Embed Size (px)
Citation preview
Page | 1
State Level Consolidated
Report of Bihar
Findings of
Community Monitoring for Improving
Informed Choice and Quality of Care in Family
Planning
Centre for Health and Social Justice, New Delhi
Page | 2
Content
List of Acronyms
ANM – Auxiliary Nurse Midwife
ASHA – Accredited Social Health Activist
AWW – Anganwadi Worker
CHSJ – Centre for Health and Social Justice
CHC – Community Health Centre
CBM –Community Based Monitoring
CMO – Chief Medical Officer
CSO – Civil Society Organisation
FGD – Focus Group Discussion
GOI – Government of India
IUD – Intra Uterine Device
MOIC – Medical Officer in-Charge
NRHM – National Rural Health Mission
PRI – Panchayati Raj Institution
PHC – Primary Health Centre
OCP – Oral Contraceptive Pills
Content Page number
1 Family Planning in India 3
2 The Process 3
3 Methodology Adopted 4
4 Major Findings -District Wise 6
5 District Level Dialogues and Sharing 8
6 State Level Score Card 10
7 District wise Findings of Community Monitoring Process 11
8 Conclusion 20
9 Annexure of Media Coverage of District Level Dialogue 21

Page | 3
1. Family Planning in India
Family planning within the context of health is one of the flagship programmes of the Government of
India (GoI). India started its national family planning programme in 1951 which has a long and
chequered history. There was an obsessive fear of explosive population growth which led to the
introduction of coercive components like targets, incentives and penalties for the community as well
as the health worker. However, the programme was often reduced to provision of female sterilisation.
In rapidly conducted sterilisation camps the quality of surgical procedures was poor. After signing on
to the Program of Action of the International Conference on Population and Development (PoA-
ICPD, 1994), the GoI made many changes in the way the family planning programme was designed
and implemented. Method specific targets were abandoned; standard operating procedures and quality
assurance mechanisms were introduced. Today the GoI has shifted its programme focus from female
sterilisation to an approach focusing more on birth spacing and temporary methods. However, India is
a large country and the manner in which programmes are delivered on the ground can be very
different from the policy intentions. There is need to understand whether couples especially women
can access high quality family planning services according to their needs and choice which is the true
intention of the family planning programme.
2. The Process
Community based monitoring (CBM) methodology has been developed within the auspices of the
National Rural Health Mission to understand the communities’ experience of service delivery. It is
also seen as an integral component of community participation as well as of accountability
mechanisms, and is aimed at improving the quality of services demanded by the community and
delivered by the health system.
CBM methodology has been used in this initiative since it increases participation of the community
and civil society organisations (CSOs). In an effort to strengthen people’s access to quality family
planning services and build understanding on quality of care in family planning, five CSOs undertook
community based monitoring on family planning services in selected villages in five districts of Bihar
Pradesh, Bhagalpur, Nawada, Nalanda, Kishanganj and Patna. The CBM exercise included
discussions with women where the experience of women who are intended as well as actual
beneficiaries of the family planning programme was understood. Interviews were conducted with a
selected group of ASHAs in each district and the Medical Officer and ANM of one Block in each
district were also interviewed. The district level public dialogues based on the findings of CBM has
been undertaken in five districts of Uttar Pradesh during last two months focussing on informed
choice and quality of care in family planning. In district level Jansamvad, score cards with findings
and experiences of family planning users were shared with community, health service providers,
Panchayati Raj Institution (PRI) members and media.
Objectives:
The main objectives of the study are:
To monitor compliance of quality standards in family planning services.
To advocate for improvement of quality and fulfillment of reproductive rights.
3. Methodology Adopted
In each of the four districts of Bihar, one village each from five panchayats in one block in the district
were selected for the study. The entire survey in five districts was done by women selected from the
Page | 4
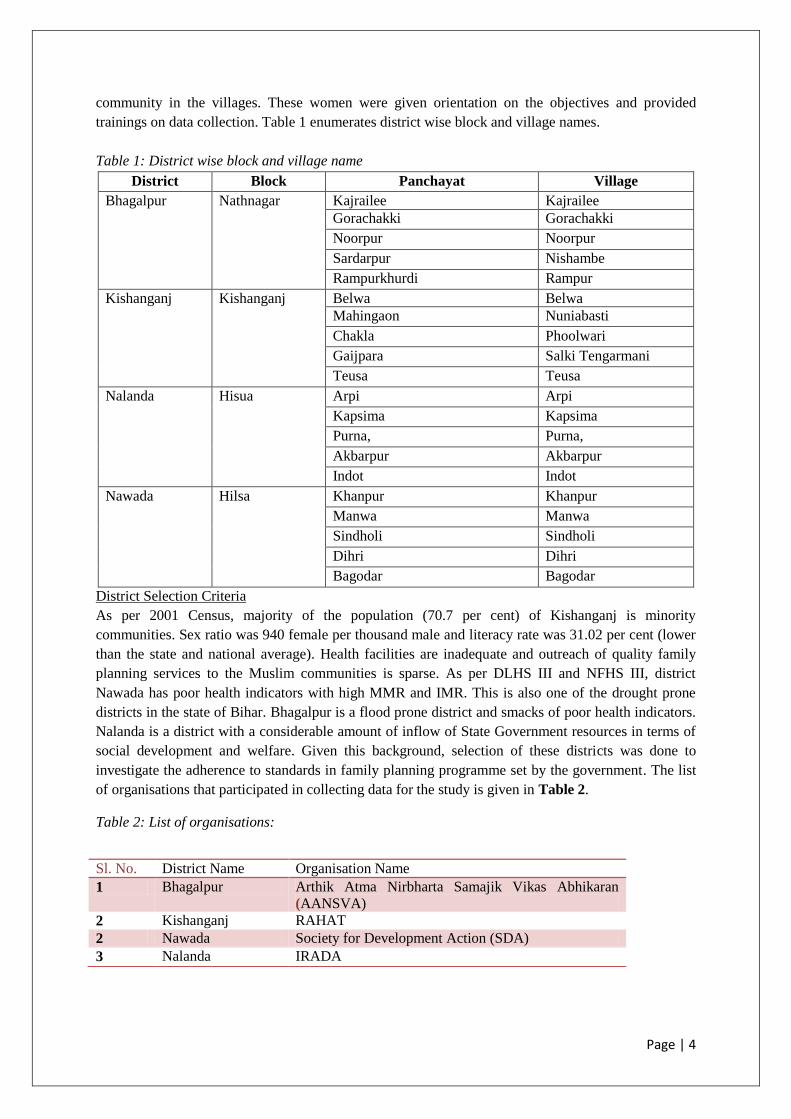
community in the villages. These women were given orientation on the objectives and provided
trainings on data collection. Table 1 enumerates district wise block and village names.
Table 1: District wise block and village name
District Block Panchayat Village
Bhagalpur Nathnagar Kajrailee Kajrailee
Gorachakki Gorachakki
Noorpur Noorpur
Sardarpur Nishambe
Rampurkhurdi Rampur
Kishanganj Kishanganj Belwa Belwa
Mahingaon Nuniabasti
Chakla Phoolwari
Gaijpara Salki Tengarmani
Teusa Teusa
Nalanda Hisua Arpi Arpi
Kapsima Kapsima
Purna, Purna,
Akbarpur Akbarpur
Indot Indot
Nawada Hilsa Khanpur Khanpur
Manwa Manwa
Sindholi Sindholi
Dihri Dihri
Bagodar Bagodar
District Selection Criteria
As per 2001 Census, majority of the population (70.7 per cent) of Kishanganj is minority
communities. Sex ratio was 940 female per thousand male and literacy rate was 31.02 per cent (lower
than the state and national average). Health facilities are inadequate and outreach of quality family
planning services to the Muslim communities is sparse. As per DLHS III and NFHS III, district
Nawada has poor health indicators with high MMR and IMR. This is also one of the drought prone
districts in the state of Bihar. Bhagalpur is a flood prone district and smacks of poor health indicators.
Nalanda is a district with a considerable amount of inflow of State Government resources in terms of
social development and welfare. Given this background, selection of these districts was done to
investigate the adherence to standards in family planning programme set by the government. The list
of organisations that participated in collecting data for the study is given in Table 2.
Table 2: List of organisations:
Sl. No. District Name Organisation Name
1 Bhagalpur Arthik Atma Nirbharta Samajik Vikas Abhikaran
(AANSVA)
2 Kishanganj RAHAT
2 Nawada Society for Development Action (SDA)
3 Nalanda IRADA
Page | 5
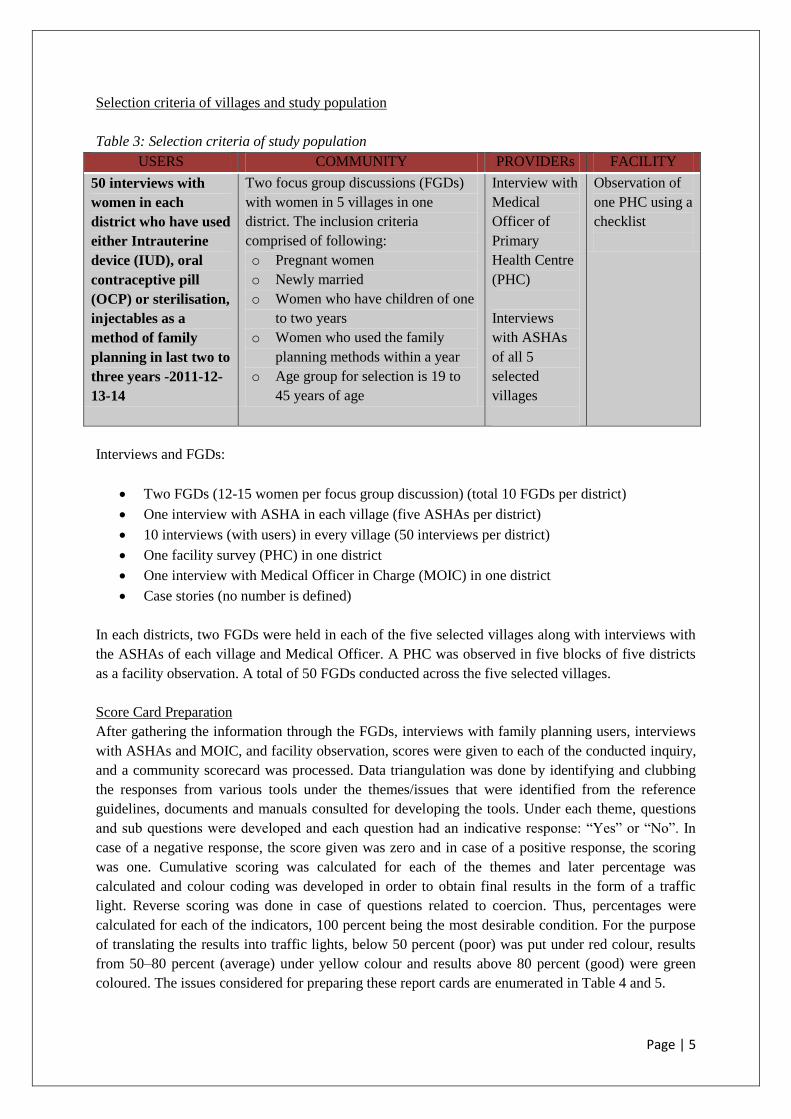
Selection criteria of villages and study population
Table 3: Selection criteria of study population
USERS COMMUNITY PROVIDERs FACILITY
50 interviews with
women in each
district who have used
either Intrauterine
device (IUD), oral
contraceptive pill
(OCP) or sterilisation,
injectables as a
method of family
planning in last two to
three years -2011-12-
13-14
Two focus group discussions (FGDs)
with women in 5 villages in one
district. The inclusion criteria
comprised of following:
o Pregnant women
o Newly married
o Women who have children of one
to two years
o Women who used the family
planning methods within a year
o Age group for selection is 19 to
45 years of age
Interview with
Medical
Officer of
Primary
Health Centre
(PHC)
Interviews
with ASHAs
of all 5
selected
villages
Observation of
one PHC using a
checklist
Interviews and FGDs:
Two FGDs (12-15 women per focus group discussion) (total 10 FGDs per district)
One interview with ASHA in each village (five ASHAs per district)
10 interviews (with users) in every village (50 interviews per district)
One facility survey (PHC) in one district
One interview with Medical Officer in Charge (MOIC) in one district
Case stories (no number is defined)
In each districts, two FGDs were held in each of the five selected villages along with interviews with
the ASHAs of each village and Medical Officer. A PHC was observed in five blocks of five districts
as a facility observation. A total of 50 FGDs conducted across the five selected villages.
Score Card Preparation
After gathering the information through the FGDs, interviews with family planning users, interviews
with ASHAs and MOIC, and facility observation, scores were given to each of the conducted inquiry,
and a community scorecard was processed. Data triangulation was done by identifying and clubbing
the responses from various tools under the themes/issues that were identified from the reference
guidelines, documents and manuals consulted for developing the tools. Under each theme, questions
and sub questions were developed and each question had an indicative response: “Yes” or “No”. In
case of a negative response, the score given was zero and in case of a positive response, the scoring
was one. Cumulative scoring was calculated for each of the themes and later percentage was
calculated and colour coding was developed in order to obtain final results in the form of a traffic
light. Reverse scoring was done in case of questions related to coercion. Thus, percentages were
calculated for each of the indicators, 100 percent being the most desirable condition. For the purpose
of translating the results into traffic lights, below 50 percent (poor) was put under red colour, results
from 50–80 percent (average) under yellow colour and results above 80 percent (good) were green
coloured. The issues considered for preparing these report cards are enumerated in Table 4 and 5.
Page | 6
Table 4: Issues for community report card
Theme Source of Information
Client identification 10 Focus Group Discussions, 50 user interviews
Counseling 10 Focus Group Discussions, 50 user interviews
Information and choice 10 Focus Group Discussions, 50 user interviews
Quality of services 10 Focus Group Discussions, 50 user interviews
Follow up and management 10 Focus Group Discussions, 50 user interviews
Coercion/incentives 10 Focus Group Discussions, 50 user interviews
Table 5: Issues for facility/provider report card
Theme Source of Information
Knowledge of methods MO Interview, Facility Checklist, ASHA Interviews
Counseling and IEC MO Interview, Facility Checklist, ASHA Interviews
Basket of options MO Interview, Facility Checklist, ASHA Interviews
Facility preparedness MO Interview, Facility Checklist, ASHA Interviews
Quality of clinical services MO Interview, Facility Checklist, ASHA Interviews
Follow up and management MO Interview, Facility Checklist, ASHA Interviews
Target/ Incentives MO Interview, Facility Checklist, ASHA Interviews
4. Major Findings
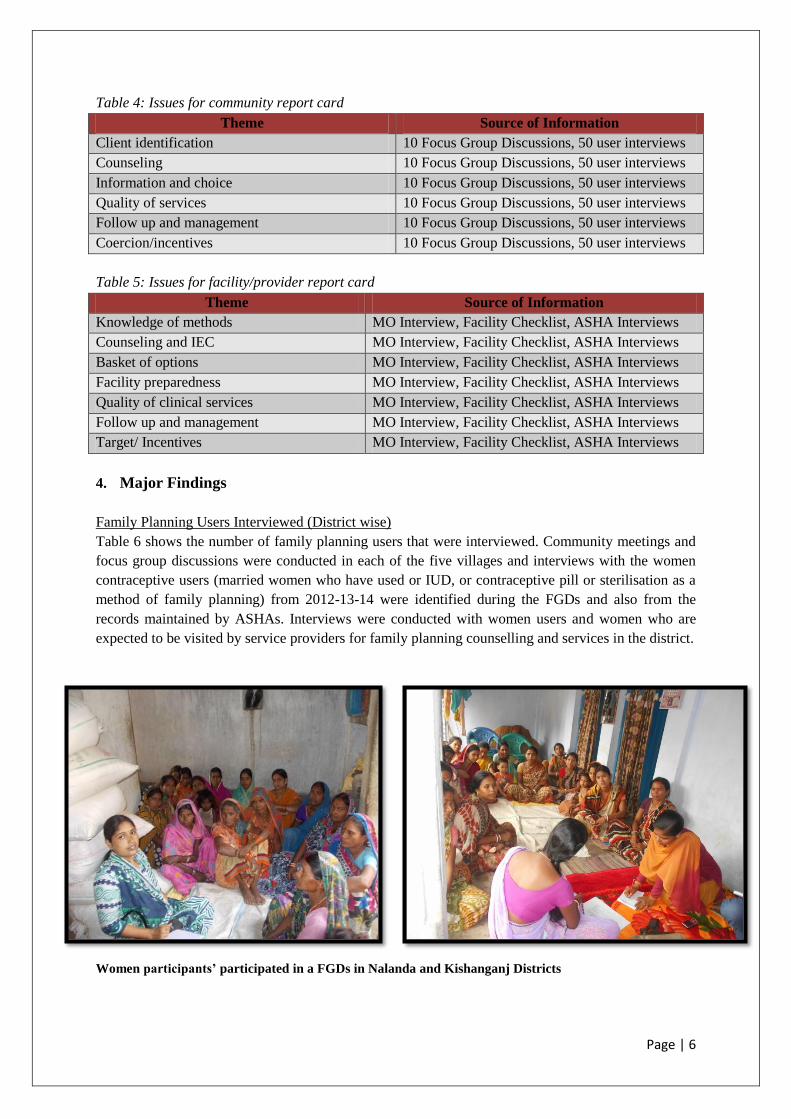
Family Planning Users Interviewed (District wise)
Table 6 shows the number of family planning users that were interviewed. Community meetings and
focus group discussions were conducted in each of the five villages and interviews with the women
contraceptive users (married women who have used or IUD, or contraceptive pill or sterilisation as a
method of family planning) from 2012-13-14 were identified during the FGDs and also from the
records maintained by ASHAs. Interviews were conducted with women users and women who are
expected to be visited by service providers for family planning counselling and services in the district.
Women participants’ participated in a FGDs in Nalanda and Kishanganj Districts
Page | 7
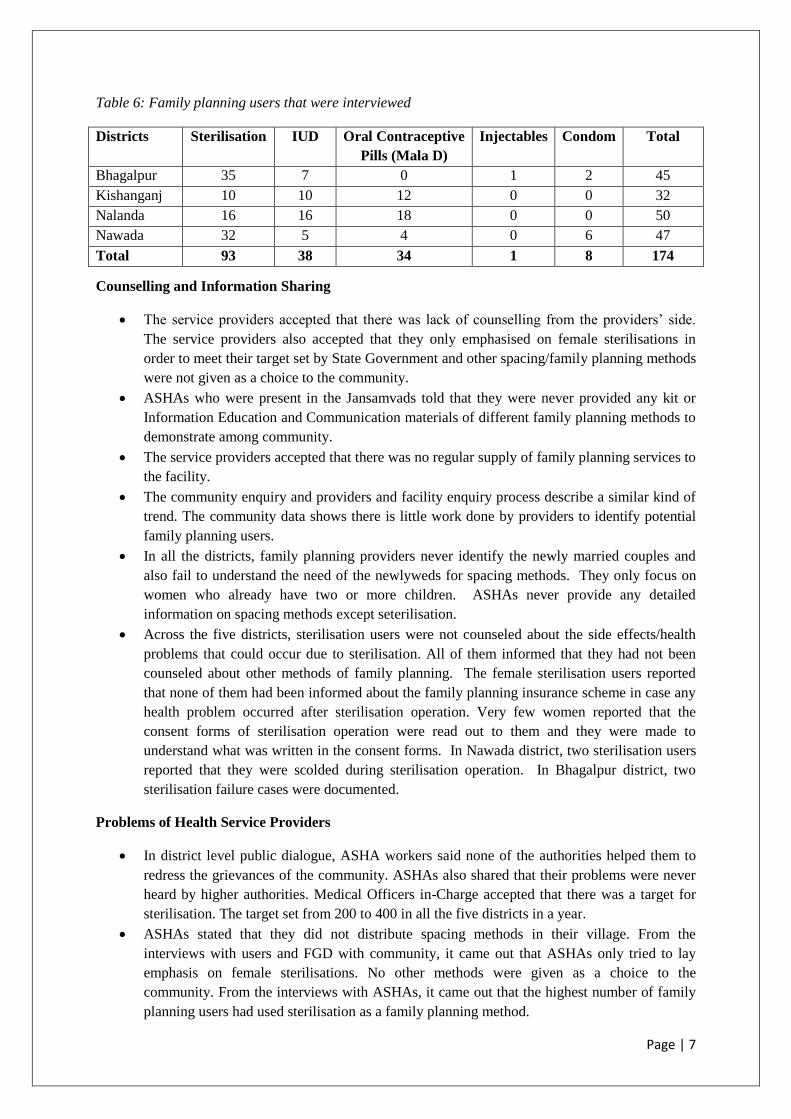
Table 6: Family planning users that were interviewed
Districts Sterilisation IUD Oral Contraceptive
Pills (Mala D)
Injectables Condom Total
Bhagalpur 35 7 0 1 2 45
Kishanganj 10 10 12 0 0 32
Nalanda 16 16 18 0 0 50
Nawada 32 5 4 0 6 47
Total 93 38 34 1 8 174
Counselling and Information Sharing
The service providers accepted that there was lack of counselling from the providers’ side.
The service providers also accepted that they only emphasised on female sterilisations in
order to meet their target set by State Government and other spacing/family planning methods
were not given as a choice to the community.
ASHAs who were present in the Jansamvads told that they were never provided any kit or
Information Education and Communication materials of different family planning methods to
demonstrate among community.
The service providers accepted that there was no regular supply of family planning services to
the facility.
The community enquiry and providers and facility enquiry process describe a similar kind of
trend. The community data shows there is little work done by providers to identify potential
family planning users.
In all the districts, family planning providers never identify the newly married couples and
also fail to understand the need of the newlyweds for spacing methods. They only focus on
women who already have two or more children. ASHAs never provide any detailed
information on spacing methods except seterilisation.
Across the five districts, sterilisation users were not counseled about the side effects/health
problems that could occur due to sterilisation. All of them informed that they had not been
counseled about other methods of family planning. The female sterilisation users reported
that none of them had been informed about the family planning insurance scheme in case any
health problem occurred after sterilisation operation. Very few women reported that the
consent forms of sterilisation operation were read out to them and they were made to
understand what was written in the consent forms. In Nawada district, two sterilisation users
reported that they were scolded during sterilisation operation. In Bhagalpur district, two
sterilisation failure cases were documented.
Problems of Health Service Providers
In district level public dialogue, ASHA workers said none of the authorities helped them to
redress the grievances of the community. ASHAs also shared that their problems were never
heard by higher authorities. Medical Officers in-Charge accepted that there was a target for
sterilisation. The target set from 200 to 400 in all the five districts in a year.
ASHAs stated that they did not distribute spacing methods in their village. From the
interviews with users and FGD with community, it came out that ASHAs only tried to lay
emphasis on female sterilisations. No other methods were given as a choice to the
community. From the interviews with ASHAs, it came out that the highest number of family
planning users had used sterilisation as a family planning method.

Page | 8
From the facility survey, it came out that the Primary Health Centres in five study districts
were not well equipped to provide family planning services and no family planning
counselors were available in the PHCs across the five districts of Bihar. There was no regular
supply of family planning services to the facility.
Health service providers accepted that the health system had been facing a dire lack of health
staff and they had to provide different types of services by engaging limited number of staff.
Follow-up Mechanism
The follow-up mechanism was also very poor in all the districts. The women said that ASHAs
did not pay visits after the selection of any family planning methods by women. ASHAs
hardly came if the family planning users felt any discomfort after using any of the methods.
Basically, family planning services are a matter of self choice and should be put into use
through proper motivation and counseling and not as a matter of compulsion as there is dearth
of staff. The providers lack proper skills of counseling and also lack in skills of carrying out
the pre conditional physical and pelvic examinations before insertion of IUD and sterilisation.
The health authorities admitted that there was a need for good Information Education and
Communication (IEC) services related to family planning. In district level Jansamvads,
service providers accepted that they should be trained on family planning counseling and how
to provide proper information to the users.
District Level Dialogues and Sharing
In district level public dialogues, ASHA workers said none of the authorities helped them to
redress the grievances of the community. ASHAs also shared that their problems were never
heard by higher authorities. Medical Officers in-Charge accepted that there was a target for
sterilisation. The target was to sterilise one percent (0.05%) in every 200 people.

Page | 9
Photographs of District Level Jansamvad in Nalanda and Kishanganj District
Page | 10
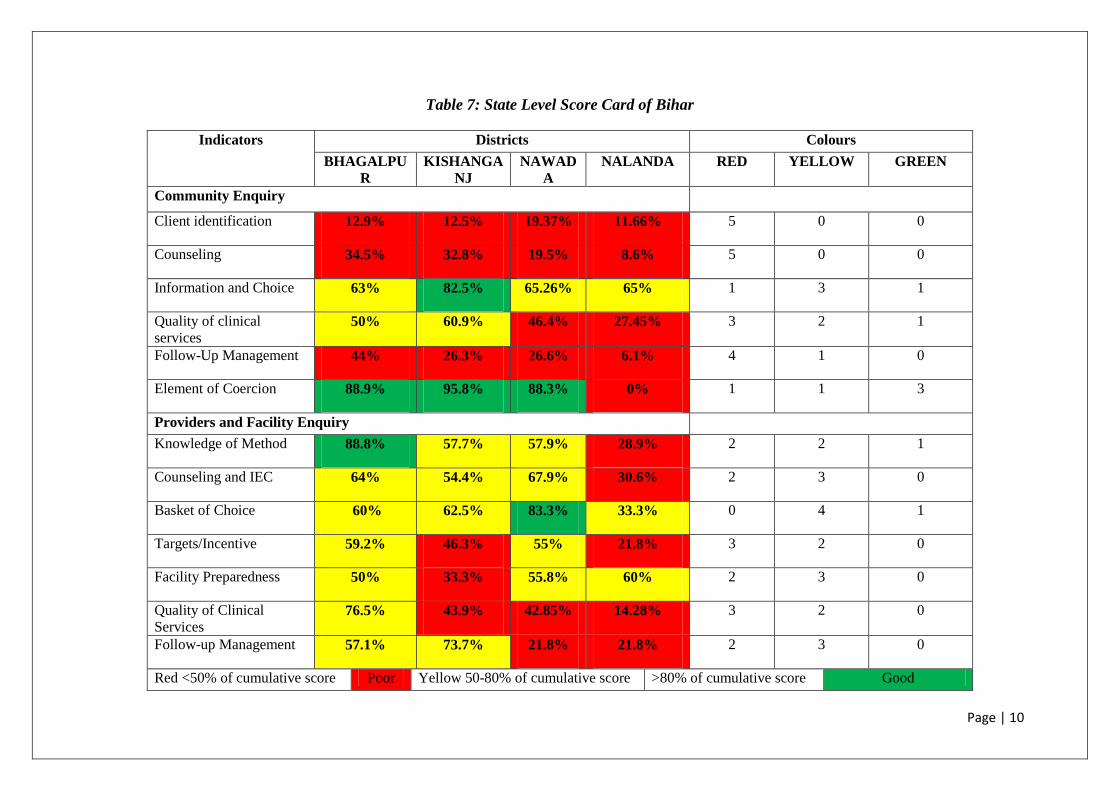
Table 7: State Level Score Card of Bihar
Indicators Districts Colours
BHAGALPU
R
KISHANGA
NJ
NAWAD
A
NALANDA RED YELLOW GREEN
Community Enquiry
Client identification 12.9% 12.5% 19.37% 11.66% 5 0 0
Counseling 34.5% 32.8% 19.5% 8.6% 5 0 0
Information and Choice 63% 82.5% 65.26% 65% 1 3 1
Quality of clinical
services 50% 60.9% 46.4% 27.45% 3 2 1
Follow-Up Management 44% 26.3% 26.6% 6.1% 4 1 0
Element of Coercion 88.9% 95.8% 88.3% 0% 1 1 3
Providers and Facility Enquiry
Knowledge of Method 88.8% 57.7% 57.9% 28.9% 2 2 1
Counseling and IEC 64% 54.4% 67.9% 30.6% 2 3 0
Basket of Choice 60% 62.5% 83.3% 33.3% 0 4 1
Targets/Incentive 59.2% 46.3% 55% 21.8% 3 2 0
Facility Preparedness 50% 33.3% 55.8% 60% 2 3 0
Quality of Clinical
Services 76.5% 43.9% 42.85% 14.28% 3 2 0
Follow-up Management 57.1% 73.7% 21.8% 21.8% 2 3 0
Red <50% of cumulative score Poor Yellow 50-80% of cumulative score >80% of cumulative score Good
Page | 11
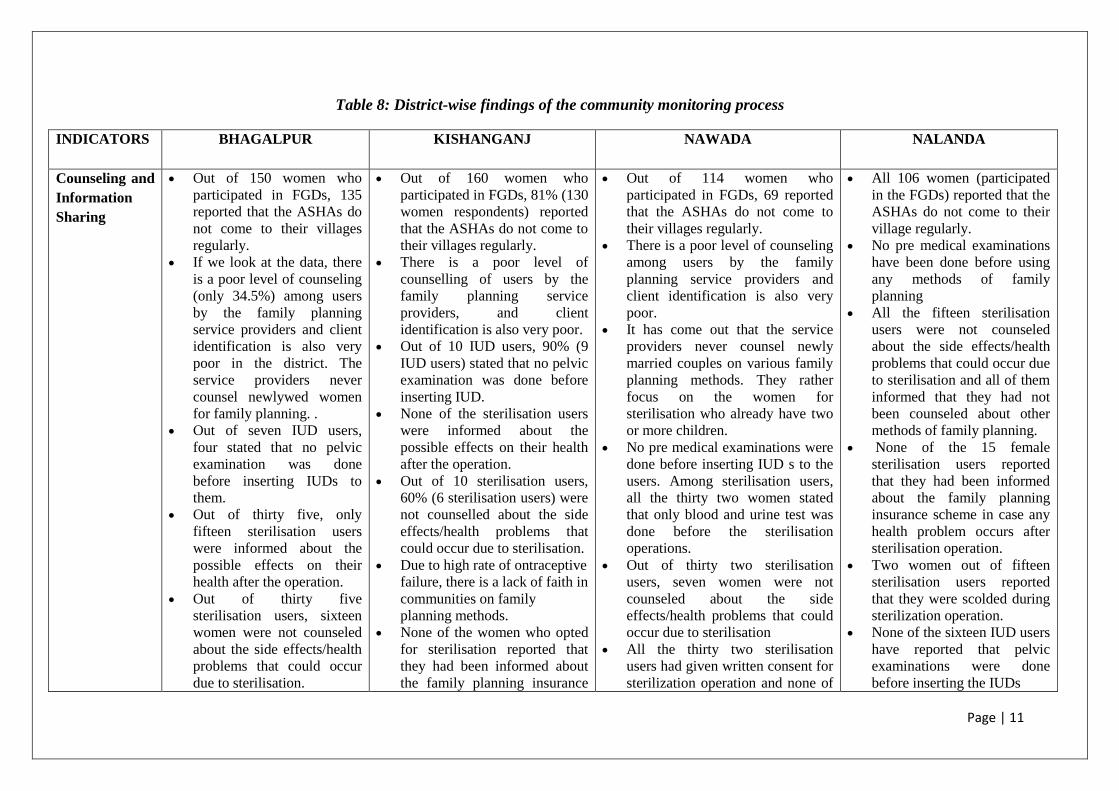
Table 8: District-wise findings of the community monitoring process
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
Counseling and
Information
Sharing
Out of 150 women who
participated in FGDs, 135
reported that the ASHAs do
not come to their villages
regularly.
If we look at the data, there
is a poor level of counseling
(only 34.5%) among users
by the family planning
service providers and client
identification is also very
poor in the district. The
service providers never
counsel newlywed women
for family planning. .
Out of seven IUD users,
four stated that no pelvic
examination was done
before inserting IUDs to
them.
Out of thirty five, only
fifteen sterilisation users
were informed about the
possible effects on their
health after the operation.
Out of thirty five
sterilisation users, sixteen
women were not counseled
about the side effects/health
problems that could occur
due to sterilisation.
Out of 160 women who
participated in FGDs, 81% (130
women respondents) reported
that the ASHAs do not come to
their villages regularly.
There is a poor level of
counselling of users by the
family planning service
providers, and client
identification is also very poor.
Out of 10 IUD users, 90% (9
IUD users) stated that no pelvic
examination was done before
inserting IUD.
None of the sterilisation users
were informed about the
possible effects on their health
after the operation.
Out of 10 sterilisation users,
60% (6 sterilisation users) were
not counselled about the side
effects/health problems that
could occur due to sterilisation.
Due to high rate of ontraceptive
failure, there is a lack of faith in
communities on family
planning methods.
None of the women who opted
for sterilisation reported that
they had been informed about
the family planning insurance
Out of 114 women who
participated in FGDs, 69 reported
that the ASHAs do not come to
their villages regularly.
There is a poor level of counseling
among users by the family
planning service providers and
client identification is also very
poor.
It has come out that the service
providers never counsel newly
married couples on various family
planning methods. They rather
focus on the women for
sterilisation who already have two
or more children.
No pre medical examinations were
done before inserting IUD s to the
users. Among sterilisation users,
all the thirty two women stated
that only blood and urine test was
done before the sterilisation
operations.
Out of thirty two sterilisation
users, seven women were not
counseled about the side
effects/health problems that could
occur due to sterilisation
All the thirty two sterilisation
users had given written consent for
sterilization operation and none of
All 106 women (participated
in the FGDs) reported that the
ASHAs do not come to their
village regularly.
No pre medical examinations
have been done before using
any methods of family
planning
All the fifteen sterilisation
users were not counseled
about the side effects/health
problems that could occur due
to sterilisation and all of them
informed that they had not
been counseled about other
methods of family planning.
None of the 15 female
sterilisation users reported
that they had been informed
about the family planning
insurance scheme in case any
health problem occurs after
sterilisation operation.
Two women out of fifteen
sterilisation users reported
that they were scolded during
sterilization operation.
None of the sixteen IUD users
have reported that pelvic
examinations were done
before inserting the IUDs
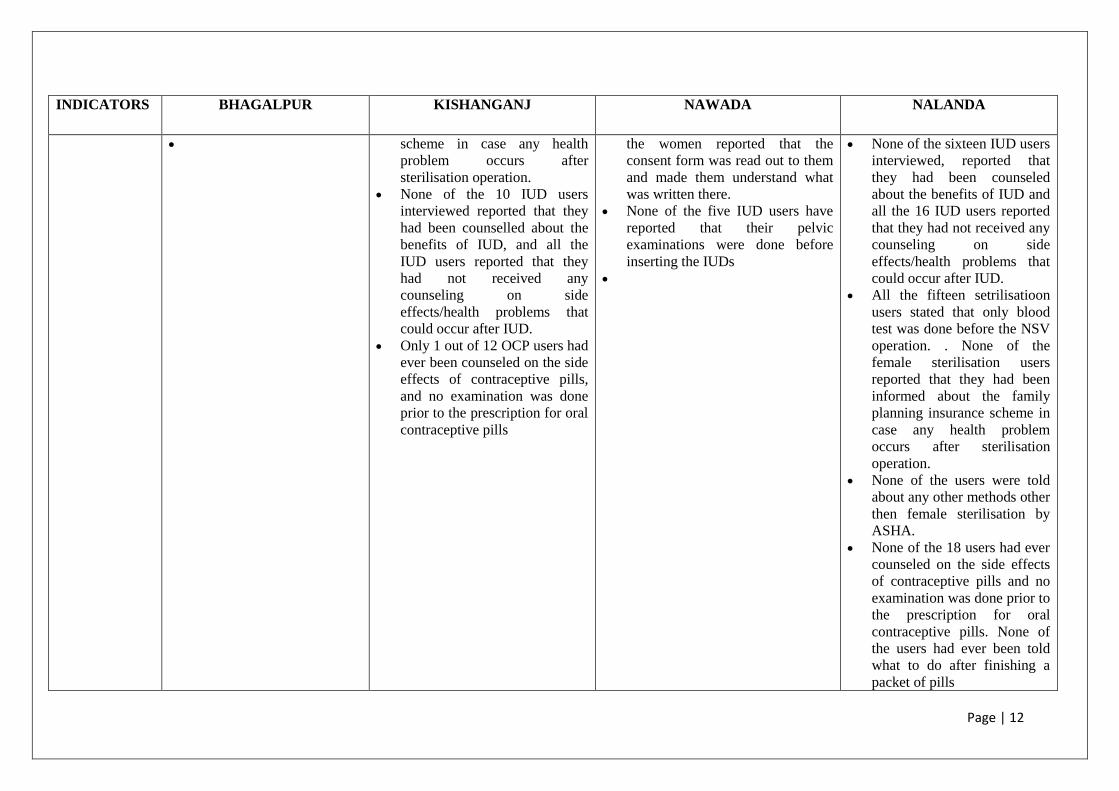
Page | 12
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
scheme in case any health
problem occurs after
sterilisation operation.
None of the 10 IUD users
interviewed reported that they
had been counselled about the
benefits of IUD, and all the
IUD users reported that they
had not received any
counseling on side
effects/health problems that
could occur after IUD.
Only 1 out of 12 OCP users had
ever been counseled on the side
effects of contraceptive pills,
and no examination was done
prior to the prescription for oral
contraceptive pills
the women reported that the
consent form was read out to them
and made them understand what
was written there.
None of the five IUD users have
reported that their pelvic
examinations were done before
inserting the IUDs
None of the sixteen IUD users
interviewed, reported that
they had been counseled
about the benefits of IUD and
all the 16 IUD users reported
that they had not received any
counseling on side
effects/health problems that
could occur after IUD.
All the fifteen setrilisatioon
users stated that only blood
test was done before the NSV
operation. . None of the
female sterilisation users
reported that they had been
informed about the family
planning insurance scheme in
case any health problem
occurs after sterilisation
operation.
None of the users were told
about any other methods other
then female sterilisation by
ASHA.
None of the 18 users had ever
counseled on the side effects
of contraceptive pills and no
examination was done prior to
the prescription for oral
contraceptive pills. None of
the users had ever been told
what to do after finishing a
packet of pills
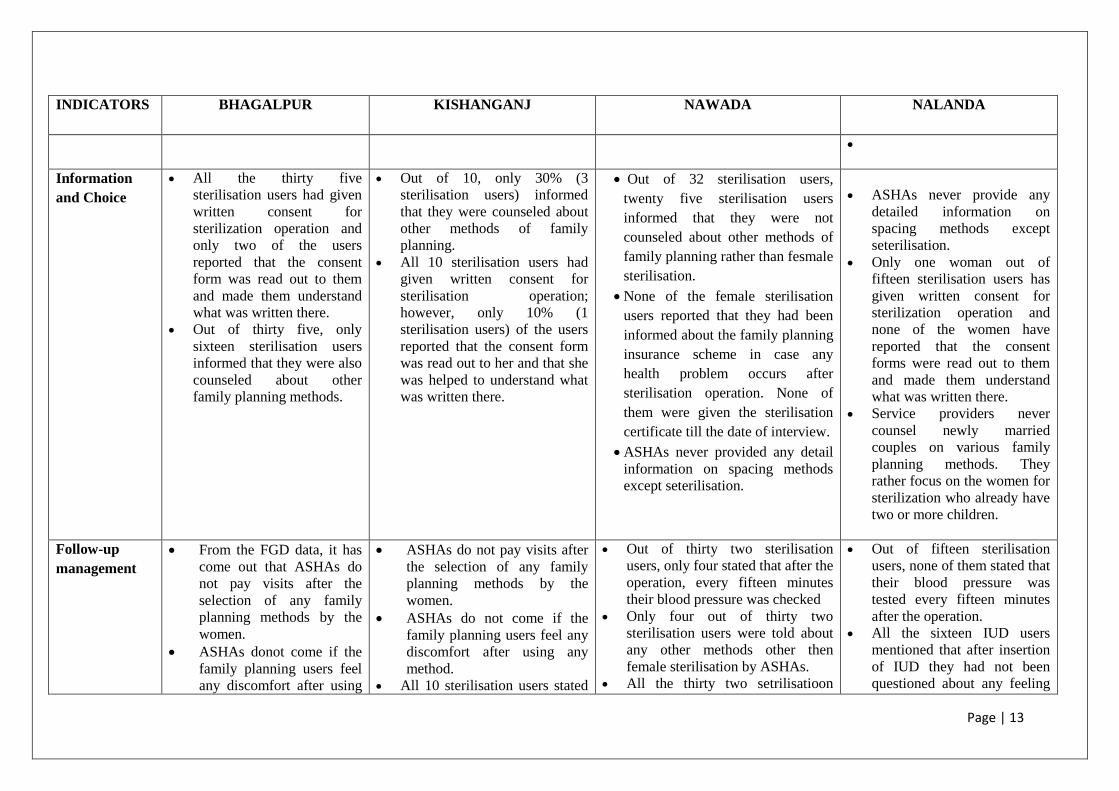
Page | 13
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
Information
and Choice
All the thirty five
sterilisation users had given
written consent for
sterilization operation and
only two of the users
reported that the consent
form was read out to them
and made them understand
what was written there.
Out of thirty five, only
sixteen sterilisation users
informed that they were also
counseled about other
family planning methods.
Out of 10, only 30% (3
sterilisation users) informed
that they were counseled about
other methods of family
planning.
All 10 sterilisation users had
given written consent for
sterilisation operation;
however, only 10% (1
sterilisation users) of the users
reported that the consent form
was read out to her and that she
was helped to understand what
was written there.
Out of 32 sterilisation users,
twenty five sterilisation users
informed that they were not
counseled about other methods of
family planning rather than fesmale
sterilisation.
None of the female sterilisation
users reported that they had been
informed about the family planning
insurance scheme in case any
health problem occurs after
sterilisation operation. None of
them were given the sterilisation
certificate till the date of interview.
ASHAs never provided any detail
information on spacing methods
except seterilisation.
ASHAs never provide any
detailed information on
spacing methods except
seterilisation.
Only one woman out of
fifteen sterilisation users has
given written consent for
sterilization operation and
none of the women have
reported that the consent
forms were read out to them
and made them understand
what was written there.
Service providers never
counsel newly married
couples on various family
planning methods. They
rather focus on the women for
sterilization who already have
two or more children.
Follow-up
management
From the FGD data, it has
come out that ASHAs do
not pay visits after the
selection of any family
planning methods by the
women.
ASHAs donot come if the
family planning users feel
any discomfort after using
ASHAs do not pay visits after
the selection of any family
planning methods by the
women.
ASHAs do not come if the
family planning users feel any
discomfort after using any
method.
All 10 sterilisation users stated
Out of thirty two sterilisation
users, only four stated that after the
operation, every fifteen minutes
their blood pressure was checked
Only four out of thirty two
sterilisation users were told about
any other methods other then
female sterilisation by ASHAs.
All the thirty two setrilisatioon
Out of fifteen sterilisation
users, none of them stated that
their blood pressure was
tested every fifteen minutes
after the operation.
All the sixteen IUD users
mentioned that after insertion
of IUD they had not been
questioned about any feeling
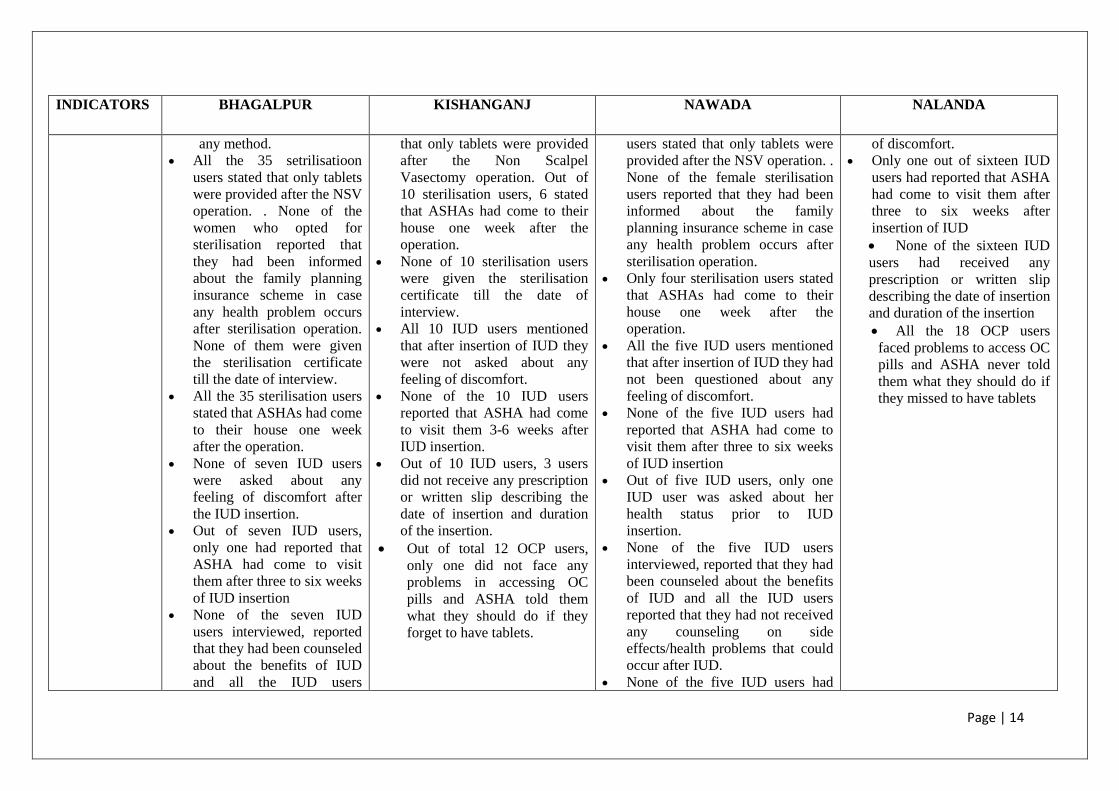
Page | 14
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
any method.
All the 35 setrilisatioon
users stated that only tablets
were provided after the NSV
operation. . None of the
women who opted for
sterilisation reported that
they had been informed
about the family planning
insurance scheme in case
any health problem occurs
after sterilisation operation.
None of them were given
the sterilisation certificate
till the date of interview.
All the 35 sterilisation users
stated that ASHAs had come
to their house one week
after the operation.
None of seven IUD users
were asked about any
feeling of discomfort after
the IUD insertion.
Out of seven IUD users,
only one had reported that
ASHA had come to visit
them after three to six weeks
of IUD insertion
None of the seven IUD
users interviewed, reported
that they had been counseled
about the benefits of IUD
and all the IUD users
that only tablets were provided
after the Non Scalpel
Vasectomy operation. Out of
10 sterilisation users, 6 stated
that ASHAs had come to their
house one week after the
operation.
None of 10 sterilisation users
were given the sterilisation
certificate till the date of
interview.
All 10 IUD users mentioned
that after insertion of IUD they
were not asked about any
feeling of discomfort.
None of the 10 IUD users
reported that ASHA had come
to visit them 3-6 weeks after
IUD insertion.
Out of 10 IUD users, 3 users
did not receive any prescription
or written slip describing the
date of insertion and duration
of the insertion.
Out of total 12 OCP users,
only one did not face any
problems in accessing OC
pills and ASHA told them
what they should do if they
forget to have tablets.
users stated that only tablets were
provided after the NSV operation. .
None of the female sterilisation
users reported that they had been
informed about the family
planning insurance scheme in case
any health problem occurs after
sterilisation operation.
Only four sterilisation users stated
that ASHAs had come to their
house one week after the
operation.
All the five IUD users mentioned
that after insertion of IUD they had
not been questioned about any
feeling of discomfort.
None of the five IUD users had
reported that ASHA had come to
visit them after three to six weeks
of IUD insertion
Out of five IUD users, only one
IUD user was asked about her
health status prior to IUD
insertion.
None of the five IUD users
interviewed, reported that they had
been counseled about the benefits
of IUD and all the IUD users
reported that they had not received
any counseling on side
effects/health problems that could
occur after IUD.
None of the five IUD users had
of discomfort.
Only one out of sixteen IUD
users had reported that ASHA
had come to visit them after
three to six weeks after
insertion of IUD
None of the sixteen IUD
users had received any
prescription or written slip
describing the date of insertion
and duration of the insertion
All the 18 OCP users
faced problems to access OC
pills and ASHA never told
them what they should do if
they missed to have tablets
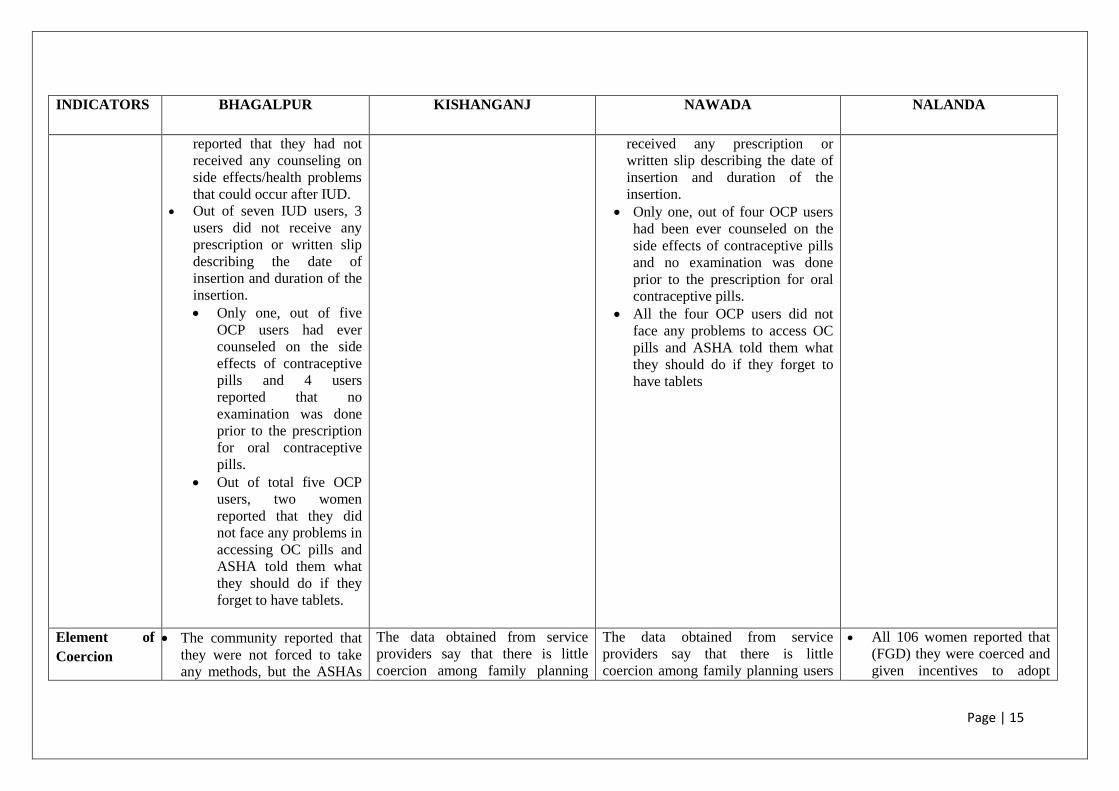
Page | 15
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
reported that they had not
received any counseling on
side effects/health problems
that could occur after IUD.
Out of seven IUD users, 3
users did not receive any
prescription or written slip
describing the date of
insertion and duration of the
insertion.
Only one, out of five
OCP users had ever
counseled on the side
effects of contraceptive
pills and 4 users
reported that no
examination was done
prior to the prescription
for oral contraceptive
pills.
Out of total five OCP
users, two women
reported that they did
not face any problems in
accessing OC pills and
ASHA told them what
they should do if they
forget to have tablets.
received any prescription or
written slip describing the date of
insertion and duration of the
insertion.
Only one, out of four OCP users
had been ever counseled on the
side effects of contraceptive pills
and no examination was done
prior to the prescription for oral
contraceptive pills.
All the four OCP users did not
face any problems to access OC
pills and ASHA told them what
they should do if they forget to
have tablets
Element of
Coercion
The community reported that
they were not forced to take
any methods, but the ASHAs
The data obtained from service
providers say that there is little
coercion among family planning
The data obtained from service
providers say that there is little
coercion among family planning users
All 106 women reported that
(FGD) they were coerced and
given incentives to adopt
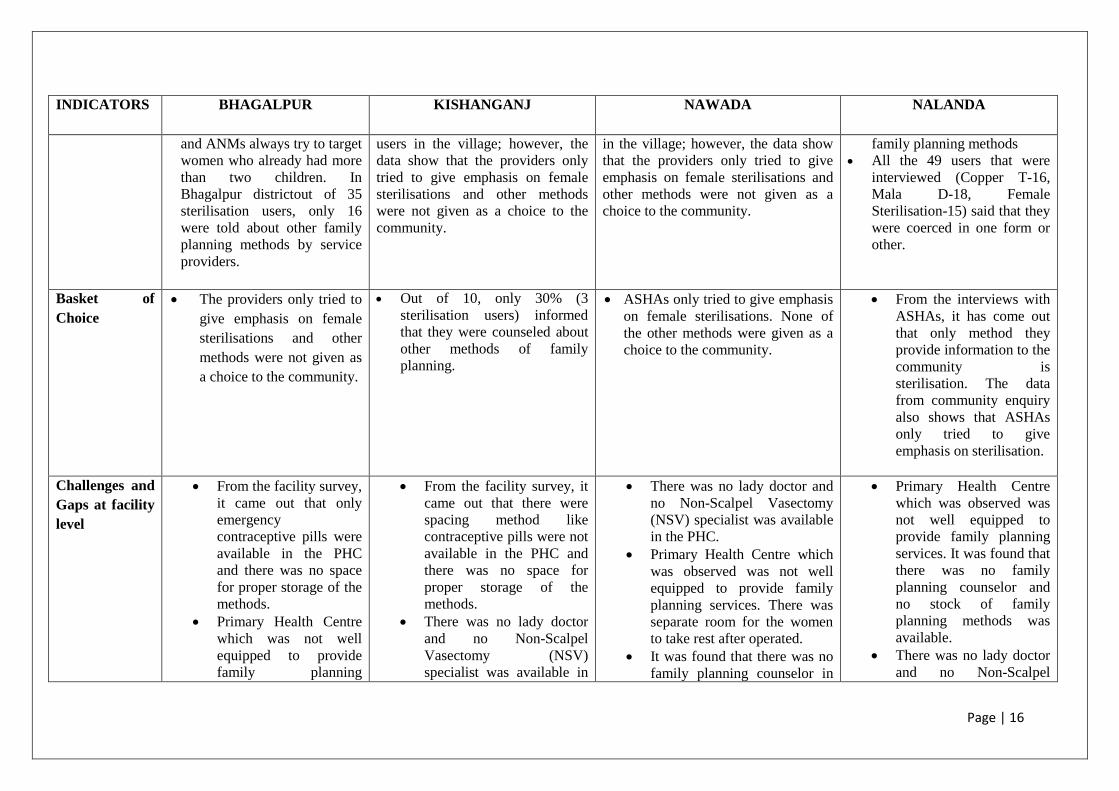
Page | 16
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
and ANMs always try to target
women who already had more
than two children. In
Bhagalpur districtout of 35
sterilisation users, only 16
were told about other family
planning methods by service
providers.
users in the village; however, the
data show that the providers only
tried to give emphasis on female
sterilisations and other methods
were not given as a choice to the
community.
in the village; however, the data show
that the providers only tried to give
emphasis on female sterilisations and
other methods were not given as a
choice to the community.
family planning methods
All the 49 users that were
interviewed (Copper T-16,
Mala D-18, Female
Sterilisation-15) said that they
were coerced in one form or
other.
Basket of
Choice
The providers only tried to
give emphasis on female
sterilisations and other
methods were not given as
a choice to the community.
Out of 10, only 30% (3
sterilisation users) informed
that they were counseled about
other methods of family
planning.
ASHAs only tried to give emphasis
on female sterilisations. None of
the other methods were given as a
choice to the community.
From the interviews with
ASHAs, it has come out
that only method they
provide information to the
community is
sterilisation. The data
from community enquiry
also shows that ASHAs
only tried to give
emphasis on sterilisation.
Challenges and
Gaps at facility
level
From the facility survey,
it came out that only
emergency
contraceptive pills were
available in the PHC
and there was no space
for proper storage of the
methods.
Primary Health Centre
which was not well
equipped to provide
family planning
From the facility survey, it
came out that there were
spacing method like
contraceptive pills were not
available in the PHC and
there was no space for
proper storage of the
methods.
There was no lady doctor
and no Non-Scalpel
Vasectomy (NSV)
specialist was available in
There was no lady doctor and
no Non-Scalpel Vasectomy
(NSV) specialist was available
in the PHC.
Primary Health Centre which
was observed was not well
equipped to provide family
planning services. There was
separate room for the women
to take rest after operated.
It was found that there was no
family planning counselor in
Primary Health Centre
which was observed was
not well equipped to
provide family planning
services. It was found that
there was no family
planning counselor and
no stock of family
planning methods was
available.
There was no lady doctor
and no Non-Scalpel
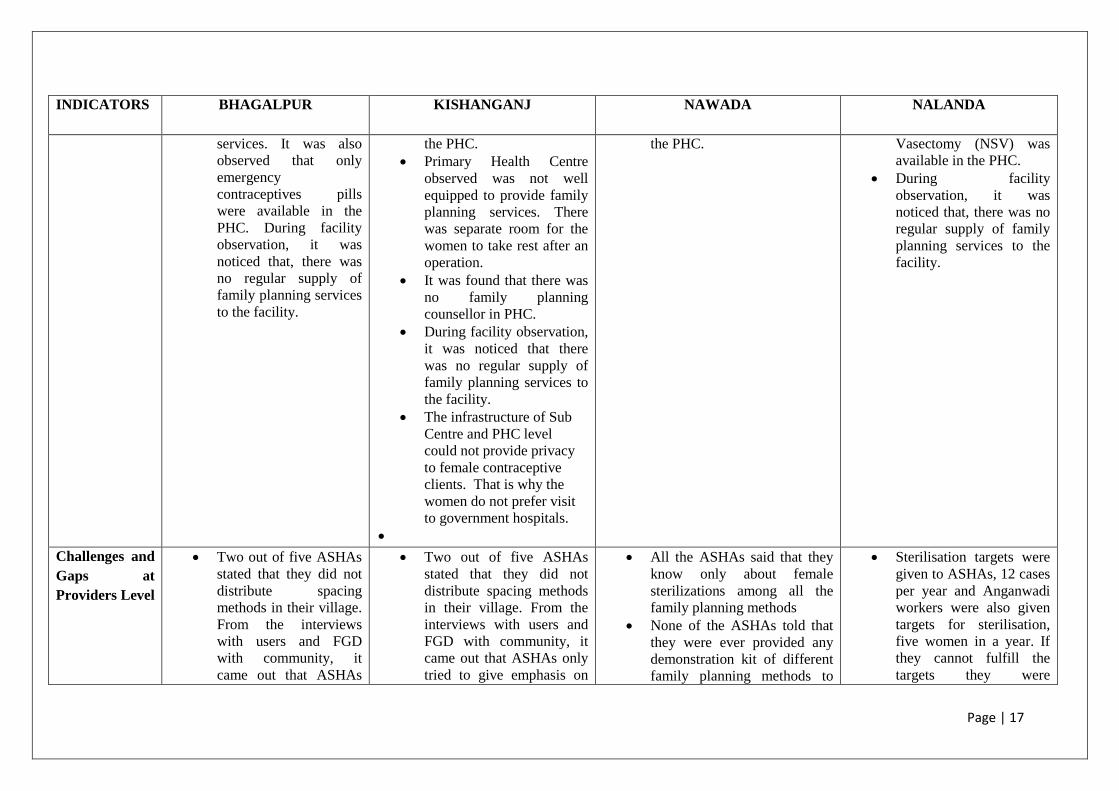
Page | 17
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
services. It was also
observed that only
emergency
contraceptives pills
were available in the
PHC. During facility
observation, it was
noticed that, there was
no regular supply of
family planning services
to the facility.
the PHC.
Primary Health Centre
observed was not well
equipped to provide family
planning services. There
was separate room for the
women to take rest after an
operation.
It was found that there was
no family planning
counsellor in PHC.
During facility observation,
it was noticed that there
was no regular supply of
family planning services to
the facility.
The infrastructure of Sub
Centre and PHC level
could not provide privacy
to female contraceptive
clients. That is why the
women do not prefer visit
to government hospitals.
the PHC.
Vasectomy (NSV) was
available in the PHC.
During facility
observation, it was
noticed that, there was no
regular supply of family
planning services to the
facility.
Challenges and
Gaps at
Providers Level
Two out of five ASHAs
stated that they did not
distribute spacing
methods in their village.
From the interviews
with users and FGD
with community, it
came out that ASHAs
Two out of five ASHAs
stated that they did not
distribute spacing methods
in their village. From the
interviews with users and
FGD with community, it
came out that ASHAs only
tried to give emphasis on
All the ASHAs said that they
know only about female
sterilizations among all the
family planning methods
None of the ASHAs told that
they were ever provided any
demonstration kit of different
family planning methods to
Sterilisation targets were
given to ASHAs, 12 cases
per year and Anganwadi
workers were also given
targets for sterilisation,
five women in a year. If
they cannot fulfill the
targets they were
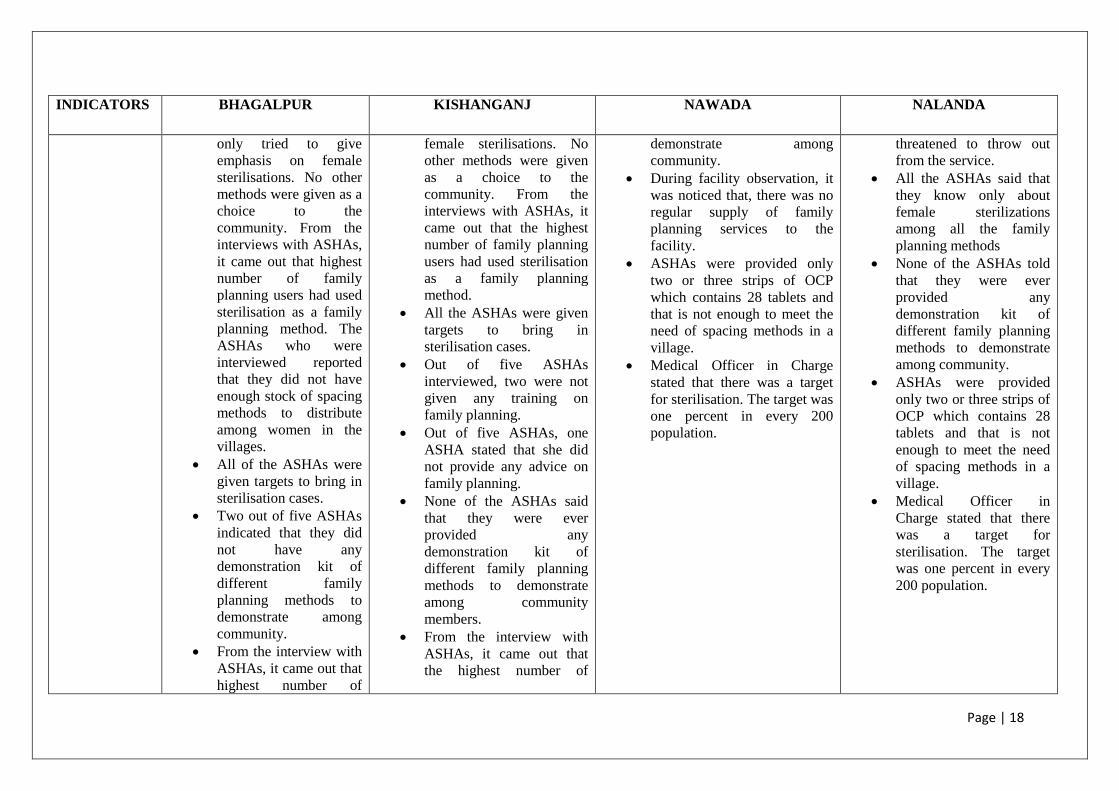
Page | 18
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
only tried to give
emphasis on female
sterilisations. No other
methods were given as a
choice to the
community. From the
interviews with ASHAs,
it came out that highest
number of family
planning users had used
sterilisation as a family
planning method. The
ASHAs who were
interviewed reported
that they did not have
enough stock of spacing
methods to distribute
among women in the
villages.
All of the ASHAs were
given targets to bring in
sterilisation cases.
Two out of five ASHAs
indicated that they did
not have any
demonstration kit of
different family
planning methods to
demonstrate among
community.
From the interview with
ASHAs, it came out that
highest number of
female sterilisations. No
other methods were given
as a choice to the
community. From the
interviews with ASHAs, it
came out that the highest
number of family planning
users had used sterilisation
as a family planning
method.
All the ASHAs were given
targets to bring in
sterilisation cases.
Out of five ASHAs
interviewed, two were not
given any training on
family planning.
Out of five ASHAs, one
ASHA stated that she did
not provide any advice on
family planning.
None of the ASHAs said
that they were ever
provided any
demonstration kit of
different family planning
methods to demonstrate
among community
members.
From the interview with
ASHAs, it came out that
the highest number of
demonstrate among
community.
During facility observation, it
was noticed that, there was no
regular supply of family
planning services to the
facility.
ASHAs were provided only
two or three strips of OCP
which contains 28 tablets and
that is not enough to meet the
need of spacing methods in a
village.
Medical Officer in Charge
stated that there was a target
for sterilisation. The target was
one percent in every 200
population.
threatened to throw out
from the service.
All the ASHAs said that
they know only about
female sterilizations
among all the family
planning methods
None of the ASHAs told
that they were ever
provided any
demonstration kit of
different family planning
methods to demonstrate
among community.
ASHAs were provided
only two or three strips of
OCP which contains 28
tablets and that is not
enough to meet the need
of spacing methods in a
village.
Medical Officer in
Charge stated that there
was a target for
sterilisation. The target
was one percent in every
200 population.
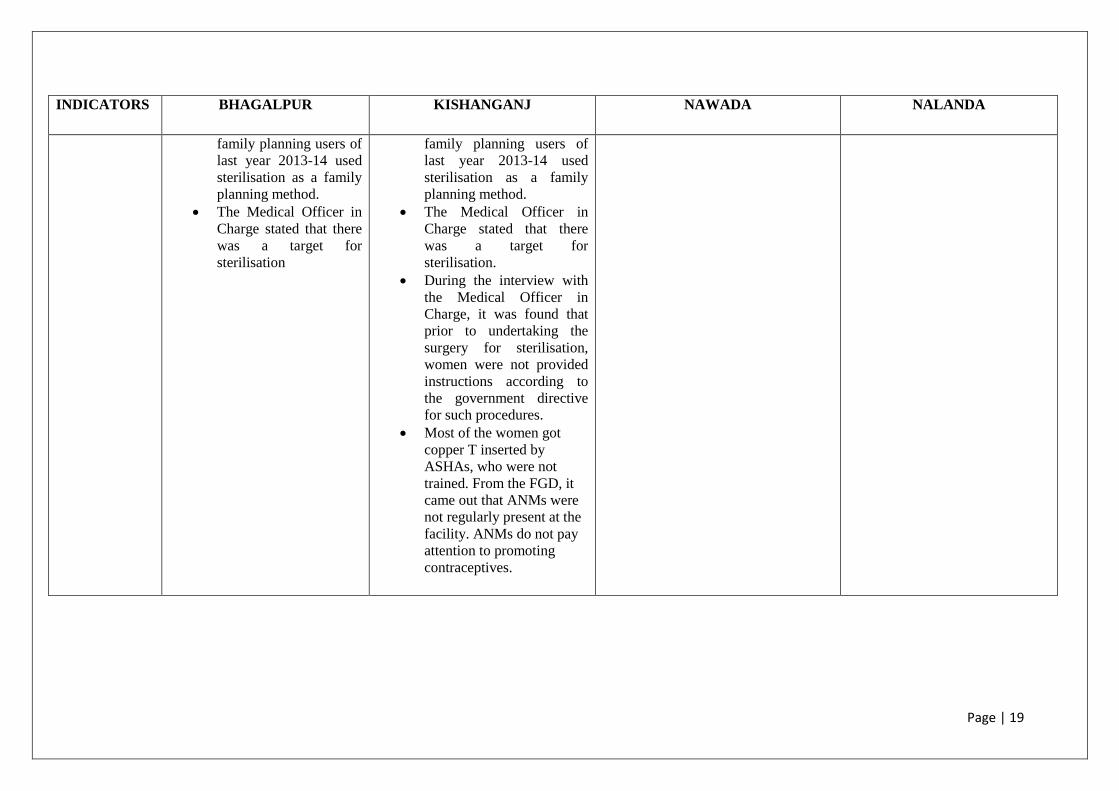
Page | 19
INDICATORS
BHAGALPUR KISHANGANJ NAWADA NALANDA
family planning users of
last year 2013-14 used
sterilisation as a family
planning method.
The Medical Officer in
Charge stated that there
was a target for
sterilisation
family planning users of
last year 2013-14 used
sterilisation as a family
planning method.
The Medical Officer in
Charge stated that there
was a target for
sterilisation.
During the interview with
the Medical Officer in
Charge, it was found that
prior to undertaking the
surgery for sterilisation,
women were not provided
instructions according to
the government directive
for such procedures.
Most of the women got
copper T inserted by
ASHAs, who were not
trained. From the FGD, it
came out that ANMs were
not regularly present at the
facility. ANMs do not pay
attention to promoting
contraceptives.
Conclusions
The score card is reinforcing community enquiry and service provider’s enquiry findings. The
findings from provider and facility observations clearly show that there is a strong gap in service
delivery of family planning. During district level public dialogues, the service providers accepted that
there was lack of counselling from the providers’ side. The service providers also accepted that they
only emphasised female sterilisations in order to meet the targets set by the State Government and that
other spacing/family planning methods were not given as a choice to the community.
The community enquiry and providers and facility enquiry process describe a similar kind of trend.
The community data also shows there is little work done by providers to identify potential family
planning users. In all the districts, family planning providers never identify the newly married couples
and also fail to understand the need of the newlyweds for spacing methods. They only focus on
women who already have two or more children. ASHAs never provide any detailed information on
spacing methods except seterilisation.
Proper counselling with informed choice and strong follow-up mechanism should be an integral part
of family planning services. Though these criteria are mentioned in family planning guidelines but
there is no evidence that these are followed in field level implementation.

Page | 21
Annexure: Media Coverage of District Level Jansamvad

Page | 22