Embed Size (px)
Citation preview

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlightMEDICARE ADVANTAGE 2011 DATA SPOTLIGHT
Special Needs Plans: Availability and Enrollment
Prepared by Marsha Goldi; and Gretchen Jacobson, Anthony Damico, and Tricia Neumanii
SEPTEMBER 2011
Special Needs Plans (SNPs), a form of Medicare Advantage plan, were authorized in 2003 to provide a managed care option for three groups of beneficiaries with significant or relatively specialized care needs, including Medicare beneficiaries who are dually eligible for Medicare and Medicaid (dual eligibles), beneficiaries living in nursing homes or other institutions, and beneficiaries with severe chronic or disabling conditions. Beneficiaries who are eligible to enroll in SNPs tend to have significant medical and support needs and use more services than others. As a result, they account for a disproportionate share of Medicare spending.1 With growing concern over rising health care costs and the management of care provided to beneficiaries with significant needs, policymakers are pursuing a number of strategies through interventions targeted to beneficiaries in the fee‐for‐service Medicare program, and through managed care plans, such as SNPs.
In this Spotlight, we begin by providing background information on SNPs, and then review trends in SNP availability and enrollment. In addition, with emerging interest in strategies designed to improve care for dual eligibles, we take a closer look at plans that are designed specifically for beneficiaries enrolled in both Medicare and Medicaid.2 The 2011 analysis is based on data published in the 2011 CMS Landscape files and March 2011 CMS Medicare Advantage enrollment report.
Today, nearly 1.3 million Medicare beneficiaries are enrolled in SNPs – equivalent to 11 percent of the Medicare Advantage population and 3 percent of the total Medicare population. SNP enrollment has remained fairly constant since 2007, despite a steady decline in the number of plans offered nationwide since 2008. Today, as in previous years, the majority of SNP enrollees are in plans for dual eligibles. Over the past few years, the number of beneficiaries enrolled in institutional and chronic condition SNPs has steadily declined, consistent with a decline in the number of plans available to serve these populations. In 2011, one or more SNPs are offered in one or more counties in all but 8 states, but enrollment is distributed very unevenly across states. SNPs currently play a relatively small role in the Medicare program, but have the potential to play a larger role as federal and state policymakers consider how to enhance care coordination and management for high‐cost, high‐need populations. BACKGROUND
SNPs, authorized in the Medicare Prescription Drug Improvement and Modernization Act (MMA) of 2003, are a specific type of Medicare Advantage plan that is permitted to limit enrollment to subgroups of Medicare beneficiaries of three types: (1) those dually eligible for Medicare and Medicaid; (2) those who require an institutional level of care; and (3) those with severe or disabling chronic conditions. SNPs can be health maintenance organizations (HMOs), local preferred provider organizations (PPOs) or regional PPOs; most, however, are HMOs. Unlike other types of Medicare Advantage plans, SNPs are required to integrate prescription drug coverage (Part D) within the plan.3
The rationale for SNPs is that specialization will help to achieve economies of scale and improve the coordination of care for Medicare beneficiaries with extensive and diverse needs that may not currently be well served either within regular Medicare Advantage plans or traditional Medicare. As initially authorized, the legislation applied the same regulatory requirements to SNPs as other Medicare Advantage plans, with relatively little specificity on how eligible enrollees were to be defined or how care was to be managed.
Author affiliations: i Mathematica Policy Research; ii Kaiser Family Foundation
special NeeDs plaNs: availability aND eNrollmeNt

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 2
The Medicare Improvements for Patients and Providers Act (MIPPA) of 2008 required SNPs to submit models of care, and restricted the types of chronic conditions that could be served by SNPs. The Centers for Medicare and Medicaid Services (CMS) subsequently issued guidance to plan sponsors specifying how to meet these new requirements.4 According to MedPAC, the models of care submitted by dual eligible SNPs include “very little discussion of the key elements of care coordination” and vary considerably in content.5
Building on new authority granted in the Patient Protection and Affordable Care Act of 2010 (ACA), the new Medicare‐Medicaid Coordination Office is examining and testing various models to improve care for dual eligibles,6 and is working with states to explore ways of supporting alternative care management strategies for dual eligibles.7 SNPs are considered by some to be a promising strategy for improving the coordination of care for dual eligibles and other high‐need, high‐cost beneficiaries.
TRENDS IN SNP AVAILABILITY AND ENROLLMENT NATIONAL TRENDS
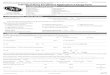
Number of SNPs. From a peak of 772 SNPs in 2008, the number of SNPs has declined by nearly half to 409 in 2011, of which 256 plans are for the dually eligible, 61 plans are for beneficiaries requiring an institutional level of care, and 92 plans are for beneficiaries with chronic conditions – mostly diabetes, chronic heart failure, or cardiovascular disorders (Exhibit 1).8 Fewer institutional SNPs are available in 2011 than in any year since 2007. Most SNPs (91%) are organized under an HMO contract, but 7 percent are under local PPO contracts and 3 percent are offered under regional PPO contracts (Table A1).
SNP Enrollment. SNP enrollment increased rapidly at the beginning of the program but has grown much more slowly since then (Exhibit 2; Table A2). In 2011, 1.3 million Medicare beneficiaries (3 percent of all Medicare beneficiaries) are enrolled in SNPs, up 2 percent from 2010 and 19 percent since 2007. In contrast, overall Medicare Advantage enrollment has more than doubled (42 percent) since 2007.9 Dual SNPs provide coverage to roughly 10 percent of all Medicare beneficiaries who are also covered under the Medicaid program, excluding Puerto Rico and other territories.
Enrollment by Plan Type. Of the three types of SNPs authorized, dual eligible plans are by far the most common. Four out of five SNP enrollees (81 percent) are in dual SNPs in 2011. While dual eligible SNPs have dominated SNP enrollment from the start, they are even more of a dominant force in the SNP market today as their enrollment continues to grow and enrollment in other types of SNPs erodes.
EXHIBIT 1
224312
440 408337
256
35
84
8987
74
6112
71
243210
151
92271
467
772705
562
409
2006 2007 2008 2009 2010 2011
Chronic ConditionsInstitutionalDual Eligibles
Number of Special Needs Plans, by Type, 2006 – 2011
NOTE: Includes Puerto Rico and other territories.SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment files, 2006‐2011.
EXHIBIT 2
439
752 853 901 968 1,045 22
145 130 118
95 79
70
184 205
251 201 160
532
1,081 1,188
1,271 1,264 1,284
2006 2007 2008 2009 2010 2011
Chronic ConditionsInstitutionalDual Eligibles
Number of Beneficiaries in Special Needs Plans, by Type, 2006 – 2011
Number of Beneficiaries in SNPs, in thousands
NOTE: Numbers may not sum to the total due to rounding. Includes enrollment in Puerto Rico and other territories.SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment files, 2006‐2011.

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 3
Enrollment in dual eligible SNPs has been gradually increasing since 2007, after a significant jump in enrollment between 2006 and 2007. In 2011, over 1 million Medicare beneficiaries are in dual eligible SNPs, up by roughly 77,000 from 2010, or 8 percent. Enrollment patterns and trends for dual SNPs differ substantially from state to state based in part on differences in state Medicaid policy and other state characteristics.10 The market share among dual eligible SNPs is more diffuse than the general Medicare Advantage market or other SNP markets, and no one firm dominates dual SNP enrollment. Together, the top two firms in the dual Medicare Advantage market (United Healthcare and Aveta) have only a quarter (25 percent) of dual eligible SNP enrollment, with one (Aveta) specializing on Puerto Rico (Table A3).
Enrollment in institutional SNPs was never very high, reaching a peak of 144,928 in 2007 and falling by almost half to 78,666 in 2011. Almost all beneficiaries enrolled in institutional SNPs are affiliated with two firms: United Healthcare and SCAN (Table A3).
Enrollment in chronic care SNPs reached a high of 251,212 in 2009 but fell thereafter. In 2011, 160,034 beneficiaries are enrolled in chronic care SNPs, down 21 percent from 2010 and 36 percent since 2009. The decline in plans offered and enrollment coincides with CMS’s change in policy on the types of chronic conditions that qualify as the basis for eligibility in these SNPs, a response to new requirements in MIPPA. Almost half (48 percent) of 2011 enrollment in chronic care SNPs is in plans offered by one firm: XLHealth (Table A3).
GEOGRAPHIC DISTRIBUTION
SNP Enrollment and Penetration by State. Nationwide, just 2 percent of all Medicare beneficiaries (excluding Puerto Rico), and 10 percent of all Medicare Advantage enrollees, currently receive their Medicare benefits from a SNP (Exhibit 3). In 5 states (AZ, AR, AL, SC, and MD) and the District of Columbia, more than 15 percent of the enrollees in Medicare Advantage plans are in SNPs. However, in most states, fewer than 6 percent of all Medicare Advantage enrollees are in SNPs. Eight states have no SNP enrollees: Alaska, Montana, New Hampshire, North Dakota, South Dakota, Vermont, West Virginia, and Wyoming. SNP enrollment rates are relatively low because most beneficiaries do not meet the eligibility criteria of being dual eligible, live in an institution, or have certain chronic conditions. And even if eligible, not all beneficiaries live in an area where SNPs are offered. Among the majority of states with SNP enrollees, all but Rhode Island have enrollees in dual eligible SNPs. (SNP enrollment in Rhode Island is limited to institutional SNPs.) In 28 states and the District of Columbia, some beneficiaries are enrolled in institutional SNPs. Just three fewer states (25 states and the District of Columbia) have some beneficiaries enrolled in chronic condition SNPs (Table A4).
SNP enrollment in Puerto Rico. SNPs are very common in Puerto Rico, which operates under modified payment rules that have enhanced enrollment in Medicare Advantage.11 Almost all dual eligibles in Puerto Rico (97%) are enrolled in dual SNPs, and about one‐third (34%) of Medicare beneficiaries in Puerto Rico are dually eligible for Medicare and Medicaid. Of the 1.3 million enrollees in SNPs, 228,734, (18 percent) are in Puerto Rico in 2011. (Other territories do not have SNPs.)
EXHIBIT 3
Share of Medicare Advantage Enrollees in Special Needs Plans, by State, 2011
<1% ‐ 5%(19 states)
6% ‐ 10%(8 states)
11% ‐ 15%(10 states)
> 15%(5 states + DC)
No MA enrollees in SNPs(8 states)
National Average, 2011 = 10%
NOTE: Puerto Rico and territories are excluded from the national average.SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment files, 2011.
DC
19%
0%
19% 16%
12% 5%
5%
14%
12%
12%
10%
2%
4% 1%1%
2% 8%
8%
8%
18%
9%
13%
11%
6%
0%
1%2%
0%
4%
4%
11%
4%
0%
2%
1%
7%
11%2%
21%
0%
15%
14%
6%
0%
1%
3%
0%
0%
18%
4%2%

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 4
Enrollment in Dual Eligible SNPs. Institutional and chronic SNPs have relatively few enrollees so much of the SNP market is driven by the dual eligible SNPs. In 2011, only about 10 percent of all dual eligibles are in a dual SNP, but the share within each state varies widely (Exhibit 4). Arizona has the largest share of its dual eligibles enrolled in dual SNPs (43%), followed by Minnesota (33%) and Hawaii (31%). In Oregon, Pennsylvania, and Utah, more than 20 percent of dual eligibles are in a SNP in 2011. In contrast, in 18 states, less than 2 percent of dual eligibles are enrolled in SNPs (Table A4).
MARKET CONCENTRATION
SNP Enrollment by Firm. Enrollment in the SNP market, like the Medicare Advantage market overall, is disproportionately concentrated in a small number of firms; however, major players in the SNP market are not necessarily the same as in Medicare Advantage overall (Table A4). United Healthcare, which has the highest general Medicare Advantage enrollment of any firm,12 also has the largest SNP enrollment, but some other dominant firms in Medicare Advantage, such as Humana and most BCBS affiliates, have a smaller presence
Understanding the Role of Medicare Advantage Plans for Dual Eligibles
Not all enrollees in dual SNPs are dual eligibles. While SNPs for the dual eligibles were originally designed to serve the dually eligible population, some SNPs for the duals (“disproportionate percentage SNPs”) were permitted to continue to serve non‐dual eligible enrollees after the plan converted to a SNP. CMS has estimated that between 25 and 40 percent of Medicare beneficiaries in these plans are not dual eligibles. These plans can continue to serve current enrollees who are non‐special needs members, but are required to limit enrollment of new non‐special needs members to no more than 10 percent of new enrollees.
Not all dually eligible Medicare Advantage enrollees are in SNPs; some dual eligibles are enrolled in other types of Medicare Advantage plans. In fact, roughly half of all dual eligibles in Medicare Advantage plans are enrolled in plans that are not SNPs and are open to all Medicare beneficiaries, according to a Kaiser Family Foundation analysis of the 2008 Medicare Current Beneficiary Survey (MCBS) Access to Care File. The fact that dual eligibles are in Medicare Advantage plans that are not SNPs may not be a concern. However, it does limit the ability of the plan to tailor its benefits to meet the needs of dual eligibles, and may make it more difficult for the plan to coordinate Medicare and Medicaid benefits. For more information, see CMS, “Medicare Program; Revisions to the Medicare Advantage and Prescription Drug Benefit Program: Proposed Rule,” 75 Federal Register 71189‐71292, November 22, 2010. Note that the MCBS Access to Care File underrepresents beneficiaries who die before the end of the calendar year, and thus may undercount the total number of dual eligibles in Medicare Advantage plans.
EXHIBIT 4
Share of Dual Eligible Beneficiariesin Dual Special Needs Plans, by State, 2011
<1% ‐ 10%(28 states + DC)
11% ‐ 20%(7 states)
21% ‐ 30%(3 states)
> 30%(3 states)
No Dual Eligiblesin Dual SNPs(9 states)
National Average, 2011 = 10%
DC
18%
0%
43% 4%
13% 11%
5%
1%
17%
3%
31%
5%
1% 1%1%
1% 6%
7%
3%
6%
6%33%
4%
3%
0%
1%<1%
0%
3%
6%
14%
3%
0%
3%
1%
21%
23%0%
2%
0%
17%
11%
27%
0%
1%
4%
0%
0%
5%
7%4%
NOTE: Puerto Rico and territories are excluded from the national average.SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment files, 2011.

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 5
in the SNP market (Exhibit 5). Conversely, some of the firms with the largest SNP enrollment (like XLHealth or SCAN) do not have a relatively large share of the general Medicare Advantage market but are heavily focused on beneficiaries eligible for SNPs.
Compared to the general Medicare Advantage market, the SNP market is less concentrated. Although SNP enrollment is just 10 percent of total Medicare Advantage enrollment (excluding Puerto Rico), almost 46 percent of firms in the Medicare Advantage market (103 of the 224 firms) offer a SNP of some type. The greater fragmentation of enrollment among firms in the SNP market is consistent with the larger role of care delivery in SNPs compared to plans available to the broader Medicare population. POLICY IMPLICATIONS
SNPs now play a relatively small role within the overall Medicare program, but have the potential to play a greater role in the future, particularly as federal and state policymakers pursue new programs and initiatives to constrain costs and improve care for dual eligibles and other beneficiaries who account for a disproportionate share of spending.13 While the number of SNPs offered nationwide has steadily declined since 2008, SNP enrollment has increased modestly over the past few years, and has more than doubled since 2006. Dual SNPs account for most of the SNP enrollment in 2011, as has been the case since 2006.
Looking to the future, SNPs face a number of challenges if they are to play a greater role in the Medicare program. For example, for many dual SNPs today, coordination between the Medicare and Medicaid programs is more a goal than a reality, posing challenges for SNPs and for enrollees who receive coverage under both programs.14 While existing dual SNPs will be required to contract with state governments by 2013, it is not clear how this requirement will be implemented and how effective it will be in coordinating benefits and care across the two programs. Dual SNPs also face enormous challenges in providing appropriate services to enrollees with heterogeneous and often highly‐specialized and diverse needs, ranging from younger beneficiaries with debilitating mental disabilities to older enrollees, with physical and cognitive impairments, living in nursing homes or trying to maintain their independence at home.
More generally, there is some concern that current risk adjustment techniques are inadequate for plans that focus on sicker, more expensive beneficiaries, and that bonus payments for Medicare Advantage plans do not include metrics that are appropriate for capturing important aspects of care provided in SNPs. As policymakers address well‐documented concerns about overpayments to Medicare Advantage plans, there is some concern that SNPs and other plans that enroll high‐risk enrollees will not be adequately compensated to provide needed care. 15
With growing concern over the federal deficit and the costs of Medicare and Medicaid, policymakers are looking for ways to improve the delivery of care and reduce spending for high‐cost beneficiaries. Improvements in health care delivery are a central part of federal health reform and a major priority for the Administration and CMS. While changes in both state and federal policies will influence the future of SNPs, the experience of the plans may inform improvements in the management of care for sick and frail Medicare beneficiaries, both within the Medicare Advantage program and in traditional Medicare. Further work is needed to assess the experiences of Medicare beneficiaries enrolled in SNPs and the capacity of these plans to improve patient care.
EXHIBIT 5
UnitedHealth Group 16%
Aveta 9%
XLHealth 7%
HealthSpring 6%
Kaiser Permanente 5%
Humana 5%Medical Card System 4%
BCBS Affiliates 4%
SCAN Health Plan 4%
Healthfirst 4%Health Net 3%
Other 33%
Enrollment in Special Needs Plans, by Firm, 2011
Total Enrollment in SNPs, 2011 = 1.28 Million
NOTE: Other includes firms with less than 3% of total enrollment. Puerto Rico and other territories are included. SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment files, 2011.

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 6
Table A1. Share of Plans and Enrollment in SNPs, by Plan Type, 2011.
Share of Plans
Share of Enrollment
Share of Plans
Share of Enrollment
Share of Plans
Share of Enrollment
Share of Plans
Share of Enrollment
HMOs 91% 89% 94% 95% 76% 78% 93% 52%Local PPOs 6% 3% 4% 2% 25% 22% 1% 0%Regional PPOs 3% 8% 2% 2% 0% 0% 7% 48%
NOTE: Includes Puerto Rico, the only territory with SNPs. Numbers may not sum to the total due to rounding.SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment and Landscape fi les, 2011.
Dual Eligibles Institutional Chronic ConditionsTotal

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 7
Table A2. Number of Beneficiaries in Special Needs Plans, by Plan Type, 2006‐2011
Year
2006 531,507 439,412 22,156 69,939
2007 1,080,593 751,784 144,928 183,881
2008 1,187,758 852,973 130,204 204,581
2009 1,270,886 901,175 118,499 251,212
2010 1,264,161 968,058 94,762 201,341
2011 1,283,772 1,045,072 78,666 160,034
% change, 2010‐2011
2% 8% ‐17% ‐21%
NOTE: Includes Puerto Rico, the only territory with SNPs.
Total Dual Eligibles Institutional Chronic Conditions
SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment and Landscape fi les, 2006‐2011.

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 8
Table A3. Top Firms by Enrollment in Special Needs Plans, 2011
All Firms 11,922,543 1,283,772 1,045,072 78,666 160,034 10,638,771 100% 11%
Firms with more than 10,000 SNP enrollees
9,194,461 1,065,703 848,363 74,872 142,468 8,128,758 83% 12%
United Healthcare 2,180,485 203,036 171,068 26,860 5,108 1,977,449 16% 9%
Aveta 191,359 120,140 112,374 313 7,453 71,219 9% 63%
XLHealth 93,619 84,362 7,603 -‐ 76,759 9,257 7% 90%
HealthSpring 327,288 80,791 69,616 1,333 9,842 246,497 6% 25%
Kaiser Permanente 1,008,556 64,453 64,453 -‐ -‐ 944,103 5% 6%
Humana 1,852,398 62,112 60,083 -‐ 2,029 1,790,286 5% 3%
Medical Card System 116,950 55,543 55,543 -‐ -‐ 61,407 4% 47%
BCBS Affiliates 2,080,873 53,243 51,992 -‐ 1,251 2,027,630 4% 3%
SCAN Health Plan 128,198 52,301 6,764 45,056 481 75,897 4% 41%
Healthfirst 92,167 47,902 47,902 -‐ -‐ 44,265 4% 52%
Health Net 230,555 35,982 35,763 -‐ 219 194,573 3% 16%
WellCare Health Plans 117,220 28,434 28,434 -‐ -‐ 88,786 2% 24%
Gateway Health Plan 26,892 26,892 26,892 -‐ -‐ -‐ 2% 100%
America's 1st Choice Holdings of Florida
57,525 25,829 3,514 -‐ 22,315 31,696 2% 45%
Molina Healthcare 25,660 19,016 19,016 -‐ -‐ 6,644 1% 74%
CareMore Medical Enterprises
53,059 18,137 441 1,310 16,386 34,922 1% 34%
University of Pittsburgh Medical Center
93,498 16,530 16,530 -‐ -‐ 76,968 1% 18%
Munich American Holding Corp. (Sterling)
69,532 13,335 12,710 -‐ 625 56,197 1% 19%
AMERIGROUP 18,214 12,184 12,184 -‐ -‐ 6,030 1% 67%
CalOptima 11,493 11,493 11,493 -‐ -‐ -‐ 1% 100%
EmblemHealth 167,588 11,461 11,461 -‐ -‐ 156,127 1% 7%
Coventry Health Care 215,647 11,385 11,385 -‐ -‐ 204,262 1% 5%
UAB Health System 35,685 11,142 11,142 -‐ -‐ 24,543 1% 31%
All Other Firms 2,728,082 218,069 196,709 3,794 17,566 2,510,013 17% 8%
SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment and Landscape fi les, 2011.
NOTE: Includes Puerto Rico, the only territory with SNPs; excludes group and employer-‐sponsored plans. BCBS includes all BlueCross BlueShield Affl iates. Aveta is the parent company for MMM Healthcare and PMC Medicare Choice plans, which are based in Puerto Rico. Medical Card System, Inc. is also based in Puerto Rico.
Enrollment in Other
Medicare Advantage
Firm Marketshare Among SNPs
Share of Firm Enrollment in
SNPsFirm or Affiliate
Total Medicare Advantage enrollment
Enrollment in SNPs
Total Dual Institutional Chronic Condition

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
Special NeedS plaNS: availability aNd eNrollmeNt 9
Table A4. Enrollment in Special Needs Plans Across States, by Plan Type, 2011
Total
Alabama 32,467 32,467 0 0 4% 18% 19%Alaska 0 0 0 0 0% 0% 0%Arizona 64,853 60,506 1,367 2,980 7% 43% 19%Arkansas 11,479 4,193 0 7,286 2% 4% 16%California 209,355 146,324 46,120 16,911 4% 13% 12%Colorado 10,064 7,942 2,035 87 2% 11% 5%Connecticut 5,563 4,109 1,454 0 1% 5% 5%Delaware 714 207 200 307 0% 1% 14%District of Columbia 1,325 1,080 133 112 2% 5% 18%Florida 122,506 91,747 1,375 29,384 4% 17% 12%Georgia 32,591 6,503 1,980 24,108 3% 3% 12%Hawaii 9,018 9,018 0 0 4% 31% 10%Idaho 1,401 1,401 0 0 1% 5% 2%Illinois 6,476 4,991 353 1,132 0% 1% 4%Indiana 1,992 1,898 94 0 0% 1% 1%Iowa 371 371 0 0 0% 1% 1%Kansas 825 618 127 80 0% 1% 2%Kentucky 9,706 9,706 0 0 1% 6% 8%Louisiana 12,226 12,226 0 0 2% 7% 8%Maine 2,921 2,921 0 0 1% 3% 8%Maryland 11,190 5,532 2,779 2,879 1% 6% 18%Massachusetts 16,595 14,850 1,463 282 2% 6% 9%Michigan 9,450 8,487 692 271 1% 4% 2%Minnesota 38,949 38,816 0 133 5% 33% 11%Mississippi 5,568 5,480 0 88 1% 4% 13%Missouri 12,626 4,323 0 8,303 1% 3% 6%Montana 0 0 0 0 0% 0% 0%Nebraska 379 379 0 0 0% 1% 1%Nevada 1,807 26 29 1,752 1% <1% 2%New Hampshire 0 0 0 0 0% 0% 0%New Jersey 6,883 5,692 444 747 1% 3% 4%New Mexico 3,479 3,361 118 0 1% 6% 4%New York 102,232 94,070 7,785 377 3% 14% 11%North Carolina 9,804 7,776 2,028 0 1% 3% 4%North Dakota 0 0 0 0 0% 0% 0%Ohio 10,705 8,167 2,538 0 1% 3% 2%Oklahoma 853 752 101 0 0% 1% 1%Oregon 18,220 17,858 362 0 3% 21% 7%Pennsylvania 92,803 86,223 1,967 4,613 4% 23% 11%Rhode Island 1,338 0 1,338 0 1% 0% 2%South Carolina 25,842 2,136 0 23,706 3% 2% 21%South Dakota 0 0 0 0 0% 0% 0%Tennessee 38,474 38,248 31 195 4% 17% 15%Texas 85,052 61,790 86 23,176 3% 11% 14%Utah 5,941 5,941 0 0 2% 27% 6%Vermont 0 0 0 0 0% 0% 0%Virginia 987 840 78 69 0% 1% 1%Washington 8,467 6,103 494 1,870 1% 4% 3%West Virginia 0 0 0 0 0% 0% 0%Wisconsin 11,541 10,759 782 0 1% 7% 4%Wyoming 0 0 0 0 0% 0% 0%Total, All States and DC 1,055,038 825,837 78,353 150,848 2% 10% 10%Puerto Rico 228,734 219,235 313 9,186 34% 97% 51%Total, Including Territories 1,283,772 1,045,072 78,666 160,034 3% 12% 11%
SOURCE: MPR/Kaiser Family Foundation analysis of CMS Medicare Advantage enrollment and Landscape files, 2011.
Total Dual Eligibles InstitutionalChronic
Conditions
% of Medicare Advantage enrollees in
SNPs
% of Medicare Beneficiaries in
SNPs
% of Dual Eligibles in Dual
SNPs
NOTE: Includes Puerto Rico, the only territory with SNPs; number of dual eligibles per state from CMS, as of December 31, 2009.

Medicare PolicyK A I S E R F A M I L Y F O U N D A T I O N
Data spotlight
the heNry J. Kaiser Family FouNDatioN
Headquarters: 2400 Sand Hill Road Menlo Park, CA 94025 650.854.9400 Fax: 650.854.4800 Website: www.kff.orgWashington Offices and Barbara Jordan Conference Center: 1330 G Street, NW Washington, DC 20005 202.347.5270 Fax: 202.347.5274
The Kaiser Family Foundation, a leader in health policy analysis, health journalism and communication, is dedicated to filling the need for trusted, independent information on the major health issues facing our nation and its people. The Foundation is a non-profit private operating foundation, based in Menlo Park, California.
this publication (#8229) is available on the Kaiser Family Foundation’s website at www.kff.org.
References 1 See Kaiser Family Foundation, “The Role of Medicare for the People Dually Eligible for Medicare and Medicaid,” January 2011. See also, Kaiser Family Foundation, “Dual Eligibles: Medicaid’s Role for Low‐Income Medicare Beneficiaries,” December 2010.2 See Medicare Payment Advisory Commission, “Chapter 5: Coordinating the Care of Dual Eligible Beneficiaries,” Report to Congress: Aligning Incentives in Medicare, Washington DC, June 2010. 3 For analysis on issues facing SNPs early in the program see J Verdier, M Gold and S Davis “Do We Know if Medicare Advantage Special Needs Plans Are Special?” Washington DC: Kaiser Family Foundation, January 2008.4 For additional information on these requirements, see Centers for Medicare and Medicaid Services, “Special Needs Plans,” at http://www.cms.gov/SpecialNeedsPlans/5 Medicare Payment Advisory Commission, “Report to Congress: Aligning Incentives in Medicare,” Chapter 5, June 2011.6 See Letter from Medicare‐Medicaid Coordination Office to State Medicaid Directors, July 8, 2011. 7 Centers for Medicare and Medicaid Services, “15 States Win Contracts to Develop New Ways to Coordinate Care for People with Medicare and Medicaid: CMS Will Work With All States to Improve Care,” April 14, 2010. For a summary of the 15 states’ proposals, see Kaiser Family Foundation, “Proposed Models to Integrate Medicare and Medicaid Benefits for Dual Eligibles: A Look at the 15 State Design Contracts Funded by CMS,” August 2011.8 At the end of 2008, CMS issued guidance specifying 15 SNP conditions that met the MIPPA definition of severe or disabling and only such plans were eligible for approval starting 2010. See http://www.cms.gov/SpecialNeedsPlans/. 9 M Gold, G Jacobson, A Damico, and T Neuman. “Medicare Advantage 2011 Data Spotlight: Medicare Advantage Enrollment Market Update,” Washington DC: Kaiser Family Foundation, September 2011.10 For more information on eligibility criteria and Medicare Savings Programs, see Kaiser Family Foundation, “The Role of Medicare for the People Dually Eligible for Medicare and Medicaid,” January 2011. 11 See Medicare Payment Advisory Commission, “Report to the Congress: Medicare Payment Policy,” Chapter 3, March 2008.12 M Gold, G Jacobson, A Damico, and T Neuman. “Medicare Advantage 2011 Data Spotlight: Medicare Advantage Enrollment Market Update,” Washington DC: Kaiser Family Foundation, September 2011.13 Medicare Payment Advisory Commission, “A Data Book: Health Care Spending and the Medicare Program,” June 2011. See also Kaiser Family Foundation, “Dual Eligibles: Medicaid’s Role for Low‐Income Medicare Beneficiaries,” December 2010. 14 Medicare Payment Advisory Commission. “Chapter 5: Coordinating Care for Dual Eligible Beneficiaries” report to Congress: Medicare and the Health Care Delivery System, June 2011.15 M Gold, G Jacobson, and T Neuman. “Firm Perspectives on the Medicare Advantage Market,” Washington DC: Kaiser Family Foundation, September 2011.