Embed Size (px)
Citation preview

TRIGEMINAL AUTONOMIC CEPHALALGIAS (M MATHARU, SECTION EDITOR)
Spinal Cord Stimulation in Cluster Headache
Tilman Wolter & Holger Kaube
Published online: 16 March 2013# Springer Science+Business Media New York 2013
Abstract Neurostimulation techniques for the treatment ofprimary headache syndromes, particularly for chronic clus-ter headache (CCH), have received much interest in therecent years. Occipital nerve stimulation (ONS) has yieldedfavourable clinical results, and is becoming a routine treat-ment for refractory chronic cluster headache in specializedcentres. Meanwhile, other promising techniques, such asspinal cord stimulation (SCS) or sphenopalatine ganglionstimulation, are emerging. This article reviews the currentstate of clinical research for neurostimulation techniques forchronic cluster headache, and particularly the pros and consof SCS and ONS.
Keywords Chronic cluster headache . Spinal cordstimulation .Neurostimulation .Occipital nervestimulation .
Sphenopalatine ganglion
Cluster Headache
Cluster headache (CH) belongs to the trigemino-autonomicheadaches. It is characterized by excruciating headacheattacks occurring from once every other day to several timesa day. The duration of a single attack is between 15 and180 min. The headaches are located orbitally, supraorbitallyor temporally, and are associated with one or more of thefollowing symptoms: conjunctival injection, lacrimation,nasal congestion, rhinorrhoea, forehead and facial sweating,miosis, ptosis and eyelid edema [1]. Attacks con occur in
series (so-called bouts or cluster periods), followed by re-mission periods of months or years. These remission periodsare missing in chronic cluster headache (CCH).
Treatment usually consists of acute therapy, short-termprophylaxis and maintenance prophylaxis. As acute treat-ment inhalation of high-flow oxygen, sumatriptan subcuta-neous injection and zolmitriptan nasal spray are used. Drugsfor transitional prophylaxis are corticosteriods and ergot-amines. First line treatment for prophylaxis is verapamil,but lithium and topiramate can also be effective [2].
Ablative Techniques
Many ablative techniques, such as glycerol injection [3],radiofrequency lesioning [4, 5] or gamma-knife lesioningof the trigeminal nerve [6–9], trigeminal tractotomy [10],trigeminal sensory nerve section [11, 12], surgical section[13] or radiofrequency [4] of the intermedate nerve, combi-nations of nerve sections [14], decompression of the facialnerve [15] and endoscopic block [16], radiofrequency treat-ment [17•] or gamma knife lesioning [18] of the sphenopa-latine ganglion (SPG), have been described with varyingresults. These techniques are associated with various risks,such as death, permanent neurological deficits, corneal an-aesthesia and visual loss. Furthermore, they sometimes havea limited duration of pain relief. Therefore, all in all, itseems doubtful whether their use is appropriate for CCH.
Neuromodulation Techniques
The lack of effective medical and lesional treatments, alongwith the advancement of neuromodulation techniques alsofor other types of chronic pain, led to trials of neurostimu-lation for CCH. These techniques should be used only incase of therapy refractory CCH. Guidelines for the defini-tion of therapy refractory CCH have recently been proposed[19•]. However, the exact proportion of patients fulfillingthese criteria is unknown.
This article is part of the Topical Collection on Trigeminal AutonomicCephalalgias
T. Wolter (*)Interdisciplinary Pain Centre, University Hospital Freiburg,Breisacherstr. 64,79106 Freiburg, Germanye-mail: [email protected]
H. KaubeNeurology and Headache Centre, Münchner Freiheit, München,Germany
Curr Pain Headache Rep (2013) 17:324DOI 10.1007/s11916-013-0324-0

Deep Brain Stimulation (DBS)
After identifying hypothalamic activation in functional im-aging during cluster attacks, [20••, 21] deep brain stimula-tion (DBS) was tried as a treatment for refractory CCH. Thefirst series showed excellent results, with 13 of 16 patientspain free or nearly pain free, and three patients improved[22, 23]. In 2008, a review summarized the results of hypo-thalamic DBS: in 38 patients, 61 % were pain free or almostpain free during a follow-up between 1 and 4 years [24]. Afatal hemorrhage was reported in 2005 by Schoenen et al.[25]. A prospective randomized crossover study DBSshowed no difference between active and sham stimulationduring the blinded crossover phase, but in the open phase,six of 11 patients had a decrease in weekly attack frequencyof >50 % [26]. The target data for DBS are derived frompositron emission tomography (PET) studies with limitedspatial resolution. Functional magnetic resonance imaging(fMRI) data, which have a better spatial resolution, suggesta locus of activation antero-superior to that found in PETstudies [27]. Therefore, it is doubtful whether previousstereotactic interventions in trigeminoautonomic cephalgiashave been targeted at the appropriate locus [28].
Occipital Nerve Stimulation for CCH
Occipital nerve Stimulation (ONS) as a treatment forintractable headache was first described by Weiner andReed in 1999 [29•]. They treated a series of 13 patientswith subcutaneously implanted electrodes placed trans-versely at the level of C1 across the base of the occip-ital nerve trunk. Since then, it has been proposed for thetreatment of various refractory headache syndromes, in-cluding migraine [30], hemicrania continua (HC) [31],short-lasting unilateral neuralgiform headache attackswith conjunctival injection and tearing (SUNCT), andshort-lasting neuralgiform headache attacks with auto-nomic symptoms (SUNA) [32].
In cluster headache, to date there are a number of studieson the effect of ONS in refractory CCH. In a study by Burnset al. on eight patients with CCH treated with ONS, sixpatients reported improvement. CCH was improved bymore than 90 % in two patients, between 40 and 80 % inthree patients, and 25 % in one patient [33]. Similar resultswere observed in a subsequent study on 14 patients (includ-ing the eight patients reported before) [34].
Magis et al. prospectively studied eight patients with amean follow-up of 15 months and found two patients painfree, three patients with a 90 % reduction in attack frequen-cy, two patients with an improvement of around 40 % andone patient with no benefit [35]. A later study on 15 patientsby the same group, including the eight patients reported
before, showed excellent results regarding reduction of at-tack frequency. However, four battery explants occurred(one due to unbearable paresthesia and three due to infec-tion) and 17 battery changes were necessary in nine patients[36].
Further studies confirmed a substantial reduction in at-tack frequency and intensity by ONS [37–40]. An overviewis given in Table 1.
The studies also showed that ONS sometimes exerts itsfull effect sometimes only after several weeks [34] or evenmonths [35]. On the other hand, patients reported an imme-diate onset of new CH in the case of technical defects of thedevice [34].
The pros of ONS include:
& That it has a proven efficacy in a number of studies.& That it is based on a simple operation technique.& That it is not very invasive and therefore carries less
inherent risks compared to other more invasivetechniques.
The cons are:
& That it is not efficacious in all cases.& That in ONS there is also a high rate of device-related
complications.& That it does not always have an immediate pain-
relieving effect, so that sometimes an IPG may beimplanted that later on turns out to be inefficient.
Sphenopalatine Ganglion Stimulation
The sphenopalatine (pterygopalatine) ganglion (SPG)plays an important role in driving the parasympatheticfeatures, and in sterile meningeal inflammation, as sub-strate for trigeminally mediated head pain, as well as inpain transmission in CH. Therefore, the SPG has beenchosen as target in a couple of lesional treatments [15, 16,17•, 18]. A case of long-term neurostimulation of the SPGwith excellent and long-lasting pain relief has beenreported [41]. A recent study showed that stimulation ofthe SPG was effective as acute treatment of clusterattacks. In this study, in six patients 18 attacks weretreated and a complete resolution of symptoms was seenin 11 attacks, a partial resolution in three attacks, andminimal or no relief in four attacks [42•]. Similar resultshave been reported after SPG stimulation as acute treat-ment for migraine [43]. These studies have led to marketapproval of an implantable device for SPG stimulation forthe acute treatment of CH. Moreover, SPG, in contrast toONS and SCS, can offer the possibility to abort an ongo-ing attack. Therefore, future studies of stimulation of theSPG are urgently warranted.
324, Page 2 of 8 Curr Pain Headache Rep (2013) 17:324

SCS as a Treatment Option for CCH
SCS has been first described by Shealy in 1967 [44••]. Sincethen, it has been used in a variety of neuropathic painsyndromes [45••], such as failed back surgery syndrome[46–49, 50••], complex regional pain syndrome (CRPS)[51–53] and postherpetic neuralgia [54]. Also in vasopathicdiseases such as angina pectoris [55••] and peripheral vas-cular disease [56], the clinical efficacy of SCS has beenreported. Cervical SCS has been described in the contextof studies regarding CRPS (including both cervical andthoracolumbar SCS) [52, 57, 58] and Raynaud’s syndrome[59]. Moreover, cervical SCS has been been described ex-clusively in two studies [60, 61] and a small case series [62].
High cervical SCS (hcSCS) has been performed by theMoossy’s group for many years, as it was pointed out in apaper from 2011 [63•]. They used paddle-type electrodesthat had to be inserted via a laminotomy C1. Their retro-spective study included 25 patients, ten with trigeminaldeafferentiation pain, five with trigeminal neuropathic pain,two with postherpetic neuralgia, one patient with post-strokefacial pain and seven with occipital neuralgia. Interestingly,five of the seven patients with occipital neuralgia had atreatment failure, while the rate of successful stimulationin the other groups was between 70 and 100 % [63•].
In CCH, hcSCS was used for the first time in 2004 [64•].This first patient had a long-lasting history of neck pain, andhad undergone several operations and interventions such ascervical spondylodesis and lesional treatments of the occipitalnerves. In the later course of his pain, disease cluster attacksbegan, first episodic, but shortly after they became chronic. Asa compassionate treatment, the patient received a single highcervical percutaneous-type lead. In this patient, a SCS elec-trode was advanced epidurally in the cervical spine analogue tousual cervical SCS, but the final lead location was at the level
C1 (instead of C3–C6, as in conventional cervical SCS in otherconditions). Under SCS, the attack rate decreased from up toeight attacks per day to one attack every other day. Stimulationcould not abort an ongoing attack, but it reduced pain intensity.
After this encouraging outcome of hcSCS, a series ofpatients fulfilling operational criteria to define pharmaco-logically intractable headache [19•] were treated withhcSCS. The overall results regarding pain relief, reductionof attack frequency, duration and intensity were comparablyor superior to the published results of ONS (Table 1).However, a number of revision operations were necessary,due to electrode breakages and electrode dislocations.
Patients treated with hcSCS had an immediate pain reliefthrough SCS. Most patients had a prophylactic effect of SCSon their CH attacks. Attack frequency was markedly reduced,but also intensity and duration of the attacks decreased. Mostpatients were not able to abort an ongoing attack with SCS,but under SCS, intensity and duration of single attacks de-creased. All patients had a paresthesia elicited by SCS thatincluded the occipital region; but in some patients, the pares-thesia also comprised the trigeminal or frontal area. Mostly,the stimulation-induced paresthesia of the occipital region wassufficient to reduce the attack frequency [65•].
The pros of SCS for CCH are:
& That it has an immediate and stable effect; attacks arereduced or abolished from the implantation day on, and
& That it has a potentially higher efficacy than ONS,
The cons are:
& That its efficacy has not yet been proven in more thanone study,
& That the lead revision rate is currently higher comparedto ONS, and
& That it is more invasive than ONS.
Table 1 Overview of results from different neurostimulation studies for CCH
Author Year Modality n Reduction of attackfrequency (%)
Reduction of attackstrength (%)
Reduction of attackduration (%)
Follow-up(months)
Burns et al., 2007 [33]* ONS 8 19 23 n.d. 20
Magis et al., 2007 [35]* ONS 9 75 50 n.d. 15.1
Burns et al., 2009 [34] ONS 14 29 6 n.d. 17.5
Magis et al., 2011 [36] ONS 14 95 −2 n.d. 15.1
de Quintana et al., 2010 [37] ONS 4 56 49 64 6
Tronnier and Rasche, 2010 [38] ONS 4 82 38 n.d. 26
Fontaine et al., 2011 [39] ONS 13 68 49 n.d. 14.6
Mueller et al., 2011 [40] ONS 10 50 25 n.d. 12
Σ/ mean 59 55.4 20.6 64 18.9
Wolter et al., 2011 [65•] SCS 7 84 41 56 23
*not included in calculation of the mean, as same patients were included in later studies
ONS occipital nerve stimulation; SCS spinal cord stimulation; n.d. not determined
Curr Pain Headache Rep (2013) 17:324 Page 3 of 8, 324

Mode of Action
Despite some evidence for the underlying physiologicmechanisms, the mode of action of SCS is still largelyunknown [66••]. It is believed to act via multiple mecha-nisms acting at the segmental level, as animal models indi-cate. Under SCS, attenuation of the hyperexcitablemultimodal wide dynamic range cells (WDR neurons) inthe dorsal horn [67] was observed, and increased γ-aminobutyric acid (GABA) release [68, 69] from inhibitoryinterneurons was demonstrated to account for that effect,particularly by activation of the GABA-B receptor [70].There also seem to be some contribution of the cholinergicsystem to SCS effects. Under SCS, release of acetylcholinein the dorsal horn was observed and later attributed toactivation of the muscarinic M4 receptor [71].
Further, supraspinal pain-modulating centres were shownto be activated via rostral projections of the dorsal columnnuclei [72]. The stimulation effect on the background painand pain intensity is believed to be due to direct modulationof trigeminal traffic through cervical sensory input at thetrigeminocervical complex in the brainstem, which is alsoaffected in ONS [73]. The modulatory effect on attackfrequency is believed to include more complex circuitry,including limbic structures and the hypothalamus due tothe overall reduced pain induced stress. Both hcSCS andONS are believed to activate the trigeminocervical complex.However, it remains to be elucidated whether there is adifference between peripheral stimulation (ONS) and centralnervous system stimulation (SCS).
Electrode Position
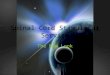
The optimal electrode position for hcSCS appears to beslightly (maximal 2–3 mm) paramedian at the craniocervicaljunction (Fig. 1). However, sometimes the posterior arch ofatlas impedes further cranial electrode movement. Inpatients with an electrode tip position below the arch ofatlas, a sufficient paresthesia, covering the occipital region,reaching up to the frontal region and also including parts ofthe trigeminal territory, was observed. Maybe the treatmentfailures in five of the seven patients with occipital neuralgiain the study by Tomycz and Moossy may be attributed to theelectrode position. Interestingly, their technique yielded ex-cellent results with different kinds of trigeminal pain, whileit was less effective in occipital neuralgia. The position ofthe lead tip in this study was directly at the craniocervicaljunction. In some cases, a small occipital craniectomy waseven performed to achieve a higher electrode position.Possibly, with an electrode tip position cranial to the archof atlas, a higher proportion of trigeminal afferents can bestimulated, while in the height of or below the atlas, more
occipital afferents are recruited. The caudal trigeminal nu-cleus is reaching at least to the C2 segment and carries closeconnections to the occipital afferents [74].
In SCS, stimulation of the dorsal columns is intended. Inthe cervical spine, due to its high mobility, this may bedifficult to accomplish. It has been postulated that the degreeof electrical conductivity is determined by the thickness ofthe spinal fluid layer [75]. Particularly in the cervical spine,this may be changed with head movements. Moreover,variances of up to 2 mm in lateral position of the spinalcord in the spinal canal have been found in MRI studies onhealthy volunteers [76].Thus, the radiological midline mustnot necessarily correspond to the functional midline. Also, aconcomitant stimulation of the C2 nerve root in hcSCScannot entirely be ruled out.
Complications
In SCS, there is a principal risk of permanent neurologicaldeficit, but it is apparently low, given the low number ofpublished cases and a number of approximately 30,000 SCSsystems implanted annually [66••]. Two reviews on SCS[77, 78] found no case of permanent neurological deficit,while in one review, one case out of 2,972 patients treated(0.03 %) was found [45••]. In the literature, there are twocases of quadriplegia secondary to cervical lead insertion[79] [80] and four cases of paraplegia post thoracolumbarSCS [81].
Despite the low risk for permanent morbidity, SCS car-ries a relatively high risk of device-related complications.The complication rate of cervical SCS is known to be higherthat that of thoracolumbar SCS [82].
Fig. 1 Optimal electrode position; the electrode tip lies directly belowthe occipital bone
324, Page 4 of 8 Curr Pain Headache Rep (2013) 17:324

In the series of seven patients with hcSCS for CCH,within a mean follow-up 23 months, two revision operationsdue to electrode dislocation and five revisions due to leadbreakage were necessary. One patient received a secondelectrode due to switch of CCH. Three patients had replace-ments of the implantable pulse generator (IPG) due to bat-tery depletion [65•]. As most patients preferred a continuousstimulation, revision surgeries due to battery depletion canbe circumvented in the future by the first-line use of re-chargeable devices.
All in all, the rate of revision operations due to leaddislocation or breakage in hcSCS is higher than that pub-lished in ONS studies for CCH [33–35, 37–40]. On theother hand, the hcSCS study had a longer follow-up thanthe ONS studies (Table 1). In comparison, in a study of ONSon 26 patients (12 migraine patients, five CCH patients andnine patients with miscellaneous headache diagnoses) 25lead revisions were necessary during a mean follow-up of37.4 months [83]. However, to date, the numbers of patientstreated with hcSCS of are still too small for definite con-clusions on the complication rate.
Variability of Stimulation with Head Movements
Under cervical SCS, particularly with high cervical leadlocation, patients often report changes in intensity or loca-tion of the stimulation-induced paresthesia triggered by headmovements. This was the case to a greater or lesser extent inmost of the patients implanted with high cervical SCSelectrodes for CCH; however, it did not change the efficacyof hcSCS. The problem of changing paresthesia wasreviewed in patients with “conventional” cervical SCS, withlead locations between C3 and C7. Here, 11 out of 14patients reported changes in paresthesia with head move-ments. These, however, did not affect the extent of painreduction elicited by SCS. Further, the overall satisfactionwith neurostimulation therapy was also not affected by thepresence of paresthesia changes with head movements [61].Presumably, the use of paddle type electrodes could at leastpartially solve this problem, as these occupy a higher pro-portion of the epidural space, thus narrow the space betweenelectrode and dura, and therefore enhance the electricalconductivity.
Conclusion
To date, the data still support the use of ONS as a first-linetherapy for refractory CCH. However, SCS may be indicat-ed in case of unsuccessful ONS. In this situation, theimplanted ONS-system can be converted into a SCS-system. Under closer consideration, ascribed problems of
SCS, such as invasiveness, variability of paresthesia andlead revisions, appear to be of minor relevance. Furtherstudies of hcSCS for CCH are necessary to define its futurerole in the neuromodulatory treatment of medication-resistant CCH.
Conflict of Interest Dr. Tilman Wolter reported receiving a travelgrant from Boston Scientific.
Dr. Holger Kaube reported no conflicts of interest relevant to thisarticle.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Silberstein SD, Olesen J, Bousser MG, Diener HC, Dodick D, FirstM, et al. The International Classification of Headache Disorders,2nd Edition (ICHD-II)—revision of criteria for 8.2 Medication-overuse headache. Cephalalgia. 2005;25(6):460–5. doi:10.1111/j.1468-2982.2005.00878.x.
2. Dodick DW, Capobianco DJ. Treatment and management of clus-ter headache. Curr Pain Headache Rep. 2001;5(1):83–91.
3. Ekbom K, Lindgren L, Nilsson BY, Hardebo JE, Waldenlind E.Retro-Gasserian glycerol injection in the treatment of chroniccluster headache. Cephalalgia. 1987;7(1):21–7.
4. Sweet WH. Surgical treatment of chronic cluster headache.Headache. 1988;28(10):669–70.
5. Mathew NT, Hurt W. Percutaneous radiofrequency trigeminal gan-gliorhizolysis in intractable cluster headache. Headache.1988;28(5):328–31.
6. Donnet A, Valade D, Regis J. Gamma knife treatment for refrac-tory cluster headache: prospective open trial. J Neurol NeurosurgPsychiatry. 2005;76(2):218–21. doi:10.1136/jnnp.2004.041202.
7. Donnet A, Tamura M, Valade D, Regis J. Trigeminal nerve radio-surgical treatment in intractable chronic cluster headache: unex-pected high toxicity. Neurosurgery. 2006;59(6):1252–7.doi:10.1227/01.NEU.0000245612.86484.7. discussion 7.
8. McClelland 3rd S, Tendulkar RD, Barnett GH, Neyman G, SuhJH. Long-term results of radiosurgery for refractory cluster head-ache. Neurosurgery. 2006;59(6):1258–62. doi:10.1227/01.NEU.0000245614.94108.4B. discussion 62–3.
9. McClelland 3rd S, Barnett GH, Neyman G, Suh JH. Repeat tri-geminal nerve radiosurgery for refractory cluster headache fails toprovide long-term pain relief. Headache. 2007;47(2):298–300.doi:10.1111/j.1526-4610.2006.00701.x.
10. Green MW. Long-term follow-up of chronic cluster headachetreated surgically with trigeminal tractotomy. Headache.2003;43(5):479–81.
11. Kirkpatrick PJ, O’Brien MD, MacCabe JJ. Trigeminal nerve sectionfor chronic migrainous neuralgia. Br J Neurosurg. 1993;7(5):483–90.
12. Jarrar RG, Black DF, Dodick DW, Davis DH. Outcome of trigem-inal nerve section in the treatment of chronic cluster headache.Neurology. 2003;60(8):1360–2.
13. Rowed DW. Chronic cluster headache managed by nervus inter-medius section. Headache. 1990;30(7):401–6.
Curr Pain Headache Rep (2013) 17:324 Page 5 of 8, 324

14. Morgenlander JC, Wilkins RH. Surgical treatment of cluster head-ache. J Neurosurg. 1990;72(6) :866–71. doi :10.3171/jns.1990.72.6.0866.
15. Solomon S, Apfelbaum RI. Surgical decompression of the facialnerve in the treatment of chronic cluster headache. Arch Neurol.1986;43(5):479–82.
16. Felisati G, Arnone F, Lozza P, Leone M, Curone M, Bussone G.Sphenopalatine endoscopic ganglion block: a revision of a traditionaltechnique for cluster headache. Laryngoscope. 2006;116(8):1447–50. doi:10.1097/01.mlg.0000227997.48020.44.
17. • Sanders M, Zuurmond WW. Efficacy of sphenopalatine ganglionblockade in 66 patients suffering from cluster headache: a 12- to70-month follow-up evaluation. J Neurosurg. 1997;87(6):876–80.doi:10.3171/jns.1997.87.6.0876. A large study on radiofrequencytreatment in episodic and in chronic CH.
18. Lad SP, Lipani JD, Gibbs IC, Chang SD, Adler Jr JR, Henderson JM.Cyberknife targeting the pterygopalatine ganglion for the treatmentof chronic cluster headaches. Neurosurgery. 2007;60(3):E580–1.doi:10.1227/01.NEU.0000255348.33582.DE. discussioin E1.
19. • Goadsby PJ, Schoenen J, Ferrari MD, Silberstein SD, DodickD. Towards a definition of intractable headache for use inclinical practice and trials. Cephalalgia. 2006;26(9):1168–70.doi:10.1111/j.1468-2982.2006.01173.x. The widely accepted def-inition of intractable headache to which in most clinical trialsis referred to.
20. •• May A, Bahra A, Buchel C, Frackowiak RS, Goadsby PJ.Hypothalamic activation in cluster headache attacks. Lancet.1998;352(9124):275–8. doi:10.1016/S0140-6736(98)02470-2.The first report of hypothalamic activation during CH attacks,an observation that later led to the advent of DBS for CCH.
21. Sprenger T, Boecker H, Tolle TR, Bussone G, May A, Leone M.Specific hypothalamic activation during a spontaneous clusterheadache attack. Neurology. 2004;62(3):516–7.
22. Franzini A, Ferroli P, Leone M, Broggi G. Stimulation of theposterior hypothalamus for treatment of chronic intractable clusterheadaches: first reported series. Neurosurgery. 2003;52(5):1095–9.discussion 9–101.
23. Leone M. Deep brain stimulation in headache. Lancet Neurol.2006;5(10):873–7. doi:10.1016/S1474-4422(06)70575-0.
24. Leone M, Proietti Cecchini A, Franzini A, Broggi G, Cortelli P,Montagna P, et al. Lessons from 8 years’ experience of hypotha-lamic s t imula t ion in c lus ter headache. Cephala lg ia .2008;28(7):787–97. doi:10.1111/j.1468-2982.2008.01627.x. dis-cussion 98.
25. Schoenen J, Di Clemente L, Vandenheede M, Fumal A, De PasquaV, Mouchamps M, et al. Hypothalamic stimulation in chroniccluster headache: a pilot study of efficacy and mode of action.Brain. 2005;128(Pt 4):940–7. doi:10.1093/brain/awh411.
26. Fontaine D, Lazorthes Y, Mertens P, Blond S, Geraud G, Fabre N,et al. Safety and efficacy of deep brain stimulation in refractorycluster headache: a randomized placebo-controlled double-blindtrial followed by a 1-year open extension. J Headache Pain.2010;11(1):23–31. doi:10.1007/s10194-009-0169-4.
27. Matharu MS, Zrinzo L. Deep brain stimulation in cluster headache:hypothalamus or midbrain tegmentum? Curr Pain Headache Rep.2010;14(2):151–9. doi:10.1007/s11916-010-0099-5.
28. Matharu MS, Zrinzo L. Deep brain stimulation in cluster headache.Expert Rev Neurother. 2011;11(4):473–5. doi:10.1586/ern.11.35.
29. •Weiner RL, Reed KL. Peripheral Neurostimulation for Control ofIntractable Occipital Neuralgia. Neuromodulation. 1999;2(3):217–21. In this study, occipital nerve stimulation was described for thefirst time.
30. Schwedt TJ, Dodick DW, Hentz J, Trentman TL, Zimmerman RS.Occipital nerve stimulation for chronic headache–long-term safetyand efficacy. Cephalalgia. 2007;27(2):153–7. doi:10.1111/j.1468-2982.2007.01272.x.
31. Schwedt TJ, Dodick DW, Trentman TL, Zimmerman RS. Occipitalnerve stimulation for chronic cluster headache and hemicraniacontinua: pain relief and persistence of autonomic features.Cephalalgia . 2006;26(8):1025–7. doi :10.1111/j .1468-2982.2006.01142.x.
32. Matharu M, Watkins L, Shanahan P. Treatment of medically in-tractable SUNCT and SUNA with occipital nerve stimulation. JNeurol Neurosurg Psychiatry. 2010;81:e51–e2.
33. Burns B, Watkins L, Goadsby PJ. Treatment of medically intrac-table cluster headache by occipital nerve stimulation: long-termfollow-up of eight patients. Lancet. 2007;369(9567):1099–106.doi:10.1016/S0140-6736(07)60328-6.
34. Burns B, Watkins L, Goadsby PJ. Treatment of intractable chroniccluster headache by occipital nerve stimulation in 14 patients.Neuro logy. 2009 ;72(4 ) :341–5 . do i :10 .1212 /01 .wn l .0000341279.17344.c9.
35. Magis D, Allena M, Bolla M, De Pasqua V, Remacle JM,Schoenen J. Occipital nerve stimulation for drug-resistant chroniccluster headache: a prospective pilot study. Lancet Neurol.2007;6(4):314–21. doi:10.1016/S1474-4422(07)70058-3.
36. Magis D, Gerardy PY, Remacle JM, Schoenen J. Sustained effec-tiveness of occipital nerve stimulation in drug-resistant chroniccluster headache. Headache. 2011;51(8):1191–201. doi:10.1111/j.1526-4610.2011.01973.x.
37. de Quintana-Schmidt C, Casajuana-Garreta E, Molet-Teixido J,Garcia-Bach M, Roig C, Clavel-Laria P, et al. Stimulation of theoccipital nerve in the treatment of drug-resistant cluster headache.Rev Neurol. 2010;51(1):19–26.
38. Tronnier V, Rasche D. Subcutaneous peripheral stimulation of thegreater occipital nerve for the treatment of chronic headache syn-dromes. Schmerz. 2010;24(5):441–8. doi:10.1007/s00482-010-0970-7.
39. Fontaine D, Christophe Sol J, Raoul S, Fabre N, Geraud G, MagneC, et al. Treatment of refractory chronic cluster headache by chronicoccipital nerve stimulation. Cephalalgia. 2011;31(10):1101–5.doi:10.1177/0333102411412086.
40. Mueller OM, Gaul C, Katsarava Z, Diener HC, Sure U, Gasser T.Occipital nerve stimulation for the treatment of chronic clusterheadache—lessons learned from 18 months experience. Cent EurNeurosurg. 2011;72(2):84–9. doi:10.1055/s-0030-1270476.
41. Ibarra E. Neuromodulación del Ganglio Esfenopalatino paraAliviar los Síntomas de la Cefalea en Racimos. Reporte de unCaso. Boletín El Dolor. 2007;46(16):12–8.
42. • Ansarinia M, Rezai A, Tepper SJ, Steiner CP, Stump J, Stanton-Hicks M, et al. Electrical stimulation of sphenopalatine ganglionfor acute treatment of cluster headaches. Headache.2010;50(7):1164–74. doi:10.1111/j.1526-4610.2010.01661.x.This study describes electrical stimulation of the SPG, a techniquefor treatment of acute CH.
43. Tepper SJ, Rezai A, Narouze S, Steiner C, Mohajer P, Ansarinia M.Acute treatment of intractable migraine with sphenopalatine gan-glion electrical stimulation. Headache. 2009;49(7):983–9.doi:10.1111/j.1526-4610.2009.01451.x.
44. •• Shealy CN, Mortimer JT, Reswick JB. Electrical inhibition ofpain by stimulation of the dorsal columns: preliminary clinicalreport. Anesth Analg. 1967;46(4):489–91. The first report ofdorsal column stimulation.
45. •• Cameron T. Safety and efficacy of spinal cord stimulation for thetreatment of chronic pain: a 20-year literature review. J Neurosurg.2004;100(3 Suppl Spine):254–67. A comprehensive and detailedreview on outcome and complication rate of SCS.
46. Meglio M, Cioni B, Rossi GF. Spinal cord stimulation in manage-ment of chronic pain. A 9-year experience. J Neurosurg.1989;70(4):519–24. doi:10.3171/jns.1989.70.4.0519.
47. De La Porte C, Van de Kelft E. Spinal cord stimulation in failedback surgery syndrome. Pain. 1993;52(1):55–61.
324, Page 6 of 8 Curr Pain Headache Rep (2013) 17:324

48. Hassenbusch SJ, Stanton-Hicks M, Covington EC. Spinal cordstimulation versus spinal infusion for low back and leg pain.Acta Neurochir Suppl. 1995;64:109–15.
49. Ohnmeiss DD, Rashbaum RF, Bogdanffy GM. Prospective out-come evaluation of spinal cord stimulation in patients with intrac-table leg pain. Spine (Phila Pa 1976). 1996;21(11):1344–50.discussion 51.
50. •• Kumar K, Taylor RS, Jacques L, Eldabe S, Meglio M, Molet J,et al. Spinal cord stimulation versus conventional medical man-agement for neuropathic pain: a multicentre randomised controlledtrial in patients with failed back surgery syndrome. Pain.2007;132(1–2):179–88. doi:10.1016/j.pain.2007.07.028. An inter-national multicentre RCT that showed that SCS provides painrelief and improves health-related quality of life and functionalcapacity in patients with neuropathic pain secondary to failedback surgery syndrome.
51. Kemler MA, Reulen JP, Barendse GA, van Kleef M, de Vet HC,van den Wildenberg FA. Impact of spinal cord stimulation onsensory characteristics in complex regional pain syndrome type I:a randomized trial. Anesthesiology. 2001;95(1):72–80.
52. Harke H, Gretenkort P, Ladleif HU, Rahman S. Spinal cord stim-ulation in sympathetically maintained complex regional pain syn-drome type I with severe disability. A prospective clinical study.Eur J Pain. 2005;9(4):363–73. doi:10.1016/j.ejpain.2004.09.003.
53. Kemler MA, de Vet HC, Barendse GA, van den Wildenberg FA,van Kleef M. Spinal cord stimulation for chronic reflex sympa-thetic dystrophy–f ive-year follow-up. N Engl J Med.2006;354(22):2394–6. doi:10.1056/NEJMc055504.
54. Harke H, Gretenkort P, Ladleif HU, Koester P, Rahman S. Spinalcord stimulation in postherpetic neuralgia and in acute herpeszoster pain. Anesth Analg. 2002;94(3):694–700. table ofcontents.
55. •• Mannheimer C, Eliasson T, Augustinsson LE, Blomstrand C,Emanuelsson H, Larsson S, et al. Electrical stimulation versuscoronary artery bypass surgery in severe angina pectoris: theESBY study. Circulation. 1998;97(12):1157–63. The ESBY studyshowed that coronary arterial bypass grafting and SCS appear tobe equivalent methods in terms of symptom relief in this group ofpatients.
56. Ubbink DT, Vermeulen H. Spinal cord stimulation for non-reconstructable chronic critical leg ischaemia. Cochrane DatabaseSyst Rev. 2005;(3):CD004001. doi:10.1002/14651858.CD004001.pub2.
57. Bennett D, Alo K, Oakley J, Feler C. Spinal Cord Stimulation forComplex Regional. Pain Syndrome I [RSD]: a Retrospective.Multicenter Experience from 1995 to 1998 of 101 Patients.Neuromodulation. 1999;2(3):202–10.
58. Forouzanfar T, Kemler MA, Weber WE, Kessels AG, van Kleef M.Spinal cord stimulation in complex regional pain syndrome: cer-vical and lumbar devices are comparably effective. Br J Anaesth.2004;92(3):348–53. doi:10.1093/bja/aeh072.
59. Francaviglia N, Silvestro C, Maiello M, Bragazzi R, Bernucci C.Spinal cord stimulation for the treatment of progressive systemicscleros is and Raynaud ’s syndrome. Br J Neurosurg.1994;8(5):567–71.
60. Simpson BA, Bassett G, Davies K, Herbert C, Pierri M. Cervicalspinal cord stimulation for pain: a report on 41 patients.Neuromodulation. 2003;6(1):20–6. doi:10.1046/j.1525-1403.2003.03003.x.
61. Wolter T, Kieselbach K. Cervical spinal cord stimulation: an anal-ysis of 23 patients with long-term follow-up. Pain Physician.2012;15(3):203–12.
62. Vallejo R, Kramer J, Benyamin R. Neuromodulation of the cervi-cal spinal cord in the treatment of chronic intractable neck andupper extremity pain: a case series and review of the literature.Pain Physician. 2007;10(2):305–11.
63. • Tomycz ND, Deibert CP, Moossy JJ. Cervicomedullary junctionspinal cord stimulation for head and facial pain. Headache.2011;51(3):418–25. doi:10.1111/j.1526-4610.2010.01829.x. Thisstudy describes long-term results of cervicomedullary junctionstimulation, a technique that comes very near to hcSCS. In con-trast to hcSCS, the authors used paddle electrodes that theyimplanted under general anesthesia via laminotomy C1.
64. • Wolter T, Kaube H, Mohadjer M. High cervical epidural neuro-stimulation for cluster headache: case report and review of theliterature. Cephalalgia. 2008;28(10):1091–4. doi:10.1111/j.1468-2982.2008.01661.x. The first case report of hcSCS for CCH.
65. • Wolter T, Kiemen A, Kaube H. High cervical spinal cord stimula-tion for chronic cluster headache. Cephalalgia. 2011;31(11):1170–80.doi:10.1177/0333102411412627. The first series of hc SCS for CCH.
66. •• Linderoth B, Meyerson BA. Spinal cord stimulation: explorationof the physiological basis of a widely used therapy.Anes the s io logy. 2010 ;113 (6 ) :1265–7 . do i :10 .1097 /ALN.0b013e3181fcf590. A comprehensive and condensed articleabout the physiological mechanisms of action of SCS.
67. Yakhnitsa V, Linderoth B, Meyerson BA. Spinal cord stimulationattenuates dorsal horn neuronal hyperexcitability in a rat model ofmononeuropathy. Pain. 1999;79(2–3):223–33.
68. Linderoth B, Stiller CO, Gunasekera L, O’Connor WT, UngerstedtU, Brodin E. Gamma-aminobutyric acid is released in the dorsalhorn by electrical spinal cord stimulation: an in vivo microdialysisstudy in the rat. Neurosurgery. 1994;34(3):484–8. discussion 8–9.
69. Stiller CO, Cui JG, O’Connor WT, Brodin E, Meyerson BA,Linderoth B. Release of gamma-aminobutyric acid in the dorsalhorn and suppression of tactile allodynia by spinal cord stimulationin mononeuropathic rats. Neurosurgery. 1996;39(2):367–74. dis-cussion 74–5.
70. Cui JG, Meyerson BA, Sollevi A, Linderoth B. Effect of spinalcord stimulation on tactile hypersensitivity in mononeuropathicrats is potentiated by simultaneous GABA(B) and adenosine re-ceptor activation. Neurosci Lett. 1998;247(2–3):183–6.
71. Schechtmann G, Song Z, Ultenius C, Meyerson BA, Linderoth B.Cholinergic mechanisms involved in the pain relieving effect ofspinal cord stimulation in a model of neuropathy. Pain.2008;139(1):136–45. doi:10.1016/j.pain.2008.03.023.
72. El-Khoury C, Hawwa N, Baliki M, Atweh SF, Jabbur SJ, SaadeNE. Attenuation of neuropathic pain by segmental and supraspinalactivation of the dorsal column system in awake rats.Neuroscience. 2002;112(3):541–53.
73. Bartsch T, Goadsby PJ. Stimulation of the greater occipital nerveinduces increased central excitability of dural afferent input. Brain.2002;125(Pt 7):1496–509.
74. Kerr FW, Olafson RA. Trigeminal and cervical volleys.Convergence on single units in the spinal gray at C-1 and C-2.Arch Neurol. 1961;5:171–8.
75. Holsheimer J, Barolat G, Struijk JJ, He J. Significance of the spinalcord position in spinal cord stimulation. Acta Neurochir Suppl.1995;64:119–24.
76. Holsheimer J, den Boer JA, Struijk JJ, Rozeboom AR. MR assess-ment of the normal position of the spinal cord in the spinal canal.AJNR Am J Neuroradiol. 1994;15(5):951–9.
77. Turner JA, Loeser JD, Deyo RA, Sanders SB. Spinal cord stimu-lation for patients with failed back surgery syndrome or complexregional pain syndrome: a systematic review of effectiveness andcomplications. Pain. 2004;108(1–2):137–47. doi:10.1016/j.pain.2003.12.016.
78. Taylor RS, Van Buyten JP, Buchser E. Spinal cord stimulation forchronic back and leg pain and failed back surgery syndrome: asystematic review and analysis of prognostic factors. Spine (PhilaPa 1976). 2005;30(1):152–60.
79. Barolat G, Peacock WJ, Staudt LA. Pain and spasticity. In: EC B,editor. Spine surgery: Techniques, complication avoidance, and
Curr Pain Headache Rep (2013) 17:324 Page 7 of 8, 324

management. 2nd ed. Philadelphia: Elsevier ChurchillLivingstone; 2005. p. 1239–52.
80. Meyer SC, Swartz K, Johnson JP. Quadriparesis and spinal cordstimulation: case report. Spine (Phila Pa 1976). 2007;32(19):E565–8. doi:10.1097/BRS.0b013e31814541dc.
81. Smith CC, Lin JL, Shokat M, Dosanjh SS, Casthely D. A report ofparaparesis following spinal cord stimulator trial, implantation andrevision. Pain Physician. 2010;13(4):357–63.
82. Rosenow JM, Stanton-Hicks M, Rezai AR, Henderson JM. Failuremodes of spinal cord stimulation hardware. J Neurosurg Spine.2006;5(3):183–90. doi:10.3171/spi.2006.5.3.183.
83. Brewer AC, Trentman TL, Ivancic MG, Vargas BB, Rebecca AM,Zimmerman RS, et al. Long-term outcome in occipital nervestimulation patients with medically intractable primary headachedisorders. Neuromodulation. 2012. doi:10.1111/j.1525-1403.2012.00490.x.
324, Page 8 of 8 Curr Pain Headache Rep (2013) 17:324