Embed Size (px)
Citation preview
9/7/2016
1
Stacy Campbell NCLE-AC, COA
Eye Care Associates [email protected]
• Pre-Fitting History taking
External exam
Prescriptions
Keratometry/Topography
• Lens Selection – Soft and RGP
• Insert and Removal (I&R)
• Tools
Pre-Fitting - History
Previous Contact Lens Experience
How long ago did they try?
Why did they stop?
Why do they want to try again?
What are their expectations
No Contact lens Experience
• Why do they want to wear contacts?
• What do they know about contact lenses?
• What are their expectations?
Things that could affect contact lens wear
Medications Oral Contraceptives
Antihistamines/decongestants
Accutane (acne medications)
Eye drops
Insulin
Thyroid medications
Diuretics
Antidepressants
Immunosuppressant's
Allergies Seasonal
Contact Allergies to materials
Latex or Silicone
Medical Conditions Diabetes
Thyroid
Pregnancy
Menopause
Epilepsy
Abnormal Blood Pressure
Psychiatric disorders
External Exam
• Lids and lashes
– Check for signs of blepharitis
– Look at the elasticity of the lids (important in RGP fitting)
– Check Fissure openings (important in RGP fittings)
9/7/2016
2
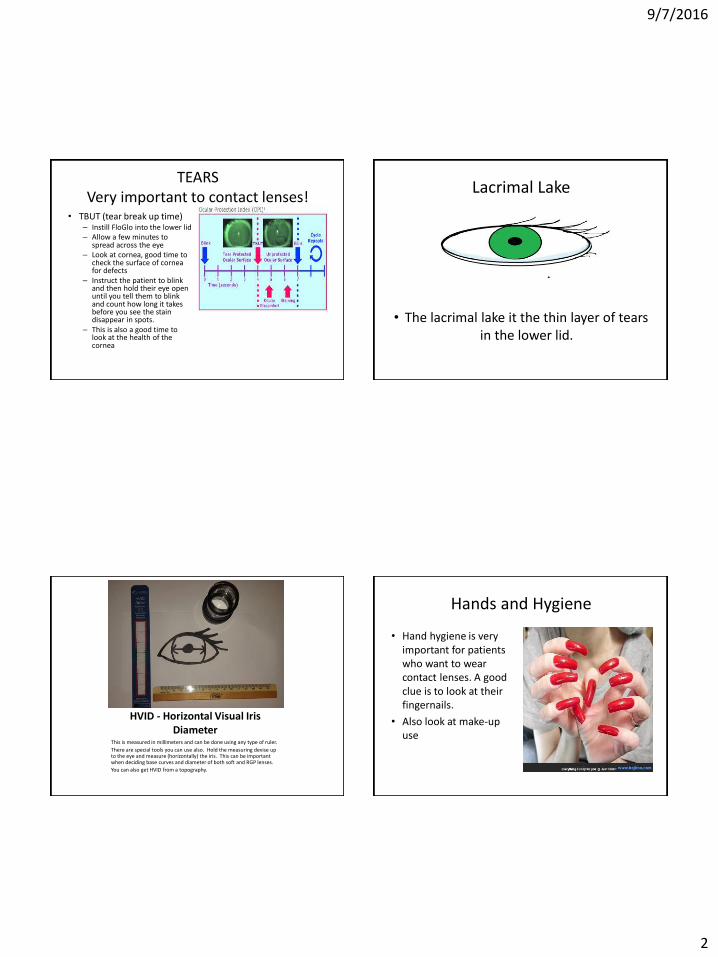
TEARS Very important to contact lenses!
• TBUT (tear break up time) – Instill FloGlo into the lower lid – Allow a few minutes to
spread across the eye – Look at cornea, good time to
check the surface of cornea for defects
– Instruct the patient to blink and then hold their eye open until you tell them to blink and count how long it takes before you see the stain disappear in spots.
– This is also a good time to look at the health of the cornea
Lacrimal Lake
• The lacrimal lake it the thin layer of tears in the lower lid.
HVID - Horizontal Visual Iris Diameter
This is measured in millimeters and can be done using any type of ruler.
There are special tools you can use also. Hold the measuring devise up to the eye and measure (horizontally) the iris. This can be important when deciding base curves and diameter of both soft and RGP lenses.
You can also get HVID from a topography.
Hands and Hygiene
• Hand hygiene is very important for patients who want to wear contact lenses. A good clue is to look at their fingernails.
• Also look at make-up use
9/7/2016
3
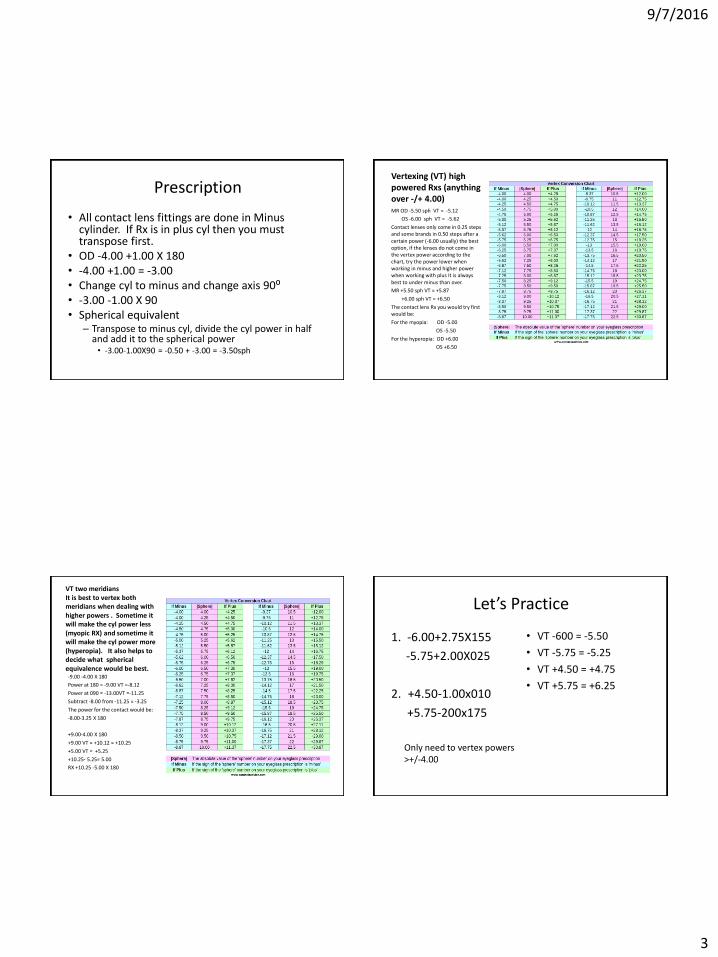
Prescription
• All contact lens fittings are done in Minus cylinder. If Rx is in plus cyl then you must transpose first.
• OD -4.00 +1.00 X 180 • -4.00 +1.00 = -3.00 • Change cyl to minus and change axis 90⁰ • -3.00 -1.00 X 90 • Spherical equivalent
– Transpose to minus cyl, divide the cyl power in half and add it to the spherical power • -3.00-1.00X90 = -0.50 + -3.00 = -3.50sph
Vertexing (VT) high powered Rxs (anything over -/+ 4.00) MR OD -5.50 sph VT = -5.12
OS -6.00 sph VT = -5.62
Contact lenses only come in 0.25 steps and some brands in 0.50 steps after a certain power (-6.00 usually) the best option, if the lenses do not come in the vertex power according to the chart, try the power lower when working in minus and higher power when working with plus It is always best to under minus than over.
MR +5.50 sph VT = +5.87
+6.00 sph VT = +6.50
The contact lens Rx you would try first would be:
For the myopia: OD -5.00
OS -5.50
For the hyperopia: OD +6.00
OS +6.50
VT two meridians It is best to vertex both meridians when dealing with higher powers . Sometime it will make the cyl power less (myopic RX) and sometime it will make the cyl power more (hyperopia). It also helps to decide what spherical equivalence would be best. -9.00 -4.00 X 180
Power at 180 = -9.00 VT =-8.12
Power at 090 = -13.00VT =-11.25
Subtract -8.00 from -11.25 = -3.25
The power for the contact would be:
-8.00-3.25 X 180
+9.00-4.00 X 180
+9.00 VT = +10.12 = +10.25
+5.00 VT = +5.25
+10.25- 5.25= 5.00
RX +10.25 -5.00 X 180
Let’s Practice
1. -6.00+2.75X155
-5.75+2.00X025
2. +4.50-1.00x010
+5.75-200x175
Only need to vertex powers >+/-4.00
• VT -600 = -5.50
• VT -5.75 = -5.25
• VT +4.50 = +4.75
• VT +5.75 = +6.25
9/7/2016
4
Answers
• -3.25-2.25X065
• -3.75-1.50x115
• -5.50-3.25= -2.25
• -5.25-3.75= -1.50
• +4.75-1.25X010
• +6.25-2.50X175
• +4.75-(+3.50) = -1.25
• +5.75- (+3.75) = -2.50
Spherical Equivalent
• SPH equivalence is done usually with low cylindrical powers.
• Transpose to minus cyl
• Divide the cyl in half and add it to the sph power
• In higher powers, if you vertex both meridians you can use the average to make a sph equivalent
• -3.00-0.50X090
• -2.75-0.50X090
• -0.50 = -0.25
• Sph E = -3.25 and -3.00
• -7.00-0.50X075
• -8.00-0.75X100
• -7.00 vt = -6.50
• -7.50 vt = -6.87 try -7.00
• -8.00 vt = -7.25
• -8.75 vt = -7.87 try -7.50
Keratometery
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Topography
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
9/7/2016
5
Lens Selection Soft vs RGP
• How do we chose between soft and RPG? – Ask the patient
• Have you worn contacts before?
• What kind of contacts have you thought about?
• What kind of activities will you be doing with your contacts on?
• What are your visual expectations?
Soft Contact Lenses
Advantages
• Very short adaptation period
• Comfortable
• Readily available, trials in office
• Available in a wide variety of Rxs
• Colors
• Wide variety of replacement schedules
• Great for active people & sports
• Some can be slept in
• Easy to clean
Disadvantages
• Doesn’t correct all vision problems, not as sharp as RGP
• Lenses have to be replace frequently
• Tears, rips, hard to keep clean, easy to lose.
• Sleeping in lenses increases risk of complications
• Difficult to handle
• More difficult to insert and remove than RGP
RGP Lenses
Advantages • Excellent Vision • Corrects most vision problems • Very easy to insert and remove • Does not tear • Easy to clean and store • A pair can last up to two years
(some people keep them longer)
• Available in tints (not for changing eye color)
• Excellent choice for a bifocal • Available for Myopia control
Disadvantages
• Longer adaptation period
• Requires constant wear to stay accustom to the feel
• Can slip of center and even pop out
• Debris can get trapped under the lenses (painful)
Soft Contact Lenses Fitting
There are several types of soft contact lenses. First you want to know, how often the patient wants to wear the contacts and much cleaning they are willing to do. Next, have a discussion with the patient of their options. Third, look at their Rx to see if they need a lens for an astigmatism, bifocal, or both.
lens modality advantages disadvantages
Single use healthy cost
no cleaning needed takes up space
plenty of extra lenses not in multifocal toric
easy to travel with
good for people with
dry eyes and allergies
come in SyHy
Week healthy not available in SyHy
easy replacement schedule cost
not in multifocal toric
needs to be cleaned
Two week less cost cleaning
comes in SyHy material people keep lenses longer
not in multifocal toric
Monthly less cost needs to be cleaned
comes in SyHy material cleaning
easy replacement schedule people keep lenses longer
comes in multifocal toric
9/7/2016
6
Fitting of a soft lens
• Once you’ve decided on a modality it is now time to try on some lenses!
• First things, look at the size of the eyes…bigger eyes = steeper eyes.
• Next, look at the Ks • Medium K is around 43.00 • Steep is over 46.00 • Flat is under 42.00 • These measurements are just a starting. The best thing to do is
try the lenses on and look at them! • The two key things to look for are: 1. Centration
2. Movement
Centration The lens rides low
1. Usually it means the lens is too loose. Try a steeper lens or larger diameter.
The lens rides high
1. Usually a sign the lens is too tight or diameter is off. Try flattening the base curve.
A perfect centered lens will be at least 2mm outside the limbus 360 degrees.
Have the patient look side to side to make sure the lens is centered in all gazes.
*One thing you should do if you have a lens that is not centering is to Flip the Eye lids! It could be a sign of GPC (Giant Papillary Conjunctivitis)
Movement of a soft lens Once you have a lens that is centered you’ll need to look at the movement.
Place patient in the slit lamp
Use a narrow beam at about 45 degree angle and look at the edge of the lens as the patient blinks. Look at both temporal and nasal sides of the eye. Have the patient look up and watch for movement. The lens should move around 1-2 mm.
Using a vein on the white of the eye as a guild to see if the lens moves.
Excessive movement could lead to irritation. Make sure when the patient blinks the lens never hits the limbus.
Sometimes it is difficult to see any movement. Another way to check is with the thumb push method.
Toric Check for Centration and movement
• One key thing with checking a toric is the hash marks on the lens they sit at 6 O’clock or 3-9 O’clock
• If they sit right or left of where the mfg. suggest you have to modify the axis- each clock is 30 degrees!
• -1.00-1.25X 180
Left ADD
-1.00-1.27X 010
LARS
Right subtract
-1.00-1.25X 170
9/7/2016
7
Presbyopia Fitting
• Multifocal • Mono Vision
Multifocals-always read the mfg. instructions they are very helpful
• Check for eye dominance! • Use fogging method • Ask the patient which eye they think is dominant.
Do they fire a weapon? What eye to they aim with? Do they use a regular camera? Which eye do they look with?
• Have them wink at you. Most people will close their nondominant eye to wink.
• When all else fails, just start putting contact lenses on and play around!
RGP “Hard” Lots of ways to fit RGP lenses
First take a good look at where the eyelids interact with the cornea
This will help decide what style of fit
Lid attachment or Apical clearance
Either way the best way to fit it to put lenses on and look at stain patterns.
Look at the Ks are they with the rule or against! You can fit both but for a beginner stick with With!
There are a few formulas – again read the instructions on your trial kits!!!!!! They will walk you through a fit.
Two types of RGP fittings
Lid Attachment
• This is where the contact is tucked under the top lid – Usually the ideal fit
Apical Clearance
• This is where the lens floats in between the lids – Pops out easier!
9/7/2016
8
Standard Fitting Guilds
• Try lenses on!
• Start with lens at flat k or slightly steeper
• Try on until the lens centers well, moves with the blink, slide on cornea when patient looks side-to-side, and there is a nice tear exchange
• Once you have a lenses that sits well, over refract
• ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Empirically Fitting RGP
• ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Problem solving RGP (call for help!)
• Lens rides low = too steep
• Lens rides high = too flat
• Lens rides temporal or nasal
– Probably against the rule cyl = try toric
_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Problem solving RGP
• Too much pool centrally = too steep
• No stain centrally = too flat
• _________________________________________________________________________________________________________________________________________________________________________________________________________________
9/7/2016
9
I&R (Insert and Removal)
• Wash hands – no antibiotic, lotion, or scented soaps
• inside out/right side
– Taco
– Bowl
– Some lenses have markings
Insert: YOUTUBE
1. Place contact lens on index finger 2. Check with taco test that it is not inside out 3. Place arm opposite of eye that will receive the lens on
top of the lash area of lids. Keep firm grip of upper lid. 4. Use other hand to grasp of lower lid while keeping
contact lens on index finger. 5. While keeping chin down, face the mirror and insert
the contact onto the cornea until it touches 6. Look down and then straight to align contact onto
cornea • https://www.youtube.com/watch?v=rKnHWfw4Azo
Removal: J method
1. Place front side of index finger onto colored part of eye
2. Tilt chin downwards.
3. Press index finger into eye and push into eye.
4. Pull contact down and roll finger outwards
Removal: Pointer method
1. Clasp hands together 2. Point both index fingers
upwards while still clasping hands
3. Open eyes wide while looking in the mirror chin down
4. Press index fingers onto eye while creating a gap between them (should be able to see self in the mirror though fingers)
5. Pinch index fingers together and pinch contact out.
9/7/2016
10
Pick out method
• Hands like you were putting in the lenses, one on top lid one on bottom
• Use index finger to slide lens down
• Pick out with thumb and index finger
RGP Inserting
• Similar to soft insertion except the lens must be applied directly to the cornea.
• Sometimes easier not to use a mirror
RGP Removal Blink Method
• Place index finger along side of eye
• Open wide
• Pull lids tight with index finger
• Blink hard
• Catch in other hand
RGP Removal 2finger or 2 hands
• This method uses either two fingers of both hands to use the lids to pop the lenses out
• You pull open the lids to the outside of the lens and then try to push them under the lens to wedge it out
9/7/2016
11
RGP Removal
• Removing an RGP lens take can be tricky. I like to instruct on how to use the plunger and always give one to my patient. I make sure they can safely use it before I let them leave the office with one.
Solutions Soft Lenses
Multipurpose • Clean Rinse Soak with one
solution. • Easy and Safe • Does not kill all “bugs” • Tendency not to do correctly.
Lenses should be rubbed or rinsed for 5 seconds….does that really happen
• Allergies to solution and preservatives in solution
• Not all solutions compatible with all contact lens material
Hydrogen Peroxide
• Easy
• Safe
• Best cleaner
• No solution sensitivity
• Can be used with all contact lenses
• Painful if not done right! Or if accidentally put in eye!
• Requires more thought and soak time
Cleaning and Storing RGP
• Cleaner
• Conditioner
• Multipurpose
• No water on soft or RGP!!!!!
• Hydrogen Peroxide for RGP!
Insert and Removal instructions
• Insert – Wash & dry hands
– Check inside out (soft)
– Put lens in
– Wearing schedule, varies by type of lens, usually a build up period
– No water no swim no sleep
– If they have pain, take lenses out and call office
– Makeup is applied after insertion
• Removal – Wash & dry hands
– Take lenses out
– Clean and store
– If you fit single use lenses this is a lot easier!
9/7/2016
12
Tools of the Trade
• Cobalt Filter
• Blue pen light
• Tyler’s Quarterly
• HVID
• Vertex chart
• Diopter to K conversion chart
Don’t be afraid of Contacts
Advanced Stuff
• Hybrid lenses
• Scleral
• Keratoconus
• Transplants
• Scars
• Prosthetics
• Pediatrics
• Bandage
• Contact lenses can be life changing for some people
• You could really make the blind see with some contact lenses all you have to do is try them on!
Questions?
Minnesota Contact Lens Society
– www.mncontactlens.com
– Fall and Spring symposiums
National Contact Lens Society of America
www.clsa.info
Conference usually in fall, on-line learning