Embed Size (px)
Citation preview
Sports and Skin
Michelle Wanna, MD
Avera Medical Group Dermatology
3rd Annual Avera Sports Medicine Symposium
June 10, 2016

Objectives
• Review skin infections that can impact sports participation
• Review common skin diseases seen in athletes
• Discuss patterns suspicious for contact dermatitis and
potential triggers
• Review acne mechanica, Isotretinoin-related sports issues,
and the impact of supplements on acne
• Recognize cholinergic urticaria
• Understand the Koebner phenomenon

Skin Infections
• Folliculitis
• Furuncles
• Impetigo
• Bullous Impetigo
• Tinea
• Herpes simplex
• Molluscum Contagiosum

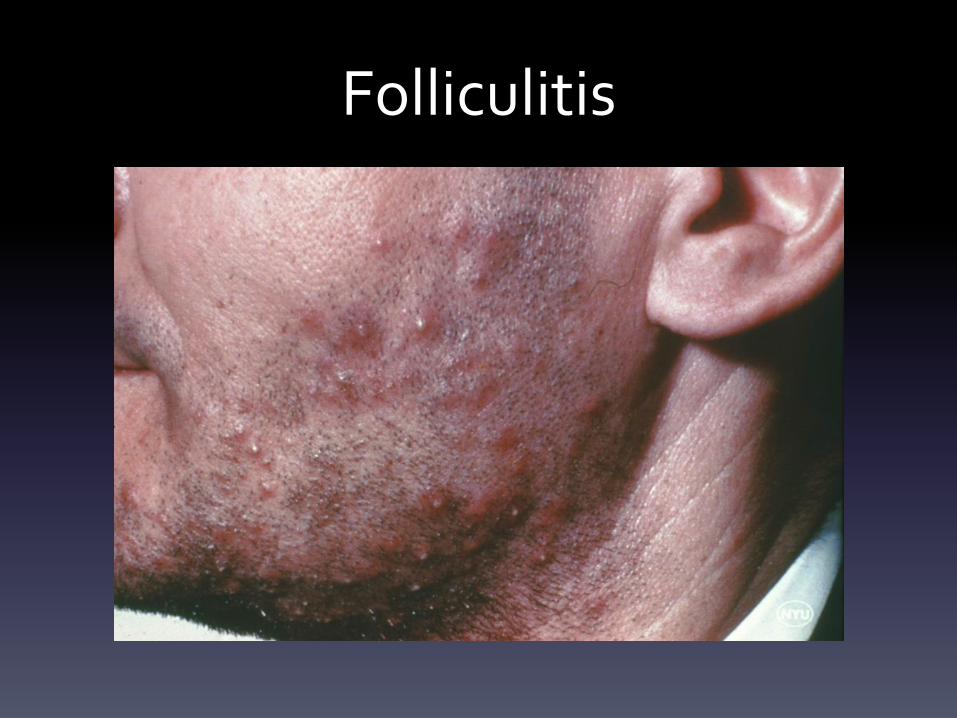
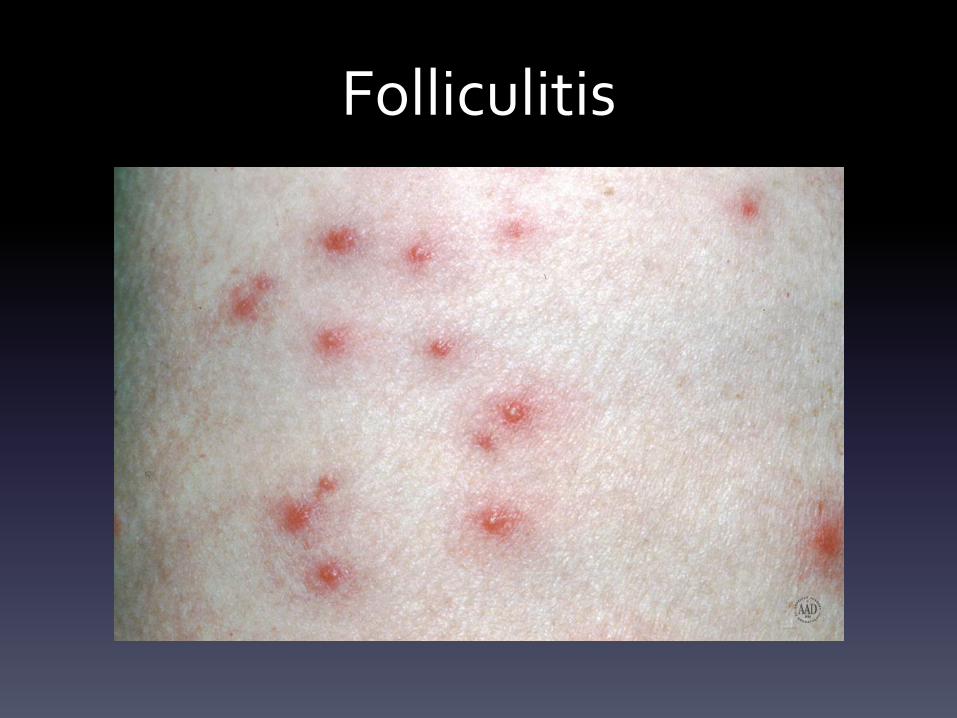
Folliculitis
• Infection of the hair follicle
• S. aureus most common infectious cause
• Risk factors include maceration, occlusion, hair removal,
environmental factors
• Superficial forms can be treated with antibacterial washes while
more extensive involvement may require oral antibiotics
• Mupirocin oint BID nares/genital area x 5 days, antibacterial
washes, dilute sodium hypochlorite baths, and cleaning of fomites
may be needed for recurrent cases

Folliculitis
Folliculitis
Folliculitis
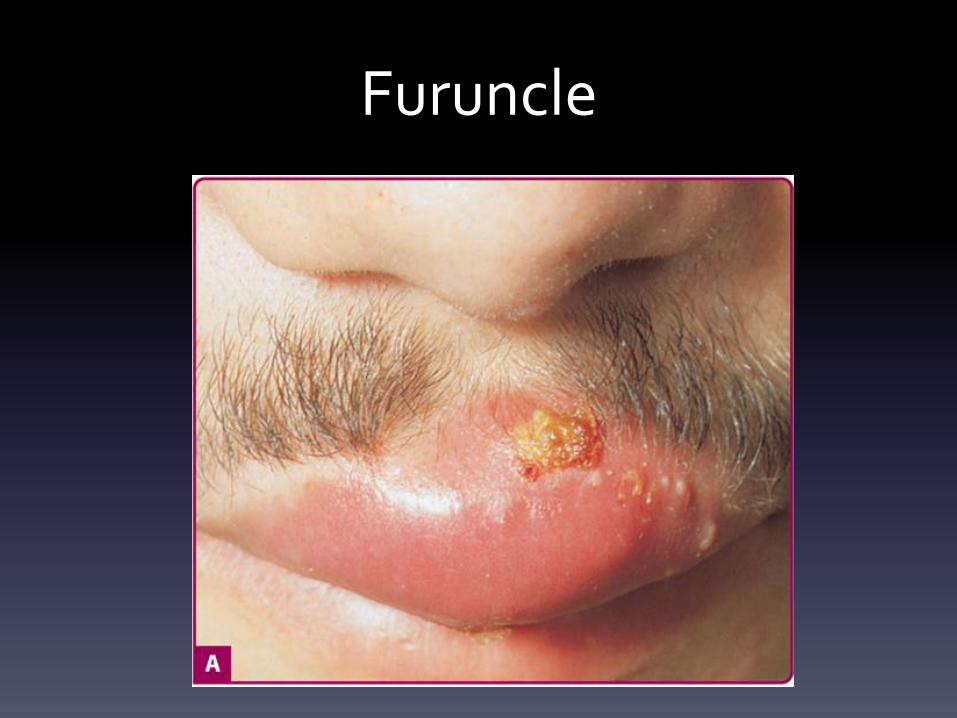
Furuncles
• Follicle based abscesses, typically caused by S.
aureus
• Frictional areas and hair-bearing regions of face,
neck, axillae, buttocks, thighs, and perineum
most common
• Painful, erythematous nodule that eventually
becomes fluctuant
Furuncles
• Treatments include:
– Warm compresses
– Incision and drainage
– Oral antibiotic therapy for high risk areas (face,
hands, genitalia), multiple lesions, associated
cellulitis, immunosuppressed, concern for MRSA
Furuncle
Impetigo
• Erythematous macule that develops fragile pustule with
associated “honey-colored” crust
• Occurs in an area of skin disruption
• S. aureus and group A beta-hemolytic Strep (Streptococcus
pyogenes)
• Contact sports is a risk factor
• 5% rate of post-streptococcal glomerulonephritis in S.
pyogenes cases

Impetigo

Bullous Impetigo
• Caused by exfoliative toxins (ETA, ETB) by S. aureus phage
group II
– Same toxins seen systemically in staphylococcal scalded skin
syndrome (SSSS)
• Small vesicles develop into large bullae which rupture
easily and leave characteristic collarette of scale
• Can occur on intact skin
• S. aureus can be cultured from vesicle/bulla fluid

Bullous Impetigo

Bullous Impetigo

Staphylococcal Scalded Skin Syndrome

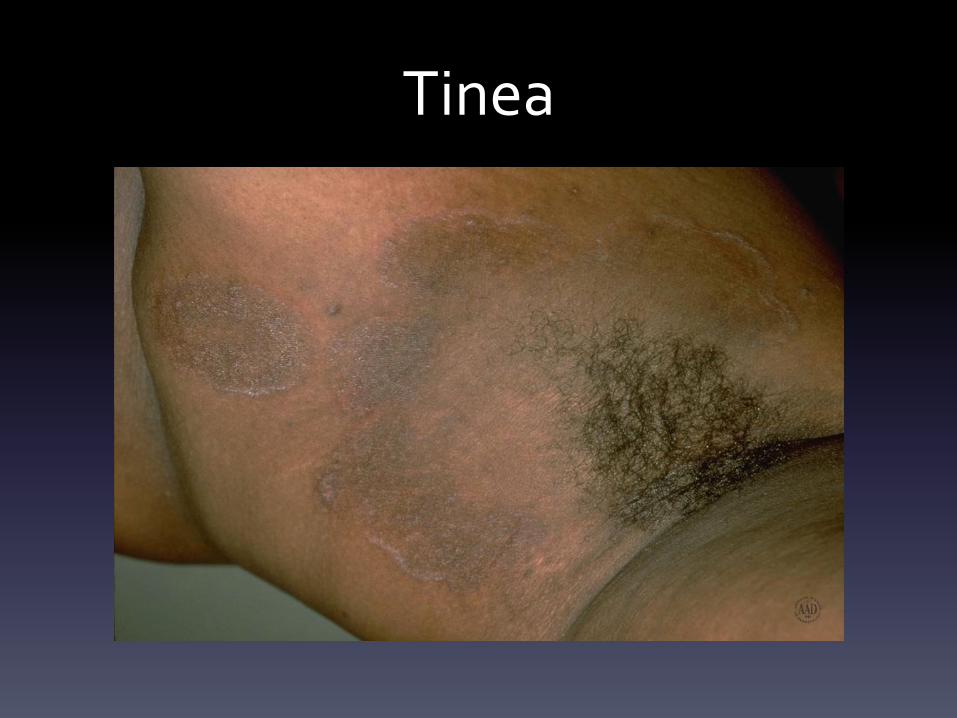
Tinea • Typically caused by Trichophyton, Microsporum, and
Epidermophyton species
• Clinical findings:
– Annular, erythematous scaly plaques trunk and extremities (tinea
corporis)
– Erythema of inguinal fold with scaling, advancing border (tinea cruris)
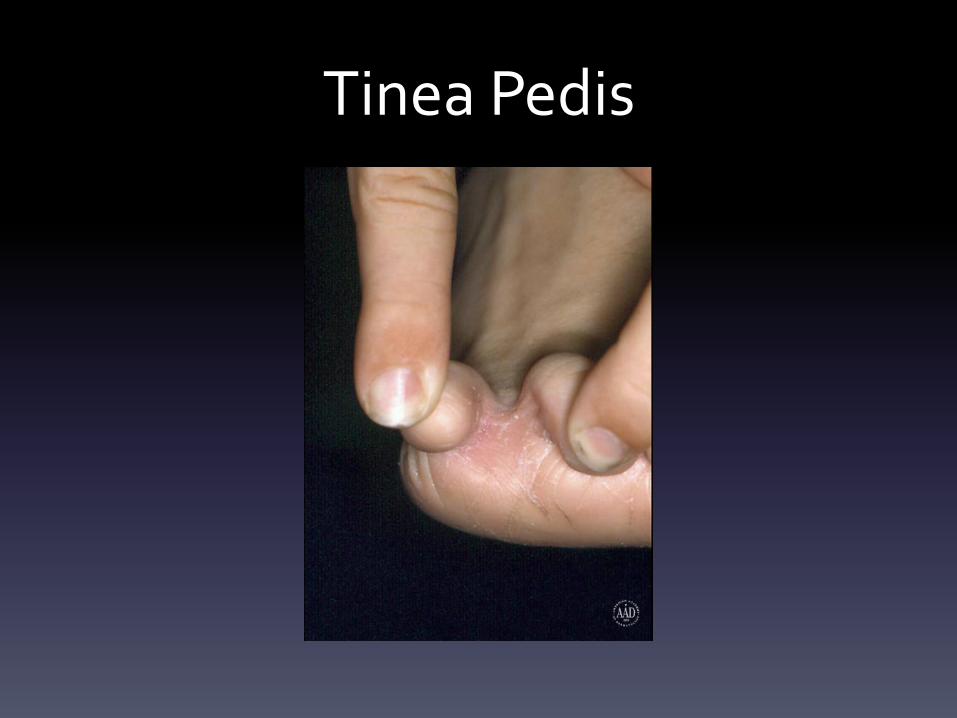
– Maceration and scaling in webspaces and surrounding areas (tinea
pedis)
– Erythema, scaling, and alopecia (tinea capitis)

Tinea Corporis/Capitis

Tinea Capitis

Tinea Capitis

Tinea Corporis

Tinea Corporis

Tinea Corporis
Tinea

Tinea Cruris
Tinea Pedis
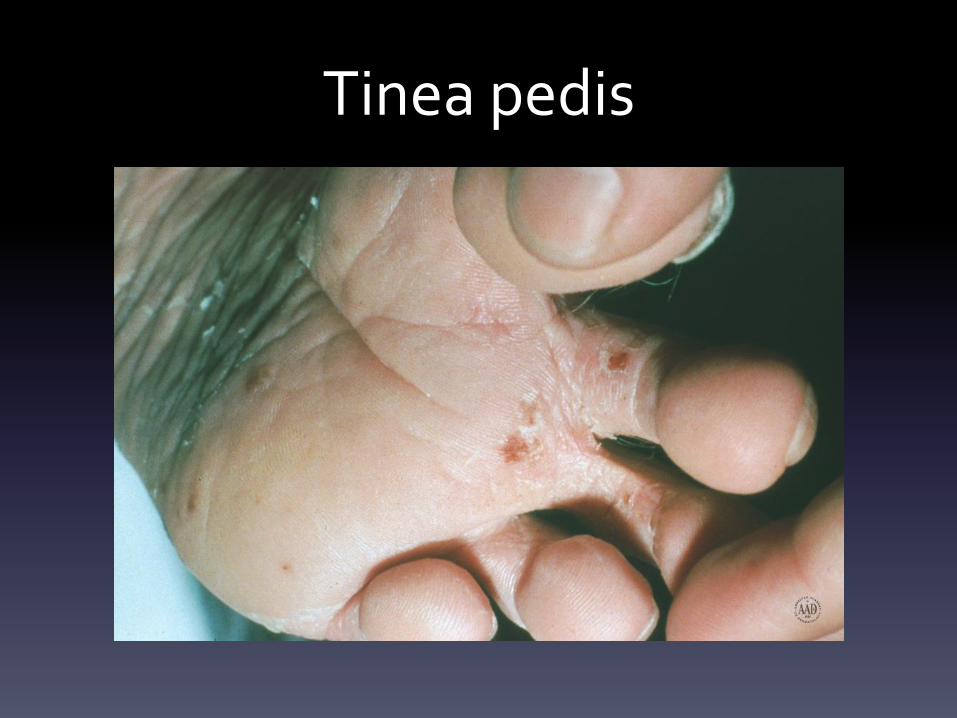
Tinea pedis

Tinea Pedis

KOH

Majocchi’s Granulomas

Majocchi’s Granulomas

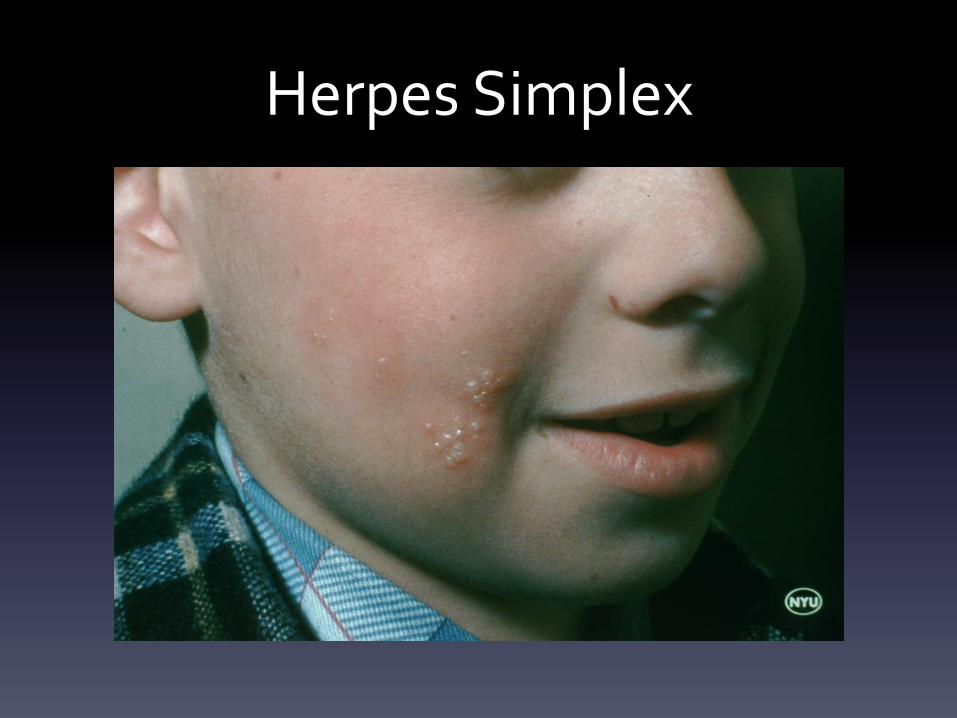
Herpes Simplex
• Herpes gladiatorum is typically HSV-1
• Grouped vesicles on erythematous base
• Spread by contact with saliva or vesicle fluid
• Occurs within 3-7 days of exposure
• Initial outbreaks can also have lymphadenopathy, malaise, fever as
prodrome prior to onset
• Lesions are painful, pruritic, or burning
• Subsequent recurrences are not typically as severe as initial
Herpes Simplex

Herpes Simplex

Herpes Simplex

Herpes Gladiatorum
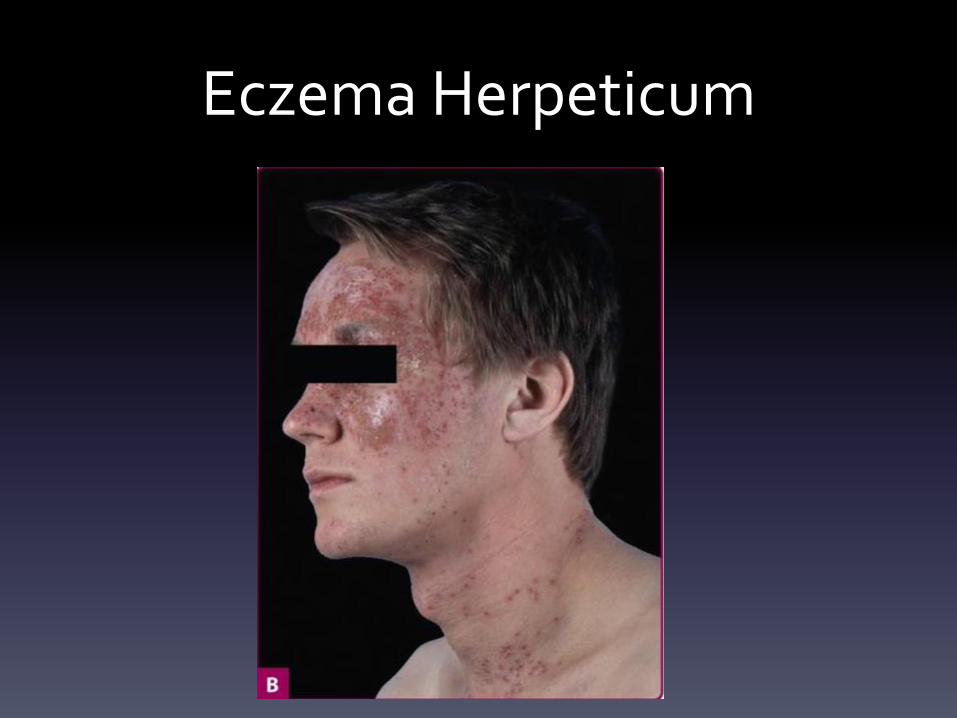
Eczema Herpeticum
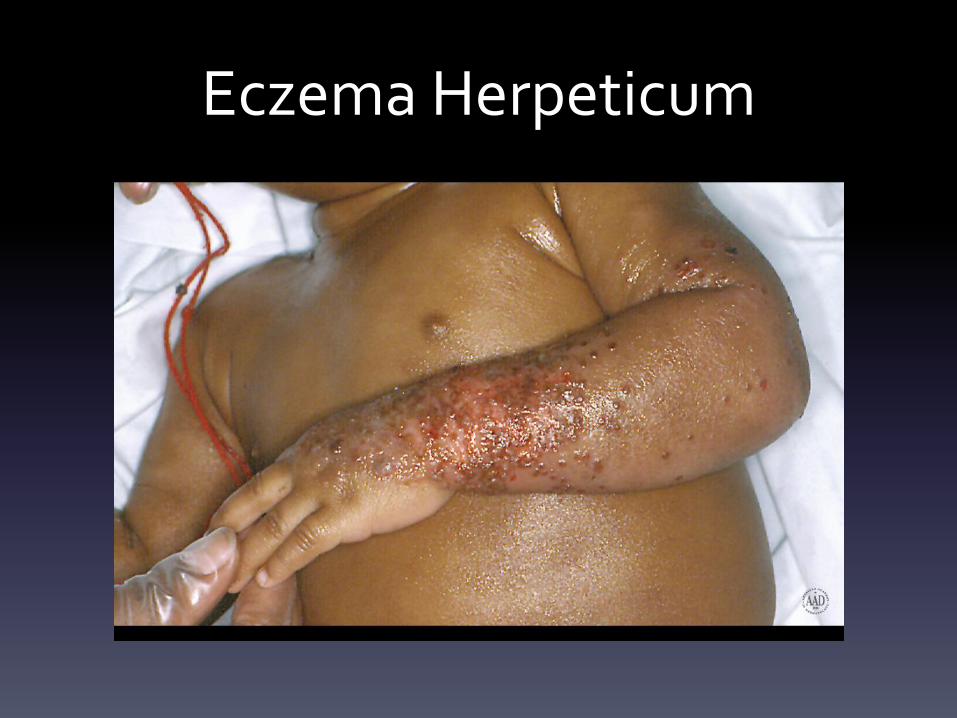
Eczema Herpeticum

Molluscum Contagiosum
• Flesh-colored umbilicated papules 2-8 mm in size
• Koebner phenomenon can be seen
• May resolve spontaneously
• Can be associated with molluscum dermatitis
• Treatments include topical cantharidin (compounded),
imiquimod (off-label use), topical retinoids (off-label
use), curettage, cryotherapy

Molluscum

Molluscum

Molluscum
Skin Diseases and Clinical Findings in Athletes
• Tinea Versicolor
• Pitted Keratolysis
• Contact Dermatitis
• Cholinergic Urticaria
• Striae
• Miliaria

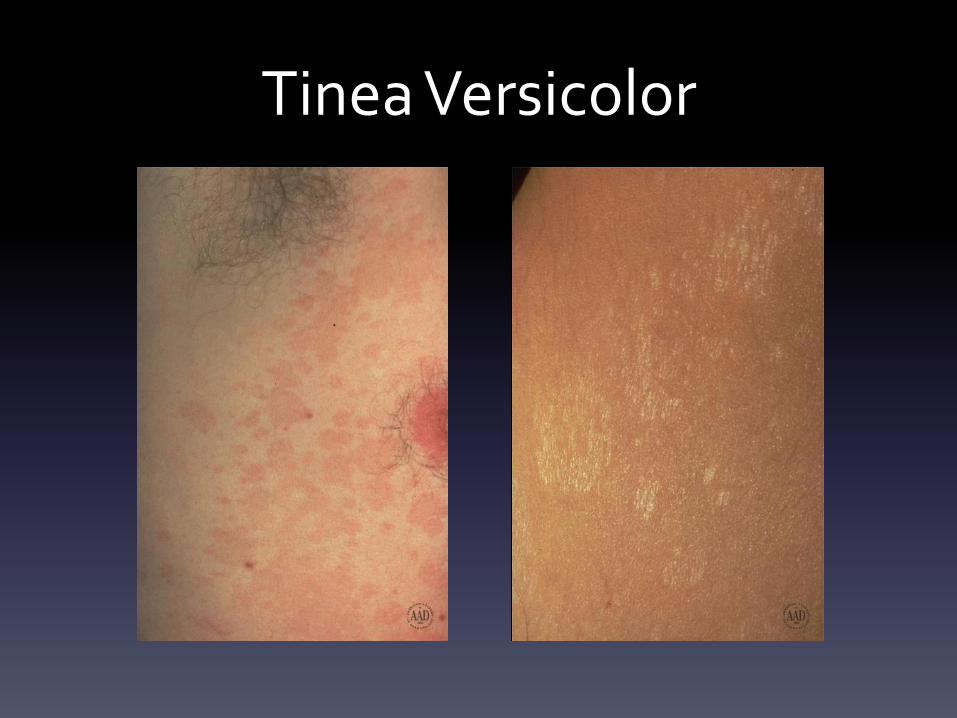
Tinea Versicolor
• Presents in adolescence
• Scaly, oval macules, thin plaques, and patches either
hyper or hypopigmented
• Yeast forms of Malassezia furfur
• Characteristic KOH findings
• Exacerbated by sweating and hot, humid
environmental conditions

Tinea Versicolor

Tinea Versicolor
Tinea Versicolor

Tinea Versicolor

KOH
Pitted Keratolysis
• 1-7 mm pits or depressions within the stratum corneum
• Associated with hyperhidrosis and malodor
• Causes include Micrococcus sedentarius and
Corynebacterium
• Treated with topical antibiotics including erythromycin,
clindamycin and aluminum chloride for hyperhidrosis

Pitted Keratolysis www.dermquest.com/image/028993H

Allergic Contact Dermatitis
• Delayed-type hypersensitivity reaction
• Occurs after exposure to a previously sensitized chemical
• Acute cases can be vesicular
• Chronic exposures tend to be lichenified, scaly
erythematous plaques
• Correspond to the area of contact with the inciting
chemical
• Patch testing is the gold standard for diagnosis

Shoe Allergic Contact Dermatitis

Shoe Allergic Contact Dermatitis

Cholinergic Urticaria
• Small 1-3 mm urticarial papules or wheals with
erythematous flare
• Occur predominantly trunk
• Persist for 30 minutes to hours, with 24 hour refractory
period
• Can be associated with systemic symptoms
• Triggered by acetylcholine action on the mast cell
• Seen in exercise, increased temperatures, stress

Cholinergic Urticaria

Striae
• Linear atrophic lesions from dermal damage
related to excessive stretching of the skin
– Seen in significant weight fluctuations,
pregnancy, puberty (30%), strength training
– Iatrogenic: topical steroid use
– Cushing’s

Striae
Miliaria
• Obstruction of the eccrine sweat duct by keratin plugs
• Results in sweat retention within the skin
• Clinical findings are based on level of obstruction
– Miliaria crystallina
• Stratum corneum – clear vesicles, easily ruptured
– Miliaria rubra (most common)
• Mid epidermis – erythematous papules, macules, vesicles, pustules
– Miliaria profunda
• Dermal-epidermal junction – 1-3mm white papules
• Occurs in settings of significant sweating and occlusion
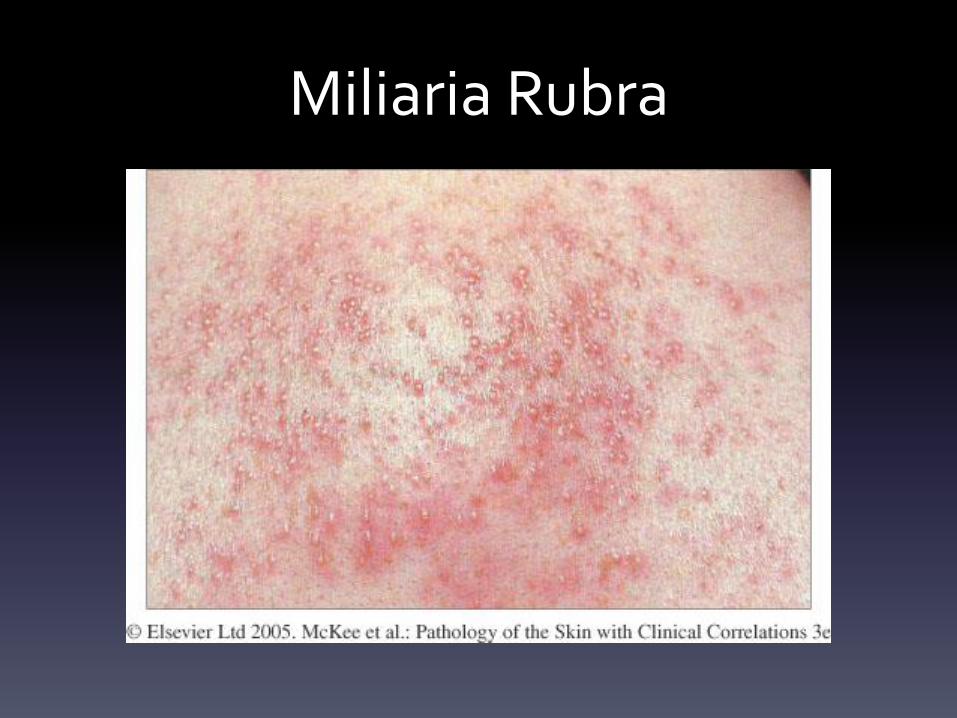
Miliaria Rubra

Acne and Sports Participation
• Acne Mechanica
• Isotretinoin Use and Sports
• Acne and Supplements

Acne Mechanica
• Triggered by:
– Occlusion
– Friction
– Moisture
– Heat
– Pressure
• Treatments include:
– Avoidance
– Removal of offending garments, helmets, pads, etc. and skin cleansing as
soon as possible after physical activity
– Traditional acne treatments
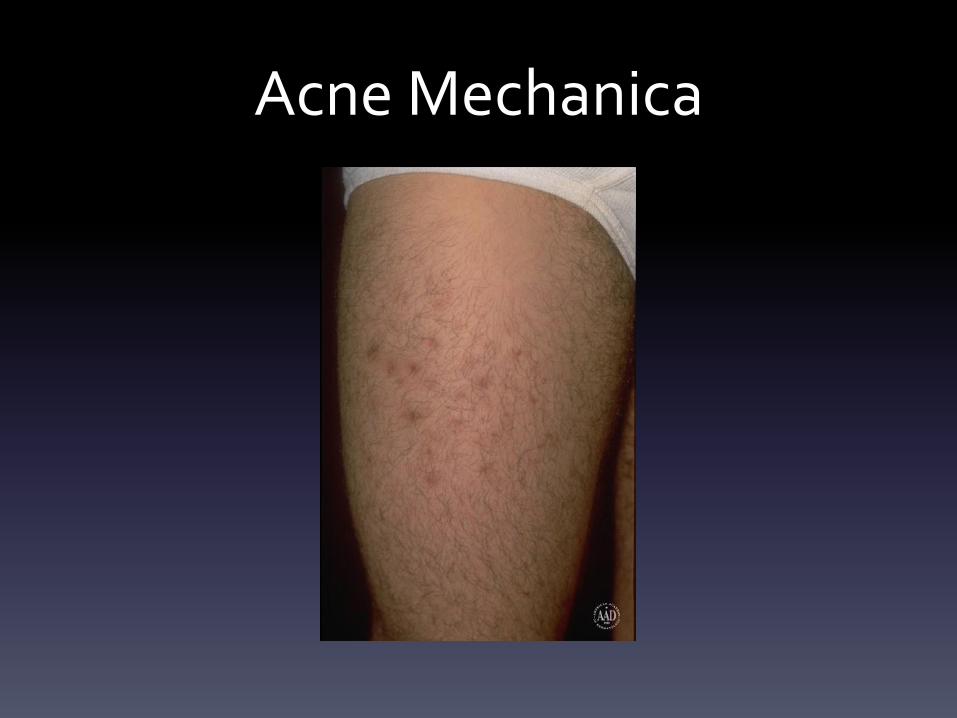
Acne Mechanica

Acne

Acne

Acne

Acne
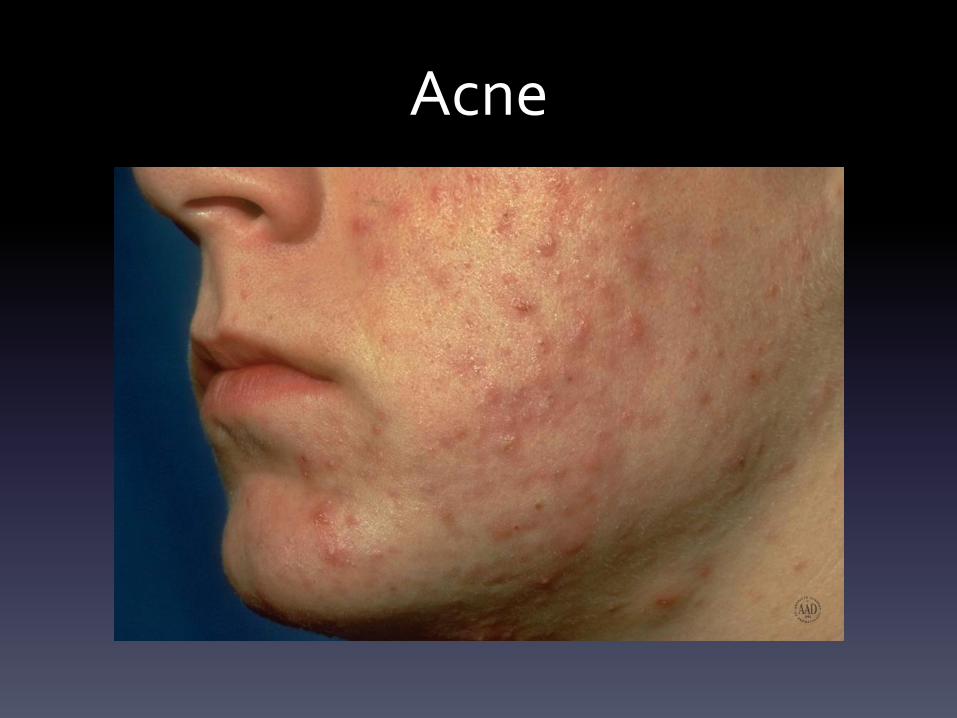
Acne
Isotretinoin and Athletes
• Increased fragility of the skin with erosions
– Increased risk of secondary infections with non-intact skin
• Tendonitis
• Myalgias in 15%
• Diffuse interstitial skeletal hyperostosis, premature epiphyseal
closure, osteophyte formation, decreased bone density
– Dose and duration dependent
– Not found in typical isotretinoin course of acne treatment
• Photosensitivity

Supplements, Diet, and Acne
• Anabolic steroid-induced acne
• Review of studies implicating whey protein, milk
consumption, and glycemic index with acne
– American Academy of Dermatology (AAD) Guidelines
of Care in the Management of Acne 2/2016

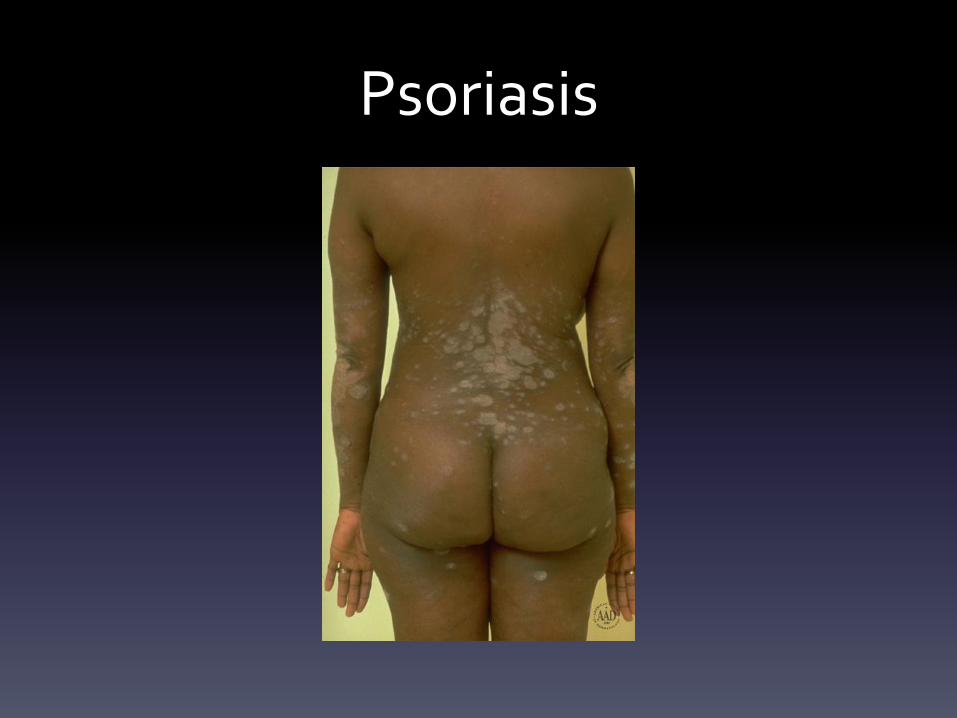
Koebner Phenomenon
• Occurrence of particular skin diseases in areas
of trauma
• Common skin diseases include psoriasis,
vitiligo, molluscum contagiosum

Psoriasis

Psoriasis
Psoriasis

Psoriasis

Psoriasis

Vitiligo

Vitiligo

References
• National Library of Dermatologic Teaching Slides (NLDTS) 4.0, American Academy of Dermatology
• Paller, A., Mancini, A. (2011). Hurwitz Clinical Pediatric Dermatology. (4th ed.). Elsevier Saunders.
• Bolognia, J., Jorizzo, J. Schaffer, J. (2012). Dermatology. (3rd ed.). Elsevier Saunders.
• James, W., Berger, T., Elston, D. (2011). Andrews’ Diseases of the Skin Clinical Dermatology. (11th ed.).
Elsevier Saunders.
• Calonje, E., Brenn, T., Lazar, A. McKee, P. (2012). McKee’s Pathology of the Skin with Clinical Correlations.
(4th ed.). Elsevier Saunders.
• Wolverton, S. (2012 ). Comprehensive Dermatologic Drug Therapy. ( 3rd ed.). Elsevier Saunders.
• Goldsmith, L., Katz, S., Gilchrest, B., Paller, A., Leffell, D., Wolff, K. (Eds.). (2012). Fitzpatrick’s
Dermatology in General Medicine. (8th ed.). McGraw-Hill.
References
• Zaenglein AL, Pathy AL, Schlosser BJ, Alikhan A, Baldwin HE, Berson DS, et al. Guidelines of care for the
management of acne vulgaris. J Am Acad Dermatol. 2016 Feb 15.
• LaRosa CL, Quach KA, Koons K, Kunselman AR, Zhu J, Thiboutot DM, Zaenglein AL. Consumption of dairy
in teenagers with and without acne. J Am Acad Dermatol. 2016 May 27. [Epub ahead of print]
• Adebamowo CA, Spiegelman D, Berkey CS, Danby FW, Rockett HH, Colditz GA, Willett WC, Holmes MD.
Milk consumption and acne in teenaged boys. J Am Acad Dermatol. 2008 May;58(5):787-93.
• Adebamowo CA, Spiegelman D, Danby FW, Frazier AL, Willett WC, Holmes MD. High school dietary dairy
intake and teenaged acne. J Am Acad Dermatol. 2005 Feb;52(2):207-14.
• Silverberg NB. Whey protein precipitating moderate to severe acne flares in 5 teenaged athletes. Cutis.
2012 Aug;90(2):70-2.
• Simonart T. Acne and whey protein supplementation among bodybuilders. Dermatology.
2012;225(3):256-8.

















![Use of a Movement System Impairment Diagnosis for Physical ... · PDF filesports physical therapy [] ().,†‡ 37 §?? ¶](https://img.pdfslide.net/doc/110x75/5a79461a7f8b9ae93a8c8c59/use-of-a-movement-system-impairment-diagnosis-for-physical-physical-therapy.jpg)