Embed Size (px)
Citation preview

Stapled haemorrhoidopexyIan Botterill
Dept Colorectal SurgerySt James’ University Hospital
Leeds

Barry Wood
Lancashire & England
Dennis Lillee
Western Australia & Australia

Ideal surgical treatment of haemorrhoids
Minimal pain, short stay, rapid recuperation, low morbidity, lasting benefit

The Longo procedure
1st performed 1993 1st reported 1998
Antonio Longo

terminology
• Stapled haemorrhoidopexyStapled haemorrhoidopexy
• Stapled haemorrhoidectomy• Circular stapled haemorrhoidectomy• Circular stapled anoplasty• PPH• Stapled prolapsectomy• Transverse mucosal prolapsectomy• Longo procedure
Premise
• haemorrhoids contribute to continence
• haemorrhoids worth preserving
• weakened of suspensory lig of rectum
• ‘pexy’ addresses the prolapse

Surgical rationale
• excision of cylinder of rectal mucosa → replacement of haemorrhoids in anal canal
• vascular interruption → shrinkage of prolapsed component
• avoidance of anal wound reduces pain
• haemorrhoidectomy only treats the consequence of prolapse

Serious adverse events
• persistent faecal urgency• persistent anal pain
• recto-vaginal fistula• retroperitoneal perforation• rectal perforation • pelvic sepsis• Fournier’s gangrene• rectal pocket syndrome
Major complications of OP care
• phenol prostatitis sclero
• pelvic cellulitis sclero / band
• retroperitoneal abscess sclero
• clostridial infection band
• tetanus band
• systemic sepsis band
• severe pain band

New technology
• apparent benefits & pitfalls
• obvious parallels -laparoscopic cholecystectomy-laparoscopic colorectal surgery-laparoscopic hernia repair
• learning curve
• NICE 2003 (& Sept 2007)

Training
• training centresLeeds, Dundee, Guildford, Colchester, Hamburg
• preceptorship
• audit-local (pathology / outcomes)-national (ACPGBI PPH database)

Patient selection-indications
- prolapsing / prolapsed haemorrhoids
- circumferential haemorrhoids
Patient selection-relative contraindications
any haemorrhoid operation• diabetics / immuno-suppressed• bleeding diasthesis• faecal incontinence• Crohn’s
specific to stapled haemorrhoidopexy• deep ‘funnel shaped’ perineum• large anal skin tags• narrow gap between ischial spines

Consent for open / stapled Prone jack-knife allows ↓engorgement of anal cushions
Pre-op GTN / diltiazem

Positioning / placement 4 quadrant suturesLubrication anal canal

Gentle dilation with obturator aloneReduction haemorrhoids

Insertion CAD & obturatorFixation of CAD
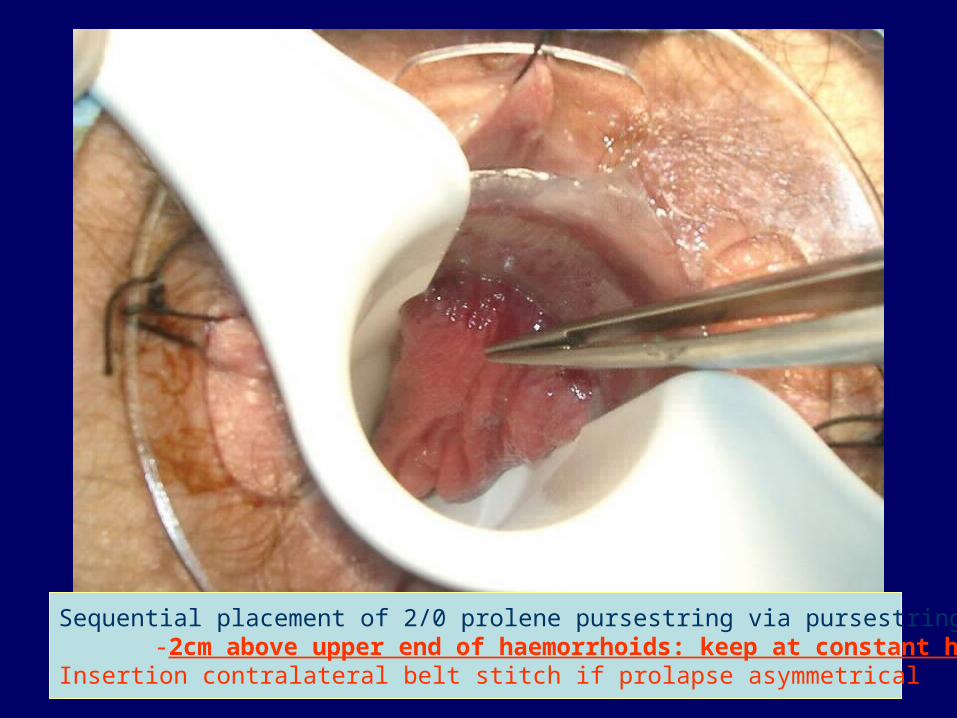
Sequential placement of 2/0 prolene pursestring via pursestring anoscope-2cm above upper end of haemorrhoids: keep at constant height
Insertion contralateral belt stitch if prolapse asymmetrical

Insertion fully opened PPH03 gun (along axis of rectum)
Crochet hook retrieval of pursestring (each side of gun housing)
Traction on pursestring during gun closure

Complete gun closure check vagina - saline infiltration helpful Ensure closed gun @ ‘4cm’ on housing prior to firing

½ turn to release gunsutured haemostasis (4/0 vicryl) – much less common using newer PPH03
avoid diathermy


Post-op pain relief
• Perineal field block -40ml 0.475% ropivicaine
-6 x 5ml columns ant & post
-2 x 5ml submucosal columns
• voltarol & paracetamol pr• lactulose• ?metronidazole• no anal canal dressing
Discharge instructions-pain / retention urine / fever
-avoidance anal intercourse
See @ 4-6/52 in case need dilation
Role of pathology
• audit -correlation with outcome -inclusion of glandular / squamous -inclusion of smooth m deep to squamous epithelium
• unexpected pathology
Role of pathology
• n=84
• 19/84 squamous epithelium in donut (M>>F) - no difference in Cleveland Clinic continence score
• 6/19 had smooth m deep to squamous epithelium- no difference in Cleveland Clinic continence
score
• 79/84 contained smooth muscle
Shanmugam et al Colorectal Dis 2005;7:172-5

Role of pathology
• n=68
• 64/68 contained smooth muscle
• 24/64 had smooth muscle with overlying squamous cell / transitional epithelium
• no outcome difference
Kam et al. DCR 2005:48:1437-41

results
• >25 RCTs
• 4 reviews (inc. 2 position statements)
• forthcoming meta-analysis
• 1 NICE appraisal (2nd planned)
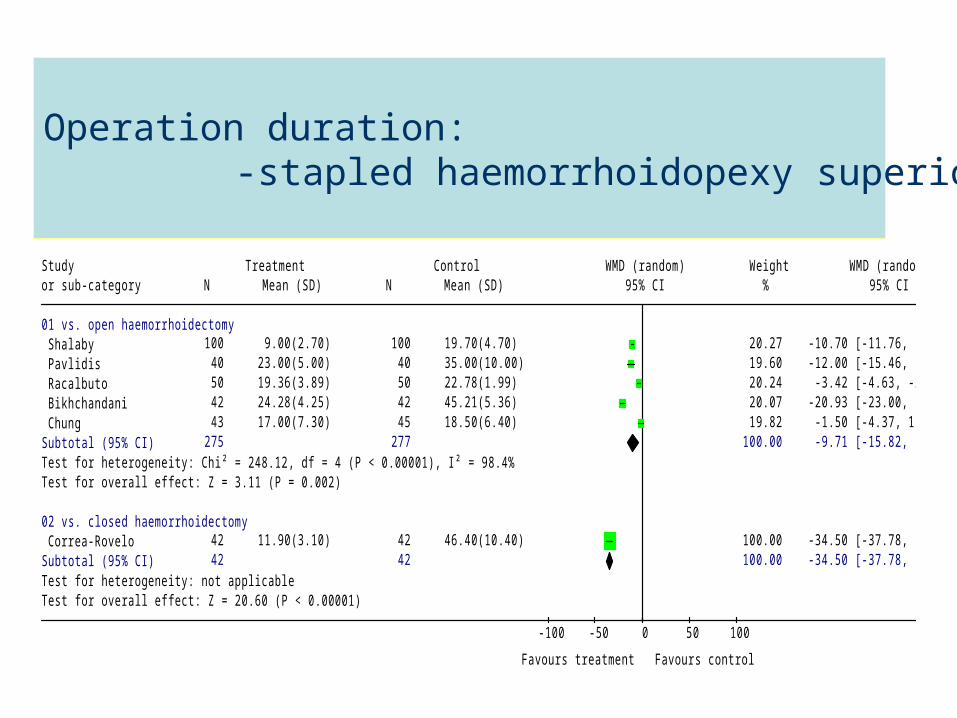
Figure 11: Operation time: subtotals vs. Milligan-Morgan/Ferguson
haemorrhoidectomy (random effects model). Review: PPH U1680Comparison: 01 PPH vs. Conventional Outcome: 22 Operation time
Study Treatment Control WMD (random) Weight WMD (random)or sub-category N Mean (SD) N Mean (SD) 95% CI % 95% CI
01 vs. open haemorrhoidectomyShalaby 100 9.00(2.70) 100 19.70(4.70) 20.27 -10.70 [-11.76, -9.64] Pavlidis 40 23.00(5.00) 40 35.00(10.00) 19.60 -12.00 [-15.46, -8.54] Racalbuto 50 19.36(3.89) 50 22.78(1.99) 20.24 -3.42 [-4.63, -2.21] Bikhchandani 42 24.28(4.25) 42 45.21(5.36) 20.07 -20.93 [-23.00, -18.86] Chung 43 17.00(7.30) 45 18.50(6.40) 19.82 -1.50 [-4.37, 1.37]
Subtotal (95% CI) 275 277 100.00 -9.71 [-15.82, -3.60]Test for heterogeneity: Chi² = 248.12, df = 4 (P < 0.00001), I² = 98.4%Test for overall effect: Z = 3.11 (P = 0.002)
02 vs. closed haemorrhoidectomyCorrea-Rovelo 42 11.90(3.10) 42 46.40(10.40) 100.00 -34.50 [-37.78, -31.22]
Subtotal (95% CI) 42 42 100.00 -34.50 [-37.78, -31.22]Test for heterogeneity: not applicableTest for overall effect: Z = 20.60 (P < 0.00001)
-100 -50 0 50 100
Favours treatment Favours control
Operation duration:-stapled haemorrhoidopexy superior

Review: PPH U1680Comparison: 01 PPH vs. Conventional Outcome: 08 pain VAS 24 h
Study Treatment Control WMD (random) Weight WMD (random)or sub-category N Mean (SD) N Mean (SD) 95% CI % 95% CI
01 vs. open haemorrhoidectomyShalaby 100 2.50(1.30) 100 7.60(0.70) 27.80 -5.10 [-5.39, -4.81] Pavlidis 40 0.70(0.20) 40 2.40(0.50) 27.90 -1.70 [-1.87, -1.53] Cheetham 15 3.30(4.88) 16 6.10(3.77) 17.22 -2.80 [-5.88, 0.28] Bikhchandani 42 3.64(1.79) 42 6.36(1.44) 27.09 -2.72 [-3.41, -2.03]
Subtotal (95% CI) 197 198 100.00 -3.11 [-5.37, -0.85]Test for heterogeneity: Chi² = 398.18, df = 3 (P < 0.00001), I² = 99.2%Test for overall effect: Z = 2.69 (P = 0.007)
02 vs. closed haemorrhoidectomyCorrea-Rovelo 42 2.80(1.40) 42 5.50(1.40) 55.22 -2.70 [-3.30, -2.10] Hetzer 20 2.70(2.20) 20 6.30(4.00) 44.78 -3.60 [-5.60, -1.60]
Subtotal (95% CI) 62 62 100.00 -2.77 [-3.35, -2.20]Test for heterogeneity: Chi² = 0.71, df = 1 (P = 0.40), I² = 0%Test for overall effect: Z = 9.48 (P < 0.00001)
-10 -5 0 5 10
Favours treatment Favours control
Pain – favours stapled haemorrhoidopexyPain: stapled haemorrhoidopexy superior

Figure 8: Persistent/occasional pain mid term (overall - fixed effects model). Review: PPH U1680Comparison: 01 PPH vs. Conventional Outcome: 12 persistent/occasional pain (mid term)
Study Treatment Control OR (fixed) Weight OR (fixed)or sub-category n/N n/N 95% CI % 95% CI
Ganio 10/50 15/50 38.25 0.58 [0.23, 1.46] Correa-Rovelo 2/41 8/41 24.25 0.21 [0.04, 1.07] Ortiz 1/27 0/28 1.48 3.23 [0.13, 82.71] Pavlidis 6/37 7/37 18.69 0.83 [0.25, 2.76] Bikhchandani 0/42 5/42 17.33 0.08 [0.00, 1.50]
Total (95% CI) 197 198 100.00 0.49 [0.27, 0.90]Total events: 19 (Treatment), 35 (Control)Test for heterogeneity: Chi² = 4.67, df = 4 (P = 0.32), I² = 14.4%Test for overall effect: Z = 2.32 (P = 0.02)
0.01 0.1 1 10 100
Favours treatment Favours control
Persistent mid-term pain: stapled haemorrhoidopexy superior

Figure 12: Hospital stay: stapled haemorrhoidopexy vs. Milligan-Morgan
(overall - random effects model). Review: PPH U1680Comparison: 01 PPH vs. Conventional Outcome: 25 hospital stay
Study Treatment Control WMD (random) Weight WMD (random)or sub-category N Mean (SD) N Mean (SD) 95% CI % 95% CI
01 vs. open haemorrhoidectomyGanio 50 1.35(0.54) 50 2.40(1.80) 13.23 -1.05 [-1.57, -0.53] Shalaby 100 1.10(0.20) 100 2.20(0.50) 28.53 -1.10 [-1.21, -0.99] Pavlidis 40 1.70(0.50) 40 3.20(0.30) 26.04 -1.50 [-1.68, -1.32] Bikhchandani 42 1.24(0.62) 42 2.76(1.01) 18.76 -1.52 [-1.88, -1.16] Gravie 63 2.20(1.20) 63 3.10(1.70) 13.44 -0.90 [-1.41, -0.39]
Subtotal (95% CI) 295 295 100.00 -1.25 [-1.50, -1.00]Test for heterogeneity: Chi² = 18.70, df = 4 (P = 0.0009), I² = 78.6%Test for overall effect: Z = 9.66 (P < 0.00001)
Total (95% CI) 295 295 100.00 -1.25 [-1.50, -1.00]Test for heterogeneity: Chi² = 18.70, df = 4 (P = 0.0009), I² = 78.6%Test for overall effect: Z = 9.66 (P < 0.00001)
-4 -2 0 2 4
Favours treatment Favours control
Hospital stay:stapled haemorrhoidopexy superior
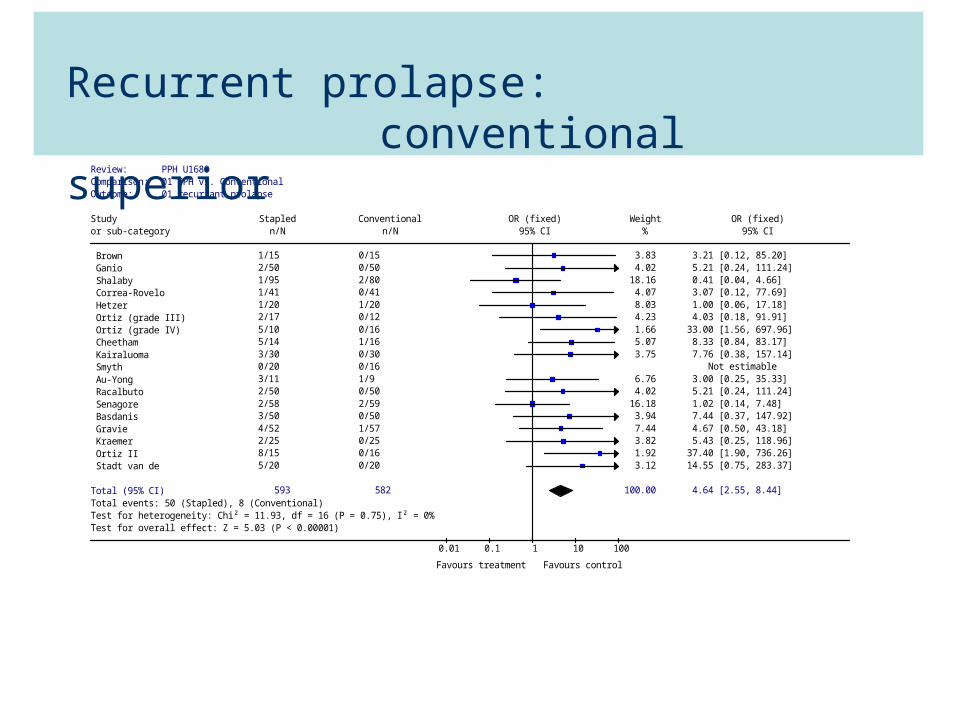
Review: PPH U1680Comparison: 01 PPH vs. Conventional Outcome: 01 recurrant prolapse
Study Stapled Conventional OR (fixed) Weight OR (fixed)or sub-category n/N n/N 95% CI % 95% CI
Brown 1/15 0/15 3.83 3.21 [0.12, 85.20] Ganio 2/50 0/50 4.02 5.21 [0.24, 111.24] Shalaby 1/95 2/80 18.16 0.41 [0.04, 4.66] Correa-Rovelo 1/41 0/41 4.07 3.07 [0.12, 77.69] Hetzer 1/20 1/20 8.03 1.00 [0.06, 17.18] Ortiz (grade III) 2/17 0/12 4.23 4.03 [0.18, 91.91] Ortiz (grade IV) 5/10 0/16 1.66 33.00 [1.56, 697.96] Cheetham 5/14 1/16 5.07 8.33 [0.84, 83.17] Kairaluoma 3/30 0/30 3.75 7.76 [0.38, 157.14] Smyth 0/20 0/16 Not estimable Au-Yong 3/11 1/9 6.76 3.00 [0.25, 35.33] Racalbuto 2/50 0/50 4.02 5.21 [0.24, 111.24] Senagore 2/58 2/59 16.18 1.02 [0.14, 7.48] Basdanis 3/50 0/50 3.94 7.44 [0.37, 147.92] Gravie 4/52 1/57 7.44 4.67 [0.50, 43.18] Kraemer 2/25 0/25 3.82 5.43 [0.25, 118.96] Ortiz II 8/15 0/16 1.92 37.40 [1.90, 736.26] Stadt van de 5/20 0/20 3.12 14.55 [0.75, 283.37]
Total (95% CI) 593 582 100.00 4.64 [2.55, 8.44]Total events: 50 (Stapled), 8 (Conventional)Test for heterogeneity: Chi² = 11.93, df = 16 (P = 0.75), I² = 0%Test for overall effect: Z = 5.03 (P < 0.00001)
0.01 0.1 1 10 100
Favours treatment Favours control
Recurrent prolapse: conventional superior

Figure 10: Redo-surgery: stapled haemorrhoidopexy vs Milligan-
Morgan/Ferguson (overall - random effects model). Review: PPH U1680Comparison: 01 PPH vs. Conventional Outcome: 07 re-surgery in total
Study Treatment Control OR (random) Weight OR (random)or sub-category n/N n/N 95% CI % 95% CI
01 vs. open haemorrhoidectomy Mehigan 1/20 3/20 5.70 0.30 [0.03, 3.15] Shalaby 1/100 2/100 5.49 0.49 [0.04, 5.55] Ortiz 3/27 0/28 3.90 8.14 [0.40, 165.53] Pavlidis 3/40 2/40 7.95 1.54 [0.24, 9.75] Cheetham 3/15 1/16 5.59 3.75 [0.34, 40.81] Kairaluoma 7/30 1/30 6.43 8.83 [1.01, 76.96] Palimento 1/37 1/37 4.36 1.00 [0.06, 16.61] Au-Yong 1/11 0/11 3.33 3.29 [0.12, 89.81] Racalbuto 7/50 3/50 10.71 2.55 [0.62, 10.49] Basdanis 1/50 1/45 4.38 0.90 [0.05, 14.79] Bikhchandani 1/42 1/42 4.37 1.00 [0.06, 16.53] Chung 3/43 1/45 5.89 3.30 [0.33, 33.02] Ortiz II 5/15 1/16 5.94 7.50 [0.76, 74.16] Stadt van de 4/20 0/20 3.94 11.18 [0.56, 222.98] Subtotal (95% CI) 500 500 77.98 2.29 [1.23, 4.25]Total events: 41 (Treatment), 17 (Control)Test for heterogeneity: Chi² = 10.36, df = 13 (P = 0.66), I² = 0%Test for overall effect: Z = 2.62 (P = 0.009)
02 vs. closed haemorrhoidectomy Correa-Rovelo 1/42 0/42 3.47 3.07 [0.12, 77.59] Hetzer 3/20 1/20 5.70 3.35 [0.32, 35.36] Senagore 4/77 15/79 12.85 0.23 [0.07, 0.74] Subtotal (95% CI) 139 141 22.02 0.97 [0.13, 7.45]Total events: 8 (Treatment), 16 (Control)Test for heterogeneity: Chi² = 5.39, df = 2 (P = 0.07), I² = 62.9%Test for overall effect: Z = 0.03 (P = 0.98)
Total (95% CI) 639 641 100.00 1.76 [0.91, 3.39]Total events: 49 (Treatment), 33 (Control)Test for heterogeneity: Chi² = 22.72, df = 16 (P = 0.12), I² = 29.6%Test for overall effect: Z = 1.68 (P = 0.09)
0.01 0.1 1 10 100
Favours treatment Favours control
Redo surgery: - stapled haemorrhoidopexy & closed equivalent- open superior to stapled haemorrhoidopexy

Figure 14: Post-operative incontinence - long-term follow-up: stapled
haemorrhoidopexy vs. Milligan-Morgan (fixed effects model) Review: PPH_U1411Comparison: 01 PPH versus MM Outcome: 01 Anal Incontinence
Study PPH MM RR (fixed) Weight RR (fixed)or sub-category n/N n/N 95% CI % 95% CI Quality
01 Small studies Au-Yong 1/11 2/9 21.01 0.41 [0.04, 3.82] D v.d.Stadt 0/20 0/20 Not estimable D Subtotal (95% CI) 31 29 21.01 0.41 [0.04, 3.82]Total events: 1 (PPH), 2 (MM)Test for heterogeneity: not applicableTest for overall effect: Z = 0.78 (P = 0.43)
02 large studies Racalbuto 0/50 3/50 33.43 0.14 [0.01, 2.70] D Gravie 6/52 5/57 45.56 1.32 [0.43, 4.05] D Subtotal (95% CI) 102 107 78.99 0.82 [0.31, 2.17]Total events: 6 (PPH), 8 (MM)Test for heterogeneity: Chi² = 2.04, df = 1 (P = 0.15), I² = 50.9%Test for overall effect: Z = 0.40 (P = 0.69)
Total (95% CI) 133 136 100.00 0.73 [0.30, 1.78]Total events: 7 (PPH), 10 (MM)Test for heterogeneity: Chi² = 2.49, df = 2 (P = 0.29), I² = 19.6%Test for overall effect: Z = 0.69 (P = 0.49)
0.1 0.2 0.5 1 2 5 10
Favours PPH Favours MM
Post-operative incontinence:no difference

Figure 13: Post-operative anal stenosis – long-term follow-up: stapled
haemorrhoidopexy vs. Milligan -Morgan (random effects model). Review: PPH_U1411Comparison: 01 PPH versus MM Outcome: 03 Stenosis
Study PPH MM RR (random) Weight RR (random)or sub-category n/N n/N 95% CI % 95% CI Quality
01 Small studies Au-Yong 2/9 2/8 61.66 0.89 [0.16, 4.93] D v.d.Stadt 0/20 2/20 20.44 0.20 [0.01, 3.92] D Subtotal (95% CI) 29 28 82.09 0.61 [0.14, 2.71]Total events: 2 (PPH), 4 (MM)Test for heterogeneity: Chi² = 0.78, df = 1 (P = 0.38), I² = 0%Test for overall effect: Z = 0.65 (P = 0.52)
02 large studies Racalbuto 0/50 0/50 Not estimable D Gravie 0/52 1/57 17.91 0.36 [0.02, 8.76] D Subtotal (95% CI) 102 107 17.91 0.36 [0.02, 8.76]Total events: 0 (PPH), 1 (MM)Test for heterogeneity: not applicableTest for overall effect: Z = 0.62 (P = 0.53)
Total (95% CI) 131 135 100.00 0.56 [0.15, 2.14]Total events: 2 (PPH), 5 (MM)Test for heterogeneity: Chi² = 0.86, df = 2 (P = 0.65), I² = 0%Test for overall effect: Z = 0.85 (P = 0.40)
0.1 0.2 0.5 1 2 5 10
Favours PPH Favours MM
Anal stenosis:no difference

Cost-benefit modelling
• gun cost £350• bed cost / night £200• theatre / hr £1000
• if the above factors are assumed- cost equivalence to provider
• disregards out of hospital costs
Leeds Colorectal

Summary
• early concerns not sustained based on the evidence
• proven benefits: - ↓operative time / ↓ I-P stay / ↑ return to work - ↓post-op pain / ↓ bleeding / ↓analgesia - ↓stenosis
• but: - ↑ recurrent prolapse (definitions vary) - ↑ rate redo surgery
Leeds Colorectal

Choose your tools appropriately

Causes of urgency• ? loss anal transitional zone:
- not proven
• ? loss of RAIR: - disproven
• ? loss of upper part of IAS: possible - long anal canal
• ? IAS fragmentation- possible
- gentle dil’n / chem. sphincterotomy / LA block
• ? pre-existing anal sphincter injury