Embed Size (px)
Citation preview

Specialist cancer and cardiovascular services: Commissioner Decision ‘Meeting in Common’
Agenda
A ‘meeting in common’ for Commissioners to receive feedback from the recent engagement phase on proposals to consolidate specialist cancer and cardiovascular services for north and east London and west Essex, and to formally decide whether to approve the proposed changes, and any necessary decisions about implementation.
DATE: Friday 25 July, 11.00-12.30 pm VENUE: MWB Business Exchange, 10 Greycoat Place, London, SW1P 1SB ATTENDEES: Representatives from: NHS England Anne Rainsberry, Regional Director, London Region Simon Weldon, Director of Commissioning, London Region Director of Finance, London Region Clinical Commissioning Groups (CCGs) Camden CCG City and Hackney CCG Enfield CCG Haringey CCG Islington CCG MEETING OBJECTIVES:
1. To receive feedback from the recent engagement phase on proposals 2. To formally decide whether to approve the proposed changes for changes to
specialist cancer services 3. To formally decide whether to approve the proposed changes for changes to
specialist cardiovascular services 4. To make any necessary decisions about implementation, if proposals are
approved
AGENDA:
1. Welcome and introductions 2. The clinical case for change 3. Update on phase two 4. Engagement feedback on the proposed options 5. The proposed implementation framework 6. Decision making
MEETING CONTACTS Beth Warmington 020 3688 2440 [email protected]

COMMISSIONER ‘MEETING IN COMMON’ – SPECIALIST CANCER AND CARDIOVASCULAR SERVICES FOR NORTH AND EAST LONDON AND WEST ESSEX
Minutes of the meeting held on Friday 9 May 2014 14.00-16.00
Portland House, Bressenden Place, London, SW1E 5RS Present: Chair: Anne Rainsberry, Regional Director (London Region), NHS England (AR) Voting Members: NHS England: Simon Weldon, Director of Commissioning, (London Region), NHS England (SW) Camden Clinical Commissioning Group Dr Lance Saker, GP Governing Body member (LS) William Roberts, Director for Strategy and Planning (WR) City and Hackney Clinical Commissioning Group Paul Haigh, Chief Officer (PH) Dr Gary Marlowe, GP Governing Body member (GM) Muriel Purkiss, Hackney Healthwatch, Lay member (MP) Enfield Clinical Commissioning Group Graham MacDougall, Director of Service Improvement (GMa) Haringey Clinical Commissioning Group Dr Gino Amato, GP Governing Body member (GA) Islington Clinical Commissioning Group Alison Blair, Chief Officer (AB) Dr Gillian Greenhough, Chair (GG) Dr Rathini Ratnavel, GP Governing Body member (RR) Non-voting attendees: David Fish, Managing Director, UCL Partners (DF) Neil Kennett Brown, Programme Director, North and East London Commissioning Support Unit (NELCSU) (NKB) Stuart Saw, Head of Financial Strategy (London Region), NHS England (SS) David Mason, Legal Advisor to Programme, Capsticks (DM) Kathleen Becker, Legal Advisor to Programme, Capsticks (KB) In attendance: Alan Shaw, (observing) Amanda White, Head of Communications, UCLP (observing) Beth Warmington, Programme team, NELCSU, (minute taking) Emdad Haque Equality Team, NELCSU (observing) Neil Davis, Programme team, NELCSU (minute taking) Ronnie Jacobson, Trustee, Age UK London (observing) Wendy Mead, Chair, Health Scrutiny Committee, City of London (observing) (WM)
1. Welcome and introduction
Anne Rainsberry (AR) introduced the purpose of the meeting which was to agree whether the commissioners should adopt the recommendations as preferred options and agree to proceed to the next phase of the programme. The commissioners were convened as they are the majority commissioners for these proposals. AR took the opportunity of thanking all clinicians and commissioners across the area, for their work on the proposals so far. AR explained that each of these commissioners were not meeting as a single committee,
and each decision has to be made by each organisation separately. She explained that this
is simply because the organisations are not currently allowed to make decisions affecting all
of them in a single joint committee. This legal position is being changed, but not within the
timescale for this programme.
AR explained that the reason behind these particular clinical commissioning groups (CCGs)
meeting together (rather than all North Central and North East London and West Essex
CCGs) is because they are the relevant direct commissioners alongside NHS England (who
is the commissioner of all specialist services). AR explained that decisions would need to
be made on each of the pathway recommendations individually by the majority
commissioners for the services under consideration. She then laid out this further as
follows:
Cancer: All the services are specialised services solely commissioned by NHS England,
with the exception of acute myeloid leukaemia (AML) services which are CCG
commissioned. The key commissioners impacted by the recommendations for the AML
proposals include the following four CCGs: Enfield, Barnet, Haringey and Camden, due to
the proposed transfer of services to UCLH from other locations.
Cardiac: All the specialist cardiovascular services are commissioned by NHS England, with
general cardiology commissioned by CCGs. The key CCGs who commission the majority of
this activity is from six CCGs (Haringey CCG, City and Hackney CCG, Enfield CCG,
Islington CCG, Camden CCG, Barnet CCG).
AR acknowledged that ahead of this meeting all of the CCGs have taken this through their
respective CCG governance processes and agreed how they will enact their decision
making role. Barnet CCG have confirmed their support for the proposals in writing, and that
they are supportive of the other CCGs working alongside NHS England in decision making
going forwards. AR explained that if a decision was reached to proceed to a further
engagement phase, the programme will of course be discussing proposals and plans with all
stakeholders. This includes members of the public, patient and support groups, clinicians, all
CCGs, and joint health and scrutiny committees.
AR explained there were three areas for decision making:
1. To agree, as commissioner preferred options, the recommendations regarding proposed
changes to specialist cancer services
2. To agree, as the commissioner preferred option, the recommendation regarding proposed
change to specialist cardiovascular services
3. Approve the proposals for a further engagement on the commissioner preferred options and
implementation issues to inform final decision making.

2. Presentation on the clinical case
Professor David Fish (DF) introduced the clinical case for change
In London 2/3rds of early deaths are caused by cancer and cardiovascular disease. There are inequalities in the locality (north and east London and west Essex) and the rest of England and within the locality. These proposals represent an opportunity to save upwards of 1,000 lives each year lost due to cancer and cardiovascular disease.
The process started with commissioner models of care in 2010
There is currently strong clinical evidence that specialist centres have better outcomes with higher volumes of procedures
UCLPartners has supported clinicians to respond to the models of care with an aim
to improve services and the quality of care across the whole pathway – from
prevention and early detection to diagnosis, treatment and long-term care
Currently not all providers are meeting national standards of minimum volumes
There is currently poor patient experience for the services in question across London which needs to be addressed
Not all patients have access to the latest technology and innovations. AR provided the opportunity for attendees to respond to DF’s introduction: Gary Marlowe (GM) noted the gap in patient outcomes from those living in west London vs east London is not necessarily due to clinical practice and that wider socio-economic issues are likely to play a significant role. DF acknowledged these inequalities and recognised the importance of providing the best clinical outcomes for everyone. GM suggested centralisation is not the only option. The Scarborough stroke service for example has similar outcomes yet did not follow a centralised model. DF agreed that different approaches can be used for different settings, however the outcomes from the major trauma networks and hyper acute stroke centres, as an example of centralised services have been impressive in London and that in a densely populated area such as London, a centralised model has performed well. GG pointed out at the time of developing the case for change for stroke services, there was a significant level of resistance. However the improvements in stroke services over the past 2-3 years is notable following implementing the recommendations and largely in part due to the close working between providers to deliver network based solutions. GM noted the number of procedures a clinician must perform in order for outcomes to plateau varies pathway by pathway and clinician by clinician. DF agreed that the link between high volumes and better outcomes was only relevant to certain cancers. The cancers within scope will benefit and in many cases the current providers are not delivering the minimum numbers of procedures as set out in the respective NICE guidance. With respect to cardiovascular services, higher volume centres will result in sufficient scale to enable further sub-specialisation e.g. mitral valve repair. This will allow services in the area to reflect the trend in clinical practice globally of sub-specialisation to deliver effective care. Lance Saker (LS) highlighted that commissioners need to ensure other parts of the pathway are not neglected by focusing on specialist centres. Most of the potential benefits can be

derived from improvements in early diagnosis and out of hospital care. DF reiterated that UCLPartners is committed to driving improvements in early diagnosis and out of hospital care. The cardiovascular improvements in stroke services seen recently are a key example of this. The priority will be to ensure these specialist centres are embedded as an integral part of the pathway. 3. Presentation and discussion on the cardiovascular proposals
DF presented the case for change for cardiovascular disease. DF noted that the London Chest Hospital is already going to move to St Barts as part of previously agreed changes. The Heart Hospital has c70 cardiac surgery beds and c15 intensive care beds. It is a relatively small standalone specialty site. Due the small scale there are weaknesses including:
High cancellation rates
Small ITU (intensive care) facility
No capacity to increase size due to location
Poor compliance with single sex accommodation. The majority of clinicians engaged would prefer a single specialist cardiovascular centre at Barts Health to take advantage of new building at St Bartholomew’s which will offer better patient experience. Given its size (c42 intensive care beds) patients can be admitted quickly and with fewer cancellations. Surgeons will begin to sub-specialise and the specialist centre is seen as a catalyst to improvements across the pathway. AR invited the attendees to comment on the cardiovascular proposals and no specific concerns were raised. Wendy Mead (WM), a member of the public confirmed her support for the proposal for a single cardiovascular centre at Barts Health given the close research relationship Barts Health has with the William Harvey Centre at Queen Mary’s Charterhouse Square. PH asked for clarification around due diligence required for the financial analysis and commissioner sensitivities applied to the modelling. SS noted that each party within the tripartite work (NHS England, University College London Hospitals NHS Foundation Trust, Barts Health) will require that the costs and revenue flows provided are reasonable. With respect to commissioner sensitivities, the modelling included two assumptions. The first was a ‘no growth’ assumption in activity. The second was application of a 20% optimism bias. Both assumptions result in more conservative modelling outputs. 4. Decision making on specialist cardiovascular recommendation
AR invited the CCG and NHS England representatives to each make their respective decisions on whether to take on the recommendation as a commissioner preferred option for further engagement. AR also requested whether commissioners had any specific equality issues relating to the recommendation. A summary of the decisions is presented in the table below.
Commissioner
Do you agree to take on the recommendation as
the commissioner preferred option?
Are there any specific equality issues?
Camden Yes Further work to understand the impact on travel times for specific protected characteristics.
Islington (Note 1) Yes No further issues
Enfield Yes No further issues
Haringey Yes No further issues

City and Hackney (Note 2) Yes No further issues
NHS England Yes No further issues
(Note 1) Welcome being involved and considers such collaborative working important. Need
assurances there is sufficient capacity to implement the change and that quality is maintained
(Note 2) City and Hackney tabled a paper which set out that the CCG supports the case for change,
with conditions on the development on commissioner assurances, in particular on Barts Health as the
provider. The paper is pasted below
From Paper:
Overall the CCG supports the case for change and the plan to develop a single integrated
cardiovascular centre.
The CCG is keen to proceed with the further engagement work as they remain concerned about the
choice of Barts Health as the single centre as outlined in their original Board decision on Friday 31
January 2014.
The CCG Board supports the proposal to develop commissioner assurances and requests that:
Clear KPIs and targets are agreed by NHS England and CCG clinical commissioners for each
of the benefits set out on page 56 of the business case;
These KPIs are used to both measure the delivery of high quality cost effective care and
improved outcomes and underpin the pathway work;
The pathway work ensures a cost effective model of care between DGH and specialist services
The CCG have indicated that in order to inform their support of the next phase and final decision, they
expect:
The explicit agreement to the KPIs and the production of a delivery plan by Barts Health to
achieve these;
The delivery plan to outline the timing and realisation of the benefits for City and Hackney CCG
patients and their health economy;
To contract for the achievement of the benefits should the proposals proceed to mobilisation
5. Presentation and discussion on the cancer proposals
DF provided the context of the proposed changes. Only a small proportion of total cancer spells (2%) are impacted by the recommendations. DF noted the work of London Cancer which has been set up to identify improvements across the whole pathway. These recommendations are an integral part of these improvements. DF set out the individual recommendations as presented in the business case. DF provided anecdotal evidence supporting the need for dedicated wards for patients with brain cancer. Outcomes are typically poor for patients with short life expectancies. The dedicated ward at Queen’s Square (UCLH) provides a calming environment for patients with quick access to health professionals. The aspiration of these proposals is to deliver this high level of patient experience. GM requested assurances that any adverse impact on the trauma service at Royal London is mitigated. DF noted that joint working relationships between providers was key. The proposals

have received support from the Medical Director at Barts Health and work is underway to address these issues. LS noted that a potential risk to centralisation is the additional time patients may have to wait from diagnosis to treatment. There is a need to address management plans following diagnosis and for the specialist centre to keep the patients and their primary care clinicians informed. WM also raised similar concerns that currently the system does not perform well at transferring patients back to their local hospital effectively. 6. Decision making for acute myeloid leukaemia (AML) services AR invited the CCG representatives to decide whether to take on the AML recommendations as the commissioner preferred option for further engagement. AR also requested whether commissioners had any specific equality issues relating to the recommendation. A summary of the decisions is presented in the table below.
Commissioner
Do you agree to take on the recommendation as
the commissioner preferred option?
Are there any specific equality issues?
Camden (1) Yes Need to make sure that we have engaged and involved the protected characteristic groups to better understand their issues and how they use the services
Enfield Yes No further issues Haringey Yes No further issues
(1) Has requested assurances that the hand-offs between specialist and non-specialist services will
work particularly in relation to communication of care plans and ensuring high quality of patient
experience.
7. Decision making on remaining specialist cancer pathways
AR invited SW as representative for NHS England to decide whether to take on the remaining specialist cancer pathway recommendations as the commissioner preferred options for further engagement. AR also requested whether NHS England had any specific equality issues relating to the recommendation. A summary of the decisions is presented in the table below.
Commissioner
Do you agree to take on the recommendations as
the commissioner preferred options?
Are there any specific equality issues?
NHS England (1) Yes No issues
(1) Concerns and key issues that have been raised by all commissioners in regards to the proposals
have been noted and these will be taken forward and addressed as part of the next stages of the
programme
8. Decision making on whether to proceed to a further engagement NKB provided an overview of the next phase of the programme which is outlined in chapter eight of the business case. The business case itself will be developed into a short consultation document which was circulated in draft format, feedback is welcome on this. This document will be written with the plain English standard (kite mark) and published on the NHS England

website as part of the launch of the engagement. A series of workshops will be held to address the key issues previously raised by stakeholders in the previous phase of engagement. In parallel, planning for implementation work and associated commissioner assurances raised during this meeting will be further developed. AR invited the commissioners to decide on whether to proceed to further engagement on the preferred options. The decisions are presented in the table below:
Commissioner
Do you approve the business case and consultation document and agree to
proceed to phase 2 of engagement on the commissioner preferred options to inform
final decision making?
Camden Yes
Islington Yes
Enfield Yes
Haringey Yes
City and Hackney Yes
NHS England Yes
9. Next steps and close AR concluded the meeting and thanked people for their attendance. AR reiterated that this is not the final decision and that a final decision on whether to proceed to implementation will only be made after the further engagement has concluded, in similar commissioner meeting towards the end of July.

1
Improving Specialist Cancer
and Cardiovascular Services
in North and East London
and West Essex
Decision Making
Navigator Paper

2
Improving Specialist Cancer and Cardiovascular Services in North and East London and West Essex Decision Making Navigator Paper

3
Table of Contents
Introduction ......................................................................................................................... 4 Where we are in the programme ......................................................................................... 5
2.1 Phase one – Early engagement and developing options .............................................................. 5
2.2 Phase two – Engagement on preferred options and decision making .................................... 8
Equality impact assessment ................................................................................................ 9 Stakeholder engagement .................................................................................................. 10
4.1 How we engaged on the preferred options ....................................................................................... 10
4.2 Key findings ...................................................................................................................................................... 10
Finance ............................................................................................................................. 12 A framework for implementation ....................................................................................... 13
Decision making ................................................................................................................ 15

4
Introduction
The Cancer Cardiac Programme has concluded its engagement on the preferred options for reconfiguration of specialist cancer and cardiovascular services. This navigator paper has been developed for commissioners to support their final decision making whether to approve the proposed changes and the supporting next steps at a joint commissioner meeting to be held on the 25th July 2014. The purpose of this paper is to:
Help commissioners navigate the papers presented at the commissioner meeting
Provide an update on the equality impact assessment
Provide summary feedback from the engagement period
Provide an overview of the implementation governance and assurance framework
Set out the decisions required by commissioners This paper supplements the business case and supporting papers presented to commissioners in May 2014. The remaining structure of this paper is as follows:
Where we are in the programme and scope of phase
Equality Act analysis
Stakeholder engagement
Finance update
A framework for implementation
Decision making on the recommendations and next steps

5
Where we are in the programme
The diagram below outlines the key steps of the programme to date. Figure 2-1 - The Development of the Programme
2.1 Phase one – Early engagement and developing options
In 2010 a clinical review made recommendations for improving cancer and cardiovascular services in London concluding that fewer specialist high-volume units would improve clinical outcomes, accelerate the uptake of new technologies, achieve greater quality and optimise efficiency. Building on the London review and using clinical evidence, local clinicians through the leadership of UCLPartners looked at how improvements could be made to specialist cancer and cardiovascular services in north and east London and west Essex. These were described in the Case for Change document developed by NHS England (London). NHS England and CCG partners engaged the a wide range of local stakeholders and residents to gain their views on, and experience of, current services and to hear their aspirations for the health services they would receive in future. This was done through a commissioner-led engagement exercise based around the case for change and clinical recommendations.
Case for change http://www.england.nhs.uk/london/engmt-consult/

6
Taking the UCLPartners clinical recommendations as its starting point, a thorough and transparent options appraisal and impact assessment was applied to develop an agreed set of preferred options for how to consolidate specialist services delivered by providers in the area. The methodology, the stakeholders consulted and the findings of the appraisal are described in detail in the Cancer Cardiac Business Case. It was the role of NHS England to lead on an internal assurance exercise to ensure the programme met the four tests which are set out in the guidance on delivering services changes published by NHS England1. An Internal Assurance Report was developed and presented to commissioners clearly stating how and where each of the four tests were met.
Supplementing the internal assurance exercise, the Programme engaged the Department of Health to conduct a gateway review and the London Clinical Senate to conduct a clinical review.
The purpose of the Department of Health Gateway Review was to assess the outcomes and objectives for the programme (and the way they fit together) and confirm that they make the necessary contribution to the relevant organisations’ strategic priorities. This first stage review was undertaken through a review of supporting documentation for the programme and interviews with key senior stakeholders. The review team assigned the programme a delivery confidence level of AMBER-GREEN, reflecting on the strong clinical support. This was considered a positive outcome for the programme at the time of review. The London Clinical Senate with expertise relevant to each of the pathways and with no known conflict of interest provided external clinical assurance. The scope of this assurance review was to test whether a sufficiently robust clinical process was adopted by lead commissioners to arrive at the recommended options, considering the clinical involvement and evidence used. The London Clinical Senate concluded the process adopted was overall, a robust one. A number of recommendations were identified. Both these and the responses by NHS England can be found on the engagement website. Further to the review of the clinical process, the London Clinical Senate was also engaged to provide advice to inform a recommendation on the future model and location(s) of radical prostatectomies in north central and north east London. This independent review was conducted in response to engagement feedback on the proposed options. Following the review, the London Clinical Senate concluded a single site model at UCLH was preferable.
1 NHS England. Planning and delivering service changes for patients (2013)
Cancer Cardiac Business Case http://www.england.nhs.uk/london/engmt-consult/ London Clinical Senate Report http://www.england.nhs.uk/london/engmt-consult/ London Clinical Senate Prostate Review http://www.england.nhs.uk/london/engmt-consult/

7
The Cancer Cardiac Business Case, the Phase One Engagement report and supporting assurance papers were presented to the lead Commissioners at a decision making meeting. The purpose of this meeting was to make the following decisions:
To agree as commissioner preferred options the recommendations regarding proposed changes to specialist cancer services outlined in the business case
To agree as commissioner preferred option the recommendation regarding proposed change to specialist cardiovascular services outlined in the business case
To approve the business case and consultation document and agree to proceed to phase 2 of engagement on the commissioner preferred options to inform final decision making
Commissioners unanimously agreed to each of the decisions enabling the programme to proceed to the next phase with a set of commissioner preferred options for engagement outlined below:
Pathway Preferred option
1.1 Brain That the National Hospital for Neurosciences (UCLH) and The Queen’s Hospital (Romford) (BHRUT) are retained as the two units in the area providing neurosurgical cancer services
1.2 Head & Neck That UCLH is retained as the single centre for specialist head and neck cancer surgery in the area.
1.3 Bladder & Prostate That UCLH is proposed as the single centre for specialist bladder and prostate cancer surgery.
1.4 Renal That the Royal Free Hospital is the single provider for renal cancer surgery for the area
1.5 HSCT That Barts Health and UCLH are retained as the two level 3 providers for AML and HSTC in the area.
1.6 AML That Barts Health, UCLH and The Queen’s (Romford) are retained as providers of AML level 2b services.
1.7 OG That an interim position is adopted that retains a service at UCLH and The Queen’s Hospital with both units operating collaboratively under a single model and sharing best practice. In three to five years’ time consideration of further consolidation should be given following a review of the volume of activity at both units against the latest standards of best practice.
2.1 Services at HH transfer to St Barts
That services at The Heart Hospital should be transferred to St Bartholomew’s Hospital to create a single integrated cardiovascular centre. The Royal Free Hospital and the integrated cardiovascular centre at St Bartholomew’s Hospital would be the Heart Attack Centres for the area.

8
2.2 Phase two – Engagement on preferred options and decision making
During Phase One, regular meetings and dialogue were conducted with the three Joint Health Overview and Scrutiny Committees (JHOSCs) and Westminster Overview and Scrutiny Committee (OSC) before and during the engagement to understand their views and any requirement for further engagement or consultation. The JHOSCs concluded the proposals did not represent substantial variation or development in services and formal consultation with local authorities is not required under section 244 of the NHS Act 2006. A five week phase of engagement was planned to engage on the preferred commissioner options. The output of this engagement is summarised below and presented in the phase two engagement report. In parallel, providers have begun scoping how they would deliver the preferred options before developing more detailed implementation plans. Any provider-led planning and implementation would need to be assured and overseen by commissioners to ensure all issues are addressed and risks mitigated prior to services switching. An implementation framework has been developed for this purpose and is described in the accompanying report. Figure 2-2 - Programme process
Phase Two Engagement Report Summary Implementation Framework Report
Options Decision
Scope Plan in detail ImplementService
delivery
Go decision
Commissioners
Providers
Assurance / Oversight
We are here

9
Equality Act analysis
The preliminary proposals to improve specialist cancer and cardiovascular services in north and east London and west Essex formed part of NHS England’s drive to reduce health inequalities and the disparities in life expected between residents within the area and in the context of London-wide life expectancies. The programme team analysed whether the proposals for change would likely have an impact on the groups identified in the Equality Impact Assessment (EqIA), including older people, people with disabilities and people from more ethnically diverse communities. The lead commissioners have considered the impacts on people with protected characteristics via their respective equality delivery systems (EDS). Any specific equality related issues were raised and recorded at the first commissioner decision meeting. While the EqIA demonstrated that there was no evidence of any group being disproportionately affected by the proposals, every effort was made in designing the plan to communicate with groups identified with protected characteristics, such as LGBT groups and Age UK, providing the opportunity to contribute to the proposals. In addition, public documents were approved by the Clear English Standard, and alternative language formats made available on request. The plan also incorporated an offer to attend existing patient groups in local communities, to discuss the proposals. The EqIA found that the proposals would not impact any of the groups disproportionately, but did show that some services would be moving out of communities that are more ethnically diverse. Hospitals providing specialist services under the proposals would need to make sure that people in those communities would not be unduly affected. Should the proposals be approved, this is an area that will continue to be monitored as part of the assurance process.
Phase Two Engagement Report Summary

10
Stakeholder engagement
4.1 How we engaged on the preferred options The second period of engagement ran for five weeks, beginning on Friday 23 May 2014 and ending on Friday 27 June 2014. The aim was to seek stakeholder views on commissioners’ preferred options and to provide people with the opportunity to contribute to the planning for implementation work, particularly around some of the themes raised in the first phase of engagement, such as travel and transport. A variety of methods were employed during this second phase, to seek the widest range of views from the community and our partners including:
Notifying over 600 stakeholders of launch of second phase of engagement
Producing a summary business case, including a questionnaire
to understand support for each of the proposals individually
Publicising the business case on the NHS England dedicated
web pages, with online feedback form
Distributing the summary business case to local hospital sites
and publication on trust intranets and CCG websites
Hosting an online feedback form, allowing respondents to
comment on each proposal individually
Advertising engagement events in local papers
Promoting the events and engagement process at provider staff
meetings and public/patient workshops
Holding four engagement workshops covering the local area.
Three workshops specifically focused on the patient pathway
and patient travel. The fourth workshop focused on the
bladder/prostate preferred option and was held at Romford,
targeting the cohort of patients that were most likely to be
impacted by the proposals.
4.2 Key findings
A number of key themes emerged from the engagement exercise. At the individual proposal level, the majority of responses were supportive. Stakeholders who were supportive, agreed with the general principle of consolidating specialised services and willingness for patients to travel for the best services available.
Phase Two Engagement Report Summary

11
A number of specific concerns were raised however including the impact on travel, particularly for patients residing in outer north east London, the possible impact on co-dependent services (such as the Major Trauma Centre at the Royal London Hospital) and the move of prostate services from BHRUT to UCLH. The programme has responded to these concerns which are outlined in this report and sought to identify sufficiently robust mitigations from the relevant parties.
A more detailed breakdown of key themes raised and the responses to these are outlined in section 6 and in Appendix E: Engagement feedback report.

12
Finance
Phase one required each party to agree in principle the required funding agreement to sustainably support the proposed implementation. This current phase has involved working through the details of this agreement and getting the necessary sign off by the relevant parties. This has included the Barts, RFH and UCLH Boards and the NHS England National Finance and Investment Committee.
Following a meeting on the 7th July, the National Finance and Investment Committee agreed to approve the Cancer Cardiac, business case and agreed to the transitional funding.
Membership of the National Finance and Investment Committee includes:
Chair: Non-Executive Director Moira Gibb
Member: Non-Executive Director Ed Smith
Member: Chief Financial Officer Paul Baumann
Member: Regional Director (M&E) Paul Watson
Member: National Director: Policy Bill McCarthy
In attendance and presenting the business case:
o Anne Rainsberry, Regional Director, London o David Slegg, Director of Finance, London Region o Prof David Fish, Managing Director, UCLPartners

13
A framework for implementation
A framework for implementation has been developed which includes a revised governance structure that will be fit for purpose to oversee the implementation period. A Commissioner assurance process has been designed to enable appropriate management and monitoring of any provider led implementation by establishing a set of commissioner ‘gates’. This will ensure any proposed change will happen in a controlled manner.
The framework is based on feedback received throughout the engagement period with stakeholders including CCGs, providers and UCLPartners. Key to designing the framework is ensuring any change is carried out safely, in a timely fashion and accompanied by a clear plan to realise the expected benefits of the proposals.
If commissioners agree to changes in service provision, they will seek assurance on the safety and readiness of services before and during reconfiguration. As such, the next phase governance structure will need to be established to deliver the following functions:
• Seek assurances from providers on each of the pathways:
• Support full pathway integration
• Ensure dependent services are not adversely affected
• Facilitate effective management of hand-offs across the pathway including the provision of timely patient information
• Ensure the continuity of patient care
• Provide for effective clinical and non-clinical staff rotas
• Be underpinned with a clear timeline with realistic and achievable phasing
• Monitor an integrated end to end plan and manage any dependencies across pathways, providers, estates, workforce and IT
• Ensure there is a consistent approach across all pathways and providers with regards to the management of support services, travel, HR, access to patient information and the provision of information for patients
• Ensure lead providers are adopting a system-wide approach in implementing the new pathways
• Ensure capacity is in place prior to any service transition
• Ensure transfer of services between providers is managed safely and effectively
Implementation Framework

14
• Define world class standards and ensure benefits are being achieved in the long run
As well as developing a framework for implementation, the programme sought to review the implementation planning currently being led by the lead providers. Key clinical and deliverability risks have been identified and the programme has sought assurances that mitigating plans are in place to address these risks.

15
Decision making
Decisions on each of the pathway recommendations are to be made individually by the lead commissioners at a meeting in common on the 25 July 2014. NHS England approved the relevant preferred options for implementation and the associated business case and transitional funding agreement at the NHS England Finance and Investment Committee held on 7th July. The remaining decision makers include the following:
Specialised cancer recommendations - All the services are solely commissioned by NHS England, with the exception of acute myeloid leukaemia (AML) services. The key commissioners impacted by the recommendations for this service include the following four CCGs: Enfield, Barnet, Haringey and Camden, due to the proposed transfer of services to ULCH from other locations. The above four CCGs will have a role in the decision-making for the AML recommendation.
For specialist cardiovascular care, around 59% of spells at The Heart Hospital (mainly general cardiology) are CCG commissioned. Of the CCG commissioned activity more than 70% is from six CCGs (Haringey CCG, City and Hackney CCG, Enfield CCG, Islington CCG, Camden CCG, Barnet CCG). The above six CCGs will have a decision-making role.
Barnet CCG has written to confirm their support for these proposals, and that they are supportive of the other CCGs working alongside NHS England in decision making going forwards.
The table below outlines the commissioners responsible for making decisions on each of the pathway recommendations.
Table 1 - Responsible decision makers by pathway
Decision maker
Decision required NHS E
Camden CCG
City & Hackney
CCG
Enfield CCG
Haringey CCG
Islington CCG
1.1 Brain
Decision made to support he
implementation of the
recommendations
1.2 Head & Neck
1.3 Bladder & Prostate
1.4 Renal
1.5 HSCT
1.6 AML
1.7 OG As per above
2.1 Services at HH transfer to St Barts
As per above

16
CCG Commissioners will be asked to make the following decisions:
1. To agree to implement the recommendation made by the programme to AML services
2. To agree to implement the recommendation made by the programme to specialist cardiovascular services
NHSE and CCG Commissioners:
3. To agree the implementation framework including the Commissioner assurance and implementation governance Each commissioner will be required to make a separate decisions on the pathways relevant to it. This will be conducted at a meeting scheduled for 25th July 2014. Each commissioner has delegated authority to a sub-committee to make the required decisions which will be binding on their organisations.
Each commissioner is invited to consider all the available papers to inform final decision making prior to the meeting. These include:
This navigator paper
The Phase Two Engagement Report
The Implementation Framework The following draft meeting structure is proposed to facilitate the decision making.
Agenda item
1. Welcome and introductions
2. Clinical case for change
3. Update on phase two of the programme
4. Engagement feedback on the proposed options
5. The proposed implementation framework
6. Decision making
?
Improving specialist cancer
and cardiovascular services
in north and east London and
west Essex
P H A S E T W O E N G A G E M E N T O V E R V I E W R E P O R T
Engagement overview report
Page 1
Document revision history
Date Version Revision Comment Author / Editor
09.07.14 0.1 First draft for internal review Programme team
11.07.14 0.2 Second draft submitted for
legal review
Programme team
Document approval
Date Version Revision Role of approver Approver
NHS England Olivia Lacey
Programme SRO Simon Weldon
15.07.14 Final Neil Kennett-Brown
Contents
1. Executive summary ................................................................................................................. 2
2. Introduction .............................................................................................................................. 4
3. Previous engagement informing the programme .................................................................. 4
4. Developing the engagement plan ........................................................................................... 6
5. Phase two engagement ........................................................................................................... 8
6. Outcomes of engagement – key themes .............................................................................. 12
7. Next steps ............................................................................................................................... 19
Appendices ........................................................................................................................................ 20
Appendix A. Communications and engagement plan ........................................................................ 20
Appendix B. Communications activity log .......................................................................................... 20
Appendix C. Event material ............................................................................................................... 20
Appendix D. Promotion and publicity ................................................................................................. 20
Appendix E. Engagement feedback report ........................................................................................ 20
Appendix F. List of stakeholders ....................................................................................................... 20
Appendix G. Provider correspondence .............................................................................................. 20

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 2
1. Executive summary
In May 2014, following a period of engagement on the Case for Change Improving specialist cancer and
cardiovascular services in north and east London and west Essex, commissioners from NHS England,
and Camden, City and Hackney, Enfield, Haringey and Islington Clinical Commissioning Groups (CCGs)
came to a common agreement on their preferred options for change and agreed to proceed to the second
stage of the programme. These preferred options are summarised below:
Pathway Preferred option
1.1 Brain That the National Hospital for Neurosciences (UCLH) and The Queen’s Hospital (Romford) (BHRUT) are retained
as the two units in the area providing neurosurgical cancer services
1.2 Head & Neck That UCLH is retained as the single centre for specialist head and neck cancer surgery in the area.
1.3 Bladder & Prostate That UCLH is proposed as the single centre for specialist bladder and prostate cancer surgery.
1.4 Renal That the Royal Free Hospital is the single provider for renal cancer surgery for the area
1.5 Haematopoietic
stem cell transfer
That Barts Health and UCLH are retained as the two level 3 providers for AML and HSTC in the area.
1.6 Acute myeloid
leukaemia
That Barts Health, UCLH and The Queen’s (Romford) are retained as providers of AML level 2b services.
1.7 Oesophago-gastric That an interim position is adopted that retains a service at UCLH and The Queen’s Hospital with both units
operating collaboratively under a single model and sharing best practice.
In three to five years’ time consideration of further consolidation should be given following a review of the volume
of activity at both units against the latest standards of best practice.
2.1 Cardiovascular That services at The Heart Hospital should be transferred to St Bartholomew’s Hospital to create a single integrated
cardiovascular centre. The Royal Free Hospital and the integrated cardiovascular centre at St Bartholomew’s
Hospital would be the Heart Attack Centres for the area.
The second stage of the programme included a further phase of engagement, planning for
implementation and the development of a commissioner assurance framework to oversee the safe
transition of services, should the proposals be approved.
The second period of engagement ran for five weeks, beginning on Friday 23 May 2014 and ended on
Friday 27 June 2014. The aim was to seek stakeholder views on the commissioner preferred options and
to provide people with the opportunity to contribute to the planning for implementation work, concerning
the themes raised in the first phase of engagement, such as travel and transport.
A variety of methods were employed during this second phase to seek the widest range of views from
the community and our partners including:
Notifying over 600 stakeholders of the launch of the second phase of engagement
Producing a summary business case, including a survey to understand support for each of the
proposals
Publishing the business case on the NHS England dedicated web page, with an online feedback
form (http://www.england.nhs.uk/london/engmt-consult/)

Engagement overview report
Page 3
Distributing the summary business case to local hospital sites and publishing on trust intranets
and CCG websites
Hosting an online feedback form, allowing respondents to comment on each proposal individually
Advertising engagement events in local newspapers
Promoting engagement events in staff meetings and local public/patient workshops
Facilitating four engagement workshops covering the local area.
Over the five week period, the programme made contact with over 600 stakeholders. NHS England
received 254 comments or views on the proposals. These ranged from requests for copies of the full
business case and included letters of support from trust medical directors, feedback via email, online
surveys and comments recorded during public events. The programme received 159 completed surveys
and 41 people attended four public workshops and two existing public/ patient meetings.
Summary of themes
A number of key themes emerged from the engagement exercise. At the individual proposal level, the
majority of responses were supportive. Stakeholders who were supportive, agreed with the general
principle of consolidating specialised services and willingness for patients to travel for the best services
available.
A number of specific concerns were raised however, including the impact on travel, particularly for
patients residing in outer north east London, the possible impact on co-dependent services (such as the
Major Trauma Centre (MTC) at the Royal London Hospital (RLH)) and the move of prostate services from
Barking, Havering and Redbridge University Hospitals NHS Trust (BHRUT) to University College London
Hospitals NHS Foundation Trust (UCLH). The programme has responded to these concerns which are
outlined in this report and sought to identify sufficiently robust mitigations from the relevant parties.
A more detailed breakdown of key themes raised and the responses to these are outlined in section 6 and in Appendix E: Engagement feedback report
Next steps
A second commissioner ‘in common’ meeting will be held on 25 July 2014, where the majority
commissioners of these services will discuss the themes and decide on the next steps. Should these
options be approved for implementation, one of the key elements in the next phase of the programme
would be to enact the appropriate governance to ensure services only switch when they are ready to do
so, and provide the oversight mechanism to enable commissioners to assure themselves of this. This
approach will ensure that any service transfer is robustly implemented and that any impacts on other
services are fully mitigated.
Should the proposals be approved, the trusts would continue to work with the local community and key
partners to develop detailed plans to communicate the reconfiguration.

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 4
2. Introduction
The purpose of this report is to provide an overview of the second phase of engagement and
communications activities that were carried out for the proposals to improve specialist cancer and
cardiovascular services in north and east London and west Essex. This report provides a narrative of
the process, while the appendices provide a more detailed breakdown of feedback and the process
followed.
NHS England, the main commissioner for specialised services, together with local Clinical
Commissioning Groups (CCGs) and UCLPartners (UCLP), an academic health science network, led
engagement on the business case and commissioner preferred options for specialist cancer and
cardiovascular services. The engagement was supported by clinicians and carried out in line with the
objectives set out in the engagement plan (see Appendix A: Communications and engagement plan).
This means that:
The local and strategic impacts and benefits of the programme should be explained in order for all parties to form a clear view of the need for specialist centres
Stakeholders should be informed in good time during the evolution of the programme, enabling them to have a meaningful say and to influence its development
All parties, ranging from formal scrutiny through to local communities and patient groups, should have good access to accurate and high quality information on the programme, communicated at all stages of the planning for implementation work.
The second phase of engagement focused on seeking people’s views on the preferred options to
centralise specialist services for five types of cancer and cardiovascular disease. The overriding aim was
to ensure that all stakeholders were given the opportunity to feedback on commissioners’ preferred
options for change, and influence the planning for implementation work.
A five week period of engagement was undertaken between Friday 23 May and Friday 27 June 2014.
Stakeholders were asked to respond by the closing date; however feedback was accepted until Friday 4
July 2014.
An overview of feedback and themes gathered throughout the engagement is outlined in this overview report. More detailed feedback gathered from patients, the public, community groups and stakeholders through the engagement process, (either by the survey, in writing, or through focused discussions), is provided as part of a separate report, see Appendix E: Engagement feedback report.
3. Previous engagement informing the programme Engagement undertaken for specialist cancer and cardiovascular services builds on previous pan-
London and local engagement exercises, namely: Healthcare for London which engaged across the
capital; the London-wide 2010 review of cancer and cardiovascular services (led by the former NHS
organisation Commissioning Support for London); and previous engagement on specialist urological

Engagement overview report
Page 5
cancer services covering north and east London and west Essex undertaken in early 2013. The clinical
recommendations involved clinical and patient recommendations from an early stage.
In developing the clinical recommendations for change to specialist cancer services in north and east
London and west Essex, UCLPartners and London Cancer had previously undertaken an extensive
programme of stakeholder engagement. A wide range of stakeholders, including patient representatives,
GPs, and other clinicians (including a range of professions e.g. Clinical Nurse Specialists, oncologists
and radiologists) from every NHS trust currently providing cancer services in the locality, were involved
in the development of the clinical recommendations. Likewise, over 100 cardiac clinicians from across
the partnership were involved in developing the preliminary specialist cardiovascular proposals following
a wider stakeholder workshop in November 2012.
Phase one engagement
In order to develop commissioners’ preferred options for the future of specialist cancer and cardiovascular
services in north and east London and west Essex, NHS England and CCG partners engaged a wide
range of local stakeholders and residents to gain their views on, and experience of current services, and
to hear their aspirations for future health services. Between 28 October and 4 December 2013 NHS
England undertook a 38-day engagement exercise.
This process was supported by a commissioner-led case for change document providing key information
about existing specialist cancer and cardiovascular services, clinicians’ recommendations for the future
configuration of these services and the context for the engagement work and formed phase one of the
engagement exercise. The Case for Change is available at http://www.england.nhs.uk/london/engmt-
consult/
In the autumn 2013 (28 October to 4 December) discussions, we ran an extensive period of engagement
which included sharing the Case for Change with over 540 stakeholders, a series of drop in sessions for
members of the public and a range of meetings with patient, clinical and local authority groups. NHS
England received 130 comments or views during this period.
Following this initial engagement period, NHS England compiled the Phase One Engagement report; an
overview report with supporting appendices. This report and appendices are available on the
programme’s dedicated page on NHS England’s website: http://www.england.nhs.uk/london/engmt-
consult/
Overall, discussions during the first phase of engagement showed broad clinical and public support for
the need to improve patient outcomes and experience across the area and the need to bring specialist
services together (consolidation). Key issues included travel and transport for patients and their families,
how the specialist centres would work with local hospitals, and how/if the proposals would affect any
other hospital services such as the MTC at RLH. The programme considered all these issues in detail
during discussions at the options appraisal meeting, with clinical leaders at the hospitals in the region,
and with commissioners.
Options appraisal process
NHS England adopted a rigorous three-step process to achieve consensus on the best set-up for
specialist cancer and cardiovascular services for north and east London and west Essex. This took
place during the first engagement phase and was conducted by appraisal panels made up of patient

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 6
groups, clinicians and commissioners for each of the proposals. For the full report and details please
refer to the Business Case, available here: http://www.england.nhs.uk/london/engmt-consult/
Step 1: Developing a long list of possible options
Step 2: Arriving at a short list of possible options
Step 3: Appraising the shortlisted options
After establishing a safe and viable shortlist of options, panels of appraisers assessed the options
formally. The panels used an agreed set of criteria and weightings, with clinical quality (45%), patients’
experience (25%), and ability to deliver the change (20%) and research education and training (10%).
More information on this process is detailed in the Business Case available online:
http://www.england.nhs.uk/london/engmt-consult/
4. Developing the engagement plan The communications and engagement strategy for this programme was developed to promote
involvement and engagement with the public about the proposed service change. Originally developed
to ensure NHS England met its duty to promote involvement and consultation in any service change, the
legislation was updated with the passing of the Health and Social Care Act in 2012; the duty to engage
with the public when proposing service change remains enshrined in legislation, and formed a key part
of the programme.
Following the first engagement phase, the three Joint Health and Overview Scrutiny Committees
(JHOSCs) for the area (North Central London, Inner North East London and Outer North East London)
agreed that formal consultation was not required because the proposals did not amount to a substantial
change. This was dependent on continued engagement with patients and the wider community in the
subsequent phases of the programme.
The engagement plan was developed to ensure that all stakeholders (including patients, the public, clinicians and others) were informed about the proposals, and had ample opportunity to comment on commissioner’s preferred options and provider plans to support patients, arising from the equality impact assessment and in the first engagement phase. The plan was based on themes raised during the first phase of engagement (including impact on co-dependent services, travel and the patient pathway), and targeted at groups/ individuals who had previously engaged with the programme and with those identified through the equalities impact assessment (see below and Appendix A: Communications and engagement plan). The programme team discussed the proposed approach for engagement with local branches of Healthwatch to agree that the final plan was appropriate for local populations.
A number of dependencies were identified for this second phase of engagement:
An equalities impact assessment (EqIA) was developed as part of the initial business case. The outcomes of the assessment were used to refine the communications and engagement strategy to ensure potentially-impacted groups were involved in the programme
Endorsement of the recommendations by commissioners as outlined in the Business Case

Engagement overview report
Page 7
Phase two engagement took place just after a time of political change, with local elections taking place in May 2014. The elections inevitably resulted in changes to our political stakeholders, as councillors lost their seats and new councillors came on board
Planning for implementation the programme has worked with each of the providers affected by the proposals to understand the current levels of planning and resource dedicated to each proposal, including identifying the key risks associated with each proposal. The programme has made a series of recommendations to mitigate specific risks and developed a commissioner assurance framework to ensure any reconfiguration of services both continues to meet core service standards and delivers the expected benefits for patients.
During the first phase, people told us they wanted to know more about how the specialist centres would
work. This included wanting more information about travel and transport options, questions around how
the proposals would affect other hospital services and impact on other elements of the health care
system. The aim, therefore, when designing the next engagement phase, was to ensure that these
concerns and queries were addressed and answered and that patients and members of the public had
the opportunity to learn more about plans and speak to commissioners and clinicians about what steps
were being taken to address these concerns.
Equality – the preliminary proposals to improve specialist cancer and cardiovascular services in north
and east London and west Essex formed part of NHS England’s drive to reduce health inequalities and
the disparities in life expected between residents within the area and in the context of London-wide life
expectancies.
The programme team analysed whether the proposals for change would be likely to have an impact on
the groups identified in the EqIA, including older people, people with disabilities and people from more
ethnically diverse communities. While the EqIA demonstrated that there was no evidence of any group
being disproportionately affected by the proposals, every effort was made in designing the plan to
communicate with groups identified with protected characteristics, such as LGBT groups and Age UK,
providing the opportunity to contribute to the proposals. In addition, public documents were approved by
the Clear English Standard, and alternative language formats made available on request. The plan also
incorporated an offer to attend existing patient groups in local communities, to discuss the proposals.
The EqIA found that the proposals would not impact any of the groups disproportionately, but did show
that some services would be moving out of communities that are more ethnically diverse. Hospitals
providing specialist services under the proposals would need to make sure that people in those
communities would not be unduly affected. Should the proposals be approved, this is an area that will
continue to be monitored as part of the assurance process.
Travel – the programme team examined the net impact on travel times for those patients who, under the
proposals, would receive care at a different location. The EqIA which was published online, showed that
under the preferred options, travel time and distance would increase for some patients, particularly those
travelling from outer north-east London and west Essex. The EqIA recommended that providers could
consider whether there should be any mitigation for cancer patients with increased long or difficult
journeys, which was included in the plan for public workshops. Attendees were asked to comment on
trust draft travel and transport plans, to shape development should the proposals be approved. The

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 8
engagement plan was also communicated to all trusts across Essex, for dissemination to their respective
stakeholders.
Financial – The case for change was clinically-led, with the key aim being to improve patient outcomes
and save lives. The Business Case and supporting appendices, developed by NHS England, outlined
financial details about the proposed changes and were published on the programme’s dedicated page
on NHS England’s website. http://www.england.nhs.uk/london/engmt-consult/
London Clinical Senate Review
The clinically developed Case for Change applied guidance from the London-wide model of cancer
care and national service specifications, and proposed the consolidation of specialised prostate cancer
services into one centre of excellence at University College London Hospitals NHS Foundation Trust
(UCLH). During the first phase of engagement some respondents raised concerns about this proposal.
These included the impact of proposals with regard to travel and patient choice, preferring a two-site
model (at Barking Havering and Redbridge University Trust and UCLH), or a single model spanning two
sites. Additionally some respondents questioned the strength of the clinical evidence for a one site
model.
To address these concerns, and as part of their advisory role, the NHS England (London) Transformation Directorate engaged the London Clinical Senate with expertise relevant to each of the pathways and with no known conflict of interest to provide external clinical assurance. The Clinical Senate sits within NHS England and their role is to be a source of independent, strategic advice and guidance to commissioners and other stakeholders to assist them to make the best decisions about healthcare for the populations they represent. The Clinical Senate provided advice on whether NHS England (London) had adopted a sufficiently robust clinical process to arrive at the recommended options for the future configuration of these specialised services, considering the clinical involvement and evidence used. The Clinical Senate also provided advice on a specific aspect of the proposals to inform a recommendation on the future model and location/s of radical prostatectomies. The Senate’s report concluded that the process had been clinically robust and that there was a strong evidence base for proposals to bring specialist surgery for prostate cancer into one centre of excellence. It found significant support for the proposals from clinicians. The report was used to develop a dedicated public event on proposals for specialised prostate cancer services which was one of the four engagement events undertaken as part of this phase of engagement. The London Clinical Senate report and NHS England’s response are available at:
http://www.england.nhs.uk/london/london-2/engmt-consult/
5. Phase two engagement Following the first phase of work, engagement continued with public and patient input into the planning
for implementation work. This involved updates at JHOSCs, and at CCG boards, meetings with provider
staff, a public meeting to discuss areas of concern around potential impact of the proposal on the MTC
at RLH, meetings with local branches of Healthwatch to discuss the proposed approach to the next
engagement phase and others. For further information, refer to Appendix B: Communications activity log.
Following the launch of the engagement period on 23 May 2014, individuals and organisations were
encouraged to give their comments, views and feedback on the preliminary clinical proposals. Over 600

Engagement overview report
Page 9
key stakeholder groups were contacted, to ensure that they were fully apprised of commissioners’
preferred options for change.
In order to ensure that we reached out to communities within the protected characteristics identified, the
programme made contact with a range of new stakeholders, who had not previously engaged with the
proposals, including local Age UK branches and a number of LGBT charities and organisations.
Engagement from the newly identified stakeholders was variable, with requests for information on public
events, but limited attendance.
Contact was also made with all CCG communication or patient leads to make full use of existing events
to publicise engagement with their respective populations. This led to discussions at two existing public
and patient fora (Whipps Cross and City and Hackney). Dedicated engagement activities and
communications targeted groups with an interest in the proposals, and included all those who had
previously engaged in the process:
Members of NHS staff within local providers and commissioning organisations
Clinical Commissioning Groups
GPs
Staff within relevant hospital trusts and stakeholders in trusts outside London
Patient participation groups and support groups
Community and voluntary sector organisations
Local branches of Healthwatch
JHOSCs
Local Medical Committees and Royal Colleges
MPs and Assembly Members
All respondents from the first engagement phase
Full details of the activities and events are outlined in the appendices.
Scrutiny
The three pre-established Joint Health Overview and Scrutiny Committees (JHOSCs) serving the
boroughs in north and east London and west Essex have a nominated officer, each of whom was in
regular contact with the programme team and was invited to the public engagement events held in
November 2013.
Regular meetings and dialogue have been maintained with the three JHOSCs and Westminster OSC
before and during the engagement to understand their views and any requirement for further engagement
or consultation.
Following the first engagement phase, the three JHOSCs formally agreed that the proposals did not
require formal consultation because the proposals did not amount to a substantial change. They were
keen to ensure that engagement with local people continued to ensure that all stakeholders were fully
informed and involved in the development of the plans.
During the second engagement phase, NHS England kept the three JHOSCs informed and presented
updates to the committees at meetings for North Central London (27 June 2014) and will present to the

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 10
Outer North East London (22 July 2014). Members of the three committees representing the area also
attended some of the workshops.
GP commissioners
Letters were issued to all CCGs in north and east London, west Essex, informing them of the launch of
the second phase of engagement. Communication leads at trusts and CCGs across north and east
London received articles to upload to their internal and external websites. The programme team followed
up to ensure that this information was being cascaded to their GPs and respective populations, and to
find out what engagement activities were being planned which could be utilised to publicise the
programme and engagement.
For a full breakdown of how the engagement was publicised, see Appendix D: Promotion and Publicity.
Phase two engagement communications and activities
NHS England developed and published a Business Case, and as part of the second engagement phase,
compiled a public facing summary of this document, approved by the Clear English Standard. Both the
full and summary documents were published on NHS England’s website on 23 May 2014, and were
available in other formats on request. Both documents sought to explain how the proposed specialised
centres for cancer and heart care would work and show how the clinical aims of the Case for Change
would be achieved.
The Business Case provided information on the expected benefits of centralising specialist services for
cardiovascular disease and five cancer pathways: brain cancers; urological cancer (bladder, prostate and
kidney); head and neck cancer; blood cancer (acute myeloid leukaemia and haematopoietic stem cell
transplantation); and oesophago-gastric cancer. It also provided information on the London Clinical
Senate Review and the Impact Analysis carried out following phase one engagement.
Alongside this document, an online survey was published allowing stakeholders to give feedback on each
of the preferred options for change.
Building on the first phase of engagement, a range of activities were organised to provide the community
and our partners with the opportunity to engage with the programme. The programme has sought to be
socially inclusive by using various ways to present and explain the preliminary clinical proposals. In order
to ensure that the programme engaged with all interested and affected patient and community groups in
the area, the programme team worked with local patient representative groups, including branches of
Healthwatch and Age UK to receive their feedback and ensure that all affected groups across the patch
engaged as part of this phase.
Activities included:
Collating the commissioners’ preferred options as a high level summary of the Business Case.
This was distributed as a hard copy document to eight locations across the area, and in an on-
line format published on the programme’s dedicated page on NHS England’s website
Distributing letters issued to over 600 stakeholders, notifying them of the second phase of
engagement, including a copy of the business case and an offer to attend meetings of local groups
extended to all stakeholders

Engagement overview report
Page 11
Facilitating three public events held across the locality to give attendees the opportunity to
feedback on the proposals. Clinicians and staff from the trusts presented at each event and were
available for questions
Facilitating a dedicated workshop discussing the results of the London Clinical Senate Review of
proposals for specialised prostate cancer services
Advertising all public events in 14 local newspapers
Publicising all public events on CCG websites, where possible
Publishing information on the engagement and listing public events on the NHS England,
UCLPartners, London Cancer and participating trust websites
Tweeting engagement details via UCLPartners to over 700 followers
Sending partner trusts updates and information about engagement events to cascade to staff and
stakeholders
Contacting all locality clinical commissioning groups to check existing patient/ public events in the
local area. Relevant information was circulated on request to ensure engagement was publicised
across the area
Updating the London Cancer patient partnership group and the Heart Hospital’s patient group
Posting a reminder article on NHS England website to encourage responses/ feedback
Receiving feedback on the commissioners preferred options by 27 June 2014 and continuing to
receive feedback after this date.
A full list of the communications and engagement activities is provided at Appendix B: Communications
activity log.
General engagement workshops
In order to provide people with the opportunity to hear more about the clinical recommendations and
preferred options, four public engagement events were held across north and east London and west
Essex (see above for more detail). Locations were chosen in order to ensure proportionate coverage of
all areas potentially affected and with good transport links for members of the public to attend. The events
were publicised through the trust and CCG communications and engagement leads via their existing
channels. Advertisements were also taken out in 14 newspapers across the locality.
Three dedicated public engagement events were held in Romford, Whitechapel and Enfield. The
programme team also attended two existing patient and public groups in City and Hackney and Whipps
Cross on request.
Each event was introduced by commissioners, with clinicians then presenting the detail of the proposals,
and providing an example of how the proposals might work in practice. Each workshop took place over
a two hour time slot with clinicians and commissioners on hand to answer questions.
Since the first phase of engagement, trusts have started to develop their travel plans and policies in order
to mitigate concerns and ensure that the specialist centres will be able to work effectively. The workshops
provided attendees with the opportunity to learn about trusts’ plans regarding travel and transport issues,
and to raise any further areas for consideration.
As the programme continues, and if proposals are approved, work with providers will continue to look at
and develop mitigations for any adverse impacts on travel in more detail.

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 12
Display boards showed artists’ impressions of the proposed cardiovascular centre at St Bartholomew’s
Hospital and the Cotton Rooms, patient hotel accommodation at University College Hospital. Draft patient
information leaflets outlining travel support were provided by the trusts in order for members of the public
to offer their feedback on content.
Other materials available included:
Copies of the high level Business Case summary
Separate copies of the survey for people to fill out or take away to complete
Feedback box for responses
Copies of the Business Case
Copies of the Business Case Appendices
Copies of the Equality Impact Assessment
Copies of the Case for Change
Existing information leaflets used by trusts to outline travel support
A case study of a patient who has undergone specialist treatment at UCLH and has used the patient accommodation (to provide attendees with more information about how this works in practice)
Cards with website, email and all other contact details for the engagement period A dedicated email address was used ([email protected]) to receive feedback and
a commissioner contact was provided in all communications and engagement activities for questions,
queries or comments.
Workshop to discuss proposals for specialised prostate cancer services
In order to share and discuss the findings of the London Clinical Senate report with interested
stakeholders, and as part of the further engagement phase, a dedicated Prostate Services workshop
was held in Romford on 26 June 2014.
At the workshop, the Chair of the London Clinical Senate review provided an overview of the process
followed by the Senate. London Cancer’s Urology Pathway Director described the recommendations for
specialist prostate cancer services. Attendees had the opportunity to review the Clinical Senate report,
business case and other supporting materials and ask questions about the proposals. Queries were
addressed by clinicians from across the area including senior clinical leadership at BHRUT who support
the proposed changes
Some of the key themes raised at the meeting were around travel for patients living in outer north east
London, the need to see comparable outcome data, patient numbers at both BHRUT and UCLH, and the
importance of ensuring that patient records are transferred safely and effectively with the patient when
they move around the system as part of their treatment. For a full breakdown of the issues raised and
responses, please see Appendix E: Engagement feedback Report.
6. Outcomes of engagement – key themes A summary of the key issues raised during engagement is provided below. A more detailed feedback
report, is provided at Appendix E: Engagement feedback report.
The table below presents the total responses to the survey received for each of the service proposals,
and what proportion of the responses were supportive. Not everyone who responded to the survey

Engagement overview report
Page 13
included a response for each of the proposals. Where concerns were raised during the engagement
process, this has translated into a smaller percentage of respondents supporting the proposals.
A total of 159 responses were received from a range of stakeholder groups including clinicians (115)
patients and patient representatives (26), and various other local representative bodies. The results of
the clinicians are however skewed towards representatives from Bart’s Health (88).
Response
Group Brain
Head
&
neck
Bladder
&
prostate Renal
Haematopoietic
stem cell
transfer
Acute
myeloid
leukaemia
Oesophago-
gastric Cardiac
Yes 107 88 110 97 133 128 89 131
No 45 59 38 42 12 17 54 22
Total 152 147 148 139 145 145 143 153
% in
support 70% 60% 74% 70% 92% 88% 62% 86%
The results of the online survey indicated a majority support for each of the pathways. Some pathways
received stronger support than others however. Both the haematology and cardiac pathways received
the most support with in excess of 80% of all responses supporting the proposals.
Of the remaining pathways, while on balance respondents are supportive there is notable concern raised
by some clinicians working at the RLH site. For example 59 respondents were not supportive of the head
and neck proposal. Over 95% of these who responded ‘no’ were clinicians at Barts Health and a
significant proportion of those were part of the anaesthetic profession at the RLH. This feedback is
consistent with the feedback received through the other engagement activities and the programme
continues to work with Barts Health to develop sufficiently robust mitigation strategies in response.
For the specialist bladder and prostate proposals, just under three quarters of the 38 respondents who
were not supportive were from Barts Health on the basis of retaining surgical expertise at the trust for
services such as major trauma. Very few unsupportive responses (3) were received from patients
(ProActive and PHASE prostate groups) and one clinician in outer north and east London. The prostate
support group PHASE has also responded separately in a letter to the programme.
For the specialist renal proposals, a similar response pattern to bladder and prostate is observed.
Typically those resistant to the proposals are from Barts Health stating the need to retain surgical
expertise and the burden of travel on local RLH patients.
For the specialist oesophago-gastric cancer proposal, those not in favour were from Barts Heath. A
number of clinicians questioned the need to move the service from Barts Health given the strong
outcomes the service is currently achieving.
In summary while the survey revealed overall support for each of the proposals, it is clear there is still
concern largely from a sub-set of clinicians at Barts Health. Subject to final decision making,
implementation will need to take this into account and ensure there is strong clinical leadership and

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 14
agreed mitigations to address these concerns. The foundations of this work is described below in the
response to the MTC issue.
The table below identifies the key themes from the other engagement events that were held across the
area and how the programme intends to address them going forward.
General themes
What we heard How this will be addressed
Support for the proposals and the need to
consolidate specialist centres, giving
patients the best access to excellent care
and improved outcomes.
Support for the proposals is welcomed
Support for the concept of integrated
cancer systems and centralisation where
appropriate, balanced with the need to
ensure that the patient remains the priority
and at the centre when planning provision
of services.
Support for the proposals is welcomed.
All proposed changes are clinically driven and are intended to
improve patient outcomes and experience.
A need to focus on the importance of
prevention and early diagnosis.
NHS England fully agree this is a priority and is working with the
transferring cancer services teams and London Cancer on this. We
recognise the need to improve prevention and earlier diagnosis.
Projects are underway to address this including understanding why
so many people are only diagnosed with cancer when they are
admitted to A&E.
In addition to their work and involvement with these proposals, a
large part of UCLPartners’ work is focussed on early prevention and
diagnosis.
Travel, transport and geography
What we heard How this will be addressed
Comments were received from patients
who were prepared to travel for the best
available service. Concerns were raised
by approximately 25 stakeholders
regarding the ability of patients and their
families/ carers to travel to specialised
centres and the lack of parking available at
some central sites.
Patients will only travel extra distances when necessary – for
specialist surgery or treatment.
Providers have plans in place to help patients mitigate these
potential impacts which were presented at the engagement
workshops.
More detail on proposed mitigation by trust is outlined in Appendix
E: Engagement feedback report

Engagement overview report
Page 15
Impact on the Major Trauma centre at the Royal London Hospital
What we heard How this will be addressed
Key concerns were raised from a number
of respondents regarding the potential
impact on support services such as the
Major Trauma Centre at The Royal
London Hospital
See the section below for the response to this concern.
Specialist prostate cancer services
What we heard How this will be addressed
Some respondents (~30) expressed
concern about the proposals to
consolidate specialist bladder and
prostate cancer services to one site based
at UCLH, therefore transferring the
specialist services away from BHRUT and
the geographic area. Two of these
respondents included PHASE and
ProActive, prostate patient support
groups.
Recognising this concern, the programme engaged an independent
clinical review of the proposals considering both locations as
potential providers of the service. The London Clinical Senate took
on national advice concluding a single site model at UCLH was
preferable.
The programme engaged on this outcome and facilitated a
dedicated workshop held at Romford to present the findings.
Supporting this engagement were key members of the London
Clinical Senate and the clinical leadership at BHRUT.
The workshop was a useful question and answer session providing
attendees with an opportunity to ask questions and raise concerns.
These queries were addressed by clinicians from across the area
including senior clinical leadership at BHRUT who support the
proposed changes.
Key outputs from the workshop include the prostate support group
PHASE continue to oppose the proposals for specialist prostate
cancer reiterating their previous concerns relating to the support for
the service at BHRUT.
Workforce
What we heard How this will be addressed
~20 respondents raised concerns around
the potential effects of the proposals on
training for staff, as well as on morale of
staff.
Specific concerns related to the risk of
clinical staff cuts and downgrading
The aim of the proposals is to become world class leaders in
cancer and cardiovascular care. It is not to cut costs across
services, but to improve services to patients both locally and
nationally. The proposals would support the development of
specialist teams through education and training improvements and
more opportunities for sub specialisation.

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 16
What we heard How this will be addressed
Respondents raised the importance of
ensuring that plans were in place to retain
key staff, keeping them motivated and
committed. The importance of ensuring
that across-site working was managed
effectively was also raised
It is expected that there will be a need for some changes to staff
roles and locations. As part of the planning for implementation work,
commissioners are working with providers to ensure that HR
processes are in place to mitigate potential impacts on staff.
A joint HR working group has been established with key HR leads
at each trust to lead on this work
With regards to the proposed creation of an integrated
cardiovascular centre at St Bartholomew’s, there are no planned
redundancies and staff will be transferred over to Barts Health, with
full support and complying with NHS Terms and Conditions
Capacity and current performance at Barts Health
What we heard How this will be addressed
Six respondents raised concerns about
capacity within the current system,
including performance at Barts Health with
regards to Referral-to-Treatment (RTT),
administration and management issues.
Related comments included the
requirement for trusts to be able to support
an increased volume of activity, e.g.
laboratory support and ITU (intensive care
unit) facilities with activity transferring from
the London Chest and Heart Hospitals.
A major performance improvement programme is in place at Barts
Health.
Overall the proposed changes are expected to have a cumulative
beneficial effect on in-patient flow and RTT in the trust. More detail
on these proposals can be found in Appendix G: Provider
correspondence.
62 day wait performance at UCLH
What we heard How this will be addressed
A few respondents raised the current poor
62 day wait performance at UCLH and the
impact the proposals will have on the
ability for UCLH to achieve this important
performance metric
The programme has sought a letter of assurance from UCLH and
an action plan to address this point. More detail on these proposals
can be found in Appendix G: provider correspondence
Cancer specific

Engagement overview report
Page 17
What we heard How this will be addressed
Support has been shown for the concept
of an integrated cancer system.
The biggest area of concern raised at the stakeholder workshops for cancer patients relate to late diagnosis and this should be prioritised as part of any planning for implementation going forward.
Agreement on importance of early diagnosis. No concerns with
quality of local diagnosis, but many people with cancer often present
late, because symptoms develop later in the disease.
Waiting for confirmation on early diagnosis work from AW at UCLP
Cardiovascular specific
What we heard How this will be addressed
Respondents stated the importance of acute treatment centres in the area that were able to treat patients with heart attacks as quickly as possible. Comments included the requirement for capacity for patients with Cardiac Diseases and Adult Congenital Heart Disease.
The new centre at St Bartholomew’s Hospital will be a Heart Attack
Centre for the area along with the Royal London Hospital. The
majority of patients would live closer to the proposed integrated
centre at St Bartholomew’s Hospital.
Response to the impact on the Major Trauma Centre (MTC) at the Royal London Hospital (RLH)
The proposals aim to replicate the success of major trauma centres and stoke units by ensuring the small
number of cancer patients who require specialist treatment receive world class care.
The potential implications on the MTC have been recognised and a significant amount of work has been
undertaken to address this at a trust level and with commissioners as part of the planning for
implementation work. On review of the work undertaken to date the programme recognises that while
there are a number of challenges and risks, these risks are not unsurmountable and can be addressed
within the timeframes stated.
The below is summarised from a letter from Barts Health Medical Director Steve Ryan dated July 2014
(which can be read in full in Appendix G: Provider correspondence). This letter sets out the approach that
Barts Health have adopted to develop cross provider solutions to the risks raised by a number of Barts
Health clinicians. Key activities have included:
Setting up of effective governance to ensure all key experts are involved. This is being considered within a wider review of emergency standards
Seeking expert advice from London Cancer on options and recommendations

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 18
Establishing a dedicated core clinical advisory group which meets weekly and contains the Medical Director, at Barts Health, leading surgeons and anaesthetists. The group is responsible for ensuring risks are adequately defined and mitigations are appropriate
Key clinical issues have been identified including: o Neurosurgery: Surgeon availability: theatre staff skills o Head and neck: Surgeon availability, managing the complex airway o Upper GI: Surgeon availability, anaesthetic skills o Renal: Surgeon availability
Establishing of a wider reference group which has met twice since May containing a wider pool of clinicians across the relevant specialties
Developing a business plan for trauma neurosurgical posts
Informing the business planning meetings held at UCLH covering research, education (including postgraduate training) and risks to debate outputs from the reference group
The merger of the cancer and surgery clinical academic groups is nearing completion with the
appointment of a surgeon as its substantive director. The major trauma centre at The Royal London
Hospital was subject to a recent peer review where need for improvement was noted in the area of
rehabilitation and a business case has been developed.
Barts Health is considering its current emergency service standards as they apply to trauma and other
acute services:
Major team job planning is underway across all services with a focus on the 7 days a week imperative, daily consultant ward rounds, more direct engagement of consultants in delivering and shaping the emergency care response
Transforming Services, Changing Lives is the sector wide transformation process, beginning in spring 2014 with acute and specialised emergency care being one of its key workstreams. An associate medical director has been appointed to support the medical director and the clinical academic group director for emergency and acute care in delivering this agenda
The clinical director for emergency care is conducting a ward by ward audit of adherence to the Trust’s standards. The system design and baseline forms a major CQUIN (Commissioning for Quality and Innovation payment) this year (value>£2.0m).
The Director of Integrated Cancer for London Cancer is now working with the Barts Health’s Medical
Director on a three month programme which will deliver recommendations and options to deliver the
relevant mitigations and make recommendations to build on service excellence and standards. This work
began in early July and is systematically working through issues from the bottom up. This week the work
has focused on head and neck cancer, with key inputs from both the cancer and trauma surgical leads.
Real opportunities to develop further trauma excellence have been identified.

Engagement overview report
Page 19
7. Next steps A final Commissioner ‘meeting in common’ will be held on Friday 25 July 2014 with the majority commissioners with responsibility for commissioning these services, namely NHS England and Camden, City and Hackney, Barnet, Enfield, Haringey and Islington CCGs.
The key themes described above and their mitigations will be support and monitored through a revised governance structure for implementation and a commissioner assurance framework. Commissioners will seek assurance on the safety and readiness of services during and after implementation. As such, the next phase governance structure will need to be established to deliver the following functions:
• Seek assurances from providers that the services models:
• Support full pathway integration
• Ensure dependent services are not adversely affected
• Facilitate effective management of hand-offs across the pathway including the provision of timely patient information
• Ensure the continuity of patient care
• Provide for effective clinical and non-clinical staff rotas
• Be underpinned by a clear timeline with realistic and achievable phasing.
• Monitor an integrated end to end plan and manage any dependencies across pathways, providers, estates, workforce and IT
• Ensure there is a consistent approach across all pathways and providers with regards to the management of support services, travel, HR, access to patient information and the provision of information for patients
• Ensure lead providers are adopting a system-wide approach in implementing the new pathways
• Ensure capacity is in place prior to any service transition
• Ensure transfer of services between providers is managed safely and effectively
• Define world class standards and ensure benefits are being achieved in the long run.

Improving specialist cancer and cardiovascular services in north and east London and west Essex
Page 20
Appendices
Appendix A. Communications and engagement plan
Appendix B. Communications activity log
Appendix C. Event material
Appendix D. Promotion and publicity
Appendix E. Engagement feedback report
Appendix F. List of stakeholders
Appendix G. Provider correspondence

Appendix E: Engagement feedback report
Introduction
NHS England undertook a second phase of engagement on the case for change for specialist cancer and cardiovascular services in north and east London and west Essex, which ran formally between 23 May and 27 June 2014, although responses continued to be accepted until 4 July 2014.
Overall, support was demonstrated for each proposal and an understanding of the need for the consolidation of specialist services within an integrated system, and the need to improve outcomes across the area. The key concerns raised include the possible impact of the proposals on other services, and on travel and transport, many of which had been raised during earlier engagement.
A number of key themes emerged from the engagement exercise. At the individual proposal level, the majority of responses were supportive. Stakeholders who were supportive, agreed with the general principle of consolidating specialised services and willingness for patients to travel for the best services available.
A number of specific concerns were raised however, including the impact on travel, particularly for patients residing in outer north east London, the possible impact on co-dependent services (such as the Major Trauma Centre (MTC) at the Royal London Hospital (RLH)) and the move of prostate services from Barking, Havering and Redbridge University Hospitals NHS Trust (BHRUT) to University College London Hospitals NHS Foundation Trust (UCLH). The programme has responded to these concerns which are outlined in this report and sought to identify sufficiently robust mitigations from the relevant parties.
Engagement activities
The engagement overview report and this feedback report describe the engagement activities undertaken as part of the second phase. In summary, over 600 stakeholders were contacted as part of the programme, a series of public workshops were held, and programme representatives attended existing public and patient meetings to seek feedback on the proposals.
Feedback
In total, there were 254 responses from individuals and organisations including:
Clinicians across the area
Public and patient groups and service users (including PHASE and ProActive)
NHS organisations
Clinical Commissioning Groups (CCGs)
Healthwatch
In addition, the programme team received letters of support for the proposals from the following providers; Barking, Havering and Redbridge University Hospitals NHS Trust, Barts Health, Royal Free London NHS Foundation Trust and University College London Hospitals NHS Foundation Trust. These can be viewed in Appendix G: Provider correspondence.

Appendix E: Engagement feedback report
Page 2 of 15
Responses ranged from emails requesting detail on the public events, to hard and soft copy survey responses, which allowed respondents to comment on each proposal individually. Comments raised during the public workshops were also captured.
The table below presents the total responses to the survey received for each of the service proposals, and what proportion of the responses were supportive. Not everyone who responded to the survey included a response for each of the proposals. Where concerns were raised during the engagement process, this has translated into a smaller percentage of respondents supporting the proposals.
A total of 159 responses were received from a range of stakeholder groups including clinicians (115) patients
and patient representatives (26), and various other local representative bodies. The results of the clinicians
are however skewed towards from representatives from Bart’s Health (88).
Response
Group Brain
Head &
neck
Bladder
&
prostate
Renal
Haematopoietic
stem cell
transfer
Acute
myeloid
leukaemia
Oesophago-
gastric Cardiac
Yes 107 88 110 97 133 128 89 131
No 45 59 38 42 12 17 54 22
Total 152 147 148 139 145 145 143 153
% in support 70% 60% 74% 70% 92% 88% 62% 86%
The results of the online survey indicated a majority support for each of the pathways. Some pathways
received stronger support than others however. Both the haematology and cardiac pathways received the
most support with in excess of 80% of all responses supporting proposals.
Of the remaining pathways, while on balance respondents are supportive there is notable concern raised
by some clinicians working at RLH, Barts Health. For example, 59 respondents were not supportive of the
head and neck proposal. Over 95% of these respondents were clinicians at Barts Health and a significant
proportion of those were part of the anaesthetic profession at RLH. This feedback is consistent with the
feedback received through the other engagement activities and the programme continues to work with Barts
Health to develop sufficiently robust mitigation strategies in response.
For the specialist bladder and prostate proposals just under three quarters of the 38 respondents who were
not supportive were from Barts Health on the basis of retaining surgical expertise at the trust for services
such as major trauma. Very few unsupportive responses (3) were received from patients and clinicians in
outer north and east London.
For the specialist renal proposals, a similar response pattern to bladder and prostate is observed. Typically
those resistant to the proposals are from Barts Health stating the need to retain surgical expertise and the
burden of travel on local RLH patients.
For the specialist oesphago-gastric cancer proposals, those not in favour were from Barts Heath. A number
of clinicians questioned the need to move the service from Barts Health given the strong outcomes the
service is currently achieving.
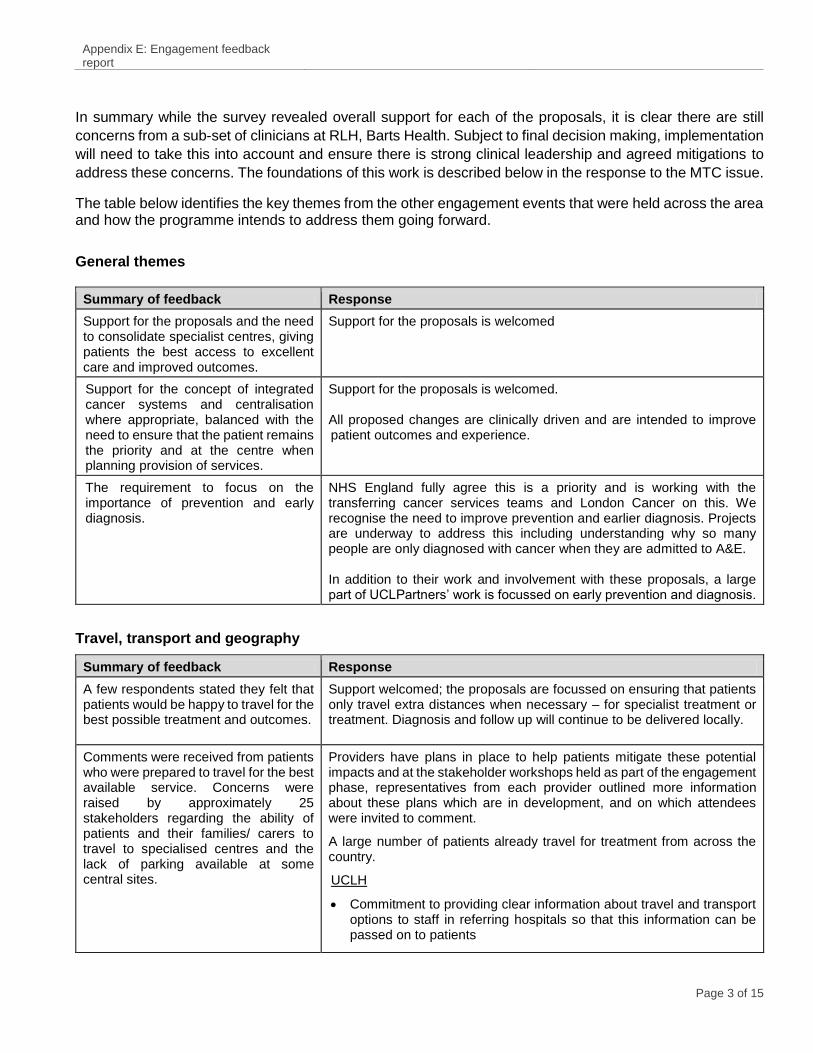
Appendix E: Engagement feedback report
Page 3 of 15
In summary while the survey revealed overall support for each of the proposals, it is clear there are still
concerns from a sub-set of clinicians at RLH, Barts Health. Subject to final decision making, implementation
will need to take this into account and ensure there is strong clinical leadership and agreed mitigations to
address these concerns. The foundations of this work is described below in the response to the MTC issue.
The table below identifies the key themes from the other engagement events that were held across the area and how the programme intends to address them going forward.
General themes
Summary of feedback Response
Support for the proposals and the need to consolidate specialist centres, giving patients the best access to excellent care and improved outcomes.
Support for the proposals is welcomed
Support for the concept of integrated cancer systems and centralisation where appropriate, balanced with the need to ensure that the patient remains the priority and at the centre when planning provision of services.
Support for the proposals is welcomed. All proposed changes are clinically driven and are intended to improve patient outcomes and experience.
The requirement to focus on the importance of prevention and early diagnosis.
NHS England fully agree this is a priority and is working with the transferring cancer services teams and London Cancer on this. We recognise the need to improve prevention and earlier diagnosis. Projects are underway to address this including understanding why so many people are only diagnosed with cancer when they are admitted to A&E. In addition to their work and involvement with these proposals, a large part of UCLPartners’ work is focussed on early prevention and diagnosis.
Travel, transport and geography
Summary of feedback Response
A few respondents stated they felt that patients would be happy to travel for the best possible treatment and outcomes.
Support welcomed; the proposals are focussed on ensuring that patients only travel extra distances when necessary – for specialist treatment or treatment. Diagnosis and follow up will continue to be delivered locally.
Comments were received from patients who were prepared to travel for the best available service. Concerns were raised by approximately 25 stakeholders regarding the ability of patients and their families/ carers to travel to specialised centres and the lack of parking available at some central sites.
Providers have plans in place to help patients mitigate these potential impacts and at the stakeholder workshops held as part of the engagement phase, representatives from each provider outlined more information about these plans which are in development, and on which attendees were invited to comment.
A large number of patients already travel for treatment from across the country.
UCLH
Commitment to providing clear information about travel and transport options to staff in referring hospitals so that this information can be passed on to patients

Appendix E: Engagement feedback report
Page 4 of 15
Summary of feedback Response
Immuno-compromised patients will continue to be eligible for NHS transport and will not have to share this with other patients
Ten free-of-charge disabled car parking bays. Commitment to increasing blue badge parking in vicinity. Also local street parking and nearby car parks.
Option of hotel accommodation prior to specialised surgery/ treatment.
Assessment of suitability/ quality of existing hospital patient transport service. Tender for new transport contract:
- A patient centric service
- A prompt timely service
- Good customer service
- Quality vehicles suitable for patient needs
- New features of service specification include; on the day reminder service of estimated pick up time, reduction in providers and commissioned for journey requirement rather than region
Barts Health
For cardiovascular care, based on patient data by borough, over three-quarters of outpatients and two-thirds of inpatients would have less distance to travel to the new centre at St Bartholomew’s Hospital, if proposals are implemented:
Current transport service for eligible patients; trust is considering its current travel arrangements.
Patients would only have to travel when absolutely necessary
Large public car park available opposite proposed new site.
The Royal Free
Draft patient information leaflet for specialised renal centre. Copies were made available at engagement workshops; feedback was welcomed.
Provision of patient navigator, whose main role is to provide advice on a range of issues including transport, parking, accommodation arrangements as well as appointments
Commitment to provide free parking for patients undergoing renal surgery.
Patient transport available for eligible patients
Patients who travel for surgery can choose if they would prefer to stay overnight prior to accommodation; room provided for the patient and immediate carer.
BHRUT
Free parking for all cancer patients undergoing treatment regardless of their home address

Appendix E: Engagement feedback report
Page 5 of 15
Summary of feedback Response
Discussion of possible improvements to local bus services
Patient transport available for eligible patients
Copies of travel information leaflets provided by the trust can be viewed in Appendix C: Event material
Work will continue between commissioners, UCLPartners and providers as part of the ongoing planning for implementation work to ensure that travel issues are identified and addressed prior to implementation.
Specialist prostate cancer services
Summary of feedback Response
Some respondents (~30) expressed
concern about the proposals to
consolidate specialist bladder and
prostate cancer services to one site
based at UCLH, therefore transferring
the specialist services away from
BHRUT and the geographic area. Two
of these respondents included PHASE
and ProActive.
Concerns encompassed issues such as
the loss of provision and skills away
from outer north east London and the
potential impact on patients (travel)
from these areas (including west
Essex).
Respondents wanted to be reassured
that there would be robust systems in
place to support urology patients in the
area having both benign and malignant
complex colorectal and gynaecological
surgery.
One respondent asked why the
prostate proposals could not be
amended to retain two centres for the
next few years, as is the case with
proposals for specialist oesophago-
gastric cancer services.
These proposals are about the creation of an integrated service which would be of significant benefit to patients.
Currently, four centres across the area currently serve over 3.2 million; services do not always meet national standards.
Following the first phase of engagement, NHS England requested an independent review led by the London Clinical Senate who in turn called on national experts from outside the area.
The London Clinical Senate reviewed the proposals for provision of specialist prostate cancer. It concluded that NICE guidance, recommending volumes of at least 150 robotic prostatectomy procedures per year per centre, should be followed. As a result of this, there can only be one compliant service in the area. A potential second site offering open or laparoscopic surgery raises equity concerns for the populations at each site.
Based on advice from and taking into consideration the options appraisal undertaken by NHS England during the first engagement phase, UCLH is proposed as the single centre for specialist bladder and prostate surgery
The programme engaged on this outcome and facilitated a dedicated workshop held at Romford to present the findings. Supporting this engagement were key members of the London Clinical Senate and the clinical leadership at BHRUT.
The workshop was a useful question and answer session providing attendees with an opportunity to ask questions and raise concerns. These queries were addressed by clinicians from across the area including senior clinical leadership at BHRUT who support the proposed changes.
Key outputs from the workshop include, the prostate support group PHASE continuing to oppose the proposals for specialist prostate cancer reiterating their previous concerns relating to the support for the service at BHRUT

Appendix E: Engagement feedback report
Page 6 of 15
Major trauma services
Summary of feedback Response
Queries included the possible impact
on co-dependent services, if
specialised services were to be
centralised. A significant cohort of Barts
Health clinicians responded to the
potential impact on the Major Trauma
Centre at the Royal London. This
included concerns about specialised
surgery for brain cancer transferring
from the site.
Concerns included questions regarding
the potential impact on recruitment,
retention and training (particular for
anaesthetists) of high quality staff and
clinicians.
Comments included support for current
services e.g. ear, nose and throat
services, and therefore questions about
the rationale for change.
The proposals aim to replicate the success of major trauma centres and stoke units by ensuring the small number of cancer patients who require specialist treatment receive world class care. The potential implications on the major trauma centre have been recognised and a significant amount of work has been undertaken to address this at a trust level and with commissioners as part of the planning for implementation work. On review of the work undertaken to date the programme recognises that while there are a number of challenges and risks, these risks are not unsurmountable and can be addressed within the timeframes stated. The below is summarised from a letter from Barts Health Medical Director Steve Ryan dated July 2014 (which can be read in full in Appendix G: Provider correspondence). This letter sets out the approach that Barts Health have adopted to develop cross provider solutions to the risks raised by a number of Barts Health clinicians. Key activities have included: Setting up of effective governance to ensure all key experts are involved. This is being considered within a wider review of emergency standards
Seeking expert advice from London Cancer on options and recommendations
Establishing a dedicated core clinical advisory group which meets weekly and contains the Medical Director, at Barts Health, leading surgeons and anaesthetists. The group is responsible for ensuring risks are adequately defined and mitigations are appropriate
Key clinical issues have been identified including: o Neurosurgery: Surgeon availability: theatre staff skills o Head and neck: Surgeon availability, managing the
complex airway o Upper GI: Surgeon availability, anaesthetic skills o Renal: Surgeon availability
Establishing of a wider reference group which has met twice since May containing a wider pool of clinicians across the relevant specialties
Developing a business plan for trauma neurosurgical posts
Informing the business planning meetings have been held at UCLH covering research, education (including postgraduate training) and risks to debate outputs from the reference group
The merger of the cancer and surgery clinical academic groups is nearing completion with the appointment of a surgeon as its substantive director. The major trauma centre at The Royal London Hospital was subject to a

Appendix E: Engagement feedback report
Page 7 of 15
Summary of feedback Response
recent peer review where need for improvement was noted in the area of rehabilitation and a business case has been developed. Barts Health is considering its current emergency service standards as they apply to trauma and other acute services
Major team job planning is underway across all services with a focus on the 7 days a week imperative, daily consultant ward rounds, more direct engagement of consultants in delivering and shaping the emergency care response
Transforming Services, Changing Lives is the sector wide transformation process, beginning in spring 2014 with acute and specialised emergency care being one of its key workstreams. An associate medical director has been appointed to support the medical director and the clinical academic group director for emergency and acute care in delivering this agenda
The clinical director for emergency care is conducting a ward by ward audit of adherence to the Trust’s standards. The system design and baseline forms a major CQUIN (Commissioning for Quality and Innovation payment) this year (value>£2.0m).
The Director of Integrated Cancer for London Cancer is now working with the Barts Health’s Medical Director on a 3 month programme which will deliver recommendations and options to deliver the relevant mitigations and make recommendations to build on service excellence and standards. This work began in early July and is systematically working through issues from the bottom up. This week the work has focused on head and neck cancer, with key inputs from both the cancer and trauma surgical leads. Real opportunities to develop further trauma excellence have been identified.
UCLPartners
Summary of feedback Response
Comments were received supporting
the excellent academic back up
provided through UCL Partners.
These comments are noted and welcomed
Workforce
Summary of feedback Response
~20 respondents raised issues around
the potential effects of the proposals on
training for staff, as well as on morale of
staff.
The aim of the proposals is to become world-class leaders in cancer and cardiovascular care. It is not to cut costs across services, but to improve services to patients both locally and nationally. The proposals would support the development of specialist teams through education and training improvements and more opportunities for sub specialisation

Appendix E: Engagement feedback report
Page 8 of 15
Summary of feedback Response
Concerns were raised the proposals
would result in clinical staff cuts and
downgrading.
Respondents raised the importance of
ensuring that plans were in place to
retain key staff, keeping them motivated
and committed. The importance of
ensuring across-site working was
managed effectively was also raised.
It is expected there will be a need for some changes to staff roles and locations. As part of the planning for implementation work, commissioners are working with providers to ensure that HR processes are in place to mitigate potential impacts on staff. With regards to the proposed creation of an integrated cardiovascular centre at St Bartholomew’s, there are no planned redundancies and staff will be transferred over to Barts Health, with full support and complying with NHS Terms and Conditions.
Capacity and current performance at Barts Health
Summary of feedback Response
Six respondents raised concerns about
capacity within the current system,
including performance at the Barts
Health with regards to Referral-to-
Treatment (RTT), administration and
management issues.
Comments around capacity included
the requirement for trusts to be able to
support an increased volume of activity,
e.g. laboratory support and ITU
(intensive care unit) facilities with
activity transferring from the London
Chest and Heart Hospitals.
A major performance improvement programme is in place at Barts Health. The below is summarised from a letter from Barts Health Medical Director dated 10 July 2014 (which can be read in full in Appendix G: Provider correspondence) There are a number of factors which are believed to have contributed to issues around Referral to Treatment standards at the trust, all of which are now being addressed and corrected. Through the use of waiting list initiatives and other methods, capacity has been created in the short term whilst longer term solutions are secured These proposals are expected to significantly assist in improving the trust’s Referral-to-Treatment (RTT) performance:
Head and neck – the proposed reconfiguration involves the largest number of patient episodes, in the order of 400 annually. A large proportion of these patients require critical care as part of their pathway of care and therefore this will free up critical care (usually HDU (high dependency unit)) capacity. This will improve flow for patients needing these pathways for other complex surgery. In addition, significant theatre capacity will be made available at The Royal London Hospital
Neurosurgery – a significant number of patients (~100 a year) needing treatment result in the neurosurgery ward being very often full. This prevents flow out of critical care and access for patients awaiting spinal surgery. The high demand of emergency pathways places a strain on the elective pathways which is often reflected in RTT difficulties in neurosurgery. Again, significant theatre capacity will also be made available
It is also expected that there will be a benefit in relation to urology patients, with more than 50 surgical episodes a year beginning to be relocated to the Royal Free Hospital.

Appendix E: Engagement feedback report
Page 9 of 15
Summary of feedback Response
With regards to the proposed changes to specialist oesophago-gastric cancer services, this will significantly improve flow in and create additional capacity in theatres which again can be used to improve RTT performance
Overall the proposed changes are expected to have a cumulative beneficial effect on in-patient flow and RTT in the trust.
62 day wait performance at UCLH
Summary of feedback Response
A few respondents raised the current poor 62 day wait performance at UCLH and the impact the proposals will have on the ability for UCLH to achieve this important performance metric
The programme has sought a letter of assurance from UCLH and an action plan to address this point. More detail on these proposals can be found in Appendix G: Provider correspondence
The current underperformance against the 62 day cancer standard has received considerable focus at executive, divisional and team levels. UCLH have as a result undertaken a range of improvements cutting across all tumour pathways. These include:
Developing a protocol to help us understand all drivers of any breach of the 62 day standard
Consolidating all learning from these breach analyses into a rolling improvement plan, along the lines of a urology action plan
Establishing a new role to strengthen corporate validation and monitoring, for example through the development of a trust-wide training programme and leading a systematic approach to the identification and dissemination of best practice and learning from breaches.
Setting up a new daily reporting and escalation process for patients on two week wait referral pathways to reduce the time taken to book their appointments.
Volume of service
Summary of feedback Response
Queries were made as to the actual volume of service likely to transfer.
The case for change and the Business Case reported on activity volumes
based over the period Feb 2012 – Jan 2013. Given the volumes for cancer
are relatively small, the exact numbers are inherently variable year by
year, however, local clinicians working on the planning for implementation
work are in general agreement regarding the approximate size of services
transferring.
The clinical case
Summary of feedback Response
There was strong support for the clinical case to support Barts Health as
The clinical case for change recognised a number of constraints of the current facilities for cardiovascular services, a number of which are the result of limited capacity within The Heart Hospital. With limited scope to

Appendix E: Engagement feedback report
Page 10 of 15
Summary of feedback Response
the provider of specialist cardiovascular services
expand due to physical constraints The Heart Hospital is unlikely to be able to achieve the volume required to meet recommended standards of care for both elective and non-elective care. Capacity at The Heart Hospital is limited as it is in a central London location with no room to expand. As a result there was no option to retain The Heart Hospital. (The decision to move services from The London Chest Hospital was made some time ago and does not form part of this review)
Barts Health currently provides good outcomes with regards to cardiovascular services and the creation of a new integrated cardiovascular centre at the trust will bring more activity to the site strengthening the trust overall.
A robust options appraisal was conducted by NHS England during the first phase of engagement to assist in developing commissioners’ preferred options for change. Further detail on this can be found from page 51 of the Business Case available online: http://www.england.nhs.uk/london/engmt-consult/
Expected benefits, quality of care and patient choice, patient pathway
Summary of feedback Response
A few respondents requested
assurance that private patients would
not be treated to the detriment of NHS
patients.
The proposals would seek to significantly improve outcomes and experience for NHS patients, not place them at a disadvantage. Any such departure from this ethos would be investigated by trust boards and the appropriate measures would be taken to prevent this from happening
A few respondents asked for further
clarification about the patient benefits of
the proposals, querying whether higher
volumes would be more beneficial to
surgeons as opposed to patients.
The benefits of the proposals are focused on improving outcomes for patients. The programme team have worked with national health analysts to examine the benefits. We are also conscious of the importance of developing effective and accurate metrics and are therefore using international benchmarks in our work with clinicians.
Respondents queried about the
availability of clinical trials for patients.
If implemented, the changes would mean much better access to the latest treatments and technology through more access to clinical trials for patients. The aim is to offer the majority of patients the option of joining a clinical trial. It would also result in specialist care available 24/7, and shorter waiting times.
Some respondents expressed concern
about the quality of care at some sites
across the area and asked that these be
addressed as part of the ongoing work.
The vision of these proposals is to create world class services as part of an integrated system of care. Currently, care is fragmented and varies across hospitals. This is because specialists, technology and research are spread across too many hospitals to provide the best round the clock care to patients. The model of care that was developed by commissioners in 2010 found that these inconsistencies could be addressed by concentrating specialised services in fewer, larger centres in order to deliver world class standards of care and address fragmentation of services.

Appendix E: Engagement feedback report
Page 11 of 15
Summary of feedback Response
Concerns were expressed by some
respondents that the transfer of some
specialist services would result in a lack
of care for patients, placing some at a
disadvantage.
The aim of the proposals is to improve outcomes and access to excellent care and treatment for all, not to place patients at any disadvantage.
A small number of respondents queried
whether the proposals would run
contrary to the NHS’ principle of
providing free, local care to those who
need it.
The NHS will remain free at the point of need for all. All specialist services being looked at as part of this review, would remain free to all who need them
Respondents were keen to ascertain
the process that would be adopted with
regards to the patient’s journey through
the system. This ranged from queries
about follow up care and appointments
to discharge procedures, to avoiding
possible duplication of pre-op
assessments.
The majority of care would continue to be provided locally. Patients would only travel to a specialist centre for specialist surgery or treatment.
Across the system, patients will only be discharged from the centre when they are fit to leave. A discharge summary would be sent to a patient’s GP, local hospital and clinical nurse specialist. In most cases, follow up appointments would be limited to one follow up appointment at the specialist centre with all other follow-up taking place locally.
As part of the planning for implementation work, providers are each developing their plans to ensure a coordinated pathway from diagnosis through to treatment and aftercare. This will form a key part of the on-going commissioner assurance framework.
One respondent queried the potential arrangements for patients diagnosed with more than one cancer.
The ultimate aim of the proposals is to save lives through the creation of centres of excellence for specialist surgery and treatment for some cancers and cardiovascular service. The vast majority of all care and treatment would remain local, including diagnosis and care after any surgery. Every patient is an individual, and therefore each patient’s journey through treatment, including the location, would be developed between the doctor, specialist and the patient, to deliver the best clinical outcomes in line with the patient’s wishes.
Some respondents were concerned
that the recommendations did not
reflect some of the current excellent
outcomes from providers across the
area.
There are some excellent examples of outstanding care being delivered across the area for patients with cancer and heart disease. However, outcomes for patients in London are not as good as the rest of the country.
The aim is to achieve a consistently high standard of care, not dependent on where people live. By concentrating services in dedicated centres of excellence, clinicians believe it is possible to improve outcomes for patients – not only survival rates but also improving the quality of life for people after specialist treatment or surgery. NHS England has looked at international evidence that demonstrates that centres seeing higher volumes of patients generally achieve better patient outcomes.
Patient records
Summary of feedback Response
Some respondents wanted to know how the different hospitals would be able to access patient records and how
We recognise it is vitally important that patient records are transferred safely and efficiently.

Appendix E: Engagement feedback report
Page 12 of 15
Summary of feedback Response
the records would be transferred through the system.
Queries were received regarding how communication between different parts of the system would work. What systems have been devised to ensure that each team at each site from GP to local hospital to specialist centre knows what is happening?
One of the workstreams of the planning for implementation work is dedicated to ensure that this is managed properly.
This is already working successfully for other services that people have to travel for, such as radiotherapy and these proposals would seek to emulate successful arrangements that are already in place.
An example of the system that is already in place across trusts is the ‘cloud system’ which is used by urology pathway clinicians. This involves the immediate uploading of scan images which are then transferred to ensure they travel with the patient through the system.
UCLP are currently expanding on this work. The aims of this are to:
Make the best use of available data across the partnership ensuring that information is managed safely and patient confidentiality is protected
Develop a single system approach so that there are consistent approaches to information sharing across the partnership and information can be used to drive improvement across whole pathways of care
Promote connectedness to ensure care providers have the information they need to deliver safe and effective care irrespective of their care setting or geography.
Finance
Summary of feedback Response
A few respondents were interested in
whether cost is taken into consideration
when planning proposed service
change. These respondents were keen
to ensure that no trust is financially
compromised by the proposed service
changes and that there is active
engagement now with commissioners,
patients and patient groups outside
London about the changes being
planned.
One respondent queried why individual
costs (i.e. cost of radical
prostatectomies) are not included in the
Business Case.
Comments were received about the
investment undertaken at individual
sites for cancer pathways and whether
this now represents a waste of money if
services are to be transferred
The key driver for the proposed changes is clinical with the focus being to save lives and improve outcomes.
In order to facilitate a funding agreement for proposals, a financial advisor was jointly appointed to work with all parties to agreed terms of reference.
All financial analysis has shown that the proposals are affordable, including the costs of implementation. Changes which would, most importantly, help save over 1200 lives a year also represent value for money for the taxpayer and all organisations involved.
The Business Case is not intended to go into procedure level detail. The analysis shows the differential cost impact, through the market forces factor of different providers. All financial analysis has shown that the proposals are affordable for providers.
All investment in individual sites is still current and will be utilised by providers and result in benefits for local patients

Appendix E: Engagement feedback report
Page 13 of 15
Scope
Summary of feedback Response
One respondent questioned the scope of the maps used in the Case for Change, asking what would happen to patients living outside the areas shown on these maps.
The maps used in the Case for Change (available here:
http://www.england.nhs.uk/london/engmt-consult/) aim to show the geography of the 12 trusts across the area only. The maps used are not designed to show catchment areas for treatment. Patients can be referred for treatment who live outside these areas, which will be dependent on patient choice and doctor’s advice.
Engagement process
Summary of feedback Response
Some respondents queried why formal
consultation was not undertaken on the
proposals and the length of time given
for engagement and notice of events.
The programme has undertaken a robust approach to engagement including two engagement phases and continued dialogue at all stages
Following the first phase of engagement, all three Joint Health Overview and Scrutiny Committees (JHOSCs) for the area agreed that the proposed service changes did not represent significant service change and did not therefore require formal consultation.
Phase two engagement activities included:
Collation of commissioners’ preferred options into a high level, Clear English Standard approved, summary. This was distributed via email and made available in hard copy at eight locations across the patch and at all engagement events, and at CCG and Healthwatch engagement events across the area (full details can be viewed in Appendix D: Promotion and publicity). This was also made available on the programme’s dedicated page on NHS England’s website and alternative formats of this were available on request
Letters were distributed including details of the second engagement phase to ~600 stakeholders and follow up phone calls were made to all local branches of Healthwatch and Age UK/Age Concern to ask them to publicise the engagement and events
In addition, the programme team made contact with all clinical commissioning groups (CCGs) and providers with several of these publishing information on their websites
Three public events were held across the locality to give attendees the opportunity to provide feedback on the proposals. Clinicians and staff from the trusts presented at each event and were available for questions.
A dedicated workshop discussing the results of the London Clinical Senate review into proposals for specialised prostate cancer services, was held in the outer north east London area
Details of these engagement events were advertised in 14 local newspapers
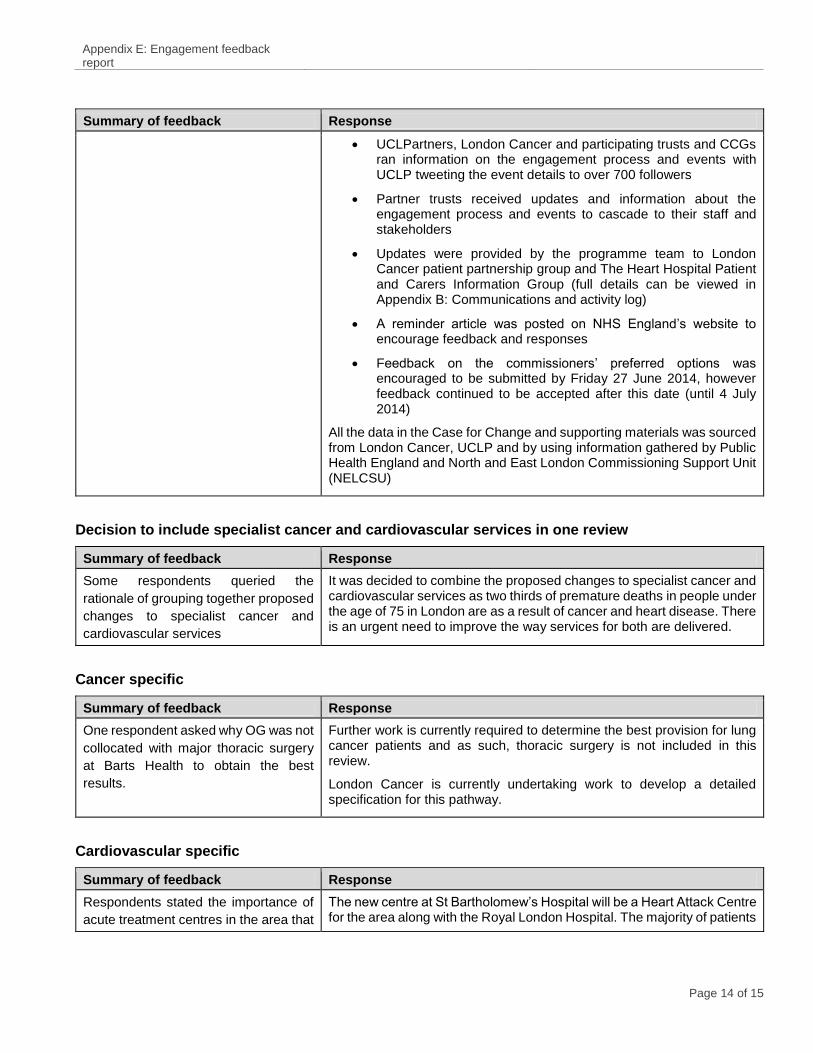
Appendix E: Engagement feedback report
Page 14 of 15
Summary of feedback Response
UCLPartners, London Cancer and participating trusts and CCGs ran information on the engagement process and events with UCLP tweeting the event details to over 700 followers
Partner trusts received updates and information about the engagement process and events to cascade to their staff and stakeholders
Updates were provided by the programme team to London Cancer patient partnership group and The Heart Hospital Patient and Carers Information Group (full details can be viewed in Appendix B: Communications and activity log)
A reminder article was posted on NHS England’s website to encourage feedback and responses
Feedback on the commissioners’ preferred options was encouraged to be submitted by Friday 27 June 2014, however feedback continued to be accepted after this date (until 4 July 2014)
All the data in the Case for Change and supporting materials was sourced from London Cancer, UCLP and by using information gathered by Public Health England and North and East London Commissioning Support Unit (NELCSU)
Decision to include specialist cancer and cardiovascular services in one review
Summary of feedback Response
Some respondents queried the
rationale of grouping together proposed
changes to specialist cancer and
cardiovascular services
It was decided to combine the proposed changes to specialist cancer and cardiovascular services as two thirds of premature deaths in people under the age of 75 in London are as a result of cancer and heart disease. There is an urgent need to improve the way services for both are delivered.
Cancer specific
Summary of feedback Response
One respondent asked why OG was not
collocated with major thoracic surgery
at Barts Health to obtain the best
results.
Further work is currently required to determine the best provision for lung cancer patients and as such, thoracic surgery is not included in this review.
London Cancer is currently undertaking work to develop a detailed specification for this pathway.
Cardiovascular specific
Summary of feedback Response
Respondents stated the importance of
acute treatment centres in the area that
The new centre at St Bartholomew’s Hospital will be a Heart Attack Centre for the area along with the Royal London Hospital. The majority of patients

Appendix E: Engagement feedback report
Page 15 of 15
Summary of feedback Response
were able to treat patients with heart
attacks as quickly as possible.
Comments included the requirement for
capacity for patients with Cardiac
Diseases and Adult Congenital Heart
Disease.
would live closer to the proposed integrated centre at St Bartholomew’s Hospital.
Next steps
The feedback the programme team received over the engagement phase has been fed into this report and will inform the planning for implementation work, should the proposals be approved to proceed.
A second commissioner ‘in common’ meeting will be held on 25 July 2014, where the majority commissioners of these services will discuss the themes and decide on next steps.
Should the proposals be approved, the trusts would continue to work with the local community and key partners to develop detailed plans to communicate the reconfiguration.
Further detail about this process can be viewed in the Engagement overview report available online at: http://www.england.nhs.uk/london/engmt-consult/

1
Cancer/Cardiac
Implementation framework
Programme team
25thJuly 2014

Table of contents
2
Section Page
Introduction 3
Proposed implementation governance 5
Key programme risks/issues and mitigations 8
Commissioner Assurance Framework 11
Current assessment against framework 14
Commissioner oversight of system wide quality benefits 20
Next steps 22
Annex: Provider Assurances 24

INTRODUCTION

Introduction
4
This paper presents the outcome of the planning for implementation work undertaken by the
programme and by the lead providers. The purpose of the paper is to:
• Define the proposed implementation governance – The current governance structure must
be revised to ensure it is fit for purpose by transitioning the responsibility for implementing the
changes to the lead providers
• Highlight the key implementation risks/issues for the programme – The programme has
identified key risks/issues both through the engagement period and implementation planning
work. The programme has sought assurances from the relevant risk/issue owners that
mitigations are in place
• Describe the proposed Commissioner Assurance Framework – The programme
recommends a series of Commissioner gates to act as key assurance check points across the
implementation period
• Assess current progress against the Commissioner Assurance Framework – The
programme has worked with providers to review the status of their current implementation
planning and identified key priorities by pathway
• Set out the key decisions and next steps

IMPLEMENTATION GOVERNANCE
5

The diagram illustrates the overarching structure with responsibility for implementing the services changes
Implementation governance
Joint Programme
Board
UCLH cancer
programme
Barts Cardiovascular
programme
Pathways
Op
era
tiona
l En
ba
lers
RFH Renal cancer
transition
Barts HealthBHRUT UCLHRFH
AHSC/N
(clinical and academic
leadership and setting
world class standards)
Op
era
tiona
l En
ba
lers
Op
era
tiona
l En
ba
lers
6
The role of the Joint Programme Board is to:
• Assure individual pathway and project plans
for service reconfiguration
• Oversee delivery of the provider and
pathway-level plans for implementation
• Review progress against provider and
pathway-level plans for implementation,
acting as a checkpoint for commissioner
assurance purposes
• Make recommendations to providers /
pathway-level plans for successful
implementation
• Maintain an overview on service
performance during reconfiguration –
advising existing commissioner quality and
performance infrastructure where
appropriate
It is proposed that membership for the Joint Programme Board is drawn from the following organisations:
Commissioning representation (NHS England, CCG Lead Commissioners)
Clinical Director lead NHS England (Medical or Nurse Director lead)
Provider/ Pathway Lead representation (management lead, with clinical leadership for pathway-specific discussions –
to be determined by reconfiguration timetable)
National Trust Development Agency
London Cancer/ UCLPartners
Transforming Cancer Services Team representation
Programme support

What does this governance structure need to do
7
If commissioners agree to changes in service provision, they will seek assurance on the safety and readiness
of services before and during reconfiguration. As such, the next phase governance structure will need to be
established to deliver the following functions:
• Seek assurances from providers that the services models:
• Support full pathway integration
• Ensure dependent services are not adversely affected
• Facilitate effective management of and-offs across the pathway including the provision of timely
patient information
• Address any adverse impacts to patients and carers from specific protected characteristic groups
• Ensure the continuity of patient care
• Provide for effective clinical and non-clinical staff rotas
• Be underpinned y a clear timeline with realistic and achievable phasing
• Monitor an integrated end to end plan and manage any dependencies across pathways, providers, estates,
workforce and IT
• Ensure there is a consistent approach across all pathways and providers with regards to the management
of support services, travel, HR, access to patient information and the provision of information for patients
• Ensure lead providers are adopting a system-wide approach in implementing the new pathways
• Ensure capacity is in place prior to any service transition
• Ensure transfer of services between providers is managed safely and effectively
• Define world class standards and ensure benefits are being achieved in the long run

KEY RISKS/ISSUES RAISED THROUGH
PHASE 2
8

The key risks/issues and mitigations (1/2)
9
A number of key clinical points of consideration were raised throughout the second phase of engagement and
as the programme supported the provider planning for implementation work. These are summarised in the
table below along with how they have been addressed.
What we have heard How will this be addressed
Major Trauma Centre
Risk that the loss of cancer surgeons
(especially neurological surgeons) will have
a destablising impact on the MTC. This risk
in turn led to some concerns from pockets
of clinicians at Barts Health
Commissioners and providers are committed to the MTC. A dedicated programme
of work has been established to mitigate this risk and is being led by the Medical
Director at Barts Health. Details of the activities currently underway to resolve the
clinical risk to the MTC and in turn build support for the proposals among Barts
Health clinicians can be found in the annex to this report
Anaesthetist training rotas
The move of services may impact the
ability of providers to meet the anaesthesia
training curriculum
Providers need to collectively engage HEE and develop a detailed solution.
Service standards
Risk that receiving providers are unable to
deliver service standards with an expanded
service
Receiving providers must be able to deliver on existing contractual obligations
regarding service standards. Commissioners must be assured that the new
service models will robustly deliver improved standards via the gateway process.
The programme has sought assurances from providers on two key performance
points which are outlined in the annex to this report:
• Barts Health RTT - A major performance improvement programme is in place
at Barts Health. Overall the proposed changes are expected to have a
cumulative beneficial effect on in-patient flow and RTT in the trust.
• UCLH 62 day waits - The programme has sought a letter of assurance from
UCLH and an action plan to address this point

10
A number of key deliverability risks were raised throughout the second phase of engagement and as the
programme supported the provider planning for implementation work. These are summarised in the table
below along with how they have been addressed.
What we have heard How will this be addressed
System leadership for the Cancer Pathways
The review recognises that to establish a strong clinical
support base it was not appropriate for any one organisation to
assume a leadership role. However going forward this will be
required to develop system-wide improvements
• Roles and responsibilities need to be agreed and
documented for sender and receiver Trusts
• UCLH as lead provider needs to ensure all workstreams
and boards ensure the appropriate involvement from
across the system (all providers) – the Workforce
workstream was identified as an area where this was
working well and should be replicated
Clinical leadership for the Cancer Pathways
Clinical leadership is not always defined both at the sending
and receiving trusts (eg the need for a cancer clinical lead at
BH). Engagement feedback suggests pockets of resistance
from clinical groups (eg anaesthetists at RLH)
• Pathway Board attendance must be facilitated from all
organisations with nominated deputies to ensure full
representation
• Boards need to be supported by the appropriate team
resources to ensure the decisions are taken forward into
detailed plans
Resourcing the change
A dedicated programme management team / PMO is needed
to work with both sending and receiving providers, and this
needs to be in place before the Programme Director arrives in
September to ensure momentum is maintained
• Funding agreed through the transitional funding agreement
• UCLH to appoint an interim PMO and ensure all
workstreams are resourced adequately beyond simply
clinical input / clinical time
The key risks/issues and mitigations (2/2)

COMMISSIONER ASSURANCE
FRAMEWORK
11

A gateway approach to commissioner assurance
12
Commissioner Gates
Scope and
approach
1 2 3
Is scope
understood and
is approach
appropriate?
Is a feasible plan
in place with
appropriate
resourcing and
governance?
Are providers
delivering against
plan?
4
Are services
ready to switch?
5
Have services
switched
successfully in
the short run?
6
Has the switch
delivered
sustainable
benefits in the
long run?
Detailed
planningDelivery
Repeated /
ongoing
Issue
resolution
Benefits
realisation
Clinical advice / oversight
One of the key elements in the next phase of the programme will be to enact the appropriate governance to ensure services only
switch when they are ready to do so, and providing the mechanisms to enable commissioners to assure themselves of this. This
approach will ensure that any service transfer is robustly implemented and that any impacts on other services are fully
mitigated. To this end, the programme proposes a staged six gate process, at which a set of service readiness indicators will be
examined for each pathway.
The programme is at the beginning of this process, and as such there is significant work to do to develop detailed plans, service
models and mitigations against key issues.
The assurance checks will be used to ensure the right elements are in place, and the right actions being taken to get them in
place. We have a double lock, with providers commitment on key risks and actions in place, as well as the framework below:
Provider activity
Repeated /
ongoing

Key points of consideration at each gate
13
Commissioner Gates
1 2 3
Is scope
understood and
is approach
appropriate?
Is a feasible plan
in place with
appropriate
resourcing and
governance?
Are providers
delivering against
plan?
4
Are services
ready to switch?
5
Have services
switched
successfully in
the short run?
6
Has the switch
delivered
sustainable
benefits in the
long run?
Repeated /
ongoingRepeated /
ongoing
• Is scope clear?
• Is a plan in place?
• Is the plan
resourced with an
appropriate team?
• Are clinical risks
identified/ are the
mitigations
defined?
• Are other risks
identified with
defined
mitigations?
• Are key
stakeholders
engaged /
supportive?
• Is a detailed
operating model
defined?
• Are detailed ways
of working
defined?
• Is plan being
delivered?
• Is the patient
pathway clearly
defined?
• Are enablers in
place?
• Are equality
issues being
addressed?
• Is capacity in
place?
• Are stakeholders
supportive?
• Is there an agreed
set of clinical,
quality and
performance
service readiness
indicators that are
specific to the
proposals?
• 1 – 2 months post
transition
• Do services
continue to
perform against
the clinical, quality
and performance
indicators?
• Ongoing
• Are services
delivering against
the expected
clinical benefits
outlined in the
original case for
change?
In order to assure readiness to switch, at each checkpoint, commissioners will assure provider plans against a
series of proposed indicators, based on contractual, quality and information requirements.

CURRENT ASSESSMENT AGAINST
FRAMEWORK
14

Approach and summary of the implementation planning
assurance
15
This section presents the findings of an assurance exercise on the planning work currently
underway by each of the pathways by applying the framework discussed in this report. The
aim is to present the current status of each of the pathways, identify key clinical and
deliverability risks and ensure appropriate structures are in place to manage these risks
through implementation.
A planning for implementation assurance framework was developed and reviewed at the
Programme Board on the 6th June 2014. This framework was shared with each of the Trusts
and Pathway Directors as an aide to gather the evidence. The programme team carried out
the review over June 2014, drawing off the following evidence:
• Pathway Board meetings
• Cross pathway business planning meetings
• One to one meetings with each of the Pathway Board Directors/Service leads/Programme
Directors
• Supplementary documentation provided individually by each pathway

Status summary by pathway (1/2)
16
Retained
providers
(Lead)
Transition
date
(Spells)
Summary
BR
AIN
AN
D S
PIN
E
(UCLH)
BHRUT
Dec
2015
It is recommended that the National Hospital for Neurosciences (UCLH) and the Queen’s Hospital (BHRU)
are retained as the two units in the area providing neurosurgical cancer services. The Pathway Board have
met frequently to oversee the development of the service specification and initial planning for the centres.
The role of the Pathway Board will largely be advisory going forward and the responsibility for
implementing the service changes will rest with UCLH and BHRUT. An agreed governance structure will be
established promptly once a commissioner decision is made to ensure dedicated resources are assigned
to implementation.
Key co-dependency issues have been identified in regards to major trauma at BH and mitigations are in
place following the leadership of the Pathway Board and the Medical Director at BH. A tentative date for
the transition of services at BH to UCLH and BHRUT has been set for the end of 2015. Close engagement
of the NHNN capital works programme is crucial. It is expected a single SMDT between BH and UCLH can
be implemented prior to the physical move on an interim basis with the BHRUT SMDT operating as it is
currently.
(120)
HE
AD
&N
EC
K
(UCLH)
July
2015
Initial planning work was outlined in the UCLH response to the London Cancer service specification and
was selected by the London Cancer Pathway Board as the preferred option.
The Pathway Board has met regularly since the London Cancer assessment and has started the process
of identifying key clinical risks and developing mitigations. These centre around the impact on co-
dependent services/support services at BH and the requirement for support services both at UCLH and
locally for diagnostics and follow up care.
The Pathway Board agree these risks can be mitigated, however detailed planning work is required in
order to meet the transition date. A governance structure to oversee the implementation will be agreed and
mobilised, following the commissioner meeting including detailed planning to define and agree the
workforce and training models with clinicians across the system.
(240)
UP
PE
R G
I
(UCLH)
BHRUT
July
2015
The London Cancer Pathway Board has met frequently since considering the proposals submitted by
BHRUT and UCLH to become specialist centres of excellence.
Through the work of the Pathway Board, significant progress has been made building the necessary
clinical support across the trusts. The pathway would benefit from a dedicated resource to lead on ongoing
planning work.
Two SMDTs are proposed including the current SMDT at BHRUT and an SMDT at UCLH which will
consolidate the existing BH SMDT. Common guidelines and protocols are already in place across both and
the Pathway Board will facilitate joined up working between the two providers to implement the pathway.
Job planning is underway and while there are a number of co-dependency related issues at BH to work
through, these are expected to be mitigated through a model of joint appointments.
(50)
Scoping Detailed
planningReady to
implement

Status summary by pathway (2/2)
17
Retained
providers
(Lead)
Transition
date
(Spells)
Summary
BL
AD
DE
R&
PR
OS
TA
TE
(UCLH)
July
2015
Initial planning work was outlined in the UCLH response to the London Cancer service specification and
was recommended by the London Cancer Board as the preferred option, agreed by Commissioners and
accepted by the Clinical Senate review process. The response described the patient pathway which has
now been adopted by UCLH.
Since the development of the response, three SMDTs are now in place across the area (UCLH, BH,
BHRUT) and the Pathway Board have overseen the development of common guidelines to ensure the
patient pathway is consistent. These guidelines will be available by August 2014. Services at Whpps X and
BCF are now provided at UCLH with minimal impact on remaining services at those sites. Key next steps
include agreeing and planning for the transition of services from BHRUT to UCLH, developing/securing a
joint appointment consultant position between BHRUT and UCLH and developing the interim capacity at
the Heart Hospital.
(90)
RE
NA
L
(RFH)
March
2015
With the transfer of surgical activity from BCF and the creation of the clinical pathways and protocols, the
SMDT and SMDT clinic, are in place and have been tested and embedded. The bed and theatre capacity
is in place (one dedicated theatre and 10 inpatient beds), currently running at 40 – 50% capacity.
The next phase will include transferring cases from BHRUT and BH. This will be achieved in a phased
manner starting with T1 tumours with the potential for nephron sparing or minimally invasive treatments
being discussed at the SMDT with tele-conferencing links involving the local surgeons from September
2014. This will allow robust links and patient pathways to be established for these few selected cases prior
to the complete transfer of renal cancer cases in March 2015.
(270)
HA
EM (UCLH)
BH
BHRUT
July
2015
The Pathway Board has drafted a programme governance structure and conducted initial scoping work for
the key workstreams to oversee the changes relating to Haematology services in the area. This
governance structure will support a programme of work to transfer services from RFH to UCLH and
reconfigure the remaining services at RFL in light of the acquisition of BCF.
Recommendations developed by the cancer/cardiac programme relate to Level 2b and 3 Services. The
Pathway Board and the respective Trusts have also identified clinical benefits of transferring Level 2a and
2b services from RFH to UCLH (while retaining BCF as a Level 2b service). The programme governance
structure and work streams have therefore been developed according to the wider configuration as the key
tasks would be performed in parallel. However the decision required for Level 2a services will require
engagement with local commissioners to understand how to take it forward. This initial scope question will
need to be resolved before detailed planning.
(70)
CA
RD
IAC
(BH)
Jan
2015
The programme has a clear approach with well defined plans and workstreams that are able to ensure a
clinical model that is operationally supported. There is strong system leadership across the pathway.
UCLPartners and Professor Richard Bohmer (Harvard Business School) are supporting the transformation
leads in developing these models. The programme is running a set of operational pathway/functional
workshops with lead clinicians and staff from UCLH and BH to develop the patient pathways / service
model. This initial design work, together with the design of the workforce models will be ongoing through
Q2 14/15. Governance of the programme will be managed through a series of staged gates to review
deliverability and workstream progress. The first of these reviews is expected in early Aug 2014 and the
second prior to transition in Nov 2014.
(5,000)
Scoping Detailed
planningReady to
implement

Status against Commissioner assurance gates and priorities
18
Pathway
Status against gate 1 + 2 checks
PrioritiesScope defined
Plan /
approach
documented
Team/
governance in
place
Clinical risks
and mitigations
identified
Delivery risks
and mitigations
identified
Stake-holders
fully engaged
Cardio-
vascular✔ ✔ ✔ ✔ ✔ ✔
BH have designed two internal readiness
checks. Share approach with
commissioners prior to first August check
Renal ✔ ✔ ✔ ✔ ✔Agreement
with BHRUT
on timing
Engagement with BHRUT regarding the
period/process of transition of services
Bladder /
Prostate✔
Not fully
documented,
but scale of
move is small
Pathway
Board but not
dedicated
team
✔
Risks identified
however
mitigations
require owners
Fuller pathway
board
representation
needed
Documentation and formalisation of
approach
Engage commissioners on 62 day
performance issues
AML /
HSCT
To determine
whether level 2a
services are
included
Level 2a issue
to be resolved ✔ ✔
Risks identified
however
mitigations
require owners
✔Resolve scope challenges on level 2a
services
OG ✔
Approach
understood
but not yet
documented
Pathway
Board but not
dedicated
team, across
both Trusts
✔
Risks identified
however
mitigations
require owners
✔
Document and formalise approach
Engage commissioners in variation
across two SMDT models and explain
how the two SMDTs will work
Head &
Neck✔
Approach
understood
but not yet
documented
Pathway
Board but not
dedicated
team
✔
Risks identified
however
mitigations
require owners
Some challenges
from anesthetists
re MT
Document and formalise approach
Resolve co-dependency issues, including
anaesthetist training
Brain ✔
Approach
understood
but not yet
documented
Pathway
Board but not
dedicated
team, across
both Trusts
✔
Risks identified
however
mitigations
require owners
Some challenges
from local
clinicians
3 plans need to
be integrated
Document and formalise approach
Resolve co-dependency issues
Clarify how two regional SMDTs will work

UCLH Tower
London Heart
NHNN
RFH
Queen’s
Hospital
King George
Hospital
Royal London
St
Bartholomew’s
London Chest
UC
LH
RF
HB
HR
UT
Bart
sH
ea
lth
Q3 14/15 Q4 14/15 Q1 15/16 Q2 15/16 H2 15/16
Head + Neck
Bladder / Prostate
OG
AML / BMT
Cardiovascular
Brain
Renal
AML / BMT
Brain
AML / BMT
OG
Bladder / Prostate
Renal
Head + Neck
Renal
Brain; OG
Cardiovascular
AML / BMT
Cardiovascular
RE-FIT
Brain
Renal
AML / BMT
Brain
AML / BMT
OG
Cardiovascular
AML / BMT
CLOSED
RE-FIT
Brain
Renal
AML / BMT
Brain
AML / BMT
OG
Cardiovascular
AML / BMT
CLOSED
Head + Neck
OG
AML / BMT
Bladder / Prostate
Brain
Renal
Brain
AML / BMT
OG
NOT SPECIALISED
Cardiovascular
AML / BMT
CLOSED
Head + Neck
OG
AML / BMT
Bladder / Prostate
Brain
Renal
Brain
AML / BMT
OG
NOT SPECIALISED
Other services
Cardiovascular
AML / BMT
CLOSED
Head + Neck
Renal
Brain; OG
Head + Neck
Brain
OGBrain
Chase Farm
BC
F
AML (2b) AML (2b) AML (2b) NOT SPECIALISED NOT SPECIALISED
Head + Neck
Bladder / Prostate
OG
AML / BMT
Head + Neck
Bladder / Prostate
OG
AML / BMT
Bladder / Prostate
RenalBladder / Prostate
Potential high level phasing of the pathway moves

COMMISSIONER OVERSIGHT OF SYSTEM
WIDE QUALITY BENEFITS
20

21
Barts HealthBHRUT UCLHRFH
CRG CQRM
Super CQRM /
Cancer
Super CQRM /
Cardiovascular
AHSC/N
CRG CQRM CRG CQRM CRG CQRM
Recommendation for introduction of system-wide quality and performance review mechanism (‘Super
Clinical Quality Review Meeting - CQRM) for cancer and cardiovascular services, for commissioner
oversight on system-wide issues, with recommendation for system-wide KPIs focusing on the following
themes:
• Core standards
• System leadership
• Clinical leadership
• Patient experience
• Outcomes
• Clinical practice
Each provider continues to
be responsible for delivery
against core contractual
standards (monitored
through existing contract
review group/ clinical quality
review groups)
Academic Health Science
Centre/ Network responsible
for provider oversight, and
for definition/ measurement
of expected world class
benefits
Overseeing benefits realisation across system

NEXT STEPS AND KEY DECISIONS
22

23
Next steps and key decisions
The following decisions are required by commissioners:
• Agree the implementation governance structure including the role of the
joint programme board
• Proposed timeline for establishing Joint Programme Board by
September 2014
• Agree the approach set out in the commissioner assurance framework
• Note the current status of the planning for implementation work by
pathway

Annex: Provider assurances
24

25
Barts Health – RTT Performance
RTT and specialist cancer surgery – Letter received from Dr Steve Ryan, Medical Director Barts Health
There have been significant issues with compliance with the Referral-to-Treatment (“RTT”) standards at Barts Health, which are well known to
commissioners. There is a major improvement programme in place to improve performance. In addition, a harm review programme has been put in
place to monitor, detect and intervene in patients and cohorts of patients where necessary. This is led by the Deputy Medical Director and assured
under the leadership of the Deputy Medical Director for NHS England (London). The issues relate to key themes: firstly, a widespread historical
practice (from our legacy organisations) in non-compliance to scheduling in precise chronological order of referral. This practice is now ended, and it
is expected that patient journeys compromised by this problem will be dealt with by year end. The second relates to demand versus capacity, which
has been a specific issue with certain pathways in urology, neurosurgical spinal care (a national issue) and orthopaedics. Work is proceeding in all
these areas to match capacity and demand and ensure in-hospital patient flow does not compromise quality of care and outcome by RTT or other
issues. Our response has been to supply additional capacity in the short term by waiting list initiatives and the use of the private sector. To sustain
this in the longer term, other initiatives are in place including a theatre productivity programme, strengthening the systems and culture for effective
daily working on wards, and improvements in outpatient flow. The proposed specialist surgical cancer reconfigurations are expected to significantly
assist in improving our RTT performance as follows:
1. Head and neck – this reconfiguration involves the largest number of patient episodes, in the order of 200 annually; since a large proportion of
these patients require critical care as part of their pathway of care, it will free up critical care (usually HDU) capacity, which will improve flow for
patients needing these pathways for other complex surgery. In addition, significant theatre capacity will be made available at the Royal ondon
Hospital to allow us to design patient flows through the programmes mentioned above.
2. Neurosurgery – a significant number of patients (> 100/year); the neurosurgery ward is often full due to high throughput and highly complex
patients requiring monitored-beds and this prevents flow out of critical care and access for patients awaiting spinal surgery. The high demand of
emergency pathways puts a real strain on the elective pathways, which is reflected in RTT difficulties in neurosurgery. Again, significant heatre
capacity will also be made available and it will also assist flow of head-injured and neurovascular patients on emergency pathways as well as
RTT issues.
3. There is also expected to be benefit in relation to urology patients, with more than 50 surgical episodes per year beginning to be relocated to the
Royal Free Hospital. This will have a clear benefit on urology RTT pathways.
4. The upper-gastrointestinal changes, again around 50 cases per year, will significantly improve flow in and create additional capacity in theatres,
which can be used to drive RTT performance.
In summary these changes have cumulative beneficial effects on two of our key “pinch-points” inpatient flow and RTT - critical care and theatres.
They will also have an effect on demand for "inepisode” diagnostics, which is helpful in RTT performance. The diagnostics, critical care and theatre
capacity for the cardiovascular changes will have no impact on our RTT problems as this capacity is ring-fenced at the St Bartholomew’s site.
I hope these comments are helpful and demonstrate that the significant population health benefits of the cardiovascular and cancer proposals will
address issues that Barts Health is dealing with in terms of RTT performance and bring a double benefit.

26
Barts Health – Major Trauma (1/2)
Improving specialist cancer and cardiovascular services: trauma co-dependencies – Letter received from Dr Steve Ryan, Medical Director
Barts Health July 2014
Further clinical engagement and progress has been made in examining the important co-dependencies, risks concerns and beginning to define the
broad mitigations and solutions.
Headlines
1. Effective governance has been set-up to ensure all key experts are involved
2. This is being considered within a wider review of emergency standards
3. Expert advice is being sought from London Cancer on options and recommendations
Governance and workstream structures
Core clinical advisory group
• Meets weekly
• Contains MD and lead surgeons and anaesthetists
• Responsible for ensuring risks are adequately defined and mitigations are appropriate
• Group is producing paper on critical care cancers
• Key clinical issues identified in May were:
• Neurosurgery: Surgeon availability, theatre staff skills
• Head and Neck: Surgeon availability, managing the complex airway
• Upper GI: Surgeon availability, anaesthetic skills
• Renal: Surgeon availability
Reference group
• Has met twice since May
• Contains wider pool of clinicians across the relevant specialties
• Each service was able to define the key areas of concern.
• For neurosurgery a business plan for trauma neurosurgical posts is to be developed.
• Business planning meetings held covering research, education (including postgraduate
• training) and risks to debate outputs from the reference group
Merger of surgery and clinical academic groups
The merger of the cancer and surgery clinical academic groups is nearing completion with the appointment of a surgeon as its substantive director.
As I said in May, the Major Trauma Centre was subject to a recent peer review where need for improvement was noted in the area of rehabilitation
and a business case has been developed.

27
Barts Health – Major Trauma (2/2)
Improving specialist cancer and cardiovascular services: trauma co-dependencies – Letter received from Dr Steve Ryan, Medical Director
Barts Health July 2014
Wider system work on emergency standards
Barts Health is considering how it improves its current emergency service standards as they apply to trauma and other acute services. Major team
job planning exercise is underway across all services with a focus on the 7 days a week imperative, daily consultant ward rounds, more direct
engagement of consultants in delivering and shaping the emergency care response.
Transforming Services Changing Lives is the sector wide transformation process, beginning in Spring 2014 with acute and specialised emergency
care being one of its key workstreams.
An associate medical director has been appointed to support the medical director and the clinical academic group director for emergency and acute
care in delivering this agenda. The clinical director for emergency care is conducting a ward by ward audit of adherence to the Trusts standards. We
are seeing real traction. The system design and baseline forms a major CQUIN this year (value > £2.0 m).
London Cancer review
Mairead Lyons the Director of Integrated Cancer for London Cancer is now walking with the Barts Health’s Medical Director on a 3 month
rogramme which will deliver recommendations and options to deliver the relevant mitigations and make recommendations to build on service and
standards. This work began in early July and is systematically working through issues “from the bottom up”. This week the work has focused on
head and neck cancer, with key inputs from both the cancer and trauma surgical leads. We see real opportunities to develop further trauma
excellence.

28
UCLH - 62 Day Wait Performance (1/2)
UCLH 62 day cancer waiting times performance assurance Nick Kirby – Cancer Divisional Manager July 2014
UCLH remain fully engaged in the ongoing process for assuring commissioners of the planning and capability at UCLH to deliver effective patient
care across the five specialist cancer pathways. I have set out below details concerning our performance management infrastructure and specific
actions being taken to improve our 62 day cancer waiting time performance.
UCLH has a strong track record for managing performance against the full spectrum of commissioner and regulatory performance standards over a
number of years. Over this time period there have been occasions where our performance has deviated from the expected standard for
performance against the 62 day standard; as an organisation we have repeatedly demonstrated our capacity to learn, recover and improve our
performance.
The current underperformance against the 62 day cancer standard has received considerable focus at executive, divisional and team levels. We
have as a result undertaken a range of improvements cutting across all tumour pathways. These include:
Developing a protocol to help us understand all drivers of any breach of the 62 day standard
We will be consolidating all learning from these breach analyses into a rolling improvement plan, along the lines of the urology action plan that I
attach to this letter
Establishing a new role to strengthen corporate validation and monitoring, for example through the development of a trustwide training programme
and leading a systematic approach to the identification and dissemination of best practice and learning from breaches.
Setting up a new daily reporting and escalation process for patients on 2 week wait referral pathways to reduce the time taken to book their
appointments.
Recent performance analysis shows that the driver underpinning the 62 day wait performance challenges relates to one tumour group: Urology. I
have attached the details of the specific action plan which has been developed to target improvement in this area. The Urology leadership team and
commissioners met on 10th July to discuss the issues associated with the failure of urology to meet the 62 day standard. We understand that
commissioners agreed that this did not in any way indicate clinical risk and that the service offered on the prostate cancer pathway was world-
leading in terms of outcomes. We feel that patients are placed at the very heart of decisions about their care and that as a result patients had a
positive experience. We agreed with commissioners that we could improve that experience further by removing some of the delays on the pathway,
and that our breach analysis and action planning would be key tools for continuously improving our service to patients. We also agreed with
commissioner that we would spread best practice concerning clinical pathways and models of care with referring trusts where this will help shorten
waits and improve care for patients across the sector.

29
UCLH - 62 Day Wait Performance (2/2)
UCLH 62 day cancer waiting times performance assurance
A long standing contributing factor to the 62 day wait performance concerns late referrals from partner organisations. Given the absence of a
binding national policy on late referrals it has been only recently and with limited success that other organisations have been prepared to accept
responsibility for breaches where patients have been referred to UCLH after day 42 of their cancer pathway. We are working with colleagues in the
sector through UCLPartners and nationally through the Shelford Group to help inform and drive this policy agenda. This will not however distract
from the prime objective, which is to work across provider boundaries to improve the entire patient pathway.
The opportunity provided by the planned integration of specialist cancer pathways in neuro-oncology, urology, upper GI, head & neck and haemato-
oncology presents a platform for UCLH to lead this improvement. The clinical leads and multidisciplinary teams are clear that there lies an
opportunity to work across the cancer healthcare system to improve patient pathways. Our intention is that this will deliver multiple benefits, most
notably in the form of clinical outcomes. It is also true that the process of pathway transformation brings a genuine opportunity to shorten the period
of time patients wait for their cancer treatment. In stating this ambition we appreciate the critical role of commissioners, patients and partner
hospitals in co-designing the changes and are realistic in understanding the effort and time it will take to realise the potential benefits in full.

30
UCLH - 62 Day Wait Plan (1/4)
Issue Action Actions & Progress Update Who Responsible By when
Late Referrals Improve the speed of referral and quality of
information received into UCLH
Mark Emberton to write a letter to London Cancer
Pathway Director (JH) to ask for support in
improving pathways at referring Trusts to reduce
late referrals. In particularly this relates to Trusts
that use TRUS and which then necessitates long
delay before MRI can provide diagnostic value.
Mark Emberton (Consultant
Urologist)
July 2014
(changes to
pathways at other
Trusts will be a
longer term action)
CWT Tracking Recruit additional support for MDT Urology
Coordinator role to improve tracking and resource
available to expedite appointments
A business case has been written to secure an
additional 1.0 WTE Urology MDT coordinator, this
post will be presented to vacancy scrutiny panel
on 14th July. In short term an existing staff
member has been deployed to this post to
support from 14th July 2014.
Sam Arthur/Becky Dennett
(Urology-Oncology Service
Managers)
July 2014
Variable MRI Quality within
London Cancer Trusts leads to
repeated scans being required
and delays when referred for
treatment decision at centre.
Standardise MRI scan quality within LC Mark Emberton to write to London Cancer
Pathway Director (JH) to ask for support in
improving MR quality across the network.
Create contact directory of Uro-Radiologists
within all LC Trusts I
Invite radiologists to participate in regular
forums to support training, research and
create protocols to include in London Cancer
Prostate Cancer Guidelines
UCLH to host radiology workshops
to support training within Network
UCLH to select LC Trust to partner with and
assist in developing another specialist uro-
radiology department within Network
Mark Emberton
Lois Roberts
Alex Kirkham (Uro-
Radologist)
Alex Kirkham
Mark Emberton
July 2014
Complete
August 2014
Ongoing
(Quarterly)
September 2014
[1] HIFU is a type of cancer treatment. Doctors give the treatment using a machine that gives off high frequency sound waves. These waves deliver a strong beam to a
specific part of a cancer.

31
UCLH - 62 Day Wait Plan (2/4)
Issue Action Actions & Progress Update Who Responsible By when
Delays in Imaging Reporting Work with Imaging to reduce
delays in time from scan to
report.
Issues have been escalated to the Imaging department DCD and DM
and Medical Director (GB) is working closely with them to reduce
reporting time.
A report is produced on a weekly basis detailing patients with outpatient
appointments and unreported scans. This is used to prioritise reporting.
Any target patients identified in this list; and any other targets identified
from the CWT tracking meeting are escalated for immediate reporting.
A new radiology consultant is to be appointed. Interview has been set
up in July 2014. In addition an existing radiology consultant has
increase sessions dedicated to uro-radiology.
Charles House (DCD) / Hugh
Jelley (DM)
Information Team / Hugh
Jelley
Hugh Jelley
Action plan
currently in place
Currently in use
Sept start date
anticipated
Aug 2014
Delays in Imaging
Appointments
Work with Imaging to reduce
delays in time from scan
request to scan appointment.
Issues have been escalated to the Imaging Department DCD and DM.
MRI and CT scanner capacity at Heart Hospital will be released early
2015.
Saturday working has commenced and basic scans will be outsourced
to release further capacity for specialist scans such as prostate MRI.
Charles House / Hugh Jelley
Jo Moss (Deputy Strategy
Director)
Hugh Jelley
Action plan in
place
April 2015
July 2014
Robotic Capacity Reduce the current wait from
DDT to Robotic Surgery
Extra equipment has been purchased to increase the number of
procedures performed on a single operation list from two to three
(on appropriate clinical cases). Additional anaesthetic consultants
and surgeons required to reduce turn-around time between cases.
First 3 session list scheduled for September.
Saturday operating commenced in June 2014 (currently monthly).
Additional scrub staff training required to expand to weekly.
The possibility of additional theatre capacity at HCA via the
Princess Grace is being investigated. Trust level negotiations have
commenced.
Capital Plan submitted to purchase second robot in 2015. Theatre
capacity will also increase when the Heart Hospital reopens in
early 2015.
Sufi Husain (Urology GM)
Therese Parker (DM
Theatres)
Lois Roberts (Surgery DM)
Lois Roberts
August 2014
March 2015
August 2014
March 2015

32
UCLH - 62 Day Wait Plan (3/4)
Issue Action Actions & Progress Update Who Responsible By when
Pathways for all Urological
Cancers
Best practice pathways for all
Urological Cancers to be
produced for reference.
Robotic pathway completed and reviewed. Focal therapy pathways
completed pending clinical sign off. Penile and bladder cancer
pathways to be designed based on current pathway guidelines.
Rebecca Dennett August 2014
Root Cause Analysis Improve RCA to record all
delays in patient pathway
More detailed RCA will be performed on all patients breaching the 62
day pathway. This will include all breach reasons and indicate all areas
where days were lost.
The last 6 months of RCA will be reviewed to look into more detailed
explanations for breach and to split breaches by type of tumour,
treatment and whether it was a tertiary referral.
If tertiary patient, send RCA to referring Trust so they are able to see
reasons for breach and any contributing factors (such late referral or
requirement to duplicate scan) will be highlighted.
MDT coordinator/Rebecca
Dennett
Rebecca Dennett
Rebecca Dennett
August 2014
August 2014
August 2014
Lack of clarity around content
of trials and definitions of when
treatment starts
Develop and circulate a clear,
written definition of treatment
for all urology trials.
Summary list of trials produced by BD
CWT review of trials
Agreement on treatment start points and definition per trial
UPDATE July 2014
A letter has been drafted in conjunction with the focal therapy clinicians
and the CWT team for patients that are referred for consideration of
focal therapy. A letter will be sent to patients that are perusing focal
therapy where the SMDT has agreed that all treatment options are
available. The letter states that the patients will be classified as
receiving active monitoring prior to any decision about whether to
pursue focal therapy. The letter references sections 3.9.48, 3.9.49 and
3.9.50 and 3.10.59 of v8.0 of CWT guidance.
Rebecca Dennett/
Prav Chitrapu (Cancer
Waiting Times Manager)
August 2014
Delays in Histology Reporting Work with histology department
to reduce reporting times for
specimens particularly template
biopsies
Waiting time for histology reports currently reduced to three weeks.
Additional histopathologist recruited and starting work in July. Target
reporting time under 2 weeks.
Mary Falzon (DCD
Histopathology)
September 2014
100 day patients not escalated
via tracking meetings
Discuss all 100 day waits as
special item at tracking
meetings. Progress to be
reported on all patients. Lack
of progress to be escalated
to speciality General
Manager, Divisional Manager
and General Manager
Cancer.
100 day patients are discussed separately at the weekly CWT
meeting plan. Actions are identified at this time for each patient. A
summary of all 100 day patients are presented to the GM and DM
directly after the CWT meeting for additional analysis. All patients
that reach 100 days are reviewed by a clinician to ensure that no
adverse effects are demonstrated due to wait for treatment.
Prav Chitrapu (all sites) COMPLETED

33
UCLH - 62 Day Wait Plan (4/4)
Issue Action Actions & Progress Update Who Responsible By when
No assurance that patients not
at risk of deterioration as result
of extended wait for treatment
Consultant urologist will review
the clinical and waiting status of
all patients monthly to provide
assurance that all appropriate
action is being taken to
expedite the patient’s clinical
treatment in the best interests
of the patient and that the
patient is not at risk of
increased harm.
All patients that reach 100 days are reviewed by a clinician to ensure
that no adverse effects are demonstrated due to wait for treatment.
Information is provided a patient level.
Lois Roberts COMPLETED
Booking processes for first
focal therapy appointment
Review current booking
processes for HIFU first
appointment (not target 14 day
appointment), clarify roles,
develop escalation procedure
for to ensure patients offered
urgent appointment slot within
14 days
It has been identified that many of these patients require additional
diagnostics before they attend their first OPA. The referral will be
graded, diagnostics requested and the OPA will take place after the
diagnostics have been performed.
Uro – Oncology coordinator to track all tertiary patients within the LC
network, regardless of whether they are a target patient or not and
escalate diagnostics dates and OPA dates where appropriate.
Rebecca Dennett COMPLETED
No standard pathway Develop an UCLH best practice
pathway for HIFU (High
Intensity Focused Ultrasound)
which will provide a framework
for treatment, processes and
timescales.
Pathway for Focal therapy completed with current and target timescales
stipulated.
Becky Dennett COMPLETED
Delay between SMDT clinic
appointment and appointment
to explore focal therapy
Reduce referral time to HIFU
specialist
Agreement in place with clinicians that patients can be booked directly
from SMDT clinic to the Focal Therapy clinic the following week.
Becky Dennett COMPLETED
Long waits for template biopsy
and multiple pathway
Develop an UCLH best practice
pathway for template / targeted
biopsies to ensure timescales
for appointments, procedures
and results are optimised.
Pathways for prostate biopsies completed. New LA targeted biopsy
service launched in November 2013 and expanded in April 2014.
Current waits for image guided biopsies now within target range at 1-2
weeks.
Rebecca Dennett / Hash
Ahmed (Consultant
Urologist)
COMPLETED
Delay in start of pathway as
inter-trust referral not sent via
correct route.
Re-confirm with all
organisations referring to
UCLH that all inter-trust
referrals should be made to
the UCLH generic inter-trust
referral email address which
is monitored daily.
Action completed Amanda Quincey (Cancer
GM)
COMPLETED
14/02/14