Embed Size (px)
Citation preview
Respiratory Therapy Society of Ontario Tel: (905) 567-0020 1-800-267-2687 Fax: (905) 567-7191 6519B Mississauga Rd, Mississauga, ON L5N 1A6 E-Mail: [email protected] Web: www.rtso.org
AIRWavesA publication of the Respiratory Therapy Society of Ontario
Spring 2008Volume 17 Number 2
As we all welcome in spring, the RTSO is already thinking ahead to the fall. In this edition of Airwaves, we are excited to provide you a preview of the RTSO Fall Education Forum to be held in Niagara Falls. Be sure to consider this coming October 2nd and 3rd as a great time for a little get-away and an excel-lent educational opportunity.
Also in this newsletter, we’ve continued our efforts to provide a venue for our members to voice their experiences and perspectives. You’ll hear from an RT in London with his reflections on train-
ing as an Anesthesia Assistant. As well, a student RT offers us his perspective regarding the health care realities he experienced in Nepal. Such articles help us appreciate the diversity in practice and experience within our profes-sion. We encourage you to continue to contact us with your stories and ideas. Sharing knowledge and experiences is important and we’ll help you do it!
Finally, get your cameras ready for this year’s RTSO/CRTO Photo Contest. Big competition and big money (enough for a few coffees, anyway) - place your
team front and centre during RT Week with your picture on our posters! Read on for more details.
I hope you enjoy this edition of Air-waves. We appreciate your membership and the opportunity to bring you this communication.
Best regards,
Patrick Nellis B.Sc, RRTPresident, RTSO
President’s Message
The RTSO is pleased to be able to provide three different awards for members. These awards highlight dedi-cation and achievement by members. Please review the criteria and nomina-tion forms on our website and consider someone you know for one of these awards. All entries are due September 1st, 2008.
STUDENT ACHIEVEMENT AWARDThe Respiratory Therapy Society of Ontario (RTSO) Student Achievement
Award is given each year to a graduat-ing student from each of the accredited programs in Respiratory Therapy in the Province of Ontario who has demon-strated outstanding professionalism during their clinical training.
THE PINNACLE AWARDThe Pinnacle Award is a premium award, awarded only to a Respiratory Therapist in Ontario who has con-tributed to the profession in a unique manner.
THE GORD HYLAND MEMORIAL LEADERSHIP AWARDThis award was established to recognize Gord Hyland and all of his contributions to the profession of Respiratory Ther-apy. The candidate should be chosen for their great leadership skills, and should exemplify many of the characteristics we saw in Gord.
RTSO Awards Submissions September 1 Deadline
Working Together, Working Smarter! Interprofessional Practice at St. Joseph’s Health Centre Jeff Dione, St. Joseph’s Health Centre
Interprofessional Practice (IPP) is the way of the future in delivering patient-centred care. At St. Joseph’s Health Centre in Toronto we strive to make Interprofessional Practice both inten-tional and collaborative. It is impor-tant to learn with, from and about one another to increase team capacities. The end result is an improvement in patient health outcomes.
Our journey began in January 2007 when we formed an IPP team com-prised of a small group of health care providers from a variety of professions, including respiratory therapy. Our first project took a snapshot of the lived experiences of IPP within the Health Centre. With the use of a variety of tools including survey, focus groups and direct observation, the following key findings emerged:
1) IPP should not be rigidly imple-mented, but rather be based on common prin-ciples which allow for variability of focus and culture in different areas of the Health Centre
2) When not all team members (i.e. house-keeping, chaplaincy, family) are present, the team is impacted
3) Space and time may not always be optimal for collabora-tion.
Our team wanted to further explore how IPP could continue to evolve within our institution. In the next project we con-ducted six-hour workshops with Point of Care Teams focusing on providing
instruction in IPP. Six Point of Care Teams within the Health Centre were randomly selected to participate in the project. Three teams were selected to receive coaching sessions while the other three teams facilitated their work-shops through the assistance of a self-directed learning manual. The project concluded that the impact of coaching was greater for teams than self-directed learning.
The content of these workshops centred around six core competencies that were identified through the first IPP project:
1) Willingness to Collaborate2) Trust Amongst Team Members3) Knowledge of Roles4) Communication5) Conflict Resolution6) Shared Decision Making
The self-directed teams received
consultation throughout the workshops facilitating each team in developing a common vision and planning how to achieve this vision. It has been shown that when team members have a per-sonal contribution to the development of the vision, they have a more vested interest towards its realization. Team
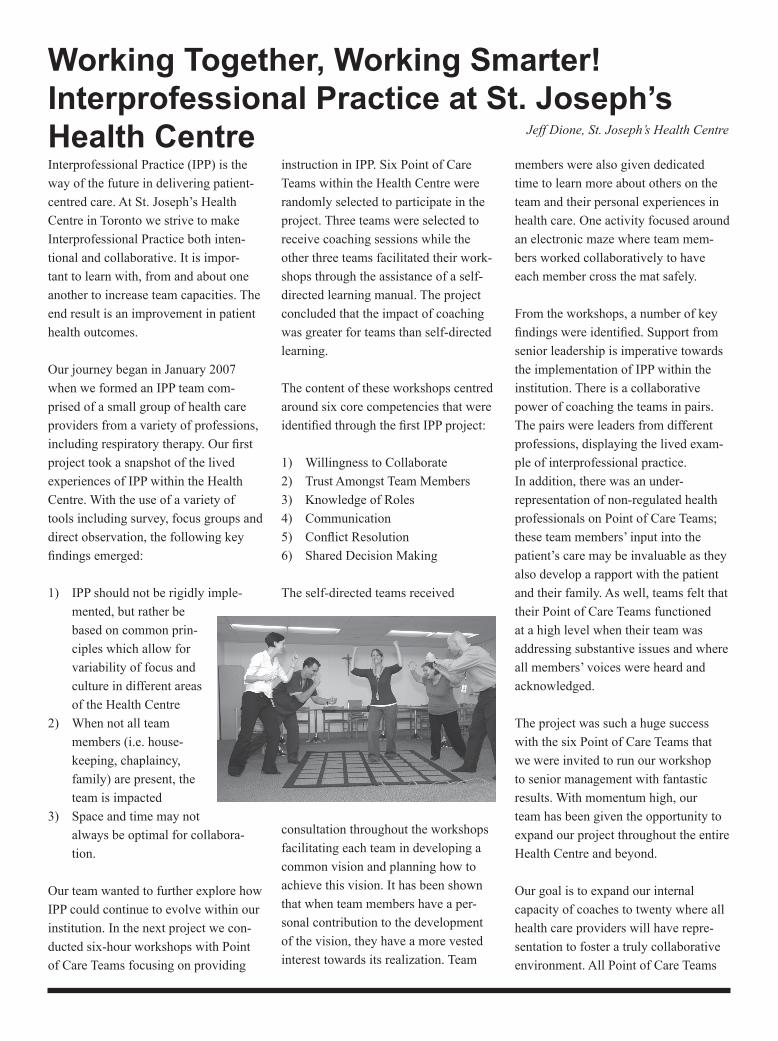
members were also given dedicated time to learn more about others on the team and their personal experiences in health care. One activity focused around an electronic maze where team mem-bers worked collaboratively to have each member cross the mat safely.
From the workshops, a number of key findings were identified. Support from senior leadership is imperative towards the implementation of IPP within the institution. There is a collaborative power of coaching the teams in pairs. The pairs were leaders from different professions, displaying the lived exam-ple of interprofessional practice. In addition, there was an under-representation of non-regulated health professionals on Point of Care Teams; these team members’ input into the patient’s care may be invaluable as they also develop a rapport with the patient and their family. As well, teams felt that their Point of Care Teams functioned at a high level when their team was addressing substantive issues and where all members’ voices were heard and acknowledged.
The project was such a huge success with the six Point of Care Teams that we were invited to run our workshop to senior management with fantastic results. With momentum high, our team has been given the opportunity to expand our project throughout the entire Health Centre and beyond.
Our goal is to expand our internal capacity of coaches to twenty where all health care providers will have repre-sentation to foster a truly collaborative environment. All Point of Care Teams

The 2007 Human Development Report (HDR) from the United Nations Devel-opment Program notes that, "There are still around one billion people living at the margins of survival on less than US$1 a day, with 2.6 billion—40 per-cent of the world's population—living on less than US$2 a day" (mainly in Asia). In an effort to become more human, I travelled to Nepal last summer with a friend to see first hand how much of the world's population lives. In particular we were there to explore the health care system in place for the general public. Due to the complexity of the situation there, I will focus only on public pediat-ric health care from a Canadian student RT perspective. Infant mortality statistics: Nepal: 62.00deaths/1000births; Canada: 5.02deaths/1000births. (CIA World Fact Book 2008 est.). Need for prenatal edu-cation is required. Our travels brought us to Kanti Bal (boy) Aspital (hospital), the only government pediatric hospital, situated in Kathmandu, the capital city of Nepal. Background: The vast majority (85+ %) of Nepalis live in rural areas where most are suste-
nance farmers; rice, corn, potato and tea are major items. This landlocked sliver of land is home to an altitude drop from 8850m (Mount Everest in the Hima-layas) to 60m above sea level (Terai region) within a 150-250km horizontal distance prone to spontaneous land-slides and flash land edema (i.e. flood-ing) during peak monsoon seasons. This makes for a very harsh and dangerous farming environment (e.g. cliffed land-scape, radical climate extremes, etc.). Lifestyle aside, words cannot describe the experience of being in a piece of natural unadulterated creation. At Kanti, patients come as a family unit — father, mother, child and any siblings. If they came from further away, only one parent may be present due to lack of resources to travel. Vaca-tion time is unheard of. The day you don't work will be the very day you don't eat. This is precisely the reason why many of the cases seen here will be end-stage. If' people have the concept of a healthcare facility, many will come only in dire straits after failed attempts of healing from local medicinals. The staffing situation is grim. The private sector is the only way to make good money. Residents will work at the government hospital to gain clinical
experi-ence. As soon as experi-ence is gained, they leave to open their own private practice working a fraction of the hours generating easily ten-fold their pay at the government hospital. Because this is the only government pediatric hospital it is arguable that there is no push to increase the stand-ards at this facility. Research does not exist as health care practitioners here are simply struggling to stay afloat. With limited supplies and expertise, treatments modalities are minimal. Kanti was a painful way to appreciate disease progression to death (e.g. hypo-plastic anemia, enterocolitis, etcetera). But many will flock here just for that reason. As patients enter the hospital com-pound, they are greeted with screams of un-anesthetized and frightened children getting an abscess drainage, lumbar puncture or burn dressing change. It is not uncommon to find fecal matter interspersed throughout the open hall where patients and their families wait to be seen. (Only 40% of Nepalis have a toilet; toilet meaning designated place for defecation). Although western style flush toilets exist at Kanti, washrooms
Healthcare in Nepal from a Canadian Student RT Perspective
will be given the opportunity to expe-rience this unique workshop. We are also expanding this project to include some of our external partners. Parkdale Community Health Centre has joined our team where five of their staff will participate as coaches to promote the lived experiences of Interprofessional
Practice with their Population Health Teams. In conjunction with the Univer-sity of Toronto and the Office of Inter-professional Practice, we are participat-ing in the development of a manual of Interprofessional Practice to further this initiative within any institution.
This project is more than an additional initiative. As members of the IPP team we believe ourselves to be the champi-ons of unheard voices honouring and appreciating uniqueness and bring-ing out the best in everyone. Working together is in fact working smarter!
Eric Cheng - SRT, Base site: Brampton Civic Hospital
have been used as storage space for unused or broken equipment. As if this was not a sight for sore eyes, an open room door reveals a squirming child held down by his father as a Roentgen ray is taken. The lead sits at the end of the table, its use unknown to the unedu-cated population. To a North Ameri-can this is an atrocity; but to the rural Nepali, this pales in comparison to their daily struggles for survival.
Unjaded by sound, sight and smell, patients line up to purchase a voucher that allows them to see a doctor. It costs 10Nepali Rupees, ~$0.17CAD which may be all the money they could save. They proceed to a public waiting area where families will join the masses in the open hall. Most families endure the 3-4 hour wait (the time it also takes to get petrol at the pumps) and are ushered into a cubi-cal where a young doctor consults. In this cubicle, 2-3 other families huddle around as the child is exposed for the doctor to examine. Other patients and their families look on curiously. To complicate matters, pharmaceuti-cal representatives interject with free samples plopped in front of the physi-cian followed by a brief colour flipbook presentation on the indications of their drug between (or even during) examina-tions. At the end of the outpatient day, several candidates for admission are ushered to their bed.
Depending on patient flow, it is not uncommon for two babies to share the same bed. Parents share the bed with the child. Meals are cooked by family members on electrical hotplates near free standing H-sized oxygen cylinders with pseudomonas growing in all the attached bubblers. The only redeeming thought is that bubblers are vapourizers.
Rounds take place with a consultant physician followed by a train of ten or so residents, foreign students, sisters (nurses) and other interested/concerned ambulating patients through the wards. The wards consist of large rooms of 4-10 beds. Curtains and privacy were obviously unheard of. While this seems intrusive, culturally they live transpar-ent lives with the people in their imme-diate community. It really shows in the rural area where each person really knows their neighbours.
The medical treatment is limited here to available resources and expertise. Due to the lack of government involvement, much of the resources used for the poor are expired goods or recycled goods (e.g. expired IV catheters, re-sterilized examination gloves). Healthcare prac-titioners have their hands tied and are limited. Moreover, they are subject to public criticism by patients that come to the hospital with false hope. Hospi-tal administration is an unfathomable nightmare with donated funds and equipment being mysteriously ‘lost‘ without fail. These are other issues that I will not divulge at this time.
Thank you for reading to this point as it is a huge burden lifted off my shoulders
to share all this with you. I assure you that nothing in this article is exagger-ated. In fact, much of it has been left out as situations in developing countries are just too extreme for anyone to describe on paper.
Health care issues from a patient perspective1. Education in hygiene: Due to the
lack of education in the rural areas, fundamentals such as hand washing and designated areas for defecation are still foreign concepts. Coupled in a farming environment where animals roam freely, children are prone to diseases uncommon in North America (e.g. hydatid cyst). In one week alone, I saw as many cases as North America sees annu-ally.
2. Education in red flags: The public does not know when they need to seek medial attention. During the surgical consults, I met kids with hemangiomas on their cheeks bigger than their fists that have persisted for 5+ years.
3. A catch 22: Even after obtaining a surgical date, the family had to turn away because they could not afford to stay in the city nor time away from their farm. Their options were limited: either go home and work harder to make up the time lost or lose their job and die of starvation in the city. Many come also with false hope looking for a miracle only to have their child die because it is too late.
4. Availability of medical facilities: for many, the trek to Kanti was far than easy. Suppose they did not have any financial trouble, they would still need to carry their child for a trek a couple of days through mountainous terrain, then hop on an overcrowded bus reeking of natural body odour and culturing bacteria. They will be on this bus for about one day.
Health care issues from a provider issue
1. Standard of practice: It is diffi-cult to practice to the best of their
abilities given the lack of resources and patient availability. E.g. Since most patients can only come in once, antibiotics are prescribed for everyone. Many of the patients that they see will never return due to personal issues as stated above. Those that do may be more likely to be antibiotic resistant due to the liberal use of antibiotics.
2. Opportunity to develop: due to the structure and corruption of man-agement the scope of medicine is severely limited. Any physician that wants to further their practice will not stay at a government hospital and eventually will move out from the country, much like most of the younger generation.
3. Public criticism: Due to the lack of education, patients come to the hospital looking for a quick fix; when they hear the bad news, physicians can be blamed or even publicly accused for killing a child. Nevertheless, the crowds remain at the hospital doors every day.
It puzzles me how the health care system survives. It poses so many obstacles for both patients and practi-tioners yet people still congregate at
hospitals. I believe that it has to do with hope. Patients hope for a favourable prognosis; practitioners and support workers hope to provide this reality. There is a lot of hope that floats around the hospital.
We are an extremely unique profes-sion in that we hope to be out of a job. Despite randomized control trials, textbook knowledge and the best diet plan, reality prevails and people get sick – and those that we see, very sick. Why is it that RTs wake up at hours non-existent to the general public to go to a place of sickness? Is it to withdraw on a young child? I think not. It is hope that drives us. It is hope that inspires us to resuscitate a patient in an arrest; it is hope that inspires us to tirelessly slave to develop coping mechanisms for chronic patients to have some sort of quality of life; it is hope that our patient will get over this pneumonia and be decannulated; it is hope that we have to celebrate life together that we see our palliative patients. We enter the hospital each day with hope, hope of something better for our patients and for our world.
As you embody the stethoscopic oath in giving hope to those that need it most, stand proud as respiratory therapists helping people breathe one breath at a time.
Peace be with you, Eric Cheng - SRT
For a listing of upcoming events, visit
www.rtso.org

The anesthesia assistant program, in general, was a positive experi-ence. Our group
of eleven RRTs came together from all three campuses in London and began our training in the summer of 2007. Our formal training ended at the end of winter, 2008. What we got out of it was what we put into it.
We all worked hard to make our sup-porters proud of us and as you can imagine, there were many supporters of this program. The London anaesthe-siologists, the Ministry of Health and Long-Term Care, the hospital admin-istrations, many nursing areas, all the OR staff from all three campuses and a special mention to the OR RRTs and RRTs of London who always made us feel at home were but a few of our strong supporters. I know from personal experience the sacrifice all our families had to give to make it work for us. I thank my wife and three children for their undying enthusiasm, their smiles and unwavering support throughout the many stages of this program.
I know we were all enthusiastic to learn as much as possible in that short time. The support we received from the anaesthesiologists in London was welcoming and generous. They were simply great! We learned and benefited from their extensive experience which had led each anaesthesiologist to prac-tice their profession a little differentlyfrom one another. They were patient teachers who welcomed us with respect.This atmosphere still remains to this day. I feel very fortunate.
We started at the advanced portion of the AA program in the fall of 2007 after completing the pharmacology course in the basic AA program that summer. The pharm course was on-line. Not only did we have to go through a large amount of material to process our pharmacology projects but we also had to learn how to do on-line discussions as a group with RRTs and RNs from all over the province from a variety of backgrounds. Both aspects of this course were a significant task. Learning how to do a course on-line is definitely a skill set.
This skill set was used often in the advanced AA course that fall. In this part of the program, the eleven London RRTs were with three other RRTs from the province and one RN. The fifteen of us got along very well. We were often told that our 30 page weekly group reports/presentations were far above the usual expectations and we were asked to tone it down a bit. “We were intense”. Our final week which was called residential week was probably the most stressful since we were away from our home base but the medical director of the program, Dr. Claire Middleton, helped reduce the anxiety through reas-surances and support.
In early January, we started our clinical rotation which we all passed with good marks. Though the formal course is over, I feel that my career as an AA will be a life long learning experience. This is just what I wanted.
Again, thank you to all my friends and colleagues for allowing me this oppor-tunity to grow.
The AA Program Experience Bill Warmels, RRT, BSc, AA
On Wednesday March 12th, the Res-piratory Therapy Student Federation (RTSF) with sponsorship from ProResp, hosted its first Inter-Professional Educa-tion Conference at Fanshawe College.The conference provided attendees with information on the latest research, diagnosis and treatment options in the field of pulmonary mechanics (iLA, NovaLung), and about trauma from the eyes of an enthusiastic emergency air transport paramedic. In attendance were Respiratory Therapy, Paramedic, and Nursing students, as well as staff and management RTs from the field of Respiratory Therapy.
The conference lead way with the RTSF’s President Anil Charran’s open-ing remarks regarding the federation “I am excited about our objectives for our third year in operation as we continue to build stronger ties amongst our colleagues”. Paula Gravelle RRT, CAE from Novalung and Dugg Steary HBOR, BA, CCP (f) from the Emer-gency Air Transport Paramedics were the two keynote speakers invited to support the RTSF The audience was treated to two great presentations and many door prizes (donated by the RTSO and ORCS) were given out in apprecia-tion for attendance. The money raised for the conference is to be donated to the Canadian Lung Association as part of the RTSF’s continuing commitment to improving lung health.
The conference was a great success and we look forward to many more similar events from the future leaders of the RTSF.
RTSF Inter-Professional Conference Denis Zaravinos SRT BSc
The RTSO Board is looking forward to socializing and learning with you at the RTSO Education Forum, October 2-3, 2008 in Niagara Falls.
Join us Thursday evening (October 2) for a Meet & Greet Wine and Cheese… a great start to the Forum.
Friday Morning (October 3) starts off with the RTSO Annual General Meeting
• Vote for your Board of 2008-2009• Celebrate RTSO accomplishments
Following the AGM, an exciting slate of education topics await you including:
• “H5N1 a Worthy Viral Contender” Dr Harry Hong
• “As the Lungs Turn: Optimizing Ventilation During the Changing Disease Process” Dr Peter Papada-kos
• “A Critical Care Team Success Story”, Dr Peter Papadakos and Rudolph Koch RRT
• “Filters, Plague and Pestilence” Ron Thiesen RRT
Circle October 2-3, 2008 on your calen-dar and watch for your registration flier in the mail.
Fast facts about the Falls• the Canadian Horseshoe Falls
plunges 52 metres (170 feet) into the Maid of the Mist Pool.
• at the American Falls the water’s vertical descent ranges from 21 to 34 metres (70 to 110 feet) to the rock at the base of the Falls.
• the Niagara Gorge extends from the Falls for 11 kilometres (7 miles) downstream to the foot of the escarpment at Queenston.
• more than 168,000 cubic metres (6 million cubic feet) of water go over the crestline every minute during peak day time tourist hours.
RTSO Education Forum - October 2-3, 2008
Allied Health Professional Development Fund Continues in 2008/2009For the third consecutive year, the government is providing financial sup-port for health professionals through the Allied Health Professional Devel-opment Fund. Practising members of nine allied health professions will be able to apply for as much as $1500 for professional development courses and programs. The purpose of the fund is to develop skills and enhance knowledge and lead-ership capacity among allied health pro-fessionals. This year, the $2.5 million fund will provide grants for professional development opportunities completed from April 1, 2008 - March 31, 2009. The eligible allied health professions are: Medical Laboratory Technology, Physiotherapy, Medical Radiation Tech-
nology, Occupational Therapy, Speech Language Pathology, Audiology, Dietet-ics, Pharmacy and Respiratory Therapy. To further support professional develop-ment, the Fund has invested in a three-year subscription to an electronic health library that will be made available to practising members of the eligible allied health professions. This library will give health professionals access to the most recent health care literature to help determine the best approach to evidence-based practice.
What’s Next?The guidelines and application form for the Fund and information on the
library service will be made available in upcoming weeks at: www.ahpdf.ca. The government recognizes and values the important contribution made by allied health professionals to the health care system. The Allied Health Profes-sional Development Fund is a Health-ForceOntario initiative. This innovative health human resources strategy is designed to ensure the people of Ontario have access to the right number and mix of health care professionals, now and in the future.
Remember the Respiratory Therapy posters sent to Respiratory Therapy departments over the past few years with slogans such as, “Ask an expert….Respiratory Therapists: Breathing is our business”,"Respiratory Therapists Working as Anesthesia Assistants" and "The many faces in many places"?
For the fifth year, the CRTO and the RTSO is again holding a photo contest for Members. The winning photo will appear on this year’s poster that will be mailed to Respiratory Therapy departments across the province before RT Week. We are looking for photos in all RT areas.
Here are the details: Photographers must receive written consent from all subjects in the photo. (Photo Release Form can be found on the RTSO website, Media Kit) Role playing is suggested. A slogan or catch phrase may also be submitted to contribute to the poster’s message.
Photo Guidelines:
JPEG compression should be “high” or “maximum” Resolution of the image should be 220 dpi or greater Minimum size of the photo should be 1.4 mb before saving as a JPEG file.
Deadline for receiving photos is June 30th. Electronic versions of the photo can be sent to [email protected] and/or [email protected]. Please make sure to include your full contact information with submissions.
Cash prizes will be awarded for the top three photos selected by the CRTO/RTSO Communications Working Group.
$100.00 for 1st place $ 75.00 for 2nd place $ 25.00 for 3rd place
Happy Shooting!
RTSO/CRTO Photo Contest for Ontario Respiratory Therapists.... The deadline for receiving photos is June 30, 2008
The goal of the Anaesthesia Care Edu-cation Series is to help create a forum for RRTs to learn about relevant clinical practices and to help develop a network of colleagues with similar interest. We hope this becomes a forum where we can share experiences as the profes-sion develops and expands its role as a clinical member of the Anaesthesia Care Team.
Inaugural Session : July 16th Toronto General Hospital, Time TBASponsored by Dräger Medical
Agenda: Low Flow AnaesthesiaRegional Anaesthesia
This inaugural education event will include dinner and be free for all regis-trants.
Keep your calendar open July 16th and your ear to the ground for further details on the RTSO Anaesthesia Care Educa-tion Series.
Please contact the RTSO by July 14th to register and reserve your spot: (905) 567-0020 or [email protected]
Anaesthesia Assistant Education Series