Embed Size (px)
Citation preview
Standardization Committee of the International Society on Throm-
bosis and Haemostasis. Thromb Haemost 1994; 71: 520–5.
2 Favaloro EJ, Grispo L, Exner T, Koutts J. Development of a simple
collagen based ELISA assay aids in the diagnosis of, and permits
sensitive discrimination between type I and type II, von Willebrand�sdisease. Blood Coagul Fibrinolysis 1991; 2: 285–91.
3 Favaloro EJ. Collagen binding assay for von Willebrand factor
(VWF:CBA): detection of von Willebrands disease (VWD), and
discrimination of VWD subtypes, depends on collagen source.Thromb
Haemost 2000; 83: 127–35.
4 Baronciani L, Federici AB, Cozzi G, Canciani MT, Mannucci PM.
von Willebrand factor collagen binding assay in von Willebrand dis-
ease type 2A, 2B, and 2M. J Thromb Haemost 2006; 4: 2088–90.
5 Baronciani L, Federici AB, Beretta M, Cozzi G, Canciani MT,
Mannucci PM. Expression studies on a novel type 2B variant of the
von Willebrand factor gene (R1308L) characterized by defective col-
lagen binding. J Thromb Haemost 2005; 3: 2689–94.
Standardization of circulating endothelial cell enumeration bythe use of human umbilical vein endothelial cells
P . K . Y . GOON, T . WATSON, E . SHAN TS I LA , C . J . BOOS and G. Y . H . L I PHaemostasis, Thrombosis and Vascular Biology Unit, University Department of Medicine, City Hospital, Birmingham, UK
To cite this article: Goon PKY, Watson T, Shantsila E, Boos CJ, Lip GYH. Standardization of circulating endothelial cell enumeration by the use of
human umbilical vein endothelial cells. J Thromb Haemost 2007; 5: 870–2.
Since Jaffe et al. [1] successfully cultured viable human
umbilical vein endothelial cells (HUVECs), HUVECs have
been essential to modern vascular research. They are consid-
ered the archetypal example of mature endothelial cells (ECs),
with a distinct and demonstrable endothelial phenotype. With
the recent advent of mature circulating endothelial cell (CEC)
analysis, the need for a reliable �positive control� cell populationfor CECs is mandatory, with HUVECs being an obvious
choice.
In recent published work, HUVEC use has been central to
the validation of CEC techniques such as immunomagnetic
bead (IB)methodology and flow cytometry (FC) [2,3]. The lack
of consensus on CEC methodology aptly illustrates the innate
difficulty facing researchers. Based on our own CEC validation
work [4], we have observed that CEC/HUVEC capture is
crucially influenced by a number of cellular characteristics of
the isolation technique used (FC vs. IB). To investigate this
further, we studied three distinct patient groups: breast cancer,
acute myocardial infarction, and following traumatic vene-
puncture. Cultured HUVECs were spiked into known quan-
tities of phosphate buffer solution and venous blood, and
analyzed using IB and FC.
Based on a well-established and validated technique [3,4], IB
capture of HUVECs was effected by incubating the sample
with CD146-conjugated IBs. CD146+ cells were then magnet-
ically separated and incubated with fluorescein isothiocyanate
(FITC)-labeled Ulex europaeus lectin. The samples were
washed and viewed under fluorescence microscopy. CECs
were defined as cells 10–50 lm in diameter, staining for
U. europaeus lectin, and bound by ‡ 4 CD146 beads [3,4]. In
the phosphate buffer solution samples, recovery of lectin-
stained HUVECs was in excess of 80%, and when spiked into
blood samples, HUVECs were easily identifiable as being
rounder in shape, significantly larger, and readily sequestrated
by large numbers of beads, compared with CECs found in
unspiked blood samples (Fig. 1).
Using the same samples, the analysis was repeated using FC.
As previously described [4], the whole blood sample was lyzed
(10 min or less), and blocked (using serum and specific Fc
receptor immunoglobulin), before final staining with conju-
gated antibodies (FITC–CD45, phycoerythryn [PE]-CD146,
PE Cy5–CD34). Crucially, red cell lysis (FACS Lysing
Solution, Becton Dickinson, Oxford, UK) before staining did
not significantly alter the relevant (CD45, CD34, CD146)
antigenic sites [confirmed during validation, using both IB and
FC methods, and with non-fixative lysing solution, e.g. High-
Yield Lyse (Caltag Medsystems, Buckingham, UK); data not
shown], whereas with 2% paraformaldehyde fixation, there
were significant differences (e.g. reduced CD146 antigen–
antibody binding). Using sequential gating with the appropri-
ate forward scatter (FSC) and side scatter (SSC) profiles
(representing size and granularity, respectively) to exclude
irrelevant events, including dead cells and anucleated fragments
(supplementary Fig. S1), CECs were defined as CD45)/146+/
34+events, a definition in keeping with previous reports [2,5–8].
Ideally, the progenitor marker CD133 would be needed to
exclude with certainty cells representing the endothelial
progenitor cell (EPC) population. However, others have shown
Correspondence: Gregory Y. H. Lip, Haemostasis, Thrombosis and
Vascular Biology Unit, University Department of Medicine, City
Hospital, Birmingham, B18 7QH, UK.
Tel.: +44 121 5075080; fax: +121 554 4083; e-mail:
Received 26 October 2006, accepted 5 January 2007
870 Letters to the Editor
� 2007 International Society on Thrombosis and Haemostasis
that the vast majority of CD133+ EPCs (including CD133+/
146+ EPCs) are invariably CD45dim or CD45+ cells [6],
whereas others have reported that CD146+ EPCs represent
only 4% of the total CD146+ CEC population [9]. CECs
enumerated by our method were exclusively CD45), thereby
excluding the majority of EPCs.
Using FC, the capture rate was low for HUVECs (5–10%).
This was a result of significant cellular differences between
HUVECs and peripheral blood CECs. Firstly, the majority of
HUVECs were significantly larger than lymphocytes, mono-
cytes, granulocytes and blood CECs, as evident from the high
FSC (supplementary Fig. S1G). With microscopy, a charac-
teristic HUVEC was seen to be approximately 1.5–2.0-fold
larger than CECs (Fig. 1). Secondly, HUVECs had greater
granularity than peripheral blood mononuclear cells (PBMCs),
as seen by the high SSC (supplementary Fig. S1). Thirdly,
unstained HUVECs showed a high degree of autofluorescence
(supplementary Fig. S1), as evidenced by positive fluorescence
in all three-color channels that had been standardized using
PBMCs. As a direct consequence, most HUVECs were gated
out into the �dump� channel (i.e. CD45+ cells), being wrongly
perceived by the cytometer to be �positive� for the CD45
marker. Inevitably, this corresponds to erroneously �low�HUVEC capture. Conversely, whenHUVEC autofluorescence
was adjusted for, only similar-sized CECs were counted (i.e.
very large CECs), excluding the majority of CECs, which were
comparable in size to lymphocytes and monocytes [confirmed
with microscopy and IB, using traumatic and atraumatic
venepuncture blood specimens (Fig. 1; supplementary
Fig. S1)], and which would then appear understained for
CD146 and CD34. Similarly, some CD45+ mononuclear cells
would erroneously appear as �understained� for CD45, thereby
contaminating G2 and contributing wrongly to the final CEC
analysis. Compared to HUVECs, CECs are more heterogene-
ous in morphology (Fig. 1), with the majority being also
smaller in size, and thus more comparable to the general
lymphocyte/monocyte population.
Overall, these findings suggest that use of HUVECs as a
positive-control population for CEC analysis using FC is
inadvisable, as HUVECs may only represent rarer, larger
CECs in peripheral blood. Depending on how the flow
cytometer is standardized, the assay could potentially lead to
spuriously low or high CEC counts when running blood
samples, making any conclusions unreliable. With the IB
technique, this is much less of an issue, as the capture of ECs
depends on CD146 antigenicity, and method-specific problems
of autofluorescence and gating are not encountered. This is
reflected by the good recovery rate of spiked HUVECs in the
tested samples.
Several obvious limitations, however, need to be mentioned.
Firstly, we only included three patient groups for our definition
of the �typical CEC�, and this may not necessarily equate to
CECs in other diseases (e.g. vasculitis, sepsis, diabetes mellitus,
and transplantation). Secondly, we did not evaluate other
available examples of cultured ECs (e.g. human umbilical
artery ECs, human dermal microvascular ECs, human brain
microvascular ECs), which could conceivably be more repre-
sentative of the general CEC phenotype. Thirdly, HUVEC
culture (including culture mediums, passaging, and trypsiniza-
tion) might crucially alter cell characteristics. A fourth consid-
eration regards the comparison of FC parameters – as the
numbers of CECs found in blood tend to be much smaller than
the numbers of spiked HUVECs, the discrepancy in numbers
makes a direct comparison of (for example) SSC and autoflu-
orescence limited. Finally, we recognize the importance of
using the CD133 progenitor marker in FC assays in order to
confidently exclude all EPCs from the CEC population. We
stress that the observations and conclusions are based on our
particular FC strategy and, as such,may not be generalizable to
other FC protocols currently in use.
CECs are increasingly recognized as sensitive markers of
endothelial damage/dysfunction. Consequently, it is essential
that CEC assays are rigorously validated, with emphasis on the
use of positive controls. Our observations suggest several
potential limitations of using HUVEC validation for CEC
work. This is particularly applicable to FC (vs. IB), and is
largely explained by morphologic and phenotypic differences.
Disclosure of Conflict of Interests
The authors state that they have no conflict of interest.
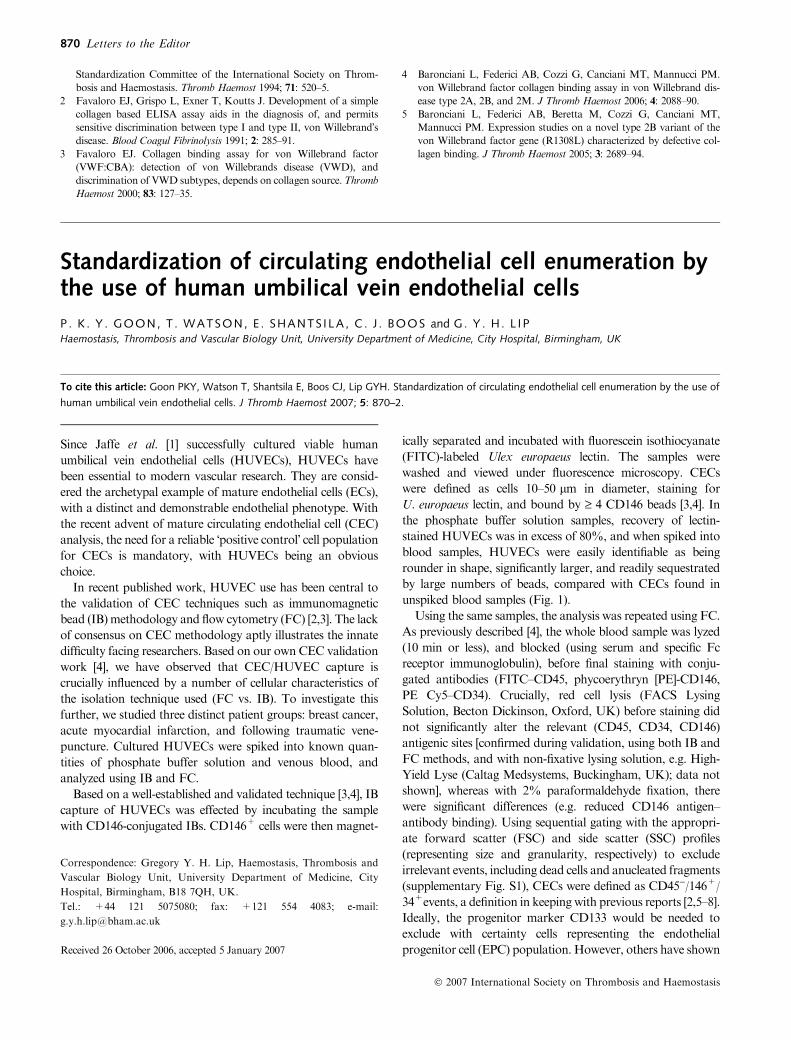
Fig. 1. Circulating endothelial cells (CECs) captured by immunomagnetic
bead technique. (A, B, C) Representative examples of typical mature
CECs captured by the immunomagnetic bead (IB) method and viewed
with fluorescence microscopy, representing three different patient groups
[traumatic venepuncture sample in a healthy individual, a breast cancer
patient and an acute myocardial infarction (AMI) patient respectively],
demonstrating Ulex lectin uptake (green–yellow fluorescence); Note that
in (C), the CEC is viewed using both white light and fluorescing light. (D)
This represents a typical human umbilical vein endothelial cell captured by
the IB method. Note that the cell appears rounder, is much larger, and has
a higher concentration of CD146 IBs rosetting it, differing significantly
from CECs [which, in the two disease states (B, C), typically have a more
attenuated, irregular appearance] (individual beads are approximately
4.5 lm in diameter; all cells viewed with the same magnification).
Letters to the Editor 871
� 2007 International Society on Thrombosis and Haemostasis

Supplementary Material
The following supplementary material can be found at http://
www.blackwell-synergy.com/loi/jth:
Fig. S1. Flow cytometric analysis of peripheral blood for
circulating endothelial cell (CEC) capture. (A, B, C). Typical
forward scatter (FSC)/side scatter (SSC) profile of blood
leukocytes [in this case, a patient with acute myocardial
infarction (AMI)], demonstrating sequential gating strategy
for mature CEC enumeration. G2 represents a gate to
exclude all non-relevant CD45+ cells, and cells of high SSC,
R1 represents CD45)/146+/34+ CECs, and R2 represents
CD34+ progenitor cells. (D, E, F) Typical FSC/SSC plots
from three different groups of subjects, demonstrating FSC/
SSC characteristics of CECs (in bold for clarity). Note that
the majority of CECs are comparable to normal peripheral
blood mononuclear cells (PBMCs). (G) A typical scatter-plot
of an unstained blood sample (from an AMI patient) spiked
with cultured HUVECs (highlighted in bold for clarity),
demonstrating their considerably different FSC/SSC charac-
teristics compared to PBMCs (A). (H) In the same unstained
sample, unstained HUVECs (boxed area) also possess a
greater degree of autofluorescence compared with other
blood leukocytes (fluorescence in FL1); compare this with a
similarly unstained sample without HUVECs (I, J). (K) A
representative plot of a pure unstained HUVEC population,
further demonstrating autofluorescence in FL2 and FL3
channels, and (L) when stained specifically for CD146 and
CD34.
References
1 Jaffe EA, Hoyer LW, Nachman RL. Synthesis of antihemophilic
factor antigen by cultured human endothelial cells. J Clin Invest 1973;
52: 2757–64.
2 Mancuso P, Burlini A, Pruneri G, Goldhirsch A, Martinelli G,
Bertolini F. Resting and activated endothelial cells are increased in the
peripheral blood of cancer patients. Blood 2001; 97: 3658–61.
3 Woywodt A,Goldberg C, Scheer J, RegelsbergerH,Haller H,Haubitz
M. An improved assay for enumeration of circulating endothelial cells.
Ann Hematol 2004; 83: 491–4.
4 Goon PKY, Boos CJ, Stonelake PS, Blann AD, Lip GYH. Detection
and quantification of mature circulating endothelial cells using flow
cytometry and immunomagnetic beads: a methodological comparison.
Thromb Haemost 2006; 96: 45–52.
5 Del Papa N, Colombo G, Fracchiolla N, Moronetti LM, Ingegnoli F,
Maglione W, Comina DP, Vitali C, Fantini F, Cortelezzi A. Circula-
ting endothelial cells as a marker of ongoing vascular disease in sys-
temic sclerosis. Arthritis Rheum 2004; 50: 296–304.
6 Delorme B, Basire A, Gentile C, Sabatier F, Monsonis F, Desouches
C, Blot-ChabaudM,UzanG, Sampol J, Dignat-George F. Presence of
endothelial progenitor cells, distinct from mature endothelial cells,
within humanCD146+blood cells.ThrombHaemost 2005;94: 1270–9.
7 Zhang H, Vakil V, Braunstein M, Smith EL, Maroney J, Chen L, Dai
K, Berenson JR, Hussain MM, Klueppelberg U, Norin AJ, Akman
HO, Ozcelik T, Batuman OA. Circulating endothelial progenitor cells
in multiple myeloma: implications and significance. Blood 2005; 105:
3286–94.
8 Furstenberger G, von Moos R, Lucas R, Thurlimann B, Senn HJ,
Hamacher J, Boneberg EM. Circulating endothelial cells and angio-
genic serum factors during neoadjuvant chemotherapy of primary
breast cancer. Br J Cancer 2006; 94: 524–31.
9 Nakatani K, Takeshita S, Tsujimoto H, Kawamura Y, Tokutomi T,
Sekine I. Circulating endothelial cells in Kawasaki disease. Clin Exp
Immunol 2003; 131: 536–40.
Influence of the Thr325Ile polymorphism onprocarboxypeptidase U (thrombin-activable fibrinolysisinhibitor) activity-based assays
J . L . WILLEMSE ,* V . MATUS ,� E . HEY LEN ,* D . MEZZANO� and D . F . HEN DR IKS**Laboratory of Medical Biochemistry, University of Antwerp, Antwerp, Belgium; and �Laboratory of Thrombosis and Haemostasis, P. Catholic
University of Chile, Santiago, Chile
To cite this article: Willemse JL, Matus V, Heylen E, Mezzano D, Hendriks DF. Influence of the Thr325Ile polymorphism on procarboxypeptidase U
(thrombin-activable fibrinolysis inhibitor) activity-based assays. J Thromb Haemost 2007; 5: 872–5.
Carboxypeptidase U is a potent attenuator of the fibrinolytic
rate present in the circulation as its zymogen procarboxypept-
idase U [proCPU, thrombin-activable fibrinolysis inhibitor
(TAFI)].
During the last few years, a large number of studies have
investigated the role of proCPU as a possible risk factor for
thrombotic disease. The outcome, however, is confusing. High
proCPU levels have been reported to be a risk factor for venous
Correspondence: Dirk F. Hendriks, Laboratory of Medical
Biochemistry, University of Antwerp, Antwerp, Belgium.
Tel.: +32 3820 27 27; fax: +32 3 820 27 45; e-mail:
Received 30 November 2006, accepted 3 January 2007
872 Letters to the Editor
� 2007 International Society on Thrombosis and Haemostasis




























