-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
1/26
Combating AMR in
Primary Carepractical antimicrobial therapy forcommon infection
in primary care setting
Dr Leong Kar NimMBBS (India) MRCP (Ireland)
Consultant Infectious Diseases
Infectious Disease Unit
Hospital Pulau Pinang
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
2/26
Percentage of Abs usage
Acute bronchitis 78%
Acute phranyngitis 65%
Acute sinusitis 81%
Nonspecific URI 33%
Broad spectrum Abs 56%
Family Medicine 2006; 38(5):349-54
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
3/26
Outpatient Antibiotic Use andPrevalence of Antibiotic-
Resistant Pneumococci inFrance and Germany: A
Sociocultural PerspectiveStephan Harbarth,* Werner Albrich, and
Christian Brun-Buisson
The prevalence of penicillin-nonsusceptible pneumococci is
sharply divided between France (43%) and
Germany (7%). These differences may be explained on different
levels: antibiotic-prescribing practices for
respiratory tract infections; patient-demand factors and
health-belief differences; social determinants,
including differing child-care practices; and differences in
regulatory practices. Understanding these deter-
minants is crucial for the success of possible interventions.
Finally, we emphasize the overarching impor-
tance of a sociocultural approach to preventing antibiotic
resistance in the community.
Emerging Infectious Diseases Vol. 8, No. 12, December 2002
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
4/26
Strep pneumo
sensitivity pattern in
Germany vs France
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
5/26
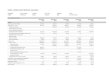
Out patient antibiotic
utilization data
Figure 3. Outpatient antibiotic utilization (18,19), France and
Germany,19851997. DDD, daily defined doses.
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
6/26
Findings:
In Germany :
lower antibiotic consumption
narrow-spectrum antibiotics
higher dosing of amino-penicillins
better treatment compliance
Lower rates of resistant pneumococcus
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
7/26
MANAGEMENT OF COMMONINFECTION IN PRIMARY CARE
SETTINGS
Adapted from CDC and UK guidelines
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
8/26
Aim :
A simple, empirical approach to the treatment of common
infections which require antibiotics in outpatient setting
Promote the safe, effective and economic use of antibiotics
Minimise the emergence of bacterial resistance in the
community
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
9/26
General principles:
Lower threshold for antibiotics in immunocompromised hosts
or those with multiple morbidities; consider culture and
seek
advice
Prescribe an antibiotic only when there is likely to be a
clearclinical benefit
Consider NO antibiotic strategy for acute self-limiting
upper
respiratory tract infections
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
10/26
Use narrow spectrum antibiotics when possible
Avoid broad spectrum antibiotics eg co-amoxiclav, quinolones
and cephalosporins
Avoid widespread use of topical antibiotics e.g. fusidic
acid
Where a best guess therapy has failed or special
circumstances exist, seek advice from
Physicians/ID/ClinicalMicrobiologists.
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
11/26
Common RTI in Primary Care
Acute pharyngitis
Non specific URTI/ILI
Acute bacterial rhinosinusitis
Acute bronchitis
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
12/26
Acute pharyngitis
Only 5-15% of adult cases of acute pharyngitis are caused by
GABHS (Group A -haemolytic strep)
Antibiotic therapy of GABHS hastens resolution by 1-2 days
if
initiated within 2-3 days of symptom onset.
Centor criteria :
History of fever
Lack of cough
Tonsillar exudates
Tender anterior cervical adenopathy
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
13/26
Patients with none or only one of these findings should NOT
be tested or treated for GABHS.
Rapid streptococcal antigen test (RAT) is recommended for
patients with two or more criteria, with antibiotic therapy
only
if test is positive Treatment :
Penicillin V 500 mg1 gm QID 10 days
Clarithromycin 250-500 mg BD 5 days
Extended BL-BLI / FQ are not indicated
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
14/26
Non specific URTI
The common cold is caused by viral pathogens eg rhinovirus,
parainfluenza, adenovirus, RSV and influenza
Bacterial rhino-sinusitis complicates only about 2% of
cases.
Symptoms may last up to 14 days with an average of 7 to 11
days
Purulent nasal secretions do not predict bacterial sinusitis
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
15/26
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
16/26
Common cold resolves without antibiotic treatment.
Treatment with an antibiotic does NOT shorten the duration
of illness nor prevent bacterial rhinosinusitis.
Patients with purulent green or yellow secretions do not
benefit from antibiotic treatment.
Cough suppressants have limited efficacy for relief of cough
Acute cough associated with the common cold may be
relieved by antihistamines and decongestants
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
17/26
Suspected Influenza
Annual vaccination is essential for all those at risk
ofinfluenza.
Pregnant (including 2 weeks post partum)
> 65 years
chronic respiratory disease (including COPD and asthma)
significant cardiovascular disease (not
hypertension),immunocompromised
diabetes mellitus
chronic neurological
renal or liver disease Treat only at risk patientswithin 48
hours of onset or in a
care home where influenza is likely.
Oseltamivir 75 mg bd x 5 days
Zanamivir 10 mg BD (2 inhalations by diskhaler) x 5 days
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
18/26
Acute bacterial rhino-sinusitis
Acute maxillary and ethmoid rhinosinusitis
Most cases of acute rhinosinusitis are due to uncomplicated
viral infections
Most rhinovirus colds last 7 to 11 days (J Clin
Microbiol1997;
35:2864;JAMA 1967; 202:158).
Bacterial rhinosinusitis may be present if symptoms have
beenpresent >7 days and there is localization to the maxillary
sinus.
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
19/26
Most patients will improve without antibiotic treatment.
About 81% of antibiotic-treated patients and 66% of controls
improved at 10-14 days (absolute benefit of 15%).
Patients with mild symptoms should NOT receive antibiotics.
Use a narrow spectrum agent that covers S. pneumoniae and
H. influenzae
Amoxicillin 500 mg TDS X 7 days
Doxycycline 100 mg BD X 7 days Consider second line agent if no
improvement or worsening after
72 hours. Co amoxy Clav 625 mg TDS X 7 days
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
20/26
Acute bronchitis
Acute coughing illness last for 3 weeks
Greater than 90% of cases of acute cough illness are non-
bacterial.
Viral etiologies include influenza, parainfluenza, RSV, and
adenovirus.
Bacterial agents include Bordatella pertussis, Mycoplasma
pneumoniae, and Chlamydophila pneumoniae.
Purulent sputum not predictive of bacterial infection.
>95% of patients with purulent sputum do not havepneumonia (J
Chron Di1984; 37:215)
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
21/26
Empiric antibiotic treatment is not indicated for acute
bronchitis.
Meta-analyses of randomized, controlled trials all concluded
that routine antibiotic treatment is not justified (BMJ
1998;316:906; Chest2006;129:95S-103S). Antibiotic treatment
decreases transmission but has little
effect on symptom resolution.
If influenza therapy is considered, it should be initiated
within
48 hours of symptom onset for clinical benefit.
Treatment:
Amoxycillin 500 mg TDS X 5 days
Doxycycline 200 mg stat and 100 mg OD X 5 days
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
22/26
Acute exacerbation of COPD
Treat exacerbations promptly with antibiotics only if
purulent
sputum and increased shortness of breath and/or increased
sputum volume
Risk factors for antibiotic resistant organisms (penicillin
R)
include co-morbid disease, severe COPD, frequentexacerbations,
antibiotics in last 3 months
Treatment: 5 days
Amoxicillin 500 mg TDS
Doxycyline 200 mg / 100 mg BD
Clarithromycin 500 mg BD
If resistance risk factors:
co-amoxiclav 625 mg TDS
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
23/26
Urinary Tract Infection
Do not use prophylactic antibiotics for catheter changes
unless
history of catheter-change-associated UTI
Do not treat asymptomatic bacteriuria; it is common but is
not associated with increased morbidity, especially
elderlypatient
Catheter in situ: antibiotics will not eradicate
asymptomatic
bacteriuria; only treat if systemically unwell or
pyelonephritislikely
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
24/26
UTI in women with severe symptoms (fever, dysuria and flank
pain): treat with empirical antibiotic
Women mild/or 2 symptoms: use dipstick to guide
treatment.
Nitrite & blood/leucocytes has 92% positive predictive value
; -ve nitrite, leucocytes, and blood has a 76% NPV
Men: send pre-treatment MSU culture OR if symptoms
mild/non-specific, useve nitrite and leucocytes to exclude
UTI
Empirical Therapy : 3-5 days in women ; in men 7 days
Co Amoxy Clav
Unasyn
Cefuroxime
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
25/26
TIPS for not overusing
antibiotics in primary care Tell patients that antibiotic use
increases the risk of an
antibiotic- resistant infection.
Identify and validate patient concerns.
Recommend specific symptomatic therapy.
Spend time answering questions and offer a contingency plan
if symptoms worsen.
Provide patient education materials on antibiotic
resistance.
-
7/29/2019 Speaker 5 - Dr Leong Combat AMR Primary Care
26/26
REMEMBER:
Effective communication ismore important than an
antibiotic for patientsatisfaction.