Embed Size (px)
Citation preview

clinical articleJ neurosurg Pediatr 17:19–26, 2016
TraumaTic brain injury (TBI) is a heterogeneous con-dition characterized by marked variability in etiol-ogy and treatment.4,5,10,26 There have been numerous
studies on the treatment of TBI in the adult population,4,6,
8,9,11,15,16,24,25,29 but less research has been performed on treating TBI in pediatric patients.2,5,7,18,21,23 These patients’ still-maturing CNS responds differently to injury and the current treatments available, making it imperative to deter-mine the best course of action to improve outcomes in this population.5,16,18,22
The 2003 Brain Trauma Foundation guidelines,5 which were most recently updated in 2012,14 summarized prac-tice standards for treatment of severe TBI in children. The overarching goal of critical care in treating TBI is to reduce secondary brain injury by limiting cerebral ischemia and optimizing cerebral blood flow.5 Despite these evidence-based guidelines, there is considerable variability in how different physicians and institutions treat severe TBI, and the strength of the evidence is low.10
A study by Pineda et al. in 2013 showed significant ben-
abbreviations CPP = cerebral perfusion pressure; GCS = Glasgow Coma Scale; GOS = Glasgow Outcome Scale; ICP = intracranial pressure; OR = odds ratio; PICU = pediatric intensive care unit; TBI = traumatic brain injury.submitted January 22, 2015. accePted May 11, 2015.include when citing Published online October 9, 2015; DOI: 10.3171/2015.5.PEDS1544.
Standardizing ICU management of pediatric traumatic brain injury is associated with improved outcomes at dischargethomas m. o’lynnger, md, mPh,1 chevis n. shannon, mPh, mba, drPh,1 truc m. le, md,2 amber greeno, nP,3 dai chung, md,3 Fred s. lamb, md, Phd,2 and John c. wellons iii, md, msPh1
Departments of 1Neurological Surgery, 2Pediatrics, Division of Pediatric Critical Care Medicine, and 3Pediatric Surgery, Vanderbilt University Medical Center, Nashville, Tennessee
obJective The goal of critical care in treating traumatic brain injury (TBI) is to reduce secondary brain injury by limit-ing cerebral ischemia and optimizing cerebral blood flow. The authors compared short-term outcomes as defined by discharge disposition and Glasgow Outcome Scale scores in children with TBI before and after the implementation of a protocol that standardized decision-making and interventions among neurosurgeons and pediatric intensivists.methods The authors performed a retrospective pre- and postprotocol study of 128 pediatric patients with severe TBI, as defined by Glasgow Coma Scale (GCS) scores < 8, admitted to a tertiary care center pediatric critical care unit be-tween April 1, 2008, and May 31, 2014. The preprotocol group included 99 patients, and the postprotocol group included 29 patients. The primary outcome of interest was discharge disposition before and after protocol implementation, which took place on April 1, 2013. Ordered logistic regression was used to assess outcomes while accounting for injury sever-ity and clinical parameters. Favorable discharge disposition included discharge home. Unfavorable discharge disposition included discharge to an inpatient facility or death.results Demographics were similar between the treatment periods, as was injury severity as assessed by GCS score (mean 5.43 preprotocol, mean 5.28 postprotocol; p = 0.67). The ordered logistic regression model demonstrated an odds ratio of 4.0 of increasingly favorable outcome in the postprotocol cohort (p = 0.007). Prior to protocol implemen-tation, 63 patients (64%) had unfavorable discharge disposition and 36 patients (36%) had favorable discharge disposi-tion. After protocol implementation, 9 patients (31%) had unfavorable disposition, while 20 patients (69%) had favorable disposition (p = 0.002). In the preprotocol group, 31 patients (31%) died while 6 patients (21%) died after protocol imple-mentation (p = 0.04).conclusions Discharge disposition and mortality rates in pediatric patients with severe TBI improved after imple-mentation of a standardized protocol among caregivers based on best-practice guidelines.http://thejns.org/doi/abs/10.3171/2015.5.PEDS1544Key words critical care; discharge; trauma; traumatic brain injury; protocol
©AANS, 2016 J neurosurg Pediatr Volume 17 • January 2016 19
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

t. m. o’lynnger et al.
J neurosurg Pediatr Volume 17 • January 201620
efit to the implementation of a neurocritical care program with standardized treatment of severe TBI using a proto-col based on the 2003 guidelines.5,21 The authors analyzed discharge disposition in pediatric patients with severe TBI at St. Louis Children’s Hospital before and after imple-mentation of a pediatric neurocritical care program. The protocol was designed to facilitate communication among specialists and to define a plan for monitoring and treat-ment of children with severe TBI. The protocol was in-stituted in 2005, and Pineda et al.’s retrospective cohort study looked at short-term outcomes in patients from 1999 to 2012, comparing preprotocol and postprotocol peri-ods. The authors found that, after protocol implementa-tion, patients had a 67% favorable disposition, defined as home with or without therapy, compared with 48% before protocol implementation. An ordinal regression model indicated that outcomes improved across the spectrum of discharge disposition status and Glasgow Coma Scale (GCS) scores after protocol implementation. Notably, a controlled trial by Chesnut et al. from 2012 demonstrated no significant survival benefit when intracranial pres-sure (ICP)–focused critical care management was used in adolescent and adult patients compared with imaging and clinical examination–based management alone.6,17,20,27 Given these conflicting results, further research into criti-cal care protocols in TBI is necessary.
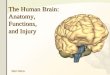
We conducted a study to evaluate short-term outcomes in children with TBI after the implementation of a pro-tocol that standardized decision-making and intervention among neurosurgeons and intensivists (Fig. 1). Our study had 2 a priori aims: 1) compare pre- and postprotocol dis-charge disposition, and 2) determine how Glasgow Out-come Scale (GOS) scores differed between the pre- and poststandardization cohorts.
methodsFor this retrospective cohort study, we used data from
the prospectively maintained Vanderbilt University Medi-cal Center pediatric trauma registry. We included patients less than 18 years of age presenting with TBI with a GCS score of less than 8 between April 1, 2008, and May 31, 2014. All patient electronic medical records with radio-graphic evidence of TBI were reviewed for this study, and the GCS score used for determination of enrollment was based on the examination by the neurosurgery team after resuscitation. This process helped to limit those patients classified as having an artificially low GCS score upon initial emergency department assessment secondary to sedating medications. Variables not maintained prospec-tively were extracted from the electronic medical record, including ICP monitoring and hyperosmolar therapy. Pa-tients were followed for the length of their hospitalization. Those who died in the emergency department were ex-cluded from the study. The Vanderbilt institutional review board approved the study protocol.
Chart review was used to extract parameters, includ-ing age, sex, race, GCS score after resuscitation, need for surgery, injury type and mechanism, discharge disposi-tion, GOS score at discharge, pediatric intensive care unit (PICU) length of stay, total length of stay, use of hyper-
osmolar therapy, use of barbiturates, and ICP monitoring. Due to the complexity of each patient’s clinical narrative and associated multiplicity of variables generated, pro-tocol adherence was challenging to assess. However, use of 3% hypertonic saline instead of mannitol was identi-fied as a surrogate measure of adherence given the 2012 guidelines’ focus on 3% NaCl as treatment for elevated ICP and its consistent availability in the medical record. Any usage of mannitol was considered a protocol devia-tion. Strict usage of solely 3% NaCl for elevated ICP was considered consistent with protocol requirements. Due to the real-time and rapid nature of patient care, we found that compliance for cerebral perfusion pressure (CPP) was challenging to adequately categorize during patients’ hos-pitalization, and it was not clear whether these data were an accurate representation of the actual clinic course. Therefore, this parameter was not used as a surrogate measure of adherence.
Protocol implementationThe TBI protocol was implemented on April 1, 2013.
Prior to 2013, no specific multidisciplinary protocols were used at the institution in the management of pedi-atric brain injury. Variation in the overall management paradigm for patients with severe TBI was common. The evidence-based protocol was developed by a multidisci-plinary group composed of local experts from pediatric services, including neurosurgery, critical care medicine, trauma surgery, and emergency medicine. Source mate-rial that was reviewed included the 2003 Brain Trauma Foundation guidelines5 and the 2012 update14 and insti-tutional protocols from St. Louis Children’s Hospital and Children’s of Alabama. The standardized clinical protocol was devised to guide medical therapy in a stepwise fash-ion, with an emphasis on maintaining CPP and ICP within strict parameters to reduce secondary brain injury by op-timizing cerebral blood flow. The tiered approach to ther-apy focuses first on optimization of oxygen delivery and cerebral perfusion, secondly on CSF diversion, thirdly on maintenance of adequate sedation/analgesia, and finally on maximization of hyperosmolar therapy prior to pro-gression to second-tier therapies, as defined by the 2012 Brain Trauma Foundation guidelines.14 Each intervention step is followed by immediate reevaluation to determine efficacy and need for further escalation. When developing the protocol, it was determined that simplifying the algo-rithm to a single hyperosmolar therapy would decrease variation in care. The protocol used hypertonic saline, so this was used as a surrogate adherence measure. In addi-tion, the 2012 Brain Trauma Foundation guidelines note Level II and III evidence for the use of hypertonic saline. There were no studies about the use of mannitol that met inclusion criteria.
outcomes of interestThe primary outcome was discharge disposition, cat-
egorized as discharge home, discharge to rehabilitation, or death. A single patient was transferred to another acute care facility per the family’s request. This patient was considered to have a “rehabilitation” discharge disposition to maintain the model with only 3 discharge categories.
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

standardizing icu management of pediatric traumatic brain injury
J neurosurg Pediatr Volume 17 • January 2016 21
Our secondary outcome was GOS score at discharge.1 We did not use the extended scale, because we did not believe that the retrospective nature of this analysis was sensitive enough to adequately reproduce the scale in a meaningful way.
statistical analysisNo trends in outcomes were detected in the 5 years of
the preprotocol cohort; as such, this group was analyzed as a whole versus the postprotocol cohort. Study outcomes measured before and after TBI protocol implementation
were compared. Mean age, GCS score, and length of stay between cohorts were compared using the Wilcoxon rank-sum test. Need for surgery, the various injury types and mechanisms, ICP monitor placement, barbiturate use, and hyperosmolar use were compared using the chi-square test and Fisher’s exact test where appropriate. Discharge dis-position and GOS scores were compared using the Krus-kal-Wallis test. Individual groups within discharge dispo-sition were compared using the Wilcoxon rank-sum test.
To compare study outcomes before and after TBI pro-tocol implementation while accounting for potential con-
Fig. 1. Traumatic brain injury protocol. CVP = central venous pressure; EEG = electroencephalogram; ETCO2 = end-tidal CO2; EVD = external ventricular drain; Hct = hematocrit; HOB = head of bed; MAP = mean arterial pressure; Na = sodium; NMB = neuromuscular blockade; NS = normal saline; NSGY = neurosurgery; pCO2 = partial pressure of CO2; TP = transpyloric.
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

t. m. o’lynnger et al.
J neurosurg Pediatr Volume 17 • January 201622
founders, we used multivariate ordered logistic regres-sion. Variables were determined a priori based on clinical significance and perceived importance. These variables were pre- and postprotocol status, GCS score after resus-citation, age, ICP monitor placement, and PICU length of stay. The number of parameters was limited to 5 to pre-vent overfitting the model. In the model, odds ratios (ORs) greater than 1 were associated with increasingly favorable discharge disposition. Ordered logistic regression was also used to predict discharge disposition based on GCS score after resuscitation across the spectrum of TBI severity and to create a plot comparing trends. Statistical significance was set a priori at p < 0.05, and the analysis was conducted using Stata statistical software (version 13, StataCorp).
resultsA total of 128 patients (preprotocol n = 99, postpro-
tocol n = 29) were included in the study. Table 1 shows demographics, injury severity, injury mechanism, length of stay, and ICP treatment parameters. Baseline demo-graphics were not significantly different in the pre- and postprotocol groups. Injury severity as assessed by initial GCS was similar, with a mean of 5.43 in the preprotocol cohort versus 5.28 in the postprotocol group (p = 0.671). Rates of patients requiring a neurosurgical operation were not significantly different (20% preprotocol vs 32% post-protocol; p = 0.648). A significant difference existed in the number of patients presenting with subdural hemorrhage as the predominant radiographic finding (33% preprotocol vs 61% postprotocol; p = 0.009). The injury mechanism was similar, except there was significantly more abusive head trauma in the postprotocol group (48% vs 20%, p = 0.003) and a trend toward fewer motor vehicle colli-sions (35% vs 17%, p = 0.064). Length of stay was not significantly different between the pre- and postprotocol cohorts. Mean PICU length of stay and overall length of stay did not differ between cohorts (p = 0.986 and p = 0.871, respectively). Before protocol implementation, ICP monitors were placed in 46% of patients compared with 28% of patients after protocol implementation (p = 0.07). Use of barbiturates was similar before and after protocol implementation (16% vs 21%; p = 0.68).
Protocol adherenceProtocol adherence was difficult to assess based on ex-
isting electronic medical records, but use of 3% hyperton-ic saline over mannitol was used as a surrogate measure. The protocol calls for preferential use of 3% hypertonic saline for treatment of elevated ICP. After protocol imple-mentation, hypertonic saline was given to a greater per-centage of patients (22% vs 41%, p = 0.04) and mannitol was administered to a smaller percentage (48% vs. 14%, p = 0.001).
short-term outcomesTable 2 shows pre- and postprotocol outcomes. In unad-
justed bivariate analysis, discharge disposition improved significantly after protocol implementation. Prior to pro-tocol implementation, 63 patients (64%) had unfavorable discharge disposition (classified as death or inpatient facil-
ity placement) and 36 patients (36%) had favorable dis-charge disposition (classified as discharge home). After protocol implementation, 9 patients (31%) had unfavorable disposition while 20 patients (69%) had favorable disposi-tion (p = 0.002). The number of deaths was significantly decreased, as were overall unfavorable outcomes. In the preprotocol group, 31 patients (31%) died while 6 patients (21%) died after protocol implementation (p = 0.041). GOS scores were generally improved after the protocol was ini-tiated, but this difference was not statistically significant (p = 0.124).
regression modelsA proportional odds ordered logistic regression model
of discharge disposition revealed that an improvement in outcomes was associated with being in the postprotocol implementation group and increasing GCS score (Table 3). Treatment in the postprotocol implementation group was associated with an OR of 4.046 (p = 0.007) of increas-ingly favorable outcomes. GCS score was associated with an OR of 1.844 (p < 0.001). ICP monitor placement itself was associated with worsening categorical outcome, with an OR of 0.206 (p < 0.001). Increasing PICU length of stay was associated with increasingly favorable outcomes, but
table 1. Patient characteristics: pre- and postprotocol comparison*
Variable Preprotocol Postprotocolp
Value
No. of patients 99 29Demographics Mean age in yrs (SD) 6.54 (5.41) 5.89 (6.03) 0.239 Sex, male 52 (53) 16 (55) 0.802 Race, white 78 (79) 25 (86) 0.375Severity of injury Mean GCS score (SD) 5.43 (1.73) 5.28 (1.85) 0.671 Neurosurgical operation 20 (20) 7 (32) 0.648 Subdural hemorrhage 33 (33) 17 (61) 0.009 Epidural hemorrhage 6 (6) 3 (11) 0.412Injury mechanism MVC 35 (35) 5 (17) 0.064 Pedestrian 7 (7) 1 (3) 0.682 Fall 14 (14) 4 (14) 0.999 Abusive head trauma 20 (20) 14 (48) 0.003 Other 23 (23) 5 (17) 0.493Length of stay in days Mean PICU stay (SD) 7.0 (6.5) 6.1 (4.9) 0.986 Mean hospital stay (SD) 12.3 (14.6) 10.6 (9.5) 0.871ICP Treatment ICP monitor placement 46 (46) 8 (28) 0.070 Hyperosmolar (only 3% NaCl) 22 (22) 12 (41) 0.040 Mannitol w/wo 3% NaCl 48 (48) 4 (14) 0.001 Barbiturates 16 (16) 6 (21) 0.680
MVC = motor vehicle collision.* Data are shown as number and percentage (%) unless otherwise indicated.
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

standardizing icu management of pediatric traumatic brain injury
J neurosurg Pediatr Volume 17 • January 2016 23
the OR close to 1 reveals this association to be clinically immaterial. Age was not associated with outcome in the model. Given that GOS scores were not statistically sig-nificantly improved in the postprotocol group, an ordered logistic regression model did not reveal a significant posi-tive relationship with postprotocol status.
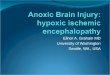
Predicted outcomes improved across the range of GCS scores based on an ordered logistic regression model. Figure 2 demonstrates a dramatic shift in the probability of discharge home in the postprotocol group, as well as a marked decline in the probability of death postproto-col. This remained consistent across the spectrum of GCS scores studied.
discussionTreatment in the postprotocol implementation group
was associated with favorable discharge disposition and decreased mortality. Our ordered logistic regression model demonstrated improved discharge disposition in the post-protocol group with increasing GCS score, as one would expect with decreasing injury severity. In the model, the OR for postprotocol status can be interpreted as follows: in the postprotocol group, patients are 4 times as likely to be discharged home versus the combined disposition of rehabilitation or death, and patients are 4 times as likely to be discharged home or to rehabilitation versus suffer death during hospitalization. Prior to protocol implemen-tation, the mortality rate for severe TBI was 31%, and the rate of discharge home was 36%. This mortality rate is consistent with that in large cohorts in the pediatric trau-matic literature.3,12,30,32 After protocol implementation, the mortality rate dropped to 21%, and the rate of discharge home increased dramatically to 69%. This is a significant improvement and demonstrates the possibility of improv-ing short-term outcomes by standardizing PICU care for pediatric patients with severe TBI.
Our results corroborate the findings of Pineda et al. and other groups that instituted standardized ICU care based on guidelines.11,20,21,29 Cuschieri et al. showed in 2012 that disease-focused implementation of standard op-erating procedures improves outcomes.9 Additionally, a 2014 study by Vavilala et al. demonstrated improvement in mortality and discharge GOS score with increasing ad-herence to clinical indicators derived from the 2012 Brain Trauma Foundation guidelines,31 including maintenance of CPP greater than 40 mm Hg and early start of nutrition. Our results build upon these findings, further reinforcing the evidence that guideline-based care can improve out-comes in pediatric patients with severe TBI.
Our primary outcome of interest was discharge disposi-tion, which was significantly improved in the postprotocol cohort. With regard to discharge status, the neurosurgery, critical care, and trauma surgery teams worked with the physical therapists and case management teams to deter-mine the optimal environment for discharge. There was no intentional influence by providers to have patients dis-charged home versus to rehabilitation. In addition, because cohorts were roughly similar, we anticipate that unmea-sured factors such as family preference and availability of outpatient therapy services would look similar between cohorts, as well. One major benefit of using a 5-year pre-protocol for comparison was that there was no general-ized trend toward discharge disposition status noted prior to protocol implementation. There was a trend toward improvement in the secondary outcome GOS scores, but with 5 distinct categories and low overall sample size, this improvement did not reach the level of statistical signifi-cance. Discharge disposition is a better measure of overall well-being at discharge compared with GOS, which more narrowly represents neurological recovery. However, we chose to additionally analyze the GOS score because of its widespread use and focus on neurological outcome.18 We were unable to use the extended scale due to the retro-spective nature of the analysis, which could not capture the finer variation in disability required of this scale.
The pre- and postprotocol cohorts were similar except the postprotocol group had a higher rate of abusive head trauma as well as a higher rate of subdural hemorrhage as the predominant radiographic finding. Studies have shown that mortality and outcomes are worse in children exposed to abusive head trauma,33 which could potentially lead to an underestimation of the overall improvement in outcomes seen in our postprotocol cohort. The finding that the rate of subdural hemorrhage in the postprotocol cohort was increased is significant given the association between subdural hemorrhage and more severe underly-
table 2. Pre- and postprotocol outcomes*
Variable Preprotocol Postprotocol p Value
Discharge Disposition Death 31 (31) 6 (21) 0.041† Rehabilitation 32 (32) 3 (10) Home 36 (36) 20 (69) 0.017‡ Unfavorable (death/rehab) 63 (64) 9 (31) Favorable (home) 36 (36) 20 (69) 0.002GOS (score) 1 (death) 31 (31) 6 (21) 2 (vegetative) 3 (3) 0 (0) 3 (severe disability) 10 (10) 3 (10) 4 (moderate disability) 19 (19) 5 (17) 5 (good recovery) 36 (36) 15 (52) 0.124§ Unfavorable (1–3) 44 (44) 9 (31) Favorable (4–5) 55 (56) 20 (69) 0.197
*All data shown as number (%) unless otherwise indicated.† Difference between death and home.‡ Difference among home, rehab, and death.§ Difference among all GOS scores.
table 3. ordered logistic regression
Variable OR 95% CI p Value
Group (pre- vs postprotocol) 4.046 1.476–11.087 0.007GCS score 1.844 1.469–2.315 < 0.001Age (yrs) 1.042 0.974–1.114 0.232ICP monitor placement 0.206 0.084–0.501 < 0.001PICU length of stay (days) 1.080 1.001–1.158 0.032
CI = confidence interval.
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

t. m. o’lynnger et al.
J neurosurg Pediatr Volume 17 • January 201624
ing intracranial injury. One would expect outcomes to be worse in the more severely injured group. However, the postprotocol cohort had improved outcomes, so we may conclude that our results are an underestimate of the true impact of the protocol on outcomes.
Our ordered logistic regression model demonstrated im-proved outcomes in the postprotocol group and increasing GCS score, as one would expect with decreasing injury se-verity. Interestingly, ICP monitor placement was a negative predictive factor despite the protocol’s focus on ICP man-agement. We postulated this might be due to bias in initial GCS score reporting, as some patients may initially dem-onstrate a lower GCS score secondary to sedation. When reevaluated prior to ICP monitor placement, some patients’ examinations may improve, resulting in no ICP monitor placement. Those patients who did receive monitors were those with the worst examinations and hence the greatest injury severity. This would decrease expected outcomes in those who ended up receiving an ICP monitor. There still remains controversy within the literature regarding the ef-fectiveness of ICP-based treatment of TBI on outcomes. Although the protocol indicated patients with GCS scores less than 8 should receive an ICP monitor, this intervention was not strictly enforced at the time of the initial examina-tion, as evidenced by an ICP monitor rate of 28% postpro-tocol. The protocol includes the overall management strat-egy, in which placement of an ICP monitor was only a part, albeit an important one. We hypothesize that the protocol, in particular neurosurgical presence and the use of short-acting sedation, enabled a second examination in which the patients may have been found to be improving and not in need of monitor placement.
While our study demonstrates that standardizing care among neurosurgeons and intensivists can improve short-term outcomes, it does not allow us to draw any conclu-sions on the particular effectiveness of ICP-focused care. Our study was not intended to measure adherence to the protocol, although we noted significantly increased use of hypertonic saline and decreased use of mannitol per guideline recommendations for the treatment of elevated ICP. Interestingly, there was a trend toward fewer ICP
monitor placements in the postprotocol cohort. While it could be concluded that the overall proportion of patients receiving ICP monitors being lower in the postprotocol group signals a lack of adherence, the overall goal of this study was not to evaluate the utility of ICP monitors, but rather a focused attention on the evaluation and manage-ment of these complex patients across multiple services, with a standardized approach to assessment and decision-making. A patient receiving an ICP monitor and elevated care in the past for a poor GCS score on the first assess-ment may now be more likely to be placed on the appropri-ate sedating medication for rapid neurological assessment and receive serial examinations over the earliest portions of their hospital course, which may show improvement beyond the need for ICP monitoring. It may be that the attention to a protocol (i.e., the Hawthorne effect) may be at play here, but the overall goal of improved care is achieved. Whether the effect is sustained in this cohort in follow-up assessments or in future patients is a source of ongoing study and remains to be seen. Our intent was to determine how a multidisciplinary approach with com-mitment from various groups to care for these challeng-ing patients impacted care. As evidenced by our results, we believe this did improve outcomes. Those who did not require a monitor were still treated under the protocol with goals to maintain adequate mean arterial pressure, nor-monatremia, adequate hematocrit, sufficient sedation and analgesia, appropriate oxygenation, and glucose control. In addition, the initial neurosurgical examination was used to guide treatment of patients rather than presenting exami-nations in the emergency department, which can often be clouded by patient sedation.
Additionally, our study did not show significant differ-ences in length of stay despite the improvement in out-comes. ICP monitoring–focused care may be associated with longer PICU stays and overall increased length of stay,6,13 but this did not hold true based on the results in this study. Although costs were not measured in this study, length of stay has been validated as a surrogate measure for cost.19 The results of this study could thus imply that out-comes were improved without increasing costs, a signifi-cant benefit in a cost-conscious environment.11,28 However, it is premature to draw conclusions in this regard, because complexity and intensity of therapy may be increased with protocol-based care, as demonstrated in a study by Palmer et al.20 This could ultimately increase overall costs despite similar lengths of stay. However, improving outcomes in pediatric patients would be justified even if costs were in-creased.
There were some limitations to the study, including the retrospective portion of the design, small sample size, and single-center involvement. However, our study attempted to account for these limitations by analyzing outcomes over several years to increase sample size and ensuring our ordered logistic regression model was not overfit with excessive parameters. Ultimately, we were able to demon-strate that short-term outcomes in pediatric patients with severe TBI were improved after a standardized protocol was implemented among caregivers. Further studies are needed that include multiple pediatric critical care centers and assess long-term outcomes.
Fig. 2. Predictive model of discharge disposition probability before and after protocol implementation.
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

standardizing icu management of pediatric traumatic brain injury
J neurosurg Pediatr Volume 17 • January 2016 25
conclusionsDischarge disposition and mortality rates in pediatric
patients with severe TBI improved after implementation among caregivers of a standardized protocol based on best-practice guidelines. This improvement occurred de-spite a higher rate of abusive head trauma in the postproto-col group. Those patients ultimately undergoing ICP mon-itor placement had worse outcomes as a subgroup. Length of stay was not increased in the postprotocol cohort.
acknowledgmentsThe initial protocol that was modified was based in part on
that designed and implemented by José Pineda, MD, and David Limbrick, MD, PhD, at Washington University in St. Louis, and James Johnston, MD, at the University of Alabama–Birmingham. We are grateful for their feedback and willingness to collaborate. In addition, the physicians and caregivers in the Vanderbilt Divi-sion of Pediatric Critical Care and the Department of Neurosurgery are to be acknowledged for their willingness to standardize care for these complex children. The project described was supported by CTSA award no. UL1TR000445 from the National Center for Advancing Translational Sciences, as well as the Vanderbilt Sur-gical Outcomes Center for Kids (SOCKs). Its contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
references 1. Beers SR, Wisniewski SR, Garcia-Filion P, Tian Y, Hahner
T, Berger RP, et al: Validity of a pediatric version of the Glasgow Outcome Scale-Extended. J Neurotrauma 29:1126–1139, 2012
2. Bell MJ, Carpenter J, Au AK, Keating RF, Myseros JS, Yaun A, et al: Development of a pediatric neurocritical care ser-vice. Neurocrit Care 10:4–10, 2009
3. Brown AW, Leibson CL, Malec JF, Perkins PK, Diehl NN, Larson DR: Long-term survival after traumatic brain injury: a population-based analysis. NeuroRehabilitation 19:37–43, 2004
4. Bulger EM, Nathens AB, Rivara FP, Moore M, MacKenzie EJ, Jurkovich GJ: Management of severe head injury: insti-tutional variations in care and effect on outcome. Crit Care Med 30:1870–1876, 2002
5. Carney NA, Chesnut R, Kochanek PM: Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Crit Care Med 31 (6 Suppl):S407–S491, 2003
6. Chesnut RM, Temkin N, Carney N, Dikmen S, Rondina C, Videtta W, et al: A trial of intracranial-pressure monitoring in traumatic brain injury. N Engl J Med 367:2471–2481, 2012
7. Chiaretti A, Piastra M, Pulitanò S, Pietrini D, De Rosa G, Barbaro R, et al: Prognostic factors and outcome of children with severe head injury: an 8-year experience. Childs Nerv Syst 18:129–136, 2002
8. Cremer OL, van Dijk GW, van Wensen E, Brekelmans GJ, Moons KG, Leenen LP, et al: Effect of intracranial pressure monitoring and targeted intensive care on functional outcome after severe head injury. Crit Care Med 33:2207–2213, 2005
9. Cuschieri J, Johnson JL, Sperry J, West MA, Moore EE, Mi-nei JP, et al: Benchmarking outcomes in the critically injured trauma patient and the effect of implementing standard oper-ating procedures. Ann Surg 255:993–999, 2012
10. Dean NP, Boslaugh S, Adelson PD, Pineda JA, Leonard JR: Physician agreement with evidence-based recommendations
for the treatment of severe traumatic brain injury in children. J Neurosurg 107 (5 Suppl):387–391, 2007
11. Fakhry SM, Trask AL, Waller MA, Watts DD: Management of brain-injured patients by an evidence-based medicine pro-tocol improves outcomes and decreases hospital charges. J Trauma 56:492–500, 2004
12. Greenwald BD, Hammond F, Harrison-Felix CL, Nakase-Richardson R, Howe LL, Kreider S: Mortality following traumatic brain injury among individuals unable to follow commands at the time of rehabilitation admission: a NIDRR TBI model systems study. J Neurotrauma [epub ahead of print], 2015
13. Haddad S, Aldawood AS, Alferayan A, Russell NA, Tamim HM, Arabi YM: Relationship between intracranial pressure monitoring and outcomes in severe traumatic brain injury patients. Anaesth Intensive Care 39:1043–1050, 2011
14. Kochanek PM, Carney N, Adelson PD, Ashwal S, Bell MJ, Bratton S, et al: Guidelines for the acute medical manage-ment of severe traumatic brain injury in infants, children, and adolescents–second edition. Pediatr Crit Care Med 13 (Suppl 1):S1–S82, 2012
15. Lane PL, Skoretz TG, Doig G, Girotti MJ: Intracranial pres-sure monitoring and outcomes after traumatic brain injury. Can J Surg 43:442–448, 2000
16. Maas AI, Harrison-Felix CL, Menon D, Adelson PD, Balkin T, Bullock R, et al: Standardizing data collection in traumatic brain injury. J Neurotrauma 28:177–187, 2011
17. Mauritz W, Steltzer H, Bauer P, Dolanski-Aghamanoukjan L, Metnitz P: Monitoring of intracranial pressure in patients with severe traumatic brain injury: an Austrian prospective multicenter study. Intensive Care Med 34:1208–1215, 2008
18. McCauley SR, Wilde EA, Anderson VA, Bedell G, Beers SR, Campbell TF, et al: Recommendations for the use of com-mon outcome measures in pediatric traumatic brain injury research. J Neurotrauma 29:678–705, 2012
19. Newgard CD, Fleischman R, Choo E, Ma OJ, Hedges JR, McConnell KJ: Validation of length of hospital stay as a sur-rogate measure for injury severity and resource use among injury survivors. Acad Emerg Med 17:142–150, 2010
20. Palmer S, Bader MK, Qureshi A, Palmer J, Shaver T, Borzat-ta M, et al: The impact on outcomes in a community hospital setting of using the AANS traumatic brain injury guidelines. J Trauma 50:657–664, 2001
21. Pineda JA, Leonard JR, Mazotas IG, Noetzel M, Limbrick DD, Keller MS, et al: Effect of implementation of a paediat-ric neurocritical care programme on outcomes after severe traumatic brain injury: a retrospective cohort study. Lancet Neurol 12:45–52, 2013
22. Potoka DA, Schall LC, Gardner MJ, Stafford PW, Peitzman AB, Ford HR: Impact of pediatric trauma centers on mortal-ity in a statewide system. J Trauma 49:237–245, 2000
23. Salorio CF, Slomine BS, Guerguerian AM, Christensen JR, White JR, Natale JE, et al: Intensive care unit variables and outcome after pediatric traumatic brain injury: a retrospec-tive study of survivors. Pediatr Crit Care Med 9:47–53, 2008
24. Saul TG, Ducker TB: Effect of intracranial pressure moni-toring and aggressive treatment on mortality in severe head injury. J Neurosurg 56:498–503, 1982
25. Saul TG, Ducker TB: Intracranial pressure monitoring in patients with severe head injury. Am Surg 48:477–480, 1982
26. Scaife ER, Statler KD: Traumatic brain injury: preferred methods and targets for resuscitation. Curr Opin Pediatr 22:339–345, 2010
27. Shafi S, Diaz-Arrastia R, Madden C, Gentilello L: Intracrani-al pressure monitoring in brain-injured patients is associated with worsening of survival. J Trauma 64:335–340, 2008
28. Shi J, Xiang H, Wheeler K, Smith GA, Stallones L, Groner J, et al: Costs, mortality likelihood and outcomes of hospital-
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC

t. m. o’lynnger et al.
J neurosurg Pediatr Volume 17 • January 201626
ized US children with traumatic brain injuries. Brain Inj 23:602–611, 2009
29. Stein SC, Georgoff P, Meghan S, Mirza KL, El Falaky OM: Relationship of aggressive monitoring and treatment to im-proved outcomes in severe traumatic brain injury. J Neuro-surg 112:1105–1112, 2010
30. Tude Melo JR, Di Rocco F, Blanot S, Oliveira-Filho J, Rou-jeau T, Sainte-Rose C, et al: Mortality in children with severe head trauma: predictive factors and proposal for a new pre-dictive scale. Neurosurgery 67:1542–1547, 2010
31. Vavilala MS, Kernic MA, Wang J, Kannan N, Mink RB, Wainwright MS, et al: Acute care clinical indicators associat-ed with discharge outcomes in children with severe traumatic brain injury. Crit Care Med 42:2258–2266, 2014
32. White JR, Farukhi Z, Bull C, Christensen J, Gordon T, Paidas C, et al: Predictors of outcome in severely head-injured children. Crit Care Med 29:534–540, 2001
33. Xiang J, Shi J, Wheeler KK, Yeates KO, Taylor HG, Smith GA: Paediatric patients with abusive head trauma treated in US Emergency Departments, 2006–2009. Brain Inj 27:1555–1561, 2013
disclosureThe authors report no conflict of interest concerning the materi-
als or methods used in this study or the findings specified in this paper.
author contributionsConception and design: O’Lynnger, Shannon, Lamb, Wellons. Acquisition of data: O’Lynnger, Greeno. Analysis and inter-pretation of data: all authors. Drafting the article: O’Lynnger, Shannon, Le, Wellons. Critically revising the article: O’Lynnger, Shannon, Le, Wellons. Reviewed submitted version of manu-script: all authors. Approved the final version of the manu-script on behalf of all authors: O’Lynnger. Statistical analysis: O’Lynnger, Shannon. Administrative/technical/material support: Greeno. Study supervision: Chung, Lamb, Wellons.
supplemental informationPrevious PresentationPortions of this work were presented in poster form at the AANS/CNS Section on Pediatric Neurosurgery, Amelia Island, Florida, December 3, 2014.
correspondenceThomas M. O’Lynnger, Pediatric Neurosurgery, Vanderbilt University Medical Center, 9222 Doctors’ Office Tower, 2200 Children’s Way, Nashville, TN 37232-9557. email: [email protected].
Unauthenticated | Downloaded 08/18/20 01:35 AM UTC