Embed Size (px)
Citation preview
SPINAL CORD DISORDERS
YARED MAMUSHET(internist,Neurologis
t)

Meninges Connective tissue membranes Dura mater: outermost layer; continuous
with epineurium of the spinal nerves Arachnoid mater: thin and wispy Pia mater: bound tightly to surface
Forms the filum terminale• anchors spinal cord to coccyx
Forms the denticulate ligaments that attach the spinal cord to the dura
Spaces Epidural: external to the dura
Anesthestics injected here Fat-fill
Subdural space: serous fluid Subarachnoid: between pia and
arachnoid Filled with CSF
12

Runs through the vertebral canal Extends from foramen magnum to L1or2 Regions
Cervical Thoracic Lumbar Sacral Coccygeal
Gives rise to 31 pairs of spinal nerves Not uniform in diameter
Cervical enlargement: supplies upper limbs
Lumbar enlargement: supplies lower limbs
Conus medullaris- tapered inferior end Ends between L1 and L2
Cauda equina - origin of spinal nerves extending inferiorly from conus medullaris.
8

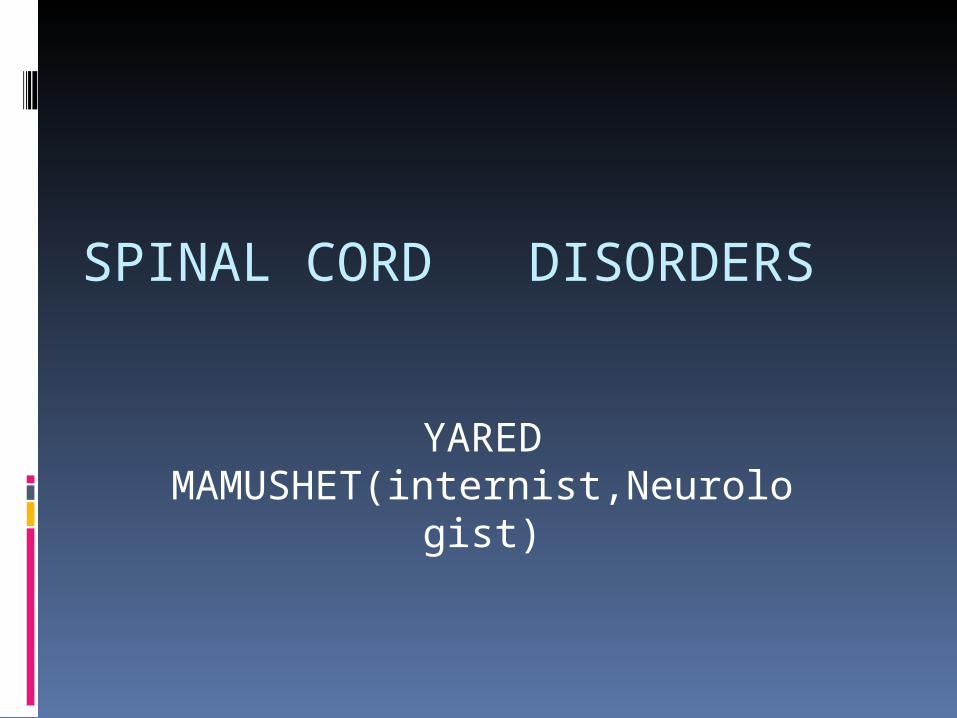
1. 1. S pinothalamicS pinothalamic Tracts (Tracts (R edR ed) = P ain, T emperature, C rude T ouch. 2. ) = P ain, T emperature, C rude T ouch. 2. P osterior C olumn T racts (P osterior C olumn T racts (G reenG reen) = P osition, Vibration, Discriminative ) = P osition, Vibration, Discriminative T ouch. 3. T ouch. 3. C orticospinalC orticospinal T racts (T racts (B lueB lue) = Motor efferent (Descending) F ibres.) = Motor efferent (Descending) F ibres.
O ut of O ut of 10 or more10 or more L ong F ibre S pinal T ractsL ong F ibre S pinal T racts coursing longitudinally in the coursing longitudinally in the spinal cord, spinal cord, only 3only 3 (shown below in R ed, B lue and G reen) are of prime (shown below in R ed, B lue and G reen) are of prime importance in clinical neurology practice:importance in clinical neurology practice:
Spinal Cord – Functional Anatomy
C ourtesy of Medical C ollege, Univers ity of F lorida.
29
19
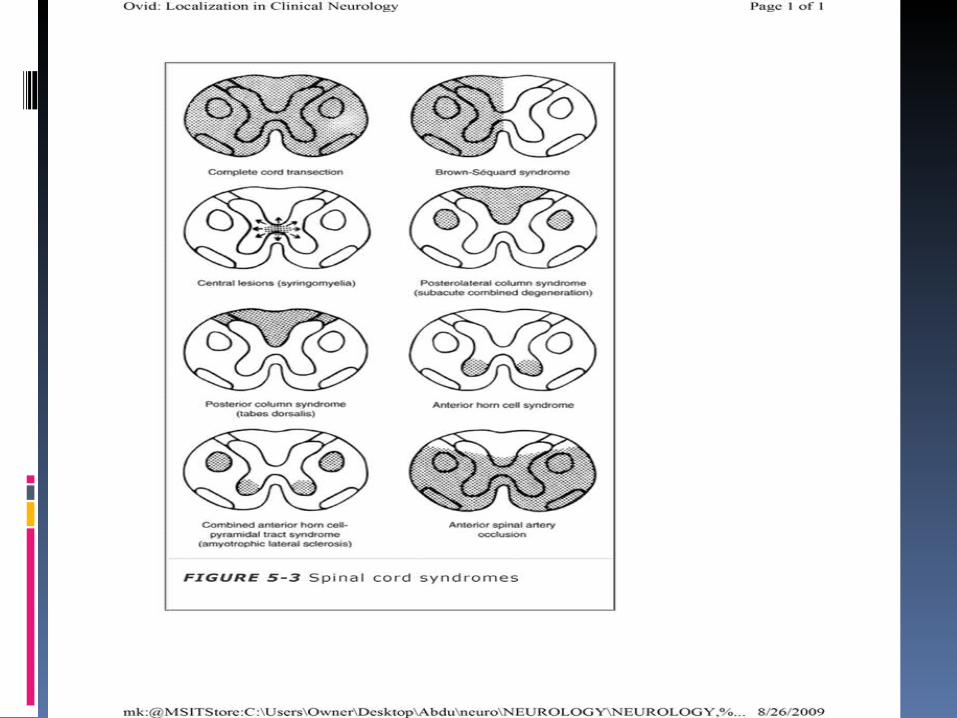
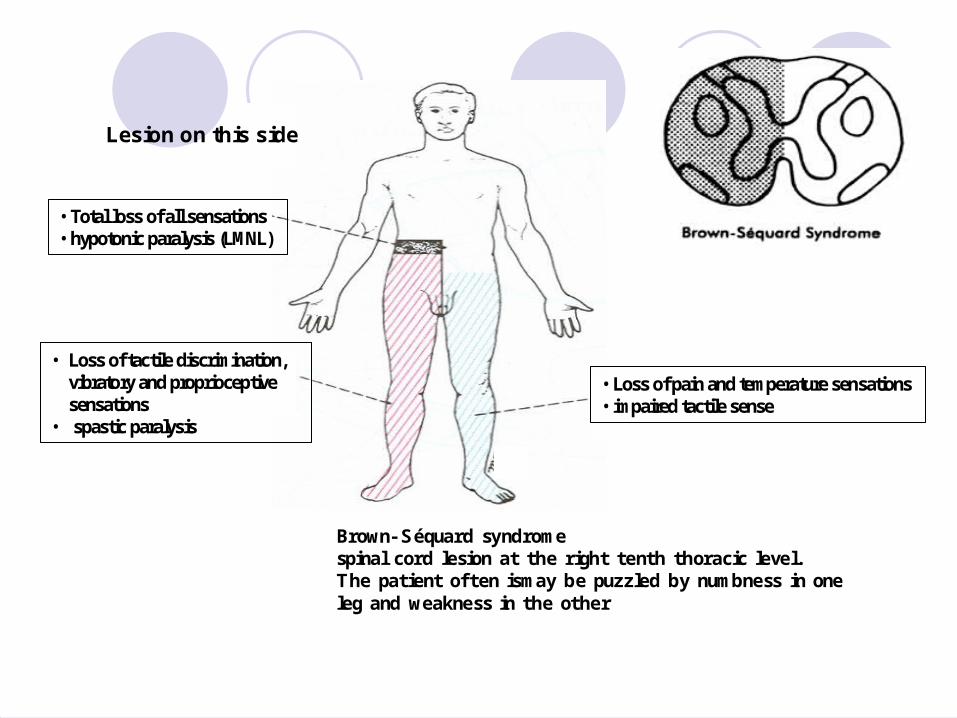
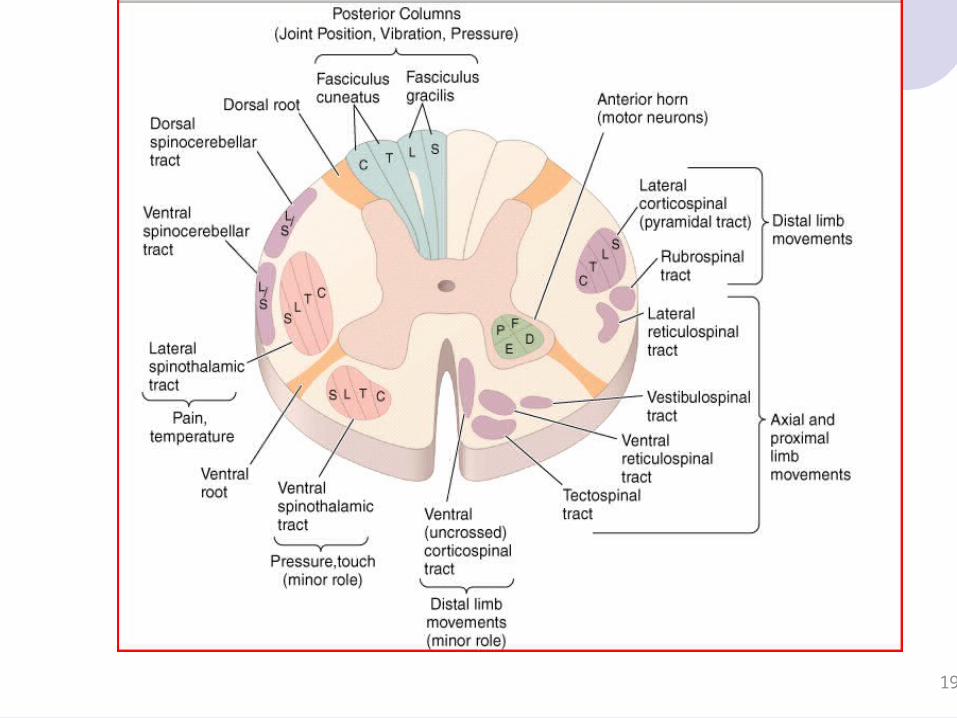
Lesion on this side
• Total loss of all sensations• hypotonic paralysis (LMNL)
• Loss of tactile discrimination, vibratory and proprioceptivesensations
• spastic paralysis
• Loss of pain and temperature sensations• impaired tactile sense
Brown- Séquard syndromespinal cord lesion at the right tenth thoracic level.The patient often ismay be puzzled by numbness in one leg and weakness in the other
•small cross-sectional area •reversible if recognized and treated at an early stage •Neurologic emergency

classification
I-Acute and Subacute Spinal Cord Diseases
Compressive Non compressiveII-Chronic spinal chord diseases

A-Compressive Myelopathies
1-TUMOURS
Extradural tumors most neoplasms are epidural
resulting from metastases Most frequent
breast, lung, prostate, kidney, lymphoma, and plasma cell dyscrasia
The thoracic cord is most commonly involved except prostate and ovarian cancer→ sacral and lumbar
vertebrae Retroperitoneal neoplasms (especially lymphomas or
sarcomas) enter the spinal canal through the intervertebral
foramina produce radicular pain and other signs of root
involvement prior to cord compression.

Pain usually the initial symptom aching and localized / sharp and
radiating worsens with movement, coughing, or
sneezing Rarely, pain is mild or absent

MRI Excellent anatomic resolution of the extent of spinal tumors
distinguishes malignant lesions from infectious ones Tumors are usually hypointense relative to a normal bone
marrow Don't cross disk space unlike infections
the whole length of the spine should be imaged when epidural malignancy is suspected 40% of patients have asymptomatic epidural disease elsewhere
Plain radiographs of the spine and radionuclide bone scans miss 15–20% of metastatic vertebral lesions fail to detect paravertebral masses

Epidural spinal cord compression due to breast carcinoma. Sagittal T1-weighted MRI scans
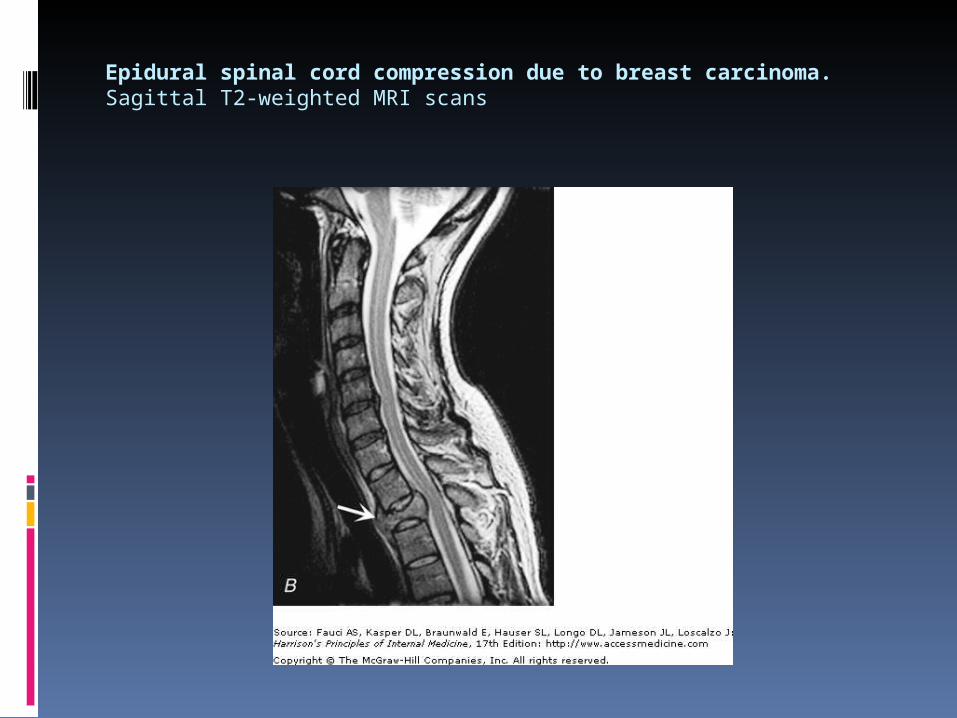
Epidural spinal cord compression due to breast carcinoma. Sagittal T2-weighted MRI scans
Treatment STROIDS to reduce cord edema
dexamethasone up to 40 mg daily Continued at a lower dose until radiotherapy is completed
LOCAL RADIOTHERAPY to the symptomatic lesion as early as possible as effective as surgery, even for radioresistant metastases new weakness is prevented some recovery of motor function in half of treated patients Fixed motor deficits established for >12 hrs do not usually
improve SURGERY
laminectomy or vertebral body resection should be considered when
signs of cord compression worsen despite radiotherapy vertebral compression fracture or spinal instability
contributes to cord compression specific therapy for the underlying tumor type
Intradural tumors slow-growing and benign Therapy is by surgical resection1. Meningiomas
can arise from the meninges anywhere along the spinal canal Usually located
posterior to the thoracic cord near the foramen magnum
2. Neurofibromas Benign tumors of the nerve sheath arise near the posterior root
Symptoms usually begin with radicular sensory symptoms asymmetric, progressive spinal cord syndrome 3. chordoma4. lipoma5. dermoid, or 6. sarcoma

MRI of a thoracic meningioma intense and uniform enhancement of a well-circumscribed extramedullary mass
Intramedullary tumors Primary intramedullary tumors are rare Secondary tumors are common in advanced
metastatic disease present as central cord or hemicord syndromes,
often in the cervical region there may be poorly localized burning pain in the
extremities and sparing of sacral sensation 1. Ependymomas, 2. Hemangioblastomas3. low-grade astrocytomas Ependymomas :Complete resection Astrocytoma (slowly growing lesions) : Debulking adjunctive radiotherapy and chemotherapy is
uncertain
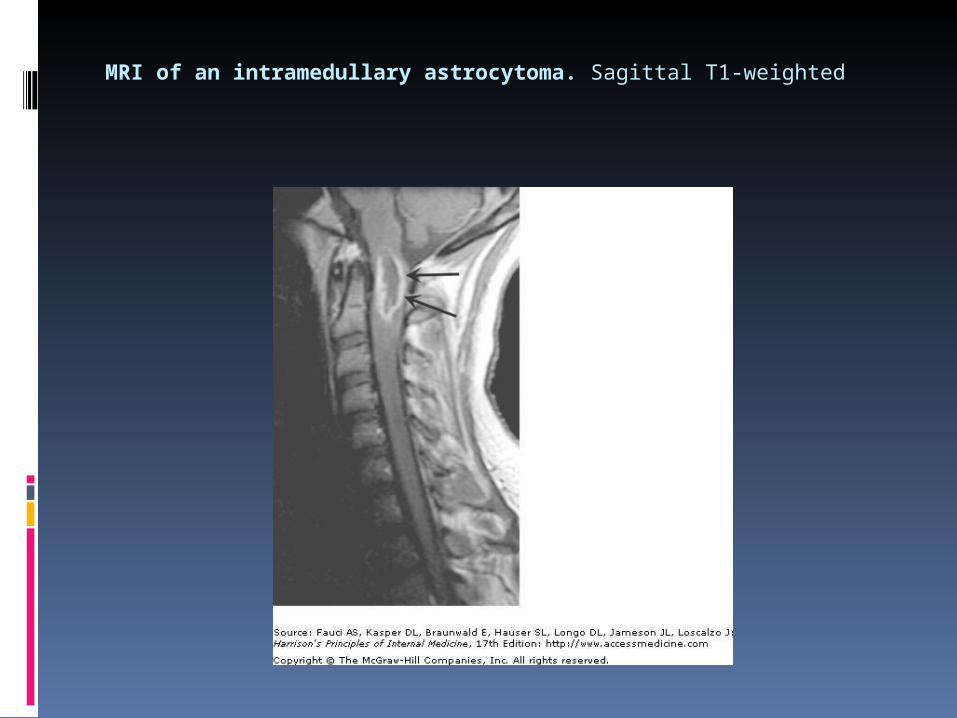
MRI of an intramedullary astrocytoma. Sagittal T1-weighted
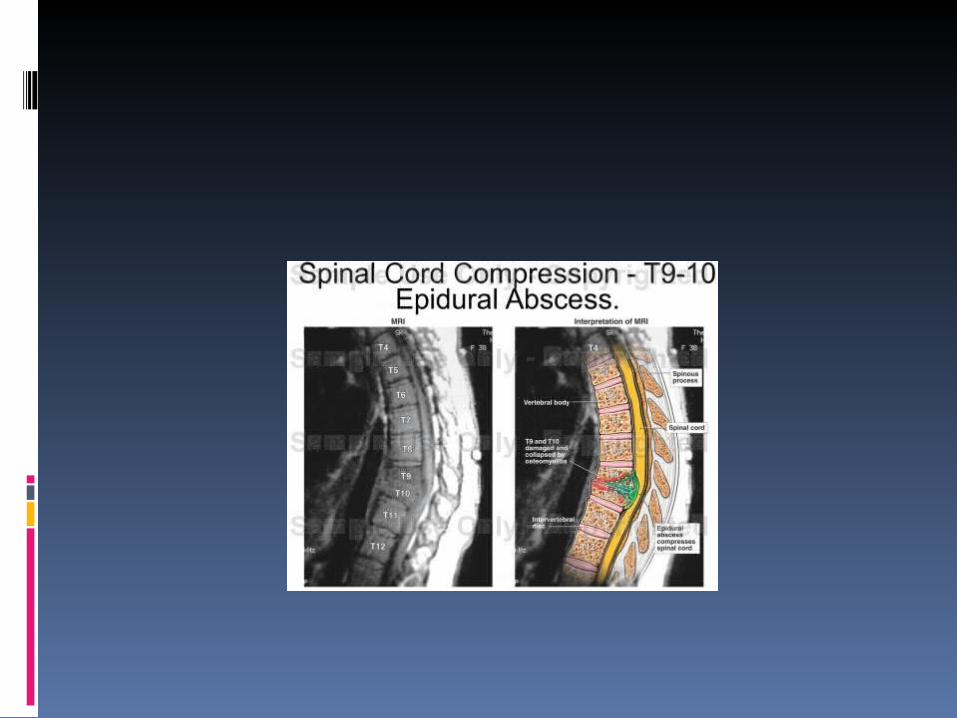
2-Spinal Epidural Abscess triad of midline dorsal pain, fever, and progressive limb
weakness Risk factors include
1. impaired immune status (diabetes mellitus, renal failure, alcoholism, malignancy)
2. intravenous drug abuse3. infections of the skin , viscera, bone and other tissues
Aching pain is almost always present either over the spine or in a radicular pattern
The duration of pain prior to presentation is generally <2 weeks
may be several months or longer Further spinal cord damage results from venous congestion
and thrombosis Once weakness and other signs of myelopathy appear,
progression may be rapid elevated white blood cell count and sedimentation rate A more chronic sterile granulomatous form of abscess is also
known, usually after treatment of an acute epidural infection.

2/3rd :hematogenous spread of bacteria from
1.the skin2.soft tissue (pharyngeal or dental abscesses) 3.deep viscera (bacterial endocarditis)
1/3rd : direct extension of a local infection 1.vertebral osteomyelitis2.decubitus ulcers3.lumbar puncture4.epidural anesthesia
Etiology Staphylococcus aureus TUBERCULOSIS in assocition with Pott Disease
(Tuberculous Spinal Osteomyelitis ) pus or caseous granulation tissue extrudes from an
infected vertebra to an epidural space gram-negative bacilli Streptococcus Anaerobes fungi Diagnosis MRI scans
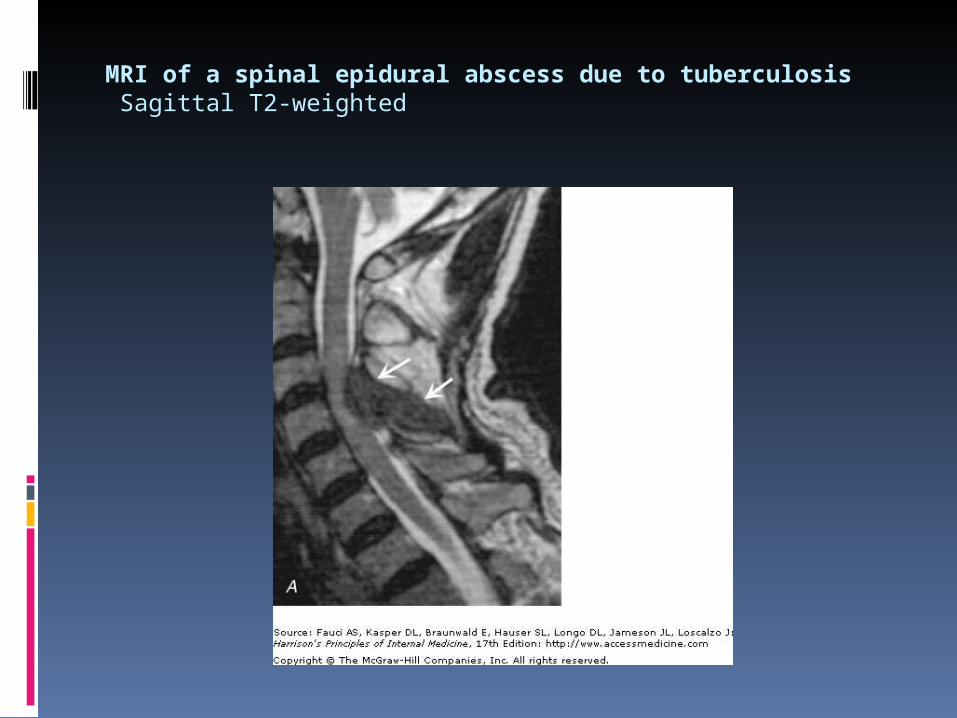
MRI of a spinal epidural abscess due to tuberculosis Sagittal T2-weighted
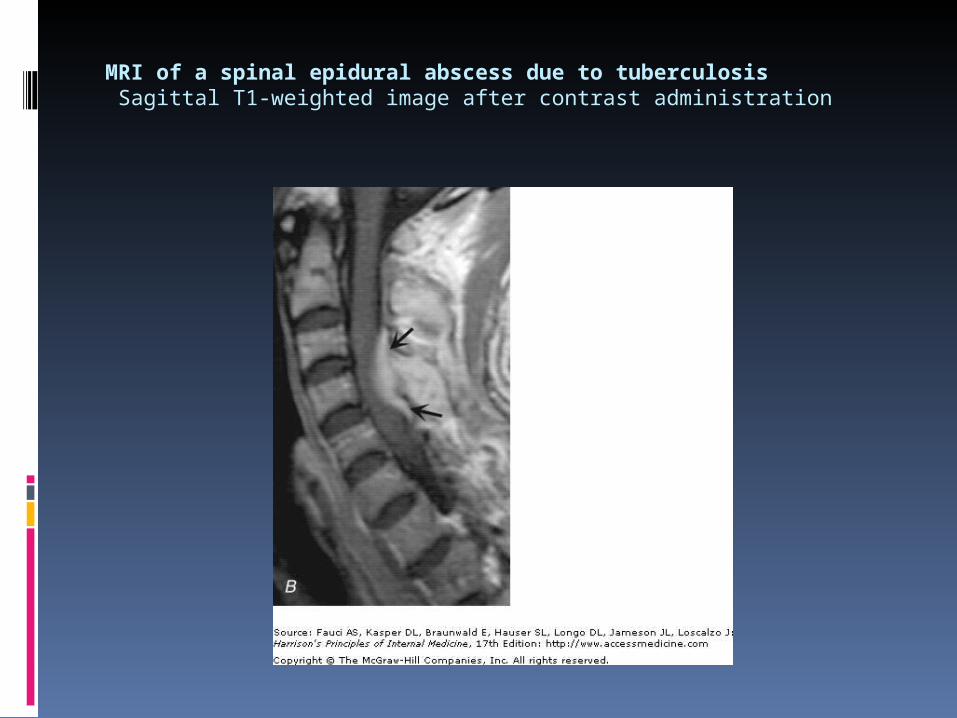
MRI of a spinal epidural abscess due to tuberculosis Sagittal T1-weighted image after contrast administration
Lumbar puncture is only required if encephalopathy or other clinical signs raise the question of associated meningitis, a feature that is found in <25% of cases passage of the needle through infected tissue or herniation A high cervical tap is often the safest approach

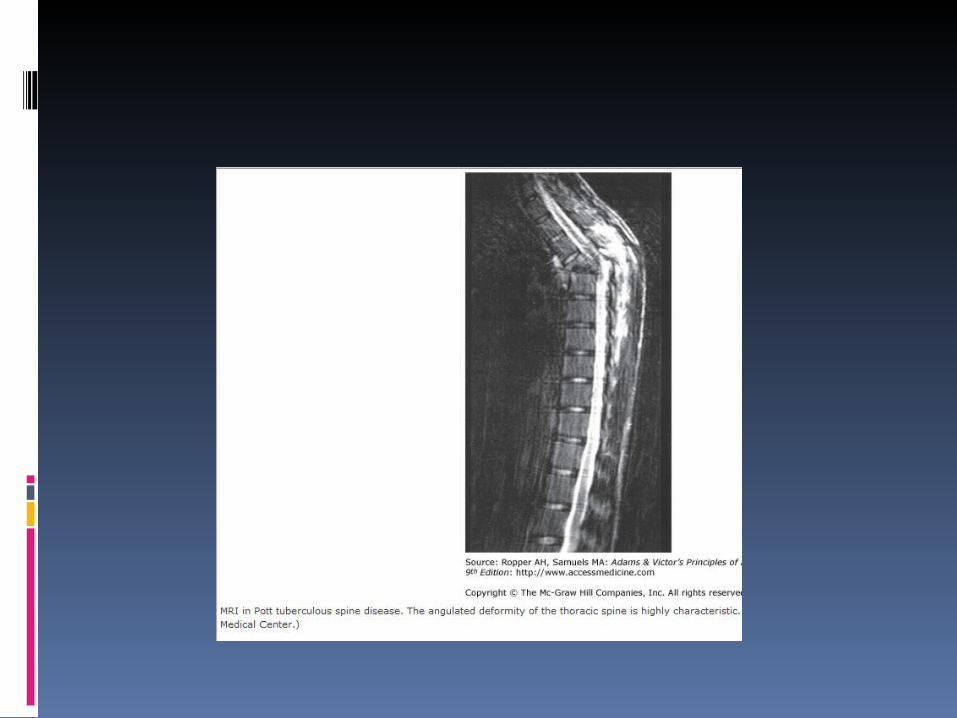
Tuberculous Spinal Osteomyelitis (Pott Disease)
Children and young adults are most often affected An infectious endarteritis causes bone necrosis collapse of a thoracic or upper lumbar (less often cervical) vertebral body resulting in a characteristic angulated kyphotic deformity
gibbus deformity Most patients have active tuberculous infection as evidenced by fever,
night sweats, and other constitutional symptoms the sedimentation rate is invariably elevated A compressive myelopathy occurs in some cases as a result of the spinal
deformity, but it is surprisingly infrequent and an epidural tuberculous abscess is a more common cause of cord compression
excellent result may be obtained by external stabilization of the spine and long-term antituberculous medication
spinal surgery required only in the presence of severe deformities or a compressive myelopathy

Treatment decompressive laminectomy with debridement
treatment of choice unless the abscess is 1. limited in size and causes few or no neurologic signs.2. If surgery is contraindicated or 3. if there is a fixed paraplegia or quadriplegia : long-
term administration of systemic and oral antibiotics may improve or reverse paralysis in evolution unlikely to improve deficits of more than several
days duration Anti Tb for tuberculous epidural abscess
3-Spinal Epidural Hematoma acute focal or radicular pain followed by spinal cord disorder predisposing conditions
Therapeutic anticoagulation Trauma Tumor blood dyscrasia lumbar puncture :Rare
lumbar puncture should be avoided whenever possible in patients with severe thrombocytopenia or other coagulopathies
Dx MRI and CT confirm the clinical suspicion Rx prompt reversal of any underlying clotting disorder surgical decompression

4-Hematomyelia Hemorrhage into the substance of the spinal cord rare result from
Trauma intraparenchymal vascular malformation vasculitis (polyarteritis nodosa, SLE) bleeding disorders a spinal cord neoplasm
acute painful transverse myelopathy extension into the subarachnoid space may occur, resulting in
subarachnoid hemorrhage Diagnosis is by MRI or CT Therapy Supportive surgical intervention not useful except in underlying vascular
malformation
s
35From Dr China T. (Prospective Neurosurgeon)
)
36From Dr China T. (Prospective Neurosurgeon)
Noncompressive Myelopathies After spinal cord compression is
excluded the following should be considered
1. spinal cord infarction2. myelitis
infectious (primarily viral) Postinfectious/ post vaccinal systemic inflammatory disorders
SLE and sarcoidosis3. demyelinating diseases
multiple sclerosis and neuromyelitis optica
1-Spinal Cord Infarction
A- With systemic hypotension cord infarction occurs at the level of
greatest ischemic risk usually T3-T4 boundary zones between the anterior
and posterior spinal artery territories rapidly progressive syndrome over
hours of weakness and spasticity little sensory change

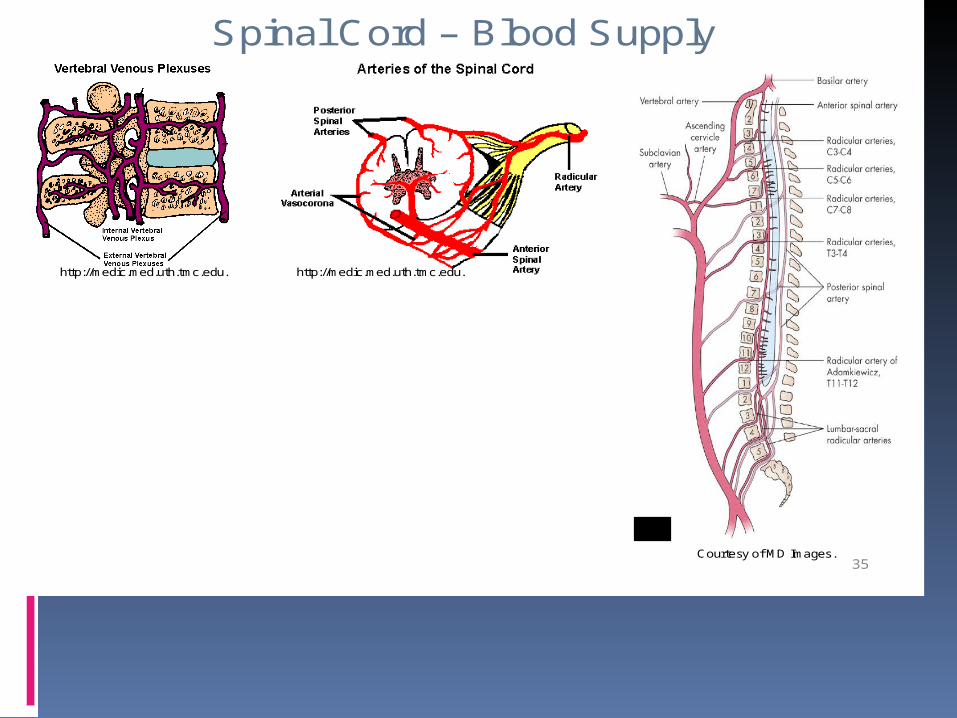
S pinal C ord – B lood S upply
http://medic .med.uth.tmc.edu.
C ourtesy of MD Images .
http://medic .med.uth.tmc.edu.
35
b-anterior spinal artery
produces "anterior cord syndrome Sharp midline or radiating back pain localized to the area of
ischemia paraplegia or quadriplegia loss of sphincter control dissociated sensory loss usually progressive over minutes or a few hours
unlike stroke in the cerebral hemispheres Areflexia due to spinal shock is often present initially with time, hyperreflexia and spasticity appear A few patients have vertigo at the onset Rarely, infarction is preceded by transient spinal ischemic attacks Many patients regain a substantial degree of motor function,
mainly in the first month but extending over a year
C- posterior spinal arteries not common
cause Atherosclerosis and thrombotic occlusion of the anterior
spinal artery is quite uncommon aortic atherosclerosis dissecting aortic aneurysm vertebral artery occlusion or dissection profound hypotension Cardiogenic emboli vasculitis intraoperative surgical occlusion cocaine users embolism of nucleus pulposus dural fistula
Diagnosis MRI
Usually detects the abnormality may fail to demonstrate limited infarctions of the cord,
especially in the first day In the chronic stages, the infarcted region collapses and
has an attenuated signal on MRI
Treatment presumed thromboembolism, acute anticoagulation is
probably not indicated, with the exception of the unusual transient ischemic attack or incomplete infarction with a stuttering or progressive course
?CSF drainage

confined to gray matter: poliomyelitis if confined to white
matter :leukomyelitis If approximately the whole cross-
sectional area of the cord is involved :transverse myelitis
multiple and widespread over a long vertical extent: diffuse or disseminated
Acute Infectious Myelitis often difficult to distinguish
from postinfectious Herpes zoster
best characterized HSV types 1 and 2
recurrent sacral myelitis in association with outbreaks of genital herpes
EBV, CMV, rabies virus, Poliomyelitis
Bacterial and mycobacterial myelitis less common most are essentially
abscesses Almost any pathogenic
species
parasitic myelitis Schistosomiasis Toxoplasmosis cause a
focal myelopathy in HIV pts
treatment
Herpes zoster, HSV, and EBV intravenous acyclovir or oral valacyclovir for 10–14 days
CMV with ganciclovir plus foscarnet or cidofovir

Post infectious /post vaccinal
The characteristic features of these diseases are (1)their temporal relationship to certain viral infections or
vaccinations(2)the delayed development of neurologic signs over the
period of a few days(3)a monophasic temporal course, i.e., a single attack of
several weeks' duration with variable degrees of recovery and no recurrence.
immunologic in nature more or less confined to spinal cord myelin
Often begins upon recovery from an AFI or in the subsequent days or weeks
infectious agent cannot be isolated If it also affects the brain it is called acute disseminated
encephalomyelitis (ADEM)

Epstein-Barr virus cytomegalovirus Mycoplasma Influenza Measles Varicella Rubeola mumps
Mycoplasma is unique in being a bacterial trigger of the disease
The list of antecedent infections is otherwise much the same as for the Guillain-Barré syndrome with the notable difference of Campylobacter jejuni, which has not led to myelitis and is a frequent precedent to the polyneuropathy
The latency between infection and myelitis :uncertain febrile episode may blend into the neurologic syndrome In others latency has been 2 weeks
In 50% of cases the patient can identify a recent infectious illness, usually upper respiratory syndrome
The illness evolves over several days, sometimes a single day or on the other extreme, over 1 or 2 weeks
fewer than half of cases are truly "transverse“ weakness and numbness of the feet and legs (less often of the hands and
arms), which typically develop over a few days the sensory symptoms ascend from the feet to the trunk
simulate a polyneuropathy, are common early symptoms Sphincteric disturbances and backache are also common
Differentiated from a rapidly progressive polyneuropathy such as the Guillain-Barré by
1. A slight asymmetry of the symptoms and signs2. sensory level on the trunk3. Babinski sign

CSF lymphocytes and other mononuclear cells :10 -100/mm3 Some times normal slightly raised protein and normal glucose content
MRI slight T2 signal abnormalities minimal gadolinium enhancement extending over 2 or 3 spinal
segments the cord may be swollen in these regions several patients with mild and partial myelitis may have normal
MRI studies

Treatment Once symptoms begin, it is not clear if any treatment is
of consistent value ?high doses of corticosteroids :no evidence that this
alters the course of the illness ?plasma exchange or intravenous immune globulin The prognosis of this illness is better than the initial
symptoms might suggest Usually the myelitic disease improves, sometimes to a
surprising degree Pain in the midthoracic region or an abrupt, severe
onset usually indicates a poor prognosis
Tabes Dorsalis
Post. Column
Now rare
Occurs 18-25 yrs after initial lesion.
presentation : -Lightning pain (sudden and severe) -Ataxia -Sensory loss and paresthesia -Visceral crisis(abdominal pain and diarrhea) -Rectal crisis(tenesmus) -Charcot jt -Associated ARP and optic atrophy
Systemic Inflammatory Disorders SLE Sjögren's syndrome mixed connective tissue disease vasculitis sarcoid myelopathy
3-Demyelinating Myelopathies

Acute Demyelinating Myelitis of MS the clinical manifestations of MS tend to evolve more slowly, over a period
of 1 to 3 weeks or even longer. antecedent infections is not often seen Only the occurrence of subsequent attacks or additional lesions revealed
by MRI or evoked potentials indicates that the basic illness is one of chronic recurrent demyelination
numbness that spreads over one or both sides of the body from the sacral segments to the feet, anterior thighs, and up over the trunk
asymmetric weakness and then paralysis of the legs When this process becomes complete, the bladder is also affected The sensorimotor disturbance may extend to involve the arms a sensory level can be demonstrated on the upper parts of the trunk. relatively painless and without fever, and the patient usually improves,
with variable residual signs

The CSF often normal may show a mild lymphocytosis, as in the postinfectious variety Oligoclonal bands may be absent with the first attack
Treatment Corticosteroids
may lead to a regression of symptoms, sometimes with relapse when the medication is discontinued (after 1 to 2 weeks)
No apparent response in some a proportion of cases have even continued to worsen on steroids
Plasma exchange and intravenous immune globulin particularly in those with an explosive onset
II-Chronic Myelopathies 1-Spondylitic Myelopathy most common cause of gait difficulty in the elderly involve the lower and midcervical vertebrae Neck and shoulder pain with stiffness are early
symptoms Radicular arm pain, most often in a C5/C6
distribution Compression of the cervical cord
fewer than one-third of cases produces a slowly progressive spastic paraparesis, at
times asymmetric accompanied by paresthesias in the feet and hands Vibratory sense is diminished in the legs positive Romberg sign
occasionally there is a sensory level for vibration on the upper thorax
coughing or straining produces leg weakness or radiating arm or shoulder pain
Dermatomal sensory loss in the arms, atrophy of intrinsic hand muscles,
increased deep-tendon reflexes in the legs, and extensor plantar responses the biceps is most often affected (C5-C6)
Urinary urgency or incontinence occurs in advanced cases
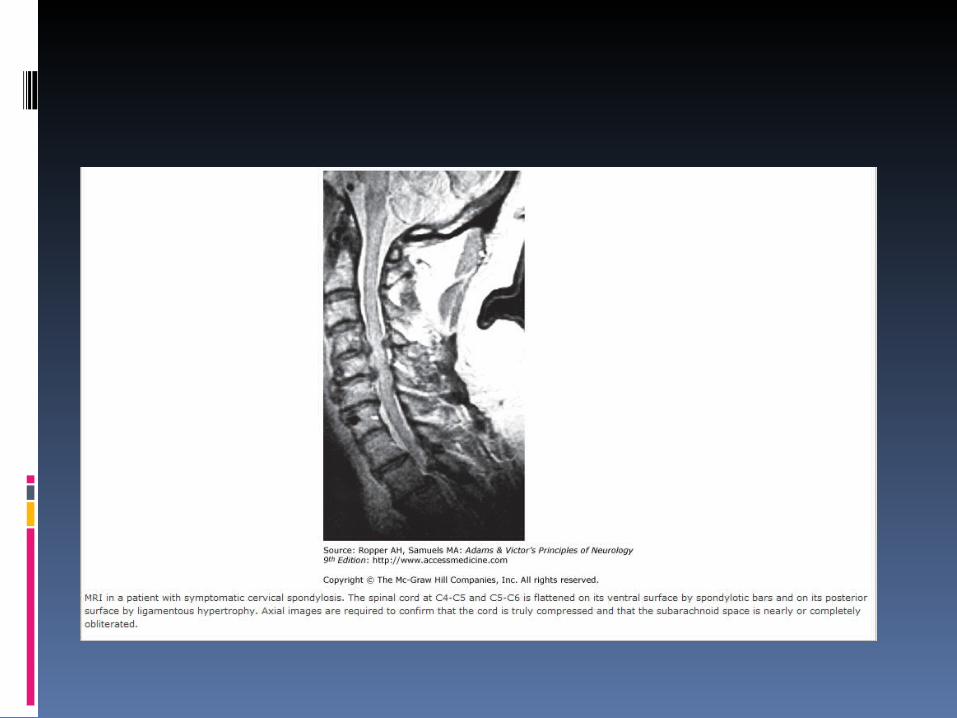
Diagnosis MRI or myelography
Treatment A cervical collar in milder cases surgical decompression : definitive
therapy Posterior laminectomy resection of the protruded disc and bony
material
2-Syringomyelia Developmental cavitary expansion of the cervical cord prone to enlarge and produce progressive myelopathy Symptoms
begin insidiously in adolescence or early adulthood progress irregularly may undergo spontaneous arrest for several years Many young patients acquire a cervical-thoracic scoliosis
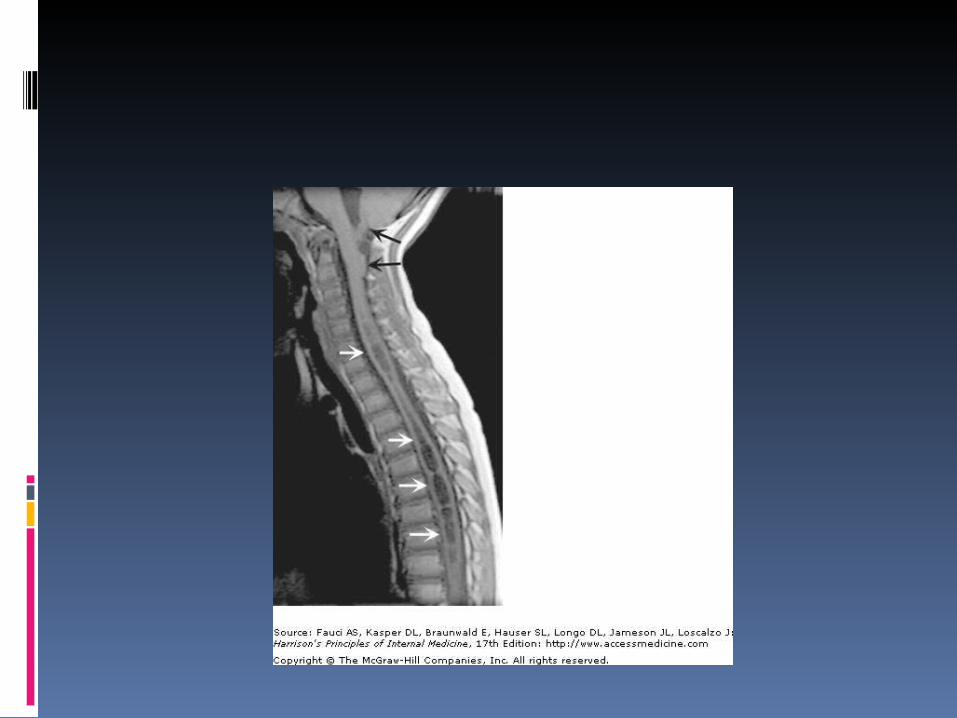
More than half of all cases are associated with Chiari type 1 malformations cerebellar tonsils protrude through the foramen magnum
and into the cervical spinal canal syrinx cavities
Acquired cavitations of the cord in areas of necrosis trauma, myelitis, necrotic spinal cord tumors, and chronic
arachnoiditis due to tuberculosis and other etiologies
classificationType I. Syringomyelia with obstruction of the foramen magnum and dilatation
of the central canal (developmental type) A. With type I Chiari malformation B. With other obstructive lesions of the foramen magnum Type II. Syringomyelia without obstruction of the foramen magnum
(developmental type) Type III. Syringomyelia with other diseases of the spinal cord (acquired types) A. Spinal cord tumors (usually Intramedullary) B. Traumatic myelopathy C. Spinal arachnoiditis and pachymeningitis D. Secondary myelomalacia from cord compression (tumor, spondylosis),
infarction, hematomyelia Type IV. Pure hydromyelia (developmental dilatation of the central canal),
with or without hydrocephalus

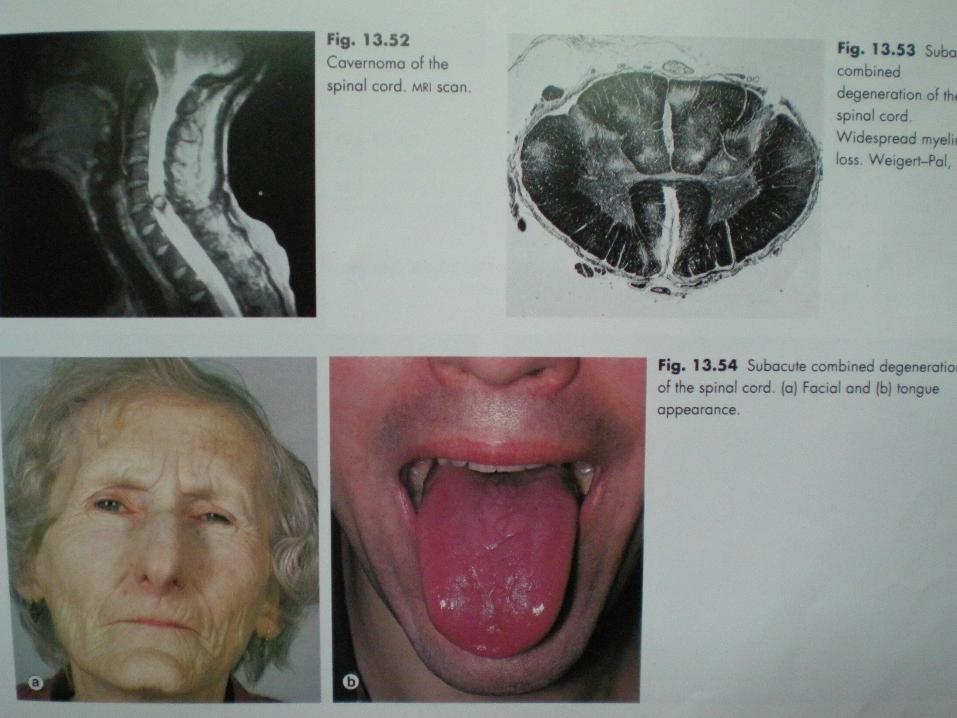
3-Subacute Combined Degeneration
Subacute paresthesias in the hands and feet A progressive spastic and ataxic weakness
Loss of vibration and position sensation Loss of reflexes due to an associated peripheral
neuropathy in a patient who also has Babinski signs, is an important diagnostic clue
Optic atrophy and irritability or other mental changes in advanced cases
Myelopathy is diffuse rather than focal signs are generally symmetric predominant involvement of the posterior and lateral
tracts Romberg's sign
DX confirmed by the finding of 1.macrocytic red blood cells2.serum B12 concentration3.elevated serum levels of homocysteine and
methylmalonic acid4.positive Schilling test
Treatment vitamin B12, beginning with 1000 µg IM repeated at regular intervals or by
subsequent oral treatment
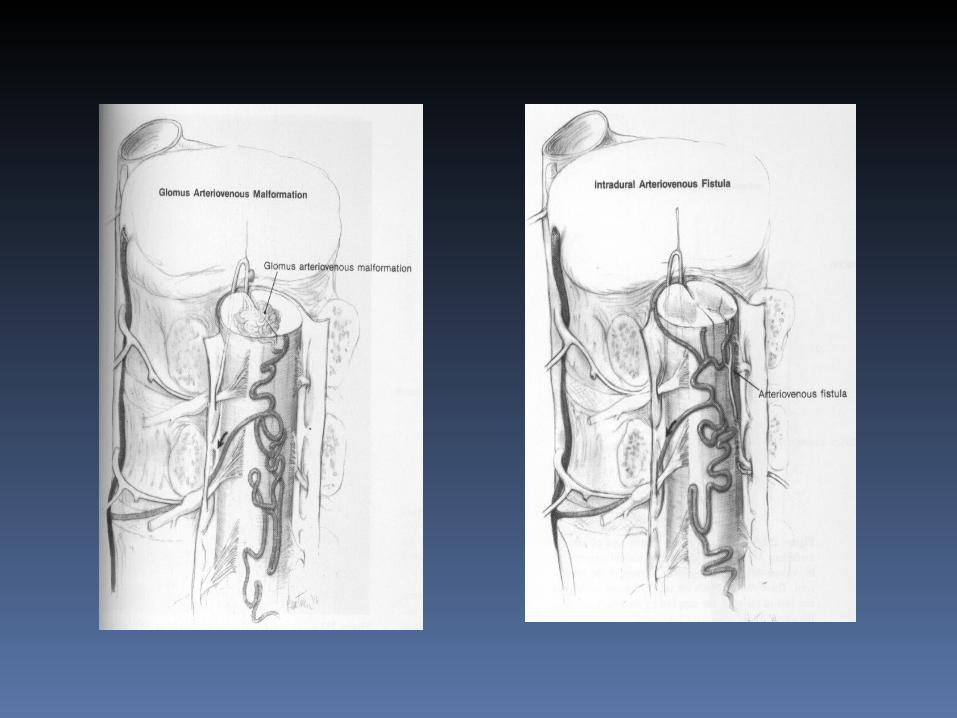
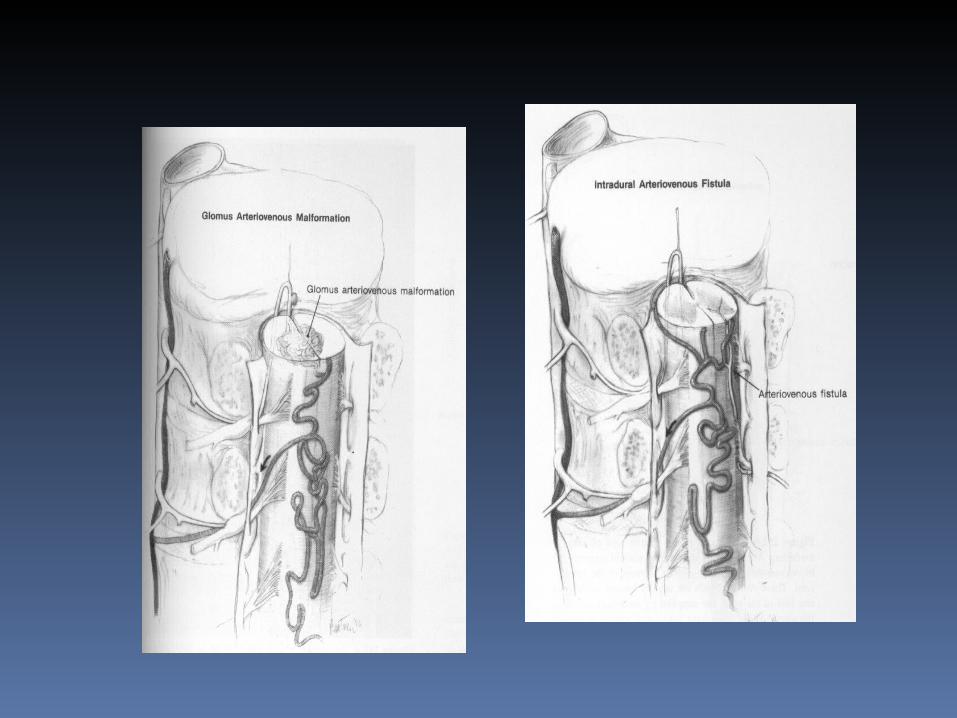
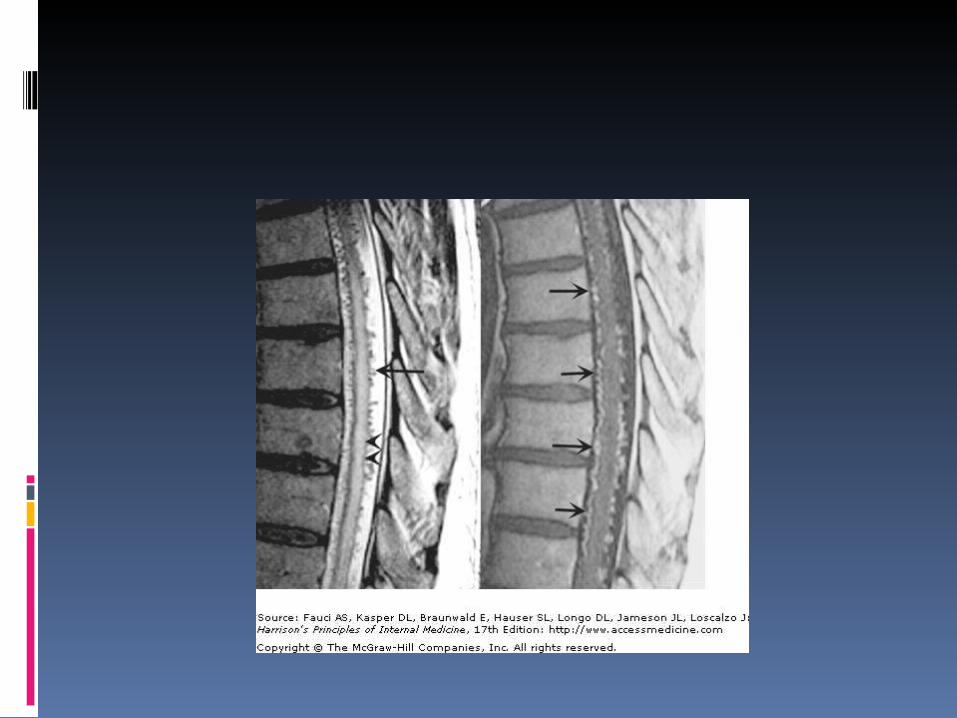
Vascular Malformations of the Cord and Dura
uncommon middle-aged men located posteriorly along the surface of the cord or within the dura Pain over the dorsal spine, dysesthesias, or radicular pain intermittent claudication Spinal bruits are infrequent
should be sought at rest and after exercise in suspected cases progressive myelopathy that worsens slowly or intermittently A saltatory progression is most common and is the result of local ischemia and edema from venous congestion.
Tropical Spastic Paraparesis
Caused by Human T-Cell Lymphotropic Virus Type I cytotoxic
The posterior columns and corticospinal tracts are the main sites of disease, most evident in the thoracic cord
slowly progressive paraparesis with increased tendon reflexes and Babinski signs most patients are unable to walk within 10 years of onset
disorder of sphincteric control is usually an early feature but symmetric paresthesias, reduced vibratory and position senses, and ataxia follow over several months or years often lack a well-defined sensory level
upper extremities usually spared (except for lively tendon reflexes)
CSF contains small numbers of lymphocytes of the T type (10 to
50/mm3), normal concentrations of protein and glucose an increased content of immunoglobulin (Ig) G with
antibodies to HTLV-I diagnosis is confirmed by the detection in the serum
of the antibodies to the virus MRI :
Thinness of the spinal cord subcortical cerebral white matter lesions may be
seen as well no effective treatment
symptomatic therapy for spasticity and bladder symptoms
Vacuolar Myelopathy with AIDS 20 of 89 successive cases of AIDS on whom a
postmortem examination was performed had it The white matter of the spinal cord is
vacuolated, most severely in thoracic segments posterior and lateral columns are affected
the lesions in the spinal cord resemble those of subacute combined degeneration levels of vitamin B12 and folic acid have been
normal symptoms and signs obscured by
a neuropathy or one or more of the cerebral disorders that complicate
AIDS

Hemi- or quadriparesis, often asymmetrical Develop over a period of weeks
sensory and sphincteric disorder A sensory ataxia has also been a common early feature
CSF a small number of lymphocytes, a slight elevation of protein occasionally bizarre giant cells
Similar vacuolar lesions may be seen in the brain in some cases
antiretroviral drugs have little effect on the myelopathy symptomatic treatment of spasticity
Familial Spastic Paraplegia onset may be as early as the first year of life or as late
as middle adulthood imperceptibly progressive spasticity and weakness in
the legs, usually symmetrical Sensory symptoms and signs are absent or mild sphincter disturbances may be present IN some families additional neurologic signs are
prominent, including nystagmus, ataxia, or optic atrophy
Only symptomatic therapies for the spasticity are currently available
konzo

MANAGEMENT Management of SC problems must
be cautious and fast because reversal of paraparesis is TIME-LOCKED .
Paraplegia beyond a certain interval may remain complete, with no prospect of future ambulation or bladder bowel control.
So again expedited evaluation and act is required
Unacceptable delay in diagnosis ,refferal,and investigation shouldn’t occur.
If traumatic or other they should immediately be transferred to institutions providing the service.
Specific diagnosis needs specific treatment.
Postoperative care, rehabilitation are very important aspects of managing patients with spinal cord lesions.
THANKS!