Embed Size (px)
Citation preview

SPASTIC CEREBRAL PALSY: POSSIBLE SPINAL INTERNEURONAL CONTRIBUTIONS
~~
Ann Harrison
A spinal interneuron model of spasticity Until recently, the most commonly offered explanation for the hyperreflexia shown by spastic cerebral-palsied individuals was exaggerated fusimotor drive. Though some abnormality of fusimotor functioning is not ruled out (Rushworth 1960, 1964; Jansen 1962; Hagbarth et al. 1973; Landau 1974), a simple model of elevated drive is not tenable (Burke et al. 1976, Burke 1983). In trying to account for various features of the spastic cerebral palsy syndrome, it seems worthwhile to shift attention to the spinal interneuron level, where supra- spinal and segmental influences are re- solved. Abnormal interneuronal function- ing could generate hyperreflexia and responsiveness to normally innocuous stimuli. The interneuronal network is thought to play an important r81e in co- ordinating activity in different muscle groups (Harrison et al. 1983). Abnormal patterns of co-ordination, such as reflex radiation and reciprocal excitation, are regularly observed in individuals with spastic cerebral palsy and are consistent with the hypothesis that spinal inter- neuronal networks are not functioning normally. While spastic cerebral palsy has its origin in central damage, this does not preclude the possibility that immature spinal pathways and abnormal peripheral
circuits play major r6les in these patients’ functional difficulties.
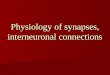
Myklebust and colleagues (1 982) believe that reciprocal excitation of antagonist muscles is characteristic of spasticity associated with congenital brain-damage. When the ankles of subjects with spastic cerebral palsy were passively manipulated, activity was recorded both in the stretched agonist and in the antagonist. Antagonist
that observed in neurologically normal subjects. Antagonist and agonist activity d began together, unlike in a shortening reaction (Sherrington 1909, Angel 1983). A conduction artefact explanation was
5 ruled out because the activity profiles of the agonist and antagonist groups were
2 markedly different. Although recording 3 conditions were identical, reciprocal is excitation was never recorded in neuro- 3 logically normal adults, or in patients
whose spasticity had its onset in adulthood. Myklebust et al. (1982) believe that .: reciprocal excitation occurs because the
excites both agonist and antagonist 8 i! -3 alpha motoneuron is abnormally weak, or
because the normal reciprocal inhibitory 4
8 activity was 20 to 100 times greater than I-
m W I-
00 00
5
s 2
aJ
3 - afferent output from the stretched muscle
motoneurons (Fig. l), either because descending inhibition of the antagonist
2
loop A is replaced (or is functionally over-ridden) by excitatory loop B. 769

P P
.I 2 a
v1
.- u I c)
a v1
770
NORMAL SPASTIC SYSTEM SYSTEM W E A K
I D E S C E N D I N G
,_--- j I N H I B I T I O N
S P A S T I C L O O P B - e x c l t a t l o n __I I n h i b i t i o n
Fig. 1. Reciprocal excitation in spastic cerebral palsy (based on Mykelbust et al. 1982). (Circles represent abha and gamma rnotoneurons and spinal interneurons.)
Further research is needed to establish whether loop B does indeed exist and whether it is more accurately described as primitive or abnormal (Bobath 1966). If loop B is primitive, then supraspinal damage would be viewed as creating conditions which stall normal ontogeny. Alternatively, supraspinal damage may have the effect of encouraging abnormal axonal sproutings, which form the ectopic loop B (Myklebust et al. 1982). In a follow-up study by Myklebust et al. (1986), reciprocal excitation was regularly observed when neurologically normal neonates were tested. The impact of the central lesion in this instance therefore appears to be one of creating conditions which prevent the development of reciprocal inhibition, or which actively or passively encourage reciprocal excitation dominance. Futagi and Abe (1985) com- pared the H-reflex responses of neuro- logically normal and spastic children, and demonstrated hyperreflexia. They argue that this form of hyperactivity cannot be fully explained by immaturity, but that abnormalities are also present.
Abnormal co-ordination patterns and hypersensitivity are features of the spastic system which have been demonstrated in a wide variety of experimental and clinical test situations. Studies of passive and active movements have revealed abundant antagonist activity (Milner-Brown and Penn 1979, Knutsson and Martensson 1980). In some patients, reciprocal
inhibition was observed at low speeds, but this broke down when faster movements were imposed. Antagonist involvement limited movement speed and made actions jerky. Barolat-Romana and Davis (1980) studied the effects of dorsal-root stimu- lation in 80 patients with spastic cerebral palsy. Neuronal hypersensitivity was demonstrated and attributed to a lack of Ia presynaptic inhibition. Hypersensitivity of this sort would explain why muscle spasms can be triggered by normally in- nocuous stimuli, e.g. cutaneous excitation. Widespread activation along polysynaptic pathways was also noted, which was aggravated by increasing the frequency of stimulation. Co-activation of synergistic and contralateral muscle groups, reflex radiation and clonus are only some of the features of spastic cerebral palsy which are characterised by an abnormal spread of activity to other muscle groups. When postural correction was studied, the main abnormality observed in ‘pure’ spastic children was an inappropriate co- ordination of activity in participating muscle groups (Nashner et al. 1983). Sometimes the prime contraction needed to produce stabilisation was disrupted by activity in a synergist or antagonist. Inappropriate sequencing produced both functional ‘hypertonus’ and ‘weakness’. Indeed, Nashner and colleagues believe that the exaggerated stretch reflexes shown by individuals with spastic cerebral palsy may be a consequence of abnormal co-ordination patterns, rather than vice versa. Abnormal sequencing of muscle activity can also affect the biomechanical properties of a limb and restrict the correction strategies that are available for motor planning, execution and correction (Nashner and McCollum 1985).
Segmental organisation and motor control Recent research has revealed the highly complex nature of the peripheral systems involved in controlling muscle activity and muscle-group co-ordination. Micro- neurography has made it possible to trace excitatory and inhibitory forces at the intracellular level, and to map inputs and interactions which cannot be discerned from extracellular recordings (Dimitrijevic et al. 1983, Harrison and Jankowska 1984). Spike-triggered and noise-triggered

averaging can be used to trace whether activity in a given channel affects the firing rate of a given spinal neuron, and to identify which channels are affected when a given spinal neuron is active (Harrison and Taylor 1983). A variety of spinal interneuronal systems have been described in the cat (Jankowska 1982-1983; Harrison and Zytnicki 1984; Harrison and Jankowska 1985a, b), and these provide for very subtle regulation by supraspinal and segmental influences. Inputs to the spinal motoneurons and interneurons of a given muscle are not restricted to direct descending nerve- fibres and sensory inputs from the muscle and its antagonist. Rather, inputs are received from distant and diverse sources (Harrison and Johannisson 1983). Similarly, spinal interneuronal output is highly fractionated. When tendon organs and spindle receptors are activated, for example, it is believed that practically all muscle groups in the limb are affected to some degree.
The balance of excitatory and inhibitory forces on relevant spinal motoneurons and interneurons will determine what pattern of muscle activity results. In the monkey, reciprocal inhibition commonly is over-ridden by supraspinal influences, but emerges when central inhibition is blocked by anaesthetic or when peripheral forces predominate (Mizuno et al. 1971). Spinal interneurons appear to be specialised for ensuring that the activity of a given muscle is functionally co- ordinated with that of other muscles (Harrison et al. 1983) so that a properly orchestrated sequence of movements is achieved. When more discrete movements are called for, it is not known whether the interneuronal system is generally inhibited, or whether central motor commands produce subtle modulation of relevant interneurons (Dimitrijevic et al. 1983).
The stereotyped patterns of movement which are characteristic of individuals with spastic cerebral palsy suggest that interneuronally mediated activity domi- nates. The human neuromuscular system differs from infrahuman models in terms of its spinal organisation, histology and neurotransmitters (Delwaide et al. 1983), so extrapolations must be made cautiously. Data from human subjects are
limited, but microneurography appears to be an acceptably safe procedure (Prochazka and Hulliger 1983).
In order to assess the possible impacts of segmental abnormalities, it is necessary to understand the r8les descending and segmental forces play in voluntary move- ments. A full range of locomotor patterns (walking, running, galloping, etc.) can be triggered in spinal preparation cats by peripheral stimulation (Grillner 1975). This led to a ‘step-generator’ model of voluntary locomotion in which such segmental patterns are used, thereby reducing motor programming demands. Flexibility is still possible because central signals select which pattern is triggered and when, and descending forces are used to modify the otherwise stereotyped output. An opposing view is that spinal patterns are incompatible with voluntary output, either because they cannot be selected or adapted by descending impulses, or because modification repre- sents a less economic solution than programming the action centrally, with- out incorporating segmental patterns. Thelen (1986) showed that when seven- month-old infants were supported on a treadmill, well co-ordinated stepping patterns were elicited which these children did not execute voluntarily until later in their development. The explanation offered is that the ‘co-ordinative linkages’ underlying more mature stepping patterns already existed, and were triggered because the treadmill action stretched the leg muscles appropriately. When children are older they have the strength, balance and control of key muscles required to trigger the same ‘co-ordinative linkages’.
Forssberg (1985) studied ‘primitive walking’ in neurologically normal children and found a gradual transformation of the primitive non-plantigrade action into mature plantigrade locomotion. He ascribed this to progressive supraspinal modulation of the primitive segmental pattern because there was no evidence of an abrupt transition, such as might be expected if intrinsic spinal co-ordination is being superseded by a fully centralised control programme. Thelen and Cooke (1987) undertook a longitudinal study of how patterns of muscle contraction and joint displacement change as children
d 00 W
2
771

C
T
- Q .- n vl
.- U
2 n *
vl
772
progress from newborn stepping to independent walking. The recorded changes varied enormously from indi- vidual to individual, but two features commonly observed were a decrease in co- contraction and replacement of tonic activity in certain muscles (such as the ankle flexor tibialis anterior) with phasic bursts at predictable points in the walk cycle. Importantly, those authors stress that such developments do not necessarily reflect changes in neural control patterns. Rather, alterations in the biomechanical properties of the limb, postural control and task demands may play major r6les in provoking the developmental changes that are observed.
Many motor factors may contribute to the movement abnormalities and diffi- culties of patients with spastic cerebral palsy. Inadequate neural control will limit what patterns of movement can be produced, and how effectively ‘co- ordinative linkages’ are triggered, sup- pressed or modulated to meet task requirements. Factors such as muscle weakness, poor postural control and in- adequate control of key muscles will directly affect which combinations of movements can be executed, and may also produce conditions which favour the retention of primitive segmental patterns, or which are incompatible with the triggering of more mature ones. Abormal, stereotyped movenlent patterns could result from abnormal ‘co-ordinative linkages’, or from abnormal modulation or blending of normal linkages. Again, abnormal neural control or abnormal peripheral components, or both, may be to blame. All these factors are likely to increase stereotypy (Erokhina et al. 1976) and limit the performance strategies the patient can use.
The reasons for the motor control problems of individuals with spastic cerebral palsy may be different at different stages in the development of the condition. Initially they will be a direct consequence of the brain damage sus- tained, but later, secondary abnormalities such as abnormal muscle growth (Ziv et al. 1984) may form major bars to normal control. Nor is it necessarily accurate to think of a one-way system in which central abnormalities produce peripheral
abnormalities (Rowlandson and Stephens 1985). Blakemore and Van Sluyters (1975) showed, for example, that normal development of the visual cortex depends on normal visual experience. When visual input is impoverished it interferes with the acquisition of mature central functioning. By analogy, central and peripheral motor immaturities and abnormalities may so restrict the movement experiences of individuals with spastic cerebral palsy that the normal development of neural motor functions is disrupted. In other words, a cycle may exist in which the original central abnormalities lead to immaturities and abnormalities at the spinal level, which in turn interfere with supraspinal development, imposing further limit- ations on how effectively the system can be used for skilful action.
Modifying segmental functioning Recent work by Wolpaw (1985) supports the idea that central forces can produce persistent, intrinsic changes in segmental functioning. He studied the changes in short-latency spinal stretch reflex ( ~ 1 ) responses observed when primates were rewarded for attenuating (enhancing or suppressing) M1 reactions. Monkeys maintained a steady elbow posture against torque motor opposition for 3000 to 6000 test trials. Computer surveillance was used to ensure that there were no signifi- cant alterations in agonist background activity or in the contributions of synergists and antagonists. This was done so that any shifts in ~1 responsiveness could only be ascribed to recalibration of the segmental loop. Substantial attenuations were achieved (Fig. 2), and these persisted even when animals were given two- or three-week breaks from the experiment. Adaptation took place in two phases. During the first six hours of training a change of approximately 8 per cent in responsiveness occurred, followed by a slow incremental change (1 or 2 per cent per day) over the next six weeks. Stretches were administered on a randomised time- schedule, so tonic changes were needed to ensure that the animal would reliably secure rewards. Since background EMG activity did not vary, Wolpaw believes the most likely explanation for the changes observed is modulation of muscle-spindle

output, either by attenuating gamma efferent activity or by presynaptic inhi- bition of the Ia synapse. Wolpaw argues that initial shifts in responsiveness were achieved by altering descending inhibition and excitation. Later changes, however, are ascribed to tonic changes at the periphery. Membrane changes could alter neuronal responsiveness and axonal sproutings could change the pattern of inhibitory and excitatory forces present. Plasticity was also evident when the training demands were altered. In just a few days, it proved possible to shift M1 responsiveness in the opposite direction from normal. Adaptation of the vestibular reflex follows a similar pattern: it occurs in two phases, it takes time to maximise and reverse, and it is thought to involve modulation of the reflex arc (Mandl et al. 1981, Miles and Lisberger 1981).
Wolpaw's findings provide an elegant demonstration of the plasticity of the neuromuscular system, and specifically of the spinal cord's potential for lasting changes in functioning. Support for this position is provided by evidence that the isolated spinal-cord can be conditioned (Dimitrijevic et al. 1983), although such findings must be treated cautiously because of the impossibility of ensuring that all descending pathways have been elimin- ated. Wolpaw's results show that the neuromuscular system can adapt to demands for altering responsiveness, and that short-term and long-term training effects can differ both quantitatively and in terms of the mechanisms responsible.
Neilson and McCaughey (1982) demon- strated that cerebral-palsied adults can learn to alter tonic stretch reflex responsiveness. Subjects were provided with two meters, one indicating muscle contraction level and the other reflex sensitivity (an index of peak-to-peak EMG expressed as a ratio of joint angle). The subject's task was to reduce reflex responsiveness for different contraction levels. Passive, sinusoidal elbow-move- ments were used to provoke tonic stretch reflexes. Subjects completed a one-hour training session each week for a year. Results from one of the two 'predomi- nantly spastic' subjects studied show the attenuations achieved (Fig. 3). The fastest
A. S S R f '#DAY 0 120 r 4 0 i60
B. SSRJ. /DAY 0 r20
L w +,+Vh* _ _ ' ,mu
:* 7 Qh"
l a n . . C lOm*.C
Fig. 2. Long-term changes in spinal stretch reflex activity. Short-latency EMG response to stretch stimulus (upper trace) significantly increased or decreased with training, depending on whether the monkey was rewarded for boosting (A) or suppressing (BJ spinal stretch reflex (SSR) activity. (From Wolpaw and O'Keefe 1984.)
B
8:Baseline period
No reflex sensitivity display
I I t I I actidn TSR on
I I
3 N D , J F M A M J J A I S O N D J F M A M
3. Modulation of tonic stretch reJtex activity.
t
Months
P&formance without feedback during first four months indicates that subject was unable to alter tonic stretch reflex (TSRJ activity. With feedback, subject learned to enhance (TSR onJ and suppress (TSR offl responsiveness. This ability was retained when subject performed without feedback in final four months of study. (From Neilson and McCaughey 1982.1 773

E
T
.- 0 I
m CL v,
changes occurred during the first few hours, just as Wolpaw (1985) reported. After training, subjects were able to vary reflex responsiveness for a given level of contraction by up to 300 per cent. Uncontrolled spasms were less frequent and subjects were able to suppress resting tonic stretch reflexes. Tracking perform- ance was assessed before and after train- ing. Improvements were very limited, which it not surprising given the fact that the demands of active and passive movements are very different (Knutsson and Martensson 1980, Knutson 1983).
Harrison and Kruze (1 987a, b) compared the reactions of neurologically normal and spastic cerebral-palsied adults to stretch perturbations introduced while they were performing a voluntary elbow extension. Initial studies indicated that the cerebral-palsied subjects’ actions were more disrupted, antagonist activity was high, movements were jerky, and periods of clonus were common. In order to compare perturbation responses properly, subjects were trained to execute equivalent arm-swings, controlling force, velocity, starting point and the precise arc traversed (Dufresne et ai. 1978). Cerebral- palsied subjects needed up to 10 hours of training before they were able to produce the set elbow extension with stringent and reliable precision. When perturbation reactions were tested after training there was no convincing evidence that the subjects with spastic cerebral palsy were any longer hyperresponsive. Antagonist activity was greatly reduced and periods of clonus were rare. Interestingly, after training, short-latency EMG responses provoked by perturbation were elevated, and more sensitively reflected the magnitude of the disturbance. Such changes increase their value as error signals (Allum 1975). But over-a11 there was a marked reduction in prime muscle- group activity and in that of other muscles. These observations are consistent with a reduction in responsiveness to the stretch stimulus. The interpretation favoured was that in order to perform the required elbow extension skilfully, subjects had to rectify segmental responsiveness. The results of Neilson and McCaughey (1982) could be accounted for in similar terms, with training leading to reduced inter- 774
ference from other muscle groups (Day et al. 1983).
Neither of the last two studies provided subjects with as long an experience of tonic suppression as that of the monkeys in Wolpaw’s study. The improvements seen, therefore, could well be due entirely to descending modulation and fall short of the larger changes achieved later, which were attributed to alterations in segmental neuronal architecture and reactivity. Arguably, these later changes would provide the basis for more general improvements in motor control, avoiding the need for the performer to adjust each voluntary programme to incorporate measures for countering segmental hyper- responsiveness. Procedures need to be found to engineer sustained tonic shifts with human subjects, possibly by develop- ing miniaturised stimulation and feedback devices which could be worn for pro- tracted periods, or possibly by drug modulation (Young and Delwaide 1981).
It is not clear from Wolpaw’s study whether active involvement is critical, i.e. whether modulation depends on the per- former receiving feedback and working to maximise rewards, or whether passive experience would be effective in triggering segmental adaptations, using an habitu- ation model in which adjustments occur as a consequence of repeated stimulation. If active involvement proves to be essential for maximum improvement, this will limit what benefits can be expected from passive drug and movement therapies.
Rehabifitation and assessment Jankowska (1982-1983) showed that a given spinal interneuron is active when very different patterns of movement are being executed. A single aberrant com- ponent therefore could produce wide- ranging problems. And the precise nature of the difficulties observed will vary depending on the starting posture and the exact movement pattern attempted (Nwaobi et al. 1983). In terms of re- habilitation, the hope is that rectifying a limited number of aberrant units may produce wide-ranging improvements. The demonstration that segmental and supra- spinal mechanisms accommodate to con- temporary demands, however, raises the worry that rectifying a component may

sometimes have negative repercussions: systems which previously were function- ing effectively may adjust to the changes in excitatory and inhibitory forces, generating new dysfunctions.
The wide range of segmental and supraspinal factors involved in producing tonic and phasic shifts in muscle activity, combined with their multiple interactions, will make diagnosis difficult. In principle, very different patterns of abnormalities could produce indistinguishable functional impairments. Also, such complexity will make it difficult to devise clinical tests which reflect the everyday motor control problems patients experience and therapies which lead to improvements in everyday skills (Sahrmann and Norton 1977, Neilson and Lance 1978, Neilson and McCaughey 1982, Knutsson 1983, Meyer and Adorjani 1983). On the other hand, this same complexity offers hope that ways for improving motor control can be found. It may not always prove possible to rectify activity, but it may still be feasible to produce more effective functioning using unorthodox strategies. Rectifying just one aspect of a per- formance may sometimes prove counter- productive. Antagonist co-activation, for example, appears to be useful for increasing joint stabilisation when muscles are weak. In this case, unless muscle power is also improved, curbing abnormal antagonist activity is likely to jeopardise postural control. McCouch et af. (1958) investigated histological changes occurring after spinal-cord transection and attributed the spasticity which developed to afferent sprouting. Spasticity clearly interferes with normal motor control, but Goldberger (1974) speculated that hyper-reflexia also has a positive effect in promoting the return of useful limb function. Sophistication is essential, therefore, when deciding what rehabilitation goals to set.
Various secondary complications have been described in the spastic cerebral palsy syndrome, including abnormal muscle growth (Ziv et al. 1984), postural deformities (Fulford and Brown 1976), and tendon and joint abnormalities (Berger et af. 1982). These could well affect both the appropriateness and the ease of rectifying patterns of muscle
activity. From this perspective, probably the earlier training is started the better the prospects for instating skilful control.
The complex functioning of the segmental system will make it difficult to describe precisely how tasks are per- formed. A 'simple' task, such as drawing with a pencil, is very difficult to characterise in electromyographic terms. When the level of analysis is shifted to the activity profiles of spinal motoneurons and interneurons and supraspinal inputs, complexity is multiplied many-fold. To describe spastic abnormalites in such terms will require sophisticated real-time models which can do justice to the full range of inputs involved, and to the qualitative, quantitative and temporal characteristics of their interactions. Only when underlying abnormalities of the system are identified can therapy be most effectively planned (Gottlieb et al. 1982). Modern techniques, such as micro- neurography, have introduced the prospect of pin-pointing what is wrong more accurately and better evaluation of the appropriateness, strengths and weaknesses of therapeutic options.
Recent information regarding segmental organisation and neuromuscular develop- ment has shed some light on the differ- ences observed clinically between spasticity associated with congenital cerebral palsy and spastic ty originating later in life (Fisher 198 b ), and on why symptoms change with time (Gerard 1961, Kandel and Spencer 1968, Nelson and Mendell 1979, Mountcastle 1980). Patients with spastic cerebral palsy are described as a very heterogeneous group. It may be that different combinations of dysfunctions will come to be understood in terms of which subtests of interneurons are affected, and which neural and segmental contributions are abnormal. In turn, these may be explained in terms of the precise location and onset of the original brain damage, how development was affected, and the precise pattern of central and peripheral immaturities and abnormalities that resulted.
With regard to rehabilitation, many key questions remain to be answered. Which segmental anomalies can be countered by central forces? Which anomalies can be rectified by intrinsic changes in segmental 775

P
;
.- 0 I z a CA
776
functioning? Which normal functions can be mimicked, or closely approximated, by novel combinations of descending and segmental inputs? How far do strategies generalise? How often does improving the performance of one task create problems for performing others? How predictable are the negative and positive repercussions of training? Only when such information is available will it be possible to gauge the true potential of individuals with spastic cerebral palsy for learning to execute skilful discrete contractions and co- ordinated patterns of movement, and to devise efficient training schedules to realize whatever potential exists.
Precedents and speculation The existing literature on functional recovery after central nervous system (CNS) damage (Almli and Finger 1984, Finger and Almli 1984) furnishes pre- cedents for the basic tenets of the spasticity model outlined above, namely that the functional impacts of CNS damage can vary depending on the stage of development at which it is incurred; that anatomical remodelling can occur in response to damage; and that training and environmental factors can boost the degree of recovery achieved. But a review of this literature also cautions against gross generalisations. Over and over again, recovery has been shown to depend on the precise nature of the CNS damage, when it was sustained, pre- and post- trauma conditions, and the method of assessment used. Sometimes species differences are also critical.
A recent study by Michejda and Bacher (1985-1986) illustrates the startling ca- pacity of the CNS for functional recovery following extensive damage, provided conditions are appropriate. Herniation of the occipital lobes (encephalocele) of fetal monkeys was produced by administering a teratogen to the mother for three days during the first month of pregnancy. In one cohort, the experimenters operated on the fetus two-thirds of the way through pregnancy, removing the occipital encephalocele and the visual cortex con- tained in it. The cranial bifidum was then covered with a bone graft to aid healing. After birth these animals displayed no obvious visual impairments. CT scanning
revealed well-developed occipital lobes and homogeneous brain density. When studied at 18 months, although the striate cortex was poorly convoluted, it was organised in the normal columnar fashion. When surgery was delayed until shortly after birth it produced a complete loss of vision, from which the animal never recovered. Brain scanning of this group at one year of age revealed fluid- filled cavities and porencephalic lesions, and the occipital lobes were very difficult to distinguish. In this instance, the remarkable capacity of the CNS for effective functional recovery, evident in the fetus, was no longer present post- natally. The clinical literature similiarly indicates that when hemispherectomy is performed on very young children, re- organisation is possible and they develop functions normally performed by the destroyed hemisphere (Smith 1983). Brain plasticity and equipotentiality (Fletcher et al. 1984) are also evident in clinical case- reports of hydrocephalic individuals with very little viable brain matter, who nonetheless display higher levels of intellectual functioning (Lewin 1980).
Various types of neuronal changes have been observed following CNS damage, with growth and regeneration producing new cell connections, pathways and tracts. The effect is to reinstate the destroyed pathway or to generate novel connections which are never observed in a normal CNS. All functional outcomes have been described: complete recovery, some margin of improvement or various degrees of impairment (Gramsbergen and Ijkema-Paassen 1984, Steward 1984). If damage occurs before the prime develop- ment period for a function, then the prospects for complete recovery generally are greater (Almli 1984). However, if part of the supporting structure already exists, changes may be limited to ones which are consistent with residual components (Fujito et al. 1984). This would explain why the complete loss of an area is sometimes less detrimental than partial damage. As already noted, the effects of reorganisation are not always positive and it is worth considering why this is so. Although not optimal for the task con- sidered, such neuronal remodelling may be beneficial for other functions, or even

for ones which develop later (Hicks and D’Amato 1970, Prendergast and Shuster- man 1982). Some changes may simply be a response to existing forces. Indeed, it is important not to imply that the brain is able to select what changes should be generated, or to predict what impact a given change will have. A trial-and-error model may be more appropriate, with changes persisting if they prove beneficial, or being replaced by others if their impact is deleterious. One of the benefits of formal training is that feedback is unambiguous and incentives are provided for changing a performance in specified ways. For this reason, active participation by animals in the Wolpaw (1985) study may indeed lead to changes in segmental functioning which would not be produced by passive habituation.
In terms of establishing appropriate therapeutic goals, a group which deserves further study is cerebral-palsied individuals who show ‘spontaneous remission’ (Taudorf et al. 1986), to try and discover what anatomical and physiological changes underlie the remissions and what factors encourage such changes. Another consideration which stems from the general literature on recovery from CNS damage is that neuronal remodelling and functional adjustments may deplete a reserve of reorganisation potential, jeopardising later modifications (Smith 1984). This could be important when planning therapy for cerebral-palsied children. In theory, the adjustments needed to recapture early stages of development may themselves prejudice the attainment of mature functions, so normal ontogeny could be an inappro- priate model. Rather, it may be that the system should be shaped from the outset to meet mature performance demands.
Currently, however, too little is known about how motor strategies and demands change during development to make this a practical consideration.
The thrust of this paper has been to explore an explanation for various features of the spastic cerebral palsy syndrome in terms of aberrant spinal interneuronal functioning, and the prospects for achieving functional im- provements. There is abundant evidence that CNS damage can lead to the development of ectopic pathways and abnormal patterns of input. Fortunately there is also evidence that suitable training and experience can lead to changes in neuronal architecture, sensitivity and patterns of excitation and inhibition. Much remains to be discovered about which therapy goals are appropriate and realistic at different stages of develop- ment, how to encourage such changes most effectively, and the short- and long- term benefits and costs of different therapeutic procedures. Modern recording techniques have made it more likely that some of these basic and clinical questions will be answered. In coming to terms with the true complexity of motor performance and development, the hope is that more powerful therapies will emerge. Accepted for publication 16th December 1987,
Acknowledgements Preparation of this manuscript was supported by Kuwait University Grant MC015. Much of it was completed on sabbatical leave at the National Institute of Communicative Disorders and Stroke, Bethesda, Maryland; and the facilities provided by the National Institutes of Health are gratefully acknowledged. Figures 2 and 3 are reproduced by kind permission of the publishers.
Author’s Appointment Dr. Ann Harrison, Department of Community Medicine and Behavioural Sciences, Faculty of Medicine, Kuwait University, P.O. Box 24923, 13110 Safat. Kuwait.
SUMMARY The author explores the possibility that abnormal and immature spinal interneuronal circuits play a rBle in spastic cerebral palsy. Interneuronal abnormalities could account for a number of characteristic signs: sensitivity to normally innocuous stimuli, hyperreflexia, abnormal and inappropriate co-ordination patterns, and limitations in acquiring, planning, executing and correcting skilful actions. The precise pattern of interneuronal anomalies present will depend on the original site of the lesion, age at onset, and on how central and segmental development were affected. Although the number of relevant studies is very small, there are indications that long-term training can produce changes in segmental response, both by altering descending inhibition and by producing lasting changes in spinal neuronal organisation and responsiveness. Modern recording techniques have introduced the prospect of tracing immature and abnormal segmental components and of establishing their impacts on movement control.
8 i--
QI W P-
00 m 0’
777

- .- C a cn
0 .- * 2 a cn
778
RESUME In firmitt! motrice ct!rt!brale spastique: possibilitt! d’une contribution midullaire interneurale Les auteurs envisagent la possibilitk que des circuits medullaires interneuraux anormaux et immatures jouent un r6le dans la spasticitt de I’IMC. Les anomalies interneurales pourraient rendre compte d’un certain nombre de signes caracttristiques: sensibilitk A des stimuli normalement inoffensifs, hyperreflexie, groupements de coordination anormaux et inappropries, limitations dans l’acquisition, la prtvision, l’execution et la correction d’actions efficaces. Le groupement precis de anomalies interneurales recontrees pourrait dependre du site original de la lesion, de l’age de debut et de la faCon dont aurait ete affect6 le dheloppement central et segmentaire. Quoique le nombre d’ktudes sur le sujet est tres faible, il existe des tltments en faveur de l’efficience d’un apprentissage a long terme sur des modifications de la rtponse segmentaire, a la fois en alterant les inhibitions descendantes et en produisant des changements durables de l’aptitude A repondre et de l’organisation au niveau neuronal mtdullaire. Les techniques d’enregistrement modernes doivent permettre de retrouver les composantes segmentaires anormales et immatures, d’ttablir leur impact sur le contr6le du mouvement.
ZUSAMMENFASSUNG Spastische Cerebralparese: mogliche spinale interneuronale Beteiligung Der Autor untersucht die Frage, ob abnorme und unreife spinale interneuronale Verbindungen bei der spastischen Cerebralparese eine Rolle spielen. Interneuronale Anomalien konnten die Ursache fur eine Reihe charakteristischer Befunde sein: Sensibilitat fur normalerweise harmlose Reize, Hyperreflexie, abnorme und unangepdte Koordinationsmuster und die Einschrankungen beim Erlernen, Planen, Ausfuhren und Korrigieren von Geschicklichkeitsaufgaben. Das genaue Muster der vorliegenden interneuronalen Anomalien hangt ab von dem urspriinglichen Sitz der Lasion, vom Eintrittsalter und davon, wie die zentrale und segmentale Entwicklung betroffen war. Obwohl die Anzahl relevanter Studien sehr klein ist, gibt es Hinweise, daR ein Langzeittraining Verhderungen bei der segmentalen Reaktion bewirken kann, sowohl durch Veranderung der descendierenden Hemmung, als auch durch den Aufbau anhaltender Veranderungen der spinalen interneuronalen Organisation und Reaktionsfahigkeit. Durch moderne Ableitungsmethoden besteht die Moglichkeit, unreife und abnorme segmentale Komponenten herauszufinden und ihre Wirkung auf die Bewegungskontrolle einzuschatzen.
RESUMEN Paralisis cerebral espastica: posible contribucidn espinal interneuronal El autor considera la posibilidad de que 10s circuitos interneuronales espinales anormales e inmaduros puedan jugar un papel en la parllisis cerebral esplstica. Las anomalias interneuronales pueden explicar un numero de signos caracteristicos: sensibilidad a estimulos normalmente inocuous, hiperreflexia, esquemas de coordinacibn anbmalos e inapropiados y limitaciones en la adquisicion, planificacibn, ejecucibn y correccibn de acciones con destreza. El patron precis0 de la anomalias interneuronales presentes dependera del punto original de la lesibn, la edad de inicio y de hasta quk punto esta afectado el desarrollo segmentario. Aunque el numero de estudios relevantes es pequeflo, hay indicios de que un entrenamiento a largo plazo puede producir cambios en la respuesta segmentaria, alterando la inhibicion descendente y produciendo cambios duraderos en la organization neuronal espinal y en su capacidad de respuesta. Las ttcnicas modernas de registro han introducido la perspectiva de registrar 10s componentes inmaduros y segmentarios y de establacer su impacto sobre el control del movirniento.
References Allum, J. H. J. (1975) ‘Responses to load
disturbances in human shoulder muscles: the hypothesis that one component is a pulse test information signal.’ Experimental Brain Research, 22, 307-326.
Almli, C. R. (1984) ‘Early brain damage and time course of behavioral dysfunction: parallels with neural maturation.’ In Finger, S., Alrnli, C. R. (Eds.) Early Brain Damage, Vol, 2: Neurobiology and Behavior. Orlando: Academic Press.
- Finger, S. (1984) Early Brain Damage, Vol. I : Research Orientations and Clinical Observations. Orlando: Academic Press.
Angel, R. W. (1983) ‘Muscle contractions elicited by passive shortening.’ Advances in Neurology, 39,
Barolat-Romana, G., Davis, R. (1980) ‘Neuro- physiological mechanisms in abnormal refle; activities in cerebral palsy and spinal spasticity. Journal of Neurology, Neurosurgery and Psychiatry, 43, 333-342.
555-563.
Berger, W., Quintern, J., Dietz, V. (1982) ‘Pathophysiology of gait in children with cerebral palsy. ’ Electroencephalography and Clinical Neurophysiology, 53, 5 38-548.
Blakemore, C., Van Sluyters, R. C. (1975) ‘Innate and environmental factors in the development of the kitten’s visual cortex.’ Journal of Physiology,
Bobath, K. (1966) The Motor Deficit in Patients with Cerebral Palsy. Clinics in Developmental Medicine, No. 23. London: S.I.M.P. with Heinemann Medical.
Burke, D. (1983) ‘Critical examination of the case for or against fusimotor involvement in disorders of muscle tone.’ Advances in Neurology, 39,
- Hagbarth, K. E., Lofstedt, L., Wallin, B. G. (1976) ‘The responses of human muscle spindlt endings to vibration of non-contracting muscles. Journal of Physiology, 261, 613-693.
Day, B. L., Rothwell, J. C., Marsden, C. D. (1983) ‘Transmission in the spinal reciprocal la
248, 663-716.
133-1 50.

inhibitory pathway preceding willed movements of the human wrist.’ Neuroscience Letters, 31,
Delwaide, P. J., Schoenen, J., Burton, L. (1983) ‘Central actions of neurotropic drugs assessed by reflex studies in man.’ Advances in Neurology,
Dimitrijevic, M. R., Faganel, J., Lehmkuhl, D., Sherwood, A. (1983) ‘Motor control in man after partial or complete spinal cord injury.’ Advances in Neurology, 39, 915-926.
Dufresne, J. R., Soechting, J . F., Terzuolo, C. A. (1978) ‘Electromyographic response to pseudo- random torque disturbances of human forearm position.’ Neuroscience, 3, 1213-1226.
Erokhina, L. G., Rekhtman, M. B., Chekneva, N. S. (1976) ‘Interaction between peripheral motoneurons of antagonist muscles in normal subjects and spastic hemiparesis studied by the H- reflex method.’ Neuroscience and Behavioral
Finger, S., Almli, C. R. (1984) Early Brain Damage, Vol. 2: Neurobiology and Behavior. Orlando: Academic Press.
Fisher, M. A. (1983) ‘Reciprocal excitation of antagonist muscles in ‘spasticity’.’ Annals of Neurology, 14, 94-95. (Letter.)
Fletcher, J . M., Levin, H. S., Landry, S. H. (1984) ‘Behavioral consequences of cerebral insult in infancy.’ In Almli, C. R., Finger, S. (Eds.) Early Brain Damage, Vol. I : Research Orientations and Clinical Observations. Orlando: Academic Press.
Forssberg, H. (1985) ‘Ontogeny of human locomotor control. 1. Infant stepping, supported locomotion and transition to independent locomotion.’ Experimental Brain Research, 51, 480-493.
Fujito, Y., Watanabe, S., Kobayashi, H., Tsukahara, N. (1984) ‘Lesion-induced sprouting in the red nucleus at the early developmental stage.’ In Finger, S., Almli, C. R. (Eds.) Early Brain Damage, Vol. 2: Neurobiology and Behavior. Orlando: Academic Press.
Fulford, G. E., Brown, J. K. (1976) ‘Position as a cause of deformity in children with cerebral palsy.’ Developmental Medicine and Child Neurology, 18, 305-314.
Futagi, Y., Abe, J. (1985) ‘H-reflex study in normal children and patients with cerebral palsy.’ Brain and Development, 7, 414-420.
Gerard, R. W. (1961) ‘The fixation of experience.’ In Delafresnaye, J. F., Fessard, A., Gerard, R. W., Konorski, J . (Eds.) Brain Mechanisms and Learning. Oxford: Blackwell.
Goldberger, M. E. (1974) ‘Recovery of movement after CNS lesions in monkeys.’ In Stein, D. G., Rosen, J. J., Butters, N. (Eds.) Plasticity and Recovery of Function in the Central Nervous System. New York: Academic Press.
Gottlieb, G. L., Myklebust, B. M., Penn, R. D., Agarwal, G. C. (1982) ‘Reciprocal excitation of muscle antagonists by the primary afferent pathway.’ Experimental Brain Research, 46, 454-456.
Gramsbergen, A., Ijkema-Paassen, J. (1984) ‘The effects of early cerebellar hemispherectomy in the rat: behavioural, neuroanatomical, and electrophysiological sequelae.’ In Finger, S., Almli, C. R. (Eds.) Early Brain Damage, Vol. 2: Neurobiology and Behavior. Orlando: Academic Press.
Grillner, S. (1975) ‘Locomotion in vertebrates; central mechanisms and reflex interaction. Physiological Reviews, 55, 247-304.
Hagbarth, K.-E., Wallin, G., Lofstedt, L. (1973) ‘Muscle spindle responses to stretch in normal and
245-250.
39, 977-996.
PhySiOlOgy, I , 232-235.
spastic subjects.’ Scandinavian Journal of Rehabilitation Medicine, 5, 156-159.
Harrison, A., Kruze, R. (1987~) ‘Perturbation of a skilled action. 1. The responses of neurologically normal and cerebral palsied individuals.’ Human Movement Science, 6, 37-65. _ _ (19876) ‘Perturbation of a skilled action. 2. Normalisinq the responses of cerebral palsied individuals. Human Movement Science, 6,
Harrison, P. J., Jankowska, E. (1984) ‘An intra- cellular study of descending and non-cutaneous afferent input to spinocervical tract neurones in the cat.’ Journal of Physiology, 356, 245-261. _ _ (1985~) ‘Sources of input to interneurones mediating group 1 non-reciprocal inhibition of motoneurones in the cat.’ Journal of Physiology, 361, 379-401.
_ _ (19856) ‘Organization of input to the interneurones mediating group 1 non-reciprocal inhibition of motoneurones in the cat.’ Journal of Physiology, 361, 403-418. - Johannisson, T. (1983) ‘Segmental actions of afferents of the interosseous nerve in the cat. Journal of Physiology, 345, 373-389.
- Taylor, A. (1983) ‘Synaptic noise-triggered averaging as a technique for investigating the origins of EPSPs.’ Brain Research, 264, 316-319.
- Zytnicki, D. (1984) ‘Crossed actions of group 1 muscle afferents in the cat.’ Journal of Physiology, 356, 263-273. - Jankowska, E., Johannisson, T. (1983) ‘Shared reflex pathways of group 1 afferents of different cat hind-limb muscles.’ Journal of Physiology,
Hicks, S. P., D’Amato, C. J. (1970) ‘Motor-sensory and visual behaviour after hemispherectomy in newborn and mature rats.’ Experimental Neurology, 29, 416-438.
Jankowska, E. (1982-1983) ‘On the multiplicity of neuronal pathways from muscle spindles and tendon organs and their selection in the cat.’ Journal de Physiologie (Paris), 78, 772-774.
Jansen, J. K. S. (1962) ‘Spasticity-functional aspects.’ Acta Neurologica Scandinavica, 38,
Kandel, E. R., Spencer, W. A. (1968) ‘Cellular neurophysiological approaches in the study of learning.’ Physiological Reviews, 48, 65-134.
Knutsson, E. (1983) ‘Analysis of gait and isokinetic movements for evaluation of antispastic drugs or physical therapies.’ Advances in Neurology, 39,
- Martensson, A. (1980) ‘Dynamic motor capacity in spastic paresis and its relation to prime mover dysfunction, spastic reflexes and antagonist co-activation.’ Scandinavian Journal of Rehabilitation Medicine, 12, 93-106.
Landau, W. M. (1974) ‘Spasticity: the fable of a neurological demon and the emperor’s new therapy.’ Archives of Neurology, 31, 217-219.
133-159.
338, 113-128.
SUPPI. 3, 41-51.
1013-1034.
(Editorial.)
Science. 210. 1232-1234. Lewin, R. (1980) ‘Is your brain really necessary?’
Mandl, G., Melvill Jones, G., Cynader, M. (1981) ‘Adaptability of the vestibulo-ocular reflex to vision reversal in strobe reared cats.’ Brain Research, 209, 35-45.
McCouch, G. P., Austin, G. M., Liu, C. N., Liu, C. Y. (1958) ‘Sprouting as a cause of spasticity.’ Journal of Neurophysiology, 21, 205-216.
Meyer, M., Adorjani, C. (1983) ‘Quantification of the effects of muscle relaxant drugs in man by tonic stretch reflex.’ Advances in Neurology, 39, 997-1011.
00 00
2 s s e h
779

E
.Y & C
F
- .- 2 a v1
- E z P
s .- u *
2 v1
Michejda, M., Bacher, J. (1985-1986) ‘Functional and anatomic recovery in the monkey brai? following excision of fetal encephalocele. Pediatric Neuroscience, 12, 90-95.
Miles, F. A., Lisberger, S. G. (1981) ‘Plasticity i? the vestibulo-ocular reflex: a new hypothesis. Annual Review of Neuroscience, 4, 273-299.
Milner-Brown, H. S., Penn, R. D. (1979) ‘Pathophysiological mechanisms in cerebral palsy.’ Journal of Neurology, Neurosurgery and Psychiatry, 42, 606-618.
Mizuno, Y.. Tanaka, R., Yanagisawa, N. (1971) ‘Reciprocal group 1 in:bition on triceps surae motoneurons in man. Journal of Neuro- physiology, 34, 1010-1017.
Mountcastle, V. B. (1980) ‘Effects of spinal cord transection.’ In Mountcastle, V. B. (Ed.) Medical Physiology, Vol. I , 14th edn. St. Louis: Mosby.
Myklebust, B. M., Gottlieb, G. L., Agarwal, G. C. (1986) ‘Stretch reflexes of the normal infant.’ Developmental Medicine and Child Neurology,
- - Penn, R. D., Agarwal, G. C. (1982) ‘Reciprocal excitation of antagonist fnuscles as a differentiating feature in spasticity. Annals of Neurology, 12, 367-374.
Nashner, L. M., McCollum, G. (1985) ‘The organization of human postural movements: formal basis and experimental synthesis. Behavioral and Brain Sciences, 8, 135-172.
Shumway-Cook, A., Marin, 0. (1983) ‘Stance posture control in select groups of children with cerebral palsy: deficits in sensory organization and muscular coordination.’ Experimental Brain Research, 49, 393-409.
Neilson, P. D., Lance, J. W. (1978) ‘Reflex transmission characteristics during voluntary activity in normal man and patients with movement disorders.’ Progress in Clinical Neurophysiology, 4, 263-299.
- McCaughey, J. (1982) ‘Self-regulation of spasms and spasticity in cerebral palsy.’ Journal of Neurology, Neurosurgery and Psychiatry, 45, 320-330.
Nelson, S. G., Mendell, L. M. (1979) ‘Enhancement in la-motoneuron synaptic transmiyion caudal to chronic spinal cord transection. Journal of Neurophysiology, 42, 642-654.
Nwaobi, 0. M., Brubaker, C. E., Cusick, B., Sussman, M. D. (1983) ‘Elecromyographic investigation of extensor activity in cerebral- palsied children in different seating positions.’ Developmental Medicine and Child Neurology,
Prendergast, J., Shusterman, R. (1982) ‘Normal development of motor behaviour in the rat and effects of midthoracic,spinal hemisection at birth on that development. Experimental Neurology, 78, 176-189.
Prochazka, A., Hulliger, M. (1983) ‘Muscle afferent function and its significance for motor control mechanisms during voluntary movements in cat, monkey, and man.’ Advances in Neurology, 39,
28,440-449.
-
25, 175-183.
93-132. Rowlandson, P. H., Stephens, J. A. (1985)
‘Maturation of cutaneous reflex responses recorded in the lower limb in man.’ Develop- mental Medicine and Child Neurology, 27, 425-433.
Rushworth, G. (1960) ‘Spasticity a;d rigidity: an experimental study and review. Journal of Neurology, Neurosurgery and Psychiatry, 23,
- (1964) ‘Some aspects pf the pathophysiology of spasticity and rigidity. Clinical Pharmacology and Therapeutics, 5, 828-836.
Sahrmann, S. A., Norton, B. J. (1977) ‘The relationship of voluntary movement to spasticity in the upper motor neuron syndrome.’ Transactions of the American Neurological Association, 102, 108-1 12.
Sherrington, C. S. (1909), ‘On plastic tonus and proprioceptive reflexes. Quarterly Journal of Experimental Physiology. 2, 109-156.
Smith, A. (1983) ‘Overview or “underview”? Comment on Satz and Fletcher’s “Emergent trends in neuropsychology: An overview”.’ Journal of Consulting and Clinical Psychology.
- (1984) ‘Early and long-term recovery from brain damage in children and adults: Evolution of concepts of localization, plasticity, and recovery. In Almli, C. R., Finger, S. (Eds.) Early Brain Damage, Vol. I : Research Orientations and Clinical Observations. Orlando: Academic Press.
Steward, 0. (1984) ‘Lesion-induced neuroplasticity and the sparing or recovery of function following early brain damage.’ In Almli, C. R., Finger, S. (Eds.) Early Brain Damage, Vol. I : Research Orientations and Clinical Observations. Orlando: Academic Press.
Taudorf, K., Hansen, F. J., Melchior, J. C., Pedersen, H. (1986) ‘Spontaneous remission of cerebral palsy.’ Neuropediatrics. 17, 19-22.
Thelen, E. (1986) ‘Treadn$l-elicited stepping in seven-month-old infants. Child Development,
- Cooke, D. W. (1987) ‘Relationship between newborn stepping and later walking: a new interpretation. Developmental Medicine and Child Neurology, 29, 380-393.
Wolpaw, J. R. (1985) ‘Adaptive plasticity in the spinal stretch reflex: an accessible substrate of memory?’ Cellular and Molecular Neurobiology,
99-1 18.
51, 768-775.
57, 1498-1506.
5, 147--165. - O’Keefe, J. A. (1984) ‘Adaptive plasticity in the
primate spinal stretch reflex:-evidence for a two- Dhase Drocess.’ Journal of Neuroscience, 4, 2718-2i24.
Young, R. R., Delwaide, P. J. (1981) ‘Spasticity.’ New England Journal of Medicine, 304, 28-33, - 96-99.
Ziv, I., Blackburn, N., Rang, M., Koreska, J. (1984! ‘Muscle growth in normal and spastic mice. Developmental Medicine and Child Neurology, 26, 94-99.
780