Embed Size (px)
Citation preview
Special KWhat Evidence for Infusions is “Bursting” at the Seams?
Sukhjinder SidhuInterior Health Pharmacy Resident
October 10, 2013

Session Objectives• Become familiar with:
– The MOA of ketamine as an analgesic– The common dosing regimens for subcutaneous
ketamine infusions– The most common adverse effects
• Be able to explain the evidence behind SC ketamine infusions in palliative care
• Be able to describe monitoring parameters for a patient receiving SC ketamine infusion for pain control
Background
• Rationale for ketamine use:– At subanesthetic doses, a synergistic effect
between ketamine and opioids has been observed in patients who are already receiving high doses of opioids
– Currently at RIH, it is used in palliative cancer pain that has failed to respond fully to opioids
http://www.yacpalliativecare.co.uk/documents/download25.pdfJ Pain Symptom Manage; 2011 Mar;41(3):640-49

Background
• MOA of ketamine:– Inhibition of NMDA receptors where it blocks
excitatory nerve activity– Agonist activity at opioid mu receptors – Inhibition of glutamate receptors facilitating GABA– Inhibition of synaptic re-uptake of monoamines– Modulates central sensitization and hyperalgesia
• Onset of action is 15-30 minutes within initiation of SC infusion
http://www.yacpalliativecare.co.uk/documents/download25.pdfJ Pain Symptom Manage; 2011 Mar;41(3):640-49
All Gwent Palliative Medicine Consultants Group July 2010

Background• Subcutaneous dosing regimens:
– 1 – 2.5 mg/kg/24 hr, then increase by 50 – 100 mg/24 hr (max 3.6 g/24 hr)
– Burst:
J Pain Symptom Manage; 2011 Mar;41(3):640-49
Background
• Contraindications– Absolute
• Intracranial HTN• Seizures• Neurological impairment
– Relative• HTN• Cardiac failure• Previous CVA
J Pain Symptom Manage; 2011 Mar;41(3):640-49All Gwent Palliative Medicine Consultants Group July 2010

Background• Adverse effects of ketamine:
– Increased muscle tone
– Tachycardia– Hypertension– Diplopia– Nystagmus
– Neuropsychiatric • Dysphoria• Hallucinations• Nightmares
– Sedation– Confusion– Disorientation– Delirium– Dizziness
http://www.yacpalliativecare.co.uk/documents/download25.pdfJ Pain Symptom Manage; 2011 Mar;41(3):640-49
Niesters M et al. Br J Clin Pharmacol. 2013 Feb; n/a-n/a

Clinical Question
• In an adult palliative patient with uncontrolled pain on optimal doses of opioids, are subcutaneous ketamine infusions as adjuvants to opioids more effective for pain relief and improve quality of life without increasing the risk of adverse events compared to opioids alone?

Literature SearchDATABASE Google Scholar, PubMed, Embase, Cochrane
SEARCH TERMS KetaminePain, intractable; pain; palliative AnalgesiaCancer; neoplasmsNOT pediatricNOT surgery
RESULTS 4 RCTs1 Cochrane Review3 Reviews2 Non-RCTs5 Case Studies1 Chart Audit1 Site Specific Guideline/Protocol
FOR REVIEW 2 RCTs1 Case Series

Salas et al.Design Prospective, randomized, double-blind, placebo-controlled
Population Inclusion:•> 18 y.o with cancer pain refractory to standard opiates •NPIS > 4/10 after 24 hrs of continuous IV morphine•Histological diagnosis of cancer (locally advanced/metastatic)•Hospitalization in a specific palliative care unitExclusion:•CI to use of ketamine•WHO performance status > 3•Sleepiness score > 16 on Epworth Slumber ScaleBaseline:N 20; age ~ 60; pain 5.8/10; Epworth Slumber Scale 9/11
Intervention Ketamine (0.5 mg/kg/day, then 1 mg/kg/day after 24 hrs) + morphine IV vs. saline + morphine IV
Primary Outcome
Change of pain level between baseline and 2 hours after baseline using NPIS
J Palliat Med. 2012 Feb;15(3):287-93

Salas et al. ResultsΔ from
baseline at 2 hrs
Δ from baseline at 24
hrs
Δ from baseline at 48
hrs
Patients with ↓ pain
Ketamine 36.4% 30.0% 50.0%
Placebo 22.2% 33.3% 25.0%
Self-reported pain
Ketamine - -1.95 + 2.82 -1.65 + 3.27
Placebo - -0.22 + 2.72 -0.38 + 2.72
Nausea, Tiredness, Depression, Anxiety, Drowsiness, Lack of appetite, Well-being, SOB, Sleepiness
- NSS NSS
Side effects - - NSS
J Palliat Med. 2012 Feb; 15(3):287-93

Salas et al. Limitations• Sample size small
– Moderate efficacy may have been missed due to low statistical power
• Short study period of 48 hours• Ketamine doses were lower than standard used at
RIH – 23 – 43 mg vs. 100 – 500 mg – Too low to detect a difference?
• Daily morphine doses could be increased daily by 50% if necessary
• No assessment of other comorbidities
J Palliat Med. 2012 Feb; 15(3):287-93

Hardy et al.Design Multi-site, dose-escalation, double-blind, randomized, placebo-
controlled phase III trial
Population Inclusion:•> 18 y.o. palliative patients•Refractory chronic pain secondary to cancer•BPI > 3Exclusion:•Received ketamine within 6 months for pain •Radiotherapy to pain site within 2 weeks•Any other procedures/therapies likely to affect painBaseline:N 185; age ~63; ~56% male; 300/410 mg morphine equivalent; average BPI score 5.3; median performance status 60%
Intervention Ketamine SC with dose titration over 5 days (100, 300, 500 mg) + opioids vs. placebo + opioids
Primary Outcome
Improvement in pain at end of 5-day study period
J Clin Oncol. 2012 Sep 10;30(29):3611-7

Hardy et al. ResultsKetamine Placebo Outcome
Improvement in pain (5 days)
27% 31% NSS
Worst pain score 5.30 6.01 SS
Average pain score 3.11 3.49 NSS
Least pain score - - NSS
Breakthrough dosing
2 (1-4)
3(1-4)
NSS
Adverse events 172 103 SS
- Most common adverse events = lightheadedness, hypoxia, and somnolence
- Serious adverse event included bradyarrhythmia and cardiac arrest
- Pyschotoxicity risk increased each day with ketamine use, becoming significant after day 3 (OR 2.53; 95% CI 1.11 to 5.78; p = 0.027).
J Clin Oncol. 2012 Sep 10;30(29):3611-7

Hardy et al. Limitations
• Short study period– No data on long-term benefits/risks of ketamine
use
• Did not assess control of other comorbidities • Small population studied
J Clin Oncol. 2012 Sep 10;30(29):3611-7

SummarySalas et al. Hardy et al.
Pain relief NSS NSSWorst pain score - SS
Increase quality of life NSS ?
Adverse events NSS SS
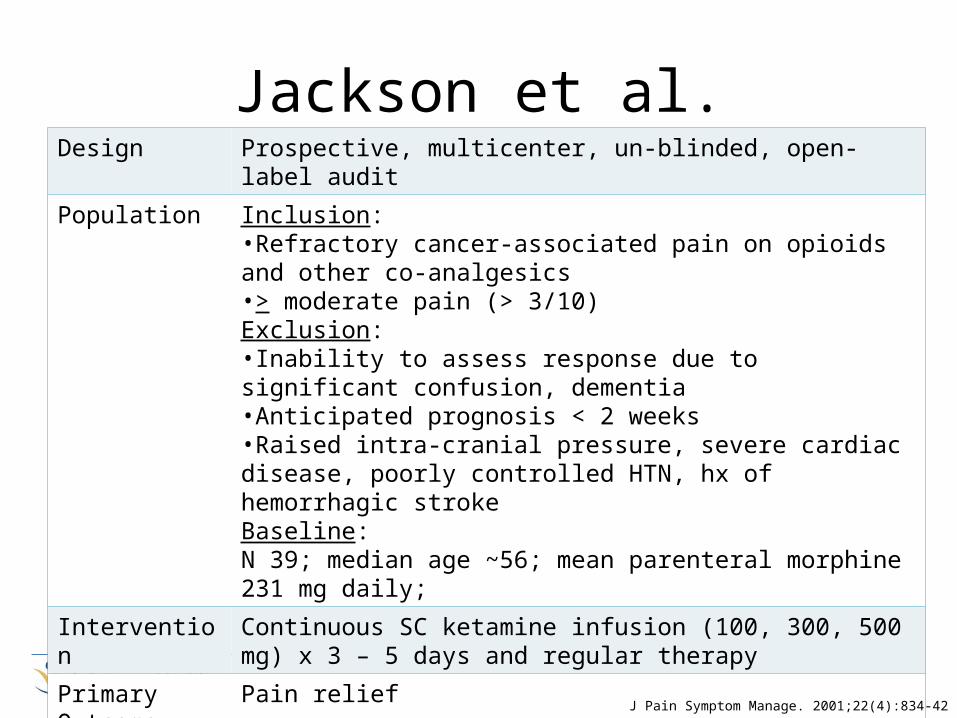
Jackson et al.Design Prospective, multicenter, un-blinded, open-label audit
Population Inclusion:•Refractory cancer-associated pain on opioids and other co-analgesics•> moderate pain (> 3/10)Exclusion:•Inability to assess response due to significant confusion, dementia•Anticipated prognosis < 2 weeks•Raised intra-cranial pressure, severe cardiac disease, poorly controlled HTN, hx of hemorrhagic strokeBaseline:N 39; median age ~56; mean parenteral morphine 231 mg daily;
Intervention Continuous SC ketamine infusion (100, 300, 500 mg) x 3 – 5 days and regular therapy
Primary Outcome
Pain relief
J Pain Symptom Manage. 2001;22(4):834-42

Jackson et al. Results• Overall response 67%
– 15/17 somatic– 14/23 neuropathic
• After cessation of ketamine, of those that responded, 24/29 maintained good pain control (8 weeks)
• 12 reported adverse psychomimetic effects; risk increasing with dose– 6 “spaced out” feeling– 3 hallucinations– 2 drowsiness– 1 dizziness
J Pain Symptom Manage. 2001;22(4):834-42

Jackson et al. Limitations
• Study design lower on hierarchy (#3) – Potential for confounders and bias
• No comparator group to conclude if results are statistically significant
J Pain Symptom Manage. 2001;22(4):834-42

Conclusion• Inconclusive evidence as to the effects of ketamine on pain and
quality of life– Higher quality studies are required– Palliative, especially end-of-life, difficult to conduct studies
• No studies stratified using PPS– Unknown if certain functional capacity will benefit
• It would be appropriate to trial burst ketamine infusion in palliative patients with severe pain refractory to opioids as a last ditch effort– Case by case – not all refractory patients will find benefit– Ensure all pain and adjuvant therapies have been optimized– Important to reiterate to patient the current evidence– Ensure healthcare team objectively evaluates outcomes
• Important to not provide false hope

Practical Question
• When initiating ketamine infusion opioids should be decreased by 25-50% for safety as ketamine decreases opioid tolerance…
• But practically, can you accomplish this in patients with uncontrolled severe pain?
Monitoring Plan
• Pain, BP, HR, RR– Day 1: baseline; 30 min, 1 hour, 4 hour– If relative CI or on long-acting opioids: Q4H until
dose titration complete– All others: daily
• Dysphoria, hallucinations, delirium– Baseline and on-going while on therapy
• Drug interactions as CYP3A4 substrate

ReferencesHardy J, Quinn S, Fazekas B, Plummer J, Eckermann S, Agar M, et al. Randomized, Double-Blind,
Placebo-Controlled Study to Assess the Efficacy and Toxicity of Subcutaneous Ketamine in the Management of Cancer Pain. J Clin Oncol. 2012 Sep 10;30(29):3611–7.
Jackson K, Ashby M, Martin P, Pisasale M, Brumley D, Hayes B. “Burst” Ketamine for Refractory Cancer Pain: An Open-Label Audit of 39 Patients. J Pain Symptom Manage. 2001;22(4):834–42.
Ketamine use in chronic pain. Available from: www.yacpalliativecare.co.uk/documents/downloads25.pdf
Niesters M, Martini C, Dahan A. Ketamine for Chronic Pain: Risks and Benefits: Ketamine risks and benefits. Br J Clin Pharmacol. 2013 Feb;n/a–n/a.
Pain management – ketamine infusions for adult patients with acute and chronic non malignant pain. Available from: www.seslhd.health.nsw.gov.au
Quibell R, Prommer EE, Mihalyo M, Twycross R, Wilcock A. Ketamine*. J Pain Symptom Manage. 2011 Mar;41(3):640–9.
Salas S, Frasca M, Planchet-Barraud B, Burucoa B, Pascal M, Lapiana J-M, et al. Ketamine Analgesic Effect by Continuous Intravenous Infusion in Refractory Cancer Pain: Considerations about the Clinical Research in Palliative Care. J Palliat Med. 2012 Feb;15(3):287-93.