discussion: Hepatosplenic T cell lymphoma is a rare, aggressive peripherallymphoma. The median survival is approximately eight months despite in-tervention with chemotherapy. Though no current treatment guidelines cur-rently exist, several different chemotherapy options are being applied in hopesof achieving remission. The only curative option currently available is allo-genic bone marrow transplantation if and when the patient achieves completeremission. Aggressive chemotherapy is warranted to halt disease progressionand reduce the mortality rate of this atypical neoplasm.
124
DYSKERATOSIS CONGENITA DUE TO A RARE DKC1GENE MUTATION
Raulji C, Gardner RV, Lacassie Y. LSUHSC Dept of Pediatrics at Children’sHospital of New orleans, New Orlenas, LA.Case Report: Dyskeratosis congenita (DC) is a severe inherited disorderinvolving rapidly dividing somatic tissues in the adult, such as bone marrowand skin. Major features include aplastic anemia, abnormal skin pigmenta-tion, nail dystrophy and leukoplakia. Other variable features may be present.The minimal clinical diagnostic criteria include the presence of at least 2 ofthe 4 major features. X-linked, autosomal dominant and recessive forms ofthe disease exist, broadly sharing the same phenotype. Three autosomaldominant genes, five autosomal recessive, and one X-linked gene, the DKC1,mapped to Xq28 encoding the protein dyskerin, have been identified.
We report a 12 year-old AA male referred to Hematology-Oncology forlow platelets and anemia (WBC 4,780, Hb 8.5, platelet count 29,000, MCV104.3, MCH 35.9 and MCHC 34.4). He was born via emergency C-sectionfor placenta previa with heavy bleeding at 39 WGA. He was SGA (2,010g).Apnea, dysphagia, pulmonic stenosis, periorbital fullness, somewhat prom-inent ears, down-slanting palpebral fissures and ptosis, and excessive nuchalskin initially suggestedWilliams, Noonan, Coffin-Lowry and other syndromes,but were ruled out. Other problems in childhood included FTT, seizure dis-order, bilateral hip dysplasia, recurrent respiratory infections, dental caries,dextroscoliosis and left clubfoot.
When evaluated by us at age 12 years, remarkable short stature (50th
percentile for 6-6.5 years) and microcephaly (50th percentile for 10 months)with severe intellectual disability, sparse hair, dental caries, palmoplantarhyperkeratosis, calloused finger joints and dystrophic fingernails were noted.The family history was remarkable for dry skin in his mother and maternalgrandmother. The family refused bone marrow examination but gene testingshowed a c.472C9T(p.R158W) nucleotide change in exon 6 of DKC1 geneon X chromosome. This change is predicted to result in replacement ofarginine at position 158 in DKC1 protein with tryptophan. To our knowledgethis is the second reported case of DC with this novel c.472C9T mutation inDKC1 further supporting the causative role of this rare mutation in X-linkedDC. We are in the process of testing the mother for the mutation.
125
A SKIN NODULE NOT TO BE IGNORED: CASE REPORTOF MERKEL CELL CARCINOMA
Rean K1, Wright S2, Smalligan RD1. 1Texas Tech University Health SciencesCenter, Amarillo, TX and 2VA Medical Center, Amarillo, TX.Case Report: An 81-year-old man presented for evaluation of a firm,red, nodular lesion on the forearm that had been growing for two weeks.Pertinent past medical history includes stage III follicular lymphoma in re-mission and numerous previous skin cancers suggestive of sun damage. Apunch biopsy identified the lesion as a high-grade neuroendocrine tumor,consistent with Merkel cell carcinoma (MCC). Histology revealed atypicalbasaloid cells with a high mitotic rate that stained positive for neuroendo-crine and endothelial markers. Lymph nodes were negative by clinical exam,and CT scans were negative for adenopathy or metastasis. One month laterthe tumor had metastasized to the face, identifying the cancer as stage 4. Thepatient agreed to radiation but refused chemotherapy. The lesions continuedto grow, covering almost the entire forearm, and many reddish-purple satel-lite lesions appeared on the face. The patient died in hospice care 7 monthsafter initial presentation.
Discussion: Merkel cells are mechanoreceptors of neural crest origin thatare scattered throughout the basal layer of the epidermis. Although Merkelcell carcinoma is relatively rare, its incidence has been steadily increasingand has tripled in the past 30 years. Affected individuals are commonly whitemen with a median age of 74. The two most prominent risk factors are ex-posure to UV light and immunosuppression. Additionally, MCC is seen at ahigher rate after diagnosis with other skin cancers or lymphoma, both ofwhich our patient had. MCC typically presents as a painless, firm, pink nod-ule on the head, neck or upper extremities (sun-exposed areas). Tumor growth israpid with a high tendency to metastasize to draining lymph nodes, distantskin sites and hematogenously. Clinical diagnosis is inaccurate, so biopsy andimmunological staining is required. Treatment is wide local excision withsentinel node dissection. Although radiation can decrease recurrence and che-motherapy may be used for distant metastases neither treatment affects sur-vival. Prognosis is 50-68% survival at 5 years with high rates of recurrencewithin two years. This case reminds physicians who treat the elderly andpractice in an area with high sun exposure to keep MCC in the differentialdiagnosis of a rapidly growing skin lesion.
126
FALSE POSITIVE HIVANTIBODY TEST IN A PATIENT WITHT CELL LYMPHOMA
Umyarova E, Hailemariam Y, Suvorava N, Alalawi R, Tijani L. TTUHSC,Lubbock, TX.Case Report: It is important to test for HIV in patients with lymphomas.HIV screening is performed by ELISA test for HIVAb-1 or particle agglu-tination assay for HIV 2, although approximately 0.5% of the patients pos-itive on a screening tests are false positives. We report a case of mature T celllymphoma presented with false positive HIV screening test results.
A 50 y.o male presented with weight loss, night sweats, fever, fatigueand generalized lymphadenopathy. Physical exam revealed multiple cervical,axillary and inguinal lymph nodes and splenomegaly. Laboratory results weresignificant for elevated total protein with increased gamma fraction on serumprotein electrophoresis. HIV immunoassay screening test was reactive forHIV 2 antibody but the HIV Western Blot and HIV RNA PCR were nega-tive. Repeated HIV screening, HIV RNA PCR and Western Blot were neg-ative, indicating an absence of infection. Imaging studies revealed bilateralbulky lymphadenopathy with splenomegaly, suggestive of lymphoma (figure 1).Core needle biopsy of the cervical lymph node was consistent with matureCD 4 positive T cell lymphoma. Patient was started on chemotherapy withEtoposide, Vincristine, Cyclophosphamide and prednisone and external ra-diation therapy.
Only few cases of cross-reaction with HIV were associated with T celllymphoma. Several mechanisms of antibody reaction to HIV were proposedalthough the exact cause is still unknown. One of the possible culprits isgamma globulins, resulted from polyclonal B cell activation, which non spe-cifically bind to immunoassay plate and react with HIV antigens to cause afalse-positive result. Our patient had polyclonal hypergammaglobulinemia,detected on serum protein electrophoresis.
Diagnosis of HIV infection should always be considered in patients withclinical symptoms of lymphoproliferative disorders. Occasionally patientspresent with false positive HIV screening tests.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
408 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

127
OSTEOPOIKILOSIS MIMICKING OSSEOUS METASTASES INA PATIENT WITH STAGE I RENAL CELL CARCINOMA
Umyarova E, Nusrat M, Suvorava N, Dar N, Laski M, Cobos E, Tijani L.TTUHSC, Lubbock, TX.Case Report: Osteopoikilosis is a rare, autosomal dominant bone dyspla-sia, characterized by multiple, discrete, round radiodensities seen in axial andappendicular skeleton. We would like to report a rare case of osteopoikilosisin a patient with early stage renal cell carcinoma.
43 y.o. woman with a PMH significant for a stage I renal cancer wasreferred for evaluation of the suspicious lesions seen on spine and pelvisbones on the CT done in 06/11.
She was diagnosed with clear cell renal carcinoma and underwent a rightand left nephrectomy in 06/09. Due to a very early stage renal cancer she didnot require any adjuvant treatment. Repeated CT scans of the abdomen andpelvis from 01/11, continued to show stable sclerotic lesions. PET/CT scanshowed non FDG-avid multiple sclerotic foci without metabolic activity. Inthe light of these findings the patient was diagnosed with osteopoikilosis.Review of her previous CT scans showed similar lesions in2006. The patientremains symptom-free. Discussion: Osteopoikilosis is a rare skeletal dys-plasia characterized by the presence of symmetric, small homogenous ovoidlesions. It presents histologically with an increase in the number and thick-ness of the trabeculae of the spongy bone. Radiologically lesions represent around foci of bone sclerosis, not affecting the cortical bone, and often ori-ented parallel to the shaft of the tubular bones. Our patient was referred dueto radiological changes suspicious for osteoblastic metastases, but there wereno hot spots indicating increased uptake or metabbolic activity on repeatedbone scan and PET/CT. Osteopoikilosis is an asymptomatic condition andfound incidentally on plain radiographs made for other reasons. This diseaseshould be kept in mind in cancer patients, since the prognosis is benign andno specific treatment is required.
128
FROM THE BOTTOM OF MY HEART: A CASE OFMETASTATIC ANGIOSARCOMA
Williams JC, Thigpen JT. UMC, Jackson, MS.Case Report: Primary cardiac tumors are a rare occurrence. Excludingatrial myxomas, the prevalence of primary cardiac tumors is 0.001-0.28%.Atrial myxomas, which are benign, comprise 75% of primary tumors of theheart. The remaining 25% are malignant tumors. Approximately 33% of themalignant tumors of the heart are sarcomas.
We present the case of a 33 year old African American woman with thehistory of a recent partial pericardial mass resection at an outside hospital in2/2012. The pathologic specimen was interpreted to be a hemangioen-dothelioma. The patient was referred to UMC Oncology shortly thereafter forevaluation and management. The patient did not attend her appointment asshe believed that her tumor was benign despite being informed otherwise.Moreover, the patient’s devout Pentecostal belief system also contributed toher belief that she was healed of her malignancy via faith.
Six months later, the patient presented to the UMC emergency room withcomplaint for abdominal pain, nausea and vomiting for 3 weeks. CT chest/abdomen/pelvis on 9/6/2012 showed a large right pericardial mass, multiplepulmonary nodules, hepatomegaly with numerous lesions causing com-pression of distal stomach and duodenum, numerous skeletal lesions, and alarge left gluteal mass. MRI of the brain revealed innumerable lesion of thebrain consistent with metastatic disease. A biopsy of one of the abdominallesions along with review of the pathology slides from the OSH revealed thatthe patient had metastatic angiosarcoma. The patient was offered chemo-therapy along with whole brain irradiation, however, she refused because shefelt that her faith in God along with fervent prayer would heal her. Afteracknowledging her faith, many discussions were had with the patient and herfamily members utilizing their belief system to encourage acceptance oftreatment. The patient agreed to therapy of weekly Gemzar/Taxol chemo-therapy along with whole brain irradiation.
Although rare, primary malignant cardiac tumors are amenable to multi-modality therapy. This case illustrates the importance of understanding and
acknowledging the biopsychosocial considerations a health care providermust address with their patients to ensure beneficience.
129
SECONDARY CUTANEOUS DIFFUSE LARGE B CELLLYMPHOMA INITIALLY DESCRIBED AS A T CELLHISTIOCYTE RICH B CELL LYMPHOMA
Zaiden R1,2, Hew JD1. 1UF JAX, Jacksonville, FL and 2UF JAX, jacksonville, FL.Case Report: Diffuse Large B cell lymphoma (DLBL) is an aggressive,high grade subtype of Non - Hodgkins Lymphoma (NHL), accounting forabout 30% of these tumors annually. Genetic analysis confirms significantheterogeneity within this population. The skin is the second most commonextranodal site of involvement behind the gastrointestinal tract. T cell/His-tiocyte Rich Large B cell Lymphoma (THRLBCL) is a rare pathologic entity,listed as an uncommon variant of DLBL in the 2008 WHO reclassification. Itis characterized by the presence of G10% neoplastic B cells in an inflam-matory background of non-neoplastic T-cells and histiocytes. It infrequentlyprimarily involves the skin. We present the case of a 64 year old maleevaluated for a large ulcerating tumor of the back. Skin biopsy performed atan outside institution was initially interpreted as a THRLBCL. Secondopinion review of the biopsy at our institution concluded that this was cu-taneous DLBCL, given the non-dispersed nature of neoplastic B cells. Thiscase highlights the subtle differences, and difficulties, often with therapeuticand prognostic implications in accurate subclassification of this disease.
Joint Plenary Poster SessionInfectious Diseases, HIV and AIDS
5:00 PMThursday, February 21, 2013130
SEPTIC EMBOLI NOT CAUSED BY ENDOCARDITIS
Almeida M, Lathia V, Engel LS, Taylor S. LSU Health Sciences Center, NewOrleans, LA.Case Report:Introduction: Septic emboli usually arise from bacterial infections in theheart valves. We present a case of bacteremia and embolic phenomenonwithout endocarditis.Case: A 50-year-old African American man with history of recurrent alco-holic pancreatitis presented to the emergency department 2 days after de-veloping epigastric pain that radiated to his back and was accompanied bynausea and vomiting. He also developed mild left sided weakness 24 hrsbefore admission. He had no fever, chills, headache, diarrhea, chest pain, orseizures. He denied illicit intravenous drugs use. Vital signs at admit were:Temperature 100oF, Pulse 90, Respiratory rate 18, Blood pressure 140/100.He appeared cachectic. His neck was supple, heart was regular and nomurmurs were heard, lungs were clear, his abdomen had normal bowelsounds but was distended, tight, tender to palpation without rebound, and thestrength in his left side was 4/5. His white blood cell count, amylase, andlipase were all elevated. Blood Cultures were positive for Enterococcusavium. Abdominal/pelvic CT scan showed ascites, atrophic appearance of thepancreatic tail and large bilateral renal infarcts. Head CT scan demonstratedsubacute infarction in the left occipital lobe, acute infarction in the rightcorona radiata. Transesophageal echocardiography demonstrated the pres-ence of a long serpigenous thrombus in the ascending aorta propagating inand out of the descending Aorta. The patient underwent thrombectomy andhe was successfully treated with IV antibiotics for 4 weeks.Discussion: Infectious thoracic aortitis (IA) is an uncommon disease thatmost frequently occurs in patients with atherosclerotic aortic disease and/orinfective endocarditis. Various microorganisms have been associated withinfectious thoracic aortitis, most commonly Staphylococcus aureus, Group AStreptococci, Streptococcus pneumoniae, Enterococcus species, and Sal-monella species. A combination of surgical and medical therapy is required toreduce mortality.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 409
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

131
A SMALL FOR GESTATIONAL AGE NEWBORN WITHMICROCEPHALY, AN UNCOMMON CASE OFCONGENITAL INFECTIONAlrifai W, Zayek M, Estrada B, Custodio H. University of South Alabama,Mobile, AL.Case Report: A 1612 gram female born at 37 weeks gestation was notedto be small for gestational age and microcephalic. She was born to a 27 yearold mother who visited daily during pregnancy, a house infested with rodents.Prenatal tests were negative for rubella, hepatitis B, syphilis, and human im-munodeficiency virus. Serial sonograms showed intrauterine growth retarda-tion and hydrocephalus. Physical exam showed weight, length, and headcircumference all below 3rd percentile. The rest of the exam was unre-markable. Computed tomography scan of the brain showed severe brain at-rophy, periventricular calcifications, ventriculmegaly, porencephaly, and cystictransformation of the periventricular white matter. Lab testing was negativefor cytomegalovirus, herpes simplex virus, enterovirus, toxoplasma, HIV, andparvovirus. An indirect fluorescent antibody test for Lymphocytic Chorio-meningitis Virus (LCMV) revealed elevated IgM and IgG antibodies.Discussion: LCMV is an enveloped single stranded RNA arena virus, forwhich the common house mouse, Mus musculus, is both the natural hostand reservoir. It is believed that congenital LCMV infection is an underdi-agnosed disease. Infection during pregnancy may lead to spontaneous abor-tion, survivors have significant risk for neurologic and ophthalmologicdysfunction. Neurologic manifestations include microcephaly, seizures, jit-teriness and abnormalities in muscle tone. Neuroimaging may add, periven-tricular calcifications, ventriculomegaly, hydrocephalus, cerebellar hypoplasia,encephalomalacia, and porencephalic cysts. Eye involvement is another char-acteristic feature with chorioretinitis seen in 93% of infants. Systemic signsoutside of the nervous system are infrequent, therefore, infants suspected tohave congenital infection but have signs limited to the central nervous sys-tem (CNS), LCMV should be considered. Diagnosis is made by immuno-fluorescent antibodies, enzyme-linked immunosorbent assay, or complementfixation detecting both IgM and IgG antibodies. The outcome is poor withcerebral palsy and other neurodisabilities may be seen. Treatment is sup-portive and management should aim for early behavioral and developmentalinterventions. As a preventive strategy, pregnant women should avoid expo-sure to rodents and their excreta.
132
DEVIL IN DISGUISE: A CASE OF TUBERCULOUS CYSTITIS
Anderson SD, Anderson RM, Rodriguez PS, Smalligan RD. Texas TechUniv Health Sciences Center, Amarillo, TX.Case Report: A 74-year-old Hispanic female who immigrated fromMexico15 years ago presented with a one week history of malaise, fever, dysuria,frequency and urgency. Three weeks prior, she was treated for a UTI withantibiotics. At that time, creatinine was 1.5. A renal sonogram showed mildcaliectasis of the right kidney. Before she could follow up with nephrology,her symptoms worsened. On admission, urinalysis showed moderate blood,large leukocyte esterase, WBC 155, RBC 12. CXR, CBC, and CMP werenormal, except for creatinine 1.65. Urine culture grew G10,000 colonies withmixed genital flora. Despite antibiotics and hydration her creatinine rose andrepeat sonogram showed hydronephrosis. Urology was consulted and cys-toscopy was performed with insertion of bilateral ureteral stents and bladderbiopsies. Pathology showed granulomatous, focally caseating cystitis withacid-fast bacilli present, consistent with tuberculous cystitis. She was placedon anti-tuberculosis therapy and is currently doing well on observed therapydirected by the local health department.Discussion: While tuberculosis classically affects the lungs, up to 20% ofcases involve extrapulmonary disease. Physicians must maintain a high levelof suspicion for these manifestations especially in the elderly, immunocom-promised, or patients from endemic countries. Tuberculosis cystitis may beeasily overlooked because it presents similarly to conventional cystitis withcomplaints such as dysuria, frequency, and suprapubic pain. Constitutionalsymptoms occur in less than 10% of cases. Suspicion should be aroused whenantibiotic treatment fails to relieve symptoms, or there is sterile pyuria (ele-vated WBC in the urine with the absence of growth on standard culturemedium). Bladder wall thickening and ulceration may be seen on cystoscopy.
Renal failure can result through a variety mechanisms. Infected kidneys canlead to ESRD and irreversible loss of function. Affected kidneys can alsocalcify and lose function. Delayed diagnosis can cause obstructive uropathyas seen in our patient. Modern multi-drug tuberculosis therapy is an effec-tive treatment for genitourinary tuberculosis. By maintaining a high level ofsuspicion, especially in high-risk populations, the disease may be treated be-fore devastating complications occur.
133
FASCINATINGLY FASTIDIOUS CASE OF EIKENELLAFACETITIS
Atkinson E, England A, McAuliffe M, Haman T, Martin DH. LSU HealthSciences Center, New Orleans, LA.Case Report:INTRODUCTION: Facet joint infection (facetitis) is an uncommon typeof pyogenic spine infection that can cause acute back pain and significantmorbidity unless promptly treated.CASE: A 63 year-old woman with mild, non-debilitating osteoarthritis pre-sented with five days of crescendo lower back pain, which was so severeon arrival that she could no longer walk. Her pain was relieved by lying onher side with hips flexed. She denied lower extremity weakness or pares-thesia, loss of bowel or bladder function, or recent trauma. Oral temperatureat triage was 39.3 -C. Palpation of her L4 spinous process greatly exacer-bated her pain, and her paraspinous muscles were rigid. She had good rectaltone and no saddle anesthesia, and the remainder of her neurologic examincluding straight leg raise was normal. There were no integument defects orsigns of infection over her lumbosacral spine, and she denied intravenousdrug use. Plain film and CT of the lumber spine were unremarkable for signsof trauma or vertebral osteomyelitis. Given her leukocytosis and elevatedinflammatory markers, she was empirically started on broad spectrum anti-biotics. Blood cultures resulted as positive for Eikenella corrodens in 4 of4 bottles by 28 hours. Echocardiogram was normal. Further review of theCT revealed inflammation and bone destruction at the L3-L4 facet joints,and gallium scan demonstrated enhancement in this region. MRI was con-traindicated in our patient due to a vascular clip in her brain. By this time,our patient was afebrile and able to walk with minimal discomfort, and herinflammatory markers had begun to normalize. She completed a four-weekcourse of intravenous ceftriaxone via an outpatient infusion center. On followup, she was completely asymptomatic.DISCUSSION: Our patient manifested a rare type of spinal infection causeby an organism which uncommonly causes disease outside the oral cavity.That the unusual sometimes happens in medicine is a powerful motivatorto remain ever vigilant. This case also highlights the importance of takinga step back when the evidence does not seem to fit. Initial interpretationof the radiologic studies focused on looking for evidence of trauma andspondylodiscitis, and the subtle manifestations of facetitis were overlooked.
134
BONJOUR VIEIL AMI, LEMIERRE
Atkinson E, Engel LS. LSU Health Sciences Center, New Orleans, LA.Case Report:Case: A 17 year-old woman presented with acute onset of sore throat andfever to her primary care physician, who presumptively diagnosed her withmononucleosis on the basis of a negative rapid strep test. Several days later,after developing tonsillar exudates and with a repeat negative rapid streptest, she was given intramuscular steroids. She developed left-sided neck painlater that day. One week later, she reported to her community hospital withfever, chills malaise, sore throat, oral ulcers, nausea, vomiting, and diarrhea.She exhibited bibasilar crackles, and chest x-ray demonstrated a large rightlower lobe consolidation. Her left anterior neck and clavicle were swollenand tender to palpation. She was given vancomycin and ceftriaxone for lo-bar pneumonia but did not improve. Chest CT demonstrated scattered smallcavitary nodules at the lung periphery, bilateral pleural effusions, cystic le-sions in the left lobe of the thyroid, and rightward deviation of the trachea.After her ceftriaxone was replaced with ampicillin-sulbactam and azithromycinshe stabilized, and her antibiotics were subsequently changed to meropenemand voriconazole. Repeat CT chest illustrated a decrease in the sizes of thepulmonary nodules and effusions, as well as the thyroid nodules, but showed
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
410 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

a rim-enhanced fluid collection at the head of the left clavicle. MRI find-ings were consistent with osteomyelitis of the clavicular head. The patientcontinued to slowly improve on the antibiotic regimen of meropenem andvoriconazole. Initial blood cultures which were allowed to incubate for an ex-tended period of time revealed GNRs at twelve days which were identified asFusobacterium necrophorum. Our patient completed a four-week course ofintravenous metronidazole, with slow but complete resolution of her symptoms.Discussion: Lemierre’s syndrome, also known as post-anginal septicemia,is a once-dreaded complication of oropharyngeal infection. Left untreated,an oropharyngeal infection can pave the way for oral flora to invade the peri-tonsillar space, great vessels of the neck, and ultimately the entire bodythrough hematologic dissemination. While antibiotics have largely elimi-nated this malady, Lemierre’s syndrome does occasionally occur in the presentday and can be fatal.
135
MORE THAN A MELODY: CAT SCRATCH FEVER IN ANIMMUNOCOMPETENT 38 YEAR-OLD MALE
Austin C, Engel LS, Thelin C. LSU Health Sciences Center, New Orleans, LA.Case Report:Case: A 38 year-old man presented to his primary care doctor’s office witha complaint of intermittent fevers for a period of three weeks and new-onset lymphadenopathy of three days duration. The patient reported a max-imum temperature of 101.4 oF at home readings. He also had general malaise,fatigue, chills, and myalgias without any associated arthralgias. Two weeksprior to his present illness, the patient had received multiple scratches on hisarms and legs after attempting to bring a feral cat to the veterinarian’s of-fice. The scratches healed, with the exception of two pustules on his rightwrist. On physical exam, the patient was noted to have a temperature of100.2 F, and all other vital signs were unremarkable. He had a 0.5 cm lesionon his right wrist with a pustular but non-indurated area surrounded by 2 cmof erythema. He also had significant right axillary lymphadenopathy, mea-suring 5 x 5 cm on physical exam, which was confirmed by ultrasoundof the axilla. Bartonella henslae IgM titers were positive at 1:160 (normalG1:20) and IgG titers were positive at 1:512 (normal G1:64). Results of aCBC with differential, chest radiograph, and metabolic panel were withinnormal limits. Discussion: Cat scratch fever is typically considered a diseasethat has a pediatric predominance, but can be found in adults with a historyof feral feline exposure, making it a part of the fever of unknown originevaluation. The differential for fever of unknown origin remains long and com-plex, but the classic presentation of disease due to Bartonella narrows thediagnosis significantly. Treatment of affected individuals is aimed at reliev-ing symptoms and discomfort. Treatment modalities, such as macrolidesand fluoroquinolones to eliminate the infection, and bedside needle drain-age of suppurative nodes are the only indicated therapies.
136
KAWASAKI DISEASE IN A PATIENT WITH ARETROPHARYNGEAL ABSCESS
Black A1, Balan A1, Faridali RG2. 1University of Oklahoma, Oklahoma City,OK and 2University of Oklahoma, Oklahoma City, OK.Case Report:INTRODUCTION: Kawasaki disease (KD) has emerged as the most com-mon cause of acquired heart disease in the developed world. KD is an idio-pathic, acute, self-limited vasculitis, with 15-25% of untreated childrendeveloping coronary artery ectasia or aneurysms. Clinically, it is character-ized by fever, rash, conjunctival injection, changes in lips/oral cavity, andcervical adenopathy. We present the rare finding of a retropharyngeal ab-scess (RPA) in a 2 year 11 month old male who was subsequently diagnosedwith KD.CASE REPORT: The patient presented with a 4-day history of fever, 3-dayhistory of rash, non-exudative bulbar conjunctivitis, cervical adenopathy,and edema and erythema of the extremities. Soft tissue films were obtainedin the ER and were consistent with prominent prevertebral soft tissue swell-ing; CT of the neck revealed a rim-enhancing, centrally hypodense lesion inthe retropharyngeal space concerning for RPA. Antibiotic therapy with clin-damycin was initiated. However, upon admittance, given patient’s clinicaland laboratory findings concerning for KD, including an elevated ESR, CRP,
hypoalbuminemia, and sterile pyuria, the patient was treated on day 4 ofillness with immune globulin intravenous (IGIV) and high dose aspirin.The patient defervesced after treatment with IGIV and his initial echocar-diogram was within normal limits. He was discharged home on high doseaspirin therapy and to complete a 7-day course of clindamycin for the RPA.Upon follow-up on day 13 of illness he was noted to have periungualdesquamation of the fingers and toes and thrombocytosis, characteristicsof the subacute phase of KD.DISCUSSION: We present the rare finding of an RPA in a patient who wassubsequently diagnosed with KD. The prevalence of retropharyngeal pa-thology in KD is unknown as routine imaging of the neck is not indicated forthe diagnosis. While a recent retrospective study found statistically signifi-cant changes in characteristics of the retropharyngeal space in KD and non-KD patients, an RPA is a rarely reported clinical finding in KD. Our patientdid not develop coronary changes, most likely due to prompt diagnosis andtreatment for KD. Our case report highlights that the presence of an RPAshould not dismiss a suspected diagnosis of KD.
137
DISSEMINATED NOCARDIA CYRIACIGEORGICA IN ALIVER TRANSPLANT RECIPIENT WITH CHRONICREJECTION
El-Bakush A, Nusrat M, Aly M, Mughal A, Yarbrough S, Desai V. TexasTech University Health Sciences Center, Lubbock, TX.Case Report:Introduction: Nocardia are slowly growing, gram-positive, beaded, branch-ing rods, partially acid-fast and are common worldwide in the soil. They be-long to a group known as aerobic actinomycetes. More than 50 species havebeen identified and more than 30 species have been associated with humandisease. N. cyriacigeorgica is one of the species associated with systemicdisease. We present a patient with liver transplant rejection on immunosu-pression that developed pulmonary and cutaneous nocardiosis.Case report: A 22 year-old female with history of liver transplant in 2005,with chronic graft rejection treated with tacrolimus and prednisone presentedwith left side chest pain, worse by cough and inspiration. She was jaundicedon exam and chest was clear. Temperature was 100.2 F. Labs were significantfor elevated liver function tests, total bilirubin of 31.3 and WBC 13.7. Chestx-ray was normal. She was discharged with a diagnosis of musculoskeletalpain. Five days later she returned with worsening chest pain and a nodule onher left wrist. Exam revealed multiple other subcutaneous nodules. WBC was19.6 and her chest x-ray was normal. A CT scan of the chest showed a sin-gle thick walled cavity of the left upper lobe. Nocardia was suspected andthe patient was started on high dose Trimethoprim-Sulfamethoxazole (TMP-Sulfa). CT scan of the head was normal. Aspiration of a nodule was per-formed and the results returned as gram positive branching rods which laterwere reported as aerobic actinomycetes. Blood cultures grew N. cyriaci-georgica. Within two weeks the skin nodules regressed. The patient’s creat-inine gradually increased from 0.6 to 3.3, TMP-Sulfa was decreased untilfinally stopped after 4 weeks of treatment, and minocycline was started.Creatinine returned back to baseline.Discussion: Nocardia infection usually occurs in those with cellular immu-nodeficiency, especially associated with transplantation, glucocorticoid therapy,lymphoma or AIDS. It can be localized or disseminated. The diagnosis can bechallenging and a high index of suspicion is required especially when initialtests are non-conclusive, in that case a suggestive clinical scenario shouldwarrant further testing. Sulfonamides are the drugs of choice for treatment.
138
CAN’T STOP THIS
Gillen J, Walker J. Texas Tech, Amarillo, TX.Case Report:Case Presentation: A 43 year old white male presented to the ED withseizures and hypoxemia. He had been a paraplegic since 2003, was bedridden, and subsequently developed multiple pressure sores and wound in-fections. He also had a history of pulmonary emboli (IVC filter placed),ESRD (on dialysis) and recurrent UTIs. His family cared for him in their home.He did not use ETOH or tobacco and his family history was non-contributory.On admission he was found to have bilateral pulmonary emboli and a
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 411
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

UTI due to Pseudomonas aeruginosa. Urine culture showed sensitivity toCeftaxidime, Gentamicin and Tobramycin but resistance to Aztreonam,Levofloxacin, and Meropenem. Tobramycin was initiated. Subsequent urineculture 3 days later grew P.aeruginosa that was resistant to all antibiotics.He chose home hospice care and died a week later.Discussion: This case is of interest because it illustrates the severity ofmulti-drug resistant organisms, and raises concern of previously susceptiblebacteria developing into ‘‘super bugs’’. P. aeruginosa is a gram negative ba-cillus that mainly infects the respiratory and urinary tracts as well as the skin.It is considered a nosocomial, opportunistic infection that can have graveoutcomes. The best course of treatment, however, is uncertain. Monother-apy with an anti-pseudomonal A-lactam can be used if the antibiotic chosenhas both a low risk of inducing resistance and high anti-pseudomonal activ-ity. If the infection is severe or resistance is suspected, however, many rec-ommend adding an aminoglycoside. Clinical outcomes between these twotreatment regimens are not significantly different, and studies have shownthat combination therapy does not reduce the emergence of resistant bacteria.
Incidence of multi-drug resistant P. aeruginosa has been increasing overthe past 20 years. There is little published data on the occurrence of theseorganisms among home care and hospice patients, but it is assumed they areacquired upon admissions to the hospital. Another concern involves the po-tential selection of these organisms through non-judicial use of antibiotics inthe home healthcare setting. The majority of home health care and hospicepatients are not cultured before receiving antibiotics and therefore sensitivi-ties are not obtained. In populations with recurrent infections, such as theone presented, this is particularly concerning.
139
THE SKIN GETS A SPANK FROM VANC: A CASE OFVANCOMYCIN INDUCED LINEAR IGA BULLOUSDERMATOSIS
Gruber M, Hooper D, Pate D, Hebert S, Engel LS. LSU Health SciencesCenter, New Orleans, LA.Case Report:Case: A 70 year old woman with a history of Interstitial Pulmonary fibro-sis secondary to rheumatoid arthritis, on chronic steroid therapy, discharged3 days prior after completing an eight day course of IV antibiotics withVancomycin, Ciprofloxacin, and Zosyn for HCAP, presented to the to theemergency department three days later with a prutitic and painful rash. Onexam, the patient was found to have multiple vesicular and flaccid bullouslesions over 27% of her body surface area on the trunk,upper extremities,face, and mucosa of the oropharynx. The initial differential included StevenJohnson Syndrome, Toxic epidermal necrolysis, disseminated varicella zos-ter, erythema multiforme, and autoimmune bullous disorders. Bedside punchbiopsy was performed and the patient underwent volume resuscitation byParkland formula standards, IV high dose steroids and IV acyclovir, placedon contact and droplet isolation in the ICU. The patient showed significantclinical improvement in less than 24 hours. Biopsy demonstrated separation ofepidermis from dermis with neutrophil accumulations within the resulting vesi-cle. The diagnosis was established as vancomycin induced Linear IgA BullousDermatosis (LABD) through further immunohistopathological examination.Discussion: Drug induced LABD is most commonly associated with van-comycin, although other drugs have been implicated. Diagnosis is typicallymade with direct immunoflourescence on a perilesional punch biopsy re-vealing a linear band of IgA at the dermoepidermal junction. In vancomycininduced LABD, IgA antibodies are produced that target 97kDa antigen and290kDa antigen, proteins that play a key role in dermal-epidermal adhesion.The reaction is not considered dose dependant and severity has not beenfound to correlate with serum vancomycin levels. Symptoms present within1-15 days of offending drug and resolve within 14 days of discontinuation.
140
PRIMARYCUTANEOUS MUCORMYCOSIS IN ACARPENTER
Ismaael T, Khasawneh F. Texas Tech Univ HSC, Amarillo, TX.Case Report:Introduction: Skin and skin structure infections are common entities thatinternists face. Bacteria are the most culprits, however, in certain patientpopulations and after specific exposures, other pathogens need to be considered.
Case: A 61yo diabetic male was admitted with progressive left knee cellulitisthat failed to respond to oral antibiotics. The patient was a carpenter whobruised his knee on the job 2 weeks prior. Despite broad spectrum intrave-nous antibiotics the infection progressed with the development of centralnecrosis. CT of the left leg demonstrated soft tissue swelling without abscessformation or knee effusion. Given the progressive inflammation and systemictoxicity, surgical debridement was performed. The surgical biopsy showedbroad, ribbon-shaped, aseptate fungal hyphae consistent with mucormycosis.The patient’s diabetes was better controlled and he was treated successfullywith liposomal amphotericin B, posaconazole and deferasirox for 6 weeksfollowed by 7 months of posaconazole.Discussion: Although it ranks third after sinus and pulmonary infections,cutaneous mucormycosis is the most common form of health care-associatedmucormycosis. Cutaneous mucormycosis results from direct innoculation ofspores into the skin and is classified as localized when it affects only the skinor subcutaneous tissues; deep if it invades muscles, tendons or bone; anddisseminated when it spreads to noncontiguous organs. A typical skin lesionconsists of a necrotic eschar with surrounding erythema and induration.Major risk factors for this infection include; uncontrolled diabetes mellitus,long-term corticosteroid use, organor stem cell transplantation, prolongedneutropenia, hematological malignancies, major trauma or burns, iron over-load states and deferoxamine use. The early diagnosis of mucormycosisrelies on having a high-index of suspicion based on appropriate riskstratification and recognition of clinical manifestations,f ollowed by or-dering CT or magnetic resonant imaging and tissue biopsies for culture andstaining. The successful treatment of this devastating infection hinges on theprompt surgical debridement and initiation of appropriate antifungal ther-apy as illustrated in our case. Reversal of risk factors, including reducingimmunosuppression if feasible, and better control of diabetes, is of para-mount importance.
141
ACUTE SENSINEURAL HEARING LOSS INSTREPTOCOCCUS AGALACTIAE (GROUP B)ENDOCARDITIS INFECTION AFTER ONE DOSEOF GENTAMYCIN
Jinenez A, Khan Y, Sachdeva B. LSU Health Center, Shreveport, LA.Case Report: The patient, a 45 year old African American male wasbrought to the Emergerncy Department after being found unresponsive andin respiratory distress. the patient, who had a history of hypertension, non-insulin dependant diabetes mellitus, end stage renal disease and medical non-complaince was noted to have a blood pressure of 234/84 mmHg. Urine drugscreen, acetaminophen, aspirin, alcohol and ammonia levels, CT scan of thehead, electrocardiogram and cardiac biomarkers were negative. The patienthad leukocytosis 14.22 k/uL, the patient was afebrile. Blood cultures weredrawn and the patient was started empirically on Vancomycin and pipercillin-tazobactam. Physical examination at the time of presentation was signifi-cant for systolic ejector mumur right upper sternal border. The urinalysis andurine cultures were negative, but blood cultures revealed Streptococcusagalactiae in all four culture samples; time to positivity was approximately8 hours. Vancomycin and pipercillin-tazobactam were stopped and Ceftazi-dime 2000 mg intravenous q 48hrs post dialysis was started. Transthoracicechocardiogram was done and revealed an ill defined echodensity on theaortic valve. Transesophagel echocardiogram was then performed and re-vealed a mobile echogenic mass in the right cusp of the aortic valve consis-tent with vegetation. Infectious diseases service was consulted and plan wasformulated to treat the patient with intravenous gentamicin and ceftriaxone.The patient was given gentamycin at a dose of 2 mg/kg a total dose of250 mg x 1 at 2pm post dialysis. Next afternoon on rounds his hearingwas noted to be decreased, by subsequent day (42 Hrs after the dose ofgentamycin) he had complete hearing loss.Audiology report:Left/Right ear: Profound sensorineural hearing loss from 250 Hz - 8000 Hz.Speech reception, patient did not respond to stimuli.
Gentamicin toxicity is is seen in less than 2% of patients, even formonth long courses of gentamicin. Factors affecting toxicity include: dose,potentiating medications, tainted drug?, genetic susceptibility, age. It is veryuncommon for gentamicin otototoxicity to develop with with less than1 week of treatment.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
412 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

142
PERSISTENT PNEUMONIA IN AN INFANT: APPEARANCESCAN BE DECEIVING
Joshi A, Balan A. OU Health Sciences Center, Oklahoma City, OK.Case Report: A 9 month old infant experienced a three month history ofrecurrent cough, tachypnea, fever, and persistent left upper lobe opacity onchest radiographs that failed to improve after various antibiotic regimens. Shewas otherwise well-appearing, and maintained appropriate weight gain. Afterreferral to a pulmonologist, computed tomography of the chest revealed leftupper lobe consolidation with bronchial obstruction, in addition to mediastinaland left hilar enlarged, necrotic lymph nodes. Since the radiographic differen-tial diagnosis included neoplasms and infected congenital cystic adenomatoidmalformation, she was referred to Pediatric Surgery at our hospital, where sheunderwent left upper lobectomy. Pathology demonstrated caseating granulomasin the lung tissue and lymph nodes, while AFB stain was positive. Epide-miologic history was negative for tuberculosis (TB) exposure risk, but tu-berculin skin test was positive and anti-TB treatment was started. Eventually,cultures grew Mycobacterium tuberculosis complex. Infant pulmonary TB isa difficult diagnosis to make in a non-endemic country, especially since itmay present with nonspecific symptoms. Even in endemic countries, it hasbeen mistaken for a congenital malformation. Our case stresses the impor-tance of evaluating for tuberculosis in infants with persistent pneumonia, as atimely, accurate diagnosis can prevent unnecessary invasive surgical diagnos-tic procedures, including lobectomy.
143
STRONGYLOIDES HYPERINFECTION SYNDROME:A FORGOTTEN DIFFERENTIAL OF BRONCHIAL ASTHMAAND ENTEROCOLITIS
Khalid H, Munn C, Winter A, Khan MU, Walters C, Kumar A, Sprabery L,Land M. University of Tennessee Health Science Center, Memphis, TN.Purpose of Study: Strongyloidiasis is not associated with significant symp-toms in most cases. However in some patients, especially those who are im-munocompromised, it may cause strongyloides hyperinfection syndrome(SHS), which has a high mortality rate.Methods Used: This is a case study of an asthmatic patient who presentedwith recurrent abdominal symptoms and was diagnosed with SHS.Summary of Results: A 31-year-old Hispanic female presented withworsening abdominal pain, nausea, vomiting and diarrhea for two days. Aweek ago, she had presented with similar symptoms, diagnosed as entero-colitis and treated with oral ibuprofen and metronidazole. She was diagnosedwith bronchial asthma 3 years ago that was getting progressively worse de-spite using albuterol, advair, montelukast and prednisone. She denied feveror other constitutional symptoms.
On physical examination she was of an average built, in apparent dis-tress. Her vitals included pulse 116/min, BP 110/60, respiratory rate 18/min.Abdominal exam revealed mild guarding and tenderness in right quadrants.Rest of her physical exam was unremarkable. Her blood counts showed aleukocytosis at 14000/mm3 with marked eosinophilia (24%). Rest of her labswas within normal limits. Abdominal CT scan revealed findings consistentwith enterocolitis involving ascending colon and adjacent ileum. Consider-ing her recurring symptoms and eosinophilia, a stool sample was sent for ovaand parasites. Meanwhile, she suffered an acute asthma exacerbation andhypoxic respiratory failure. Her CT thorax showed bilateral alveolar infil-trates. Later, results of her stool studies revealed the presence of Strongy-loides stercoralis larva and her blood cultures came positive for Escherichiacoli. Her steroid therapy was withdrawn and she was started on ivermec-tin and ceftrioxone. After a few days, her symptoms were completely resolvedand a repeat stool exam was negative for ova and parasites. She was dis-charged in a stable condition.Conclusions: Strongyloidiasis should be considered in patients with bron-chial asthma and gastro-enteritis, especially if they are immunocompro-mised. An early diagnosis and appropriate treatment can prevent and/ orcontrol SHS, which has high morbidity and mortality rates.
144
A CASE OF STREPTOCOCCAL TOXIC SHOCK SYNDROME
Mansfield J, Caruthers C, Pham K, Khan M, Happel K, Engel LS. LSUHealth Sciences Center, New Orleans, LA.Case Report:Case: A 76-year-old African-American woman with a history of penicillinallergy, ischemic cardiomyopathy (EF less than 20%), chronic kidney dis-ease, peripheral vascular disease status post left SFA stents placed threeweeks prior to presentation with ischemic ulcers on the toes of her left footpresented to the emergency department with shortness of breath, orthopnea,fatigue, claudication and bilateral lower extremity edema. On presentationthe patient was afebrile. Her BNP was elevated, WBC of 12.4 and bands of13%. She was admitted for treatment of heart failure exacerbation. On hersecond day in the hospital, the primary team noticed some new hemorrhagicbulla on her right popliteal fossa which seemed to be progressing. Her men-tal status deteriorated and she was transferred to the MICU with empiricciprofloxacin, vancomycin, clindamycin, and tigecycline. Repeat labs demon-strated a decreased WBC of 2.6 with 13% bands, and the early stages of he-patic and renal failure, as well as a new onset coagulopathy. The bullous lesionsexpanded and spread to the patient’s thigh, suprapubic area, and eventuallyto her right upper extremity. Several of the bullae ruptured with subsequentdesquamation of her skin. She became unresponsive, hypotensive despitepresser support, pulseless, and had to be resuscitated with epinephrine andchest compressions and intubation. Intravenous immunoglobulin was admin-istered after preliminary blood cultures grew a Gram-positive cocci in chains.Her family decided that her ultimate wishes were to be a DNR status. Soonafter this decision, the patient became bradycardic and passed away. Her finalblood cultures and bullae aspiration culture revealed Group A streptococcus(GAS), and the final diagnosis was established to be streptococcal toxic shocksyndrome.Discussion: Streptococcal toxic shock syndrome (STSS) is made with theclinical findings of hypotension plus multi-organ failure - including liverinvolvement, renal impairment, coagulopathy, ARDS, rash, and soft-tissuenecrosis - and subsequent isolation of GAS from a normally sterile site. Thetreatment of choice includes penicillin, clindamycin, and supportive therapy.New studies show some evidence for the use of IVIG to lower the mortalityassociated with STSS.
145
FEVER IN AN INTERNATIONAL TRAVELER
Menendez D, Chandranesan AS, Capraro GA, King JW. LSU HealthSciences Center, Shreveport, LA.Case Report: A 23 year-old Caucasian woman presented to our emergencydepartment (ED) with complaints of fever and headache for five days. Hertravel history included a two-week trip to Haiti after which she returned to theUnited States for a month before going on a 30-day trip to Ghana. Beforeleaving for Haiti she began taking doxycycline for malaria prophylaxis andcontinued through the first 25 of 30 days in Ghana. Ten days after returningfrom Ghana she developed fever, headache and myalgias. Initially she wasseen in an urgent care clinic where she was started on atovaquone - proguanilfor suspected malaria. Because of continued headache and fevers she pre-sented to our ED the following day. Initially, meningitis was considered andafter a negative CTof the head, a lumbar puncture was done which revealed anormal opening pressure, glucose of 67 mg/dl, protein of 20 mg/dl and nu-cleated cell count of 0. Peripheral blood smears from the outside facility withadditional thick and thin smears from our hospital were consistent with Plas-modium falciparum. Cultures of blood and urine were negative. On the secondday of hospitalization the patient developed visual hallucinations and con-fusion. Blood smears from admission showed a parasitemia of 5%. Becauseof CNS symptoms consistent with cerebral malaria, the patient was trans-ferred to the ICU. Following a discussion with the Centers of Disease Control(CDC), she was started on intravenous quinidine gluconate 400mg loadingdose with maintenance at 0.0125 mg/kg/min and clindamycin 600 mg load-ing dose with 300mg every 8 hours for maintenance. Repeat blood smearsshowed a parasitemia of G0.1%. She was transferred out of ICU to the floorwith oral quinine plus clindamycin and discharged home in stable conditionafter 8 days of anti-malarial therapy. This case emphasizes the importanceof inclusion of malaria in the differential diagnosis of fever, headache and
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 413
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

recent foreign travel. When malaria is considered, prompt diagnosis requiresrapid evaluation of peripheral blood smears. Early identification of a highparasite burden with severe disease should prompt admission to the ICU forintravenous anti-malarial therapy and close monitoring. Compliance with che-moprophylaxis is essential in preventing the disease.
146
THE HIPS HAVE IT
Metoyer C, Stephenson LR, Thomas WH, Hodges L, Bocchini J. LSU HealthShreveport, Shreveport, LA.Case Report: A 12- year old male presented to our institution complainingof fever and hip pain. His past medical history is significant for congenitalHIV. For the last three years, he was lost to follow up in our infectious diseaseclinic. He presented twoweeks prior, with right hip pain, at an outside facility.He was diagnosed with a hip strain, and given a steroid injection into his hip.At presentation, mom says that his hip pain had worsened, and he had becomefebrile. His initial workup at the outside facility including blood, CSF, and plainfilms was negative. On arrival to our facility, he was found to be exquisitelytender to palpation of the right hip, as well as on external rotation. He had noredness, warmth, or swelling of the joint. An MRI was suggestive of earlyosteomyelitis of the right hip. Infectious disease was consulted, and lab workincluding CBC, Blood culture, and HIV genotype, Viral Load, and CD4 countwere performed. Mom initially reported compliance with HAART therapy, buthis CD4 count was 10 per mm3. At that time, Vancomycin and Clindamycinwere initiated for broad spectrum coverage, including MRSA. The patient’spain abated over one week’s time, with aggressive antibiotics and pain man-agement. A repeat MRI one week after initiation of therapy showed littlechange. The patient’s blood cultures remained negative throughout his stay.The patient had a PICC line placed in anticipation of long-term antibiotictherapy. The patient was intermittently febrile throughout admission, withthe only source found being a single-port colonization of his PICC with Staphhominis. After the patient’s HIV genotype returned, he was started on Stra-bild, a new single-pill HAART therapy. Subsequent lab draws were signif-icant for pancytopenia, which was attributed to his HIV status. A manualdifferential was performed, which showed 31% blast forms. His peripheralsmear was consistent with Precursor B cell acute lymphoblastic leukemia,which has only been reported once in the literature in an HIV-infected pa-tient. A bone marrow biopsy confirmed the diagnosis. In addition, he wasfound to have a gain of the MLL gene, and a loss of the TEL gene, poorprognostic indicators. Pediatric Oncology was consulted and further workupis in process.
147
I AM BREATHING OK BUT MY TONGUE IS SORE? A CASEOF LINEZOLID-INDUCED BLACK HAIRY TONGUE
Moti D, Zorek J, Islam A, Khasawneh F. Texas Tech Univ Health ScienceCenter, Amarillo, TX.Case Report:Introduction: Tongue discoloration is a rare complaint. The problem iscommonly drug-induced and is self-limited in most cases. Linezolid has beenlately reported to cause an extreme form of tongue discoloration, black hairytongue (BHT).Case presentation: A 56-year-old male was admitted with community-acquired pneumonia that failed to respond to levofloxacin 750 mg daily. Hewas started on linezolid and meropenem and was subsequently dischargedhome on oral linezolid 600 mg every 12 hours and intravenous ertapenem 1 gdaily. On a follow up clinic visit, day 14 of linezolid therapy, his pneumo-nia symptoms had resolved but he complained of dysgeusia and his tongueexam was consistent with BHT. After he finished his antibiotic course, hiscomplaints resolved with regular tongue brushing.Discussion: Black hairy tongue is a self-limiting disorder characterized byabnormal hypertrophy and elongation of filiform papillae on the surface ofthe tongue. BHT is usually asymptomatic though occasionally patients maycomplain of tickling or burning of the tongue, nausea, halitosis, and dys-geusia. The color black has been used to characterize this condition histori-cally; however, brown, yellow and green discolorations have been reported.Several factors have been implicated in causing and/or aggravating BHT;these include smoking or chewing tobacco, drinking alcohol, poor oral
hygiene, smoking crack cocaine or other street drugs, using peroxide con-taining mouthwash, radiation therapy, trigeminal neuralgia, using drugs thatcause xerostomia like anticholenergics, antihypertensives and antidepressants,and antibiotics such as tetracyclines and penicillins.
The treatment of this condition is supportive and includes stopping theoffending drug while performing meticulous mouth hygiene. Health careprofessionals should be aware of the possibility of linezolid-induced blackhairy tongue. Thorough history for other possible contributing factors shouldbe obtained. Patients on linezolid should be counseled to perform good oralhygiene.
148
SOMETHING CRYPTIC ABOUT CRYPTOCOCCUS
Panchal GB, Guha B, Patel P. East Tennessee State University,Jonesborough, TN.Case Report: A 75 year old male was admitted with generalized mal-aise, weakness. He was on prednisone and cyclophosphamide for necrotizingcrescentric glomerulonephritis. He denied any other symptoms. On exami-nation he was afebrile with stable hemodynamics. He did have some leu-kocytosis with predominant lymphocytosis and worsening kidney function.Pan cultures were done. Chest X-ray showed bilateral pulmonary infiltrates.Patient was started on empiric antibiotics. His blood cultures grew Crypto-coccus neoformans and intravenous Fluconazole was started due to renalinsufficiency. He underwent lumbar puncture with normal opening pressure,Cryptococcal titer 1:4 and negative culture. Due to persistent positive blood,he was switched to combination of Amphotericin B and Flucytosine. Bloodcultures were negative within 2 weeks of the treatment and he was laterswitched to long term Fluconazole. He is in remission now.***DISCUSSION***C. neoformans is opportunistic encapsulated yeast, acquired by inhalationof aerosolized infectious particles. Cryptococcosis occurs predominantlyin immunocompromised hosts such as those with, hematological malignan-cies, transplant recipients on immunosuppressants, patients on chronic ste-roid treatment and advanced HIV.Cryptococcosis is defined as isolation of organism from blood, sterile bodyfluids or tissue except lungs. CNS, disseminated disease and lungs are themost common involved. Meningoencephalitis, cranial nerve palsies, papille-dema are few of the CNS manifestations. Pulmonary cryptococcosis manifestsas fever, cough and dense non-homogenous lesions. The organism gives adistinct appearance on Indian ink preparation. Detection of cryptococcalantigen in CSF and blood as well as culture helps in diagnosis. CSF evalu-ation is important in all patients who are diagnosed with cryptococcosis inorder to guide treatment.
In case of meningitis, Amphotericin B with Flucytosine can be given asan induction treatment followed by oral fluconazole. Pulmonary involvementalone can be managed by oral fluconazole. HIV patients may require lifelongfluconazole suppressive therapy. The disease in invariably fatal if left un-treated and even with treatment carries high rate of morbidity and mortality.This makes it important to consider the diagnosis in susceptible individuals.
149
A NOT SO SIMPLE UTI
Patel J, Lacour A, Engel LS, Mohan M. LSU Health Sciences Center, NewOrleans, LA.Case Report:Case: A 49-year-old woman with a history of kidney stones and COPD wasadmitted to the hospital with an unrelieved headache. One month prior toadmission she was seen at an outlying facility secondary to urinary symptomsand flank pain. She was diagnosed with kidney stones and hydronephrosis,urine cultures were drawn which showed mixed flora and she was sent homeon ciprofloxacin. She worsened over the next few days and was admitted fromthe urology clinic for intravenous antibiotics and placement of stents forpyelonephritis. Urine cultures, drawn prior to discharge, were negative. Shewas treated with gentamicin and sent home with ciprofloxacin and clindamy-cin. She returned for successful laser ablation of the kidney stone, but 2 weekslater, she presented to the hospital complaining of a headache. A cat scanshowed a possible subarachnoid hemorrhage and she was admitted by neu-rosurgery. A repeat head CT showed a stable subarachnoid hemorrhage.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
414 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Following discharge, she re-presented 3 days later with persistent headache.A lumbar puncture was done and Gram negative rods and elevated whiteblood cell count were seen in the cerebrospinal fluid examination (CSF). CSFand blood cultures grew E. coli resistant to ciprofloxacin and sensitive toaztreonam. After switching to appropriate antibiotics she improved and wastransferred to the floor. Repeat blood and CSF cultures demonstrated clear-ance. Approximately one week after her admission, she became more le-thargic with a decreased level of consciousness; a stat CT demonstrated a newsubarachnoid hemorrhage with midline shift. Neurosurgery emergently tookher for hemicraniectomy however she never recovered and the family with-drew care.Discussion: E. coli is an uncommon pathogen for adult meningitis (G3.6%).E. coli meningitis occurs most frequently after accidental or surgical traumato the head or spine and is much less common in patient with septicemia.Despite adequate treatment with antibiotics, the sequelae of changes frommeningitis can cause significant morbidity and has mortality rate of 50 to90%. Although E. coli is an infrequent cause of meningitis in adults, this bac-terium should still be considered, particularly in patients who have recentlyundergone urological procedures.
150
LEMIERRE’S SYNDROME: A POTENTIALLY FATALDISEASE
Pepper DJ, Harris A. UMMC, Jackson, MS.Purpose of Study: Lemierre’s syndrome is a rare devastating form ofthrombophlebitis caused by Fusobacteria. This thrombophlebitic nidus causeshematologic seeding of bacteria. We present a case of a young adult whomanifested with this potentially fatal disease.Methods Used: Case ReportSummary of Results: A 28-year-old African American man presented toour emergency department with a 3-day history of an altered mental stateand increased work of breathing. Physical exam showed a hyperemic oro-pharynx, a firm left submandibular gland with overlying ecchymosis, anddecreased breath sounds and tactile fremitus over the right lower lobe of thelung. His CXR showed a hazy opacification of the right base, while labora-tory tests revealed leukocytosis, thrombocytopenia, acute kidney injury, andelevated transaminases. He was initially treated for severe sepsis with broad-spectrum antibiotics but failed to improve. A subsequent CT chest showedmultiple septic emboli within his lungs as well as two loculated pleuraleffusions. Thoracentesis confirmed culture negative emypemas and Fuso-bacterium nucleatum grew on blood cultures. Imaging of his neck and faceshowed multifocal abscesses and thrombophlebitis of the left jugular vein -consistent with Lemierre’s syndrome. The patient received appropriate anti-coagulation and antibiotics with subsequent clinical improvement.Conclusions: With the advent of antibiotics, mortality due to Lemierre’ssyndrome has decreased from 90% to 5%. However, survival with Lemierre’ssyndrome depends on early recognition and appropriate treatment as depictedin our patient. Physicians need to be cognizant of this syndrome, particularlywhen pharyngitis does not respond to initial treatment.
151
WEST NILE VIRUS ENCEPHALITIS
Prabhakar A, Coleman R, Kemp N, Engel LS, DeBoisblanc B. LSU HealthSciences Center, New Orleans, LA.Case Report:Introduction: The prevalence of West Nile virus (WNV) in the continentalUnited States has greatly increased. Manifestations of the virus range fromasymptomatic carriers to rapidly progressive neurological and muscular decline.Case: A 40 year old male with no past medical history presented to a ruralemergency department with a 3 day history of acute onset headache, severeneck pain, fever, drowsiness, weakness, and poor PO intake. A lumbar punc-ture was performed and treatment with vancomycin, ceftriaxone, and acy-clovir was begun. Initial cerebrospinal fluid (CSF) studies were significantfor an elevated WBC with predominance of segmented neutrophils, elevatedprotein, and normal glucose. CSF was also sent for West Nile and EBV studies.The patient was subsequently transferred to another facility for further neu-rological evaluation. Notable physical exam findings upon presentation werefever of 102 oF, normal sensation throughout, and decreased upper extrem-ity motor strength bilaterally. Magnetic resonance imaging (MRI) of thecervical and thoracic spine was significant for inflammatory myelopathy.MRI of brain was unremarkable. The patient’s symptoms progressivelyworsened over the course of 2 days with continued neuromuscular declineand weakness coupled with symmetric loss of reflexes. The patient was sub-sequently intubated secondary to impending respiratory failure. EMG findingswere consistent with Guillain-Barre syndrome Miller Fisher variant. The pa-tient was initiated on IVIG treatment. Eight days after his initial presentation,his serum IgM was found to be positive for WNV. The patient had a long andprotracted hospital course with particular difficulty being weaned from theventilator. One and a half months after his initial presentation, the patient wasdischarged with a tracheotomy to an outside center to continue his neuro-muscular rehabilitation.Discussion: West Nile virus is a single stranded RNA virus that was firstdocumented in the United States in 1999. Neuroinvasive disease is extremelyrare among individuals less than 65 years old. This case illustrates that thereremains a certain amount of unpredictability with WNV disease progressionand severity and it is important to recognize WNV in a patient’s differentialdiagnosis, particularly in areas with higher prevalence.
152
TUNGIASIS IN ATRAVELER RETURNING FROM TANZANIA
Rean K, Waller J. Texas Tech University Health Sciences Center, Amarillo, TX.Case Report: After a recent trip to Tanzania, a 54 year-old male presentedwith a chief complaint of black dots coming out of his toes. Physical ex-amination revealed small white nodules surrounding a black insect on each ofthe fifth toes bilaterally. What appeared to be eggs and fecal strands werepresent at the base of the nail bed. The insects were surgically excised and thesurrounding tissue curretted. Examination of the excised material showed asmall black flea surrounded by a web of white mucoid eggs. This presenta-tion was highly suggestive of tungiasis so a histological examination was notperformed.Discussion: Most cases of tungiasis seen in the United States appear inpeople who have recently travelled to an endemic area: South America, theCaribbean, or sub-Saharan Africa. Tungiasis is caused by Tunga penetrans, asmall flea that resides in warm, sandy soils and is often found around sta-bles and pigsties. Poverty-stricken locations are the most affected, because ofpoor sanitation. Other common findings include lack of footwear, homeswithout solid floors, and animal hosts, including pigs, dogs, and cats, insidethese homes. Clinical manifestations of tungiasis correspond to the phase ofthe flea’s lifecycle at presentation. First, a pregnant flea penetrates the epider-mis, then its midsection rapidly hypertrophies so the affected skin stretchesto resemble a white halo surrounding a black dot. The flea emits feces andeggs, and if seen, these are virtually pathognomonic for tungiasis. Associ-ated symptoms include erythema, warmth, pruritus, and pain. After the fleadies a brownish-black crust appears, and a divot may remain for months.Because these fleas reside in sand, the majority of lesions appear on the feet. Thediagnosis of tungiasis is clinical and treatment requires sterile surgicalexcision followed by a topical antibiotic. The infestation is often self-limitedin returning travelers; however, devastating consequences can develop in
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 415
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

individuals of endemic areas, including necrosis and foot deformation. Pre-vention of infestation follows community-wide measures that improve san-itation, pave concrete floors, confine loose animals, and spray insecticideindoors. Patients traveling to endemic regions of tungiasis should be advisedto wear protective shoes and check their feet for fleas.
153
PROTECTIVE EFFECT OF ANGIOTENSIN CONVERTINGENZYME INHIBITOR THERAPY IN PATIENTS WITH HIVAND PROTEINURIA
Rosales CB1, Khan MF2, Shakhashiro A2, Frontini M2, Clark R2. 1LSUHSCSchool of Public Health, New Orleans, LA and 2LSUHSC School ofMedicine, New Orleans, LA.Purpose of Study: To determine the protective effect of angiotensin con-verting enzyme (ACE) inhibitor therapy in patients with HIVand proteinurea,a retrospective review of a large ambulatory clinic population with HIV basedin New Orleans was performed.Methods Used: Patients were eligible for the study if they were 9 18 andhad at least 2 valid urinalyses between 7/06 and 6/08. Urinalyses showingblood (defined 9 10 red blood cells per high power field) and or pyuria (de-fined as 9 10 WBC per high power field) were considered invalid. Patientsmeeting the study criteria were followed up through 6/11 for outcomes ofincident opportunistic processes, hospitalization, and all-cause mortality.Summary of Results: Of the 140 patients having at least 2 valid urinaly-ses, 41 (29%) had 92 tests, 43 (31%) had only 1, and 56 (40%) had nourinalyses demonstrating proteinuria at levels of 9 25 ng/ml. Characteristicsof the cohort showed 38 (27%) were female and 109 (78%) were AfricanAmerican. Median baseline age, CD4 cell count, and HIV RNA copies were45 years, 154 cells /mm3 and 63,900 copies/mL, respectively. Of the 140patients, 39 (28%) were on an ACE inhibitor.Bivariate analysis showed that ever proteinuria was not associatedwith sex, race, age, substance use, antiretroviral therapy, body mass index,systolic or diastolic blood pressure, ACE therapy, or selected medical con-ditions (including diabetes, hypertension, renal disease, hepatitis). Protein-uria (levels 9 25mg/dl on 9 1 urinalysis) was associated with ever having aCD4 cell count G 200 (p=0.03), a detectable HIV RNA level 9400 copies(p=0.03), or a baseline albumin level of G 3.5 mg/dl.On bivariate analyses proteinuria was also significantly associated withhospitalization or death, but only in patients not on an ACE inhibitor. Onmultivariate analyses the association between proteinuria and hospitaliza-tion remained significant after controlling for confounding factors (includ-ing sex, race, CD4 count, HIV RNA level, creatinine and baseline albumin).Conclusions: Low level proteinuria was a predictor for selected adverseoutcomes among patients not on an ACE inhibitor. Our results suggest thatpatients with HIV and any proteinuria, even episodic low levels, may benefitfrom ACE therapy.
154
A SEVERE CASE OF STAPHYLOCOCCAL SCALDED SKINSYNDROME IN A CHILD
Sicard C, Bocchini J. LSU Health Shreveport, Shreveport, LA.Case Report: Staphyloccocal scalded skin syndrome (SSSS) was once acommon disorder, frequently associated with outbreaks in hospital nurseries.In recent years, SSSS is rarely seen in developed countries. SSSS most com-mon often occurs in infants and its severity varies widely from being localizedto the site of infection to a severe exfoliation affecting almost the entire body.A 5 year old female was transfered to the our facility from an outside hospitalwith skin desquamation. 2 days prior she was in her usual state of health andawoke with clear rhinorrhea, fatigue, blisters on her forehead, and skin des-quamation of her nose. She denied taking medications, prolonged sun ex-posure, contact with animals, or recent travel. She had one sick contact atsummer camp with a staphylococcal skin infection. Upon arrival, her phys-ical exam was remarkable for widespread skin desquamation involving thetrunk and face with sparing of her extremities. Dependent areas of the bodywere more affected. A positive Nikolsky’s sign was elicited. She was startedon vancomycin 80 mg/kg/day and clindamycin 40 mg/kg/day. Blood andurine cultures were negative. Skin cultures grew S. epidermidis., CMP, CBCwith differential, and CRP were unremarkable. A skin biopsy showed sub-
corneal splitting with acantholysis consistent with SSSS. Maintenance fluidsand a morphine PCAwere started. The Burn Service was consulted for skincare. They recommended Acticoat dressings to the lesions, and followed thepatient for dressing changes. Over the next few days the desquamationworsened to include her extremities before it began healing. She was dis-charged home after a 6 day hospital stay with significant skin healing.Although now seen infrequently, SSSS should be considered in the differ-ential diagnosis of infants and children with an acute onset of a desquamatingskin disorder. The gold standard for diagnosis is a skin biopsy showingsubcorneal splitting. Treatment consists of monitoring the patient’s fluidstatus closely, providing a skin barrier to prevent superimposed infection,and symptomatic relief.
155
OPPORTUNISTIC INFECTIONS: YOU CAN’T HAVE JUST ONE
Smith MM, Ruiz M, Engel LS, Lopez FA. LSU Health Sciences Center, NewOrleans, LA.Case Report:Introduction: Antiretroviral therapy has greatly reduced the incidence ofopportunistic infections (OIs). However, patients who lack access to care mygo undiagnosed until the development of AIDS defining OIs.Case: A 54 year old homeless man with no significant past medical historypresented to the emergency department complaining of ‘sticking’ non radi-ating, 7/10 left side chest pain that occured every day for approx. 1-5 minutesand productive cough with green sputum. He denied fever, night sweats, orweight loss. He had a significant history of tobacco and crack cocaine use.Physical exam revealed a left sided T11 dermatomal vesicular rash withexcoriations diagnostic for zoster. He had thrush as evidenced by whiteplaques on his oropharynx and tongue that were easily lifted. He was startedon intravenous acyclovir and oral fluconazole, and put in respiratory isola-tion secondary to severe cough with copious productive sputum. A rapid HIVtest administered in the emergency department was positive and reflex test-ing confirmed the result. CD4 count was 27 cells/mm3. A chest radiographwas unremarkable however computed tomography scans revealed a left lowerlobe cavitary lesion. Pulmonary was consulted for bronchoscopy, howeverone sputum sample was found to have 4+ acid fast bacilli (AFB). The patientwas started on RIPE therapy plus vitamin B6. Serum cryptococcal Ag waspositive but the patient refused a lumbar puncture: treatment with liposomalamphotericin B was initiated. Mycobacterium kansasii was identified as theAFB in the sputum sample and the pyrazinamide was discontinued. Hiszoster resolved and patient was discharged after 14 days of liposomalAmphotericin B therapy with continued fluconazole therapy and HIV out-patient clinic referral.Discussion: Opportunistic infections, localized or systemic, can occur any-where on the body. Susceptibility to opportunistic infections correlates withthe CD4 count; more than 30% of OIs occur with a CD4 count less than200 cells/mm3. Furthermore, the presence of multiple opportunistic infec-tions is not usual with advanced AIDS and it is important to investigate fullyto ensure proper treatment of our patients. Further reduction in the incidenceof OIs can be established through vigorous HIV screening.
156
LUMBOSACRAL OSTEOMYELITIS CAUSED BY CANDIDAKRUSEI
Stal D1, Shah CJ1,3, Arya M2,3, Weatherhead J1, Yasukawa K2. 1BaylorCollege of Medicine, Houston, TX; 2Baylor College of Medicine, Houston,TX and 3Ben Taub General Hospital, Houston, TX.Case Report: Learning Objectives:
1. Candida species are an important cause of vertebral osteomyelitisin high risk individuals. Risk factors include being immunocompro-mised, having indwelling central venous catheters, recently receivedbroad-spectrum antibiotics, and injection drug use.
2. Consider adding antifungal medications when traditional broad spec-trum antibiotics are not showing improvement in clinical symptoms forvertebral osteomyelitis.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
416 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

3. Among the Candida species, Candida krusei is a rare cause of ver-tebral osteomyelitis. This organism is notably resistant to fluconazole.
Case Presentation: A 54 year old African American female with a historyof hypertension and intravenous drug abuse presented to the emergencyroom with a two month history of lower back pain and new onset right lowerleg radicular pain and paresthesia. The patient had an emergent lumbosacralMRI revealing inflammatory changes at L4-L5 and L5-S1 worrisome for os-teomyelitis and discitis. The patient was immediately admitted and underwenta right L5 hemilaminectomy and right L5-S1 foraminotomy with microdis-cectomy and disk biopsy the following day and started on empiric antibioticsconsisting of Vancomycin and Ceftriaxone. Post-operatively, the patient waspersistently tachycardic (130-140s) and spiking intermittent fevers despitethe above antibiotics and a stable white blood cell count. On day five, thesurgical cultures came back positive for Candida Krusei. Review of the pub-lished literature revealed only 3 cases of Candida Krusei vertebral osteo-myelitis. The patient was started on IV Micafungin 100 mg QD and oralVoriconazole 200 mg BID. Soon after starting these antifungals, her tachy-cardia and fevers resolved. In addition, her right lower leg radicular pain andparesthesias started to improve. Blood fungal cultures were negative, and oph-thalmic exam was negative for evidence of Candida endophthalmitis. It wassuspected that the patient contracted C. Krusei through contaminated intra-venous needles, as her last drug use was six months prior to surgery.
157
WEST NILE VIRUS ENCEPHALITIS IN AN ADOLESCENT
Stephenson LR, Thomas W, Rhodes L, Hodges L, Bocchini J. LSU HealthShreveport, Shreveport, LA.Case Report: West Nile Virus meningoencephalitis in children can presentitself as a varied collection of non-specific clinical signs and symptoms. Ahigh index of suspicion, along with clinical correlation, is necessary toprompt serologic studies.A 15 year old female who presented to the ambulatory clinic complaining ofweakness of 5 days duration. The patient had subjective fever one week priorto presentation, which prompted a visit to an outside ER. She was subsequentlydiagnosed with a simple URI. The fever subsided, and the patient remainedafebrile for the duration of her illness. At the cessation of her fever, she begancomplaining of proximal leg pain and weakness. Her pain was such that sherequired a wheelchair for mobility. On initial clinical exam, she had diffusepain to palpation and manipulation of bilateral hips, The remainder of herneurologic exam was within normal limits, including negative Kernig’s andBrudzinski’s signs. Infectious disease and Neurology were consulted. Subse-quently, an MRI of the Brain and spine, as well as an LP, were performed.
The LP Results are listed in the table.The MRI showed hyperintensities of the meninges overlying the
cerebellum, as well as enhancement of the cauda equina. The MRI resultsalong with the results of her lumbar puncture were highly suggestive of viralmeningitis. Secondary to the patient’s apparent neuroleptic pain, Neurontinwas started and titrated to effect. After one week of parenteral and oral painmanagement along with physical therapy, the patient’s West Nile from bloodand CSF were consistent with West Nile Viral Infection. At discharge, thepatient still required significant assistnace with ambulation, and aggressiveoutpatient physical therapy was arranged.
This patient represents a classic case of West Nile Encephalitis, with non-specific clinical findings and devastating neurologic sequelae.
158
STAPHYLOCOCCAL PARASPINAL ABSCESS COMPLICATEDBY EPIDURAL ABSCESS AND BACTERIAL MENINGITIS
Swe EK, Pepper D, Pressler J. University of Mississippi Medical Center,Jackson, MS.
Purpose of Study: Staphylococcus aureus is responsible for less than 5%of adult meningitis and is typically associated with penetrating head traumaor neurosurgery. Most paraspinal abscess and epidural abscess are causedby intravenous drug use, HIV infection, trauma or immunosuppression. Herewe report a case of S. aureus paraspinal abscess complicated by epidural ab-scess and subsequent bacterial meningitis.Methods Used: Case Report.Summary of Results: Our patient, a 39 year old Caucasian male knownwith hypertension and chronic alcohol abuse, presented to the emergency de-partment with high fever (104.5F), diaphoresis and altered mental status. Hewas obtunded and no collateral history could be obtained from any fam-ily members. As he had a significant history of alcoholism, was obtunded andmet criteria for severe sepsis, he was admitted to the intensive care unit. Hereceived volume resuscitation and empiric intravenous antibiotics while await-ing his culture results. His blood and cerebrospinal fluid subsequently culturedmethicillin sensitive S. aureus. Collateral information obtained from his fam-ily at this time suggested a chronic history of severe lower back pain, which wasnot relieved by pain medications or oral steroids. An MRI of his lumber,thoracic and cervical spine revealed a large multi-loculated paraspinal ab-scess measuring 9x6x12 cm (from L1-5 level) in his left psoas, left iliop-soas and left posterior paraspinal musculature. A small epidural abscess(1.3x0.5x2.0 cm) was noted at the level of L2-3. The paraspinal abscess wasdrained and the fluid cultured methicillin sensitive S. aureus. The patientreceived intravenous vancomycin and ceftriaxone during his hospitalisa-tion. Subsequent history and laboratory testing revealed that he was HIVuninfected, his TB skin test was negative, and he had no prior history of backsurgery.Conclusions: Bacterial meningitis should always be considered when apatient presents with an altered mental state and fever, especially when col-lateral information is not readily available. Spinal cord or paraspinal ab-scess should be investigated in cases of S. aureus meningitis, particularly witha history of prior steroid use and in the absence of prior head trauma orneurosurgery.
159
FIRST CASE OF HAFNIA ALVEI UROSEPSIS IN THEUNITED STATES
Touchan J, Bellardini J, Maharaj J, Alexandraki I. University of Florida-Jacksonville, Jacksonville, FL.Case Report: We describe the first case of septic shock due to urinary tractinfection caused by Hafnia alvei in the United States. A 59-year-old womanpresented with a five day history of left lower extremity swelling. She had ahistory of Crohn’s disease complicated by small bowel resection and multi-ple fistula repairs, and recurrent deep vein thrombosis and pulmonary em-bolism. In the emergency department, venous Doppler showed DVT of theLLE and the patient was admitted for anticoagulation therapy. On day 8 ofhospitalization, the patient developed tachypnea, hypoxia, tachycardia, andhypotension refractory to fluid resuscitation. The patient was transferred tothe Intensive Care Unit as she required vasopressors. Her white blood cellcount was 21,800 with a left shift. The patient was started on meropenem andvancomycin empirically, after blood and urine cultures were sent. The pa-tient’s urine culture grew H. alvei 9100,000 colonies/ml, resistant to ampi-cillin and cefazolin but sensitive to ceftriaxone. Blood cultures remainednegative. The antibiotics were changed to ceftriaxone. The patient’s conditionimproved after 24 hours. She was weaned off vasopressors. The patient’sseptic shock was attributed to her urinary tract infection caused by H. alvei.H. alvei is a member of the Enterobacteriaceae family that rarely affects hu-mans. Only 12 cases of infections caused by H. alvei have been reported inthe US with only one case of pyelonephritis. Our case is unique, being thefirst case of H. alvei urinary tract infection leading to septic shock. Hafniacauses a variety of systemic infections, including septicemia and pneumo-nia. Our patient’s presentation was consistent with previous literature thatshows higher rates of H. alvei infection in patients with Crohn’s disease,previous abdominal surgery and female sex. Hafniae are typically resistant topenicillin and their susceptibility to tetracyclines and cephalosporins is variable.Most reported H. alvei cases are polymicrobial; monomicrobial infectionsare uncommon. Conclusion: Although H. alvei infections are rare in the US,clinicians should have a high level of suspicion due to their potential mor-bidity in the susceptible host.
CSF Studies
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 417
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

160
ODD STATE OF MIND: AEROBIC ACTINOMYCETECULTURED FROM AN IMMUNOCOMPROMISED PATIENT
Yates R1, Burton M2,1, Abdo A2,1. 1University of Mississippi MedicalCenter, Jackson, MS and 2G.V. (Sonny) Montgomery Veterans Affairs MedicalCenter, Jackson, MS.Case Report: The aerobic actinomycetes are a diverse group of soil-inhabiting bacteria. Found worldwide, they can cause significant morbid-ity and mortality in immunocompromised patients. A 48-year-old AfricanAmerican man with HIV/AIDS (absolute CD4 lymphocyte count 59 cells/uL),end-stage renal disease, and cirrhosis presented to the emergency departmentwith mental status changes and headache. He was afebrile and hemody-namically stable. Physical exam revealed lack of meningismus, asterixis, andfocal neurological deficits. He had pancytopenia and hypoalbuminemia con-sistent with advanced liver disease. Computed tomography (CT) scan of thehead without intravenous (IV) contrast showed no acute abnormality. Lumbarpuncture was unremarkable. Cerebrospinal fluid (CSF) cultures revealed nogrowth at 48 hours, and serum cryptococcal antigen was negative. On day 2,magnetic resonance imaging (MRI) of the head without IV contrast revealeda 1.5 cm focus in the right parietal lobe. The patient developed fever (101.2 -F)on day 3 and received broad spectrum antibiotics and fluconazole. Mentalstatus improved, and antimicrobials were stopped on day 8. He was dis-charged home on day 10 but returned 48 hours later with confusion and fever(102.9 -F). Labs and lumbar puncture were repeated and essentially un-changed. He was again placed on broad spectrum antimicrobials. SerumToxoplasma serology returned positive for immunoglobulin G (IgG). Hecontinued to spike fevers, and brain biopsy was considered until aerobicactinomycetes were detected from his initial CSF cultures by high performanceliquid chromatography. The patient was prescribed a prolonged course ofceftriaxone and was discharged two days later to a long term acute carefacility. Serum Histoplasma antigen returned positive after his discharge, butthe patient had elected to forgo treatment and assume hospice care. Diagnosisof CNS disease in advanced HIV/AIDS can be challenging. While Toxo-plasma encephalitis, cryptococcal meningitis, and CNS lymphoma are pri-mary considerations, rarer infections sometimes occur and should beincluded in the differential. This case also demonstrates that multiple etiol-ogies often coexist in the immunosuppressed individual.
161
POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROMEIN AN HIV POSITIVE PATIENT
Hutchins K, delahoussaye-Shields R, Graugnard W, Mezu-Patel N, Engel LS,Hull A. LSU Health Sciences Center, New Orleans, LA.Case Report:Introduction: HIV is associated with multiple intracranial processes, suchas lymphoma, toxoplasmosis, and CMV.We present a patient with AIDS whodeveloped encephalopathic symptoms while hospitalized, requiring an in-tensive work-up, ultimately leading to the diagnosis of Posterior ReversibleEncephalopathy Syndrome (PRES).Case: A 20 year old African American man with a past medical historysignificant for untreated HIV presented with a four day history of SOB,fevers, chills, and cough with blood tinged sputum, and seizures. Chest x-rayrevealed a hazy right middle lobe infiltrate. His initial CD4 count was 34/mm3;however, his CD4 percentage was 17.7%, suggesting lesser degree of im-munosuppression. He was found to be in renal failure, with a Creatinine of28.2mg/dL and BUN of 162mg/dL, nephrotic range proteinuria, and a serumalbumin of G 1, consistent with HIV associated nephropathy (HIVAN). Hewas started on hemodialysis. A few days after his admission, he developedworsening respiratory distress secondary to acute heart failure and fluidoverload requiring intubation. His PCP sputum was positive, and he wastreated with sulfamethoxazole-trimethoprim and steroids. During his hospi-tal course, he had a seizure that was felt to be due to electrolyte abnormalitiesfrom his renal failure, but after a week of dialysis he had recurrent tonic-clonic seizures. The patient was started on Phenytoin. A brain MRI withoutcontrast showed multifocal irregular areas of abnormal T2 signal increasethroughout the brain, mostly in the peripheral grey matter. A thorough work-up for the usual suspects was non-diagnostic. His seizures subsided over thenext few days. A repeat brain MRI without contrast performed 10 days after
the first scan showed resolution of the majority of the T2 hyperintensities.This finding was consistent with PRES, which was thought to be due to thepatient’s renal failure/HTN and HIV.Discussion: There are numerous opportunistic infections and processesmanifest in patients with advanced HIV/AIDS, thus multiple etiologies arepossible when CNS lesions are present. Although not thought of commonly,PRES is possible in a patient with a low CD4 count and elevated bloodpressure with characteristic findings on MRI.
Joint Plenary Poster SessionPediatric Clinical Case
5:00 PMThursday, February 21, 2013162
SARCOIDOSIS AND SARCOMERES: A CASE OF ACUTEMYOSITIS
Adimora-Nweke DE, Huntwork M, Humphrey J. Tulane University HealthScience Center, New Orleans, LA.Case Report: A 16 year-old African American boy developed myalgia andswelling of the right arm over one week. Two years prior, he had developedsimilar symptoms. Previous right forearm muscle biopsy had demonstratedinflammatory infiltrate consistent with myositis. All other labs were normal.He was treated with corticosteroids, NSAIDS, and methotrexate over thefollowing year and remained symptom free. One week prior to presentation,he developed acute swelling and pain at the right ankle. He had anemia,thrombocytopenia, and hypoalbuminemia with elevated ESR at 71cells/mm3.An MRI of the right arm demonstrated patchy multifocal edema in the muscleand bone marrow. Pathology slides from the previous muscle biopsy werereviewed and demonstrated discrete granulomatous lesions characteristic ofsarcoidosis. Previous bone marrow biopsy also showed patchy areas of fi-brosis with areas consistent with early granuloma formation. A CT scandemonstrated no intrathoracic abnormalities. Uveitis was found. Serum ACElevel was normal. He was started on prednisone and methotrexate for acutesarcoid myositis.Sarcoidosis may present at any age with a variety of clinical manifestations.Asymptomatic skeletal muscle involvement is common, but acute symp-tomatic myositis occurs in less than 2% of patients. This rare presentation issuggested by proximal weakness, myalgia, or swelling. Additional systeminvolvement such as arthropathy, uveitis, and laboratory markers of inflam-mation are more common presentations and help to suggest the diagnosiswhen present. Notably, our patient did not have evidence of pulmonary in-volvement, but pulmonary involvement eventually occurs in over 90% ofindividuals with sarcoidosis.This diagnosis of exclusion requires histologic demonstration of non-caseating granulomas of any involved site. MRI may be used to localizemusculoskeletal lesions, while chest radiography and CT scan may delineatepulmonary involvement. Serum angiotensin converting enzyme is elevatedin 50-80% of patients with sarcoidosis, and indicates intrathoracic involve-ment and disease activity rather than diagnosis of the disease. Corticosteroidsare the mainstay of therapy, and disease modifying antirheumatic drugsshould be reserved for the more severe forms of the disease.
163
A COMPLEX CASE OF SECONDARYHYPERHOMOCYSTEINEMIA IN A PRETEEN NICUGRADUATE
Austin C1,2, Lawson S2, Engel LS1. 1LSU Health Sciences Center, NewOrleans, LA and 2LSU Health Sciences center, New Orleans, LA.Case Report:Case: A 12 year-old boy with a significant past medical history of prema-ture birth at 32 WGA, gastroschisis with resection during his infancy, andNICU hospitalization for six months, presented with a syncopal event. Thepatient was well-appearing on presentation, and maintained systolic bloodpressures in the 80s after an additional bolus in the emergency room. Thepatient had an additional episode of syncope, and the pediatric hospitalist
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
418 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

team was consulted to evaluate and treat the patient. On interview, he de-scribed feeling ‘‘like he didn’t have enough strength.’’ The patient wastachypneic, with a respiratory rate near 30 and pulse oximeter reading from92 to 94% on room air. He appeared thin, with long fingers and extremities,and had a normal cardiovascular and chest exam. However, his lower ex-tremities were asymmetric, with his left calf measuring 25 cm and his rightcalf measuring 29 cm in circumference. Bilateral lower extremity ultrasoundsrevealed venous thromboembolism (VTE) in the patient’s right femoral andpopliteal veins. A CT of the chest confirmed the source of the patient’ssyncopeVpulmonary embolism (PE). Hypercoagulable investigation demon-strated normal protein S, slightly low protein C level at 50 (normal 55-110),increased homocysteine levels and heterozygosity for MTHFR C677T. Thepatient also had a low vitamin B12 level, which was ultimately thought tobe the cause of his hyperhomocysteinemia.Discussion: A pediatric patient presenting with syncope is a quite com-mon occurrence in pediatric emergency facilities; however, the source of thepatient’s syncopal event being a pulmonary embolus is a far less frequentevent. Any child without significant risk factors for venous thromboembo-lism warrants an evaluation for hypercoagulable states that could potentiallypredispose that individual to a VTE or PE.
164
ISOLATED ARTERIAL TORTUOSITY IN A NEWBORN WITHHYPERTENSION
Broge T1, Shipon C1, Freysdottir D2, Davenport J3. 1Florida State UniversityPediatric Residency, Sacred Heart Hospital, Pensacola, FL; 2PediatrixMedical Group, Pensacola, FL and 3Nemours Children’s Clinic, Pensacola, FL.Case Report: The newborn male was born at 33 6/7 weeks to a 37 year-oldG2P1 female. Family history was unremarkable and a 3 year-old sibling wasnormal. He was transferred to a level three NICU for feeding intolerace andelevated blood pressures. Four-limb blood pressures were elevated, with the
highest being 113/87 in the right lower extremity. Physical exam was unre-markable. Computed tomography angiography showed tortuosity of the ar-terial tree throughout the chest, abdomen, and pelvis. Brain imaging revealedmultiple areas of vessel tortuosity. Mutations in gene loci involved in the con-nective tissue disorders were excluded through DNA sequencing and chro-mosomal microarray was normal. The infant was stabilized on anti-hypertensivemedication and monitored on an ambulatory basis. At 6 months he remainsstable on therapy and is meeting developmental milestones and growingappropriately.Discussion: Multiple congenital arterial anomalies in children are rare andare usually found with one of several known connective tissue disorders.Ehlers-Danlos, Loeys-Dietz, and Arterial Tortuosity syndrome are associ-ated with arterial tortuosity. Isolated arterial anomalies in a newborn in ab-sence of metabolic or systemic disease have not previously been described. Itis possible that this case may represent a partial genetic phenotype of theknown connective tissue disorders or a novel genetic defect in the connectivetissue of the arterial system.
165
COSLEEPING THAT CAUSED SUDDEN INFANT DEATH
Callaway D, Singh D, Yosypiv IV. Tulane University Hospital, New Orleans, LA.Case Report: A 2 month old previously healthy male presented to the EDafter being found pulseless and apneic after sleeping in the bed next to hismother for approximately 30 minutes. Past medical history included intra-uterine opiate exposure and pre- and postnatal tobacco exposure. Pulse wasrecovered after two doses of epinephrine and the patient was intubated in thefield by EMS. Admission temperature was 98.0o F, pulse 111, blood pressure74/31 mmHg. Initial laboratory investigations revealed an undetectable bloodpH, potassium of 5.8 mEq/L, bicarbonate of 5 mEq/L, BE of -26.3, serum ureanitrogen of 36 mg/dL, creatinine of 1.7 mg/dL, lactic acid of 9.16 mg/dL,PTT of 69.5 seconds and INR of 3.8. Despite administration of packed redblood cells (PRBC), fresh frozen plasma (FFP), albumin, bicarbonate andvasopressor support, he developed multisystem organ failure. Because of pro-longed multisystem organ failure, renal replacement therapy was not initi-ated. The patient expired on hospital day 2. Sudden Infant Death Syndrome(SIDS) is defined as unexplained death before 1 year of age and accounts forapproximately 2,300 deaths annually in the U.S. Risk factors include pronesleep position, prenatal tobacco exposure, environmental tobacco smoke, andlow socioeconomic status (SES). A more recently described phenomenon isAccidental Suffocation and Strangulation in Bed (ASSB), which likely oc-curred in this case. Risk factors include prone sleep position, soft bedding,and bed sharing. Current risk reduction strategies include supine sleep po-sition, no bed sharing, firm sleep surface without other objects in crib, ade-quate ventilation, swaddling, breastfeeding, and use of pacifiers. It is imperativethat pediatricians address these issues during early visits to further reduce therate of SIDS and ASSB.
166
AN UNUSUAL PRESENTATION OF 22Q11 DELETIONSYNDROME IN THE NEWBORN PERIOD
Cuna A, Philips J. University of Alabama at Birmingham, Birmingham, AL.Case Report: A two-day-old term baby girl was transferred for surgicalmanagement of an imperforate anus with rectoperineal fistula. Other dysmor-phic features included craniosynostosis, hypodeveloped thumbs, and atrial sep-tal defect. Baller Gerold syndrome (BGS) was suspected. However, at 1 weekof age she developed hypocalcemia, which raised suspicion for 22q11 de-letion syndrome (22q11DS). Florescence in situ hybridization testing wasdone which confirmed microdeletion of chromosome 22q11. She was treatedwith oral calcium supplementation, and underwent successful anorectoplasty.This case illustrates a well known medical saying - ‘‘uncommon presentationsof common diseases are more common than common presentations of un-common diseases’’. BGS, an extremely rare (G1 in 1 million) autosomalrecessive disease, was initially suspected because the patient presented withits classic features - craniosynostosis (100%), radial limb defect (100%),anorectal anomalies (40%), and cardiac defects (25%). On the other hand,22q11DS is a far more common genetic disorder (1 in 4,000) that has awide range of phenotypic variability. A European collaborative study in-volving 23 centers reported on the spectrum of clinical features associated
Angiography showing dilatation and tortuosity of the descendingaorta and renal arteries
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 419
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

with 22q11DS. Of the over 500 patients in the study, only 0.9% had cra-niosynostosis, 2% had anorectal malformations, 1.5% had isolated atrialseptal defects, and 4% had unspecified skeletal limb abnormalities. Of note,more than 60% had hypocalcemia and it was this finding together with a highindex of suspicion that led to the diagnosis of 22q11DS in this patient.To our knowledge, this is the first reported case of 22q11DS with craniosy-nostosis, radial ray defect, and anorectal malformation all presenting in asingle patient.
167
NOVEL MUTATION IN THE WT1 GENE CAUSINGCONGENITAL NEPHROTIC SYNDROME PRESENTING ASLIFE-THREATENING HEART FAILURE
Day C1, Evans M2, Self S3, Robinson JC3, Allen RK3, Sas DJ4, Shatat IF4.1Medical University of South Carolina, Charleston, SC; 2Medical Universityof South Carolina, Charleston, SC; 3Medical University of South Carolina,Charleston, SC and 4Medical University of South Carolina, Charleston, SC.Case Report: We report on a term three month-old female with severehypertension and dilated cardiomyopathy, who was found to have an unde-scribed mutation of the Wilms’ tumor suppressor (WT1) gene and diffusemesangial sclerosis. She presented in acute respiratory failure requiring intu-bation, with tachycardia and hypertension (157/90 mmHg). A chest radiographshowed an enlarged cardiac silhouette, bilateral pleural effusions, and dif-fuse pulmonary edema. Laboratory evaluation was significant for troponin I5.85 ng/ml, B-type natriuretic peptide 4643 pg/ml, hemoglobin 7.3 gm/dl,blood urea nitrogen 23 mg/dl, creatinine 0.6 mg/dl, serum albumin of 1.1 g/dl,and total cholesterol 241mg/dl. Echocardiography showed severely dimin-ished systolic function and a dilated left ventricle. Afterload reduction wasinitiated with intravenous antihypertensives. A twenty-four hour urine collec-tion demonstrated 11.8 g protein. A renal ultrasound revealed no renal arterystenosis. Genetic evaluation revealed a heterozygous WT1 (11p13) mutationnot previously described. Kidney biopsy demonstrated diffuse mesangialsclerosis. Immunohistochemistry revealed normal expression of the WT1nuclear protein and down-regulation of one of its target genes, paired boxgene 2 (PAX2). Mutations in the WT1 gene are associated with nephroticsyndrome (NS), hypertension, diffuse mesangial sclerosis, genitourinary ab-normalities, Wilms’ tumor, and other anomalies. It is most likely that ourpatient’s WT1 gene mutation resulted in isolated NS with associated diffusemesangial sclerosis. Although hypertension is a rare diagnosis in infants, itis imperative that healthcare providers remain aware of the possible non-specific presentation. Careful evaluation of hypertension in infants present-ing with non-specific symptoms such as difficulty breathing, poor feeding,emesis, increased irritability, and even cardiovascular collapse may promoteearlier diagnosis and more timely management.
168
GLUTARIC ACIDEMIA TYPE 1: A CASE SERIES
Felton H, Schwenk K. University of Louisville, Louisville, KY.Case Report: Glutaric academia type 1 (GA-1), an autosomal recessivedisorder, can manifest clinically in many ways during a metabolic crisis. Theincidence is one in thirty thousand Caucasian births in the United States.Most patients with GA-1 present in the first year of life, but rarely becomesymptomatic in the newborn period. We describe a 3 day old male who pre-sented with poor feeding and indirect hyperbilirubinemia. 18 months prior tohis presentation, his older brother died at 7 days of life following initialsymptoms of poor feeding and indirect hyperbilirubinemia. This siblingeventually became unresponsive and suffered a massive and fatal intracranialhematoma. He had an extensive post-mortem work up without diagnosis. Ourpatient’s initial bilirubin was 16.9, but peaked at 17.4. He was started on IVfluids for dehydration and phototherapy. He had a normal abdominal ultra-sound that was obtained because his sibling was found to have a fatty liveron autopsy. Genetics was consulted for this presentation and family history.Work up revealed that his urine glutaric acid was 4.5mcg/mg creatinine (nor-mal G15) and urine 3-hydroxyglutaric acid was 22.2mcg/mg creatinine (normalG20) which was positive for GA-1. After two days of IV fluids his hydrationstatus improved. His bilirubin decreased to 13 off of phototherapy. His feed-ing also improved with the help of a lactation consultant. We will explore the
genetic screening, diagnosis, clinical manifestations of these siblings andwhy they had very different outcomes.
169
A CASE OF INTERNATIONAL ADOPTION: ATTENDING TOTHE MEDICAL, SOCIAL AND EMOTIONAL NEEDS OFTHE FAMILY ADOPTING AN HIV+ CHILD
Henderson N, Owen EB, Marshall G. University of Louisville, Louisville, KY.Case Report: With the growing number of international adoptions from theAfrican continent, namely Ethiopia, Human Immunodeficiency Virus (HIV)is not only a concern for resource limited countries, but one affecting pe-diatricians here in the United States. HIV, a retrovirus that destroys humans’CD4 cells and ultimately their immune systems, affects thirty four millionpeople worldwide, two million of which are children. Of these infected twomillion children, only one quarter of them is receiving antiretroviral ther-apy (ART), with only six to nine percent of children in northern and easternAfrica receiving treatment. Children are predominantly infected perinatallywith 480,000 newly infected infants reported worldwide in 2008. Our son isa recently adopted a five year old boy who is HIV positive. He was not onART at initial medical screen in 2010. After two year s of ART, he demon-strated improved growth velocities for age in weight from the 5th to 25thpercentile and 10th to 50th in height. He arrived in the home on combinationARTunavailable in the United States with undetectable viral loads and a CD4count approaching 1600, well within the normal range. The difficult deci-sion of continuing to manage his HIVand ART in light of surprisingly normallaboratory values and exam findings was now present. Uniquely qualifiedboth as a pediatrician and a parent, I will explore the issues affecting parentswith HIV positive children, specifically through adoption, and the implica-tions for pediatricians caring for these patients. Should his ART be contin-ued? If so what meds should he take? Who should the parents inform abouthis HIV status?
170
A CASE OF DIPLOID/TRIPLOID MOSCICISM IN A SET OFMONOZYGOTIC-DIZYGOTIC TWINS
Hightower HB1, Philips J1, Faye-Petersen OM2. 1University of Alabama atBirmingham, Birmingham, AL and 2University of Alabama at Birmingham,Birmingham, AL.Case Report: Diploid/triploid mosaicism is a rare chromosomal abnor-mality associated with mental and growth retardation, dysmorphic features,and genital abnormalities depending on the sex chromosome complementof the two cell lines. In most cases, the lymphocyte karyotype is normal anda diagnosis is made only after analysis of other tissue.The twins were born at 26/0 weeks due to preterm labor. Girl A had a normalexam except for bilateral postaxial polydactyly. Twin B had macrocephaly,low set and posteriorly rotated ears, corneal clouding, cleft palate, heartmurmur, and ambiguous genitalia. Twin B died at twoweeks from multiorganfailure following a complicated NICU course.Due to ambiguous genitalia and severe illness of twin B, there was concern forcongenital adrenal hyperplasia in both twins but it was ruled out with normal17-OH progesterone. Girl A also had a normal abdominal ultrasoundshowing a uterus and no testes. Head ultrasound on Twin B demonstratedmultiple intracranial anomalies. An echocardiogram showed a PDA, ASD,VSD, and decreased ejection fraction of 40%. An abdominal ultrasound wasunable to identify a uterus or gonads.Both twins had rapid aneuploidies resulting XX with no trisomies. Twin B’sinitial karyotype was 46,XX in five analyzed cells and a CGH array showed a17p12 microdeletion. Following an autopsy, karyotype of fibroblasts was69,XXY that was confirmed by FISH studies. Lymphocytes were reevaluatedwith 99.6% being diploid XX and 0.4% were triploid XXY suggesting a lowproportion of cells with a 69,XXY karyotype. Girl A had the same 17p12deletion in all analyzed lymphocytes. They also showed 2/22 cells with a69,XXY karyotype and the remaining cells had 46,XX with these resultsconfirmed by FISH studies. Her fibroblasts were 46,XX.Since most diploid/triploid mosaics have normal karyotypes, as in this case, itis important to consider studying the fibroblasts to evaluate for additional celllines. Even though the surviving twin had a normal exam it is important to
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
420 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

evaluate for low-level mosaicism due to possible occurrence of dysgeneticgonads and increased risk for gonadoblastoma.
171
I CAN’T PEE, ULTRASOUND ME!
Huntwork M1, Malhotra S2. 1Tulane University, New Orleans, LA and2Tulane-Ochsner Pediatric Residency Program, New Orleans, LA.Case Report: A one-month-old dysmorphic Hispanic boy presented with atwenty-four hour history of anuria. Mother reported an uneventful pregnancywith routine prenatal care. The baby boy had an asymmetric face with rightside smaller than left, a small right eye, and cupped ears. He had an imper-forate anus and ileal atresia, and underwent ileal cecal anastamosis and di-vided sigmoid colostomy in the NICU. Additionally, he had a patent ductusarteriosus, an atrial septal defect, and pulmonary stenosis. Laboratory studiesrevealed sodium of 122, potassium of 5.5, bicarbonate of 18, and creatinineof 2.9. Renal ultrasound revealed a multicystic dysplastic left kidney anddilation of the collecting system in the right kidney. A nuclear medicine scanrevealed that the left kidney demonstrated virtually no function. The patientwas ultimately diagnosed with a multicystic, virtually nonfunctional leftkidney, a mild hydronephrosis in his right kidney, and a renal tubular acidosis,Type 4.Discussion: Pediatricians frequently encounter a variety of genetic disor-ders. Goldenhar’s Syndrome, or oculo-auriculo-vertebral dysplasia, is a dis-ease associated with maldevelopment of the structures derived from the firstand second branchial arches. The exact etiology of this syndrome is unclear.The symptoms are heterogeneous and vary greatly, but generally include earanomalies, hemifacial microsomia, and vertebral anomalies. At least 5% ofthese patients have renal anomalies. Our patient demonstrates that when renalanomalies occur, they have a considerable impact on the patient’s health. Thepercentage of patients diagnosed with Goldenhar’s Syndrome who undergorenal ultrasound as part of their initial workup is unknown, but a screen-ing renal ultrasound (indicated in initial workup of many other genetic dis-orders) prior to Goldenhar baby’s initial discharge might help foreshadowor even prevent renal complications such as hydronephrosis, urinary reten-tion, and renal tubular acidosis.
172
LEFT-RIGHT-LEFT, LEAD PLACEMENT ERRORS INPEDIATRIC ELECTROCARDIOGRAMS
Kleinman JA, Stockwell E, Darwin S, Snyder C. Ochsner FoundationsHospital for Children, New Orleans, LA.Purpose of Study: Electrocardiograms (ECGs) are a frequently used pe-diatric diagnostic tool. Lead placement errors, specifically lead limb reversal,are common problems for this test. No studies exist in pediatrics regardingfrequency of lead placement errors on ECGs. The purpose of this study wasto capture how frequently lead placement errors occur in pediatric ECGs.Methods Used: A single-center, IRB-approved, retrospective review wasconducted of all ECGs performed from January 2011 through March 2011.Inclusion criteria were age KG18 years and an ECG performed at or trans-mitted to our center. All ECGs were re-reviewed by a blinded pediatricelectrophysiologist. All ECGs with lead reversal or smear were deemedpositive.Summary of Results: A total of 945 ECGs were identified by the search.The average age of the patient was 10.3 years old. The majority of the ECGswere performed in an outpatient clinic (637, 67%) followed by the ED (165,17%), and the hospital (143, 15%). Abnormal lead placement was identifiedin 35 (2.7%). The most common form was reversal of the left arm and legleads (42%), followed by left arm and right arm leads (35%). Smear wasidentified in 3 (11.5%). The majority of lead placement errors occurred inthe outpatient clinic (8.6%). A majority of the ECGs identified by pediatricelectrophysiologists as abnormal were previously interpreted by the samegroup as normal (42%).Conclusions: This is the first study conducted to assess lead placementerrors in the pediatric population. Lead placement abnormalities occur com-monly and are routinely missed by the interpreting physician. Pediatric leadplacement abnormalities occur at similar rates to adults (2.7% compared to4%). These errors may lead to a delayed diagnosis and treatment, and wasted
healthcare resources. We suggest further training and quality improvementseminars on how to obtain accurate ECGs to avoid unnecessary and costlyerrors.
173
ALL CHOKED UP: VELOPHARYNGEAL INCOMPETENCEPRESENTING AT A NEWBORN HEALTH SUPERVISIONVISIT
LeJeune G, Broussard M, Bocchini J. LSUHSC, Shreveport, LA.Case Report: A 3-day old Caucasian female born at term without prena-tal or perinatal complications presented to the outpatient clinic for a new-born health supervision visit. During the examination the patient’s motherreported difficulties with feeding. At this time the infant was being exclu-sively breastfed. During feedings she would detach from the breast, arch herback and appear to choke. Nasal regurgitation of milk and peri-oral cyanosiswas described by the mother. Family history was positive for ‘‘paralyzedpalate.’’ Review of systems was also positive for nasal congestion and clearrhinorrhea that had been present since birth. No recent fever, signs of in-fection, change in activity or appetite was reported. Upon physical exam hergag reflex was absent. No other neurological lesions were observed. Nostructural abnormalities of the oropharynx were present. The remainingphysical exam was unremarkable. This presentation and physical examina-tion prompted admission to the pediatric ward for further investigation.Sepsis was ruled out, Otolaryngology was consulted and a swallow study wasobtained. Her swallow study revealed severe oral and pharyngeal dysphagiawith no velum movement, an uncoordinated suck, swallow, breathe synchronyresulting in significant nasal regurgitation and desaturation to 73%. Thisstudy prompted recommendation for continued NPO status with alterna-tive means of nutrition/hydration. Pediatric Surgery was then consulted forplacement of a percutaneous endoscopic gastrostomy tube.
Velopharyngeal incompetence, typically involving the 9th and 10th cra-nial nerves, is due to the dysfunctional movement of the velopharyngealstructures. It is extremely rare to present in absence of a structural abnormalityor injury, such as cleft palate or following tonsillectomy and adenoidectomysurgery. Complete paralysis of the soft palate leads to nasal regurgitation, lossof gag reflex and trouble swallowing foods which place patients at high riskfor aspiration. Typical treatment usually includes a surgical procedure orprosthetic device to correct the dysfunction.
174
NINE YEAR OLD BOY WITH HEADACHE, VOMITING ANDALTERED MENTAL STATUS
Lucke AM, Pyle A. University of Texas Southwestern Children’s MedicalCenter of Dallas, Dallas, TX.Case Report: A 9 year old boy presented with fever, headache, vomitingand altered mental status. The headache and fevers developed 4 days priorwith fatigue and decreased appetite. On the day of presentation he com-plained of non-bloody, non-bilious emesis and progressive confusion. He wasfully immunized and recent exposures included a community pool and theOklahoma Red River. Past medical history is significant for bilateral myr-ingotomy, tonsillectomy and adenoidectomy.On initial exam he was febrile, tachycardic and responsive only to noxiousstimuli (GCS 9). Pupils equal and reactive, HEENT benign, 1/6 soft sys-tolic murmur, lungs clear, abdomen benign. No edema or rash, capillary refill3-4 seconds.Initial laboratory studies show mild leukocytosis (15.7K/mm3) but other-wise normal CBC, normal chemistry panel, CRP and ESR. Negative urinal-ysis and drug screen. CSF was frank pus with opening pressure 55mmHg,9,442 nucleated cells (1% bands, 85% polys, 6% lymphs, 8% monos), 133RBCs, glucose 12, protein 462. CSF gram stain was negative. Head CTshowed mild cerebral edema, patchy mucosal thickening of ethmoid sinuses.With fever and evolving loss of mental status meningitis/encephalitis washigh on the differential. With a negative CSF gram stain and freshwater ex-posures special consideration for amebic etiologies was given. ID was con-sulted who identified amebic bodies in CSF cytospin later confirmed to beNaegleria Fowleri. Due to progressive somnolence he was intubated and EVDplaced to manage intracranial pressure. Treatment consisted of IV rocephin,
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 421
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

fluconazole, rifampin, amphotericin and cranial intra-ventricular amphotericin(via EVD). Although he initially improved his ICP continued to rise withtentorial herniation. The patient expired on hospital day four.Naegleria fowleri is an ameboflagellate that invades the brain via nasal mu-cosa causing acute, fulminant hemorrhagic meningoencephalitis which isnearly always fatal. Initial signs and symptoms onset within 1-14 days afterexposure. Disease progression is rapid and death occurs within 3-7 days ofsymptom onset. There is some theory that ENT surgical procedures lead toincreased susceptibility which could explain why our patient was effectedwhile many others swimming that day were not.
175
END STAGE RENAL DISEASE DUE TO FIBRILLARYGLOMERULONEPHRITIS IN A FOUR YEAR OLD CHILD
Mandava M1, Sankararaman S1, Habib S1, Gu X2. 1Louisiana StateUniversity Health Sciences Center, Shreveport, LA and 2Louisiana StateUniversity Health Sciences Center, Shreveport, LA.Case Report: A four-year-old African-American male with no significantpast medical history presented with a two weeks history of cold symptomsand cola colored urine. He has a strong family history of IgA nephropathy. Onevaluation, he had macroscopic hematuria, severe proteinuria and a serumcreatinine of 1.2mg/dl. Two days later his renal functions worsened with aserum creatinine of 3.3mg/dl and serum potassium of 6 meq/L. Further labsshowed ASO 1659, low C3, normal C4, normal ADAMTS 13, normal Fac-tor H, negative serology and urine protein of 1.6gm/day. Renal biopsy showedcoarsely granular capillary loops and mesangial deposits with IgG, C3 andfibrin in all glomeruli. Electron microscopy showed proliferative glomeru-lonephritis with fibrillary deposits (Fig.1). He did not improve with steroidsand required peritoneal dialysis. Patient was then started on cytoxan. He dem-onstrated transient improvement in renal function and despite treatment hedeveloped end stage renal disease within a month. He developed membranefailure and switched to hemodialysis. Fibrillary glomerulonephritis (FGN)is a very rare disease and only few pediatric cases have been reported so far.Most of the patients had persistent proteinuria and hematuria without pro-gression to renal failure. This is an atypical case of FGN with rapid pro-gression to ESRD with a coincidental family history of IgA nephropathy.
176
A NEWBORN WITH BILATERAL NEPHROMEGALY
Martinez T, Chong E, Singleton T, Narumanchi T, Yosypiv I. Tulane Schoolof Medicine, New Orleans, LA.Case Report: Antenatal fetal ultrasonography (US) performed at 20 weeksof uncomplicated gestation in a 23-year-old G3P3 female demonstrated thepresence of enlarged kidneys in a single male fetus. Birth weight at 37 weeksof gestation was 4.29kg. Blood pressure (76/52 mmHg) and urine output werenormal. Physical examination demonstrated an enlarged tongue, posteriorlyrotated ears, enlarged abdomen with palpable kidneys bilaterally and hepa-tosplenomegaly. Laboratory findings included serum glucose of 114 mg/dL,total protein of 6.4 gm/dL, AST 44 u/L, creatinine 0.7 mg/dL, alpha-feto
protein of 280,000 ng/mL and normal urinalysis. Renal US showed bilat-eral nephromegaly (RK- 8.5, LK- 7.5 cm), increased echogenicity and poorcorticomedullary differentiation. Renal biopsy performed on second week oflife revealed renal dysplasia without cysts. Subsequent elevation of bloodpressure required initiation of renin system inhibitor. Microarray CGH wasnormal. Gene sequencing of GPC3 revealed a characteristic deletion of exon1 consistent with the diagnosis of Simpson-Golabi-Behmel syndrome (SGBS).Subsequent surveillance US and CT at 18 months revealed a discrete 5x5 cmmass in the left kidney. Histologic examination of the mass showed pureepithelial type nephroblastoma. Chemotherapy with Dactinomycin, Doxo-rubicin, and Vincristine per AREN0534 protocol resulted in decreased tu-mor size. SGBS is a rare congenital overgrowth syndrome with macroglossia,macrosomia, renal/skeletal abnormalities and an increased risk of embryo-nal cancers. GPC3 gene at Xq26 encodes cell surface heparan sulfate pro-teoglycan that controls growth factor signaling and tight regulation of cellproliferation/apoptosis during kidney development. This case illustrates arare case of bilateral nephromegaly with dysplasia in a patient with SGBSassociated with later Wilm’s tumor. Because the underlying molecularmechanisms that cause birth defects are largely unknown, development ofnew strategies aiming at their prevention, preservation of renal function andavoidance of associated cardiovascular morbidity is needed.
177
SUPERIOR MEDIASTINAL SYNDROME ASSOCIATEDWITH TUMOR LYSIS AS THE INITIAL PRESENTATION OFT-LYMPHOBLASTIC LYMPHOMA
Melethil S, Hooda B. University Of Texas Medical Branch, Galveston, TX.Case Report: Introduction: Superior Mediastinal Syndrome (SMS) is acomplication of pediatric malignancy with high tumor burden and occurs atpresentation in 12% of the cases. SMS is the direct result of pressure on vitalmediastinal structures including trachea and superior vena cava. This oncologicemergency may be accompanied by respiratory embarrassment resulting incardio pulmonary failure. Tumor Lysis Syndrome (TLS) is frequently a com-ponent of overall presentation of pediatric malignancy presenting as SMS.Objective: To recognize SMS and TLS in children with malignancies andunderstand the rationale for management of these potentially life threateningconditions.A 6 year old male presented to the Urgent Care with a 2 week historyof neck swelling and otalgia. Otitis Media was the initial diagnosis and wastreated with a course of Amoxicillin without success. Fever, cough, weightloss and dyspnea developed a week later. Physical examination revealed bi-lateral cervical and axillary lymphadenopathy and significantly diminishedbreath sounds on the left side. Chest X-ray showed left sided opacity withpleural effusion. Chest CT scan showed mediastinal lymphadenopathy. Echo-cardiogram confirmed pericardial effusion. Lymph node Biopsy establishedthe diagnosis of T lymphoblastic lymphoma. The patient was treated with hy-perhydration, intravenous Allopurinol and alkalinization for TLS followed bychemotherapy. The patient went in remission within 4 weeks without any re-quirement for cardiothoracic surgical procedure or intensive care monitoring.Discussion: This case reflects the importance of identifying malignancy andits complications as differential diagnosis when a child presents with non-specific respiratory symptoms. Metabolic abnormalities of TLS from thebreakdown of rapidly proliferating cells should be expected and preemptivelyaddressed.Conclusion: Recognizing and managing critical conditions like SMS andTLS at an early stage will significantly reduce morbidity and mortality inPediatric cancer patients and may minimize unnecessary surgical interven-tions and intensive monitoring. This may also reduce the health care costsassociated with care of pediatric patients having oncologic emergencies.Revenues saved this way maybe utilized for other patients and services.
178
THROMBOTIC EVENTS IN CONGENITAL DISORDERS OFGLYCOSYLATION
Mohamed M1, Morava E2,1. 1Radboud University Nijmegen Medical Center,Nijmegen, Netherlands and 2Tulane University Medical School, New Orleans, LA.Purpose of Study: Congenital disorders of glycosylation are a grow-ing group of inborn errors of metabolism with psychomotor retardation and
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
422 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

severe coagulation abnormalities. The most common type, presenting withhypotonia, strabismus and abnormal fat distribution, caused by PMM2 mu-tations, is a clinically recognizable syndrome. Many proteins regulating nor-mal coagulation, including factor IX, factor XI, Antithrombin-III, Protein C andProtein S are deficient in CDG. Because of the imbalance in pro- and anti-coagulation factors, some patients develop acute vascular events, such as throm-bosis. Identifying patients at high risk of thrombotic events could preventserious complications, irreversible damage and even mortality.Methods Used: We performed a meta-analysis involving patients reportedwith PMM2-CDG between 1990 and 2012 and also included our own patientcohort of 15 patients with PMM2-CDG In total, 191 patients were included.Patients with and without a thrombotic event were compared based on thealterations of the following factors: PT, aPTT, Antithrombin-III, Protein C,Protein S, factor IX and XI. Additionally we evaluated the family history andprovoking events.Summary of Results: In the total group of 191 PMM2-CDG patients 14had suffered a thrombotic event, either venous or arterial. Low activity ofseveral anticoagulation factors correlated with thrombotic events. Howeverrelatively high factor IX and XI activity were not predictive for thrombo-sis. Prolonged PT and aPTT did not seem to protect against thrombosis inthe patients. Immobility was a moderate risk factor and operations highlycorrelated with thrombotic events.Conclusions: Low activity of several anticoagulation factors correlated withthrombotic events. Evident and easily preventable risk factors like immobil-ity could be treated with regular physiotherapy. We advise to avoid electivesurgical procedures in PMM2-CDG patients. Adequate fluid intake in caseof inevitable operations is crucial.
179
PROGRESSION OF OCULAR MYASTHENIA GRAVIS TOGENERALIZED MYASTHENIA GRAVIS IN THE PEDIATRICPATIENT
Morris ME, Carothers BS. University of Louisville, Louisville, KY.Case Report: A 3 year old African American female with a history offailure to thrive presented to primary care for follow-up of conjunctivitis. Shehad an acute onset bilateral ptosis, left worse than right, which prompted abrain and orbit MRI, both normal. Diagnosis was delayed until the charac-teristic worsening of ptosis throughout the day was identified and acetyl-choline receptor binding antibodies were positive. She started pyridostigmineand prednisone without significant improvement in symptoms. IVIG helpedher short term, but she had four hospital admissions for myasthenic crises andprogression to dense generalized symptoms. Thymectomy was not performeddue to a normal thymus on imaging. She ultimately succumbed to the effectsof a myasthenic crisis, triggered by bronchiolitis, within less than a year ofdiagnosis. Our case report shows the importance of early recognition of symp-toms of ocular myasthenia gravis as well as the possibility for progression togeneralized myasthenia gravis and even death.
Myasthenia gravis is an uncommon diagnosis in the pediatric pop-ulation caused most frequently by an acquired autoimmune process calledJuvenile Autoimmune Myasthenia Gravis. Autoantibodies target the ace-tylcholine receptors in the post synaptic membrane of the neuromuscularjunction, causing degradation of the acetylcholine receptors and blockingacetylcholine from binding to its receptor. 1 Common presenting complaintsof pediatric patients with myasthenia gravis are ptosis, diplopia, strabismusor ophthalmoplegia. Case series have noted the incidence of progressionto generalized symptoms between 23-43% in the pediatrics. 2 Death resul-tant from complications of generalized myasthenia gravis in children is arare complication. Treatment options include pyridostigmine, steroids, thy-mectomy, IVIG, or azathioprine. Some patients achieve medication freeremission. 3
1. Gilhus Nils E. Myasthenia and the Neuromuscular Junction. CurrentOpinion in Neurology 2012; 25:523-529.
2. Pineles Stacy et al. Visual and Systemic Outcomes in Pediatric OcularMyasthenia Gravis. American Journal of Ophthalmology. 2010150(4):453-459.
3. Mullaney et al. The Natural History and Ophthalmic Involvement in
Childhood Myasthenia Gravis at The Hospital for Sick Children.Ophthalmology. 2000; 107(3):504-510
180
LATE PRESENTATION OF LIFE-THREATENINGCONGENITAL HEART DISEASE
Mullin MG, Singh D, Sernich S. LSU School of Medicine in New Orleans,New Orleans, LA.Case Report:Objective: to emphasize the importance of recognizing late presentationof potentially life-threatening Congenital Heart Disease (CHD).Methods: A retrospective chart review was performed on three patients withCHD who presented to our institution at a later-than-expected age. For eachpatient, we describe clinical presentation and findings of 2D echocardiog-raphy, CTA, MRI, and electrophysiology studies identifying the underly-ing heart disease. We also give an overview of the corrective proceduresand clinical progress of each patient following their diagnosis.Results: Our first patient is a 5 year old who had an asymptomatic heartmurmur discovered on a routine exam. Upon further study, the patient wasfound to have an anomalous left coronary artery arising from the main pul-monary artery (ALCAPA). Our second patient is a 6-month old with devel-opmental delay who was previously healthy until he presented with cyanosis,low oxygen saturations, and heart murmur and on exam before an electivebrain MRI; he was later found to have D-TGA with a large ASD. Our thirdpatient is a 14 year old who had been previously healthy until he collapsedafter football practice. He was found to be in cardiac arrest with ventricularfibrillation. He survived a prolonged resuscitation and was found to have ananomalous left coronary artery arising from the right coronary sinus.Conclusion: The importance of recognizing life-threatening CHD early inlife cannot be understated. We present three cases in which patients presentedwith life-threatening CHD long after the neonatal period. There is a uniquechallenge faced in diagnosing CHD in an asymptomatic patient. Although athorough cardiac exam performed on every newborn is critical in detectingCHD, it is not always a reliable screening method. The US Department ofHealth and Human Services recommends that pulse oximetry be included aspart of universal newborn screening, but some studies have found this methodto yield a high false-positive rate. Finding a reliable screening method for CHDhas proven to be an arduous task. Nevertheless, it is of the utmost importancethat primary care physicians have an awareness of these rare and potentiallylife-threatening cases of CHD, regardless of the child’s age or lack of classicsigns and symptoms.
181
EXPANDINGTHE PHENOTYPE OF DISTAL PARTIALTRISOMY 6q
Mumphrey CG, Zeringue A, Rivera D, Zambrano R. LSUHSC, NewOrleans, LA.Case Report: We present an infant born vaginally at 36 weeks gestation as aresult of a consanguineous mating. Genetics evaluation was requested due tomultiple congenital anomalies and parental consanguinity.A single nucleotide polymorphism (SNP) array was sent. In addition toidentifying long contiguous regions of homozygosity in multiple chromo-somes consistent with common descent, it revealed a 49.35MB terminalduplication of 6q22.31-qter. Concurrent cytogenetic analysis discovered anunbalanced rearrangement between chromosomes 6 and 14, resulting in apartial trisomy 6q22.31 and partial monosomy 14p11.2.Our patient’s phenotype is consistent with the commonly described featuresof distal partial trisomy 6q in the literature, including microcephaly, dys-morphic facies (ocular hypertelorism, bilateral epicanthal folds with down-slanting palpebral fissures, peri-orbital fullness, short nose with a flat nasalbridge and anteverted nares, carp shaped mouth) and short neck. Additionalfeatures are global developmental delay, pre and post-natal growth retarda-tion, cardiovascular, renal, genital, skeletal and CNS anomalies. Our patient’sphenotype also includes findings that have not been commonly reported.These uncommon findings include persistent left superior vena cava, con-genital knee dislocation associated with developmental dysplasia of the hip
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 423
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

and skeletal anomalies including 11 pairs of ribs with synostosis betweenthe left 4th and 5th ribs, L1/L2 hemivertebrae and a short left tibia and fibula,providing additional features that help further delineate the phenotype.In this case a regular karyotype would have allowed identification of thechromosomal aberration responsible for her phenotype, but the use of newermolecular technologies such as single nucleotide polymorphism (SNP) arrayallow us to better define the breakpoints and the genes involved, therebyimproving our understanding of genotype-phenotype correlations. The iden-tification of extended contiguous regions of homozygosity by SNP array is alsoimportant, especially in cases where autosomal recessive disorders are con-sidered in the differential diagnosis.
182
A CASE OF AMENORRHEA AND SHORT STATURE
Paccione R, Hutchins K, Spiller C. LSU Health Sciences Center, NewOrleans, LA.Case Report:Introduction: Turner syndrome is a chromosomal abnormality that affectsfemales. It most often presents as short stature, amenorrhea and early lossof ovarian function. The case below details a new diagnosis of Turnersyndrome.Case: A 16 year old female initially presented to clinic with complaints ofamenorrhea and headache. She has never had a menstrual cycle, although hermother started menses at the age of thirteen. Vital signs were: blood pressure136/86 mm Hg, heart rate 108 bpm, respirations 20/min, height 59.4 in (4 feet11 inches), weight 156 lbs (3% on growth curve for stature, 90% on growthcurve for weight for girls age 2-20), BMI 31 kg/m2 (96% on growth curve forBMI for girls age 2-20) . Remarkable physical exam findings included shortstature, abdominal obesity, Tanner stage three breasts and pubic hair, broadchest and acanthosis nigricans noted on her neck fold. Pertinent laboratoryfindings included TSH 3.54 mIU/L, HgbA1c 6 %, triglycerides 162 mg/dL,total cholesterol 198 mg/dL, LDL 126 mg/dL, HDL 40 mg/dL, testosterone15 ng/dL which was consistent with Tanner stage II, prolactin 16.5 ng/mLconsistent with Tanner stage II-III, FSH 71.2 mIU/mL and LH 23.5 mIU/mLwhich were both consistent with a postmenopausal female. A pelvic ultra-sound showed a small uterus measuring 3.9cm� 1cm� 1.8cm, as well as theabsence of ovaries. A CT of her head showed no significant intracranial find-ings. An echocardiogram was normal. Karyotype revealed 45, X consistentwith the clinical diagnosis of Turner syndrome. A bone age test revealed de-layed bone age and the patient is following up with endocrine to start growthhormone injections.Conclusion: Turner syndrome affects 1 in 1500-2500 females. Diagnosis isoften based on a combination of physical exam findings and genetic chro-mosomal analysis. These findings include webbing of the neck, a low pos-terior hairline, broad chest, small mandible, epicanthal folds, short stature andamenorrhea. Turner syndrome is associated with cardiac defects, hypertension,hyperlipidemia, abnormal thyroid function and renal malformations. Thediagnosis tends to occur prior to the onset of puberty; however this patientwas not diagnosed until puberty. Turner syndrome should be included in adifferential when presented with a patient with amenorrhea and short stature.
183
DIAGNOSIS OF LOEYS-DIETZ SYNDROME IN THENEONATAL PERIOD
Patrick J1, Price E1, Webb L2, Lacassie Y1. 1LSUHSC-New Orleans, NewOrleans, LA and 2LSUHSC-New Orleans, New Orleans, LA.Case Report: Loeys-Dietz Syndrome (LDS) is an autosomal dominantdisorder described by Loeys et al. in 2005. It is characterized by aggressiveaortic and arterial aneurysms and a Marfanoid phenotype. LDS type I mayalso have bifid uvula/cleft palate, hypertelorism and craniosynostosis. It isdue to mutations in the TGFBR1 or 2 genes. We report a premature neo-nate born with some unusual features. The diagnosis of LDS was raised aftermeeting his mother who presented, until then, an undiagnosed disorder. Hav-ing had limited prenatal care, she presented with advanced cervical dilation anddisclosed a history of multiple abdominal aneurysms.The proband, a 34 6/7 WGA male was born to a 25yo G4P0121 mom viaemergent C-section. Due to RDS, he was admitted to the NICU. On exam,macrocephaly, hypertelorism, arachnodactyly, pectus excavatum and hyper-
extensible joints were noted. Imaging showed sacral agenesis, bilateral con-natal and subependymal cysts, and a suspected arachnoid cyst. aCGH requestedthe day of delivery, before meeting his mother, was reported as normal. TheNB was transferred to a tertiary care facility for persistent pulmonary hy-pertension. Echocardiogram revealed a moderate PDA. Abdominal ultra-sound was negative for aneurysms. The examination of his mother revealeda repaired bifid uvula, hypertelorism, and a Marfanoid phenotype with longfingers and joint hypermobility. Further studies showed hepatic, renal andsplanchnic aneurysms, aortic root dilation and mitral valve regurgitation.Sequencing analysis showed a heterozygous deletion in the TGFBR1 gene,confirming the clinical diagnosis of LDS, in the mother.Our patient exhibits some of the phenotypic features of LDS, but also someunreported such as sacral agenesis, and connatal and subependymal cysts.Due to the aggressive nature of the aortic and arterial aneurysms, with poorvital prognosis and high mortality during delivery, it is of utmost impor-tance to diagnose this disorder early in life. The early diagnosis in this patientwill allow close follow up and appropriate interventions on the baby and hismother. Losartan was recommended to his mother to decrease the progressionof the aneurysms through an inhibitory effect on the TGF-A activity. She wasreferred to the vascular surgeon and other specialists.
184
CARDIO-ANKLE VASCULAR INDEX IN CHILDREN
Philip R, Alpert B. University of Tennessee, Memphis, TN.Purpose of Study:
1. To establish the first baseline Cardio-ankle vascular index (CAVI)scores by age and gender for children aged 10-18 years.
2. To compare CAVI scores between 3 different ethnic groups- Caucasian(white), African-American(black) and Hispanic populations to test thehypothesis that the CAVI scores in blacks are higher than in the his-panics and whites.
3. To compare CAVI scores between the obese and non-obese childrenin order to test the hypothesis that the extent of arterial changes isgreater in obese children than in normal children.
Methods Used: Study subjects were 294 children, obese (BMI 985th per-centile for age) & non-obese(BMI between 5th and 85th percentile); white,black or hispanic, from 10-18 years old. The VaSera VS-1500N machine wasused to measure CAVI scores. ANCOVA was used to compare the adjustedLS means between groups. SAS version 9.2 was used for data analysis.Summary of Results: Of the 294 children, there were 133 males and 161females of which blacks, whites and Hispanics comprised 90, 101 and 103subjects respectively.When controlled for sex, weight and age, CAVI scoresin whites were lower than non-whites. (p = 0.02) Contrary to our hypothe-sis, CAVI values were lower in overweight children compared to normal child-ren when adjusted for age, sex and ethnicity (4.68 vs 5.26, pG0.0001).Conclusions:
1. CAVI scores may be useful in long term intervention studies like dietand exercise and hence may be a cost effective tool in comparison toother non-invasive and invasive markers.
2. The non-white ethnicities have increased CAVI scores; early detectionmay help determine timing for individualized intervention.
3. The negative impact of obesity on CAVI may be related to :a) volume overload in the obese subjects which blunted the impact of
the reflecting waves in the pulse wave contour.b) greater central vessel elasticity and compensatory vasodilatory
mechanisms caused by the increased mechanical work that over-weight bodies perform with activity.
185
ENALAPRIL INDUCED RENAL FAILURE IN A PRETERMINFANT
Pushkas M, Albright J, Shah D. ETSU Pediatrics, Johnson City, TN.Case Report: A 30 4/7 weeks gestation Caucasian female was born byemergent caesarian section due to twin-twin transfusion syndrome with abirth weight of 1920 grams. Recepient twin was intubated and ventilated afterbirth and noted to have poor cardiac function, polycythemia, and hypoten-sion. Initial ECHO showed fractional shortening of 11%. Treatment wasinitiated with Dopamine, Dobutamine and Milrinone was added later. Patient
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
424 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

also underwent partial exchange transfusion. She developed significant me-tabolic acidosis and was treated with normal saline boluses and eventually asodium bicarbonate infusion. On 7th day of life Milrinone, Dopamine, andDobutamine were stopped and Enalapril (0.05 mg/kg) and Digoxin werestarted by cardiologist. Eleven days after starting Enalapril, infant had 3 epi-sodes of borderline low blood pressures, followed a day later by oliguria,creatinine of 2.48, BUN of 56, potassium of 9.3 (in venous blood) and sodiumof 121. Enalapril and Digoxin were stopped, hyperkalemia was treated withGlucose -Insulin drip, Calcium Gluconate, and hyponatremia was treated withsodium infusion at slow replacement dose. Infant showed significant im-provement in 12-24hrs. Follow up ECHO showed improved fractional short-ening of 42%. Infant made a full recovery and was discharged home on allpo feeds.Discussion: Enalapril is occasionally used along with inotropic agents inpreterm infants with cardiac failure to reduce afterload; however it can causerenal failure as it reduces blood pressure and prevent auto-regulation in thekidneys. The dosage of enalapril for preterm infants is not well established.Previous studies have suggested that smaller infants are more prone to ACEinhibitor induced renal failure. This risk is increased by left to right shunt andprematurity. A smaller dose of 0.01 mg/kg of enalapril have been suggested,but it may have low efficacy. Careful evaluation before starting the drug, closemonitoring of blood pressure and urine output, daily measurements of serumcreatinine and electrolytes are of utmost importance.
Lab Tests before, during and after the renal failure
186
INVASIVE PENICILLIUM CHRYSOGENUM INFECTIONIN AN IMMUNOCOMPETENT CHILD
Ramasamy P, Arora A, Custodio H, Estrada B. University of South Alabama,Mobile, AL.Case Report: An 11 month old Caucasian male with ventriculoperitonealshunt (VP) for hydrocephalus and arachnoid cyst presented with intermittentfever for 5 weeks. The temperature was around 100F with highest at 101F andlasted for about 3-4 days per week. He initially had a cough that lasted fora week but otherwise, he had no other symptoms with the recurrences offever. The infant was born full term and had his VP shunt placed at 2 monthsof age. He had been illness free since then. Family history was unremark-able for any immune deficiency, malignancy or autoimmune diseases. He hadno animal exposure, however, he did have significant exposure to aerosolizedchicken manure used in the neighbor’s farm land several weeks prior to on-set of illness. On admission, he looked well and had no abnormal findings.Laboratory tests showed white blood cell count 10,200/mcl, hemoglobin7.7 g/dl, hematocrit 24.1%, neutrophils 45%, lymphocytes 42%, monocytes7%, eosinophils 6%, platelet 565 thousand/mcl, CRP 6.2 mg/dl and ESR71 mm/hr. Blood, respiratory viral and urine cultures, EBV and CMV se-rology, as well as imaging of the chest, abdomen, pelvis and VP shunt wereall unremarkable. A bone marrow biopsy was performed and Penicilliumchrysogenum was isolated from multiple cultures. A comprehensive evalu-ation of his humoral and cellular immune systems did not reveal any sig-nificant abnormality. His HIV serology was nonreactive. He received 6 weeksof liposomal amphotericin B, followed by 6 weeks of itraconazole. Soon afterinitiation of antifungal treatment he became asymptomatic.DISCUSSION: In this unusual case, extensive evaluation for fever of un-known origin revealed invasive Penicillium chrysogenum infection in animmunocompetent infant. Penicillium species, a group of low pathogenic-ity organisms, are widely distributed in the environment and can be found insoil, decaying vegetation, fertilizers, and in air. We hypothesize that theexposure to chicken manure in our patient was a significant risk factor for hisinfection. Although optimal treatment is not known, amphotericin B seems to bethe most effective antifungal drug. Based on our experience with this pediatricimmunocompetent patient, a 12-weeks course of therapy with an antifungaldrug combination was effective in leading to resolution of his symptoms.
187
HYPERBARIC OXYGEN THERAPY IN THE TREATMENT OFDECUBITUS ULCERS COMPLICATED BY REFRACTORYOSTEOMYELITIS IN THE PEDIATRIC PATIENT
Sexton TD, Wright LA, Jubran I. University of South Alabama, Mobile, AL.Case Report: Decubitus ulcers are an uncommon problem in the pediat-ric population. They are difficult to treat in spite of traditional wound care.Hyperbaric Oxygen Therapy (HBOT) is a treatment in which a patient breathes100% oxygen while inside a chamber pressures higher than sea level and isused for the treatment of problem wounds and osteomyelitis.To present a case of novel treatment of chronic wound in a pediatric patient and todiscuss the therapeutic benefits of hyperbaric medicine in wound care.A 13 year old male with spina bifida was admitted for worsening ul-cer. Despite conservative management, his wound continued to increase insize. On presentation he was febrile. He had under developed lower extremi-ties. There was a 7.5cm � 3.5cm wound above the gluteal cleft. Laboratoryfindings included a CRP 23.2mg/dl. Intravenous antibiotics and wound carewas started. MRI showed osteomyelitis and obturator abscess. Wound de-bridement and drainage was done. This management was continued for sixweeks with worsening CRP and ESR. The lack of improvement led to hy-perbaric therapy treatments. A US Navy Table 66 consisted of 90 minutetreatments, 5�’s/week. Within weeks the CRP and ESR dropped. The patientcompleted a total of 30 hyperbaric treatments, his wound size at dischargewas 1.5cm � 2.75cm, CRP was 1.1mg/dl and ESR was 35mm/hr.Chronic osteomyelitis is characterized by sources of ischemia. HBOT reducestissue edema. It promotes collagen formation and angiogenesis in hypoxicbone and surrounding tissues.Refractory osteomyelitis is chronic osteomyelitis that persists or recurs afterappropriate interventions or when acute osteomyelitis has not responded tosurgical and antibiotic intervention. It can present a high probability ofmorbidity or mortality. It is then that hyperbaric oxygen therapy should beconsidered. Leukocyte mediated killing is restored when the low oxygen ten-sions are increased. Additionally, HBOT has a direct suppressive effect onanaerobic infections.When a child presents with a decubitus ulcer or osteomyelitis, conservativemanagement of antibiotics and wound care should begin. With little im-provement after 6 weeks or the osteomyelitis is refractory, adjunctive HBOTshould be considered.
188
POOR SUCKING AS A PRESANTATION OF SEPTO OPTICDYSPLASIA
Shehata M, Shah D. East Tennessee Statae University, Johnson City, TN.Case Report: A term male, AGA, was born via SVD to a 19 YO, whitefemale with G2 P0 with uncomplicated pregnancy & labor. APGARS were 3,6, & 8 at 1, 5, & 10 minutes. Baby required brief initial respiratory supportwith CPAP and was able to be weaned to room air in 2 days. PE was normalexcept for umbilical hernia & penile length of 1.9 - 2 cm. He has persistentindirect hyperbilirubinemia. Poor sucking was the main complained &feeding maintained mainly by gavage. TSH, serum amino acids & urineorganic acid were normal. CT head showed absent septum pellucidum. MRIalso showed ectopic posterior pituitary & left optic nerve hypoplasia. Workup for panhypopituitarism showed central hypothyroidism & secondary ad-renal insufficiency. New born screen were normal. Baby was started onLevothyroxyl & Hydrocortisone. After 2 days there were an obvious im-provement of baby alertness, sucking & was able to achieve full PO feedingin one week.Discussion:Septo optic dysplasia (SOD) is a syndrome characterized by optic nervehypoplasia, midline forebrain defects & pituitary hypoplasia with variablehypopituitarism usually present with hypoglycemia.We report a case of SOD presented with unexplained persistent weak suckingwith an initial brief neonatal depression. Baby’s symptoms were secondary tothe hormone deficiency. Secondary hypothyroidism is rarely picked up withthe state of screen. Hormone replacement is very important for survival, &normal mental development. Multidisciplinary care is mandatory. Associa-tion with HESX1 gene is found in rare genetic form.Poor sucking needs to be investigated!!!
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 425
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

189
LUPUS-RELATED NEUROLOGICAL CHANGES:RECOGNIZING THE MANY FACES OF SYSTEMICINFLAMMATION
Sittig MP, Kwak M, Stanculescu A, Keane M. Tulane University School ofMedicine, New Orleans, LA.Case Report: A 19 year-old woman with systemic lupus erythematosus(SLE) presented with a two-day history of slurred speech and unsteady gait.Her past medical history was significant for lupus nephritis and cerebritis. AnMRI of the brain demonstrated acute non-hemorrhagic vascular insult as wellas edema concerning for vasculitis. She had thrombocytopenia, leukopenia andelevated ferritin levels. On admission she was treated with low-dose aspirinand mycophenolate. Methylprednisolone was added per lupus flare protocolas her neurologic status continued to decline, and mycophenolate was re-placed by cyclophosphamide.The patient experienced a period of symptom improvement, but later re-gressed. She developed recurrent fevers, pancytopenia, and worsening of hercognitive status despite therapy. Ferritin peaked over 4000mg/dL triglycer-ides and soluble IL2 were elevated, and NK cell function was decreased.Bone marrow biopsy showed numerous hemophagocytic histiocytes, fulfill-ing five of eight criteria needed for diagnosis of hemophagocytic lymphohis-tiocytosis (HLH). She was started on etoposide and dexamethasone. Hermental status slowly began to improve.DISCUSSION: HLH is an increasingly recognized complication in SLE aswell as other rheumatologic diseases. Its pathophysiology is not well under-stood, but reflects uncontrolled immune activation with increasing numbersof phagocytosing histiocytic cells infiltrating organs such as the bone mar-row, liver, spleen, lymph nodes, and brain.Distinguishing HLH from lupus cerebritis is challenging. In HLH, more thanone-third of patients will present with neurologic symptoms, including sei-zures, irritability, decreased level of consciousness, cranial nerve palsy, andataxia. Diagnosis is made by identifying five of eight of the following criteria:fever, splenomegaly, cytopenias affecting at least two of three lineages in theperipheral blood, hypertriglyceridemia and/or hypofibrinogenemia, hemo-phagocytosis in bone marrow, spleen, or lymph nodes, low or absent NK-cellactivity, hyperferritinemia, and high levels of sIL-2r. Recognition of HLH as apotential diagnosis is important as treatment differs and there is a highmortality rate if not treated promptly.
190
UNCOMMON PRESENTATION OF HENOCH-SCHONLEINPURPURA IN 5 YEAR OLD FEMALE
Subedi L, Jubran I. University of South Alabama Children’s & Women’sHospital, Mobile, AL.Case Report: This is a 5 year old female previously healthy who presentedwith 5 days of bumps all over her body with one lesion on foot, bruises onher arm. 5 days prior to that she complained of pain in her legs so her parentstook her to PCP where she was given Ibuprofen and the pain resolved thenext day. The lesions on dorsum of her left foot gradually enlarged and started
to drain. She also spiked a low grade fever. Mom noticed some bruise onher arms so she was brought to EC where labs showed increase WBC, CRP,PT, INR, D-dimer. So, with clinical presentation and lab finding sepsis wassuspected and she was admitted for IVantibiotics. Next day she started to c/osevere abdominal pain with distention, guarding and decreased bowel sound,blood was seen in her stool and heme occult was positive and the foot lesiongrew GAS with negative B/C. ACTabdomen was done which showed diffuseedematous bowelwall thickening with areas of enhancement involvingmultipleintermittent loops of small bowel and ascending colon. Surgery was consultedfor acute abdomen and recommended observation.The patient was kept NPO and her albumin level was very low so TPN wasstarted. On the third day of admission she started to have red color urine withclots. As her PT, INR and D-dimer were consistently elevated and with thenew onset hematuria, we decided to give FFP and transfer her to PICU forclose observation. During her stay in PICU she was still the same clinically.On the second day of PICU she developed rash on her left hand with swellingboth disappeared the next morning. Her hematuria was still the same, ab-domen was not getting better, her albumin went up and she was transferredback to the floor. After two days of transfer she developed palpable, non blanch-ing, petechial rash over her legs with left ankle swelling suggestive of HSPand she was started on steroid after which she improved significantly, also herabdominal symptoms and the hematuria disappeared.
191
SEVERE CONGENITAL ANOMALIES ASSOCIATED WITHMETHOTREXATE AND MISOPROSTOL FAILED INDUCEDABORTION
Subedi L, Martinez J. University of South Alabama Children’s & Women’sHospital, Mobile, AL.Case Report: A 36+5 wk Caucasian female infant was born with multi-ple congenital anomalies to a 25 yr old G2-P0-A1 mother. According to themother she had a prenatal ultrasound ( US ) at 6 week gestation for suspectedpregnancy and showed a product of conception. With the intention of ter-minating the pregnancy, she was given one IM dose of Methotrexate and oralMisoprostol at 7 week gestation. The mother had a negative US one monthlater but a urine pregnancy test remained positive. A pregnancy test was re-peated at 3 month gestation and it was negative but a month later both a urinepregnancy test and a US were repeated and found to be positive and at thesame time she noticed increased abdominal girth. The US showed multiplefetal anomalies. The pregnancy was continued and the infant was deliveredvia spontaneous vaginal delivery. At birth the baby had a weight of 1456 gram(G3%ile), length of 43 cm (G3%ile), HC 28.5 cm (G3%ile). Her APGAR scoreswere 4 @ 1min, 6 @ 5 min and 7 @ 10 min. She was intubated in the deliveryroom for respiratory distress and Surfactant was given. On examination shehad multiple anomalies including a malformed skull, microcephalus, low sethypoplastic ears, dysmorphic facial features with micrognathia, prominenteyes, shallow supraorbital ridges, hypertelorism, short palpebral fissures, mi-crophthalmia and broad and depressed nasal bridge. Her thorax and torso wereshort. She also had short digits with syndactyly, under developed foot bi-laterally with a single toe and anteriorly displaced anus. Chest x-ray showed‘‘handlebar’’ clavicles and thinning and fragmentation of multiple bilateralribs, hyperinflated lungs, cardiomegaly and a narrow thoracic cavity. A CTofthe head showed multiple osseous defects along with enlarged lateral andthird ventricles. An echocardiogram showed 2mm PDA, a small PFO with lowvelocity left to right shunting, mild right atrial and ventricular enlargement.Abdominal US showed small amount of ascites, and normal kidneys.This patient presents with multiple anomalies consistent with a teratogeniceffect of methotrexate and misoprostol. Symmetric craniofacial and limbabnormalities suggest that a characteristic phenotype could be recognized ininfants prenatally exposed to these drugs.
192
RARE BRAIN TUMOR DISGUISED AS ATAXIA IN A 23MONTH OLD MALE
Wright L, Richerson J. USA, Mobile, AL.Case Report: Ataxia is a common presenting symptom in healthy children.When parents note unsteadiness of gait, the physician must consider the longlist of benign and serious causes of acute ataxia.
Ectopic posterior pituitary
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
426 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

We present this unusual case of ataxia in an otherwise healthy 23 month oldmale and discuss a rare pediatric brain tumor.A 23 month old male presented with a five day history of unsteady gait andtwo day history of vomiting. His vital signs were stable and he was in no acutedistress running around with obvious ataxia. Cranial nerves were intact andpapilledema was not appreciated. He had 2+ deep tendon reflexes andstrength was 5/5 in all extremities.A comprehensive work up including a complete blood cell count and serumelectrolytes were all normal. Computer tomography brain showed an ill-defined linear hyperdensity with hydrocephalus He was started on IV deca-dron. Magnetic resonance imaging showed a large fourth ventricle mass withhydrocephalus with mass effect on the pituitary gland and optic chiasm. Atumor biopsy with ventriculostomy and ventriculoperitoneal shunt placementwas done.Pathology report returned as Atypical Teratoid Rhabdoid Tumor.Ataxia is a challenging complaint. The difficulty increases the younger thepatient and suspicion must be maintained for more serious causes. Theclassic symptom of an intracranial neoplasm is headache. Most complain of achange in headache pattern or vomiting. Weakness, seizures and syncopemay occur.Atypical teratoid rhabdoid tumor (AT/RT) is a rare tumor that comprises 2-3%of tumors in children. They are usually diagnosed in childhood with mostcases in children less than 3 years old. Two-thirds are located in the posteriorfossa and up to 30% are disseminated upon presentation. In the United States,it has an incidence of 3 children per 1,000,000.Prognosis is poor with a mean survival of only 6 months. Optimal treatment forthis very rare tumor still remains unclear. A combination of surgery, chemo-therapy and radiation therapy are usually used, however a clear consensus hasnot been reached.Acute ataxia is a common complaint. It is crucial to determine whichsymptoms are concerning and require further investigation. Our case high-lights the importance of taking a thorough history and physical exam as thisvery rare brain tumor presented disguised as ataxia.
Joint Plenary Poster SessionPerinatal Medicine
5:00 PMThursday, February 21, 2013193
HYPERCAPNIC ACIDEMIA: RISK FOR SEVEREINTRAVENTRICULAR HEMORRHAGE IN EXTREMELYPRETERM INFANTS
Alrifai W1, Eyal F1, Whitehurst R1, Kua K1, Martino A2, Zayek M1.1University of South Alabama, Mobile, AL and 2University of SouthAlabama, Mobile, AL.Purpose of Study: In extremely low birth weight infants (ELBWI), thesafety of minimal ventilation and its consequent permissive hypercapniaduring the first days of life is yet to be determined. We wanted to establishwhether permissive hypercapnic acidemia is a risk factor for severe intra-ventricular hemorrhage (IVH) in ELBWI.Methods Used: In order to isolate the effects of hypercapnic from meta-bolic acidemia, ELBWI (n=580), born at a gestation G28 weeks with birthweight G 1000 g, were classified into two groups, ‘‘Metabolic acidemia’’(n=289) and ‘‘No-metabolic acidemia’’ (n=291) groups.Summary of Results: In all ELBWI, the predicted odds with its 95%confidence interval for severe IVH were 2.76 (1.61-4.74) for each 0.1 unitdecrease in levels of arterial pH. In the ‘‘No-metabolic acidemia’’ group,higher levels of arterial carbon dioxide (PaCO2) and lower levels of ar-terial pH were associated with increased risk for severe IVH. This relation-ship was level-dependent. In the ‘‘Metabolic acidemia’’ group, however,neither higher base deficit nor higher PaCO2 levels were significant.Nevertheless, acidemia remained inversely associated with the risk forsevere IVH.Conclusions: In ELBWI, acidemia, hypercapnic or metabolic, is a risk factorfor severe IVH. The strategy using mild permissive hypercapnia (45-55 mm Hg)in ELBWI should be avoided during the first 48 hours of life, mainly if
it is associated with acidemia. Safety of corrective measures for metabolicacidemia is yet to be determined.
194
GENDER SPECIFIC MORBIDITY TRENDS IN PRE-TERMBORN NEONATES
Banga G, Chennasamudram S, Sheehan C, Vasylyeva T. TTUHSC, Amarillo,Amarillo, TX.Purpose of Study: According to the USA Center for Disease Control andPrevention, more than a half million babies in the United States are bornpremature each year. Infants born preterm remain vulnerable to many com-plications, including respiratory distress syndrome, chronic lung disease,injury to the intestines, a compromised immune system, cardiovascular dis-orders, hearing and vision problems, and neurological insult.Objective of this study was to identify gender differences in adverse outcomesamong premature and low birth weight born babies.Methods Used: A retrospective chart review of general pediatric clinicrecords (Texas Tech University Health Science Center at Amarillo Pediatricdepartment and private clinic ) was conducted for children and adolescentswhowere born premature at or G 37 weeks gestational age and /or G2500gms.All children 10-21 years were reviewed. Charts were identified using theICD-9 code for prematurity or birth weight G 2500gms. Demographic, ma-ternal, family, neonatal and postnatal data were abstracted.Summary of Results: Of the 160 charts reviewed - 62% were males andonly 38% were females. Of all the small for gestational age (SGA) babies,with a birth weight G 10th percentile, the incidence was higher among thefemale babies (66% vs 33%), most of the male babies although pre-term wereborn as appropriate for gestational age (AGA) . The incidence of complica-tions associated with prematurity were all found to be at a higher incidence inmale babies viz. jaundice- (64% vs 35%), metabolic issues- (59% vs 40%),sepsis- (52% vs 48%) , intracranial hemorrhage (ICH) - (75% vs 25%),hypertension (HTN)-(62% vs 37%), respiratory distress syndrome (RDS)-(60% vs 39%).Conclusions: Among pre-term born children gender related health dis-parity exists. Most males, although born AGA, had a higher incidenceof prematurity and consequences requiring healthcare support comparedwith females. Girls had higher probability to be born SGA, but had lesscomplications.
195
NEWBORN WITH POSTERIOR FOSSA ABNORMALITY
Bennie L, Shah DS. ETSU Quillen College of Medicine, Johnson City, TN.Case Report: A 39-week gestation female was born to a 44-year-old pri-migravida mother via C-section due to breech presentation and worsen-ing ventriculomegaly. The pregnancy was the result of IVF with donor oocyteand advanced paternal age. Worsening prenatal ventriculomegaly in lastmonth from 1.3-1.7cm prompted the C-section. At birth, physical examshowed a large anterior fontanelle and separation of the sagittal suture withnormal head circumference. CT scan of the head demonstrated mild en-largement of the lateral ventricles and posterior fossa fluid collection withcompression of the cerebellum, most consistent with mega cisterna magna.MRI additionally showed a right parietal lobe developmental venous anom-aly. ECHO and abdominal ultrasound ruled out associated congenital de-fects. A genetics consult was done secondary to advanced maternal andpaternal age, which noted no obvious abnormalities. Patient was dischargedhome on day two of life to be followed up in 2 days by her primarypediatrician.Posterior fossa abnormalities are congenital malformations differentiated bystructural characteristics of the cerebellum, vermis, fourth ventricle, and pos-terior fossa. The cystic malformations in this group include Dandy-Walkermalformation, arachnoid cyst, megacisterna magna, and Blake’s pouch cyst.Neurological consequences of these abnormalities range from normal tosevere based on extent of the structural change and coexisting abnormalities.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 427
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

196
COMPARISON OF METHADONE-EXPOSED VSBUPRENORPHINE-EXPOSED INFANTS REQUIRINGADMISSION TO NICU FOR TREATMENT SHOWS NODIFFERENCE IN LENGTH OF STAY
Bonta BW, DeVoe WM, Shah D, Bharti D. Quillen College of Medicine,Johnson City, TN.Purpose of Study: Retrospective study of infants admitted to NICU @JCMCH who required monitoring/therapy for neonatal abstinence syndromefrom antenatal exposure to either methadone or buprenorphine during thetime period: 1/1/2000 through 8/31/2012. During this time period, 4,866admissions occurred in the NICU at JCMCH, Johnson City, TN; of these, 323(6.6%) comprised infants between 36-40 weeks gestation with symptomaticneonatal abstinence syndrome [NAS]. 182 infants were exposed to eithermethadone [82] or buprenorphine [100] while another 141 infants were ex-posed to other medications associated with symptomatic NAS.Methods Used: Chart reviews of infants 36-40 weeks gestation requiringadmission for NAS exposed to buprenorphine or methadone were evaluatedfor treatments required and length of stay during the period 1/1/2000 through8/312/2012.Summary of Results: Average lengh of stays were equivalent among infantswho required treatment: buprenorphine [24.4 days] vs methadone [25.8 days].Both methadone exposied infants and buprenorphine exposed infants fre-quently required multiple medications to provide adequate sedation whilethey recovered from in-utero exposure.Conclusions: No statistically significant advantage to either maternal bupre-norphine or methadone therapy was noted when comparing infants for re-quired length of stay when sedation therapy required.
197
B-TYPE NATRIURETIC PEPTIDE AS A MARKER OFPULMONARY HYPERTENSION IN PRETERM INFANTSWITH BRONCHOPULMONARY DYSPLASIA
Cuna A, Fineberg N, Sims B. University of Alabama at Birmingham,Birmingham, AL.
Purpose of Study: B-type natriuretic peptide (BNP) is a cardiac biomarkercommonly used in adults for screening and follow up of pulmonary hyper-tension (PH). Currently, there is no evidence that BNP could also be used asa potential marker for PH among infants with bronchopulmonary dysplasia(BPD). This study sought to investigate the relation of serum BNP levels withechocardiographic evidence of PH in infants with BPD.Methods Used: We performed a retrospective chart review from 2010to 2011 of preterm infants with BPD to identify patients who (1) under-went echocardiography for screening or follow up of PH and (2) had serumBNP levels measured within 3 days of echocardiography. Identified in-fants were divided into two groups based on presence or absence of PH asdetermined by echocardiography. Demographics and clinical characteristicswere compared, and mean BNP levels correlated with echocardiographyresults.Summary of Results: Twenty infants (mean gestational age 25.8 T 2 weeksand mean birth weight 825.4 T 353 grams) had 30 paired echocardiogramsand BNP measurements available. Twenty (67%) had PH based on echocar-diography. No significant differences were found in gestational age, birthweight, sex, race, or medications for PH between the two groups. Infants withPH had significantly higher BNP values compared to infants without PH(1032 T 1328 pg/ml vs. 44 T 39 pg/ml, p=0.027). A BNP value greater than125 pg/ml was found to be strongly associated with PH diagnosis.Conclusions: High serum BNP levels appear to correlate with a di-agnosis of PH on echocardiography and could be an attractive bio-marker that may be useful for screening and follow up of PH in infantswith BPD.
198
RISK FACTOR DETERMINATION FOR ADVANCEDRESUSCITATION MEASURES IN Q34 WEEK GESTATIONALAGE NEWBORNS
Dannaway D1, Anderson M2, Hanna A1. 1University of Oklahoma HealthSciences Center, Oklahoma City, OK and 2University of Oklahoma HealthSciences Center, Oklahoma City, OK.Purpose of Study: Approximately 1% of newborns will require advancedresuscitation in the delivery room. While the need for advanced procedures isrightfully anticipated in the preterm and low-birthweight populations, there isno definitive literature on what risk factors might predict the need of ad-vanced neonatal resuscitation in more mature babies. This observationalstudy involves the collection of intrapartum, prenatal, and maternal riskfactors in neonates Q34 weeks gestation who required advanced resuscitationtechniques.Methods Used: This is a observational, prospective case-control study.Salient prenatal, intrapartum, and postpartum information is collected from amother of at least 34 weeks gestational age when her baby requires eitherendotracheal intubation, chest compressions, or resuscitative medication inthe delivery room. The same information is then collected on the mothers ofnext four babies born who do not require advanced resuscitation. The datawill then be compared utilizing both parametric and non-parametric statisticalmethods.Summary of Results: Nine mothers of babies Q34 weeks gestation re-quired advanced resuscitation and consented for information collection, asdid 36 controls. Deliveries that resulted in babies more likely to need ad-vance resuscitation involved older mothers (29.8 y vs. 24.6 y, p= 0.02), fetalbradycardia (p=0.04), significant intrapartum bleeding (p=0.04), emergencysections (p G 0.001), sections with previous labor (p=0.01), and maternalgeneral endotracheal anesthesia (p=0.008). Vaginal deliveries were signifi-cantly less likely to result in babies requiring advanced resuscitation(p=0.02).Conclusions: Certain labor and delivery-related risk factors do seem toportend a greater chance of a late preterm or term baby requiring advancedneonatal resuscitation. Further enrollment may strengthen some of these find-ings, or perhaps determine additional factors that would necessitate theseadvanced measures in the delivery room. These data may serve as the basisfor development of a risk factor scoring system to allow appropriate provi-sion of neonatal-trained personnel for those babies who are at high risk inwhat is now considered a low-risk group as a whole.
MRI demonstrating poster fossa abnormality
Treatment Comparison of Buprenorphine vs Methadone Exposed Infants
*some infants required multiple drugs for adequate sedation
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
428 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

199
CAN A RESIDENT EDUCATIONAL TOOL FORRETINOPATHY OF PREMATURITY IMPROVE PARENTALUNDERSTANDING?
Davidson A, Gong A. UTHSCSA, San Antonio, TX.Purpose of Study: To determine if the use of an educational tool forPediatric Residents would improve parental understanding of Retinopathyof Prematurity.Methods Used: A quality improvement model was used to study the ef-fects of an educational tool that included on-line didactic lessons on ROP forresidents and pictorial forms with scripts for parental education. Pediatricresidents were given access to the online educational tool with a pre- andpost-test. Laminated, color-coded pictorial forms with scripted messageswere made available in the NICU for Pediatric residents to use in discussionswith parents. Residents then provided information to parents at prescribedintervals: before first ROP exam, after each exam, before laser treatment ifneeded, and before discharge. A survey that included a likert scale of 1-10 ofgeneral knowledge of eye disease and open-ended questions about knowl-edge of ROP was given to parents of VLBW infants in our follow-up clinicbefore and after the intervention (resident training).Summary of Results: Thirty-one residents took the pre-test with a meanscore of 55T12; post-test scores (n=24) were 78T15 (pG0.001). Initial surveysof parents rated understanding of their child’s eye disease at 4.9 T1.2; thisincreased significantly to 6.9 T 2.2 (p = 0.018) after the intervention started.Conclusions: The use of a standardized educational tool for residents im-proved their knowledge about ROP as well as parental understanding of acondition that has been difficult for them to grasp.
200
CHARACTERISTICS AND NATURAL HISTORYOF TRISOMY13 AND 18
Dereddy NR, Upadhyay K, Dhanireddy R, Talati AJ. UTHSC, Memphis, TN.Purpose of Study: Historically Trisomy 13 and 18 are considered lethal,but data on the natural history of these disorders are scant. There are nostudies to our knowledge looking at the percentage of infants with thesedisorders that get discharged home from the NICU. Hence we studied the 1)Characteristics and natural history of infants with Trisomy 13 and 18 whilein the NICU.2) Factors that predict survival to discharge from the NICU.Methods Used: This is a retrospective study of infants with a confirmeddiagnosis of Trisomy 13 and 18 born at The Regional Medical Center in thepast 20 years. Fisher exact test and t-test for independent samples wereperformed.Summary of Results: Out of 107,088 live births in the past 20 years, therewere 14 neonates with Trisomy 18 and 12 with Trisomy 13. Clinical char-acteristics are described in the table. Out of the 26 infants, 16 expired in theNICU; 2 died on the first day of life, 5 within the first week, 8 within 2 weeksand 15 by 1 month of life. On comparing the infants that survived to dis-charge versus those that did not, the survivors had a higher mean birth weight(2343g vs 1641g:pG10.5) and higher mean gestational age (38.1wks vs33.6 wks:pG0.01). Also a higher percentage of infants that survived to dis-charge were female (80% vs 62.5%), black race (80% vs 56%) and not placed
on mechanical ventilation (60% vs25%), although these were not statisticallysignificant.Conclusions: In our cohort, a significant number (38.5%) of infants withTrisomy 13 and 18 survived to discharge. 50% of NICU deaths occurred inthe first 2 weeks and 94% in the first month of life. These data are helpfulfor clinicians and families to consider in the optimal management of pa-tients with these lethal trisomies.
201
EPIDEMIOLOGYOF INVASIVE GROUP B STREPTOCOCCUSSEPSIS IN A LEVEL III NEONATAL UNIT - A 20 YEAREXPERIENCE
Dolapo O, Dhanireddy R, Talati AJ. University of Tennessee Health ScienceCenter, Memphis, TN.Purpose of Study: To determine the GBS infection rates, associated mor-bidity and mortality and to describe the demographic trend of the disease inthe last two decades of evolving prevention strategies.Methods Used: A review of the institution perinatal database for all GBSpositive blood culture cases in the last 20 years - period January 1st 1990 toDecember 31st 2009. There was classification of cohorts into two basicperiods of 1990 - 1999 (the initial cohort) and 2000 - 2009 (latter cohort).Comparison of incidence rates of early and late onset GBS sepsis, demo-graphics, mortality and associated risk factors were described in the twocohort groups.Summary of Results: There were 317 cases of invasive GBS sepsisidentified during 1990 - 2009, including 30 deaths. The overall incidence ofinvasive GBS disease significantly decreased from 3.62 per 1000 live births(LB) in 1990-1999 to 2.19 per 1000 LB in 2000-2009 (p=0.0001). Incidenceamong infants from birth through 6 days also significantly decreased from2.94 per 1000 LB by 1999 to 1.34 per 1000 live LB by 2009 (p=0.0001).Incidence among infants aged 7 through 111 days has increased over the twoperiods (0.68 vs. 0.84 per 1000 LB), however not significant statistically(p=0.754). The mortality rates were 10.5% and 7.3% in the initial and lat-ter cohorts respectively.Conclusions: Overall incidence of neonatal group B streptococcal infec-tion has been in decline in the last two decades in our hospital, particularlyamong infants from birth through 6 days. This reduction possibly reflects thebenefit of evolving prevention guidelines and the recommendation of intra-partum antibiotic prophylaxis in the last decade
202
PHOCOMELIA AND THROMBOCYTOPENIA IN A NEONATE
Gupta D, Shah D, Kalwinsky D, Psychogios A, Bradley J. East TennesseeState University, Johnson City, TN.Case Report: A term male neonate presented on day of life (DOL) 0 withpetechiae and purpura on the lower extremities born via C- section with an-tenatal diagnosis of phocomelia and prenatal growth deficiency with APGARsof 8, 9 at 1 and 5 minutes respectively. Mom was 26 yo G1P1 white femalewith hypothyroidism and mitral valve prolapse on multivitamins and levo-thyroxine prenatally. Prenatal labs normal. Mother denied smoking,alcoholand drug abuse. Family history positive for cardiac disease and hyperten-sion,otherwise non-contributory. Physical exam findings include short stat-ure (G2%), brachycephaly, hypertelorism, low set posteriorly rotated ears,nuchal skin folds, systolic ejection murmur along the left sternal border,bilateral upper limb phocomelia, thumbs present, dorsal lymphedema of feetand bleeding at umbilical catheter insertion sites. Initial labs showed symp-tomatic thrombocytopenia (platelets 9000), hemoglobin 11g/dL, white cellcount 35,600/uL, 44% neutrophils, 4% bands, 42% lymphocytes and 37%nucleated red blood cells.Normal coagulation studies. X ray showed absenthumerus, radius and ulna and no other skeletal abnormalities. Renal ultra-sound normal. Echocardiogram (DOL 0) showed patent foramen ovale ver-sus small secundum atrial septal defect, 5 mm patent ductus arteriosus (PDA),small mid muscular ventricular septal defect (VSD), mild biventricular hy-pertrophy and mild tricuspid regurgitation. Echocardiogram (DOL 6) showed1 mm PDA, persistent VSD and peripheral pulmonic stenosis. Chromosomebreakage analysis negative for Fanconi’s syndrome. Microarray analysisshowed 357.73 kb loss from 1q21.1 implying susceptibility for thrombo-cytopenia absent radii (TAR) syndrome.Patient was initially receiving
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 429
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

bi-weekly platelet transfusions which were weaned to weekly transfusions byDOL 20.Upper limb abnormalities along with nuchal translucency have abroad differential. Hence,while evaluating infants with phocomelia, it is im-portant to obtain history of maternal drug exposure,initial complete blood cellcount (CBC) to look for any abnormalities as highlighted in our case, chro-mosome breakage analysis in cases with anemia noted on the CBC or withpresence of thumb anomalies. It is important to obtain a microarray analysisif patient is thrombocytopenic to rule out TAR due to high mortality frombleeding despite adequate platelet support.
203
TRENDS IN MATERNAL AND INFANT COMPLICATIONSFOR HISPANIC WOMEN (1990-2008)
Halloran DR1, Marshall N2, Caughey A2. 1Saint Louis University, St Louis,MO and 2OHSU, Portland, OR.Purpose of Study: The objective of this study was to determine the trendin maternal and infant complications in a growing Hispanic population inthe Midwest.Methods Used: This is a retrospective cohort study of birth records forall liveborn, non-anomalous singleton infants born between 1990 and 2008to Missouri residents (N=1,407,728). We examined factors associated withincreased risk of perinatal complications. The infant complication variableis a composite of the presence of any complication including low birthweight, macrosomia, low Apgar score, birth trauma, meconium aspirationsyndrome, respiratory distress syndrome, and prolonged length of stay. Weassessed trends over time using ordinary least squares regression analysesafter confirming linear trend analysis was appropriate.Summary of Results: The percent of deliveries to Hispanic women in-creased from 2.2% in 1990 to 9.4% in 2008 (pG0.001). The remaininganalyses included 46,210 Hispanics over the study period. Between 1990and 2008, advanced maternal age increase from 7.0% to 10.1%, high edu-cation decreased from 37.9% to 23.2%, marriage decreased from 26.9%to 52.3%, tobacco use decreased from 14.3% to 4.7%, nulliparity decreasedfrom 42.4% to 33.2%, and more intensive prenatal care increased from47.7% to 52.8%. Maternal complications also increased including elevatedprepregnancy body mass index (28.6% to 51.1%), chronic hypertension(0.2% to 0.5%), diabetes (2.8% to 5.9%), and cesarean delivery (22.6% to25.2%). Percent of infants with perinatal complications increased from2.5% to 5.3%. All of these trends were statistically significant (pG0.001).Conclusions: The percent of Hispanics delivering in Missouri increasedsignificantly between 1990 and 2008. The characteristics of this Hispanicpopulation also changed significantly with increased maternal and perinatalcomplications. Utilizing remote data on Hispanic deliveries may provide aless accurate picture of outcomes in this population.
204
PULMONARY AND NEURODEVELOPMENTAL EFFECTS OFHYDROCORTISONE VS DEXAMETHASONE IN EXTREMELYLOW BIRTHWEIGHT INFANTS - A RETROSPECTIVE STUDY
Kua K1, Zayek MM2. 1University of South Alabama Children’s and Women’sHospital, Mobile, AL and 2University of South Alabama Children’s andWomen’s Hospital, Mobile, AL.Purpose of Study: To compare somatic growth, time to extubation, sur-vival without bronchopulmonary dysplasia (BPD) and neurodevelopmental(ND) disability rates between extremely low birth weight infants (ELBWI)who received hydrocortisone (HC) or dexamethasone (DEX).Methods Used: We included ELWBI, ventilated for 914 days and treatedwith DEX (N=42) from 1998 to 2002 or HC (N=38) from 2004 to 2009.Each eligible infant was matched to 3 controls from the same period forbirthweight, gestational age and survival beyond day of steroid initiation.ND outcome was assessed at 18 months of corrected age using Bailey Scalesof Infant Development (BSID). We defined mental impairment as Men-tal Developmental Index (BSID II) or cognitive/language score (BSID III)G70, and motor impairment as Psychomotor Developmental Index (BSID II)or motor score (BSID III) G70.Summary of Results: Extubation and survival without BPD rates weresimilar between steroid groups. Infants who received DEX had lower weight
gain compare to control at 56 days old (Table). Conditional logistic regres-sion showed that DEX use remained as an independent risk for mental im-pairment (OR: 6.0; 95%CI: 2.1-17). ND outcome in infants in the HC werenot different from their own controls but cerebral palsy rate is lower (Table).Conclusions: HC seems to be a safe alternative as it did not adversely affectsomatic growth or ND outcome. Respiratory benefits such as weaning frommechanical ventilation and survival without BPD were not different be-tween ELBWI treated with HC or DEX. Further studies are needed to con-firm our findings.
205
MATERNAL ENVIRONMENT ALTERS PANCREATICENDOCRINE CELL DEVELOPMENT IN FETAL BABOONS
Panda S3, Quinn A1, Sorrell M1, Nathanielsz P2, Blanco C1. 1UTHSCSA,San Antonio, TX; 2UTHSCSA, San Antonio, TX and 3Driscoll Children’sHospital,Texas A&M, Corpus Christi, TX.Purpose of Study: The fetal and neonatal pancreas show developmen-tal plasticity to their metabolic environment. We have previously demon-strated significant developmental differences in the endocrine pancreas infetal and neonatal baboons (PMID:22723715); we hypothesized that peri-natal environmental exposures will lead to morphological changes on >-A-$pancreatic cells in non-human primate fetuses. The objective of the studywas to examine histological differences in the endocrine pancreas of fetusesexposed to antenatal corticosteroids (ANS), maternal obesity (MO) and ma-ternal nutrient restriction (MNR).Methods Used: Fetal baboons were delivered via c-section at 0.9 gestationto healthy (CTR), MO, MNR or ANS exposed mothers (n=4 group). Con-secutive sections from pancreatic tissue were immunostained for insulin, glu-cagon, and somatostatin. Relative volumes and absolute mass of the microscopicstructures were calculated utilizing the Computer Assisted Stereology Tool-box (CAST) 2.0 system. Plasma insulin and glucagon were measured byELISA. Statistical calculations were performed utilizing SPSS version 17.0.Summary of Results: Birth weight was significantly lower in MNR andMO fetuses compared to CTR and ANS fetuses (pG0.01); however, the to-tal pancreas weight as a percent of body weight was similar between allgroups. Fetal >-A-$ cell percent area comprised 10.3T1.6, 11.7T1.3 and13T2.5 (mean, TS.E.) of endocrine pancreas in CTR animals respectively.Alpha cell percent area was significantly increased in fetuses exposed to ANS(1.7 fold) and MNR (1.8 fold) when compared to CTR fetuses (p=0.01). Betacell area was increased by 1.5 fold and 1.7 fold in MNR and MO exposedfetuses but did not reach statistical significance (p=0.1, p=0.09 respectively).Delta cell percent area was not altered. No differences in baseline fetal plasmainsulin and glucagon were found between groups so far.Conclusions: Fetal pancreatic endocrine cell development is specificallyaltered depending on the type of environmental exposure in non-human pri-mates; these alterations may have long lasting consequences depending on thecell line affected. Whether these changes persist and correlate with meta-bolic derangements remain to be determined.
206
COMPARISON OF OUTCOMES IN PRETERM INFANTSTREATED WITH PORACTANT ALFAVS CALFACTANT- ARETROSPECTIVE STUDY
Murugesan C, Eyal F University of South Alabama, Mobile, AL.Purpose of Study: Background: Neonatal respiratory distress syndrome(RDS) continues to be the leading cause of morbidity in preterm infants born
Characteristics and outcome of infants
* P<0.05 comparing control vs steroid group of same time period
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
430 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

in United States. Although many studies have evaluated the efficacy of sur-factant treatment for RDS, there are only few studies comparing differentnatural surfactants. Poractant Alfa and Calfactant have higher proportions ofsaturated di-palmitoyl phosphatidyl-choline (DPPC) and surfactant protein Bwhich theoretically makes them better choices among the natural surfactants.Objective: To compare the outcomes of two natural surfactant preparations-Poractant Alfa and Calfactant in the treatment of preterm infants less than29 weeks.Methods Used: The study was designed as retrospective study in the set-ting of level IIIb neonatal intensive care unit at University of South Alabama.Preterm babies less than 29 weeks who received surfactant between the years2003 and 2011 were included in study. The use of Poractant Alfa and Cal-factant was not dictated by clinical criteria but based on financial one makingthis a semi randomized setup. The rates of primary outcomes (broncho-pul-monary dysplasia (BPD) and survival) and secondary outcomes (severe intra-ventricular hemorrhage (IVH), pulmonary interstitial emphysema (PIE) andair-leak) were compared between two groups using Chi square analysis. Thecomparison between surfactant in terms of primary outcomes of BPD andsurvival was based on multivariate logistic regression model.Summary of Results: No statistically significant difference in BPD (oddsratio (OR):0.85, 95% confidence interval (CI):0.46- 1.49, P= 0.55) or sur-vival (OR: 1.17, 95% CI: 0.78- 1.76, P= 0.43) were observed between twotreatment groups after adjusting for various risk factors. There was no sig-nificant difference in secondary outcomes like severe IVH (Poractant Alfa8.91% vs. Calfactant 10.62%p=0.43), air-leak (Poractant Alfa 12.4% vs. Cal-factant 14.21%, p=0.47) and PIE (Poractant Alfa 10.85% vs. Calfactant12.83% p=0.41) between the treatment groups.Conclusions: No significant difference in rates of BPD and Survival wereobserved among the premature infants treated with Poractant Alfa or Cal-factant. Complications like severe IVH, air-leak and PIE were also not sig-nificantly different among treatment groups.
207
THE WHOLE NINE YARDS: LISSENCEPHALY IN ANEONATE WITH A PEROXISOMAL DISORDER
Pryor J, Singh P, Apostolos P, Mohon R, Shah D. East Tennessee StateUniversity, Johnson City, TN.Case Report: Term AGA female was born via a scheduled caesarian sec-tion to a 40-year old diabetic mother. Apgar scores were 3 and 6 at 1 and5 minutes, respectively. Minutes after birth, the newborn had recurrent tonic-clonic seizures. Glucose levels were normal. Physical exam revealed dys-morphic features including large fontanelles, high arched palate, lamellarcataracts, and generalized hypotonia. The liver was not enlarged. CT of thehead demonstrated lissencephaly that was confirmed with MRI. Micro-array,postnatal karyotype, and FISH for Miller-Dieker syndrome returned nor-mal. Prenatal amniocentesis had yielded a normal 46, XX karyotype. Lab-oratory abnormalities included urine dicarboxylic aciduria, aminoaciduriaand very long chain fatty acid (VLCFA) defects diagnostic of peroxisomalbiogenesis disorders (PBD). X-rays of the knees showed bony stippling of thepatella. Family history was not informative.Lissencephaly is a malformation of cortical development resulting from de-fective neuronal cell migration, proliferation, or apoptosis. This condition isevidenced by absence of gyri and a thickened cerebral cortex. Infants oftenpresent with microcephaly, developmental delay, and seizures during the firstyear of life. Lissencephaly can be sporadic, syndromic (Miller-Dieker syn-drome), metabolic (PBD) or of mitochondrial etiology. Newborns with PBDstypically have micrognathia, prominent forehead, and malformed nostrils. Todate, there are rare documented associations of lissencephaly and PBDs in-cluding Zellweger syndrome. Stippling of the patella(e) occurs in classic casesand should be differentiated from other etiologies including chondrodyspla-sia punctuata. Diagnosis of PBD etiology is usually suggested by demon-stration of abnormalities on biochemical assays including plasma VLCFAand RBC plasmalogens. In conclusion, the presence of lissencephaly in aninfant with large fontanelle, cataracts, bony stippling, and multiple congeni-tal anomalies, should alert the pediatrician to rule out PBDs due to their sig-nificant morbidity and high mortality. A multispecialty management teamshould include clinical geneticists who can help with the appropriate test-ing and can provide the necessary family genetic counseling.
208
REAL TIME HUMAN MILK ANALYSIS CONTRIBUTES TOMORE COMPREHENSIVE NUTRITIONAL MANAGEMENT
Radmacher PG1, Sparks B1, Lewis S2, Serke L3, Northam AT2, Adamkin D1.1University of Louisville, Louisville, KY; 2Kosair Children’s Hospital,Louisville, KY and 3University of Louisville Hospital, Louisville, KY.Purpose of Study: To evaluate the contribution of onsite human milk(HM) analysis to individualized nutritional management of VLBW infants.Methods Used: Pooled, 24-hour samples of HM were analyzed 1-2 timesweekly and results provided to the health care team. HM was fortified using30 kcal/oz preterm formula (PTF) as directed. Protein (g/k/d) and energy(kcal/k/d) intakes were calculated by adding together the proportional con-tributions from HM and PTF. Demographics, daily intake, growth and labdata were collected from the week prior to fortification (PF) and for 4additional weeks or until discharged or transitioned to primarily formulafeeding.Summary of Results: 14 VLBW infants were included in the analysis. Themedian age at initiation of enteral feedings was 3 days. The median age atfortification was 19 days; 3 of 14 infants (21%) had not yet returned to BWonday 1 of fortification. Weight gain improved from 10.8 T 6.9 g/k/d (PF) to15.1 T 3.4 in week 4 (pG0.02 PF vs. wks 2 and 3); HC averaged 0.8 cm/wkacross the study period. Mean protein intake increased from 1.7 T 0.9 g/k/d inthe PF week to 3.1 T 0.5 in week 4. Mean energy intake rose from 82.8 T 16.8kcal/k/d (PF) to 112.5 T 12.0 in week 4. The proportion of HM (mother’s ownor donor) was reduced from 100% (PF) to a mean of 53% by week 4. Themajority of infants were fed their own mother’s milk; only 2 of 14 were feddonor HM. Mean HM protein content decreased from 1.43 T 0.3 (PF) to 1.36T 0.3 g/dL (wk 4). Energy ranged from 16.9 T 2.3 kcal/oz to 17.4 T 0.8 acrossthe period. Mean BUN (mg/dL) decreased significantly from 14.7 T 9.3 in thePF week to 5.1 T 2.4 in week 2 (p = 0.003), and continued to decline to 3.5 T1.2 by week 4. Mean serum creatinine was stable at 0.4-0.5 mg/dLConclusions: The onsite analysis of protein and energy in pooled HMsamples enabled actual nutrient intake calculations for VLBW infants. Dur-ing the study period, weekly growth approached intrauterine rates but did notallow for catch up growth, most likely due to limited protein and energyintakes. BUN values decreased dramatically during the study period and maysuggest inadequate protein intake.
209
FACTORS ASSOCIATED WITH THE INCREASES IN THEPREVALENCE OF GASTROSCHISIS IN SOUTHERNMISSISSIPPI AND ALABAMA
Salameh M, Whitehurst R, Zayek M. University of South Alabama, Mobile, AL.Purpose of Study: To determine whether the recent increase in gastro-schisis was related to any of the following: particular geographical areas, race,younger maternal age, and marital status.Methods Used: We retrospectively collected 18553 charts of all new-borns admitted to our neonatal intensive care unit (NICU) from 1991-2011.Among these infants, we searched for independent risk factors associatedwith gastroschisis (n=117), using multivariate analysis. In addition, we ob-tained the total number of live births from state health agencies, as wellas the number of births to mothers with the risk factors identified amongour NICU population, which are: teenage, white, non-white, married andunmarried mothers, by county (Baldwin, Clark, Conecuh, Escambia, Mobile,Monroe, Washington, in Alabama and Jackson and Harrisson in Mississippi).We divided the study period in 3 different epochs: 1991-1997, 1998-2004,and 2005-2011. Using chi square test, we compared the prevalence of gas-troschisis among the periods, by counties and by the significant factors foundin the logistic regression, i.e. maternal age, race, and marital status.Summary of Results: After adjustment of maternal risk factors obtainedfrom NICU charts, we found that maternal age G26, white and single mothersremained independent risk factors for gastroschisis. The increase in gastro-schisis occurred in all counties. The prevalence per 10,000 live births hasincreased from 2.28 to 5.35 in the 3 periods (p=0.257) in all regions. Whileit was seen mainly in white mothers during the first period, the increase in theprevalence occurred in white (p=G0.05) and non-white mothers (p=G0.05).Also, the increase in the prevalence of gastroschisis mainly occurred in teen-age (p=G0.05) and unmarried mothers (p=G0.05).
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 431
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Conclusions: In our region, the increase in gastroschisis was similar to pub-lished reports. The increase was mainly seen in non-white, young, and un-married mothers. Further evaluations are needed to identify environmentalrisk factors in this high risk group of population.
210
PACO2 IN RELATION TO OUTCOME IN CONGENITALDIAPHRAGMATIC HERNIA
Salas AA, Bhat R, Dabrowska K, Leadford A, Anderson S, El-Ferzli G,Ambalavanan N. University of Alabama at Birmingham, Birmingham, AL.Purpose of Study: It is important to determine whether higher survivalnoted after use of gentle ventilation in CDH (congenital diaphragmatic her-nia) are due to higher PaCO2 (permissive hypercapnia).Methods Used: Survival rates of infants with CDH from the pre-gentleventilation era (1987-96) and during the current era (2002-2010) were com-pared and analyzed in relation to PaCO2. We analyzed PaCO2 from the firstpostnatal arterial blood gas (ABG) and from the pre-ECMO ABG.Summary of Results: We evaluated 133 CDH cases. PaCO2 e 60 mmHgin the first ABG was associated with higher survival (HR: 2.23; p=0.02). Themean PaCO2 in the first ABG in non-survivors was similar in both eras(83 mmHg vs. 85 mmHg, p=0.87). During the gentle ventilation era, nosignificant differences were observed between the PaCO2 from the firstblood gas and the PaCO2 before initation of ECMO (means 85 vs. 82 mmHg;p = 0.62). Survival of infants with PaCO2 G55 mmHg in the first ABG was84%. Survival of infants with PaCO2 9 88 mmHg before initiation of ECMOwas 11% (Figure)Conclusions: Our data indicate that PaCO2 is useful for risk stratificationin CDH. Better survival with PaCO2 G 60 mmHg in the first ABG may in-dicate absence of pulmonary hypoplasia. A PaCO2 60 - 80 mmHg in the firstABG and before ECMO suggests less severe pulmonary hypoplasia com-patible with survival. Persistence or development of severe hypercapnia(PaCO2 9 80 mmHg) indicates poor prognosis in CDH.
211
ARYL HYDROCARBON RECEPTOR DYSFUNCTIONALNEWBORN MICE ARE MORE SUSCEPTIBLE TOHYPEROXIA-INDUCED INFLAMMATION, OXIDATIVESTRESS, AND ALVEOLAR SIMPLIFICATION
Shivanna B, Jiang W, Wang L, Moorthy B. Baylor College of Medicine,TexasChildren’s Hospital, Houston, TX.
Purpose of Study: Hyperoxia causes bronchopulmonary dysplasia (BPD)in preterm infants. We showed that adult mice deficient in aryl hydrocar-bon receptor (AhR) are more susceptible to hyperoxic lung injury than wildtype (WT) controls due to marked decreases in the expression of cytochromeP450 (CYP) 1A enzymes. Whether AhR protects newborn mice againsthyperoxia-induced alveolar simplification is unknown. Therefore, we testedthe hypothesis that AhR dysfunctional newborn mice have increased inflam-mation, oxidative stress, and alveolar simplification compared to WT new-born mice upon exposure to hyperoxia.Methods Used: One-day old C57BL/6J (WT) and aryl hydrocarbon re-ceptor dysfunctional (AhRd) mice were exposed to air or hyperoxia (FiO285%) for 14 d. Following exposure to air or hyperoxia, the lungs and bron-choalveolar lavage fluid (BALF) of the mice were collected to determine AhRactivation, inflammation, oxidative stress, and alveolarization. Pulmonary AhRactivation was assessed by analyzing the expression of pulmonary CYP1A1, NAD(P)H quinone oxidoreductase-1, and microsomal glutathione S-transferase 1. Lung inflammation was determined by macrophage infiltra-tion and monocyte chemoattractant protein 1 expression, and alveolarizationwas determined by lung morphometry. Oxidative stress was determined byanalyzing protein carbonyls expression in the BALF.Summary of Results: In both newborn WT and AhRd mice, exposureto hyperoxia increased lung inflammation and oxidative stress. However,hyperoxia-induced lung inflammation and oxidative stress was significantlyincreased in AhRd mice compared to WT mice. Likewise, hyperoxia in-creased alveolar simplification in both newborn WTand AhRd mice with thelatter being more significantly affected than the former. Interestingly, acti-vation of the AhR was inversely related to hyperoxia-induced lung inflam-mation, oxidative stress, and alveolar simplification.Conclusions: AhRd newborn mice have increased inflammation, oxidativestress, and alveolar simplification compared to WT newborn mice uponexposure to hyperoxia. Our data suggest that strategies directed towards in-creasing the functional activation of the AhR would be effective in the pre-vention and treatment of BPD in preterm infants.
212
THE VIRTUAL NICU: USING SOCIAL MEDIA TOOLS TOREDUCE STRESS AND INCREASE SATISFACTION INPARENTS OF VERY LOW BIRTH WEIGHT INFANTS
Song C2, Patel RM1, Hunt L2, Gillaspy S1, Willeitner A2. 1OklahomaUniversity Health Sciences Center, Oklahoma City, OK and 2OklahomaUniversity Health Sciences Center, Oklahoma City, OK.Purpose of Study: An ample body of research demonstrates a high prev-alence of depressive symptoms, anxiety and stress among parents of verylow birth weight infants (VLBW). Strong evidence shows that postnataldepression and anxiety negatively impact parental-infant and cognitive de-velopment. A decrease in parental depressive symptoms and anxiety may ul-timately augment the neurodevelopmental health of these high-risk infants. Theobjective of this project is to provide parents with an online resource foremotional support and information which may help them cope with the stressof having a child hospitalized in the NICU.Methods Used: This is a prospective study conducted at a tertiary carepediatric academic center with a level IIID NICU. The population of inter-est is parents of VLBW infants: birth weight of 1500 grams or less.The observational study design is biphasic, with baseline data established inPhase I where the tests will be applied to parents of VLBW infants before theonline support group is available. Phase II will follow immediately, where theonline group will be offered to all parents. Due to its popularity and ac-cessibility, Facebook.com was chosen as the social media site for familiesof VLBW infants in the NICU at Children’s Hospital at OU Medical Center(OU NICU), the University of Oklahoma Health Sciences Center (OUHSC).The outcomes will then be compared, using the data from Phase I as con-trols. Parents in both phases will be asked to complete the Parental StressorScale: Neonatal Intensive Care Unit (PSS: NICU) on admission to and upondischarge from OU NICU. A parental satisfaction questionnaire will also beadministered to the parents at the time of discharge.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
432 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: Currently, we are in the preliminary phase of datacollection. We have enrolled 5 control subjects and are in the process of dataanalysis. We plan to enroll 30 subjects in the control group and 30 subjectsin the study group.Conclusions: We anticipate the introduction of an online networking com-munity will reduce the occurrence or intensity of postnatal stress and/or in-crease the level of satisfaction for parents during the NICU stay of theirVLBW infants.
213
TRANSIENT HYPOTHYROIDISM IN A NEONATE
Velayuthan S, Gungor N, McVie R. Louisiana State University HealthSciences Center, Shreveport, LA.Case Report: A 2-week old Caucasian baby boy was referred to pediat-ric endocrine clinic upon detection of high thyroid stimulating hormone(TSH) by newborn screen (NBS). The infant was born at full term by emer-gency caesarean section secondary to fetal distress. He required short termNICU care for respiratory distress. Family history was remarkable for ma-ternal hypothyroidism and Hashimoto’s thyroiditis diagnosed at age 16. Themother continued to receive levothyroxine during pregnancy. The NBS onday 3 of life revealed a high TSH of 182 uIU/ml. Repeated tests showedsignificantly elevated TSH (Day of life 9 and 13, respectively; TSH=186and 176 uIU/ml). and normal Free T4 (FT4 =1.4 ng/dl ). Thyroid scan withTechnetium 99m showed no uptake in thyroid lodge or ectopically. Thebaby was started on levothyoxine 25 mcg daily. Anti thyroid peroxidase (TPO)(557 IU/ml, normalG9) and TSH receptor blocking antibodies (TRAb) (161 IU/ml,normal G1.5) were elevated. On subsequent follow up TSH levels graduallynormalized and FT4 remained in normal range. By 6 months of age TRAband TPO also normalized. The infant continued to grow and develop well withwell-controlled thyroid tests and no requirement for increase in levothyroxinedose. This patient is presented to highlight the potential diagnosis of transienthypothyroidism in patients with abnormal TSH in NBS. Congenital hypo-thyroidism (CH) due to transplacental antibody transfer accounts for 1-2% ofcases of CH. Investigating both the infant and the mother following a raisedTSH in NBS is important. The identification of infants with transient CH dueto maternal transfer of TRAb is essential for optimizing management duringchildhood (including potential withdrawal of thyroxine replacement in thelonger term) and in any subsequent pregnancy.
214
HUMAN MILK AS THE FIRST FEEDING IS ASSOCIATEDWITH EXCLUSIVE HUMANMILK FEEDING AT DISCHARGEIN INFANTS REQUIRING NEONATAL INTENSIVE CARE
Walker T, Keene S, Patel RM. Emory University School of Medicine, Atlanta, GA.Purpose of Study: Exclusive human milk (EHM) feeding is the ideal dietfor infants and an important quality indicator in the neonatal intensive care unit(NICU). Of infants receiving human milk, only some are successful at EHMfeeding at hospital discharge and health benefits may vary between EHM andpartial human milk (PHM) feeding. The goal of this study is to evaluatedemographic and clinical characteristics associated with EHM at hospitaldischarge in a cohort of EHM and PHM fed infants receiving NICU care.Methods Used: This retrospective cohort study included a consecu-tive sample of all infants discharged to home from two Atlanta NICUs overa 12 month period who received any human milk during the 24 hours priorto hospital discharge. Patient characteristics were compared between EHMand PHM fed infants. Logistic regression, with adjustment for confounders,was used to evaluate early feeding factors associated with EHM at discharge.A pG0.05 was considered significant.Summary of Results: A total of 264 infants met inclusion criteria. EHMinfants had more private insurance (48% vs 19%) and less government in-
surance (51% vs 69%) compared to PHM infants (pG0.01). Prematurity wasmore common in EHM infants (66% vs. 51%, p=0.01). Both groups had asimilar frequency of any enteral feeding by 7 postnatal days (100% vs 98.4%;p=0.15) although the mean age at initial enteral feed was longer in EHMinfants vs. PHM infants (1.5 days vs 0.9 days; pG0.01). EHM infants were morelikely to receive human milk at the first feeding compared to PHM infants(65% vs 32%; pG0.01). After adjustment for gestational age, race, type ofinsurance and center, infants receiving human milk as the initial feeding, com-pared to non-human milk, had a significantly greater odds of EHM feedingat NICU discharge (aOR 3.2; 95% CI 1.7-5.8, pG0.01). In subgroup analy-ses, initial human milk feeding was associated with EHM at discharge interm, late-preterm, and G34wk gestation infants (pG0.01 for each subgroup).Conclusions: Infants receiving human milk as the initial feeding were morelikely to receive EHM at discharge. Improving the use of human milk as theinitial feed may be a potential strategy to increase EHM feeding at dischargein infants requiring neonatal intensive care.
215
INFANT WITH DELETION 4Q32.3-QTER AND BILATERALULNAR DEFICIENCY: A RARE PHENOTYPE OF4Q DELETION SYNDROME
Zeringue A1,2, Mumphrey C1,2, Barkemeyer B1,2, Marble M1,2. 1LSUHSC-New Orleans, New Orleans, LA and 2Children’s Hospital, New Orleans, LA.Case Report: Chromosome 4q deletion syndrome is rare with varying phe-notypes including developmental delay, facial dysmorphism, micrognathia,cleft palate, heart defects, and limb anomalies. Limb defects described in theliterature are typically minor deformities. A few major limb anomalies havebeen reported usually involving the left side. We present an unusual caseof this chromosomal syndrome with some of the classical features of chro-mosome 4q deletion but with more severe bilateral limb malformations thanpreviously reported in the literature. The patient, a full term female, had facialdysmorphism, micrognathia, cleft palate, atrial septal defect, and bilateralupper and lower limb anomalies. Pregnancy was complicated by IUGR, oligo-hydramnios, and maternal cocaine and quetiapine use. The patient’s upperextremity anomalies included shortened humeri, flexion deformity at the el-bows, absent ulnae, hypoplastic metacarpals, and a single digit bilaterallywith well-developed proximal and distal phalanges and absence of the mid-phalange. The second and third toes were overlapping. Chromosome micro-array analysis using a whole genome oligonucleotide array detected a large21.98 Mb deletion of 4q32.3 through terminal 4q35.2 including the geneHAND2.Our patient’s phenotype of deletion 4q32.3-4q35.2 is consistent with previousreports of 4q chromosome deletions but with more profound bilateral limbmalformations. Varying limb defects have been reported with most beingminor reduction deformities involving the fifth digit and nail hypoplasia. Thefew major limb anomalies that have been reported include a shortened hu-merus and reduction deformities involving the ulnar ray such as absent ulna,metacarpals, and phalanges similar to our patient. Most of these major limbdefects reported have been left-sided unlike our patient with bilateral severedefects. Genes in the terminal region of 4q, such as HAND2, have beenimplicated in cardiac, facial, and central nervous system development as well aslimb development. It is likely that the chromosomal region 4q32.3-4q35.2contains gene(s) which play a significant role in ulnar ray development asdemonstrated in our patient.
Joint Plenary Poster SessionPulmonary and Critical Care Medicine
5:00 PMThursday, February 21, 2013216
IMPACT OF GASTRO-ESOPHAGEAL REFLUX (GERD)THERAPY ON SPUTUM MICROBIOLOGY IN CYSTICFIBROSIS ADULTS
Chaudary N, Malik S. UMMC, Jackson, MS.Purpose of Study: Nonacid gastro esophageal reflux disease (GERD)in patients taking acid suppression has been associated with respiratory
Laboratory Results
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 433
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

infections. We hypothesize that adults with cystic fibrosis (CF) and on treat-ment of GERD therapy have higher prevalence of resistant pathogensmethicillin resistant staphylococcus aureus (MRSA), multi- drug resistantPseudomonas ( MDR PA) in their sputum than patient not on GERD therapy.Methods Used: We did retrospective review of adult cystic fibrosis patients.Sputum microbiology was compared in 2 groups of patients, those who wereand were not taking GERD therapy. CF pulmonary exacerbations requiringintravenous antibiotics over previous year was also compared. GERD ther-apy included patients using proton pump inhibitor therapy or H2 blockertherapy. MDR PA included resistance to 2 antibiotic class ( beta lactams,quinolones and aminoglycosides) in 5 years. MRSA included patients ifthey ever had the organism grown in their sputum cultures. Pulmonary ex-acerbations included where intravenous antibiotics were given for treatment.Summary of Results: 33 of 54 patients were on GERD therapy. 22 of 33patients on GERD therapy and 8 of 21 patients not on GERD therapy wereinfected with MRSA. 22 of 33 patients on GERD therapy and 5 of 21 pa-tients not on GERD therapy were infected with MDR PA. 16 of 33 patientson GERD therapy had both resistant micro-organisms as compared to 4 of21 patients who were not on GERD therapy. 20 of 33 patients on GERDtherapy and 7 of 21 patients not on GERD therapy had pulmonary exac-erbations. 12 out of 20 patients who had exacerbations and were on GERDtherapy had resistant organisms compared to 2 out of 7 patients not on GERDtherapy. According to Pearson Chi-square values, there is a statistically sig-nificant (p=0.02) association between GERD therapy and resistant patho-gens in CF patients.Conclusions: GERD therapy may predispose patients to resistant patho-gens. Research has shown that MRSA and MDR PA lead to decline in lungfunction in CF patients.Pulmonary exacerbations trended more frequently in patients taking GERDtherapy however remained statistically non-significant.Alternatives to GERD therapy may help decrease prevalence and incidenceof resistant pathogens in cystic fibrosis adults.
217
MYSTERY SOLVED: A CASE OF RECURRENT LOWERRESPIRATORY TRACT INFECTIONS DUE TOMOUNIER-KUHN SYNDROME
Del Rosario R1, Abu Grara H1, Jou Tindo A2, Khasawneh F1. 1Texas TechUniversity Health Sciences Center, Amarillo, TX and 2Northwest TexasHospital, Amarillo, TX.Case Report: Recurrent lower respiratory tract infections pose a challeng-ing dilemma for clinicians. The possibilities are broad and diagnostic testsat hand have limitations.Case: A 30-year-old female was admitted with community-acquired pneu-monia and was started on intravenous levofloxacin. Her medical history wassignificant for recurrent pneumonias and bronchitis since childhood. Ex-tensive work up in the past was unrevealing. Human immunodeficiency virustesting was negative. Immunoglobulin, complement levels and lymphocytesubpopulations were normal. A chest computed tomography angiogram doneon admission was initially reported as negative but on closer review showeddilation of the trachea and main stem bronchi with a tracheal diverticulum inthe upper right side of the trachea. She was diagnosed with tracheo-bronchomegaly (Mounier-Kuhn syndrome (MKS). She responded well toantibiotic therapy and discharged home on oral levofloxacin.Discussion: MKS is a rare congenital condition characterized by dilation ofthe trachea and major bronchi. It is more common in males and usuallypresents in the third or fourth decade of life. Autopsy studies demonstrateelastic fibers and smooth muscle atrophy in the trachea and first to fourthorder bronchi. Despite enlarged airways, patients with MKS have inefficientcough and impaired mucociliary clearance. There are 3 subtypes of the dis-ease; 1st, the trachea and major bronchi show subtle diffuse enlargement;2nd, the enlargement becomes more obvious with bizarre eccentric configu-ration and diverticula formation; 3rd, sacculation and diverticulosis extend-ing to distal bronchi. The walls of acquired tracheal diverticula in MKSconsist of respiratory epithelium only. This distinguishes them from con-genital diverticula, where walls consist of purely tracheal layers. Chest CTscan is the diagnostic modality of choice. It shows the above changes andenables accurate measurement of airway diameters. The treatment of MKSin its early stages is supportive consisting of physiotherapy to assist in ex-
pectoration and antibiotics to treat lower respiratory tract infections. In ad-vanced cases, Y-shaped tracheobronchial stenting and lung transplantationhave been used.
218
INPATIENT ARTERIAL BLOOD GAS USE: WHY LESS ISSOMETIMES MORE
DellaVolpe J, Romero C, Cerreta K, Nielsen N. Tulane Internal Medicine,New Orleans, LA.Purpose of Study: The implementation of a protocol for arterial bloodgas (ABG) measurement results in fewer unnecessary tests and greater costsavings. We hypothesize that development and use of a protocol will char-acterize the indications for ABG measurement and identify unnecessaryABGs.Methods Used: We adapted previously published guidelines to the needsand practices of our institution by incorporating the inputs and suggestions ofrespiratory therapists and critical care faculty. Five parameters were demar-cated for ordering ABGs: hemodynamic instability, oxygenation, metabolicacidosis/alkalosis, respiratory distress, and ventilator adjustments. ABGs thatdid not fit these parameters were marked as ‘‘other/unknown’’. Exclusioncriteria included age G 18, stroke patients, and venous blood gases.Summary of Results: In a 6 week period, 2098 ABGs were measured. Ofthese, 356 met exclusion criteria and an additional 143 were improperlycoded. 187 ABGs were performed for oxygenation issues, of which 75 hada PaO2 9 75. 82 ABGs were measured for metabolic acidosis/alkalosis ofwhich 47 had either normal parameters or primary respiratory acidosis/al-kalosis. Of the 179 ABGs done for respiratory distress, 122 had normal orlow PaCO2. There were 771 ABGs ordered on mechanically ventilated pa-tients. Of these ABGs, ‘‘daily ABGs’’ accounted for the highest number ofnormal blood gases (56), while ABGs taken after change in FiO2 had thehighest percentage of normal parameters (27.6%).Conclusions: We identified 311 of the 1599 properly coded ABGs wherethe indication was unknown and an additional 332 gases where the indica-tion was known but the ABG was within normal parameters. These findingssuggest that over 40% of ABGs taken in a 6 week period may have beenunnecessary. At our institution, ABGs are billed at a minimum of $1051. Inthe 47 days that data was collected, the 643 potentially unnecessary tests ac-counted for at least $675,793 in healthcare expenditures. The limitation ofthis study is that it offers only an approximation of unnecessary ABG mea-surement as ABGs are ordered in clinical contexts that are impossible to fullyevaluate based on an analysis of de-identified data. This study stratifies theindications for ABGs, approximates the number of unnecessary tests, andquantifies the cost-savings of tests which are unlikely to be useful in a spe-cific clinical setting.
219
REFRACTORY STATUS EPILEPTICUS IN A PREVIOUSLYHEALTHY CHILD: A CASE REPORT
Dishong MM1, Rutledge C2, Winkler M2, Prabhakaran P2. 1University ofAlabama School of Medicine, Birmingham, AL and 2University of AlabamaSchool of Medicine, Birmingham, AL.Purpose of Study: Febrile infection-related epilepsy syndrome (FIRES)is a relatively new entity in pediatric medicine, consisting of refractory statusepilepticus with acute onset after a febrile illness in previously healthy child-ren, with a wide range of outcomes from mild developmental delay, refractoryepilepsy to death. We present a 14 year old patient who was admitted to thepediatric intensive care unit (PICU) in refractory status epilepticus.Methods Used: A case reportSummary of Results: The patient was a previously healthy child whodeveloped 5 days of fever and headaches which progressed to altered mentalstatus and then seizures at home. She was admitted to the PICU in statusepilepticus and received multiple anti-epileptic regimens in order to maintainburst suppression, which was successful with phenobarbital and pentobarbi-tal drips. Initial brain MRI, MRA and CT scans were normal. CSF studiesshowed mild leukocystosis but was otherwise normal. A complete infectiouswork up was performed which returned negative. She received severalcourses of multiple antibiotic, antiviral, and antifungal medications. An
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
434 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

extensive immunologic work up was also performed which revealed positiveANA screen and positive RNP and SSA antibodies. Immunomodulatingtherapy was given including IV methylprednisolone, plasmapheresis, IVIg,and anakinra, which provided no significant benefit. She was started on aketogenic diet but had difficulty obtaining ketosis due to concomitant steroiduse. She eventually developed culture-negative sepsis and succumbed to herdisease approximately 4 months after her admission. The final diagnosis forthis case was FIRES.Conclusions: FIRES, while still a rare disorder, is becoming increasingprevalent and should be considered with any patient presenting with refrac-tory status epilepticus. Many cases in the literature have also shown that most,if not all, anti-epileptics along with immunotherapy are not helpful in thesecases. Only the ketogenic diet may have some utility and should be consid-ered early on in the patient’s course.
220
UP-REGULATION OF REVERSION-INDUCING-CYSTEINE-RICHPROTEIN WITH KAZAL MOTIFS (RECK) IN LUNG FIBROSIS
Dong C1, Luo F1, Zhuang Y1, Shan B1, Chandrasekar B2, Lasky J1. 1TulaneUniversity School of Medicine, New Orleans, LA and 2Tulane UniversitySchool of Medicine, New Orleans, LA.Purpose of Study: Idiopathic pulmonary fibrosis (IPF) is characterized bythe aberrant accumulation of extracellular matrix. However, the mechanismsunderlying matrix remodeling have not been fully investigated. In this study,we evaluated the expression of reversion-inducing-cysteine-rich protein withKazal motifs (RECK), a negative regulator of matrix-degrading metallopro-teinases, over the time course of lung fibrosis.Methods Used: Western blot was employed to measure the expression levelof RECK in lung tissue. Immunohistochemistry was conducted to investigatethe localization of RECK in mouse lung tissue.Summary of Results: RECK protein expression is up-regulated in bothTGF-beta1 overexpression- and bleomycin-induced murine models of lungfibrosis. Interestingly, its level is increased significantly only at day 14 fol-lowing bleomycin inhalation when fibrogenesis is at its peak, but not atearlier inflammatory (day 5 and 7) or later resolution (day 40) phases. Im-munohistochemical staining localized RECK to epithelial cells and macro-phages in fibrotic lung tissue.Conclusions: Our results suggest a positive correlation between RECKprotein expression and active fibrogenesis. RECK may play a role in thedevelopment of lung fibrosis through inhibition of matrix metalloprotein-ases, which could in turn contribute to collagen accumulation.
221
UNUSUAL MANIFESTATION OF SJOGREN’S SYNDROME
Garcia D1, Neto LC2, Macedo FY3. 1University of Miami, Miami, FL;2School of Medicine of Valenca, Valenca, Brazil and 3Jackson MemorialHospital, Miami, FL.Case Report: Introduction:Lymphocytic interstitial pneumonia (LIP) isan inflammatory pulmonary reaction to systemic inflammation. It is associ-ated in 40% with autoimmune diseases like Sjogren’syndrome (SS), SLE,Hashimoto’s disease, and 14% infectious processes. LIP occurs mainly inmiddle-aged women presenting with dyspnea, dry-cough, weight loss, and chestpain. It is characterized by diffuse hyperplasia of lymphoid tissue within theairways with polyclonal-lymphoid infiltrate.Case description: 47- year-old woman with SLE admitted for dyspnea, sub-sternal chest pain, dry mucosas, and difficulty swallowing. Physical examrevealed bilateral vesicular breath sounds bilaterally. Laboratory work showedANA (speckled pattern, 1:40), SSA positive and negative DS-DNA, C3, C4,C50, Anti-Jo1, Anti-SSB. A high-resolution chest-CT demonstrated multiplebronchial cysts and diffuse interstitial infiltrates. Surgical lung biopsy re-vealed emphysematous changes and mild lymphocytic infiltrate around thebronchioles compatible with lymphocytic interstitial pneumonia diagnosis.Discussion: This case illustrates a patient with primary SLE overlappedby initial manifestation secondary SS (sSS) presenting with autoimmune as-sociated lung disease. Anti-body markers, high-resolution chest CT scan, andsurgical lung biopsy were essential in evaluating this patient and confirmingthe interstitial lymphocytic infiltration of the lung. Primary SS is the mostcommon associated-disease to LIP (25%). High-resolution chest CT presents
areas of ground-glass attenuation, and infiltrative interstitial disease. Surgicallung biopsy shows pathologic increase of mature lymphocytes cells, andhistiocytes. Most of the cases it has a benign presentation with relapse.Superimposed infection, pulmonary fibrosis and lymphoma develop in lessthan 20% of cases. Corticosteroids are the primary therapy. While pSS iscommonly associated with interstitial lung involvement, sSS is rarely asso-ciated. It has been described the initial sSS presentation by Sica symptomsdevelopment only, and our case is the first report of LIP on initial manifes-tation of sSS. Our patient remained stable after corticosteroids and hydox-ychloroquine therapy and no progression of disease after 6 months follow-up.
222
POLYSOMNOGRAPIC CHARACTERISTICS OF NOCTURNALGASTRO-ESOPHAGEAL REFLUX AMONG VETERANSWITHOBSTRUCTIVE SLEEP APNEA
Gharaibeh K1,2, Ullah I1, Campbell D1,2, Tamanna S1,2. 1University ofMississippi Medical Center, Jackson, MS and 2G.V. (Sonny) Montgomery VAMedical Center, Jackson, MS.Purpose of Study: Nocturnal gastro esophageal reflux (nGER) is commonamong patients with obstructive sleep apnea (OSA). Few recent studiesshowed that continuous positive airway pressure (CPAP) reduces the symp-toms of nGER among patients with OSA. However, polysomnographic (PSG)characteristics of the patients of OSA with different levels of nGER havenot been well documented.We examined the association of severity of nGER symptoms with CPAPpressure requirement, apnea hypopnea index (AHI), Epworth sleepiness scale(ESS) and demographic characteristics of the patients with OSA. We alsoexamined if the polysomnographic characteristics vary along with severity ofnGER symptoms.Methods Used: We interviewed 74 veterans with OSA to assess their day-time sleepiness (by ESS) and frequency of nGER symptom [on a scale of1(never) to 5 (always)] at their visit to the sleep lab following overnight PSGswith CPAP titration. The CPAP titration data and demographics were re-viewed. Simple and multiple linear regression analyses were performed toidentify factors predicting severity of nGER.Summary of Results: Eighty four percent (84%) patients complained ofexperiencing nGER symptoms during their visit. In multiple linear regressionmodel, reduced frequency of nGER was best predicted by increasing CPAPpressure (pG0.001) and Body mass index (p=0.008, R2=0.49). Supine AHIand ESS were significant when assessed alone, but became statistically in-significant in the multiple regression models. There were no significant dif-ference in mean total AHI, supine AHI, REM sleep AHI, wake after sleeponset, and sleep efficiency among patients of with or without nGER symptoms.Conclusions: Nocturnal gastro esophageal reflux is common among vet-erans with OSA. High CPAP pressure requirement and high BMI predictsincrease in severity of nGER symptoms. However, polysomnographic char-acteristics were not different between the two groups of patients with andwithout nGER.
223
A RARE PRESENTATION OF BILATERAL PLEURALEFFUSION WITH PERICARDIAL EFFUSION DUE TO ABRONCHOGENIC CYST
Habib S, Ahmed M Texas Tech Univ HSC, Amarillo, TX.Case Report: Bronchogenic cysts are rare cystic malformations resultingfrom embryological budding of the bronchial tree, with walls similar to thoseof normal bronchi. Mediastinal bronchogenic cysts can be complicated byinfection, compression of the trachea or superior vena cava, intra-cystic hem-orrhage, rupture, hemoptysis, and malignant transformation.Case:
A 30-year-old female was admitted with shortness of breath for one week.She was initially treated for suspected community acquired pneumonia withantibiotic when bilateral pleural effusion was noted on chest x-ray in out-patient clinic. Her symptoms did not improve and her breathing difficulty wasworsening with chest tightness, particularly whenever she lay flat on the back.On admission, the initial chest x-ray showed only pleural effusions bilaterallywith no widening of the mediastinum. CT of the chest revealed a large cysticlesion in the anterior mediastinum, pericardial effusion and pleural effusions.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 435
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Biopsy of the cystic lesion confirmed a bronchogenic cyst. Cultures werenegative. The patient underwent median sternotomy with excision of the an-terior mediastinal mass. She recovered completely post procedure.Discussion: Bronchogenic cysts are the most common cystic lesions of themediastinum and account for 18% of all primitive mediastinal masses. Theprevalence is difficult to estimate because they frequently are asymptomatic.Most commonly they are found near the carina (È51%) and some are at-tached to it, although only 5% communicate with an airway. Atypical loca-tions have also been reported, including the neck, the spinal dura mater andthe diaphragmatic region. The cysts are usually smooth, convex or roundmasses of homogenous density. Common symptoms are cough, dyspnea, pain,fever, pneumonia, upper respiratory tract infection and dysphagia. Symptomsare more frequent in patients whose cysts have a communication with theairway. CT scan is the best imaging modality with the appearance of well-defined masses of variable density that may contain rim calcifications. Earlysurgical resection provides better conservation of pulmonary parenchyma, alower incidence of inflammatory lesions, and a reduced rate of complications.
224
A CASE OF CONCOMITANT OSTEOMYELITIS, SEPSIS,AND MENINGITIS PRESENTING TO THE PEDIATRICEMERGENCY DEPARTMENT
Hoops K, Gran K. University of Alabama Birmingham, Homewood, AL.Case Report: Staphylococcus aureus is an increasingly common causeof localized infections and toxin-mediated syndromes (1, 2). We present acase of a common pathogen causing sepsis and two uncommon diseases: cal-caneal osteomyelitis and meningitis.Our patient is a 12 year old Caucasian male who presented to the pediat-ric emergency department with right ankle pain for one week and fever for twodays. One week prior to presentation, he sprained the affected ankle whileplaying in a pond.In the emergency department, the patient was tachycardic (HR 154) andtachypneic (RR32) but afebrile. Exam revealed an cantankerous boy withpronounced right ankle edema and erythema, tenderness greatest over thecalcaneous and lateral malleolus, and positive Kernig and Brudzinski’s signs.Due to concern for sepsis and osteomyelitis, critical care and orthopedic sur-gery teams were involved early in the care of this patient. Lumbar puncturewas performed. He was endotracheally intubated for progressive shock. Hewas then sedated for joint aspiration and washout. Initial studies demon-strated acidemia (venous pH 7.29), leukocytosis with left shift (WBC 12000with 71% neutrophils and 20% bands), meningitis (CSF WBC 27, RBC 3),synovitis vs osteomyelitis (joint aspirate WBC 44,000) and systemic inflam-mation (ESR 68, CRP 43). He was started on broad empiric coverage. Withinhours, cultures of the blood, joint aspirate, and cerebrospinal fluid had growngram positive cocci in clusters. Following stabilization in the emergency de-partment, our patient was admitted to the pediatric intensive care unit forseptic shock.Calcaneal osteomyelitis accounts for 3-10% of all cases of pediatric osteo-myelitis (3-5). Distinguishing it from other ostemyelitides, calcaneal osteo-myelitis is more commonly associated with trauma (6). Staphylococcalmeningitis is uncommon in children, and it is exceedingly rare in childrenwithout indwelling foreign bodies, such as ventriculoperitoneal shunts (1). Areview of current literature yields case reports of staphylococcal meningitisin immunocompetent children associated with sacral vertebral osteomyeli-tis, mastoiditis, preseptal cellulitis, and an infected cephalohematoma (7-11).However, no cases are previously documented of MRSA meningitis associ-ated with extra-axial osteomyelitis.
225
THE ASSOCIATION BETWEEN GLUCOSE LEVELS ANDHOSPITAL OUTCOMES IN PATIENTS WITH CHRONICOBSTRUCTIVE PULMONARY DISEASE
Islam E, Limsuwat C, Nantsupawat T, Berdine G, Nugent K. Texas TechUniversity Health Sciences Center, Lubbock, TX.Purpose of Study: To determine whether corticosteroids used for COPDexacerbations cause hyperglycemia in hospitalized patients and if blood glu-
cose levels are associated with mortality, length of stay (LOS), or readmis-sions in patients admitted to the MICU.Methods Used: We did three retrospective studies using charts from July2008 through June 2009, January 2006 through December 2010, and October2010 through March 2011. Patients admitted in the ICU were excluded in thefirst group, but were included in the second group. A discharge diagnosis ofa COPD exacerbation was included in the third group. Data compiled in-cluded FEV1, history of diabetes, blood glucose levels (all reported in mg/dl)and maximum dose of corticosteroids.Summary of Results: The first database included 35 patients. 22 non-diabetics patients (non-DM) had a mean initial glucose of 121 (83-238).Seven of these patients had a max glucose above 200; the change inglucose (max in hospital minus initial) ranged from 0 to 205. Thirteenpatients with diabetes (DM) had a mean initial glucose of 180, 10 had amax glucose above 200, and the change in glucose ranged from 0 to 416.The initial, max, and change in glucose levels in DM group were higherthan in the non-DM group (pG0.05, all comparisons). The corticosteroiddose had no apparent effect on the glucose levels. The second databaseanalyzing mortality and length of stay included 217 patients admitted tothe intensive care unit with initial blood glucoses of 156 (60 to 485).Blood glucose was higher in patients who died by bivariate analysis(p=0.015; OR 1.01) but not in multivariate analysis. Multivariate logisticregression analysis demonstrated that glucose levels did not have an effecton LOS. The third database analyzing COPD readmission rates included81 patients with a mean blood glucose of 212T 105.There was no statis-tical difference between early rehospitalization and non-early rehospitali-zation groups (p=0.551).Conclusions: Our data demonstrate that both DM and non-DM COPDpatients treated with steroids developed significant hyperglycemia. The in-crease in blood glucose levels with corticosteroids did not correlate with themaximum dose. Blood glucose levels were not associated with mortality,length of stay, or readmission.
226
ATYPICAL LUNG DISEASE IN AN ADOLESCENT
Johnson AB. UAB, Birmingham, AL.Case Report: A 17 year-old previously healthy male presented with chiefcomplaint of ‘‘chest tightness and difficulty breathing.’’ Additional symp-toms included 4 days of fever, productive cough, and progressive dyspnea.Review of systems was positive for night sweats and several episodes ofemesis, but revealed noweight loss, travel, sick contacts, or rashes. He did nottake any medications. He smoked several cigarettes per day and drank alcoholon occasion. He admitted to prior cocaine use, 6 months before presentation.He denied recent sexual activity. On initial physical exam, he was in moder-ate respiratory distress, speaking in short sentences. He required 15 liters ofoxygen via non-rebreather face mask to maintain saturations in the high 90sVital Signs included: Temp of 99.1 F, HR of 87 beats/min, RR of 59 breaths/min, and BP of 111/56 mm Hg. His lung exam revealed coarse breath soundswith bilateral crackles but no wheeze, and accessory muscle use. The remain-der of the physical exam was normal. Patient was admitted to the PediatricIntensive Care Unit (PICU) and placed on continuous positive airway pres-sure (CPAP). He required intubation after CPAP provided no improvementin his respiratory status. He was started on broad spectrum antibiotic cov-erage. His admission labwork revealed a serum leukocyte count of 13,600 /mm3, with a differential of 80% neutrophils, 7% bands, 4% lymphocytes,7% monocytes, and 2% eosinophils. His C-reactive Protein was elevated at14, but his erythrocyte sedimentation rate was normal. A bronchoscopy andbronchoalveolar lavage (BAL) was performed. The BAL from both the leftand right lung fields had an elevation of Red and White Blood Cells, with apredominance of eosinophils on the differential (61% and 69% respec-tively). Gram stain showed no organisms. Culture of the lavage fluid wasnegative for bacteria, fungi, and parasites. Given the acute presentation, ra-diologic changes, and significant eosinophilic count on BAL, the diagnosis ofAcute Eosinophilic Pneumonia (AEP) was made. Our patient was started onhigh dose systemic steroids. Antibiotics were stopped after negative cul-ture results. He improved throughout his hospital stay, was extubated within48hrs of intubation, and was able to be discharged home on room air withinone week.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
436 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

227
PULMONARY REHABILITATION IMPROVES QUALITY OFLIFE MEASURED BY THE SF-36 QUESTIONNAIRE
Limsuwat C, Mcclellan R, Amiri HM, Nugent K. Texas Tech UniversityHealth Science Center, Lubbock, TX.Purpose of Study: Pulmonary rehabilitation (PR) improves physical per-formance and health-related quality of life in patients with chronic lung dis-eases, especially COPD.We evaluated the effect of PR using the Short Form-36(SF-36) to determine if rehab had more effect on certain subcomponents ofthis survey.Methods Used: We retrospectively reviewed the rehabilitation files of 119patients who completed pulmonary rehabilitation in 2010 and 2011. We col-lected information on demographics, symptoms, pulmonary function tests,baseline gait speed calculated from 6 minute walks, and responses on the SF-36 survey. Forty-one patients completed surveys before and after rehabilitation.Summary of Results: The study population included 19 women and 22men. The mean age was 69.8 T8.5 years. The diagnoses included COPD (31),asthma (3), restrictive ventilatory defects (5), and OSA (2). The mean FEV1was 1.16 T0.52 L (60.5 T15.9% of predicted), and the mean 6-minute walkdistance was 728 T283 feet. The patients completed 21.6 T7.8 weeks of rehab.The mean baseline total SF-36 score was 301.9 T55.6. The correlation be-tween initial and last SF-36 was 0.97 with PG0.01. There were improvementsin the vitality subcomponent (p=0.051 by paired t test), role function sub-component (p=0.005), and general health component (p=0.06).There was noassociation between the change in the role function subcomponent scoresand age, gender, FEV1, six minute walk distance, or gait speed.Conclusions: Pulmonary rehabilitation improves some of the subscales ofthe SF-36 survey. However, baseline characteristics did not identify patientswho would most likely benefit. We need a more detailed analysis of socialand mental factors which influence SF-36 scores to determine all the factorswhich might limit improvement. These patients likely need additional eval-uation and/or treatment.
228
BNP AS AN AID IN DIAGNOSING ACUTE PULMONARYEMBOLISM
Mabry C1, Grewal H1, Thoppil DR2, Engel LS1. 1LSU Health SciencesCenter, New Orleans, LA and 2West Jefferson Medical Center, Marrero, LA.Case Report: Introduction: Acute pulmonary embolism (PE) is a commonand often fatal diagnosis. The diagnosis is often missed because of vaguesymptoms at presentation. In many cases, there is an elevated Brain Natri-uretic Peptide (BNP) which may correlate with the severity and prognosisof the patient.Case: A 57 year-old woman with a history of normal pressure hydrocephaluspresented to the emergency department complaining of cough for one weekand shortness of breath for one day. At admission, abnormal vital signsincluded a blood pressure of 97/73 (repeat 100/70), pulse rate of 81 beats/min, respiratory rate of 20 breaths/min, oxygen saturation of 80% on roomair, and 98% using a non-rebreather. On exam, there were no murmurs noted,there was bilateral pitting lower extremity edema to the mid calves, andbilateral crackles in the lung bases. Lab work showed: sodium 157 Mmol/L,potassium 2.9 Mmol/L, chloride 121 Mmol/L, creatinine 1.53 mg/dL, andBNP 2795 pg/ml. An ABG revealed: pH 7.50, pCO2 32, O2 87, 100% FiO2.The patient’s ECG showed sinus tachycardia and right ventricular strain pat-tern. Echocardiogram showed an enlarged RV. The patient was treated for apulmonary embolism with IV heparin. She quickly decompensated, was giventissue plasminogen activator, but unfortunately did not survive.Discussion: BNP is a marker of left ventricular stretch. It is used to determinecardiac versus pulmonary source of dyspnea. In recent studies, there has beena strong correlation between the levels of BNP and the prognosis of patientswith PE. These studies have shown that patients with elevated BNP levels andechocardiographic findings of right ventricular strain have a poorer prog-nosis. Although the BNP level is insensitive and not specific for PE, clin-icians can use it in conjunction with echocardiography to help in thediagnosis and consequent treatment of patients with a large PE. Thus, mea-suring BNP levels may play a role in the prognosis of these patients.
229
POST-INTUBATION SORE THROAT CAN BECOME MISHAP?
Mankongpaisarnrung C, Laengvejkal P, Dumrongmongcolgul N, Limsuwat C,Nugent K. Texas Tech University Health Sciences Center (TTUHSC),Lubbock, TX.Case Report: Background: Sore throat is a common symptom after endo-tracheal intubation (ETT) and occurs in up to 40% during the first two post-operative days. Other common complications from ETT are laryngeal injury(more likely in women), impaired swallowing, and tracheo-bronchitis. Thesesymptoms usually resolve spontaneously. Small cuffs, lubricants, or topicallidocaine may prevent postoperative sore throat. Persistent sore throat afterintubation needs to be reviewed carefully.Case: A 69-year-old woman with a past history of hypertension pres-ented with progressive sore throat on post-operative day 5 after right totalhip arthroplasty. During the procedure, she had a difficult ETT. Afterwards,she had a sore throat, was unable to swallow water, and had a dry cough. Shewas in acute distress. With the use of a tongue depressor, she had limitedmouth opening and mild erythema over the posterior oropharynx withoutuvular deviation or local swelling. She was afebrile and had no tachypnea ordrooling. Inspiratory stridor was audible with a stethoscope. CBC showedWBC 9.1, Hb 30.1, Plt 361, and N 46.9 %. Other lab was unremarkable.Computed tomography (CT) of neck showed a 6-cm retropharyngeal air-fluid collection with soft-tissue swelling. Retropharyngeal abscess (RPA)with early UAO was diagnosed. Clindamycin was initiated promptly. Finallyshe underwent incision and drainage by an otolaryngologist. She recoveredwell postoperatively and was discharged home on postoperative day 2.Discussion: RPA is usually caused by penetrating trauma from a foreign bodybut also occurs as a post-ETT complication. In this case, it is likely from adifficult intubation. However, the positive pertinent physical finding point-ing toward RPA might not be clinically apparent due to its anatomical loca-tion. Therefore, if this complication remains uncertain, a CT of the neckshould be obtained. We also highlight the importance of scrutiny of red flagsigns, such as progressive dysphagia, fever, and difficult breathing, in thosewith recent ETT to prevent complications from RPA, such as respiratoryfailure from UAO or acute mediastinitis.
230
FACTOR ASSOCIATED WITH REINTUBATION IN PATIENTSWITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Nantsupawat N1,2, Nantsupawat T1, Limsuwat C1, Sutamtewagul G1, NugentK1. 1TTUHSC, Lubbock, TX and 2Chiang Mai University, Muang, Thailand.Purpose of Study: Acute exacerbations of chronic obstructive pulmonarydisease (AECOPD) increase morbidity, mortality, and health-care costs inpatients with COPD. Many patients require intensive care unit admission andassisted ventilation. Patients who fail extubation often have longer hospitalstays and/or increased mortality. Determining predictors to identify patientswho require reintubation might help physicians and care teams manage thesepatients.Methods Used: We retrospectively reviewed data of COPD patients overa three-year period (2008-2010). Inclusion criteria were: AECOPD patients,age945, mechanical ventilation (MV) for more than 48 hour. Exclusioncriteria were: tracheostomy, unplanned extubated, reintubation for reasonsother than respiratory failure. Demographic data, APACHE II scores, bloodgas parameters, cough assessment and sedation used were recorded and com-pared in patients who required reintubation and who did not.Summary of Results: Eighty-eight patients required intubation with me-chanical ventilation. The overall reintubation rate was 12.5%, 69.3% weresuccessfully extubated, and 18.2% were not extubated. The baseline variablesand other variables - emergent intubation status, admission APACHE IIscores, and severity of the COPD - were not different in the two groups. Themean duration of MV in the reintubation group was twice as larger as thesuccessful group. Patients with successful extubation were more likely tohave a ‘‘Good cough’’ assessment and receive less sedative drugs than pa-tients who failed extubation (pG0.05). ICU and all hospital stay, tracheostomyevent, and mortality rate were higher in the reintubation group (p=0.001).Multiple logistic regression indicated that reintubation was significantly as-sociated with sedation given (odds ratio [OR], 8.6; 95% confidence interval[CI] 1.23-60.8) and with length of ICU stay (OR 0.77; 95% CI 0.64-0.92).
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 437
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

However, the difference in APACHE II scores between admission and 24 hrbefore extubation, blood gas parameters, and pulmonary complications werenot associated with reintubation.Conclusions: Two clinical variables, sedative drug use before extubationand the duration of ICU stay 9 5 day, help predict the need of reintubationafter planned extubation in the AECOPD patients.
231
INPATIENT HOSPITALIZATIONS FOR CROUP
Narayanan S. University of Alabama at Birmingham, Birmingham, AL.Purpose of Study: Croup is one of the most common respiratory diseasesof childhood, but little attention has been focused on patients who requireinpatient hospitalization for their illnesses. We sought to describe the inpa-tient experience of croup at a tertiary care hospital and characterize patientswith low- and high-acuity illness and prolonged length of stay.Methods Used: We conducted a retrospective study of discharged patientsfrom a children’s hospital with an ICD-9-CM diagnosis code for croup oracute laryngotracheitis (464.�). Eligible patients were admitted from January1, 2006 through December 31, 2010. Data was manually extracted fromcharts using a data collection spreadsheet. Admission criteria were at thediscretion of the treating physician. Fisher’s exact tests and Student’s T-testswere performed to compare demographic and illness-related data of specificsubgroups.Summary of Results: The final analysis included 365 hospitalizationsinvolving 327 patients, 72.3% male, 61.6% white, with a mean age of 23.1months. The mean length of stay was 42.9 hours, with a mean of 1.33 racemicepinephrine treatments after admission (range 0-13; median 0). Intubation orescalation in level of care occurred in 28 cases (7.7%), while 186 cases(51.0%) required no further respiratory treatments within 3 hours of initialED evaluation.Oxygen saturation of G95% in the ED was associated with a high-acuityhospitalization (12% vs 6%, pG0.05), defined as escalation of level of care orintubation for respiratory failure. Patients who did not require further respi-ratory treatments after admission were indistinguishable based on age, gender,past medical history, or ED vital signs. Patients with a history of croup orintubation, or oxygen saturation of G95% in the ED, had increased lengthof stay compared to those without these criteria.Conclusions: The majority of patients admitted with croup did not requirefurther respiratory treatments once hospitalized. A significant percentage ofpatients required an escalation of level of care after being admitted, and thusa complicated hospital course may be predictable for certain subgroups.Larger prospective studies may be helpful to validate criteria for patientsat high risk of intubation for respiratory failure and to identify those whocan safely be discharged from the emergency room or treated in a lower-acuity observation unit.
232
UTILITY OF CHEST RADIOGRAPHY IN INPATIENTSWITH ASTHMA
Narayanan S. UAB, Birmingham, AL.Purpose of Study: Chest radiographs are not routinely indicated for hos-pitalized children with asthma, but they are still obtained frequently. The goalof this study was to identify factors associated with ordering of chest ra-diographs in children hospitalized with acute asthma exacerbations, and theoverall clinical impact of these radiographs.Methods Used: A retrospective study was performed with children Q2 yearsof age with a history of asthma who were admitted from a pediatric emer-gency department to a general inpatient bed on an asthma clinical pathwaybetween June 2011 and May 2012. The asthma clinical pathway excludescritically ill patients requiring continuous albuterol nebulization and patientswith chronic respiratory illnesses such as cystic fibrosis. 100 of the 292 in-patient visits were randomly selected and data was collected on history ofthe acute illness and the subsequent hospital course, including clinical wors-ening and initiation of antibiotics.Summary of Results: The final analysis included 100 hospitalizationsof children ages 2-19 years (median 5.5 years). A total of 45 radiographs wereordered on 41 patients, 25 in the Emergency Department (55.5%) and 20(44.5%) after hospital admission. Of the 41 patients with radiographs,
3 (7.3%) had a radiographic diagnosis of pneumonia and were started onantibiotics. This accounted for 4 of the 45 (8.9%) total radiographs ordered.Of the 3 patients with pneumonia, one had a history of fever prior to ad-mission, two were removed from the asthma pathway due to clinical wors-ening, and all were treated with oral azithromycin. There were no cases ofpneumothorax or pneumomediastinum.Ordering of chest radiography was associated with history of fever (positiveOR 1.66 [95% CI: 1.04-2.62] and lower O2 saturations in ED triage (92.6 vs94.2%; pG 0.05). Patients with pneumonia were older (10.61 vs 6.29 years;pG0.05) and had lower O2 saturations in ED triage (90.3 vs 93.6%; pG0.05),but history of fever or abdominal pain was not significant.Conclusions: The vast majority of chest radiographs ordered in pediatricinpatients with asthma exacerbation do not provide clinically relevant in-formation. The prevalence of concurrent pneumonia or air leak was very lowin this non-critically ill population. Selective ordering of radiographs in olderchildren with ED triage hypoxemia or clinical worsening after admission mayreduce unnecessary testing.
233
PSEUDOMONAS LUNG ABSCESS -UNUSAL CAUSE FORCAVITARY LUNG LESION
Nusrat M, Aly M, Nugent K, Sherif K, Fenire M. Texas Tech UniversityHealth Science Center, Lubbock, TX.Purpose of Study: Pseudomonas aeruginosa rarely cause lung abscess orempyema. In this report we present a case with bilateral empyemas and lungabscesses caused by P. aeruginosa and anaerobes that failed medical andsurgical treatment.Methods Used: case report and a review literature.Summary of Results: A 78-year-old man with hypertension and coro-nary artery disease presented with fever, shortness of breath, and right sidedpleuritic chest pain for one week. His initial chest X - ray showed a small rightside pleural effusion and an infiltrate in the right lung base. A CT chestshowed multiple pleural fluid collections more on the right side. Fluid from aCT guided biopsy showed a mixed growth of Pseudomonas aeruginosa andPrevotella loescheii. His condition gradually deteriorated requiring intubationand mechanical ventilation. He was treated with levofloxacin, vancomycin, andpiperacillin-tazobactam and supportive measures. A right thoracotomy wasdone and all loculated collections were removed, the right lower lobe wasdecorticated, and chest tubes were placed. However, the patient continued todeteriorate and developed multiorgan failure. His chest X - ray at this pointshowed two cavitary lesions, a large loculated pleural effusion on the rightside, and a left sided pleural effusion. A repeat CT chest showed two largeabscesses with air fluid levels in the right lung and multiple loculated effu-sions on both sides. Later his family decided to withdraw careConclusions: The most common bacteria causing lung abscess are Pep-tostreptococcus spp, Prevotella spp, Bacteroides spp (usually not B. fragilis),and Fusobacterium spp. P. aeruginosa is an important cause of nosocomialpneumonia, especially in immunocompromised patients, but in general theseinfections present as bronchopneumonia and not as empyema or lung ab-scess. However, Gluck reported a patient who developed nosocomial pneu-monia due to P. aeruginosa which eventually led to lung abscess formationand acute empyema. Our patient had lung abscesses and multifocal empyemaswhich progressed despite treatment. Microbial synergy and thick abscesswalls likely caused this patient’s deterioration. Clinicians need to rememberthat Pseudomonas lung abscess has a very poor prognosis.
234
A LARGE PLEURAL EFFUSION FOLLOWING ABDOMINALAORTIC SURGERY
Ramsaran VK, Seeram VK, Cury JD, Shujaat A. Uinversity of FloridaCollege of Medicine - Jacksonville, Jacksonville, FL.Case Report: Chylous ascites and coexistent Chylothorax is a rare butimportant complication following retroperitoneal abdominal surgery.The diagnosis of chylothorax is usually made based on the clinical scenario,the gross appearance and biochemical analysis of the pleural fluid. Chylousascites can occur from operative trauma to the cisterna chyli or its tributariesor the thoracic duct. Chylothorax in the setting of chylous ascites is an ex-ample of a porous diaphragm syndrome with the movement of fluid through
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
438 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

diaphragmatic pores or defects, similar to how a hepatic hydrothoraxdevelops.We present the case of a gentleman who developed Chylous ascites withChylothorax following retroperitoneal surgery.
235
HIV-MEDIATED INHIBITION OF PU.1 GENE EXPRESSIONIN THE ALVEOLAR EPITHELIUM DOES NOT APPEAR TOBE MEDIATED BY NRF2
Staitieh B1, Fan X1,2, Guidot D.1,2 1Emory University, Atlanta, GA and2Atlanta VAMC, Decatur, GA.Purpose of Study: Previously we determined that HIV-1 transgene ex-pression in experimental animal models decreases the expression of Nrf2,the master transcription factor that activates the anti-oxidant response ele-ment (ARE), within the lung. As Nrf2-ARE signaling is required to induce theexpression of a wide range of anti-oxidant defenses, the inhibition of Nrf2could explain how HIV-1 causes the profound oxidative stress within thealveolar space that we have identified in both experimental models and inhuman subjects. Previously we had determined that PU.1, the master tran-scription factor required for CM-CSF-mediated priming of alveolar epithelialand macrophage function, is also inhibited by HIV-1 transgene expression.Interestingly, we recently identified that Nrf2 and PU.1 appear to bind DNAin an interactive fashion, suggesting that these two fundamental responsepathwaysmay be coordinately regulated. Therefore, in this study we sought toelucidate the mechanism(s) by which the Nrf2 and PU.1 pathways may interact.Methods Used: Alveolar epithelial cells were isolated from HIV-1 trans-genic and littermate wild type rats and PU.1 mRNA expression was deter-mined by RT-PCR. In separate experiments, Nrf2 expression in cells from thewild type rats was suppressed via transfection with an RNA silencing vector48 hrs before quantifying PU.1 mRNA expression.Summary of Results: HIV-1 transgene expression decreased PU.1 ex-pression in the alveolar epithelium as we have previously shown. However,suppressing Nrf2 expression in alveolar epithelial cells from wild type ratsdid not reproduce the HIV-mediated inhibition of PU.1 expression.Conclusions: Although Nrf2 and PU.1 appear to cooperatively bind DNAand may thereby coordinately activate cellular responses to stress within thealveolar space, they do not appear to influence each other’s expression at themRNA level. Further experiments are therefore necessary to delineate howthese two pathways interact and are the focus of our current studies of themechanisms by which HIV-1 and other chronic oxidative stresses such asalcohol abuse render the lung susceptible to injury.
236
A RARE PNEUMONIA CAUSED BY A DIFFICULT BUG!
Thayalakulasingam T1, Lavie J2, Sanders C3, Ali J1. 1LSUHSC, New Orelans,LA; 2LSU School Of Medicine, New Orleans, LA and 3LSUHSC, NewOrleans, LA.Case Report: Introduction:Nutritionally variant streptococci (NVS) is an important human patho-gen most often implicated in endocarditis and septicemia. It is extremely rarecause of pneumonia and difficult to treat.
Case Presentation:A 33 year old African American man with a history of schizophrenia andtobacco abuse presented from prison after an altercation with the guards. Thepatient complained of worsening dyspnea over the previous two weeks,subjective fever, chills, weight loss, cough with brown/black sputum for thelast week, and generalized fatigue with drenching night sweats over the lastfour days prior to admit. Recent tuberculin skin test was negative.On physical exam, he was febrile at 101.3, tachycardic, and sating 96% onroom air. He was ill appearing and thin with poor oral hygiene. Lung examrevealed diffuse crackles bilaterally. CT showed multifocal parenchymal bi-lateral opacities. Patient had a WBC of 14.1x103/UL.Antibiotics were started for community acquired pneumonia with the additionof vancomycin due to continued fevers. He remained febrile. Bronchoscopywas performed with biopsies and all samples grew nutritionally variantstreptococcus. Antibiotics were switched to piperacillin/tazobactam. He ex-perienced resolution of his fevers and clinical improvement and was dis-charged on hospital day 14 with amoxicillin/clavulanate with follow-upappointments in pulmonary and infectious disease clinics.Discussion:NVS are part of normal oral, upper airway, gastrointestinal and urogenital florabut have been reported as an important human pathogen. NVS have beenimplicated in as many as 5% of endocarditis, as well as important causes ofbacteremia in patients with intestinal or postpartum sepsis, pneumonia, os-teomyelitis, and cancer. Risk factors for NVS infection include poor oralhygiene, dental manipulation, immunosuppresion, and pre-existing heart dis-ease in endocarditis.In general NVS respond poorly to antibiotic therapy and has high ratesof relapse. Significant morbidity and mortality is described in the literaturefor NVS infection (9-25%). Currently, no guidelines exist for the treatmentof NVS pneumonia, as it has been so rarely reported.
237
A HOT BLOODED YOUNG MAN!
Thayalakulasingam T1, Englert D2, deBoisblanc B1. 1LSUHSC, New Orleans,LA and 2LSUHSC, New Orleans, LA.Case Report: IntroductionHeatstroke is the most severe form of heat-related illness and is common inhumid climates during the summer months. Timely identification and treat-ment is crucial in order to improve survival and decrease complications.Case Presentation
A 22 year old male was found down by EMS after breaking into aneighbor’s home. He was hyperthermic at 107 OF, tachycardic, tachypneic,and hypotensive, with a GCS of 3. He was intubated and conductive cool-ing was initiated. Pertinent physical exam findings included multiple su-perficial abrasions and lacerations on his arms, hands and legs; decreaseddeep-tendon reflexes; absence of any spontaneous movement; and no signs ofrigidity. Laboratory data included a bicarbonate of 13 mmol/L, INR of 1.4,creatinine of 2.2 mg/dL, CPK of 530 U/L, and lactic acid of 7.9 mmol/L.Over the next several hours, his INR increased to 3.5, and the patient de-veloped disseminated intravascular coagulopathy (DIC), rhabdomyolysis,and worsening of the acute kidney injury for which he later required dialysis.Over the next three days, he required multiple blood products to correct hiscoagulopathy, and the coagulation profile eventually stabilized. His mentalstatus slowly improved, and he was extubated on hospital day five. At thetime of hospital discharge, patient returned to his baseline function withresolution of renal dysfunction.Discussion
Hyperthermia occurs when there is an alteration in the balance betweenheat production and dissipation. The differential diagnosis of hyperthermiaincludes hyperthyroidism, drug-induced hyperthermia, malignant hyper-thermia, neuroleptic malignant syndrome, serotonin syndrome, and envi-ronmental heat related illnesses. Distinguishing these is often difficult aspatients typically have altered mentation, and history may be difficult toobtain. Early signs of environmental heat related illness include hyperpneaand tachycardia. Symptoms can evolve to fatigue, nausea, syncope, head-ache, weakness, and muscle cramping. Heat stroke is defined by central ner-vous system dysfunction and multi-organ failure, as was the case in our patient.Complications are common, and can include DIC, and renal dysfunction. Afterthe temperature is returned to normal, treatment is largely supportive.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 439
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

238
A RARE CYSTIC LUNG DISEASE
Thayalakulasingam T1, Tung LL2, Burns B3. 1LSUHSC, New Orelans, LA;2Ochsner Medical Center, New Orleans, LA and 3Ochsner Medical Center,New Orleans, LA.Case Report: Introduction:Lymphoid Interstitial Pneumonia (LIP) is a rare lung disease characterized bydiffuse hyperplasia of bronchus-associated lymphoid tissue. Here, we presenta case of diffuse cystic lung disease in an HIV infected individual who hadbiopsy proven LIP.Clinical Presentation:41 year old woman with a history of HIV Infection(CD4 count 176) presentedwith two month history of worsening shortness of breath, cough, & fever.Patient was hypoxemic and ill appearing on admission and was empiricallyplaced on treatment for pneumonia with broad spectrum antibiotics, howeverwithout clinical improvement. CTof chest revealed cystic lung lesions, with bi-basilar predominance concerning for intestinal lung disease.A diagnostic video-assisted thoracoscopic surgery performed and it re-vealed LIP. With clinical improvement, patient was discharged home withpulmonary and infectious disease follow-up. However, patient did not keepher appointment and was lost to follow-up for two years.On her second admission to the hospital, she presented with similar com-plaints: worsening dyspnea, productive cough, fevers, and chills. She un-derwent a bronchoscopy and pneumococcus and influenza were isolated andtreated. Even after the treatment of her infections, patient continued to behypoxemic and had a persistent dry cough with a new CT chest showing wors-ening extensive cystic appearing lung disease. She was started on steroidtherapy for her LIP. Within three days of starting the steroid treatment, pa-tient reported a noticeable improvement in her symptoms and her hypoxemiaalso resolved.Discussion:Lymphoid Interestial Pneumonia is a rare lung disease classically associ-ated with variety of conditions such as Sjogren’s syndrome, variable im-munodeficiency syndrome, bone marrow transplantation, and HIV. Clinicalpresentation includes dyspnea, dry cough, and weight loss. Pulmonary func-tion studies show a restrictive defect with a decreased carbon monoxide dif-fusing. Surgical lung biopsy is required for definitive diagnosis. Treatmentincludes supportive care, corticosteroids and immunosuppressive agents aswell as treatment directed at the underlying disease process. Malignant trans-formation to lymphoid malignancy has been also reported.
Joint Plenary Poster SessionRenal, Electrolyte, and Hypertension
5:00 PMThursday, February 21, 2013239
CRESCENTIC GLOMERULONEPHRITIS (GN) IN A CHILDWITH X-LINKED AGAMMAGLOBULINEMIA (XLA)
Afshan S1, Eison TM1, Hastings MC1,2, Michael C1, Maltby K1, WalkerPD3, Conley ME1, Ault BH1. 1UT, Memphis, Memphis, TN; 2UT, Memphis,Memphis, TN and 3Nephropath, Little Rock, AR.Case Report: Background: XLA is caused by a mutation in Bruton’s tyrosinekinase gene resulting in absent or marked reduction in antibody synthesis.Case Description: A five year-old Caucasian male with XLA received gam-maglobulin from age three months. Two weeks prior to presentation, he hadsore throat and fever; four days prior to presentation he developed cola-colored urine. On presentation blood pressure was 152/112 mm Hg and hehad periorbital edema and ascites. Laboratory studies revealed blood ureanitrogen 24 mg/dL, creatinine 0.98 mg/dL, albumin 2.4 g/L, C3 16.6 mg/dLand C4 3.3 mg/dL. Urinalysis showed 3+ blood, 3+ albumin, 316 RBC, 112WBC, and 1-2 RBC casts/hpf. Plasma IgG (316 mg/dL, normal 470-1400)and IgM (28.1 mg/dL, normal 37-117) were obtained one day after a gamma-globulin dose. Blood culture grew Streptococcus pneumoniae. Kidney biopsyshowed crescentic GN with diffuse mesangial expansion of intact glomerulion light microscopy (LM); 3 of 9 glomeruli were globally sclerotic. Plas-macytoid cells were noted in the interstitium. Immunofluorescence showed3+ IgG, trace IgA, 3+ C3, 3+ kappa and 3+ lambda. Electron microscopy
showed subendothelial and mesangial immune complex type electron densedeposits and rare intramembranous deposits. Six doses of 30 mg/kg intra-venous methylprednisolone (MP) and then oral prednisone 2 mg/kg/day wasgiven. Serum creatinine fell to 0.58 mg/dl after the fourth dose of MP.Conclusions: Two cases of GN in XLA are reported, one with membranousand one with membranoproliferative GN. Presence of immune complexeswould seem unusual in XLA. Measurable plasma IgM and interstitial plas-macytoid cells on LM and trace IgA on IF suggest that the antibody in theimmune complexes could be endogenous. Immune dysregulation resultingfrom patient’s immunodeficiency likely contributed to his severe immunecomplex GN.
240
FREE SOLUBLE (PRO)RENIN RECEPTOR LEVELS AREDECREASED IN THE URINE OF DIABETIC PATIENTS
Arita DY1,3, Luffman C1, Theti T2, Prieto MC1. 1Tulane University, NewOrleans, LA; 2Tulane University, New Orleans, LA and 3Federal Universityof Sao Paulo, Sao Paulo, Brazil.Purpose of Study: In vitro evidence indicates that the prorenin recep-tor ((P)RR), a new component of the renin-angiotensin system (RAS), bybinding renin or prorenin, enhances renin activity and fully activates pro-renin. Inappropriate intrarenal RAS activation is a common feature in dia-betes and hypertension. The urine of angiotensin II hypertensive rats containsincreased soluble (P)RR (s(P)RR) and renin content. Diabetic patients displaylow-to-normal plasma levels of renin but increased prorenin levels. In contrast,their urine contains high levels of active renin but low prorenin. We tested thehypothesis that s(P)RR enhances renin enzymatic activity in urine of diabeticpatients.Methods Used: This is a pilot study in which urine levels of s(P)RR weremeasured by enzyme-linked immunosorbent assays (ELISA; IBL, Japan) in atotal of 60 patients. This method detects levels of free s(P)RR. Data (pg/mg)were expressed as meanTSE after corrections by urine creatinine (uCre).P values G0.05 were considered significant.Summary of Results: Twenty-seven (48.2%) were women, with a medianage of 51 T 13 years and 30 (50.8%) were men with 50 T 16 years of age. Thesubjects were divided into three groups: control (CT) (n = 18), diabetics (DM)(n = 8) and diabetic and hypertensive (DM+HTN) (n = 20). uCre levels weresimilar among groups. Urinary s(P)RR concentrations were significantly de-creased in DM and DM+HTN patients compared to CT (DM: 579.5T130.9and DM+HTN: 500.0T84.79 vs. CT: 1248.0T345.6 pg/mg; pG0.05). Urinarys(P)RR levels between DM and DM+HTN patients were not different. In DMand DM+HTN patients, urinary renin content was higher than in CT patients(DM: 134T16 and DM+HTN: 162T31 vs. CT: 9.7T1.2 ng AngI/mL/hr;pG0.0001).Conclusions: The lower levels of s(P)RR in DM and DM+HTN patientsindicate that most of the s(P)RR in the urine of DM patients may be bound torenin or prorenin which could explain the increases in active renin in theurine of these patients. This study did not rule out that this method detectssPRR bound to renin and prorenin.
241
SURVEILLANCE BIOPSIES IN PEDIATRIC RENALTRANSPLANT RECIPIENTS
Atherton JG1, Hastings MC1,2, Oulimata GK1, Delos Santos N1, Eison TM1,Wyatt RJ1, Walker P3, Ault B1. 1UT HSC, Memphis, TN; 2UT HSC,Memphis, TN and 3NephroPath, Little Rock, AR.Purpose of Study: Benefits of pediatric kidney transplant surveillencebiopsy (SBx) are not well established. We describe findings of SBx per-formed at Le Bonheur Children’s Hospital from 2004 to 2012.Methods Used: Transplant biopsies are routinely done at our institution atthree months (59-121 days) and 12 months (300-422 days) post transplan-tation. Children with en-bloc or intra-abdominal allografts are excluded.Percutaneous SBx are performed using a 16 G needle with ultrasound guid-ance. Thymoglobulin\ is used for induction. Corticosteroids, tacrolimus, andmycophenolic acid are used for initial maintenance immunosupression.Summary of Results: There were 28 patients having at least one SBxduring the period of study. There were 21 males, 17 African-American, and10 Caucasian patients. Mean age at time of transplant was 13.8 T 4.1 years.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
440 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Primary renal diseases were obstructive uropathy (n=8), dysplasia/hypoplasia(n=7), hereditary nephritis (n=3), cystic disease (n=2), and other causes(n=8). Ten kidneys were from living donors. Three were second transplants.There were 42 SBx performed; 24 were performed at three months and 18were performed at 12 months. All patients tolerated the biopsy well and nonehad an extended hospital stay. Though serum creatinine was thought to be atpatient’s usual baseline at the time of biopsy, two of the biopsies showedcalcineurin inhibitor toxicity including one with a thrombotic microangiop-athy, two showed BK (polyoma) virus nephropathy, and three showed acutetransplant rejection. Changes in medical management included pulse meth-ylprednisolone and or Thymoglobulin\ in three, decreased immunosup-pression in one, and change to alternate immunosuppressive agent in three.Conclusions: Performance of SBx is not without risk, cost, and inconve-nience to the patient. However, SBx revealed unsuspected abnormalities andled to changes in medical management in 25% of the patients in this pediatriccohort.
242
INITIATING DIALYSIS WITH A CATHETER IS NOT THEBIGGEST RISK FOR BACTEREMIA IN HIV POSITIVEDIALYSIS PATIENTS
Baer SL1,2, Whitlow M2, Colombo R2, Chebrolu P2, Ellington C2, Kheda M1,Nahman NS1,2, Kintziger K1,2. 1Augusta VA Medical Center, Augusta, GAand 2Georgia Health Sciences University, Augusta, GA.Purpose of Study: Bacteremia (BAC) is a common complication in he-modialysis (HD) patients and may be associated with distinct risk factors.Recognized risk factors for BAC include the form of vascular access, can-didemia, diabetes, and hepatitis C (Chebrolu, accepted, IDSA 2012). In HIVpatients on HD, the contribution of each of the above risk factors to thedevelopment of BAC is undefined. To address this question, we queried theUnited States Renal Data System (USRDS) for HIV positive HD patientsand potential risk factors for BAC.Methods Used: All incident HD cases from the USRDS for 2005-2008were queried for a diagnosis of BAC, HIV, and potential clinical covariates,using ICD-9 diagnosis codes. Form 2728 was used to define access type atinitiation of HD. Descriptive statistics and adjusted log-binomial regressionanalyses were performed.Summary of Results: For the 4-year period of study, 362,799 patients wereavailable for analysis. Of these, 2946 (0.8%) were HIV (+). The median agewas 47 years, 70.6% were male, and 81.5% African American. On initiationof HD, access types included 7.7% arterio-venous fistulas, 2% grafts, and89.5% catheters. When compared to HIV (-), HIV (+) had significantly moreBAC episodes (43.6 vs 22%). In HIV (+) HD patients, having a catheter wasnot a significant risk factor for BAC [relative risk (RR) 1.31, 95% confidenceinterval (CI) 0.89-1.93.]. Factors associated with increased risk of for BAC inthe HIV (+) included pancytopenia [RR 1.64, 95% CI 1.40-1.92], methicil-lin resistant Staphylococcus aureus (MRSA) colonization [RR 1.60, 95% CI1.42-1.80], candidemia [RR 1.50, 95% CI 1.04-2.16], total parenteral nutri-tion (TPN) [RR 1.49, 95% CI 1.18-1.89], and decubitus ulcer [RR 1.36, 95%CI 1.18-1.92]. Having a prior or concurrent diagnosis of an AIDS definingillness (ADI) was also a significant risk factor for BAC; 1 ADI was associ-ated with less risk than 4 or more [RR 1.16, 95% CI 1.07-1.27; RR 1.50, 95%CI 1.20-1.88, respectively].Conclusions: BAC occurred in almost half of HIV patients from 2005-2008. Risk factors included MRSA colonization, candidemia, TPN, pancyto-penia, decubitus ulcer, and ADI. Initiating HD with a catheter did not confersignificant risk for subsequent BAC.
243SALICYLATE TOXICITY: DOES ALKALINIZING URINEWORKS?
Baudy A, Grewal RK, Kumbala D, Lukitsch I. Tulane School of Medicine,New Orleans, LA.Case Report: A 65 year old white male with history of squamous celllaryngeal cancer, polysubstance abuse, suicidal tendencies, hepatitis C pre-sented with shortness of breath and cough with clear sputum. He wasconfused, restless but oriented to time, person and alert enough to providehistory. He denied any nausea, vomiting or any headaches. Medications in-clude Aspirin, Metoprolol, Diltiazem, and Percocet. Physical exam included
diffuse bronchial breath sounds and rhonchi bilaterally otherwise rest ofexam was benign. Lab data showed pH 7.6, pCo2 18, pO2 115, HCO3 17.7,Na 142, K 5.3, Cl 112,Bicarb 11, BUN 43,creatinine 1.9 ,glucose 108, lacticacid 5.1, CK 50. Urine pH 5.0 ,specific gravity 1.027, ketones 5,urine os-molality 759. Toxicology screen was positive for salicylate and levels are asbelow. The patient was started on intravenous fluids with sodium bicarbonate.Increasing urine pH from 5 to 7.7 increased the renal clearance of salicylateand the levels of salicylate decreased. Alkalization with sodium bicarbonateresulted in enhanced excretion of ionized acid form of salicylate and pro-moted the transfer of the drug out of the CNS. The patient’s symptoms werecompletely resolved with bicarbonate therapy and never required any extra-corporeal therapy.
244
RISK FACTORS FOR BACTEREMIA IN HEPATITIS CVIRUS-INFECTED HEMODIALYSIS PATIENTS
Chebrolu P1, Colombo R1, Baer S2, Nahman N1,2, Kheda M1, KintzigerK1,2. 1Georgia Health Science University, Augusta, GA and 2Charlie NorwoodVAMC, Augusta, GA.Purpose of Study: Hepatitis C virus (HCV) is a major cause of liver diseasein hemodialysis (HD) patients and a known modulator of the innate andadaptive immune systems. We have previously shown that HCV infection isassociated with an increased risk of bacteremia (BAC). However, little isknown about the factors that influence this risk. We hypothesized that pre-vious infectious, autoimmune and/or immunosuppression-associated comor-bidities may impact risk of bacteremia in HCV positive HD patients.Methods Used: All HCV+ incident HD cases from the years 2005-2008from the United States Renal Data System were included in the analysis.Comorbidities were defined by ICD9 diagnosis codes, and included infec-tious comorbidities, autoimmune conditions, immunosuppressive states, andother known risk factors for BAC.Summary of Results: The analysis included 7596 HCV+ HD patients fromthe 4 yr period of study. BAC occurred in 39% of the group. The median agewas 63.4 years, 67% were male, 53% African American, and 44% Cauca-sian. Catheter was the vascular access type at the time of first dialysis for85%, AVfistula for 10%, and AVgraft for 4%. 8% had a history of IV druguse, and 25% had cirrhosis.Of factors significantly associated with increased risk of BAC on univariableanalysis, prior or concurrent methicillin resistant Staphylococcus aureus(MRSA) colonization [adjusted relative risk (aRR) 1.89, 95% confidenceinterval (CI) 1.65-2.15], total parenteral nutrition (TPN) [aRR 1.72, 95% CI1.39-2.12], candidemia [aRR 1.71, 95% CI 1.28-2.28], and catheter as initialvascular access type [aRR 1.59, 95% CI 1.36-1.85] were associated with thehighest risk of BAC after adjusting for all other significant vari-ables including cirrhosis. Evaluated autoimmune conditions, diabetes mel-litus, IV drug use, age, race and gender were not significantly associated withrisk of BAC. Having undergone a transplant was negatively associated withBAC on adjusted analysis.Conclusions: Infectious comorbidities, such as MRSA colonization andcandidemia, represent major risk factors for BAC in HD patients with HCV.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 441
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

In contrast, autoimmune disorders presented a non-significant association.Clinical suspicion for BAC should be heightened in HCV+ HD patients whoare affected by infectious comorbidities.
245
RISK FOR MORTALITY IN HEMODIALYSIS PATIENTS WITHBLOOD STREAM INFECTION: A COMPARISON OFBACTEREMIA AND CANDIDEMIA
Colombo RE1, Chebrolu P1, Baer S2,1, Whitlow M1, Kheda M1, EllingtonC1, Baulkmon E1, Nahman N1,2, Kintziger K1,2. 1Georgia Health SciencesUniversity, Augusta, GA and 2Charlie Norwood VAMC, Augusta, GA.Purpose of Study: Blood stream infection (BSI) is a common cause ofmortality in hemodialysis (HD) patients. Most data for BSI in this groupfocuses on bacteremia (BAC). However, we have shown that HD patientsare also susceptible to candidemia (CAN), the risk of which is magnified byprior or concurrent BAC (Colombo, IDSA presented, 2012). On this basis, wesought to characterize the risk of death in HD patients from BSI accordingto BAC or CAN.Methods Used: All incident HD cases from the United States Renal DataSystem for calendar years 2005-2008 were queried for a diagnosis of BAC,CAN and several potential clinical covariates, using ICD-9 diagnosis codes.The first episode of a BSI was used in the analysis. Descriptive statistics,adjusted log-binomial regression, and survival analysis were performed.Summary of Results: For the 4-year period of study, 362,799 incidentHD patients were available for analysis. BSI was identified in 79,838 (22%).BAC accounted for the majority (99.26%) of BSI. CAN was identified asthe primary BSI in 174 (0.22%); concomitant CAN+BAC was found in 418(0.52%) patients. Risk factors for BSI included age 9 65 years, diabetes mel-litus, HIV, Candida colonization, total parenteral nutrition and HD vascularaccess. In this regard, the adjusted relative risk for BSI from a dialysis cath-eter when compared to a fistula was 1.80 (95% confidence interval (CI) 1.76-1.85). BSI represented a significant risk for death [hazard ratio (HR) 1.61,95% CI: 1.59-1.63]. When compared to BAC, primary CAN was associatedwith a greater hazard of death [HR 2.16; 95% CI: 1.82-2.55 vs. 1.61; 95%CI: 1.59-1.63, for CAN vs. BAC, respectively]. Concomitant CAN+BAC in-fection conferred a hazard of death of 1.99 (95% CI: 1.77-2.23).Conclusions: Nearly one quarter of incident HD patients may experienceBSI due to BAC or CAN. In HD patients, BSI is associated with increasedrisk of death; initial infection with CAN confers the greatest risk of mortal-ity. Heightened awareness of the risk factors for both BAC and CAN mayhelp decrease the risk of death from BSI in HD patients.
246
DELAYED DIAGNOSIS OF A CLASSIC PRESENTATION OFGITELMAN SYNDROME
Crespo-Salgado J, Straatmann C. LSUHSC, New Orleans, LA.Case Report: Gitelman syndrome is an autosomal recessive disorder thatcan present with variable symptoms and characteristic set of metabolic ab-normalities including metabolic alkalosis, hypokalemia, hypomagnesemia,hypocalciuria and increased plasma renin level with normal blood pressure(BP.) We present a case report of an adolescent who presented with severeleg weakness in whom diagnosis of Gitelman syndrome was delayed. Patientis a 17 y/o female with noncontributory past medical history who presentedto the ER with chief complaint of 3 days of progressive lower extremityweakness, foot paresthesias and difficulty ambulating with unsteady gait. Shealso had complaint of chronic posterior cervical pain. Physical exam revealedmild ptosis of left eye and decreased strength in bilateral lower extremities.Patellar and Achilles reflex were unable to be elicited and patient was unableto ambulate without assistance. Additionally our patient had a 5 cm hardcalcified nodule at posterior cervical region consistent with chondrocal-cinosis. Vital signs including BP were normal. Because of her impressiveweakness and abnormal gait, she was admitted to neurology service for furtherevaluation. MRI of the head and spine was normal. Laboratory work revealedserum sodium of 142mmol/L, potassium 1.8mmol/L, calcium 8.9mmol/L,magnesium 0.9mg/dL and bicarbonate of 39mmol/L. She was transferred toICU and nephrology was consulted for severe hypokalemia and hypomag-nesemia. ABG revealed a pH of 7.54 and pCO2 of 37.6mmol/L consis-tent with metabolic alkalosis. Her urine calcium:creatinine was 0.03 mg/mg
(nl G0.2 mg/mg) and plasma renin level was elevated at 1135ng/dL/hr (nl 70to 330 ng/dL/hr.) Family history revealed a sister with Gitelman syndromediagnosed at 9 y/o. Our patient’s striking laboratory abnormalities, examfindings and positive family history confirmed the clinical diagnosis ofGitelman syndrome.Weakness is a frequent chief complaint and clinicians should be aware ofother non-neurologic differential diagnoses such as Gitelman syndrome forprompt diagnosis and treatment. Early recognition of Gitelman syndrome canavoid unnecessary consultations and procedures. Knowledge of the diseaseand appropriate treatment with electrolyte supplementation can limit mor-bidity and mortality.
247
PRORENIN LEVELS IN THE URINE OF PATIENTS WITHDIABETES: A POTENTIAL BIOMARKER OF INTRARENALRAS ACTIVATION?
Dawkins G1, Accavitti M1, Luffman C1, Thethi T1,2, Prieto M1,2,3. 1TulaneUniversity School of Medicine, New Orleans, LA; 2Tulane University Schoolof Medicine, New Orleans, LA and 3Tulane University School of Medicine,New Orleans, LA.Purpose of Study: During diabetes there is increased activity of intrare-nal renin-angiotensin system (RAS) in animals and humans. Prorenin ishighly secreted by the collecting duct cells in animal models of diabetes. Wehypothesize that type II diabetic patients exhibit increased levels of urinaryprorenin due to activation of intrarenal RAS.Methods Used: Cross-sectional study that included urines from 72 dia-betics and 180 non-diabetics. The urine samples were concentrated 10X usingMillipore filters (Catalog UFC801096, EMD Millipore, Billerica, MA). Spe-cific human prorenin concentrations were measured by enzyme-linked im-munosorbent assays (ELISA, Catalog HPRENKT-NP, Molecular Innovations,Novi, MI), and by urine creatinine concentration, and reported as ng ofprorenin/g of creatinine.Summary of Results: Diabetics showed higher levels of urinary prore-nin (263.4T36.07 ng prorenin/creat) than non-diabetics (65.54T13.69 ngprorenin/creat; pG0.0001). Over 60% of the diabetic and non-diabeticpatients were women. Diabetic men exhibited higher levels than non-diabeticmen (pG0.0001). Similar findings were observed in women (pG0.001). 61.1%of the diabetics and 38.9% of the non-diabetics were African-American. Al-though urine levels of prorenin were significantly higher in diabetic Caucasiansthan non-diabetic Caucasians (pG0.05) this difference was even greater inAfrican-Americans (pG0.0001).Conclusions: The data indicates that urinary prorenin levels are signifi-cantly higher in diabetic than non-diabetic patients. Urinary prorenin levelsdid not display sex- or racial disparities. Thus, urinary prorenin could be apotential biomarker of intrarenal RAS activation in diabetic patients. Inves-tigations on the effects of direct renin inhibition on collecting duct prore-nin and its consequences on tubulointerstitial and renal microvascular injuryin diabetic patients, are needed.
248
VIRAL INFECTION AS A RISK FACTOR FOR DELAYEDGRAFT FUNCTION IN KIDNEY TRANSPLANTATION
Ellington CL1, Ghaffari A2, Merchen T2, Colombo R1, Baer S1, Kheda M1,Chebrolu P1, Whitlow M1, Nahman NS1, Kintziger K3. 1Georgia HealthSciences University, Augusta, GA; 2Georgia Health Sciences University,Augusta, GA and 3Georgia Health Sciences University, Augusta, GA.Purpose of Study: Delayed graft function (DGF), defined as a need fordialysis in first week after transplantation, is a major risk factor for chronicallograft loss. Ischemia time is a primary cause of DGF and current clinicalprotocols strive to minimize this period. Despite the dominance of ische-mia with DGF, other factors may play a role. In previous work we haveshown that viral infection may increase the risk of vascular access failure indialysis patients, presumably through subclinical vascular damage. It is un-clear if viral infection in kidney recipients may also be a risk factor for DGF,and so we queried the U.S. Renal Data System (USRDS) for the effects ofviral infection on DGF in kidney transplant recipients.Methods Used: All adult, first-time renal transplant cases reported to theUSRDS from 1994-2009 were queried for HCV, HBV, CMV, EBV, and HIV
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
442 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

serologies and assessed for an association with DGF. Descriptive statisticsand multivariate logistic analysis were performed.Summary of Results: During the study period, 235,449 patients wereavailable for analysis and 38,347 had complete data for DGF and all viralserologies. Demographics included a mean age of 51yrs, 61% male, 60% Cau-casian and 25% AA. 65.6% of transplants were from deceased donors. DGFwas identified in 6,335 (16.5%) patients. The percent with positive viralserologies included: HCV (5%), HBV (7.8%), CMV (64.2%), EBV (83.3%)and HIV (0.5%). Using multivariate analysis, the odds ratio (OR) and 95%CL of DGF associated with each virus were: HCV (OR: 1.424; 1.271, 1.595),HBV (OR: 1.072; 0.972, 1.183), CMV (OR: 1.197; 1.125, 1.273), EBV (OR:1.198; 1.107, 1.296) and HIV (OR: 2.394; 1.739, 3.295). Cold ischemia time,donor creatinine, and donor type were also significantly associated with DGF.Conclusions: DGF was identified in 16.5% of kidney transplant patientsfrom the USRDS. After controlling for donor creatinine, cold ischemia time,and donor type, all viral test results were significantly associated with DGF,except for HBV. Addressing the potential vascular and immune effects ofviral infection in kidney recipients may improve the risk of DGF followingtransplantation.
249
EXTREME PSEUDOHYPERKALEMIA IN A PATIENT WITHACUTE MYELOGENOUS LEUKEMIA
Elmahi N, Basu A. University of Mississippi Medical Center, Jackson, MS.Case Report: Background: Pseudohyperkalemia is a challenging diag-nosis, which is often linked to patients with extreme leukocytosis. We de-scribe a unique case of possible pseudohyperkalemia associated with extremeleukocytosis.Case History: 55 year old African American diagnosed with acute myelog-enous leukemia and refused chemotherapy. His WBC was moderately ele-vated with normal potassium (K) during a routine onclogy visit on July 282011. Subsequent visits revealed progressive hyperkalemia and worseningleukocytosis. On August 18, he refused hospital admission for K Llevel of8.8 mmol/l with normal ECG. On August 22 he came to the hospital forevaluation of shortness of breath. Initial work up was significant for K of15.3 mmol/l, WBC of 403 th/cmm and Creatinine of 1.6 mg/dl. Repeat K thenext day was 15.5 mmol/l (Table 1).Initial and repeat ECGs showed atrial flutter with no findings suggestive ofhyperkalemia. Careful handling of the sample, measurement of plasma po-tassium and measurement of potassium in arterial blood gas (ABG) were nothelpful in establishing the diagnosis of possible pseudohyperkalemia.The patient and family refused aggressive interventions (dialysis and leu-kophresis) and chose comfort care. Diagnosis of pseudohyperkalemia wasassumed and no further treatment was offered. His EKG continue to showno evidence of hyperkalemia.Conclusions: Our case illustrates the importance of considering pseudo-hyperkalemia as a cause of elevated potassium in patients with substan-tial leucocytosis who do not have clinical findings or ECG changes suggestiveof hyperkalemia. The comparison of serum and plasma potassium and mea-surement of potassium in ABG may help in establishing the diagnosis ofpseudohyperkalemia. However, the diagnosis should not be fully excludedbased on negative results. The diagnosis should be considered in the rightclinical setting even in the absence of confirmatory tests since aggressivetreatment can lead to life-threatening hypokalemia.
250
SOLITARY KIDNEY AUTOTRANSPLANTATION; ANALTERNATIVE TO DIALYSIS COMMITMENT IN A PATIENTWITH SIGNIFICANT VASCULAR DISEASE
Elmahi N, Kokko K, Fulop T, Hamrahian S. University of MississippiMedical Center, Jackson, MS.
Case Report: Case Report: 41 yr old African American female presentedto the hospital with bilateral lower extremities and mesenteric ischemia dueto extensive thrombosis of the abdominal aorta (AA). Computer topographicangiography showed an isolated patent segment of the AA at the level ofrenal arteries. The patient underwent a complex thoraco-abdominal bypasssurgery with a four-limb graft; 1st limb to the superior mesenteric artery,2nd limb to the isolated patent segment of AA, and 3rd and 4th limbs tofemoral arteries. Further work up revealed low levels of protein C, proteinS and antithrombin III. Patient was discharged on long-term anticoagula-tion, but unfortunately she lost follow up and stopped her anticoagulation.Two years later she presented to the hospital with acute kidney injury (AKI)and volume overload that required intermittent hemodialysis (HD). Herblood pressure (BP) remained elevated despite ultrafiltration and multipleantihypertensive medication use. Extensive work up without use of con-trast revealed inoperable occluded graft limb to AA and a non-functionalatrophic left kidney with inadequate blood flow to the right kidney. Renalbiopsy of the right kidney showed severe tubular necrosis and viable tis-sue. Based on the tissue viability, she underwent renal autotransplantationof the right kidney. Following her procedure, she recovered from AKI andhad BP well controlled on a single agent. Her creatinine was 0.75 mg/dl 3months post RAT.Conclusions: In conclusion renal autotransplantation is a rare procedurethat is technically demanding with several potentially serious complications.The procedure is underutilized and in the correct settings, it may be ofgreat utility. It should be considered as alternative to dialysis in patientswith severe peripheral artery disease. Our case illustrates an alternativetherapeutic approach to lifelong HD commitment and to resistant hyper-tension in a patient with solitary kidney and inoperable renal vascular per-fusion disorder. Multidisciplinary team approach is the key factor for such achallenging surgery.
251
DESMOPRESSIN, AN EFFECTIVE ADJUNCT TREATMENT,FOR REVERSING RAPID CORRECTION OFHYPONATREMIA AND PREVENTION OF OSMOTICDEMYELINATION SYNDROME
Elmahi N, Hamrahian S, Fulop T. University of Mississippi Medical Center,Jackson, MS.Case Report: Background: Osmotic demyelination syndrome (ODS) is adevastating consequence of rapid correction of chronic hyponatremia. Thepresence of hypokalemia at the time of presentation will add to the risk ofODS. Uncontrolled large free water diuresis could complicate the correc-tion of hyponatremia, once underlying etiology (e.g. nausea) is controlled.We present a unique case illustrating the added value of ADH analog ineliminating erratic polyuria and simplifying management of these patients.Case History: A 50-year-old male was admitted to the intensive care unit after3 seizure episodes. He had nausea and vomiting for two weeks prior toadmission and was drinking large amounts of water and carbonated beveragesin an attempt to control his chronic hiccups. Laboratory results on admissionshowed sodium 107 mmolL, potassium G 1.5 mmol/L, chloride G 60 mmol/L,bicarbonate 38 mmol/L, PH of 7.60 and a serum osmolality 217 mOsm/kg.He was treated with 3% saline and then maintained on 0.9% saline. Aftersuccessful medical management of his nausea, he developed polyuria of 6 Lover 8 hours with low urine osmolality of 60 mOsm/kg. His serum Na+increased to 126 mmol/L within 12 hours after admission. His free water deficitwas replaced over 10 hours (initial Na+ target of 120 mmol/L). Desmopressinwas initiated at 1 mcg IV and then increased to 2 mcg IV twice daily. Fewhours after initiation of desmopressin, his Na+ dropped to 118 mmol/L andhis urine output decreased to around 2 L/day. His sodium was then correctedby 2-3 mmol/L/day. His hypokalemia and metabolic alkalosis was correctedslowly over the period of few days. At the time of discharge, the serum Na+was 130 mmol/L, hypokalemia was corrected and he had fully recoveredwithout neurologic sequelae.Conclusions: Overcorrection of hyponatremia is often blamed on overzealouscorrection with hypertonic IV fluids. The condition is often complicated byuncontrolled large free water diuresis. Use of ADH analog could provide acontrolled correction of hyponatremia by limiting urine output and controlunpredictable free water losses.
Lab Results
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 443
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

252
MAINTENANCE OF RESIDUAL RENAL FUNCTION WITHLOW DOSE IMMUNOSUPPRESSIVE THERAPY INPERITONEAL DIALYSIS PATIENT WITH ALLOGRAFTFAILURE
Elmahi N, Kokko K, Fulop T. University of Mississippi Medical Center,Jackson, MS.Case Report: Background: Many patients with failed allograft progressto end stage renal disease (ESRD) and require dialysis. Immunosuppressivetherapy is often withdrawn in those patients and this can lead to an acceler-ated loss of residual renal function (RRF). While maintenance of RRFappears to provide a survival benefit to peritoneal dialysis (PD) patients, it isnot clear whether this benefit of maintaining RRF in failed allograft pa-tients returning to PD outweigh the risks of maintaining immunosuppression.This case report addresses the role of minimal dose of immunosuppressionin maintaining RRF in PD patient with failed allograft.Case History: A 49 year-old Caucasian male developed progressive allo-graft failure nine years after living-donor renal transplantation (LDRT).Hemodialysis was initiated via tunneled dialysis catheter (TDC) and immu-nosuppression was gradually withdrawn. Two weeks after the withdrawalof the immunosuppressive therapy he developed a febrile illness, which ne-cessitate removal of the TDC and conversion to PD. He was maintainedon small dose of tacrolimus (1 mg daily) and prednisone (5 mg daily).Currently (1 year later) he is doing exceedingly well on cycler-assisted PD.Residual urine output ranges between 600-1200 mL/day. Total weekly Kt/Vachieved 1.82.Conclusions: When a renal transplant fails, the nephrologists will bechallenged by two major decisions: optimal management of immunosup-pression and whether or not to perform graft nephrectomy. The use of lowdose immunosuppressive medications in failed renal allograft is the mostreasonable approach. There is no clear evidence to support the superiority ofhemodialysis or peritoneal dialysis in the treatment of patients with failedallograft who progress to ESRD. Our patient failed renal transplant and wasdeclared ESRD. Peritoneal dialysis was initiated and he was maintainedon minimal immunosuppressive regimen, which helped to maintain goodRRF. This strategy will need further study in well-defined cohorts of PDpatients with failed allografts and residual renal function to determine effi-cacy and safety.
253
TUNNELED DIALYSIS CATHETER INFECTION ANDTROPONINE-I LEVELS IN END-STAGE RENALDISEASE PATIENTS
Gharaibeh K1, Guild CS1, Hamrahian SM1, Lengvarszky Z2, Csongradi E3,Fulop T1. 1University of Mississippi Medical Center, Jackson, MS;2Louisiana State University, Shreveport, LA and 3University of Debrecen,Debrecen, Hungary.Purpose of Study: End-stage renal disease (ESRD) patients on dialysisare known to have elevated levels of cardiovascular enzyme markers, suchus troponin-I. Our hypothesis was that infection of tunneled hemodialysiscatheters (TDC) may be associated with such enzyme leakMethods Used: We performed a retrospective cohort review of our con-secutive 3-year experience (01/2007 - 12/2009) with bedside TDC removalat the University of Mississippi Renal Fellowship Program. We collecteddata on multiple patients and procedure-related variables. The study was re-viewed and approved by the University of Mississippi Human Research Office.Data was analyzed with PAWS Statistics 18 and reported with means TSDor medians 25-75% IQR for descriptive data; Pearson’s correlation andindependent-samples T test was utilized for statistical comparisons.Summary of Results: During the index period, we had 55 inpatient TDCremovals by the renal training program. Indication at the time of removalincluded bacteremia, fever or clinical sepsis with hemodynamic instabilityor respiratory failure. The majority of TDC removals took place on generalfloor (63.6%), with the rest of them either in ED (12.7%) or ICU (16.3%)settings, with a median time of 3 days [IQR 1-13] elapsed since admission orTDC placement. Four (7.2%) patients were hypothermic, 33 (60%) febrile orsubfebrile (T937 Co) at time of removal; 7 (12.7%) on vasoactive pressors. Ator around the time of removal, mean heart rate was 95.6T20.6 beat/min,
systolic BP nadir 116.5T20.7 mmHg and diastolic 64.9T12.3 mmHg. PeakC-reactive protein (available in 63.6% of cohort) measured was 12.9T8.4 mg/dl (nlG0.49) and mean troponin-I (34% available) was 0.127 ng/ml[IQR 0.03-0.9] (nlG0.034) and they did not correlate with each other.Troponin-I had a strong trend with proven bacteremia (p=0.075) but notwith fever, systolic and diastolic BP or clinical sepsis.Conclusions: While our results are suggestive of a possible associationof TDC-induced bacteremia and elevated troponin-I levels in ESRD patients,additional investigations are warranted for definitive conclusion.
254
DESMOPRESSION FOR HYPONATREMIAOVERCORRECTION: AN EFFECTIVE ADJUNCTTREATMENT FOR REVERSING RAPID OVERCORRECTIONAND OSMOTIC DEMYELINATION SYNDROME
Gharaibeh K1, Elmahi N1, Csongradi2, Fulop T1. 1University of MississippiMedical Center, Jackson, MS and 2University of Debrecen, Debrecen,Hungary.Case Report: Background. Correction of hyponatremia, particularly in thepresence of coexisting electrolyte abnormalities, can be challenging espe-cially when water diuresis emerges during therapy. We present a uniquecase illustrating the added value of desmopressin in eliminating erratic largeurine output and simplifying management of severe hyponatremia in thesepatients.A 50 year old African American male with hypertension and chronic in-tractable hiccups presented to our hospital after three episodes of seizure andwith nausea and daily vomiting for two weeks. In an attempt to control hishiccups, he had been drinking large amounts of water and carbonated bev-erages. Laboratory tests revealed sodium 107 mM/L, unmeasurably lowpotassium (G1.5 mM/L), chloride G 60 mM/L, bicarbonate of 38 mM/L,blood pH of 7.60, and serum osmolality 217 mOsm/kg. Seizures were con-trolled with 3% saline IV bolus, and hiccups, nausea and vomiting werecontrolled promptly with antiemetics. However, shortly after admission, hedeveloped large volume free water diuresis with 6 L of dilute urine in 8 hours(initial Uosm 60 mOsm/kg; repeated 40 mOsm/kg) and serum Na+ climbedto 126 mM/L over just 12 hours. On exam, he was alert but drowsy. Desmo-pressin was initiated at 1 mcg IV, and then increased to 2 mcg twice daily, toconcentrate the urine. To temporarily reverse the sodium increase, the patientwas simultaneously treated for 10 hours as if a free water deficit existed.Serum sodium dropped to 118 mM/L, and urine output decreased to e2 L/dayfor the next several days. Serum sodium was then corrected by 2-3 mM/L perday until reaching 130 mM/L. Potassium was slowly corrected with resultantcorrection of metabolic alkalosis. The patient experienced no further neu-rologic sequelae.Conclusion. Overcorrection of hyponatremia with aggressive hydration canlead to uncontrolled free water diuresis, with polyuria being a warning sign.The addition of an antidiuretic hormone analog, such as desmopressin, canlimit urine output and prevent unpredictable free water losses to enable tar-geted correction, simplifying management for these complex scenarios.
255
CORYNEBACTERIUM AMYCOLATUM BACTEREMIAIN A HEMODIALYSIS PATIENT
Grewal RK1,2, Simon E1,2. 1Tulane School of Medicine, New Orleans, LAand 2The Veterans Affairs Hospital, New Orleans, LA.Case Report: Corynebacterium species except C. diptheriae are part of nor-mal skin flora and mucous membranes and are usually considered as con-taminants when isolated from diagnostic specimens. There are only a fewcase reports of C. amycolatum causing infections including endocarditis andmastitis. The majority of these infections were either in immunocompro-mised patients or patients with intravascular devices. To date, it remainsan uncommon cause of bacteremia. Here we describe a case of C. amyco-latum bacteremia in a hemodialysis (HD) patient.A 52 yr old male with history of end stage kidney disease on HD via tunneledHD catheter was admitted to the hospital with fevers, chills and cough withyellow sputum. The patient was diagnosed with pneumonia and treated withvancomyin and piperacillin/tazobactam. Blood cultures grew diptheriodsand were considered as contaminants. The patient remained afebrile after
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
444 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

finishing a 7 day antibiotic course. One month later in the HD unit, the patientstarted complaining of feeling febrile and having chills at home. Bloodcultures were sent which grew diptheroids and were again considered ascontaminants. One week later, the patient developed chills while on HD andspiked a fever up to 102F. The patient was started on vancomycin and cef-tazidime after two sets of blood cultures were drawn. All four bottles grewdiptheroids again and were sent to an outside laboratory for further strainand sensitivity testing. The final culture report showed C. amycolatum sensitiveto vancomycin only.Ceftazidime was discontinued and the patient received4 weeks of vancomycin with HD. The HD catheter was also changed over aguidewire and tip culture from catheter did not grow any diptheriods butthe patient was already receiving antibiotics.Transthoracic echocardiogramdid not show any vegetations. The patient remained afebrile and his symptomsresolved.
Isolation of diptheroids from blood cultures are generally skin con-taminants However, this case emphasizes the importance of consideringdiptheriods as a significant pathogens in the appropriate setting and the needfor thorough investigation to identify the strain and antibiotic sensitivities.
256
NEW ONSET MALIGNANT HYPERTENSION WITHTHROMBOTIC MICROANGIOPATHY ASSOCIATED WITHPRIMARY HYPERALDOSTERONISM IN A PATIENT ONPERITONEAL DIALYSIS
Heegard K, Penagaluru N, Salazar M, Bansal S. UTHSCSA, San Antonio, TX.Case Report: End stage renal disease (ESRD) patients rarely developmalignant hypertension (HTN), especially in the absence of hypervol-emia. Thrombotic microangiopathy (TMA) is a common complication ofmalignant HTN but has not been reported in setting of malignant HTN in adialysis patient. Malignant HTN and TMA in euvoelmic dialysis patientraises concern for secondary HTN. Here we report a case of new onsetmalignant HTN with TMA despite aggressive ultrafiltration secondary toprimary hyperaldosteronism.Case: 21 yo male with ESRD of unknown etiology, on Peritoneal dialysis for26 months with normal BP without need for antihypertensive medications, pre-sented with sudden onset headache, blurry vision and BP of 190/110 mm/Hg. Hewas euvolemic on examination. Chest X-ray revealed only mild interstitialedema. He remained hypertensive despite increasing ultrafiltration, and es-calating antihypertensive therapy including enalapril, metoprolol and nifed-ipine. Retinal exam showed copper wiring, cotton wool spots and flamehemorrhages consistent with malignant HTN. His Hgb decreased from 10.2to 4.4 gm/dl and platelets from 140 to 33x109/L. A hemolysis work up wasconsistent with TMA, which was attributed to malignant HTN sinceADAMTS13 activity and vasculitic work up were negative. Initial evaluationfor secondary HTN demonstrated negative drug screen, normal catechol-amine levels, plasma aldosterone (PAC) of 23 ng/dl and plasma renin activity(PRA) of 2.1 ng/ml/hr. Later off enalapril his PAC was 85.3 ng/dl and PRA0.8 ng/ml/hr with PAC:PRA of 106 concerning for primary hyperaldo-steronism. CT abdomen did not find any adrenal pathology. A confirmatorysaline infusion test was not pursued due to risk of volume overload in ESRDpatient. His BP normalized with increasing doses of above medications, Hgbremained stable after blood transfusion, platelets gradually increased to 92 x109/L and visual symptoms resolved at one month follow up. Conclusion:This case is a rare example of TMA as a result of malignant HTN in ESRDpatient without hypervolemia which highlights the importance of early di-agnosis of malignant HTN and evaluation for secondary causes of HTN inabsence of response to aggressive ultrafiltration.
257
THROMBOCYTOPENIA AFTER INITIATIONOF HEMODIALYSIS
Hernandez AJ, Nimkevych O, Owen J. LSUHSC-NO, New Orleans, LA.Case Report: INTRODUCTION: The incidence of heparin-induced throm-bocytopenia in newly treated dialysis patients is estimated at 3.9%. Dialyzermembrane reactions resulting in thrombocytopenia have also been documented
with the use of electron-beam sterilized membranes. We present a case of apatient who became thrombocytopenic after initiation of hemodialysis.CASE: An 82 year-old woman with chronic kidney disease stage 4, hyper-tension, and uncontrolled diabetes mellitus type 2 was admitted to the hos-pital with hypoglycemia, altered mental status, deep venous thrombosis andworsening kidney function. She was afebrile and hemodynamically stable.Physical examination was unremarkable, except for confusion and a chronicopen wound in the medial aspect of her right foot. The CBC showed WBC9.1 x 103/KL, hemoglobin 9.2 g/dL, hematocrit 27% and platelets 276,000/KL.Glucose was 48 mg/dL, BUN 12 mg/dL, creatinine 3.26 mg/dL, esti-mated GFR of 16 mL/min/1.73m2. Phosphorus was 5.2 mg/dL. The patientwas started on hemodialysis seven days after admission due to worseningkidney function. Heparin was given during placement of the dialysis cath-eter and during the first three dialysis treatments. Her platelets droppedsignificantly from 276,000/KL to 14,000/KL and heparin was held. Heparininduced thrombocytopenia (HIT) was considered the likely diagnosis andtreatment with argatroban was initiated. Platelets failed to recover and later,HIT was ruled out with HIT antibodies of 0.444 (0.000 to 0.4000) and anegative serotonin release assay. Further laboratory values showed that theplatelet count decrease post dialysis, and increase during her intradialyticdays. A correlation between dialysis treatment and thrombocytopenia wasestablished. After reviewing the literature about dialysis associated throm-bocytopenia, the electron-beam sterilized dialyzer membrane was changed toa polysulfone non-e-beam sterilized hemodialysis membrane with resolu-tion of her thrombocytopenia.DISCUSSION: The proper therapy of thrombocytopenia that develops inpatients undergoing hemodialysis requires the correct diagnosis. Although un-common, adverse reactions to hemodialysis membranes can occur. The lackof improvement of the thrombocytopenia and the pattern of platelet count preand post dialysis help establish an association between the dialyzer mem-brane and thrombocytopenia.
258
ACUTE KIDNEY INJURY FOLLOWING RETROGRADEPYELOGRAM
Hirachan P1, Polnaszek NM1, Martinez M1, Wagner B1,2. 1University ofTexas Health Science Center at San Antonio, San Antonio, TX and 2SouthTexas Veterans Health Care System, San Antonio, TX.Case Report: Introduction:Acute kidney injury (AKI) is a rare complica-tion following retrograde pyelogram. Case:A 59 yrs old man presented forevaluation of abdominal pain and decreased urine output for 24hrs dura-tion. He denied any symptoms of infection or NSAID use. A day prior topresentation, he had undergone a cystoscopy with bilateral (b/l) retrogradepyelogram for evaluation of chronic hematuria. His past medical historyincluded CKD III (baseline creatinine of 1.6 mg/dl), HTN, sleep apnea, obes-ity, severe diastolic dysfunction and dyslipidemia. Per Urology, cystoscopywas unremarkable, except that high pressures were encountered while in-jecting the contrast medium (Loversol) during retrograde pyelogram. Onadmission, physical exam revealed b/l pulmonary rales, lower extremityedema and blood urea nitrogen (BUN)/creatinine of 38/3.9 (mg/dl). Urinemicroscopy revealed numerous non-dysmorphic red blood cells without anycasts appreciated. Initial workup for acute kidney injury was unremarkableexcept for evidence of mild b/l hydronephrosis and contrast material withinthe renal parenchyma on CT scan of abdomen and pelvis. On the next day ofadmission, his clinical course deteriorated with worsening shortness of breathand urine output of only 30 cc/24 hr. Repeat imaging revealed stable mild b/lhydronephrosis with persistent contrast material within the renal parenchyma.He had potassium of 5.7 mmol/L with BUN/Creatinine of 65/7.25 (mg/dl).He was started on hemodialysis emergently. The patient required daily dial-ysis for 6 consecutive days. Finally, the patient’s urine output and creatinineimproved and no further dialysis treatments were required. He was dis-charged home at his baseline creatinine of 1.6 mg/dl after 12 days in thehospital. Conclusion: We presume this unusual episode of anuria follow-ing retrograde pyelogram is secondary to a combination of pyelotubular andpyelolymphatic reabsorption of contrast medium along with contrast inducedinterstitial inflammation and edema. Our patient’s initial presentation, clinicalcourse requiring renal replacement therapy and renal recovery is similar to
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 445
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

that documented in the literature for contrast-induced nephropathy post ret-rograde pyelogram.
259
A CASE REPORT OF MUCKLE-WELLS SYNDROME ANDSECONDARY AMYLOIDOSIS (AA) WITH NEPHROPATHY
Javed T. 1Ochsner Clinic Foundation, Neo Orleans, LA and 2OchsnerHospital Center, Metairie, LA.Case Report: A case report of Muckle-Wells Syndrome and SecondaryAmyloidosis (AA) with Nephropathy.T. Javed MD, C. Staffeld MD, S. Bodana DO, Department of Nephrol-ogy, Ochsner Clinic Foundation, New Orleans, Louisiana.A 75 year old white male presented to the hospital with nausea, vomiting andabdominal pain. He was also found to have acute on chronic renal failure withnephrotic range proteinuria along with episodic fever and hearing loss. Hispast medical history is significant for BPH, GERD, arthritis, anxiety and skinrash. His son and daughter also have similiar symptoms. Rheumatologicalwork up was negative. He was clinically diagnosed with Muckle-Wellssyndrome on this admission. Patient underwent a renal biopsy which showedseconday Amyloidosis (AA). Incidence of AA amyloidosis in Muckle-Wellssyndrome is 25 percent. Muckle-Wells syndrome consists of periodic fever,urticaria, arthralgia and deafness. Muckle-Wells syndrome is transmitted byan autosomal dominant trait. In Muckle-Wells syndrome, there is a mutationin cryopyrin gene (CIAS1) on chromosome 1q44. In clinical practice, renalfailure due to amyloidosis and Muckle-Wells syndrome is rare and should beconsidered as differential diagnosis in difficult cases of renal failure.
260
MEMBRANOUS NEPHROPATHY SECONDARYTO SYPHILIS
Kumbala D, Alper A. Tulane University School of Medicine, New Orleans, LA.
Case Report: A 41-year-old African American male with a past medicalhistory of HIV for last 16 years, the last CD4 count being 1474, was admittedto the hospital complaining of leg swelling and macular papular rash. He wason valsartan atazanavir, combivir; allergies include penicillin which causedSteven Johnson reaction.On exam 145/87; 1 to 2+ pitting edema extending to the knees bilater-ally and maculopapular rash involving the hands and soles of his feet. Renalfunction was normal, albumin level of 1.6; RPR positive at 1:128 with con-firmatory MHA-TP Urine studies showed protein 600mg/dl and 18 red bloodcells; urine-protein-creatinine ratio of 5.7gm, renal biopsy showed mem-branous glomerulopathy..IF positive for granular IgG and C3 along the capillary loops fig 1, fig 2 EMshows sub epithelial deposits.He was started on doxycycline, furosemide and lisinopril. After completion ofantibiotic course, his symptoms, signs and proteinuria resolved completely.
261
PSEUDOHYPERKALEMIA- LOOK BEFORE YOU TREAT
Kumbala D, Pasala R, Batuman V. Tulane University School of Medicine,New Orleans, LA.Case Report: 57 year old African American male presented with massiveleukocytosis and elevated potassium levels. He was diagnosed with chroniclymphocytic leukemia nearly one year agowas admitted to university hospitalfor induction chemotherapy, tests prior to the induction therapy showed el-evated potassium level of 8.4 with normal renal function. Patient was treatedwith calcium gluconate, dextrose and insulin, kayexalate which brought downthe potassium to 7.2. His review of systems was negative for any symptoms.His medications included amlodipine and hydrochlorothiazide. Normal phys-ical examination including the vitals.Laboratory data showed normal basic metabolic panel except for elevatedpotassium. His complete blood picture was significant for elevated whiteblood cell count of 136,000 with normal platelet count. (EKG) was unre-markable, subsequently plasma potassium level was drawn to rule out pseudohyperkalemia were found to be 4.5, which was 1 mEq/L lower than serumpotassium obtained at the same time. A diagnosis of pseudo hyperkalemiasecondary to leukocytosis was made and he did not recieve any unneces-sary potassium lowering measures He was started on chemotherapy and hisWBC count trended down and also hyperkalemia was resolved. (FiG-1).Series of Blood draws showed in fig 1
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
446 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

262
P53 REGULATES PROGENITOR CELL RENEWAL ANDSURVIVAL IN THE NEPHROGENICNICHE OF THEDEVELOPING KIDNEY
Liu J, Saifudeen Z, El-Dahr S. Tulane Medical School, New Orleans, LA.Purpose of Study: To detect the role of P53 in self-renewal potential ofembryonic stem cells.Methods Used: Microarray. FACS. immunoprecipitate. real-time PCR. in-situ hybridization.Summary of Results: 1. genetically labeled GFP+/Six2p53-/-and GFP+/WT CM consistently gave 30% fewer cap cells from mutant than wild-typekidneys 2. the caps are loosely organized in contrast to the compact aggre-gates of wild-type cap cells around the ureteric tip and exhibit decreased N-cadherin immunostaining. 3. Six2p53-/- caps have greatly diminished Cited1and amphiphysin immunoreactivity at E13.5-14.5. By P0, the CM is com-pletely devoid of Cited1. QPCR analysis of CM markers at E15.5 showedsignificant reduction in expression of Cited1 4. A significant decrease inproliferation, measured by phospho-histone H3-P-S10 immuno-staining, wasobserved in Pax2+ cap cells at E13.5 in Six2p53-/- kidneys. 5. Apoptosismeasured by TUNEL was significantly higher in the caps surrounding ure-teric tips at E13.5. 6.Pax8 and Fgf8 expression was significantly (pG0.05)lower by ISH and qPCR.Conclusions: Based on our data, we propose a model in which p53 pro-motes self-renewal of the multipotent NPCs (Cited1+/Six2+) while pro-moting the differentiation of the induced Six2+ sub-population of NPC tonascent nephrons.
263
LITERACY RATES AMONG HEMODIALYSIS AND KIDNEYTRANSPLANT PATIENTSPerveze Z, Amit P, Podolsky R, Mulloy L. GHSU, Augusta, GA.Purpose of Study: End stage renal disease is a life-long health problemcommonly treated with hemodialysis (HD) or kidney transplantation (KT).The decision to pursue a kidney transplant depends in part on patient un-derstanding of the causes, treatment and prognosis of both modes of therapy.Patient comprehension and understanding of these issues may influence decisionsabout the pursuit of KT. Information relevant to this issue is many times de-pendent on written material provided to patients. Others have shown that lowliteracy rates affect patient decision making. Given the necessity to com-prehend a high volume of complicated issues surrounding KT, often presentedin writing, we theorized that transplant recipients would exhibit a higher rateof literacy than patients on dialysis. To address this question we surveyedHD and KT patients and assessed their reading and comprehension skills.Methods Used: HD patients in the Augusta area and KT recipients fromGHSU were studied. Reading comprehension was assessed using a 66-wordrecognition test which provides an estimate of reading skills in less than3 minutes (Rapid Estimate of Adult Literacy in Medicine - REALM).Summary of Results: 50 HD and 50 KT patients completed the study. AllHD patients were from 3 HD units in Augusta. There were 27 dialysis units oforigin represented in 43/50 KT patients with 22% from Augusta. Seven KTpatients were from unknown dialysis units. When compared to KT, HD patientswere older (55+13 vs 49+15 mean+SD years for HD vs KT, respectively, p G0.05) and primarily African American (AA) (88% vs 48% for AAvs Caucasian,respectively, p G 0.05). There were no differences in the gender distributionbetween the two groups. KT patients scored significantly higher on the REALMtest when compared to HD (96+6% vs 87+14% correct for KT vs HD,respectively, p G 0.05). These data indicate that literacy rates are higher amongKT patients when compared to HD, and that HD patients tended to be AA.Conclusions: KT patients have higher literacy rates than HD, and tend to beCaucasian. Socioeconomic, geographic, and/or educational factors may in-fluence these results. Literacy programs focused on HD patients may improvethe rate of KT.
264
CONGENTIAL NEPRHOTIC SYNDROME WITH WT1MUTATION AND HYPERTENSIVE CRISIS - A TREATMENTCONUNDRUM IN NEWBORN
Rana D, Talati A. University of Tennessee Health Science Center, Memphis, TN.
Case Report: Background: Missense mutations in the Wilm’s tumor (WT1)have been described as cause of Denys’ Drash Syndrome (DDS) which is aprogressive glomerulopathy with urogenital abnormalities in genotypic malesand a predisposition to Wilm’s tumor.
Objective: We present an unusually severe case of Congenital Nephroticsyndrome with severe systemic hypertension associated with WT1 mutationin a newborn.
Case report: A 40 week gestational age African American newborn trans-ferred to our tertiary center for ambiguous genitalia and hypertension withsystolic pressures between (BP) 135 to 141 mm of hg and diastolic BP of 89to 97 mm of hg at day of life (DOL) two. Chromosome karyotype and chro-mosome microarray were normal male, 46 XY. Ultrasound kidneys showedmarkedly increased echotexture of the renal cortices bilaterally. He progressedfrom DOL 4 to DOL 6, with tremendous increase in weight, marked gen-eralized edema and ascites leading to respiratory distress, a large pericar-dial effusion that required pericardiocentesis and bilateral pleural effusions.Also, oligouria with marked proteinuria,persistently low Serum sodiumlevels 125-128 mg/dl and serum albumin 1- 2.4 gm/dl, resistent to anyform of correction. He further developed hypertensive crisis with systolicBP 170-180 mm hg and diastolic BP 110-133 mm hg, requiring nicardipineand beta blocker drips. Despite maximum therapy his clinical course wors-ened and infant died. Autopsy was denied and a renal biopsy was not done.WT1 mutational analysis revealed a novel germline heterozygous nucleotideexchange from T to G at position 1181, resulting in an amino-acid substi-tution from Leu to Arg.
Conclusion: WT1 mutation presenting at birth as congential nephroticsyndrome,ambiguous genitalia with severe systemic hypertension with quickprogression to end stage renal disease can be a fatal disease. This account canhelp clinician provide appropriate counseling and treatment options forfamilies.
265
COLLAPSING VARIANT FOCAL SEGMENTALGLOMERULAR SCLEROSIS WITH COMPLEMENT3 DEPOSITION AND GLOMERULAR BASEMENTMEMBRANE THINNING
Salahuddin M1, Shamim Q1, Salameh J1, Leighton J1, Monteiro C2.1University of Florida, Jacksonville, FL and 2University of Florida,Jacksonville, FL.Case Report: Focal segmental glomerular sclerosis (FSGS) is a clinico-pathologic entity that is associated with various genetic lesions, underly-ing infections or causes yet to be delineated (idiopathic). Collapsing variantFSGS has been described in association with HIV associated nephropathyparticularly in African Americans. We describe the case of a 31 year old whitemale with a history of polysubstance abuse who was ‘‘found down’’ and onpresentation to hospital had oliguria, acute kidney injury (AKI) and a positivetoxicology screen for opiates, benzodiazepines and cocaine. His muscle en-zymes (CPK) were elevated (65,000 Units/Liter) and the patient was diagnosedwith oliguric AKI secondary to rhabdomyolysis. He underwent hemodialysisfor the AKI and tolerated it well. During the diagnostic evaluation, the patientwas noted to have nephrotic range proteinuria (urine Protein/Creatinine 19.2)and normal-sized, non-echogenic kidneys. Of note, he also had staphylo-coccus aureus bacteremia in conjunction with thrombocytopenia, not asso-ciated with indirect hyperbilirubinemia or an acute decline in hemoglobin.Serologic workup was normal with the exception of low C3 and C4 levelsof 34 mg/dl (90-180) and 7 mg/dl (10-40) respectively. Further history re-vealed early onset renal failure in 2 of his relatives and suspected renalcarcinoma in his father. Renal biopsy revealed glomeruli collapse, but nosclerosis was seen. There was increased mesangial matrix without prolifer-ative changes and tubulointerstitial disease was present with regeneration oftubular cells. Immunofluorescence revealed granular C3 staining but no im-munoglobulins were present. Electron microscopy revealed effacement of thefoot processes but no areas of electron dense deposits. In addition, there werefocal areas of thinning of the glomerular basement membrane (GBM). Thisreport highlights a case of FSGS characterized by overt glomerular C3deposits in the absence of immunoglobulins and intramembranous densedeposits which is an uncommon condition and to our knowledge has neverbeen previously reported.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 447
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

266
DELAYED GRAFT RESPONSE IN A NEW RENALALLOGRAFT REVEALS NEW COMPLICATION
Schwartz DW1, Rao V2. 1University of Tennessee, Memphis, TN and2University of Tennessee, Memphis, TN.Case Report: A patient who recieves a renal allograft must be monitoredfor several days as an inpatient to assess allograft function, as well as to ob-serve for potential allograft or surgical complications. We present a case ofa surgical complication that did not present itself until the allograft, under-going a delayed function, began to function.
A 29 year old AAM with ESRD secondary to HTN presented for a de-ceased donor renal allograft transplantation. The patient was noted to haveminimal urine output in the first days of transplant, and quickly becamehyperkalemic and required hemodialysis emergently. A DSA was sent, andplans for biopsy were made. Ultrasound showed a developing hematomaanterior to the allograft. The patient began to experience abdominal pain onPOD 8. Small bowel obstruction was ruled out on KUB. The patient was takenback to OR on POD 9 for evacuation of hematoma after repeat ultrasoundshowed worsening. They could not find a hematoma and the ureteral-bladderanastomosis appeared secure. A drain was placed. The patient’s abdom-inal pain continued. Creatinine of the drain fluid was largely elevated aboveserum creatinine. A renal flow scan showed a possible anastamotic leak. Thepatient was taken back to the OR where a leak was confirmed and repaired. Assoon as the abdominal pain began, SCr began to decline and the patient’sdifficult to control hyperkalemia resolved. Since the fluid was confirmed to beurine, it appears that the problematic urine build up began as the patient’s de-layed function resolved.
Phelan et al described numerous causes of allograft loss in the first monthpost-operatively. The absolute incidence of failure was 4.6%, with a major-ity due to allograft thrombosis. Other causes were acute rejection, deathwith a functional allograft, and primary non-function. Mean time to failurewas 7.3 days. However, these patients had functional allografts to start.
There are numerous post operative complications from renal allograft,as well as numerous causes of a failed allograft. However, this case presentsan unusal situation where the delayed initial functioning of an allograft re-vealed the surgical complication 10 days postoperatively.
267
PYRIDIUM INDUCED ACUTE RENAL INJURY
Shamim Q, James L, Salahuddin M. University of Florida, Jacksonville, FL.Case Report: Phenazopyridine (Pyridium) is a urinary tract analgesic. Ithas been associated with methemoglobinemia, and acute renal failure. We re-port a 31-year-old female with no previous history of renal disease presentedwith acute renal failure and methemoglobinemia following a suicidal at-tempt with Xanax, alcohol, Tramdol and Pyridium. The patient had a pro-gressive nonoliguric renal failure with Creatinine change from 0.78 mg/dl to5.12 mg/dl following the ingestion. She was treated with Methylene blue,hydration and supportive treatment. After 9 days of conservative management,she was discharged home with improving kidney function.
Southern Society for Clinical Investigation and Southern AmericanFederation for Clinical Research Plenary SessionSSCI Young Investigator Award FinalistsSAFMR/SSCI Trainee Research Award PresentationSAFMR/SSCI Young Faculty Award Presentation
8:00 AMFriday, February 22, 2013268
CORONARY VASCULAR ENDOTHELIALTETRAHYDROBIOPTERIN PROTECTS CARDIOMYOCYTESAGAINST HYPOXIA-REOXYGENATION INJURY DURINGHYPERGLYCEMIA
Leucker T1,2, Ge Z2, Procknow J2, Liu Y2, Kersten J2. 1University ofLouisville, Louisville, KY and 2Medical College of Wisconsin, Milwaukee, WI.
Purpose of Study: Tetrahydrobiopterin (BH4) is an essential cofactor forcoupling of endothelial nitric oxide synthase (eNOS) to produce the cardi-oprotective mediator nitric oxide (NO). Hyperglycemia (HG) leads to sig-nificant increases in oxidative stress, oxidizing BH4 to dihydrobiopterin. Theaim of this study was to examine whether increased endothelial BH4 bypharmacological and genetic approaches may generate a cytoprotective ef-fect during HG.Methods Used: Langendorff-perfused mouse hearts were treated by tritonX-100 to produce endothelial dysfunction and subsequently subjected to30 min of ischemia followed by 120 min of reperfusion. Cardiomyocytes(CMs) were co-cultured with endothelial cells (ECs) and subsequently sub-jected to 120 min of hypoxia followed by 120 min of reoxygenation.Summary of Results: The recovery of left ventricular systolic and dia-stolic function during reperfusion, in Langendorff-perfused mouse hearts,was impaired in triton X-100 treated hearts compared with vehicle-treatedhearts. Addition of ECs to CMs at a ratio of 1:3 significantly increased NOproduction and decreased lactate dehydrogenase activity compared with CMsalone. This EC-derived protection was abolished by HG. The addition of100 KM sepiapterin (a BH4 precursor) or overexpression of GTP cyclohy-drolase 1 (the rate-limiting enzyme for BH4 biosynthesis) in ECs, enhancedendothelial BH4 levels, the ratio of eNOS dimer/monomer, eNOS phos-phorylation, and NO production and decreased lactate dehydrogenase activ-ity in the presence of HG.Conclusions: These results demonstrate that increased BH4 content in ECsby either pharmacological supplementation or genetic approach reduces myo-cardial damage during hypoxia-reoxygenation in the presence of HG. Main-tenance of adequate amounts of endothelial BH4 is crucial for cardioprotectionagainst hypoxia-reoxygenation injury.
269
NOVEL ANTIOXIDANT PROPERTIES OF NEBIVOLOLCONFER CARDIOPROTECTION IN HYPERTENSIVEHEART DISEASE
Khan MU, Zhao W, Zhao T, Ahokas RA, Sun Y, Bhattacharya SK, Gerling IC,Weber KT. University of Tennessee Health Science Center, Memphis, TN.Purpose of Study: Chronic aldosteronism, inappropriate for dietary salt(ALDOST), leads to hypertensive heart diseases (HHD) with nonischemiccardiomyocyte necrosis and scarring. Its pathophysiologic origins are rootedin cytosolic free [Ca2+]i and mitochondrial (mt) [Ca2+]m overloading coupledto mt-mediated oxidative stress that overwhelms Zn2+-based antioxidantdefenses with inner membrane permeability transition pore (mPTP) opening.Like atenolol (Aten), nebivolol (Neb) is a A1 adrenergic receptor antagonist;it also acts as a A3 receptor agonist (A3Ra) to promote nitric oxide (NO)production via NOS activation. We hypothesized Neb-mediated NO releasewould: a) raise [Zn2+]i, derived from inactive intracellular metallothionein(MT1)-bound Zn2+, to activate its sensor, metal responsive transcription fac-tor (MTF)-1, with ensuing upregulation of antioxidant defense genes, includingMT1; and b) reduce Ca2+ entry by increased [Zn2+]i, a competitive cotrans-porter via L-type Ca2+ channels.Methods Used: Eight-week-old male Sprague-Dawley rats underwent uni-nephrectomy, subcutaneous minipump implantation releasing ALDO, 0.75 Kg/hr, and received standard chow and drinking water fortified with 1% NaCl/0.4%KCl. Four groupswere studied: ALDOSTalone; ALDOST cotreated witheither Neb (10 mg/kg/daily gavage) or Aten (100 mg/kg/daily gavage), eachequipotent in attenuating the rise in arterial pressure; and untreated age-/sex-matched controls. Cardiomyocytes and subsarcolemmal mt were harvested at4 wks.Summary of Results: ALDOST alone, compared to controls (pG0.05):increased [Ca2+]i, [Ca
2+]m and [Zn2+]i coupled to increased mt H2O2 pro-duction, 8-isoprostane and mPTP opening. Neb, not Aten, prevented [Ca2+]iand [Ca2+]m overloading while raising [Zn2+]i (pG0.01). Only Neb increasedplasma NO3/NO2 and upregulated gene and protein expression of eNOS andiNOS and antioxidant defenses with MTF-1 and MT1. Cardiac fibrosis, afootprint of necrosis, with increased collagen volume fraction (pG0.05), wasprevented by Neb (pG0.05), not Aten.Conclusions: Neb revealed a novel antioxidant profile based on eNOS andiNOS activation with NO acting as cardioprotectant in HHD via Zn2+-basedantioxidant responses.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
448 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

270
THE ROLE OF ENDOTHELIN-1 IN COLLECTING DUCTRENIN SYNTHESIS AND SECRETION
McGuire C1,2, Liu L2,3, Prieto M1,2,3. 1Tulane University, New Orleans,LA;2Tulane University, New Orleans, LA and 3Tulane University, NewOrleans, LA.Purpose of Study: While the regulation of juxtaglomerular (JG) renin hasbeen extensively studied, much less is known about the regulation of col-lecting duct (CD) renin. Growing evidence shows that renin in principal cellsof the CD is stimulated by angiotensin II (AngII) independently of bloodpressure via an AngII type I receptor-mediated mechanism dependent onPKC. Alterations in renin synthesis and activity in the CD may provide acritical pathway to increase intrarenal and intratubular AngII content therebyincreasing sodium reabsorption and contributing to hypertension. However,the regulation of renin by hormones targeting the CD, such as endothelin-1(ET-1), has not been established. In the present study we aimed to determinethe effects of ET-1 on renin synthesis and secretion in the CD cells. We hy-pothesize that ET-1 stimulates CD renin synthesis and secretion via PKG ac-tivation by nitric oxide or via activation of PKC.Methods Used: Mouse M-1 CD cell culture, quantitative real-time RT-PCR,Western blot, measurements of intracellular cAMP content (ELISA).Summary of Results: In M-1 cells, ET-1 (5�10-9M) treatment for six hoursincreased renin mRNA levels (pG0.01). Surprisingly, the same treatment in thepresence of non-specific inhibition of all NOS isoforms by L-NAME (10-7 M)further increased the stimulatory effect of ET-1 on renin mRNA in CD cells(pG0.001). However, treatment with L-NAME or an NO donor (10-6 M) alonehad no effect on CD renin mRNA expression. Activation of PKC with PMA(10-6 M) did not stimulate CD renin mRNA expression. However, non-specific inhibition of PKC with calphostin C (10-7 M) in the presence of5x10-9 M ET-1 attenuated the ET-1 dependent increase in CD renin mRNAexpression (pG0.001).Conclusions: The data indicate that ET-1 stimulates CD renin synthesis andsecretion by activation of both NOS/GC/cGMP/PKG and PKC pathways. It ispossible that the mechanism involved relies on potential cross-talk betweenthe NOS/GC/cGMP/PKG and PKC pathways, via ETBR-dependent activa-tion by ET-1. Further studies are being undertaken to examine this possibility.
271
NEPHROGENIC SYSTEMIC FIBROSIS: REDOXSENSITIVITY, DERMAL CCR7-EXPRESSING FIBROCYTES,AND EVIDENCE OF PULMONARY INVOLVEMENT IN ARAT MODEL
Sewell J1, Wagner B2,1. 1University of Texas Health Care System at SanAntonio, San Antonio, TX and 2South Texas Veterans Health Care System,San Antonio, TX.Purpose of Study: In patients with renal insufficiency, gadolinium-basedmagnetic resonance imaging (MRI) contrast use is the highest risk factor fornephrogenic systemic fibrosis (NSF). Circulating fibrocytes express C-C che-mokine receptor (CCR) type 7, and this may contribute to recruitment of thesecells to affected sites. No one has explored this with respect to NSF. Addi-tionally, given the similar mechanism to idiopathic pulmonary fibrosis, theeffect of MRI contrast on pulmonary fibrosis was examined.Methods Used: Female Fischer 344 rats underwent 5/6 nephrectomy at8 weeks and randomized to MRI contrast (Omniscan/gadodiamide, caldia-mide) treatment, MRI contrast plus the superoxide dismutase (SOD) mimetictempol, or control for 3 weeks. Serum analysis was by Luminex assay.Summary of Results: Half of the contrast-treated animals demonstratedgross skin abnormalities, whereas none of the tempol- and contrast- co-treatedanimals did. Serum monocyte chemotactic protein (MCP)-1 and interferon F-induced protein (IP)-10 were significantly increased in the contrast-treatedanimals with respect to control, and these were abrogated by tempol. Skinfrom MRI contrast-treated animals had increased expression of fibronec-tin, CCR7, and cathepsin-L when compared to control. Immunofluorescencedemonstrated that the CCR7+ cells in the dermis were bone marrow-derived.There was an increase in fibronectin in lung, which was mildly abrogated bytempol.Conclusions: There is an increase in dermal CCR7-expressing bone marrow-derived cells in MRI contrast-induced dermal fibrosis. Furthermore, MRI
contrast induces pulmonary fibronectin accumulation. These observationsnot only support the theory that circulating fibrocytes mediate the disease in asystematic manner, but suggest mechanisms and therapeutic targets for thisdevastating disease.
272
SMOOTH MUSCLE-TARGETED PPAR GAMMAOVEREXPRESSION ATTENUATES HYPOXIA-INDUCEDPULMONARY HYPERTENSION IN MICE
Green D, Klienhenz J, Sutliff R, Hart C. Emory University, Decatur, GA.Purpose of Study: Pharmacological activation of the nuclear hormonereceptor, PPAR gamma (PPARF), attenuates pulmonary hypertension (PH)in rodent models. The mechanisms and sites of action for these therapeu-tic effects continue to be defined. We hypothesized that the vascular smoothmuscle cell compartment was an important locus through which the thera-peutic effects of PPARF activation were mediated in PH. We examined thishypothesis by employing a genetic strategy to constitutively activate PPARFin vascular smooth muscle cells.Methods Used: C57Bl/6 mice with floxed alleles for PPARF driven bythe constitutively active VP16 promoter were bred with mice expressingCre recombinase driven by a tamoxifen-inducible smooth muscle myosinpromoter. After genotyping, adult offspring that demonstrated smooth muscle-targeted overexpression of constitutively active PPAR gamma (smVP16-PPARF) or littermate controls (LC) were treated with tamoxifen and exposedto normoxia or hypoxia (10% O2) for 4-weeks. Right ventricular systolic pres-sure (RVSP) was measured with a pressure transducer, and right ventricularhypertrophy (RVH) was assessed by calculating the ratio of the weight of theright ventricle to the left ventricle + septum. Pulmonary vascular remodel-ing was assessed by staining lung sections with antibodies to alpha smoothmuscle actin.Summary of Results: Compared to LC, smVP16-PPARF mice demon-strated overexpression of VP16 and PPARF in aortae and weighed approxi-mately 20% less. There was no significant difference in RVSP between LCand smVP16-PPARF mice exposed to normoxia. As expected, compared tonormoxic controls, hypoxia increased RVSP in LC mice, whereas hypoxicincreases in RVSP were reduced by approximately 50% in smVP16-PPARFmice. Hypoxia-induced increases in muscularization of small pulmonaryvessels (G20 K diameter) in LC mice was attenuated in smVP16-PPARFmice. In contrast, genotype had no significant effect on hypoxia-inducedincreases in RVH.Conclusions: These findings provide novel evidence that smooth muscle-targeted PPARF activation attenuated hypoxia-induced PH and vascular re-modeling and that previously observed therapeutic effects on RVH are likelyattributable to activation PPARF in the ventricular myocardium.
Southern Society for Pediatric Research Plenary SessionYoung Investigator Award Finalists
8:00 AM Friday, February 22, 2013273
ABILITY OF PEDIATRIC EMERGENCY MEDICINEPHYSICIANS TO IDENTIFYANATOMIC LANDMARKS WITHULTRASOUND PRIOR TO LUMBAR PUNCTURE IN ASIMULATED OBESE MODEL
Restrepo C1, Baker MD1, Gullett JP2, Pigott DC2. 1University of Alabama atBirmingham, Birmingham, AL and 2University of Alabama at Birmingham,Birmingham, AL.Purpose of Study: Lumbar punctures (LPs) are typically performed usinganatomical surface landmarks. However, surface landmarks are accurate only30% of the time and as BMI increases, identifying landmarks becomes moredifficult. Ultrasound has been proposed as a tool for identifying these land-marks prior to LP. This study evaluates the effectiveness of a brief trainingprogram in ultrasound identification of anatomical landmarks in a simulatedobese model prior to completing a LP.Methods Used: Pediatric emergency medicine faculty and fellows from 1 in-stitution were recruited for this educational intervention. Subjects completed
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 449
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

a pre-test questionnaire on ultrasound familiarity prior to a 1 hour didacticultrasound educational session. Participants utilized ultrasonography with-out the assistance of palpation on a simulation LP model (Blue Phantom)saving orthogonal images for review. Participants attempted LP on 2 phantommodels with simulated BMIs of 35 and 40. Time to image acquisition andsuccessful aspiration of CSF from the model were recorded. Two expert sonol-ogists independently reviewed all images for correct landmark identification.Summary of Results: Five of the 14 participants had previous familiaritywith ultrasound. The mean time to lumbar image acquisition significantlyimproved for all individuals from 182 seconds to 110 seconds (p 0.03). Com-fort level with ultrasound improved (p G 0.01) as well as comfort level inperforming a lumbar ultrasound (p G 0.001). Adequate images were obtainedin 97.6% of the attempts (41/42). The success rate at performing LP was 93%(39/42) while using only ultrasound to obtain the location of needle inser-tion. No individual was able to perform a successful LP without an adequateimage.Conclusions: After a brief education intervention, pediatric emergencymedicine physicians with little to no previous training in ultrasound can ob-tain adequate lumbar anatomic images and successfully perform lumbarpuncture in a simulated obese model. Comfort level with ultrasound alsosignificantly improves with a short course in ultrasound fundamentals andtime to image acquisition quickly improves.
274
BLOOD CULTURES ARE NOT USEFUL IN THE EVALUATIONOF CHILDREN WITH UNCOMPLICATED SKIN AND SOFTTISSUE INFECTIONS
Malone J1, Durica S1, Bogie A1, Thompson D2, Naifeh M1. 1University ofOklahoma Health Sciences Center, Oklahoma City, OK and 2University ofOklahoma Health Sciences Center, Oklahoma City, OK.Purpose of Study: To determine the yield and cost-effectiveness of bloodcultures in the evaluation of immunocompetent children with uncompli-cated skin and soft tissue infections (SSTI) in the era of methicillin-resistantStaphylococcus aureus.Methods Used: This IRB-approved, retrospective chart review was con-ducted at an urban, university affiliated pediatric emergency department (ED)with an annual census of about 40000. A query of electronic medical recordsidentified children admitted to the hospital between Jan 1, 2007 and Dec 31,2009 following ED evaluation and diagnosis of cellulitis or abscess. Chartswere reviewed for demographic, historical, microbiologic, and laboratory data.We compared 482 patients with uncomplicated SSTI to 98 with complicatedSSTI (cSSTI). cSSTI was defined as surgical or traumatic wound infec-tion, abscess or cellulitis requiring surgical intervention, or infected ulcersor burns. SSTI included patients without complicating factors.Summary of Results: There were no positive blood cultures in the SSTIgroup; the chance of obtaining a positive blood culture during an episodeof uncomplicated SSTI is less than 1% (CI: 0%, 0.81%). Within the cSSTIgroup, 12.5% of blood cultures were positive (CI: 6.2%, 22.0%). Children withcSSTI are more likely than those with SSTI to be bacteremic (pG0.0001). Themean length of hospital stay (LOHS) in children with SSTI was shorter thanthose with cSSTI (3.18 vs. 6.62 days; pG0.0001). Within the SSTI group,obtaining a blood culture was associated with an increased mean LOHS(3.24 vs. 2.33 days; p=0.044).Conclusions: Blood cultures are neither useful nor cost effective in theevaluation of uncomplicated SSTI, and on average result in nearly 1 day in-crease in LOHS. Zwang et al. (2006) indicated that the annualized costs as-sociated with a negative blood culture were around $900, and those associatedwith a contaminated blood culture were as high as $32000. Applied to thisstudy’s SSTI group, those figures amount to a total cost of over $500000without detecting a single positive blood culture. Proper identification andevaluation of children with cSSTI is important, given their high rate of bac-teremia and need for prolonged care.
275
A RANDOMIZED TRIAL OF RE-FEEDING GASTRICRESIDUALS IN PRETERM INFANTS
Salas AA, Cuna A, Bhat R, McGwin G, Carlo WA, Ambalavanan N.University of Alabama at Birmingham, Birmingham, AL.
Purpose of Study: If gastric residuals are present, a decision has to be madewhether to re-feed the residual, or to discard the residual and feed fresh for-mula or human milk. Currently, there is no evidence to support either ap-proach. We tested the hypothesis that re-feeding of gastric residuals wouldreduce the time needed to establish enteral feedings in preterm infants.Methods Used: This study was a single-center randomized controlled trial(Clinicaltrials.gov: NCT01420263). Infants with gestational ages between23 0/7 and 28 6/7 weeks receiving minimal enteral nutrition were eligible.Following informed consent, infants were randomized within the first week afterbirth to receive either gastric residuals or fresh formula/human milk if gas-tric residuals (9 1/3 of previous feed or 9 2 ml) were found. The primaryoutcome was time to achieve full enteral feedings (Q120 ml/kg/day) for twoconsecutive days. The study was powered to identify a 2-day difference be-tween groups assuming a standard deviation of 3 days.Summary of Results: We enrolled 72 infants between Aug 2011 and Sep2012. Baseline characteristics of the study participants are shown in the Table.In the re-feeding group, 3 infants were diagnosed with spontaneous intesti-nal perforation (SIP) and 4 infants had medical necrotizing enterocolitis be-fore establishment of full feeding. In the fresh feeding group, 2 infants diedand 4 infants developed SIP. The primary outcome was assessed in 59 infants.Median time to full feedings was 9 days (IQR: 7 - 11) after randomization inthe re-feeding group and 10 days (IQR: 8 - 12) in the fresh feeding group(p=0.25). SIP/death after randomization and before full feeding was 8% inthe re-feeding group and18% in the fresh feeding group (p=0.28).Conclusions: Re-feeding gastric residuals did not reduce time to reach fullfeedings in preterm infants.
276
JET-NEBULIZED MEDICATIONS FOR PREMATUREINFANTS ON AVENT - DO WE BRING MORE HARMTHAN GOOD?
Ivanov VA, Freeland J. OUHSC, Oklahoma City, OK.Purpose of Study: Nebulized medications (NM) are used in NICUs despitethe lack of empirical evidence for their efficacy. Frequently, NM are ad-ministered via a jet nebulizer in-line with the fresh gas arm of a ventilatorcircuit. This method is approved for use with some ventilators and is used offlabel with others. It is likely that the addition of an in-line nebulizer increasesthe flow in the circuit and adds pressure into it. This effect has not been quantifiedand no empirical data on this effect have been published. Our study fills thisgap by measuring the effect of the flow added into the circuit by an in-linejet nebulizer.Methods Used: Servo-I (S) and Babylog VN 500 (B) ventilators were testedin neonatal setup, with pressure (PR), volume and pressure regulated volumecontrol ventilation modes, with a test lung attached. PEEP was set at 5 cm ofH2O, PIP was set on 20 cm of H2O in the PR mode, and the upper pressurelimit was set at 40 cm of H2O for the volume modes. The tidal volumes (TV)were set at 4 and 10 ml for the volume modes. Both ventilators had a jetnebulizer in-line and the delivered pressures and TVs were measured usingthe ventilator flow meters with the nebulizer off, and running gas flow at 2.5,8 l/min (S) and 6 l/min (B).Summary of Results: In the PR mode, nebulizer-added flow resultedin PEEP increase to 6 at 8 l/min (S) and 6 l/min (B) but no PEEP increaseat 2.5 /min (S). PIP increased to 24, 25 and 22 cm of H2O at flows of 2.5 and8 l/min (S) and 6 l/min (B) respectively. TVs increased from 7.8 at thebaseline to 8.5 and 9.5 at 2.5 and 8 l/min in S, but were not measured in theB ventilator.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
450 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

In the volume modes (S only) PEEP was 5 at 2.5 l/min and 6 at 8 l/min.PIP more than doubled in both modes at flow 2.5 l/min at both TV. At 8 l/minof flow the PIP was increased up to the pressure limit and the actual TVs wereincreased to 17.5 in all settings.Conclusions: Using a jet nebulizer in-line with a neonatal ventilator leadsto measurable increases in delivered pressures. Thus, NM administration inventilated patients must account or control for the effects of increased pres-sures. In volume control modes, these pressure elevations are significant andpotentially dangerous. These findings call for the elimination of the use ofjet nebulizers in parallel with volume control ventilation.
277
RETINAL MULLER CELL SURFACTANT PROTEIN AIMPAIRS RETINAL ENDOTHELIAL CELL FUNCTION
Bhatti F1,2, Ball G1, Akram R1, Elliott M2. 1University of Oklahoma HealthSciences Center, Oklahoma City, OK and 2University of Oklahoma HealthSciences Center, Oklahoma City, OK.Purpose of Study: We have previously demonstrated that Surfactant Pro-tein A (SP-A) is present in the mouse retina and that toll like receptor 2 and4 (TLR-2 and TLR-4) activation leads to up regulation of SP-A expressionusing an in vivo mouse model. We further wanted to elucidate the cell typeswhich express SP-A in the human retina and study the effects of SP-A onhuman retinal endothelial cell (HREC) function.Methods Used: Retinas were harvested from C57B6/J mice and analyzedby fluorescent immunohistochemistry (IHC) with antibodies against SP-Aand retinal cell markers including glutamine synthase (GS) for Muller cells,neurofilament M for ganglion cells, Rhodopsin for rods and cones and cd31for blood vessels. In order to confirm SP-A expression, cultured immortalizedhuman Muller cells (MIO-M1) were treated with TLR-2 and TLR-4 ligandsand SP-A expression measured using ELISA. To study the effect of SP-A onHREC functions, cultured HREC’s were treated with purified SP-A and func-tion quantified using migration and proliferation assays.Summary of Results: Using IHC, we showed co-localization of SP-AwithGS in Muller cells in the mouse retina. This was confirmed in vitro by quan-tifying SP-A expression in human MIO-M1 cells after stimulating cells withTLR-2 and TLR-4 ligands. SP-A expression peaked at 6 hours after treatmentwith LPS and at 12 hours after stimulation with PamC3. SP-A expression wasalso quantified in the cell media from the stimulated cells, which was signifi-cantly increased compared to control. In endothelial cell function assays,HREC proliferation was significantly impaired after 6 hours of treatment withSP-A and this difference was further accentuated after 12 hours of treatment.HREC migration was significantly reduced after treatment of cells with SP-A.Conclusions: SP-A is both expressed and secreted by mouse and humanretinal Muller cells and this expression is up regulated by TLR-2 and TLR-4ligand stimulation. SP-A secreted byMuller cells impairs function of HREC’sassayed by endothelial cell function assays. Thus SP-A secretion in responseto systemic and local inflammation may impair adequate function of reti-nal endothelial cells and may contribute to disorganized angiogenesis in thedeveloping retina.
278
CEREBROVASCULAR PROTECTIVE EFFECTS OF HEADCOOLING DURING SEIZURES IN NEWBORN PIGLETS
Harsono M1, Parfenova H2, Leffler CW2,1, Pourcyrous M1,2. 1University ofTennessee HSC, Memphis, TN and 2University of Tennessee HSC, Memphis, TN.Purpose of Study: Selective head cooling therapy has been shown to pro-vide neuroprotective effect in hypoxic ischemic encephalopathy. However,cerebrovascular (CV) effects of head cooling during seizures have not beeninvestigated yet. We hypothesized that selective head cooling during sei-zures protects postictal loss of CV function in newborn piglets.Methods Used: Newborn piglets were anesthetized and paralyzed withketamine, xylazine and pancuronium. Piglets were intubated and mechani-cally ventilated to maintain adequate ventilation, and were placed on thermo-controlled pad. In head-cooling groups, rectal temperature was maintainedat 34 - 35 degree C during head cooling. Head cooling was provided with icepads placement around the piglet’s head. Bicuculline was used for seizures-induction. When fully conscious, piglets were extubated and placed at ani-mal care facility. Cerebrovascular reactivity (CVR) to physiologically relevant
vasodilators was tested 48 hours later using closed cranial window. CVR wastested in 4 groups of piglets: (1) no head cooling, no seizures; (2) no headcooling, seizures; (3) head cooling 30 min before seizures-induction, conti-nued during seizures; (4) head cooling 20 min after seizures-induction, con-tinued during seizures.Summary of Results: No major complications were noted in any groupduring 48 hours postictal recovery period. Core body temperature duringhead cooling was decreased from 37.2 T 0.2 to 34.6 T 0.3 degree C. PostictalCVR was tested 48-hours later using endothelium-dependent (bradykinin andhemin), astrocyte-dependent (glutamate) and smooth muscle-dependent (so-dium nitroprusside and isoproterenol) vasodilatory stimuli. Postictal CVR tosmooth muscle-dependent vasodilators was preserved. In contrary, postictalCVR to astrocyte-dependent and endothelium-dependent vasodilators was re-duced in the no head cooling seizures group, but completely preserved in bothhead cooling groups regardless of the head cooling initiation time.Conclusions: Head cooling during epileptic-seizures has protective effecton postictal CV dilatory function in newborn piglets. It prevents loss of CVendothelial function, and therefore preserves cerebral blood flow regulationwhich may reduce adverse neurological outcome of seizures.
279
TARGETED INACTIVATION OF THE PRORENIN RECEPTORIN THE URETERIC BUD INHIBITS URETERIC BUDRANCHING MORPHOGENESIS
Song R, Preston G, Monlezun D, Yosypiv I. Tulane University, New Orleans, LA.Purpose of Study: The PRR is the cell-surface receptor for renin and pro-renin, and an accessory subunit of the vacuolar proton pump H+-ATPase. Inthis study, we tested the hypothesis that targeted inactivation of the PRR(Atp6ap2) in the UB epithelia is essential for normal UB morphogenesis.Methods Used: PRR-floxed (PRRflox/+) mice were bred with mice thatexpress the Cre recombinase under the control of the UB-specific promoter(Hoxb7Cre+). The resulting Hoxb7Cre+/PRRflox/flox mice represent UB-specific PRR-knockout mice. RT-PCR demonstrated that isolated intactembryonic (E) day E11.5 mouse UBs, cultured UB cells and E12.5 intactmetanephroi express PRR mRNA. Kidney (P)RR protein levels, determinedby Western blot, are high throughout gestation and decline gradually duringpostnatal development. Immunohistochemistry localized PRR in the UB onE13.5 and in the collecting duct on E16.5 and E18.5.Summary of Results: The number of UB tips was reduced on E12.5 inmutant Hoxb7Cre+/PRRflox/flox (n=4mice) compared to control (Hoxb7Cre-/PRRflox/flox, n=6 mice) kidneys (5.2T0.5 vs. 13T0.5, pG0.01). The numberof caspase 3-positive apoptotic cells was higher in the UB of mutant com-pared with control E12.5 kidneys (7.6T1.2 vs. 0.6T0.1, pG0.01) (n=3 mice/genotype). qRT-PCR demonstrated that Ret (0.48T0.02 vs. 1.0T0.02, pG0.001),Wnt11 (0.19T0.01 vs. 1.0T0.02, pG0.001), Etv4 (0.54T0.03 vs. 1.0T0.02,pG0.001) and Etv5 (0.76T0.03 vs. 1.0T0.02, pG0.01) mRNA levels were de-creased in mutant compared to control kidneys.Conclusions: We conclude that PRR present in the UB epithelia performsessential functions during UB branching morphogenesis and renal collectingsystem development via control of Ret/Wnt11 pathway gene expression andUB cell survival. These results support the hypothesis that PRR mutationsmay be causally linked to renal hypodysplasia in humans.
Cardiovascular Club IIYoung Clinician Scientist Award Competition
11:00 AMFriday, February 22, 2013280
ALTERATION IN THE CHRONOBIOLOGY OF ONSET OFACUTE MYOCARDIAL INFARCTION IN NEW ORLEANSRESIDENTS FOLLOWING HURRICANE KATRINA
Peters MN, Katz MJ, Moscona JC, Turnage TA, Delafontaine P, Irimpen AM.Tulane University Health Sciences Center, New Orleans, LA.Purpose of Study: The onset of acute myocardial infarction (AMI) hasbeen shown to occur in a non-random pattern, with peaks in mid-morning,
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 451
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

and weekdays (especially Monday). Increases in AMI have been shown tooccur locally following natural disasters, but, to our knowledge, the effect onbiorhythms is unknown. To better elucidate the pathophysiology of AMI, wecompared the chronobiology of AMI in the 6 years before, and the 3 yearsafter Hurricane Katrina.Methods Used: We identified AMI patients at Tulane University HealthSciences Center (TUHSC) using ICD 9 codes 410.1 to 410.9. All subjectshad typical ischemic symptoms at rest and elevated troponin I levels. Weexcluded non-New Orleans residents, hospital transfers, patients withsymptom onset while hospitalized and patients with inadequate documen-tation of day/time of symptom onset. There were 2 cohorts: Pre-Katrina: 8/29/99 to 8/28/05 (storm landfall); and Post-Katrina: 2/16/06 (when TUHSCbecame first downtown hospital to reopen) to 2/15/09. Medical records wereretrospectively assessed to identify onset of symptoms, demographic, clinicaland laboratory data.Summary of Results: In the Post-Katrina group, there were significantdecreases in AMI on weekdays, Mondays and mornings and a significantincrease on nights and weekends (Table). There were no significant differ-ences in AMI pattern between years 1, 2 and 3 post-Katrina.Conclusions: The normal pattern of AMI onset was altered following Hur-ricane Katrina and expected morning, weekday and Monday peaks wereeliminated. Although the mechanism of these changes is unknown, our find-ings suggest a likely relationship to stress associated with the almost univer-sal devastation in the New Orleans area. Traditional patterns of AMI onsetassociated with stressful times of the day and week may be altered during nat-ural disasters and these patterns may persist for prolonged periods of time.
281
SURVIVAL AND DISCHARGE RATES FOR OCTOGENARIANSUNDERGOING CORONARY REVASCULARIZATIONPROCEDURES AFTER ACUTE MYOCARDIAL INFARCTION
Pant S1, Deshmukh A2, Hayes K2, Kumar G3, Sachdeva R4, Mehta JL2.1University of Arkansas for Medical Sciences, Little Rock, AR; 2Universityof Arkansas for Medical Sciences, Little Rock, AR; 3Emory University,Atlanta, GA and 4Medical College of Wisconsin, Milwaukee, WI.Purpose of Study: Octogenarians constitute a significant proportion oftotal acute coronary syndrome burden. Large randomized trials and meta-analyses have examined the appropriateness of intervention in patients lessthan 80 years but whether these data can be extrapolated to octogenarians isunknown. This study has been undertaken to evaluate the survival and dis-charge rates of octogenarians undergoing coronary revascularization for acutemyocardial infarction (AMI) from a nationwide database.Methods Used: Using the Nationwide Inpatient Sample (NIS) database2007, patients age Q 80 years discharged with the primary diagnosis of AMIwere identified. Outcome variables included in-hospital mortality, length ofstay (LOS), coronary revascularization procedures performed and dischargedisposition. Multivariate regression analysis was performed using appropriatesurvey commands in Stata IC, version 11.0.Summary of Results: Of the 117,282 discharges with primary diagnosis ofAMI, 28,429 patients (24.24%) were aged Q80 years. The unadjusted mor-tality in octogenarians was 10.4% (vs. 3.7% in non-octogenarians, pG0.001),as was the adjusted mortality (OR 3.4; 95% CI 3.1-3.6; pG0.001). Thenumber of procedures performed was 19% in octogenarians (vs. 44.8% innon-octogenarians, OR 0.35; 95% CI 0.33-0.37; pG0.001). Mortality wassignificantly lower in octogenarians undergoing any coronary revasculari-zation procedure (6.5% vs 11.3%, OR 0.34; 95%CI 0.29-0.40; pG 0.001).Octogenarians undergoing no coronary revascularization procedures hadsignificantly longer LOS compared to those undergoing revascularization forAMI (5.7 vs. 4.8 days; pG0.001). Finally, octogenarians undergoing revas-cularization for AMI were less likely to be discharged to a nursing home thanthose undergoing conservative management (17.3% vs 33.8%, pG0.001).
Conclusions: The ‘‘treatment paradox’’ in the octogenarian needs furtherexploration given the findings of better outcomes in octogenarians receiv-ing same degree of aggression in treatment of acute coronary syndrome asyounger population.
282
CORONARY VASCULAR ENDOTHELIALTETRAHYDROBIOPTERIN PROTECTS CARDIOMYOCYTESAGAINST HYPOXIA-REOXYGENATION INJURY DURINGHYPERGLYCEMIA
Leucker T1,2, Ge Z2, Procknow J2, Liu Y2, Kersten J2. 1University ofLouisville, Louisville, KY and 2Medical College of Wisconsin, Milwaukee, WI.Purpose of Study: Tetrahydrobiopterin (BH4) is an essential cofactor forcoupling of endothelial nitric oxide synthase (eNOS) to produce the cardio-protective mediator nitric oxide (NO). Hyperglycemia (HG) leads to signif-icant increases in oxidative stress, oxidizing BH4 to dihydrobiopterin. Theaim of this study was to examine whether increased endothelial BH4 bypharmacological and genetic approaches may generate a cytoprotective ef-fect during HG.Methods Used: Langendorff-perfused mouse hearts were treated by tri-ton X-100 to produce endothelial dysfunction and subsequently subjected to30 min of ischemia followed by 120 min of reperfusion. Cardiomyocytes(CMs) were co-cultured with endothelial cells (ECs) and subsequently sub-jected to 120 min of hypoxia followed by 120 min of reoxygenation.Summary of Results: The recovery of left ventricular systolic and diastolicfunction during reperfusion, in Langendorff-perfused mouse hearts, was im-paired in triton X-100 treated hearts compared with vehicle-treated hearts.Addition of ECs to CMs at a ratio of 1:3 significantly increased NO pro-duction and decreased lactate dehydrogenase activity compared with CMsalone. This EC-derived protection was abolished by HG. The addition of100 KM sepiapterin (a BH4 precursor) or overexpression of GTP cyclohy-drolase 1 (the rate-limiting enzyme for BH4 biosynthesis) in ECs, enhancedendothelial BH4 levels, the ratio of eNOS dimer/monomer, eNOS phosphor-ylation, and NO production and decreased lactate dehydrogenase activity inthe presence of HG.Conclusions: These results demonstrate that increased BH4 content in ECsby either pharmacological supplementation or genetic approach reduces myo-cardial damage during hypoxia-reoxygenation in the presence of HG. Main-tenance of adequate amounts of endothelial BH4 is crucial for cardioprotectionagainst hypoxia-reoxygenation injury.
283
NOVEL ANTIOXIDANT PROPERTIES OF NEBIVOLOLCONFER CARDIOPROTECTION IN HYPERTENSIVEHEART DISEASE
Khan MU, Zhao W, Zhao T, Ahokas RA, Sun Y, Bhattacharya SK, GerlingIC, Weber KT. University of Tennessee Health Science Center, Memphis, TN.Purpose of Study: Chronic aldosteronism, inappropriate for dietary salt(ALDOST), leads to hypertensive heart diseases (HHD) with nonischemiccardiomyocyte necrosis and scarring. Its pathophysiologic origins are rootedin cytosolic free [Ca2+]i and mitochondrial (mt) [Ca2+]m overloading coupledto mt-mediated oxidative stress that overwhelms Zn2+-based antioxidantdefenses with inner membrane permeability transition pore (mPTP) opening.Like atenolol (Aten), nebivolol (Neb) is a A1 adrenergic receptor antagonist; italso acts as a A3 receptor agonist (A3Ra) to promote nitric oxide (NO) pro-duction via NOS activation. We hypothesized Neb-mediated NO release would:a) raise [Zn2+]i, derived from inactive intracellular metallothionein (MT1)-bound Zn2+, to activate its sensor, metal responsive transcription factor (MTF)-1, with ensuing upregulation of antioxidant defense genes, including MT1;and b) reduce Ca2+ entry by increased [Zn2+]i, a competitive cotransporter viaL-type Ca2+ channels.Methods Used: Eight-week-old male Sprague-Dawley rats underwent un-inephrectomy, subcutaneous minipump implantation releasing ALDO, 0.75 Kg/hr, and received standard chow and drinking water fortified with 1% NaCl/0.4%KCl. Four groups were studied: ALDOST alone; ALDOST cotreated witheither Neb (10 mg/kg/daily gavage) or Aten (100 mg/kg/daily gavage), each
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
452 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

equipotent in attenuating the rise in arterial pressure; and untreated age-/sex-matched controls. Cardiomyocytes and subsarcolemmal mt were harvested at4 wks.Summary of Results: ALDOST alone, compared to controls (pG0.05):increased [Ca2+]i, [Ca
2+]m and [Zn2+]i coupled to increased mt H2O2 pro-duction, 8-isoprostane and mPTP opening. Neb, not Aten, prevented [Ca2+]iand [Ca2+]m overloading while raising [Zn2+]i (pG0.01). Only Neb increasedplasma NO3/NO2 and upregulated gene and protein expression of eNOS andiNOS and antioxidant defenses with MTF-1 and MT1. Cardiac fibrosis, afootprint of necrosis, with increased collagen volume fraction (pG0.05), wasprevented by Neb (pG0.05), not Aten.Conclusions: Neb revealed a novel antioxidant profile based on eNOS andiNOS activation with NO acting as cardioprotectant in HHD via Zn2+-basedantioxidant responses.
Adolescent Medicine and PediatricsConcurrent Session
2:00 PMFriday, February 22, 2013284
PEDIATRIC ENDOTRACHEAL TUBE CUFF PRESSURES INMANNEQUINS DURING HELICOPTER TRANSPORT
Orsborn J1,2, Moss M2, Graham J2,1, Stroud M2. 1Arkansas Children’sHospital, Little Rock, AR and 2UAMS, Little Rock, AR.Purpose of Study: Cuffed endotracheal tubes (ETTs) are frequently used inchildren, allowing fewer air leaks and helping prevent ventilator associatedpneumonia. Intubated pediatric patients are frequently transported via heli-copter. Previous studies have shown that tracheal mucosal perfusion is com-promised at a pressure of 30cmH2O and blood flow is completely absentat 50cmH20. Damage in animal models is seen in as little as 15 minutesat such pressures. dA recent adult study showed increases in ETT cuffpressure from 28.7cmH2O to 62.6cmH20, measured at ground level andpeak altitude during helicopter transport. Currently, ETT cuff pressures arenot routinely measured before or during helicopter transport. The purpose ofthis study was to compare pediatric sized ETT cuff pressures at ground leveland various altitudes during helicopter transport..Methods Used: Simulating the transport environment, a neonatal sized man-nequin head (Laerdal\), was intubated with 3.0 and 3.5 cuffed ETTs andtransported by helicopter. ETT cuff pressure was set between 10 and 20cmH20prior to transport. Cuff pressures were measured with a standard manome-ter at 1000ft intervals until peak altitude was reached or cuff pressure ex-ceeded 60cmH20. Peak altitude ranged from 3,500 to 5,000ft Mean Sea Level(MSL).Summary of Results: Mean cuff pressures were compared at baseline andat 1000ft intervals. There was a statistically significant increase in measuredpressures at all altitudes. Values are expresses as MeanTSD; p values are double-sided with a significance set at p=0.05; baseline: 14.5T5.3cmH2O, 1000ftMSL:26.0T8.3cmH2O (p=0.0005), 2000ftMSL: 40.8T9.1cmH2O (p=0.0002),3000ftMSL: 53.8T7.6cmH2O (p=0.0006), 4000ftMSL: 64.1T9.4cmH2O (p=0.01).All values at 5000ftMSL were 960cmH2O.Conclusions: Though not routinely measured during helicopter transport,cuff pressures in pediatric sized ETTs routinely exceed recommended pres-sure limits at relatively low altitudes. This has the potential to decrease bloodflow to tracheal mucosa, possibly increasing risk of subsequent tracheal ste-nosis, rupture, and other complications. Future studies should evaluate varyingsizes of ETTs and consequences in human subjects. This knowledge maywarrant a change in air transport procedures for pediatric patients.
285
VACCINE HESITANCY AMONG PARENTS OF TEENS
Roberts JR1, Hale J2, Thompson D2, Darden P2. 1Medical University ofSouth Carolina, Charleston, SC and 2Oklahoma University Health SciencesCenter, Oklahoma City, OK.Purpose of Study: Addressing parents’ hesitancy to obtain vaccines rec-ommended for teens could improve immunization rates. This study’s purposeis to evaluate the hesitancy of parents’ toward getting their teen vaccinated.
Methods Used: We adapted a validated vaccine hesitancy survey of youngchildren (Opel) and administered the modified version to adolescents aged11-17 and their parents in 6 pediatric practices in OK and SC. The surveyincluded 18 items that rated hesitancy to obtain vaccines and permittedresponses on a 3, 5, or 10 point scale. Patients’ up-to-date (UTD) status as ofthe date they completed the survey was determined via chart review for tetanus,diphtheria and acellular pertussis (Tdap), meningococcal vaccine (MCV) andhuman papilloma virus (HPV). We compared the frequency distribution ofsurvey responses to UTD status using Fisher’s exact test. Factor analysis wasperformed to evaluate the consistency and utility of survey items.Summary of Results: We analyzed data on 375 parents who answered thesurvey and whose teens’ immunization status was known. UTD rates in theOK and SC practices were 80% and 83% for Tdap, 68% and 72% for MCV,and 37% and 50% for HPV. Twenty-five percent of parents consider them-selves to be ‘unsure about vaccines for teens overall’. Parents were concernedabout vaccine efficacy (40%) and safety (43%). Parents frequently disagreed(46%) with the statement ‘Teens can get all vaccines they are due in one visit’.Parents whose teen was not UTD for HPV were more likely to have delayed avaccine for reasons other than illness or allergy (p G.05). The same parentswere less likely to agree than parents of adolescents UTD for HPV that ‘teensget more vaccines than are good for them’, and less likely to be able to openlydiscuss vaccine concerns with their teen’s doctor (p G .05). Not UTD for Tdapwas associated with the item ‘It is better for my teen to develop immunity bygetting sick than by getting a vaccine’ (p G .05). Factor analysis found 14items with loadings of 0.4 or higher on 1 of 4 factors. Most items loaded on asingle factor that can best be described as ‘‘safety concerns’’.Conclusions: Although UTD status was good for MCV and Tdap, rateswere marginal for HPV. Vaccine hesitancy in parents of teenagers appeared tobe a contributing factor for being not UTD for HPV.
286
GONORRHEA AND CHLAMYDIA SCREENING: WHOSHOULD WE SCREEN?
Jennings AL, Theriot JA, Franco SM. University of Louisville, Louisville, KY.Purpose of Study: Gonorrhea and Chlamydia (GC/C) are sexually trans-mitted diseases reported in United States youth. In females untreated diseasecan lead to infertility, pregnancy complications and invasive disease. Screen-ing is recommended for all sexually active females less than 25 years of age.Studies have shown an almost equal prevalence of GC/C between males andfemales. Currently there are no screening recommendations for males. Basedon national surveys conducted from 1999-2008 chlamydia prevalence is 6.8%in sexually active 14-19 year olds.
Our study objective was to determine the prevalence and appropriatescreening of GC/C in adolescents that attend our clinic.Methods Used: Our clinic is an inner-city university affiliated pediatricclinic; the majority of the patients are Medicaid recipients. There were 2642patients age 12-18 years old during the study period. In 2010 we screened alladolescents for GC/C at their preventive visits and visits for birth control; in2011 only the adolescents that stated they were sexually active were screened.A chart review was conducted of all patients that had a urine GC/C sentduring the 2 year study period. Demographic data, type of visit, sexual ac-tivity status, GU symptoms, GC/C results, past history of STI were recorded.Children less than 11 years of age were excluded.Summary of Results: 1491 urine screens were sent for GC/C; 908 in 2010and 583 in 2011. Overall 66% were on females and 34% on males; 90% AA,5.9% C, 2.4% H and 1.3% other. A total of n=195 (13.1%) were positive. Seetable. In 2010 2.8% (3/106) of patients with a STI stated they were asymp-tomatic and not sexually active. It is estimated that the more focusedscreening policy will result in missing 16% of STIs.Conclusions: Our inner-city clinic has a very high rate of STIs. One in tenasymptomatic patients had a STI. This data suggests that a broader screen-ing policy, including screening asymptomatic males, would be beneficial inthis population.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 453
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

287
COMPARISON OF EFFECTIVE RADIATION DOSE INPEDIATRIC HEAD COMPUTED TOMOGRAPHY SCANSBETWEEN COMMUNITY AND PEDIATRIC HOSPITALS
Manley-Markowski RN1,3, Stanford K1,3, Glasier C2,3. 1University of Arkansasfor Medical Sciences, Little Rock, AR; 2University of Arkansas for MedicalSciences, Little Rock, AR and 3Arkansas Children’s Hospital, Little Rock, AR.Purpose of Study: In both the medical and lay communities, increasedawareness concerning radiation exposure to patients undergoing diagnosticstudies and therapeutic interventions has prompted changes in computedtomography (CT) scanning protocols, as well as the passage of statutes re-quiring greater accountability and monitoring of radiation dose. The scan’sdose frame includes values to estimate radiation exposure; without this data,there is no way to determine radiation imparted to the patient. Our primaryobjective is to compare effective dose in pediatric patients undergoing headCTs in a pediatric hospital versus a community hospital. We also aim to ex-amine the proportion of scans that include a dose frame. We hypothesize thatradiation dose will be greater in patients scanned at a community hospital.Methods Used: We are currently conducting a retrospective observationalstudy utilizing data uploaded to a radiographic archiving system at ArkansasChildren’s Hospital (ACH) comparing 1) mean effective dose (ED) in non-contrast head CTs performed in community hospitals with scans performedat ACH during 2011; and 2) proportion of scans that include a dose frame.Summary of Results: Data collection is ongoing. Of the 81 scans entered,64 (79%) were performed at ACH and 17 (21%) at a community hospital. Themean effective dose in scans from a pediatric facility was 1.71 (SD 0.708) and62/64 (96.8%) included a dose frame. In scans done at a community hospital,mean ED was 2.396 (SD 0.871) and 15/17 (88.2%) included a dose frame.The difference in mean ED was statistically significant with a p-value of0.00687, however the difference in proportion of scans including a dose framewas not.Conclusions: Preliminary data suggest that pediatric patients undergoingnon-contrast head CTs at community hospitals are at greater risk of exposureto significantly more radiation. This study demonstrates a need to updatepediatric CT protocols in community hospitals to mirror current practices atdedicated pediatric facilities in order to minimize medical radiation exposurein this vulnerable population.
288
KNOWLEDGE ASSESSMENT OF CAREGIVERS OF YOUNGSOCCER PLAYERS REGARDING SPORT RELATEDCONCUSSION
Cantville AM, Joseph M, Kalynych C, Dyer M, Smotherman C, Kraemer D.University of Florida College of Medicine, Jacksonville, FL.Purpose of Study: Much of the media and medical community attentionon sports-related concussion has been focused on athletes at the professional,collegiate, and more recently high school levels. To our knowledge, there is apaucity of research regarding parental understanding of concussion in chil-dren and its potential consequences. The aim of this study was to evaluateparental knowledge of concussion in young children who participate inrecreational soccer.Methods Used: Parents of children aged 4-17 years enrolled in recrea-tional soccer were asked to complete an anonymous survey (23 questions)based on the CDC’s ‘‘Heads Up: Concussion in Youth Sports’’ quiz. Parentswere asked about their level of agreement in regard to statements represent-ing the definition, symptoms, treatment of concussion as well as the sourceof information.Summary of Results: A total of 354 out of 360 parents completed thequestionnaire (98% response rate), where 84% were White, with more thanhalf (63%) female. Most had more than a high school education (96%). Forty-six percent of the children were aged between 8-10 years; 23% between 5-7,and 26% between 11-13. Ninety-two percent of parents believed their childhad never suffered a concussion. However, only 15% (n=55) could correctlyidentify all 7 statements addressing various aspects of concussion. Most didnot identify that a concussion is considered a mild traumatic brain injury andnearly 40% did not identify that a concussion can be achieved from some-thing other than a direct blow to the head. Fifty-two percent of parents re-ported someone had discussed the definition of concussion with them and
61% the symptoms of concussion; with less information provided by theirhealthcare provider (35% and 42% respectively). Of interest, caregivers re-ceiving education about concussion from the internet did better at identify-ing the correct concussion statements compared to those who received it fromother sources (p G .001).Conclusions: While most parents of soccer players received some educationregarding concussion from various resources, important misconceptions re-main regarding the definition, symptoms, and treatment of concussion. Thisstudy highlights the need for healthcare providers to increase educationalefforts among parents of young athletes regarding concussion.
289
REASONS FOR REPEAT IMAGING IN THE PEDIATRICEMERGENCY DEPARTMENT (ED) AND THE IMPACT OF ASTATE WIDE TRAUMA IMAGE REPOSITORY SYSTEM
Thompson TM1, Lovvorn J1, Lynch A1, Hunter E2. 1Univ of Arkansas forMedical Sciences, Little Rock, AR and 2Children’s Mercy, Kansas City, MO.Purpose of Study: Many patients transferred from outside facilities havethe same radiographic studies repeated in the ED for a variety of reasons. Thispractice exposes patients to addition radiation which can have harmful ef-fects on and increase costs to the patient. Previously we determined the rea-sons for repeat radiographic imaging in our ED. With the advent of a state wideTrauma Image Repository (TIR) in 2012, which can send high quality imagesahead of the patient to the receiving hospital, we are evaluating whether thetypes and reasons for repeat imaging in our ED has changed.Methods Used: A prospective study was designed to identify patients whorequire repeat radiographic imaging upon arrival to the ED of a tertiarypediatric hospital, commencing in January 2011 and currently ongoing. Uponarrival, an evaluation sheet was filled out by ED staff to identify the typeof study and the reason it was obtained. The results were analyzed usingSSPS and reported in aggregate.Summary of Results: To date, 139 subjects were identified in the pre TIRstudy period; approximately 45% were identified as trauma patients. 70.3%of these patients had repeat plain films, 16.7% had a repeated CT scan, and7.2% had both a repeated CT scan and plain films. The most common reasonscited for repeat imaging were poor quality film/inadequate views (43%), nofilms sent with patient at time of transfer (20%), and inability to open the filmdisk that was sent (12%). Only 18% of repeat images were clinically indicateddue to a patient status change that warranted further evaluation. Data col-lection in the post TIR period is currently ongoing but preliminary dataanalysis indicates an approximate 8% decrease in repeat trauma imagingstudies.Conclusions: Repeat imaging for intra-hospital transfer to a tertiary facilityis sometimes unavoidable. However, in our institution, clinical indication wasnot the primary reason for repeat studies. This practice incurs both a monitorycost and additional radiation exposure to the patient. The use of a state wideTIR, which can send images to the receiving facility may be one way todecrease radiation exposure and costs to the patient.
290
WHY ARE THERE SO FEW LATINO DOCTORS? LATINOPARENTS’ PERSPECTIVES ON BARRIERS AND POTENTIALSOLUTIONS
Valadez D, Romero R, Garcia J, Jackson A, Villasenor B, Shetgiri R, Flores G.UT Southwestern, Dallas, TX.Purpose of Study: Latinos constitute 16% of the US population, but G 3%of US physicians. Little is known about the reasons for this disparity, par-ticularly from the perspective of Latino parents. The study aim was to ex-amine parental perspectives on barriers to Latino adolescents’ pursuit ofa career in medicine, and potential solutions for increasing the number ofLatino doctors.Methods Used: Focus groups and interviews were conducted of parentsof Latino teens, stratified by children’s immigration status and enrichment-program participation. 14 questions were asked about barriers to a medicalcareer, diversity in medicine, enrichment programs, and solutions for in-creasing the number of Latino doctors. Sessions were audiotaped, transcribed,and analyzed using margin coding and grounded theory. Themes were in-dependently identified by 3 coders; disagreements were resolved by consensus.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
454 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: The 15 participants had a mean age of 42 years.Participants stated that medicine is a demanding profession with a lengthycareer path. Barriers to pursuing a medical career include lack of informa-tion about higher education and medical careers. One participant said, ‘‘Theydon’t know of all the opportunities that could help them, they have to reallylook for them. It’s not advertised.’’ Financial barriers, immigration status, cul-tural stereotypes and racism, and lack of support from families and schools alsowere noted. Participants stated that the growing Latino population requiresmore Latino doctors and that shared language and culture lead to improvedcare. Suggested solutions include better access to educational information,parental and school support, government-assisted financial aid, and more en-richment programs. Enrichment programs are beneficial by providing infor-mation, enhancing motivation, and increasing exposure to medicine.Conclusions: Parents identified many barriers to medical careers for Latinoyouth and the need for more Latino doctors. Parental and school supportand financial aid were noted to be important for Latinos to pursue a medicalcareer. Providing information for parents and teens on careers in medicineand financial assistance may be potential solutions. Incorporating this infor-mation into enrichment programs and increasing access to such programs mayincrease the number of Latino doctors.
291
ORAL ANTIOXIDANTS IMPROVE ENDOTHELIALFUNCTION IN PATIENTS WITH CYSTIC FIBROSIS
Fox B, Harris RA. Georgia Health Sciences University, Augusta, GA.Purpose of Study: Cystic fibrosis (CF) is a genetic disorder which hasdetrimental effects onmany organ systems throughout the body. Several studieshave demonstrated that patients with CF exhibit systemic oxidative stress,which may in turn contribute to vascular endothelial dysfunction. The bra-chial artery flow mediated dilation (FMD) test is a non-invasive bioassay ofendothelial function. This study sought to determine if an oral antioxidantcocktail improves endothelial function in patients with CF.Methods Used: 14 patients with CF (age: 18.6 + 7.9 yrs.) participated inthis study. Following an overnight fast, brachial artery FMD was assessed.Patients were then given an oral antioxidant cocktail (1000 mg vitamin C, 600 IUvitamin E, and 600 mg >-lipoic acid) and allowed to rest for two hours beforeanother FMD test was performed.Summary of Results: The oral antioxidant cocktail significantly improvedFMD (5.23T2.7 vs. 7.46T4.7%; p=0.039) and FMD normalized for shearstimulus (0.096T0.06 vs. 0.152T0.06%/s-1, AUC; pG0.001) in patients withCF. Moreover, FMD and FMD normalized for shear were restored to valuesof healthy controls (7.54% and 0.151%/s-1, AUC, respectively).Conclusions: These data demonstrate that an oral antioxidant cocktail notonly improves endothelial function in patients with CF, it also restores en-dothelial function to a level seen in healthy controls. This study providesevidence that oxidative stress contributes to endothelial dysfunction in pa-tients with CF.
292
THE ROLE OF STIGMA IN PARENTAL HELP-SEEKING FORCHILD BEHAVIOR PROBLEMS AMONG URBAN AFRICANAMERICAN PARENTS
Davis DW1, Dempster RM2, Jones V1, Ryan L1. 1University of Louisville,Louisville, KY and 2Ohio State University, Columbus, OH.Purpose of Study: The present study examined the relationship betweenstigma and parental help-seeking after controlling for demographic variables,child behavior, and barriers to treatment for African American families in anurban, low SES community.Methods Used: Parents (n=148) of children ages 2-8 were recruited in anurban, primary care practice with 92% Medicaid recipients. Parents com-pleted surveys assessing demographics, child behavior, barriers to treatment,perceived stigma regarding parenting classes (parental self-stigma, publicstigma, and personal impact of stigma), and perceived likelihood of enroll-ing in parenting classes. Linear regression analyses and a paired t-test wereconducted.Summary of Results: Linear regression identified control variables fromdemographic variables, barriers to treatment, and child behavior. Child andparental age, parental education, single parent status, and barriers to treatment
did not significantly predict parental likelihood of attending parenting classes.Parents rated themselves as more likely to attend classes when they perceivedgroup classes as effective for child behavior problems (A=.36, pG.01) andendorsed more child behavior problems on the Pediatric Symptom Checklist(A=.28, p=.03). Likelihood of attending parenting classes was related to lowerratings of self-stigma (A=-.32, p=.02). The inclusion of stigma toward thechild did not significantly increase the variance explained in perceived likeli-hood of attending parenting classes. No significant difference was found inpublic stigma and personal impact of stigma toward self or child for attendingclasses in a post-hoc paired t-tests.Conclusions: Self-stigma for attending parenting classes is associated withthe likelihood of African American parents attending classes over and aboveperceived effectiveness of classes and child behavior. When providers aremaking referrals to African American families for behavioral parenting ser-vices, it is important to consider stigma as a barrier to treatment and addressthese concerns. Future research is needed to better understand cultural dif-ferences in perceived stigma and the relationship between stigma and help-seeking behaviors.
293
EVALUATING THE EFFECTIVENESS OF A TRAUMACENTER-BASED DRIVING CLASS FOR TEENAGERS
Frascogna MN, Foster E, Isbell SK, Massey K. University of MississippiMedical Center, Jackson, MS.Purpose of Study: The IMPACT (Improving Motor Vehicle Practices andAwareness in Community Teens) program is a trauma center-based class forteenage drivers who have received traffic violations that incorporates defen-sive driving curriculum with a demonstration of the medical consequencesof reckless driving. The purpose of this study is to evaluate for changes inplanned driving behaviors of participants before and after the class.Methods Used: Class participants were asked to complete a questionnaireon personal driving habits before the class and at the completion of theprogram. Responses were entered into Microsoft SSPS\ (version 16.0) andanalyzed with descriptive statistical charts and one-way ANOVA.Summary of Results: A total of 110 students completed the IMPACTprogram between August 2011 and August 2012. The majority of participantswere between 16 to 18 years of age, with 58% male and 42% female. Therewas a statistically significant increase in the number of participants who re-ported seatbelt usage before the class compared to those who reported plan-ning to wear a seatbelt after the class (p=0.00). The number of participantswho reported texting while driving showed a significant decrease before andafter the class (p=0.00). The number of participants who reported drivingover the speed limit also showed a significant decrease before and after theclass (p=0.00).Conclusions: Participants of the IMPACT program demonstrated a signif-icant improvement in planned driving practices after completion of the class.
294
PROXIMITY TO MAJOR BODIES OF WATER ANDKAWASAKI DISEASE
Burns JJ1, Broge T1, Grisset R1, Taylor S1, Hommeida S1, Onuegbu P1,Amin R2. 1Florida State University, College of Medicine, Pensacola, FLand2University of West Florida, Pensacola, FL.Purpose of Study: To determine if KD patients reside closer to mainbodies of water or live in Census tracts with higher density of water com-pared to a matched control group.Methods Used: Shapefiles for five categories of Florida Panhandle lakes,rivers, coastal water, swamps and an offshore Gulf of Mexico boundary wereadded as layers to a map in ArcMap\. Addresses for children admitted withKD to the only Children’s Hospital in the Florida panhandle from 2/16/2008to 9/10/2011 were subsequently plotted and added as a layer to the same map.A control group consisting of patients admitted to the same hospital for non-KD medical problems were matched for age, gender and date of admissionwith the KD cases. Their addresses were also mapped in a layer superimposedon the bodies of water layers. A spatial join was performed between the bodiesof water to the KD cases and controls generating distance to nearest water inmeters (m) for each category of water. KD and control group distances werecompared using Mann Whitney non-parametric test. To account for five
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 455
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

comparisons in this analysis, significance was set at p e0.01 using Bonferonnicorrection. Additionally, the water to land ratio for each census tract was cal-culated and geographically linked to cases and controls. The ratios were thenalso compared using Mann Whitney test.Summary of Results: There were no differences between KD cases andcontrols for median distances to lakes (control 8727m vs. KD cases 6229m;p=0.199), coastal water (control 479m vs. KD cases 407m; p = 0.185), Gulfof Mexico (control 30275m vs. KD cases 33820m; p = 0.033) or rivers(control 10534m vs. KD cases 7901m; p = 0.117). Also, the ratio of waterto land was not different (control 0.020 vs. KD cases 0.020; p = 0.298).Conclusions: No differences in distance to main bodies of water or Cen-sus tract water density was noted when KD cases were compared to controls.It is still possible that smaller drainage ditches or streams would be relatedas was noted in prior studies.
Allergy, Immunology, and Rheumatology IConcurrent Session
2:00 PMFriday, February 22, 2013295
IL-21 PROMOTES A GERMINAL CENTER REACTION BYREGULATING TFR/TFH IN AUTOIMMUNE BXD2 MICE
Ding Y, Hsu H, Mountz JD. The University of Alabama at Birmingham,Birmingham, AL.Purpose of Study: Follicular T helper (Tfh) cell is critical for germinalcenter (GC) B cells to develop into long-lived plasma cells, while follicularregulatory T cell (Tfr) is a Treg subset that suppresses GC B cell differen-tiation. Interleukin 21 (IL-21) promotes Tfh differentiation but inhibits Treg.It is, however, not known if IL-21 promotes an autoreactive GC response viainhibition of Tfr. The aim of this study is to determine whether and how IL-21regulates Tfrs in autoimmune BXD2 mice that develop spontaneous GCs.Methods Used: Spleen cells from WT and BXD2-Il21-/- mice were sub-jected to FACS and confocal imaging analyses; In vitro stimulation by rmIL-21on CD4 T cells and in vivo administration of IL-21 producing adenovirus(AdIL21) in BXD2-Il21-/- mice were performed to investigate the effects ofIL-21 on Tfrs. The suppressive function of Tfrs on B cells and T cells wasstudied by a co-culture assay.Summary of Results: There were significantly reduced GL-7+Fas+GC Bcells and ICOS+CXCR5+ Tfhs in BXD2-Il21-/- mice; however, the conven-tional FoxP3+ Treg were equivalent in Il21-/-mice in the spleen compared towild type (WT) BXD2 spleen. Analysis of ICOS+CXCR5+CD4 Tfh subsetin BXD2-Il21-/-mice showed that most these cells expressed FoxP3+, thetranscription factor for Treg. The frequency of Tfr in BXD2-Il21-/- mice was2-folds higher than that in WT. The Tfr cells in BXD2-Il21-/- mice also ex-pressed other markers of Tregs including CTLA4,TGF-A1, and GITR. Con-focal imaging showed that there was an increased number of FoxP3+ CD4 Tcells in spleen follicles of BXD2-Il21-/- mice. In vitro treatment of CD4 Tcells with IL-21 increased Tfhs but decreased Tfrs. AdIL-21 increased GC Bcells but decreased the ratio of Tfr/Tfh in the spleen of BXD2-Il21-/- micein vivo. Tfrs suppressed survival of B cells and proliferation of Tfhs, whilermIL-21 counteracted the effect of Tfrs in vitro.Conclusions: In autoimmune BXD2 mice, IL-21 positively promotes anautoreactive GC reaction via increasing Tfhs, decreasing Tfrs, and inhibitingthe suppressive function of Tfrs on B cells and Tfhs. Manipulating Tfr/Tfh andIL-21 signaling may be an important novel therapy for autoimmune patientswith increased Tfhs.
296
ABSENCE OF CD19 EXPRESSION ALLOWS PASSAGE OFB CELLS WITH MORE CHARGED AND HYDROPHOBICCDR-H3 AMINO ACID CONTENTS
Khass M1, Freeberg L2, Zhuang Y1, Carter R4, Justement L4, Schroeder H3.1UAB, Birmingham, AL; 2University of Alabama at Birmingham,Birmingham, AL; 3UAB, Birmingham, AL and 4UAB, Birmingham, AL.Purpose of Study: CD19 is a cell surface protein that modulates thethreshold of signaling through B cell receptor. Reduced CD19 expressionhas been observed in some human patients with common variable immunedeficiency (CVID), a disease which is characterized by decreased produc-
tion of mature B cells with increase in their auto- reactivity. B cell repertoirein absence of CD19 expression has not been well characterized. We previ-ously showed that, B cell repertoire is controlled by the sequence char-acteristics of the complementary determining region heavy chain (CDR-H3)which lies at the center of the antigen binding site. We sought to examine theCDR-H3 repertoire in mice lacking CD19 expression, using our novel bio-informatics system, to test whether its absence can affect the control of Bcell repertoire development and auto reactive antibody production.Methods Used: We analyzed the CDR-H3 based on its length, reading frameusage and average hydrophobicity of its amino acid contents.Summary of Results: Our results show that follicular B cells lackingCD19 expression had an increase of the use of disfavored highly chargedas well as highly hydrophobic CDR-H3 sequences.Conclusions: This might suggest a lack of control of mature B cell develop-ment at follicles which might promote the production of auto-reactive antibody.This information can help to explain the mechanism by which auto reactiveB cells might be produced in human CVID patients.
297
MANAGEMENT OF LOWER EXTREMITY FRACTURES INMEN WITH SPINAL CORD INJURIES
Jessee R1, Weaver F2,3, Chin A2, Burns S4,5, Svircev J4,5, Hoenig H6,Heggeness M7,8, Carbone L1,9. 1University of Tennessee Health Science Center,Memphis, TN; 2Edward J. Hines, Jr. VA Hospital, Hines, IL; 3Stritch School ofMedicine, Loyola University, Maywood, IL; 4VA Puget Sound Health CareSystem, Seattle, WA; 5University of Washington, Seattle, WA; 6Durham VAMC,Durham, NC; 7VA Medical Center, Houston, TX; 8Baylor College of Medicine,Houston, TX and 9Memphis VA Medical Center, Memphis, TN.Purpose of Study: To describe characteristics of men with spinal cordinjuries (SCI) who received surgical compared with nonsurgical treatmentfor lower extremity fractures.Methods Used: A population-based study of 1,056 male veterans enrolledin the VA Spinal Cord Dysfunction Registry from FY2002-2007 who had anincident lower extremity fracture and were followed for one-year post fracture.Summary of Results: There were no significant differences in demo-graphics (age, race), SCI-related factors (level of injury, duration of injury)and Charlson comorbidity scores in those who received surgical comparedwith nonsurgical treatment for lower extremity fracture (p90.07 for all). Thenonsurgically treated group had a higher proportion of complete extent ofSCI, and the surgically treated group had a higher proportion of incompleteand missing levels of injury. Based on location, surgical treatment was mostlikely to be performed on hip fractures, including fractures of the femoralneck (36%) and intertrochanteric area (20%), and least likely for patella frac-tures (0%). Nonsurgical management was most likely to occur for patella(100%) and tibia/fibula (95%) fractures. Overall, surgical treatment forincident lower extremity fractures occurred in a minority (9.5%) of patients.Conclusions: Surgical therapy for lower extremity fracture repair in menwith SCI is done in approximately 10% of these fractures and is more likelyto be used in the setting of hip fractures. Specific patient characteristics donot appear to be associated with choice of fracture management. Limitationsincluded lack of upper extremity fractures, women, those with acute SCIinjury (less than two years duration) or non-traumatic causes of SCI. Also, wedid not include fracture treatments done outside the VA medical system.
298
ROLE OF DA GERMLINE SEQUENCE ON CONSTRAININGTCR CDRA3 DIVERSITY
Levinson M, Silva Sanchez A, Zhuang Y, Schroeder HW. University ofAlabama at Birmingham, Birmingham, AL.Purpose of Study: A highly diverse T cell receptor (TCR) repertoire isnecessary for the recognition of exogenous antigens. This diversity is devel-oped through V(D)J rearrangement and N addition during TCR development.The product of V(D)J rearrangement in the beta chain of the TCR is theCDRA3, a region of high variability that recognizes antigen and includes allof the D gene. Interestingly, the DA sequence, the D gene for the beta chain ofthe TCR, is highly conserved across various species, from trout to mouse tohumans. This suggests that there are some natural constraints on the TCR;these constraints are thought to limit deleterious T cells from reaching the
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
456 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

periphery. We hypothesize that altering the D region will have an effect on thedevelopment of thymocytes.Methods Used: Both developing thymocytes and mature splenic T cellswere sorted by flow cytometry based on their expression of either CD44, CD25and CD28 or CD4 and CD8. RNA from the thymocytes was extracted and theVDJ-beta genes were sequenced using primers to the VB13-1 and to the VBC1.In frame sequences were analyzed using IMGT junction analysis program.Summary of Results: We have preliminary data comparing the T cell re-pertoires of WTand altered DAmutants. The mutants are a DA2 KO (DA1); areplacement of the DA locus with a charged DA (DADKRQ); and a replace-ment of the DA locus with a hydrophobic DH (DAYTL). When compared toWTmice, the mutant DAmice have an altered T cell repertoire in both CDRA3amino acid composition and CDRA3 length and these differences can beattributed to the changes in the germline sequence. Changing the DA alsochanges the total T cell number in both developing and mature T cells, witha charged DA being selected against.Conclusions: The DA germline sequence is clearly affecting the TCR re-pertoire. In DADKRQ mice, the repertoire is skewed toward a shorter, morecharged distribution. In DAYTL mice, CDRA3 repertoire appears skewedtowards a more hydrophobic, longer, BCR-like distribution. However, thealtered TCR repertoire isn’t as hydrophobic as the BCR repertoire, suggest-ing mechanisms of somatic selection by preferring a less charged CDRA3.Ongoing experiments using varied TCR DA locus mutants will elucidate therole of the germline sequence on the development of thymocytes.
299
THE INCIDENCE AND RELIABILITY OF SELF REPORTEDPENICILLIN ALLERGY IN A COMMUNITY HOSPITAL
Katzen S, Woolbert A, Anderson S, Parker M, Anderson R, Slaton M,Khasawneh F. Texas Tech University Health Sciences Center, Amarillo, TX.Purpose of Study: The majority of antibiotic allergies are self-reported andpenicillin (PCN) allergy accounts for most cases. Reported allergy deprivesthe patient from this class of antibiotics and creates hesitancy in using otherbeta-lactam antibiotics. Up to 20% of patients with reported PCN allergy arefound to be truly allergic when assessed by skin testing. The reasons behind thisover reporting include mixing side effects for allergic reactions and beinginformed of their alleged allergy by a parent without a first hand-recall of it.Methods Used: The aim of this prospective observational study is to re-port the incidence of PCN allergy among adult patients admitted to a com-munity hospital in Amarillo, TX. Patients 18 years-of-age or older who wereadmitted to Texas Tech Internal Medicine (TT IM) service between 07/25/11until 01/25/12 were included. The investigators screened admitted patients ona daily basis and approached those with reported PCN allergy for partici-pation. Consented patients were asked to complete a questionnaire.Summary of Results: During the study period, 2589 patients were admittedto TT IM service. Among the admitted, 378 patients (14.6%) had self-reportedPCN allergy and 193 of those (51.1%) consented and answered the studyquestionnaire. The mean age of patients at the time of the allergic reactionwas 20.3 T 15.0 years. The most common allergic symptoms reported wereitchy rash followed by angioedema and urticaria. Thirteen patients (6.7%)reported possible side effects as allergic reactions. Out of the participants, 121patients (62.7%) had probable PCN allergy, 55 patients (28.5%) had possiblePCN allergy and 17 patients (8.8%) had unlikely PCN allergy. Fifty one pa-tients of the consented cohort (26.4%) had subsequent exposure to PCN and itwas tolerated in 86.3% of them. Fifty patients (25.9%) had subsequent ex-posure to a first generation cephalosporin and it was tolerated in 80.0% ofthem. Forty two patients (21.8%) were admitted to the hospital with an in-fection, 24 of whom received and tolerated cephalosporins and carbapenems.Conclusions: Taking a detailed history from patients with self-reportedPCN allergy helps in excluding true PCN allergy and allows the clinician touse this important class of antibiotics when indicated.
300
THE RISK OF FRACTURES WITH ALPHA BLOCKERS AND5-ALPHA REDUCTASE INHIBITORS IN BENIGN PROSTATEHYPERPLASIA: A META-ANALYSIS
Lim S, Laengvejkal P, Nugent K. Texas Tech University Health SciencesCenter, Lubbock, TX.
Purpose of Study: Benign prostate hyperplasia (BPH) is the most com-mon benign neoplasm affecting older men. More than 14 million men in theUnited States have symptoms of lower urinary tract symptoms, the mostcommon cause being BPH. Symptomatic BPH is usually treated medicallyif there is no absolute indication for surgery. 5-alpha reductase inhibitorsand alpha blockers are often used in the medical management. The asso-ciation of exposure to alpha blockers and 5-alpha reductase inhibitors andfractures is still unknown.Methods Used: Studies were identified by searching Pubmed, Embase, theCochrane library, ISI Web of Knowledge and reference list of articles. Pub-lications involving BPH patients exposed to either alpha blockers or 5-alphareductase inhibitors that compared fractures cases with controls and reportedthe odds ratio or relative risk estimates with 95% confidence intervals wereincluded. We defined a study as an analysis of exposure to either alphablockers or 5-alpha reductase inhibitors. Two authors extracted data inde-pendently and assessed study quality. Pooled odds ratios were calculatedusing the random effects model.Summary of Results: Of 436 publications identified, four publications re-ported fracture risk in BPH patients exposed to either 5-alpha reductase in-hibitors or alpha blockers. Three studies addressed fracture risk in patientsexposed to 5-alpha reductase inhibitors (21366 fracture cases). Four studiesaddressed fracture risk in patients exposed to alpha blockers (17828 fracturecases). There was good interrater agreement regarding inclusion and exclu-sion of studies involved (inter-rater agreement statistic Kappa=0.713). Thepooled OR for fractures with 5-alpha reductase inhibitor use was 0.85 (95%confidence interval (CI) 0.38-1.89). The pooled OR for fractures with alphablocker use was 1.19 (95% CI 0.97-1.47).Conclusions: Use of 5-alpha reductase inhibitors and alpha blockers in BPHpatients are not associated with a statistically significant change in fracturerisk. However, more studies are needed to further evaluate the effects of thesedrugs on fracture outcomes in view of their increasing use in the long termmedical management of BPH.
301
A SURVEY TO EXPLORE THE TYPES OF FOOD CAUSINGFOOD ALLERGIC REACTIONS AMONG ADULTS ANDCHILDREN OF ASIAN INDIAN ORIGIN
Motiani RA1, Dinakar C1. 1East Tennessee State University, James H QuillenCollege of Medicine, Johnson City, TN, TN and 2Children’s Mercy Hospital,University of Missouri at Kansas City, Kansas City, MO.Purpose of Study: 1. Explore the Types of Foods causing Food- allergicReactions among Adults and Children of Asian Indian Origin 2. Developstandardized allergy testing in future for Asian Indian population for theidentified substances.Methods Used: It is a descriptive pilot survey of a convenience sample ofAsian Indians attending a health fair at the Hindu Temple at Kansas City onApril 10, 2010 (single-site). IRB approval was obtained at Children’s MercyHospital, Kansas City. A survey questionnaire was developed and subjectswere questioned on demographic data, type and nature of food allergic re-actions, types and nature of foods, presence and type of other allergies, eczemaand asthma. No identifiers were asked or recorded. All subjects registeringat the registration desk of the Hindu Temple were offered the opportunityto participate in the survey. Parents were requested to fill out the forms fortheir children.Summary of Results: In our pilot survey, allergies to wheat, egg, carrot,meat, Suji (cream of wheat), Peanut, Iron pills, almond, soy, spinach, corn, appleand pineapple were reported. In this small study, allergy to ethnic ingredientSuji was reported by one subject, which is also called cream of wheat. Twoother subjects reported allergy to wheat. Interestingly, six out of 12 subjectshad associated eczema, only one had associated asthma and two subjectsreported associated environmental allergies.Conclusions: In Asian Indian populations, food allergies although pre-served, have not been systematically studied. Because of the unique dietspecific to Asian Indian population, the food allergies reported tend to be‘unusual’ and ‘different’ from those reported in the Western populace. It isdocumented in one previously reported similar case that various forms ofwheat including flour, daliya, maida, suji and wheat bran can cause urticariaand angioedema. Apart from the challenges of being unfamiliar with thesefoods, there are no currently available standardized tests that can be per-formed to diagnose these food allergies. No such research survey assessing
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 457
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

food allergic reactions in Asian Indian population was previously availablein our knowledge.
302
OSTEOPOROSIS SCREENING IN MEN: PATIENTCHARACTERISTICS THAT PREDICT SCREENING IN APRIMARY CARE SETTING
Lim S, Lim J, Mojazi Amiri H, Okamura R, Nguyen D, Nugent K. TexasTech University Health Sciences Center, Lubbock, TX.Purpose of Study: Osteoporosis in men is an under-recognized and un-dertreated condition. Current National Osteoporosis Foundation (NOF) guide-lines recommend osteoporosis screening in (1) men above age 70 (2) menaged 50-69 with clinical risk factors. Despite these guidelines being initiallypublished in 2008, screening rates in men in the United States remains un-defined. Determination of predictors that affect screening are important inimproving screening efforts.Methods Used: We performed a retrospective chart review of male pa-tients who were seen in between January 1st, 2011 and January 1st, 2012 atthe Internal Medicine Clinic at Texas Tech University Health Science Center,a major primary care setting in West Texas. We included males age 70 andabove and those aged 50-69 with clinical risk factors. Clinical risk factorswere defined as a BMI less than 25, past medical history of fracture or rheu-matoid arthritis, and prolonged use of corticosteroids, or antiandrogens. Weidentified patients who had established the Internal Medicine Clinic as theirprimary care provider by including patients who had been seen at least twiceover a 3 year period. Demographic information and BMD testing status weredetermined from electronic medical records. Logistic regression was used todetermine patient characteristics that affected screening.Summary of Results: 1062 patients age 50 and above were seen at ourclinic during the study period. There were 310 males age 70 and above. 121males aged 50-69 had clinical risk factors for osteoporosis. The DEXA scanscreening rate was 13.9%. Patient characteristics more likely to be associ-ated with screening were a history of fracture (odds ratio (OR) 6.2, 95% confi-dence interval (CI) 2.6-14.6), glucocorticoid use (OR 3.3 95% CI 1.1-9.8),antiandrogen use (OR 17.6, 95% CI 1.7-178.8), and past medical history ofrheumatoid arthritis (OR 5.8, 95% CI 1.9-18.2). Current smokers were lesslikely to be screened (OR 0.1 95% CI 0.04-0.5).Conclusions: Osteoporosis screening rates in men remain low despite the2008 NOF recommendations. Smokers are less likely to be screened andshould be targeted in screening programs.
303
A CASE OF CONCOMITANT COCAINE INDUCEDVASCULITIS AND HEPATITIS C ARTHROPATHY
Bruce J1, Compton S1, Majithia V1,2. 1University of Mississippi, Jackson, MSand 2GV Sonny Montgomery VA, Jackson, MS.Case Report: Introduction:ANCA associated vasculitits and neutropeniahas been seen in patients who use cociane contaminated with levamisole,which has been found in up to 70% of the cocaine bought in the US. Upto 20% of patients with Hepatitis C can develop arthritis, which in 2/3 isrheumatoid-like. It is often difficult to distinguish from rheumatoid arthri-tis, though treatment is different.
Case Presentation: A 30 yo female with history of Hepatitis C admittedwith orbital cellulitis also had a two year history of lower extremity rash andjoint pain in her hands,shoulders,knees and ankles.On exam,rash was con-sistent with panniculitis.There was no evidence of synovitis on exam. Perti-nent labs: previous urine drug screen cociane + ;WBC 1.8,CRP 2.8;ESR 13;+ANA,Hep C Ab,MPO,PR3 and dsDNA.No evidence of erosions on x-ray.Skin biopsy revealed perivascular dermatitis with dermal necrosis on both leftand right thigh.It was determined her rash was caused by cocaine-inducedvasculitis and joint pain was caused by Hepatitis C associated arthritis. Herrash improved with prednisone.She is being followed in our clinic.
Discussion and Conclusion: This case highlights a case of cocaine in-duced vasculitis and hepatitis C arthropathy.Our patient had symptoms sec-ondary to her cocaine use and history of viral hepatitis that are difficult todistinguish from autoimmune connective tissue disease.However, it’s im-portant to distinguish the etiology as treatments are different and agentstraditionally used to treat arthritis from connective tissue disease can’t be used
to treat hepatitis-associated arthritis.Cocaine-induced vasculitis is causedfrom levamisole, an immunomodulatory agent that is added to 70% of co-caine bought in US.It is associated with an ANCA vasculitis and the mostcommon clinical symptoms are arthralgias,skin lesions and sometimes neu-tropenia.The vasculitic skin lesions have been reported in various forms andare usually responsive to steroids.Hepatitis C has been associated with anarthritis that is similar in presentation to rheumatoid arthritis and may also haverheumatoid factor positivity. It can be associated with a vasculitis as well.Treatment with conventional agents may be problematic,which is why it isimportant to determine the etiology.
304
SARCOIDOSIS GETS ON THE NERVES
Compton S, Bruce J, Majithia V, Vedanarayanan V. University of MississippiMedical Center, Jackson, MS.Case Report: Introduction:
Sarcoidosis is a granulomatous disorder of unknown etiology that canaffect multiple organ systems. Neurologic manifestations occur in 5% of pa-tients with sarcoid. As it is a relatively uncommon manifestation, diagnosiscan prove challenging.
Case Description:A 21 year old African American female was seen by a neurologist for
increasing pain in her feet over three weeks. Symptoms began in her left greattoe started to hurt; it eventually encompassed the whole foot and extended upthe ankle. Shortly after, similar symptoms arose in her right foot and even-tually changed her gait. She had also been diagnosed with acute iritis andtreated successfully with steroid drops recently. There was concern for a neu-ropathy related to vasculitis and an electromyelogram (EMG) was planned. Onthe day of her EMG, she was noted to have a new onset right-sided Bell’spalsy. Her EMG showed acute denervation, and she subsequently received asural nerve biopsy that was concerning for mononeuritis multiplex. ACE and1,25 OH Vitamin D levels were both elevated with hilar adenopathy seen onimaging. Other causes for vasculitis were ruled out. A presumptive diagnosisof sarcoid associated vasculitis was made; she was admitted and placed onpulse dose intravenous steroids. Her lower extremity pain improved dramati-cally. Prior to discharge, she was transitioned to oral prednisone and azathio-prine. At her four week follow up visit, she was ambulating without difficulty,her Bell’s palsy had largely resolved, and she had resumed working.
Discussion:This case illustrates sarcoidosis manifesting with both mononeuritis mul-
tiplex and Bell’s palsy. Neurologic complications occur in approximately 5%of sarcoid patients with the majority experiencing cranial nerve disorderssuch as Bell’s palsy. The incidence of simultaneous cranial and peripheralneuropathy is less published. While the presentation may be uncommon, asystematic, multi-specialty approach can lead to a prompt diagnosis. Once thediagnosis is reached, a favorable outcome can be reached by appropriate ther-apy. Systemic steroids remain the mainstay of therapy, but steroid-sparing im-munosuppressants can be considered to minimize the dose of glucocorticoids.
Cardiovascular IConcurrent Session
2:00 PMFriday, February 22, 2013305
PULMONARY ARTERY SYSTOLIC PRESSURE BYECHOCARDIOGRAPHY STRONGLY PREDICTS OUTCOMESIN STABLE OUTPATIENTS WITH HEART FAILURE
Siwamogsatham S1,2, Georgiopoulou VV1, Marti CN1, Butler J1,Kalogeropoulos AP1. 1Emory University, Atlanta, GA and 2KingChulalongkorn Memorial Hospital, Bangkok, Thailand.Purpose of Study: Pulmonary hypertension (PH) by right heart catheteri-zation is associated with worse prognosis in heart failure (HF). However, dataamong pulmonary artery systolic pressure (PASP) derived by echocardiog-raphy (echo) on prognostic value are limited, especially in outpatients onoptimal therapy.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
458 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Methods Used: We evaluated 200 stable HF outpatients with availableecho derived PASP at baseline in our prospective cohort study. We definedecho PH as PASP 945 mmHg. We studied the association of baseline echo-PH with (1) survival free of clinical events (death, urgent heart transplantation(HTx), ventricular assist device [VAD] implantation, or HF hospitalization)and (2) all-cause and HF hospitalization rates.Summary of Results: Patient characteristics are shown in Table1. 61 pa-tients (30.5%) had PH (PASP 945 mmHg). After 24T11 months, there were98 clinical events (death:23; HTx:3; VAD:1; HF hospitalizations:71). Riskfor events was significantly higher in patients with PH (hazard ratio [HR]:2.61; 95% confidence interval [CI]: 1.56 to 4.32; PG0.001). In models ac-counting for age, HF etiology, LVEF, E to A ratio, and deceleration time, PHwas still associated with a higher risk for events (HR: 2.00; 95% CI: 1.03 to3.89; P=0.04). Patients with echo-PH also had higher rates of all-cause hos-pitalizations (137 vs. 81 per 100 patient-years) and HF hospitalizations (69 vs.26 per 100 patient-years); adjusted incidence rate ratio 1.64 (95% CI: 1.29 to2.10; PG0.001) and 2.92 (95% CI: 2.00 to 4.28; PG0.001), respectively.Conclusions: In stable HF outpatients, an echo derived PASP 945 mmHgstrongly predicts higher risk of clinical events and hospitalizations.
306
BIOMARKERS OF CENTRAL AND SYSTEMIC CONGESTIONIN MONITORING RECOVERY FROM DECOMPENSATEDHEART FAILURE
Adeboye AA, Wheeler BJ, Iwueke IC, Weber KT. University of TennesseeHealth Science Center, Memphis, TN.Purpose of Study: In patients having a dilated (idiopathic) cardiomyopathywith reduced systolic function, the appearance of decompensated heart failurewith its disabling symptoms and signs has its pathophysiologic origins rootedin a salt-avid state. Effector hormones of the renin-angiotensin-aldosteronesystem orchestrate the accompanying retention of salt and water with anensuing congestion of central and systemic vascular compartments. Distentionof atria and ventricles serve to release a family of natriuretic peptides, in-cluding brain natriuretic peptide (BNP), while with hepatic congestion cobal-amin, or vitamin B12, is released from the endothelium of sinusoids. Hence,consequent elevations in serum BNP and B12, respectively, serve as bio-markers of central and systemic congestion. We hypothesized these bio-markers could be used to gauge decompensated and compensated states ofheart failure.Methods Used: 16 patients (54T3 yrs; 11 males) having a nonischemic di-lated cardiomyopathy, with or without reduced ejection fraction, were followedwith serum BNP and B12 obtained on: a) the day of hospital admission fordecompensated heart failure; b) the day of hospital discharge; and c) 5T1 wksafter discharge when compensated and followed in the outpatient clinic.Summary of Results: At the time of hospitalization, evidence of centraland systemic congestion was present with elevations in both serum BNP(1487T256 pg/mL) and B12 (806T69 pg/mL; normal G600). At the time ofdischarge (5T2 days) after bedrest, modified Na+ diet and pharmacologic in-tervention, serum BNP had fallen to 403T84 pg/mL). During outpatient follow-up, evidence of compensated failure without central and systemic congestionwas present accompanied by serum BNP (417T56 pg/mL) and normalizedB12 (481T41 pg/mL).Conclusions: Serial monitoring of serum BNP and B12 provide usefulancillary information in the clinical assessment of the recovery from de-compensated failure and resolution in central and systemic congestion withattainment of a compensated state of heart failure. Furthermore, serum B12
provides specific information as to the resolution of splanchnic congestionwhich would facilitate optimal absorption of oral medications.
307
RISK FACTORS FOR HEART FAILURE READMISSION
Siegfried JS, Sagiv O, Berkowitz E, Patel S, Eltom A, Takhalov Y, Benjamin R,Alemu B, Osahan D, Siller J, Ullman J, Panagopoulos G, Messineo F,Coplan NL. Lenox Hill Hospital, New York, NY.Purpose of Study: Readmission within 30 days of a hospitalization forheart failure (HF) is common and portends a poor prognosis. This study wasdesigned to determine the rate and reason for readmission and to identity as-sociated risk factors.Methods Used: Patients with an index admission for HF were followedprospectively for 30 days. Data regarding demographics, risk factors anddischarge plan was collected during the index admission and any readmissionwithin 30 days. Patients who were not readmitted within 30 days were con-tacted and interviewed.Summary of Results: 133 patients were studied; 40 (30%) were readmittedwithin 30 days - 13 (32.5%) for HF, 2 (5%) for pneumonia, and 25 (62.5%)for other reasons (most commonly other infections, 20%). Patients admittedto a cardiac unit were less likely to be readmitted than those admitted to amedical unit (23.9% vs 47.2%, p=0.04). After the index admission, patientsdischarged to a nursing facility were more likely to be readmitted than pa-tients discharged home (57.1% vs 24.8%, p=0.004). Those initially dischargedhome were more likely to be readmitted if they lived alone than if they livedwith family (47.6% vs 13.8%, p=0.004). Readmitted patients were less likelyto have followed up with a cardiologist after discharge (33.3% vs 80.2%,p=G0.001). No single comorbidity was associated with a significantly in-creased readmission rate (Table).Conclusions: After an index HF admission, readmission rates for HF weresimilar to nationally observed rates. The majority of patients were readmittedfor reasons other than HF. Living independently with support and physicianfollowup are factors associated with decreased readmissions. This suggeststhat future efforts to decrease HF readmission rates should focus on dis-charge planning and outpatient followup.
308
ENDOTHELIAL DYSFUNCTION AND INFLAMMATIONAMONG ADOLESCENTS WITH TYPE 1 DIABETESMELLITUS: COULD FLAVANOIDS HELP?
Chennasamudram S, Singh R, Vasylyeva T. Texas Tech University HealthSciences Center, Amarillo, TX.Purpose of Study: Diabetes mellitus (DM) is a chronic metabolic disor-der characterized by persistent hyperglycemia followed years later by micro-and macro-vascular complications. Endothelium is responsible for the controlof vasoconstriction and vasodilation. Endothelial dysfunction often leads todiabetes related vascular complications. Natural food supplements with anti-inflammatory and antioxidant activities, such as flavanoids, may have a pos-itive impact on endothelial function.
The goal of the study was to study the effects of flavanoids on endothe-lial function and inflammatory markers in adolescents with type 1 DM.Methods Used: A total of 12 DM patients between the ages of 12- 21 yearswere enrolled in the study. The protocol was approved by the local TTUHSCInstitution Review Board. Before the beginning of the study, informed con-sents and assents were obtained. Patients were given flavanoid rich supple-ment capsules twice a day for 14 days. Before the beginning and end oftreatment, a non-invasive measurement of endothelial function was used for
Table 1. Baseline patient characteristics
Continuous variables are mean T SD or median (Q1, Q3)
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 459
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

each subject using an Endo-Pat 2000 device, to measure the reactive hy-peremia index (RHI). Also, urine was collected from the subjects before andafter treatment to analyze inflammatory markers such as tumor necrosisfactor-alpha (TNF->) and interleukin-6 (IL-6).Summary of Results: The average RHI before treatment was 1.30T0.09and significantly increased to 1.57T0.12 (p=0.036) after treatment.The con-centration of TNF- > before and after treatment was 1.65T0.24 pg/mL and0.94T0.1 pg/mL respectively (p=0.05). Also, after flavanoid treatment, theconcentration of IL6 in urine significantly decreased from 0.5T0.1 pg/mL to0.29T0.04 (p=0.049).Conclusions: Flavanoid rich food supplement has significant impact onmicrovascularity in adolescents with type 1 DM, which is characterized byimprovement in flow mediated dilation. The effect most likely links to de-crease of low grade chronic inflammation and might have long-term effect ontheir cardiovascular health.
309
INCIDENCE AND SEVERITYOF CATION DYSHOMEOSTASISON ADMISSION TO TRAUMA UNITS: ACUTE BODILY VS.CLOSED HEAD INJURIES
Yusuf J, Weber KT. University of Tennessee Health Science Center,Memphis, TN.Purpose of Study: A hyperadrenergic state accompanies bodily injury.Elevations in circulating catecholamines induce a rapid translocation ofcations from the circulation into intracellular compartment of skeletal mus-cle and adipose tissue, to account for the acute appearance of hypokalemiaand hypomagnesemia and increased propensity for cardiac arrhythmias. Theextents to which epinephrine and norepinephrine rise in response to injurydepend on its nature and severity. We hypothesized the hyperadrenergic re-sponse to closed head injury will be larger than seen with acute bodily injury,and hence the incidence and severity of the dyshomeostasis of these cationson admission will be greater.Methods Used: A retrospective analysis of serum K+ and Mg2+ at the timeof hospitalization in 468 consecutive admissions (43.2T0.7 yrs; 349 men)to our Trauma Center at the Regional Medical Center in Memphis during2008-10 with acute bodily injury. 167 of these cases involved traumatic andatraumatic closed head injury (47.9T1.2 yrs; 122 men). Hypokalemia (mmol/L)was graded as mild (3.9-3.5), moderate (3.4-3.0) or severe (G3.0) and hy-pomagnesemia (mg/dL) as mild (1.9-1.8), moderate 1.7-1.6) or severe (G1.6),respectively.Summary of Results: Serum K+ on admission for the 468 patients was3.55T0.02 mmol/L with 78% having hypokalemia of mild, moderate andmarked severity in 46%, 33% and 7%, respectively, while hyperkalemia(95.0 mmol/L) was seen in 1%. Serum Mg2+ was 1.94T0.01 mg/dL) withhypomagnesemia of mild, moderate and marked severity seen in 23%, 19%and 10%, respectively. In patients with closed head injury serum K+ was3.35T0.03 (vs. 3.65T0.44 mmol/L with acute bodily injury) and was of mild,moderate and marked severity in 44%, 42% and 14%, respectively; and serumMg2+ was 1.89T0.03 mg/dL, with 24%, 18% and 15% having hypomagnese-mia of mild, moderate and marked severity. Compared to acute bodily injury,the overall severity and incidence of hypokalemia (vis-a-vis hypomagnese-mia) was greater with closed head injury.Conclusions: A majority of patients hospitalized with either acute bodily orclosed head injuries will present with hypokalemia and hypomagnesemia onadmission, but the incidence and severity of hypokalemia will be greater inthose with closed head injury.
310
STRESS-INDUCED (TAKOTSUBO) CARDIOMYOPATHY:CATION DYSHOMEOSTASIS, PROLONGED MYOCARDIALREPOLARIZATION WITH CARDIAC ARRHYTHMIAS ANDNECROSIS
Khalid H, Khan MU, Weber KT. University of Tennessee Health ScienceCenter, Memphis, TN.Purpose of Study: Stress-induced cardiomyopathy, also called takotsubocardiomyopathy (TTC), is a disorder characterized by transient systolic dys-function of the apical segment of the left ventricle that mimics myocardialinfarction (MI), but in the absence of obstructive coronary artery disease.
Although an exact pathophysiologic mechanism of TTC is unknown, it issuggested that myocardial stunning induced by elevated plasma catechola-mines is involved. This hyperadrenergic state promotes the translocation ofcirculating cations into soft tissues. The resultant dyshomeostasis of extra-and intracellular cations is accompanied by delayed myocardial repolarization,QTc interval prolongation on the ECG, a greater propensity for atrial andventricular arrhythmias, and nonischemic cardiomyocyte necrosis. We stud-ied serum electrolytes and troponin-I (trop-I), QTc, and the appearance ofarrhythmias in patients hospitalized with TTC.Methods Used: A retrospective chart review of 20 women (57T3 yrs)whowere admitted and diagnosed with TTC (Mayo Clinic diagnostic criteria)since July 2008. Echocardiographic and cardiac catheterization findings, totalserum [Ca2+] and ionized [Ca2+]o, K
+, Mg2+, and trop-I, together with QTc(ms) and cardiac rhythm, obtained within 0-72 h of admission, were noted.Summary of Results: We found 18 patients had apical while 2 had mid-LVhypokinesis with mean left ventricular ejection fraction 38T2 %; hypocalcemiain 80% and ionized hypocalcemia in 83%; K+ G4.0 in 95% and in 75% it wasG3.6; and Mg2+ G2.0 in 72% and G1.8 in 55%. Prolonged QTc (9440 ms) in90% when K+ was either G4.0, Mg2+ G2.0, and/or hypocalcemia was present.New-onset arrhythmias in 60% when QTc was prolonged and 2 patients diedof ventricular arrhythmias. Nonischemic cardiomyocyte necrosis accountedfor elevated trop-I (2.3T0.5 ng/mL; normal G0.04 ng/mL).Conclusions: A hyperadrenergic acute stressor state seen in TTC is ac-companied by a dyshomeostasis of extracellular cations and QTc prolongationwith a predisposition to arrhythmias and nonischemic myocardial necrosis.Serial surveillance and maintenance of QTc and cations within strictly de-fined normal limits is recommended to avoid arrhythmias.
311
EARLY LIFE STRESS DECREASES DIASTOLIC FUNCTIONIN ANGIOTENSIN II SENSITIZED RATS
Bazacliu C1,2, Loria AS2, Murdison KA1, Pollock JS.2 1GHSU, Augusta, GAand 2GHSU, Augusta, GA.Purpose of Study: To test the hypothesis that early life stress (ELS) inducesang II-mediated diastolic dysfunction in adult male rats.Methods Used: Maternal separation (MS) is a model of ELS in rodents.Male pups of Wistar-Kyoto rats were separated from the mother 3h/day (post-natal days 2-14). The control littermates were left undisturbed. All pups wereweaned on day 28. Diastolic and systolic function was assessed by cardiacultrasound on anesthetized rats. Diastolic function was evaluated by the early(E) and late (atrial - A) ventricular filling velocity (E/A) ratio. Systolicfunction was evaluated as ejection fraction (EF). Rats were implanted withosmotic mini-pumps that delivered ang II at 150 ng/kg/min for 14 days.Echocardiogram was performed prior to ang II infusion (baseline), after day13 of chronic ang II infusion, then 8 and 24 weeks post-ang II infusion in4 control and 6 MS rats.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
460 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: In the control group, the E/A ratio decreased grad-ually with advancing in age, but no significant decrease in response to ang IIinfusion was observed. In the MS group, the E/A ratio decreased significantlyduring the ang II infusion (PG0.05) and remained low, but stable 8 and24 weeks post treatment (figure). EF was unchanged by ang II treatment in bothcontrol and MS group.Conclusions: ELS decreased diastolic function in response to chronic angII infusion earliy in life in male rats.
312
REGULATION OF NATRIURETIC PEPTIDE RECEPTOR-AGENE TRANSCRIPTION BY HISTONE DEACETYLASEINHIBITORS IN MOUSE MESANGIAL CELLS
Neerukonda S, Kumar P, Nguyen V, Pandey KN. Tulane University HealthSciences Center, New Orleans, LA.Purpose of Study: Activation of guanylyl-cyclase/natriuretic peptide re-ceptor-A (GC-A/NPRA) by cardiac hormones atrial and brain natriureticpeptides (ANP and BNP) produces the second messenger cGMP, which ac-tivates downstream signaling and biological effects of ANP/NPRA includingvasorelaxation, antimitogenic responses, and cardiac anti-hypertrophic ef-fects. Npr1 gene (coding for GC-A/NPRA) expression is regulated by anumber of external and internal stimuli, but the molecular mechanism me-diating Npr1 gene regulation and expression is not well understood. Theobjective of this present study is to determine the epigenetic regulation ofthe Npr1 gene transcription involving histone deacetylase (HDAC) inhibitorstrichostatin A (TSA) and MGCD0103 in mouse mesangial cells (MMCs).Methods Used: Cells were cultured in Dulbecco’s modified Eagles medium(DMEM) containing 10% fetal bovine serum and ITS (insulin, transferrin,and sodium selenite) and maintained at 37-C in an atmosphere of 5% CO2/95% O2. Cells were transiently transfected using Lipofectamine-2000 andincubated with increasing concentrations of class 1 and class 2 HDAC inhi-bitors. Western blot analysis was performed to determine the effect ofHDAC-inhibitors on histone H3 and H4 acetylation levels in isolated histonesof inhibitor treated cells.Summary of Results: The results showed that broad-spectrum histone de-acetylase inhibitor trichostatin A (TSA) and class I HDAC inhibitor MGCD0103significantly increased Npr1 promoter activity. Both TSA and MGCD0103significantly induced the mRNA levels of NPRA in MMCs. TSA andMGCD0103 enhanced the protein levels of acetylated histones H3 at lysineresidues 9 and 14 and H4 at lysine residue 12. On the other hand, over-expression of class I HDACs (HDAC1 and HDAC2) significantly inhibitedNpr1 gene expression.Conclusions: Collectively, our results demonstrate that class I HDAC in-hibitors affect Npr1 gene transcription and expression by enhanced histoneacetylation.
313
REGULATORY ACTION OF ALL-TRANS RETINOIC ACIDAND SODIUM BUTYRATE IN THE MODULATION OFCARDIAC REMODELING IN GUANYLYL CYCLASE/NATRIURETIC PEPTIDE RECEPTOR-AGENE TARGETEDMICE
Subramanian U, Kumar P, Mani I, Pandey KN. Tulane University, NewOrleans, LA.Purpose of Study: Mice carrying targeted-disruption of guanylyl cyclase/natriuretic peptide receptor-A (GC-A/NPRA) gene (Npr1) demonstrate in-creased blood pressure, cardiac hypertrophy, and congestive heart failure, similarto untreated human hypertensive patients. The objective of this study was todetermine whether Npr1 gene-knockout mice treated with all-trans retinoicacid (RA) and sodium butyrate (NB) show altered expression of cardiachypertrophic markers.Methods Used: In the present study, Npr1 +/- heterozygous mutant (1-copy) mice were treated with RA (0.5 mg/kg/day) and NB (0.5 mg/kg/day)for 14 days and the heart tissues were isolated and used for real-time quan-titative reverse transcription-polymerase chain reaction (qRT-PCR) andWestern blot analyses. Together, systolic blood pressure (SBP), heart weight-to-body weight (HW/BW) ratio, left ventricular end-diastolic dimension(LVEDD), left ventricular end-systolic dimension (LVEDS), and percentfractional shortening (FS) were analyzed.
Summary of Results: The results showed that Npr1 +/- mice treated withRA and NB showed significant attenuation in the expression of hypertrophicmarkers such as A-myosin heavy chain (A-MHC, 5-fold; pG0.001), >-skeletalactin (>-SK, 4-fold; pG0.001) and >-smooth muscle actin (>-SMA, 4-fold;pG0.001) compared with untreated control Npr1 +/- mice. In addition,treatment with RA and NB effectively down-regulated the expression ofproto-oncogenes (c-fos, 5-fold; c-jun, 3-fold) in Npr1 gene knockout micecompared to untreated control Npr1 +/- and age matched wild type ani-mals. Npr1 +/- mice treated with the hybrid drug (RA + NB) showed thenear normal SBP, HW/BW ratio, LVEDD, LVEDS and %FS values.Conclusions: The results of the present study suggest that treatment ofNpr1 +/- mice with RA and NB inhibits the development of cardiac hyper-trophy and remodeling process.
314
INSULIN-LIKE GROWTH FACTOR INCREASESCOLLAGEN-1> AND CONTRACTILE PROTEIN EXPRESSIONIN VASCULAR SMOOTH MUSCLE: MECHANISMSOF ATHEROSCLEROTIC PLAQUE STABILIZATION
Blackstock C, Higashi Y, Sukhanov S, Delafontaine P. Tulane UniversitySchool of Medicine, New Orleans, LA.Purpose of Study: To determine mechanisms responsible for our previousfindings in which IGF-1-infusion in Apoe-/- mice caused increased expressionof collagen and contractile smooth muscle phenotype within atheroscleroticplaque.Methods Used: Human aortic smooth muscle cells (HASMCs) were cul-tured ex-vivo and exposed to 0-100ng/mL IGF-1 in presence of various sig-naling-inhibitors. Time-course gene expression was determined by real timeRT-PCR and protein expression by western blot. Collagen synthesis was de-termined by 3H-proline incorporation. siRNAwas transfected via electroporation.Summary of Results: IGF-1 induced a dose-dependent increase in ex-pression of procollagen-1> (È2.4-fold with 100ng/mL IGF-1, pG0.001,n=10) and SMC contractile proteins, alpha-actin (>SMA) and SM22> (È2-fold, pG0.01, n=8). IGF-1 did not alter Col1a1, Col1a2, >SMA, or SM22>mRNA expression, and IGF-1 upregulation of procollagen-1>, >SMA, orSM22> was not blocked by actinomycin D, indicating a posttranscriptionalmechanism. Cycloheximide completely abrogated the IGF-1-induced expres-sion of procollagen-1> and >SMA, indicative of a translation-dependentmechanism. PI3K-inhibitor (LY2940032) prevented the IGF-1-induced ex-pression of procollagen-1>, >SMA, and SM22>, while an Erk1/2-inhibitor(PD98059), and rapamycin, an inhibitor of mTOR, had no effect.
Remarkably, IGF-1 caused a rapid increase in the rate of collagen syn-thesis (2.2-fold increase at 2 hours, pG0.0001, n=6). A novel mRNA bindingprotein, LARP6, binds to the 5’UTR of Col1a1 and Col1a2 and coordinatescollagen assembly. Here we show that IGF-1 increases protein expression ofLARP6 and knockdown of LARP6 via targeted siRNA causes a reduction inprocollagen-1>, both basally and in presence of IGF-1.Conclusions: IGF-1 induces collagen-1>, >SMA, and SM22> protein ex-pression via a PI3K-mediated, but mTOR-independent, translational mech-anism. Furthermore, IGF-1 induces a rapid increase in the rate of collagensynthesis and the expression of collagen-1> is mediated via LARP6. Thesefindings provide new insights into mechanisms whereby IGF-1 induces VSMCdifferentiation and collagen expression, thus supporting IGF-1 to offer a pro-tective role from plaque rupture in atherosclerosis.
315
ABNORMAL CHEST X-RAYAS A PREDICTOR OF HOSPITALSTAY INRIGHT-SIDED INFECTIVEENDOCARDITISPATIENTS
Sutamtewagul G, Mankongpaisarnrung C, Dumrongmongcolgul N,Nantsupawat T, Nugent K. Texas Tech University Health Science Center,Lubbock, TX.Purpose of Study: To collect demographic data, hospital course of right-sided infective endocarditis (IE) patient, to identify its relationship with echo-cardiographic findings compatible with pulmonary hypertension (PHT), andto determine if PHT contributes to poorer clinical outcome.Methods Used: We performed a retrospective review of the patient data-base from University Medical Center from October 2000 to September 2011.We reviewed medical records with diagnosis of IE for demographic parameters,
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 461
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

hospital course, treatment, chest X-ray (CXR) findings, and echocardio-graphic parameters. Frequency tables with cross-tabulation were used toanalyze data. LOS and pulmonary artery systolic pressure (PASP) were com-pared between groups by t-test or equivalent nonparametric method.Summary of Results: Nineteen medical records were retrieved; 8 cases(42.1%) were male. Most patients were Caucasian (72%). Median age was39 years. Most patients had histories of IVDU (73.7%). Two had history ofprosthetic valve placement. They presented with fever (55.6%), dyspnea (55.6%),cough (27.8%) and chest pain (22.2%). CXR was abnormal in 77.8% ofcases. Parenchymal involvement was found in 72.2%; cardiomegaly and rightpleural effusion were found in 22.2% and 10.5%, respectively. Tricuspidvalve was affected (100%). Size of vegetation was large in 62.5%. 12 hadpositive blood cultures; MSSA is the most prevalent organism (58.3%).Patients were treated empirically with vancomycin (68.4%) and gentamicin(52.6%). Surgical treatment was needed 31.6%. One (5.6%) died. Mean LOSwas 12 days (range 3-51 days). We found no significant association betweenPASP and LOS and between PASP and mortality, neither culture positivityand PASP or LOS. Also, we found no association between type of micro-organism and LOS/PASP. However, there is a significant association betweenabnormal CXR and LOS (Mann-Whitney U test p=0.008).Conclusions: Right-sided IE is usually caused by septicemia, mostly fromIVDU. Prognostic factors include microorganism and size of vegetation.Although PHT, which may be a consequence of right-sided IE or from IVDU,can influence the outcome, we found no association between PASP andclinical outcomes. However, abnormal CXR was significantly associatedwith LOS in this group.
Gastroenterology IConcurrent Session
2:00 PMFriday, February 22, 2013316
RESPONSE TO VITAMIN E FOR NON-ALCOHOLICSTEATOHEPATITIS (NASH): WHAT IS THE MECHANISM?
Cheng J1, Joyce A2, Yates K3, Sanyal A1. 1Virginia CommonwealthUniversity, Glen Allen, VA;2Venebio Group, LLC, Richmond, VA and3JohnsHopkins University, Baltimore, MD.Purpose of Study: The PIVENS (Pioglitazone versus Vitamin E versusPlacebo for the Treatment of Nondiabetic Patients with Nonalcoholic Steato-hepatitis (NASH)) trial demonstrated that Vitamin E improved NASH in 43%of the treated subjects. The mechanisms for the histological improvementare unknown. Elucidation of this mechanism will aid in understanding whyonly some subjects respond to vitamin E.Methods Used: Available excess liver tissues from baseline and end of treat-ment biopsies were analyzed from two sets of subjects enrolled in the PIVENStrial: (1) vitamin E responders (Vit.E R, n=12), (2) vitamin E non-responders(Vit.E NR, n=12). Among them, 8 subjects had paired baseline and post treat-ment tissue (3 Vit.E R and 5 Vit.E NR). Response was defined as meeting theprimary histological end-point of the trial. Pathway focused real time polymerasechain reaction (RT-PCR) arrays were used to investigate expression changes inoxidative stress and antioxidant defense and fatty acid metabolism genes.Summary of Results: Analysis of the limited set of subjects with paireddata revealed that GPX5 (glutathione peroxidase 5) expression was signifi-cantly down-regulated in vitamin E responders relative to vitamin E non-responders (Fold change (FC) =0.04, p=0.01). Analysis of post treatment data(8 Vit.E R, 6 Vit.E NR), identified 7 genes from oxidative stress and anti-oxidant defense pathway with significant differential expression. DGKK,DUOX2, GPX6, LPO, NOS2, PRG3, and TPO were all significantly down-regulated in vitamin E responders relative to vitamin E non-responders. Neitherset of analyses revealed significant changes in the fatty acid metabolism genesthat were investigated.Conclusions: Down regulation of a select number of oxidative stress andantioxidant defense genes is associated with histologic improvement fol-lowing vitamin E treatment for NASH in PIVENS subjects. Interestingly,none of the investigated fatty acid metabolism genes appear to be associatedwith histologic improvement. These findings are consistent with previouslyconducted metabolomics profiles analysis with both analyses suggesting thathistologic improvement is related to decreased glutathione turnover and ox-idative stress.
317
FUNCTIONAL GASTROINTESTINAL DISORDERSDOMINATE PEDIATRIC GASTROENTEROLOGYOUTPATIENT PRACTICE
Rouster A1,2, Silver D2,1, Tomb L2,1, Rosenblum H2,1, Hyman P1,2. 1LSU,New Orleans, LA and 2Children’s Hospital, New Orleans, LA.Purpose of Study: Symptom-based diagnostic criteria have improved rec-ognition and standardization of pediatric functional gastrointestinal disorders(FGIDs). We used Rome diagnostic criteria to determine the ratio of FGIDsto organic disease in outpatients.Methods Used: We enrolled all new patients e18y referred to pediatricGI clinic over 3 mo. Subjects or parents completed a demographic surveyand a validated Rome Diagnostic Questionnaire (QPGS-RIII for children Q4years or a new infant-toddler questionnaire) before visiting with a clinician.We recorded the chief complaint and clinician’s diagnosis following the visit.Summary of Results: We acquired data from 203 subjects (93 male), 117subjects Q4y, 86 subjects G4y, 112 white, 62 African American and 10 Latino.There was no significant difference in frequency of FGIDs among racialgroups. Of those Q4 years old, 61 (52%) met criteria for a FGID on thequestionnaire. Of those G4 y, 37 (43%) met criteria for a FGID. Twenty-three(20%) of older children and 7 (8%) of infants and toddlers met criteria for2 FGIDs. Common FGIDs included: IBS (27%), functional constipation (17%),abdominal migraine (10%), functional dyspepsia (5%), infant regurgitation(4%), functional abdominal pain syndrome (3%). Of 14 infants referred for chiefcomplaints of ‘‘reflux’’ ‘‘vomiting’’ or ‘‘spitting up’’, 10 infants met symptom-based criteria for infant regurgitation, 2 for infant dyschezia, 3 with cyclic vom-iting, and 1 with functional constipation on the questionnaire. Clinicians didnot diagnose gastroesophageal reflux disease in any of these infants. In 54of 98 children meeting symptom-based criteria there was concordance be-tween clinician and questionnaire diagnosis.Conclusions: Close to half of the new patients to pediatric GI clinic metsymptom-based diagnostic criteria for one or more FGIDs. Satisfyingsymptom-based diagnostic criteria may facilitate diagnosis on the first visit.
318
DYSMOTILITY AND FEEDING MANAGEMENT IN INFANTSWITH GASTROSCHISIS WITH AND WITHOUT SHORTBOWEL SYNDROME
Vashishtha N, Connelly R, Crissinger K. University of South Alabama,Mobile, AL.Purpose of Study: To compare the outcomes of dysmotility and shortbowel syndrome (SBS) in infants with gastroschisis on time to first feed, timeto attain full feeds, and length of hospital stay (LOS), and to evaluate erythro-mycin as a prokinetic agent for feeding intolerance in infants with gastroschisis.Methods Used: Retrospective chart review from 2005 to 2012 of babieswith gastroschisis born at the University of South Alabama Children’s andWomen’s Hospital. Categorical variables were compared using Chi square andmeans between groups were compared using paired t-test.Summary of Results: A total of 63 patient charts were reviewed with 56%male, 75% Caucasian, 19% African American, and 6% other. Overall, 42%of infants were first born and 95% of mothers were younger than 24 years.In all, 27% of babies had dysmotility and 23% developed SBS. Infants withSBS had significantly higher mean number of days to first feed, time to fullfeeds, and LOS than non-SBS with 39 vs 16 (p=0.002, SD 20.3, 95% CI 15-27.4 ), 83 vs 29 (pG0.001, SD 30, 95% CI 44-59.1), and 115 vs 33 (p G0.001,SD 51, 95% CI 36.5-64.3), respectively. Infants with dysmotility had sig-nificantly higher mean number of days to first feed, time to full feeds, andLOS than no dysmotility with 34 vs 16 (p=0.006, SD 20.1, 95% CI 14.8-27 ),50.1 vs 25.7 (p=0.004, SD 26.1, 95% CI 21.3-30.5), and 95 vs. 31 (p G0.001,SD 49.5, 95% CI 35.7 - 61.7), respectively. Out of 16 infants who haddysmotility, erythromycin (15 mg/kg/dose TID) was used in 9 infants andimprovement in symptoms was noted in all of these patients.Conclusions: SBS and dysmotility increased the time to first feed, time tofull feeds, and LOS. While more prokinetics were used in infants with SBS,many infants without SBS still suffered from dysmotility. Erythromycin (15mg/kg/dose TID) appears to have some benefit for treatment of dysmotility ininfants with gastroschisis, but larger numbers of patients are necessary toconfirm this result.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
462 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

319
PENTASA FOR TREATMENT OF INFANTS WITHPERSISTENT BIOPSY-PROVEN PROCTOCOLITISCONSISTENT WITH MILK PROTEIN INTOLERANCEDESPITE 100% AMINO ACID-BASED FORMULA FEEDING
Alwazeer M, Crissinger KD. University of South Alabama, Mobile, AL.Purpose of Study: Evaluate the outcome of Pentasa treatment for procto-colitis due to MPI refractory to treatment with Amino Acid-Based formula ininfants G12 months of age.Methods Used: Retrospective chart review.Summary of Results: Twenty-two patients were identified with 64% fe-male and 72% Caucasian. Symptoms were excessive irritability, vomiting,choking/gagging, coughing/wheezing, gassiness, watery or hard stools, vis-ible mucus/blood in stool, weight loss, skin rash, and sleeping difficulties.Fecal occult blood was present in 73% before the use of AAF. Before EGD &flexible sigmoidoscopy, 68% of patients were on AAF while 32% were on acasein-hydrolysate formula. There was no statistically significant improve-ment in symptoms on AAF. Stool hemoccult was positive in 64% after usingAAF (p=0.5). Before Pentasa treatment, 82% of patients were treated withAAF for G1 months. When Pentasa was started, 77% were between ages 12-6 months and 23% were between 6-10 months. Statistically significant im-provements in vomiting, visible mucus in stool, watery stool, excessive ir-ritability, choking, gagging, gassiness, and weight loss were seen with Pentasa.Stool hemoccult was negative in all patients after starting Pentasa (p=G0.001).Pentasa was used for 12-4 months in 50% and 4-10 months in 46%. Onepatient did not return for follow-up. There were no patients with recurrentsymptoms after stopping Pentasa and no side effects were noted during Pentasatreatment.Conclusions: Short-term treatment with Pentasa for refractory proctocoli-tis due to MPI in infants G12 months appears to be effective based on thisretrospective chart review, but a prospective study with a larger patient popu-lation is necessary to confirm these preliminary results.
320
PREDICTORS OF EARLY TREATMENT FORHEPATOCELLULAR CARCINOMA
Cahill M1, Burke J1, Jafarimehr E1, Farooq S1, Weir A2,1, Tombazzi C2,1,Waters B2,1. 1University of Tennessee Health Science Center, Memphis, TNand 2Memphis Veteran Affairs Medical Center, Memphis, TN.Purpose of Study: Hepatocellular carcinoma (HCC) is a growing burdenworldwide. Curative treatments are available and effective if employed whenlesions are small and not metastatic. Many HCC patients do not receive earlytreatment. We aim to elucidate the patient-specific and tumor-specific fac-tors that predict early treatment for HCC.Methods Used: After obtaining institutional review board approval, we per-formed a retrospective chart review of all patients with HCC referred to theMemphis Veteran Affairs Medical Center (VAMC) multi-specialty liver tu-mor board. We defined early treatment as treatment that occurred within90 days of HCC detection. For statistical analysis, we performed univari-ate analysis with Chi-Square test and T test, and multivariate analysis withlogistic regression.Summary of Results: 103 patients with HCC were referred to the livertumor board from March 2003 through January 2012. 102 (99%) were male,54 (52%) were Caucasian, 49 (48%) were African American, the median ageat diagnosis was 61 (range 44-88), and 59 (57%) are now deceased. The me-dian MELD score at diagnosis was 8 (range 6-27). 43 patients (42%) receivedtheir first HCC treatment within 90 days of HCC detection. The median timefrom HCC detection to first treatment was 120 days. On univariate analy-sis, factors that predicted early treatment include patients who are unmarried(p=0.015), have hepatitis C (p=0.041), and have more than one lesion(p=0.0001). Additional factors predicting early treatment include higher AFP(p=0.01), higher INR (p=0.02), higher MELD-Na score (p=0.03), and loweralbumin (p=0.009). On multivariate analysis, only tumor number predictedearly treatment (p=0.003), though marital status, disability Q50%, high AFP,and high INR trended toward significance.Conclusions: We identified several factors that predict early treatment forHCC. Identification of patients who do not have these favorable character-
istics should prompt the healthcare delivery system to provide them withadditional resources designed to facilitate early treatment.
321
CHRONIC TRANSCUTANEOUS ELECTROACUPUNCTUREAMELIORATES DYSPEPTIC SYMPTOMS IN PATIENTSWITHDIABETIC GASTROPARESIS
McCallum R2, Chen J1,4, Sarosiek I2, Abell T3, Sun Y4, Chen J4, Yin J.11Division of Gastroenterology, University of Texas Medical Branch,Galveston, TX; 2Texas Tech University Health Sciences Center, El Paso,TX; 3University of Mississippi, Jackson, MS and4Transtimulation ResearchInc., Oklahoma City, OK.Purpose of Study: The aims of this project were 1) to develop a novelmethod of transcutaneous electroacupuncture (TEA) using a custom-madewireless microstimulator and to assess the efficacy of chronic TEA in treatingdyspeptic symptoms in diabetic gastroparesis (DM-GP) patients.Methods Used: 26 pts DM-GP were enrolled and 18 of them (50.4T10.8 yrs, 5M, 13F) completed the study. In a crossover design, each pt wasblindly treated at home with 4-week TEA and 4-week sham-TEA in a ran-domized order. TEA was performed via surface ECG electrodes placed atacupoints PC6 and ST36 using pulse trains: train on of 2s and off of 3s,0.5ms, 25Hz and 2-6mA (appropriate and well tolerated). Sham-TEA wasperformed using same parameters via non-acupoints. The pts were asked toself-apply TEA/sham-TEA for 2 hrs after lunch/dinner. The electrogastrogram(EGG) and ECG were recorded during 4 visits (beginning and end of each4-week treatment). Gastroparesis cardinal symptom index (9 questions) andQuality of Life (SF36) were assessed weekly.Summary of Results: 1) Watch-size stimulators allowed the pt to resumedaily activity; 2) Good compliance was noted: the usage of the therapy was300.3T82.5 min/day vs. requested 300min/day. 3) 4-wk TEA significantlyimproved 5 of 9 GP symptoms: nausea by 29.7% (P=0.005 vs. baseline),vomiting by 39.3% (P=0.055), abdominal fullness by 21.4% (P=0.0047),bloating by 20.6% (P=0.006), and retching by 31.1% (p=0.006). A signifi-cant improvement in body pain was also noted with TEA. 4) 4-week TEAincreased % of normal slow waves in both fasting (72.8T14.1% vs. 79.9T13.5%, P=0.05) and fed (69.5T12.1% vs. 77.4T16.5%, P=0.04) states. 5)4-week TEA resulted in a trend of increase in vagal activity in the fed state(P=0.08).Conclusions: TEA therapy is feasible and effective in treating GP symp-toms and mechanisms involving central, gastric and autonomic functionsrequire further elucidation.
322
CECAL DIVERTICULITIS MASQUERADING ASAPPENDICITIS IN A 13 YEAR OLD
Stephenson LR, Thomas W, Sicard C, Bocchini J. LSU Health Shreveport,Shreveport, LA.Case Report: A 13 year old female with no significant past medical his-tory presented to our emergency department complaining of abdominalpain, vomiting, and fever for one days. Her maximum termperature 102.5 F athome. The vomitus was described as non-bilious, and non-bloody. She re-ported poor appetite since the onset of symptoms. The abdominal pain was10/10 at its peaks, localized to the left lower quadrant, and intermittent innature. On exam, she had rebound and guarding, localized to the left lowerquadrant. Lab work in the emergency department revealed a leukocytosiscount of 18,000, with a neutrophil predominance of 95%. Visualization ofthe appendix was unsuccessful with ultrasound; therefore a CT of the ab-domen and pelvis with IV and oral contrast was performed. The CT revaledthickening of the cecal wall and free air surrounding the attachment of theappendix. A perforated appendicitis was diagnosed. The patient was taken tothe OR for laparoscopic appendectomy. At the time of surgery, a normal-appearing appendix was found, along with a large abscess next to the ce-cum covered in omentum. The official CT reading confirmed the presence ofright-sided diverticulitis with abscess. These findings prompted the surgicalteam to perform an ileocecectomy with primary anastomosis. The patientreturned from the OR, and was discharged without adverse event three dayspost-operatively.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 463
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

This case presents an adolescent with an atypical cause of abdomi-nal pain. Cecal diverticulitis is a very rare entity in pediatric populations. Thediagnosis, however, should be considered when a patient presents with ab-dominal pain not typical for that of an appendicitis.
323
RENAL CELL CARCINOMA IN PATIENTSWITH HEPATITIS C
Burke J1, Cahill M1, Waters B2,1. 1University of Tennessee Health ScienceCenter, Memphis, TN and 2Memphis Veteran Affairs Medical Center,Memphis, TN.Purpose of Study: To elucidate an association between renal cell carci-noma (RCC) and hepatitis C virus (HCV).Methods Used: With institutional review board approval, we performed aretrospective chart review of patients diagnosed with RCC at the MemphisVeteran Affairs Medical Center (VAMC) from 2002-2012.Summary of Results: As of 2011, the number of veterans in the US whohave ever had HCV viremia is 170,119. Of all US veterans with HCV viremia,1,250 (0.7%) have ever been diagnosed with RCC. At the Memphis VAMC,there have been 180 biopsy-proven diagnoses of RCC from 2002-2012. Ofthese patients, 140 (78%) have been tested for HCV infection. Among thosetested for HCV infection, 27 (19%) had antibody seropositivity. Among the27 HCV seropositive patients, 19 (70%) were viremic, 5 (19%) had an un-dectable viral load, and 3 (11%) were never tested for HCV viremia. Evenassuming that the 40 RCC patients who were never tested for HCV infectionwere indeed HCV negative, the prevalence of past or current HCV infectionamong RCC patients is 15% (27 of 180 cases). Among the 27 HCV sero-positive patients, the average age at diagnosis of RCC was 57 (range: 45-77),100% were male, 59% were African American, 85% were tobacco abusers,33% were obese, 11% had ESRD requiring hemodialysis prior to RCC diag-nosis, 89% had hypertension, and 30% had diabetes mellitus.Conclusions: Over the last 10 years at the Memphis VAMC, 180 patientshave been diagnosed with RCC. The prevalence of past or current HCVinfection in this RCC population is 15%. This rate is likely an underestimateof the true HCV prevalence given the fact that 22% of the 180 RCC cases hadno prior HCV testing. Even at this conservative estimate, the 15% prevalenceof HCV in the RCC population is far in excess of the HCV prevalence amongthe general VA and US populations, which have been estimated at 6% and2%, respectively. Our data add further support to the emerging associationbetween HCVand RCC and herald a need for additional research examiningthis link.
324
MANAGEMENT OF CHOLEDOCHOLITHIASIS INPREGNANCY
Gendusa P, Martinez I, Reiss GM, Landreneau SW. LSU Health SciencesCenter, New Orleans, LA.Case Report: Case: A 36 year old African American woman presented withcomplaints of painless jaundice and pale stools for one week. At presenta-tion, she was afebrile with normal vital signs with mild scleral icterus and anormal abdominal exam. Initial laboratory data was significant only for el-evation of transaminases, alkaline phosphatase, and bilirubin. Abdominalultrasound and MRCP demonstrated cholelithiasis and choledocholithiasiswith a common bile duct of 9mm in diameter and associated intrahepaticbiliary dilation. Numerous biliary stones were removed from the common bileduct by ERCP after sphincterotomy and a stent was placed due to incom-plete stone extraction. Laparoscopic cholecystectomy was performed two dayslater, and pathology was consistent with chronic cholecystitis. Three weeksfollowing discharge, she presented for ERCP for stone and stent removal andwas found to have a positive pregnancy test. The procedure was postponed,and obstetric evaluation confirmed a six week intrauterine pregnancy pre-senting a dilemma of when to treat her now asymptomatic choledocholithiasis.After extensive multidisciplinary discussions occurred with the patient detail-ing the various endoscopic treatment options and conservative management,the decision was made to proceed with an ERCP with choledochoscopy usingSpyGlass Direct Visualization System (Boston Scientific, Natick, MA, USA)during the second trimester to avoid fluoroscopy.
Disscussion: Choledocholithiasis in pregnancy can be managed in mul-tiple ways including no intervention or with ERCP. Techniques to minimize
radiation exposure to the fetus include ERCP with lead covering the pel-vis, ERCP without fluoroscopy performed after first aspirating bile from thecommon bile duct followed by sphincterotomy, and the use of endoscopicphotographs instead of spot radiography. ERCP can then be followed byelective cholecystectomy preferably after the first trimester to decrease riskof spontaneous abortion or birth defects in the fetus. Additional techniqueswhich can reduce radiation exposure time include the use of balloon cathetersafter sphincterotomy, endoscopic ultrasound and choledochoscopy duringERCP. This is the 9th case report of choledochoscopy use during pregnancy.
325
SECONDARY HEMOPHAGOCYTICLYMPHOHISTIOCYTOSIS MASQUERADING AS BILIARYPANCREATITIS: A RARE DIAGNOSTIC DILEMMA &LESSONS FOR THE UNWARY
Bilal M, Nair S. UTHSC, Memphis, TN.Case Report: Hemophagocytic lymphohistiocytosis (HLH) in adults is anelusive and life-threatening condition (mortality approaching 50%) associ-ated with multiple organ dysfunction. A 34-year-old black female with SLEwas admitted for persistent high grade fever. She had been taking 800 mgof ibuprofen on daily basis for the past 3 months for joint aches and pains.Her examination was significant only for a fever of 103F. Initial laboratorywork up showed pancytopenia, total bilirubin of 1 mg/dl, alkaline phos-phatase of 647 unit/L, AST of 461 unit/L, ALT of 181 unit/L and lipase of2000 unit/L. CT abdomen was negative and ultrasound only showed gall bladdersludge. Further work up showed a serum ferritin of 9 40,000 ng/ml, stronglypositive ANA but negative anti-smooth muscle antibody, elevated triglycerideof 600 mg/dl, low haptoglobin and elevated lactate dehydrogenase. Hemo-chromatosis gene mutation testing and CMV/EBV PCR were negative. Bonemarrow biopsy was negative although specimen was inadequate. Subse-quently patient developed acute cardiac decompensation with elevated tro-ponins upto 7 ng/ml and EF of 20% with negative cardiac stress test. She wasdiagnosed with HLH and started on IV immunoglobulins, IV steroids andcellcept. She recovered completely over the course of next 2 weeks with repeatechocardiogram showing an EF of 60%. This was a unique case which pre-sented as a diagnostic challenge with differentials including biliary pancre-atitis, lupoid hepatitis, autoimmune hepatitis, NSAID induced liver/pancreaticinjury or systemic illness. We believe her subclinical pancreatitis was a con-sequence of hemolysis. Additionally patient developed acute heart failurewhich has never been reported as a complication of HLH. Recent studiesshow a clear role of chemokines in patients with severe heart failure whichcould link the two diagnoses. This case calls for prompt precognition andtreatment of this potentially fatal condition.
Hematology and Oncology IConcurrent Session
2:00 PMFriday, February 22, 2013326
DISCOVERY OF NOVEL FETAL HEMOGLOBIN INDUCINGDRUGS TO TREAT SICKLE CELL DISEASE
Okonkwo AI1, Li B1, Takezaki M1, Arbiser JL2, Pace BS1. 1Georgia HealthSciences University, Augusta, GA and 2Emory University School of Medicine,Atlanta, GA.Purpose of Study: The purpose of this study was to determine the abilityof the pharmacologic compound Honokiol and its analog, Hexafluoro, toinduce fetal hemoglobin (HbF).Methods Used: The KU812-FF/AR dual reporter stable cell line was createdwith a construct comprised of the A-globin promoter linked to the Renillaluciferase gene and the F-globin promoter driving the Firefly luciferase genewith the G418 selectable marker. Cells were treated for 48 hr with Honokiol(20 and 40KM) and Hexafluoro (30, 40, and 60KM). Firefly and Renillaluciferase activity was measured using the Dual-Glo\ Luciferase Assay Kit(Promega, Madison, WI); total protein was measured by Bradford assay andused for data normalization. HbF induction was evaluated using the F/F+Aratio compared to untreated controls.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
464 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: The KU812-FF/AR dual reporter stable cell line wascreated with a construct comprised of the A-globin promoter linked to theRenilla luciferase gene and the F-globin promoter driving the Firefly lucif-erase gene with the G418 selectable marker. Cells were treated for 48 hr withHonokiol (20 and 40KM) and Hexafluoro (30, 40, and 60KM). Firefly andRenilla luciferase activity was measured using the Dual-Glo\ LuciferaseAssay Kit (Promega, Madison, WI); total protein was measured by Bradfordassay and used for data normalization. HbF induction was evaluated using theF/F+A ratio compared to untreated controls.Conclusions: Our data demonstrated Honokiol and Hexafluoro to be HbFinducers at micromolar concentrations thus supporting both compounds aspotential therapeutic agents for the treatment of sickle cell disease.
327
LUNG DYSFUNCTION IN PATIENTS WITH SICKLE CELLDISEASE: A RETROSPECTIVE CHART REVIEW
Almannai M, Wislon F, Howell D, Connelly R. University of South AlabamaChildren’s & Women’s Hospital, Mobile, AL.Purpose of Study: 1. To describe the types of lung dysfunction in patientswith Sickle cell Disease
2. To describe the trend of pulmonary function tests over time in differentsubtypes of Sickle cell Disease
3. To evaluate the effect of inhaled steroids and Hydroxyurea on pul-monary function in patients with Sickle cell disease
4. To evaluate the incidence of acute chest syndrome episodes and itseffects on pulmonary function over timeMethods Used: Retrospective chart review of patients with Sickle celldisease aged 8-18 years old in the Sickle Cell Clinic at the University ofSouth Alabama, Mobile, AL.Summary of Results: Pulmonary function tests results were available for99 patients, ranging from 1 to 9 tests per patient. Fifty-eight percent of pa-tients were female, 49% had HbSS disease, 31% had HbS/Beta thalassemia,and the remaining 20% had HbSC disease. Results from initial pulmonaryfunction tests showed that 30% of patients had an obstructive pattern. In 58%of those, the obstruction was irreversible (p=0.002). Mean FVC was 80%predicted (range 45-112, SD=14). Mean FEV1 was 75% predicted, (range 37-108%, SD=16). Mean FEV1/FVC ratio was 83% (range 57-100%, SD=8).Initial PFTs of patients with HbSS disease were compared to patients withother types of Sickle cell disease, and there was no statistically significantdifference between the two groups, neither in percentage of patients who hadan obstructive pattern (p=0.7), nor in the degree of reversibility (p=0.11).Conclusions: Data analysis is still ongoing. Multivariate analysis on thisdata will be performed to study the effects of inhaled steroid use, Hy-droxyurea use, and number of acute chest syndrome episodes on PFTs as wellas the trend of lung function in this group of patients over time. I expect tohave results by February 2013, in time for the SSPR meeting.
328
MERKEL CELL CARCINOMA
Dang P1, Dang N2, Trieu D3. 1Tulane School of Medicine, New Orleans, LA;2Baylor College of Medicine, Houston, TX and 3Tulane School of Medicine,New Orleans, LA.Purpose of Study: Merkel cell carcinoma is a rare primary malignantneuroendocrine carcinoma of the skin. These tumors display highly aggres-sive behavior with non-specific clinical features. In general, it has been foundthat adjuvant radiation therapy associated with improved survival in Merkelcell carcinoma of skin. In this study, we attempted to perform subgroupanalysis to identify patients who may or may not benefit from adjuvant radi-ation treatment.Methods Used: 5520 cases of Merkel cell carcinoma were identified fromthe Surveillance, Epidemiology, and End Results (SEER) Program of theNational Cancer Institute 1973-2009. The JMP 10 statistical software wasused to compare the difference in race, age, sex and tumor characteristics-extension of disease, size, lymph node involvement, surgical therapy type,and location. Estimates of overall survival were performed using the Kaplan-Meier method.
Summary of Results: There were 3375 males and 2145 females includedin this study. Primary site distribution included lips (2.6%), salivary gland(0.6%), external ear (3.4%), orbit or periorbit (2.3%), skin of face non-otherwise-specified (26.6%), skin of scalp and neck (9.5%), trunk (10%),upper extremity and shoulder (22.5%), and lower extremity and hip (14.7%).Overall, patients who received radiation had better survival than those whodid not. The 10-year OS in both sex who received adjuvant radiotherapy ex-ceeded those that did not, 26.3% vs 16.5% in male and 33.7% vs. 27% infemale, respectively. There were better outcome in all extension of disease,tumor size, and lymph nodal involvement that received adjuvant therapy.Conclusions: Adjuvant radiation therapy following surgery showed benefitsto overall survival in the majority of cases. The groups that did not benefitfrom adjuvant radiotherapy include patients G50 year old and tumors that hadinvaded into the underlying bone, cartilage, skeletal muscle. According tothis study, we would recommend radiotherapy for any merkel cell carcinoma,with the exception of deep tissue invasion tumor.
329
INVESTIGATING HEMOSTASIS IN PATIENTS WITH NEWLYDIAGNOSED HEMATOLOGIC MALIGNANCIES USING ATHROMBOELASTOGRAPHY PROTOCOL
Liszewski WJ, Safah H, Leissinger C. Tulane University, New Orleans, LA.Purpose of Study: Hematologic malignancies are associated with an in-creased risk of thrombosis, but there currently are no assays that can identifythe risk of thrombosis in these patients. Thromboelastographic technology hasshown the potential to assess global hemostasis and hypercoagulability in somecircumstances. The purpose of this study was to determine if there are hemo-static changes detectable using a rotational thromboelastography (ROTEM)assay in patients with newly diagnosed hematologic malignancies.Methods Used: 21 patients with newly diagnosed hematologic malignan-cies and 4 control patients were enrolled into the study. Of the 21 patients, 4were diagnosed with CLL, 7 were diagnosed with B-cell non-Hodgkin’slymphoma (3 large B-cell, 3 follicular, 1 mantle), 3 were diagnosed with mul-tiple myeloma, 4 were diagnosed with myeloproliferative disorders (2 CML, 2myelofibrosis), and 3 were diagnosed with non-myeloma plasma cell dys-crasias (2 MGUS, 1 Waldenstrom). To be eligible, patients could not have beenpreviously diagnosed with cancer, previously received chemotherapy, have ahistory of blood clots, be on anticoagulants, or be on hormone replacementtherapy. Patient blood samples were obtained at the time of diagnosis, andplasma samples were run on the ROTEM instrument. Three parameters generatedby ROTEM were compared to assess changes in coagulability: maximum clotformation (MCF), which measures the maximum strength of a clot; alpha-angle,which measure how quickly a clot is formed in the initial minutes of coagu-lation; and clot formation rate (CFR), which measures the rate of clotting.Summary of Results: Significant changes suggesting hypercoagulabilitywere only observed in the MCF of multiple myeloma patients; none of theother samples were significant for a change in coagulation. However, varia-tion in the range of ROTEM parameters for CLL, myeloproliferative disorders,and multiple myeloma samples suggest a range of coagulability in patients withthese malignancies.Conclusions: We demonstrated that our small multiple myeloma patientcohort had thromboelastographic findings suggestive of hypercoagulability,which is consistent with the known clinical clotting risks of multiple mye-loma. Additional work is ongoing in our laboratory to enroll more patientsand further investigate our findings.
330
UTILITY OF ROTEM ASSAY TO DISTINGUISHCOAGULATION FACTOR INHIBITORS FROM LUPUSANTICOAGULANTS
Minter S, Savage J, Meserve J, Dupre Vaughn C, Greenberg C. MedicalUniversity of South Carolina, Charleston, SC.Purpose of Study: To test the use of whole blood coagulation assay(ROTEM) to distinguish speciific coagulation factor inhibitors from lupusanticoagulants.Methods Used: Compare the ROTEM (TEM Innovations, GmbH) wholeblood assay versus routine plasma based coagulation tests in acquired FactorV deficiency and lupus anticoagulants. The effect of adding a platelet acti-vating agent in vitro was also evaluated.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 465
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: A factor V inhibitor patient presented with a PT of53.6 sec, aPTT 9 200 sec, fibrinogen 387 mg/dL, and thrombin time 21(16.2-19.6 sec). The aPTT did not correct when mixed with an equal volumeof normal plasma. Factor X and II assays increased from 12-99% as sampleswere diluted. The Factor V assay was less than 1% nhibitor assay and an in-hibitor titer of 23 Bethesda Units.. The ROTEM assay demonstrated an abnormalEXTEMwith clotting time (CT) of 1559 (38-79 sec), alpha-angle: 12 degrees(63-830 degrees), and maximum clot firmness (MCF) of 31mm (50-72 mm)recorded after 30 minutes. INTEM assay performed by ROTEM had a CTof 924 sec (100-240 sec), alpha-angle of 60degrees (70-83 degrees) andMCF of 68mm (50-72 mm). EXTEM measures the extrinsic pathway ofclotting triggered by tissue factor. Adenosine diphosphate (ADP) added towhole blood caused a concentration-dependent correction in the EXTEMassay by activating platelets and inducing the release of factor V. ADP short-ened CT to 506 sec from 1599 sec, while the addition of arachidonic acid andADP combined shortened the CT to 410 sec and the MCF corrected to withinthe normal range of 61 mm. The alpha-angle corrected from 12 to 50 degrees(60-83). The addition of ADP to normal volunteers’ blood did not cause anyshortening of CT or prolongation of the MCF. All clinical laboratory testsreturned to normal after 3 months of therapy.In contrast, EXTEM andINTEM assay on whole blood in patients with documented lupus inhibitorswere normal ( n= 5).Conclusions: The ROTEM assay can distinguish lupus anticoagulants fromspecific coagulation factor inhibitors.
331
EXCESS FACTOR XIII CONSUMPTION DURINGCARDIOPULMONARY BYPASS SURGERY
Janbain M, Leissinger C. Tulane Medical Center, New Orleans, LA.Purpose of Study: FXIII is an essential component of normal hemostasis.Congenital deficiency of FXIII activity is a rare autosomal recessive bleedingdisorder with an estimated incidence of one in 3 million. A fibrin-stabilizingFXIII concentrate that provides both A and B subunits of FXIII was FDA ap-proved last year for routine prophylactic treatment of congenital FXIII de-ficiency. There are few data available on replacement of FXIII concentratein patients with congenital deficiency undergoing surgery especially thoseundergoing cardiopulmonary bypass (CPB) surgery.Methods Used: A 52 year old man with congenital FXIII deficiency(baseline level 20%) underwent an aortic valve replacement surgery. Imme-diately prior to surgery, he was given a 100% correction dose of FXIII con-centrate (42 u/kg). However, the patient became hypotensive, so the chest wasopened urgently, he underwent internal CPR and was then placed on CBP. Heexperienced heavy bleeding intraoperatively. Factor XIII levels were checkedat 3 and 7 hrs post pre-op dose, and were 40% and 43% respectively; Theywere lower than expected based on his previous FXIII pharmacokinetic studies.He received an additional dose of FXIII concentrate (42 U/kg) 8 hrs afterthe first dose. During surgery he also received 9 U of PRBCs, 3 U of plts, 7 Uof FFP and 90mcg/Kg of rFVIIa, with ultimate control of bleeding.Summary of Results: He recovered uneventfully and his post-operativeFXIII levels were consistent with the published FXIII concentrate half-lifeof 6-8 days.Conclusions: Studies have shown that plasma levels of FXIII decrease by10-33% in a general population of patients undergoing CPB surgery. Thisraises concerns for effective replacement of FXIII in cases of congenitalFXIII deficiency. In our case, FXIII levels were approximately 60% less thananticipated based on pre-op pharmacokinetic testing of FXIII concentrate,and likely resulted in significant clinical bleeding intraoperatively. More in-formation is needed on surgical management, especially in cases with extra-corporeal circulation; a registry of these cases may be helpful to improve ourunderstanding on how to care for these patients. For now, we recommendusing an increased dose of FXIII prior to such surgeries.
332
DISEASE & TREATMENT CHARACTERISTICS OF BREASTCANCER IN AN URBAN, LOW-INCOME HOSPITAL IN NEWORLEANS
Schwab Keeport ML, Shin AJ, Gadinsky N, Collins-Burow B, Sheen M,Kruse-Jarres R. Tulane University, New Orleans, LA.
Purpose of Study: The Medical Center of Louisiana in New Orleans(MCLNO) serves the metropolitan area of New Orleans and is the onlyhospital delivering care to the indigent population. New Orleans was devastatedby Hurricane Katrina on 8/29/2005. No oncology services were available forseveral months and a large proportion of patients were displaced. Oncologyservices resumed in Oct. 2007. This study aimed to examine a cross section ofthis population and to characterize the care received by breast cancer patientsin the years after Katrina.Methods Used: This study received ethical approval by the IRB at Tulane.We reviewed charts from 142 patients (141 women, 1 man) who establishedcare for breast cancer at MCLNO between 1/2008 and 9/2011.Summary of Results: DEMOGRAPHICS
Median patient age was 56.9 years. Ethnicity: 71.8% African-American(AA), 14.8% White, 12.0% Other, 1.4% Unknown. Health insurance: 24.6%uninsured, 63.8% Medicare or Medicaid (MC/MA), 9.9% PPO, 2.1% other.MC/MAwas the predominant insurance type, except for Stage IV which hadpatients 50% uninsured and 50% MC/MA.
DISEASE CHARACTERISTICSInitial presentation: 32.4% patient-noted abnormality, 28.9% screening
mammogram, 4.9% physician-noted abnormality, 33.8% unknown. In ourpatient population, 21.8% were diagnosed at Stage 0 (national average amongAA patients 19.7%), 16.2% Stage I (national 28.8%), 28.9% Stage II (na-tional 31.8%), 16.2% Stage III (national 6.5%), 11.3% Stage IV (national4.7%), 5.6% unknown (national 8.5%).
TUMOR CHARACTERISTICS66.9% of all (66.7% of pre-menopausal) patients were hormone recep-
tor status positive, 18.3% (15.2% of pre-menopausal) were Her2/Neu+,14.8% (27.3% of pre-menopausal) were triple negative.
TREATMENT117 patients (82%) had surgical treatment; 46% had lumpectomies, 54%
had mastectomies. There was no racial difference in selection of surgery.Among the 30 DCIS & LCIS patients, all received hormonal ablation, withthe exception of 1 who declined treatment and 2 who were lost to follow-up.Of the 63 stage II or III patients, 51% received neoadjuvant, 33% adjuvant,16% no chemotherapy.Conclusions: Our patient population was predominantly AA and had eitherMC, MA, or no insurance. Overall, patients presented for care at later stages(III, IV) compared to national data, especially the uninsured.
333
INITIATING CHEMOTHERAPY IN THE ICU: BENEFICENCEOR MALEFICENCE?
Maronge GF, Zacharia G, Puligothram S, Narmala SK. LSU Health SciencesCenter, New Orleans, LA.Case Report: Case: A thirty-seven year old woman presented to the emer-gency department (ED) at an outside facility with complaint of shortness ofbreath and back pain. She reported the back pain had started 6 months ago andalso reported 2 weeks of abdominal pain. MRI performed in the ED wasconcerning for spinal cord compression and she was transferred to UniversityHospital in New Orleans. On arrival, she quickly decompensated and wasintubated for respiratory failure and hypotension. CT of the chest showed alarge pericardial effusion and multiple bone metastasis to the vertebra, bilat-eral humeri and clavicles. Transthoracic echo demonstrated evidence of car-diac tamponade and pericardiocentesis revealed serosanguinous fluid, withcytology positive for ovarian adenocarcinoma. CT of the abdomen confirmedthis diagnosis, showing a 16.7cm � 18.7cm mass arising from the left adnexa.The oncology service was consulted by the ICU team to discuss the prognosiswith the patient’s family. Respiratory failure was her only organ failure at thattime and the team elected to start treatment. She received one cycle of che-motherapy and the patient remained intubated and managed by the ICU team.On day 7 after chemo, the medical oncology team noted that an aggressivesedation and ventilation weaning approach was not in place. Though this wouldnormally be employed in a young and healthy patient, this had not been imple-mented due to an assumed poor prognosis. The patient underwent weaning anddid require tracheostomy 1 week later, however this was decannulized ap-proximately nine days after that. The patient was discharged at that time, am-bulating independently and performing all ADL’s. She received her second cycleof chemo before hospital discharge and followed-up in the clinic three weekslater feeling well except fatigue.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
466 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Discussion: This case underscores the importance of good communica-tion among specialties, being a patient advocate, and using evidence basedmedicine and objective measures when available in treatment decisionsof cancer patients. This patient was a young healthy person with no priormedical problems and no signs of organ failure except respiratory failure.Due to aggressive treatment in the ICU, she was able to enjoy prolongedsurvival with preserved quality of life.
334
COMPLEX PATHOPHYSIOLOGYOF HYPONATREMIAWITHBRAIN TUMOR CHEMOTHERAPY, AN ILLUSTRATIVECASE PRESENTATION
LeBlanc Z, Watts R. University of Alabama at Birmingham, Birmingham, AL.Purpose of Study: Determine the etiology of hyponatremia in a patientreceiving chemotherapy for a childhood brain tumor.Methods Used: Review of literature and case presentation.Summary of Results: CW is a 7-month-old Caucasian female diagnosedwith a brain tumor (atypical teratoid rhabdoid tumor (ATRT)). One weekfollowing incomplete resection and 4 days after placement of a ventriculo-peritoneal shunt, CW received multiagent chemotherapy consisting of metho-trexate, cyclophosphamide, etoposide, vincristine and cisplatin. The chemotherapytreatment was complicated by significant hyponatremia (nadir 121 MMOL/L-normals 134-143). While multiple possible etiologies of the hyponatremiawere entertained (syndrome of inappropriate anti-diuretic hormone (SIADH),post-operative, iatrogenic and nutritional), treatments for these etiologies didnot correct the defect. Supra-physiologic (25-30 mEq/kg/day of Na) dailysodium input along with an increased fluid requirement led to a diagnosis ofcerebral salt wasting (CSW). CSW is a poorly understood phenomenon thatdescribes hyponatremia in the face of a cerebral insult, most commonly post-traumatic hemorrhage. The key to distinguishing SIADH from CSW is apatient’s volume status; SIADH by definition must occur in a hypervolemicstate. For this patient, despite excessive IV fluids, she maintained a urineoutput of 6-8 ml/kg/hr for a week. Additionally, there was no evidence ofincreased weight or hypertension, nor was there edema noted on physicalexam. Lastly it was determined that this patient’s daily sodium requirement, tomaintain serum levels above 132, was more than 20 mEq/kg/day.Conclusions: Hyponatremia is an important complication of treatment forchildhood brain tumors. Diverse etiologies include post-operative, chemo-therapy associated, SIADH, iatrogenic, nutritional or CSW. Definition ofexact etiology and correct therapy is often complex. Our patient clearly il-lustrates the complex interplay of these diverse etiologies and treatments.
335
DRAMATIC RESPONSE TO BEVACIZUMAB ANDGEMCITABINE IN METASTATIC DUODENALADENOCARCINOMA - CASE REPORT
Agloria M1,2, Shows R1,2, Cheema FN1,2, Jafri SH1,2. 1Louisiana StateUniversity, Shreveport, LA and 2Feist Weiller Cancer Center, Shreveport, LA.Purpose of Study: Duodenal adenocarcinoma (DA) is a rare malignancywith limited data available to guide therapeutic decisions. Recent literaturesuggests Vascular Endothelial Growth Factor (VEGF) as a viable target. Tothe best of our knowledge this report represents the first description of the useof anti-VEGF agents in metastatic DA with pulmonary involvement.Methods Used: A 46 year old otherwise healthy African American femalewith Stage II (T3 N0 M0), moderately differentiated DA diagnosed January2007. Initially treated with curative resection without adjuvant chemother-apy. Post operative positron emission tomography scan showed no evidenceof disease. Disease recurred in March 2010; a CT chest performed for cough,hemoptysis and weight loss revealed extensive bilateral cavitary masses.Bronchosopic biopsy confirmed a thyroid transcription factor negative andCDX-2 positive adenocarcinoma consistent with a gastrointestinal primary.Summary of Results: Modified FOLFOX administered between April andAugust 2010 with no oxaliplatin in last 5 treatments due to grade 2 neu-ropathy. Switched to FOLFIRI in August 2010 due to progression of diseaseand received 5 cycles till October 2010 when disease progressed again. Re-ceived Irinotecan/Cetuximab as third line treatment with no response andhospice vs further treatment discussed. Patient with good performance statusopted for further treatment and in Jan 2011 Gemcitabine (G) 1000 mg/m2 days
1,8, 15 and Bevacizumab (B) 10 mg/kg every 2 weeks was initiated . RepeatCT scan in 2 months showed dramatic response with bilateral bulky massesin lungs replaced by cavitary lesions. In July 2011; after 6 cycles, she de-veloped a mycobacterium-avium intracellulare infection in the pulmonarycavitary lesions and treatment was held. Due to rapid progression of diseaseon repeat imaging, declining PS and increasing O2 requirements, chemother-apy was re-initiated with G+B in September 2011. After 3 cycles a CT scanagain revealed a remarkable response with subsequent improvement in O2requirement and improvement in PS.Conclusions: Impressive response with bevacizumab and gemcitabine inmetastatic duodenal cancer underlines the importance of VEGF targetting inmetastatic DA. Further prospective studies and search for biomarker is essential.
336
T-CELL LYMPHOBLASTIC LEUKEMIA: TAKE TWO
Evans J, Elkins S. University of Mississippi Medical Center, Jackson, MS.Case Report: T-cell lymphoblastic leukemia (T-LBL) diagnosed in child-hood is an overall highly treatable disease that is often curable. Despite this,relapses occur in almost 1 out of every 4 children, with most happeningwithin the first 2 years after completing therapy. We report a case of a manwith relapsed T-LBL 28 years after initially being diagnosed.
A 45yo male with a history of T-LBL and stroke was sent to the emer-gency department by his primary care provider after being found to have amass in his mediastinum on chest radiography. The patient reported having7 to 10 days of swelling in his face and the right side of his neck. These symp-toms were worsened when lying flat at night to sleep. On physical exam hewas noted to have engorged veins in his neck with associated soft tissueswelling that was more prominent on the right side. While in the emergencydepartment the patient underwent a CT scan of the chest that revealed a 5.4�8.0 � 9.5 cm mass within the anterior right mediastinum with near completeocclusion of the superior vena cava. Initial complete blood count on ad-mission included a white blood cell count of 6,400, hemoglobin of 15.6 g/dL,and platelet count of 144,000. Patient was admitted to the hospital and sub-sequently underwent biopsy of mass in mediastinum, with results consistentwith T-cell lymphoblastic lymphoma. A bone marrow biopsy performed showedevidence of marrow involvement. His current presentation had several sim-ilarities to his initial one as a child, including a mass in his mediastinum aswell as disease in his bone marrow. After obtaining these results the patientwas started on induction chemotherapy with CALGB 8811 protocol and iscurrently undergoing intensification therapy as an outpatient.
While reported relapses of T-LBL after 10 years is less than 1%, this caseillustrates the need for long-term follow in all patients diagnosed in child-hood. Late relapses raise the question of whether this is a true relapse of theprior cancer or a new disease process altogether, with the current evidenceavailable in the literature supporting the former.
Infectious Diseases IConcurrent Session
2:00 PMFriday, February 22, 2013337
EFFECTIVENESS OF A HAND HYGIENE CAMPAIGN INADDIS ABABA, ETHIOPIA
Schmitz K1, Kempker R1, Tenna A2, Tiadesse L3, Stenehjem E1, Kacha E2,Abebe E2, Blumberg HM1. 1Emory University School of Medicine, Atlanta,GA; 2Addis Ababa University, Addis Ababa, Ethiopia and 3St. Paul’sMillennium Medical College, Addis Ababa, Ethiopia.Purpose of Study: Hand hygiene (HH) is the cornerstone of infectioncontrol and has been proven to reduce rates of healthcare associated infection.There are limited data evaluating HH compliance and HH campaign effec-tiveness in resource poor settings, especially in sub-Saharan Africa. This studyassessed the impact of implementing a WHO-recommended multimodal HHcampaign in Ethiopia.Methods Used: The study took place at a 250-bed teaching hospital in AddisAbaba, Ethiopia. HH observations were made before and after the imple-mentation of a HH program. The intervention was implemented over 1 monthand included 4 components: 1) infrastructure change; providing a commercial
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 467
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

hand sanitizer to all healthcare workers (HCWs) 2) formal didactic training 3)visual reminders and 4) development of a monitoring/feedback system. A knowl-edge, attitudes, and practices (KAP) survey of HCWs on HHwas also performed.Summary of Results: At baseline, soap and towels were not available atsinks; only 36% of wards had hospital made sanitizer. There was a significantincrease in HH adherence among HCWs following implementation of a HHprogram. Adherence increased from 2% at baseline (21/1000) to 13% (127/1000) after the implementation of the HH campaign (OR=6.5, 95% CI 4.1-10.4). HH rates significantly increased among all HCW types except at-tending physicians. In the post-intervention period, HCWs in the EmergencyDepartment were more likely to perform HH than those in other departments[OR=3.4, 95% CI 2.4-5.1] and nurses were more likely to perform HH com-pared to other HCWs (OR=2.4, 95% CI 1.5-3.4). HCWs were more likely toperform HH after patient contact than before patient contact (OR=2.1, 95% CI1.4-3.3). The KAP survey of 199 HCWs revealed that HCWs found the WHOformulation for alcohol based sanitizer to be poorly tolerated and 73% indicatedtheir HH adherence would improve with a commercially available sanitizer.Conclusions: There was a significant increase in HH among EthiopianHCWs following the implementation of a multimodal HH campaign. Dissat-isfaction with theWHO hand sanitizer formulation was identified as one barrierfor poor HH compliance. Much work remains to ensure sustainability and tocontinue to increase rates of HH adherence.
338
COMBINATION OF AMPICILLIN AND AZITHROMYCINIMPROVED OUTCOMES IN MOUSE MODEL OF GROUP BSTREPTOCOCCUS SEPSIS
Upadhyay K, Meals E, English BK, Talati AJ. UTHSC & Children’s ResearchFoundation at LBCH, Memphis, TN.Purpose of Study: Group B streptococcus (GBS) is a leading cause of lifethreatening infections in neonates for which ampicillin (AMP) is the pre-ferred antibiotic. However, evidence suggests that A-lactam monotherapy ofother streptococcal infections may be inferior to combination therapy with,usually a macrolide. We proposed to develop a mouse model for GBS sepsisand observe the difference in clinical signs, mortality and serum cytokinelevels when treated with AMP, Azithromycin (AZM) and combination ofAMP+ AZM.Methods Used: Swiss Webster 9 mice (wt-18g, Age-4wks) were injectedintraperitoneally (IP) with GBS Ia (log 5-9 cfu/ml) to 2 mice each andmonitored using ‘‘clinical sepsis score (CSS)’’. After deciding optimal dos-ing of GBS (log 7, 8 cfu/ml), mice were divided in 4 groups (grp). Grp I -noantibiotics, Grp II- treated with AMP (100mg/k/d, MIC e0.25 mcg/ml), GrpIII- treated with AZM (10 or 50mg/k/d, MIC e0.125ug/ml) and Grp IV-treated with AMP+AZM. Antibiotics or PBS (control) were administered q24hIP. After 5 days mice were sacrificed and serum cytokines (TNF->, IL-6, IL-10), chemokine (MIP-1>) and blood culture were obtained.Summary of Results: Case fatality rate was 60% in grp I (n=9), 25% in grpII (n=8) and 0% in both grp III (n=8) & grp IV (n=8). Mean serum IL-6 waslower in grp III (66T52 pg/ml) & grp IV(52T22 pg/ml) compared to grp II(260T160 pg/ml) (pe0.005). No difference was found in mean TNF->, IL-10and MIP-1> between grps. The CSS was significantly lower in grp II & grpIV compared to grp I & grp II (figure). Blood culture of control mice showedGBS, but rest remained sterile at 5 days.Conclusions: We were able to develop a GBS sepsis model in mice. Themice infected with GBS had less pronounced IL-6 response, decreased mor-tality and morbidity when treated with AMP+AZM compared AMP alone.
339
AZITHROMYCIN INHIBITS MACROPHAGE TUMORNECROSIS FACTOR SECRETION IN RESPONSE TOSTIMULATION WITH EITHERAZITHROMYCIN-SUSCEPTIBLE ORAZITHROMYCIN-RESISTANT CLINICAL ISOLATES OFCOMMUNITY-ASSOCIATED METHICILLIN-RESISTANTSTAPHYLOCOCCUS AUREUS
Fesmire A1,3, Ingram K2,3, Meals E2,3, English BK2,3. 1University of TennesseeHealth Science Center, Memphis, TN; 2Univ of Tennessee Health Sci Ctr,Memphis, TN and 3Children’s Foundation Research Institute, Memphis, TN.Purpose of Study: Infections caused by community-associated methicillin-resistant strains of Staphylococcus aureus (CA-MRSA) are a serious problemand often are associated with intense and prolonged host inflammatory re-sponses. Optimal therapy of these infections is uncertain, but most pediatricpatients are treated with vancomycin (VAN). We and others previously havereported that combination antimicrobial therapy of other serious Gram-pos-itive infections that includes a macrolide such as azithromycin (AZM) may besuperior to monotherapy with cell-wall active antibiotics such as penicillin orVAN. We hypothesized that the addition of AZM would reduce the macro-phage TNF response to VAN-treated CA-MRSA isolates, whether or not theywere susceptible to AZM.Methods Used: Three previously characterized CA-MRSA isolates wereused: 6U24 was susceptible to AZM (MIC 4 mg/L) while LAC and 7U20were resistant to AZM (MIC 9 256 mg/L). RAW 264.7 murine macrophageswere exposed to live bacteria at concentrations of 10(5)- 10(8) cfu/mL im-mediately after the addition of VAN (20 mg/L) alone or VAN + AZM (1, 5, or20 mg/L) to the culture medium. Cells were cultured overnight and ELISAwas used to quantitate TNF concentrations in cell supernatants.Summary of Results: Macrophages stimulated with all three CA-MRSAisolates in the presence of AZM secreted substantially less TNF than mac-rophages in the presence of bacteria exposed to VAN alone. The magnitude ofthe reduction was greatest for the AZM-susceptible 6U24 strain (30 - 74%,depending on the inoculum) and less for the two AZM-R strains (0 to 67 %,depending on the inoculum), but was statistically significant for each of thethree strains at at least one inoculum.Conclusions: Exposure of both AZM-susceptible and AZR-resistant CA-MRSA isolates to combinations of AZM and VAN leads to a blunted macro-phage response to these bacteria. The potential benefits of combination anti-microbial therapy of severe CA-MRSA infections deserves additional study.
340
MOLECULAR QUANTIFICATION OF HERPES SIMPLEXVIRUS(HSV) DNA IN THE CSF AND NEURORADIOLOGICALOUTCOMES IN PATIENTS
Ramirez K1,2,3, Choudhri A1,2, Thompson R2, Patel A1,2, DeVincenzo J1,2.1Univ of Tennessee, Memphis, TN; 2LeBonheur Children’s Hosp, Memphis,TN and 3St Jude Children’s Research Hosp, Memphis, TN.Purpose of Study: New molecular diagnostics allow both sensitive HSVdetection and quantification within CSF. Rigorous studies of HSV load andneurological severity have not been performed. Understanding relationshipsbetween infection timing, viral load and disease severity is necessary to ad-vance new therapeutic concepts for this devastating disease. We developed aquantitative HSV molecular assay and studied the correlation of CSF viralload with neuroradiological (MRI) outcomes.Methods Used: Pts included had a (+)HSV CSF PCR result, and Q1 MRIduring hospitalization. Electronically stored Ct(crossing threshold) valuesgenerated by real-time PCR were read off the mean of repeated standardcurves generated by quantified HSV whole virus purified DNA. Patient’s Ctvalues were converted to viral loads(log10 copies/ml). A blinded neurora-diologist quantified MRIs based on extent (volume) and severity of CNSinvolvement (degree of vasogenic edema, cytotoxic edema, and hemorrhageidentified on T2, DWI, and T2/DWI/FLAIR, respectively).Summary of Results: 24 pts with HSV meningitis had lower CSF viralloads than 33 with HSVE (p=0.035). Within HSVE pts, 22 (15 neonates, 4children, 3 adults) had 42 images reviewed. Time from symptom onset to firstlumbar puncture (LP) and time from first LP to first MRI was mean 4.2(SD3.4) and 5.7(9.4) days, respectively. Initial viral loads were mean 5.0 (range
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
468 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

2.5-8.0) log10 copies/ml. Loads were similar between age groups, sex, anddespite duration from symptom onset to the first LP (p all 90.05). There wereno statistically significant correlations between initial and/or peak viral loads(if Q1 LP) and extent or distribution of MRI abnormalities in images obtainednearest to time of LP and/or in the worst image in a series (p all 90.05).Conclusions: HSV CSF viral load is higher in pts with encephalitis com-pared to meningitis. In pts with HSVE, viral load in CSF was not associatedwith extent or severity of subsequent MRI imaging suggesting inflammatorycomponents of disease are under appreciated. Ongoing research will evaluateindependent effects of these variables via logistic regression models and eval-uate relationships between HSV CSF viral load, MRI, and long-term clinicaloutcomes.
341
SOCIOECONOMIC RISK FACTORS FOR VIROLOGICFAILURE IN DURBAN, SOUTH AFRICA
Hare AQ1, Johnson B1, Ordonez C2, Wu B1, Hampton J2, Gordon M5,Kuritzkes D4, del Rio C1, Sunpath H2, Marconi V1,3. 1Emory University,Atlanta, GA; 2McCord Hosp, Durban, South Africa; 3Atlanta VA Med Ctr,Decatur, GA; 4Brigham and Women’s Hosp, Boston, MA and 5Doris DukeMed Rsch Inst, Durban, South Africa.Purpose of Study: Little is known about sociodemographic risk factors forvirologic failure (VF) to first antiretroviral therapy (ART) in South Africa.We hypothesized that unemployment and economic insecurity are associatedwith VF.Methods Used: A case-control study of VF was conducted among pa-tients recruited from the outpatient clinic at McCord Hospital (MCC) in Durban,South Africa between October 1, 2010 and June 30, 2012. Cases were thosefailing first ART, defined as VL 9 1000 copies/mL. For each case, twocontrols (VLe1000 copies/mL while on ART) were recruited. Univariatelogistic regression was performed on sociodemographic data gathered fromsemi-structured interviews and chart review for the outcome of VF. Variablesfound significant (pG.05) were included in multivariable (MV) models. Awealth index was constructed using principal component analysis on indi-cators of wealth (assets, utilities, housing type, food security) and used toadjust the MV model.Summary of Results: Of 458 patients (158 cases, 300 controls) includedin the study, 35% were male, with median age of 40 yrs, median CD4 of300 cells/uL, median HIV viral load 3393 copies/mL . In univariate analy-sis lack of income (OR 1.76, p=.015), unemployment (OR 1.72, p=0.025),living with family (OR 1.56, p=0.026), matriculation from high school (OR1.43, p=0.071), and who pays for ARTwere significantly associated with VF.Family (non-spouse) paying for ART was associated with VF (OR 2.38,p=0.001) while self-paying for ARTwas correlated with not having VF (OR0.634, p = 0.051). In a MV model including these variables and known riskfactors for VF (age, gender, treatment duration), only family paying for ARTremained significantly associated with VF (OR 2.642, p=.040), even afteradjusting for wealth (p=.046).Conclusions: Lack of income, unemployment, living with family, and fam-ily paying for ART are associated with VF. Family paying for ART remainedsignificantly associated with VF after adjusting for other significant factors.These data suggest either insecurity of funds when family pay for care or thatpersonal investment in medical care is important to achieve viral suppressionin this setting.
342
CHARACTERISTICS OF VIREMIC CONTROLLERS INSOUTHERN HIVAMBULATORY CLINIC
Lynch MA1, Frontini M2,1, Clark R2,1. 1LSUHSC, New Orleans, LA and2LSUHSC, New Orleans, LA.Purpose of Study: A small subgroup, approximately 2 - 15%, appear tomaintain low HIV RNA levels and high CD4 cell counts and are termed long-term non-progressors (LTNP). LTNPs have been further defined into viremiccontrollers (VC) (HIV RNA level 50 - 2,000 copies) and elite controllers (EC)(HIV RNA level G 50 copies) in the absence of antiretroviral therapies (ART)for prolonged periods of time. Previous studies have not found associationbetween EC status and demographic characteristics, but there appears to be anover-representation of protective HLA alleles (HLA B5701 and HLAB5703).
Methods Used: To better define characteristics of VCs and ECs in theSouth, a retrospective chart review was performed on patients enrolled in theHIVOutpatient Program (HOP) clinic between 1/1/07 and 12/31/10. Patientshad to have had 9 3 clinic visits, 9 2 HIV RNA levels G 2000 copies off ART,and have no HIV RNA levels 9 2,000 copies.Summary of Results: The prevalence of VCs was only 10 in 2015 HOPpatients or approximately 0.5 %. Other selected demographic characteristicsin VC and HOP general populations are shown in the table below.Conclusions: HOP VCs were likely to be women, African American, andhave + HLAB5701 testing. The relatively large proportion of + HLAB57 re-sults in the VCs compared to the general HOP population is in alignment withthe literature which suggests a HLAB57 correlation with an EC designation.Compared to other study populations described in the literature, the preva-lence of VCs and ECs in the HOP clinic population was low. One consid-eration to partially explain the low HOP prevalence could be that healthypatients may not have maintained regular clinic visits due to a lack of symp-toms. This population also may be more likely to be employed and insuredwhich would expand their options for health care providers. Further epide-miologic research on LTNPs, VCs, and ECs from diverse geographic and de-mographic populations is warranted.
343
INAPPROPRIATE URINE TOXICOLOGY SCREENS AMONGHIV OUTPATIENTS WITH PAIN SYNDROMES
Peters J1, Frontini M2,3, Almeida M2, Seal P2,3, Clark RA2,3. 1LSUHSCSchool of Public Health, New Orleans, LA; 2LSUHSC-MCLNO HIVOutpatient Program, New Orleans, LA and 3LSUHSC School of Medicine,New Orleans, LA.Purpose of Study: In 2011 the HIV Outpatient Program (HOP) formalizedthe clinic pain management program and required all patients prescribed long-term opiates to undergo periodic urine toxicology screens (UTS). The fre-quencies of opiate misuse and substance abuse among HOP patients withpain syndromes are of interest for future planning.Methods Used: A retrospective review was performed to determine theprevalence of inappropriate UTS which were defined as either the presence ofillicit substances, the presence of selected drugs in the absence of documentedprescribing, or the absence of selected drugs in the presence of documentedprescribing (suggesting diversion).Summary of Results: Charts from a convenience sample of 47 patientsenrolled in the HOP clinic were reviewed. The prevalences of UTS positivefindings (positive results in the absence of documented prescribing) by drugclass were benzodiazepines (14.9%), THC-20 (23.4%), opiates (4.26%), car-isoprodol (0%), cocaine (6.38%), and amphetamines (2.13%). The prevalencesof UTS negative findings (negative results in the presence of documentedprescribing) by drug class were benzodiazepines (2/14 or 14.3%), and opiates(10/32 or 31.3%).
The only factor significantly associated with inappropriate UTI was limbpain (p=0.01). Ever cocaine use was a borderline for significant association(p=0.06). Factors that were not significantly associated with inappropriateUTS included selected medical and mental health diagnoses, other referralpain syndromes, and social factors (smoke at baseline, homeless at base-line, ever incarcerated, recent life stressor, ever cocaine on prior toxicology screen,and ever other illicit substance on prior toxicology screen), a CD4 G 200 cells,and a VL 9 400 copies.Conclusions: The prevalence of inappropriate UTS is relatively high. Themost common illicit substance is THC-20 followed by cocaine use. Althoughthe absence of benzodiazepines and opiates in the presence of documentedprescribing is frequent, additional research is needed to determine if thisfinding represents diversion.
Characteristics in HOP general population and HOP VC
*estimate from literature **Results were available on only 4 patients
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 469
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

344
HUMAN IMMUNODEFICIENCY VIRUS IN THE EARLYTWENTY-FIRST CENTURY: GENDER DIFFERENTIAL ATTIME OF PRESENTATION FOR ANTIRETROVIRALINITIATION
Chu K1,2, Zuver A1, Nguyen D1,2, McDowell K1, Nguyen MT1. 1EmoryUniversity School fo Medicine, Decatur, GA and 2Emory University, Atlanta,GA.Purpose of Study: The HIV epidemic continues to evolve in the twenty-first century with the epicenter in the south. This study reports the char-acteristics of HIV+ individuals presenting for antiretroviral treatment (ART)at our urban Ryan-White-funded HIV clinic. The gender differential of theseindividuals also provides a snapshot of HIV infected patients who start ARTsin a southern urban clinic, which will allow us to determine what improve-ments can be made in the future as necessary.Methods Used: This is a retrospective review of a cohort of 1015 patientswho started ART between June 2004 and December 2011. Charts and elec-tronic medical records were abstracted for demographics, Cd4, and viral load.Summary of Results: Among the 1015 individuals with a predominance ofAfrican Americans (90% in women (W) and 80% in men (M)), only 24% wasfemale. Women are older at the time of HIV diagnosis (W 40 vs M 36 yearsold, pG0.001) and ART initiation (W 43 vs M 38 years old, pG0.0001). Thereis a significant delay in ART initiation for women (40 months vs 30 months,pG0.0001). We also found a higher proportion of overweight and obesity inwomen than in men (W 20% vs M 5%, pG0.0001). Sex with men representsthe principal risk factor for HIV (W 89%, M 63%). Cd4 cell count at ARTinitiation was higher in women than men (W 98 vs M 81 cells/mm3, p=0.012).We found a lower prevalence of Hepatitis B infection in women than in men(W 5 vs M 9, p=0.03) while the prevalence of Hepatitis C is similar betweenwomen and men (W 8 vs M 8.5%).Conclusions: In the late ART era in an urban Ryan-White-clinic, patients,women significantly more so than men, are started late on ART with a lowmedian Cd4 count. Based on our findings, efforts in starting HIV infectedpatients on medication earlier are needed.
345
CERVICAL DYSPLASIA IN HIV POSITIVE WOMEN IN THELATE ANTIRETROVIRAL ERA
Lofgren S1, Nguyen J1, Herring- Bailey G3, Tadros T3, Birdsong G3,Mosunjac M3, Flowers L2, Nguyen M1. 1Emory University, Atlanta, GA;2Emory University, Atlanta, GA and 3Emory University, Atlanta, GA.Purpose of Study: Women living with HIV/AIDS (WLHA) have higherrates of cervical cancer and faster progression of dysplasia than HIV negativewomen. However there is scant data in the established ARTera. We evaluatedthe evolution of cervical dysplasia in WLHA.Methods Used: This is a longitudinal retrospective review of cervical papsmears of WLHAwith an intact cervix who received care between 6/2004 and12/2011 and 2+ years of follow up. Progression is defined as having follow-up smears with squamous intraepithelial lesion (SIL) following a pre-SIL papor LGSIL followed by HGSIL. Regression is defined as a pap smear with SILfollowed by at least 2 negative pap smears. Patients’ demographics, CD4+counts, viral load, gynecological history, cytology and pathology results wererecorded. Measures of association were assessed using chi square test usingSAS9.3.Summary of Results: The majority of 310 were black (93%). At enrollment,median age was 40(IQR: 33-47), median Cd4+ count was 287(IQR=118-477);67% were on ART, 46% had an undetectable viral load, and 39% smoked.The median follow up was 57 months (IQR: 38-78). 50% NILM remainpersistently negative, while17% progress to SIL; 40% ASCUS progress toSIL; 7% LGSIL progress to HGSIL and 39% regress to normal ;13% ASC-Hiprogress and 38% regress to normal; 50% HGSIL regress without surgicalintervention and 20% progress to squamous cell cancer. In a multivariatemodel, the most significant predictor of progressioin was the initial CD49350 cells/mm3 (OR =2,95%CI:1.0-4.0).Conclusions: Our cohort comprised WLHA who had long standing HIVinfection and are older, which would put them at higher risk for cervicaldysplasia, yet 21% had persistently negative pap smears and 17% progressedto higher grade lesions. Given the low rate of progression and the low rate of
precancerous lesions found at colposcopy in LGSIL, new strategies are neededfor follow up of LGSIL.
346
CO-SHEDDING OF HUMAN PAPILLOMAVIRUS ANDEPSTEIN-BARR VIRUS IN THE DEVELOPMENT OFLONG-TERM CERVICAL DYSPLASIA IN HIV-POSITIVEWOMEN
Oddo H, Sutton K, Meyaski-Schluter M, Hagensee M. LSU Health SciencesCenter, New Orleans, LA.Purpose of Study: Human papillomavirus (HPV) is the most commonviral sexually transmitted disease and is the causative agent of cervicalcancer. HPV is present in approximately 90% of cervical cancer cases, yet italone is not sufficient to cause malignancy. Two-thirds of cervical dysplasiacases have been shown to spontaneously resolve within eighteen months. Wehave previously identified Epstein-Barr Virus (EBV) as a possible cofactorwhen coupled with HPV in increasing rates of cervical dysplasia by two- tofour-fold in an HIV+ population. Basic investigations of the role of HPVandEBV co-infections are necessary in order to better understand the interactionbetween these two viruses.Methods Used: Subjects were HIV+ women currently enrolled in a lon-gitudinal study examining the interaction of HPV and EBV in the develop-ment of cervical dysplasia. Participants are followed every three months overthe course of five years, with Pap smears and cervical swabs collected at eachvisit. Cervical swabs were DNA-extracted using a Qiagen\ kit. HPV was de-tected using Roche\ linear array targeting the L1 gene. To test for the presenceof EBV, a PCR assay was run to detect the BamH1-W gene. These resultswere correlated with concomitantly obtained cervical Pap smears. Long-termcervical dysplasia was indicated by either absence of resolution or progres-sion to a more severe state as determined by the Bethesda classificationsystem.Summary of Results: Forty-three HIV+ women completed an average of11.5 visits. Initial analyses indicates a strong correlation between co-sheddingof both EBV and HPV from the cervix with a consistently abnormal (non-progressive) Pap smear over time (21%) in comparison with those sheddingneither virus (5%) or HPV only (9%). A weaker correlation was also foundwith those who progressed to a more severe dysplasia in the presence of co-infection (2%).Conclusions: In HIV+ women, co-shedding both HPV and EBV from thecervix, resolution of dysplasia does not occur over time leaving these womenat risk for cervical cancer. Studies are still ongoing and a greater sample sizeis needed in order to gain a better understanding of the relationship betweenco-shedding of these two viruses and their role in continuing cervical dys-plasia and progression to cancer.
347
HIV1 RESISTANCE MUTATIONS IN NAIVE HIV INFECTEDINDIVIDUALS ATTENDING A RYAN WHITE CLINIC
Kim AY, Zuver A, Chu K, Nguyen D, Wang W, Tran C, Marconi V, Nguyen M.Emory University, Atlanta, GA.Purpose of Study: The rate of resistance mutation among HIV infectedpatients is rising with the widespread use of antiretroviral therapy (ART). Wereport the frequency of reverse transcriptase inhibitor (RT) and protease in-hibitor (PI) resistance mutations among people living with HIV/AIDS in theestablished antiretroviral (ART) era in a Ryan White funded AIDS clinic.Methods Used: This is a retrospective review of ART naive patients whohad a genotype resistance before starting ART between 6/2004 and 12/2011.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
470 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Medical clinic charts and electronic medical records were abstracted for de-mographic data as well as CD4, viral load and HIV genotype.Summary of Results: The cohort consists of 1015 ART naive patients,with 76% males, 80% African Americans, with median age at HIV1 diag-nosis of 36, and baseline CD4 cell count of 85 cells/mm3. There were 653(64%) available baseline genotypes. 90 (14%) had at least one significant RTor PI mutation, 48 (7%) had an NRTI mutation, 53 (8%) had an NNRTI mutationand 11 (2%) had a PI mutation. The most commonly occurring RT mutationsinclude K103N (44), M184V (18), M41L(8), K65R(7), and L74V (4). Themost common PI mutations are L90M (5) and D30N (3). The most commondual RT mutations are M184V/K103N (12). Of interest there is a trend to lessART overall resistance mutations in the later part of the study.Conclusions: In the established ART era, HIV1 resistance mutations wereidentified in naive patients. Baseline genotype testing should be performed todirect ART. The evolution of resistance acquisition needs further study.
Medical Education and Medical EthicsConcurrent Session
2:00 PM Friday,February 22, 2013348
THE IMPACT OF CHANGING DUTY HOURS ON RESIDENTLEARNING
Hough-Telford C, Nassetta LB, Wall TC, Hartig JR. University of Alabamaat Birmingham, Birmingham, AL.Purpose of Study: In order to comply with new ACGME duty hour guide-lines, in July 2011 our program instituted a wards shift system wherein a dayteam admits patients to themselves (primary admit day) and a night teamadmits patients to another team (secondary admit day). Thus, teams receivenew patients twice per call cycleVone group they admitted themselves and onegroup admitted by the night team. Our study aims to prospectively examinehow these changes impact resident learning, experience, and autonomy.Methods Used: Between April-June 2011 and April-June 2012, GeneralInpatient Pediatric Service (Ward) residents completed electronic and papersurveys on primary and secondary admit days. Responders reported the fol-lowing: team role, number of initial assessments personally performed, totaladmissions, estimated time spent reading, and need for guidance in caring fornew patients. Comparisons between questions were analyzed with Fisher’stest on 2�2 contingency tables; unpaired T tests were used to obtain p-values.Summary of Results: Residents completed 232 surveys during the periodsof interest. Prior to duty hour changes, PGY-1 residents participated in anaverage of 9.1 admissions per call, compared to 4.0 admissions per primaryadmit day in 2012 (pG0.05). Residents of all levels of training (PGY 1-4)averaged 7.4 initial assessments in 2011, versus 4.1 in 2012 (pG0.05). Re-ported reading time did not change significantly over studied periods. A sig-nificant difference existed regarding resident comfort level in the independentmanagement of new patients; in 2011 only 23% of residents needed attend-ing guidance a majority of the time, versus 59% in 2012 (pG0.05).Conclusions: While complying with new work hour restrictions, residentsadmitted fewer patients during their primary admit day. Despite performingless total admissions, residents in 2012 reported similar time spent reading astheir counterparts in 2011. Residents asked for attending guidance more fre-quently after duty hour changes, which may be a result of less involvement withinitial assessments and less familiarity with patients. While our study haslimitations, it highlights the need for leaders in medical education to continueevaluating the impact of duty hour guidelines on resident learning, experi-ence, and autonomy.
349
DIAGNOSTIC ERROR IN THE CARE OF SIMULATEDPEDIATRIC INPATIENTS
Nassetta L1, Tofil NM1, Youngblood A2, Zinkan J2, Eschborn S1, TaylorPeterson D1,2, White ML1. 1University of Alabama at Birmingham,Birmingham, AL and 2Children’s of Alabama, Birmingham, AL.Purpose of Study: Diagnostic errors in medicine result in substantial harmto patients. Premature closure, the tendency to accept a diagnosis before it hasbeen verified, is the most common type of error in the care of inpatients. Thusfar, research on use of simulation to evaluate this error is limited and mostcommonly involves emergency medicine physicians. We hypothesized thatpremature closure could be demonstrated during simulation with residents oninpatient pediatrics rotations.Methods Used: Residents participated in teams (PGY1 + PGY2-4). Eachteam received two cases in which they were asked to evaluate and treatsimulated patients. A text page to the resident with a brief description of thepatient started each case. The description contained either an incorrect di-agnosis (Stem A) or a symptom (B). The remainder of each case was scriptedand presented identically. Cases were paired such that residents who receivedthe A stem for Case 1 received the B stem for Case 2, and vice versa (Tablebelow). Data regarding evaluation, treatment, and correct diagnosis was col-lected in real time on a standardized recording tool. Comparisons betweenstems (A vs. B) were analyzed with Fisher’s exact test.Summary of Results: Sixty-five residents participated. Residents whowere given the symptom either considered or made the correct diagnosis 86%
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 471
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of the time, vs. 72% for those given the incorrect diagnosis (pG0.05). Sim-ilarly, those who received the symptom initiated appropriate therapy morefrequently than those who received the incorrect diagnosis, at 60% and 53%of the time, respectively (pG0.05). Often those teams receiving the incorrectdiagnosis initiated treatments prior to examining or reviewing key featuresof the disease.Conclusions: Premature closure can be demonstrated during simulated pa-tient encounters in the pediatric inpatient setting. Residents given a symptomwere more likely to determine the correct diagnosis and begin therapy be-cause they were not drawn to close prematurely on the incorrect diagnosis.Simulation provides an excellent venue in which to evaluate cognitive errorand to teach metacognitive strategies for avoiding it.
350
CRANIOFACIAL DYSMORPHISM IDENTIFICATION: WHEREDO WE STAND?
Trairatvorakul P, Martinez J, Swingle HM. University of South Alabama,Mobile, AL.Purpose of Study: 1) Assess pediatric residents’ & medical students’ skillin identifying craniofacial dysmorphism (CFD) in photographs of childrenseen in a university-based developmental clinic. 2) Train pediatric residentsto identify distinct and subtle CFD. 3) Re-evaluate skills after a single di-dactic teaching session on the recognition of CFD.Methods Used: A clinical dysmorphologist provided a 30-minute lectureon CFD identification in children with DD. USA pediatric residents & med-ical students completed 10 minute pre- & post-tests, each test consisting of 20clinic photographs, 10 of which included children with distinct CFD. Sta-tistical analysis was done using the paired t-test.Summary of Results: Residents & medical students correctly classifiedonly 65% of the photographs. Scores did not improve on the post test. Pedi-atric residents tended to misclassify children with no CFD as having CFD,rather than the converse. See Table 1.Conclusions: Pediatric resident skills are limited in recognizing CFD. Wespeculate that failure to see improvement in the post-test scores may be dueto the didactic teaching format, limited exposure time, resident fatigue, lackof interest and/or motivation. Implications for future studies should explorealternative teaching methods and determine if the skills learned are actuallyapplied in the clinical setting.
351
IMPROVED PHYSICAL EXAM SKILLS USING ACLERKSHIP-BASED INTERVENTION
Horn MM, Gearhart JG, Ibrahim J, May W, Geraci SA. University ofMississippi Medical Center, Jackson, MS.Purpose of Study: Physical examination (PE) skills are key to becominga clinically competent physician. At our institution, concerns arose that ourmedical students’ PE skills were suboptimal at the end of their third year,as our traditional second year Introduction to Clinical Medicine course pro-vided their only formal training in this area. Scores on our standardized inter-nal clinical skills examination, designed to parallel the USMLE Step 2 CS,confirmed this observation.
Methods Used: We divided the complete physical exam into 9 compo-nents. Educators in each third-year clinical clerkship were assigned primaryresponsibility for teaching one or more components during their 2011-12clerkship, using case-based training and determining mastery via a standard-ized mini-clinical evaluation exercise for each component.
In May 2012, the intervened third-year class (N=115) took our internalstandardized exam and scores (mean +/- SD) were compared to pooled av-erages for the three preceding classes (N=339, as a pre-intervention baseline).Overall clinical skills scores (PE plus other Step 2 clinical exam test com-ponents), total PE scores (composite of all PE components), and individualcomponent PE scores were compared to baseline values via independentsamples t-tests.Summary of Results: Overall scores improved from 79.3 +/- 4.0 to 82.8 +/-3.1. Total PE scores improved from 66.2 +/- 10 to 71.0 +/- 7.2. ComponentPE scores for pulmonary, neurologic, and abdominal examinations also im-proved. All these improvements were statistically significant (pG.05). Scoresfor other PE components were not different following the intervention.Conclusions: Our data support that additional training and assessment of PEskills during the third year clerkships may improve PE performance on astandardized evaluation, which in turn contributes to higher overall clinicalskills test scores. Further investigation and collection of additional data pointswill be needed to determine if individual component training can be en-hanced to achieve improvement in other areas of the physical examination.
352
IMPACT OFA PARENT-LED CURRICULUM IN DISABILITIESON RESIDENTS NOW IN PRACTICE
Kube DA, Bishop E, Roth J, Palmer F. University of Tennessee HealthScience Center, Memphis, TN.Purpose of Study: Families of children with special health care needs(FCSHCN) want to partner with their physicians to provide family-centeredcare and a medical home for their children. A parent group developed a parent-led curriculum to assist in the training of pediatric residents for this purpose.The residents felt this experience would be relevant to their future practice.The objective of this study was to evaluate the impact the experience had onformer residents currently in practice.Methods Used: 188 former residents participated in a parent interview anda home visit with FCSHCN through the parent-led curriculum lProject DOCC(Delivery of Chronic Care) as part of their developmental disabilities rota-tion from 2002-09. In 2012, all participants were contacted by e-mail andasked to voluntarily complete an anonymous on-line qualitative survey re-garding the impact Project DOCC had on their current practice. Areasassessed were changes in attitude toward FCSHCN (attitude), skills to im-prove their relationships with FCSHCN (relationships), and practice changesto assist FCSHCN (practice). Participants selected items from lists providedin the survey and wrote qualitative comments regarding their experiences.Comments were reviewed as favorable (F), neutral (N) or unfavorable (U).Summary of Results: 58 participants (31%) responded. 48 (83%) werecurrently practicing pediatrics. 32 (59%) have been in practice 2-3 years, 17(32%) 4-6 years, and 5 (9%) 7-9 years. A total of 56 comments were received;73%-F, 18%-N, and 9%-U. Of these, 59 percent (76%-F, 9%-N, 15%-U)related to attitude, 21 percent (83%-F, 17%-N, 0%-U) related to relationships,and 20% percent (55%-F, 45%-N, 0%-U) related to practice. Examples ofpositive comments included: ‘‘I realize how a child with a disability affectsthe family’’; neutral: ‘‘Unsure, I can’t think of an example,’’; negative: ‘‘It wasan opportunity to bash doctors.’’Conclusions: A parent-led curriculum designed to enhance residents’ atti-tudes and skills about FCSHCN, and perceived as relevant to their futurepractice, was viewed favorably by pediatricians 2-9 years after receiving theirtraining. The greatest impact was reported in former residents’ attitudes andclinical skills related to the care of FCSHCN. Fewer reported concretechanges in their practices.
353MOCK CODES IN PEDIATRICS RESIDENCY
Cantu R1,2, Keane M1. 1Tulane University, New Orleans, LA and 2Tulane-Ochsner Pediatric Residency Program, New Orleans, LA.Purpose of Study: To assess resident-reported confidence in various rolesof pediatric resuscitation before and after implementation of a mock codecurriculum.
Table 1.
p = 0.15577
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
472 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Methods Used: Anonymous surveys before and after introduction of amock code curriculum.Summary of Results: There was a significant increase in pediatric resi-dents’ confidence in airway management, code leadership, and chest com-pressions after participating in at least one mock code.Conclusions: Mock codes increase resident confidence in pediatric codesituations.
354
EXAMINATION OF PEDIATRIC RESIDENT COMPETENCYWITH SIMULATED PATIENTS FOLLOWING AMOTIVATIONAL INTERVIEWING (MI) TRAINING MODULE
Gillaspy S1, Leffingwell T2, Claborn K2, Miller M2, Meier E1, Cherry A.11University of Oklahoma Health Sciences Center, Oklahoma City, OK and2Oklahoma State University, Stillwater, OK.Purpose of Study: As MI techniques are increasingly recommended forfacilitating behavior change, incorporating MI training into residency cur-riculum is important. In 2010, a Residency Training Grant awarded fromHRSA allowed for the development & implementation of a MI training modulein the peds & med/peds residency program. The purpose of the study is todetermine if residents can demonstrate minimum competency in MI skillsafter completing a MI training class.Methods Used: The MI training was presented to residents (n=52) in a 4 hrclass. Following the training module, trainees completed a MI encounter witha simulated patient. Encounters were coded using the MI Treatment Integrity(MITI), which provides competency ratings on the 5 principal aspects of MI:Collaboration; Evocation; Autonomy; Direction; & Empathy. Residents com-pleted the Behavior Change Counseling Index (BECCI) & simulated patients &
expert observer completed a modified version of the BECCI rating the trainees’performance on the same scale.Summary of Results: Results of the MITI ratings of aspects of MI spirit(rated 1-5), revealed that trainees overall fell short of the minimum compe-tency level of 4 or better on all aspects except Direction. Only 42-48% ofthe trainees met or exceeded the minimum threshold for competency thoughmost with ratings less than 4 were rated a 3. In terms of specific skills, traineesalso asked too few open questions (M=40%, competency threshold = 70% orgreater) & underutilized reflections (Mratio= 0.26:1, competency threshold =2:1). Scores on the BECCI were most similar between observational coder &simulated patients (r=.40, p G.001) & both were significantly correlated withMITI ratings & behavior counts.Conclusions: Although most trainees demonstrated MI skills that approachminimum levels of competency, it is clear that the single training module wasinadequate to ensure competent practice of MI. Results indicate the need forongoing practice & consultation to further develop resident competency inMI. Future research will evaluate resident competency in MI with additionalpractice sessions with simulated patients & personalized feedback on theirsimulated patient encounters.
355
PEDIATRIC ADVOCACY CURRICULUM RESULTS INIMPROVED RESIDENT KNOWLEDGE
Hart N1, Linz A1, Hale J1, Thompson D2, Dunlap M1, Gillaspy S.11University of Oklahoma Health Sciences Center, Oklahoma City, OK and2University of Oklahoma Health Sciences Center, Oklahoma City, OK.Purpose of Study: New proposed ACGME guidelines mandate develop-ment of an advocacy rotation to prepare residents to advocate for the healthof children in their communities. This represents an opportunity to surveyresidents about advocacy, collaborate with community partners, and developa resident advocacy curriculum. This study examined pediatric intern atti-tudes and knowledge regarding advocacy before and after their advocacyrotation.Methods Used: Pediatric interns (n=14) were surveyed anonymously re-garding advocacy topics and ideas at the beginning of their intern year andagain after their advocacy rotation. The interns assessed their ability/pre-paredness by ranking the topics (1-5): 1 (not at all prepared), 3 (somewhatprepared), or 5 (extremely prepared). Responses between surveys were com-pared using exact permutation tests (SAS PROC NPAR1WAY). Funding forthe curriculum development and this study were provided by an AAP Com-munity Partners Training Initiative grant.Summary of Results: At baseline, residents felt ‘‘not at all’’ to ‘‘somewhatprepared’’ regarding advocacy knowledge and issues. After completion oftheir rotation, residents expressed improvement in their preparedness andability for most survey questions. Specifically, residents felt more prepared tobe an advocate for patients (pG0.001), to find community resources forpatients (pG0.001), to provide for special needs of different populations ofchildren (pG0.001), and to describe available child care options for families(pG0.001).Conclusions: Overall, resident responses demonstrated significant im-provement after their advocacy rotation in their preparedness and ability todefine advocacy, to assess patient needs, to identify appropriate communityresources, and to advocate for patients. These responses demonstrate success ofthe initial advocacy curriculum implementation. Future plans include evalua-tion of advocacy knowledge and behavior change as this group of residentscontinues through their training. Information from the resident surveys for thisstudy is being utilized to adapt the current advocacy curriculum.
356
END OF LIFE PATIENTS: DO WE PRESCRIBE TOO MANYMEDICATIONS? A PROSPECTIVE COHORT STUDY INHOSPICE AGENCIES
Munshi NS1, McNulty JP2, Muller GB2, Azevedo BM1, Sullivan DV1,Anwar DM1. 1Tulane University School of Medicine, New Orleans, LA and2Hospice of St. Tammany, Covington, LA.Purpose of Study: Patients referred for hospice care may receive a widerange of medications including some considered futile or redundant. Theobjectives of this study are to assess the number of medications received
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 473
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

by patients when referred to hospice, focusing primarily on futile ones, and toassess if hospice intervention helps to decrease this number.Methods Used: During a six-month period, all consecutive home or nurs-ing home based patients admitted at six Louisiana hospice agencies werefollowed. Demographics, Karnofsky scores, and lists of diagnoses and med-ications were collected at day 1 and 15. Medication lists were ranked in-dividually by two palliative care/hospice physicians and one compoundingpharmacist after which the panel met to achieve consensus rankings. Medi-cations were ranked into five categories: Appropriate, Questionable, Futile,Duplicate, or Insufficient patient data. Tentative guidelines addressing themedications categorized as futile or questionable were established by thepanel.Summary of Results: 397 patient records were analyzed. The median(range) number of medications prior to hospice admission was 7 (0-27). 49%of patients received either futile or duplicate medications, or both. Of themedications ranked futile, 67% were vitamins or minerals while 21% werestatins (n=272). Anticoagulant and antiplatelet medications (36%) and Alz-heimer treatments (18%) were the most prevalent medication classes con-sidered questionable (n=365). 7.3% of patients experienced a reduction inprior-to-admission futile medications at day 15.Conclusions: These data illustrate the significant prevalence of hospicepatients referred with a large number of medications, including several futileor duplicate ones. It is difficult for hospice teams assuming patient care tomake all the necessary changes. Therefore, decreasing the number of medi-cations before referring patients to hospice, focusing on futile or duplicateones, may be beneficial for improving patient comfort, safety, and cost ofcare. Evidence-based data reviewed by the authors to help in this decision-making process will be presented. The findings of this study highlight thebenefits of policy and practice modifications both before and after the transi-tion to hospice care.
357
TO ABORT OR NOT TO ABORT? A CASE OF ETHICALDILEMMA
Narmala SK, Puligothram S, Jahangir KS, Reske TM. LSU Health SciencesCenter, New Orleans, LA.Case Report: Case: A 42-year old woman presented to the emergency de-partment (ED) with complaints of headache, nausea and projectile vomitingfor 3 days. She was worked up in the ED with a CT of the head whichrevealed two areas concerning for hemorrhagic malignant neoplastic pro-cesses, likely metastatic. A subsequent MRI revealed two large masses andseveral smaller ones throughout the brain. A urine pregnancy test was donein the ED that was positive and it was followed up by transvaginal ultra-sound, which showed an intrauterine pregnancy of 9 weeks 2 days gesta-tional age. The patient was admitted and further work up was done, whichincluded a craniotomy for an excisional biopsy of the right temporal lesion.This came back as adenocarcinoma of lung origin. Subsequent imagingshowed a right upper lobe pulmonary nodule compatible with primary pul-monary carcinoma.
The Patient was evaluated by medical oncology, radiation oncology andobstetrics. It was determined that the best course of action for the patient wasto treat with cranial irradiation and chemotherapy, as she wanted everythingpossible done to prolong her life, even if it meant that she had to terminateher pregnancy. The patient was discharged home to follow up with obstetricsto facilitate the abortion. The patient was brought back to the ED a week laterwith new onset generalized tonic clonic seizures resulting from a hemorrhagein the brain met. During this admit, the patient became reluctant about pro-ceeding with the abortion. The ethics committee was consulted to evaluate theissue and discuss the possible implications of either course of action. Thiscommittee met and discussed various social, legal, medical and ethical aspectsthat surrounded the pregnancy and the unborn child. In the end, a decision wasmade to respect the patient’s autonomy and to proceed with pregnancy andcranial irradiation and not start any chemotherapy during the first twotrimesters.
The patient had an uneventful pregnancy and delivered a baby boy at34 weeks of gestation. The patient was started on chemotherapy after thecompletion of the pregnancy, has received two cycles so far and continues todo well. This was a most interesting case from an ethical standpoint and il-lustrates management of a patient with a perplexing ethical problem.
358
ETHICAL DILEMMA: WHEN A PATIENT REFUSES LIFESAVING THERAPY
Coleman-Pieron R, Kemp N, Prabhakar A, Engel LS. LSU Health SciencesCenter, New Orleans, LA.Case Report: Case: A 42 year old woman who was a Jehovah’s Witnesswith history of SLE, hypertension, diabetes mellitus type 2, and hypothy-roidism presented after having a syncopal episode following a one weekhistory of daily nausea, vomiting and diarrhea. Initially, the patient wasthought to be volume depleted and was fluid resuscitated with normal saline.After resuscitation, the patient’s hemoglobin and hematocrit dropped from10.8 and 32.1 to 7.3 and 22.1. She was found to be fecal occult blood positiveand iron studies suggested anemia of chronic disease. Given the patient’sreligious beliefs, she was started on erythropoietin, iron, vitamin B12, andfolate supplements. She was later found to have a right lower extremity deepvein thrombosis and an IVC filer was placed. Two days later, she becametachypnic and workup for pulmonary embolism in the ICU was negative.While in the ICU, her hemoglobin and hematocrit slowly decreased and heroverall condition worsened. The patient maintained her refusal of blood pro-ducts secondary to her religious beliefs. Lab draws were minimalized. Workupfor hemolysis, HIV, Parvovirus, and Hepatitis were negative. Rheumatologywas consulted and treated the patient with IV steroids for possible lupus flare.Reticulocyte count was inadequate for anemia. A bone marrow biopsy wasnot done given the patient’s clinical state. The patient was made comfortableuntil her death.
Discussion: Over one million active Jehovah’s witnesses live in NorthAmerica. Devout Witnesses will not accept transfusion of whole blood or anyother blood products. Due to the First Amendment’s right of religious free-dom, patients have the right to refuse lifesaving medical therapy due toreligious preferences. After extensive communication with the patient andher family, this Jehovah’s Witness was found to be an adult capable ofmaking her own decisions with full awareness of the consequences. Legallyand ethically, there was no other course of action but to respect the pa-tient’s autonomy and withhold a measure that would have likely prolongedher life.
Neurology and NeurobiologyConcurrent Session
2:00 PMFriday, February 22, 2013359
ASEPTIC MENINGITIS, RASH, AND ACUTE URINARYRETENTION: A CLUE FOR DIAGNOSIS OF WEST NILEVIRUS MENINGITIS
Mankongpaisarnrung C, Chen T, Copeland S, Nusrat M, Argueta E, Nugent K.Texas Tech University Health Sciences Center (TTUHSC), Lubbock, TX.Case Report: West Nile virus (WNV) is an RNA arbovirus in Flaviviridaefamily. It has become more prevalent in the US since the 1999 outbreakin NY. The mode of transmission is primarily from the Culex mosquito bite.However, non-mosquito transmission is feasible through blood transfu-sion, solid organ transplant, and trans-placental route. Of infected humans,70-80% are asymptomatic and 20-30 % develop West Nile Fever (WNF).
A previously healthy 26-year-old man presented with high-grade fever,chills, headache, nausea, vomiting, severe body aches, and a rash for a weekafter being in Denton, Texas. He then started to have suprapubic pain and acuteurinary retention (AUR) for 2 days. He was recently diagnosed with Strepto-coccal pharyngitis, and he broke into rash after amoxicillin given. However,EBV infection was tested negative. Initially, his vitals were unremarkableexcept tempertaure 103.9-F. He was in acutely ill and was shivering. Macu-lopapular rash was present over his body and both cheeks. Full urinary blad-der was palpable. Neurological examination was intact except positive nuchalrigidity and 3+ DTR. Bladder catheterization drained 1400 ml of urine. CTofthe brain was unremarkable. Lumbar puncture was performed with openingpressure of 16 cmH2O. CSF analysis showed elevated WBC of 225 (N 54%,L 45%) with elevated protein of 115 mg/dL, normal glucose of 60 mg/dL. He
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
474 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

was diagnosed with aseptic meningitis. Broad-spectrum antibiotics and anti-virals were started promptly. MRI of the brain and spinal cord were performedfor AUR workup but unremarkable. Blood and CSF WNV IgM became pos-itive. The antibiotics were discontinued; his AUR resolved.
This case highlights an unusual presentation of WNV meningitis withAUR. Less than 1% with WNV presents with neuroinvasive disease. Rashoccurs in 20-30% of cases. Based on one previous case report, we hypoth-esize that AUR could have been from viral myelitis, which resolved in thiscase. Even though the mainstay treatment of WNV infection is supportivetreatment, treatable causes of aseptic meningitis should be treated empiricallyduring workup. The suspicion of WNV meningitis should be raised in asepticmeningitis patient with new-onset acute urinary retention and rash.
360
A LINGERING PATHWAY FOR A POSTERIOR CIRCULATIONSTROKE
Martinez RC1, Vidal G2,1, Luka J.3 1Louisiana State University, NewOrleans, LA; 2Ochsner Medical Center, New Orleans, LA and 3TulaneUniversity, New Orleans, LA.Case Report: A 46-year-old male presented with a two day history ofpressure-like, frontal headache and bilateral retro-orbital pain. Symptomswere associated with nausea, generalized weakness, disorientation, and visualfield deficit. Past medical history included hyperlipidemia and Hodgkin’slymphoma in remission. Physical exam was significant for a blood pressureof 162/100 and a right homonymous hemianopsia. Laboratory studiesreported triglycerides 205, HDL 27, LDL 106. A head CT scan showed asubacute infarct in the left parietal-occipital lobe. Carotid ultrasound revealeda right carotid artery stenosis of 60-70% and a hypo-echoic, calcified plaquein the mid-right internal carotid artery. Brain MRI demonstrated a large areaof restricted diffusion signal abnormality (6.2cm x 4.1cm) involving the leftoccipital lobe consistent with acute infarction. The head and neck CT angi-ography (CTA) identified a persistent trigeminal artery arising from the rightinternal carotid artery prior to its cavernous portion supplying the distalbasilar artery. The P3 segment of the left posterior cerebral artery was notvisualized and a 1.5cm stenosed segment was evident distal to the rightinternal carotid origin.
The persistent trigeminal artery (PTA) is one of the four carotid-vertebro-basilar anastomosis derived from the embryonic development of the circle ofWillis. These transitory structures seldom persist into adulthood. The PTA isthe most frequently reported with an incidence of 0.1%-0.6%. If a PTApersists, a less than normal amount of blood will be carried to the ipsilateralposterior communicating artery from the ICA to the basilar artery. The vas-cular flow is re-routed with the blood coursing from the PTA to the carotidartery and then to the mid-basilar. Consequently, the PTA supplies distally tothe superior cerebellar and posterior cerebral arteries. In the course of thisflow, the PTA has the potential to serve as a conduit of an embolus from thecarotid artery distribution into the posterior circulation, in our case, into thecontralateral territory. Thus, the presence of a PTA may in fact predisposeindividuals to ischemia in the presence of arterial obstructive disease.
361
ANOTHER CHILD WITH A MIGRAINE, OR IS ITSOMETHING ELSE?
Peek ML, Puri V. University of Louisville, Louisville, KY.Case Report: Introduction: Children frequently present to the emergencydepartment complaining of headaches with or without focal neurologicalfindings. Often, the neurological findings resolve prior to arrival or shortlyafter arrival to the ED. It is left to the ED clinician to determine which patientscan be treated and which need additional work-up to determine the etiology.
Case Description: A.D. is a previously healthy nine year old male whowoke up with a headache. After arriving home from school, he developedexpressive and motor aphasia, transient bilateral arm weakness, right facialdroop, difficulty speaking, and decreased proprioception. Upon presentationto the ED, he had slight blunting of his right nasolabial fold, a sensationdeficit in his distal right upper extremity, and a slight pronator drift on hisright. Within an hour, his neurological deficits had resolved. An MRI andMRA showed no flow signal in the left internal carotid artery, proximal leftmiddle and anterior cerebral arteries. A CT angiography of the head and
neck showed an asymmetry in size of the common and internal carotid ar-teries, with the right being greater than the left. He was started on anti-coagulation and discharged from the hospital once stable. Subsequently, hismother recalled an incident three days prior to admission where hewas jumpingon his trampoline at home and fell and hit his neck. An outpatient angiographyof the brain showed a dissection of the left internal carotid artery distally. Itwas determined that he had a carotid dissection secondary to trauma whichpresented as a transient ischemic attack.
Discussion: This case underscores the difficulty in clinically distinguish-ing a complex migraine from a TIA in the pediatric population. In pediatricpatients who present with focal neurological findings, a TIA should be in-cluded in the differential and the appropriate studies should be conducted todetermine the etiology of the neurological deficits. Since this is such a rareoccurrence, there is not a substantial amount of data available to assist theclinician in determining the best treatment course. For our patient, a combi-nation of Low Molecular Weight Heparin, Coumadin, and Aspirin in additionto consultation with a pediatric neurologist has been successful in preventingfurther neurologic insult.
362
PATHOLOGIC LAUGHING AND CRYING DUE TOMULTIFOCAL SMALLVESSEL ISCHEMIA: A CASE REPORT
Hidarilak N, Issa A, Blaya M. Tulane University, New Orleans, LA.Case Report: Pseudobulbar affect (PBA) which is characterized by invol-untary and inappropriate outbursts of laughter and/or crying is an affectivedisinhibition syndrome associated with various neuropathologies. We reporta case of PBA in a patient due to multifocal small vessel ischemia.
A 56-year-old right-handed African American male with the past medicalhistory of hypertension and stroke with the mild residual weakness wasbrought to the hospital after collapsing to the ground. Recently, his brothernoted that he has developed slurred speech, general weakness, and change ofmental status as frequent uncontrolled laughing/crying spells for no appar-ent reason. His family history was significant for stroke and chronic kidneyinjury.
On initial presentation, vital signs and physical examination were essen-tially within normal limits. However, his neurological examination was sig-nificant for disorientation to time; labile affect with sudden outbursts ofinvoluntary, exaggerated laughter and/or crying to questions; nasal dysar-thria; and mild decreased strength in left upper and lower extremities from theprevious stroke. Laboratory work-up was negative. Brain MRI revealed mul-tifocal small vessel ischemia with related atrophy, and severe chronic hyper-tensive brain injuries. He was ruled out for a new onset of cerebrovascularaccident.
Although the mechanisms of pathological laughing and crying remainunknown, that is a frequent problem in patients with brain ischemia. The PBAsyndrome which can be socially and occupationally disabling should not beoverlooked by physicians.
363
FULMINANT LEWY BODY DISEASE: AN UNUSUAL CASEREPORT
Hidarilak N, Blaya M. Tulane University, New Orleans, LA.Case Report: A 53 yr old male was admitted to the hospital for mentalstatus change, gait imbalance and dizziness. His initial symptoms were head-ache, and nausea which started 2 months before the admission and was diag-nosed and treated as acute sinusitis. He later developed an unsteady gait,memory loss and visual hallucination. His family reported the couple emer-gency visits and admissions due to worsening of memory loss and ataxia.In each admission, He was ruled out for stroke, encephalitis and transientglobal amnesia.
His mother had a history of Alzheimer at age of 60. The physical examwas positive for fluctuation in orientation and alertness; rotational nystagmus;positive finger-to-nose dysmetria; positive heel-to-shin dysmetria, positiveRomberg test; and ataxia. He was initiated on acyclovir and ampicillin withpossible diagnosis of rhombencephalitis vs. Creutzfeldt-Jakob disease (CJD)vs. paraneoplastic neurologic syndrome . An extensive work up included brainCT; brain MRI; autoimmune, virology, and bacteriology tests; and paraneoplas-tic biomarkers was normal, except cerebral spinal fluid (CSF) analysis which
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 475
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

revealedWBC of 15 (97% lymphocytes) and protein of 89.2 mg/ml. HoweverCSF- viral and bacterial studies as well as protein 14-3-3 were negative.
The patient had a wax and wane pattern of symptoms at the hospi-tal course. He was discharged with close follow up. However, 5 months later,he passed away in another hospital with unknown cause of death. The autopsyrevealed numerous Lewy bodies and lewy neuritis in the neocortex, and brainstem.
In our opinion, this case illustrates a fulminant Lewy body disease (LBD).Extremely rapid disease progression, leading to death in 5 months is highlyunusual for DLB. In fact, this fulminant course appeared consistent withsporadic CJD. However, we as physician should be aware of all varieties ofa disease.
364
A MYSTERIOUS CASE: CHRONIC LYMPHOCYTICINFLAMMATION WITH PONTINE PERIVASCULARENHANCEMENT RESPONSIVE TO STEROIDS (CLIPPERS)SYNDROME
Hidarilak N, Traylor A. Tulane University, New Orleans, LA.Case Report: Chronic lymphocytic inflammation with pontine perivascularenhancement responsive to steroids (CLIPPERS) is a newly named pontine-centric inflammatory disorder with a predilection for the hindbrain and re-sponsive to immunotherapy. We report a 53 year old female who presentedwith the features of CLIPPER.
The disease started at the age of 52 years with left sided body weak-ness and gait ataxia. Her initial physical exam showed no evidence of subtlesystemic involvement. The brain MRI showed T2 hyperintensity with con-trast enhancement on the posterior margin of the lower pons, and moderatelydense patchy contrast enhancement within the lesion concerning a broad dif-ferential diagnosis including CNS lymphoma vs. neurosarcoidosis vs. inflam-matory diseases. However neurosurgery avoided a brain biopsy due to locationof the lesion and symptoms were attenuated with a dose of decadron.
Later on, she successively developed other brainstem symptoms includ-ing diplopia, gait ataxia, dysartheria and right sided facial numbness. Ex-tensive laboratory investigations were normal or negative for any possible viral/bacterial/fungal infection; multiple sclerosis; sarcoidosis. Spinal MRI and ce-rebral angiography alsowere normal. She was started on steroid and the follow-up MRI showed partial resolution of contrast enhancement.
3 months later, she was admitted with a rapidly progressive right occularpalsy associated with gait ataxia, dysarthria, and tetraparesia. With the possiblenon-infectious inflammatory disease, empiric immunomodulatory treatment(azathioprine and oral prednisone) was started. The symptoms improveddramatically with mild persistent spastic ataxia and remained relapse freeduring the subsequent 5 months. The last brain MRI showed spectacularimprovement in size of lesions.
The CLIPPERS appears to be clinical overlap with other brainstem pre-dominant pathologies. Therefore neurologists should be aware of the con-dition and the typical manifestations as prompt and appropriate treatmentmay limit permanent neurological sequelae. Our report suggests that patientswith clinical and MRI features typical of CLIPPERS could be treated withoutpathological examination, after excluding differential diagnosis.
365
A CASE OF MYASTHENIA GRAVIS IN AN ADOLESCENT
Sicard C, Stephenson LR, Thomas WH, Holley K, Bocchini J. LSU HealthShreveport, Shreveport, LA.Case Report: Myasthenia Gravis is an uncommon clinical entity in child-hood and adolescence characterized by several neurologic findings, includingprogressive muscle weakness, ptosis, and diplopia. In addition, the treatmentregimen is lifelong, and requires frequent adjustments.
Our patient is an obese 15 year old female, who presents to our hospitalafter a prolonged stay at an outside facility. She initially presented with a one-week history of diplopia, ataxia, headache, and occasional full body tremors.The patient’s symptoms started abruptly, and most concerning was the ataxiaand diplopia. The patient had a full neurologic workup at the outside hospital,including MRI and EEG, which were normal. She had a positive rapid streptest, ASO, and Anti-DNase B titers. Therefore, the patient was treated for, anddischarged with, a diagnosis of PANDAS. Her mother felt that her clinical
status was deteriorating, so she brought the patient to our facility for a secondopinion. On initial exam, she was found to have prominent ptosis and eso-tropia of the left eye, generalized weakness, and full body tremors. She wasevaluated by pediatric neurology and subsequent diagnoses were suggested.Several diagnostic recommendations were made, including a Tensilon test anda lumbar puncture. The LP was performed, and results were negative formeningitis. The Tensilon test showed immediate improvement in the patient’ssymptoms, suggestive of a diagnosis of Myasthenia Gravis. She was thenstarted on pyridostigmine, and the dose was titrated up to effect. A CT of herchest showed a small amount of nonspecific retrosternal soft tissue, nega-tive for thymoma. The patient was doing well upon discharge, but did returnsoon after with a recurrence of symptoms at home. The patient then received5 days of IVIG, in addition to an increase in her pyridostigmine dose. Shecontinued to have mild symptoms, including ptosis and tremors, so steroidswere initiated, and the patient was discharged home with a tapered dose ofsteroids. Symptoms continued to improve.
This case illustrates the elusive diagnosis and difficult treatment of a childwith myasthenia gravis, which can be found with careful history and detailedneurologic exam.
366
SEVERE HEADACHE WITH BLURRYVISION _ INTRACRANIAL HYPERTENSION ORHYPOTENSION
Panikkath R, Lik Lim S, Nusrat M, Lado J. TTUHSC, Lubbock, TX.Case Report: Introduction
Intracranial hypertension and hypotension are on the opposite ends ofthe CSF pressure spectrum, but both can cause headaches. However it is un-common for both to occur in the same patient.
MethodsThis is a case report of a patient who developed intracranial hypotension
after lumbar puncture for intracranial hypertension.ResultsA 36 year old man presented with history of diffuse headache, 3/10 in
intensity, constant and associated with blurry vision. He was afebrile with nofocal neurological signs or signs of meningitis. His blood pressure was nor-mal. Both brain CT and MRI (with and without contrast) were unremarkableshowing normal sized ventricles without meningeal enhancement. Ocular fun-doscopy revealed bilateral papilledema. Lumbar puncture showed a cerebro-spinal fluid (CSF) opening pressure of 44cm. CSF analysis showed protein22 mg/dl, glucose 54 mg/dl and 3 lymphocytes. A diagnosis of idiopathicintracranial hypertension was made. However post lumbar puncture thecharacter and intensity of headache changed with excruciating headache inupright position and relief in supine position. Post dural puncture headachewas suspected. Patient did not get relief with conventional medical manage-ment, including caffeine. A contrast enhanced MRI of brain and spine showeddiffuse pachymeningeal enhancement suggestive of intracranial hypotension.An epidural blood patch was performed which relieved the headache within ashort time. Patient did not have recurrence of headache on assuming uprightposition subsequently nor did he have any neurological deterioration after theprocedure.
ConclusionRepeated lumbar puncture or cerebrospinal fluid shunts are considered
the treatment of choice for idiopathic intracranial hypertension. However it isparadoxical that in such a patient, headache developed due to intracranialhypotension after lumbar puncture and got relieved by an epidural bloodpatch. To our knowledge, this is the first case where a male patient (and thirdcase in adults) with idiopathic intracranial hypertension developed intracra-nial hypotension after lumbar puncture with complete symptomatic im-provement after an epidural blood patch.
367
ACHALASIA IN ACUTE PANDYSAUTONOMIC NEUROPATHY
Hiebert R, DeLeon S. University of Oklahoma, Oklahoma City, OK.Purpose of Study: To present an interesting case of achalasiaMethods Used: Literature reviewSummary of Results: The incidence of achalasia is 1/100,000 in the gen-eral population and significantly more unusual in children.We present a 15 year
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
476 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

old female with acute onset achalasia, along with several neurologic mani-festations including tonic pupil, orthostatic hypotension, diffuse allodynia,and urinary/fecal incontinence concerning for acute pandysautonomic neu-ropathy. Only one case of achalasia from pandysautonomic neuropathy hasbeen reported in the literature.
Our patient was a previously healthy 15 year old female who presentedinitially to the ED with diffuse myalgias and chills. She was diagnosed with aviral illness, but over the next week returned twice with progressive symp-toms including anorexia, insomnia, erythematous maculopapular rash on theforehead, and pain and dizziness limiting ambulation. She followed up withPCP and was found to have right anisocoria. She was hospitalized immedi-ately with a tonic right pupil; she then had rapid progression of symptomsincluding straining with urination, severe diffuse allodynia, orthostatic hy-potension, and difficulty swallowing. Dysphagiogram revealed delayedswallow reflex, and the following day she suffered an aspiration event. CTchest demonstrated a grossly distended esophagus filled with particulate mat-ter concerning for achalasia.
She further developed fecal incontinence, severe nausea, and requirednutritional support with TPN. Her respiratory status began to deteriorate untilshe was transferred to the PICU emergently for further support. Among herextensive work up she was found to have an increased CSF protein of 78 onher second LP. Based on her unique and multi-system symptoms, she wasdiagnosed with acute pandysautonomic neuropathy. She began therapy withIVIG, but after 6 doses had not significantly improved. She was also givensteroids without significant improvement. Management was then focused onsymptom control and treatment. Our patient was eventually discharged homefor follow-up with intense outpatient PT, OT, and speech therapy. Only 1/3 ofthese patients with pandysautonomic neuropathy will improve substantiallyover several months, while treatment with IVIG has shown variable results.Conclusions: Achalasia is a rare occurrence in pediatrics with an uncom-mon presentation in pandysautonomic neuropathy.
Perinatal Medicine IConcurrent Session
2:00 PMFriday, February 22, 2013368
ORAL FEEDING WITH LACTOBACILLUS RHAMNOSUSGG INCREASES INTESTINAL EPITHELIUM CELLPROLIFERATION IN IMMATURE MICE
Richardson A, Patel RM, Myers L, Denning P. Emory University, Atlanta, GA.Purpose of Study: Recent clinical trails suggest that oral administrationof probiotics reduces the risk of necrotizing enterocolitis (NEC) in pretermneonates, but the mechanism behind this is largely unknown. The intestinalepithelial cell (IEC) proliferative response is essential for repair and func-tional recovery from injury. Murine models indicate that commensal bacteria,especially Lactobacillus species can increase IEC proliferation via activationof ERK MAPK pathways. The aim of this study is to investigate the roleof live and heat-killed Lactobacillus rhamnosus GG (LGG) in immaturemouse IEC proliferation and its potential to mitigate NEC in affected infants.We hypothesize that oral feeding of live or heat-killed LGG increases IECproliferation in mouse pups.Methods Used: Two-week-old mouse pups were administered phosphatebuffered saline (PBS) with or without live or heat-killed LGG via oral gavage.Animals were sacrificed 4 h post-treatment and intestines were excised for IECproliferation analysis. Patterns of IEC proliferation were assessed by immu-nohistochemical staining for Ki67. To confirm ERKMAPK pathway activationIEC samples were probed for phospho-ERK (pERK) using SDS-PAGEWestern immunoblot.Summary of Results: IEC proliferation in proximal small intestine, distalsmall intestine and colon was significantly higher (PG0.05) in animals ad-ministered LGG than in those given the PBS vehicle only. The highest in-crease in IEC proliferation after LGG administration was observed in thecolon (8.193T0.227 vs. 14.17T0.421 cells per crypt; pG0.0001), followed bythe distal small intestine (8.380T0.130 vs.12.87T0.208; pG0.0001) and theproximal small intestine (11.34T0.209 vs. 13.46T0.574; pG0.001), respec-tively. pERK was expressed in proximal small intestine, distal small intestine,and colon samples of animals given live or heat-killed LGG.
Conclusions: The results indicate that either live or heath-killed LGG canincrease IEC proliferation via activation of ERK MAPK pathway in imma-ture mice. We speculate that LGG may prevent NEC by improving intestinalepithelial repair following injury. Because the safety of oral administration oflive probiotics to human infants is a concern, heat-killed probiotics withsimilar efficacy may be a better option for NEC treatment.
369
INTER-ALPHA INHIBITOR PROTEIN REDUCES THE TOXICEFFECTS OF EXTRACELLULAR HISTONES
Chaaban H1, Keshari RS2, Lim Y3, Lupu F2. 1Oklahoma University HealthSciences Center, Oklahoma, OK; 2Oklahoma Medical Research Foundation,Oklahoma, OK and 3Prothera Biologics, East Providence, RI.Purpose of Study: Histones released during sepsis and trauma are cyto-toxic, thrombogenic,and contribute organ failure and death.In vitro, histonescytotoxicity is significantly decreased in presence of plasma.Inter-alpha In-hibitor Proteins (IAIP) are abundant serine protease inhibitors that are pro-tective in neonatal sepsis.We hypothesize that IAIP reduces histones inducedcytotoxicity.Methods Used: Histones (50Kg/ml) were incubated with HL60 cells in thepresence or absence of IAIP (25,50,100Kg/ml) for 1 hr at 37-C.Cell damagewas measured by flow cytometry using propidium iodide staining. Plateletaggregation induced by histones with/without preincubation with IAIP wasdetermined by Aggregometery.ADP and heparin were used as positive or nega-tive control agonists,respectively. Statistical analysis was performed using Prismsoftware.One-way ANOVA tests were used to determine significance.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 477
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: IAIP significantly reduced histone induced cyto-toxicity compared to control(60 +/- 1.4 % vs 17.23 +/- 1.8 %,P G0.0001) ina concentration dependent manner (Fig 1).Similarly, platelet aggregation in-duced by histones was inhibited by IAIP as efficiently as heparin, an estab-lished histone inhibitor.Conclusions: These results suggest a novel role for IAIP in neutralizationof histone-induced cytotoxicity and highlight the use of IAIP as a potentiallyefficient therapeutic agent for organ failure after acute inflammation, sepsisand trauma.
370
THE ROLE OF T CELLS IN A MODEL OF NEONATALGRAM-NEGATIVE SEPSIS
Turner KM, Blosser EG, Randolph DA. University of Alabama, Birmingham,Birmingham, AL.Purpose of Study: Sepsis is a leading cause of morbidity and mortalityin the neonatal ICU. T cells, which usually are only activated clonally in anexquisitely specific fashion, are polyclonally activated during sepsis. In adults,polyclonal activation of Th1 and Th17 memory populations may contributeto the inflammatory cytokine milieu seen in sepsis. Neonates, however, lackthese T cell subsets and have only naBve and regulatory (Treg) populations.We sought to define the role of T cells in neonatal sepsis using a mouse modelof Gram-negative sepsis.Methods Used: 7 day-old wild-type (WT) C57BJ/6 and TCR>-/-$-/- pupsor adults were given intracardiac injections K. pneumoniae (10e2 CFU) andthen were treated with gentamicin beginning at 16 hours post infection. In someexperiments, Tregs were depleted prior to infection using an anti-CD25 an-tibody. Serum cytokines were measured by multiplex array and mortality curveswere generated. Splenocytes were collected 24h post infection, stained forT cell activation markers (CD69, CD62L, and CD25), and examined usingflow cytometry. RNA was isolated from splenic CD4 T cells 24 hours postinfection, and gene expression was analyzed by real time PCR.Summary of Results: Infected WT pups demonstrated polyclonal CD4 andCD8 T cell activation. Neonatal T cells from septic animals showed increasedIL-2 and IL-10 expression, consistent with activation of naBve and regulatorypopulations. Survival for TCR>-/-$-/- pups was significantly higher than forWT pups (pG0.01). Increased survival in the TCR>-/-$-/- pups correlatedwith more rapid induction of inflammatory cytokines (TNF->, IL-1, IL-6, IL-10, MCP-1) and lower pathogen burdens suggesting that T cells dampen theearly response of other components of the immune system. Depletion of Tregsin WT pups resulted in increased survival (pG0.05) that was also associatedwith higher levels of early inflammatory cytokine production.Conclusions: Neonatal T cells are polyclonally activated during sepsis andcontribute to mortality. Lack of T cells or depletion of Tregs is associatedwith increased inflammatory cytokines early during neonatal infection and im-proved survival. Manipulation of T cell function may offer a novel therapeuticapproach in neonatal sepsis.
371
INTERLEUKIN-10 REDUCES NEC INCIDENCE BYBLOCKING INTESTINAL PRO-INFLAMMATORY CYTOKINEPRODUCTION IN A MURINE MODEL
Jakaitis BM, Myers LE, Denning TL, Denning PW. Emory University SOM,Atlanta, GA.Purpose of Study: Necrotizing enterocolitis (NEC) is one of the mostdevastating diseases of prematurity. The anti-inflammatory cytokine, IL-10,has been postulated to play a protective role. However, the mechanisms ofaction and primary sources of IL-10 in the developing gut are uknown. Here,we investigated whether blocking the IL-10 receptor would increase the in-cidence of NEC by enhancing pro-inflammatory cytokine production in amurine NEC model.Methods Used: We injected 2 week old C57BL/6J mice with 100Kg ofanti-IL-10 receptor antibody (anti-IL-10R Ab) or carrier control intraperi-toneally (IP) 24 hours and 0 hours prior to NEC induction. We induced NECwith a single IP injection of two key pathogenic mediators of NEC, plate-let activating factor (100Kg/kg) and lipopolysaccharide (1mg/kg). Two hourslater, mice were sacrificed and distal small intestines isolated for RNA iso-lation and H&E stain. Intestinal expression of the key pro-inflammatory
cytokines, IL-6 and TNF->, was assessed by qRT-PCR. NEC incidence wasdetermined by histologic severity score (NEC defined as score Q2).Summary of Results: Mice subjected to NEC induction demonstratedstable intestinal IL-6 mRNA expression and a 15-fold increase in intestinalTNF-> mRNA expression compared to untreated controls. Mice treated withanti-IL-10R Ab prior to NEC induction demonstrated increased mRNA ex-pression of both IL-6 (3 fold) and TNF-> (6-fold) when compared to miceundergoing NEC induction alone. Further, mice were more susceptible toNEC as determined by histologic score if pretreated with anti-IL-10R Ab(100% incidence) when compared to those pretreated with carrier alone (75%incidence).Conclusions: Blockade of IL-10 action by administration of anti-IL-10R Abincreased the incidence of NEC and intestinal pro-inflammatory cytokineexpression in a murine model. These results suggest that IL-10 may play akey role in regulating the intestinal inflammatory response in the immatureintestine. We speculate that lack of endogenous IL-10 may predispose pre-term infants to NEC. Future experiments using genetically modified mice willelucidate both the source and ontogeny of intestinal IL-10 production so thattargeted therapies or preventive strategies can be developed for this devas-tating disease.
372
PULMONARY SURFACTANT PROTEIN A REDUCESADVERSE OUTCOMES IN A RAT PUP MODEL OFNECROTIZING ENTERCOLITIS
Quintanilla HD, Alcorn J, Liu Y, Atkins C, Rhoads J. University of TexasHealth Science Center at Houston, Houston, TX.Purpose of Study: Necrotizing Enterocolitis (NEC) may result from anexaggerated inflammatory response of the premature intestine to environmen-tal insults. Mouse pups deficient in pulmonary surfactant protein A (SP-A)present with a pathology resembling NEC when raised in a bacteria-ladenenvironment. We hypothesized that SP-A would prevent or ameliorate thedevelopment of NEC induced by episodic hypoxia treatment in formula-fedSprague-Dawley rat pups.Methods Used: Formula-fed (F) and NEC (Formula-fed Hypoxia, FH) pupswere gavaged daily with and without purified SP-A (5 mcg). The severity of NECin ileal sections of surviving pups was assessed by histological examination.Summary of Results: Survival in FH group was 65 % (13/20) compared to95% (1/20) in the hypoxic pups treated with SP-A (FHS). 61% of FH pupshad NEC, while NEC was significantly reduced upon SP-A treatment (FHS)(15%), P = 0.021. SP-A significantly reduced Toll-like receptor 4 expressionin the gut of FHS pups compared to FH (P G0.001). In addition, levels of IL-4,IL-5 and IFN-F in FH pups were reduced 2-fold in the gut of FHS pups.Conclusions: These results suggest that administration of purified humanSP-A may ameliorate the complications of NEC by reducing the inflamma-tory environment and modulating Toll-like receptor 4 levels in the gut.
Histological scoring among groups
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
478 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

373
GASTRIC RESIDUAL MEASUREMENT BY OSMOLALITYAND REFRACTOMETRY AS AN INDICATOR OF FEEDINGINTOLERANCE AND/OR GASTROINTESTINAL DISEASEIN THE NICU POPULATION: A PILOT STUDY
Havener K, Radmacher P, Adamkin D. University of Louisville, Louisville, KY.Purpose of Study: Feeding intolerance is a well known diagnosis amongneonatal care but is nonspecific and not predictive of an impending diagnosisof necrotizing enterocolitis (NEC). The purpose of this study was to estab-lish osmolality and refractory index (RI) values of gastric aspirates in criti-cally ill infants exhibiting symptoms of feeding intolerance.Methods Used: Gastric residuals obtained at the time feeding intolerancewere noted by the bedside nurse were analyzed for RI and osmolality. Clinicaldata included estimated and corrected gestational age (EGA and CGA, re-spectively), birth weight, current medications, feeding type and known diag-noses. After the specimen was collected, overall clinical status was monitoredfor possible correlation to the development of NEC, continued intolerance tofeedings, or resolution of symptoms. Cohorts were constructed based on CGAG29 weeks, 29-32 weeks and 932 weeks, denoted as groups 1 (n=13), 2 (n=20)and 3 (n=19), respectively. Data analysis was conducted with SPSS v. 20.Summary of Results: Seventy specimens were analyzed from 46 differ-ent infants. Mean RI values were 5.78T2.74, 5.38T3.64 and 3.59T2.64, fromgroups 1, 2 and 3 respectively. Mean osmolality values (mOsm/kg H2O) were447T330, 310T69 and 347T69. There were no statistical differences in RI orosmolality results when grouped by CGA. Of the 70 samples collected, 12were from 8 infants who exhibited pneumatosis intestinalis on radiographs orwere diagnosed with NEC near the time of sample collection. Mean RI andosmolality values for this group were 4.9T3.9 and 298T62, respectively. Therewas no statistical difference in the RI or osmolalities of those samples com-pared to infants without that finding or diagnosis.Conclusions: Overall, there appears to be no correlation between osmolalityand RI in infants displaying signs of feeding intolerance. Except for a fewoutliers, the osmolality of gastric residuals remained well within the recom-mended AAP guidelines for formula osmolality, even for infants with activeor impending NEC, suggesting that osmolality is unlikely to be a factor infeeding intolerance. Although not statistically significant, the trend for theosmolality to be lower at a more mature gestational age is intriguing.
374
EVALUATION OF THE EFFECTS OF URSODIOL FOR THETREATMENT OF PARENTERAL NUTRITION ASSOCIATEDCHOLESTASIS IN THE NEONATAL POPULATION
Naik M1, Domonoske C1, Graves A1, Khan A2. 1Children’s MemorialHermann Hospital, Houston, TX and 2University of Texas Health ScienceCenter at Houston, Houston, TX.Purpose of Study: The purpose of this study was to evaluate the effects ofursodiol for the treatment of parenteral nutrition associated cholestasis(PNAC) in the neonatal population.Methods Used: This was a retrospective observational study that includedpatients admitted to the neonatal intensive care unit at Children’s MemorialHermann Hospital who received ursodiol for PNAC from September 1, 2008to August 31, 2011. Patients were excluded if they received ursodiol for G7 daysor if they had metabolic or autoimmune diseases, viral infectious diseasesor hypoxic ischemic encephalopathy.Summary of Results: 66 patients were enrolled. The mean birth weightwas 1.24 T 0.8 kg and gestational age at birth was 28.8 T 4.6 wks. At the timeof ursodiol initiation, the mean age was 76 T 40 days, weight 2.83 T 1.37 kgand corrected gestational age 39.3 T 6.7 wks. Baseline liver function tests, withthe exception of albumin, were elevated in all patients. The average duration ofparenteral nutrition prior to initiation of ursodiol was 66 T 40 days. Theaverage ursodiol dose was 25 T 5 mg/kg/day given for an average of 42 days.
During the first month of ursodiol therapy, there was an overall slight risein direct bilirubin (Dbili) levels. During months 2 and 3 of therapy, there wasa 38% and 13% reduction in the average Dbili levels respectively. In sub-sequent months, there was a rise in Dbili levels. Of note, Dbili reductionswere greater in patients who also received increasing amounts enteral feed-ings. Average aspartate aminotransferase and alanine aminotransferase valuesrose throughout the duration of ursodiol therapy. Average alkaline phos-
phatase values fluctuated and remained above normal throughout the durationof ursodiol therapy. Side effects were not observed with ursodiol therapy.Other strategies to treat PNAC (i.e. lipid minimalization,etc) were not utilizedduring this time period.Conclusions: This study showed limited evidence on the efficacy of urso-diol for the treatment of PNAC in neonatal patients.
375
DIFFERENCES BETWEEN NEONATAL AND ADULTNEUTROPHILS DUE TO MATURATIONAL DEVELOPMENT
Eckert J, Lawrence SM, Pereira A. The University of Oklahoma HealthSciences Center, Oklahoma City, OK.Purpose of Study: Neonatal neutrophils are known to have quantitative andqualitative defects including impairments of chemotaxis, rolling adhesion,and margination. We have shown through analysis of RNA markers that fol-lowing delivery, neonates have more immature circulating neutrophils thanadults. Thus, we want to determine: (1) if there was a difference based ondelivery method (vaginal vs. Cesarean Section) and (2) if microbicidal pro-tein production was increased in neonates as compared to adults.Methods Used: We isolated neonatal neutrophils from cord blood and adultneutrophils by venipuncture. We next labeled the cells as per Fujimoto et al(Cytometry 2000) and determined the percentage of immature to mature cellsvia flow cytometry and CBC with manual differentials. We then verified ma-turational stage of neutrophil development by determining neutrophil granuleRNA production via Luminex QuantiGene Plex Assays and determined pro-tein concentration via ELISA.Summary of Results: Flow cytometry and complete blood counts withmanual differential show a trend towards more immature neutrophils inneonates as compared to adults, which is most likely due to small sample size.There was no difference in regards to delivery method. Preliminary studiesshow a 1.5 times increase in >-defensin protein concentration in neonatalneutrophils as compared to adults. We are currently analyzing protein con-centrations of lactoferrin, azurocidin, and elastase as well as RNA markersfor neutrophil development.Conclusions: Neonates have more circulating immature neutrophils as com-pared to adults, but the significance of this finding remains unknown. Newfindings are that demargination of neutrophils occur without the onset oflabor and that protein concentrations of >-defensin are approximately 1.5times higher in neonatal as compared to adult neutrophils.
376
NECROTIZING ENTEROCOLITIS, HEMATOCRIT, ANDBLOOD TRANSFUSIONS; IS THERE AN ASSOCIATION?
Lawrence SM, Nandyal R, Hallford G, Hart N. OU Health Sciences Center,OKC, OK.Purpose of Study: Transfusion Associated Necrotizing Enterocolitis(TANEC) is defined as the onset of necrotizing enterocolitis (NEC) within48 hours of receiving a blood transfusion in preterm neonates. We wanted todetermine if abrupt increases in hematocrit (HCT) levels following a bloodtransfusion are associated with an increased risk of NEC.Methods Used: This is a retrospective analysis of inborn neonates, e
34 weeks gestational age, from January 1, 2007 and December 31, 2010 diag-nosed with NEC. Those meeting TANEC criteria were identified and an analysiscompleted to evaluate if abrupt changes in HCT levels following the neonate’sfirst transfusion or that closest to 3 weeks of age, a critical period for NEC devel-opment in this patient population, was associated with an increased risk for NEC.Summary of Results: Of 1891 neonates studied, 19 of 75 (25%) infantswith NEC met the criteria for TANEC. We found no statistically significant
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 479
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

differences in degree of illness between NEC and TANEC patients, includ-ing time of NEC onset, modified Bell staging of NEC, length of stay, ormortality. In addition, there were no statistically significant differences inHCT levels prior to or following the first transfusion or transfusion closestto the third week of life in either NEC group as compared to control infantswithout NEC.Conclusions: The dramatic onset of NEC following transfusion occurs witha frequency which invites investigation regarding causation. However, our dataindicates NO association between transfusion factors and NEC.
Pulmonary and Critical CareConcurrent Session
2:00 PMFriday, February 22, 2013377
ALCOHOL INDUCES LUNG FIBROBLAST OXIDATIVESTRESS VIA TRANSFORMING GROWTH FACTOR-A1ACTIVATION AND NRF2 SUPPRESSION
Sueblinvong V1, Saghafi R1, Mills S1, Fan X1,2, Guidot D1,2. 1EmoryUniversity, Atlanta, GA and 2Atlanta VA, Decatur, GA.Purpose of Study: We have previously shown that chronic alcohol inges-tion induces the expression and activation of transforming growth factorbeta1 (TGFA1) in the lung. In parallel, alcohol also inhibits the expressionand function of Nrf2, the master transcription factor that activates the anti-oxidant response element (ARE). Therefore, in this study we hypothesizedthat alcohol induces oxidative stress via a feedback loop of TGFA1 activationand Nrf2 suppression.Methods Used: 3T3 lung fibroblasts (passage G 18) were exposed to al-cohol (60 mM) for 24-72 hours T sulforaphane (5 KM; a naturally-occurringcompound that induces and/or activates Nrf2) T the TGFA receptor inhibitorSB431542; we then assessed 1) the expression and activity of Nrf2, 2) theexpression of TGFA1, and 3) the expression of two anti-oxidant enzymes (GSTand NQO1) that are activated by Nrf2-ARE signaling. In parallel experiments, cellswere treated with Nrf2 siRNA and TGFA1 protein expression was quantified.Summary of Results: Alcohol treatment increased cellular TGFA1 ex-pression while simultaneously suppressing cytosolic Nrf2 expression anddecreasing Nrf2-ARE activity and the downstream expression of GST andNQO1. Interestingly, treatment with the TGFA1 receptor inhibitor mitigatedthe effects of alcohol on Nrf2-ARE activity. In parallel, inhibiting Nrf2 ex-pression by siRNA increased the expression of activated TGFA1 and therebyreproduced the effects of alcohol.Conclusions: Alcohol exposure induces TGFA1 expression and simulta-neously suppresses Nrf2 expression and Nrf2-ARE activity via a previouslyunrecognized feed-back loop. We speculate that alcohol-induced oxidativestress in the lung is mediated by the induction of TGFA1 that, in turn, inhibitsthe expression and activity of Nrf2 which then propagates a vicious cycle of
further TGFA1 activation and Nrf2 suppression. As a consequence, the abilityof the lung to activate its anti-oxidant defenses is impaired. However, thesepathophysiological effects of alcohol can be reversed by pharmacologicallyactivating the Nrf2-ARE signaling pathway with sulforaphane, suggesting thatthis naturally-occurring compound could have therapeutic benefits and mitigatemany of the harmful effects of chronic alcohol abuse on the lung.
378
CIGARETTE SMOKE INDUCES SYSTEMIC DEFECTS INCYSTIC FIBROSIS TRANSMEMBRANE CONDUCTANCEREGULATOR (CFTR) ION TRANSPORT
Raju S1, Jackson PL1, McNicholas C1, Tang L1, Mazur M1, Clancy JP2,Accurso FJ3, Blalock J1, Dransfield M1, Rowe SM1. 1University of Alabamaat Birmingham, Birmingham, AL; 2Cincinnati Children’s Hospital MedicalCenter, Cincinnati, OH and 3University of Colorado, Denver, CO.Purpose of Study: Cigarette smoke (CS) decreases expression and functionof airway epithelial CFTR and is associated with chronic bronchitis, delayedmucociliary transport, and airways obstruction, pathology similar to CF. CS isalso associated with CF-related systemic disorders like pancreatitis, constipa-tion and male infertility and suggesting a potential pathogenic role for CFTRdefects in organs distant from direct CS exposure. Here, we have determinedthe distribution and severity of CFTR dysfunction in cigarette smokers.Methods Used: Age-matched subjects with and without chronic obstructivepulmonary disease (COPD) and cigarette smoking participated. Demo-graphics, spirometry, exercise tolerance, symptom questionnaires, CFTRgenetics and sweat chloride analysis were obtained. CFTR activity wasmeasured in human bronchial epithelial cells (HBE) and and murine tissuesin modified Ussing chambers. Serum acrolein levels were estimated withmass spectroscopy and western blots.Summary of Results: Healthy smokers (31.1 mEq), COPD smokers(30.7mEq) and COPD former smokers (24.5 mEq) had elevated sweat chloridelevels compared to normal controls (14.5 mEq). These results reflect com-promised CFTR activity in a non-pulmonary organ. CFTR activity was de-creased in HBE cells exposed to plasma from smokers by 68%, suggesting acirculating factor could confer CFTR dysfunction. CS exposed mice haddecreased CFTR activity by NPD (28.9% of controls), tracheal Isc (53%) andintestinal Isc (84.3% and 45%, after 5 and 17 weeks, respectively). Acrolein,a reactive component of CS, was higher by 35% (PG0.05) in smokers. InHBEs, acrolein reduced CFTR function, probably of opening (Po) and N-acetyl cysteine attenuated these effects.Conclusions: Cigarette smoke causes a systemic defect in CFTR functionand provides potential explanation for the increased incidence of CFTR-associated disorders like pancreatitis, constipation, diabetes mellitus, andmale infertility in smokers.
379
EFFECT OF CONTINUOUS POSITIVE AIRWAY PRESSURETHERAPY ON NIGHTMARES IN PATIENTS WITHPOST-TRAUMATIC STRESS DISORDER AND OBSTRUCTIVESLEEP APNEA
Gharaibeh K1,2, Tamanna S1,2, Ullah M2, Geraci SA2. 1University ofMississippi Medical Center, Jackson, MS and 2G.V. (Sonny) Montgomery VAMedical Center, Jackson, MS.Purpose of Study: About 1 in 6 veterans suffers from post-traumatic stressdisorder (PTSD). Nightmares may improve with continuous positive airwaypressure (CPAP) therapy if obstructive sleep apnea (OSA) is also present, butCPAP compliance is low among these patients.
We hypothesized that among PTSD-afflicted veterans with OSA, 1) CPAPtherapy reduces nightmares and 2) CPAP compliance associates directly withsymptom improvement. We also sought to determine if CPAP effectivenessdiffered if OSA was rapid eye movement (REM) or Non-REM- related.Methods Used: We retrospectively reviewed medical records to identifyOSA patients treated in a VA medical center sleep clinic between May 2011and May 2012 who also carried a PTSD diagnosis. Epworth sleepiness scoresand mean number of nightmares/week (pretreatment and up to 6 monthsafter CPAP prescription) were extracted. Compliance (% nights with 94 hrsCPAP use) was determined from memory cards. Baseline polysomnogramsdetermined patients’ assignment to REM or Non-REM -related OSA cohorts.
Duncan Multiple Range Test
* 1st Transfusion Data N=41; Week 3 not calculated due to insufficent s;**1st Transfusion Data N=149; Week 3 N=131; Means with same letter notsignificant; significance with unlike letters
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
480 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Repeated-measures t-tests were performed, comparing mean nightmare fre-quency and degree of daytime sleepiness before and after treatment. Simple andmultiple linear regression analyses were performed to identify factors (com-pliance, total AHI, REM AHI, age, BMI) predicting fewer nightmare attacks.Summary of Results: Forty-three patients (25 REM-related, 18 Non-REM-related) had complete data. The mean number of nightmares/week fell sig-nificantly with CPAP use in both groups (pG0.01). Reduced nightmarefrequency after starting CPAPwas best predicted by CPAP compliance (R2=0.55,pG0.01), which was higher in Non-REM (75.3%) than REM (55.8%) -relatedOSA patients (p=0.04).Conclusions: In veterans, CPAP therapy reduces PTSD-associated night-mares in patients with either REM- or Non-REM-related OSA, and compliancepredicts the magnitude of treatment benefit. Lower compliance in REM-related OSA patients may reduce net CPAP benefit for this subpopulation.
380
TGF-BETA1 INDUCES SENESCENCE IN VITROAND IN VIVOBY UP-REGULATING PROMYELOCYTIC LEUKEMIAPROTEIN (PML)
Luo F, Dong C, Zhuang Y, Lasky JA. Tulane University, New Orleans, LA.Purpose of Study: Idiopathic pulmonary fibrosis (IPF) is a devastating diseasethat primarily affects older adults. Older animals appear to develop worse fibrosisin comparison to young animals, and higher numbers of senescent epithelial cellshave been observed in IPF lungs compared to control lungs. TGF-A1 is a potentfibrogenic growth factor that promotes cell differentiation into fibrogenic phe-notypes, and has the capacity to inducecellular senescence. Promyelocyticleukemia protein (PML)has various functions, including tumor suppression,transcription regulation and senescence induction. This study investigates howTGF-A1 regulates PML expression and senescence in vivo and in vitro.Methods Used: Bleomycin and TGF-A1 adenovirus vector were used to inducefibrosis in C57BL/6 mice. Immortalized human alveolar epithelial cells (HPL1Ds)were treated with TGF-A1. Quantitative real-time PCR, western blot and immuno-fluorescent staining were used for evaluating PML and other protein expression.Summary of Results: An increase in PML protein and enlargement ofPMLnuclear bodies was observed in TGF-A1 adenovirus infected and bleo-mycin exposed mouse lungs compared to control lungs. PML expression wasalso up-regulated in IPF lungs in comparison to age matched control lungs.Expression of the senescence marker, P21, was increased in IPF lungs andbleomycin treated mouse lungs compared to controls. In vitro, TGF-A1 inducedP21 and PML protein expression as well as PML nuclear body enlargement inHPL1D cells. UO126, a specific Erk phosphorylation inhibitor, blocked theTGF-A1-mediated induction on PML expression. In contrast, inhibition ofAkt, P38 and JNK phosphorylation did not affect PML expression.Conclusions: Our data indicate that TGF-A1 induces PML expression invitro and in vivo through Erk activation. The induction of PML expression byTGF-A1may contribute to the pathogenesis of IPF.
381
REQUIREMENT OF HDAC6 FOR THE NOTCH SIGNALINGPATHWAY DURING THE TGF-A RESPONSE
Deskin BJ1, Zhuang Y1, Lasky JA1, Shan B1,2. 1Tulane School of Medicine,New Orleans, LA and 2Tulane University, New Orleans, LA.Purpose of Study: The purpose of this study is to investigate the role ofHDAC6-mediation of the notch signaling pathway when activated by TGF-A.Methods Used: Using the human adenocarcinoma lung epithelial cell line,A549, the TGF-A cytokine was used to induce an epithelial-mesenchymaltransition phenotype. Pharmacological inhibition of HDAC6 with tubacinand siRNA against HDAC6was used to investigate the role of HDAC6 in notchsignaling when compared to pharmacological inhibition of the F-secretasecomplex using DAPT. Quantitative RTPCR was performed to determine foldexpression changes in downstream targets of the Notch signaling pathway -HES1 and HEY1- upon treatment with TGFA or with inhibition of HDAC6or F-secretase. Immunofluorescence microscopy and Western analysis wasused to visualize Notch-1 intracellular domain translocation. Immunopre-cipitation of cell lysate with anti-HDAC6 followed by immunoblot for Notch-1 was performed to investigate direct interaction of HDAC6 with Notch-1.Summary of Results: In this study we show that pharmacological inhibitionand small interfering RNA against HDAC6 attenuates activation of Notch-1
downstream target genes both at the transcriptional level and the protein level;similarly, pharmacological inhibition of the F-secretase complex results in at-tenuated expression of notch target genes. We also report a direct interaction ofHDAC6with Notch-1 and an increase in this interaction when exposed to TGF-A.Conclusions: Our findings indicate a novel function of HDAC6 mediat-ing the notch signaling cascade, further implicating HDAC6 as a key regu-lator of EMTand tumorigenesis, making it an ever-more attractive therapeutictarget for protection against fibrogenesis and metastasis.
382
LUNG FIBROBLAST-MYOFIBROBLAST DIFFERENTIATIONIN RESPONSE TO TGFB1 IS CONCOMITANT WITH ADEFICIENT AUTOPHAGIC RESPONSE, WHEREASTHERAPEUTIC INDUCTION OF AUTOPHAGY INMYOFIBROBLAST TARGETS COLLAGEN I FOR DEGRADATION
Sosulski M, Changala M, Luo F, Lasky J, Sanchez C. Tulane University,New Orleans, LA.Purpose of Study: TGFA1 inhibits autophagy in lung fibroblasts; and theestablishment of autophagy-competent myofibroblasts favors the degrada-tion of collagen Type I.Methods Used: qRT-PCR and Western blot (WB) techniques were usedto measure the expression of fibrotic markers, Col1 and >-SMA, in NormalHuman Lung Fibroblasts (NHLFs) in the presence of TGFA1. RT-PCR arraywas performed on NHLF cultured in the presence of low doses of Resveratrol,an inducer of autophagy, and also in the presence or absence of TGFA1 toassess changes in expression of autophagic markers. NHLF were differenti-ated into myofibroblasts and treated in the presence and absence of highdoses of Resveratrol with different concentrations of Bafilomycin A, an in-hibitor of lysosome-autophagosome fusion.Summary of Results: TGFA1 inhibited the lipidation of LC3b (LC3bII).Light LC3bII bands were observed in lung fibroblasts treated with TGFA1and low doses of Resveratrol, or an mTOR inhibitor, compared to resveratrolalone or the mTOR inhibitor alone. TGFA1 decreases the expression of thechaperone-mediated autophagy marker, lamp2a, in lung fibroblasts. Murinelung infected with Adenovirus- TGFA1 shows a 20% decrease in Lamp2AmRNA compared to adenovirus control. Autophagy expression array dataindicate that TGFA1 induces IGF-1 expression, while it down-regulates theexpression of several genes involved in selective autophagy, including p62.Resveratrol reverses the autophagy deficiency induced by TGFA1 duringmyofibroblast differentiation and stimulates collagen I degradation inestablished myofibroblasts; and this effect is inhibited by Bafilomycin A1.Conclusions: The fibrogenic factor TGFA1 impairs the normal autophagicresponse in lung fibroblasts, which could potentially promote fibrosis. Pre-liminary studies suggest a possible role of autophagy in the pathobiology ofpulmonary fibrosis.
383
INHIBITION OF TGF-A-INDUCEDFIBROBLAST-MYOFIBROBLAST DIFFERENTIATIONBY HDAC6 INHIBITION
Saito S, Zhuang Y, Shan B, Sanchez C, Lasky J. Tulane University, NewOrleans, LA.Purpose of Study: Transforming growth factor (TGF)-A has been shown topromote epithelial-mesenchymal transition (EMT) as well as differentiationof fibroblasts into myofibroblasts. We have previously shown that inhibitionof histone deacetylase (HDAC) 6, one of HDAC class II enzymes, abrogatesTGF-A induced EMT. In this study, we investigated a role of HDAC6 in TGF-A-induced myofibroblast differentiation.Methods Used: Normal human lung fibroblasts (NHLFs) were treated withTGF-A (1ng/ml) and HDAC inhibitors, including trichostatinA (TSA; panHDAC inhibitor), MC1575 (HDAC class II inhibitor) and tubastatin (HDAC6inhibitor). Expression of fibrosis makers such as >-smooth muscle actin(>-SMA) and type I collagen were assessed via RT-PCR and immunoblot-ting. Stress fiber formation was also assessed via immunocytostaining.Summary of Results: TSA, MC1575 and tubastatin inhibited TGF-A-induced >-SMA and type I collagen expression. The inhibition of >-SMAexpression by tubastatin appeared to be associated with reduced phosphor-ylation of Akt, independent of Smad 2/3 pathway. Tubastatin also blockedTGF-A-driven stress fiber formation in NHLFs.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 481
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Conclusions: Our data suggest that HDAC6 plays an important role in thedifferentiation of NHLFs to myofibroblasts, probably via phosphorylationof Akt, and inhibition of HDAC6 is a promising strategy for the treatmentof pulmonary fibrosis.
384
SMOOTH MUSCLE-TARGETED PPAR GAMMAOVEREXPRESSION ATTENUATES HYPOXIA-INDUCEDPULMONARY HYPERTENSION IN MICE
Green D, Klienhenz J, Sutliff R, Hart C. Emory University, Decatur, GA.Purpose of Study: Pharmacological activation of the nuclear hormonereceptor, PPAR gamma (PPARF), attenuates pulmonary hypertension (PH) inrodent models. The mechanisms and sites of action for these therapeuticeffects continue to be defined. We hypothesized that the vascular smoothmuscle cell compartment was an important locus through which the thera-peutic effects of PPARF activation were mediated in PH. We examined thishypothesis by employing a genetic strategy to constitutively activate PPARFin vascular smooth muscle cells.Methods Used: C57Bl/6 mice with floxed alleles for PPARF driven by theconstitutively active VP16 promoter were bred with mice expressing Crerecombinase driven by a tamoxifen-inducible smooth muscle myosin promoter.After genotyping, adult offspring that demonstrated smooth muscle-targetedoverexpression of constitutively active PPAR gamma (smVP16-PPARF) orlittermate controls (LC) were treated with tamoxifen and exposed to normoxiaor hypoxia (10% O2) for 4-weeks. Right ventricular systolic pressure (RVSP)was measured with a pressure transducer, and right ventricular hypertrophy(RVH) was assessed by calculating the ratio of the weight of the right ventricleto the left ventricle + septum. Pulmonary vascular remodeling was assessed bystaining lung sections with antibodies to alpha smooth muscle actin.Summary of Results: Compared to LC, smVP16-PPARF mice demon-strated overexpression of VP16 and PPARF in aortae and weighed approxi-mately 20% less. There was no significant difference in RVSP between LCand smVP16-PPARF mice exposed to normoxia. As expected, compared tonormoxic controls, hypoxia increased RVSP in LC mice, whereas hypoxicincreases in RVSP were reduced by approximately 50% in smVP16-PPARFmice. Hypoxia-induced increases in muscularization of small pulmonaryvessels (G20 K diameter) in LC mice was attenuated in smVP16-PPARFmice. In contrast, genotype had no significant effect on hypoxia-inducedincreases in RVH.Conclusions: These findings provide novel evidence that smooth muscle-targeted PPARF activation attenuated hypoxia-induced PH and vascularremodeling and that previously observed therapeutic effects on RVH arelikely attributable to activation PPARF in the ventricular myocardium.
385
DIFFUSING CAPACITY IN SMOKING AND OBESITY
Carpenter J1,2, Haynes D1,2, Petrini M1,2. 1University of Mississippi Medical Center,Jackson, MS and 2GV Sonny Montgomery VA Medical Center, Jackson, MS.Purpose of Study: Obesity is known to result in restriction or a restrictivepattern, but the contribution of obesity to pulmonary function abnormalitiesto those resulting from lung diseases is not known. We hypothesized that thediffusing capacity (DLco) may help with this distinction.Methods Used: We compared DLco in two groups of male currentsmokers, expected to have abnormal DLco, lean (LS, BMI G 25 Kg/m2) andobese (OS, BMI Q 30 Kg/m2) with obese non-smokers (ON). Only DLcomeasurements that met the 2005 ERS/ATS criteria and were corrected forhemoglobin (Hb) and for carboxyhemoglobin (HbCO) were used. Patientswith confounding lung pathologies (interstitial lung diseases, lung cancer,and pulmonary hypertension) or congestive heart failure NYHA classes IIIand IV were excluded. Data were collected from 2010 to present and analyzedby ANOVA, with Newman-Keuls for post-test when results were different.Smoking history between LS and OS was analyzed with the unpaired t-test;P G 0.5, Pw = 90%, and corrected for multiple comparisons as appropriate.Summary of Results: Obese non-smokers have a statistically significantlarger DLCO as % of predicted when compared to lean and obese smokers.Conclusions: Obese non-smokers have larger DLco as % of predicted thantheir lean and obese smoking counterparts. DLco can help differentiate be-tween PFT lung abnormalities from those due solely to obesity.
386
PULMONARY REHABILITATION INCREASES GAIT SPEEDIN PATIENTS WITH CHRONIC LUNG DISEASES
McClellan R, Mojazi Amiri H, Limsuwat C, Nugent KM. Texas TechUniversity Health Sciences Center, Lubbock, TX.Purpose of Study: Patients with chronic lung diseases are often frail andhave low gait speeds. Pulmonary rehabilitation improves aerobic fitness,muscular strength, and quality of life. It should improve gait speed and, there-fore, improve frailty markers. This study used information from 6 minute walksto analyze the effect of pulmonary rehab on gait speed.Methods Used: We retrospectively reviewed clinical files of 119 patientswho completed pulmonary rehabilitation in 2010 and 2011. We collected infor-mation on demographics, symptoms, pulmonary function tests, and baseline gaitspeeds calculated from 6 minute walks. We used this information to determinethe percentage and characteristics of patients with gait speeds greater than60 meters per minute (m per min) before and after completion of the program.Rehab sessions included aerobic exercise, strength training, and education.Summary of Results: The mean age was 68.8 T 10.1 years; 52 % ofparticipants were men. Ninety-five (79.8%) had obstructive lung disease;97.5% had dyspnea and 54.6% had cough. The mean FEV1 was 1.3T 0.7 L(47.2T 19.7 % predicted). These patients completed 19.3 T 7.4 weeks ofrehab. The mean gait speed before rehab was 41T 15 m per min. The meanspeed after rehab was 47 T 15 m per min. Ten patients (8.4 %) had a gaitspeed 9 60 m per min before rehab, and 29 (24.4 %)had a speed 9 60 m permin post rehab (pG 0.001). Univariate analysis indicated that patients with agait speed greater than 60 m per min post rehab had less dyspnea, were lesslikely to use oxygen, and had a higher baseline gait speed. Multivariateanalysis demonstrated that that only the initial baseline gait speed predictedwho would have a speed greater than 60 m per min post rehab.Conclusions: Pulmonary rehabilitation improves exercise performance, andthe percentage of patients with a gait speed greater than 60 m per min in-creased after rehabilitation. This simple assessment tool provides a goodmethod to evaluate pulmonary rehab outcomes. Patients who do not improvemay need additional assessment to evaluate gait limitations and/or alterna-tive approaches to pulmonary rehabilitation.
387
PREDICTIVE VALUE OF FLUID BALANCE ON EXTUBATIONFAILURE
Burkhart RE, Chatterjee AB, Hite RD. Wake Forest School of Medicine,Winston Salem, NC.Purpose of Study: Determining when to extubate patients who have re-covered from respiratory failure is important and must consider risks ofdelayed extubation versus those of extubation failure. Daily spontaneousbreathing trials (SBTs) are routinely used to help predict extubation readi-ness; but even with SBTs, extubation failure rate (need for reintubationwithin 48-72 hours) can still be 10-20%. In this study, we, therefore, sought todetermine if other additional factors could be used to help predict extubationreadiness and reduce extubation failures.Methods Used: We conducted a retrospective chart review of patientstreated from January to June 2011, in any medical-surgery ICU at WakeForest Baptist Hospital, a large tertiary-care university hospital in Winston-Salem, North Carolina. Patients were included in the study if they had beenintubated for at least 48 hours and underwent planned extubation. Patientswere excluded if they were extubated for purposes of withdrawal of supportor tracheostomy, or if they were re-intubated within 48 hours simply forplanned OR procedures. We used t-tests and chi-square testing to determinefactors associated with extubation failure.
Summary of Results
*LS different from OS and ON, OS and ON not different; comparison betweensmokers only; ON different from LS and OS, LS and OS not different.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
482 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: Among the 569 consecutive patients who receivedmechanical ventilation, 281 met inclusion criteria and did not meet exclusioncriteria. Of these, 28 (10.0%) were re-intubated within 48 hours. We identi-fied the following factors to be associated with extubation failure: older ageand a positive fluid balance the day prior to extubation. Among the factorsfound not to be significantly associated with extubation failure were: gender,pre-existing cardiopulmonary disease, RSBI, minute ventilation prior toextubation, and presence of fever (including new fever).Conclusions: One of the strongest predictors of extubation failure in patientsmechanically ventilated for at least 48 hours was a positive fluid balance the dayprior to extubation. In order to further validate this finding, we plan to continue tocollect retrospective data for the remainder of 2011 and to also develop a pro-spective trial to examine the impact of improved fluid status on extubation failure.
Renal, Electrolyte and Hypertension IConcurrent Session
2:00 PMFriday, February 22, 2013388
DIMETHYLSULFOXIDE AS A PROTECTIVE AGENTAGAINST KIDNEY ISCHEMIC-REPERFUSION INJURY:AN EXPERIMENTAL STUDY IN AN ANIMALISCHEMIA-REPERFUSION MODEL
Rivas AM1, Castaneda JR2, Sotello DA1, Hoyos WA3. 1Texas TechUniversity Health Science Center, Lubbock, TX; 2AtlantiCare RegionalMedical Center, Atlantic City, NJ and 3Universidad Doctor Jose MatiasDelgado, Santa Tecla, El Salvador.Purpose of Study: To evaluate the effect of dimethylsulfoxide (DMSO) onkidney injury in an animal model of ischemia/reperfusion syndrome.Methods Used: 29 male rabbits with right nephrectomy distributed ran-domly in 3 groups: A sham-operated group (n=5), an Ischemia-reperfusion-normal saline group (n=12) and an ischemia-reperfusion- DMSO group(n=12). Acute ischemic injury was induced with non-traumatic clamping ofthe left renal artery for 30 minutes. During reperfusion phase, the experi-mental group received DMSO 40%, while the control group was treated withNaCl 0.9% solution. Renal function was evaluated after 8 hours of reperfu-sion using serum creatinine. Kidney samples were obtained and sent formicroscopic analysis, focused on 17 variables indicative of kidney injury,each was reported as mild, moderate or severe by the pathologist.Summary of Results: DMSO attenuated kidney damage significantlywhen compared to conventional treatment with normal saline solution duringreperfusion phase in the ischemia-reperfusion model. Kidney function wasbetter preserved in the experimental group compared to the control group (p=0.003) - serum creatinine levels were found to be lower in the experimentalgroup compared to the control group, with an increase in post-reperfusioncreatinine compared to baseline of 245% and 318% respectively. Based onthe increase in serum creatinine, the severity of kidney damage afterischemia-reperfusion was classified as risk, injury or failure according to theRIFLE classification; 83% of the experimental group was categorized as‘‘injury’’, while 92% of the control group fell into ‘‘failure’’ category. Histo-pathological analysis also showed significant differences between the controland the experimental group; the presence of kidney injury variables were de-scribed as mild (50%) to moderate (50%) for samples of the experimentalgroup, compared to moderate (75%) to severe (25%) for the control group.Conclusions: DMSO significantly attenuates renal ischemia-reperfusion in-jury when administered during the reperfusion phase.
389
PDGF RECEPTOR ANTAGONISM PREVENTS THEINCREASE IN URINARY ANGIOTENSIN II EXCRETION INCYP1A1-REN2 TRANSGENIC RATS WITH ANGIOTENSINII-DEPENDENT MALIGNANT HYPERTENSION
Milani CJ, Howard CG, Seth DM, Davis PD, Mitchell KD. TulaneUniversity, New Orleans, LA.
Purpose of Study: Previous studies demonstrated that chronic adminis-tration of the PDGF receptor kinase inhibitor, imatinib mesylate, amelioratesthe renal injury and improves renal hemodynamics in transgenic rats[TGR(Cyp1a1Ren2)] with angiotensin (ANG) II-dependent malignant hy-pertension. The present study was performed to determine if chronic ad-ministration of the PDGF receptor antagonist, imatinib mesylate, prevents theaugmentation of urinary ANG II excretion that occurs in Cyp1a1-Ren2transgenic rats with ANG II-dependent malignant hypertension.Methods Used: Male Cyp1a1-Ren2 rats (n=6/group) were induced to de-velop malignant hypertension by dietary administration of indole-3-carbinol(I3C, 0.3% wt/wt) for 10 days. One group was chronically treated withimatinib mesylate by oral gavage (60 mg/kg/d) starting 3 days before initi-ating I3C induction and maintained on imatinib for the duration of the study.Systolic blood pressures (SBP) were measured daily by tail-cuff plethys-mography. Rats were periodically placed in metabolic cages for measurementof 24-hour urine output and urinary protein and ANG II excretion.Summary of Results: Dietary I3C resulted in pronounced increases in SBP(152T6 to 209T6 mmHg, PG0.001) and urine output (8.5T0.7 to 60T5 ml/day,PG0.001), marked proteinuria (26.8T3.0 to 72.2T11.8 mg/day, PG0.01), andaugmented urinary ANG II excretion (448T12 to 987T119 fmol/hr, PG0.05).Chronic imatinib administration did not prevent the development of hyper-tension (204T3 vs. 157T8 mmHg, PG0.001) or the increase in urine flow(61.8T5.0 vs. 8.5T0.6 ml/day, PG0.001), but prevented the I3C-inducedincreases in proteinuria (21.8T2.2 vs. 21.8T0.8 mg/day) and urinary ANG IIexcretion (263T30 vs. 492T43 fmol/hr).Conclusions: The present findings demonstrate that PDGF receptor antago-nism with imatinib mesylate prevents the marked proteinuria and augmentedurinary ANG II excretion independent of changes in blood pressure that occurin Cyp1a1-Ren2 rats with ANG II-dependent malignant hypertension. The dataalso indicate that PDGF receptor activation contributes importantly to the increasein intratubular ANG II generation and, thus, to the augmentation of urinaryANG II excretion that occurs in ANG II-dependent malignant hypertension.
390
HISTONE H3K79 METHYL TRANSFERASE, DOT1L, ISDEVELOPMENTALLY REGULATED BUT IS DISPENSABLEFOR KIDNEY DEVELOPMENT
Wang F, Saifudeen Z, El-Dahr S. Tulane University, New Orleans, LA.Purpose of Study: Histone modifications are critical effectors of geneexpression thereby regulating cell lineage, identity and cell fate. Dot1l, as the solehistone methyltransferase specific for Histone 3 lysine 79, plays an essential rolein DNA damage, cell cycle and differentiation pathways. Germ-line inactivationof Dot1l results in embryonic lethality. This study examines the role of H3K79methylation in kidney development and response to injury and regeneration.Methods Used: QPCRWB IF conditionally KO in mice.Summary of Results: Dot1l expression and H3K79 methylation showspatio-temporal changes during mouse kidney development. Dot1l expres-sion (RT-QPCR) and H3K79me3 (western blot) are low in early embryonicstages but increases significantly with postnatal renal maturation. Moreover,Dot1l expression and K79 modification levels are higher in the collectingduct cell line than in mesenchyme-derived cell lines. In the maturing kidney,H3K79me3 correlates strongly with terminal differentiation of the renal ep-ithelium, specifically glomerular podocytes, proximal tubules, loop of henleand collecting ducts. Human proximal tubule cells, HK-2, exposed to hyp-oxia in vitro led to a rapid reduction in Dot1l mRNA as early as 6h. Similarly,ischemia/reperfusion injury in vivo provoked a marked reduction in Dot1land K79me3 predominantly in the proximal tubules at 24-72h, while re-generation at 7d correlated with re-expression of Dot1-H3K79methylation.Based on these data we hypothesize that Dot1L-H3K79methylation functionin renal tubule differentiation and repair, as well as in collecting duct de-velopment. To test the lineage-specific role of Dot1l in kidney development,we conditionally deleted Dot1l specifically in renal ureteric bud lineage cellsby crossing Dot1l floxed mice with Hoxb7-cre mice. Surprisingly, condi-tional Dot1l deletion from the UB lineage did not produce an abnormalphenotype, with preservation of collecting duct and proximal tubule markers.The conditionally knockout mice are also viable and fertile without detectableweight loss or disease compared with wt mice.Conclusions: These data demonstrate that Dot1l is dispensable for uretericbud branching and collecting system development. Experiments are underway to examine the effect of conditional Dot1l deletion on functional andstructural recovery from acute kidney injury.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 483
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

391
THE p53 REGULON UNRAVELS DISTINCTDEVELOPMENTAL FUNCTIONS OF p53Li Y1, Liu J1,2, McLaughlin N1, Bachvarov D3, Saifudeen Z1,2, El-Dahr S1,2.1Tulane University Health Science Center, New Orleans, LA; 2TulaneUniversity Health Science Center, New Orleans, LA and 3Universite Laval,Quebec, QC, Canada.
Purpose of Study: To delineate the genome-wide pattern of p53 tran-scriptional regulation in organogenesis.Methods Used: Microarray, ChIP-Seq, qPCR, luciferase reporter assay.Summary of Results: In this study we identify p53 targets in the embry-onic kidney, an organ which develops via mesenchymal-epithelial inter-actions. To identify direct targets of p53 that regulate nephrogenesis, weperformed chromatin immunoprecipitation followed by high-throughput se-quencing (ChIP-Seq) on embryonic mouse kidneys coupled with microarrayon embryonic kidneys from p53+/+ and p53-/- embryos. ChIP-Seq data re-vealed 7,893 p53-enriched genomic regions, 99.5% of which contain one ormore consensus p53 binding site. The vast majority of the p53 peaks (78%)in the developing kidney are located in the proximal promoters of genes, incontrast to only 3% of genes in cancer cells. Interestingly, there is no directcorrelation between ChIP-Seq tag density and change in gene expression notedin the microarray. Of 3,233 genes that showed significant differential expres-sion (pG0.05) in p53-null kidneys, 1,683 (52.06%) are potential p53 directtargets as they are also enriched in the ChIP-Seq binding profiles. Genes in-volved in morphogenesis and metabolism accounted for almost half of thep53-regulated transcriptome in the developing kidney and in cancer cells. Incomparison, cell cycle and apoptosis genes are three-fold more prevalentin cancer than developing kidney. Novel p53 targets were identified, includingkey renal development regulators, Wnt, BMP, FGF, and Notch signaling andciliogenesis genes.Conclusions: This study demonstrates the wide-encomapssing nature ofthe p53 regulation but also highlights the distinctive features of p53 as atranscriptional regulator in development versus cancer.
392
CHANGES IN PLASMA AND RENAL TISSUE LEVELS OFINFLAMMATORY CYTOKINES DURING CHRONIC HIGHSALT INTAKE IN WILDTYPE AND ENOS KNOCKOUT MICE
Singh P, Stephenson R, Majid DS. Tulane University Medical School, NewOrleans, LA.Purpose of Study: We have recently demonstrated that systemic inhibitionof nitric oxide (NO) in anesthetized mice increases tumor necrosis factor->(TNF->) but reduces interleukin-10 (IL-10) in plasma and in renal tissues.However, the status of these cytokines during chronic high salt (HS) intake inthe conditions associated with NO deficiency is not yet definitely known.In the present study, we examined the hypothesis that HS intake in NOdeficient condition enhances the production of pro-inflammatory cytokinesin different organs including the kidney.Methods Used: Using appropriate ELISA kits, the levels of pro- (TNF->,and IL-6) and anti-inflammatory (IL-10) cytokines were measured in plasmaand renal tissues collected from wild type (WT; C57BL6) and eNOS enzymeknockout (eNOS-KO) mice (È8 wks old) which were fed either normal (NS)or HS (4% NaCl) containing diet for 2 weeks.Summary of Results: Mean arterial pressure (measured by tail-cuff pleth-ysmography) was significantly increased in eNOSKO (111T4 to 136T8mmHg)
but not in WT (99T5 to107T4 mmHg) due to HS intake. The changes incytokines levels are summarized in the table below.Conclusions: These findings indicate that HS intake generally suppressesthe levels of both pro- as well as anti-inflammatory cytokines, particularlyin the kidney. These data suggest that NO inhibition induced by deficientactivity of eNOS enzyme is mostly responsible for upregulation of inflam-matory cytokines in the kidney.
393
NEPHROGENIC SYSTEMIC FIBROSIS: REDOX SENSITIVITY,DERMAL CCR7-EXPRESSING FIBROCYTES, AND EVIDENCEOF PULMONARY INVOLVEMENT IN A RAT MODEL
Sewell J1, Wagner B2,1. 1University of Texas Health Care System at SanAntonio, San Antonio, TX and 2South Texas Veterans Health Care System,San Antonio, TX.Purpose of Study: In patients with renal insufficiency, gadolinium-basedmagnetic resonance imaging (MRI) contrast use is the highest risk factor fornephrogenic systemic fibrosis (NSF). Circulating fibrocytes express C-Cchemokine receptor (CCR) type 7, and this may contribute to recruitment ofthese cells to affected sites. No one has explored this with respect to NSF.Additionally, given the similar mechanism to idiopathic pulmonary fibrosis,the effect of MRI contrast on pulmonary fibrosis was examined.Methods Used: Female Fischer 344 rats underwent 5/6 nephrectomy at8 weeks and randomized to MRI contrast (Omniscan/gadodiamide, caldia-mide) treatment, MRI contrast plus the superoxide dismutase (SOD) mimetictempol, or control for 3 weeks. Serum analysis was by Luminex assay.Summary of Results: Half of the contrast-treated animals demonstratedgross skin abnormalities, whereas none of the tempol- and contrast- co-treated animals did. Serum monocyte chemotactic protein (MCP)-1 andinterferon F-induced protein (IP)-10 were significantly increased in thecontrast-treated animals with respect to control, and these were abrogatedby tempol. Skin from MRI contrast-treated animals had increased expressionof fibronectin, CCR7, and cathepsin-L when compared to control. Immu-nofluorescence demonstrated that the CCR7+ cells in the dermis were bonemarrow-derived. There was an increase in fibronectin in lung, which wasmildly abrogated by tempol.Conclusions: There is an increase in dermal CCR7-expressing bonemarrow-derived cells in MRI contrast-induced dermal fibrosis. Further-more, MRI contrast induces pulmonary fibronectin accumulation. Theseobservations not only support the theory that circulating fibrocytes mediatethe disease in a systematic manner, but suggest mechanisms and therapeutictargets for this devastating disease.
394
COLLECTING DUCT-SPECIFIC INACTIVATION OFHEPATOCYTE NUCLEAR FACTOR-1A LEADS TO CYSTICDISEASE AND POLYURIA
Noureddine L1, Cobo-Stark P1, Patel V1, Pontoglio M3, Igarashi P1,2.1University of Texas Southwestern, Dallas, TX; 2University of TexasSouthwestern, Dallas, TX and 3Institut Pasteur, Paris, France.Purpose of Study: Hepatocyte nuclear factor 1 beta (HNF-1A) is an es-sential transcription factor that binds to promoters of cystic kidney diseasegenes and regulates their transcription. In humans, mutations of HNF-1Acause maturity onset diabetes of the young type 5 (MODY-5), a rare diseasewhich leads to diabetes mellitus, renal cysts, congenital renal and genito-urinary tract anomalies. Kidney-specific inactivation of HNF-1A mediatedby Ksp/Cre transgenic mice, leads to rapid tubular cyst formation, hydro-nephrosis (hydro), and postnatal mortality. To allow further postnatal char-acterization, we produced a mouse with longer survival time.Methods Used: Pkhd1/Cre transgenic mice express cre exclusively in thecollecting duct (CD). We crossed Pkhd1/Cre mice to HNF-1A f/f mice togenerate Pkhd1/Cre; HNF-1A f/f mutants.Summary of Results: Mutants showed no postnatal mortality. Histologyrevealed medullary cysts at postnatal day (p) 21. At p35, cysts increased insize and number, and 88% of mutants developed hydro. To investigatewhether hydro occurred as a result of polyuria, we placed mice in metaboliccages and collected 24 hour (hr) urine. Compared to controls, mutants (n=11)
WT eNOS-KO
Cytokines NS (n=6) HS (n=6) NS (n=6) HS (n=6)
TNF-> Plasma (pg/mL) UD 202T146 UD 175T68*
Renal (pg/mg protein) 325T73 114T17* 624T67 115T18*
IL-6 Plasma (pg/mL) 13T11 UD 180T44 UD
Renal (pg/mg protein) 166T61 81T14* 619T106 56T7*
IL-10 Plasma (pg/mL) 701T54 344T52* 510T125 327T67*
Renal (pg/mg protein) 3929T378 865T130* 6087T567 882T14*
UD, undetected; *, PG0.05 vs corresponding NS; , PG0.05 vs WT-NS
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
484 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

developed polyuria (1.96 vs 4.15 ml, pG0.0001) and a urinary concentrat-ing defect (UCD) (1667 vs 826 mosmol/kgH20, p=0.0011). Both polyuria(0.79 vs 1.71 ml, pG0.0001) and UCD (2472 vs 1360 mosmol/kgH20,pG0.0001) persisted after 24 hr water deprivation. When hydro was excluded,mutants (n=7) were persistently polyuric (1.81 vs 4.10 ml, p=0.001) with aUCD (1821 vs 852 mosmol/kgH20, p=0.0007). After DDAVP challenge(n=4), both controls and mutants were able to concentrate urine similarly(94% vs 63%, p=0.49), but mutants continued to have dilute urine (4854 vs2579 mosmol/kgH20, p=0.0008).Conclusions: CD-specific inactivation of HNF-1A in mice leads to cystformation and hydro. HNF-1A mutant mice develop polyuria and UCD,independent of hydro. Neither primary polydipsia, nor central or nephro-genic diabetes insipidus is the cause of polyuria. Future experiments willexamine whether polyuria precedes cyst formation, and determine the molec-ular mechanisms by which the loss of HNF-1A leads to cyst formationand polyuria.
395
THE ROLE OF ENDOTHELIN-1 IN COLLECTING DUCTRENIN SYNTHESIS AND SECRETION
McGuire C1,2, Liu L2,3, Prieto M1,2,3. 1Tulane University, New Orleans, LA;2Tulane University, New Orleans, LA and 3Tulane University, New Orleans, LA.Purpose of Study: While the regulation of juxtaglomerular (JG) renin hasbeen extensively studied, much less is known about the regulation of col-lecting duct (CD) renin. Growing evidence shows that renin in principal cellsof the CD is stimulated by angiotensin II (AngII) independently of bloodpressure via an AngII type I receptor-mediated mechanism dependent onPKC. Alterations in renin synthesis and activity in the CD may provide acritical pathway to increase intrarenal and intratubular AngII content therebyincreasing sodium reabsorption and contributing to hypertension. However,the regulation of renin by hormones targeting the CD, such as endothelin-1(ET-1), has not been established. In the present study we aimed to determinethe effects of ET-1 on renin synthesis and secretion in the CD cells. Wehypothesize that ET-1 stimulates CD renin synthesis and secretion via PKGactivation by nitric oxide or via activation of PKC.Methods Used: Mouse M-1 CD cell culture, quantitative real-time RT-PCR,Western blot, measurements of intracellular cAMP content (ELISA).Summary of Results: In M-1 cells, ET-1 (5�10-9M) treatment for sixhours increased renin mRNA levels (pG0.01). Surprisingly, the same treat-ment in the presence of non-specific inhibition of all NOS isoforms byL-NAME (10-7 M) further increased the stimulatory effect of ET-1 on reninmRNA in CD cells (pG0.001). However, treatment with L-NAME or an NOdonor (10-6 M) alone had no effect on CD renin mRNA expression. Acti-vation of PKC with PMA (10-6 M) did not stimulate CD renin mRNAexpression. However, non-specific inhibition of PKC with calphostin C(10-7 M) in the presence of 5�10-9 M ET-1 attenuated the ET-1 dependentincrease in CD renin mRNA expression (pG0.001).Conclusions: The data indicate that ET-1 stimulates CD renin synthesis andsecretion by activation of both NOS/GC/cGMP/PKG and PKC pathways. Itis possible that the mechanism involved relies on potential cross-talk betweenthe NOS/GC/cGMP/PKG and PKC pathways, via ETBR-dependent activa-tion by ET-1. Further studies are being undertaken to examine this possibility.
396
ROLE OF TOLL-LIKE RECEPTORS AND REACTIVEOXYGEN SPECIES IN THE PATHOPHYSIOLOGY OFLUPUS NEPHRITIS
Khan A1, Maderdrut JL2, Coy DH2, Simon EE1,3, Batuman V1,3. 1TulaneUniversity, School of Medicine, New Orleans, LA; 2Tulane University,School of Medicine, New Orleans, LA and 3Southeast Louisiana VeteransHealth Care System, New Orleans, LA.Purpose of Study: Lupus nephritis is a common and severe manifesta-tion of systemic lupus erythematosus (SLE) and often leads to renal failure.However, it is not clear what controls the progression of lupus nephritis.In this study, we explored the role of Toll-like receptors (TLRs) and re-active oxygen species (ROS) in the development of SLE-like pathology ina mouse model.
Methods Used: We used male NZB/NZW (NZB/W) F1 mice, whichspontaneously develop SLE-like pathology, as the model for lupus nephri-tis. NZW mice served as the controls. Mice were euthanized at 22, 29, or41 weeks of age (wk), and blood samples and kidney samples were harvestedto assess renal function and pathology.Summary of Results: Creatinine and cystatin C levels in serum ofNZB/W F1 mice were increased significantly (p G 0.05) compared to NZWmice at 22 wk, indicating a decline in renal function. The mRNA levels forthe major TLR adaptor protein MyD88, the inflammatory cytokines MCP-1and TGF-A1, and the kidney injury markers KIM-1 and CD11b in the kidneywere also significantly (p G 0.5) increased in NZB/W F1 mice compared toNZW mice at 22 wk. Creatinine and cystatin C levels in serum from NZB/WF1 mice, and the mRNA levels for MyD88, MCP-1, TGF-A1, KIM-1, andCD11b in the kidney from NZB/W F1 mice increased significantly (p G 0.5or p G 0.01) between 22 wk and 41 wk. The mRNA levels for the ROSgenerating enzymes Nox2 and Nox4 were significantly (p G 0.01) increased,while the mRNA levels for the anti-apoptotic proteins Bcl-2 and Ube2v1(a TLR effector protein) were significantly (p G 0.01) decreased at 41 wkin NZB/W F1 mice compared to NZW mice. Changes in cytokine levelsmeasured by ELISA tended to parallel the changes in mRNA levels.Conclusions: (1) NZB/W F1 mice develop significant signs of renalpathology at least as early as 22 wk. (2) TLRs play an important role inthe regulation of ROS and inflammation during the development of lupusnephritis in mice.
397
ANALYSIS OF USRDS DATASET INDICATES VIRALINFECTIONS ARE ASSOCIATED WITH INCREASED RISKOF FISTULA FAILURE IN INCIDENT HEMODIALYSISPATIENTS
Garapati H1, Paulson W2,1, White JJ1, Kintziger K1, Nahman S1, ColomboR1, Baer S1, Chebrolu P1, Kheda M1. 1Georgia health Sciences University(GHSU), Augusta, GA and 2Charlie Norwood VAMC, Augusta, GA.Purpose of Study: ESRD is associated with arteriosclerosis and increasedarterial stiffness. This stiffness impairs vessel dilatation after native arterio-venous fistula (AVF) creation, thereby promoting AVF thrombosis andfailure (Kheda NDT 2010). Viral infections, such as HIV and hepatitis C(HCV), are also associated with increased stiffness. We tested the hypothesisthat HIV, HCV, and hepatitis B (HBV) infection are independently associatedwith AVF failure in incident hemodialysis (HD) patients.Methods Used: All incident HD cases in the USRDS dataset for calendaryears 2005-07 were queried. Demographics were obtained from validatedUSRDS data, and access type was derived from form CMS-2728, sub-mitted to Medicare on every new outpatient HD patient. The criteria for AVFfailure were derived from Medicare A datasets containing ICD-9 and CPTbilling codes for AVF related complications. HIV, HCV or HBV infectionwas inferred from serologies and determined from the appropriate ICD-9billing codes.Summary of Results: For the 3 year study period, 259,224 patients with80,825,083 claim observations were analyzed. AVF was the access used inthe first dialysis in 33,925 patients, and 49.8% met criteria for AVF failure.Mean age was 64 years; 65% were male, 68% were Caucasian, 26% wereAfrican American. Positive viral serologies: HIV (N=204, 0.6%), HCV(N=712, 2.1%) and HBV (N=274, 0.8%). Relative risk (RR) of AVF failurewas highest among HIV positive patients (RR 1.54, 95% confidence interval[CI] 1.42-1.68). RR of AVF failure in HCV was 1.25 (CI 1.20-1.31) and inHBV was 1.21 (CI 1.13-1.30).Conclusions: AVF failure occurred in nearly 50% of incident HD patients.Positive serologies for HIV, HCV, and HBV were associated with increasedrisk of AVF failure, with HIV having the highest risk. We speculate thatincreased arterial stiffness in these patients may help explain these adverseoutcomes.
398
VASCULAR ACCESS MANAGEMENT IN PATIENTS WITHFAILING KIDNEY TRANSPLANTS
Dawoud D, Harms J, Williams T, Kumar V, Allon M. University of Alabamaat Birmingham, Birmigham, AL.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 485
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Purpose of Study: Despite recommendations by NKF/KDOQI and FistulaFirst to increase pre-dialysis vascular access (VA) placement in CKDpatients, onlyÈ20% of U.S. patients initiate HD with a permanent access.The proportion is higher among those patients with at least 1 year of pre-HD nephrology follow up. There has been extensive publication on pre-HD VA management in patients with advanced CKD, but very little on VAplanning in those with failing kidney transplants (KTx). The goal of ourstudy was to compare pre-HD VA management in the 2 groups.Methods Used: We compared VA management in 2 groups of patientswho initiated HD during a 5-year period:(1) those with a failed KTx,and(2) those with advanced CKD.
The analysis was restricted to patients with Q1 year of follow up andQ3 nephrology visits prior to initiating HD. Patient demographics, comor-bidities, and pre-HD VA surgery were extracted. Differences between groupswere analyzed by the t-test and Chi-square test.Summary of Results: As compared to patients initiating HD after ad-vanced CKD, those initiating HD after a failed KTx were younger, less likelyto be black, and less likely to have diabetes or CHF (Table). The proportion ofpatients with pre-HDVA surgery was lower in the group with the failing KTx(41 vs 60%; hazard ratio 0.69; 95% CI 0.54-0.87, p=0.0008). The proportionof fistulas placed was similar in both groups (70 vs 75%,p=0.54).Conclusions: Patients with a failing KTx are substantially less likely toreceive VA surgery prior to initiation of HD, as compared to patients withCKD. This difference occurred despite the younger age and lower comor-bidity in the failing KTx group, factors that would favor fistula success.The reason for this discrepancy is unknown, but may be due to a greaterfocus on salvaging the failing KTx, at the expense of advanced VA plan-ning. Systematic efforts are needed to increase VA surgery in patients withfailing KTx.
Cardiovascular II
9:00 AMSaturday, February 23, 2013
399
CAUSES OF PERSISTENT HYPOMAGNESEMIA IN PATIENTSREFERRED WITH CARDIAC ARRHYTHMIAS
Farah V, Adeboye AA, Yusuf JA, Weber KT. University of Tennessee HealthScience Center, Memphis, TN.Purpose of Study: Hypomagnesemia is pathophysiologically linked tocritical supra- and ventricular arrhythmias and serious morbidity. Gastroin-testinal losses and diuretic-related urinary losses are frequent causes oftransient hypomagnesemia readily corrected by Mg2+ supplementation. Notto be overlooked are disorders responsible for a persistent hypomagnesemiadue to urinary Mg2+ wasting. Herein we review such cases, with or withouthypokalemia, and which could not be easily corrected with cation supple-mentation in patients with cardiac arrhythmias. We identified 3 disorders inwhich urinary Mg2+ wasting was present.Methods Used: 18 patients were referred to the cardiology service at theRegional Medical Center in Memphis for management of their cardiacarrhythmias and who were found to have hypomagnesemia. Evaluationincluded serial monitoring of serum electrolytes and Mg2+ with ECG inter-pretation and assessment of repolarization using QTc interval. Cation sup-plements were used to correct hypomagnesemia and hypokalemia. Whenhypomagnesemia was persistent a random spot urine (U) sample was ob-tained to determine fractional excretion (FE) of Mg2+: FEMg=UMg�
PCr�100�(0.7�PMg)�UCr. Urinary Mg2+ excretion is markedly reducedwith dietary Mg2+ deficiency. P, plasma; Cr, creatinine.Summary of Results: 5 normotensive patients (51T15 yrs; 4 males) who pre-sented with hypomagnesemia (1.2Y1.7 mg/dL), hypokalemia (2.7Y3.7 mEq/L)and QTc prolongation (470-50 ms) were found to have the Gitelman syn-drome, where FEMg (4.7T14.8%) and transtubular K+ gradient (6.8Y24.8)were increased. 10 hypertensive patients (63T4 yrs; 6 females) with Connsyndrome (aldosterone:renin 55T10; normal G23), having reduced serumMg2+ and K+ in 7 patients and QTc prolongation (473T5 ms) in all 10.3normotensive patients (51T10 yrs; 3 females) with an inherited renal tubulardisorder, where serum Mg2+ was low (mean 1.6 mg/dL), K+ was normal(mean 4.46 mmol/L) and FEMg was increased (6.62; normal G2.0%). Spiro-nolactone and supplemental Mg2+ led to correction of hypomagnesemia andelimination of supra- and ventricular arrhythmias in all cases.Conclusions: Urinary Mg2+ wasting associated with the syndromes ofGitelman and Conn or due to tubular defects is an important cause of per-sistent hypomagnesemia that can lead to arrhythmias.
400
ANGIOTENSIN II INHIBITS SATELLITE CELLPROLIFERATION AND PREVENTS SKELETAL MUSCLEREGENERATION
Yoshida T1, Galvez S1, Tiwari S1, Rezk B1, Semprun-Prieto LC1, SukhanovS1, Higashi Y1, Yablonka-Reuveni Z2, Delafontaine P1. 1Tulane UniversitySchool of Medicine, New Orleans, LA and 2University of Washington Schoolof Medicine, Seattle, WA.Purpose of Study: Cachexia is a serious complication of many chronicdiseases, such as congestive heart failure (CHF) and chronic kidney disease(CKD). Although patients with advanced CHF or CKD often have increasedangiotensin II (Ang II) levels and cachexia and Ang II causes skeletal musclewasting in rodents, the potential effects of Ang II on muscle regeneration areunknown. We aimed to analyze the effect of Ang II on skeletal muscle stem(satellite) cell function and skeletal muscle regeneration.Methods Used: Cardiotoxin was injected into hindlimb muscles ofC57BL/6 mice and Ang II (1.5 Kg/kg/min) was infused via osmotic mini-pump. The number of regenerating myofibers was quantified by H/E stain-ing, and expression of satellite cell (SC) proliferation/differentiation markers(MyoD, myogenin and active-Notch) was analyzed by quantitative RT-PCR(qPCR) and immunoblotting. SC number was quantified in Myf5nLacZ/+
mice, in which SCs express A-galactosidase (A-gal), and using SC markersCD45-/Sca-1-/CD11b-/CD31-/CD34+/Integrin >7+. SC proliferation was ana-lyzed by BrdU incorporation assay. Left anterior descending artery (LAD)ligation was used as a mouse model of CHF post-myocardial infarction.Summary of Results: Ang II reduced the number of regenerating myo-fibers compared to control (71.9% decrease at day 5, pG0.001), and MyoDand myogenin exression (56.5% and 62.5% decrease, respectively, pG0.001).Ang II reduced SC number (39.4 % and 16.7% reduction in A-gal positivityin Myf5nLacZ/+ mice and in SC markers at 7 days, respectively, pG0.01),and this decrease was inhibited by AT1R blockade. There was a high expres-sion of AT1R in SCs, and Ang II suppressed MyoD and active-Notch expres-sion in SCs both in vivo and in vitro, and inhibited SC proliferation in vitro.In LAD-ligated mice, there was a skeletal muscle wasting and reducedSC number.Conclusions: These data show that Ang II signals via the AT1aR on SCsand prevents SC proliferation by suppressing MyoD and Notch signaling,thereby inhibiting normal skeletal muscle regeneration. Ang II-mediated inhi-bition of skeletal muscle regeneration is likely a critical mechanism that plays amajor role in muscle wasting in chronic diseases such as CHF and CKD.
401
ENDOTHELIAL MANIFESTATION OF TUMORALCALCINOSIS
Garcia D, Caperton C, Oregel K, Symes S. University of Miami/JacksonMemorial Hospital, Miami, FL.Case Report:Introduction: Tumoral calcinosis is soft tissue calcification disorder thatcommonly presents at the second or third decade of life, with calcium-rich
Variable Failed TX Advanced CKD p-value
N pts 123 219
Pt age, yrs 47T14 60T14 G0.0001
Age 965 yrs 14 (11%) 84 (38%) G0.0001
Male sex 67 (54%) 109 (50%) 0.40
Black race 71 (58%) 170 (78%) G0.0001
Diabetes 57 (38%) 130 (59%) 0.02
CHF 11 (9%) 41 (19%) 0.02
Pre-HD VA surg 51 (41%) 132 (60%) 0.0008
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
486 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

forming tumor mass forming near large joints such as hip, elbow, andshoulder. Usually its presentation is characterized by the presence of pain-less, calcified masses in juxta-articular sites, particularly around the mainjoints.
Case This is a 57 year old woman with a past medical history of hyper-tension, diabetes, tumoral calcinosis and schizophrenia paranoid type admittedfor psychotic features. Upon admission, she denied chest pain, palpitations,or shortness of breath, but did endorse stable angina for the past 3 months.She was stable hemodynamically, EKG showed normal sinus rhythm withoutST-T wave changes. Laboratory work revealed a normal calcium level of 8.8but positive troponins (0.32 and 0.33). 2D echo revealed normal ventricularsystolic function with 65% ejection fraction. Coronary CT angiography re-vealed moderate to severe disease in the three main coronaries and one totallyoccluded branch. An outpatient stress test was recommended. The patient re-mained clinically stable, was started on aspirin, amlodipine, metoprolol andstatin and discharged home.Discussion: This case illustrates a presentation of tumoral calcinosis withendothelial invasion of the coronary arteries. Tumoral calcinosis is a depo-sition of calcium in subcutaneous tissues in the absence of abnormal serumcalcium or phosphorus levels; the disease has no other known associationwith renal pathology, metabolic disorders, or collagen diseases. Its mani-festation rarely occurs within endothelial tissue, being more specific andcharacteristic for muscle and subcutaneous tissue in weight-dependent areassuch as the hip, buttocks, and shoulders. The diagnosis can be made by theradiographic findings called ‘‘chicken wire’’ or fibrous wall (radiolucent) inthe tumor and histological analysis with calcium-rich tissue.Conclusion: We present this first documented case of a patient with knowntumoral calcinosis presenting with elevated troponins and severe calcifiedcoronary lesions viewed on coronary CT as a secondary manifestation of hercalcinosis from her tumoral disease.
402
INSULIN-LIKE GROWTH FACTOR-1 PREVENTSPREMATURE CELL SENESCENCE IN VASCULARENDOTHELIAL CELLS VIA UPREGULATION OF GPX1EXPRESSION: A NOVEL MECHANISM FOR IGF-1PREVENTION OF ENDOTHELIAL DYSFUNCTION
Higashi Y, Goodwin B, Pandey A, Delafontaine P. Tulane University, NewOrleans, LA.Purpose of Study: Premature senescence of endothelial cells (ECs) is akey underlying mechanism for the development of endothelial dysfunction,a critical early event in atherogenesis. Insulin-like growth factor 1 (IGF-1)has vascular anti-inflammatory and anti-oxidant effects, thereby preventingatherogenesis in Apo E-/- mice; however precise mechanisms are unclear.We investigated potential effects of IGF-1 on oxidative stress-induced cellsenescence in vascular ECs.Methods Used: Senescence-associated A-galactosidase (A-gal) and gluta-thione peroxidase (GPX) activities were determined by commercially avail-able kits. GPX gene and protein expression levels were assessed byquantitative RT-PCR (qPCR) and western blot. Associations of GPX1 mRNAand RNA binding proteins were assessed by immunoprecipitation followedby qPCR.Summary of Results: In ECs, hydrogen peroxide increased A-gal posi-tivity (2.2T0.2-fold, PG0.05, n=3), however preconditioning with IGF-1(100ng/mL) completely prevented this effect. IGF-1 increased GPX1 ex-pression and activity (2.6T0.2-fold and 4.8T0.5-fold, respectively, n=4,pG0.01), thereby suppressing reactive oxygen species levels by 83T2 %(PG0.01, n=4). These results suggest that IGF-1’s antioxidant effect con-tributes to prevention of cell senescence in ECs and that the effect is, at leastin part, mediated by upregulation of GPX1. IGF-1 did not change GPX1mRNA levels, and 10 ug/mL cycloheximide inhibited the IGF-1 upregula-tion, suggesting translational mechanisms. Translation of GPX1 requiresa unique step of selenocysteine (Sec) incorporation, controlled by Sec-incorporation sequence Binding Protein 2 (SBP2) and eukaryotic elongationfactor Sec-specific (eEFsec). IGF-1 did not alter SBP2 and eEFsec expres-sion levels but decreased GPX1 mRNA levels which co-immunoprecipitatedwith SBP2 by 40 % (PG0.01, n=8), indicating that IGF-1 modulated com-plex formation between SBP2 and GPX1 mRNA, leading to upregulationof GPX1.
Conclusions: IGF-1 regulates Sec-incorporation and GPX1 translationin ECs, thereby upregulating GPX1 synthesis and antioxidant activity andpreventing premature EC senescence. This effect of IGF-1 likely plays acritical role in preventing endothelial dysfunction and atherosclerosis.
403
THE ROLE OF PLASMA D-DIMER TESTING IN DIAGNOSISOF PATIENTS SUSPECTED WITH ATRIAL SOURCETHROMBI
Kadle N1, Ibebuogu U2,1, Gladysheva IP2,1, Yang M1, Robinson VJ1,Figueroa RE1, Sharma GK1, Sazonova IY1. 1Georgia Health SciencesUniversity, Augusta, GA and 2University of Tennessee Health SciencesCenter, Memphis, TN.Purpose of Study: Transesophageal echocardiography (TEE) is the ac-cepted standard to diagnose cardiogenic thromboemboli in patients withatrial fibrillation and ischemic stroke. To minimize costs and risks of TEEwe evaluated the usefulness of a D-dimer test as a supplemental work-upprocedure for patients with suspected atrial source thrombi.Methods Used: Blood samples were collected from 49 patients withmean age 63T15 years (55% males) who were clinically suspected with intra-cardiac thrombi. TEE was requested for indications including: ischemicstroke (47%), atrial fibrillation and flutter (59%). D-dimer levels and hemo-static cell counts were assessed. A non-parametric t-test and Pearson test wereused for statistical analysis.Summary of Results: At a cutoff value of G200 ng/ml, the fibrin D-dimerassay had a sensitivity, specificity, positive predictive value and negativepredictive value of 100%, 19%, 15% and 100% respectively for the diagnosisof intra-cardiac clot. However, it was apparent that an elevated D-dimer level(1877 ng/ml) supported diagnosis of cardio-embolic stroke in a patient byMR angiography, despite negative CT angiography and TEE. Groups witheither negative (n=8) or positive D-dimer levels had comparable clinical char-acteristics with the exception of hyperlipidemia, which was less in the nega-tiveD-dimer group (P=0.034).The only clinical and demographic predictors thatcorrelated with elevated D-dimer were atrial fibrillation (P=0.016; r=j0.345),decreased basophil count (P=0.017), and advanced age (P=0.013; r=0.356).Compared with patients with positive D-dimer test but no clot, those withpositive D-dimer test and confirmed intra-cardiac clot (n=6) had lower LAAvelocity (23.7T8.4 cm/sec vs. 44.2T25.2 cm/sec, P=0.0016), lower eosinophil(0.05T0.05 vs. 0.21T0.05, PG0.001) and basophil (0.00T0.00 vs. 0.03T0.04,PG0.001) counts (103/mm3).Conclusions: The gold standard for clot determination should not be lim-ited to cardiac assessment with TEE and may be supplemented by D-dimerand hemostatic markers. The exclusion of intra-cardiac clot with TEE alonedoes not eliminate the risk of prior thromboembolic events.
404
GLYCERALDEHYDE-3-PHOSPHATEDEHYDROGENASE-INDUCED PRO-SURVIVAL EFFECT INVASCULAR SMOOTH MUSCLE CELLS: POTENTIAL ROLEIN STABILIZATION OF ATHEROSCLEROTIC PLAQUE
Sukhanov S, Yoshida T, Kim C, Snarski P, Delafontaine P. TulaneUniversity, New Orleans, LA.Purpose of Study: We have shown that oxidized low density lipoprotein(OxLDL) co-localized with apoptotic smooth muscle cells (SMC) in athero-sclerotic plaque and that OxLDL downregulated expression of glyceraldehydes-3-phosphate dehydrogenase (GAPDH) in cultured SMC via a redox-sensitivemechanism. We studied whether GAPDH downregulation mediates SMCapoptosis and would GAPDH overexpression protects SMC against oxidant-induced cell death.Methods Used: GAPDH expression was measured by immunoblotting,cytotoxicity - LDH release assay, cell apoptosis - Annexin V assay, apoptosis-associated DNA fragmentation - TUNEL, protein oxidation - N-tyrosine immu-nostaining, DNA oxidation - staining for 8-oxo-2’-deoxyguanosine.Summary of Results: OxLDL (80 ug/ml) or H2O2 (220 uM, 16h) de-creased GAPDH protein by 78T5% and 55T5%, respectively and inducedSMC apoptosis and DNA fragmentation. Koningic acid (a specific inhibitor
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 487
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of GAPDH activity) potentiated H2O2-induced cytotoxicity (4.0T0.3-foldincrease, PG0.01) and DNA fragmentation induced by OxLDL (2.5T0.2-fold,PG0.05) or by H2O2 (8.5T0.6-fold, PG0.001). A/GAPDH siRNA (50 nM)reduced GAPDH protein by 88T6% and potentiated OxLDL- and H2O2-induced DNA fragmentation (1.9T0.2 and 7.0T0.9-fold increase, respec-tively) suggesting that maintenance of GAPDH activity is critical for DNAintegrity and cell survival under oxidative stress. GAPDH overexpression withpCMV-GAPDH vector reduced H2O2-induced cytotoxicity (68T5% decrease,PG0.01) and partially blocked DNA fragmentation (74T4% decrease, PG0.005).Alpha-smooth muscle actin-positive and mainly apoptotic SMC in mouseatherosclerotic plaque fibrous cap had increased levels of oxidative stressmarker (43T10% increase in N-tyrosine staining, PG0.05), reduced GAPDHlevels (48T5% decrease, PG0.05), and elevated DNA oxidation (22T5% in-crease, PG0.05) vs. medial SMC.Conclusions: GAPDH downregulation mediates oxidant-induced SMCapoptosis and forced expression of GAPDH protects SMC from H2O2-induced cell death, potentially via activation DNA repair. Plaque SMC haveincreased oxidative stress, reduced GAPDH and damaged DNA. These datademonstrate that GAPDH is critical molecule for SMC survival and preven-tion of plaque destabilization.
405
IMMUNOFLUORESCENCE STUDY DEMONSTRATES THEINTERNALIZATION AND TRAFFICKING OF GUANYLYL(GUANYLATE) CYCLASE/NATRIURETIC PEPTIDERECEPTOR-A IN HUMAN EMBRYONIC KIDNEY-293 CELLS
Mani I, Garg R, Nguyen VA, Pandey KN. Tulane University, New Orleans, LA.Purpose of Study: Cardiac hormone atrial natriuretic peptide (ANP)modulates blood pressure and blood volume by activation of the guanylylcyclase/natriuretic peptide receptor-A (GC-A/NPRA) and subsequent intra-cellular second messenger cGMP. Advances in the development of proteinsconjugated with the enhanced green fluorescence protein (eGFP) providefluorescence based analysis of protein trafficking in individual cells. Theaim of this study was to analyze internalization and trafficking of NPRAin human embryonic kidney-293 (HEK-293) cells through immunofluores-cence and confocal microscopy.Methods Used: A chimeric protein consisting of the natriuretic peptidereceptor-A and enhanced green fluorescence protein (NPRA-eGFP) was usedfor analyzing receptor internalization, trafficking, and recycling in HEK-293Cells. Cells were stably transfected with cDNAs encoding wild type NPRA-eGFP. HEK-293 cells were treated with natural ligand ANP at different timecourse (0, 1, 2.5, 5, 10, 15, and 30 minutes) and internalization of receptorwas analyzed through confocal immunofluorescence microscopy.Summary of Results: In control cells without ANP treatment, all recep-tors were localized on plasma membrane. Internalization of NPRA-eGFPwas optimum at 5 min and was almost completed at 10 min. Colocalizationof NPRA-eGFP with early endosomal marker 1 (EEA1) and lysosome-associated membrane proteins-1(LAMP-1) was gradually increased from5 and 10 min. After 10 min receptors were recycled back on plasmamembrane and it was confirmed with Pan-cadherin marker. Colocalizationof NPRA and Pan-cadherin was again observed after 10 and 15min. After15Y30 min incubation with ligand, the internalized receptor was recycled toplasma membrane.Conclusions: Our results suggest that after ligand binding, NPRA is rapidlyinternalized and trafficked from the cell surface to cell interior and redistrib-uted to the early endosomes and lysosomes.
406
THE THERAPEUTIC USE OF SYSTEMICALLYADMINISTERED ENDOTHELIAL CELLS FOR VASCULARDYSFUNCTION IN A RAT MODEL OF CHRONICKIDNEY DISEASE
Pacurari M, Xing D, Hilgers RH, Guo Y, Chen Y, Oparil S, Hage FG. UAB,Birmingham, AL.Purpose of Study: Endothelial dysfunction is a hallmark of CKD. Dueto high risk of cardiovascular morbidity and mortality in CKD, finding noveltherapeutic modalities to improve endothelial function in CKD warrants thedevelopment of new interventions. This study tested the hypothesis that
systemic transfusion of rat aortic endothelial cells (EC), via increasing nitricoxide synthase (NOS) activity, improves vascular function in a rat modelof CKD.Methods Used: Male Sprague-Dawley rats (11 wk) underwent bilateralsham surgery (S) or 5/6 nephrectomy (Nx). Six wks after Nx, EC (1.5 �106 cells/rat) or vehicle (Nx+Veh) were transfused intravenously. One wklater, serum creatinine, serum asymmetric dimethylarginine (ADMA), andvascular reactivity of mesenteric artery was assessed.Summary of Results: Sensitivity of endothelium-dependent relaxation(pEC50) to acetylcholine (ACh) was significantly decreased by Nx comparedto S (7.21 T 0.1 vs 8.01 T 0.06) and improved by EC transfusion (7.56 T 0.05).Maximum vasodilation (Emax to 10 KM ACh) was significantly impaired byNx (17% decrease vs S), and improved by EC transfusion (14 % increase vsNx). Using selective NOS inhibitors L-NPA (2KM) for nNOS, L-NIO (10KM)for nNOS, and 1400W (10 KM) for iNOS, we demonstrate that Nx im-paired eNOS activity (1.9-fold vs S), and EC transfusion improved eNOS ac-tivity (1.7-fold vs Nx). Non-selective inhibition of NOS isoforms, COX, andsoluble guanylate cyclase with L-NAME (100 KM) + indomethacin (10 KM) +ODQ (10 KM) eliminated the effects of Nx and EC transfusion on Emax,indicating that these effects were mediated by NOS. Serum creatinine wassignificantly increased by Nx, and EC transfusion had no effect on serumcreatinine. Plasma ADMA (natural inhibitor of eNOS) was significantly in-creased by Nx, and decreased by EC transfusion. mRNA expression of DDAH(enzyme that degrades ADMA)was significantly decreased by Nx, and restoredby EC transfusion.Conclusions: EC transfusion attenuates CKD-induced endothelium-dependent vascular dysfunction by regulating DDAH1 expression and en-hancing eNOS activity. These results suggest that EC-based therapy couldprovide a novel cell therapeutic strategy to improve vascular function in CKD.
Allergy, Immunology, and Rheumatology IIConcurrent Session
1:00 PMSaturday, February 23, 2013
407
PHENOTYPIC B CELLS ANALYSIS IN IDENTICAL TWINSDISCORDANT FOR COMMON VARIABLEIMMUNODEFICIENCY
Szymanska Mroczek E1, Ippolito G5, Zemlin M6, Osborne J1, Crossman D3,Hwangpo T2, Lefkowitz E1, Georgiou G5, Brown E4, Schroeder H1,2.1University of Alabama at Birmingham, Birmingham, AL; 2University ofAlabama at Birmingham, Birmingham, AL; 3University of Alabama atBirmingham, Birmingham, AL; 4University of Alabama at Birmingham,Birmingham, AL; 5University of Texas at Austin, Austin, TX and 6UniversityMarburg, Marburg, Germany.Purpose of Study: Common Variable Immune Deficiency (CVID) is themost common primary immune deficiency under the care of immunologistsand defined by unexplained immunoglobulin (Ig) depression. Family mem-bers of CVID patients also often suffer with recurrent sinopulmonary in-fection (RESPI) with normal Ig levels. We identified a set of HLA B44positive identical female twins (IT) who suffer recurrent pulmonary infec-tions and are discordant for CVID (IgM 45, IgG 477, IgA 91 mg/dL) andRESPI (IgM 107, IgG 733, IgA 95 mg/dL).Methods Used: To better define the block in BC development, we isolated6 distinct BC populations: memory IgD+/IgD-, plasmacyte, immature, tran-sitional, and mature from blood of discordant IT. Deep sequencing of Ig(DSIg) transcripts was analyzed.Summary of Results: Flow cytometric analysis of BC revealed similarimmature BC, but decreased numbers of transitional and mature BC in theCVID twin. DSIg repertoires expressed by transitional and mature BC shownsignificant divergence in VH family gene segments use, CVID favoring VH4and RESPI favoring VH1. The RESPI IT used JH6 more frequently whileCVID IT used JH3. The amino acid composition of CDR-H3 in ITwas com-pared to control; both patients and control tyrosine usage in transitional BCwas similar (È15%). Tyrosine usage greatly diverged in mature BC, withcontrol maintaining the 15% level, RESPI twin increasing to 25% and CVIDtwin decreasing to 10%. Whole genome sequencing revealed homozygosity
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
488 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

for a rare S639N polymorphism (0.984 POlyPhen score, 0.05 SIFT score)and heterozygosity for L174V (SIFT 0.04).Conclusions: These findings suggest that in addition to an acquired blockin BC development at the transitional stage, CVID IT produces an Ig rep-ertoire that is markedly depleted of tyrosine. This may help explain why thefunction of Ig repertoire in CVID is more impaired than what might beexpected by serum Ig level alone.
408
CHARACTERIZATION OF B CELL SUBSETS IN CVID ANDRESPI PATIENTS
Hwangpo T2,1, Szymanska E1, Liu C1, Brand M1, Schroeder H1. 1Universityof Alabama at Birmingham, Helena, AL and 2University of Alabama atBirmingham, Birmingham, AL.Purpose of Study: Recent studies suggest that disease severity in CVIDcan correlate with a reduction in the memory B cell compartment. We havepreviously noted that classed switched memory B cells to be deficient inCVID patients compared to controls and that IgM Memory B cells are de-creased in RESPI patients. Now, we have expanded our panel to examineimmature, transitional, and naBve B cells in this study.Methods Used: Whole blood was collected from our patients from fromFebruary to September 2012. Marginal zone-like memory B cells, IgMmemory B cells, class-switched B cells, immature B cells, naBve B cells, andtransitional B cells were examined via FACS. Unpaired t-test was used toanalyze the means of these cells.Summary of Results: We collected 126 patient samples that fit our defi-nitions of CVID, RESPI, and control subjects. Of which, 67% were females,and the average age was 52. When comparing class-switched B cell popu-lations, there was a significant trend for less class-switched B cells in CVIDpatients than control healthy patients (pG0.0001) and in CVID patientscompared to RESPI patients (pG0.02). There were less total transitionalcells, immature B cells, and naBve B cells in CVID patients compared tocontrols (pG0.004, pG0.04, pG0.0004, respectively). There were less totalnaBve and transitional cells in RESPI compared to controls as well ( pG0.04and pG0.14, respectively).Conclusions: We postulate that the transition from RESPI patients toCVID patients may involve the development of defects in B cell maturationsignaling and B cell memory generation. Further detailing of IgA and IgGmemory B cell subsets will be our next endeavor.
409
AGE OF SYSTEMIC LUPUS ERYTHEMATOSUS ONSETAMONG CIGARETTE SMOKERS
Aggarwal R1,2, Thompson DM1, Namjou B2, Scofield HR1,2,3. 1OUHSC,Okc, OK; 2OMRF, Okc, OK and 3VA, Oklahoma City, OK.Purpose of Study: Recent epidemiological studies have proposed thattoxic agents in cigarette smoke may operate to release or alter autoantibodiesand may cause mutations in immunoregulatory genes. We undertook this studyto enhance our understanding of the association of smoking as a risk factorin systemic lupus erythematosus (SLE).Methods Used: Dataset 1 = 1711 patients with SLE who responded to thequestion ‘‘Have you ever smoked cigarettes?’’ on a standard questionnaire.Dataset 2 = (subset of Dataset 1) included 611 SLE patients who smokedand were matched for age within five years, gender and ethnicity with 611non-smoking SLE patients. Dataset 3 = 821 SLE patients and 821 healthycontrols matched for age within five years, gender and ethnicity. To addresssmoking as a risk factor for SLE in our cohort, we studied matched SLE pa-tients and healthy controls. All SLE patients met at least four AmericanCollege of Rheumatology classification criteria. Independent t-tests comparedthe mean age of onset for SLE in dataset 1 and dataset 2 between smokersand non-smokers. The proportion of smokers in matched pairs of SLE casesand controls (Dataset 3) were compared using a McNemar Chi Square test.SAS version 9.1 was used for statistical analysis.Summary of Results: Dataset 1=Independent t-tests found the mean ageof onset for smokers was 37.7(n=696,SD=12.73) and for non-smokers was32.6 (n=823, SD=13.28) which is 5.06 years later than for non-smokers(95% CI: 3.75, 6.38, pG0.0001). Dataset 2= t-tests found the mean age of
onset for smokers was 36.52 (n=611,SD=12.35) and for non-smokers was34.94 (n=611, SD=12.58) which is 1.6 years later than for non-smokers(95% CI:3,0.2, pG0.026). Dataset 3= the odds ratio of smokers (821 cases-control pairs) by McNemar Chi Square test was found to be 1.27 (W2=5.18;df= 1; p=0.02).Conclusions: In a large cohort of SLE patients and matched controls,smoking tobacco was confirmed as a risk factor for disease with odds ratiossimilar to those found for genes that contribute to the susceptibility of SLE.Meanwhile, smoking SLE patients had a later onset of disease than non-smoking patients. Interpretation of these data, which differ from the effect ofsmoking on ulcerative colitis but may be similar to the effect on Crohn’sdisease, is difficult. Cigarette smoking may be a particular risk factor for lateonset SLE.
410
PERSISTENT PLEURAL EFFUSION DUE TO NICKELALLERGY FOLLOWING USE OF IMPLANTABLE BARFOR PECTUS EXCAVATUM REPAIR
Korah-Sedgwick M1, Wall L1,2, Paris K1,2. 1LSUHSC, New Orleans, LAand 2LSUHSC, New Orleans, LA.Case Report:Purpose: Allergic reaction to surgical hardware due to metal allergy iswell described in the adult literature. In pediatrics, surgically-related nickelallergy has recently gained more attention in those receiving the Nuss pro-cedure which involves an implantable stainless steel bar for pectus ex-cavatum repair. We report such a case in a patient with no prior history ofmetal allergy, rash, or atopy.Methods: Skin patch testing was performed using T.R.U.E. TEST\.Results: A 16-year-old male with history of pectus excavatum status postNuss procedure presented with a one week history of fever, night sweats,and shortness of breath which persisted despite oral antibiotics. Evaluationrevealed eosinophilia, elevated WBC, ESR, CRP, and pleural effusion. Hewas admitted by Pediatric Surgery with subsequent chest tube placement andIV antibiotics. Clinical improvement was demonstrated by decreased short-ness of breath and resolution of fever. Despite negative blood and pleuralfluid cultures, chest tube drainage remained significant. Pleural fluid showedlymphocyte and eosinophil predominance. Allergy/Immunology was con-sulted for the possibility of an allergic reaction to the implantable steel bar.Patch testing showed clear positivity to nickel. With nickel allergy thus iden-tified, antibiotics were discontinued and a two week course of oral steroidswas started which led to rapid cessation of chest tube drainage. He remainsasymptomatic 3 months following treatment with steroids.Conclusion: Stainless steel surgical hardware contains several potentiallyallergenic metals including nickel. Presenting signs and symptoms may bedelayed and include rash, granuloma, fever, or effusion which may be con-fused with infection. Physicians must consider an allergic reaction as partof the differential. A pre-operative screening questionnaire may identify pa-tients who have previously reacted to nickel or other metals. However, asin our patient, there may be no prior history of metal allergy or atopy. Treat-ment with oral steroids is often sufficient, although hardware removal maybe indicated. Patients who respond to steroids should be monitored closely forpossibility of recurrence of symptoms.
411
A CASE OF ABDOMINAL PAIN RESULTING IN THEDIAGNOSIS OF SUSPECTED IGG4-RELATED DISEASE
McCoy E, Fontenot E, Houser K. University of Tennessee Health ScienceCenter, Memphis, TN.Purpose of Study: IgG4-related disease is a fibroinflammatory condi-tion characterized by tissue infiltration by IgG4-positive plasma cells andT lymphocytes with resultant tissue fibrosis, often, but not always accom-panied by elevated serum IgG4 levels. We report a case of aortitis thatresulted in a presumptive diagnosis of IgG4-related disease.Methods Used: Case ReportSummary of Results: A 48 year old African American male with historyof cerebrovascular accident, essential hypertension, superior vena cava syn-drome, and fibrosing mediastinitis presented to our emergency department
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 489
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

with abdominal pain and CT findings of aortitis extending from the distalabdominal aorta to the bilateral common iliac arteries. Laboratory evaluationincluded white blood cell count, which was within normal limits, as well aspurified protein derivative, human immunodeficency virus antibody, rapidplasma reagin, anti-nuclear antibody, rheumatoid factor, anti-citrullinatedprotein, anti-neutrophil cytoplasmic antibodies, anticardiolipin antibody, andlupus anticoagulant, all of which were negative. The erythrocyte sedimen-tation rate was elevated at 56mm/hr (NR 0-20). Immunoglobin G subclass3 levels were elevated at 166mg/dl (NR 41-129). Immunoglobin G subclasses1, 2, and 4 were within normal limits. Tissue biopsy was not done becausethere was no site on the aorta which would have been technically feasible.Further history was obtained regarding the patient’s previous diagnosis offibrosing mediastinitis. Surgical pathology from a right middle lobectomyperformed 20 years prior to presentation showed fibrotic infiltration butpreparation did not include IgG4 staining. In light of the history of two IgG4related conditions, fibrosing mediastinitis and aortitis, a presumptive diag-nosis of IgG4 -related disease was made and prednisone 1 mg/kg/day wasinitiated. At four week follow-up, the abdominal pain has resolved and thepatient is doing well. Prednisone doses are being tapered and a repeat CTof the aorta will be done at 6 weeks.Conclusions: This case highlights the fact that IgG4-related disease isa diverse, increasingly recognized clinical entity. A high index of suspicionfor IgG4-related disease should exist in the presence of diseases such asfibrosing mediastinitis and aortitis, even if IgG4 levels are normal.
412
THE EFFECT OF TEMSIROLIMUS ON TNF SECRETIONOF RAW 264.7 MACROPHAGES STIMULATED BYCOMMUNITY-ACQUIRED METHICILLIN-RESISTANTSTAPHYLOCOCCUS AUREUS
Spentzas T1,2, Meals B1,2, English B1,2. 1University of Tennessee, Memphis,TN and 2Children’s Research Foundation, Memphis, TN.Purpose of Study:Introduction: S. aureus is a major cause of pediatric sepsis. Sepsis resultsfrom a massive cytokine release by macrophages in part through the NMDAsignaling pathway. Rapamycin’s binding to the mammalian target of rapa-mycin complex 1 (mTORC1) increases TNF-> production at low doses, butdiminishes TNF production at high doses. Temsirolimus is an ester analog ofrapamycin with better solubility.Hypothesis: Is temsirolimus suppressing, the septic inflammatory macro-phage reaction similarly as rapamycin?Methods Used: RAW 264.7 murine macrophages were exposed toMidwest-2 wild type (MW-2) methicillin-resistant S. aureus. Cells were ex-posed to temsirolimus, and incubated for 18-24 hours. ELISAs for TNF weredone on supernatants.Summary of Results: Temserolimus suppressed the TNF production ofthe MW2 stimulation was 0.86*, 0.74*, 0.69*, 0.68* of the control (SE 0.06)for doses 2, 20, 100, 200 ng/mL of temsirolimus respectively. The (*) indi-cates significant difference from the control at pG0.05.
Comparing temsirolimus 20 ng/mL and rapamycin 100 ng/mL (LACinduced stimulation), temsirolimus at 20 ng/ml reduces the TNF 0.65* ofthe control compared to 0.62* induced by rapamycin 100 ng/ml and 0.62*induced by both together (SE =0.06). All are different from the control atpG0.05 but not from each other. In similar setting but MW 2 stimulation,temsirolimus at 20 ng/ml suppresses the TNF 0.62* of the control comparedto 0.63* suppressed by rapamycin 100 ng/ml and 0.59* of both together(SE =0.06). All are different from the control at pG0.05 but not from eachother and the pattern is similar with the LAC stimulation.Conclusions: Temsirolimus has a dose related suppression of TNF in-duced by S.aureus stimulated murine macrophages. When combined withrapamycin, the effects were not augmented.
413
DERMATOMYOSITIS DEVELOPING AFTER NON-HODGKINLYMPHOMA: NOT A PARANEOPLASTIC PROCESS
Mohamed N, Dare J, Morris P. UAMS, Little Rock, AR.Purpose of Study: Case Report.Methods Used: Medical record and literature review.
Summary of Results: A 5 year old girl was referred to a pediatric rheu-matologist for lower extremity pain. After evaluation, the rheumatologistwas concerned about the possibility of malignancy. She was referred to theoncologist, and was ultimately diagnosed with non-Hodgkin’s lymphoma(NHL). The lymphoma was treated, and she achieved remission.
Sixteen months into remission, the child developed a rash. The rashoriginally involved the face, but spread to involve the chest, elbows, andknuckles. She was also complaining of muscle pain, fatigue, and a 4 poundweight loss.
The girl was referred back to rheumatology, and her physical findingsand laboratory data were consistent with juvenile dermatomyositis (JD).The rheumatologist and the oncologist agreed that relapse of malignancymust be considered before finalizing her diagnosis and starting treatment. Acomplete evaluation revealed no malignancy. Therapy including steroidsand methotrexate was initiated, and the child has had an excellent responseto date. Oncology surveillance continues for her previous lymphoma.Conclusions: Approximately 13-42% of adults diagnosed with dermato-myositis (DM) are found to have an associated malignancy.(1-3) However,a review of paraneoplastic JD concluded that pediatric patients do not de-mand a rigorous malignancy evaluation unless circumstances suggest thepresence of a malignancy.(4) In rare reported cases of paraneoplastic JD,the two events occur an average of 12 months apart.(4)
This child appears to have two unrelated diagnoses. Ironically, she ini-tially presented to the rheumatologist with NHL, and subsequently presentedto the oncologist with JD.
References:
1. Buchbinder R, Forbes A, Hall S, Dennet X, Giles G. Incidence ofmalignant disease in biopsy proven inflammatory myopathy.Ann Intern Med 2001;134:1087Y95.
2. Chen Y-J, Wu C-Y, Shen J-L. Predicting factors of malignancyin dermatomyositis and polymyositis: a case-control study.Br J Dermatol 2001;144:825Y31.
3. Hill CL, Zhang Y, Sigurgeirsson B, Pukkala E, Mellemkjaer L, Airio A,et al. Frequency of specific cancer types in dermatomyositis andpolymyositis: a population-based study. Lancet 2001;357:96Y100.
4. Morris P, Dare J. Juvenile Dermatomyositis as a ParaneoplasticPhenomenon: an Update. J Pediatr Hematol Oncol 2010Apr;32(3):189Y91.
414
EVALUATION OF ANAPHYLAXIS MANAGEMENT IN APEDIATRIC EMERGENCY DEPARTMENT
Sidhu N, Jones S, Storm E, Thompson T. Arkansas Childrens Hospital,Little Rock, AR.Purpose of Study: The purpose of this study is to assess the efficacy ofan updated guideline to improve the medical management of Pediatric ana-phylaxis in the Emergency Department.Methods Used: This is a retrospective study involving chart review only.Patients (children between the ages of 0-18) who presented to the ArkansasChildren’s Hospital Emergency Department between January 2004 throughJanuary 2006 and those from July 2007 through July 2011 for the treatmentof allergy/anaphylaxis have been evaluated. Subjects were identified usingICD-9 codes for anaphylaxis. The following variables are being collectedvia chart review and entered into excel spreadsheets: patient demographics(age, gender, race/ethnicity), insurance information, initial presentation (symp-toms, time of arrival), allergen source, time elapsed from initial symptomsto epinephrine usage, amount/dosage of epinephrine used, other treatmentmodalities used, patient education, referral to PCP and/or Allergy Immunol-ogy clinic, self-injectable epinephrine prescription and user education, dis-position (home vs. admit), observation period length, and occurrence ofbiphasic reaction.Summary of Results: Currently 1894 charts have been assessed thatcontain relevant ICD-9 code diagnosis. Of those charts, 100 have beenreviewed. 44 (44%) were removed from the study due to incorrect ICD 9diagnosis, 32 (32%) were allergic reactions, and 24 (24%) were determinedto be anaphylaxis secondary to multiple causes. Of those with the diagnosis
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
490 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of anaphylaxis, 9 patients (37.5%) received epinephrine (at home vs. hos-pital) and 15 patients (62.5%) did not receive epinephrine. The most com-mon cause of anaphylaxis was unknown in 9 patients (37.5%) followed bynuts in 5 patients (20.8%). Chart review is ongoing.Conclusions: This study will allow investigators to evaluate the efficacyof an updated guideline to improve the medical management of pediatricanaphylaxis in the emergency department. We anticipate that with the estab-lishment of such guidelines there has been improvement in management andeducation of anaphylaxis with persistent deficiencies without full guidelinecompliance. The study will also help in the establishment of prospectiveguidelines-based anaphylaxis protocol that would be subsequently imple-mented in the Emergency Department at Arkansas Children’s Hospital.
415
THE PULSELESS CLINIC PATIENT: A CASE OFEXTRACRANIAL GIANT CELL ARTERITIS
Lirio EA, Majithia V, Sandhu A. University of Mississippi, Jackson, MS.Case Report: Giant Cell Arteritis is a large vessel vasculitis that affectsbranches off the carotid artery in patients older than age 50. Isolated extra-cranial manifestations of this disease are becoming increasingly more rec-ognized with the advent of newer imaging modalities.
A 65 y.o. caucasian lady was seen in consultation for bilateral upperextremity pain, weight loss and fatigue that began one year prior. No com-plaints of headaches or vision changes. Physical exam was significant forcoolness and dusky discoloration of the hands. Blood pressure was un-attainable except in the lower extremities. Radial pulses were also absent. Lababnormalities included a markedly elevated sedimentation rate and c-reactiveprotein. ANCA, cyroglobulins and serology for Hepatitis B and C were allnegative. Antiphospholipid antibody screen was likewise negative. MRAdemonstrated stenosis plus adventitial enhancement of the bilateral subclavianarteries. There was subtotal stenosis of the left subclavian with total stenosisseen of the right axillary artery with collateral flow to the brachial. Adven-titial enhancement also involved the aortic arch. The patient was started ona high dose of prednisone with improvement in her constitutional symp-toms. Prednisone was decreased and azathioprine added as a steroid sparingagent successfully. Extremities still remained cyanotic with absence of pulses.Follow up MRA revealed gradual improvement of the left subclavian stenosisand decreased enhancement of these vessels.
Giant Cell Arteritis is characterized by inflammation of the branchesoff the carotid artery, resulting in headaches and retinal ischemia if left un-treated. Up to 30% of GCA patients have isolated extracranial manifestationsdiagnosed primarily with newer imaging modalities. Cohorts have identifiedbranches off the subclavian and aorta as frequent areas of involvement. Indi-viduals with large vessel vasculitis experience a good clinical course withearly treatment. Late sequelae include large artery stenosis and aortic aneu-rysm formation seen in delayed treatment and longstanding symptoms.
416
I AM GETTING TIRED AND SHORT OF BREATH
Musa F, Engel LS, Espinoza LR. LSU Health Sciences Center, NewOrleans, LA.Case Report:Case: A 54 year old woman with history of systemic lupus erythematosus(SLE) presented with dry cough, dyspnea and fatigue for one week. Thepatient was taking hydroxychloroquine, prednisone, lisinopril, and HCTZfor years without rheumatology follow up. Vital signs at admission were un-remarkable and physical examination revealed pale conjunctiva and bilateralsclera icterus. The initial laboratory work-up demonstrated a hemoglobinof 5.9g/dL, hematocrit of 17.6%, reticulocyte count of 14 %, platelets of34,000/ul, total billirubin 6.2, indirect billirubin 5.9, LDH 514 u/l, fibrinogen249, D.dimer 285, haptoglobin 15, and peripheral smear did not show schis-tocytes. Coagulation studies were normal, direct antiglobulin test was positivefor warm antibodies IgG. Chest x ray was unremarkable. Based on the clini-cal presentation, a lupus history and laboratory findings, a diagnosis of auto-immune hemolytic anemia was made. The patient was initially treated withmethylprednisolone for one day and then switched to oral prednisone, folicacid, and intravenous immunoglobulin (IVIG). The patient had a poor responseafter 2 days of treatment and plasma exchange was initiated. She received
6 sessions of plasma exchange along with blood transfusion as needed, afterwhich her hemoglobin, hematocrit and platelets stabilized. The patient wasdischarged with a prednisone taper over 4-5 weeks and with regular rheu-matology and hematology follow up.Discussion: Autoimmune hemolytic anemia (AIHA) is a rare and lifethreatening disease. Warm antibody IgG induced AIHA accounts for 75%of the cases (cold antibodies induce 25% of the cases). Eighty percent ofpatients respond promptly to corticosteroid. Splenectomy results in a 60%response rate and should be considered if the patient does not respond tosteroids. Rituximab is an alternative choice with 50 % success. There areseveral case reports that demonstrate the effectiveness of using plasma ex-change in refractory and severe cases but no prospective studies exist. Ourcase demonstrates beneficial results with plasma exchange in fulminantAIHA to remove immunoglobulin G and immunoglobulin M, complement(C3, C4), and reduced antibody titers. Further studies are needed to elucidatethe role of plasma exchange in autoimmune hemolytic anemia.
Clinical Epidemiology and Preventive MedicineConcurrent Session
1:00 PMSaturday, February 23, 2013
417
LEADERSHIP AND COMMITMENT: THE IMPACT OF AGRASS ROOTS ORGANIZATION OF THE WELL BEING OFA COMMUNITY - AN ORAL HISTORY PROJECT
Aggen A3,1, Fisher L2,1, Irvin E2,1, Wiley S2,1, Hansberry S1, Sanders M3,Crook ED1,3, Arrieta MI1,3. 1University of South Alabama, Mobile, AL;2Bay Area Women Coalition, Mobile, AL and 3University of South Alabama,Mobile, AL.Purpose of Study: The neighborhood of Trinity Gardens (TG) has longheld the reputation as one of Mobile’s most dangerous communities. Fol-lowing tragic incidents that personally affected its founding members, theBay Area Women Coalition, Incorporated (BAWC) was formed to combatthe community’s rampant crime. The purpose of this study is to chroniclethe actions of the BAWC and conceptualize them within the social deter-minants of health model in order to describe the coalition’s impact on theTrinity Gardens community. Special emphasis is placed on the BAWC’s tran-sition from a reformative organization, to a proactive organization centeredon community health.Methods Used: We: a) researched the history of TG and the BAWC inorder to develop a questionnaire, b) interviewed the organization’s threeleading members, c) researched previously written works or alternative pri-mary sources to confirm oral histories collected; and d) performed secondaryanalysis of a community needs assessment.Summary of Results: The BAWC took a multifaceted and collaborativeapproach to the eight social determinants of health affecting their neigh-borhood: home ownership, access to care, lack of transportation, living ina deprived area, poverty, unemployment, nutrition, and inadequate opportu-nities to participate in society. Some examples include transformation ofthe community by enhancing home ownership, directly combating the drugtrade, beautification efforts, and development of a community health careclinic. The journey has taken over 15 years and included partnerships withlaw enforcement, developers, all facets of government, and academia.Conclusions: Via community collaboration, the BAWC has addressed thecore social determinants of health by decreasing crime and increasing civicpride and responsibility. In a domino effect, increasing home ownershiphas in turn enhanced residents’ sense of investment in their own well-being,neighborhood, and community.
418
A PATIENT CENTERED MEDICAL HOME PROSPECTIVEBEFORE AND AFTER EVALUATION
Laan DJ, Cohen S. University of Alabama School of Medicine, Birmingham, AL.Purpose of Study: In spring of 2011, Internal Medicine 1 (IM1) at KirklinClinic changed many aspects of its practice in order to become a patientcentered medical home (PCMH) based on conditions set forth by the NCQA.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 491
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

The goal of this project was to report differences in outcomes following thefirst year of PCMH implementation for IM1 patients.Methods Used: Using baseline (2011) and 1 year preventive care mea-sures, we performed a before and after cohort study comparing the studypopulation (IM1, N=1759) to a control (IM2/IM3 patients, N,890). Mea-sures of comparison (MoC) were generated using VIVA Health claims andbilling data. Inclusion/exclusion criteria were set using 2011 Healthcare Effec-tiveness Data and Information Set (HEDIS) parameters. MoC included colo-rectal cancer, breast cancer and glaucoma screenings as well as multiplescreening measures exclusive to those with diabetes mellitus-II (A1C andLDL-C screening, nephropathy monitoring, etc.).Summary of Results: With the exception of colorectal screening, all othermeasures declined more steeply for patients enrolled in the PCMH group(Image 1). The average pre-post % change for all measures was -2.7% forthe PCMH unit and +5.1% for the control groups. Controlling for patientcharacteristics (i.e. age, gender, comorbidities), the best predictor of the postdiabetes processes was the pre diabetes process score.Conclusions: The effects of a PCMH vary depending on patient popula-tion and measures considered. This study showed that, in general, preventivemeasures were not augmented by PCMH changes to practice. Further stud-ies need to be done in order to better understand the advantages and dis-advantages of implementing a PCMH.
419
DIABETES CONNECT: FEASIBILITY OF A PEERSUPPORT DIABETES INTERVENTION FOR LOW-INCOMEAFRICAN AMERICANS
Maduforo U1,2, Falola M1,2, Agne A1,2, Cherrington A1,2. 1University ofAlabama at Birmingham, Birmingham, AL and 2University of Alabama atBirmingham, Birmingham, AL.Purpose of Study: The objective of this study was to test the feasibility ofa peer support intervention for low-income African Americans with Type 2Diabetes (DM) living in Birmingham Alabama.Methods Used: We recruited a convenience sample of patients with dia-betes from within the local safety-net health system. Inclusion criteria wereage 9 19, African American, Type 2 DM, and community-dwelling. Fourteenindividuals participated in a one day diabetes education class held in the com-munity and were assigned to a trained diabetes Community Health Advisor(CHA). Participants then received 8 weekly phone calls from the CHA, whoprovided support, encouragement and advice. Outcomes were measured be-fore and immediately after the intervention. Height and weight were measuredusing standardized protocols, diabetes self-care activities, confidence over-coming barriers and perceived stress were measured using validated instru-ments. Pre and post means were compared using paired t-test analyses.Summary of Results: Nine participants completed the study for a reten-tion rate of 64%. Mean age was 59; 7 participants were male and 2 werefemale, 6 of 9 had completed high school, 7 were unemployed and 2 wereretired, 2 were married. All of the participants had cell phones but only1 reported using text messaging. Most of them (7/9) reported never using
the internet and 1 reported rarely using the internet. After the study, meanweight went down (-7.1lb, p=0.76), diabetes self-care activities increased(1.5, p=.74), confidence overcoming barriers to disease management wentup (7.04, p=0.5) and perceived stress went down (-3, p=0.5). Participantsreported high levels of satisfaction with the program.Conclusions: This study demonstrates the feasibility of a peer supportintervention for low income African Americans with diabetes management.Although the sample size limited our ability to demonstrate statistical sig-nificance, outcomes were all in favorable direction. Future large studiesare needed to examine the impact of peer support on diabetes outcomes inunderserved communities.
420
EXPOSING ALL-TERRAIN VEHICLES: THE VALUE OF ASTATEWIDE EDUCATIONAL CAMPAIGN
Fettig C1, Frascogna N2, King W1, Monroe K1. 1University of Alabama,Birmingham, AL and 2University of Mississippi Medical Center, Jackson, MS.Purpose of Study: Striving to reduce the number of children injured by All-Terrain Vehicles (ATV), Children’s of Alabama (COA) in conjunction withthe AAP and Alabama Department of Health launched a statewide multi-media campaign in 2008 exposing the hazards of ATV use and promotingATV safety in the pediatric population. This study evaluated the efficacy ofthe intervention as measured by the trend of ATV-related injuries treatedat COA both prior to and following the campaign.Methods Used: The educational campaign consisted of multimedia adver-tisements targeted at pediatricians, parents, and children throughout Alabama.Pre- and post-campaign ATV injury data was obtained by accessing the COAtrauma database and emergency department (ED) electronic medical record.This study included all patients seen in the COA ED for ATV-related injuriesfrom 2007-2011.Summary of Results: Analysis of ATV injury data prior to and followingthe 2008 campaign revealed an overall decrease in the number of patientstreated in the COA ED for ATV-related injuries. However, the downwardtrend of ATV-associated injuries was transient; by 2011, Children’s witnesseda rise in total ATV injuries as the number of ATV trauma alerts increased withminimal change in the number of ED visits.Conclusions: The educational intervention demonstrated that although effec-tive statewide education proves invaluable in raising awareness and improvingATV injury and death rates, education alone is insufficient for injury prevention.
421
TRENDS IN ALABAMATEEN DRIVING DEATH AND INJURY
Irons E1, Monroe K1, King W1, Norris J2, Nichols M1. 1UAB, Birmingham,AL and 2University of Alabama, Tuscaloosa, AL.Purpose of Study: Motor vehicle crashes (MVC) are a leading cause ofmorbidity and mortality in teens. Alabama has had the second highest MVCfatality rate among teens in the U.S. for several years. Interventions such as aGraduated Driver’s License law and media campaigns to increase public aware-ness have been employed to decrease MVC death and injury. Recently, weevaluated twelve years of teen MVC deaths and injuries to discern if changesin trend have occurred subsequent to legislative and educational interventions.Methods Used: A retrospective analysis of Alabama teen MVC deaths andinjury for the years 2000-2011 was conducted. The Spearman rank correlation
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
492 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

was used to test for correlation of deaths and injury over time. MVC data wereobtained from a FARS dataset managed by the Center for Advanced PublicSafety at the University ofAlabama. A Lowess regression - scattergram analysiswas used to identify period specific changes in deaths and injury over time. TheMann Whitney U test was used to evaluate median differences in deaths andinjury comparing pre 2007 and post 2007 data. Statistical analysis was con-ducted using True Epistat 5.0 software.Summary of Results: Alabama teen MVC deaths and injury demonstrateda significant negative correlation over the twelve year time period (R subs for deaths and injury = -0.87, pG0.001 and -0.92, pG0.001, respectively).Lowess regression identified a notable decline in deaths and injury after theyear 2006. Median deaths and injury for the pre-2007 time period were sig-nificantly higher than the post 2007 time period, (U=35.0, p=0.003).Conclusions: Alabama teen driver deaths and injury have decreased overthe study 12 year period, most notably after 2006. There are many factorsthat may have contributed to this trend. These factors may include stricterlaws for teen drivers (enacted in 2002 and updated in 2010), less teen drivingdue to a nationwide economic downturn, delayed licensing in teens, steadyimprovements in overall seat belt use, and heightened public awareness ofrisky behaviors in teen driving.
422
POSTMORTEM CANDIDEMIA AT UNIVERSITY HOSPITAL(JANUARY 2008-JUNE 2011)
Donthamsetty S1, Collinsworth AL2, Alquist CR1, Figueroa J3, McGoey R1.1Louisiana State University Health Sciences Center, New Orleans, LA;2University of Florida College of Medicine, Gainesville, FL and 3LouisianaState University Health Sciences Center, New Orleans, LA.Purpose of Study: Candida is the primary cause of opportunistic mycosesworldwide. This accounts for a third of fungal fatalities annually. Mortality ofinvasive Candida species is largely attributed to delays in antifungal therapy.This is further complicated by the low sensitivity of blood cultures to detectdisseminated candidiasis.Methods Used: To evaluate the incidence of candidiasis in the New Orleansdecedent population, autopsy cases occurring between January 2008 and June2011 were reviewed for the presence of Candida species in post-mortem bloodcultures. After the chest plate was removed and pericardial sac opened, a10 gauge needle was introduced into the inferior vena cava for blood aspira-tion and injected into a BacT/Alert culture bottle. Cultures were performedusing an in situ method.Summary of Results: Of the 208 cases with postmortem blood cultures,28 cases of candidiasis were identified. Of these, only 2 (7%) had correlativepositive ante-mortem cultures for Candida. 14 (50%) of these patients wereadmitted to the intensive care unit in the perimortem period. 22 (79%) ofthese patients had evidence of liver disease while the remaining 6 patientshad other risk factors for fungal infection such as HIV (3) and urosepsis (1).Conclusions: Antemortem Candidemia may be underappreciated in ourpopulation, which suggests prophylactic antifungal therapy should be consid-ered in patients with extended intensive care unit stays and the followingknown risk factors: broad spectrum antibiotic treatment, chemotherapy, muco-sal colonization with Candida species, indwelling vascular catheters, total par-enteral nutrition, neutropenia, prior surgery and renal failure with or withoutconcurrent hemodialysis.
423
INFLUENZA IMMUNIZATION OF HEALTHCARE WORKERSIN LOUISIANA
Fricke KL1,2,3, Gastanaduy M2,1, Klos R2, Begue R2,3. 1Baylor University,Waco, TX; 2Children’s Hospital, New Orleans, LA and 3Louisiana StateUniversity Health Sciences Center, New Orleans, LA.Purpose of Study: Since 4 CDC has recommended influenza (flu) immuni-zation for healthcare workers (HCW) to decrease transmission to patients. Yet,vaccination rates remain low (È60%). The DHHS has set a goal of 90% vaccina-tion for 2020 and medical societies have proposed ‘‘mandatory’’ immunization.
The aim is to describe practices utilized for HCW flu immunization inhospitals in Louisiana with emphasis on those that correlate with increasedvaccination rates.Methods Used: A list of all hospitals was obtained from the Directoryof the Louisiana Hospital Association (www.lhaonline.org). Hospitals were
contacted by phone, fax, mail or email and invited to participate. A 17-itemquestionnaire was sent inquiring about the hospital type, patients served,characteristics of the flu vaccination campaign, and the resulting vaccinationrate. Data was entered in Excel and analyzed with GraphPad Prism5.Summary of Results: 256 hospitals were listed. In the first 8 weeks,115 responses representing 142 hospitals (55%) in 46 Parishes (72%) werereceived. Most programs demanded that the HCW either receive the vaccineor sign a declination form (74%) and the rest were exclusively voluntary pro-grams (36%); no program had flu vaccination as a condition of employment.The overall vaccination rate was 66%, significantly (pG0.05) higher amonghospitals who provided acute care (72%), served children (72%), pregnantwomen (73%) or had an ICU (72%), required a signed declination (74%) orimposed consequences (most commonly wearing a mask on patient contact)to those unvaccinated (86%). There was an incremental vaccination rate(median; IQR) in hospitals that did not implement all CDC recommended fluvaccination practices (50%, 28Y50%), versus those that did implement CDCpractices (59%; 57Y63%), those that added a signed declination (75%; 69Y80%)and those that added a consequence (86%; 81Y91%) (pG0.0001 for trend).Conclusions: Flu vaccination among HCW remains suboptimal. Implement-ing CDC recommended practices may not be enough to approach 90% rates;it may be necessary to add a signed declination and institute consequencesto unvaccinated HCWs. Wearing a mask is a strong consequence. Demandingflu vaccination as condition of employment is not a common practice.
Endocrinology and MetabolismConcurrent Session
1:00 PMSaturday, February 23, 2013
424
RISK FACTORS FOR THE SEVERITY OF SLEEP APNEA
Martin T1, Villemarette-Pittman N2, Mader EC2, Friday KE3. 1LSU Schoolof Medicine-New Orleans, New Orleans, LA; 2LSU School of Medicine-NewOrleans, New Orleans, LA and 3LSU School of Medicine-New Orleans,New Orleans, LA.Purpose of Study: Sleep apnea has been shown to adversely affect glu-cose and blood pressure regulation and may potentiate the development ofcardiovascular disease, stroke and type 2 diabetes. There is a high preva-lence of obstructive sleep apnea (OSA) in people with type 2 diabetes. Thepurpose of this cross-sectional analysis was to investigate risk factors forthe severity of sleep apnea and to determine if sleep apnea is more severein patients with diabetes.Methods Used: Polysomnography and lab data were obtained on 456patients at Interim LSU Hospital from 2008Y2012. 362 out of the 456 (79.4%)patients were diagnosed with obstructive sleep apnea (OSA), 42 patients(12%) had glucose intolerance (GI) and 134 (37%) had type 2 diabetes (DM).OSA severity was measured by number of breathing events per hour ofsleep or apnea/hypopnea index (AHI). Variables examined included sex, age,weight, BMI, Epworth Sleepiness Score (ESS), neck circumference, meanHgbA1c, mean fasting glucose, AHI, lowest oxygen desaturation, numberof oxygen desaturations G90%, waking and sleeping heart rate, and the con-tinuous positive airway pressure (CPAP) that minimizes apnea/hypopnea andoxygen desaturations.Summary of Results: Using stepwise linear regression, neck circumfer-ence, gender, fasting glucose, and waking heart rate predicted AHI (pG.001).Gender, BMI, and average waking heart rate predicted OSA diagnosis(pG.001). Univariate ANCOVA showed that AHI differed by gender (p=.001)with greater AHI in men, but not by DM Group (Non-DM vs. GI/DM;p=.118). OSA diagnosis differed by gender (pG.001) with more males diag-nosed with OSA, as well as by DM Group (Non-DM vs. GI/DM; pG.001)with OSA diagnosed more often in GI/DM. The Sex by DM Group in-teraction was not significant (p=.052). Waking heart rate differed by DMGroup (Non-DM vs. GI/DM; p=.028) with higher heart rate in GI/DM thanNon-DM.Conclusions: Sleep Apnea diagnosis and severity are associated withgender, obesity, and glucose control. Future research is needed to further ex-amine relationships among OSA, gender and diabetes, as well as identifyother factors contributing to OSA.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 493
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

425
RECURRENT HYPOGLYCEMIAS: DEFINING A NOVEL,TREATABLE INBORN ERROR WITHPHOSPHOGLUCOMUTASE 1 DEFICIENCY
Morava-Kozicz E1,4, Raymond K2, Marquardt T3, Lefeber D4. 1TulaneUniversity Medical Center, New Orleans, LA; 2Mayo Clinic College ofMedicine, Rochester, ME; 3Universitatsklinikum Munster, Munster, Germanyand 4Radboud University Nijmegen Medical Center, Nijmegen, Netherlands.Purpose of Study: We define a novel pediatric disorder with recurrentepisodes of severe hypoglycemia associated with mild increase of glyco-gen storage in the liver and late onset, progressive dilated cardiomyopathy.Most patients have a split uvula, or Pierre Robin syndrome. Some patientsdevelop rhabdomyolysis and life-threatening malignant hyperthermia in thecourse of disease. The new disorder involves two metabolic pathways, oneaffecting glycogen degradation and the other affecting glycosylation of proteins.Methods Used: Next generation sequencing and detailed studies of sugarmetabolites and glycosylation were performed to elucidate the molecularbasis and underlying pathomechanism of this novel disease.Summary of Results: As cause of the disease, mutations in phosphoglu-comutase 1 (PGM1) in 13 families were identified. Mass spectrometry oftransferrin showed a loss of complete N-glycans in addition to the presenceof truncated glycans lacking galactose. Patient fibroblasts supplementedwith galactose showed restoration of protein glycosylation and no evidenceof glycogen accumulation. Dietary galactose intake significantly improvedthe glycosylation abnormalities and clinical features in patients.Conclusions: PGM1 deficiency is a novel metabolic disorder with fea-tures of glycogen storage disease as well as congential disorders of glyco-sylation that is easily detectable, likely treatable and that untreated mayend with cardiac arrest. Selective screening in patients with soft palate cleftby a diagnostic transferrin glycosylation profile will allow the identifica-tion of individuals, presymptomatic regarding further clinical manifestations.PGM1 deficiency disrupts the connection between glycogen and glucosemetabolism. Metabolites of the PGM1 reaction may be supplemented by dietin order to attenuate the consequences of PGM1 deficiency.
426
HEMOGLOBIN A1C HAS LOW POSITIVE PREDICTIVEVALUE FOR DIAGNOSIS OF PREDIABETES
Gosmanov AR1, Wan J2. 1UTHSC, Memphis, TN and 2UTHSC, Memphis, TN.Purpose of Study: Hemoglobin A1c (HbA1c) is recommended for predi-abetes screening despite the test‘s low specificity. The aim of this studywas to determine the positive predictive value of HbA1c for diagnosis of pre-diabetes and identify factors that may improve utility of this test in clinicalpractice.Methods Used: We identified subjects with newly diagnosed prediabetesby HbA1c criterion (values of 5.7-6.4%) in our general endocrinology clinic.All subjects subsequently underwent confirmatory 2-hr oral glucose toler-ance test (OGTT), the gold-standard test for diagnosis of normal glucosetolerance, prediabetes, or diabetes. Clinical and biochemical characteristicsof subjects with true-positive and false-positive HbA1c-based diagnosis ofprediabetes were analyzed using Mann-Whitney or chi-square tests. Logisticregression model was used to estimate the effect of several variables on pre-dictive power of HbA1c.Summary of Results: Among 45 subjects (31 females, 25 blacks/20whites) diagnosed with prediabetes based on HbA1c criterion, the OGTTconfirmed the diagnosis only in 21 subjects demonstrating a positive pre-dictive value of 47%. Among the 24 persons with false-positive test, 7 haddiabetes and 17 had normal glucose tolerance. In unadjusted analysis,patients with true-positive and false-positive tests had similar HbA1c(6.03T0.21 vs 5.92T0.18%, P=0.11), however patients in the true-positivegroup were older (56.9T13.2 vs 49.1T11.6 yrs, P=0.03), had higher numberof comorbidities (4.6T1.1 vs 3.2T1.2, PG0.001), and were taking more pre-scription medications (6.0T2.4 vs 3.1T2.0, PG0.001). Personal history ofhyperlipidemia or hypertension, gender distribution, body mass index, hemat-ocrit, plasma creatinine and fasting insulin and family history of diabeteswere not different between the groups. In the multivariate logistic regressionanalysis, age was no longer significant between the groups (P=0.22), however
the difference in prescription medications (P=0.024) and medical problems(P=0.064) persisted between true-positive and false-positive groups.Conclusions: HbA1c has a low positive predictive value for the diagnosisof prediabetes compared with OGTT. Currently recommended HbA1c cut offlevels for diagnosis of prediabetes are more likely to be true in persons whohave significant burden of associated diseases.
427
STUDIES OF THE IMMUNOPATHOGENESIS OF DM1 BYPROTEOME ANALYSIS OF SPLEEN LEUKOCYTES NUCLEIFROM NON-OBESE DIABETIC MICE
Brodskiy Y1, Lenchik NI1,2, Beranova-Giorgianni S1, Giorgianni F1, GerlingIC1,2. 1University of Tennessee Health Science Center, Memphis, TN and2VA Medical Center, Memphis, TN.Purpose of Study: Non-Obese Diabetic (NOD) mice are a model of DM1.Leukocyte infiltration around the islets of Langerhans is first seen at 5 weeksof age. To gain a deeper insight into the molecular events that lead to initiationof DM1, we used 2D-gel proteomic analysis to evaluate nuclear protein ex-pression in NOD mice compared to two control strains (C57BL/6 and NOR).Methods Used: Spleen monocytes were isolated from NOD, NOR andC57BL/6 mice at 2,3 and 4 weeks of age and a purified nuclear proteinfraction was obtained and subjected to 2D gel proteome analysis. Genespringsoftware was utilized to define groups of differentially expressed proteinspots. Spots of interest were identified by mass spectrometry, and IngenuityPathway Analysis was used to identify specific pathways connecting thesegroups of differentially expressed proteins.Summary of Results: Nuclei of 5 independent spleen monocyte sam-ples from each of the 3 strains (NOD, NOR and C57Bl/6), at each age (2, 3and 4 weeks), were isolated; for a total of 45 samples. A one-way ANOVA(p G 0.05) determined that 359 spots were differentially expressed betweenthe strains at one or more ages. At 2, 3 and 4 weeks of age, 41, 13, and 1 spots,respectively, were differentially expressed between NOD and both of the con-trols. Ingenuity Pathway Analysis (IPA) demonstrated that multiple proteinsactivating NFkB or being activated by NFkB were differentially expressed in2 week old NOD mice. However, already at 3 weeks of age few NFkB asso-ciated proteins were different between NOD and control mice. Both at 2 and3 weeks of age proteasome members and other proteins involved in antigenpresentation were differentially expressed.Conclusions: These experiments give insight into strain differences ofnuclear protein expression in NOD monocytes in the pre-diabetic phase. Atotal of 55 spots were differentially expressed between NOD and controls.Pathway analysis suggested that many of these proteins were associated withtissue stress, activation of the NFkB pathway and antigen presentation. Thisdata suggests a very early activation of the immune system in pre-diabeticNOD mice and points to specific transcriptional regulators involved, that mayrepresent potential future therapeutic targets.
428
ROLE OF PTEN IN TNF-> INDUCED INSULIN RESISTANCE
Bulger D1,2, Conley J2, Majumdar G1,2, Solomon SS1,2. 1University ofTennessee Health Science Center, Memphis, TN and 2VA Medical Center,Memphis, TN.Purpose of Study: Type 2 Diabetes Mellitus (DM2) has increased notablyin the last 10 years. With over 80% of DM2 patients being obese, the abilityof TNF-> released from adipose tissue to cause insulin resistance (IR) pres-ents a major causal factor. Blocking TNF-> helps DM2 patients regain insulinsensitivity. However, the mechanism by which this occurs is still unknown.Previous genomics and proteomics studies on TNF-> induced IR from ourlaboratory revealed significant differences in PTEN (phosphatase and tensinhomolog deleted on chromosome 10), which dephosphorylates phosphatidyli-nositol 3-phosphate and induces IR. As insulin resistance can then be pro-duced by an increase in PTEN, we designed this study to determine if PTENplays a role in TNF-> induced IR.Methods Used: H411E rat hepatoma cells were treated with insulin(10,000 KU/ml), TNF-> (1.0 nM), and insulin + TNF->. Protein and mRNAwere extracted from the harvested cells and analyzed by Western blot (Wb)and Real Time RT-PCR respectively. The levels of total PTEN were compared
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
494 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

to untreated control using A-actin as a loading control. Also, changes in p-Aktwere measured by Wb. These results reflect sensitivity or resistance to insulin.Summary of Results: PTEN/A-actin mRNA levels as measured by quan-titation of Wb bands are calculated as percentages of control: insulin (80%, ,);TNF-> (197%, jjj, p G 0.05); and insulin + TNF-> (122%, j). For PTEN/A-actin mRNA levels as measured by Real Time RT-PCR, percentages ofcontrol were the following: insulin (65.8%, ,,); TNF-> (198%, jjj); andinsulin + TNF-> (98%, ,). Insulin inhibited and TNF-> stimulated PTENlevels. Phospho-Akt (p-Akt) expression by Wb was increased by insulin anddecreased by TNF->. Hence, insulin decreased PTEN and stimulated p-Akt.In contrast, TNF-> stimulated PTEN and decreased p-Akt. Experiments donewith metformin (MET) and 3-hydroxypicolinate vanadium(IV) complex(VO-OHpic) were consistent with the known ability of MET to decrease IR,and VO-OHpic to mimic insulin action by inhibiting PTEN.Conclusions: Insulin inhibits and TNF-> stimulates PTEN. Insulin stim-ulates and TNF-> inhibits p-Akt. These combined effects of TNF-> leadto IR. Therefore, our data identifies PTEN as a potential therapeutic targetfor the treatment of DM2.
429
LEUKOCYTES FROM A SUBSET OF PATIENTS WITHDIABETES MELLITUS AND THOSE FROM SUBJECTSCHALLENGED WITH IN VIVO ENDOTOXIN EXHIBITNOVEL CHANGES IN AMPK AND HIF-1 EXPRESSION,WHICH ARE INDICATIVE OF METABOLIC DYSFUNCTION
Amorosa LF1, Zhang Z2, Lubitz SE1, Macor MA2, Coyle S2, Haimovich B2,Lowry SF2. 1UMDNJ-Robert Wood Johnson Medical School, NewBrunswick, NJ and 2UMDNJ-Robert Wood Johnson Medical School, NewBrunswick, NJ.Purpose of Study: Chronic, sub-clinical inflammatory responses havebeen implicated in the pathogenesis of Type 2 diabetes mellitus (T2DM),but the mechanism of this relationship is currently undetermined. Here,we sought to identify aberrant metabolic proteins expression commonalitiesshared by leukocytes from subjects challenged with in vivo endotoxin andthose from T2DM patients.Methods Used: Healthy volunteers (n=5) were intravenously administeredNIH reference endotoxin at a dose of 0.1 ng/kg body weight. Blood sampleswere collected, and peripheral blood leukocytes (PBL) were isolated beforeendotoxin infusion and for 24 hours post-infusion. Western blots were usedto examine temporal changes in AMPKa, HIF-1a, and LC3-I/II expression.Similar analyses were completed using PBL from T2DM patients. Thesepatients attended clinic under ad lib dietary conditions.Summary of Results: HIF-1, a transcription factor, and AMPK, a serine/threonine kinase, are key regulators of cellular metabolism. Autophagy isa process used to degrade macromolecules and organelles. During periods ofnutrients deficiency autophagy contributes to ATP production. An increasein LC3-II expression is indicative of autophagy. PBL from healthy subjectsexhibit AMPKa expression, but not HIF-1a or LC3-II expression. In markedcontrast, PBL isolated from subjects challenged with in vivo endotoxinfor 2Y4 hours exhibit AMPKa degradation, and robust HIF-1a and LC3-IIexpression. Unexpectedly, PBL from four out of six T2DM patients alsoexhibited diminished AMPKa expression, and enhanced HIF-1a and LC3-IIexpression. This protein expression signature was not detected in PBL fromnon-diabetic patients.Conclusions: These observations support the concept that inflamma-tory factors contribute to cellular metabolic dysfunction in T2DM patients.Further studies are underway to determine whether these changes can be usedas early markers for the onset of diabetes mellitus.
430
DISCRIMINATIVE KEYS IN THE METABOLIC DIAGNOSISOF CUTIS LAXA SYNDROMES
Gardeitchik T1,2, Mohamed M1,2, Morava E3,1. 1Radboud University MedicalCenter, Nijmegen, Netherlands; 2Institute for Genetic and Metabolic Disease,Nijmegen, Netherlands and 3Tulane University, New Orleans, LA.Purpose of Study: Cutis laxa is a disorder in which patients have wrinkled,abundant skin with abnormal elasticity. Skin symptoms may be associated
with variable systemic involvement. Recently, several new genetic defectshave been discovered to cause cutis laxa. Surprisingly, a number of these syn-dromes are inborn errors of metabolism. These include disorders of glycosyl-ation: COG7-CDG, ATP6V0A2-CDG as well as deficiencies in mitochondrialenzymes (P5CS and PYCR1). Discriminating between these syndromes re-mains challenging due to several overlapping clinical features: the severelyaffected skin, microcephaly, facial dysmorphisms, joint hyperlaxity, cognitivedeficits, growth delay and late closing of the fontanel.Methods Used: We prospectively evaluated the clinical, metabolic and neu-rological features of eight patients with ‘metabolic’ cutis laxa caused diag-nosed with a novel genetic defect in either PYCR1 or ATP6V0A2.Summary of Results: Here we report on the metabolic and clinical featuresof eight patients with metabolic cutis laxa. The four children diagnosed withARCL2B due to PYCR1 mutations had a triangular face with prominent earsand progeroid appearance, abnormal wrist position and two of them showedathetoid movements.
Cerebral MRI detected a hypoplastic corpus callosum in three of the fourpatients. Two patients had increased serum alanine levels. In the four patientswith ATP6V0A2-CDG, in the absence of the above described abnormalities,a cobblestone like brain dysgenesis was detected on MRI. Biochemical eval-uation revealed glycosylation abnormalities and elevated liver enzymes.Conclusions: The four patients with ATP6V0A2-CDG had glycosylationabnormalities and typical facial features. MRI revealed a neuronal migrationdefects in three patients. In contrast to the ARCL 2B patients who had differentfacial features and had elevation of serum alanine. Awareness of clinical andbiochemical differences between these patient groups should lead to a timelydiagnosis. We therefore suggest to measure lactate and alanine and perform cere-bral MRI additional to screening for glycosylation in patients with cutis laxa.
431
IMPACT OF HYPERGLYCEMIA AND DIABETES INANTIPSYCHOTIC-TREATED PATIENTS ADMITTED TOACUTE PSYCHIATRIC UNITS
Eisenberg A1, Powell W1, Aram P1, Khaliqdina S1, Gillespie C2, Peng L3,Umpierrez G1, Smiley D1. 1Emory University School of Medicine, Atlanta,GA; 2Emory University School of Medicine, Atlanta, GA and 3Rollins Schoolof Public Health, Atlanta, GA.Purpose of Study: The association between diabetes (DM) and chronicuse of antipsychotics is well established. However, the acute effects of anti-psychotics on glycemic control and clinical outcome in patients admittedto psychiatric units are not known.Methods Used: We conducted a retrospective study to determine theprevalence and impact of diabetes and hyperglycemia (blood glucose [BG]9140 mg/dl) on clinical outcome (hospital complications, length of stay[LOS], and transfer to medical units) in antipsychotic-treated patients ad-mitted to acute psychiatric units between 1/1/08 and 12/31/08 at 3 academiccenters in Atlanta, GA.Summary of Results: Among 1212 patients (age: 57T20 yrs, male: 55%,AA: 55%, BMI: 27T7 kg/m2, LOS: 13T19 days, mean daily BG concentra-tion 122T40 mg/dL), 21% had a history of DM and 6% were diagnosedwith hyperglycemia on admission. Compared to patients with normoglyce-mia, those with DM or hyperglycemia had a higher rate of hospital com-plications (p=0.023), particularly infections (p=0.033). Patients with DMrequired more transfers to medical units than those with hyperglycemia ornormoglycemia (p=0.033). There was no difference in LOS between patientswith hyperglycemia or DM compared to those with normoglycemia. Overall,6% of patients were treated with typical antipsychotics, 52% with atypical, and17% with a combination: we observed no differences in mean daily BGconcentration or LOS between these 3 groups (p=0.17). In addition, weobserved no differences in mean daily BG concentrations or hospitalcomplications between newly started patients on antipsychotics comparedto those not treated with antipsychotics or those continued on their previousantipsychotic regimen.Conclusions: Hyperglycemia and diabetes are common in acute psychiatricunits and are associated with a higher risk of hospital complications comparedto patients with normoglycemia. The acute use of antipsychotics is not as-sociated with higher glucose concentrations or with an increased risk ofhospital complications. Randomized controlled studies are needed to deter-mine the optimal approach to manage hyperglycemia and diabetes in acutepsychiatric units.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 495
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

432
PREDICTORS OF RESOLUTION IN PATIENTS WITHDIABETIC KETOACIDOSIS: SERUM BICARBONATEVERSUS ANION GAP
Awoniyi O, Nyenwe E. University of Tennessee Health Science Center,Memphis, TN.Purpose of Study: The American Diabetes Association (ADA) definesDiabetic Ketoacidosis (DKA) resolution as a blood glucose G200 mg/dl andtwo of the following: serum bicarbonate level Q15 mEq/l, pH 97.3 or aniongap e12 mEq/l. We observed that clinicians often use anion gap rather thanbicarbonate in making this diagnosis. Furthermore, blood gas analysis may notbe available in some centers especially in developing countries where DKAmorbidity and mortality remain high. Therefore we investigated the predictorsof DKA resolution using the basic metabolic panel which is readily available.Methods Used: We conducted an analysis of patients admitted withDKA at The Regional Medical Center, Memphis Tennessee from October2003 - October 2008. Only subjects with complete data were included inthe analysis and DKA was managed according to current ADA guidelines.Data analysis was done using multivariate regression model.Summary of Results: Forty patients aged 37.9 T 11.3 years (72% males)were included in the analysis. Both serum bicarbonate and anion gap correlatedwith pH at admission (r = 0.62, PG0.0001; r = -0.49, PG0.001 respectively);but only bicarbonate correlated with pH at resolution (r = 0.67, PG0.0001).Furthermore, logistic regression model showed bicarbonate to be the only in-dependent predictor of pH at admission and resolution of DKA (PG0.0001).Conclusions: We conclude that serum bicarbonate is a better predictor ofpH at admission and resolution of DKA than anion gap. Therefore serumbicarbonate should be preferred over anion gap in determining resolution ofDKA in the absence of blood gas analysis.
433
mRNA EXPRESSION PROFILING OF HUMAN PANCREATICISLETS FROM NON-DIABETIC AUTO-ANTIBODY POSITIVEVS ANTIBODY NEGATIVE INDIVIDUALS
Ahrari B1, Lenchik NI1,2, Matta SG1, Gerling IC1,2. 1University of TennesseeHealth Science Center, Cordova, TN and 2VA Medical Center, Memphis, TN.Purpose of Study: With new advances in genetics and molecular biology,it is now possible to examine the expression of entire genomes rather than afew specific genes. In this study we compared comprehensive mRNA expres-sion profiles of islets of Langerhans from non-diabetic auto-antibody positivehuman organ donors (aab+) with age/sex matched aab- controls (C). The pur-pose was to define cellular processes and molecular pathways whose activa-tion in the islets are associated with presence of islet autoantibodies in serum,a critical event in the early stages of type 1 diabetes development.Methods Used: Cryo-sections (8Km thick) were obtained from the nPODhuman pancreas tissue bank. Slides were fixed, dried, and 60-80 islets obtainedfrom each donor by laser-capture microscopy. RNAwas immediately extractedfrom the tissue and stored at -80C. The quantity and integrity (RIN) of totalRNA was determined and expression profiles obtained using Affymetrix HumanGene 1.0 ST expression arrays.Summary of Results: Tissue slides from 8 aab+ and 8 age and sex matchedaab- control pancreata were used for laser capture. On slides from one (an aab+)donor pancreas we were not able to find any islets of Langerhans. All RNAisolated from the 15 islet samples had RIN Q3.2 and were processed for ex-pression profiling on the Affymetrix arrays using ‘‘low RIN’’ protocols. Thedata was analyzed on GeneSpring software to identify differentially expressedgenes and then Ingenuity Pathway Analysis was used to mine the data. We
looked for differences in gene expression between aab+ and controls. The listof differentially regulated genes had a highly significant enrichment of genesrelated to mitochondrial dysfunction and the EIF2 signaling pathway. Fur-thermore, HLA class I, oxidative stress related genes and genes in the HNF4Apathway were up-regulated.Conclusions: Development of aab is a common feature of pre-type 1 dia-betes. We studied gene expression in islets from individuals with aab’s vscontrols. Our results indicate that aab+ status is associated with mitochon-drial dysfunction, oxidative stress, endoplasmic reticulum stress, apoptosis,and increased expression of HLA class I and other genes consistent withmetabolic stress and/or viral infections in islets of Langerhans.
434
EFFECT OF HIGH PROTEIN VS HIGH CARBOHYDRATEDIETS ON SATIETY AND CARDIOVASCULAR FACTORS
Kineish O, Stentz FB, Kitabchi AE. University of Tennessee, Memphis, TN.Purpose of Study: The rise in the number of overweight and obese in-dividuals is an alarming trend that has far-reaching health consequences.Obesity has been related to an increased risk for diabetes, cardiovasculardisease, and numerous other medical problems. Behavioral changes in dietand exercise have been shown to be very effective in reduction of obesity.However, these changes often can be difficult for patients, leading to a lack ofcompliance. Our study of the effect of dietary macronutrients on metabolicparameters show that a high protein (HP) diet [30% protein, 30% fat, and40% CHO] compared to a high carbohydrate (CHO) diet [(HC) (55% CHO,30% fat, 15% protein] results in greater reduction in oxidative stress, lipidperoxidation, cardiovascular risk factors(CVRF) and less insulin resistance(HOMA-IR) in the HP group than the HC group after 6 months(mo) on thediets compared to baseline. Studies have shown that HP diets can potentiallyinduce satiety and suppress hunger. Since the hormone ghrelin is associatedwith satiety determined if the HP and HC diets affected the ghrelin levels inthese subjects studied. Additionally, since CVRF decreased more in the HPthan the HC diet, we wanted to determine if the B-Type Natriuretic Peptide(BNP) released from the heart was affected by either diet.Methods Used: 24 obese, non-diabetic, pre-menopausal women were ran-domized to HP(12) or HC(12) diets. All food was provided for the 6 mostudy with weekly food pickups and weigh-in. Ghrelin and NT-proBNP levelswere determined at baseline and after 6 mo on the HP and HC diets.Summary of Results: The table shows the reults of the effect of HP andHC diets on ghrelin and NT-proBNP.Conclusions: HP ghrelin results demonstrate that HP diet can induce satietyand is more effective than the HC diet. The BNP decrease in both groupsdemonstrates the improvement in heart tissue with the HP diet having agreater effect than the HC diet. Although weight loss was similar (9.8% in HPgroup and 9.3% in HC group) this study demonstrates that the HP diet hasadditional health benefits compared to the HC diet.
Gastroenterology IIConcurrent Session
1:00 PMSaturday, February 23, 2013
435
GASTRO-PERICARDIAL FISTULA: A RARE LATEPOST-FUNDOPLICATION COMPLICATION PRESENTINGWITH PNEUMOPERICARDIUM
Mankongpaisarnrung C, Sutamtewagul G, Dumrongmongcolgul N,Meyerrose G, Nugent K. Texas Tech University Health Sciences Center(TTUHSC), Lubbock, TX.
Parameter
HP
(n=12)
Baseline
HP
(n=12)
6 mo
p* HP
Baseline
vs 6 mo
HC
(n=12)
Baseline
HC
(n=12)
6 mo
p* HC
Baseline
vs 6 mo
p** HP
vs HC
(6 mo)
Ghrelin (ng/ml) 5.7 1.2 .02 5.3 4.9 .27 .02
NT-proBNP (pmol/L) 492 359 .01 486 390 .04 .03
p*=Wilcoxan Signed Rank Test. p**= Wilcoxan Rank Sum Test for 6 mo HP vs HC
Admission Resolution
pH 6.86 T 0.19 7.33 T 0.07
Glucose (mg/dL) 770 T 283 163.5 T 72.7
Bicarbonate (mEq/L) 8.5 T 4.2 19.5 T 4.6
Anion gap (mEq/L) 26 T 7.2 8.1 T 3.4
Osmolality (mOsmol) 299 T 19.3 283.7 T 14.6
Potassium (mEq/dL) 5.6 T 1.4 3.8 T 0.5
Clinical and biochemical characteristics of patients at admission and resolution of DKA
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
496 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Case Report:Background: Gastro-pericardial fistula (GPF) is an abnormal connectionbetween the stomach and pericardial sac. It is associated with conditions,such as prior Nissen’s fundoplication (FP), refractory gastric ulcer especiallyon fundus and cardia, esophagogastric malignancy, and Zollinger-Ellison’ssyndrome. The mortality is as high as 50-80 %. The presentation includes sub-sternal chest pain, referred shoulder pain, pneumopericardium, subphrenic ab-scess, and cardiac tamponade.Case: A 74-year-old woman with a history of FP 6 years ago presentedwith 1-day history of progressive shortness of breath and sharp chest painradiating to back. Her abdomen was distended and diffusely tender. Herlaboratory results showed WBC 13.3 with 27 % immature neutrophils, Plt334, and Hb 10.6. ABG revealed severe metabolic acidosis and respiratoryacidosis. The chest X-ray showed a soft-tissue mass in the left lower lung andrightward deviation of the cardiomediastinal silhouette. CT chest revealed apneumopericardium and rightward mediastinal shift from thoracic herniationof the stomach. TTE depicted a large pericardial effusion with heterogeneousechogenic particle swirling. Therefore, GPF was suspected, and pericardiot-omy, distal esophagectomy, and subtotal gastrectomy were performed. Intra-operative findings revealed gastric content in the pericardial space and thefistulous tract. Her hospital course was complicated by comorbidities; how-ever, a month later, she was discharged to a nursing facility.Discussion: GPF is a rare, often lethal complication associated with ulcerin the lesser curvature in close proximity to FP. Most common risk factoris a history of prior gastro-esophageal surgery (3-5% after Nissen’s FP).This can develop within 3 months, but the average time is 7 years. GPFmay be caused by the angulation from recurrent hernia on lesser curvature,chronic mechanical irritation from diaphragmatic crus, and/or technical fail-ure. This case underscores the possibility of late and lethal complication fromFP, which can occur years after surgery. The recognition of this late postoper-ative complication can lead to more timely care.
436
MALIGNANT ASCITES: AN ATYPICAL INITIALPRESENTATION FOR PANCREATIC ADENOCARCINOMA
Bennett B, Grover I. University of Mississippi, Jackson, MS.Case Report: Malignant ascites is a known complication of advanced stagepancreatic cancer; however, it is rarely if ever the sole presenting symptom.Here we present a case of metastatic pancreatic adenocarcinoma found inci-dentally in an AIDS patient presenting with ascites and acute kidney injury.
A 55 yr old male with DMII,HTN and AIDS was admitted for acute kid-ney injury and hyperkalemia. On exam,the patient was afebrile with normal vitalsigns and physical exam was remarkable only for large volume ascites and apositive fluid wave. Laboratory data was notable for a pre-renal etiology of acutekidney injury,anemia of chronic disease and a normal liver panel.
Paracentesis results were negative for infection and a serum-ascitesalbumin gradient of 0.8. Cytology was positive for adenocarcinoma and CTevaluation revealed a mass at the body and tail of the pancreas with promi-
nent peripancreatic lymph nodes. Biopsy confirmed the diagnosis of pancre-atic cancer and the patient was transferred to the Oncology service.
In this case we highlight a patient who was found to have advancedpancreatic cancer incidentally. Data suggests an increased prevalence ofpancreatic cancer in patient’s with AIDS receiving HAART leading to theincreased mortality. This leads one to question the possibility and utility ofscreening for underlying malignancy in the patients receiving HAART. Morestudies are needed to establish benefits of screening for malignancy in patientswith AIDS receiving HAART.
437
ESOPHAGEAL PERFORATION POST PNEUMATICDILATION FOR ACHALASIA MANAGED BYESOPHAGEAL STENTING
Elhanafi S, Said S, Cooper C, Alkhateeb H, Othman M, McCallum R.Texas Tech University Health Sciences Center, El Paso, TX.Case Report:Background: Pneumatic Dilatation is one of the most effective methodsfor treating achalasia. Esophageal perforation is the most serious complica-tion after pneumatic dilatation and has been reported to occur in the rangeof 1-5%. The appropriate management of esophageal perforation can rangefrom conservative medical treatment to surgical intervention.Method: We report a case of an 82 year old male who had an 8 monthhistory of dysphagia for solid and liquids, a 10lb weight loss and nocturnalregurgitation. The diagnosis of achalasia was established by endoscopic;barium and manometric criteria. He underwent a pneumatic dilation with a30mm Rigiflex balloon. A confined or limited esophageal perforation project-ing into the mediastinum just 1-2 cm above the GE junction was confirmedby a gastrografin swallow study performed immediately after the procedure.There was some accompanying abdominal pain. Patient was treated later thatday by placing a fully covered metallic esophageal stent in addition to anti-biotics, proton pump inhibitor, and fasting. Patient was discharged home3 days later able to eat liquid-soft foods. Follow up endoscopy 2 weeks laterand a gastrografin swallow showed a completely healed perforation and thestent was removed. Symptomatically he has done well, with no dysphagia orheartburn at two months follow up.Conclusion: Early esophageal stenting for esophageal perforation afterpneumatic dilation for achalasia is a treatment option which accelerates heal-ing, shortens recovery period, as well as decreasing hospital stay and costs.Key words: Esophageal perforation; Pneumatic dilation; Esophagealachalasia; Esophageal Stenting.
438
RECURRENT RHABDOMYOLYSIS AND PANCREATITISDUE TO CARNITINE PALMITOYLTRANSFERASE IIDEFICIENCY
Cucalon Calderon JR, Martinez J, Ponnambalam A. USA Children & WomensHospital, Mobile, AL.Case Report: 17 year old girl with recurrent rhabdomyolysis, presentedwith muscle pain, epigastric pain and dark colored urine. She had no fever.She had episodes of muscle pain and weakness after exertion once a yearfor the past five years. On examination she was dehydrated with diffuselytender abdomen and bilateral extremity tenderness. Her creatinine kinasewas 12,325 with elevated aldolase, AST and ALT indicative of rhabdomy-olysis. CT of the abdomen showed peripancreatic stranding. Work up foretiology of pancreatitis including lipid panel, ultrasound and hereditarypancreatitis profile were negative. Metabolic work up showed elevated acyl-carnitine with normal carnitine. CPT II sequencing showed a heterozygousmutation c.338C9T (p.S113L) and a heterozygous novel variant c.534_558delinsT. She completely recovered after conservative management.
CPT II deficiency is a fatty oxidation disorder affecting mostly males.S113L is the most common mutation occurring in about 60% of the patients.There is only one other report in the literature presenting with pancreatitis.The exact mechanism of pancreatitis is not known. More studies are neededto know whether the novel variant described in this patient affects the pan-creas. Treatment consists of avoidance of strenuous exercise and low fat diet.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 497
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Prominent pancreas with peripancreatic stranding
439
CHRONIC DIARRHEA: CASE OF MISTAKEN IDENTITY,A CASE REPORT
Fuller W, Grover I. University of Mississippi, Jackson, MS.Case Report: Patients with chronic diarrhea can have underlying malabsorp-tion syndromes vs infections enterocolitis. Association of Giardia Lamblia andCeliac disease is rare, although, Giardiasis can present with chronic diarrheaand may cause atrophy of intestinal villi in rare cases. We present a case wherea 33 year old Caucasian female presented with chronic diarrhea of 4 monthduration with seronegative but biopsy suggestive of Celiac disease, who waslater found to have positive stool antigen for Giardia. Patient was given a trialof gluten free diet after biopsy results without improvement of diarrhea butsymptoms improved with a course of Flagyl. The coexistence of Giardiasiswith underlying Celiac disease is rare but with negative anti endomysial andanti tissue transglutaminase antibodies, absence of anemia, as in our patient,the other etiologies of malabsorption and diarrhea should be ruled out beforemaking a diagnosis of Celiac disease as the wrong diagnosis can lead to gamutof other problems for the patient. Take away message is that chronic diarrheaunresponsive to antibiotics should be worked up with fecal leukocytes, stoolfor ova and parasites and referred to a Gastroenterologist sooner for furtherwork up and endoscopy.
Blunting of villi in Duodenum
440
STRONGYLOIDES HYPER-INFECTION SYNDROME ANDASSOCIATED DIFFUSE INTESTINAL HEMORRHAGE
Little BD, St. Hilaire RJ. University of Tennessee, Memphis, TN.Case Report: 75 yo male with a PMH significant for type II diabetesmellitus and two recent hospitalizations for COPD exacerbations who pre-sented with 2 week history of generalized weakness, epigastric pain worsenedwith po intake, early satiety, and constipation. Physical exam was significant
for faint bilateral expiratory wheezes, hypoactive bowel sounds, and mild epi-gastric tenderness to palpation with a WBC count of 10.7 without significanteosinophilia. CT scan of the abdomen revealed mild wall thickening of theproximal small bowel and a 2 cm polypoid lesion within the duodenum.EGD was completed revealing multiple shallow based esophageal ulcerationsand an adherent mucopurulent exudative material beginning in the secondportion of the duodenum with a hyperemic and ulcerated underlying mucosa.Biopsies specimens revealed HSV esophagitis and strongyloides sterocoralisinfection involving the small intestine. Patient was treated with po ivermec-tin and iv acyclovir. He required ICU management due to GNR bacteremia,pneumonia with associated respiratory failure, and neurologic dysfunction.Ten days after beginning treatment with ivermectin the patient developedsignificant hematachezia. EGD and colonoscopy were unrevealing, but atechnetium labeled TRBC scan was completed revealing diffuse bleedingfrom the small intestine. Angiography identified the bleeding from the proxi-mal jejunal branch supplying the small intestine, but embolization was notundertaken due to concern for diffuse small intestinal infarction. The patientrequired 48 units of PRBC during the prolonged episode of intestinal bleed-ing, but he did recover and survive until discharge.
Strongyloides hyper-infection syndrome is secondary to massive hema-togenous dissemination of larvae. Patients can present with sepsis, pneumo-nia, GNR bacteremia, fungemia, and or meningitis. Significant GI bleeding hasbeen reported in association with strongyloides infection. It is felt that mucosalinjury may result from direct invasion of larvae or secondary to massive deathof intramural and intraluminal larvae. Typically bleeding involves diffusesegments of intestine making intervention difficult. Aggressive supportive carewithPRBC transfusion and correction of coagulation are themainstayof treatment.
441
METABOLIC MODULATION OF INTESTINALENDOTHELIAL CELL ADHESION MOLECULES: ROLE OFTNF > AND AGLYCEMIA: A POSSIBLE MECHANISM INNEC INJURY?
Huda SA1, Pramanik AK1, Ganta CV2, Jennings M2, Jordan PA3,Alexander JS2. 1LSU-Health, Shreveport, LA; 2LSU-Health, Shreveport,LA and 3LSU-Health, Shreveport, LA.Purpose of Study: In gut injury, tumor necrosis factor > (TNF >) acti-vates inflammatory response results in dysregulation of epithelial junctionsand epithelial growth factor receptor (EGFR) signaling, and apoptosis.Endothelial cells adhesion molecules (ECAMs) play an important role ininflammation by enrolling macrophages and modulating the adaptive andinnate immunity. However, the relationship of cell inflammation and metab-olism including aglycemia, to intestinal ECAMs expression in inflammationare not well understood.
We studied the effect of TNF >, aglycemia and combined aglycemiaand TNF > on expression of Intracellular Adhesion Molecule-1 (ICAM-1),E-selectin, Mucosal Vascular Addressin Cell Adhesion Molecule (MAdCAM-1)and Vascular Cell Adhesion Molecule 1 (VCAM-1).Methods Used: ‘Immortomouse’ intestinal endothelial cells were culturedfrom H-2K(b)tsA58 mice in 10% DMEM medium in 24/48 wells and ex-posed, 20ng/ml TNF >, aglycemia, and TNF > and aglycemia. Cell surfaceenzyme linked immunosorbent assay was used to analyze ECAM expression.Data were analyzed with Dunnetts’ multiple comparisons test.Summary of Results: Intestinal endothelial cells exposed to TNF > in-creases MAdCAM-1; similarly E-selectin is increased with aglycemia.In contrast combined TNF > and aglycemia increases both ICAM-1 andE-Selectin. However, VCAM-1 not affected by TNF > or aglycemia aloneor in combination. (Table).Conclusions: Metabolic stresses provoke varied responses in ECAMs ex-pression. The extent of synergism and antagonism from TNF > +/- aglycemiaon ECAMs expression remains to be defined.
Summary of the effects Aglycemia and TNF- > on ECAMs
ECAM Control TNF-> Aglycemia TNF-> + Aglycemia
ICAM-1 j j j p G0.01
E-Selectin j j p G0.01 p G0.01
MAdCAM-1 j p G0.05 j j
VCAM-1 j j j j
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
498 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

442
EXTRAMEDULLARY PLASMACYTOMA PRESENTING ASAN UPPER GASTROINTESTINAL BLEED
Fontenot EC1, Tombazzi C2. 1University of Tennessee Health SciencesCenter, Memphis, TN and 2University of Tennessee Health Sciences Center,Memphis, TN.Purpose of Study: Highlight an unusual presentation of extramedullaryplasmacytoma.Methods Used: Case Report.Summary of Results: A 64 year-old African-American male was ad-mitted to the medicine service of our hospital for weight loss and anemiaof approximately one month’s duration and a three day history of melena.Esophagogastroduodenoscopy revealed bleeding angioectasia in the gastricantrum that was treated by argon plasma coagulation. Despite treatment ofthe gastric angioectasia, the patient’s melena persisted, and colonoscopywas performed with no active bleeding seen. Capsule endoscopy was nextperformed, which revealed two slowly bleeding masses in the jejunum; onewas exophytic and partially obstructive. Enteroscopy was thus performed andrevealed a polypoid duodenal mass and two polypoid jejunal masses withbiopsy results indicating extramedullary plasmacytoma. Serum and urineprotein electrophoresis, serum free light chains, and skeletal survey were allnegative. Bone marrow biopsy revealed no clonal proliferation and positronemmison tomography demonstrated activity in the third portion of the duo-denum, proximal jejunum, and mid jejunum correlative with the masses seenendoscopically.Conclusions: This case highlights an unusual presentation of multiple ex-tramedullary plasmcytomas, without evidence of multiple myeloma, present-ing as an upper gastrointestinal bleed.
Bleeding Jejunal Mass
443
ONE ORDER OF ACUTE PANCREATITIS, PLEASE I HOLDTHE ENZYMES
Atkinson E, Engel LS, McKay M. LSU Health Sciences Center, NewOrleans, LA.Case: A 47 year-old woman presented with three days of unrelentingabdominal pain, which began shortly after she ate a meal. Her pain wassharp, severe, generalized but worst across her upper abdomen with someradiation to her back, and exacerbated by laying flat. She reported associ-ated nausea, vomiting, and diarrhea but denied blood in her emesis or stool.She reported occasional alcohol use, with no episodes of binge drinking.Examination revealed hyperactive bowel sounds and tenderness prominentover her left upper quadrant with voluntary guarding. She exhibited no peri-umbilical or flank ecchymosis. Laboratory studies were notable for an ele-vated WBC, total bilirubin, AST, ALT, with a normal serum amylase andlipase. Ultrasound of her right upper quadrant revealed a distended gall-bladder with stones and sludge but without wall thickening, pericholecysticfluid, dilation of the biliary ducts, or positive radiographic Murphy’s sign.
Abdominal radiograph showed a dilated transverse colon with abrupt cutoffat the splenic flexure. CT scan of the abdomen with oral contrast demonstrateddiffuse inflammation of the pancreas. The patient’s symptoms improved withbowel rest, intravenous fluids, and empiric antibiotics. Elective laparoscopiccholecystectomy was done on hospital day 3. She was discharged on hospitalday 4 and continued to do well at home. Microscopic examination of hergallbladder revealed chronic but not acute cholecystitis, and her final diag-nosis was gallstone pancreatitis. Retrospective analysis of a refrigerated urinespecimen provided on admit revealed a urine amylase of 1184 U/L, with anamylase-creatinine clearance ratio of 4.5%.Discussion: Acute pancreatitis is typically diagnosed by positive laboratoryfindings in the context of a compatible clinical presentation. While assays ofserum amylase and lipase are very useful for diagnosing acute pancreatitis,normal values do not definitively rule-out the diagnosis, nor do they reliablypredict a mild course. Cases of pancreatitis with normal lipase and amylase havebeen rarely reported in the literature, and in none of these cases was urine amylasemeasured. Our patient’s case calls to attention the utility of less frequently em-ployed but useful assays such as this when diagnostic uncertainty remains.
444
I’M JUST A GI FELLOW, BUT I KNOW WHY YOU HAVEJOINT PAIN.
Heard R, Ismail K. University of Tennessee Health Science Center,Memphis, TN.Case Report: A 41 year-old male with a past medical history significantfor joint pains, being evaluated by the orthopedic surgery team, is referredto GI clinic for elevated transaminases. Patient is without complaints otherthan his joint pain. He has no other medical problems, and has never hadany surgery. He drinks alcohol occasionally on weekends, but no significantamount. He does not smoke and has never abused drugs. His mother andfather both have diabetes, and his father died with ‘‘heart failure.’’
Laboratory testing reveals a hematocrit of 49, AST 37, and ALT 64.In the workup of his elevated transaminases, it was discovered that he hadan iron of 187, a total iron binding capacity of 200, and a percent saturationof 94%. His ferritin was 2360. Viral hepatitis serologies were negative.He was sent for HFE gene testing, where he was found to be homozygousfor the c282y mutation. A liver biopsy showed, ‘‘excessive iron deposition...consistent with hemochromatosis,’’ and, ‘‘portal/periportal fibrosis andbridging fibrosis grade 3.’’
Hemochromatosis is a hereditary disorder where mutations in the HFEgene lead to increased intestinal iron absorption. It is autosomal recessive,and is also associated with heart failure, diabetes, arthropathy, hypothyroid-ism, and hypogonadism secondary to iron overload. Progressive iron de-position in the liver leads to elevated transaminases, hepatomegaly, andeventually fibrosis/cirrhosis. Damage to the liver is usually reversible withtreatment. However, unfortunately for our patient, arthropathy is not usuallyreversible.
Hemochromatosis is treated with phlebotomy to decrease iron stores. Inour patient, we performed weekly phlebotomy with weekly CBC, iron, fer-ritin, and total iron capacity. His transaminases have normalized, but he iscontinuing with phlebotomy until his iron studies normalize. One shouldhave a low threshold to test for this disease, as iron studies are easily ob-tained, and the disease is easily treated.
Health Services ResearchConcurrent Session
1:00 PMSaturday, February 23, 2013
445
RESIDENT ACADEMIC PERFORMANCE AND PATIENTOUTCOMES DURING CODE BLUES AND RAPID RESPONSESARE SIMILAR DESPITE IMPLEMENTATION OF NEWACGME DUTY HOURS
Pepper DJ, Schweinfurth M, Herrin V. UMMC, Jackson, MS.Purpose of Study: From July 1 2011, new ACGME duty hours wereimplemented nationwide in the United States. Perceptions of residents and
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 499
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

faculty vary on the effectiveness of new duty hours. This study aimed todetermine whether new ACGME duty hours achieved the intended goalsof excellent patient care and improved resident learning.Methods Used: Retrospective cohort study of two 12-month periods(July 2010 to June 2011; July 2011 to June 2012) at an academic hospital. Forpatient outcomes we used the hospital registry for code blues and rapidresponses to compare the proportion of deaths and transfers to an intensivecare unit. For resident learning we compared percentile scores for annualin-service training examinations.Summary of Results: 656 events occurred during the 24-month period:187 code blues and 469 rapid responses. 48 (7.3%) deaths, 374 (57.0%)transfers to the intensive care unit and 234 (35.7%) stabilizations on the floorwere recorded. No significant differences were observed before and afterimplementation of new duty hours. Of all transfers to the intensive care unit,the proportion with a code blue decreased after implementation of new dutyhours (36% [63/174] vs. 25% [49/200], P=0.017). This finding was con-firmed in multivariate regression analyses (adjusted OR= 0.59, 95% CI:0.37Y0.92). The significant increase in percentile score (PG0.001, paired stu-dent t-test) for resident in-service training examinations after implementation ofnew duty hours (2010 to 2011) was similar to previous years (2009 to 2010).Conclusions: Resident academic performance and patient outcomes duringcode blues or rapid responses are similar despite implementation of new dutyhours. However, we did observe a reduced proportion of transfers to the ICU with acode blue. Larger, multicenter trials are needed to corroborate these findings. Strat-egies are needed to improve patient outcomes during code blues and rapid responses.
446
ROBOTIC TELEMEDICINE : TESTING IN A SIMULATIONSETTING
Islam AM, Muniz S, Gilbert G, Smoot J, Smalligan RD. Texas Tech UnivHSC, Amarillo, TX.Purpose of Study: Telemedicine is becoming an important method ofproviding specialty care to underserved areas across the United States. Atelemedicine robot that can travel throughout a facility and be operatedquickly and efficiently by a physician from a remote computer is underdevelopment. The face of the operating physician appears on the head of therobot with voice heard by the patient and nurse at the bedside. This pilotstudy sought to determine the ease of use, acceptability to residents andattendings, and the accuracy of the robot’s telemedicine system.Methods Used: Incoming residents and faculty were asked to first listento various heart and lung sounds on a high fidelity mannequin and note thefindings. Next, each participant operated the telemedicine robot from a re-mote site using a laptop to listen to the same sounds (in a different order).The robot’s high definition camera and otoscope were used to evaluate pupilsize and reactivity as well as to read small print from a medicine bottle.Summary of Results: As shown in the table, agreement was excellentbetween in person evaluation of breath/heart sounds versus remote evalua-tion using the robot’s equipment. All participants were also able to accuratelydetermine pupillary size using the robot’s camera and read a small wordof text using the otoscope. All participants answered affirmatively to thequestion ‘‘did you hear/see well using the robot’s equipment?’’Conclusions: This pilot project demonstrated that a prototype mobile andmaneuverable medical robot can provide timely and accurate history andphysical exam findings to the user physician. Given there are several com-munity hospitals with small ICUs that lack intensivists within 2 hoursof the university, there is an immediate need for this type of technologywhich would allow intensivists and other specialists to provide initial andongoing medical advice to clinicians in surrounding rural areas. The nextstep is to evaluate the acceptability and accuracy of the equipped robot withlive patients under an IRB approved study.
447
PILOT SURVEY OF COMPONENTS OF EMERGENCYMEDICAL SERVICES EMERGENT HANDOFFS
Lindsay LP1, White ML1, Campbell K2, Pruitt C1, Wang H3. 1University ofAlabama at Birmingham, Birmignham, AL; 2University of Alabama Schoolof Medicine, Birmignham, AL and 3University of Alabama at Birmingham,Birmignham, AL.Purpose of Study: Communication is an essential element of the transi-tion of care between Emergency Medical Services (EMS) and EmergencyDepartment (ED) providers. However, the salient elements of patient hand-offs are not known. We sought to determine EMS providers’ perceptions ofthe patient handoff process.Methods Used: We studied BLS and ALS EMS providers who transportpediatric patients to a regional children’s hospital. We developed a 12 itemsurvey regarding perceptions of the handoff process. Survey questions encom-passed components of, approaches to, and education for emergent handoffsbetween EMS and ED providers.Summary of Results: We received completed surveys from 105 respon-dents, including 23 (22%) EMT basic and 80 (76%) paramedics. Mostrespondents (63%) reported over 10 years of experience. Seventy-two percent(95% CI=62 to 80%) reported that their agency encourages standardization,but only 42% (95% CI=32 to 52%) have received training. Of those receiv-ing training 79% (95% CI=64 to 89%) indicated that their training was effec-tive or highly effective. Thirty-five percent of respondents (95% CI=26 to45%) described their handoffs as complete, while 15% (95% CI=9 to 25%)stated their handoffs had some or very little of the necessary information.Sixty-five percent of respondents (95% CI=55 to 74%) organized their hand-offs chronologically. Fifty percent (95% CI=40 to 59%) agreed that emergenthandoffs were fundamentally different from non-emergent ones. Handoffswere reported strongly or somewhat affected by multiple interruptions (91%,95%CI=82 to 95%), high noise level (84%, 95% CI=76 to 91%), and inter-activity with other providers (73%, 95% CI= 63 to 81%). EMS providersrated the most essential components of handoffs as chief complaint, mecha-nism of injury, medications given, response to medications, and physicalinterventions. Components rated lowest in priority were name, sex, weight,comorbid factors, and lab results (ie glucose).Conclusions: While identifying ideal elements, EMS providers reportedmultiple barriers to learning and delivering effective handoffs, thus provid-ing prospective on EMS provider priorities and serving as a basis for devel-opment of a standardized handoff tool.
448
EFFECT OF ELECTRONIC ORDER ENTRYON EMERGENCYDEPARTMENT ADMISSION TIMES
Narayanan S. UAB, Birmingham, AL.Purpose of Study: Long emergency department (ED) waiting times for ad-mitted patients may have a negative effect on timely medical care and patientsatisfaction. Electronic admission order entry was introduced at our institu-tion on June 1 2012, starting with a one-unit trial and expanding to all non-critical units on the General Inpatient Pediatric (GIP) Service in September 2012.Our goal was to compare ED admission times across this transition period.Methods Used: Data were collected from all ED admissions to the GIPService between May 2012 and September 2012. Times were noted for theadmission call, placement of admission orders, and patient departure from the ED.Direct admits from outside facilities were excluded. Patients with electronicorders were sent to their inpatient bed independent of order entry time, butpatients with paper orders required those orders before departure from the ED.Summary of Results: Pre-Electronic Order Entry - 240 patients were ad-mitted in May 2012 with a mean ED stay of 104.1 minutes after admissioncall, while orders were written at a mean of 59.6 minutes after admission call.
One-Unit Trial Period - 237 patients were admitted in July 2012 with amean ED stay of 107.4 minutes, with mean time to orders of 80.9 minutes.74 of the 237 patients (31.2%) received electronic orders. They had shorterED stay compared to those with paper orders (89.5 vs 115.5 minutes, pG0.05),but a longer time to orders written (104.5 vs 70.2 minutes, pG0.05).
Full Expansion Period - 303 patients were admitted in September2012 with a mean ED stay of 102.2 minutes and mean time to orders of101.7 minutes. 201 of the 303 patients (66.3%) received electronic orders
Sound Correct in person Correct with robot
Normal heart 17 17
Systolic murmur 17 17
Wheezing 17 17
Normal breath 17 16
Crackles 17 16
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
500 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

and had mean ED stay of 83.5 minutes, shorter than the One-Unit Trialgroup (pG0.05). However, time to orders written for the Full Expansiongroup was 113.1 minutes, significantly longer than the One-Unit Trial andPre-Electronic groups (pG0.05 and pG0.001, respectively.)Conclusions: Mean ED wait times decreased once strict criteria were inplace for usage of electronic versus paper orders. During a one-unit pilot,prescribers were often unsure whether to write paper or electronic orders. Thismay have remained a problem during expansion, as evidenced by increas-ing delays in writing admission orders. Institutions should be mindful of thedelays associated with multi-phase initiation of a new electronic system.
449
ADOLESCENTS AND ADULTS WITH CONGENITAL HEARTDISEASE IN U.S. EMERGENCY DEPARTMENTSAND HOSPITALS
King A, Collins R, Robbins J. University of Arkansas for MedicalSciences, Little Rock, AR.Purpose of Study: With advances in the care of congenital heart disease(CHD), 90% of patients are expected to survive to adulthood. In 2005, themean hospital charge for adults with CHD was $43,496. The purpose of thestudy was to evaluate hospital care utilization in this population includingemergency department (ED) visits and admissions, and identify common co-morbid medical conditions.Methods Used: Nationally representative data from the 2009 Nation-wide Emergency Department Sample (NEDS) and the Nationwide InpatientSample (NIS) were used to identify patients Q 11 years old with an ICD-9-CMcode for a major congenital heart defect who were treated in an ED oradmitted to an acute care hospital. National estimates of ED visits, hospitali-zations, and patient charges were compiled. Prevalences of common comorbidmedical conditions were also determined. Statistical analyses were weightedto adjust for the complex sampling design of the NEDS and NIS.Summary of Results: CHD was reported in an estimated 4,046 ED visitsand 4,781 hospitalizations for adolescents (11-20 years-old), and 47,871ED visits and 72,031 hospitalizations for adults (Q 21-years). Atrial septaldefect and ventricular septal defect were the most common CHDs. The mostcommon comorbid medical conditions in hospitalized CHD patients werehypertension (49%), chronic obstructive pulmonary disease (19%), diabetesmellitus (19%), anemia (15%), and renal failure (11%). The mean length ofhospital stay of patients Q 11 years of age was 6.5 days, with a mean totalhospital charge per visit of $66,716. The estimated cost of hospital admis-sions for patients Q 11-years-old in 2009 was $5.1 billion.Conclusions: Hospital care utilization by adolescents and adults with CHDsignificantly impacts the resources of the US healthcare system. The costof hospitalizations for these patients continues to increase. Comorbid medi-cal conditions are common in this population and contribute to increasedhealthcare utilization.
450
A RANDOMIZED, DOUBLE BLIND,PLACEBO-CONTROLLED TRIAL OF TOLVAPTAN INHYPONATREMIC PATIENTS WITH CANCER
Ali N, Palla S, George M, Salahudeen A. MD Anderson, Houston, TX.Purpose of Study: To test the efficacy of tolvaptan in cancer patientswith hyponatremia using a double blind placebo controlled trial based onadaptive randomization. The primary endpoint was to compare rate of tolvaptan-treated hyponatremia correction with that of placebo over 14 days whileboth receiving standard of care. The secondary objectives were to compare thelength of hospital stay (LOS) and the change in mental test score (MTS).Methods Used: Patients admitted to University of Texas MD Andersoncancer center (MDACC) were screened daily using electronic laboratorydata. The inclusion criteria were adult patients and euvolemic hyponatremia(125-130 mE/L). The exclusion criteria were critical illness, renal failure,correctable hyponatremia and use of Cyp-3A4 modulators.Summary of Results: 52 eligible patients were consented and were ran-domized by Investigational Pharmacy to receive either tolvaptan 15 mg dailyor matching placebo. Doses were titrated up for a daily increase of 6-12 mEq/Lserum sodium to attain a target of 136-145 mEq/L. Nine patients weremoved to ICU or hospice care, 3 discontinued due to polydipsia, 11 patients
withdrew consent or lost to follow up. 30 patients completed the study,13 received placebo and 17 tolvaptan. On day 14, the primary objective ofcorrection of hyponatremia was met in 16 out 17 patients on tolvaptan and1 out of 13 patients on placebo (P G0.05). The length of stay (table) was lowerin the tolvaptan group but did not reach statistical significance.Conclusions: Tolvaptan is more effective in correcting hyponatremia incancer patients compared to placebo in the setting of standard of care.
451
MEDICATION ADHERENCE IN OLDER ADULTS: A FOCUSGROUP STUDY
Holt EW1, Rung AL2, Ruiz R1, Krousel-Wood MA1. 1Ochsner ClinicFoundation, New Orleans, LA and 2Louisiana State University HealthSciences Center, School of Public Health, New Orleans, LA.Purpose of Study: To effectively address medication adherence and im-prove cardiovascular health among older adults, a deeper understandingis needed of the barriers that this age group faces and approaches that wouldbe most effective and feasible for improving adherence. We conducted afocus group study (n=25) in a diverse population of older adults with hyper-tension recruited from the Cohort Study of Medication Adherence in OlderAdults (CoSMO).Methods Used: Participants were assigned to one of four focus groupsbased on their previously measured medication adherence scores. A struc-tured guide was used to collect feedback on barriers to adherence and accept-ability and feasibility of intervention strategies. Qualitative data analysis wasperformed by four independent coders using directed content analysis.Summary of Results: Sixty-eight percent of participants were white, 54%were between the ages of 70 and 75 (age range = 68-82), the majority (64%)of participants were women, 56% were married, and 43% were taking 3 ormore classes of antihypertensive medications. The final coding framework out-lines factors at the individual, relationship, health care system, and environ-mental or policy level which affect adherence in older adults, including memory,knowledge, attitudes and beliefs, side effects, social support, interaction withhealth care providers, and cost and convenience of medication filling.Conclusions: Patient responses highlighted the varied nature of barriersand the need for interventions which are both multi-faceted and tailored.
452
TELEMETRY USE IN HOSPITALIZED GENERALMEDICINE PATIENTS
Loftley AE, Edwards W, Roberts T, Holmes-Maybank K, Caton C, Mauldin P.Medical University of South Carolina, Charleston, SC.Purpose of Study: The American College of Cardiology (ACC) and theAmerican Heart Association (AHA) have published guidelines for telemetryuse in the inpatient setting. However, we believed adherence was suboptimaland patients were placed on telemetry without meeting criteria at our institu-tion. We sought to determine the degree of adherence to the ACC and AHAguidelines for the use of telemetry among general medicine inpatients.Methods Used: We reviewed 100 charts of general medicine inpatientsplaced on telemetry between January 1, 2011 and December 31, 2011. Datawas extracted from chief complaint, history of present illness, past medicalhistory, and plan of care to determine compliance to the guidelines. Length ofstay and date (season) of admission were also abstracted.Summary of Results: Our review revealed approximately 39% of patientswere placed on telemetrywhile hospitalizedwithoutmeeting the guideline criteria.
Seasonal variance in compliance was also analyzed. Non-compliancewith the telemetry guidelines was highest in the winter (44%) and lowestin the summer (34%) months. The average length of stay also varied: winter(4.40 days), summer (6.16 days), fall (7.29 days) and spring (8.16 days).Conclusions: A large percentage of inpatients at our institution are placedinappropriately on telemetry, not meeting the criteria of the ACC and AHA
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 501
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

guidelines. We believe many practitioners are unaware of the guidelinesfor telemetry monitoring of hospitalized patients. Therefore, we are imple-menting a guideline-based decision support at time of order entry to facilitatea reduction in the number of patients inappropriately placed on telemetry.The seasonal variation of telemetry guideline compliance was unexpected.The relationship between seasonal variance in non-compliance and length ofstay during each season will be analyzed.
453
SEX DIFFERENCES IN BARRIERS TO ANTIHYPERTENSIVEMEDICATION ADHERENCE: FINDINGS FROM THECOHORT STUDY OF MEDICATION ADHERENCE AMONGOLDER ADULTS (COSMO)
Holt EW1, Joyce C2, Dornelles A1, Ruiz R1, Morisky DE3, Webber LS2,Muntner P4, Krousel-Wood MA1. 1Ochsner Clinic Foundation, New Orleans,LA; 2Tulane School of Public Health and Tropical Medicine, New Orleans,LA; 3Fielding School of Public Health, UCLA, Los Angeles, CA and4University of Alabama at Birmingham, Birmingham, AL.Purpose of Study: We assessed whether socio-demographic, clinical,health care system, psychosocial, and behavioral factors are differentiallyassociated with low antihypertensive medication adherence scores amongolder men and women.Methods Used: We conducted a cross-sectional analysis using baseline datafrom the Cohort Study of Medication Adherence in Older Adults (CoSMO,n=2,194). Low antihypertensive medication adherence was defined as a scoreG6 on the 8-item Morisky Medication Adherence Scale. Risk factors for lowadherencewere collected using telephone surveys and administrative databases.Summary of Results: The prevalence of low medication adherencescores did not differ by sex (15.0% in women and 13.1% in men p=0.208).In sex-specific multivariable models, having issues with medication costand practicing fewer lifestyle modifications for blood pressure control wereassociated with low adherence scores among both men and women. Factorsassociated with low adherence scores in men but not women includedreduced sexual functioning (OR = 2.03; 95% CI: 1.31, 3.16 for men andOR = 1.28; 95% CI: 0.90, 1.82 for women), and BMI Q25 (OR = 3.23;95% CI: 1.59, 6.59 for men and 1.23; 95% CI: 0.82, 1.85 for women).Factors associated with low adherence scores in women but not men in-cluded dissatisfaction with communication with their healthcare provider(OR = 1.75; 95% CI: 1.16, 2.65 for women and OR =1.16 95% CI: 0.57, 2.34for men) and depressive symptoms (OR = 2.29; 95% CI: 1.55, 3.38 forwomen and OR = 0.93; 95% CI: 0.48, 1.80 for men).Conclusions: Factors associated with low antihypertensive medication ad-herence scores differed by sex. Interventions designed to improve adherence inolder adults should be tailored to account for the sex of the target population.
454
SPIROMETRY IS NOT AN ADEQUATE PREDICTOR OFHOSPITALIZATION IN CYSTIC FIBROSIS PATIENTS
Keeton KL1,2, Haynes D1,2, Petrini M1,2. 1University of Mississippi, Jackson,MS and 2GV Sonny Montgomery VA Medical Center, Jackson, MS.Purpose of Study: Spirometry is obtained at routine follow-up every threemonths for patients with CF as recommended by the CF Foundation withoutdata to support this practice. We hypothesized that there is no associationbetween hospitalizations and a significant decrease in FEV1.Methods Used: The patient population consisted of 104 patients who arecurrently greater than 18 years old with a confirmed diagnosis of CF withdata collected from 1/2002 until 5/2012. Hospitalization dates and spirometrydata were obtained from the medical record. The criterion of a 10% decreasein FEV1 considered a clinically significant change in CF was used. Because10% may represent G 0.2L, and thus within the scatter of the technique, datawere re-analyzed combining a 10% and at least 0.2L decrease, a criterion usedin other patients. Flow volume loops were paired with hospitalizations andanalyzed by Fisher’s Exact Test to determine association.Summary of Results: From the 104 patients, 33 were excluded for lackof hospitalizations or spirometry. In the remaining 71 patients, there were146 hospitalizations matching with an FEV1 and 753 FEV1s that did notmatch a hospitalization. There was no association between FEV1 and hospi-talization. (P = 0.32) when the Q 10% decrease criterion was used, or when
the combined 10% and 0.2 L was used as shown below; 74 FEV1 were con-sidered significant by the 10% criterion but decreased by only 0.14 L.Conclusions: There is no association between hospitalization and a sig-nificant decrease in FEV1. Routine spirometry is not useful in predictinghospitalization. A combination of 10% and 90.2L decrease in FEV1 shouldbe used to determine a clinical significance change to avoid those that fallwithin the repeatability of the measurement.
455
IMPROVING ACCESS TO CARE USING COMMUNITYHEALTH WORKERS ON A MOBILE CLINIC
Portillo E1, Moyer V1,2, Goetz M1,2, Si X1. 1Baylor College of Medicine,Houston, TX and 2Texas Children’s Hospital, Houston, TX.Purpose of Study: We evaluated the effectiveness of using communityhealth workers (CHWs) to assist families of children seen on the TexasChildren’s Hospital SuperKids Mobile Clinic (SKMC) to 1) increase thenumber of eligible children who successfully enroll in SCHIP or Medicaid,2) increase the number of uninsured family members not eligible for SCHIPor Medicaid who successfully obtained access to community health resources,and 3) increase parents’ understanding and use of a medical home. We alsoaimed to identify characteristics common to children and families who ob-tained insurance compared to those who did not.Methods Used: The SKMC provides service in Houston’s Gulfton neigh-borhood to uninsured and underinsured children, the majority of whomcome from non-English-speaking, Latino immigrant households. FromJanuary 2011-April 2012, families were asked if they would like to speak toa CHW regarding applying for insurance coverage, using low cost resources,and identifying a permanent medical home. For families who agreed to beseen, CHWs recorded age, gender, country of origin, and insurance status forall family members. CHWs provided application materials, reviewed insur-ance application forms, and offered assistance filling out applications, makingcopies of required documents, and submitting applications. At least 3 follow-upphone calls were made to families over 3-9 months. The final telephone sur-vey included validated medical home assessment items from the NationalSurvey of Children’s Health. Analysis including descriptive statistics andlogistic regression will be completed using EpiInfo.Summary of Results: During the study period, 654 families (representing2,627 individuals) were enrolled and met with a CHW at least once, and498 families (76%) completed the final survey. Follow up data collection iscomplete, and preliminary analysis of the first 6 months of data suggests that theintervention increased insurance coverage for previously uninsured children, andincreased in the number of families able to identify a permanent medical home.Conclusions: The effects of the CHW intervention on access to insuranceand to a medical home, and characteristics predictive of attainment of bothwill be presented.
Hematology and Oncology IIConcurrent Session
1:00 PMSaturday, February 23, 2013
456
RECURRENT PANCREATITIS DURING MAINTENANCECHEMOTHERAPY FOR PRE-B ACUTE LYMPHOBLASTICLEUKEMIA
Erker CA1, Sandler E2, Taufiq S3. 1University of Florida, Jacksonville, FL;2Nemours, Jacksonville, FL and 3Nemours, Jacksonville, FL.Case Report: Acute Pancreatitis is a relatively common complication oftreatment for children with acute lymphoblastic leukemia. The vast majority
Significant FEV1 Decrease and Hospitalization
Hospitalized Not Hospitalized
Significant Decrease 27 131
Non-significant Decrease 119 622
P= 0.84, Sens= 0.18, Spec= 0.83, PPV = 0.17, NPV = 0.84 FEV1 Significant Decrease basedon 10% decrease in FEV1 and FEV1 decrease 90.2L
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
502 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

of cases are attributable to treatment with asparaginase. In this report, wedescribe two patients with ALL who developed several episodes of recurrentacute pancreatitis temporally unrelated to treatment with asparaginase. Wereview other potential etiologies, including other medications commonlyused to treat children with ALL. When children with ALL present with symp-toms of pancreatitis, especially when it does not appear related to asparagi-nase treatment, it is important to consider other etiologies and adjust therapyaccordingly.
457
ANTICANCER HORMONES MADE IN THE HEART TARGETBETA-CATENIN IN HUMAN CANCERS
Vesely DL1,2, Skelton WP1,2, Skelton MN1,2. 1James A. Haley VA MedicalCenter, Tampa, FL and 2University of South Florida Morsani College ofMedicine, Tampa, FL.Purpose of Study: To determine if Beta-catenin is a central target in theanticancer effects of four cardiac hormones, namely atrial natriuretic factor,vessel dilator, long-acting natriuretic peptide and kaliuretic peptide which havepotent anticancer effects on some of the most lethal cancers, eliminating up to80% of human pancreatic cancers, 86% of human small-cell lung cancersand 2/3rds of human breast cancers growing in athymic mice. Once thesehuman cancers are eliminated secondary to these heart hormones, the cancersnever return in the lifespan of the mice. Beta-catenin is a multifunctionalprotein located on the intracellular side of cytoplasmic membrane that causesgrowth of pancreatic, colorectal and renal cancers.Methods Used: Beta-catenin was measured with an ELISA (R&D Sys-tems, Minneapolis, MN) in dose-response evaluations secondary to four car-diac hormones in three different human cancers, i.e. pancreatic, colorectal andrenal cancer cells.Summary of Results: We found that a central target of these heart hor-mones is Beta-catenin. In dose-response relationships each of these fourheart hormones decreased the concentration of Beta-catenin up to 88% inhuman pancreatic cancer cells, up to 83% in human colorectal adenocar-cinoma cells, and up to 73% in human renal adenocarcinoma cells.Conclusions: These results provide molecular insight into why Beta-catenin should be considered central to these hormones’ anticancer effectsas the heart hormones also inhibit upstream Ras kinase which activatesBeta-catenin and the downstream c-Jun-N-terminal kinase 2 and vascularendothelial growth factor which are activated by Beta-catenin.
458
DIFFERENCE IN PROGNOSTIC FACTORS BETWEENADULTS AND PEDIATRIC PATIENTS WITHPARATESTICULAR RHABDOMYOSARCOMA
Dang P1, Dang ND2, Samuelian J2. 1Tulane School of Medicine, NewOrleans, LA and 2Baylor College of Medicine, Houston, TX.Purpose of Study: Paratesticular rhabdomyosarcoma (PTRMS) is themost common primary solid tumor arising from the mesenchymal tissueof the testis, spermatic cord, epididymis, and tunica vaginalis. Several studieshave reported an inferior survival outcome in adults compared to childrenwith PRRMS. In this study, we analyzed the difference in prognostic factorsbetween adult and pediatric patients including tumor characteristics, patientcharacteristics, and survival outcome.Methods Used: 255 cases of PTRMS were identified from the Surveillance,Epidemiology, and End Results (SEER) Program of the National CancerInstitute 1973-2009. The JMP 10 statistical software was used to compare thedifference in patient and tumor characteristics between adult and pediatricpatients. Estimates of overall survival were performed using the Kaplan-Meier method.Summary of Results: There were 87 adults (34%) and 168 children (66%).The racial distribution is similar between the two groups. Pleomorphic his-tology is more common in adults (15%) than in children (1%) (p=0.0002).Embryonal histology is the most common histologic subtype in both adultand children accounting for 64% of cases in adults and 78% of cases inchildren. The 5- and 10-year overall survival (OS) is 63% and 61% for adultsand 90% and 87% for children (pG0.0001). Adults tend to present with largertumor size compared to children (56% vs. 47% 95 cm). Also, a higher
proportion of adults present with positive nodal involvement and positivedistant metastasis than children, 40% vs. 24% and 33% vs. 24%, respectively.Conclusions: Children diagnosed with PTRMS have better survival out-come than adults. Adults tend to present with larger tumor than that ofchildren. Adult patients are more likely to present with node involvement anddistant metastasis that dictate the worse prognosis in adults.
459
EBVAS A CO-FACTOR WITH HPV IN THE DEVELOPMENTOF ANAL CANCER
McKinnies E1,2, Dargas J1,2, Sutton K1,2, Meyaski-Schluter M1,2, HagenseeM1,2. 1LSUHSC, New Orleans, LA and 2LSU Health Sciences Center, NewOrleans, LA.Purpose of Study: We have previously shown that Epstein Barr Virus(EBV) may act as a cofactor along with Human Papillomavirus (HPV) inthe development of cervical cancer. EBV is a large dsDNA virus which canbe shed from the cervix and is the etiologic agent of Burkitt’s Lymphomaand Nasopharyngeal Carcinoma. There is a 2-4 fold increased risk of cer-vical dysplasia among HIV+ women who are co-shedding both EBV andHPV from their cervices, and HIV+ women with HPV-related cervical dys-plasia are at a high risk for developing similar pathology of the anus. Theincidence of anal cancer is increasing in HIV+ individuals, particularly inHIV+ men who engage in sexual activity with men (MSMs). We hypothe-size that anal shedding of EBV along with HPV also serves as a risk factorfor the development of anal dysplasia.Methods Used: HIV+ men and women were enrolled in an ongoing studyof the role of EBV and HPV induced cervical and anal disease. Anal swabscollected at 3 month intervals were tested for HPV by the Roche linear arrayassay and for EBV by a specific PCR assay and correlated with concurrentlyobtained anal Pap smears.Summary of Results: Anal samples were obtained from 94 HIV+women with 363 anal swabs and 224 anal Pap smears. Over 50% of theseanal Paps were abnormal with 39% ASCUS, 15% LSIL and 3% HSILdiagnoses. Anal shedding of high-risk HPV types was 79%. By sample,EBV and HPV were found in 52%, HPV only in 31% and EBV only in6% of the anal samples. Abnormal anal Pap smears (80%) or anal dysplasia(62%) were seen more often in those women co-shedding EBV and HPVas compared to those shedding only HPV (40 and 35% respectively). Tenanal samples were also obtained from 7 HIV+ men. All of these anal Papswere abnormal with 10% ASCUS, 80% LSIL, and 10% HSIL. Anal shed-ding of the high-risk HPV types was also 100%. EBV and HPV were foundin 70% of the anal sample.Conclusions: Anal HPV infection and dysplasia are common in HIV+ menand women. Shedding of EBV and HPV from the anus is a marker of currentdisease and may be utilized to improve the clinical care of HIV+ individuals.Future work is focused on correlating HPV and EBV anal shedding with analbiopsy results. HIV+ men, particularly MSMs, will continue to be screenedfor anal dysplasia, as well as anal HPVand EBV shedding.
460
CO-SHEDDING OF EPSTEIN-BARR VIRUS AND HUMANPAPILLOMAVIRUS AND THE INCREASED RISK OFCERVICAL DYSPLASIA
Plant JD, Sutton K, Hagensee M. LSUHSC, Metairie, LA.Purpose of Study: Previous studies have concluded that HPV, especiallyhigh risk (HR) HPV, is associated with the development of cervical dysplasiaand increased risks of cervical cancer. Even though HPV is linked to in-creased risks of cervical cancer, most who contract HR-HPV often spontane-ously resolve the infection without development of long-term dysplasia andsubsequent development of cervical cancer. Therefore, it has been proposedthat Epstein-Barr Virus, an oncogenic virus, and HPV co-infection can increaseHPV’s oncogenic effect.Methods Used: Cervical Vaginal Lavage (CVL) fluid from 26 HIV+women enrolled from the Woman’s Interagency HIV Study (WIHS) wascollected with each woman receiving follow-ups at six-month intervals. CVLfluid was tested for the presence of EBV at the time of development ofcervical dysplasia (low grade or high grade squamous intraepithelial lesions,SIL), 5 visits prior and 5 visits after by sensitive PCR assay and subsequent
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 503
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

gel electrophoresis. Additionally, samples were HPV genotyped for highrisk and low risk HPV based upon the IARC’s definition. If patient waspositive for EBV or HPV on visits 5, 6, and/or 7, she was deemed EBV orHPV positive at the time of censor. Dysplasia was recognized as LSIL orworse as per the Bethesda 2000 criteria.Summary of Results: Average age of the study women was 38 with amean CD4 cell count of 542 and HIV viral load of 87,000. EBV was de-tected in at least one of the eleven visits in 85% (n=22) of the patients. Ofthe women who developed dysplasia, 14 of 17 (82%) were co-sheddingHPV and EBV versus 3 of 9 women co-shedding who did not developdysplasia (p=.02, OR = 9.33, CI 1.1-102). Of the 14 women co-shedderswho developed cervical dysplasia, 3 shed EBV prior to HPV, 6 shed HPVprior to EBV, and 5 co-shed both together.Conclusions: This small data set supports the notion that HPV/EBV co-shedding increases risk of cervical dysplasia and amplifies HPV oncoge-nicity. The temporal relationship between EBV and HPV cervical sheddingcould not be determined by this small sample size. In the future, additionalwomen who develop cervical dysplasia will be tested for HPV and EBVcervical shedding.
461
LATE ONSET POST TRANSPLANT LYMPHOPROLIFERATIVEDISORDER, A DIFFUSE LARGE B-CELL LYMPHOMAWITH CYCLIN-D1 EXPRESSION AND COMPLICATEDBY PREGNANCY
Nagireddy S1, Milner C1, Herrin VE1, Lam J2. 1University of MississippiMedical Center, Jackson, MS and 2University of Mississippi Medical Center,Jackson, MS.Case Report: A 19 year old African American female with historyof Live Donor Renal Transplantation (LDRT) (mother was donor) at theage of 3 years for dysplastic kidney and immunosuppression with aza-thioprine, prednisone and tacrolimus was admitted to the hospital withcomplaints of abdominal pain, nausea and vomiting for one week. Shealso reported fullness in the left side of the abdomen for one month. Shewas 10 weeks pregnant on admission. Abdominal ultrasound showed a largeheterogeneous mass in the left abdomen. On further evaluation with MRI, alarge soft tissue mass of 14 X 10 cm was noted in the left side of the abdomenpossibly arising from the small intestine. Ultrasound guided left biopsy wasdone and pathology showed an atypical infiltrate of large lymphoid cells withscattered mitotic figures, positive for cyclin-D1, EBV-LMP 1, CD20, PAX5,BCL2, Ki-67 (80%), negative for CD3, CD5, CD10, CD30, CD138, Kappaand lambda. FISH for CCND1/IgH, t(11;14) was negative. She was diagnosedwith monomorphic PTLD, DLBCL 16 years after her renal transplant.
Her immunosuppression was downgraded to prednisone; we then facedan ethical issue with the timing of chemotherapy initiation during the preg-nancy. While contemplating pregnancy termination, she had a spontaneousabortion; CHOP-R was subsequently started. Following the first cycle of chemo-therapy, her hospital course was complicated by tumor lysis syndrome, lacticacidosis and neutropenic fever.
PTLD is a heterogeneous lymphoid neoplasm associated with immuno-suppression after solid organ transplant or allogeneic hematopoietic stem celltransplant. A majority of PTLD’s are associated with EBV. Early PTLDdevelops within one year and is more common than late PTLD. Also, B-cellPTLD is common than T-cell. Histopathology and immunophenotyping areessential for diagnosis. Reduction in immunosuppression, immunotherapywith Rituximab or/and chemotherapy is the main stay of the treatment. Inour case PTLD presented as late onset, 16 years after the transplant and wascyclin-D1 positive which is unusual for DLBCL; the case was further com-plicated by the patient’s first pregnancy.
462
THE ROLE OF LEVOFLOXACIN PROPHYLAXIS FORBK VIRUS INFECTION IN PEDIATRIC HEMATOPOIETICSTEM CELL TRANSPLANT
Fletcher M, Harry J, Velasco-Gonzales C, Yu L. LSUHSC, New Orleans, LA.Purpose of Study: BK virus (BKV) remains a source of significant mor-bidity and mortality among pediatric hematopoietic stem cell transplant(HSCT) recipients. Recent efforts have evaluated prophylaxis with fluoro-
quinolones to reduce the burden of BKV with promising results. This studyaims to determine the effectiveness of levofloxacin (LF) prophylaxis in pre-venting BKV infection in a cohort of pediatric HSCT patients.Methods Used: Retrospective chart review of all patients who under-went HSCT at our institution from 2009 through 2012 was conducted.Data collected included: demographic information, LF use, date/type ofHSCT, conditioning/immunosuppressive regimen, use of antiviral medica-tions, date of onset/grade of GVHD, BKV PCR levels in blood/urine, andhematuria onset date/peak grade. Outcome measures were peak BKV urineand blood PCR levels, time to onset of BKV viruria/viremia/hematuria,grade of hematuria and overall/100-day survival. Multivariable logistic regres-sions were used to evaluate the association of LF prophylaxis with outcomevariables.Summary of Results: 47 patient records were reviewed. 15 patients (32%)received LF prophylaxis. No significant differences were present betweenthe prophylaxis and no prophylaxis cohorts. In multivariate modeling, LFprophylaxis did not lower the incidence of BK, BK viremia or hematuria,nor did it decrease the peak BKV PCR level in the urine or blood (SeeTable 1). LF also did not affect the time to the development of BK viruria,BK viremia or hematuria (data not shown). LF prophylaxis did not improveoverall survival, although there was a trend towards significant improvementin 100-day survival.Conclusions: Levofloxacin for BKV prophylaxis was not effective in re-ducing the incidence or severity of BKV infection in this cohort of pedi-atric HSCT patients. There was a trend towards decreased 100-day mortalityamong those patients receiving LF prophylaxis.
463
TIME TO ANTIBIOTIC ADMINISTRATION IN CHILDRENWITH FEVER AND CHEMOTHERAPY-INDUCEDNEUTROPENIA
Cohen CT1, Parsons K1,2, King A1,3, Kutny M1,4, Friedman GK1,4. 1UABDepartment of Pediatrics, Birmingham, AL; 2Children’s of Alabama,Birmingham, AL; 3UAB Department of Pediatrics, Birmingham, AL and4UAB Department of Pediatrics, Birmingham, AL.Purpose of Study: Patients with chemotherapy-induced neutropenia areat high-risk of significant morbidity and mortality from infectious causes.Prompt and appropriate antimicrobial therapy is essential for children withfebrile neutropenia (FN). Studies have demonstrated that decreasing thetime from presentation to administration of antibiotics in FN significantlyimproves outcomes. We hypothesized that patients presenting to the emer-gency department (ED) with FN would receive antibiotics sooner and haveimproved outcomes compared to patients presenting to the hematology/oncology clinic.Methods Used: A retrospective chart review was undertaken of patientswho presented to Children’s of Alabama ED and hematology/oncologyclinic with FN to determine the length of time from presentation to antibioticadministration and outcomes. Between August 2010 and December 2011,there were 134 visits of chemotherapy-induced FN (ANCG500).Summary of Results: A source of the fever was identified in 13.4% ofthe cases (18 patients). These include 8 patients with positive blood cul-tures (ED=4, clinic=4), three positive viral respiratory panels, three positiveurine cultures, two positive brochoalveolar lavage cultures, one bacterialmeningitis, and one positive throat culture. The most common bacterialorganisms identified were Streptococcus species (31%) Escherichia coli
Levofloxacin
(n=15)
No prophylaxis
(n=32)
Relative
risk
95%
C.I. P
BK viruria (%) 33.3 31.2 0.75 0.34-1.64 0.7
BK viremia (%) 26.6 15.6 1.1 0.36-3.34 0.82
Hematuria (%) 33.3 31.2 1.0 0.42-1.48 0.94
Mortality (%) 20.0 31.2 0.64 0.20-1.99 0.66
G100 day mortality (%) 0 15.6 0.82 0.22-3.03 0.057
Peak urine BKV PCR,mean (copies)
2.38E+09 2.53E+09 n/a n/a 0.92
Peak blood BKV PCR,mean (copies)
1829 2422 n/a n/a 0.69
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
504 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

(23%), and Staphylococcus species (15%). There were 9 ICU admissions(ED=5, clinic=4) and two deaths (ED=2). Antibiotics were administeredat a mean of 97T58 minutes for patients assessed in the ED (N=100) and86T69 minutes in the clinic (N=34) (p=0.37).Conclusions: We conclude that presentation to the ED compared to theclinic did not improve time to antibiotic administration. A higher percentageof patients presenting to the clinic had a positive blood culture (12% vs. 4%)and required an ICU admission (12% vs. 5%) compared to ER. We are estab-lishing standard guidelines to improve time from presentation to antibioticadministration for FN patients in the ED and clinic. Future studies will ex-amine if these new guidelines improve patient outcomes.
464
A 10-YEAR RETROSPECTIVE STUDY OF LYMPHOMA INTHE MONOCLONAL ANTIBODIES ERA
Fletcher M, Jones M, Velasco-Gonzales C, Velez MC. LSUHSC, NewOrleans, LA.Purpose of Study: To analyze the cases of lymphoma treated at ourinstitution over the last 10 years, with emphasis on the role of monoclonalantibodies in the treatment of non-Hodgkin’s lymphoma (NHL).Methods Used: A retrospective chart review for all patients diagnosedwith lymphoma at Children’s Hospital of New Orleans between 2001 and2010 was performed. Comparison to a previously described cohort ofpatients from 1995-2000 and from the 2008 Survival, Epidemiology andEnd Results (SEER) report was performed. Data collected included: disease,stage, location, bone marrow and/or CNS involvement, chemotherapy received,including the use of rituximab, underlying immunodeficiencies, date/type ofbone marrow transplant, and dates of relapse/death. Cox regression analysiswas performed to determine correlation between clinical variables and overall/disease-free survival.Summary of Results: Records from 69 patients were available for re-view (38 cases of HD and 33 cases of NHL). Mean duration of follow-upwas 3.6 years. Overall survival (OS) of all cases was 93% (See Figure 1),with a significant improvement in 5-year OS in NHL patients and slightimprovement in HD patients compared to the prior cohort. Advanced stagedisease (III/IV) at presentation was more common in our population thanthe national average. Relapse rates remained stable, and relapse was theonly variant associated with increased mortality (hazard ratio 18.2, [95% CI2.0-163.2], p=0.002). Fourteen patients received a monoclonal antibody,and the use of monoclonal antibodies did not improve survival among pa-tients with NHL.Conclusions: Survival of both NHL and HD improved in the moderncohort as compared to the previous cohort. In addition, outcomes at our insti-tution compared favorably to national survival data, in spite of a higher per-centage of patients presenting with advanced disease. The use of monoclonalantibodies in the modern cohort had no impact on survival.
465
SEBACEOUS ADENOCARCINOMA: SURVIVAL ANALYSISOF 2385 CASES
Dang P1, Trieu D2, Dang N3. 1Tulane School of Medicine, New Orleans, LA;2Tulane School of Medicine, New Orleans, LA and 3Baylor College ofMedicine, Houston, TX.Purpose of Study: Sebaceous gland carcinoma is a rare malignant tumorof the epithelium of the sebaceous gland. Sebaceous glands occur through-out hair-bearing areas of the body, but they are most abundant in the skinof the head and neck. In this study, we analyzed the different regions ofprimary tumor, methods of management, and ultimately outcomes.Methods Used: 2385 cases of sebaceous carcinoma were obtained bythe Surveillance, Epidemiology, and End Results (SEER) Program of theNational Cancer Institute 1973-2009. The JMP 10 statistical software wasused to compare the difference in patient and tumor characteristics. Character-istics of patients included sex, age at diagnosis, and race. Tumor character-istics included grade, size, and therapy. Estimates of overall survival wereperformed using the Kaplan-Meier method.Summary of Results: The most common site of sebaceous carcinomawas the head area (66.2%). There was a higher incidence in male (57%)and in Caucasian (85%). The overall survival (OS) rates were similar for
male and female, 47.2% and 46.3% at 10-year, respectively. Older age wasassociated with worse survival outcome. The 10-year OS rate was 76.3%for patients G65 years, 52.2% for patients between 65 and 75 years, and 52.5and 22% for patients 9 75 years of age (pG0.0001). The 10-year OS ratesfor grade I, II, III, and IV were 54.5%; 52.2%; 38.2%; and 46%, respectively(p=0.047). Tumor 92 cm had a worse prognosis than smaller ones with 10-yearOS rates of 33.1% and 48.7% , respectively (p=0.01). Those who had surgeryas part of the treatment had better survival outcome than those who did not(10-year OS of 47.4% vs 41.3%, respectively, p=0.0003).Conclusions: Male and female have roughly the same overall survivalrates. Older age at diagnosis is associated with worse outcome. Low tumorgrade, tumor size G2 cm, and surgery are associated with improved survivaloutcome. Aggressive surgical therapy also resulted in better outcome thanlocal excision.
466
N-ACETYL CYSTEINE IN MANAGEMENT OFMETHOTRAXATE INDUCED KIDNEY DAMAGE
Shah RK, Singh R, Regueira O, Turner C, Vasylyeva T. Texas Tech HealthScience Center at Amarillo, Amarillo, TX.Case Report: High Dose Methotrexate(HD MTX)/Leucovorin Rescue(LCV) alternating with Doxorubicin/Cisplatinum is the current therapy forOsteosarcoma in the Pediatric Population. N-Acetyl Cysteine(NAC) has beendemonstrated to decrease MTX induced renal damage in preclinical models.We describe the use of NAC to reverse MTX induced nephrotoxicity in anadolescent treated with MTX/LCV for osteosarcoma and evaluated a possi-ble mechanism of NAC renal protective properties.
18-year old women initiated chemotherapy for osteogenic sarcoma of theleft proximal humerus with alternating cycles of Doxorubicin/Cisplatinum(Doxo/CDDP) and HD MTX/LCV. Pretreatment serum creatinine (Scr) levelwas 0.57 mg/dl and received prehydration with IV fluids at 3000 cc/m2. Thepatient was admitted for a sixth overall systemic chemotherapy encounter(Doxo/CDDP - cycles 1 and 3) and specifically the fourth admission for in-travenous HDMTX which was administered at a dose of 12 g/m2 over 4 h.She received post hydration intravenous fluids and LCV 15 mg/ m2 IV/POevery 6 h beginning at 0 hour. Serum MTX levels at 24, 48 and 72 hoursafter MTX infusion demonstrated toxic range. Serial Scr levels increased to0.87 and 1.43 mg/dl at 24 and 48 hours respectively. Sixty hours after theMTX infusion, we began NAC 600 mg orally every 8 hours. The Scr leveldecreased to 1.01 and 0.80 mg/dl on day 4 and day 5 respectively.
Scr levels decreased to 1.01 and 0.80 mg/dl on day 4 and day 5 respectively.For subsequent admissions for HD MTX/LCV therapy, we co-administeredprophylactic NAC and Scr level remained between 0.65 to 0.95 mg/dl. MTXlevels have remained in therapeutic levels.
To understand underlining mechanisms leading to renoprotection weperformed in vitro study. Mouse mesangial cells (MMC) were exposed with10KM MTX, 10mM NAC and 10KM MTX+ 10mM NAC for 15, 40, 60and 120 minutes.ROS production was measured by standard technique. After60 minutes, there was a slight increase in ROS production in cells exposedto MTX while decrease in ROS production in cells exposed to MTX+NAC.Summary: NAC may be considered in MTX containing treatment proto-cols as a renoprotective agent, which most likely act as an antioxidant andreduce of ROS formation in renal cells.
Infectious Diseases IIConcurrent Session
1:00 PMSaturday, February 23, 2013
467
IMPROVING TUBERCULOSIS SCREENING AND ISONIAZIDPREVENTATIVE THERAPY IN AN HIV CLINIC IN ADDISABABA, ETHIOPIA
Zaeh S1, Kempker R1, Stenehjem E1, Blumberg H1, Ofotokun I1, Tenna A2.1Emory University School of Medicine (SOM), Decatur, GA and 2AddisAbaba University SOM, Addis Ababa, Ethiopia.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 505
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Purpose of Study: The World Health Organization recommends using asymptom algorithm (cough, weight loss, fever, night sweats) to screen forpulmonary tuberculosis (TB) among HIV-infected patients in resource lim-ited settings and offering isoniazid preventive therapy (IPT) in those whoscreen negative. We evaluated the rates of adherence to these recommenda-tions and the impact of a quality improvement (QI) intervention in a settingwith high rates of HIV/TB co-infection.Methods Used: The study took place in the HIV clinic of Tikur AnbessaHospital in Addis Ababa, Ethiopia. TB symptom screening and IPT admin-istration rates were recorded before and after a QI intervention. The inter-vention took place over two weeks and consisted of 1) education sessionswith health care workers, 2) strategic placement of posters in the clinic,and 3) the addition of a screening checklist to each patient’s chart.Summary of Results: 751 HIV+ patient visits were evaluated from June -August 2012. The mean age was 39 years and 64% were female. Of 751patient visits, 480 (64%) were seen by nurses and 271 (36%) by physicians.Prior to the intervention, 22% of patients were screened for TB symptomscompared to 94% after the QI intervention(PG.001). Physicians improvedscreening rates from 51% to 81%(PG.001) and nurses improved from 3%to 100%(PG.001).
Of those screened, 278 patients were symptom screen negative and 106were symptom screen positive. Of the 278 patients with negative screensand eligible for IPT, 4% were prescribed IPT prior to the intervention com-pared to 81%(PG.001) after the intervention. Of 106 patients with positivesymptom screens, orders for sputum AFB evaluation increased from 26%before the intervention to 69% after the intervention(PG.001).Conclusions: We found an intervention consisting of brief education andthe use of a screening checklist significantly increased rates of TB screeningand IPT administration. Additionally, nurses play an important role in TBscreening and prescribing IPT. Interventions based on operational researchcan play an important role in improving health care systems in resourcelimited settings.
468
NEXT GENERATION GROUPA STREPTOCOCCALVACCINES
Niedermeyer SE1,2, Penfound TA1,2, Pullen MF1,2, Courtney HS1,2, DaleJB1,2. 1University of Tennessee Health Science Center, Memphis, TN and2Veterans Affairs Medical Center, Memphis, TN.Purpose of Study: Group A streptococcal (GAS) infections result inÈ500,000 deaths/yr worldwide, with invasive infections and rheumatic heartdisease as the major contributors to mortality. Multivalent GAS vaccines in-corporating type-specific N-terminal M peptides from as many as 30 sero-types of GAS have been developed previously. Although these vaccines havepotential to afford broad protection in North America and Europe, the epide-miology of GAS infections in resource-poor countries indicates that addi-tional protective antigens may be needed to enhance vaccine efficacy. In thecurrent study we evaluated another GAS surface protein, M-related protein(Mrp), to determine its potential as a vaccine component that may broaden thecoverage of current M protein-based vaccines.Methods Used: Preliminary sequence analyses of mrp genes indicatedthat there were three families of structurally related Mrp’s. N-terminal pep-tides of Mrp2, Mrp4 and Mrp49, representing the three families, were clonedand purified. Rabbit antisera against the Mrp’s were assayed by ELISA andin bactericidal tests to assess the cross-protective potential against multipleserotypes of GAS.Summary of Results: Analysis of additional mrp sequences from a totalof 29 serotypes of GAS confirmed that only three structurally distinct fam-ilies exist. The Mrp rabbit antisera reacted in high titer with the homologousMrp, as determined by ELISA, and some cross-reactivity against heterologousMrp’s was observed. To determine the functional activity of Mrp antibodies,bactericidal assays were performed against a number of GAS serotypesexpressing Mrp. The Mrp antisera were bactericidal against homologous andheterologous serotypes, indicating the presence of cross-opsonic (shared) epi-topes on the surface of multiple GAS. Combinations of M and Mrp antiserashowed greater bactericidal activity than either antiserum alone, indicating anadditive functional role for each antibody population.Conclusions: Taken together, these results indicate that Mrp peptides couldbe important additions to multivalent vaccines composed of M peptides andthat a combination vaccine may provide much broader coverage against arange of GAS serotypes prevalent around the world.
469
EPIDEMIOLOGY OF METHICILLIN-RESISTANTSTAPHYLOCOCCUS AUREUS BLOODSTREAMCO-INFECTION AMONG PATIENTS WITH CANDIDEMIA
Reno JR1, Doshi S2, Scott J1, Stein B1,2, Farley MM1,2, Ray S1,2, JacobJT1,2. 1Atlanta Research and Education Foundation, Georgia EmergingInfections Program, and Atlanta Veterans Affairs Medical Center, Decatur,GA and 2Emory University School of Medicine, Atlanta, GA.Purpose of Study: Patients with candidemia are often at risk for otherinvasive infections, and methicillin-resistant Staphylococcus aureus (MRSA)is one of the most commonly co-isolated bacteria. We sought to identify therisk factors for, and outcomes of, Candida spp. and MRSA co-infections.Methods Used: The Georgia Emerging Infections Program conductedpopulation-based surveillance for candidemia and invasive MRSA in Atlanta.Medical records were reviewed. Candidemia cases with an incident culture datebetween March 1, 2008 and December 31, 2011 were analyzed. Co-infectionwas defined as incident MRSA bloodstream infection (BSI) within 30 days ofincident candidemia. We compared the healthcare-associated risk factors andoutcomes of co-infection cases to candidemia cases without MRSA BSI.Summary of Results: Of the 1,706 adult candidemia cases, most wereC. albicans (721; 42.3%), C. glabrata (487; 28.5%), C. parapsilosis (312;18.3%), and C. tropicalis (156; 9.1%). Among these cases, 94 (5.5%)were co-infections. With candidemia, co-infection was most frequent withC. tropicalis (13/156; 8.3%), C. glabrata (31/487; 6.4%), and C. albicans(40/721; 5.6%). Of the 94 cases of co-infection, MRSA BSI onset wascoincident with candidemia in 19 cases (20.2%) and occurred within 7 daysfor an additional 27 (28.7%). The median ages of the candidemia (60 years)and co-infection (58 years) groups were similar. No statistical association wasfound between co-infection and recent surgery, diabetes, or presence of cen-tral line, but the risk of co-infection was significantly increased by recentdialysis (25.5% vs. 14.9%, pe0.01). Mortality was higher among co-infectioncases (46.4% vs. 36.7%), but the difference was not significant (p=0.12).Conclusions: A small but important proportion (5.5%) of patients withCandidemia have co-infection with MRSA, suggesting the need to monitorblood culture results after one major pathogen is identified. Co-infectionwas the most common with C. tropicalis, and dialysis was a more importantrisk factor than a central line. Further studies are needed to determine patho-gen and host factors that may contribute to these increased risks.
470
THE ASSOCIATION OF PROTEINURIA AND OTHERSELECTED CHARACTERISTICS TO VITAMIN DDEFICIENCY
Rosales CB1, Frontini M2, Shakhashiro A2, Clark R2. 1LSUHSC School ofPublic Health, New Orleans, LA and 2LSUHSC School of Medicine, NewOrleans, LA.Purpose of Study: Vitamin D deficiency (defined as levels G 10 ng/ml) hasbeen shown to be independently associated with higher protein excretionamong diabetic HIV-infected injection drug users (IDUs).Methods Used: To determine if this association exists in a cohort of pre-dominantly non-IDUs, a retrospective study was performed on a conveniencesample of patients enrolled in the HIV Outpatient Program (HOP) clinic.Patients were eligible for this study if they met the following criteria: 9 18years of age, documentation of 92 valid urinalyses between 7/06 and 6/08,and documentation of 9 1 vitamin D level. Urinalyses showing blood (de-fined as 9 10 red blood cells per high power field) or pyuria (defined as 9 10WBC per high power field) were considered invalid.Summary of Results: Of the 66 patients meeting inclusion criteria, 7(11%) had a vitamin D level G10 ng/ml. The characteristics of the cohortshowed 21 (32%) were female, 53 (80%) were African American (AA), andmedian age was 45 years. Patients with a vitamin D level G 10 ng/ml werelikely to be 9 45 years (4 of 7), women (5 of 7), and AA (7 of 7). Avitamin Dlevel G 10 ng/ml was only significantly associated with female sex (p = 0.03).Bivariate analysis showed that vitamin D deficiency was not associatedwith race, age, body mass index, CD4 cell count G200, detectable HIV RNAlevel9400 copies, antiretroviral therapy, ACE therapy, or selected medicalconditions (including diabetes and hepatitis C). Although the frequencyof proteinuria 9 25 ng/ml was higher among patients with vitamin D levels
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
506 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

G 10 ng/ml compared to those with levels 9 10 ng/ml (5 of 7 (71%) vs 33 of59 (56%)), the prevalence difference did not reach statistical significance.Among diabetics all those with proteinuria levels 9 25 ng/ml showed lowlevels of Vitamin D. Only 1 of the 8 diabetic patients was deficient. Thesmall numbers precluded statistical analyses of the results.Conclusions: The prevalence of vitamin D deficiency appears to behigher among patients with proteinuria of 9 25 ng/ml compared to thosewithout proteinuria, but the small numbers of patients in this study limitedthe power to determine a significant difference. The HOP population athighest risk for vitamin D levels G 10 ng/ml are AA women.
471
NONTUBERCULOUS MYCOBACTERIAL INFECTIONS INHEMODIALYSIS PATIENTS
Colombo RE1, Chebrolu P1, Kheda M1, Nahman N1,2, Kintziger K1,2.1Georgia Health Sciences University, Augusta, GA and 2Charlie NorwoodVAMC, Augusta, GA.Purpose of Study: Nontuberculous mycobacteria (NTM) are ubiquitousenvironmental organisms associated with infection in both immunocompetentand immunocompromised patients. In end-stage renal disease (ESRD) patients,NTM peritonitis in peritoneal dialysis, and sporadic cases of cutaneous andpulmonary NTM in hemodialysis (HD), have been reported. To our knowl-edge, however, a systematic review of NTM infection in the HD populationhas not been previously performed. On this basis, we sought to characterizeNTM infections among ESRD patients on HD in the United States (US).Methods Used: All HD cases from the United States Renal Data System(USRDS) from 1998-2008 were queried for a diagnosis of NTM infectionand potential clinical covariates using ICD-9 diagnosis codes. Classificationof NTM disease was achieved via querying separate codes for pulmonary(PULM), disseminated (DISS), cutaneous (CUT), and ‘‘other’’ (OTH) NTM.Demographics and geographic distribution by region were also examined.To assess NTM independent of HIV, the HIV negative (-) patients were alsoassessed separately from HIV positive (+).Summary of Results: 1748 (0.16%) HD patients were diagnosed withNTM infection during the 11-year period of study. Demographics included:61% male, 57.5% aged 50 years or above, 45% African American, 28.4%HIV(+), and 27.0% transplant recipients. PULM infection (39.5%) was themost common type, followed by DISS (29.1%), OTH (27.3%), and CUT(4.8%). The majority (50.2%) of patients resided in the South; of these,57.5% lived in the South Atlantic region.
HIV (-) patients tended to be female [43.2% HIV (-), 26.5% HIV (+)],Caucasian [64.7% HIV (-), 10.2% HIV (+)], and aged 50 years or older[74.1% HIV (-),15.9% HIV (+)]. Nearly all (99.2%) of the transplant pop-ulation diagnosed with NTM were HIV (-). NTM type in HIV(-) patientswere: OTH 47.7%, PULM 42.6%, DISS 29%, and CUT 6.6%. The Southremained the most common region of residence regardless of HIV status[46.9% HIV (-), 59.4% HIV (+)].Conclusions: Greater than 70% of NTM infections diagnosed in HDpatients in the US from 1998-2008 occurred in HIV(-) individuals and27% were in transplant recipients. Patient demographics varied accordingto HIV status. Patients residing in the Southern US were disproportionatelyaffected by NTM.
472
NO ASSOCIATION OF CRYPTOCOCCAL ANTIGENEMIAWITH DEATH OR LOSS TO FOLLOW UPAMONG HIVPATIENTS IN ETHIOPIA
Smitson CC4, Tenna A2, Tsegaye M3, Shiferaw A5, Aseffa A5, BlumbergH1, Kempker R1. 1Emory School of Medicine, Atlanta, GA; 2Addis AbabaUniversity, Addis Ababa, Ethiopia; 3All Africa Leprosy, TB and RehabilitationTraining Centre, Addis Ababa, Ethiopia; 4Emory School of Medicine, Atlanta,GA and 5Armaeur-Hansen Research Institute, Addis Ababa, Ethiopia.Purpose of Study: WHO guidelines recommend cryptococcal antigen(CRAG) screening among HIV+ antiretroviral therapy (ART)-naBve adultswith a CD4 count G 100 cells/Kl in areas with a high burden of cryptococcaldisease. There is limited data on clinical outcomes of ART-experiencedpatients with cryptococcal antigenemia. We assessed clinical outcomes of apredominantly asymptomatic, ART-experienced cohort of HIV+ patients witha high (8.4%) prevalence of cryptococcal antigenemia.
Methods Used: The study took place at two ART clinics in Addis Ababa,Ethiopia. A retrospective study design was used to perform 12-month follow upof HIV-infected patients (CD4 G 200 cells/Kl) previously screened for crypto-coccal antigenemia. Medical chart abstraction was done to obtain data on clinicvisit history, ART use, CD4 count, opportunistic infections, and patient out-come. We evaluated the association of cryptococcal antigenemia and a com-posite outcome of death and loss to follow up (LFU) using logistic regression.Summary of Results: Among 367 HIV+ patients who underwent CRAGscreening, 323 (88%) were alive, 8 (2%) dead, and 36 (10%) LFU 12-monthsafter testing. Among 31 patients with a CRAG+ test (titers Q1:8), 28 werealive (titers e 1:512), 1 dead and 2 LFU (titers Q 1:1024). Only 3 CRAG +patients received fluconazole and none had lumbar puncture performed. Inmultivariate analysis, cryptococcal antigenemia was not predictive of death/LFU (aOR=1.3, 95% CI 0.3-4.8). Significant risk factors for death/LFUamong the entire cohort included CD4 count G 100 cells/Kl at baseline (aOR3.0, 95% CI 1.4-6.7), increasing CD4 count (aOR 0.1, 95% CI 0.1-0.3) andreceiving ART at last follow up visit (aOR 0.1, 95% CI 0.02-0.2).Conclusions: In an asymptomatic HIV+ cohort with high rates of ARTuse, cryptococcal antigenemia is not predictive of death or LFU. Our resultssupport recent WHO guidelines recommending screening for cryptococcaldisease only in ART-naBve patients with a CD4 G 100 cells/Kl and suggestthat ART is adequate in controlling low level cryptococcal antigenemia.
473
COCCIDIOIDES MENINGITIS IN AN IMMUNOCOMPETENTMAN IN NORTHEAST FLORIDA
Maraj P, Maharj J, Foster M. University of Florida College of Medicine-Jacksonville, Jacksonville, FL.Case Report: Coccidiodomycoses are endemic to the southwestern UnitedStates and northern Mexico. Outside the arid areas of Arizona and California,coccidioidomycoses are rare. In 2009, the Center for Disease Control andPrevention reported no cases of coccidiodomycosis in Florida. We report thecase of a 23 year old immunocompetent, male in Northeast Florida who pre-sented with headache and ataxia for one month. His headache was constant,dull, originated in the occipital area, radiated down the spine and was accom-panied by difficulty walking. He had associated blurry vision and photopho-bia. He denied any fever, cough, weight loss, night sweats, bowel or bladderincontinence. On examination he was afebrile with stable vital signs. He hadneck stiffness, but all systems were otherwise normal with negative Kernig’sand Brudzinski’s signs. CT Head revealed ventriculomegaly with high attenu-ation in the basal cisterns and Sylvian fissures. Tuberculosis and HIV testingwere negative. Lumbar puncture revealed elevated protein, low glucose andelevated white cell count with 62% lymphocytes. CSF was negative for AFB,HSV PCR, histoplasma antigen/antibodies, gram-stain and culture. CSF waspositive for coccidioidal IgM and IgG antibodies. Treatment was initiatedwith oral fluconazole, which resulted in improvement of his symptoms andstabilization of hydrocephalus within two weeks. Coccidioides may result ina wide spectrum of disease, mostly pulmonary. Of the extrapulmonary mani-festations, untreated coccidioidal meningitis has a mortality rate of almost100%. Even in the setting of appropriate treatment, Coccidioidal meningitiscan result in progressive hydrocephalus and sometimes necessitates ventricu-loperitoneal shunt placement. No radiological features distinguish coccidioi-dal meningitis from other granulomatous CNS infections. The treatment ofCoccidioidomycoses has been revolutionized by the discovery of azole drugswith most disease treatable on life-long oral medications such as fluconazole.Previously, the only treatment available was amphotericin B which had a highrate of complications. A high index of suspicion for coccidioides meningitis istherefore important in non-endemic areas, since migration and an expandingpopulation mean that disease is no longer confined to traditional areas.
474
GRAVES’ DISEASE IN A PEDIATRIC PATIENT WITH ACUTEEPSTEIN-BARR VIRUS INFECTION
Stoltenberg J, Dasari P, Balan A. The Children’s Hospital at The Universityof Oklahoma, Oklahoma City, OK.Case Report: Infection due to Epstein-Barr virus has a broad spectrumof possible clinical manifestations, ranging from self-limited mononucleosisin normal hosts to progressive and devastating infections in patients with
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 507
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

immune disorders. EBV has also been linked with an increased risk of devel-oping autoimmune diseases. We present a patient with new onset Graves’disease associated with acute EBV infection. While this association has beenreported in adults, to our knowledge, this is the first reported pediatric case.
Our patient is a 9 year-old Vietnamese boy with Down syndrome whopresented with fever and symptoms of upper respiratory infection, whichprogressed to respiratory failure requiring mechanical ventilation. His physi-cal exam was significant for tonsillar hypertrophy, a palpable goiter, systoliccardiac murmur, hepatosplenomegaly, generalized lymphadenopathy, and apetechial rash.
Laboratory findings were significant for Coomb’s negative hemolytic ane-mia, mild hepatitis, and acute elevation of inflammatorymarkers.We had a highindex of suspicion for EBV infection due to lymphadenopathy and hemolyticanemia. EBV serology was consistent with acute infectious mononucleosiswith elevated EBV Capsid IgG (2.93 ISR (0-0.9)) and IgM (0.95 ISR (0-0.9)),elevated EBV Early Antigen (2.05 ISR (0-0.9)), and negative EBV NuclearAntigen antibody. EBV DNA quantitative titers showed 1900 copies/ml. Thepatient had no prior history of thyroid disease or symptomatology, but thy-roid function testing was obtained due to tachycardia and the severity of hisacute illness. Results demonstrated an elevated Free T4 (2.9mcg/dL) and lowTSH (0.01mIU/ml). Thyroid ultrasound was consistent with thyroiditis andserology confirmed a diagnosis of Graves’ disease with Anti-Thyroglobulinof 93000 IU/ml (0-40) and Microsomal antibodies of 48 IU/ml (0-18).
It has been postulated that infection may play a role in the onset ofGraves’ disease. EBV reactivation has previously been shown to have aninfluence on Graves’ disease, possibly due to chronic immune stimulationof host B-lymphocytes. Primary EBV infection may play a role in Graves’disease and further study of this association could lead to better understandingof the pathogenesis of autoimmune thyroid disease.
475
COSTANALYSIS OF LABORATORY TESTING FOR SYPHILISSCREENING AFTER INSTITUTION OF REVERSESEQUENCE ALGORITHM IN 2011 IN COMPARISON WITHSTANDARD SYPHILIS TESTING IN 2009
Tangham G, Choudhary M, Tiller T, Matthews-Greer J. LSU Health SciencesCenter, Shreveport, LA.Purpose of Study: LSU Health Sciences center at Shreveport, a highendemic area for syphilis, instituted Syphilis IgG in 2010 as the initialscreening test due to high sensitivity and ease of automation of testing toreduce laboratory time and labor. In accordance with Louisiana Departmentof Health and Hospital requirements, Infection Control practice has beento report all positive nontreponemal and treponemal test results, and thispractice did not change over the study period. We hypothesized that syphilisIgG screening leads to excess secondary confirmation tests, overall increasedcost and additional health department notification.Methods Used: We conducted a retrospective review of syphilis samplestested positive and reported to the health department in 2009 using traditionalalgorithm of RPR screening followed by MHATP or FTA-ABS. We com-pared this with samples received, tested positive and number of reportingevents in 2011 using reverse algorithm of screening by Syphilis IgG, reflexedto RPR if positive/equivocal and further confirmatory test only on providerrequest. Cost charged by Laboratory per test for Syphilis IgG, RPR, MHATP,FTA-ABS and TP-PA were $48, $18, $55, $55 and $48 respectively. Costincurred by Infection control of $8.45 per positive test was calculated bycombining cost of printing hard copy, personnel time of 15 minutes for inves-tigation, completion of health department case report form, and postal costof batch mailing to health department.Summary of Results: In 2009, 556 RPR were reactive. Total positiveconfirmatory tests were 310; 273 by MHATP and 37 by FTA-ABS withtotal laboratory charges of $27,058. Cost incurred by Infection Control was$7,317.70 for reporting 886 positive tests. In 2011, 1248(12%) of 10,356 sub-mitted samples were reactive by IgG and 24(0.2%) equivocal. 750/1474(50%)of reflexed RPR were reactive. 79 underwent 3rd testing by MHATP orFTA-ABS and 77% were reactive. Cost incurred by Infection Control was$17,398 for reporting 2059 positive tests and total laboratory charges in-creased 3.3 fold to $90,779.Conclusions: Cost incurred by Infection Control for reporting increased137% and laboratory cost per reactive syphilis screen increased from $48to $72 after institution of reverse algorithm.
476
DISPROPORTIONATE INCIDENT CASES OFNON-HODGKIN’S LYMPHOMA IN AN URBAN CLINIC INTHE 21ST CENTURY
Silverton A1, Nguyen M1,2, Adamski M2, Mosunjac M1,2, Gunthel C1,2.1Emory University School of Medicine, Atlanta, GA and 2Grady HealthSystem, Atlanta, GA.Purpose of Study: Population-based studies have shown a dramaticdecrease in the incidence of HIV-associated NHL (HA-NHL) in the lateantiretroviral therapy (ART) era. We present our experience with HA-NHL.Methods Used: This is a retrospective descriptive analysis of a cohort ofPLWHA with NHL who received care at the Infectious Diseases Poncede Leon Center in Atlanta, Georgia from 1/1/2004 to 12/31/2010. Medicalrecords and electronic charts were abstracted for demographic data, cancerstage, CD4 count, HIV viral load, ART, International Prognositic Index (IPI),chemotherapy, and mortality.Summary of Results: 35 patients with HA-NHL were identified. Amongthese patients, 7 had BL, 20 had DLBCL, 7 had PL and 1 had PrimaryEffusion Lymphoma. 83% presented with advanced disease and 63% werenot on ART at diagnosis (dx). Overall, patients completed 67% of plannedchemotherapy (CX) cycles. Common causes for Cx termination were per-sistent myelosuppression (18.2%), social/patient preference (22.7%), anddeath (36.4%). 2-year overall survival was 40% for all non-Hodgkin’s Lym-phoma. Half of patients with DLBCL and only 14.3% of patients with BLwere alive at 2 years, the majority with suppressed viral loads.Conclusions: Despite national trends showing a decreased incidence ofHA-NHL in the late ART era, HA-NHL remains a significant problem inurban settings. Underutilization of care may be attributed to socioeconomichardships, poor adherence or substance dependence. Management of patientsin an urban setting with limited resources remains a challenge. Continuedefforts to provide prompt and continuous antiretroviral therapy as well as ap-propriate chemotherapy to patients with HA-NHL should be a high priorityin this population.
477
THE DOUBLE EDGED SWORD: TUBERCUOLSIS ANDDIABETES MELLITUS IN GEORGIA, USA
Foote MM1, Kempker RR1, Magee MJ2, Maggio DM3, Ray SM1,3. 1EmoryUniversity, Atlanta, GA; 2Emory University, Atlanta, GA and 3GeorgiaDepartment of Public Health, Atlanta, GA.Purpose of Study: Diabetes mellitus (DM) confers a significant risk ofdeveloping active tuberculosis (TB), yet questions remain regarding thecharacteristics of this association. This report is a comparison between dia-betic and non-diabetic pulmonary TB cases reported to a state TB program inGeorgia, USA.Methods Used: All verified TB cases reported 2009-2011 were reviewedusing the State Electronic Notifiable Disease Surveillance System (SENDSS).Associations between DM and TB characteristics were assessed using chi-square, t-tests, and multivariable logistic regression.Summary of Results: Among 1,168 reported TB cases in Georgia, 133(11.4%) had DM and 612 (52.4%) were sputum culture positive (cPTB).Among cPTB patients, those with DM (n=76) were on average older (54 vs.43 years, p G0.05) and had lower prevalence of HIV (2.6% vs. 14.4%,
Characteristics of the 35 HIV-associated NHL cases.
DLBCL Burkitt’s Plasmablastic
Number 20 7 7
Age (IQR) 46 (40, 51) 36 (34, 45) 38 (29, 52)
Race Black:white:other 14:4:2 5:1:1 5:2:0
CD4 at diagnosis (IQR) 110 (66-203) 98 (34-214) 165 (36-199)
ART at diagnosis yes:no 7:13 2:5 4:3
IPI 0:1:2:3:4 1:1:7:5:6 1:0:1:3:2 0:2:1:4:0
Cancer stage at presentation 1 or 2: 3 or 4 2:18 1:6 1:6
Treatment: Cx alone: Cx +ARV: ARV alone 6:14:0 0:7:0 0:6:1
Median survival (months) (IQR) 21 (12, 54) 8 (5, 21) 16 (3, 60)
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
508 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

pG0.05) than those without DM (n=536). After adjusting for HIV, age, andsex, DM was independently associated with a positive AFB smear at diagno-sis (aOR 2.0, 95% CI 1.1-3.6) and cavitary disease (aOR 1.8, 95% CI 1.1-3.1).There were no significant associations between DM and race/ethnicity, drugresistance, or death.Conclusions: TB patients with DM have evidence of more severe dis-ease at the time of presentation. The increased severity may be due to fasterprogression or later recognition of disease in these patients. TB patients withDM also pose a higher infectious risk given the association with sputumsmear positivity and cavitary disease. Prioritizing DM detection and man-agement should be an essential component to future TB control efforts.
NutritionConcurrent Session
1:00 PMSaturday, February 23, 2013
478
EFFECTS OF HIGH-DOSE CHOLECALCIFEROL ON SERUMMARKERS OF INFLAMMATION AND IMMUNITY INPATIENTS WITH EARLY CHRONIC KIDNEY DISEASE
Alvarez JA1, Zughaier SM2, Law J1, Hao L1, Wasse H3, Ziegler TR1,Tangpricha V1,4. 1Emory University School of Medicine, Atlanta, GA;2Emory+Children’s Center for Cystic Fibrosis Research, Atlanta, GA; 3EmoryUniversity School of Medicine, Atlanta, GA and 4Atlanta Veterans AffairsMedical Center, Atlanta, GA.Purpose of Study: Vitamin D has anti-inflammatory and immune-regulating properties. We aimed to determine if high-dose cholecalciferolsupplementation for 1 yr in subjects with early CKD improved circulatingmarkers of inflammation and immunity.Methods Used: In this double-blind, randomized, placebo-controlled trial,46 subjects with early CKD (Stage 2-3) were supplemented with oral chole-calciferol (50 000 IU weekly for 12 weeks followed by 50 000 IU everyother wk for 40 wks) or a matching placebo for 1 yr. Serum tumor necrosisfactor->, interleukin-6, monocyte chemoattractant protein-1 (MCP-1), inter-feron gamma-induced protein-10, and neutrophil gelatinase-associated lipo-calin were measured at baseline, 12 wks, and 1 yr. Serum cathelicidin (LL-37)was measured at baseline and 12 wks. An in vitro experiment was performedto investigate the effect of 1,25-dihydroxyvitamin D3 (1,25(OH)2D3) treat-ment on MCP-1 secretion in THP-1 monocytes activated with lipopolysac-charide (LPS) and Pseudomonas aeruginosa.Summary of Results: By 12 wks, serum MCP-1 decreased in the chole-calciferol group (66.2 T 2.5 to 60.8 T 2.6 pg/mL, group-by-time interactionP = 0.02) but was not different from baseline at 1 yr. Other markers of in-flammation and immunity did not change. In vitro, LPS- and Pseudomonas-activated monocytes treated with1,25(OH)2D3 had significantly less MCP-1secretion compared to untreated cells.Conclusions: High-dose cholecalciferol decreased serum MCP-1 con-centrations by 12 wks in patients with early CKD, although the decreasewas not maintained for the remainder of the year. In vitro results confirman MCP-1-lowering effect of vitamin D. Future studies should determine ifvitamin D-mediated reductions in MCP-1 concentrations reflect improvedclinical outcomes.
479
TRENDS IN FAT-SOLUBLE VITAMIN INTAKES ANDBLOOD CONCENTRATIONS IN ADULT SUBJECTS WITHCYSTIC FIBROSIS
Siwamogsatham O, Alvarez J, Tangpricha V. Emory University, Atlanta, GA.Purpose of Study: Pancreatic insufficiency is common in patients withcystic fibrosis (CF) leading to malabsorption of fat-soluble vitamins. Multi-vitamins including vitamins A, D, E and K have been routinely prescribed topatients with CF to prevent vitamin deficiencies. There has been increasedattention to prevention of vitamin deficiencies in patients with CF over thepast several years. The objective of our study was to examine whether in-creased supplementation in adults with CF resulted in improved serum con-centrations of fat soluble vitamins.
Methods Used: We conducted a retrospective chart review of patientswith CF who have been treated at Emory Clinic and Emory Hospital during2008-2012. We collected demographic information, fat-soluble vitamin con-centrations in blood and amount of fat-soluble vitamins prescribed duringeach year between 2008-2012.Summary of Results: One hundred and eighty-eight charts were reviewed.One hundred and one were male (53.7%) and 87 (46.3%) were female. Meanage (SD) was 31.4 (10.2) years. Mean (SD) body weight and BMI were 62.0(13.5) kg and 21.9 (4.0) kg/m2, respectively. Ninety-one percent of patientsused pancreatic enzyme replacement for malabsorption. Prescription for fat-soluble vitamins increased in the past 5 years (p G0.001). Based on post-hocanalyses, however, there was no significant increase in blood concentrationsof these fat-soluble vitamins over time (Table 1).Conclusions: Despite a near doubling of fat soluble vitamin intake overthe past 5 years, the changes of these vitamins serum concentrations werenot clinically significant. Potential reasons for vitamin levels not to par-allel the near doubling of intake levels include: sub-optimal dosages ofthese supplements, low adherence to these vitamins, or ongoing issues withmalabsorption.
480
MEASURING LIVER FATNESS IN OVERWEIGHTAND OBESECHILDREN WITH MAGNETIC RESONANCE IMAGING
Elam RE1,2, Allison JD3, Pollock N2,4, Rawson JV3, Davis CL2,4. 1GeorgiaHealth Sciences University, Augusta, GA; 2Georgia Health SciencesUniversity, Augusta, GA; 3Georgia Health Sciences University, Augusta, GAand 4Georgia Health Sciences University, Augusta, GA.Purpose of Study: Non-alcoholic fatty liver disease affects 38% of obesechildren and is associated with insulin resistance and metabolic syndrome.Current clinical methods of measuring liver fat fraction are invasive (biopsy)or have insufficient validity (ultrasound). Magnetic resonance (MR) imaging
Fat-soluble vitamins intake and serum concentration
Intake
Mean
(SD)
p
value
Serum
level
Mean
(SD)
p
value
Vitamin A (IU)
2008 (n=74)
2009 (n=112)
2010 (n=137)
2011 (n=161)
2012 (n=146)
10,095 (10,691)a
14,942 (15,072)b
17,700 (14,841)bc
19,194 (15,517)cd
20,189 (16,855)d
G0.001 Retinol (mg/L)
2008 (n=58)
2009 (n=95)
2010 (n=118)
2011 (n=135)
2012 (n=82)
Retinyl Palmitate
(mg/L)
2008 (n=57)
2009 (n=94)
2010 (n=116)
2011 (n=131)
2012 (n=81)
0.45 (0.21)ab
0.40 (0.17)b
0.43 (0.19)ab
0.44 (0.22)a
0.40 (0.19)ab
0.03 (0.02)
0.03 (0.02)
0.02 (0.01)
0.03 (0.04)
0.03 (0.04)
0.008
0.27
Vitamin D (IU)
2008 (n=77)
2009 (n=118)
2010 (n=144)
2011 (n=170)
2012 (n=150)
948 (691)a
1,570 (2,339)ab
1,779 (1,943)b
1,972 (1,896)b
2,013 (1,426)b
G0.001 25(OH)D (ng/mL)
2008 (n=89)
2009 (n=113)
2010 (n=127)
2011 (n=145)
2012 (n=87)
29.1 (13.0)bc
28.8 (11.1)c
32.1 (12.1)ab
32.6 (14.9)a
30.9 (15.0)abc
0.003
Vitamin E (IU)
2008 (n=76)
2009 (n=111)
2010 (n=139)
2011 (n=161)
2012 (n=146)
218 (223)a
279 (287)a
325 (298)b
342 (288)b
348 (296)b
G0.001 > Tocopherol (mg/L)
2008 (n=85)
2009 (n=104)
2010 (n=123)
2011 (n=138)
2012 (n=79)
A/F Tocopherol
(mg/L)
2008 (n=84)
2009 (n=102)
2010 (n=122)
2011 (n=135)
2012 (n=74)
8.9 (4.4)
8.9 (4.3)
8.1 (3.9)
8.3 (4.0)
8.1 (3.6)
1.0 (0.7)ab
1.0 (0.6)a
0.8 (0.6)b
0.9 (0.6)ab
1.0 (0.7)a
0.05
0.004
Vitamin K (IU)
2008 (n=73)
2009 (n=108)
2010 (n=135)
2011 (n=157)
2012 (n=142)
400 (573)a
575 (633)a
738 (662)b
794 (690)b
831 (694)b
G0.001 Vitamin K (ng/mL)
2008 (n=60)
2009 (n=48)
2010 (n=12)
2011 (n=3)
2012 (n=1)
0.84 (1.10)
0.71 (0.76)
1.15 (2.07)
0.73 (0.51)
0.06
0.73
Repeated measures ANOVA used to determine differences between the years. Values notconnected by the same letter are significantly different (Tukey’s Post-Hoc analyses).
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 509
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

is an alternative method, however few MR liver fat data exist in children.This study evaluated reliability and validity of noninvasive liver fat measuresusing MR imaging, in a cohort of overweight and obese children.Methods Used: MR images from 47 overweight children (age 8-11 years,43% male, 98% black, 70% obese) were scored twice (to assess test-retestreliability) for 3 liver fat measures: LIPO-Quant, Dixon 2-pt method ona single MR slice of the liver (Dixons), and Dixon 2-pt method averaging4 of 18 MR slices spanning the liver (Dixonw). Correlations of liver fat mea-sures with each other assessed concurrent validity. Correlations of liver fatmeasures with cardiometabolic risk markers (including central obesity, ele-vated blood pressure, raised fasting glucose and insulin, and dyslipidemia)assessed convergent validity.Summary of Results: All measures were reliable (ICC Q .98). LIPO-Quantcorrelated with Dixons and Dixonw (r = .41, .51, both P G .01), suggestingsome concurrent validity for all measures. LIPO-Quant correlated with per-cent body fat, visceral adipose tissue (VAT), and triglycerides (all .33 e re .36, P G .05) while Dixons correlated with BMI, waist circumference,percent body fat, VAT, and subcutaneous abdominal fat (all .45 e r e .50,P G .01). No significant associations were seen between Dixonw and cardi-ometabolic risk. The data suggests convergent validity for LIPO-Quant andDixons but not Dixonw.Conclusions: Dixons and LIPO-Quant are reliable, valid, noninvasive liverfat measures in overweight and obese children. Both have potential use inpediatric, prospective intervention studies. LIPO-Quant, a quantitative fatfraction, might be more clinically relevant.
481
THE EFFECTS OF PROTEIN INTAKE ON BODY FATPERCENTAGE IN PRETERM INPATIENT INFANTS
Atchley CB1, Williams PK1, Fields DA2, Anderson MP3, Bower A4.1University of Oklahoma Health Sciences Center, Oklahoma City, OK;2University of Oklahoma Health Sciences Center, Oklahoma City, OK;3University of Oklahoma Health Sciences Center, Oklahoma City, OK and4University of Oklahoma Health Sciences Center, Oklahoma City, OK.Purpose of Study: Most preterm babies have weights less than the 10thpercentile by the time they reach term-equivalent age. Traditional nutritionalstrategies in preterm infants result in higher rates of body fat accretion andabnormal fat distribution. Newer strategies emphasize early initiation ofamino acids and preterm formulas. Presently, the optimal nutritional strate-gies for ideal growth in preterm infants are poorly understood. We hypoth-esize that the percentage of fat mass will be reduced in premature infantswho consume more protein while in the neonatal intensive care unit.Methods Used: In this prospective, longitudinal study we are enrolling21 premature infants born at 24 0/7-28 6/7 weeks gestational age. Beginningat 30 weeks gestational age, babies are assessed for entry into the study.Growth and body composition are measured at study weeks 0, 2, and 4 usingair displacement plethysmography (i.e. Pea Pod) and anthropometry withmeasurements by dual energy x-ray absorptiometry at the beginning and endof the study. Nutritional information, including protein and caloric intake, iscollected during the study period and analyzed to determine the relationshipbetween protein intake and body fat percentage.Summary of Results: At this time, 12 subjects have been enrolled and8 have completed the study. The average caloric intake over 4 weeks was121.5 kcal/kg/day with an average protein intake of 3.2 g/kg/day. Subjectshave gained an average of 25 g/day over 4 weeks. Six of the 8 subjectswere discharged with weights greater than the 10th percentile. On prelimi-nary analysis, as protein increases by 1 g/kg/day, percent fat decreases by0.2656% for Pea Pod measures and decreases by 0.7505% for DXA mea-sures. However, the relationship does not yet reach statistical significance(Pea Pod p=0.8251; DXA p=0.1825).Conclusions: Additional patients will be evaluated to determine if thepreliminary findings between protein intake and body composition will reachsignificance.
482
FACTORS ASSOCIATEDWITH RAPID INFANT WEIGHT GAIN
White M, Kanafani N, Guild C, Rademacher S, Halloran D. Saint LouisUniversity, St. Louis, MO.
Purpose of Study: Many studies have shown that rapid infant weightgain (RIWG) is a risk factor for obesity in early childhood and adulthood.We explored the association between potential risk factors and RIWG in-cluding maternal demographics, behaviors and social risks, as well as infantfeeding practices, media use and sleep duration.Methods Used: 60 infants and their mothers were recruited from asingle academic pediatric practice in the Midwest during the neonatal visit.We obtained infant weight, length and survey data at each well-child visitthrough 12 months of age. Survey data included: maternal demographics,BMI, smoking status, perceived physical activity, diet, social support, riskof depression and intimate partner violence, and the infant’s diet (juice,cereal, fruit, vegetables, etc.), media use and sleep duration. RIWG wasdefined as an increase of Q0.67 SD in weight-for-length z-score betweenbirth and 12 months. Mann-Whitney U, W2 and t-tests were performed, asappropriate.Summary of Results: Mothers mean age was 25.6 years, 83.3% wereAfrican-American, 86.7% on Medicaid and 26.7% had less than a highschool education. Based on prepregnancy BMI, 3.3% were underweight,41.7% were normal weight, 11.7% were overweight and 38.3% were obese.50% of infants were male. 13 infants had under growth, 11 normal growth,3 rapid growth and 22 very rapid growth for a total of 41.7% with RIWG.37 infants had elevated weight at 12 months. Prepregnancy BMI was a riskfactor for RIWG; normal weight women were 1.87 times more likely tohave a child with RIWG than obese women (90% CI 1.03, 3.41). Maternalrace, marital status, education, smoking status, social support, perceivedphysical activity, diet, risk of depression and intimate partner violencewere not associated with RIWG. Infants who had cereal at 4 months were1.91 times more likely to have RIWG (90% CI 1.08, 3.38). No other infantfood groups showed an effect on RIWG. Duration of breastfeeding and in-fant sleep duration and media use at 6 and 9 months were not associatedwith RIWG.Conclusions: Other than early introduction of cereal at 4 months, noneof the maternal characteristics/behaviors or infant exposures were associ-ated with RIWG. Future research could examine maternal or infant physicalactivity and diet more closely or perinatal factors.
483
WOMEN, INFANT & CHILDREN NUTRITION PROGRAMHOUSED WITHIN A PEDIATRIC CLINIC: IS IRONDEFICIENCY ANEMIA IMPACTED?
Schwartz JD, Theriot JA, Franco SM, Nota MF. University of Louisville,Louisville, KY.Purpose of Study: Anemia, a low hemoglobin concentration or low hemat-ocrit level, is defined by age-and gender specific cutoff values. Iron defi-ciency anemia affects 2.4 million US children. It is associated with behavioraland cognitive delays. The Special Supplemental Nutrition Program for Women,Infants, and Children (WIC) is a federally funded nutritional program provid-ing iron rich foods to at risk children and pregnant mothers. Our indigentinner-city pediatric clinic has a WIC office onsite.
Our objective was to determine if having a WIC office on site staffedby nutritionists reduced the incidence of iron deficiency anemia in our clinicpopulation as compared to national WIC data.Methods Used: Charts of 12 month olds seen for a well-child visit fromJuly 2009 through June 2010 were reviewed. Demographic data, lengths ofbreast feeding, daycare attendance, hemoglobin and hematocrit values wererecorded. All patients were WIC participants. Anemia was defined as a hemo-globin value less than 11 grams. Multiple logistic regression techniques wereused to evaluate what demographic and behavioral variables were associatedwith anemia. We explored the treatment rate for anemia and whether treatmentreduced the odds of anemia at follow-up.Summary of Results: During the study period 580 patients received a12 month checkup. Anemia was diagnosed in 19.7% (114/580); (22.3%anemia rate for African-American, 13.6% for Whites, and 11.9% for His-panics). Compared to national WIC data there was no difference in theoverall anemia rate (19.7% vs 18.1% p=0.347). Duration of breastfeeding(OR=1.15 95% CI 1.04-1.26, p=0.005) significantly increase the odds ofanemia, while daycare attendance (OR=0.32, 95% CI 0.14-0.73, p=0.006)significantly decreased the odds of anemia. A vast majority (n=90, 78.3%)of anemic infants were treated, which significantly reduced the odds ofhaving anemia at follow-up (OR=0.45, 95% CI 0.16-0.78, p=0.041).
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
510 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Conclusions: Coupling a WIC office with nutritional counseling withinthe clinic site made no difference in anemia rates for our WIC patients com-pared to national values. Iron supplementation for infants of breastfeedingmothers who recieve WIC services is an improtant adjunct to prevent irondeficiency anemia.
484
DEVELOPING CULTURALLY APPROPRIATEINTERVENTIONS ADDRESSING CHILDHOOD OBESITYAMONG LOW INCOME AFRICAN AMERICAN FAMILIES
Jones VF1, Rowland M1, Young L2, Atwood K2, Thompson K2, Sterrett E1,Honaker S1, Williams J3. 1University of Louisville, Louisville, KY; 2PacificInstitute for Reseach and Evaluation, Louisville, KY and 3ClemsonUniversity, Clemson, SC.Purpose of Study: The purpose of the study was to understand the facil-itators and barriers that inner city African American (AA) children andtheir families face in engaging in exercise and healthy eating and how theirexperiences and opinions of community health experts could be used tocreate a successful, culturally adapted healthy lifestyle intervention forlow-income minority families.Methods Used: This qualitative study involved semi-structured focusgroup interviews with 8 AA children clinically identified as overweight orobese (BMI985) and 9 caregivers from an inner city, urban pediatric clinicto identify attitudes, perceptions and barriers towards achieving a healthylifestyle. An expert panel consisting of community stakeholders was alsoconvened to provide insights into possible culturally appropriate interventionstrategies.Summary of Results: Child and parent focus group analysis revealed13 themes (Healthy/Unhealthy Eating; Fast foods, Balancing family needs;Family rules and eating; Physical activity; Indoor activity; Sleep/obesity;Causes of childhood obesity; Parent’s struggle with weight; Desperate forhelp; Bullying; Parents’ intervention ideas; Parents distrust of technology andoutreach) and expert panel analysis revealed three themes (Key healthymessaging; Physical activity; Intervention suggestions).Conclusions: Our data suggest there are numerous options and venuesto consider when designing an intervention program. A key element shouldinclude parenting classes that provide more concise messaging about nutri-tion, meal planning and active play. An intervention needs to have a strongcounseling program to help families who are dealing with major psycho-logical stresses that made healthy eating and healthy lifestyles receive lowpriority. Since many of the families seemed to lack a structured home envi-ronment with children often guiding food selections and bedtimes, counselingfocused on effective parenting and family structure should be incorporated inan intervention.
485
A TEACHING KITCHEN BASED MODEL OF NUTRITIONEDUCATION: THE MISSING COMPONENT IN IMPROVINGMEDICAL STUDENT NUTRITIONAL COUNSELINGCOMPETENCY?
Abushamat L, Kay D, Leong B, Monlezun D, Harlan T. Tulane Institutefor Culinary Medicine, Tulane University, New Orleans, LA.Purpose of Study: A study by Spencer et al. (2006) surveyed 16 medi-cal schools across the US about medical students’ perceived importance ofnutritional counseling and personal dietary habits. The study suggested thatstudents were not adequately trained to provide nutritional counseling inreal patient encounters. In response to such findings, Tulane UniversitySchool of Medicine (TUSOM) founded the Tulane Center for CulinaryMedicine, which offers a medical student culinary nutrition elective as wellas community cooking classes facilitated by medical students. The electiveteaches students cooking skills and the basics of building a well-balancedrecipe. The goal is to not only promote healthy habits in the community,but to give medical students the skills and knowledge base to effectivelycounsel future patients. This study aims to create a baseline from which wecan assess the efficacy of a teaching kitchen based model of education.Methods Used: A survey was sent to TUSOM students to assess perceivedimportance of nutritional counseling, perceived competency in providingsuch counseling, and students’ dietary habits. Mean perceived competency
was calculated based on students’ perceived ability to counsel patients onthe metabolic role of carbohydrates, proteins, and fats; the role of cholesteroland saturated fat in increasing lipids; and recommended dietary patterns forobesity and type 2 diabetes. The means for each medical school year werecompared.Summary of Results: Results show that proficiency significantly in-creases from first to second year (p=0.02) and from second to third year(p=0.0001), but not significantly from third to fourth year (p=0.48). Thesefindings suggest that while classroom learning and patient experience im-prove competency, students’ perceived competency level peaks at ‘‘somewhatcompetent.’’Conclusions: An additional component to nutritional education shouldbe added to the medical school curriculum. We hope to observe whetherthe center’s goal of increasing student self-efficacy in cooking skills and inmaking healthy dietary choices will translate to increased perceived com-petency in advising patients about eating habits.
486
AN EVALUATION OF COMPLEMENTARY ANDALTERNATIVE (CAM) THERAPIES FOR ASTHMA ONTHE INTERNET
Patel A, Tharpe C, Marshall G. University of MIssissippi Medical Center,Jackson, MS.Purpose of Study: Many websites promote CAM therapies for asthmaand our goal is to investigate these websites and create awareness amongsthealth care providers regarding what exactly is being promoted and whatclaims are being made.Methods Used: We searched Google using 5 different search criteria thatwould possibly be used by lay people (i.e. our patients) to investigate whatthey are finding out about CAM therapies and asthma.Summary of Results: Our studies demonstrate that out of the hundredsof dietary supplements and folk remedies we observed, garlic, ginger, honey,licorice and mullein were the most frequent CAM therapies recommendedfor asthma. The overwhelming majority of sites made claims about the speci-fic CAM therapies they promoted and a substantial number of the claimsstated that the therapies will cure or eliminate asthma.Conclusions: There is a myriad amount of medical information aboutasthma on the internet and well-documented use of CAM therapies forasthma. Knowledge about these therapies would help influence individualtreatment plans and help the health care provider monitor for adverse effects,drug interactions and exacerbations of co-morbid conditions. Thus, it is pru-dent to be aware of this information as it can have a major impact on asthmatreatment plan and the overall well-being of the patient.
487
A REVIEW OF HERBAL AND DIETARY SUPPLEMENTSIN CKD AND ESRD ON THE INTERNET
Vamenta-Morris H, Glisson J, Dreisbach A, Shoemaker-Moyle M. Universityof Mississippi, Jackson, MS.Purpose of Study: The use of complementary and alternative medicine(CAM) has risen in the last decade in the United States. Herbs and otherplant derivatives are some of the most commonly consumed in the UnitedStates. This study aims to systematically identify and evaluate herbal anddietary supplement recommendations on CKD and ESRD on the internet.Methods Used: Search results were generated using common lay termsrelated to kidney disease. Eight search terms were used on Google andBing. The top 150 websites and advertisements were logged, and irrelevantsites were discarded. Irrelevant sites included products that do not pertainto CKD or ESRD, products that are recommended for animal use, and pagesthat are defunct. Of the pertinent 184 sites, data regarding each site wererecorded into a questionnaire that was formulated to assess key areas of inter-est. Two independent reviewers evaluated the final websites, one of whomevaluated only the Google sites, which constituted about two-thirds of thedata. The final data was a composition of the two independent reviewers’findings. Any differences in answers were resolved by giving defaulting tothe answer deemed most favorable to the website. Two different statisticalanalyses were performed on both the combined data and the data plus theremaining Bing sites.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 511
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: We found no significant difference between thetwo different analyses. About 30% of the sites are commercial and 70%informational. For the site location 35% had unknown location, whereas44% and 21% were from USA and outside USA, respectively. Only 6% usedthe standard NKF definition for CKD. 28% claimed to decrease the pro-gression of CKD. 60% did not advise to consult a doctor before takingthe supplement. Over 90% had no mention of potential drug interaction,no mention of potential disease interaction, or any caution against useduring pregnancy or in children.Conclusions: The internet is a ubiquitous source of information as wellas a market for herbal and dietary supplements. With the increase in dietaryand herbal supplement use in the CKD/ESRD population, healthcare provi-ders need to be more informed of the most common supplements used.More importantly we need to be more cognizant of how information is pre-sented in these websites and the psychological impact it has on patients.
Perinatal Medicine IIConcurrent Session
1:00 PMSaturday, February 23, 2013
488
FACTORS AFFECTING NEURODEVELOPMENTALOUTCOMES IN PRETERM INFANTS WITHINTRAPARENCHYMAL HEMORRHAGE
Tsai A, Evans PW, Kennedy KA. University of Texas Medical School atHouston, Houston, TX.Purpose of Study: Intraparenchymal hemorrhage is a serious complica-tion of premature birth and surviving infants are at a high risk for poorneurological outcomes such as cerebral palsy. The objective of this studyis to identify whether neuroimaging findings and selected perinatal andneonatal clinical and sociodemographic factors are predictive of neurode-velopmental outcomes at 18-22 months age.Methods Used: This an observational study of preterm infants born be-tween 1998-2008 who had an intraparenchymal hemorrhage identified inthe first 42 days after birth. Cranial ultrasound scans were reviewed forhemorrhage location, ventriculomegaly and other abnormalities. Selectedperinatal, neonatal, and sociodemographic factors were extracted from anexisting database. Surviving infants were seen for neurodevelopmental test-ing at 18-22 months corrected age. The primary outcome was cerebral palsyand secondary outcomes included vision impairment, deafness, seizures, grossmotor function and cognitive development.Summary of Results: 1168 preterm infants were included in the birthcohort. 141 of those infants had an intraparenchymal hemorrhage identi-fied. Mortality was 60%. 48 infants (mean GA 25 weeks and BW 726 g)were seen in follow up. The majority of infants had parietal lobe hemorrhagesand 13% had extensive hemorrhages involving 3 lobes. 54% of the infantsseen in follow up had cerebral palsy, 40% had vision impairment and 8%had hearing impairment. From the univariate analysis, there was a signifi-cant association between ventriculomegaly (identified on any image before42 days of age) and the development of cerebral palsy. Ventricular shuntplacement was significantly associated with cerebral palsy after adjusting forventriculomegaly with 73% having moderate to severe motor impairment.Preliminary analysis showed no association between hemorrhage location andcerebral palsy. Further analysis of contribution of late imaging findings andclinical/social factors to neurodevelopmental outcomes is in progress.Conclusions: If our study is successful, the ability to better predict neuro-developmental outcomes in preterm infants surviving with an intraparenchy-mal hemorrhage would provide important prognostic information for parentsand caregivers.
489
THE EFFECTS OF PROLONGED HYPERCAPNIA ONCEREBROVASCULAR REACTIVITY IN NEWBORN PIGS
Chilakala SK1, Pourcyrous M1, Parfenova H2, Leffler C2. 1UTHSC,Memphis, TN and 2UTHSC, Memphis, TN.
Purpose of Study: Permissive hypercapnia means accepting higherPaCO2. This is an acceptable practice in order to minimize the ventilator-associated lung injury i. It is not clear whether hypercapnia related cerebro-vasodilation will remain intact during prolonged hypercapnia and whethercerebral vessels respond appropriately to vasodilator and vasoconstrictor stim-uli during prolonged hypercapnia.Methods Used: Newborn piglets were anesthetized with ketamine andxylazine. Anesthesia was maintained using -chloralose. Piglets were intubatedand ventilated. A closed cranial window was implanted over the left parietalcortex. Pial arteriolar diameters were measured with a stereo-microscope witha video micrometer. CVR was evaluated during normocapnia and prolongedhypercapnia .Endothelin which causes cerebrovasodilation at 10-10M andvasoconstriction at 10-8M and U46619 which causes vasodilation at 10-8Mand vasoconstriction at 10-6M were used to assess the cerebrovascular re-activity during normocapnia and hypercapnia. Each reagent was administeredfor 5 min periods and reactivity in small and large pial arterioles was mea-sured. Artificial CSF was used to irrigate under the cranial window in be-tween the application of reagents to allow return of diameters to the baseline.CVR was measured both under normocapnia and under hypercapnia. Duringhypercapnia, CVR to topical reagents were measured at 30, 60 and at 120minutes. Blood gases were monitoredSummary of Results: Cerebrovasodilatory responses to Hypercapniathat was reached within minutes, sustained during the 120 mins of Hyper-capnia in both small and the large arterioles . Also, vasodilatory responsesto Endothelin 10-10M (17T5%) and U46619 10-8M (15T2%), and vaso-constrictor responses to Endothelin 10-8M (17T4%) and U46619 10-6M(28T5%) were preserved during prolonged Hypercapnia and similar tonormocapnia.Conclusions: Surprisingly and in contrast to the initial hypothesis 1) Cere-brovasodilatory responses to hypercapnia were maintained during prolongedhypercapnia and 2) CVR in terms of dilation and constriction was also pre-served during the entire 120 min of hypercapnia. These data suggest that pro-longed hypercapnia may not alter CVR.
490
THE INCIDENCE AND IMPACT OF CMV INFECTION INPRETERM INFANTS
Turner KM1, Lee HC2, Boppana SB1, Carlo WA1, Randolph DA1.1University of Alabama, Birmingham, Birmingham, AL and 2University ofCalifornia, San Francisco, CA.Purpose of Study: Congenital cytomegalovirus (CMV) is the leadingcause of non-genetic deafness in children in the U.S. and can cause of neuro-developmental impairment (NDI) in term infants. Limited data exist regard-ing whether congenital CMV is associated with preterm delivery. The extentto which CMV infection increases the risk of adverse outcomes in very lowbirth weight (VLBW) preterm infants is also unknown. We aimed to deter-mine the incidence of congenital CMV in VLBW infants, and to describeand role of congenital and acquired CMV in modifying outcomes of VLBWpreterm infants.Methods Used: This was a retrospective case controlled study of infantsadmitted to the UAB nursery where CMV screening is part of routine admis-sion orders. All infants admitted between the years 1993-2008 and weighingG1500 grams were included. CMV status and clinical outcomes were queriedusing two internal patient databases and hospital-based medical records. Forclinical outcomes analysis, the 5 consecutive VLBW infants born before andafter each CMV-positive case were used as controls. The primary outcomewas death or NDI. Secondary outcomes included sensorineural hearing loss,intraventricular hemorrhage, periventricular leukomalacia, bronchopulmonarydysplasia, necrotizing enterocolitis, retinopathy of prematurity, and cultureproven late-onset sepsis. Multivariate analysis was performed.Summary of Results: Seventeen of 4,594 VLBW infants queried hadcongenital CMV (0.37%), a lower rate than that published for term infants.An additional 16 infants (0.35%) acquired CMV in the nursery. Com-pared to controls, congenitally infected VLBW infants were more likely tohave hearing loss (64% vs. 10%, pG0.0001) and abnormal neuroimaging(71% vs. 28%, pG0.0001). Developmental motor outcomes were also sig-nificantly worse for CMV infected infants (50% vs. 12%, p=0.03), althoughthis information was available for only 6 congenital CMV infants and33 controls. Congenital CMV was not associated with death. Acquired CMVwas only associated with gastrointestinal perforation (p=0.008).
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
512 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Conclusions: CMV infection is not positively associated with prematurity.Congenital but not acquired CMV in VLBW infants is associated withhearing loss and neurologic deficits.
491
GLUCOSE METABOLISM IN PREMATURITY: EVIDENCEOF HEPATIC INSULIN RESISTANCE AND MOLECULARDEVELOPMENTAL DIFFERENCES IN NON-HUMANPRIMATES
McGill-Vargas L, Johnson M, Seidner S, Mccurnin D, DeFronzo R, BlancoC. UTHSCSA, San Antonio, TX.Purpose of Study: Abnormal glucose control is prevalent in preterminfants. In particular, persistent endogenous glucose production (EGP) hasbeen documented despite hyperglycemic conditions. The goal of this projectis to examine developmental differences in hepatic insulin sensitivity andgluconeogenic pathways in fetal/newborn baboons.Methods Used: Eighteen fetal baboons were delivered at 125 day (d)gestational age (GA), 140dGA and 175dGA (term=185dGA) via c-sectionand were sacrificed immediately after birth. Fifteen baboons were deliv-ered at 125dGA or at term; animals were sedated, electively intubated, andchronically ventilated if preterm. A hyperinsulinemic euglycemic clampalong with 3H3 glucose to quantify EGP were performed at day of life(DOL) 5 and 14. Plasma insulin, glucagon, catecholamines, and alanine werecorrelated with EGP. Protein content and gene expression of key gluconeo-genic and insulin signaling molecules were measured: phosphoenolpyruvatecarboxykinase-cytoplasmic (PEPCK-1), PEPCK-2 (mitochondrial), glucose-6-phosphatase-alpha (G6Pase->), G6Pase-A, fructose-1,6-bisphosphatase, in-sulin receptor substrate-1 (IRS-1), and transcription factor forkhead box-01(FOXO1). Statistical Calculations were performed utilizing SPSS 17.0.Summary of Results: Preterm baboons had abnormally suppressed EGPwhen compared to term animals (7.3T6.6 vs. 100.0 EGP percent suppression,pG0.01) under maximal insulin stimulated conditions (plasma insulin, mean1,049T421 KIU/L), whereas term animals had normal responses at DOL 5and 14. Abnormal EGP responses did not improve with postnatal age inpreterm baboons. In fetal baboons, the protein content of PEPCK-1 and 2increased as gestational age increased (2.5 fold and 9.6 fold increase from125dGA to 175dGA respectively, pG0.001). In contrast, G6Pase-> tran-siently decreased at 140dGA (pG0.01). FOXO1 tended to be higher at125dGA when compared to 175dGA (p=0.1). No significant differenceswere seen in other gluconeogenic or insulin molecules.Conclusions: Preterm baboons have hepatic insulin resistance demon-strated by the abnormal suppression of EGP which places them at high riskfor hyperglycemia; these abnormalities are accompanied by gestational dif-ferences in hepatic gluconeogenic molecules.
492
INSULIN LIKE GROWTH FACTOR- I FAILS TO PROTECTAGAINST DEXAMETHASONE-INDUCEDNEURODEGENERATION IN NEONATAL RATS
Bhatt AJ, Feng Y. University of Mississippi Medical Center, Jackson, MS.Purpose of Study: Routine use of dexamethasone (Dex) for the preventionor treatment of chronic lung disease of premature infants is not recommendedbecause of its neurotoxicity. However, the use of steroids is still prevalent inthis population. Previously we showed that Dex via glucocorticoid receptordecreased insulin-like growth factor-I (IGF-I) and caused neurodegenerationin the neonatal rat brain. IGF-I is neuroprotective against hypoxic-ischemicbrain injury in newborn rats. The purpose of this study was to determinewhether treatment with exogenous IGF-I can protect against Dex-inducedneurodegeneration in the developing rat brain.Methods Used: Pups in each litter were randomly divided into the vehicleor Dex-treated groups. To induce neurodegeneration, rat pups received oneof the two different regimens of i.p. Dex, which included tapering doses(DexTD) on postnatal day (PD) 3 to 6 (0.5, 0.25, 0.125 and 0.06 mg/kg,respectively), or repeated doses (DexRD) of 0.5 mg/kg/day on PD 4 to 6.Animals in the corresponding vehicle groups received equivalent volumesof saline. To evaluate the effect of IGF-I, in the first experiment rat pupsreceived 50 Kg of recombinant human insulin-like growth factor-1 (rhIGF-1)by intranasal (iN) administration at 2 h following each dose of Dex in
the DexTD group. In the second experiment rat pups received 0.5 Kg ofrhIGF-1 via intracerebral ventricular (i.c.v.) route at 30 min following thefirst Dex dose in the DexRD group. The neurodegeneration was evaluatedby measurement of brain weight and caspase-3 activity at 24 h after thelast dose of Dex.Summary of Results: The results showed that rhIGF-1 administered viaiN was successfully delivered into the brain. Treatment with DexTD orDexRD significantly decreased the gain of body weight and brain weightand increased caspase-3 activity. DexTD also decreased phosphorylationof protein kinase B (p-Akt). Neither iN nor i.c.v. administration of rhIGF-1prevented the Dex-induced decrease in body and brain weight gain or thedecreased expression pAkt. Nor did they prevent the Dex-induced increasein the caspase-3 activity in the brain.Conclusions: Our results suggest that exogenous IGF-I has no protectiveeffects against Dex-induced neurodegeneration in the newborn rat brain.
493
PERIPHERAL INSULIN RESISTANCE AND IMPAIREDINSULIN SIGNALING CONTRIBUTE TO HYPERGLYCEMIAOF PREMATURITY
Sorrell MW, McGill-Vargas L, Anzueto D, Seidner S, McCurnin D, Musi N,Blanco C. UTHSCSA, San Antonio, TX.Purpose of Study: Hyperglycemia is highly prevalent in premature infantsand has been associated to increased morbidity and mortality. Baboons de-velop hyperglycemia when born prematurely and have 97% phylogeneticproximity with humans. The objective of the study is to examine maturationaldifferences in peripheral insulin sensitivity and insulin signaling pathwaysthroughout the early postnatal period.Methods Used: Fifteen baboons were delivered via c-section at 125days(d) gestational age (GA) or at term (185dGA). Animals were sedated andintubated for experiments but remained chronically ventilated if born pre-maturely. To investigate if insulin signaling and insulin sensitivity is im-paired in premature baboons, the euglycemic hyperinsulinemic clamp wasperformed on day of life (DOL) 5 and 14. Key insulin signaling proteincontent and gene expression were measured in skeletal muscle during basaland insulin stimulated conditions: insulin receptor (IR) and IR substrate 1(IRS-1), p85 subunit, Akt and glucose transporters (GLUT1 and GLUT4).Insulin sensitivity was calculated from the glucose infusion rate (mg/kg/min)and expressed as an M value. Statistical calculations were performed utilizingSPSS 17.0Summary of Results: Preterm baboons had reduced peripheral insulinsensitivity when compared to their term counterparts on DOL 5 (M value11.7T0.4 vs. 20.3T0.7, pG0.001) and DOL 14 (M value 11.6T0.7 vs.21.0T0.3, pG0.001); insulin sensitivity did not improve with postnatal age.Tyrosine phosphorylation of Akt increased after insulin stimulation in pre-term and term baboons (pG0.01); however, the response of Akt to insulinfrom baseline levels was significantly lower in preterm baboons (3.7 fold vs.13.5 protein fold increase in preterms vs. term, pG0.05). Preterm baboons hadreduced GLUT1 protein content on DOL 5 (12% of term newborns, pG0.05)and trended to remain low at DOL 14 (8% of term at DOL 14, p=0.09); nodifferences were identified in other insulin signaling molecules.Conclusions: Preterm baboons have decreased peripheral insulin sensitivityand impaired insulin signaling in skeletal muscle when compared to termcounterparts. Such weak responses to insulin and persistent impairments ininsulin signaling early in postnatal life may place preterm infants at high riskof developing hyperglycemia.
494
ANTENATAL CORTICOSTEROID EXPOSURE MODIFIESINSULIN SIGNALING IN PERIPHERAL TISSUES
Anzueto D1, Johnson M1, McGill-Vargas L1, Musi N2, Blanco C1.1UTHSCSA, San Antonio, TX and 2UTHSCSA, San Antonio, TX.Purpose of Study: Antenatal glucocorticoids (aGC) are extensively usedto accelerate lung maturation in premature neonates. Young adults bornpreterm, and exposed to aGC, have altered glucose metabolism. Skeletalmuscle is the main site for insulin-stimulated glucose disposal. We hadpreviously demonstrated up-regulation of Akt and IR-A (key molecules forgrowth and insulin signaling) along with down-regulation of GLUT1/GLUT4
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 513
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

(glucose transport) in skeletal muscle of baboons delivered prematurely. Thegoal of this study is to examine the effect of exposure to aGC on key insulinsignaling molecules in preterm and term fetal baboons.Methods Used: Twenty fetal baboons were delivered via c-section fromhealthy, non-diabetic mothers. Baboons were euthanized immediately afterbirth at 125 days (d) gestation (GA)(0.67GA) or near term (175dGA=0.95GA). Half of the pregnant mothers received no intervention (n=5 per gesta-tional group) and were utilized as controls (CTR) and ten received two in-tramuscular betamethasone doses at a 24 hour interval (170 Kg.kg-1) priorto delivery (n=5 per gestational group). Vastus lateralis muscle was obtainedto measure protein content and gene expression of: insulin receptor (IR)-A,pIR-A, IR substate-1 (IRS-1), subunit of PI3-kinase (p85), Akt, pAkt, Akt-1,Akt-2 and glucose transporters (GLUT1 and GLUT4). ANOVAwas utilizedto assess significance with SPSS 17.0.Summary of Results: Muscle from 125dGA baboons exposed to aGC hadmarkedly reduced protein content of IR-A, Akt and Akt-1 in the skeletalmuscle (15%, 26% and 28% of 125dGA CTR, pG0.001); GLUT 1 andGLUT4 had a tendency to increase with aGC exposure in preterm animalsbut did not reach statistical significance. Affected insulin signaling molec-ules seem to be modified towards enhanced maturation. In contrast, no dif-ferences were found in insulin signaling molecules between animals born atterm regardless of aGC exposure.Conclusions: Exposure to a single course of aGC during fetal life modi-fies the insulin signaling pathway in the muscle of fetal baboons, specificallywhen exposure occurs earlier in gestation. These perturbations may contributeto short and long lasting abnormalities in glucose metabolism.
495
IMMUNODYSREGULATION, POLYENDOCRINOPATHY,ENTEROPATHY X-LINKED SYNDROME IN A NEONATEWITH A NOVEL FOXP3 MUTATION
Smith E1, Philips J1, Dimmitt R1, Atkinson P1, Goldman F1, Torgerson T3,Greeley S2. 1UAB, Birmingham, AL; 2University of Chicago, Chicago, ILand 3Seattle Children’s Research Institute, Seattle, WA.Case Report: A 37-week SGA (1.8 kg) male infant was referred to ourcenter at 3 weeks of age with poor weight gain, hyperglycemia requiringinsulin, rash, and profuse diarrhea. Labs showed a non anion gap metabolicacidosis, eosinophilia, and low insulin levels. The diarrhea improved withcessation of feeds initially but later changed to a secretory diarrhea. He wasplaced on different formulas (high MCT oil content, carbohydrate free)without sustained improvement in stool output. At 5 weeks of age, biopsyfrom an upper endoscopy showed villous atrophy, increased cellularity in thelamina propria, and inflammation consistent with autoimmune enteropathy.Shortly thereafter, he developed thrombocytopenia and had a Coombs +hemolytic anemia. Due to the clinical findings of autoimmunity, Immuno-dysregulation, Polyendocrinopathy, Enteropathy X-linked (IPEX) syndromewas considered. Sequencing of the FOXP3 gene revealed a novel mutationresulting in an in-frame 9bp deletion near other known causative mutations.Protein expression, assessed by flow cytometry, demonstrated reducedFOXP3 expression in T regulatory cells (CD4+ CD25+). The patient wasstarted on immune suppression therapy with cyclosporine A and within oneweek had marked improvement in his diarrhea and cytopenias. IPEX is arare condition with a variable clinical phenotype, likely related to the specificmutation and degree of FOXP3 protein expression and/or function. FOXP3is a transcription factor whose expression is primarily confined to a subsetof T cells (T regs) whose function is to regulate immune responses. Whileimmunosuppressive therapy can alleviate symptoms, hematopoietic stem celltransplantation remains the only known cure for severe IPEX. In summary, wereport a novel FOXP3 mutation causing IPEX, which should be consideredin the differential diagnosis of any male with early onset diabetes and otherautoimmune manifestations. Recognition of such clinical features allows forearly genetic diagnosis to guide prognosis and treatment.
496
THE EFFECTS OF PERINATAL OXYCODONE EXPOSUREON THE HYPOTHALAMIC-PITUITARY-ADRENAL (HPA)AXIS AND LIMBIC SYSTEM
Sithisarn T1, Legan S2, Bada H1, Wilson M2. 1University of Kentucky,Lexington, KY and 2University of Kentucky, Lexington, KY.
Purpose of Study: The use of Prescription opiate pain killers such as oxy-codone (OXY) is more prevalent in the past five years. We have previouslydescribed changes in HPA axis: increased plasma adrenocorticotropic hor-mone (ACTH) in response to acute stress in OXYoffspring without changesin corticosterone response. Limbic and higher cortical structures have majorroles regulating HPA axis functions. Thus we further study the limbic andhigher cortical structures to identify the mechanisms by which the pituitaryresponse to stress was enhanced.
We aimed to study the effects of perinatal OXY exposure in the HPAaxis circuitry. We hypothesized that perinatal OXYexposure may alter geneexpressions of the cortocotropin releasing neurons (CRH), estrogen receptorbeta (ERB), estrogen receptor alpha (ERA), glucocorticoid receptor (GR),mineralocorticoid receptor (MR) at the paraventricular nuclei (PVN) of hypo-thalamus or higher cortical centers and limbic structures that also control PVNfunction (prefrontal cortex (PFC), hippocampus (HPC) or central nucleus ofamygdala (CEA), which may result in increased HPA response.Methods Used: Pregnant dams were given either intravenous OXY(2 mg/kg/day) mg/kg/day) or vehicle daily from gestation day 8 until post-natal day 5. At adulthood brains were harvested and snapped frozen andtissues from those areas were punched out for quantitative polymerase chainreaction (QPCR) for CRH, ERB, ERA, GR, MR gene expression analysis.Summary of Results: In the PVN, OXY male but not female rats hadhigher MR gene expressions compare to controls (p=0.003). There is inter-action between gender within OXY group (p=0.002). In the CEA, OXYmales had increased while OXY female had decreased CRH gene expressions(p=0.002). In the CA3 area of HPC, OXY females had decreased MR geneexpression compared to control females (p=0.017); males had no changes. Thedecreased MR expression in CA3 may lead to impairment of the negativefeedback which in turn, leads to enhanced ACTH response to stress.Conclusions: Our results demonstrate that perinatal OXY is associatedwith changes in several gene expressions in the PVN and limbic system.Some changes may explain the enhanced pituitary response to stress. Thesechanges are gender specific.
497
BUGS BEHAVING BADLY: A CASE OFCOMMUNITY-ACQUIRED ENTEROBACTER CLOACAEEMPYEMA IN A NEONATE
Pryor J, Hathaway J, Bradley J, Macariola D. East Tennessee State University,Johnson City, TN.Case Report: 14-day-old previously healthy male infant was admittedwith respiratory distress & hypoxia. Two days earlier, he was observed inthe hospital briefly for RSV bronchiolitis & managed with supportive care.His chest x-ray demonstrated pneumonia with pleural effusion. Shortly afteradmission, he had several episodes of apnea & bradycardia. Full septicseptic work-up was initiated & he was empirically treated with ampicillin &cefotaxime. The infant developed increasing oxygen requirements and re-quired intubation. Laboratory tests repeatedly returned negative, includingTORCH titers & immunoglobulins. On his third hospital day, he developedright sided pneumothorax, requiring chest tube insertion. From his pleuralfluid cultures, methicillin-susceptible Staphylococcal aureus (MSSA) & Entero-bacter cloacae were isolated. Antibiotics were changed to vancomycin, genta-micin, & meropenem. Repeat pleural fluid cultures were positive for E. cloacaedespite several days of appropriate IV antibiotics. Due to lack of improvement& persistent positive pleural fluid cultures for E. cloacae, decortication wasperformed. Significant empyema with abscesses in the pleural cavity weredemonstrated intraoperatively, which were debrided & drained. Post decorti-cation, he was weaned from mechanical ventilation and had full recovery.
Enterobacter is a gram-negative aerobic bacillus that is a typical nosocomialpathogen transmissed via urine catheterization or respiratory equipment. It isalso known to be an opportunistic infection in immunocompromised or other-wise debilitated patients. In recent years E. cloacae has emerged as an importantnosocomial pathogen. It has been documented that the gastrointestinal tract inboth adults and neonates can be colonized by E. cloacae. E. cloacae may causepneumonia during the neonatal period usually as a nosocomial infection inneonates who have underlying medical conditions. Our case is unique in thesense that E. cloacae pneumonia with its severe complications had developedin a newborn without underlying immunodeficiency or chronic pulmonarycondition. Clinicians should therefore be aware that neonatal E. cloacae infec-tion might be acquired in the community as demonstrated in our case.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
514 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

498
IMPACT OF SPECIALIZED NURSERY CARE ON COST OFCARE OF LATE PRETERM INFANTS
Hunt LT1, Patel RM1, Rice D1, Anderson M2, Song C1. 1University ofOklahoma Health Sciences Center, Oklahoma City, OK and 2University ofOklahoma Health Sciences Center, Oklahoma City, OK.Purpose of Study: We hypothesize that late preterm infants with similarbaseline characteristics will be able to receive appropriate care at a loweroverall cost through specialized nursery care within a pre-existing Level Icouplet care unit, as compared to the Level IV NICU.Methods Used: This is a subgroup analysis of a retrospective cohortstudy that utilized chart review of infants delivered at 35 0/7 to 36 6/7 weeksgestation from April 1, 2010 to May 31, 2011. The specialized nurseryconsists of a four-bed monitored area, staffed by NICU nurses, where IVfluid/antibiotics, gavage feeds, phototherapy, and supplemental oxygen canbe provided. Two additional infants may receive the same nursing carefrom this unit while remaining physically in the mother’s room (off monitors).The combined detail cost of all hospital resources plus professional feesfor each patient was obtained by direct correspondence with hospital admin-istration and billing staff. Wilcoxon-Mann-Whitney testing was used to com-pare the median costs between groups.Summary of Results: We reviewed charts of 393 late preterm infants.221 met pre-defined inclusion criteria, including medical eligibility forspecialized nursery care at time of birth, without necessity for NICU ad-mission (ie G 35 weeks gestation or immediate critical care needs). We pre-viously demonstrated that median length of stay was 6 days in the NICUversus 3 days in the specialized nursery (p=0.0027). There were no deathsin either group. Of the 221 infants included, 89 were admitted to the NICUor specialized nursery (depending on census/staffing in the nursery andphysician discretion) and included in this analysis. Median total cost was$4246.76 for the 33 infants in the specialized nursery versus $9787.13(p=0.0160) for the 20 infants in the NICU during the same time period and$10780.85 (pG 0.0001) for all 56 infants admitted to the NICU at any time.Conclusions: Preliminary data shows that specialized nursery care sig-nificantly reduces total cost of care from roughly $10K per patient to $4kper patient, representing a 60% cost savings. Multivariable linear regressionanalysis is pending to control for potential confounding factors.
Renal, Electrolyte and Hypertension IIConcurrent Session
1:00 PMSaturday, February 23, 2013
499
THE >2-ADRENOCEPTOR AGONIST, DEXMEDETOMIDINE,ELICITS PRONOUNCED DECREASES IN ARTERIAL BLOODPRESSURE AND RENAL HEMODYNAMICS IN CYP1A1-REN2TRANSGENIC RATS WITH ANGIOTENSIN II-DEPENDENTMALIGNANT HYPERTENSION
Thorngren CK1, Patterson ME2, Davis PD1, Mitchell KD1. 1TulaneUniversity, New Orleans, LA and 2Ochsner Health System, New Orleans, LA.Purpose of Study: Previous studies have demonstrated that increasedsympathetic nervous system activity contributes to the pathogenesis of vari-ous forms of hypertension. However, the contribution of increased sympatheticnervous system activity to the elevated arterial blood pressure in transgenicrats [TGR(Cyp1a1Ren2)] with angiotensin (ANG) II-dependent malignanthypertension remains unclear. The present study was performed to determinethe effects of acute administration of the highly selective >2-adrenoceptoragonist, dexmedetomidine, on mean arterial blood pressure (MAP) and renalhemodynamics in Cyp1a1-Ren2 transgenic rats with ANG II-dependentmalignant hypertension.Methods Used: Male Cyp1a1-Ren2 rats (n=5) were induced to developmalignant hypertension by dietary administration of indole-3-carbinol (I3C,0.3% wt/wt) for 10 days. Mean arterial pressure (MAP) and renal hemody-namics were measured in pentobarbital-anesthetized male Cyp1a1-Ren2 ratsduring control conditions and during continuous infusion of dexmedetomidine(5 Kg/kg/min, iv).
Summary of Results: Dexmedetomidine administration decreased MAP inthe hypertensive rats (172T6 to 89T6 mmHg, PG0.001). The dexmedetomidine-induced decrease in MAP was associated with marked reductions in renalplasma flow (2.22T0.37 to 0.80T0.34 ml/min.g, PG0.05) and glomerular filtra-tion rate (0.70T0.07 to 0.23T0.09 ml/min.g, PG0.01).Conclusions: The present findings demonstrate that acute administrationof an >2-adrenoceptor agonist elicits pronounced decreases in MAP andrenal hemodynamic function in Cyp1a1-Ren2 transgenic rats with ANGII-dependent malignant hypertension. Thus, the data indicate that increasedsympathetic nervous system activity plays an important role in maintainingthe elevated MAP that occurs in ANG II-dependent malignant hypertension.
500
NOVEL MISSENSE MUTATION IN CELL CYCLE GENEFGS7 IS A CAUSE OF AUTOSOMAL DOMINANT FOCALSEGMENTAL GLOMERULSCLEROSIS
Hall G, Gbadegesin R, Homstad A, Wu G, Winn M. Duke University,Durham, NC.Purpose of Study: Focal segmental glomerulosclerosis (FSGS), a conditionthat is characterized by segmental scarring of the kidney, is a leading causeof kidney failure. Identification of genes causing familial FSGS has im-proved our understanding of the disease mechanisms and points to defects inthe glomerular epithelial cell, the podocyte, as a major factor in the patho-genesis of the disease.Methods Used: We identified a family with autosomal dominant FSGSwith nine affected individuals and carried out genome-wide linkage analysis(GWLA) using the Illumina Infinum II HumanLinkage-24 beadchip geno-typing assay. We performed whole-exome sequencing on the proband andconfirmed all identified novel variants by Sanger sequencing.Summary of Results: We identified a missense mutation R431C in FSGS7an F-actin binding cell cycle gene as a new cause of FSGS. The mutationsegregates with the disease in the family and we did not find the change in1600 control chromosomes. The change is conserved in evolution and it ispredicted to be deleterious by in-silico simulation. FSGS7 is upregulated inproliferating podocytes in kidney biopsies from individuals with collapsingFSGS. Knockdown of FSGS7 in zebrafish recapitulated the human pheno-type. Additionally, FSGS7 gene knockdown in a human immortalized podocytecell line resulted in reduced podocyte motility while overexpression of theFSGS7R431C mutant induced enhanced basal motility in cells.Conclusions: Collectively, these findings suggest that FSGS7 is impor-tant in maintaining the podocyte actin cytoskeleton and emphasizes theimportance of cell proliferation, cell migration and filopodia formation inthe pathogenesis of FSGS. Molecular dissection of the pathways by whichFSGS7 cause FSGS will provide insight into the mechanisms of podocyterenewal in health and disease.
501
INHIBITION OF THE RENIN-ANGIOTENSIN SYSTEMIMPROVES THE LONG-TERM GRAFT SURVIVAL OFSINGLE PEDIATRIC DONOR KIDNEYS TRANSPLANTEDIN ADULT RECIPIENTS
LaGuardia HA1, Khan E1, Kumbala D1, Mills K3, Paramesh A2, KillackeyM2, Slakey DP2, Simon E1, Zhang R1. 1Tulane University, New Orleans, LA;2Tulane University, New Orleans, LA and 3Tulane University School ofPublic Heath and Tropical Medicine, New Orleans, LA.Purpose of Study: Transplanting single pediatric donor kidneys intoadults has an increased risk of hyperfiltration injury and graft loss. Renin-angiotensin system (RAS) blockers are known to protect native kidneysfrom intraglomerular hypertension and hyperfiltration. It is unknown if theyare beneficial in pediatric donor kidney transplants.Methods Used: Retrospective analysis was performed on adults whoreceived single kidneys from pediatric donors G10 years old from 1996 to2009 at our center. The recipients were divided into group 1 with RASblockers (n=40) and group 2 without RAS blockers (n=54).Summary of Results: There was no significant difference in any donor/recipient demographic between the two groups. Graft function, as well as theincidences of delayed graft function, acute rejection and persistent protein-uria, was not statistically different in the two groups. Kaplan-Meier estimated
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 515
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

death-censored graft survivals were significantly better in group 1 than ingroup 2 over 7 years: 95 vs. 81.2%, 82.4 vs. 61.2%, 72.6 vs. 58.5%, and68.5 vs. 47.2% at 1, 3, 5, and 7 years, respectively (log rank p=0.043).Group 1 also had a trend for better patient survival than group 2: 100 vs.92.6%, 94.9 vs. 83.3%, 92.1 vs. 79.4%, and 86.6 vs. 75.4% at 1, 3, 5, and7 years, respectively (log rank p=0.107). Multivariable analysis found per-sistent proteinuria was a risk factor for graft loss (OR 2.70, 95% CI1.33-5.49, p=0.006), while RAS blockers reduced the risk of graft loss(OR 0.38, 95%CI 0.18-0.79, p=0.009).Conclusions: RAS blockade therapy is associated with superior long-termgraft survival among adults transplanted with single pediatric donor kidneys.
502
ANGIOTENSIN II STIMULATES RENIN SYNTHESIS ANDSECRETION VIA A PKC-MEDIATED CAMP STIMULATIONIN COLLECTING DUCT M-1 CELLS
Liu L1, Lara LS1,3, Gonzalez AA1,2, Bourgeois CR1, Seth DM1, PrietoMC1,2. 1Tulane University School of Medicine, New Orleans, LA; 2TulaneUniversity School of Medicine, New Orleans, LA and 3Universidade Federaldo Rio de Janeiro, Rio de Janeiro, Brazil.Purpose of Study: In angiotensin (Ang) II-dependent hypertension, Ang IIstimulates synthesis and secretion of prorenin and renin in the principal cellsof the collecting ducts (CD) via Ang II type 1 receptors. The mechanismsregulating CD renin were further elucidated using primary cultured rat innermedullary CD (IMCD) cells. Ang II treatment increases renin mRNA andprotein levels via Protein Kinase C (PKC) activation. In primary cultured ratIMCD cells and mouse renal CD cell line (mpkCCDc14), Ang II treatmentincreases intracellular cyclic AMP (cAMP) levels. However, it is unknown ifcAMP is responsible for the Ang II-mediated stimulation of renin synthesisand secretion by the CD cells. We hypothesized that Ang II stimulates reninsynthesis and secretion in the principal cells of CD via activation of PKCwhich subsequently results in stimulation of cAMP/PKA/CREB pathway.Methods Used: M-1 CD cell culture, Immunofluorescence, Quantitativereal-time RT-PCR, Western blot, Renin content in the culture media (RIA),Intracellular cAMP content (ELISA).Summary of Results: In M-1 cells, Ang II (100 nM) treatment increasedrenin mRNA and protein levels. Renin content measured in the cell culturemedia was augmented in Ang II-treated cells by 6 hrs (Ang II: 31T4 vs.19T4 ng Ang I/hr/ml; pG0.05). Ang II increased cAMP levels by 1 min(148T32 pmol/mg protein) and reached a peak at 30 min (290T27 vs.44T0 pmol/mg protein; pG0.05). The adenlyate cyclase activator, forskolin(100 pM) and the analogue of cAMP, dibutyryl-cAMP (100 uM) both sig-nificantly increased renin transcript. Augmentation of renin mRNA byAng II was prevented by PKA inhibition with H89 or PKI, and it wasfollowed by increased pCREB levels. Importantly, PKC inhibition eitherwith calphostin C (100 nM) or a PKC> dominant negative prevented theaugmentation of intracellular levels of cAMP, pCREB and renin mRNAin M-1 cells treated with Ang II.Conclusions: Ang II stimulates renin synthesis and secretion via a PKC>-mediated cAMP stimulation and PKA/CREB activation in mouse collectingduct cells.
503
DECREASED HEART RATE VARIABILITY IS ASSOCIATEDWITH INCREASED TRANSCRANIAL DOPPLERVELOCITIESIN CHILDREN WITH SICKLE CELL DISEASE
Jones JB1, Shatat IF3, Paulo RC2. 1Medical University of South Carolina,Charleston, SC; 2MUSC Children’s Hospital, Charleston, SC and 3MUSCChildren’s Hospital, Charleston, SC.Purpose of Study: Sickle cell disease (SCD) is an inflammatory conditionassociated with multiple comorbidities and affects multiple tissues includ-ing the cardiovascular endothelium. Abnormal transcranial Doppler velocities(TCDV) are associated with increased risk of stroke in children with sicklecell disease. Decreased heart rate variability has been associated with cardio-vascular disease in adult populations, but the relationship between heart ratevariability and risk of stroke in pediatric sickle cell populations has not yetbeen defined.
To explore the relationship between blood pressure variability (BPV),heart rate variability (HRV), and TCDV in a cohort of pediatric sickle cellpatients.Methods Used: This is a retrospective study of 11 children with SCD whopreviously underwent 24-h ABP monitoring and TCDV measurements.Medical records were reviewed for TCDV and 24-hour ABP data. TCDV inthe right and left middle cerebral artery (MCA) were examined, and thehighest velocity was recorded. HR and BP standard deviations were usedas markers of variability. The relationships between daytime, nighttime, and24-h BP and HR variability were examined.Summary of Results: Mean age, BMI and Hb levels were 11.2 T 3.0 years,18.7 T 3.4 kg/m2, and 9.1 T 1.7 g/dl, respectively. Median TCDV was136cm/s (125-142). Decreased day, night, and 24-h HR variability weresignificantly associated with increased TCDV (R=-0.69, p=0.02; R=-0.82p=0.002; R=-0.66, p=0.03, respectively). BP variability did not correlatewith TCDV. Nighttime BP indexes were higher than daytime.Conclusions: Decreased HRV is associated with increased TCD velocitiesin children with SCD. No correlation between measurements of BP vari-ability and TCDV was found. This study provides new information on HRand BP variability and TCDV; a surrogate marker of stroke risk in SCD.Larger multicenter studies are needed to confirm our findings.
504
URINARY ANGIOTENSINOGEN: A PROGNOSTICBIOMARKER OF ACUTE KIDNEY INJURY
Alge J1, Karakala N1, Neely B1, Janech M1,2, Arthur J1,2. 1MedicalUniversity of South Carolina, Charleston, SC and 2Ralph H Johnson VAMC,Charleston, SC.Purpose of Study: We previously identified angiotensinogen as a prog-nostic biomarker of AKI after cardiac surgery. Our objective was to qualifyangiotensinogen as an AKI biomarker and test the hypothesis that it pre-dicts outcomes in the setting of AKI due to other causes.Methods Used: Liquid chromatography tandem mass spectrometry wasused to compare the relative abundance of proteins in the urine of post-cardiac surgery patients who developed severe post-op AKI to those whodid not (n=8). Samples were collected at a mean of 9 hrs post-op. Serumcreatinine (sCr) was not elevated in two AKI patients at collection. The urineof rats (n=6) and mice (n=10) with AKI induced by glycerol injectionor renal ischemia-reperfusion injury, respectively, was compared to that ofcontrols. Mean fold change and the Wilcoxon Rank-Sum test were used toselect differentially abundant proteins. Urine angiotensinogen was mea-sured by ELISA in samples obtained from ICU patients with AKI (n=45).The area under the ROC curve (AUC) was used to evaluate the ability ofurine creatinine-corrected angiotensinogen to predict adverse outcomes.Summary of Results: Urine angiotensinogen discriminated betweenthe experimental groups in each proteomics study (Table 1). The urineangiotensinogen-to-creatinine ratio (uAnCR) was lower in patients withpre-renal AKI compared to AKI of other etiologies (median 11.3 and80.2 ng/ mg; p=0.02). uAnCR was elevated in the group of patients whomet the composite outcome need for renal replacement therapy or death(median 89.4 vs 29.4 ng/mg; p=0.02) and predicted this outcome(AUC=0.73). uAnCR also predicted worsening of AKI (defined as an ad-ditional increase in sCr 90.3 mg/dL after the time of samples collection;AUC=0.74) and discharge 97 days or death (AUC=0.77).Conclusions: Angiotensinogen could be used to identify ICU patients atincreased risk of adverse outcomes related to AKI.
TABLE 1. Proteomics Data
Study Mean Fold Change p-value Direction of Change
AKI vs No AKI a N/A 0.43 Up
Rat AKI 10.5 0.1 Up
Mouse AKIa N/A 0.01 Up
RRT vs No RRT b 9.7 0.002 Up
aAngiotensinogen was undetectable in controls without AKI; bPreviously published datashown for comparison
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
516 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

505
LEVELS OF RENIN IN THE URINE ARE AUGMENTEDIN DIABETIC AND HYPERTENSIVE PATIENTS: ISURINARY RENIN (UREN) A POTENTIAL MARKER OFINTRARENAL ACTIVATION OF THE RENIN-ANGIOTENSINSYSTEM (RAS)?
Luffman C, Seth D, Thethi T, Prieto MC. Tulane University School ofMedicine, New Orleans, LA.Purpose of Study: Increased urinary excretion of angiotensinogen (AGT)has been associated with increased urinary angiotensin (Ang) II levels andsystolic blood pressure in Ang II-dependent hypertensive animal models(Kobori et al 2003; Liu et al 2011) and patients with diabetes and hyper-tension; thus it has been proposed as an indicator of inappropriate activa-tion of intrarenal RAS. Nonetheless, because the urinary excretion of AGTparallels with proteinuria, its use for these purposes still remains controver-sial. In the present study, we aimed to assess the excretion of renin in the urineof patients from a blind cross-sectional study on obesity currently ongoing atTulane University. Demographic characteristics of the patients used in thepresent study are shown in Table 1.Methods Used: Using a modified plasma renin activity protocol, excess ofexogenous renin substrate tetradecapeptide was added to saturate the enzymeand thus measure urinary renin content as ng Ang I/ml/hr. The assay was runin the absence and the presence of the human renin inhibitor Aliskiren\ tosubtract non-specific enzyme activity.Summary of Results: The urinary renin content was significantly higherin diabetics (n=82) compared with non-diabetics (87) patients (110.2 T3.57 vs. 24.4 T 13.4 ng AngI/ml/hr). In patients exhibiting hypertension(n=41; SBP 9140 mmHG and DBP990 mmHg) urinary renin content was93.9 T 17.4 ngAngI/ml/hr, while in non-hypertensive patients (n=128) thelevels were 46.3 T 5.1 ng AngI/ml/hr.Conclusions: Urinary levels of renin did not correlate with those of pro-teinuria. These data indicate that urinary renin levels could be used as apotential biomarker of intrarenal RAS activation in diabetic and hypertensivepatients.
506
URINE HAPTOGLOBIN TO CREATININE RATIO PREDICTSWORSENING RENAL FUNCTIONS IN PATIENTS WITHTYPE 2 DIABETES
Bhensdadia N1, Hunt K1, Lopes-Virella M1,2, Tucker M1, Neely B1, JanechM1,2, Arthur J1,2. 1Medical University of South Carolina, Charleston, SCand 2Ralph H Johnson VA Medical Center, Charleston, SC.Purpose of Study: Diabetic nephropathy is the leading cause of EndStage Renal Disease. Urine albumin to creatinine ratio (ACR) is commonlyused as predictor for the development and progression of diabetic nephrop-athy but it is neither sensitive nor specific. Discovery phase proteomic analy-sis in our lab identified urinary haptoglobin concentration as a candidatebiomarker that could predict progression of diabetic nephropathy.Methods Used: We analyzed 204 randomly selected diabetic patient’surine samples with eGFR Q 60 ml/min and ACR G 300 mg/g from VADT(VA Glycemic Control and Complications in Diabetes Mellitus Type 2 trial)group for urine haptoglobin concentration (ng/ml) and urine creatinineconcentration (mg/ml) to calculate urine haptoglobin to creatinine (ng/ng)ratio. Urine haptoglobin concentration was measured by ELISA and urinecreatinine concentration was measured by Jaffe’s reaction. Early renal func-tion decline (ERFD) was defined as a loss of Q 3.3% eGFR/year.Summary of Results: 204 patients divided in two groups. Group A - 153patients who didn’t have ERFD and group B - 51 patients who had ERFD.Log normalized geometric mean values of urine haptoglobin to creatinineratio (HCR) were different between groups (P=0.0079) after adjusting forVADT treatment and use of ACE Inhibitor. In separate models comparingthe highest to lowest tertile, the odds ratio for having ERFD was 2.70 (95%CI: 1.15, 6.32) for HCR and 2.50 (1.14, 5.48) for ACR. The integrateddiscrimination improvement (IDI) with addition of HCR to a model con-taining ACR was statistically improved demonstrating that haptoglobin im-proves the ability to predict ERFD. The addition of HCR to the ACR modelincreased the sensitivity for prediction of ERFD from 37.3% to 47.1%while specificity was unchanged at 78.4%.
Conclusions: HCR is a novel biomarker that can predict accelerated lossof renal functions in patients with type 2 diabetes. The predictive ability ofHCR appears equivalent to ACR in this study. Combining HCR with ACRincreases the predictive ability.
507
CIRCULATING 24,25(OH)2 D CONCENTRATIONS DURINGTREATMENT OF VITAMIN D DEFICIENCY
Alshayeb HM1,3, Showkat A3, Gyamlani G2, Quarles LD3, Wall BM2,3.1Hashemite University, Zarqa, Jordan; 2VAMC, Memphis, TN and 3UTHSC,Memphis, TN.Purpose of Study: We have previously reported resistance to correctionof vitamin D deficiency with cholecalciferol therapy in CKD patients, ascompared to subjects with normal kidney function (J Invest Med, 2012).Elevated FGF23 levels in CKD stimulate Cyp24a1 expression, suggestingthat Cyp24-mediated catabolism of 25(OH)D may contribute to this resis-tance. To test this possibility 24,25(OH)D2 levels were measured before andafter treatment of vitamin D deficiency with cholecalciferol.Methods Used: Prospective study of 28 patients with 25OHD levelG 20 ng/ml who received 10,000 IU/week of cholecalciferol for 8 weeks.CKD (n=14) were matched with non-CKD group (n=14) for age, sex ,race,and diabetes. Response to cholecalciferol was assessed by measuring thechanges in serum 25(OH)D and 24,25(OH)2D3 levels.Summary of Results: There were no significant differences betweenCKD and non-CKD patients in baseline concentrations of serum albumin,25(OH)D,1,25(OH)2D , 24,25(OH)2D3. Baseline intact PTH (PTH) andFGF-23 levels were higher in CKD patients. In a multivariable analysislow pre-treatment 24,25(OH)2D3 level was predicted by low 25(OH)D,high PTH and high FGF23 levels. Cholecalciferol treatment resulted inincreases in serum 25(OH)D (18.6 T 8 ng/ml vs 12.2 T 9, pG0.03),1,25(OH)2D (15.7 T 32.3 pg/ml vs 4.3 T 23.6, p=0.31), and 24,25(OH)2D3(1.14 T 0.89 ng/ml vs 1.02 T 0.74, p=0.73) in non-CKD and CKD, respec-tively. 24,25(OH)D2 levels were not higher in CKD, either before or aftercholecalciferol, despite higher FGF23. PTH levels decreased after treat-ment in CKD patients (-42T68 pg/ml, pG0.05), but not in non-CKD patients(-10T25, p=0.16). Cholecalciferol also resulted in an increase in serumFGF23 (81 T 35 pg/ml vs 125T 42, p=0.052) in non-CKD, but was unchangedin CKD. In a multivariable analysis, low post-treatment serum 24,25(OH)2D3level was predicted by low baseline serum 24,25(OH)2D3 (p= 0.09), low post-treatment 25(OH)D (pG0.03), and high baseline PTH (pG0.01).Conclusions: 24,25(OH)2D3 increases with cholecalciferol therapy in bothCKD and non-CKD subjects, consistent with substrate dependent production.Despite decreased nephron mass in CKD, there was a similar increment in24,25(OH)2D3 following cholecalciferol.
508
EFFECT OF ERGOCALCIFEROL ON ANEMIA ANDMINERAL METABOLISM MANAGEMENT INHEMODIALYSIS PATIENTS - A CASE CONTROL STUDY
Hirachan P, Penagaluru N, Williams K, Fanti P, Bansal S. UTHSCSA, SanAntonio, TX.Purpose of Study: Vitamin D deficiency is prevalent in chronic kidneydisease but literature on its supplementation is scarce. Following anecdotalreports of positive effects of Ergocalciferol (D2) supplementation on anemiaof renal disease, we conducted this study to evaluate the effect of D2 onerythropoietin (EPO) requirement and on mineral metabolism in hemodial-ysis (HD) patients.Methods Used: We reviewed the medical record for a 6-month periodin maintenance HD patients under our care. Patients with baseline serum25(OH)D level G35 ng/ml who did or did not receive D2 (47 cases vs.41 controls) were included in the study. Cases and controls were comparedbefore and after D2 supplementation for parameters of erythropoiesis, ironand mineral metabolism, and for monthly doses of erythropoietin, intrave-nous iron and paricalcitol.Summary of Results: Baseline characteristics were similar between the2 groups. After 6 months of D2 supplementation, the cases showed an in-crease in 25(OH)D level (from 17.15 T 8 ng/ml to 33.66 T 10.3 ng/ml ), 15%decrease in EPO use (from 35,451 T 26,192 to 29,960 T 22,395 IU/ month;
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 517
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

p=0.03) and 16% decrease in paricalcitol dose (from 26.15 T 17.4 to21.85 T 14.1 Kg/month; p=0.04). Serum calcium increased from 9.0 T 0.5to 9.4 T 0.7 mg/dl (pG0.001) with a non-significant down trend in iPTHlevel. Monthly hemoglobin, ferritin, iron saturation, albumin, and phospho-rus levels did not change during the same period. In contrast, the controlgroup displayed a decrease in 25(OH)D (from 19.4T7.9 to 15T8.8 ng/ml),65% increase in EPO dose (from 28.983T30,267 to 47,933T75,430 IU/month;ns), 23% decrease in paricalcitol dose (29.02T22.16 to 22.1T19.18 Kg/month;ns) and no change in hemoglobin and iPTH levels. Comparison between thetwo groups showed a non-significant difference in change of EPO require-ment following implementation of D2 supplementation.Conclusions: In summary, despite a significant 15% decrease in EPO dosein the cases and 65% increase in the controls, the change in EPO requirementwas not different between the two groups. The likely reason for which couldbe small sample size and short duration of follow up.The large sample sizestudy is required to identify significant pleiotropic effects of 25(OH)D in dial-ysis patients.
509
PREDICTORS OF CHRONIC KIDNEY DISEASEPROGRESSION IN PATIENTS WITH SICKLE CELL ANEMIA
Gosmanova E1, Zaidi S1, Adams-Graves P1, Wan J2. 1University ofTennessee HSC, Memphis, TN and 2University of Tennessee HSC,Memphis, TN.Purpose of Study: It has been shown that prevalence of macroalbumin-uria and reduced estimated glomerular filtration rate (eGFR) G90ml/min per1.73m2 in patients with sickle cell anemia (SCA) is 10-28% and 20-25%,respectively. However, little is known about risk factors for chronic kidneydisease (CKD) progression in these individuals. We evaluated changes ineGFR and macroalbuminuria in a cohort of patients with SCA followed for5 years at the Diggs-Kraus Sickle Cell Clinic, Memphis, TN.Methods Used: We studied 100 individuals with SCA [mean age 31.6T10.6years, 93% African-Americans, 43% males, 56% with Hemoglobin SSdisease and 44% with other sickling hemoglobinopathies, and 25% with hy-pertension]. The development of kidney dysfunction was defined as newmacroalbuminuria, new CKD (eGFR G90ml/min per 1.73m2), or worsening ofpreexisting CKD stage based on eGFR grades (stage 2: eGFR 60-89ml/min per1.73m2, stage 3: eGFR 30-59ml/min per 1.73m2, stage 4: eGFR15-29ml/minper 1.73m2, stage 5: eGFRG15ml/min per 1.73m2).Summary of Results: At baseline, 49% of patients had eGFR in hyper-filtration range (9130ml/min per 1.73m2 for females, 9140ml/min per1.73m2 for males), 13% of patients had eGFRG90ml/min per 1.73m2, and19% had macroalbuminuria. After a mean follow up of 5.0+0.9 years, 7%of patients developed new macroalbuminuria and 10% of patients developednew CKD or progression in CKD stage. Baseline eGFR was a strong pre-dictor of CKD development and progression in both univariate and multi-variate analysis (adjusted OR=2.58, p=0.006 for each 10ml/min per 1.73m2
decrease in eGFR). Additionally, baseline macroalbuminuria (adjustedOR=4.52, p=0.014) was associated with eGFR worsening. Higher baselinehemoglobin level was protective for CKD progression (adjusted OR=0.70,p=0.039 for every 1mg/dL increase in hemoglobin). Age, gender, presenceof hypertension, baseline systolic or diastolic blood pressure, type of hemo-globinopathy, and baseline total bilirubin concentration were not associatedwith CKD progression.Conclusions: In patients with SCA, baseline macroalbuminuria and lowereGFR were associated with significant risk of CKD development and pro-gression, while higher baseline hemoglobin level was protective.
SSGIM Research Abstract Session A
8:30 AMFriday, February 22, 2013
510
INTEGRATING LGBT CONTENT INTO MEDICALSCHOOL CURRICULA
Sequeira G1, Panunti B2, Chakraborti C1. 1Tulane, New Orleans, LA and2Ochsner Medical Center, New Orleans, LA.
Purpose of Study: The lesbian, gay, bisexual and transgender (LGBT)community is a diverse, underserved, and often stigmatized group that facesmany barriers to accessing quality healthcare. The Institute of Medicine(IOM) recognizes that few practicing physicians are knowledgeable aboutand sensitive to the needs of LGBT patients. A recent survey of medicalschool deans found that a median number of five hours was being spentcovering LGBT related content.Methods Used: Three optional, 1-hour sessions were provided to students.Sessions entitled ‘‘Intro to Transgender Health’’ and ‘‘Taking an LGBT In-clusive Sexual History’’ were conducted as components of the Tulane Schoolof Medicine LGBT Health Week. The final lecture entitled ‘‘HormoneTherapy for Transgender Patients’’ was presented during the EndocrinePharmacology unit of the second year curriculum. Students completed ret-rospective surveys following each session to assess the relevance of theLGBT content. The results of the surveys were analyzed thematically toidentify trends. In a separate mandatory session, students practiced advancedcommunication and interviewing skills in an encounter with a LBGT stan-dardized patient. Pre-session work oriented participants to taking an LGBTinclusive sexual history, and a post-encounter session was used to debrief stu-dents on the implications of making assumptions.Summary of Results: 44 surveys were collected from the LGBT Healthweek sessions and 30 surveys were collected from the pharmacology session.82% of the sexual history session respondents clearly articulated how toappropriately inquire about the gender of sexual partners and behaviors inan LGBT inclusive way. 87% of respondents stated that the content presentedwas ‘‘applicable to their work as a future physician’’ and ‘‘relevant enoughto be incorporated into the required medical school curriculum.’’Conclusions: Our results validated the assumption that this underrepre-sented content is meaningful and actively requested. While this primarilyqualitative study has some limitations, these sessions can serve as a resourcefor institutions working create robust LGBT curricula. The sessions incorpo-rate training in interpersonal skills and communication, medical knowledge,patient care and cultural competency, all of which are critical to student andphysician professional development.
511
AWEB-BASED CULTURAL COMPETENCY TRAINING FORMEDICAL STUDENTS: A RANDOMIZED TRIAL
Carpenter R1, Estrada C1, Medrano M2, Smith A1, Massie FS1. 1Universityof Alabama at Birmingham, Birmingham, AL and 2CommuniCare HealthCenters, San Antonio, TX.Purpose of Study: To examine the effects of two cultural competencytraining strategies on students’ attitudes.Methods Used: We randomized all 180 first-year medical students intoa web-based (intervention group) or a lecture-based (control group) culturalcompetency training. The primary outcome was the overall score on theHealth Belief Attitudes Survey (HBAS)(1=lowest, 6=highest). Secondaryoutcomes were HBAS sub-scores (identified using factor analysis andmapped to the Tool for Assessing Cultural Competency Training [TACCT]domains).Summary of Results: No differences were observed in the overallmedian scores between the intervention (median 5.2; 25th percentile [Q1]4.9, 75th percentile [Q3] 5.5) and the control groups (5.3, Q1 4.9, Q35.6)(p=0.77). We also did not observe differences between the two groupson any of the sub-scores (all p90.20).Conclusions: A web-based and a lecture-based cultural competency train-ing strategies were associated with equally high positive attitudes amongfirst-year medical students. TheHBAS itemsweremapped to TACCT domains,which suggests construct validation for the instrument. Our findings warrantfurther evaluation of low-engagement cultural competency interventions usinga validated tool for assessing attitudes.
512
EVALUATION OF AN ADVANCED PHYSICAL DIAGNOSISCOURSE USING NOMINAL GROUP TECHNIQUE
Coker J, Castiglioini A, Kraemer R, Massie FS, Morris J, Rodriguez M,Russell S, Shaneyfelt T, Willett L, Estrada C. University of Alabama atBirmingham, Birmingham, AL.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
518 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Purpose of Study: To explore whether a technique to study consumerpreferences - the nominal group technique (NGT) - would elicit prioritizedevaluation from senior medical students regarding an advanced physical diag-nosis course.Methods Used: Prospective. Students enrolled in an advanced physicaldiagnosis course. Responses at four NGT sessions (before, after); studentsweighted top three responses (top=3, middle=2, bottom=1).Summary of Results: 12 students generated 45 responses. Before thecourse, students identified 23 topics they expected to learn; the top 3 werereview sensitivity/specificity and high yield techniques (percent of totalweight, 18.5%), improving diagnosis (13.8%), and reinforce usual andless well known techniques (13.8%). After the course, students generated22 topics learned; the top 3 were: practice and reinforce advanced maneu-vers (25.4%), gaining confidence (22.5%), and learn the evidence (16.9%).We observed no differences in the priority of responses before and afterthe course (P=0.07, figure).Conclusions: The course appears to meet student expectations regardingeducation of the evidence based physical exam, building skills and confi-dence on the proper techniques and maneuvers, and experiential learning.
513
GAMIFICATION OF BOARD REVIEW: A CURRICULULMINNOVATION FOR INTERNAL MEDICINE RESIDENTS
Snyder ED, Hartig JR. University of Alabama at Birmingham, Birmingham, AL.Purpose of Study: Guiding residents in initial ABIM certification pre-paration, many residency programs sponsor ‘board review conferences’ uti-lizing question banks. Due to patient care, duty-hour restrictions or otherlimitations residents may be unable to attend. To meet this learner need, wedesigned an electronic, curriculum-integrated enhancement which empha-sized multiple adult learning principles and was constructed using popularconcepts of gamification.Methods Used: Weekly board review questions chosen to reinforce di-dactic activities were emailed to all internal medicine and combined house-staff. Participation was voluntary and names were only used by player choice.Weekly small prizes were awarded, to the first correct and to a randomly chosencorrect player.
Descriptive data on resident participation and responses were collected,player results were anonymized, and a survey on participant impressionswas administered.Summary of Results: Over 2 years, residents received 87 quizzes, eachwith 1-2 questions on a topic. Median number players per week was 40(range 17-65). There were 3208 total responses, with 2256 correct responsesgiven (70%). Out of approximately 181 residents contacted over 2 years,there were at least 169 (80%) different players (number of different anony-mous players could not be assessed). All training levels were represented
with 35% of players in post-graduate year (PGY) 1, 28% PGY 2, 27%PGY 3/4.PGY3/4 residents responded correctly 77% of the time, followed by PGY 2(71%) and PGY 1 (65%) residents.
Evaluation of the program was positive. 96% of responders to an evalu-ation survey reported just the right level of difficulty for questions. 67%were happy with the frequency of games; 30% requested more questions.Conclusions: An online board review series was well received by our in-ternal medicine residents. Participation may have been enhanced by creatinga game environment with a clear outcome (correct or incorrect responsewith designated winners) and a well-defined winning condition with a tokenprize. Such gamification of traditional teaching methods may be useful toenhance participation, and provide novel teaching platforms for GIM edu-cators as they seek to provide additional opportunities for resident educationin the setting of restricted duty hours.
514
SATISFYING INTERNAL MEDICINE COMPETENCIES INTHE AMBULATORY TEAM MEETING
Brownfield E. MUSC, Charleston, SC.Purpose of Study: Internal Medicine (IM) educators and policy makershave stressed the need to train physicians within highly functional ambulatorycare settings and to develop physicians to lead multidisciplinary teams in thecare of patients. Projects stemming from brief, weekly multidisciplinary teammeetings may address the ABIM residency competencies while developingresident skills as team leaders.Methods Used: The Medical University of South Carolina (MUSC) Uni-versity Internal Medicine (UIM) faculty physicians began weekly, 40 minutepatient care meetings. Regular attendees include IM resident physicians, UIMfaculty, social worker, nurse case managers, Certified Medical Assistants andPharm D’s. Using explicitly defined and effective team behaviors, the teamreviews previous solutions, works on outstanding projects, then discussesa new patient case. The presentation of each case is followed by a groupdiscussion of the impediments to effective care followed by a listing of pos-sible solutions then the selection of one project which can ideally be im-plemented over the following week. The majority of team communicationduring the week is accomplished via personal conversations during theworkday and e-mail.Summary of Results: Between January and October of 2012, 33 separatecases have been presented in 40 team meetings. A total of 45 projects havebeen developed as a result of these meetings and are associated with all sixcore competencies for residency training. The majority have been related toSystems-Based Practice, and Practice-Based Learning and Improvement.Conclusions: A brief, patient-centered meeting in the ambulatory settingutilizing multidisciplinary medical teams can involve residents in meaning-ful projects across the six core competencies. This type of team meetingwould be applicable to most Internal Medicine residency programs.
515
RESEARCH AND INNOVATIONS IN MEDICAL EDUCATION(RIME) WEEK: AN INNOVATIVE APPROACH TO FACULTYDEVELOPMENT
Vick A, Snyder E, Estrada C, Kraemer R, Tofil N, Morris J, Roy B.University of Alabama at Birmingham, Birmingham, AL.Purpose of Study: In spite of radical changes in medical education, aca-demic medical centers remain focused on research and patient care withless emphasis on education. Despite this,medical education research occurs
Internal Medicine Competencies Associated with a Multidisciplinary Team Meeting
Competency Number of distinct topics covered (%) N= 45
Patient Care 5 (11.1)
Medical Knowledge 2 (4.4)
Professionalism 1 (2.2)
Systems-based Practice 19 (42.2)
Practice-based Learning and Improvement 10 (22.2)
Communication Skills 8 (17.8)
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 519
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

throughout the medical center, often in isolation. In order to highlight medicaleducation and foster collaboration, we developed a weeklong event highlight-ing Research and Innovations in Medical Education (RIME Week).Methods Used: RIME week consisted of faculty development workshops,simulation demonstrations, a poster session for abstracts, innovations, andvignettes, and lectures by local and national experts. Events were targeted tofaculty and fellows interested in graduate and undergraduate medical educa-tion. Workshops were evaluated using a 4-point Likert scale (range: 1=belowaverage to 4=outstanding). Participants evaluated the events as a whole basedon readiness to change and recommendation to others.Summary of Results: Forty-five attendees rated the workshops; 36%from the department of medicine, 22% from pediatrics, 44% from otherdepartments: 31% assistant or associate professor, 20% professors, 20%were fellows.
Across all workshops (n=106 total evaluations), 50% were rated asoutstanding and 36% truly above average (median 3.5, 25th percentile 3, 75thpercentile 4).
Of the 45 respondents, the most valuable sessions were workshops forgraduate medical education (38%), simulation activities (29%), undergrad-uate medical education (11%), and medical education poster session (4%);33% were definitely planning to implement a lesson learned, 36% very likely,and 20% likely; 33% will recommend to others (as ‘‘must attend’’), 40%very likely to recommend, and 16% likely.
Of the 47 posters, 26 were educational innovations,13 research abstracts,and 8 were clinical vignettes; 51% were submitted by faculty,26% by medicalstudents, 11% by fellows, and 11% by residents.Conclusions: The broad participation and positive evaluations of RIME weeksuggest that this venue appears to fulfill an unmet need for faculty develop-ment and allows for avenues for collaboration throughout the medical center.
SSGIM Research Abstract Session B
10:30 AMFriday, February 22, 2013
516
LEADERS IN ESTABLISHING PATIENT CENTEREDMEDICAL HOME FOR INDIGENT POPULATION
Aggarwal A1, Hood K2, Kaur S1, Hurdle B3, Oswald J3, Smith W1. 1VirginiaCommonwealth Univeristy, Richmond, VA; 2Mississippi State University,Mississippi State, MS and 3National Association of Public Hospitals andHealth Systems, Washington, DC.Purpose of Study: The Patient-Centered Medical Home (PCMH) modelhas emerged as a promising approach to providing high-quality, patient-centered care, complete with adequate reimbursement mechanisms. Thisabstract focuses on the qualitative data collected as part of a mixed methodevaluation of Virginia Coordinated Care (VCC), a PCMH program targetingthe indigent population to explore successes and challenges in implementingthis type of program.Methods Used: In-depth interviews were performed with nearly all 12 cur-rent and former executive leaders of the VCC program, as identified byprogram staff. The study explored goals of program establishment, the effec-tiveness in improving utilization and outcomes, as compared to the traditionalsafety net delivery system. Emphasis was given to know the engagementof primary care providers and success as a PCMH. Audio recordings ofthe interviews were transcribed then reviewed and coded using Nvivo 10 viathematic analysis and coding.Summary of Results: A total of 22 codes emerged from the analysis,and were assigned data units based on frequency. Codes were then groupedby similarity and relevance, revealing 3 themes and 8 subthemes. Majorthemes included the desire to improve access to care, perceived benefitsof providing patients a medical home, and barriers to providing care suchas transport and financial restraints. Sub themes included goals to decreaseurgent care and increase primary care engagement to establish PCMH.Conclusions: Motivation amongst leaders is strong to enlist new ap-proaches to increasing access to health care for indigent populations, de-creasing emergent room visits and establishing PCMH. Despite the potentialof PCMH to improve access and quality, the barriers patients face are numer-ous and stem from a variety of both personal, logistic and program limitations.
More study is needed to explore health care leaders’ ideas for programimprovements.
517
A PATIENT CENTERED MEDICAL HOME FOR SICKLECELL DISEASE
Martin TD1, Mauldin P2, Moran W1. 1Medical University of South Carolina,Charleston, SC and 2Medical University of South Carolina, Charleston, SC.Purpose of Study: Sickle cell anemia is a life limiting disease associatedwith painful crises and complications resulting in frequent need for hospi-talization and emergency department use. Based on analysis of acute utili-zation at our institution, we identified an initial high risk subset of 25 patientswith a high frequency of hospitalizations and emergency department visits,primarily for painful crises. This subset group also had low adherence withoutpatient care and treatment recommendations.Methods Used: In July 2012, we implemented an outpatient sickle cellmedical home to build a relationship with these high risk patients, improvequality of care, decrease emergency department visits and rates of hospital-ization, increase compliance, improve management of the secondary com-plications, and improve overall management of pain associated with sicklecell anemia. Diagnosis, comorbidity, and utilization data was used to tierpatients with sickle cell disease. The clinic team is comprised of a physician,nurse practitioner, nurse case manager, certified medical assistant, pharmacist,and social worker. Baseline clinical data was obtained at the initial visit andpatients were oriented to the structure and goals of the clinic. The clinic pro-vided routine monthly visits for medical assessment, pain medication refills,pain contract renewals, health maintenance, and management of secondarycomplications. Day treatment appointments and walk-in visits were availablefor patients with uncontrolled pain to provide intravenous fluids and parenteralnarcotic therapy. Clinic protocols were developed for individualized plans ofcare for pain crises, appropriate initiation and maintenance of Hydroxyurea,iron overload due to repeated transfusions, and routine screening and treatmentof depression.Summary of Results: Wewill present results based on 6 months of findingsfrom the sickle cell medical home strategy including rates of hospitalizationand emergency department visits, adherence to treatment, Hydroxyurea com-pliance, iron overload treatment, identification and treatment of depression,patient satisfaction, and pain control.Conclusions: We will present conclusions based findings at 6 months basedon the impact of the sickle cell medical home strategy.
518
DEVELOPMENT OF A NEW HOMELESS PRIMARY CAREASSESSMENT SURVEY USING QUALITATIVE METHODSAND ITEM RESPONSE THEORY
Kertesz S1, Jones R2, Roth D5, Gordon A3, Granstaff U6, Holt C4, Pollio D6,Austin E1. 1Birmingham VA, Birmingham, AL; 2Hebrew Senior Life, Boston,MA; 3Pittsburgh VA Health System, Pittsburgh, PA; 4U. Maryland, Baltimore,MD; 5Johns Hopkins University, Baltimore, MD and 6University of Alabama,Birmingham, AL.Purpose of Study: A national focus on patient-centered care has spurredthe use of surveys such as the Consumer Assessment of Health Plans(CAHPS). Such generic questionnaires may not capture the priorities ofunique populations like the homeless. We detail a systematic method fordeveloping a patient-centered primary care (PC) assessment survey, com-bining qualitative interviews, administration to homeless patients, and psy-chometric selection of the most informative items applying factor analysisand Item Response Theory analysis.Methods Used: We interviewed 36 patients, 24 expert clinicians and 4focus groups, exploring 11 major quality concepts. A resulting 78-item draftsurvey was administered to 601 homeless-experienced PC patients from3 mainstream PC sites and 2 homeless-tailored programs. We use confir-matory factor analysis and Item-Response Theory to choose the items mostinformative for each construct of interest. IRT analysis combined study ofitem information curves and Test Information Functions (TIFs), a graphicdisplay of how a collection of items captures a latent construct.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
520 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

Summary of Results: The analyses produced a 33-item final instrumentwith 4 scales: patient-clinician relationship (PCR), cooperation (COOP),access/coordination (A/C) and Homeless-Specific Needs (HSN). Examplesof highly informative items were: ‘‘If my primary care provider and I wereto disagree about something related to my care, we could work it out’’;‘‘This place helps me get care without missing meals or a place to sleep’’and ‘‘My primary care provider makes sure health decisions fit with theother issues in my life.’’ The scales had good convergent and divergentvalidity. As predicted, two homeless-tailored primary care programs out-performed 3 ‘‘mainstream’’ programs (all pG.05).Conclusions: For unique populations, the combination of qualitative re-search, and scale development using IRT permits the selection of an intuitively-appealing and valid patient survey. Programs that tailor primary care servicedelivery measurably enhance the patient care experience.
519
WHERE IS THAT BLUE PHONE AGAIN?: OPINIONS ANDBEHAVIORS REGARDING THE USE OF INTERPRETERSIN NEW ORLEANS
Sandler R. Tulane University Health Sciences Center, New Orleans, LA.Purpose of Study: Resident physicians are typically most involved phy-sicians in the daily care of patients at academic medical centers, yet themajority state that they have little training in the proper use of interpreters.Lack of time and poor access to trained medical interpreters are cited asreasons for using untrained, rather than trained professionals. In NewOrleans, demographic changes after Hurricane Katrina have led to increasesin the patient population with limited English proficiency and subsequentneed for interpreters in the healthcare setting. The purpose of this studywas to examine the patterns of use and perceived barriers to use of inter-preters by resident physicians in New Orleans.Methods Used: An email-based survey was distributed using the programSurvey Monkey to all residents in Internal Medicine, Pediatrics, and Com-bined Internal Medicine/Pediatrics at Tulane and LSU Health Science Centerin New Orleans. Microsoft Excel was used for data analysis.Summary of Results: 92.4% of subjects surveyed stated that they hadused an interpreter during their residency with interpreter services via tele-phone and patient family members being the most commonly used types ofinterpreters (41.3% and 30.5%, respectively). Other types of interpreterscommonly used included other staff members (14.9%) and professional on-site interpreters (8.3%). 86.3% of subjects felt that there were barriers tousing interpreters at the hospitals where they train and 81% of residentsrecalled difficulty communicating with patients due to difficulty locating aninterpreter. Residents cited lack of availability of interpreter services, lack oftime, and lack of knowing how to access interpreters as the major barriers tousing interpreters. The frequency of use of interpreters during initial historytaking was significantly more often than during daily patient visits (pG0.005).Conclusions: Resident physicians training in New Orleans generally haveexperience utilizing interpreter services during their training; however, theyare not always using trained professional services nor are they using inter-preters for every element of the hospital encounter. Further training targetedat modifiable barriers to interpreter use, like where to access interpreters, mayhelp improve use of interpreters for patients with limited English proficiencyin New Orleans.
520
IT’S A GAME CHANGER: TRANSFORMING PATIENT CAREWITH THE EXTERNAL MEDICATION HISTORY
Wolver S, Aggarwal A. VCUHS, Richmond, VA.Purpose of Study: Electronic prescribing within an Electronic HealthRecord typically includes a feature known as the External Medication His-tory (EMH). The EMH is an embedded query which allows providers to viewthe fill history of medications patients have obtained from pharmacies. Thisstudy seeks to determine the impact of this new feature for both providersand patients.Methods Used: Two self-administered surveys were used to collect the data.A 21 question survey was emailed to 600 providers (faculty and housestaff)
and a 24 question survey was administered to patients recruited from twogeneral internal medicine primary care clinics: a faculty practice and a residentpractice.Summary of Results: Of the 157 completed provider surveys, 61% wereaware that the external medication history feature existed. Of the 39% thatwere not aware, 82% said they would now use it. The most common reasonsfor looking at the EMH included checking for compliance (45%), confirm-ing and reconciling medication dosages (41%), checking for controlledsubstance prescription history (36%), making sure the most up to datemedications were on the patient’s medication profile within the EHR (29%),and identifying the patient’s pharmacy (25%).
Providers felt their practice was most changed by discovering medica-tions, including controlled substances, prescribed by other providers. In fact,40% of respondents found medications on the EMH that they were notaware their patient was taking. About 60% of the providers tell their patientsthey look at the EMH and 10% feel that discussing this with their patientsmight change their medication taking behavior. 37% thought that, with thisknowledge, their patients might be more likely to take their maintenancemedications.
Of the 105 patient surveys completed, 70% knew their providers couldsee if they were filling their medications and 45% indicated their providerdid this during a visit. 34% of patients felt the EMH feature might changetheir medication taking behavior and 48% responded that it already hadchanged their behavior.Conclusions: The EMH feature has significant impact on both providersand patients. Use of the EMH enhances patient safety by giving providers amore complete picture of a patient’s medication profile and compliance.Additionally, patient knowledge of this feature has the potential to improvetheir medication compliance.
SSGIM Research Abstract Session C
1:30 PMFriday, February 22, 2013
521
MOTIVATION, SELF-EFFICACY, AND WEIGHT LOSS IN ACLINIC-BASED WEIGHT LOSS PROGRAM
Rose SA1, Zephyr PD2, Smith JT2, Masero C1, Webber K3. 1University ofKentucky, Lexington, KY; 2University of Kentucky, Lexington, KY and3University of Kentucky, Lexington, KY.Purpose of Study: Motivation can predict success in weight loss programs.We explored motivation, self-efficacy, and perceived autonomy support forpatients enrolled in a weight loss program, and assessed BMI change in asubset of patients.Methods Used: Patients enrolled in a 12-week clinic-based medically-managed weight loss program based on the Diabetes Prevention Programbetween January 2011 and April 2012 completed a baseline quantitativesurvey with questions from the Treatment Self-Regulation Questionnaire, theHealth Care Climate Questionnaire, and the Perceived Competence Scale.Summary of Results: 36 overweight and obese patients (body massindex (BMI) Q25 kg/m2) agreed to participate. 88.9% reported having seentheir PCP at least once in the past year. All but one reported their PCPhad ever told them they needed to lose weight. 62% felt that their PCP wasable to help them with weight loss, but only 44% felt it was their PCP’sresponsibility to do so. Mean autonomous motivation (AM) was 6.02 (SD0.79) (scale of 0 to 7), mean controlled motivation (CM) was 2.70 (SD 1.21),mean self-efficacy was 4.78 (SD 1.32), and mean perceived PCP supportof AM was 4.58 (SD 1.69). There was a positive correlation between self-efficacy and AM (r=0.30); and a negative correlation between self-efficacyand CM (r=-0.17), PCP support of AM and AM (r=-0.08), and perceivedPCP support of AM and CM (r=-0.39). Patients with linked outcome andsurvey data (n=8) demonstrated a mean BMI change of -1.44 kg/m2 (range -4.3 to +0.7). For these patients, there was a negative correlation betweenBMI and AM (r=-0.27), CM (r=-0.10), and self-efficacy (r=-0.14); and apositive correlation between BMI and perceived PCP support of AM(r=0.39).Conclusions: Patients reported higher mean levels of AM versus CMand a positive correlation between self-efficacy and AM. The small subset
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 521
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

demonstrated an overall mean weight loss. Higher levels of AM and self-efficacy were linked to decrease in BMI, as was higher levels of CM,although the correlation was not as strong. Future goals include expandingthe sample size to strengthen the results and an intervention to promotepatient and provider self-efficacy and AM.
522
PATIENT AND PROVIDER PERCEPTIONS TOWARDOBESITY CARE IN THE PRIMARY CARE SETTING
Rose SA1, Conigliaro J2, Schoenberg N3. 1University of Kentucky, Lexington,KY; 2North Shore-LIJ, New Hyde Park, NY and 3University of Kentucky,Lexington, KY.Purpose of Study: Physicians are not routinely screening and counselingfor obesity. We evaluated role perceptions and barriers and facilitators toweight loss care in primary care.Methods Used: Based on previous findings, we conducted focus groupsfor primary care providers (PCPs) and adult (Q18 years of age) patients (pts)at four rural and urban primary care settings. PCPs and pts were invited toparticipate in separate 90-minute focus groups run by a trained facilitator.Topics included 1) reasons for discrepancies in prevalence of PCP and ptreport of discussion of weight loss (100% vs 44%); 2) reasons for differencesin sense of PCP responsibility for pt weight loss (93% vs 41%); 3) types ofweight loss programs recommended by PCPs; 4) barriers to PCP provision ofweight loss care; and 5) ideas for improvement for PCP provision of weightloss to pts. Focus group sessions were audiotaped and transcribed and sub-jected to content analyses.Summary of Results: Several main themes emerged. PCPs felt thatpts underreported PCP weight loss counseling due to lack of informationretention and inadequately explicit discussion, while pts felt that PCPsmay overreport counseling and may be reluctant to provide counseling dueto concern of offending pts. PCPs reported giving explicit tips such asmaintaining food diaries, calorie counting, and referring to programs likeWeight Watchers, while pts generally reported receiving modest informa-tion including dietary advice or none at all. PCP-reported barriers includedconcerns about patient sedentary lifestyle and inadequate office tools forweight loss. Pt-reported barriers to weight loss included lack of time andpoor communication between PCPs and pts, as well as pt socioeconomicand lifestyle barriers. PCPs recommended improving pt access to programsaddressing healthy lifestyle, while pts focused on specific weight loss goals,incentives, frequent follow-up, and increase in communication.Conclusions: Inadequate PCP weight loss counseling represents a missedopportunity, as pts appear receptive to weight loss advice. These results moveus closer to developing useful tools for weight loss in primary care.
523
EFFICACY OF SMOKING CESSATION METHODS: COLDTURKEY VERSUS ALL OTHER METHODS
Bharadwaj RM, McClure SC. Texas Tech University Health Sciences Center,Amarillo, TX.Purpose of Study: This study was performed to determine the mostcommon and successful method of smoking cessation. Older studies suggestthe most common method is cold turkey or reduction before quitting; how-ever, to date, clinical guidelines neglect this as a viable option.Methods Used: Data were collected by a short survey to different setsof individuals, including clinic patients and from community. Survey wasdiscarded if there was no history of smoking or a person never tried toquit smoking. Cold turkey method was compared to all other methods. Sta-tistical analysis was done by comparing the methods used to quit by twogroups ‘‘people who quit successfully’’ with ‘‘people who failed to quit’’. SAS9.2 was used to calculate basic analysis, frequency and Odds Ratio (OR) forsmoking cessation with different methods. P-value of G0.05 was consideredstatistically significant.Summary of Results: One hundred and six subjects (58 male and48 female) were identified who smoked in the past and tried to quit.Mean age was 45.14 Yrs (SD 15.5) in cold turkey group and 47.09 Yrs(SD 12.37) in other group (p=0.498), predominantly involving white subjects(80.19%).
Sixty three subjects (59.43%) tried the cold turkey method whereas43 subjects (40.57%) tried all other methods. Fifty seven subjects (53.77%)quit smoking altogether and 79% of them used the cold turkey method ascompared to only 21% who used other methods.
OR for smoking cessation with cold turkey method was 6.46 (95%CI 2.73; 15.29) pG0.0001 compared to other methods. A significant gendereffect was also present; OR for females who quit smoking with cold turkeymethod was 14.06 (95% CI 3.77; 15.35) pG0.0001, as compared to malesOR 2.75 (95% CI 0.81; 9.39) p=0.10.Conclusions: This study suggests that cold turkey method remains themost common and effective way for smoking cessation as compared to allother methods and clinicians should counseled their patients regarding thisas a viable option.
524
INCIDENCE AND ASSOCIATION OF SEVEREHYPOGLYCEMIA IN HOSPITALIZED PATIENTS
Carnegie RS2,1, Meadows RY1,2. 1Ochsner Medical Center - New Orleans,New Orleans, LA and 2Tulane University, New Orleans, LA.Purpose of Study: This single-center, retrospective cohort study aims tocorrelate means of insulin therapy, diabetes mellitus (DM) type, and patientfactors with the incidence of severe hypoglycemia (SHG) upon or within48 hours of hospital admission.Methods Used: 650,525 BG values obtained in an academic tertiary carehospital from 1/1/2010 to 3/31/2012 were analyzed for SHG (blood glucose(BG) G 40 mg/dL). Children and 8 adults were excluded for care locationoutside the defined units or medication error-related hypoglycemia. Onsetof SHG was calculated from time of presentation to first SHG episode.Characteristics including route of insulin administration, type of DM, A1c,renal function (GFR), and care location were recorded.Summary of Results: Of 274 subjects, 130 (47.4%) incurred SHG within48 hours of admission. Ninety-eight (75.4%) incurred SHG within the first24 hours of admission, 21 (16.2%) within 24-36 hours, and 5 (3.8%) within36-48 hours. Only 18 (13.8%) received treatment with infusion insulinwhile 112 (86.2%) received conventional subcutaneous insulin regimensand/or monitoring, Thirty-six (27.7%) had type 1 DM, 89 (68.5%) had type2, and 5 (3.8%) had gestational DM or other. Seventy-two (55.4%) werecared for in non-critical care units, 25 (19.2%) in step-down units, andonly 33 (25.4%) in traditional ICU beds. Normal renal function was foundin 47 (36.2%) while 52 (40%) had GFR G 30 or were on hemodialysis. Of118 patients with recent A1c levels, 29 (24.6%) had A1c of 6.5 or less, 55(46.6%) had A1c 6.6 to 9.0, and 34 (28.8%) had A1c 9.1 to 14. There wasno significant difference in mortality in any group.Conclusions: Reanalysis of NICE-SUGAR data has raised questionsconcerning association of hypoglycemia, and SHG in the absence of insulintherapy, with risk of death. Our study shows that almost half of the patientssuffering SHG during their hospital stay arrive with SHG or develop it within48 hours of conventional (non-intensive insulin) therapy. Primary diagnosisdid not predict risk, though a majority had impaired GFR. Most patients de-veloped SHG in less than 24 hours and had type 2 DM. Additionally, mostpatients were not treated with intensive insulin regimens or insulin infusion,nor were cared for in a traditional ICU.
Compare Cold Turkey method with Other Methods
Cold turkey
Method
Other
method
Mean Age
45.14
(SD 15.5)
47.09
(SD 12.37) P=0.498
Total Number QuitSuccessfully Failedto Quit
N=63 45 18 N=43 12 31 OR 6.46 (95% CI2.73,15.29)
PG0.0001*
Successful Females 23 4 OR 14.06 (95% CI3.77,52.35
PG0.0001*
Successful Males 22 8 OR 2.75 (95% CI0.81,9.39
P=0.102
*(pG0.05 is considered significant)
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
522 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

525
SYSTEMATIC LITERATURE REVIEW OF EMERGENCYDEPARTMENT INTERVENTIONS TO AVOIDHOSPITALIZATION FOR ACUTELY DECOMPENSATEDCONGESTIVE HEART FAILURE
Harris LJ, Bailey JE. University of Tennessee Health Science Center,Memphis, TN.Purpose of Study: Acutely decompensated congestive heart failure(ADCHF) is a common cause of hospital readmissions. Based on AmericanCollege of Cardiology guidelines, 1 it has been suggested that up to 50%of admitted patients would have been candidates for outpatient therapy aftersymptom reduction if adequate post-discharge systems were in place. 2,3Emergency Department (ED) observation units (OU) have achieved lowerrates of inpatient hospitalizations, but their effectiveness is unknown.
Question What ED interventions are evidence based to safely decreasehospitalizations for ADCHF?Methods Used: pubmed.gov search (‘‘Heart Failure/economics’’[Mesh]OR ‘‘Heart Failure/therapy’’[Mesh]) AND (‘‘Ambulatory Care’’[Mesh] OR‘‘Emergency Service, Hospital’’[Mesh]) The reference lists of review articles4, 5 were searched for additional literature.
ClinicalTrials.gov was searched for ‘‘CHF AND Observation ANDUnit.’’
Studies were selected for analysis if they specifically evaluated EDOU’sfor ADCHF.
Summary of Results: There are no comparative effectiveness trialsongoing.
Of 98 clinical trials on the initial search, only two studies specifically ex-amined the effect of EDOU’s.
The first is an observational, sequential, cohort study out of the Uni-versity of Cincinnati. 6 The second is a retrospective analysis of patientstreated in a 19-month period in the Cleveland Clinic CHF EDOU.7
The results of these two studies suggest OU management of the low/moderate-risk HF patient results in a safe and cost-effective alternative todisposition to ‘‘upstairs.’’ In one pilot study, cost savings in the patientsplaced in the OU were estimated to amount to approximately $3600 perpatient over historical controls.
Currently the Emergency Heart Failure Risk Mortality score is recom-mended to help physicians identify patients appropriate for observation.8, 9 One of the primary criticisms of OU care is that patients are placed inthe unit when they would otherwise have been discharged. Until low-riskpatients can be reliably identified, electing patients that may be safely dis-charged home remains difficult.6Conclusions: Emergency department risk stratification tools for ADCHFare being actively investigated with NHLBI funding. Current systems of careare built on expert opinion and observational studies.
SSGIM Research Abstract Oral Plenary Session - Joint withVignette Plenary
9:45 AMSaturday, February 23, 2013
526
USABILITYOFA FAMILY HEALTH HISTORYAND CLINICALDECISION SUPPORT TOOL FOR PATIENTS AND PRIMARYCARE PROVIDERS
Wu RR1, Himmel T2, Powell K3, Hauser E4, Agbaje A5, Ginsburg G2,Henrich V3, Orlando L2. 1Department of Veterans Affairs Medical Center,Durham, NC; 2Duke Univ, Durham, NC; 3UNCG, Greensboro, NC; 4DukeUniv, Durham, NC and 5Cone Health System, Greensboro, NC.Purpose of Study: Family health history (FHH) is the single strongestpredictor of disease risk, yet is significantly underutilized in primary care.We developed a patient facing FHH collection tool, MeTree*, with em-bedded education for patients and providers on the collection and importanceof FHH, as well as decision support for breast, colon, and ovarian cancers,hereditary cancer syndromes, and thrombosis.Methods Used: Non-adopted adult English speaking patients with anupcoming routine appointment with their provider at 2 primary care clinics
with 14 physicians in the Cone Health System were invited to participateby completing MeTree some time prior to their appointment. Patients andphysicians completed surveys on their experience, patients after their ap-pointment and at 3 and 12 months post-visit, physicians after 3 months ofintegration.Summary of Results: Patient enrollment=1184. 44% (521) met criteriafor more intensive prevention strategies, 30% for genetic counseling. Aver-age min. to complete MeTree=27. Patients found MeTree: easy to use (93%),easy to understand (97%), useful (98%), raised awareness of disease risk(81%), and changed how they think about their health (82%). Of the 26%asking for assistance to use MeTree, age (mean 65 sd 9.4 vs 57 sd 11.7, p-value0.00) and large pedigree size (24.5 sd 9.81 vs 22.3 8.41, p-value 0.00)were significant factors. Patients learned: more relatives had diseases thanthey realized (20%), relatives had diseases they didn’t know about (39%),they were mistaken about what diseases some relatives had (18%), and learnedhow old relatives were when they got a disease (39%). Providers (n=14)found MeTree: improved their practice (87%), improved their understandingof FHH (63%), made practice easier (75%), and worthy of recommending totheir peers (93%).Conclusions: Our study shows that FHH collection can be a positiveexperience for patients and providers and can be implemented without dis-ruption to workflow.
527
A META-ANALYSIS OF THE RAPID ANTIGENSTREPTOCOCCUS TEST
Davis B1, Stewart EH1, Clemans-Taylor BL1, Centor R1, Estrada C2,1.1University of Alabama at Birmingham, Birmingham, AL and 2BirminghamVAMC, Birmingham, AL.Purpose of Study: To examine the accuracy of the rapid antigen strepto-coccus test (RAST) to diagnose group A streptococcal pharyngitis.Methods Used: Meta-analysis. MEDLINE search and reference lists,2000 -2012. We included clinical studies using RAST and a reference stan-dard. We used the 14 Quality Assessment of Diagnostic Accuracy Studies(QUADAS) criteria to assess quality. We obtained hierarchical summaryreceiver operating characteristic (HSROC) using metandi (Stata).Summary of Results: We included 41 of 737 studies; the overall preva-lence was 29.3% (12,956/45,594 patients; range 4-67%). The setting wassolely in the emergency department (27%) or outpatient clinic (56%);22% were solely in children; 14% were retrospective; 32% reported com-mercial funding (51% no data). Of QUADAS criteria, eight were fulfilledby over 90% of studies, five by 60-80%, and one by 22% (standard inter-preted without knowledge of results). The pooled sensitivity was 88.2%(95% confidence interval [CI], 83.9 to 91.4%; range 52.6% to 99.9%). Thepooled specificity was 98.5% (95% CI, 96.7 to 99.3%; range 68.8% to100%). Figure shows the HSROC curve (solid line), summary point (filledsquare), and 95% regions (confidence, smaller; prediction, larger).Conclusions: The RAST is moderately sensitive and highly specific todiagnose group A streptococcal pharyngitis.
Journal of Investigative Medicine & Volume 61, Number 2, February 2013 Southern Regional Program Abstracts
* 2013 The American Federation for Medical Research 523
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.

528
EDUCATION IN DELIVERING PATIENT-CENTERED CARE:PROVIDER COMFORT LEVEL IN COUNSELINGWOMEN AGES 40-49 REGARDING BREAST CANCERSCREENING OPTIONS
Bryan T1,3, Snyder E1,3, Estrada C1,3, Castiglioni A2. 1University of Alabamaat Birmingham, Birmingham, AL; 2University of Central Florida College ofMedicine, Tampa, FL and 3Birmingham VA Medical Center, Birmingham, AL.Purpose of Study: US Preventive Services Task Force recommendscounseling women in their 40’s about the risk and benefit of Mammographyin order to come to a shared decision about screening. We assessed the impactof a brief education intervention on knowledge and attitudes of providers re-garding breast cancer screening recommendations for women ages 40-50.Methods Used: Quasi-experimental (before-after) academic detailing inter-vention consisting of a single interactive case-based discussion (30 minutesof risk/benefits, individual risk assessment, counseling methods). Participantswere providers and nursing staff in outpatient Veterans Affairs clinics.
Outcomes were: a) knowledge assessment of mammogram recommen-dations for 40-49 year old women, b) counseling practices on risk/benefitscreening, c) comfort level on counseling risk/benefit screening (2 questions;5 point Likert scale, 0=not comfortable and 5=very comfortable).Summary of Results: Thirteen outpatient VA clinics in Alabama receivedthe intervention. We received a total of 165 surveys (78 pre, 87 post) from RNs(43%), LPNs (38%), physicians (13%), or other (6%).
Breast cancer screening recommendations were different between preand post- intervention: screen all women aged 40-50 (82% vs. 9%), waituntil age 50 to screen (12% vs. 38%), and discuss patient’s preferences(5% vs. 53%)(pG0.001).
After the intervention, attitudes favoring discussion of benefits increasedfrom 94% to 99%; however, not statistically significant (p=0.08); attitudesfavoring discussion of risks increased from 34% to 90% (pG0.001)).
After the intervention, the comfort level of discussing benefits increasedfrom a mean of 3.8 (SD 1.1) to 4.5 (SD 0.7) (pG0.001), of discussing risks in-creased from 2.7 (SD 1.3) to 4.3 (SD 0.8) (pG0.001), and of discussing risks andpreferences for women ages 40-50 from 3.2 (SD 1.2) to 4.3 (SD 0.8)(pG0.001).Conclusions: An educational intervention detailing recommendations andcounseling methods affects knowledge and attitudes about breast cancerscreening for women ages 40-49. Hence, the delivery of patient-centeredcare may be enhanced by education of providers and nursing staff.
529
CO-MANAGEMENT OF CHEMOTHERAPY PATIENTSBETWEEN ONCOLOGISTS AND HOSPITALISTS AT ANACADEMIC MEDICAL CENTER
Liles EA, Edwards E, Curl D. UNC School of Medicine, Chapel Hill, NC.Purpose of Study: Given the expanding bed capacity at the North CarolinaCancer Hospital, recent restrictions on resident duty hours, and patient capson oncology teaching services, we elected to involve hospitalists in the careof patients admitted for scheduled chemotherapy. This retrospective cohortstudy seeks to describe the characteristics and outcomes of patients cared forin this model compared to traditional teaching services.Methods Used: Patients appropriate for hospitalist co-management arecollaboratively selected by the oncology consult team and hospital medi-cine faculty prior to admission. Most commonly, these patients are return-ing for consolidation therapy for hematologic malignancies. A hospitalistis responsible for the initial history and physical as well as admission orders.The oncology consult team of attending, fellow and PharmD are respon-sible for prescribing chemotherapy. A team of one hospitalist and mid-level provider address the patients’ co-morbid conditions, complicationsrelated to the chemotherapy itself and prevention of neutropenic infectionsafter discharge. Discharge planning is performed with the assistance of anurse navigator. We reviewed data submitted to the University HealthcareConsortium by UNC Hospitals. Our outcome measures included numberof admissions, case mix index, average length of stay, mortality index, lengthof stay index, and readmission rate. Currently data is available throughJune 2012.Summary of Results: During the study period (July 2011-June 2012),228 patients were admitted to the hospitalist service for scheduled chemo-therapy, compared with 85 patients to our oncology teaching services. Theaverage case mix index (CMI) for the hospitalist service was 1.38 vs. 1.53 forthe oncology teaching service. Average length of stay (LOS) was 4.1 dayson the hospitalist service (LOS index 0.95) vs. 6.05 (LOS index 1.3) dayson oncology teaching services. The 30-day readmission rate was 16.5% vs.21.5% for hospitalist and oncology services respectively.Conclusions: Patients admitted to a hospitalist service for scheduled che-motherapy had a shorter length of stay and a lower 30-day readmission ratecompared with patients admitted to an oncology teaching service. Our datasupports the concept of co-managing of patients undergoing scheduled con-solidation chemotherapy.
Southern Regional Program Abstracts Journal of Investigative Medicine & Volume 61, Number 2, February 2013
524 * 2013 The American Federation for Medical Research
Copyright © 2013 American Federation for Medical Research. Unauthorized reproduction of this article is prohibited.





























