Embed Size (px)
Citation preview

r
REVIEW
Spontaneous bacterial peritonitis in patients with liver cirrhosis and
ascites - New insights using cytokine and cytokine receptor
analysis in ascites
T1 w A N nus, MD, JURl;EN SCJ l( lLM ERll'l I, M D
T ANous, J SCH6LMERICH. Spontaneous bacterial peritonitis in patients with liver cirrhosis and ascites - New insights using cytokine and cytokine receptor analysis in ascites. Can J Gastroenterol 1992;6(3): 141-146. The cloning and expression of cytokines and their receptors has led to the development of sensitive and specific immunoassays for their determination in bio logical fluiJs such as ascites. Using such assays, the cycokines lL-lP, JL-6, IL-8 and TNFa. were found in ascitic fluid samples of patienrs with infected and malignant asci tes. IL-6 was found in high concentra tio ns even in ascites samples of not infected hepatic ascites. In adJition, high concentrations of soluble TNF receptor p55 and p75 were found in asci tes. IL-1 and IL-6 concentratio ns were increased in infected asci tes while concentrations of both TNF receptors were increased in infectcJ and malignant ascites, indicating that the combined measurement of cycokines and cytokinc receptors may be helpful for the differential diagnosis o f ascites (allowing the differentiation among infected , malignant and uncomplicated hepatic ascites). High concentrations of cytokines and soluble cyrokine recepcors in ascites, their increase during infection and malignancy, and their high potency co regulate inflammatory processes and other mediators indicate that they play an important role in the pathogenesis of ascites. Thus, measuring cytokines and soluble cytokine receptors in ascitic fluid opens a new window to study the pathogenesis of ascitcs and eventually may lead to the development of new methods of medical treatment of nscitcs using specific cytokine antagonists. (Pour resume, voir page 14 2)
Key Words: Ascites , Cytol<ines , lnterleul<in, Soluble cytol<ine receptors, Spontaneous bacterial peritonitis , Tumour 11ecrosis factor
De/>arrmenr of Internal Medicine I, U11i11er.1ity of Reg.:nslnll'g, Franz}mef Scnms., A llee, W-8400 Regemlntrg, Germany
Con·cspondence and re/mnts: Professor Dr J Sc/1/ilmcric/1. Medizinische Klinik und Poliklinik I, Universitat Regm.ihurg Fmnz ]osef Srraim Alice I I , \'v'-8400 Hcgernh11rg, Gm11w1y. Telephone 094 I /944-700 I . Fax 0941 /944-7002
Receit,ecl for /mhl,cminn April IO, 199 2. Acce/ned Ma)' 11 . J 99 2
ASCITES IS A FREQUENT COMPLl
cauon of severe liver J i~ea~c~ with portal hypert ension and nf ma lignant tumnurs metastatic to the peri toneum ( 1,2 ). Whi le malignan t asc ites me rarely infected, r arien t~ with hepatic asc ites frequen tly develop spo ntaneous hacteria l peritoni1 is; often wi thout any ,,hvious pri mary source of infec tion (3 ) . T he prevalence of sr ontancou~ hactcrial peritoni t is in ho~pirn lized patients wi th hera tic cirrhosis and ascites is arpmximatcly 15%. Sr onraneous hacterial peritoni1 is ,~ ,, severe complicatiun wi th a morta lity rate o( more than 50% and a h igh ra te of recurrence (approx imately 70% per year). T ypical symptom~ of spontaneous hacrerial peritoni tis arc ahdomi nal pain , feve r, hepatic enccphalnr athy nr unexr laincd clinical deterioration. Bacteria cultured from infccteJ ascites usuall y represent the normal acrnhic flora of the gut, bur J ue en the low num ber of bacteria in ascites (usually one/ml) , diagnosis of infection by cul ture of ascit ic fl uid is often difficult or not possible ( 4 ).
T here arc several pred isposing factors for 1hc manifes ta t ion of sponta-
CAN J GA:,TROENTI'RDI VOi 6 No 3 MAY/JUNE I 992 141

AN DUS AND SCI IOLMFRICI I
Peritonite bacterienne spontanee chez des patients presentant une cirrhose et de l'ascite: nouvelles approches a base de cytokines et analyse des recepteurs de cytokines dans l'ascite
RESUME: Le clonage ct !'expression des cytokines e t de leurs rcceptcurs ont mene ~1 la mise au poin t d'essais immunologiques sensibles ct spccifiques pour lcur detection clans !es liquidcs b iologiqucs tels que l'ascitc. A l'aidc de tc lles epreuves, lcs cyrokines lL- I B, IL-6, IL-8 et TNFa. ont ete decelees clans des echantillons J'ascice chez des pacienls presentant une ascite infectee et malignc. L'lL-6 a e te notec en concentration elevec, mcme Jans des echamillons non infecres. En outrc, des concentrations clcvees de recepteurs de TNF solubles p55 ct p75 ont etc trouvecs clans l'ascitc. Des concentrations d'IL-1 ct d'lL-6 etaicnt clcvees Jans l'ascite infectcc a lors quc des concentrations des recepteurs de TNF se trouvaicnt augmentes clans l'ascicc infcctee e t maligne, ce qui donne a penscr que la mesure combincc des cytokines ct de recepteurs de cytokincs pcuc sc revele r utile clans le diagnostic differentiel de l'ascitc ( en permettant la differenciation entre l'ascitc hepatiquc infcctce maligne et non compliqucc). Des concentrations elevees de cytokines ct des rccepteurs solubles de cytokines clans l'ascite, leur augmentation au COurs J e !'infection et Je la malignite Ct leur pOtenticl elcve a reg[cr le proccssus inflammatoirc ct d'autrcs mcdiateurs indiqucnt qu'ils joucnt un ro le important dans la pathogcnese de l'ascite. A insi, la mcsure des cytokincs ct des rcceptcurs solubles de cytokincs clans l'ascilc ouvre unc nouvelle avenue pour !'crude de la pathogcncsc de l'ascitc ct pourra mencr a la misc au point de nouvelles thcrapeutiqucs mcdicalcs contre l'ascite a !'aide d'antagonistcs specifiques de cytokines.
neous hactcrial peri tonitis: an impaired liver function weakens the immune system locally and sysLcmically (5-7); intra- and cxtrahcpalic shunt ing leads to a decreased clearance o( bacteria by the hepatic rcticulocndochclia l system and to rccurrcnL systemic bacceriemia; and pat ients with low ascitic tota l prote in concenLrat ions (8) and low opsonic activity in a c itic fluids and scrum have a higher risk for spontaneous bacteria l peritonitis (5,7,9).
Cyrokincs arc important med iators play ing a key role in immune system regulation and synthesis of hepatic acute phase prote ins such as complement factors ( 10- 12). Most cycokincs arc glycoprotcins with a molecula r mass below 80,000 D. Cytokines usua ll y act in picomnlar concentrations via specific, high affini ty cell surface receptors. Cells involved in cytokinc synthesis include: blood cel ls such as monocytcs, lymphocytes and platelets; stromal cells uch as fibroblasts, enc.lorhelia l cells
and smomh muscle eel Is; and parcnchymal cells such as kcratin ocytcs and hcpatocytcs. Most cytokines may not only he produced hy a variety of cell L ypes as a reacLion to diffe rent
stimuli, hut a lso may have numerous biological effects on several d ifferent target cel ls.
Mo lecular cloning of cytokincs and thei r receptors led to the development of sensitive and specific assays which facilitated their measurement in blood and other body fluids such as ascitcs. T he following review summarizes the current knowledge about cytokines and their receptors in ascites and discus cs possible clinical applications of their measurement.
CYTOKINES IN ASCITES Although scrum concentrations of
cytokines have been determined in patients with liver diseases for several years ( I 3-22), cytokincs o nly recentl y have been detected in asc ites. In patients with hepatic asciLcs the cywkincs found in ascitic fluid were intcrleukin(I L)- 113 (23), lL-6 (23-29), IL-8 (23) and tumour necrosis factor a lpha (TNfo) (23-25,28) . ll -6 was by forthc most abundant cytokine in ascitcs, wiLh concentrations ranging between 200 and 100,000 pg/ml (23 -27,29). ln contrast, IL-1 13 was undcLcctablc in most ascitic flu id samples and o nly was found
in cu lture-positive asc itcs (23). Abo, lL-8 and TN Fa were only de tectable in some ascit ic nuid samples (23 ).
Ascitic concentratio n IL- I B (23 ), IL-6 (23-27,29) and T NFa (23-25) were h igher in patients with spontaneous bacterial peritonitis than in patients with uninfected hepatic a,c ites, and were found to be reduced tn lower concentrations after succcs ·ful an tib iotic treatment (23-2 5); finding could be used to separate culture-positive from culture-negative ascitc~. Ill B and I L-6 were found to separate the two groups with a d iagnosLic accuracy of 98% at cutoff levels of IO and 8000 pg/ml. Interestingly, patients with the culture-negative variant o( spontaneous bacterial peri toni tis had no elevated concentrations of cyLOkines.
In six patients withou l pcritonilis, concentrations of I L-6 anJ TN Fa. were only slighdy h igher in ascitcs than in serum (24,25 ); however, in 21 patients without peri toni tis, ascitcs conccntra- , tions were about I 00-fold higher than corresponding plasma conccntrarions (23,26,27,29). This ratio was 500-fold h igher in patients with periton itis. T hese find ings strongly suggest Lhat JL-6 is produced locally in the pcriLOncal cavity. Furthermore, since half of the ascites fluid shifts back and fonh every hour through the large capi llary bed of the splanchn ic peri toneum (3 l,32) :md since IL-6 rapidly d iffuses into the plasm.a (33) ( where it is cleared within a few minutes 134]), in traperiLOncal production of IL-6 must be continuously high to maintain the high concenlrations found in all patients with asci tes. This, in turn, suggests that there is continuous timu la Li on of peritoneal inflammatory cells even in patients with uncom.plicaccd asci Lcs. Among these cells, pcri roneal macrophages probahly arc the most importanl source of lL-6 production since isolated peri toneal macrophages from patients with ov;i
rian carci noma (35) and from mice (36-38) have been shown to release IL- I (35, 37,38), IL-6 (35,38) and TNFa 06,37).
LipopolysacchariJes prcsumcihly arc the major st imula ling factor of cytokinc synthesis in hepat ic ascitcs since they strongly stimula te cytokinc synLhesis ( l0,39), and h igh lipnpolys:ic-
142 CAN J GASHOENTEROL VOi 6 No 3 MAY/j UNL 1992

Cytokines and soluble cytokine receptors in ascites
charidc levels have been founJ frequently in ascitcs (791){,) and plasma of cirrhotic patients wiLh ascitcs (76% ) (40). The Gram-nega tive flora of the gut provide~ a huge pool of I ipopolysaccharides which mny emer systemic circulation and asc1uc nuid ( when hepatic clearance is impaired hy portal systemic shunting and there is decreased Kupffcr cell function a~ during li ver disease) (41,42). In ,1ddition, ev idence for lymphatic uptake nf lipopolysaccharidcs and even viahle G ram-negative bacteria ha~ hccn shown (43-45).
ROLE OF CYTOKINES IN A SCITES
Since cytokine~ arc ve ry potent inflammatory mediaL,)rs affect ing a broaJ range of effector cells, the presence of cycokines in asci tic fluid may have a great impact on the pathnphysiolngy of ascitcs. Increased ascitic cy toki nc concentrations during spontaneous bacterial pcritoniri~ indicate that Lhcy may act locally as p,irt of the host's ddcnce system againM infectious agents. For example, IL-8 induces migrntion and act ivation ofneutrophils (46), and IL- l (47), IL-6 ( 10 ) and TN Fa. (48) incrca~c T and B cell acti vity and mmspecific resistance to infection. High concen trations of the anri- inflammarory cytokinc IL-6 (found in all asc iLcs s,1mplcs) may protect the host from the pmcntially d,mgcrous systemic effects tif high concentrat ion~ of pm-inflammatory cytokines (ic, IL- I , IL-8 and TNFa.), since IL-6 can inhibit the synthesb o(
IL- I and TNFa in mononuclear cells (49,50).
Besides their protective ,1ction, an animal s tudy ( 51) showed tha t cycokincs may he involved in ascitcs formation. Cytnkincs 1rn1y induce asc iLcs formation hy sever.ii mechanisms. Cytokines such as I L- 1, interfcron-y and TNFa induce the production of nitrogen oxides in macrophages and endothelial cells (52,53) whi ch leads co periph eral vasodilmion a nd subsequent fluid retention. Furthermore, cytokines increase vascular pcrmeabilit y resulring in the trnnsudation nf plasma from the circulation inw extrnvascular sp,1cc (5 1,54 ).
Diffusion of cytuk ines lL- l , I L-6, IL-
8 ,rnd TNFa in to ch1: systemic c irculation can cause clinical signs suc h as fever, pain, wasting, hypot ens ion and septic shock anJ can contribute co the clinical picture of spontaneous bacter ial peritonitis.
SOLUBLE CYTOKINE RECEPTORS
Cytokincs act specifically on target cdls hy binding lll specific surfacehound receptors which trigger Mx:ond messenger mechanisms that lead to changes in the transcription of cytokinc-rcgulatcd prote ins. In addition to the surface-bound receptors, there arc soluble cyLOkinc receptors.
Elevated concentration~ of low ,1ffinity soluhlc IL-2 receptors have hecn found in the scra of pa tiems with herni titis R ( 55 ), autoimmune hepatitis ( 56), a wide variety of mhcr diseases ( 57) and after liver transpla ntation ( 58). S1,lublc reccpwrs for lL-6 and imcrforon-y can he purific1..I (mm normal human urine ( 59). The cltming and expression uf the murine IL-7 receptor led to detection of a soluble form which was secreted into the medium hy transfcc tcd cclb (60). Soluble inhibitory forms of IL- l (61, 62) and TNF (63-66) have hccn fllltnd in human scrum and urine. Recently, elevated scrum conccntrmion~ of w luhlc TNF reccptms were found in patients wi th burns o r renal failure, hut no increase was found in paticnb with c hronic polyarthritis (67).
Few daw exist ahout soluhlc cytokinc reccpLOrs in ascites. Soluble, high affini ty lL-4 rcccpLOrsarc present in the ascitcs fluid , scrum and urine of normal mice (68). Soluhlc IL-4 receptor con ccnLratio n w;is reduced in severe combined immuntKlcficicncy mice (68).
High conccntrntiom of ~oluhlc TN F receptor p55 and p7 5 were detec ted in all ascitcs and plasma samples of 34 patients with hcp<1 tic infected, nnnin fected and rmdignancy-rc latcd ascitcs (28, 30). ln all patients, molar TN F receptor cuncc ntrations were about 500-fold higher than molar TN Fa concentrations in the asc itcs; scrum samples ranged from 2.5 to 35 ng/mL in ascitcs ,md from 1.5 to 60 ng/mL in scrum . The mean concentrations of TNF rcceptm p55 and p75 were
CAN J GASTRtlENTER,)I. Vm 6 No 3 M AY/JUN!· 1992
e levated ahout 2.5 and 3.5 times, respecLively, i.n hmh infec ted hepatic and malignant asc iLes compared wid1 uncomplicated hepatic ascitcs. The asci Lcs TNF receptor conccntraLions were similar in patienrt- with infected ,ind malignant ascites. Plasma con centrations of TNF receptor p55 and p75 were elevated in Lhcsc subgroups, but showed a large overlap wid1 die non infected hepatic ascitcs samples.
The conccntrnti.ons ofTNF receptor p55 were higher th;:in TNF receptor p75 in asciLes, whereas TNF receptor p 7 5 was h ighc r in plasma conccntra-1 inns. The e lcv.ned cuncentratitms of TNF rcccpror p55 (24.2±15.2 ng/mL) and p75 (20.2± 14.4 ng/mL) found in 111fcctcd asci tic fluid decreased to lowe r levels ( L0.7± 1.89 and 7.50±1.80 ng/mL, rc~pcctivc ly) afrcr successful antibimic treatment.
1 ligh concen trmions of ~o luhle cytokine receptors, which increusc or decrease during the course of disease, misc several questions: what 1s the source of the soluble rcccprors?; hy what mcch a nibms a rc the receptors released ?; and htiw is the synthe~i~ and rclca~c of Lhc cytokinc receptor~ regu lated ?
ROLE OF CYTOKINE RECEPTORS IN ASCITES
High conccnwuions of soluble cyrokine receptor~ suggest an important immunorcgulamry role. The large amnunrs of soluble TNF receptors (500-fold molar exec~~ ahnve TNFa), for example, strongly impair TNF bioavai lahility in ascitcs and plasma. Sllluhle JL-2 rcccpwrs found in scra of patients with inflammatory disease~ may have similar immunomodulating cffccu, on Lhe activ,1tion ofT lymphocyLcs.
These high receptor concentrations may be an important, hcncficial part of the immuno logicc1I regulatory mcchani~m~ by minimizing tissue destruction caused hy cxcc~sivc cywkinc rc lca~e of innammatory cells during defence against infcctiou~ agent~ and t>thcr injuries. Al though cycokincs usually contribute to protection of the organism againsL infectious agents and to healing from injury, the ir act ions may become pern1cmu~ in certain patho logical ~ituatiom (cg, ~cptic shock, a more
14 l

AN11lJS AN!) SC! Jt)LMl:RICI I
hepatic infacled
~ TNFAp55
CTJ TNFAp75
malignant
! .. Q,
10000
1000
100 !BJ ll-6
10
0.1 hepalic infected malignant
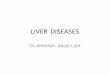
Figure I) Co11centrwiom of imerlCHkin ( I L! -1. I L-6, nono,ir 11ecrosis facror (TNF) rccepwr />55 and />75 memured hy enzyme-linked i1nmrn10,orhc111 ,1s.1ay. in mcite.1 of J>utients with /ic/latic. i11fcc1ed a11d malignam lLICites. Dara an' expre.1sed as means l. scandard deviwion
~evere JesLruc tion results than rhnc inJuced by the pathogen itself). Regulators of the biological activity of cytokincs, such as the deLccLeJ TNF receptors, which counteract potentially harmful effect~ of TNF me therefore essential to maintain physinlogic;i l homeosLasis during infection and mal ignancy.
On the other hand, release of TNF recepwrs in malignant ascites may be a defe nsive mechanism of malignant cclb to proLCCt them from cyto tox ic effects ofTNF. High concentrations of TNF recepturs in malignant asc ites -which a lso can strongly Jiminish hioavailability of locally <1dminisLered TNF in the trcatmenL o f cancer patient~ (65) - should be considered in such clinica l trials.
CLINICAL APPLICATIONS The finding of cytokines and soluble
cytok ine receptors in ascitic fluid is an important sLep co unJerstand the parhophysiology of asciLes. It also 1m1y lead ro several c linical applications. The fi rst studies suggest that measure-
REFERENCES I. Conn 110. The d1.1gm1,1, and
exarninatilm of as..:it ic f1uid. In: Beker S. ed. Diagnu,tic Procedure, in the Evalumion of I lepnric Disea,e,. New Yurk: Alan R Liss, 1983:529-65.
Z. R,)CCO VK, W,1re AJ. C irrh,nic ascire,. Ann Intern ML·d 1986; [05;573-85.
3. Run yon BA. Spon t,mellu, hacterial periwni1.is: An explnsiun of informa1.iLm. I lepatnlogy 1988;8: 171-5.
4. Hr,ef.~ JK. Spontaneous hac1erial pcriLtmttis: Prevent ion anJ therapy.
144
ment of cytokincs and soluble cytokine receptors can help differentiate between asc itcs of different origins; for example, of IL- IP and IL-6 in the asc iLic flu id separated with a diagnost ic accuracy of 98% herween cuhure-pt)Sitivc and culture-negat ive spontaneous bac terial peritonitis (this can be especially important when antibinLic t reatment is interfering with Jiagnosis by bacLerial cultures) (23,27,29,30). AsciLic fluid concentrations of both TNF receptor p5 5 and p 75 differentiated with d iagnostic accuracie· of 94 and 89%, respectively, between patients with malignant or infec ted ascites and patients with uncomplicatcJ hepatic asc ites.
A lthough IL- lp and IL-6 did not separate between uncomplicated hepatic asc ites and malignant asc itcs, and soluhlc TNF receptor concentrations did nnL differ hetween infected and malignant asciLes, the comhination may be helpful. Whereas in infected ascires, IL- l p, IL-6 and both soluble TNF receptors a rc higher than in uncomplicated ascites, in malignant as-
1-lepac,,logy 1990; 12:776-81. 5. Runyon BA, M,1rri,ey RL. Hoefs JC.
Wyle FA. Opsonic net ivity of human ascitic fluid: A potentially important prrnective mechanism flga insl spontaneous bacterial pcritoniLi,. 1-lepatology 1985;5:634-7.
6. Rajkovic IA, Williams R. Abnormalities of neutrophil phagocytosi,, inLracellular killing and metabolic activity in nlcnlwl ic cirrhosb and hepatit is. 1-lepmology I 986;6:252-62.
cites o nly the conccntrnt ion.s of the soluble TNF rcceptnr arc e levated (Figure I ). Although these first result, are very promising, further studies arc required for confirmation. The inclusion of other cytnkinc, and snluble cytokinc receptors in future studies 1m1y detect additional helpful p,irameters for dif ferential diagnosis.
The hacterial culture of asc ite~ flurd remains the gold standard for chc diagnosis of spontanc\lus bacterial peritonitis, bur measuremenL of cytokine, a lso may he helpful when patients have been prcLreated with an t ihio1 ics and tn
study the response to antibi tltic trcarmenL.
The study of cytokincs nnd their soluble receplors wi II lead to a hetrcr understanding of the parhophysiology and paLhogencsis of ascit es. If cyttikinc, play an essenLial role in the pathogenesis of ascites, an understand ing of their actions probably wi II lead tn development of new therapie, using specifil cywkincs or cyrok ine an tagonists ;inJ may he lp assess the prognosis nl paticnls with asc it es.
7. Runyon BA. Patient, with deficient ascitic flu id op,nnic .ic11vny arc predisposed to spontanctiu, bm.:rcrial perilllniti,. Hepatolugy l 988;8:6 32-5 .
8. Runyon BA. Luw-pmtc1n-concen1 ration a,cit ic flu id is predisposed to sponwncnw, hacterial peri ton i Lis. Gaslroemcrology 1986;9 I : I H 3-6.
9. Tito L, R1mola A. G ines r. Lh,ch J, Arroyn V, Rodes A Recurrence nf spontaneow, h,1ctenal pcriwni l i, in cirrhosis: Fre4ucncy and predictive
CAN J GASTROENTEROI V n 1 6 No 3 M AY/JUNE 1992

L1ct,,r,. I le pat, ,l,>g\ 1988;8:27- H. IL\ I lc111m:h Pl', Ca,1cll J\, Andu, T.
l 111c·rleuk 111-6 and the au11c pha,e n,-p, ,n,e. H1ochc111 J I l)lJl\265:621- i6.
11. Andu, T. l\1ucr J. l,emk W. Elkll ,,I cywk m,·, on I he Ii l'l'r I k•p,11, ,log\ 1991;1 H64-75
12. Peter, M, V1erl111g J, (,,·r,hw111 Ml·, l\ltl1d1 D. Clm.in F\'. l lo11ln.1gk JI I. lmmunol,>g\ and dw li,·,·r. I lcpa1,,l11g) 1991;13:977-94.
Ii. Mel 'l,1in l'J, C11hen DA. 1)111,m.•II" CA, Cann,m Jl,. ~hl·,11,,1,k) SI. K,1plan AM. Senim 111terleuk111 I (IL I) atfl\ It\" 111 ,1kohnlic hq,a11tis. Life Su 191'16;N:1479-85.
14. An,1,ra":1k," ( ', Alex.m,kr (,JI\ I, W,,l,tcnnoft RA. ,·t ,11. ln1c·rleuk111 .ind mtcrk·ukm-2 ,Kt l\"11\' m d1r11111c hcpanu, R urus mll'ct1<m G.is, ro,•ntnnlog\ 1988;94:999- 10L1'i.
15. M1nuk UY. L,1Fren1cre R. lnterleukm-1 ,md mtcrlcukm-2 111 chmnic I yp,· R hcp:1t 1u,. G,1,t rnenten ,Ing\ 1988:94- I 094-6.
16. l)l·,·1cr,· J, C,mlent J, Deny, C. ,·1 ,ii. I ligh 1n1crl,•ukin-6 ,erum level, :ind 111lr,·a,cd pmd11L111111 h, kuko,yte, Ill :1 lcnhnlic I I\ er (I rrh, ,,1.,. ( 'nrrela11011 \\'Ith lgA serum le\'cl, and I) mph,,kme, pnxluccion ( ' Im F,p lmmunol l989;77:221 -'i
17. l\,kCla111 ( 'J, Coh,·n DA Tumrn neno,is hK tor m akoholic hcpal II is. G,Nn,e111emlugy 1989:97-1056-7.
lb. Yo,h1nb K, K,1kumu S, Ar.1,, 1\1. T,ut,um1 Y, ln,n1,· M. Tum,>r necn,,1, l,1ct,H u pn 1duc1 tnn h\ pcnpher,tl blood m,,m>11uck·ar t·elb ,,t patients w11h ,hrnntc liv,·r,lisc,is,· I lep.11PI,>)!\ 1989; I 0: 769-n.
19. Mu:e, G. l k1k (,, Lmg L. Gnn::1le:Cahell" R. (,crgl·ly I'. Fl'her J. l),·prc"ed m,>nuc\ll' pn>dlll.:111m ,>I i111,·rleuk111 I and ltltnllr necrrn,is foctnr-alpha 111 p,111e111, 111th aknh,>l1t 11\W c1rrlm,i,. L1wr 1989;9: 302 6.
20. Rird (,LA. ~hernn N. <,,ik.i Al>:J, Ak,.mdcr ( ,J. W1l11am, RS. li1trl',1,,·d pl.i-ma wn1<,r 1wcrn,is t.1unr 111 ,l',·l'rl' abilwlic lwpariu,. Ann Intern Med I 99L\ I I 2 ·9 I 7-2L1
21. FelvlT ME:., Mc:l'\ E, Mc.:( ,u1re M, ,·t al. Pla,m,1 tumor necr,>,1, factor .i pr,·d1ct, dl't rea,cd long/term ,1ir,• I\ .1 I 111 ,,.,.l'rl' :tln>h,iliL h,·pat11 is. Akoh,,li,m. ( ' 1111 hp Re, 1990;77:221-5.
n. Kh,H'llb A, St,1hnkl· L, l\,k( 'Li 1n ( 'J. Logan G, Allen JI. Cirud,11111g tum,,r nc,ro,is fa.tor, 1111nkuk111 I and 1111erleuk1n-6 c011tcn1 r.111011, in d1n1111c ,1ln1h,,l1L p;iricnt,. I lepa1nl<1g\ 1991;13:267-76
Zi. Andu, T, (,rn,, \I, I lobtl'gc A, e1 al. Evidence fpr tlw IPc.1l prnd11cttnn of mtc·rh.~uk 111- l ~. lllt,·rleuk I n-6, interleukin 8 ,md tumnr n,·c:ni-1, t.1,1,n .1111 urrhullL .111,l mali!,!n,m1 ,1'Lllc·,
Cyto kines and soluble cytokine receptors in asc ites
I lepa1nlog\ llJ91;14:97A. (Ah,t) 24 l)l'' 1crc J. C.>n1en1 .f, ))11p1111t E.
lntrnpn11nm·,1l ,ccrct1,m ,if TNFu and IL-6 , ltmng ,p,>1ll,111,·,>11, ha, renal pernun11 "· ( ,,istmcnll'n>logy 1990;98:A '>H2 ( Ah,1)
25. l)e\'lcr,· J, l \intent J, l 'nN,1u, A, I \1prnll E. II -6 ,md TN Fu 111 asut ll il111d durmg 'l'<llll,lllt'<>u, baol'n,11 pern,111111,. 1)1g 1)1, ~LI 1991; '6: 121 4. ( Lw \
26. And11, T. C.,n>" \'. ()11 M. cl ,11. I lnhe lntcrk11k111-6 Knn:1.•ntrnt1<m,•n 1111 mli:11.·rten und n1ch1 1nli:1,·n,·n A,:11,·,. L:n,·n1e Pcntnnu1, h,·1 .1s1·111p1, ,m:111>d1en Pa11cntl'n ! L C,,is1 rncllll'r11l I 991 :28:6S2. (t\b,1)
27. 1\ndu, T, Gn>" V. Wl'hl.'t M. Ott 1\1, Ucr11k W, Schiilm,·mh J. I ligh mtcrleukm-6 k,·el, 111 ,1,L1ll'' wi1h .111,I "nhou1 ,prn11ane,111, 1wnron111,. ( ,,1,1 n >c'nt en 11, >l.!Y I l)\J I ; I L1L) A 714 (Ah,1)
2H. And11, T. (,n1" V, 11,ibtegl' ;\, e1 :d l'rc,cnc,• ofh1gh c,Hlll.'lllra111>11s 111 ,olublc t1111u>r nccrn,is f,Klnr reccp1,>r, (p55 .md p75 m .i,c1tl''· I k·p:11,1l11g1 ( In pre")
21>. /\ndu, T, (Jn>s, V. I h>lst.:ge A, Sch,1lml'n, h J I ligh 1nterk-l1k111-6 n •ncen1 r,111011, 111 hcpatK ,i-ure,. l)ig [)1, Sci. (Len) (In pre.")
k' t\ndu, T, Uni ... , V. I l,1br,·c,· :-\, ,·t .11. lnrcrk·ukm I, llltl'rk11k111-6, 111tcrle11ktn-8 .md tum,ir m·Lr'"'' fa,1,,r n· 111 ,lsc nc,. Lnden,c for IPc.11 pn,,luct1,>n ,>I IL-6 .1n,I nii-,·,I lc·1·1.·l, lll IL-Im an,! IL(, 111 pl.'rn,m111,. Dig [),, Sc1. ( In prl',,)
, I. Prrnllcl' T( ', :Sin W, J,>inl.'r l·E. Quanllt.Hl\'l' ,tud1<'' ,>f ,i-,111t fluid urutl,1111u1 \\'1t h tnt1um-L1h,·led 11':lln.
Am J Mc,I 1952; I 1:M8-n 12 R1rkrnkkl L W. L,·1hm.111 J. L)'l\.k.11.1
MP T<>t,tl cxch,mg,·ahlc ">d111m. to1.tl l'X,h:111gc,1hk pnt,i-,111111, .md t1>1 ,1 l hnd~ 11,Her 111 c,lem.1t11u, palll'llls \\'llh Ltrrhpsi, of 1he 11,·,·r and ,,mgl•,11,·,· hcan t.11lurl' J Clm lme,t 19'i8; l 7:687 -98.
n. (,c1g,·1 T, .\nd11, T, KL,ppr.Hh .I. I lir,mP T. J....1,h1mPt<> T. I k·11mLh l'l '. lndu,t 1,m Pl r,11 ,lCllll' phasc· pnllem, h, mr,·rleuktn 6 111 ,w,>. Eur .I lmmu11Pl l9/-lti,IB:717-21.
H. C.1,tl·ll JV, ( •l'lgcr T, Gru" \/, c1 ;11. l'la,m.1..:lcar,111e,•, ,1rgan d1,1nhut1Pn ,tnd target cl·ll, nf intl'rlcukm-6/ hcpat,>c yte ,11mul.1t1ng f,1, 1,1r 111 the r.n. Fur J R1udwm 198o;l77 157-61
i5 Erro1 A, Sirnn1 M, l 'h1.11fonnu r. l 'hen /(,, l\kngn::1 l\l, l\.l,1111,>,,1111 A. 11 I ,md IL 6 r,·ka,e hy 1umur-;is."1c1,lll'd macrophage·, (n,m hum,111 n,·erian ,,1r, 111,1111.1 Int J C.m,cr 1989;44: 79'i KO I.
16 Remick LX,. :S1ree1,'I' R;,-..1. F,kand,m MK, ,·1 .11. R,>le ,it t111111>r lll'Ll'<Ns
fallPr•,llph.1111 lipPp<>h ,,llth,m,k mdu,ed pa1hul,>g1t ,tl1,•1.1t1rn1>. .\m I l'at h,11 I 1NO: I 16:49-6t1
i7. I I.in l'H, l no1x·r RL. hnl.,, jPn,·, II II 4 ,uppr1.·"c' II -I h,·t,1, TNf .dpha .ind l'<.,l:2 prod11tt11m h h11m:111 pento1w.1l 111,1, 1, ,ph.ig,·,. I 1111111111, ,!, >gv 1991:72-144-9
"18. U,>ngJI I. Ren- I I, ,11111'1, l,un,.1 l), lnrerlcukm I ,1, ,1 llltlll>r c~111,t,111, mcd1,1tnr rclea,ed ln,m llllllPlll ,1,,11,·, . l rc.ncd m.icmph.,l.!c,. I mmunnh1<>IPg\ 1988: 177: nlJ-51.
W. Northnff l I. And11, T, 1 r.m 1 h1 T-A. ct al. Tlw 111fl .1mmat1<>11 llll'd1.11or, intcrleuk1n-l and hep,IIP<'\'l<' ,t 11nul,n 111g f.Ktor ,ire d1th.:rcnd) rl'gltlatcd 111 human monncytl''· Eur J lmmunol 1987;17:707 11.
40. Taran K, "o K, l\h,mt T, u ,,1. l )c1ec11,,n o( ,·ndntnxm 111 pl:1,ma ,md ,hLlllL fl1 11d of p,H1ent, 111th (lrrhn,1,: 11sclm1,.tl ,1gn1IK.mLe. ( o,ht r11l'llll-'Wl11g~ 1977;7 I :5 39-42.
41 Pryr: J, I l,11,r-Chn,rl'n'l'tl J, 1'Pmer I). l'Pn.11 n:n11u, ,md ,y,tl'tn1c ,·nd,Hnx,·mta m p,ll tl'nt, I\ tth1>lll ll\·c1 d1,ca,c .ind ,y,1cm1c l'ndntox,·mi.1 111 p.111cn1, with li,·l'r cirrhn,1s. ~c.md .J
G1,1nll.'ntewl 1976: l I :H57-6 3 42. I 11mb,en, AR, I lend,·rs1m M, Kurne,
1\111 EndPt,,xin le1·cl, mea,url·d by ,l 1. hn >mogl'lllL ,1",t\ 111 porwl, hep.me ,tnd peripheral \'l•now, hl,1od in p.111cnt, ,1 II h LI fth, ""· I lepatology I 98H;h 2 "\2 6.
4 l l )l,>i"Hl l). NyL111dcr ( ,, l)ls,on I'. Fnd,>tmrn1 R11utl'' uf tr,m,pori 111 ,·xpemm•111:1l pentun1t 1, Am J ~urg I 9H6; I 51 ·44 3 6
44. D,11111.·le R. "mgh 11, Appert l IF, l'a1rcen1 rW, I hl\\ar JM. Lymph,n ic ,lh" 1rpt 11111 <lf tnll ,lrCrtlllllL';\' ,·nd111,,,1111111he ,11,g. '-,111'):l'r\ 1970;6 7 484-7
4'i. R11nynn HA, 'x1111er L,LJ Tran,lncat1<>n ,,I gur h.1u,·n;1 <1I L1ffl1,H1L r,its 1,> nw,cntcril hmph np,k, m,11 p;irtta lh t·,plain thl' p,ll)lll[.!l.'11L''I' ,if 'l'<'llL11wnu, h:iLlenal pl'rll<Hlll1.,. I k·p.11nh,g1 199 1;14:91A. (Ah,i)
46. H.1g[.!1ol1111 1\1, W.11: A, Kunkd SL. Ncutrnphtl-nu I v,11111!.! pl·pt ,de- I/ 1111erll'uk111-~ .. 1 nnvcl L\lnl..inl.' that ,1(11, a,,., m·11troph11'. J ( ·1 111 lnl'cst I 98l):H+ I 045-9
47. P1n,1rcllo(A lntcrleukm-1 :m,I 1n1vrlcukm-l ;1nragon1sm. HlnPd 1977:1627 52.
4t-. Ja,i11el.11\1 R1olPg) of ,lt,c,hl'. R11>lng1c ,1L111•1tic, and meLhan1,m, nf ,1<1 1,m ,>I tum,ir lll'Lr<"I' f.Kt,1r-,1/L 1chcL1111. L.1h lme,t 1991;64:724-42.
49. '\,k·rb I), Ll' J, V1k,•k J IL-6 1nh1h11, l1p, 11'<>l\',.t(ch,tr1dl.'·llldun·,l 111111, >r necmsi, faLtnr pr,,durt1<1111n u1ltun:d human m,111<>c\lc,. U9H cells. .md 111 1111t,·. I lmmun111198lJ; 14):1517-21.
145

50. Schindler R, t,..,\ancill.1 J, End re', S, l,hmh,1111 R, Clnrk SC. D111,irelll1 CA. Corn.:lat1nn, and illlc'rnct1<m, in thl' rroductil1n lll 111ll:rlcukin-6 (lL-6), IL- I., ,ind tunll1r nl'cni,b factor (TNF) 111 human n111nnn11ckar cell,: I L-6 ,upprL'sse, IL-I and TNF. Blllnd l 990;i5:40-7.
51. l,u,1rner F, Wall.i..:e JL, M,1cNaughtlll1 WK. lhhotsP11 l;c, Arr()yo V, Rnde,J. Endn1ox111-inclucecl .i,cites f,mn,111,m 111 tlw rat: P.iri ial medial ion hy pLnekc-:1ct1\',1t 111g I act, ,r. I le pat, ,I, ,g\ I 989;5:788-94.
'i2. Kilhnurn RlJ. C,mss SS, Juhr:111 A, ct al. NG-methyl-I -argmmc mhihit, tum"ur nccrnsi, lac1nr-111duced hyporemi,1n: Implication, fl,r the 1n\'l1lvement nf n1tnc mmle. Prnc Nari A..:,1d Sli USA J 990;87: 3629-12.
5 >. Kilbourn Rl\ Bcll"ni I'. EndPthdinl u:11 produClllln ol 1111 rogcn ,1xidc', 111 re,pnn,e ru in terfr:n 111 gamma 111
comhmarinn with tumor 11l'cros1, foct,,r, interleuk111- l, pr endntoxin. J Nari Cancer ln,t 1990;82:772-6.
54 Kube, I'. Su:uk1 M, Grnngc'r DN . M,,dulai 1011 ol PAF-induced leukllcyte adherence an,I tnCrl',i,,c,l micrnva,cular permcnhilll\ . Am J Phy~il,I 1990;2 59:l,859-64.
55. Alhc'rti A, Chcmellu L, Fmwvich Ci, c't al. Scrum lc\'d, nf soluhle mterkukm-2 receptor, in acute and
146
chronic viral hcpatiti:,. Dig [)i,, Sci l 989; H: I 5 59-63.
56. Rubin LA, Ncbon DL. The soluble mtcrleukin-2 receptor: Biulogy, lunc1 ion. and di111cal application. ,<\ nn Intern Med 1990;113:619-27.
57. L,,hP-YcP A. Micli-Vergnni G, Mowat Al', Vcrgan1 D. S,,luhle interleukin-2 rc•ceptnr, in .n1to1mmune chronic ,icLi\'e hepa1 itb. Gut L 990; 31 :690-3.
58. A,lam, l)H, Wang L, 1 lubscher SC, Eli,1' E, Neuberger JM. Soluble mrerleukm-2 reccpwrs in ~erum and hile ,,I liver trnn,plam recipient,. Lancet I989;i:469-7 1.
59. N11vick l), Engelmann I l, Wnllach D, Ruh111,tc111 M. Snluble cytnkinc re.::eptnrs arc present 111 normal human unne. J Exp Med 1989; 170: 1404-9.
60. G,.,,d\\'111 Rl,, Friend D, Ziegler SF, ct ;11. C lnning d the human ,111d munne tnterlcukin-7 reccpwrs: Dcm\instniu,111 nf ,1 s,1luhlc form and h11111nln1sy t,, .1 ne11 rcccpH1r sup,·rf.imily. Cell 1990;60:94 l -5 I.
61. Seckmgcr P, Willmm,on K, Ralavn1nc Jr, Cl nl. A urine tnhihitnr llf 1111erlcuk111 I acunry effects both interleukin la :md Ip hut 1wt tumour necrosis facwr Cc'. J lmmunol 198i;lN:1541 -5.
62. Seckmger I', Lowenthal JW, Willi.11mnn K, Dayer J-M, Shnll' AR, Schmei,sncr U.
A unnc 1nhibit11r ,,I 111Ll'rlcuk1n I acuvity 1hat hl"cb lig,md hmding. J lmmun11l 1987; I 39: 1546-9
61. ()!,,son I, Lani: M. N1ls,nn E, c't ,11. l,l1h1tion and ch,1rnctcn:at1<m ,1f.1 tumor nccrn,i, f.ic ror hinding protein Imm unnc. Eur J I l.1cm,11,1l L 989;42:270-5.
64. Seckinger I', baa: S, l\1yer 1-M. Purificatiun and h1L1l,ig1c charnclen:al1un of a spcufic tumor nccni,,is lactm ,1 inhih11or. I R1,1l CIK·m 1989;265: t t 966-n
65. Engelmann H, N,wick l), Wall,1ch l\ Two turnur nelrt1'1s fac tor-hin,ling protcm, purified Imm human uri11l'. J Biol Chem J 990;26'i: I 511-6.
66. Gntanagn T, Lent: R, tvhrn,unub l. c:t ,ii. ldt:nt ific.m,u1 "I TNF-L T hlocking lacwr(,) 111 ,erum an,I ultrnfiltrate, ol hum,m cancer par1L'nt, Lymphnkinl' Res I 990;9:225-9.
67. Ad11 lfGR, Apllcr I. A mrn1<Klona l .inribc1dy-basl'd cn:ym<.: 1mm,mn,iss.1y (orquanut,Hi,m ,1fhum,111 turn,,r necm~1s fac t11r h111d1ng prorcm I, a soluble frngmcn1 nl lhl' 60 kl)n TNF rcccpt\1r. J lmmunnl ~kth 1991;143: 127-36.
67. Fernandc:-8n1ran R, V1teua I::.. A soluhlc, high affinity, 1n1l'rleuk111-4-hinding protein 1, present in thc hi,1l<>g1cal fluid, ,if m1c,'. l'rnc N,nl Acad Sci 1990:87:4202-6.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com