Embed Size (px)
Citation preview
1
UPDATED
March 3rd, 2014
Standard of procedures
Special Authorization Drugs
1) General Section For all of the following drugs:
Claims should be coordinate with the Provincial government program when available.
The administration site should be validate for injectable drugs.
For Quebec residents, authorization RAMQ criteria predominate on the criteria of this table.
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
ABSTRAL (FENTANYL CITRATE)
Sublingal Tablet
DIN : 02364174 (100µg)
DIN : 02364182 (200µg)
DIN : 02364190 (300µg)
DIN: 02364204 (400µg)
DIN: 02364212 (600µg)
DIN: 02364220 (800µg)
Cancer pain
Management of breakthrough pain in patients
with cancer who are already receiving and who
are tolerant to opioid therapy for their
persistent baseline cancer pain
18 years of age or older
3 months
6 months
ACTEMRA (TOCILIZUMAB)
Intravenous Solution
DIN 02350092 (80 MG / 4 ML)
DIN 02350106 (200 MG / 10 ML)
DIN 02350114 (400 MG / 20 ML)
Rheumatoid
Arthritis (RA)
Systemic Juvenile
Idiopathic Arthritis
(JIA)
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
2 years of age or older
5 or more affected joints and failure or
contraindications to methotrexate and to
another disease modifiying antirheumatic drugs
for a period of 3 months or more
Or
1 or more affected joints and at least one
systemic manifestation (fever, rash,
adenomegaly, hepatomegaly, splenomegaly,
serous effusion)
5 months
5 months
1 year
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or HAQ or
return to work
1 year
Improvement of 20 % for
affected joints
And
Improvement of systemic
manifestations if appropriate
And
Improvement of 20 % for
SRV or CRP or improvement
of CHAQ or return to school
2
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
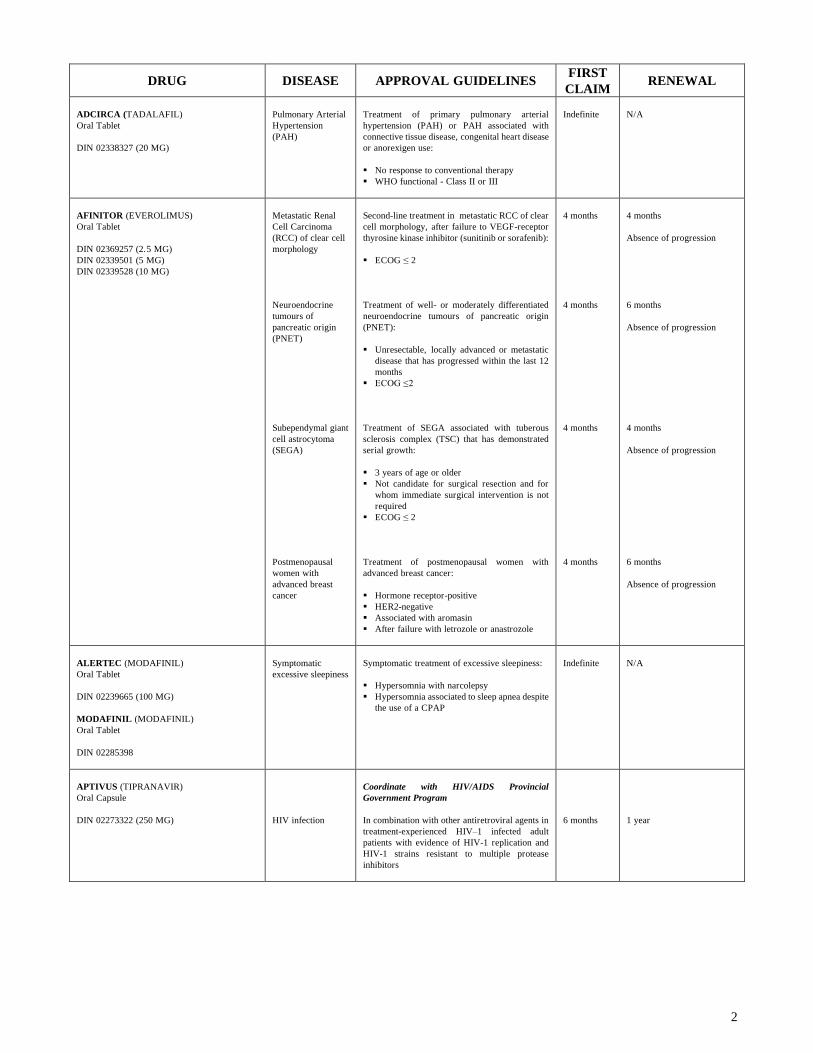
ADCIRCA (TADALAFIL)
Oral Tablet
DIN 02338327 (20 MG)
Pulmonary Arterial
Hypertension
(PAH)
Treatment of primary pulmonary arterial
hypertension (PAH) or PAH associated with
connective tissue disease, congenital heart disease
or anorexigen use:
No response to conventional therapy
WHO functional - Class II or III
Indefinite
N/A
AFINITOR (EVEROLIMUS)
Oral Tablet
DIN 02369257 (2.5 MG)
DIN 02339501 (5 MG)
DIN 02339528 (10 MG)
Metastatic Renal
Cell Carcinoma
(RCC) of clear cell
morphology
Neuroendocrine
tumours of
pancreatic origin
(PNET)
Subependymal giant
cell astrocytoma
(SEGA)
Postmenopausal
women with
advanced breast
cancer
Second-line treatment in metastatic RCC of clear
cell morphology, after failure to VEGF-receptor
thyrosine kinase inhibitor (sunitinib or sorafenib):
ECOG ≤ 2
Treatment of well- or moderately differentiated
neuroendocrine tumours of pancreatic origin
(PNET):
Unresectable, locally advanced or metastatic
disease that has progressed within the last 12
months
ECOG ≤ 2
Treatment of SEGA associated with tuberous
sclerosis complex (TSC) that has demonstrated
serial growth:
3 years of age or older
Not candidate for surgical resection and for
whom immediate surgical intervention is not
required
ECOG ≤ 2
Treatment of postmenopausal women with
advanced breast cancer:
Hormone receptor-positive
HER2-negative
Associated with aromasin
After failure with letrozole or anastrozole
4 months
4 months
4 months
4 months
4 months
Absence of progression
6 months
Absence of progression
4 months
Absence of progression
6 months
Absence of progression
ALERTEC (MODAFINIL)
Oral Tablet
DIN 02239665 (100 MG)
MODAFINIL (MODAFINIL)
Oral Tablet
DIN 02285398
Symptomatic
excessive sleepiness
Symptomatic treatment of excessive sleepiness:
Hypersomnia with narcolepsy
Hypersomnia associated to sleep apnea despite
the use of a CPAP
Indefinite
N/A
APTIVUS (TIPRANAVIR)
Oral Capsule
DIN 02273322 (250 MG)
HIV infection
Coordinate with HIV/AIDS Provincial
Government Program
In combination with other antiretroviral agents in
treatment-experienced HIV–1 infected adult
patients with evidence of HIV-1 replication and
HIV-1 strains resistant to multiple protease
inhibitors
6 months
1 year

3
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
ARANESP (DARBEPOETINE ALFA)
Intravenous, Subcutaneous Solution
DIN 02246354 (10 MCG / 0.4 ML)
DIN 02246355 (20 MCG / 0.5 ML)
DIN 02246357 (30 MCG / 0.3 ML)
DIN 02246358 (60 MCG / 0.3 ML)
DIN 02246360 (150 MCG / 0.3 ML)
Anemia
If available, coordinate with the Provincial
Government Program
Treatment of anemia associated with chronic
kidney disease (CKD), including patients on
dialysis and patients not on dialysis
Or
Treatment of Anemia due to Chemotherapy in
Patients with Non-Myeloid Malignancies
Or
AIDS related anemia
Indefinite
N/A
AUBAGIO (TERIFLUNOMIDE)
Oral Tablet
DIN 02416328 (14 MG)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
Treatment of relapsing-remitting multiple
Sclerosis (RRMS):
18 years of age or older
Prescribed by a neurologist
Monotherapy
EDSS ≤ 5.5
Number of disabling clinical relapses in the
last 12 months
MRI
6 months
1 year
AVONEX (INTERFERON BETA-1A)
Prefilled Serynge or Autoinjector
DIN 02269201 (30 MCG / 0.5 ML)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
Chronic
Progressive
Multiple Sclerosis
(CPMS)
Single
demyelinating event
with two clinically
silent lesions
typical of MS
(MRI+ )
If available, coordinate with the Provincial
Government Program
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
If isolated
clinical
syndrome
(ICS): 1
year
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
ICS : 1 year
BANZEL (RUFINAMIDE)
Oral Tablet
DIN 02369613 (100 MG)
DIN 02369621 (200 MG)
DIN 02369648 (400 MG)
Lennox-Gastaut
Syndrome (LGS)
Adjunctive treatment of seizures associated with
Lennox-Gastaut syndrome:
4 years of age or older
Inadequate response or failure to one or more
other antiepileptic drugs
6 months
1 year
BARACLUDE (ENTECAVIR)
Oral Tablet
DIN 02282224 (0.5 MG)
Hepatitis B virus
infection
If available, coordinate with the Provincial
Government Program
Treatment of chronic hepatitis B virus infection
with 0.5 mg daily
No resistance to lamivudine and according viral
load
Treatment of chronic hepatitis B virus infection
with 1 mg daily:
Resistance to lamivudine and according viral
load
Failure of treatment with adefovir or being
intolerant to adefovir
Indefinite
N/A
4
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
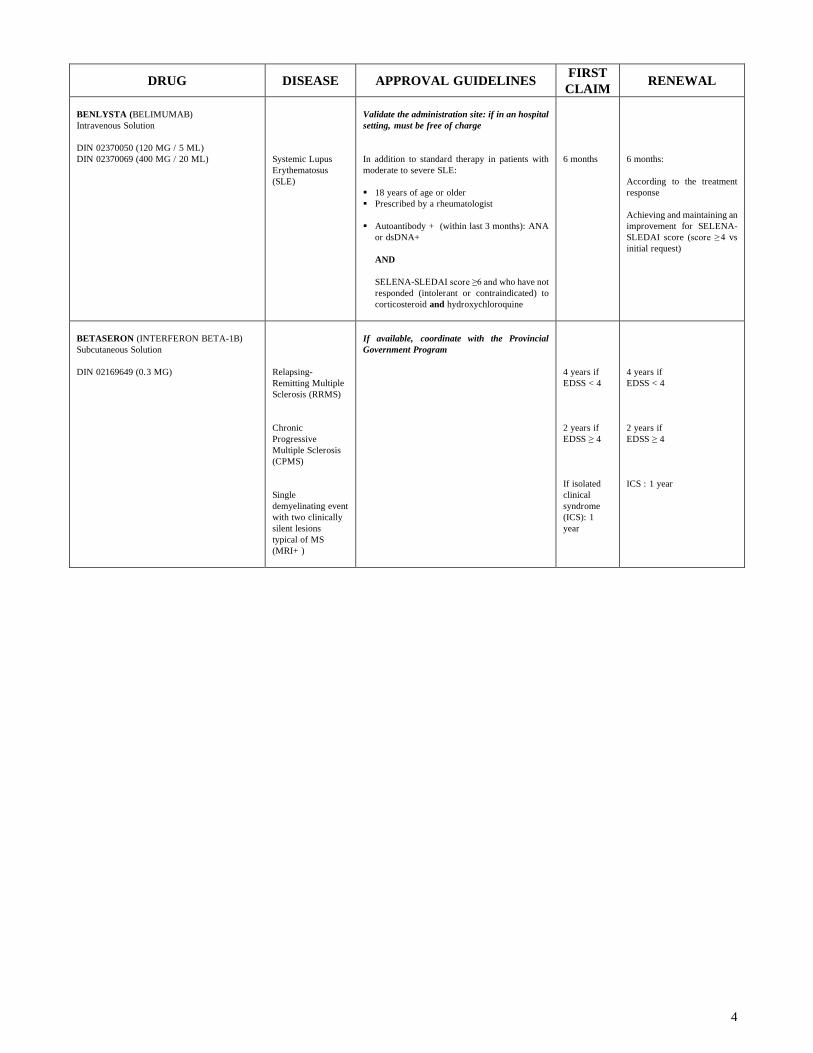
BENLYSTA (BELIMUMAB)
Intravenous Solution
DIN 02370050 (120 MG / 5 ML)
DIN 02370069 (400 MG / 20 ML)
Systemic Lupus
Erythematosus
(SLE)
Validate the administration site: if in an hospital
setting, must be free of charge
In addition to standard therapy in patients with
moderate to severe SLE:
18 years of age or older
Prescribed by a rheumatologist
Autoantibody + (within last 3 months): ANA
or dsDNA+
AND
SELENA-SLEDAI score ≥ 6 and who have not
responded (intolerant or contraindicated) to
corticosteroid and hydroxychloroquine
6 months
6 months:
According to the treatment
response
Achieving and maintaining an
improvement for SELENA-
SLEDAI score (score ≥ 4 vs
initial request)
BETASERON (INTERFERON BETA-1B)
Subcutaneous Solution
DIN 02169649 (0.3 MG)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
Chronic
Progressive
Multiple Sclerosis
(CPMS)
Single
demyelinating event
with two clinically
silent lesions
typical of MS
(MRI+ )
If available, coordinate with the Provincial
Government Program
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
If isolated
clinical
syndrome
(ICS): 1
year
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
ICS : 1 year
5
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
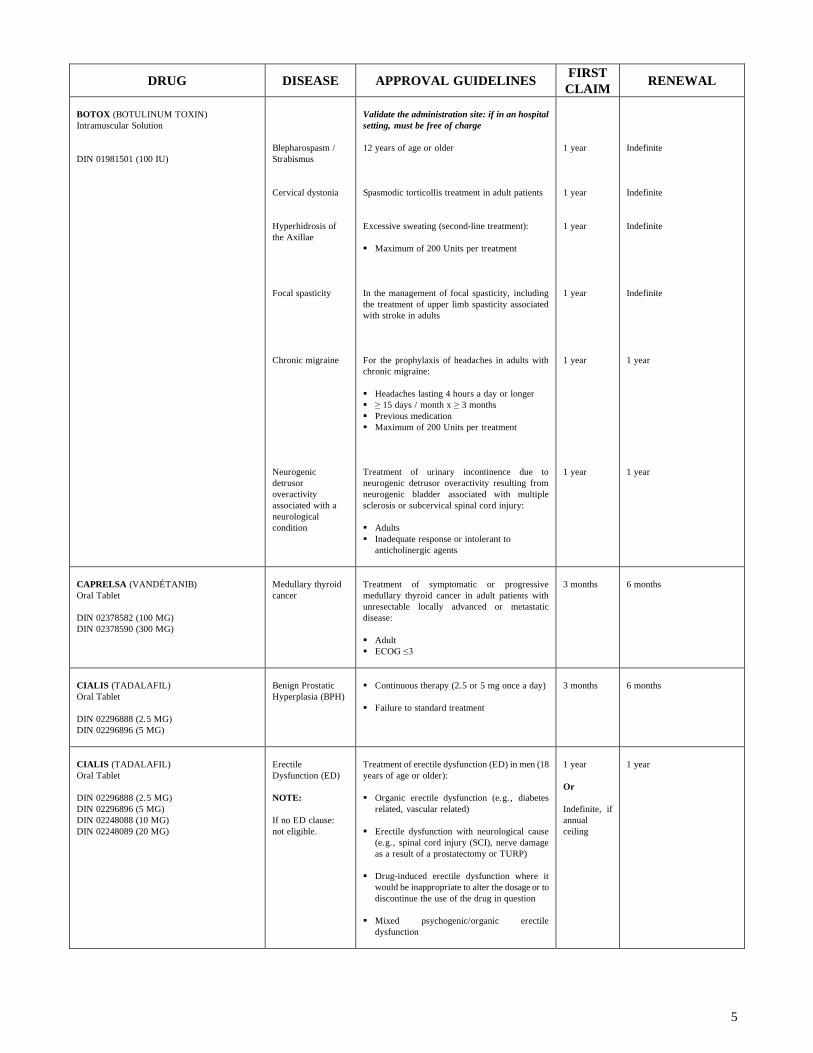
BOTOX (BOTULINUM TOXIN)
Intramuscular Solution
DIN 01981501 (100 IU)
Blepharospasm /
Strabismus
Cervical dystonia
Hyperhidrosis of
the Axillae
Focal spasticity
Chronic migraine
Neurogenic
detrusor
overactivity
associated with a
neurological
condition
Validate the administration site: if in an hospital
setting, must be free of charge
12 years of age or older
Spasmodic torticollis treatment in adult patients
Excessive sweating (second-line treatment):
Maximum of 200 Units per treatment
In the management of focal spasticity, including
the treatment of upper limb spasticity associated
with stroke in adults
For the prophylaxis of headaches in adults with
chronic migraine:
Headaches lasting 4 hours a day or longer
≥ 15 days / month x ≥ 3 months
Previous medication
Maximum of 200 Units per treatment
Treatment of urinary incontinence due to
neurogenic detrusor overactivity resulting from
neurogenic bladder associated with multiple
sclerosis or subcervical spinal cord injury:
Adults
Inadequate response or intolerant to
anticholinergic agents
1 year
1 year
1 year
1 year
1 year
1 year
Indefinite
Indefinite
Indefinite
Indefinite
1 year
1 year
CAPRELSA (VANDÉTANIB)
Oral Tablet
DIN 02378582 (100 MG)
DIN 02378590 (300 MG)
Medullary thyroid
cancer
Treatment of symptomatic or progressive
medullary thyroid cancer in adult patients with
unresectable locally advanced or metastatic
disease:
Adult
ECOG ≤ 3
3 months
6 months
CIALIS (TADALAFIL)
Oral Tablet
DIN 02296888 (2.5 MG)
DIN 02296896 (5 MG)
Benign Prostatic
Hyperplasia (BPH)
Continuous therapy (2.5 or 5 mg once a day)
Failure to standard treatment
3 months
6 months
CIALIS (TADALAFIL)
Oral Tablet
DIN 02296888 (2.5 MG)
DIN 02296896 (5 MG)
DIN 02248088 (10 MG)
DIN 02248089 (20 MG)
Erectile
Dysfunction (ED)
NOTE:
If no ED clause:
not eligible.
Treatment of erectile dysfunction (ED) in men (18
years of age or older):
Organic erectile dysfunction (e.g. , diabetes
related, vascular related)
Erectile dysfunction with neurological cause
(e.g., spinal cord injury (SCI), nerve damage
as a result of a prostatectomy or TURP)
Drug-induced erectile dysfunction where it
would be inappropriate to alter the dosage or to
discontinue the use of the drug in question
Mixed psychogenic/organic erectile
dysfunction
1 year
Or
Indefinite, if
annual
ceiling
1 year
6
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
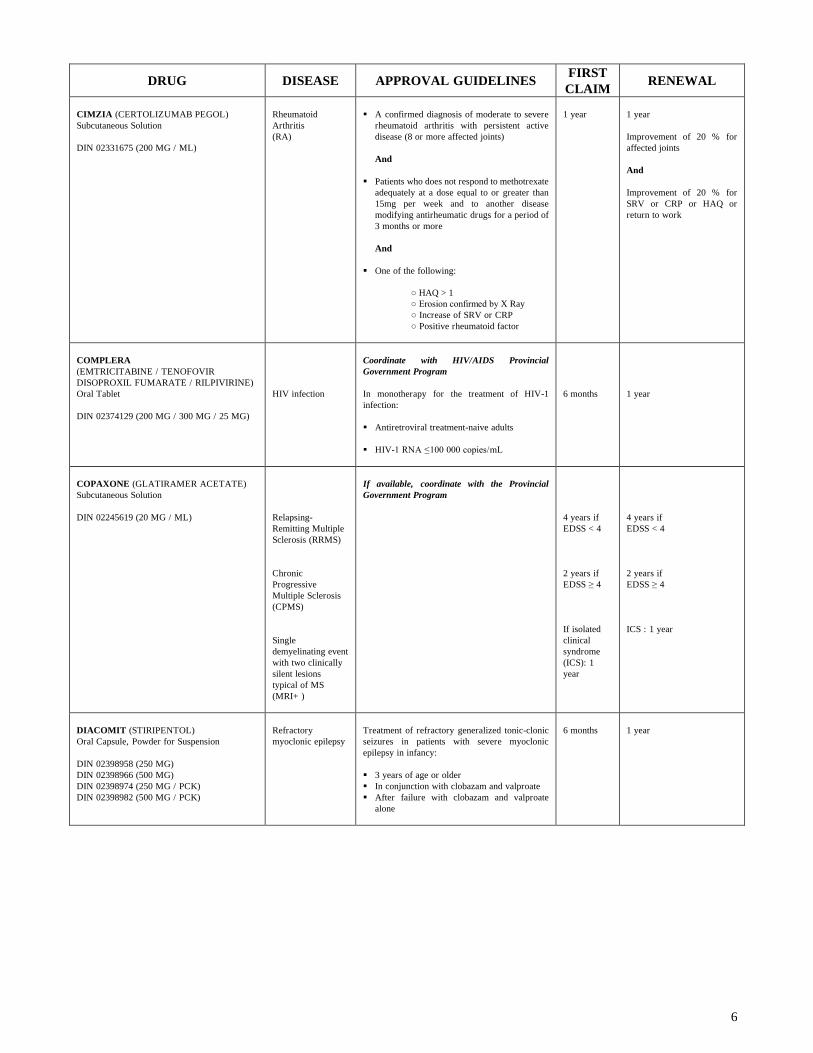
CIMZIA (CERTOLIZUMAB PEGOL)
Subcutaneous Solution
DIN 02331675 (200 MG / ML)
Rheumatoid
Arthritis
(RA)
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
1 year
1 year
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or HAQ or
return to work
COMPLERA
(EMTRICITABINE / TENOFOVIR
DISOPROXIL FUMARATE / RILPIVIRINE)
Oral Tablet
DIN 02374129 (200 MG / 300 MG / 25 MG)
HIV infection
Coordinate with HIV/AIDS Provincial
Government Program
In monotherapy for the treatment of HIV-1
infection:
Antiretroviral treatment-naive adults
HIV-1 RNA ≤ 100 000 copies/mL
6 months
1 year
COPAXONE (GLATIRAMER ACETATE)
Subcutaneous Solution
DIN 02245619 (20 MG / ML)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
Chronic
Progressive
Multiple Sclerosis
(CPMS)
Single
demyelinating event
with two clinically
silent lesions
typical of MS
(MRI+ )
If available, coordinate with the Provincial
Government Program
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
If isolated
clinical
syndrome
(ICS): 1
year
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
ICS : 1 year
DIACOMIT (STIRIPENTOL)
Oral Capsule, Powder for Suspension
DIN 02398958 (250 MG)
DIN 02398966 (500 MG)
DIN 02398974 (250 MG / PCK)
DIN 02398982 (500 MG / PCK)
Refractory
myoclonic epilepsy
Treatment of refractory generalized tonic-clonic
seizures in patients with severe myoclonic
epilepsy in infancy:
3 years of age or older
In conjunction with clobazam and valproate
After failure with clobazam and valproate
alone
6 months
1 year

7
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
ENBREL (ETANERCEPT)
Subcutaneous Solution
DIN 02274728 (50 MG / ML)
DIN 02242903 (25 MG)
Rheumatoid
Arthritis
(RA)
Juvenile Idiopathic
Arthritis (JIA)
Psoriatic Arthritis
(PA)
Ankylosing
Spondylitis (AS)
Chronic moderate
to severe plaque
psoriasis
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
4 years of age or older
5 or more affected joints and failure or
contraindications to methotrexate and to
another disease modifiying antirheumatic drugs
for a period of 3 months or more
0.8mg/kg (max 50mg) sc every week
A confirmed diagnosis of moderate to severe
psoriatic arthritis with persistent and active
disease (more than 3 affected joints)
Failure or contraindications to methotrexate
and to another disease modifiying
antirheumatic drugs for a period of 3 months
or more
HAQ > 1
No response to NSAIDs
BASDAI score ≥ 4
Treatment of adult patients with chronic
moderate to severe plaque psoriasis who are
candidates for systemic therapy or phototherapy:
No response, contraindications, intolerance or
inaccessibility to phototherapy
18 years of age or older
Treated by a dermatologist
Failure (or inappropriate) to systemic therapy
by two of the following antipsoriatic agents:
methotrexate, cyclosporine or acitretin
Psoriasis Area Severtiy Index (PASI) ≥10 or
extensive plaques on the face, the palms of the
hands, the soles of the feet or the genital area
And
Dermatology Life Quality Index (DLQI) ≥10
1 year
1 year
1 year
1 year
4 months
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or HAQ or
return to work
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or improvement
of CHAQ or return to school
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work
2 years
A 2.2 points diminution for
the BASDI score (or 50%) or
return to work
1 year
Improvement of 75% for the
PASI score
Or
Improvement of 50% for the
PASI score and a 5 points
improvement for DLQI
Or
Significant improvement of
lesions on the face, the palms
of the hands, the soles of the
feet or the genital area

8
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
EPREX (EPOETINE ALFA)
Intravenous, Subcutaneous Solution
DIN 02243239 (20000 IU / 0.5 ML)
DIN 02288680 (30000 IU / 0.75 ML)
DIN 02231587 (10000 IU / ML)
DIN 02126591 (10000 IU / ML)
DIN 02231583 (1000 IU / 0.5 ML)
DIN 02231584 (2000 IU / 0.5 ML)
DIN 02126575 (2000 IU / ML)
DIN 02231585 (3000 IU / 0.3 ML)
DIN 02240722 (40000 IU / ML)
DIN 02231586 (4000 IU / 0.4 ML)
DIN 02126583 (4000 IU / ML)
DIN 02243400 (5000 IU / 0.5 ML)
DIN 02243401 (6000 IU / 0.6 ML)
Anemia of Chronic
Renal Failure /
Dialysis
Anemia in HIV-
infected Patients
Anemia due to
chemotherapy
Chronic non-
hemolytic anemia*
If available, coordinate with the Provincial
Government Program
Treatment of anemia associated with chronic renal
failure, including patients on dialysis and patients
not on dialysis with Hb ˂ 100g/L
Treatment of transfusion-dependent anemia
related to therapy with zidovudine in HIV-
infected patients:
Endogenous serum erythropoietin level is ≤500
mU/mL and when patients are receiving a dose
of zidovudine ≤4200 mg/week
Treatment of anemia due to chemotherapy in
patients with non-myeloid malignancies
Treatment of symptomatic non-hemolytic anemia
not caused by iron deficiency, folic acid or
vitamin B12 for non cancerous persons whose
hemoglobin level is ˂ 100 g//L *
*: Quebec only, according to Quebec Prescription
Drug Plan
Indefinite
Indefinite
Indefinite
Indefinite
N/A
N/A
N/A
N/A
ERIVEDGE (VISMODEGIB)
Oral Capsule
DIN 02409267 (150MG)
Basal cell
carcinoma
Treatment of basal cell carcinoma:
18 years of age or older
Matastatic
Or
Advanced basal cell carcinoma inappropriate
for surgery
or radiotherapy
Confirmed by biopsy
PPG-E
4 months
6 months
If response to treatment
(decrease of at least 30% of
the size of the tumour and
stabilisation or a subsequent
improvement)
Note: Treatment to follow
until progression of disease or
unacceptable toxic reactions
ESBRIET (PIRFENIDONE)
Oral Capsule
DIN 02393751 (267 MG)
Idiopathic
Pulmonary Fibrosis
(IPF)
Treatment of mild to moderate idiopathic
pulmonary fibrosis (IPF):
18 years of age or older
Prescribed by a pulmonologist or a specialist
physicians experienced in the diagnosis and
treatment of IFP
Mild to moderate stage
Diagnosis confirmed by bronchoscopy and/or
tomography
6 months
6 months
Well-tolerated medication
Clinical condition of the
patient to be evaluated
(disease evolution)
9
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
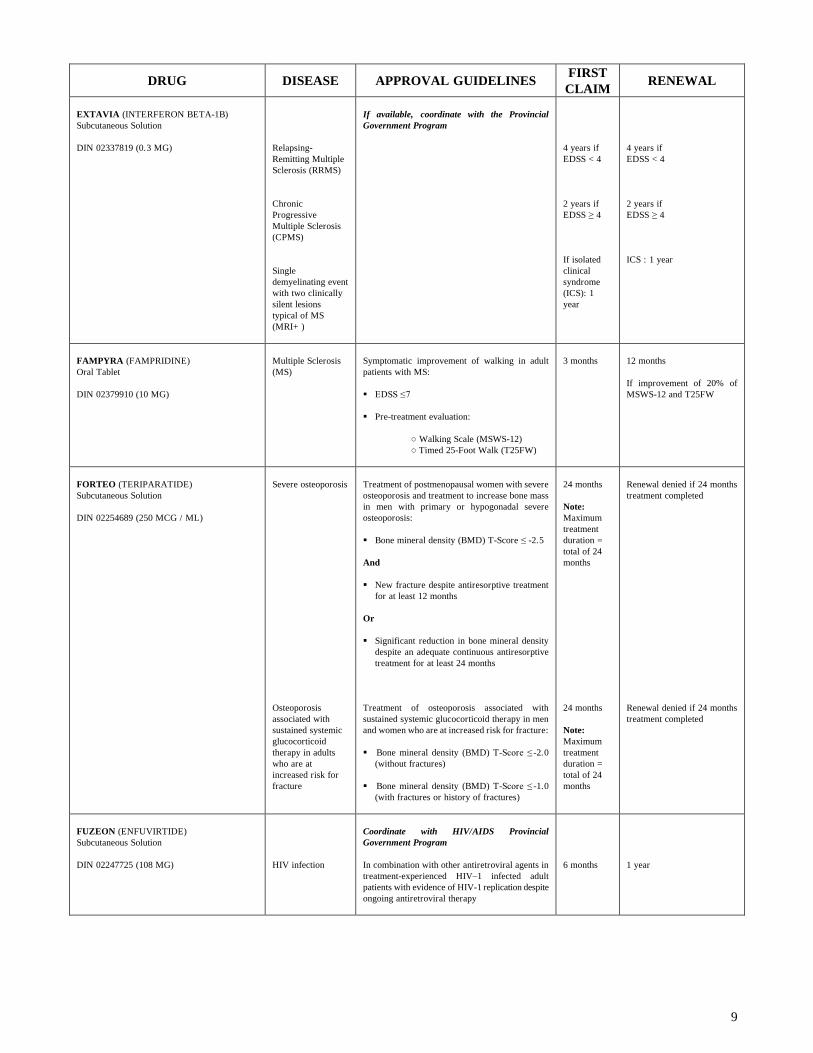
EXTAVIA (INTERFERON BETA-1B)
Subcutaneous Solution
DIN 02337819 (0.3 MG)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
Chronic
Progressive
Multiple Sclerosis
(CPMS)
Single
demyelinating event
with two clinically
silent lesions
typical of MS
(MRI+ )
If available, coordinate with the Provincial
Government Program
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
If isolated
clinical
syndrome
(ICS): 1
year
4 years if
EDSS < 4
2 years if
EDSS ≥ 4
ICS : 1 year
FAMPYRA (FAMPRIDINE)
Oral Tablet
DIN 02379910 (10 MG)
Multiple Sclerosis
(MS)
Symptomatic improvement of walking in adult
patients with MS:
EDSS ≤ 7
Pre-treatment evaluation:
○ Walking Scale (MSWS-12)
○ Timed 25-Foot Walk (T25FW)
3 months
12 months
If improvement of 20% of
MSWS-12 and T25FW
FORTEO (TERIPARATIDE)
Subcutaneous Solution
DIN 02254689 (250 MCG / ML)
Severe osteoporosis
Osteoporosis
associated with
sustained systemic
glucocorticoid
therapy in adults
who are at
increased risk for
fracture
Treatment of postmenopausal women with severe
osteoporosis and treatment to increase bone mass
in men with primary or hypogonadal severe
osteoporosis:
Bone mineral density (BMD) T-Score ≤ -2.5
And
New fracture despite antiresorptive treatment
for at least 12 months
Or
Significant reduction in bone mineral density
despite an adequate continuous antiresorptive
treatment for at least 24 months
Treatment of osteoporosis associated with
sustained systemic glucocorticoid therapy in men
and women who are at increased risk for fracture:
Bone mineral density (BMD) T-Score ≤ -2.0
(without fractures)
Bone mineral density (BMD) T-Score ≤ -1.0
(with fractures or history of fractures)
24 months
Note:
Maximum
treatment
duration =
total of 24
months
24 months
Note:
Maximum
treatment
duration =
total of 24
months
Renewal denied if 24 months
treatment completed
Renewal denied if 24 months
treatment completed
FUZEON (ENFUVIRTIDE)
Subcutaneous Solution
DIN 02247725 (108 MG)
HIV infection
Coordinate with HIV/AIDS Provincial
Government Program
In combination with other antiretroviral agents in
treatment-experienced HIV–1 infected adult
patients with evidence of HIV-1 replication despite
ongoing antiretroviral therapy
6 months
1 year
10
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
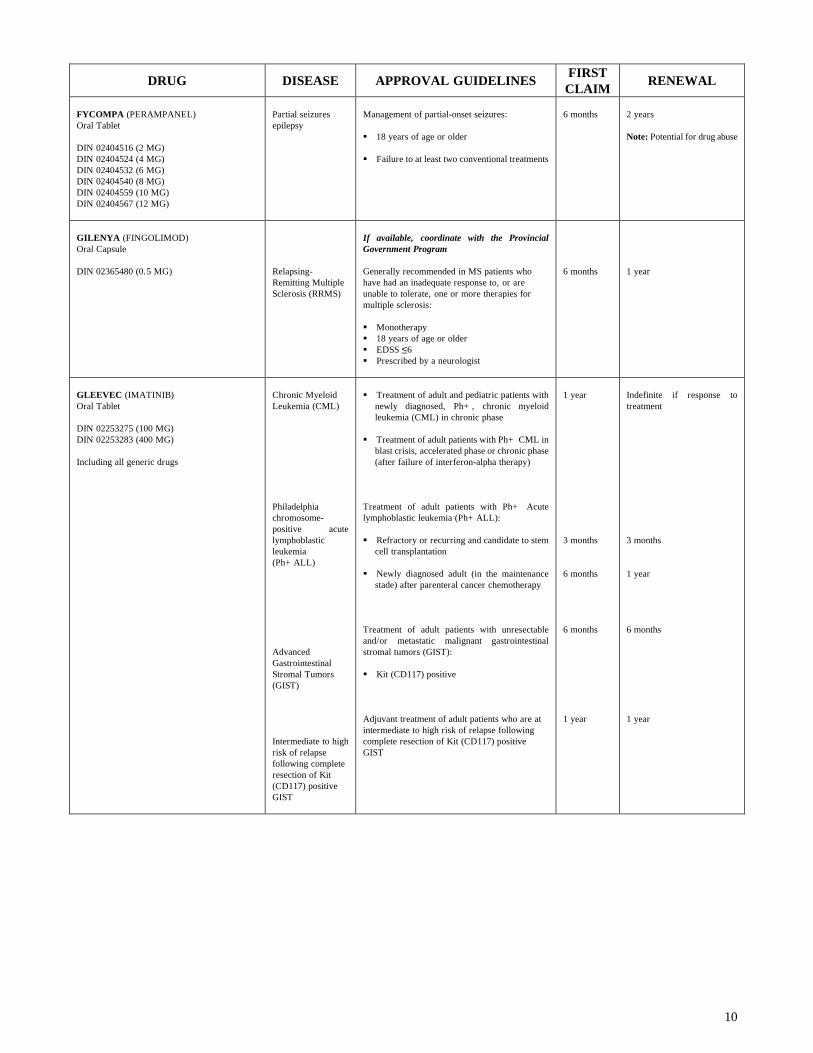
FYCOMPA (PERAMPANEL)
Oral Tablet
DIN 02404516 (2 MG)
DIN 02404524 (4 MG)
DIN 02404532 (6 MG)
DIN 02404540 (8 MG)
DIN 02404559 (10 MG)
DIN 02404567 (12 MG)
Partial seizures
epilepsy
Management of partial-onset seizures:
18 years of age or older
Failure to at least two conventional treatments
6 months
2 years
Note: Potential for drug abuse
GILENYA (FINGOLIMOD)
Oral Capsule
DIN 02365480 (0.5 MG)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
If available, coordinate with the Provincial
Government Program
Generally recommended in MS patients who
have had an inadequate response to, or are
unable to tolerate, one or more therapies for
multiple sclerosis:
Monotherapy
18 years of age or older
EDSS ≤ 6
Prescribed by a neurologist
6 months
1 year
GLEEVEC (IMATINIB)
Oral Tablet
DIN 02253275 (100 MG)
DIN 02253283 (400 MG)
Including all generic drugs
Chronic Myeloid
Leukemia (CML)
Philadelphia
chromosome-
positive acute
lymphoblastic
leukemia
(Ph+ ALL)
Advanced
Gastrointestinal
Stromal Tumors
(GIST)
Intermediate to high
risk of relapse
following complete
resection of Kit
(CD117) positive
GIST
Treatment of adult and pediatric patients with
newly diagnosed, Ph+ , chronic myeloid
leukemia (CML) in chronic phase
Treatment of adult patients with Ph+ CML in
blast crisis, accelerated phase or chronic phase
(after failure of interferon-alpha therapy)
Treatment of adult patients with Ph+ Acute
lymphoblastic leukemia (Ph+ ALL):
Refractory or recurring and candidate to stem
cell transplantation
Newly diagnosed adult (in the maintenance
stade) after parenteral cancer chemotherapy
Treatment of adult patients with unresectable
and/or metastatic malignant gastrointestinal
stromal tumors (GIST):
Kit (CD117) positive
Adjuvant treatment of adult patients who are at
intermediate to high risk of relapse following
complete resection of Kit (CD117) positive
GIST
1 year
3 months
6 months
6 months
1 year
Indefinite if response to
treatment
3 months
1 year
6 months
1 year

11
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
HUMATROPE (SOMATROPIN)
Intramuscular, Subcutaneous Solution
DIN 02243077 (6 MG)
DIN 02243078 (12 MG)
DIN 02243079 (24 MG)
DIN 00745626 (1 MG / ML)
Growth hormone
deficiency
Turner syndrome
If available, coordinate with the Provincial
Government Program
Pediatric patients:
Treatment of pediatric patients who have
growth failure due to an inadequate secretion
of normal endogenous growth hormone or to a
renal failure
Should not be used for treatment of pediatric
patients with closed epiphyses
Treatment covered until 15 years old of bone
age for girls and 16 years old of bone age for
boys and growth rate > 2 cm / year
Adult patients:
For replacement of endogenous growth hormone
in adults with growth hormone deficiency if:
GH Peak ≤ 5 mcg/L
And
Adult Onset: Patients must have GHD, either
alone or associated with multiple hormone
deficiencies (hypopituitarism), as a result of
pituitary disease, hypothalamic disease,
surgery, radiation therapy, or trauma
Or
Childhood-onset: if GHD during childhood and
confirmed as an adult
Long-term treatment of idiopathic short stature
defined by height at least 2.25 standard
deviation scores (SDS) below the mean for age
and sex
Treatment of short stature or growth failure in
children with SHOX deficiency
Long-term treatment of short stature
associated with Turner syndrome
Should not be used for treatment of pediatric
patients with closed epiphyses
1 year
1 year
1 year
1 year
1 year
1 year

12
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
HUMIRA (ADALIMUMAB)
Subcutaneous Solution
DIN 02258595 (40 MG / 0.8 ML)
Rheumatoid
Arthritis
(RA)
Psoriatic Arthritis
(PA)
Ankylosing
Spondylitis (AS)
Crohn' s disease
Chronic moderate
to severe plaque
psoriasis
Juvenile Idiopathic
Arthritis (JIA)
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
A confirmed diagnosis of moderate to severe
psoriatic arthritis with persistent and active
disease (more than 3 affected joints)
Failure or contraindications to methotrexate
and to another disease modifiying
antirheumatic drugs for a period of 3 months
or more
HAQ > 1
No response to NSAIDs
BASDAI score ≥ 4
Treatment of adult patients who have had an
inadequate response to conventional therapy
(including corticosteroids and/or
immunosuppressants), no response, intolerant or
contraindications
Treatment of adult patients with chronic
moderate to severe plaque psoriasis who are
candidates for systemic therapy or phototherapy:
No response, contraindications, intolerance or
inaccessibility to phototherapy
18 years of age or older
Treated by a dermatologist
Failure (or inappropriate) to systemic therapy
by two of the following antipsoriatic agents:
methotrexate, cyclosporine or acitretin
Psoriasis Area Severtiy Index (PASI) ≥10 or
extensive plaques on the face, the palms of the
hands, the soles of the feet or the genital area
And
Dermatology Life Quality Index (DLQI) ≥10
4 years of age or older
5 or more affected joints
Failure to methotrexate as a monotherapy and
to another disease modifiying antirheumatic
drugs for a period of 3 months or more
In combination with methotrexate except if
intolerance or contraindications
24mg/m2 (max 40mg) sc every other week
1 year
1 year
1 year
1 year
4 months
1 year
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or HAQ or
return to work
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work
2 years
A 2.2 points diminution for
the BASDI score (or 50%) or
return to work
2 years
1 year
Improvement of 75% for the
PASI score
Or
Improvement of 50% for the
PASI score and a 5 points
improvement for DLQI
Or
Significant improvement of
lesions on the face, the palms
of the hands, the soles of the
feet or the genital area
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or improvement
of CHAQ or return to school
13
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
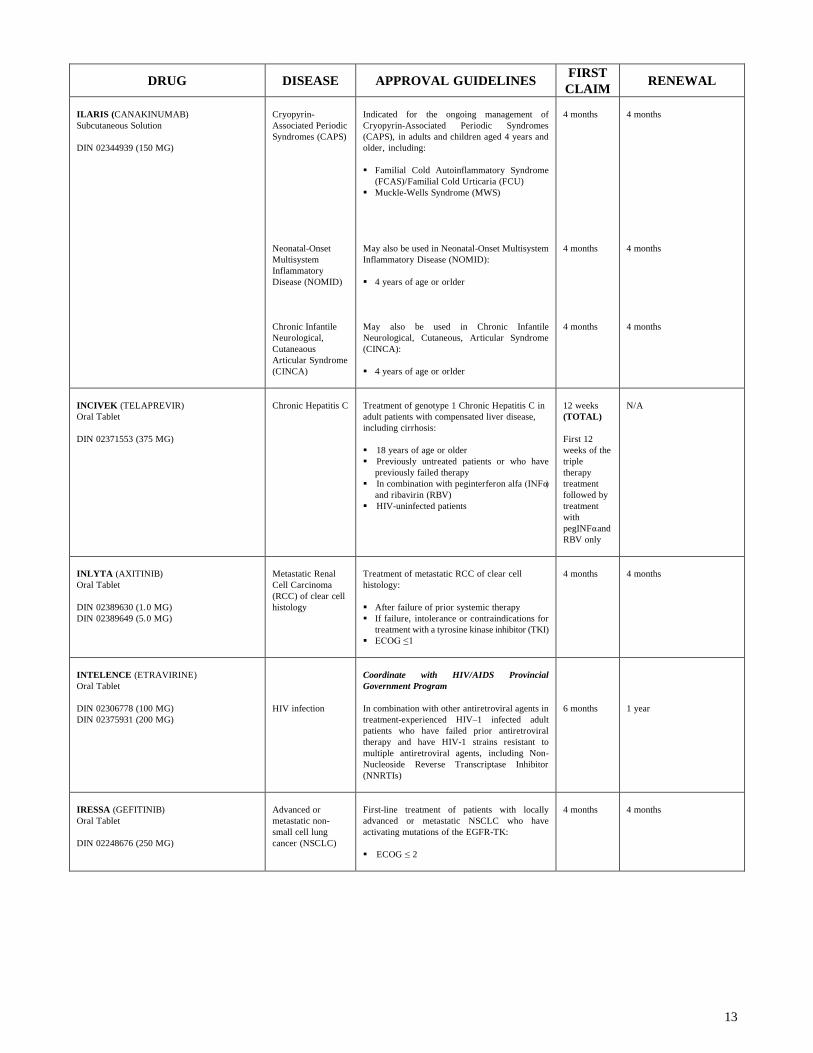
ILARIS (CANAKINUMAB)
Subcutaneous Solution
DIN 02344939 (150 MG)
Cryopyrin-
Associated Periodic
Syndromes (CAPS)
Neonatal-Onset
Multisystem
Inflammatory
Disease (NOMID)
Chronic Infantile
Neurological,
Cutaneaous
Articular Syndrome
(CINCA)
Indicated for the ongoing management of
Cryopyrin-Associated Periodic Syndromes
(CAPS), in adults and children aged 4 years and
older, including:
Familial Cold Autoinflammatory Syndrome
(FCAS)/Familial Cold Urticaria (FCU)
Muckle-Wells Syndrome (MWS)
May also be used in Neonatal-Onset Multisystem
Inflammatory Disease (NOMID):
4 years of age or orlder
May also be used in Chronic Infantile
Neurological, Cutaneous, Articular Syndrome
(CINCA):
4 years of age or orlder
4 months
4 months
4 months
4 months
4 months
4 months
INCIVEK (TELAPREVIR)
Oral Tablet
DIN 02371553 (375 MG)
Chronic Hepatitis C
Treatment of genotype 1 Chronic Hepatitis C in
adult patients with compensated liver disease,
including cirrhosis:
18 years of age or older
Previously untreated patients or who have
previously failed therapy
In combination with peginterferon alfa (INFα)
and ribavirin (RBV)
HIV-uninfected patients
12 weeks
(TOTAL)
First 12
weeks of the
triple
therapy
treatment
followed by
treatment
with
pegINFα and
RBV only
N/A
INLYTA (AXITINIB)
Oral Tablet
DIN 02389630 (1.0 MG)
DIN 02389649 (5.0 MG)
Metastatic Renal
Cell Carcinoma
(RCC) of clear cell
histology
Treatment of metastatic RCC of clear cell
histology:
After failure of prior systemic therapy
If failure, intolerance or contraindications for
treatment with a tyrosine kinase inhibitor (TKI)
ECOG ≤ 1
4 months
4 months
INTELENCE (ETRAVIRINE)
Oral Tablet
DIN 02306778 (100 MG)
DIN 02375931 (200 MG)
HIV infection
Coordinate with HIV/AIDS Provincial
Government Program
In combination with other antiretroviral agents in
treatment-experienced HIV–1 infected adult
patients who have failed prior antiretroviral
therapy and have HIV-1 strains resistant to
multiple antiretroviral agents, including Non-
Nucleoside Reverse Transcriptase Inhibitor
(NNRTIs)
6 months
1 year
IRESSA (GEFITINIB)
Oral Tablet
DIN 02248676 (250 MG)
Advanced or
metastatic non-
small cell lung
cancer (NSCLC)
First-line treatment of patients with locally
advanced or metastatic NSCLC who have
activating mutations of the EGFR-TK:
ECOG ≤ 2
4 months
4 months
14
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
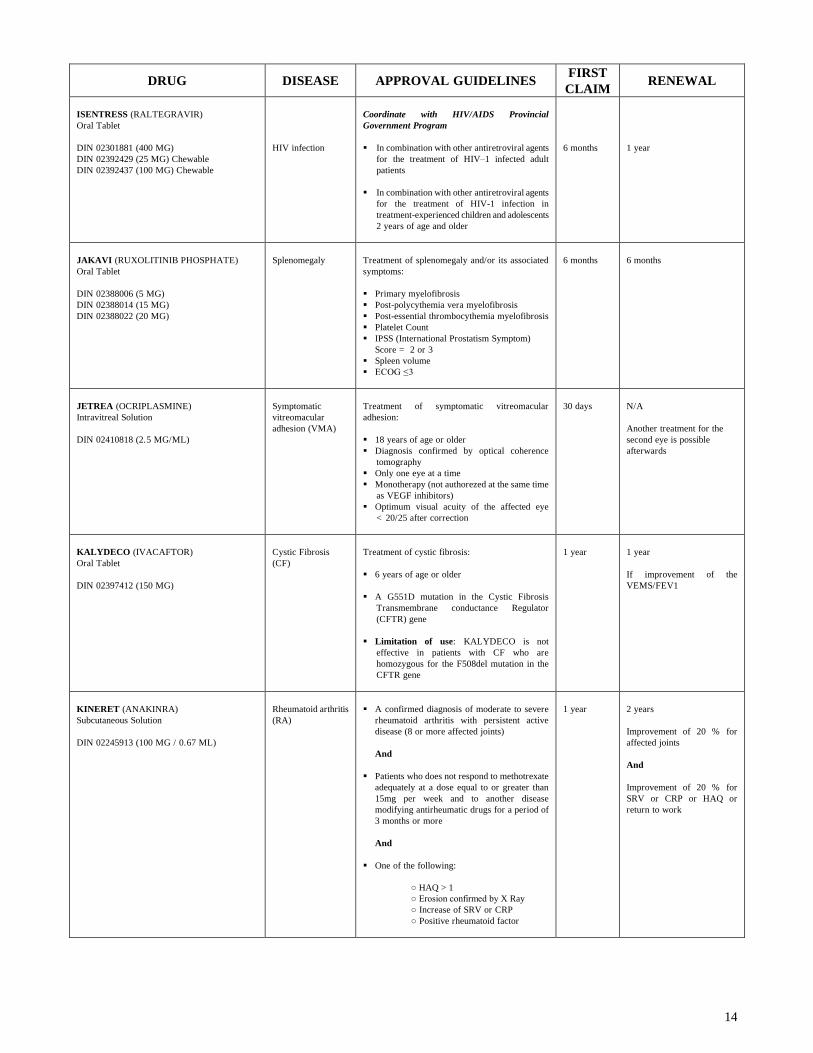
ISENTRESS (RALTEGRAVIR)
Oral Tablet
DIN 02301881 (400 MG)
DIN 02392429 (25 MG) Chewable
DIN 02392437 (100 MG) Chewable
HIV infection
Coordinate with HIV/AIDS Provincial
Government Program
In combination with other antiretroviral agents
for the treatment of HIV–1 infected adult
patients
In combination with other antiretroviral agents
for the treatment of HIV-1 infection in
treatment-experienced children and adolescents
2 years of age and older
6 months
1 year
JAKAVI (RUXOLITINIB PHOSPHATE)
Oral Tablet
DIN 02388006 (5 MG)
DIN 02388014 (15 MG)
DIN 02388022 (20 MG)
Splenomegaly
Treatment of splenomegaly and/or its associated
symptoms:
Primary myelofibrosis
Post-polycythemia vera myelofibrosis
Post-essential thrombocythemia myelofibrosis
Platelet Count
IPSS (International Prostatism Symptom)
Score = 2 or 3
Spleen volume
ECOG ≤ 3
6 months
6 months
JETREA (OCRIPLASMINE)
Intravitreal Solution
DIN 02410818 (2.5 MG/ML)
Symptomatic
vitreomacular
adhesion (VMA)
Treatment of symptomatic vitreomacular
adhesion:
18 years of age or older
Diagnosis confirmed by optical coherence
tomography
Only one eye at a time
Monotherapy (not authorezed at the same time
as VEGF inhibitors)
Optimum visual acuity of the affected eye
< 20/25 after correction
30 days
N/A
Another treatment for the
second eye is possible
afterwards
KALYDECO (IVACAFTOR)
Oral Tablet
DIN 02397412 (150 MG)
Cystic Fibrosis
(CF)
Treatment of cystic fibrosis:
6 years of age or older
A G551D mutation in the Cystic Fibrosis
Transmembrane conductance Regulator
(CFTR) gene
Limitation of use: KALYDECO is not
effective in patients with CF who are
homozygous for the F508del mutation in the
CFTR gene
1 year
1 year
If improvement of the
VEMS/FEV1
KINERET (ANAKINRA)
Subcutaneous Solution
DIN 02245913 (100 MG / 0.67 ML)
Rheumatoid arthritis
(RA)
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
1 year
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or HAQ or
return to work

15
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
KUVAN (SAPROPTERIN)
Oral Tablet
DIN 02350580 (100 MG)
Hyperphenylalani-
nemia (HPA)
Indicated to reduce blood phenylalanine (Phe)
levels in patients with HPA due to
tetrahydrobiopterin-(BH4)-responsive
Phenylketonuria (PKU)
In conjunction with a Phe-restricted diet
4 years of age or older
3 months
3 months
LEVITRA (VARDENAFIL)
Oral Tablet
DIN 02250462 (5 MG)
DIN 02250470 (10 MG)
DIN 02250489 (20 MG)
Erectile
Dysfunction (ED)
NOTE:
If no ED
clause: not
eligible.
Treatment of erectile dysfunction (ED) in men (18
years of age or older):
Organic erectile dysfunction (e.g. , diabetes
related, vascular related)
Erectile dysfunction with neurological cause
(e.g., spinal cord injury (SCI), nerve damage
as a result of a prostatectomy or TURP)
Drug-induced erectile dysfunction where it
would be inappropriate to alter the dosage or to
discontinue the use of the drug in question
Mixed psychogenic/organic erectile
dysfunction
1 year
Or
Indefinite, if
annual
ceiling
1 year
LEVULAN (AMINOLEVULINIC ACID)
Topical Solution
DIN 02243933 (20%)
Actinic keratoses
History of basocellular carcinoma confirmed
by biopsy
No response to conventional therapy
In combination with photodynamic therapy
(PDT)
Sold by a licensed pharmacist
3 months
3 months
LUCENTIS ( RANIBIZUMAB)
Intravitreal Solution
DIN 02296810 (10 MG / ML)
Neovascular (wet)
age-related macular
degeneration
(AMD)
Macular edema
secondary to retinal
vein occlusion
(RVO)
Diabetic Macular
Edema (DME)
If available, coordinate with the Provincial
Government Program
Validate the administration site: if in an hospital
setting, must be free of charge
For all disease:
Sold by a licensed pharmacist
Maximum one injection per month per eye
Treatment of neovascular (wet) AMD
Treatment of visual impairment due to macular
edema secondary to retinal vein occlusion (RVO)
Treatment of visual impairment due to diabetic
macular edema (DME)
1 year
6 months
6 months
Renewal is permitted if
demonstrated by clinical
beneficial effect (stabilisation
or improvement of the
medical condition confirmed
by a medical examination)
1 year
1 year
1 year
MEKINIST
(TRAMETINIB)
Oral Tablet
DIN 02409623 (0.5 MG)
DIN 02409658 (2.0 MG)
Unresectable or
metastatic
melanoma
Treatment of unresectable or metastatic
melanoma:
Stage
BRAF V600 mutation-positive confirmed by
a validated BRAF V600 test
Monotherapy
ECOG ≤ 1
* Not covered if failure with Zelboraf
4 months
4 months

16
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
METVIX
(METHYL AMINOLEVULINATE)
Topical Cream
DIN 02323273 (168 MG / G)
Primary superficial
basal cell
carcinoma
Treatment of primary superficial basal cell
carcinoma:
Confirmed by biopsy
In combination with photodynamic therapy
(PDT)
No response to conventional therapy
Sold by a licensed pharmacist
4 months
N/A
NEULASTA (PEGFILGRASTIM)
Subcutaneous Solution
DIN 02249790 (10 MG / ML)
Neutropenia
If available, coordinate with the Provincial
Government Program
Indicated to decrease the incidence of
infection, as manifested by febrile neutropenia,
in patients with non-myeloid malignancies
receiving myelosuppressive anti-neoplastic
drugs
1 year
1 year
NEUPOGEN (FILGRASTIM)
Intravenous, Subcutaneous Solution
DIN 01968017 (300 MCG/ ML)
Neutropenia
If available, coordinate with the Provincial
Government Program
Indicated for the treatment of the following:
Cancer patients receiving myelosuppressive
chemotherapy
Patients with acute myeloid leukemia
Cancer patients receiving myeloablative
chemotherapy followed by bone marrow
transplantation
Cancer patients undergoing peripheral blood
progenitor cell (PBPC) collection and therapy
Patients with severe chronic neutropenia
(SCN): congenital, cyclic or idiopathic
Patients with HIV Infection: to maintain a
normal absolute neutrophil count (ANC) (e.g.,
between 2× 109 and 10× 109/L)
Note: Not a pre-authorization drug for Quebec
residents.
1 year
1 year
NEXAVAR (SORAFENIB)
Oral Tablet
DIN 02284227 (200 MG)
Renal Cell
Carcinoma (RCC)
(clear cell)
Hepatocellular
Carcinoma (HCC)
Second-line treatment for locally advanced /
metastatic RCC (clear cell):
After failure of cytokine-based therapy or
unsuitable for cytokine-based therapy
ECOG ≤1
Treatment of patients with unresectable
hepatocellular carcinoma (HCC):
ECOG ≤ 2
Child-Pugh score “A”
5 months
5 months
5 months
5 months
NPLATE (ROMIPLOSTIM)
Subcutaneous Solution
DIN 02322854 (250 MCG / 0.5 ML)
DIN 02322862 (500 MCG / ML)
Chronic Immune
(idiopathic)
Thrombocytopenic
Purpura (ITP)
Indicated to increase the platelet levels in adult
patients with ITP:
Who are non-splenectomized and have had an
inadequate response or are intolerant to
corticosteroids and/or immunoglobulins
Or
Who are splenectomized and have had an
inadequate response to splenectomy
6 months
1 year
17
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
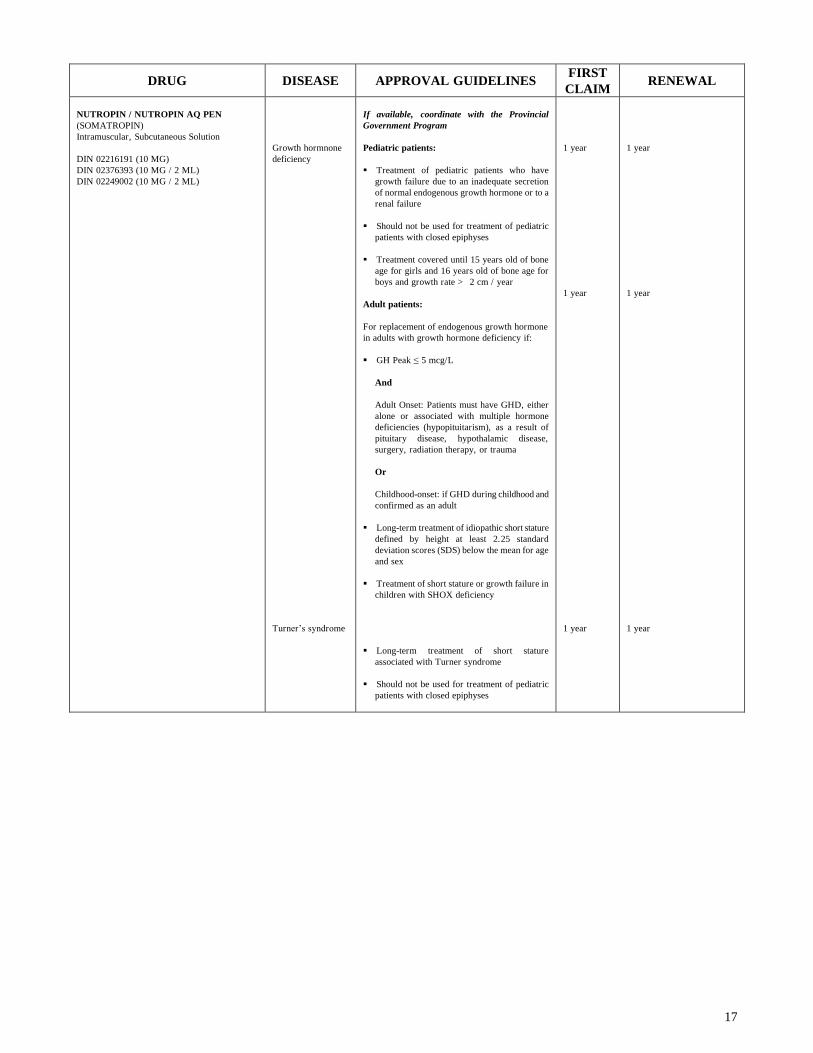
NUTROPIN / NUTROPIN AQ PEN
(SOMATROPIN)
Intramuscular, Subcutaneous Solution
DIN 02216191 (10 MG)
DIN 02376393 (10 MG / 2 ML)
DIN 02249002 (10 MG / 2 ML)
Growth hormnone
deficiency
Turner’s syndrome
If available, coordinate with the Provincial
Government Program
Pediatric patients:
Treatment of pediatric patients who have
growth failure due to an inadequate secretion
of normal endogenous growth hormone or to a
renal failure
Should not be used for treatment of pediatric
patients with closed epiphyses
Treatment covered until 15 years old of bone
age for girls and 16 years old of bone age for
boys and growth rate > 2 cm / year
Adult patients:
For replacement of endogenous growth hormone
in adults with growth hormone deficiency if:
GH Peak ≤ 5 mcg/L
And
Adult Onset: Patients must have GHD, either
alone or associated with multiple hormone
deficiencies (hypopituitarism), as a result of
pituitary disease, hypothalamic disease,
surgery, radiation therapy, or trauma
Or
Childhood-onset: if GHD during childhood and
confirmed as an adult
Long-term treatment of idiopathic short stature
defined by height at least 2.25 standard
deviation scores (SDS) below the mean for age
and sex
Treatment of short stature or growth failure in
children with SHOX deficiency
Long-term treatment of short stature
associated with Turner syndrome
Should not be used for treatment of pediatric
patients with closed epiphyses
1 year
1 year
1 year
1 year
1 year
1 year

18
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
OMNITROPE (SOMATROPIN)
Subcutaneous Solution
DIN 02325063 (5 MG / 1.5 ML)
DIN 02325071 (10 MG / 1.5 ML)
Growth hormone
deficiency
If available, coordinate with the Provincial
Government Program
Pediatric patients:
Treatment of pediatric patients who have
growth failure due to an inadequate secretion
of normal endogenous growth hormone or to a
renal failure
Should not be used for treatment of pediatric
patients with closed epiphyses
Treatment covered until 15 years old of bone
age for girls and 16 years old of bone age for
boys and growth rate > 2 cm / year
Adult patients:
For replacement of endogenous growth hormone
in adults with growth hormone deficiency if:
GH Peak ≤ 5 mcg/L
And
Adult Onset: Patients must have GHD, either
alone or associated with multiple hormone
deficiencies (hypopituitarism), as a result of
pituitary disease, hypothalamic disease,
surgery, radiation therapy, or trauma
Or
Childhood-onset: if GHD during childhood and
confirmed as an adult
Long-term treatment of idiopathic short stature
defined by height at least 2.25 standard
deviation scores (SDS) below the mean for age
and sex
Treatment of short stature or growth failure in
children with SHOX deficiency
1 year
1 year
1 year
1 year

19
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
ORENCIA (ABATACEPT)
Intravenous Solution
DIN 02282097 (250 MG)
Subcutaneous Solution
DIN 02402475 (125 MG)
Rheumatoid
Arthritis
(RA)
Juvenile Arthritis
(JA)
DIN 02282097
only
Validate the administration site: if in a hospital
setting, must be free of charge
(DIN 02282097 only)
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more or an Anti-TNF.
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
6 years of age or older
5 or more affected joints
Failure to methotrexate as a monotherapy and
to another disease modifiying antirheumatic
drugs for a period of 3 months or more
< 75kg : 10mg/kg/dose
1 year
1 year
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or HAQ or
return to work
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or improvement
of CHAQ or return to school
OZURDEX (DEXAMETHASONE)
Intravitreal Implant
DIN 02363445 (0.7 MG)
Macular edema
following central
retinal vein
occlusion (CRVO)
Non-infectious
uveitis
Treatment of macular edema following central
retinal vein occlusion (CRVO):
18 years of age or older
Sold by a licensed pharmacist
No simultaneous bilateral treatment
Maximum of two injections and an interval of
6 months between the two
Prescribed by an ophthalmologist
Treatment of non-infectious uveitis affecting the
posterior segment of the eye:
18 years of age or older
Sold by a licensed pharmacist
No simultaneous bilateral treatment
Maximum of two injections and an interval of
6 months between the two
Prescribed by an ophthalmologist
1 year
(max 2
implants /
year / eye)
1 year
(max 2
implants /
year / eye)
N/A
N/A
20
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
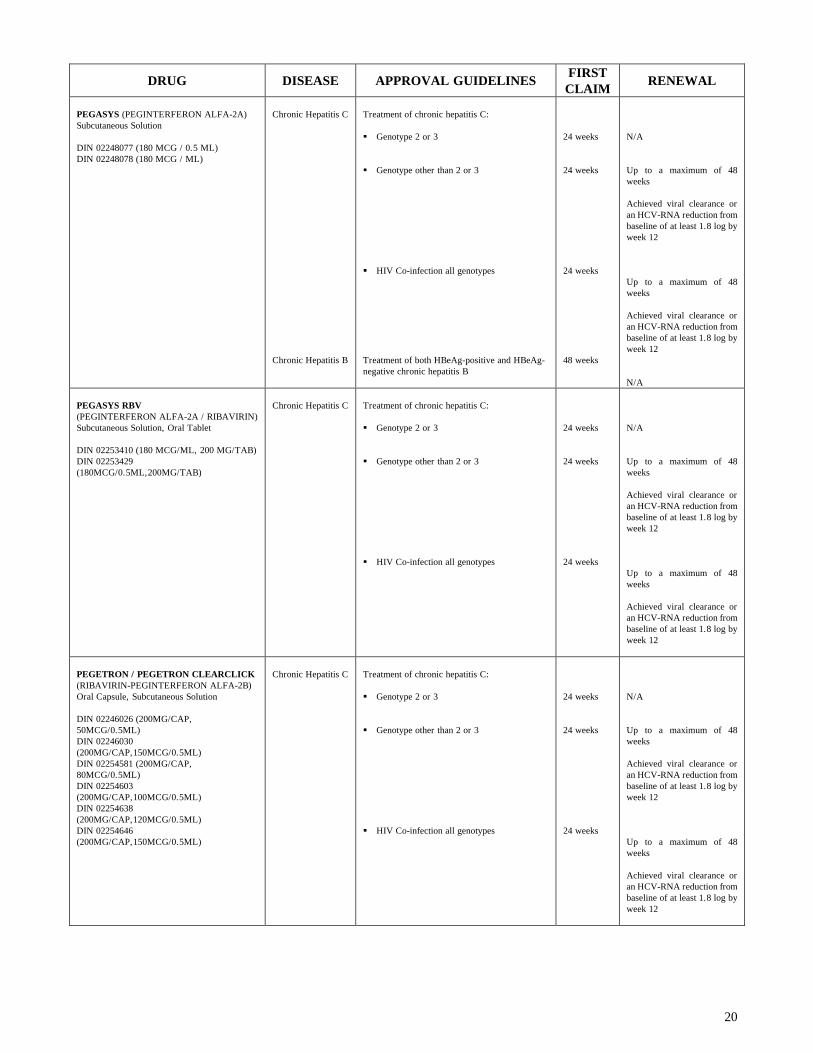
PEGASYS (PEGINTERFERON ALFA-2A)
Subcutaneous Solution
DIN 02248077 (180 MCG / 0.5 ML)
DIN 02248078 (180 MCG / ML)
Chronic Hepatitis C
Chronic Hepatitis B
Treatment of chronic hepatitis C:
Genotype 2 or 3
Genotype other than 2 or 3
HIV Co-infection all genotypes
Treatment of both HBeAg-positive and HBeAg-
negative chronic hepatitis B
24 weeks
24 weeks
24 weeks
48 weeks
N/A
Up to a maximum of 48
weeks
Achieved viral clearance or
an HCV-RNA reduction from
baseline of at least 1.8 log by
week 12
Up to a maximum of 48
weeks
Achieved viral clearance or
an HCV-RNA reduction from
baseline of at least 1.8 log by
week 12
N/A
PEGASYS RBV
(PEGINTERFERON ALFA-2A / RIBAVIRIN)
Subcutaneous Solution, Oral Tablet
DIN 02253410 (180 MCG/ML, 200 MG/TAB)
DIN 02253429
(180MCG/0.5ML,200MG/TAB)
Chronic Hepatitis C
Treatment of chronic hepatitis C:
Genotype 2 or 3
Genotype other than 2 or 3
HIV Co-infection all genotypes
24 weeks
24 weeks
24 weeks
N/A
Up to a maximum of 48
weeks
Achieved viral clearance or
an HCV-RNA reduction from
baseline of at least 1.8 log by
week 12
Up to a maximum of 48
weeks
Achieved viral clearance or
an HCV-RNA reduction from
baseline of at least 1.8 log by
week 12
PEGETRON / PEGETRON CLEARCLICK
(RIBAVIRIN-PEGINTERFERON ALFA-2B)
Oral Capsule, Subcutaneous Solution
DIN 02246026 (200MG/CAP,
50MCG/0.5ML)
DIN 02246030
(200MG/CAP,150MCG/0.5ML)
DIN 02254581 (200MG/CAP,
80MCG/0.5ML)
DIN 02254603
(200MG/CAP,100MCG/0.5ML)
DIN 02254638
(200MG/CAP,120MCG/0.5ML)
DIN 02254646
(200MG/CAP,150MCG/0.5ML)
Chronic Hepatitis C
Treatment of chronic hepatitis C:
Genotype 2 or 3
Genotype other than 2 or 3
HIV Co-infection all genotypes
24 weeks
24 weeks
24 weeks
N/A
Up to a maximum of 48
weeks
Achieved viral clearance or
an HCV-RNA reduction from
baseline of at least 1.8 log by
week 12
Up to a maximum of 48
weeks
Achieved viral clearance or
an HCV-RNA reduction from
baseline of at least 1.8 log by
week 12
21
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
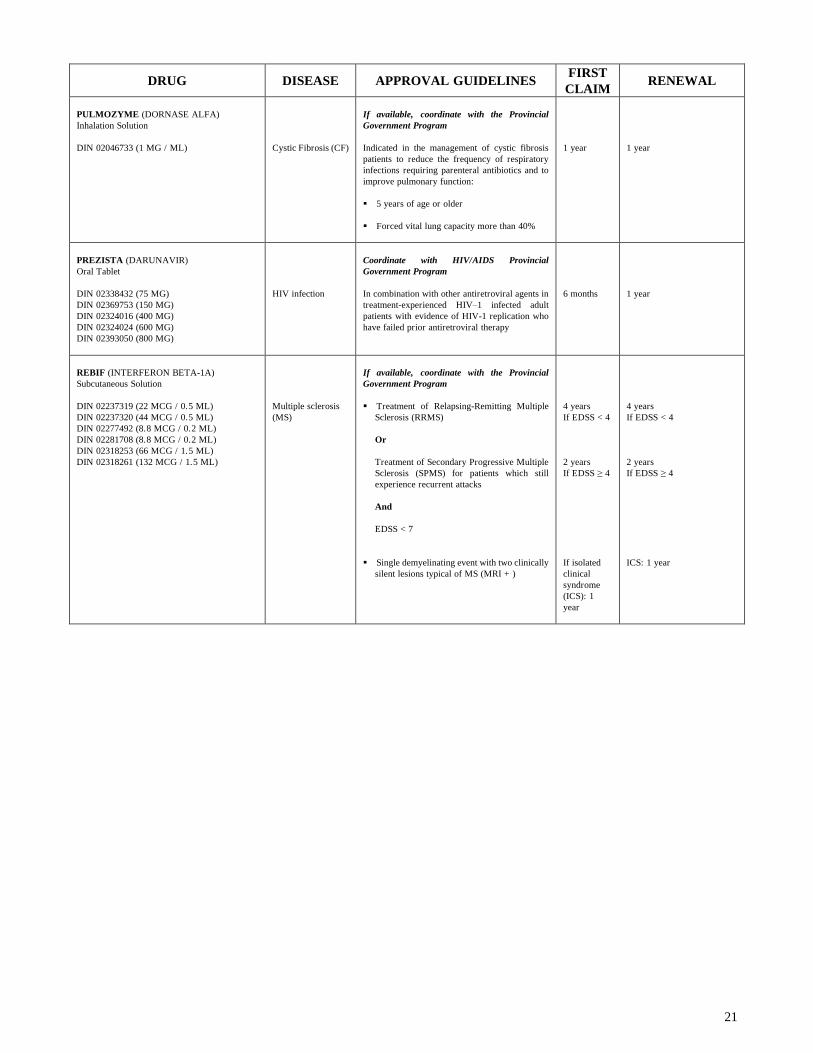
PULMOZYME (DORNASE ALFA)
Inhalation Solution
DIN 02046733 (1 MG / ML)
Cystic Fibrosis (CF)
If available, coordinate with the Provincial
Government Program
Indicated in the management of cystic fibrosis
patients to reduce the frequency of respiratory
infections requiring parenteral antibiotics and to
improve pulmonary function:
5 years of age or older
Forced vital lung capacity more than 40%
1 year
1 year
PREZISTA (DARUNAVIR)
Oral Tablet
DIN 02338432 (75 MG)
DIN 02369753 (150 MG)
DIN 02324016 (400 MG)
DIN 02324024 (600 MG)
DIN 02393050 (800 MG)
HIV infection
Coordinate with HIV/AIDS Provincial
Government Program
In combination with other antiretroviral agents in
treatment-experienced HIV–1 infected adult
patients with evidence of HIV-1 replication who
have failed prior antiretroviral therapy
6 months
1 year
REBIF (INTERFERON BETA-1A)
Subcutaneous Solution
DIN 02237319 (22 MCG / 0.5 ML)
DIN 02237320 (44 MCG / 0.5 ML)
DIN 02277492 (8.8 MCG / 0.2 ML)
DIN 02281708 (8.8 MCG / 0.2 ML)
DIN 02318253 (66 MCG / 1.5 ML)
DIN 02318261 (132 MCG / 1.5 ML)
Multiple sclerosis
(MS)
If available, coordinate with the Provincial
Government Program
Treatment of Relapsing-Remitting Multiple
Sclerosis (RRMS)
Or
Treatment of Secondary Progressive Multiple
Sclerosis (SPMS) for patients which still
experience recurrent attacks
And
EDSS < 7
Single demyelinating event with two clinically
silent lesions typical of MS (MRI + )
4 years
If EDSS < 4
2 years
If EDSS ≥ 4
If isolated
clinical
syndrome
(ICS): 1
year
4 years
If EDSS < 4
2 years
If EDSS ≥ 4
ICS: 1 year
22
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
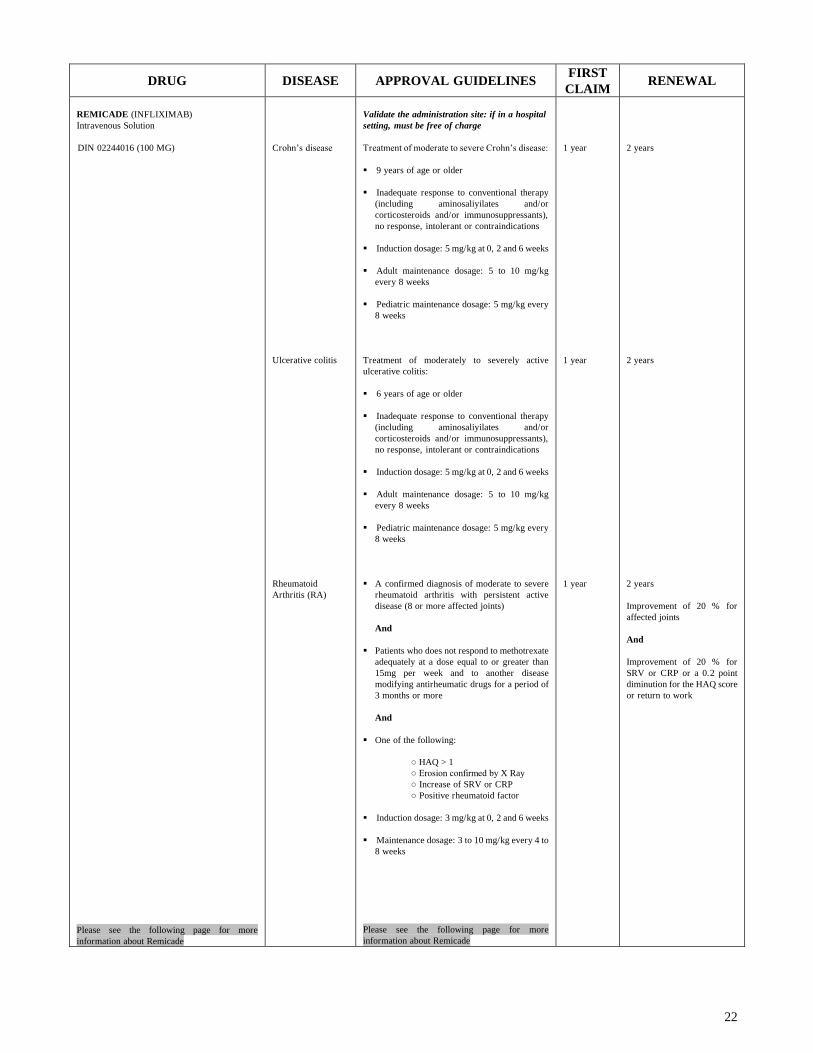
REMICADE (INFLIXIMAB)
Intravenous Solution
DIN 02244016 (100 MG)
Please see the following page for more
information about Remicade
Crohn’s disease
Ulcerative colitis
Rheumatoid
Arthritis (RA)
Validate the administration site: if in a hospital
setting, must be free of charge
Treatment of moderate to severe Crohn’s disease:
9 years of age or older
Inadequate response to conventional therapy
(including aminosaliyilates and/or
corticosteroids and/or immunosuppressants),
no response, intolerant or contraindications
Induction dosage: 5 mg/kg at 0, 2 and 6 weeks
Adult maintenance dosage: 5 to 10 mg/kg
every 8 weeks
Pediatric maintenance dosage: 5 mg/kg every
8 weeks
Treatment of moderately to severely active
ulcerative colitis:
6 years of age or older
Inadequate response to conventional therapy
(including aminosaliyilates and/or
corticosteroids and/or immunosuppressants),
no response, intolerant or contraindications
Induction dosage: 5 mg/kg at 0, 2 and 6 weeks
Adult maintenance dosage: 5 to 10 mg/kg
every 8 weeks
Pediatric maintenance dosage: 5 mg/kg every
8 weeks
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
Induction dosage: 3 mg/kg at 0, 2 and 6 weeks
Maintenance dosage: 3 to 10 mg/kg every 4 to
8 weeks
Please see the following page for more
information about Remicade
1 year
1 year
1 year
2 years
2 years
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work

23
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
REMICADE (INFLIXIMAB)
Intravenous Solution
DIN 02244016 (100 MG)
Psoriatic Arthritis
(PA)
Ankylosing
Spondylitis (AS)
Chronic moderate
to severe plaque
psoriasis
Validate the administration site: if in a hospital
setting, must be free of charge
A confirmed diagnosis of moderate to severe
psoriatic arthritis with persistent and active
disease (more than 3 affected joints)
Failure or contraindications to methotrexate
and to another disease modifiying
antirheumatic drugs for a period of 3 months
or more
HAQ > 1
Induction dosage: 5 mg/kg at 0, 2 and 6 weeks
Maintenance dosage: 5 mg/kg every 8 weeks
No response to NSAIDs
BASDAI score ≥ 4
Induction dosage: 5 mg/kg at 0, 2 and 6 weeks
Maintenance dosage: 5 mg/kg every 6 to 8
weeks
Treatment of adult patients with chronic
moderate to severe plaque psoriasis who are
candidates for systemic therapy or phototherapy:
No response, contraindications, intolerance or
inaccessibility to phototherapy
18 years of age or older
Treated by a dermatologist
Failure (or inappropriate) to systemic therapy
by two of the following antipsoriatic agents:
methotrexate, cyclosporine or acitretin
Psoriasis Area Severtiy Index (PASI) ≥10 or
extensive plaques on the face, the palms of the
hands, the soles of the feet or the genital area
And
Dermatology Life Quality Index (DLQI) ≥10
1 year
1 year
4 months
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work
2 years
A 2.2 points diminution for
the BASDI score (or 50%) or
return to work
1 year
Improvement of 75% for the
PASI score
Or
Improvement of 50% for the
PASI score and a 5 points
improvement for DLQI
Or
Significant improvement of
lesions on the face, the palms
of the hands, the soles of the
feet or the genital area
REMODULIN (TREPROSTINIL)
Intravenous, Subcutaneous Solution
DIN 02246552 (1 MG / ML)
DIN 02246553 (2.5 MG / ML)
DIN 02246554 (5 MG / ML)
DIN 02246555 (10 MG / ML)
Pulmonary Arterial
Hypertension
(PAH)
If available, coordinate with the Provincial
Government Program
Treatment of primary pulmonary hypertension or
treatment of pulmonary hypertension secondary to
scleroderma:
No response to conventional therapy
WHO functional - Class III or IV
Indefinite
N/A
RESOTRAN
(PRUCALOPRIDE SUCCINATE)
Oral Tablet
DIN 02377012 (1 MG)
DIN 02377020 (2 MG)
Chronic idiopathic
constipation in
adult female
Treatment of chronic idiopathic constipation in
adult female after failure of laxatives:
Women
18 years of age or older
Patients in whom laxatives failed to provide
adequate relief
Symptoms since at least 6 months and not
induced by secondary causes of constipation
6 months
2 years

24
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
RESTASIS (CICLOSPORIN)
Ophtalmic Emulsion
DIN 02355655 (0.05%)
Aqueous Deficient
Dry Eye Disease
Treatment of moderate to moderately severe
aqueous deficient dry eye disease:
No response to conventional therapy
18 years of age or older
Severity Level 2 or 3 according to DEWS
Guidelines
Indefinite
N/A
RETISERT
(FLUOCINOLONE ACETONIDE)
Intravitreal Implant
DIN 02306980 (0.59 MG)
Non-infectious
uveitis
Treatment of chronic non-infectious uveitis
affecting the posterior segment of the eye:
No response to conventional therapy
18 years of age or older
Sold by a licensed pharmacist
Administered in a private clinic
Prescribed by an ophthalmologist
One implant / eye / 36 months
1 month
N/A
REVATIO (SILDENAFIL)
Oral Tablet
DIN 02279401 (20 MG)
RATIO-SILDENAFIL R (SILDENAFIL)
Oral Tablet
DIN 02319500 (20 MG)
APO-SILDENAFIL R (SILDENAFIL)
Oral Tablet
DIN 02418118 (20 MG)
Pulmonary Arterial
Hypertension
(PAH)
Treatment of primary pulmonary arterial
hypertension (PAH) or treatment of pulmonary
hypertension secondary to connective tissue
disease:
No response to conventional therapy
WHO functional - Class II or III
Indefinite
N/A
REVLIMID (LENALIDOMIDE)
Oral Capsule
DIN 02304899 (5 MG)
DIN 02304902 (10 MG)
DIN 02317699 (15 MG)
DIN 02317710 (25 MG)
Myelodysplastic
Syndrome (MDS)
Multiple myeloma
Treatement of transfusion – dependent anemia
due to low or intermediate-1 risk myelodysplastic
syndromes (MDS) associated with a deletion 5q
cytogenetic abnormality:
Hg ≤ 90g/L
Max 10 mg / day
In combination with dexamethasone
Failure to at least one prior therapy
ECOG ≤ 2
6 months
6 months
6 months
12 months
REVOLADE (ELTROMBOPAG)
Oral Tablet
DIN 02361825 (25 MG)
DIN 02361833 (50 MG)
Chronic Immune
(idiopathic)
Thrombocytopenic
Purpura (ITP)
Indicated to increase platelet counts in adult
patients with ITP:
Who are splenectomized and refractory to
corticosteroids and/or immunoglobulins
Who are non-splenectomized (if surgery is
contraindicated) and inadequate response to
corticosteroids and/or immunoglobulins
Platelet counts < 30 x 109/L
Child-Pugh Score < 10
4 months
8 months
Platelet counts ≥ 50 x 109 /L
without Ig
REVOLADE therapy should
not exceed 1 year of
continuous treatment. After 1
year of continuous treatment,
therapeutic options should be
reassessed.
If prolonged treatment, the
authorization may be 1 year.
25
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
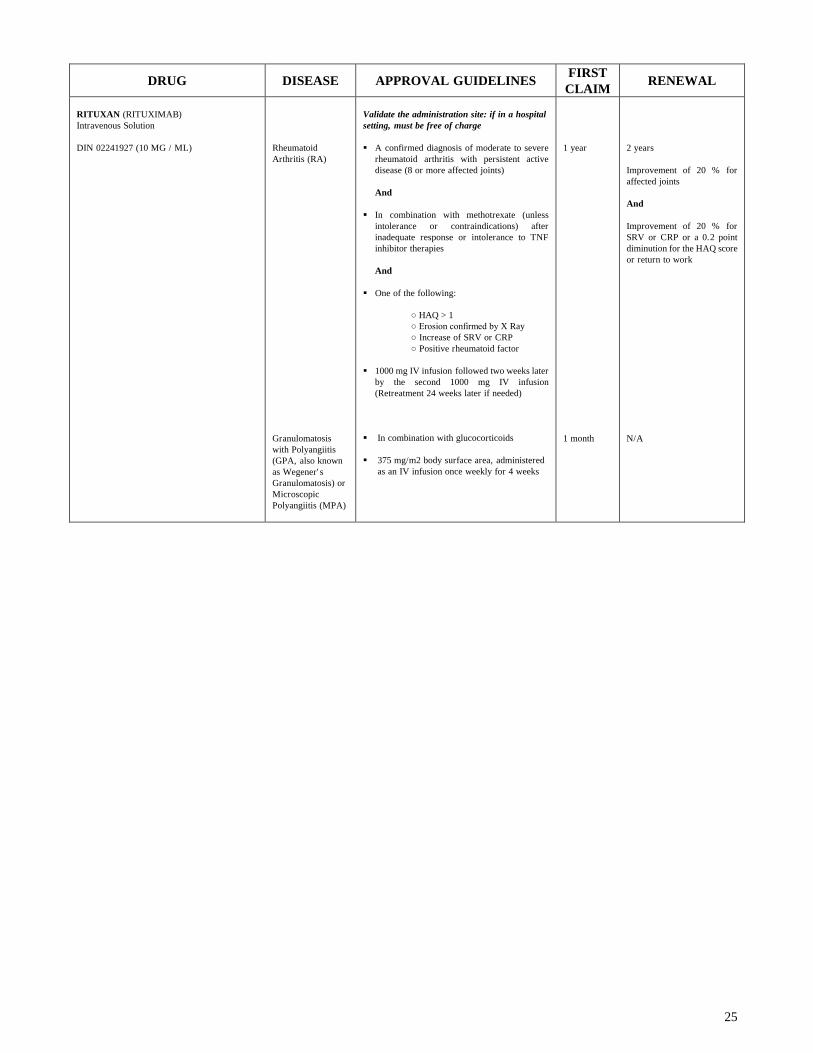
RITUXAN (RITUXIMAB)
Intravenous Solution
DIN 02241927 (10 MG / ML)
Rheumatoid
Arthritis (RA)
Granulomatosis
with Polyangiitis
(GPA, also known
as Wegener' s
Granulomatosis) or
Microscopic
Polyangiitis (MPA)
Validate the administration site: if in a hospital
setting, must be free of charge
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
In combination with methotrexate (unless
intolerance or contraindications) after
inadequate response or intolerance to TNF
inhibitor therapies
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
1000 mg IV infusion followed two weeks later
by the second 1000 mg IV infusion
(Retreatment 24 weeks later if needed)
In combination with glucocorticoids
375 mg/m2 body surface area, administered
as an IV infusion once weekly for 4 weeks
1 year
1 month
2 years
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work
N/A

26
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
SAIZEN (SOMATROPIN)
Intramuscular, Subcutaneous Solution
DIN 02237971 (5 MG)
DIN 02272083 (8.8 MG)
DIN 02350122 (5.83 MG / ML)
DIN 02350130 (8 MG / ML)
DIN 02350149 (8 MG / ML)
DIN 02215136 (10 IU / KIT)
Growth hormnone
deficiency
Turner syndrome
If available, coordinate with the Provincial
Government Program
Pediatric patients:
Treatment of pediatric patients who have
growth failure due to an inadequate secretion
of normal endogenous growth hormone or to a
renal failure
Should not be used for treatment of pediatric
patients with closed epiphyses
Treatment covered until 15 years old of bone
age for girls and 16 years old of bone age for
boys and growth rate > 2 cm / year
Adult patients:
For replacement of endogenous growth hormone
in adults with growth hormone deficiency if:
GH Peak ≤ 5 mcg/L
And
Adult Onset: Patients must have GHD, either
alone or associated with multiple hormone
deficiencies (hypopituitarism), as a result of
pituitary disease, hypothalamic disease,
surgery, radiation therapy, or trauma
Or
Childhood-onset: if GHD during childhood and
confirmed as an adult
Long-term treatment of short stature
associated with Turner syndrome
Should not be used for treatment of pediatric
patients with closed epiphyses
1 year
1 year
1 year
1 year
1 year
1 year
SAMSCA (TOLVAPTAN)
Oral Tablet
DIN 02370468 (15 MG)
DIN 02370476 (30 MG)
Non-hypovolemic
hyponatremia
Treatment of non-hypovolemic hyponatremia:
18 years of age or orlder
Serum sodium < 130mEq/L or symptomatic
hyponatremia
3 months
3 months
SATIVEX
(CANNABIDIOL / DELTA-9-
TETRAHYDROCANNABINOL)
Buccal Spray
DIN 02266121 (25 MG + 27 MG / ML)
Multiple Sclerosis
(MS)
Cancer pain
Treatment for the symptomatic relief of
neuropathic pain in adult patients with multiple
sclerosis (MS)
Treatment of spastic hypertonia associated with
MS in patients unresponsive to prior therapies and
showing an improvement following a first trial
Treatment of moderate to severe cancer pain:
18 years of age or older
Failure to the highest tolerated dose of strong
opioid therapy
1 year
1 year
1 year
1 year
1 year
1 year

27
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
SENSIPAR (CINACALCET)
Oral Tablet
DIN 02257130 (30 MG)
DIN 02257149 (60 MG)
DIN 02257157 (90 MG)
Chronic Kidney
Disease (CKD)
Parathyroid
carcinoma
Primary
Hyperparathyroidis
m
(HPT)
If available, coordinate with the Provincial
Government Program
Treatment of secondary hyperparathyroidism
(HPT) in patients with Chronic Kidney Disease
(CKD) receiving dialysis
Or
Controls parathyroid hormone levels, calcium and
phosphorous levels, and the serum calcium-
phosphorous product (Ca× P), in patients with
CKD receiving dialysis
Indicated for the reduction of hypercalcemia in
patients with parathyroid carcinoma
Indicated for the reduction of clinically significant
hypercalcemia if parathyroidectomy is not
clinically appropriate or is contraindicated
Indefinite
1 year
1 year
N/A
1 year
1 year
SEROSTIM (SOMATROPIN)
Subcutaneous Solution
DIN 02239046 (5 MG)
DIN 02239047 (6 MG)
Cachexia - AIDS
Treatment of HIV wasting associated with
catabolism, weight loss or cachexia:
18 years of age or older
3 months
3 months
(only one renewal, up to a
maximum of 6 months for
treatment)
28
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
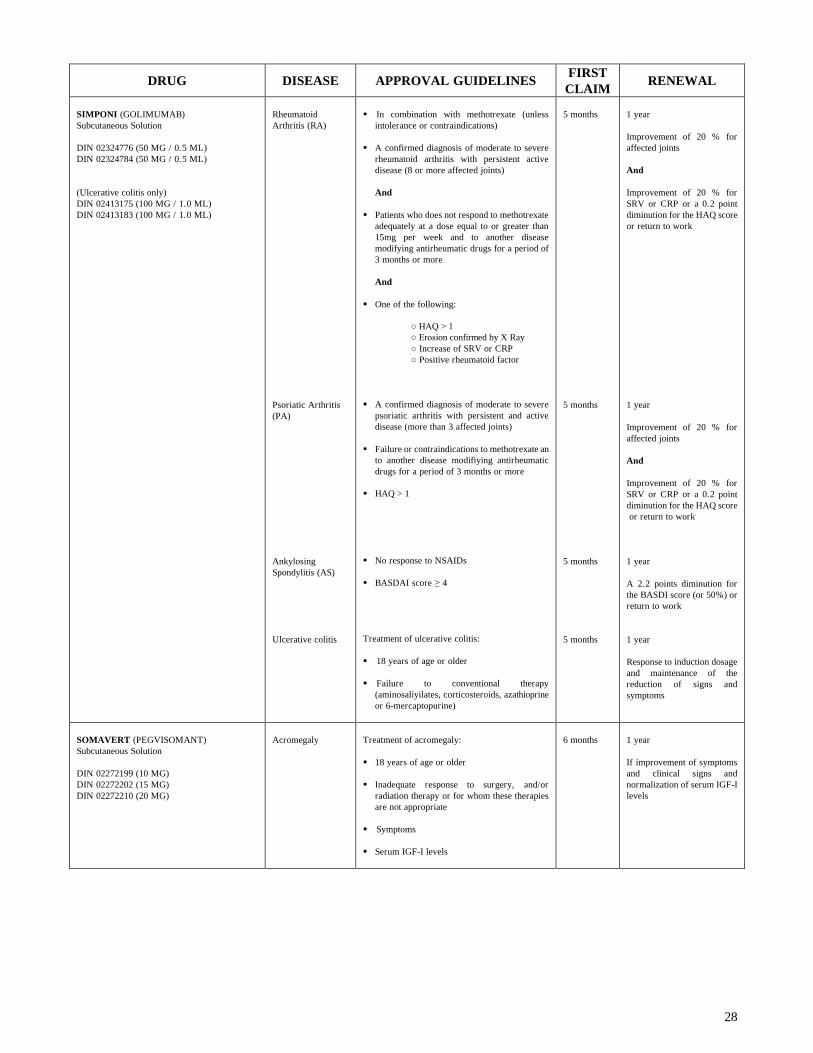
SIMPONI (GOLIMUMAB)
Subcutaneous Solution
DIN 02324776 (50 MG / 0.5 ML)
DIN 02324784 (50 MG / 0.5 ML)
(Ulcerative colitis only)
DIN 02413175 (100 MG / 1.0 ML)
DIN 02413183 (100 MG / 1.0 ML)
Rheumatoid
Arthritis (RA)
Psoriatic Arthritis
(PA)
Ankylosing
Spondylitis (AS)
Ulcerative colitis
In combination with methotrexate (unless
intolerance or contraindications)
A confirmed diagnosis of moderate to severe
rheumatoid arthritis with persistent active
disease (8 or more affected joints)
And
Patients who does not respond to methotrexate
adequately at a dose equal to or greater than
15mg per week and to another disease
modifying antirheumatic drugs for a period of
3 months or more
And
One of the following:
○ HAQ > 1
○ Erosion confirmed by X Ray
○ Increase of SRV or CRP
○ Positive rheumatoid factor
A confirmed diagnosis of moderate to severe
psoriatic arthritis with persistent and active
disease (more than 3 affected joints)
Failure or contraindications to methotrexate an
to another disease modifiying antirheumatic
drugs for a period of 3 months or more
HAQ > 1
No response to NSAIDs
BASDAI score ≥ 4
Treatment of ulcerative colitis:
18 years of age or older
Failure to conventional therapy
(aminosaliyilates, corticosteroids, azathioprine
or 6-mercaptopurine)
5 months
5 months
5 months
5 months
1 year
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work
1 year
Improvement of 20 % for
affected joints
And
Improvement of 20 % for
SRV or CRP or a 0.2 point
diminution for the HAQ score
or return to work
1 year
A 2.2 points diminution for
the BASDI score (or 50%) or
return to work
1 year
Response to induction dosage
and maintenance of the
reduction of signs and
symptoms
SOMAVERT (PEGVISOMANT)
Subcutaneous Solution
DIN 02272199 (10 MG)
DIN 02272202 (15 MG)
DIN 02272210 (20 MG)
Acromegaly
Treatment of acromegaly:
18 years of age or older
Inadequate response to surgery, and/or
radiation therapy or for whom these therapies
are not appropriate
Symptoms
Serum IGF-I levels
6 months
1 year
If improvement of symptoms
and clinical signs and
normalization of serum IGF-I
levels

29
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
SPRYCEL (DASATINIB)
Oral Tablet
DIN 02293129 (20 MG)
DIN 02293137 (50 MG)
DIN 02293145 (70 MG)
DIN 02360810 (80 MG)
DIN 02320193 (100 MG)
DIN 02360829 (140 MG)
Chronic Myeloid
Leukemia (CML)
Acute
Lymphoblastic
Leukemia (ALL)
Treatment of adult patients with Ph+ chronic,
accelerated, or blast phase CML with resistance
or intolerance to prior therapy including imatinib
Or
Treatment of adult patients with newly diagnosed
Ph+ CML in chronic phase
ALL in adult patients with Ph+ if resistance or
intolerance to prior therapy
6 months
6 months
6 months
6 months
STAXYN (VARDENAFIL)
Oral Tablet
DIN 02372436 (10 MG)
Erectile
Dysfunction (ED)
NOTE:
If no ED clause:
not eligible.
Treatment of erectile dysfunction (ED) in men (18
years of age or older):
Organic erectile dysfunction (e.g. , diabetes
related, vascular related)
Erectile dysfunction with neurological cause
(e.g., spinal cord injury (SCI), nerve damage
as a result of a prostatectomy or TURP)
Drug-induced erectile dysfunction where it
would be inappropriate to alter the dosage or to
discontinue the use of the drug in question
Mixed psychogenic/organic erectile
dysfunction
1 year
Or
Indefinite, if
annual
ceiling
1 year
STELARA (USTEKINUMAB)
Subcutaneous Solution
DIN 02320673 (45 MG / 0.5 ML)
DIN 02320681 (90 MG / 1.0 ML)
Chronic moderate
to severe plaque
psoriasis
Treatment of adult patients with chronic moderate
to severe plaque psoriasis who are candidates for
systemic therapy or phototherapy:
No response, contraindications, intolerance or
inaccessibility to phototherapy
18 years of age or older
Treated by a dermatologist
Failure (or inappropriate) to systemic therapy
by two of the following antipsoriatic agents:
methotrexate, cyclosporine or acitretin
Psoriasis Area Severtiy Index (PASI) ≥10 or
extensive plaques on the face, the palms of the
hands, the soles of the feet or the genital area
And
Dermatology Life Quality Index (DLQI) ≥10
5 months
1 year
Improvement of 75% for the
PASI score
Or
Improvement of 50% for the
PASI score and a 5 points
improvement for DLQI
Or
Significant improvement of
lesions on the face, the palms
of the hands, the soles of the
feet or the genital area
STIVARGA (REGORAFENIB)
Oral tablets
DIN 02403390 (40mg)
Metastatic
Colorectal Cancer
(CRC)
Treatment of patients with metastatic CRC who
have been previously treated with
fluoropyrimidine-based chemotherapy, oxaliplatin,
irinotecan, an anti-VEGF therapy (bevacizumab),
and, if KRAS wild type, an anti-EGFR therapy
(cetuximab, panitumumab):
ECOG ≤ 1
3 months
3 months
30
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
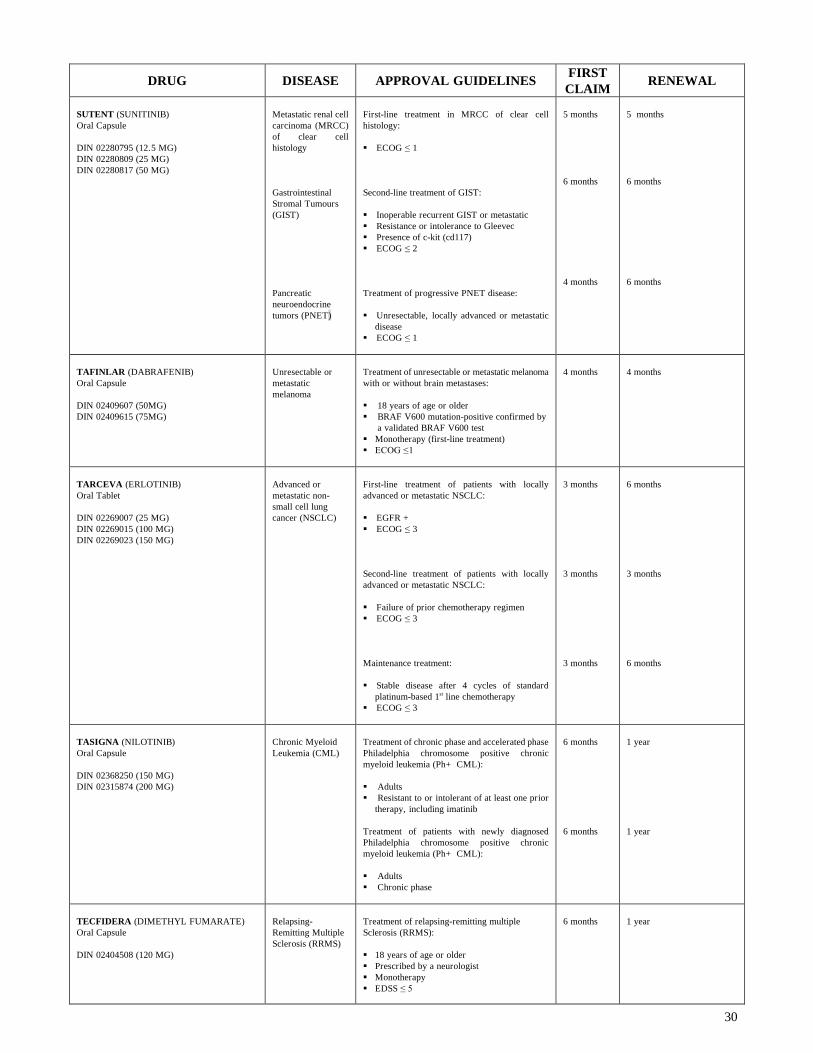
SUTENT (SUNITINIB)
Oral Capsule
DIN 02280795 (12.5 MG)
DIN 02280809 (25 MG)
DIN 02280817 (50 MG)
Metastatic renal cell
carcinoma (MRCC)
of clear cell
histology
Gastrointestinal
Stromal Tumours
(GIST)
Pancreatic
neuroendocrine
tumors (PNET)
First-line treatment in MRCC of clear cell
histology:
ECOG ≤ 1
Second-line treatment of GIST:
Inoperable recurrent GIST or metastatic
Resistance or intolerance to Gleevec
Presence of c-kit (cd117)
ECOG ≤ 2
Treatment of progressive PNET disease:
Unresectable, locally advanced or metastatic
disease
ECOG ≤ 1
5 months
6 months
4 months
5 months
6 months
6 months
TAFINLAR (DABRAFENIB)
Oral Capsule
DIN 02409607 (50MG)
DIN 02409615 (75MG)
Unresectable or
metastatic
melanoma
Treatment of unresectable or metastatic melanoma
with or without brain metastases:
18 years of age or older
BRAF V600 mutation-positive confirmed by
a validated BRAF V600 test
Monotherapy (first-line treatment)
ECOG ≤ 1
4 months
4 months
TARCEVA (ERLOTINIB)
Oral Tablet
DIN 02269007 (25 MG)
DIN 02269015 (100 MG)
DIN 02269023 (150 MG)
Advanced or
metastatic non-
small cell lung
cancer (NSCLC)
First-line treatment of patients with locally
advanced or metastatic NSCLC:
EGFR +
ECOG ≤ 3
Second-line treatment of patients with locally
advanced or metastatic NSCLC:
Failure of prior chemotherapy regimen
ECOG ≤ 3
Maintenance treatment:
Stable disease after 4 cycles of standard
platinum-based 1st line chemotherapy
ECOG ≤ 3
3 months
3 months
3 months
6 months
3 months
6 months
TASIGNA (NILOTINIB)
Oral Capsule
DIN 02368250 (150 MG)
DIN 02315874 (200 MG)
Chronic Myeloid
Leukemia (CML)
Treatment of chronic phase and accelerated phase
Philadelphia chromosome positive chronic
myeloid leukemia (Ph+ CML):
Adults
Resistant to or intolerant of at least one prior
therapy, including imatinib
Treatment of patients with newly diagnosed
Philadelphia chromosome positive chronic
myeloid leukemia (Ph+ CML):
Adults
Chronic phase
6 months
6 months
1 year
1 year
TECFIDERA (DIMETHYL FUMARATE)
Oral Capsule
DIN 02404508 (120 MG)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
Treatment of relapsing-remitting multiple
Sclerosis (RRMS):
18 years of age or older
Prescribed by a neurologist
Monotherapy
EDSS ≤ 5
6 months
1 year
31
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
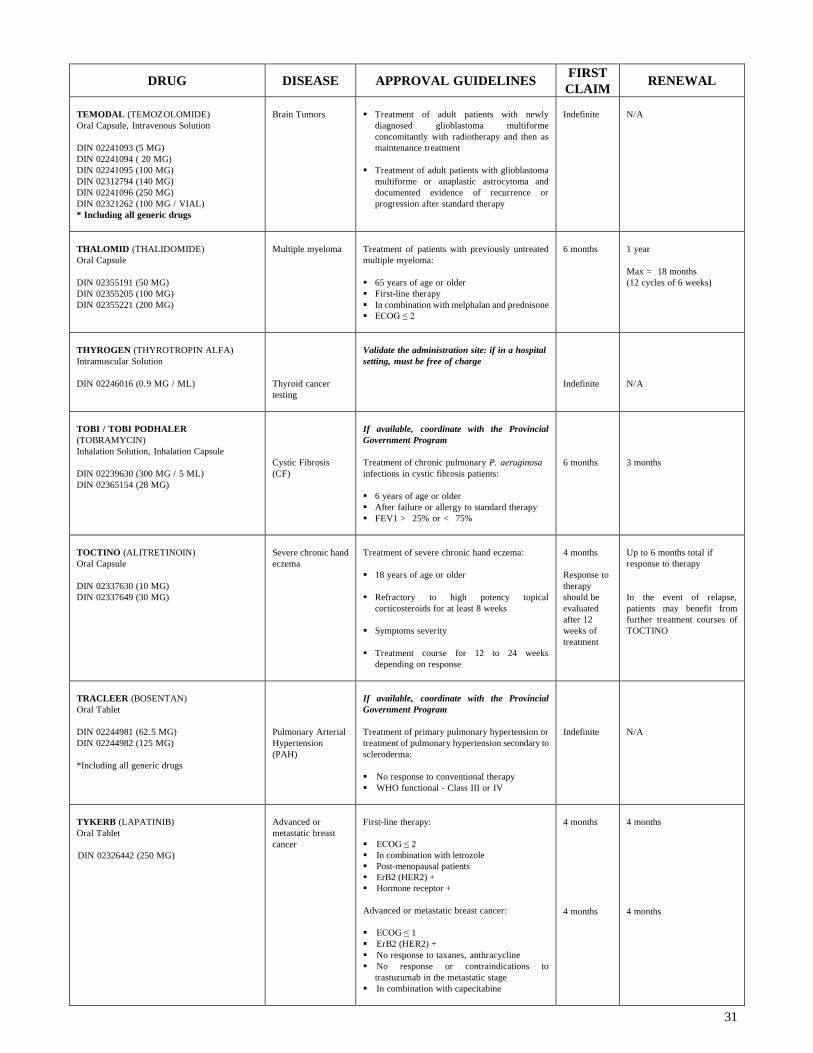
TEMODAL (TEMOZOLOMIDE)
Oral Capsule, Intravenous Solution
DIN 02241093 (5 MG)
DIN 02241094 ( 20 MG)
DIN 02241095 (100 MG)
DIN 02312794 (140 MG)
DIN 02241096 (250 MG)
DIN 02321262 (100 MG / VIAL)
* Including all generic drugs
Brain Tumors
Treatment of adult patients with newly
diagnosed glioblastoma multiforme
concomitantly with radiotherapy and then as
maintenance treatment
Treatment of adult patients with glioblastoma
multiforme or anaplastic astrocytoma and
documented evidence of recurrence or
progression after standard therapy
Indefinite
N/A
THALOMID (THALIDOMIDE)
Oral Capsule
DIN 02355191 (50 MG)
DIN 02355205 (100 MG)
DIN 02355221 (200 MG)
Multiple myeloma
Treatment of patients with previously untreated
multiple myeloma:
65 years of age or older
First-line therapy
In combination with melphalan and prednisone
ECOG ≤ 2
6 months
1 year
Max = 18 months
(12 cycles of 6 weeks)
THYROGEN (THYROTROPIN ALFA)
Intramuscular Solution
DIN 02246016 (0.9 MG / ML)
Thyroid cancer
testing
Validate the administration site: if in a hospital
setting, must be free of charge
Indefinite
N/A
TOBI / TOBI PODHALER
(TOBRAMYCIN)
Inhalation Solution, Inhalation Capsule
DIN 02239630 (300 MG / 5 ML)
DIN 02365154 (28 MG)
Cystic Fibrosis
(CF)
If available, coordinate with the Provincial
Government Program
Treatment of chronic pulmonary P. aeruginosa
infections in cystic fibrosis patients:
6 years of age or older
After failure or allergy to standard therapy
FEV1 > 25% or < 75%
6 months
3 months
TOCTINO (ALITRETINOIN)
Oral Capsule
DIN 02337630 (10 MG)
DIN 02337649 (30 MG)
Severe chronic hand
eczema
Treatment of severe chronic hand eczema:
18 years of age or older
Refractory to high potency topical
corticosteroids for at least 8 weeks
Symptoms severity
Treatment course for 12 to 24 weeks
depending on response
4 months
Response to
therapy
should be
evaluated
after 12
weeks of
treatment
Up to 6 months total if
response to therapy
In the event of relapse,
patients may benefit from
further treatment courses of
TOCTINO
TRACLEER (BOSENTAN)
Oral Tablet
DIN 02244981 (62.5 MG)
DIN 02244982 (125 MG)
*Including all generic drugs
Pulmonary Arterial
Hypertension
(PAH)
If available, coordinate with the Provincial
Government Program
Treatment of primary pulmonary hypertension or
treatment of pulmonary hypertension secondary to
scleroderma:
No response to conventional therapy
WHO functional - Class III or IV
Indefinite
N/A
TYKERB (LAPATINIB)
Oral Tablet
DIN 02326442 (250 MG)
Advanced or
metastatic breast
cancer
First-line therapy:
ECOG ≤ 2
In combination with letrozole
Post-menopausal patients
ErB2 (HER2) +
Hormone receptor +
Advanced or metastatic breast cancer:
ECOG ≤ 1
ErB2 (HER2) +
No response to taxanes, anthracycline
No response or contraindications to
trastuzumab in the metastatic stage
In combination with capecitabine
4 months
4 months
4 months
4 months

32
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
TYSABRI (NATALIZUMAB)
Intravenous Solution
DIN 02286386 (300 MG / 15 ML)
Relapsing-
Remitting Multiple
Sclerosis (RRMS)
If available, coordinate with the Provincial
Government Program
Validate the administration site: if in a hospital
setting, must be free of charge
No response or intolerance to interferons or
glatiramere in highly active disease
Monotherapy
18 years of age or older
EDSS ≤ 6
Prescribed by a neurologist
1 year
1 year
VIAGRA (SILDENAFIL)
Oral Tablet
DIN 02239766 (25 MG)
DIN 02239767 (50 MG)
DIN 02239768 (100 MG)
* Including all generic drugs
Erectile
Dysfunction (ED)
NOTE:
If no ED clause:
not eligible.
Treatment of erectile dysfunction (ED) in men (18
years of age or older):
Organic erectile dysfunction (e.g. , diabetes
related, vascular related)
Erectile dysfunction with neurological cause
(e.g., spinal cord injury (SCI), nerve damage
as a result of a prostatectomy or TURP)
Drug-induced erectile dysfunction where it
would be inappropriate to alter the dosage or to
discontinue the use of the drug in question
Mixed psychogenic/organic erectile
dysfunction
1 year
Or
Indefinite if
annual
ceiling
1 year
VICTRELIS (BOCEPREVIR)
Oral Capsule
DIN 02370816 (200 MG)
VICTRELISVICTRELIS TRIPLE
(BOCEPREVIR / RIBAVIRIN /
PEGINTERFERON ALFA-2B)
Oral Capsule, Subcutaneous Solution
DIN 02371448 (200 MG, 80 MCG / 0.5 ML)
DIN 02371456 (200 MG, 100 MCG / 0.5 ML)
DIN 02371464 (200 MG, 120 MCG / 0.5 ML)
DIN 02371472 (200 MG, 150 MCG / 0.5 ML)
Chronic Hepatitis C
Treatment of genotype 1 Chronic Hepatitis C in
adult patients with compensated liver disease,
including cirrhosis:
18 years of age or older
Previously untreated patients or who have
previously failed therapy
In combination with peginterferon alfa (INFα)
and ribavirin (RBV) for Victrelis (included in
Victrelis triple package)
Starts 4 weeks after pegINFα/RBV
First authorization: 24 weeks
The authorization will be renewed for an
additional 8 to 16 weeks depending on
response to treatment, previous treatment or
the patient' s medical condition
24 weeks
Up to a maximum of 32 to 44
weeks
If confirmed undetectable
HCV-RNA levels at week 24
VIDAZA (AZACITIDINE)
Subcutaneous Suspension
DIN 02336707 (100 MG)
Myelodysplastic
Syndrome (MDS)
Acute Myeloid
Leukemia (AML)
Treatment of adult patients who are not eligible
for hematopoietic stem cell transplantation with:
Intermediate-2 and High-risk Myelodysplastic
Syndrome (MDS) according to the
International Prognostic Scoring System (IPSS)
AML with 20-30 % blasts and multi-lineage
dysplasia according to WHO classification
ECOG ≤ 2
6 months
6 months
VOLIBRIS (AMBRISENTAN)
Oral Tablet
DIN 02307065 (5 MG)
DIN 02307073 (10 MG)
Pulmonary Arterial
Hypertension
(PAH)
If available, coordinate with the Provincial
Government Program
Treatment of primary pulmonary arterial
hypertension (PAH) or associated with connective
tissue disease:
No response to conventional therapy
WHO functional - Class II or III
Indefinite
N/A
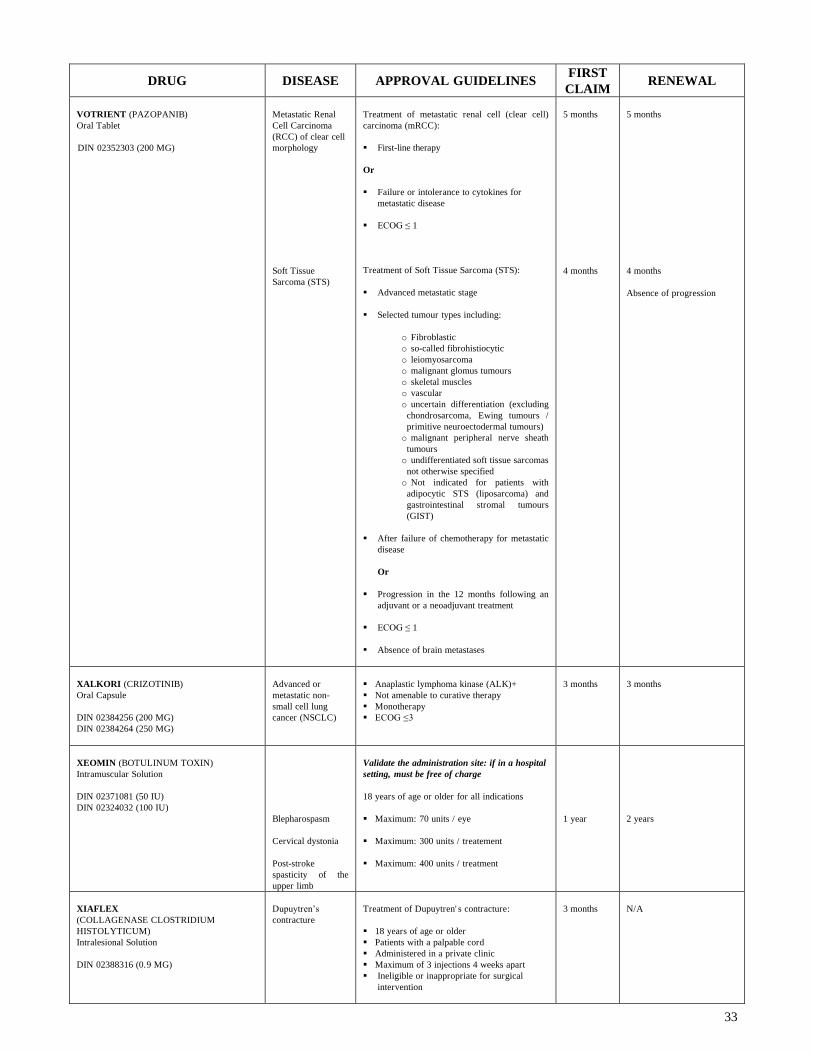
33
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
VOTRIENT (PAZOPANIB)
Oral Tablet
DIN 02352303 (200 MG)
Metastatic Renal
Cell Carcinoma
(RCC) of clear cell
morphology
Soft Tissue
Sarcoma (STS)
Treatment of metastatic renal cell (clear cell)
carcinoma (mRCC):
First-line therapy
Or
Failure or intolerance to cytokines for
metastatic disease
ECOG ≤ 1
Treatment of Soft Tissue Sarcoma (STS):
Advanced metastatic stage
Selected tumour types including:
o Fibroblastic
o so-called fibrohistiocytic
o leiomyosarcoma
o malignant glomus tumours
o skeletal muscles
o vascular
o uncertain differentiation (excluding
chondrosarcoma, Ewing tumours /
primitive neuroectodermal tumours)
o malignant peripheral nerve sheath
tumours
o undifferentiated soft tissue sarcomas
not otherwise specified
o Not indicated for patients with
adipocytic STS (liposarcoma) and
gastrointestinal stromal tumours
(GIST)
After failure of chemotherapy for metastatic
disease
Or
Progression in the 12 months following an
adjuvant or a neoadjuvant treatment
ECOG ≤ 1
Absence of brain metastases
5 months
4 months
5 months
4 months
Absence of progression
XALKORI (CRIZOTINIB)
Oral Capsule
DIN 02384256 (200 MG)
DIN 02384264 (250 MG)
Advanced or
metastatic non-
small cell lung
cancer (NSCLC)
Anaplastic lymphoma kinase (ALK)+
Not amenable to curative therapy
Monotherapy
ECOG ≤ 3
3 months
3 months
XEOMIN (BOTULINUM TOXIN)
Intramuscular Solution
DIN 02371081 (50 IU)
DIN 02324032 (100 IU)
Blepharospasm
Cervical dystonia
Post-stroke
spasticity of the
upper limb
Validate the administration site: if in a hospital
setting, must be free of charge
18 years of age or older for all indications
Maximum: 70 units / eye
Maximum: 300 units / treatement
Maximum: 400 units / treatment
1 year
2 years
XIAFLEX
(COLLAGENASE CLOSTRIDIUM
HISTOLYTICUM)
Intralesional Solution
DIN 02388316 (0.9 MG)
Dupuytren’s
contracture
Treatment of Dupuytren' s contracture:
18 years of age or older
Patients with a palpable cord
Administered in a private clinic
Maximum of 3 injections 4 weeks apart
Ineligible or inappropriate for surgical
intervention
3 months
N/A
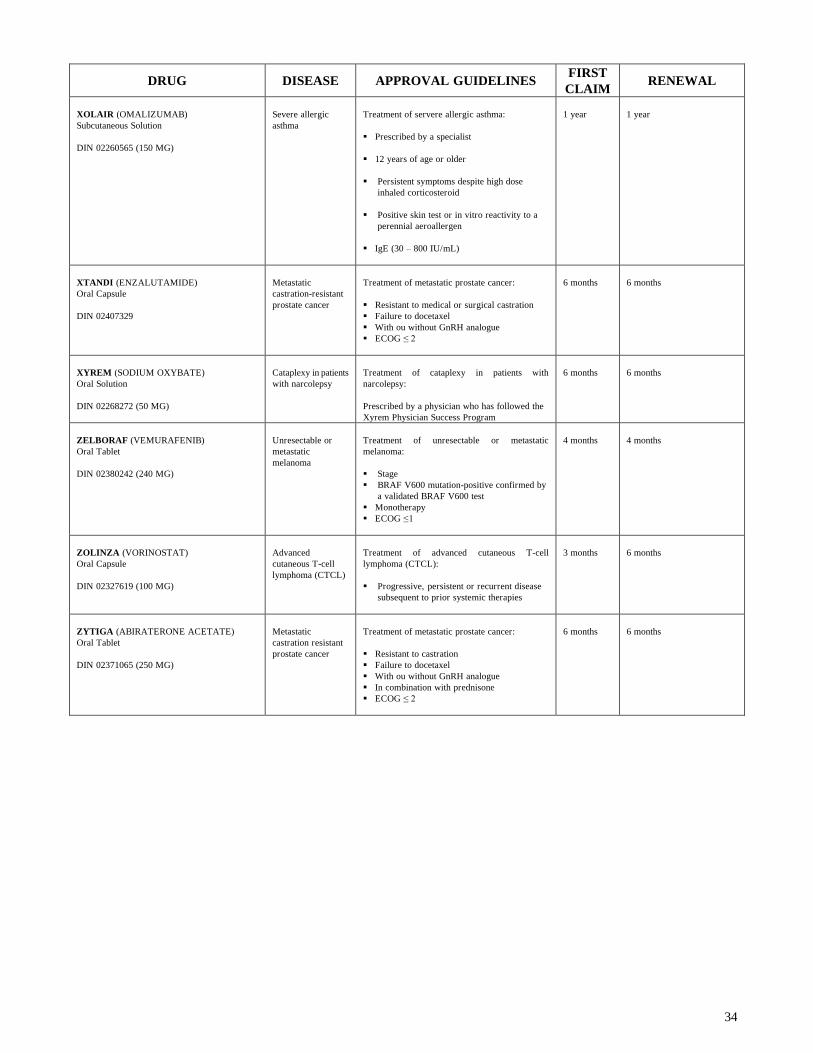
34
DRUG DISEASE APPROVAL GUIDELINES FIRST
CLAIM RENEWAL
XOLAIR (OMALIZUMAB)
Subcutaneous Solution
DIN 02260565 (150 MG)
Severe allergic
asthma
Treatment of servere allergic asthma:
Prescribed by a specialist
12 years of age or older
Persistent symptoms despite high dose
inhaled corticosteroid
Positive skin test or in vitro reactivity to a
perennial aeroallergen
IgE (30 – 800 IU/mL)
1 year
1 year
XTANDI (ENZALUTAMIDE)
Oral Capsule
DIN 02407329
Metastatic
castration-resistant
prostate cancer
Treatment of metastatic prostate cancer:
Resistant to medical or surgical castration
Failure to docetaxel
With ou without GnRH analogue
ECOG ≤ 2
6 months
6 months
XYREM (SODIUM OXYBATE)
Oral Solution
DIN 02268272 (50 MG)
Cataplexy in patients
with narcolepsy
Treatment of cataplexy in patients with
narcolepsy:
Prescribed by a physician who has followed the
Xyrem Physician Success Program
6 months
6 months
ZELBORAF (VEMURAFENIB)
Oral Tablet
DIN 02380242 (240 MG)
Unresectable or
metastatic
melanoma
Treatment of unresectable or metastatic
melanoma:
Stage
BRAF V600 mutation-positive confirmed by
a validated BRAF V600 test
Monotherapy
ECOG ≤ 1
4 months
4 months
ZOLINZA (VORINOSTAT)
Oral Capsule
DIN 02327619 (100 MG)
Advanced
cutaneous T-cell
lymphoma (CTCL)
Treatment of advanced cutaneous T-cell
lymphoma (CTCL):
Progressive, persistent or recurrent disease
subsequent to prior systemic therapies
3 months
6 months
ZYTIGA (ABIRATERONE ACETATE)
Oral Tablet
DIN 02371065 (250 MG)
Metastatic
castration resistant
prostate cancer
Treatment of metastatic prostate cancer:
Resistant to castration
Failure to docetaxel
With ou without GnRH analogue
In combination with prednisone
ECOG ≤ 2
6 months
6 months

35
2) Cancer drugs / Injectables Section Important Notice:
Intravenous (IV) or intravesical (into the bladder) drugs are generally administered in an hospital setting (H code)
and should therefore be declined : DIN not covered.
o Exceptional situations should be evaluated on a case by case basis with all the clinical information available
using an appropriate drug evaluation form filled and signed by a physician (information required: patient’s
name, certificate number, date of birth, patient’s weight, if available, diagnosis, previous medications used,
drug required, dosage, quantity provided and duration of drug treatment). The drug would need to be
purchased in pharmacy and administered outside the hospital.
All intravenous chemotherapy are usually covered by the various provincial programs and administered in specialist
oncology hospitals. So all claims for payment for intravenous chemotherapy, including chemotherapy not included
in this list should usually be denied. Do not hesitate to contact the SSQ pharmaceutical team for any question about
eligibility or not of a drug.
The following intramuscular (IM), subcutaneous (SC) or implant cancer drugs, purchased in pharmacy and
administered outside the hospital, would require prior authorization according to the diagnosis and usual adult
dose provided.
Drug
Name Active Ingredient DIN Diagnosis Usual Adult Dose
First
Claim Renewal
ALIMTA
PEMETREXED
02253437
First line therapy in
combination with cisplatin for
Malignant pleural
mesothelioma, in patients
whose disease is unresectable
disease or who are not
candidates for curative surgery
Second line therapy for locally
advanced or metastatic Non-
small cell lung cancer
IV infusion 500mg/m2 body surface area
on day 1 of each 21 day cycle
6 months
Only if
clinical
benefit
AMSA PD
AMSACRINE
00582212
Second line therapy for Acute
lymphocytic leukemia
Up to 125mg/m2 body surface area per
day IV infusion for 5 days, repeated
every 3 to 4 weeks
Maintenance: half the starting dose every
4 to 8 weeks
1 year
2 years
AVASTIN
BEVACIZUMAB
02270994
First line therapy in
combination with 5FU
chemotherapy for Metastatic
colorectal cancer
In combination with
carboplatin / paclitaxel
chemotherapy for unresectable
advanced, metastatic or
recurrent non-sqamous non-
small cell lung cancer
As a single agent for the
treatment of patients with
malignant glioma (WHO
Grade IV) – glioblastoma after
relapse or disease progression,
following prior therapy
IV infusion 5mg/kg body weight once
every 14 days
IV infusion 15mg/kg of body weight once
every 3 weeks
IV infusion 10mg/kg body weight once
every 14 days
1 year
6 months
(in
combination
with
chemotherapy
for up 6
cycles)
3 months
2 years
As a single
agent, if
clinical
benefit
6 months
BEXXAR*
TOSITUMOMAB 131I-TOSITUMOMAB
02270471
Second line therapy for Non
Hodgkin’s lymphoma
IV infusion 450mg tositumomab
followed by 185MBq 131I-tositumomab
(35 mg) day 0; 450mg tositumomab
followed by variable mCi (65-75 cGy
TBD) 131I-tositumomab between day 7 to
14 following the first dose
1 month
N/A
* If treatment administered as an outpatient: It should be with the appropriate license conditions as granted by the Canadian Nuclear Safety

36
Commission
N/A = Not applicable
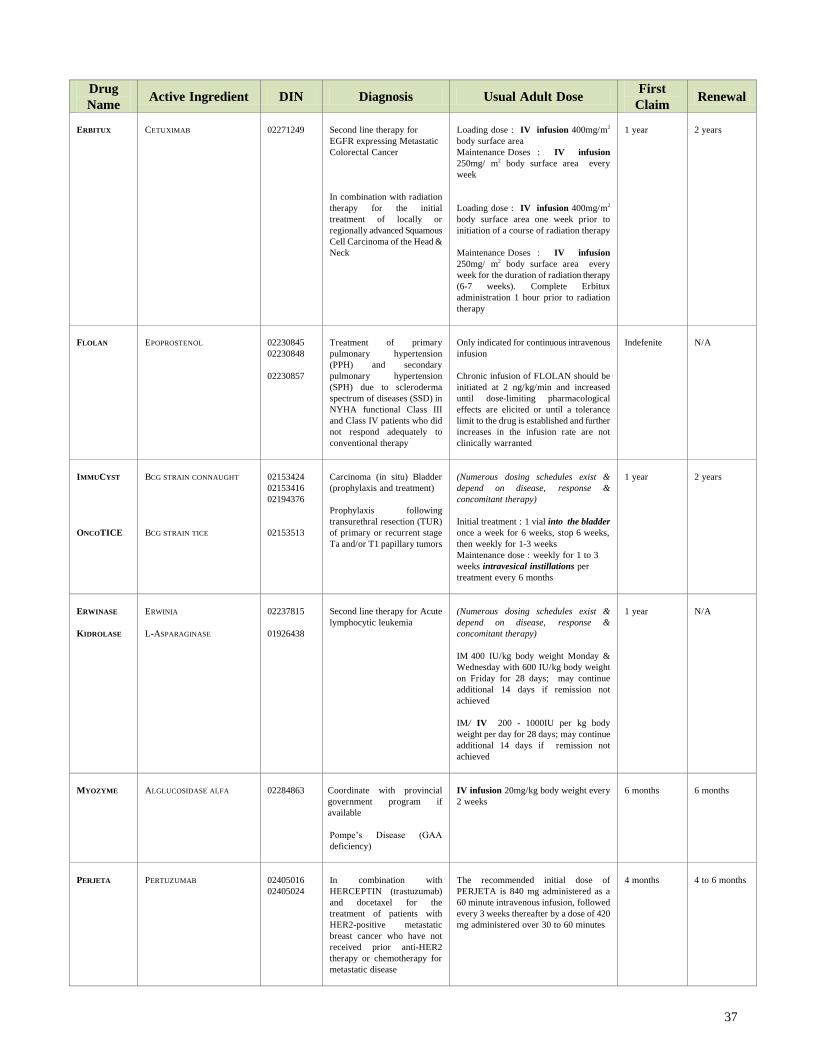
37
Drug
Name Active Ingredient DIN Diagnosis Usual Adult Dose
First
Claim Renewal
ERBITUX
CETUXIMAB
02271249
Second line therapy for
EGFR expressing Metastatic
Colorectal Cancer
In combination with radiation
therapy for the initial
treatment of locally or
regionally advanced Squamous
Cell Carcinoma of the Head &
Neck
Loading dose : IV infusion 400mg/m2
body surface area
Maintenance Doses : IV infusion
250mg/ m2 body surface area every
week
Loading dose : IV infusion 400mg/m2
body surface area one week prior to
initiation of a course of radiation therapy
Maintenance Doses : IV infusion
250mg/ m2 body surface area every
week for the duration of radiation therapy
(6-7 weeks). Complete Erbitux
administration 1 hour prior to radiation
therapy
1 year
2 years
FLOLAN
EPOPROSTENOL
02230845
02230848
02230857
Treatment of primary
pulmonary hypertension
(PPH) and secondary
pulmonary hypertension
(SPH) due to scleroderma
spectrum of diseases (SSD) in
NYHA functional Class III
and Class IV patients who did
not respond adequately to
conventional therapy
Only indicated for continuous intravenous
infusion
Chronic infusion of FLOLAN should be
initiated at 2 ng/kg/min and increased
until dose-limiting pharmacological
effects are elicited or until a tolerance
limit to the drug is established and further
increases in the infusion rate are not
clinically warranted
Indefenite
N/A
IMMUCYST
ONCOTICE
BCG STRAIN CONNAUGHT
BCG STRAIN TICE
02153424
02153416
02194376
02153513
Carcinoma (in situ) Bladder
(prophylaxis and treatment)
Prophylaxis following
transurethral resection (TUR)
of primary or recurrent stage
Ta and/or T1 papillary tumors
(Numerous dosing schedules exist &
depend on disease, response &
concomitant therapy)
Initial treatment : 1 vial into the bladder
once a week for 6 weeks, stop 6 weeks,
then weekly for 1-3 weeks
Maintenance dose : weekly for 1 to 3
weeks intravesical instillations per
treatment every 6 months
1 year
2 years
ERWINASE
KIDROLASE
ERWINIA
L-ASPARAGINASE
02237815
01926438
Second line therapy for Acute
lymphocytic leukemia
(Numerous dosing schedules exist &
depend on disease, response &
concomitant therapy)
IM 400 IU/kg body weight Monday &
Wednesday with 600 IU/kg body weight
on Friday for 28 days; may continue
additional 14 days if remission not
achieved
IM/ IV 200 - 1000IU per kg body
weight per day for 28 days; may continue
additional 14 days if remission not
achieved
1 year
N/A
MYOZYME
ALGLUCOSIDASE ALFA
02284863
Coordinate with provincial
government program if
available
Pompe’s Disease (GAA
deficiency)
IV infusion 20mg/kg body weight every
2 weeks
6 months
6 months
PERJETA
PERTUZUMAB
02405016
02405024
In combination with
HERCEPTIN (trastuzumab)
and docetaxel for the
treatment of patients with
HER2-positive metastatic
breast cancer who have not
received prior anti-HER2
therapy or chemotherapy for
metastatic disease
The recommended initial dose of
PERJETA is 840 mg administered as a
60 minute intravenous infusion, followed
every 3 weeks thereafter by a dose of 420
mg administered over 30 to 60 minutes
4 months
4 to 6 months

38
PROLEUKIN
INTERLEUKIN
02130181
Metastatic renal cancer
Metastatic malignant
melanoma
600 000 IU/kg body weight IV infusion
every 8 hours for a max of 14 doses.
Stop 9 days; repeat for another 14 doses
(max 28 doses per course)
1 year
N/A

39
Drug
Name Active Ingredient DIN Diagnosis Usual Adult Dose
First
Claim Renewal
REVATIO
SILDENAFIL
02341611
Treatment of primary
pulmonary arterial
hypertension (PAH) or
treatment of pulmonary
hypertension secondary to
connective tissue disease
The recommended dose of REVATIO
intravenous administration is 10 mg
(corresponding to 12.5 mL) three times a
day administered as an intravenous bolus
injection
Indefinite
N/A
SANDOSTATIN
SANDOSTATIN
LAR
OCTREOTIDE
02248639
00839191
02248640
00839205
02248642
02049392
02248641
00839213
02299437
02299445
02299453
02239323
02239324
02239325
Symptomatic metastatic
carcinoid syndrome
Symptomatic vasoactive
intestinal peptide-secreting
tumor (VIPoma)
Acromegaly
Usual adult dose
Immediate release dosage form :
50-1500 μg SC or IV per day
Long acting dosage form (LAR):
30 mg IM every 4 weeks; after 2 months,
may be ↓ to 10 mg or ↑ to 30 mg
depending on response
1 year
2 years
TREANDA
BENDAMUSTINE
02392569
02392550
Relapsed indolent B-cell non-
Hodgking lymphoma (NHL)
who did not respond to or
progressed during or shortly
following treatment with a
rituximab regimen
Symptomatic chronic
lymphocytocytic leukemia
(CCL) who have received no
prior treatment
In monotherapy: 120mg/m2 IV Days 1
and 2 of a 21-day cycle up to 8 cycles
In monotherapy: 100mg/m2 IV on Days 1
and 2 of a 28-day cycle, up to 6 cycles
6 months
6 months
N/A
N/A
VALTAXIN
VALRUBICIN
02242466
Second line therapy for BCG
refractory Bladder cancer
(carcinoma in situ)
800 mg intravesical instillation once a
week for 6 weeks
6 weeks
N/A

40
Drug
Name Active Ingredient DIN Diagnosis Usual Adult Dose
First
Claim Renewal
VANTAS
HISTRELIN
02278383
Advanced prostate cancer
One implant SC once yearly
1 year
1 year
VECTIBIX
PANITUMUMAB
02308487
Second line therapy for
metastatic colorectal cancer
with non-mutated or “wild
type” KRAS gene:
After failure of
fluoropyrimidine,
oxaliplatin and irinotecan-
containing chemotherapy
regimens
IV infusion 6 mg/kg body weight once
every 2 weeks
6 months
1 year
VELCADE
BORTEZOMIB
02262452
As part of combination
therapy for previously
untreated multiple myeloma in
patients unsuitable for stem
cell transplantation
Second line therapy for
multiple myeloma
IV 1.3 mg/m2 body surface area for nine
6-week treatment cycles: Cycles 1-4:
twice weekly; Cycles 5-9: once weekly
(in combination with oral melphalan &
oral prednisone)
Starting dose : 1.3 mg/m2 body surface
area IV twice a week for 2 weeks (days
1,4,8,11) then 10 days rest period
(days12-21); then repeat for a maximum
of 8 cycles
54 weeks
8 months
Only if clinical
benefit
Up to 2 cycles
in patients
with
complete
response (CR)
N/A = Not applicable





























