Embed Size (px)
Citation preview
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 1/18
State of Indiana Refugee Health Program
Annual Report: Federal Fiscal Year 2015
December 2015
THAM HIN REFUGEE CAMP: http://interpares.ca/news/aid-refugees-refugees
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 2/18
Table of Contents
I. Executive Summary……………………………………………………………………….1
II.
Data and Statistics…………………………………………………………………….…...2
a. Demographic Data …………………………………………………………....…..2
b. Health Screening…………………………………………………………………..6
III. Successes & Challenges…….…………………………………………………….……...12
IV. The Year Ahead…………….……………………………………………….…………...13
V. Glossary…………………………………………………………………………….……14
VI. References………………………………………………………………………………..15
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 3/18
1
I.
Executive Summary
The United Nations High Commissioner for Refugees (UNHCR) defines a refugee as a
“ person who, owing to well-founded fear of being persecuted for reasons of race, religion,
nationality, membership of a particular social group or political opinion, is outside the country of
his nationality and is unable or, owing to such fear, is unwilling to avail himself of the protection
of that country, or who, not having a nationality and being outside the country of his former
habitual residence as a result of such events is unable or, owing to such fear, is unwilling to
return to it.” Each year, these refugees fleeing persecution and war in their home country are
resettled throughout the United States, including within Indiana. In Indiana, the overwhelming
majority of refugees are from Myanmar (Burma), with other refugees arriving from the
Democratic Republic of Congo, Somalia, Iraq and elsewhere.
Before being granted the status of refugee, individuals receive comprehensive background checks while in UNHCR custody, which may occur while the individual or family is
living in a refugee camp or within a temporary country of refuge. Once they are granted the
status of refugee, they are resettled in the U.S. as legal aliens by non-profit voluntary agencies
that receive their funding from the federal government and private donors. In addition to the
criminal background checks and overall screening process, all refugees receive multiple health
screenings. Guidelines for these health screenings are established by the Office of Refugee
Resettlement (ORR) and include screening for infectious diseases, chronic diseases and mental
health. Refugees first receive a health screening before they travel to the U.S. from a registered
panel physician in their temporary country of refuge. In addition, they receive a domestic health
screening in the U.S. within 30 to 90 days of arrival.
The Refugee Health Program at the Indiana State Department of Health (ISDH) is
responsible for providing oversight and coordination of health services to refugees in Indiana.
The mission of the Refugee Health Program is to support the resettlement of refugees by
providing access and resources for an initial health screening upon arrival to the United States,
by identifying emerging health issues in refugee populations and to provide ongoing support
through relationships with community, state and federal partners.
The ISDH Refugee Health Program has made significant progress, including reaching the
milestone of 100 percent of refugees receiving screening within 30 days of arrival during the lastquarter of 2015 and the expansion of screening services to include newborn, tobacco and mental
health screening. However, new challenges such as diabetes, cancer and high blood pressure are
looming on the horizon for the next refugee generations.

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 4/18
2
II. Data and Statistics
The following data is compiled from the Immigrant, TB, and All Refugee Application
(ITARA), the online database used by the ISDH Refugee Health Program. ITARA is a
centralized data collection system used by both ISDH and local refugee screening programs to
collect information on all arrivals to Indiana, including demographic and health screening data.
Unless otherwise indicated, the term “refugee” hereby refers to all arrivals served by the ISDH
Refugee Health Program, which includes primary refugees, secondary refugees, asylees, victim
of human trafficking, parolees and special immigrant visa holders. All data shown is for the
federal fiscal year 2015 (FFY 2015), which includes all refugees who arrived between October 1,
2014 and September 30, 2015.
a. Demographic Data
There were 1,885 refugee arrivals to the State of Indiana in FFY 2015, a 16.9 percent
increase over FFY 2014. According to the U.S. State Department, Indiana is projected to receive1,685 primary refugee arrivals during FFY 2016.
Figure 1.
There has been anoverall 63.1 %
increase in refugee
arrivals to Indiana
in the last four
years.
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 5/18
3
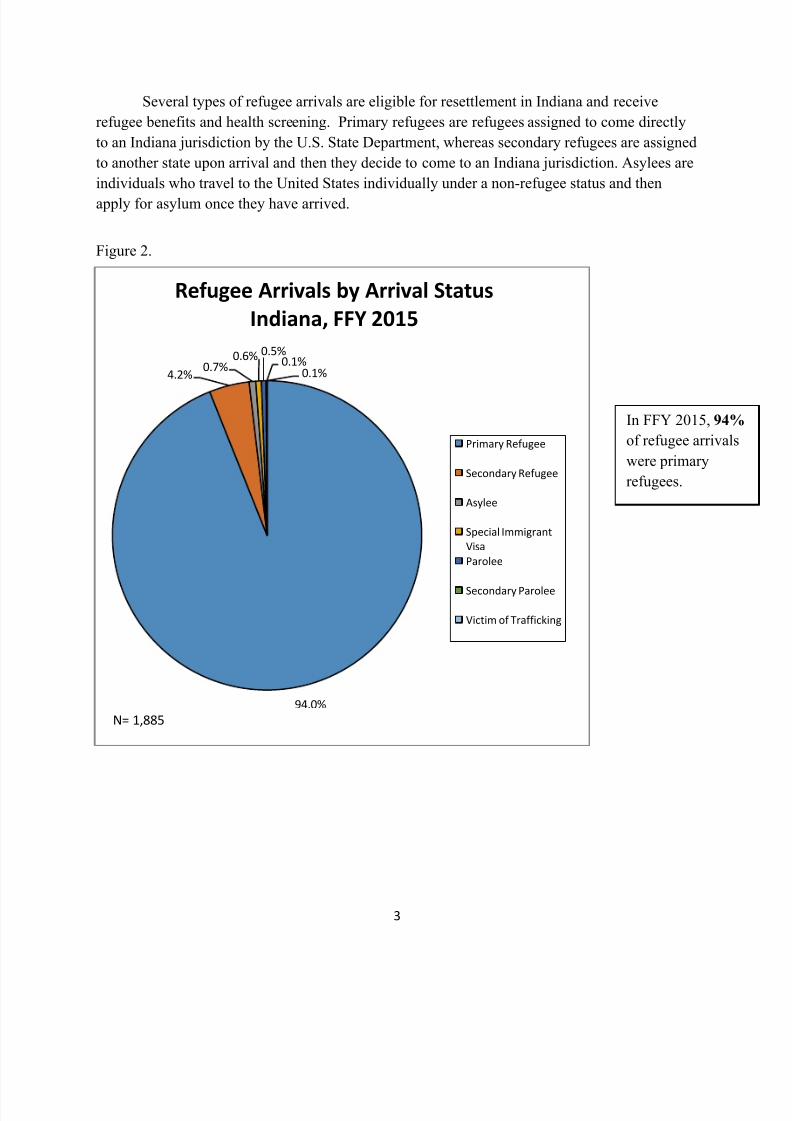
Several types of refugee arrivals are eligible for resettlement in Indiana and receive
refugee benefits and health screening. Primary refugees are refugees assigned to come directly
to an Indiana jurisdiction by the U.S. State Department, whereas secondary refugees are assigned
to another state upon arrival and then they decide to come to an Indiana jurisdiction. Asylees are
individuals who travel to the United States individually under a non-refugee status and then
apply for asylum once they have arrived.
Figure 2.
94.0%
4.2%0.7%
0.6% 0.5%
0.1%0.1%
Refugee Arrivals by Arrival Status
Indiana, FFY 2015
Primary Refugee
Secondary Refugee
Asylee
Special Immigrant
Visa
Parolee
Secondary Parolee
Victim of Trafficking
N= 1,885
In FFY 2015, 94%
of refugee arrivals
were primary
refugees.

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 6/18
4
In FFY 2015, refugees from 28 nations arrived in Indiana. The top country of origin was
Burma/Myanmar, comprising more than 80 percent of all arrivals. Table 1 shows FFY 2015
arrivals by CDC regions.
Table 1.
Primary refugees are resettled in either Allen County or Marion County, with Marion
County taking the majority of arrivals. Other refugees, such as asylees and secondary refugees,
can settle in any county within Indiana but receive their health screening in either Allen County
or Marion County.
Figure 3.
SOUTHEAST ASIA 1547
CENTRAL AFRICA 182
MIDDLE EAST 71
EAST AFRICA 44
INDIAN SUBCONTINENT 15
CARIBBEAN 11
NORTH AFRICA 5
MEXICO and CENTRAL AMERICA 4
EAST ASIA 2
EASTERN EUROPE and N.I.S. 2
Unknown 2
Total 1885
Refugee Arrivals by Country Of Origin
Region, Indiana, FFY 2015
80.4% of FFY 2015
arrivals in Indiana
resettled in Marion
County.
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 7/18
5
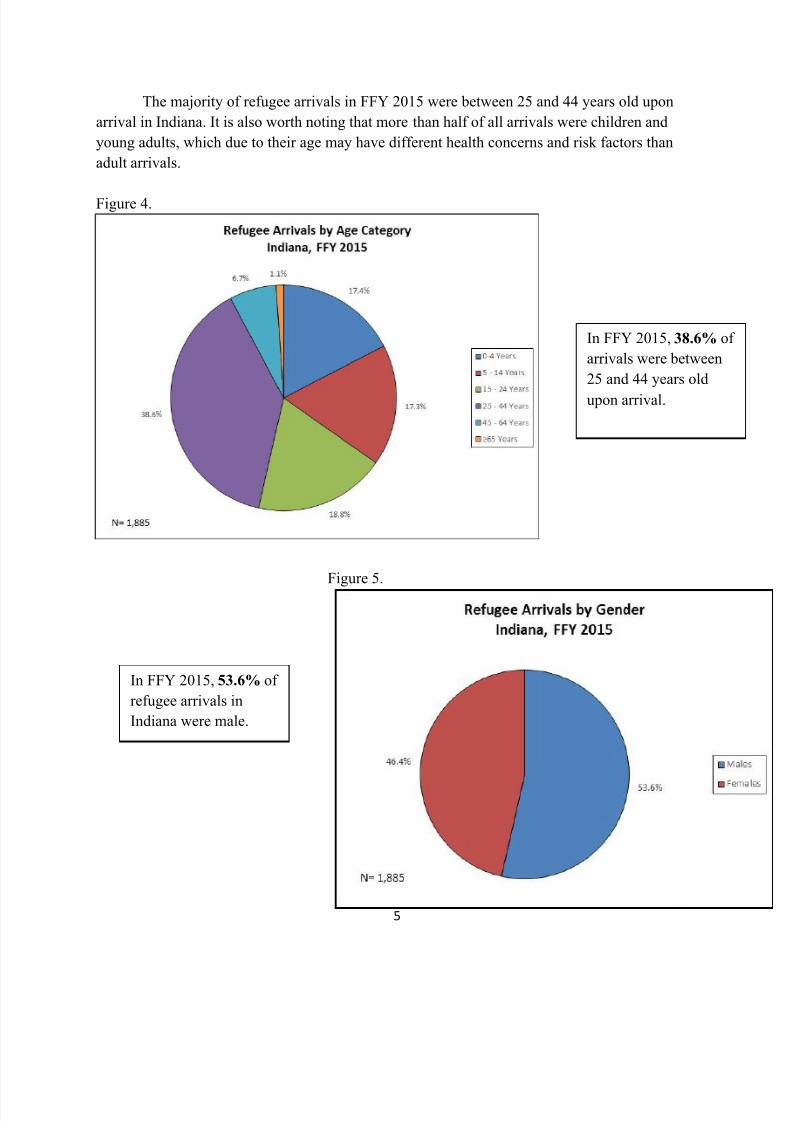
The majority of refugee arrivals in FFY 2015 were between 25 and 44 years old upon
arrival in Indiana. It is also worth noting that more than half of all arrivals were children and
young adults, which due to their age may have different health concerns and risk factors than
adult arrivals.
Figure 4.
Figure 5.
In FFY 2015, 38.6% of
arrivals were between
25 and 44 years old
upon arrival.
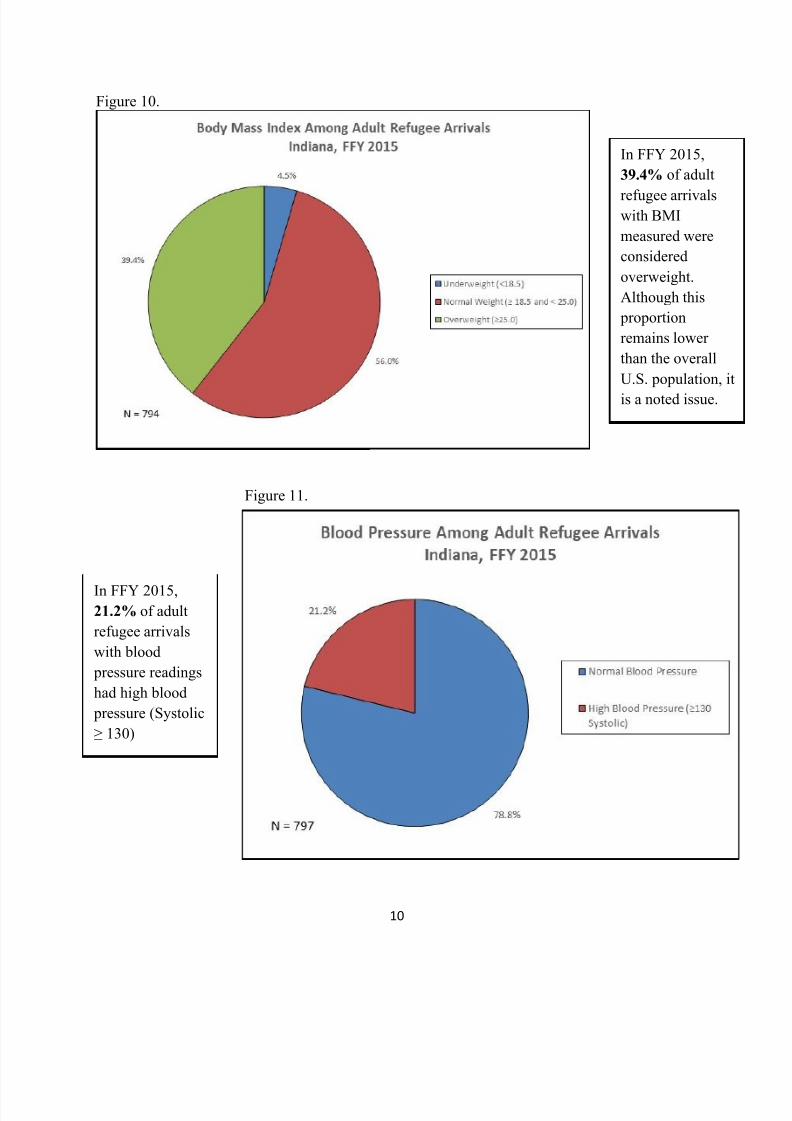
In FFY 2015, 53.6% of
refugee arrivals in
Indiana were male.

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 8/18
6
b. Health Screening
Refugees, regardless of whether they have lived in refugee camps, often have been exposed
to dire living conditions, including poor sanitation, insufficient or unhealthy food and lack of
access to clean, running water. While sanitation and malnutrition are common health threatsrefugees may be exposed to, they are not the only conditions they face. Refugees can suffer from
varying physical and emotional illnesses, some of which can affect them for life. In order to help
address these possible health issues, refugees receive two health screenings, one before entering
the United States and one 30 to 90 days within arrival in Indiana (ORR, 2012). The ISDH
Refugee Health Program is responsible for ensuring the domestic health screening of refugees
entering the State of Indiana. The results of these health screenings are collected in a database so
that the results can be monitored and used to identify ongoing health issues.
After an individual undergoes the application process and becomes a registered refugee, a
U.S. Overseas Processing Entity (OPE), a federal agency in collaboration with the UNHCR, provides the overseas health screening for all refugees (ORR, n.d.). If a refugee is found to have
health issues that could pose a threat to the public, such as active tuberculosis, then the refugee
will not be permitted to enter the U.S. until the issue is resolved. Documentation of this overseas
health screening is sent with the refugee to the U.S. so the domestic health screening will have a
baseline.
Like the overseas health screening, the domestic health screening is intended to protect the
American people from illnesses that could pose a threat to the public. This domestic health
screening is also designed to ensure refugees are linked to health care in the U.S. and are able to
join the workforce in order to be self-sufficient and be less of a burden on U.S. government
assistance programs. Although it does not screen for specific chronic disease, it does include
measures such as Body Mass Index (BMI) and blood pressure that may indicate a need for a
referral for further evaluation.
Prior to their initial health screening in the U.S., refugees apply for health coverage
through Medicaid. If they are not eligible for traditional Medicaid, they receive benefits through
the Refugee Medical Assistance (RMA) program. The RMA is a federal fund used to assist
refugees in covering the cost of medical care during the first eight months of their transition.
After the initial eight-month period, refugees can apply for the Healthy Indiana Plan (HIP 2.0) orget coverage through other means, such as an employer.

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 9/18
7
Figure 6.
Table 2.
Primary Care 1263
Dental 1101
Optometry 189
Pediatrics 113
OBGYN 75
Hearing 38
Mental Health 29
Other 29
ENT 10
Dermatology 8
GI 5
Neurology 4
Urology 3
PHN 1
Family Planning 1
Family Practice 1
WIC 1
Number of Refugee Arrivals Referred by Referral Type
Indiana, FFY 2015
Increased efforts
by the ISDH
Refugee Health
Program and local
health departments
have more than
doubled the
number of refugees
screened within 30
days since 2012.
The most common referral
for refugees in FFY 2015
was for primary care,
followed by dental andoptometry.
During the domestic health
screening, refugees are
referred for further healthservices for any specific
health issues and to ensure
linkage to continued health
care.

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 10/18
8
Intestinal parasites are a concern in the refugee population and are part of the domestic
medical evaluation. Refugees arriving from Thailand and Malaysia are given presumptive
treatment overseas and therefore are excluded from screening upon arrival to the U.S. Refugeeswho screen positive for intestinal parasites during their evaluation are offered treatment and
education on how to prevent further infection.
Figure 7.
Refugees who have identified risk-factors for sexually transmitted infections are screened
for gonorrhea, chlamydia and syphilis during their domestic health screening and are offeredtreatment and education if diagnosed with any infection. During FFY 2015, only 2 percent of
refugees screened for syphilis were found to be infected, and no refugee was found to be infected
with gonorrhea or chlamydia.
Since FFY 2012,
there has been a
160% increase in
the proportion of
screened refugees
that test positivefor intestinal
parasites.

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 11/18
9
Although refugees found to have active tuberculosis (TB) on their overseas health
screening are not permitted to enter the U.S. until they are treated and no longer infectious, all
refugees are still screened for tuberculosis infection and disease during their domestic healthscreening. Refugees found to have latent TB infection are not infectious and cannot spread TB
infection to others (CDC, 2014) and are offered treatment at no cost to them.
Figure 8.
Since January 4, 2010, HIV status is no longer considered grounds to prevent refugee
entry into the U.S. and may even be used as a reason to be granted asylum status (USCIS, 2009).
Figure 9.
26.9% of
refugees were
diagnosed with
LTBI in FFY
2015. Less than
1% were
diagnosed withactive TB disease.
Among screened
refugee arrivals in
FFY 2015, 1.1%
were HIV
positive.
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 12/18
10
Figure 10.
Figure 11.
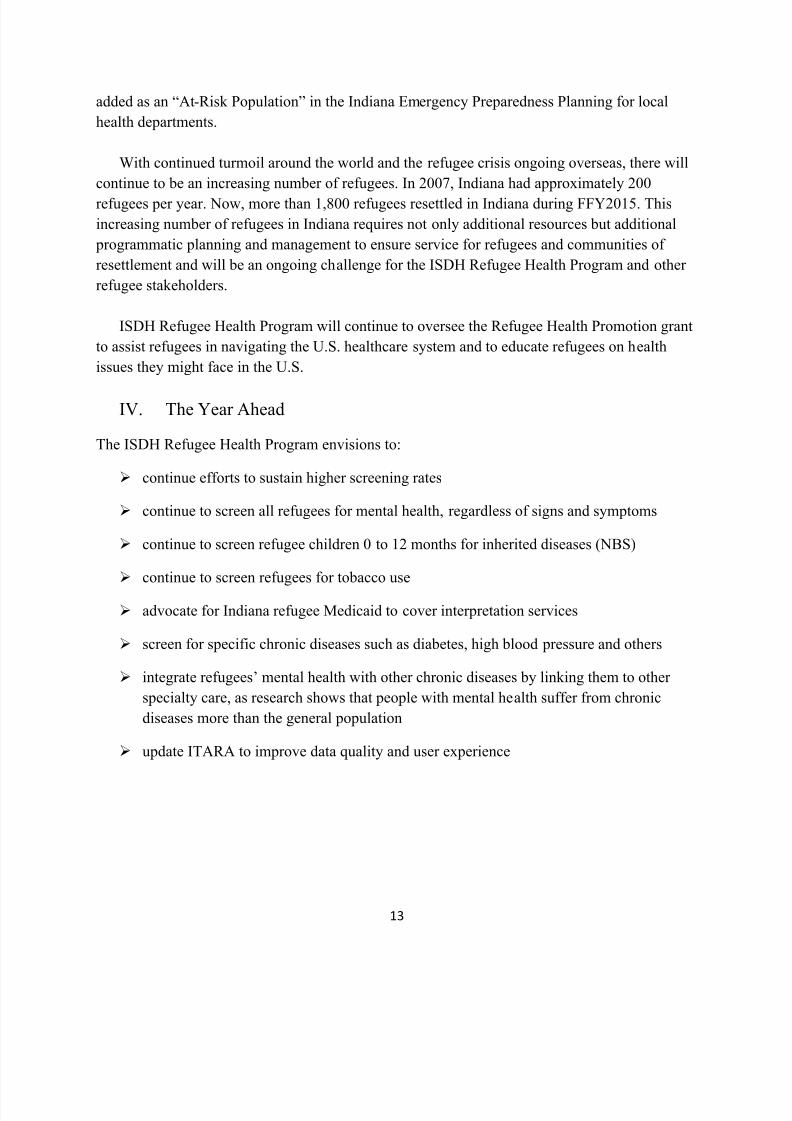
In FFY 2015,
39.4% of adult
refugee arrivalswith BMI
measured were
considered
overweight.
Although this
proportion
remains lower
than the overall
U.S. population, it
is a noted issue.
In FFY 2015,21.2% of adult
refugee arrivals
with blood
pressure readings
had high blood
pressure (Systolic
≥ 130)

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 13/18
11
Refugee children living in camps or poor housing overseas are at high risk for lead
poisoning. Although they are not screened during the overseas health screening, CDC requires
all refugee children age 6 months to 16 years to be screened for lead poisoning during theirdomestic health screening. According to a CDC study, refugees tend to live in older housing
structures upon resettlement in the U.S., so CDC also recommends that refugee children age 6
months to 6 years be retested for lead poisoning after three months of resettlement. The localhealth departments currently are not providing this second screening, since this falls beyond the90 day initial screening period.
Figure 12.
Table 3.
Refugee Arrivals by Pregnancy Status
Indiana, FFY 2015
Total Female Arrivals ≥ 16 Years Old 557
Pregnant 29
Not Pregnant 382
Not Tested 146
Among refugeearrivals under age
17, 10.6% had
elevated blood
lead levels ≥ 5
µg/dl.
Per ORR
guidelines,
screening for
female refugees
age 16 and olderincludes
pregnancy testing
with an opt-out
approach

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 14/18
12
III. Successes & Challenges
Since the ISDH Refugee Health Program began in Indiana, refugees were entitled to receive
traditional Indiana Medicaid upon arrival to provide access to medical services. Following
changes to Indiana Medicaid, newly arrived refugees in FFY 2015 between 19 and 64 years old
in Indiana were assigned to the new Indiana health insurance: Healthy Indiana Plan (HIP). HIP
does not provide the same services as traditional Medicaid, including transportation and
interpretation, which are very important components of healthcare access for refugees. In
addition to the limited services, HIP requires monthly monetary contributions to a health saving
account or the payment of co-pays in order to receive services. This change in health insurance
negatively impacted access to domestic health screening and thus screening rates for the first half
of 2015, along with resettlement agencies’ overall ability to serve refugees.
In response, the ISDH Refugee Program worked collaboratively with other refugee
stakeholders to advocate for refugees’ access to traditional Medicaid. In June, the Family andSocial Services Administration granted access to traditional Medicaid for eight months for
refugees. This eight-month period is sufficient for refugees to have their initial health screening
and receive follow-up for any referrals. The eight-month Medicaid coverage has also boosted the
initial health screening rate to 100 percent for the months of July and August and 98 percent in
the month of September. The slight decrease in September was due to an influx of refugees in
that particular month that placed a higher burden on screening resources.
In an effort to provide extensive services to refugees per ORR State Letter #12-09, the ISDH
Refugee Health Program has initiated and implemented several new services to refugees. Mental
health screening is now provided to all refugees age 14 years and older using the Refugee Health
Screener-15 (RHS-15). This screening tool is not diagnostic but allows the screening clinic to
determine which refugees may be at higher risk for mental health issues and need referral for
further services. Newborn Screening (NBS), provided to U.S.-born babies at the hospital, is now
also provided to all refugee children resettled in Indiana age 12 months and under at time of
arrival. The goals of providing this service include diagnosing inherited diseases as well as
reducing infant mortality. The NBS brochures will be translated into refugees’ native languages
for further education to families. Additionally, tobacco screening and education for tobacco
cessation are now provided to refugees age 12 years and older at the time of U.S. arrival. This
tobacco screening, as well as the NBS, are in line with Governor Pence’s road map.
With limited English proficiency, refugees are vulnerable in case of natural or manmade
disasters. Therefore, the ISDH Refugee Health Program has developed an emergency
preparedness brochure for refugees that will be translated into refugees’ native languages and
distributed during cultural orientation at resettlement agencies. In addition, refugees will be
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 15/18
13
added as an “At-Risk Population” in the Indiana Emergency Preparedness Planning for local
health departments.
With continued turmoil around the world and the refugee crisis ongoing overseas, there will
continue to be an increasing number of refugees. In 2007, Indiana had approximately 200
refugees per year. Now, more than 1,800 refugees resettled in Indiana during FFY2015. This
increasing number of refugees in Indiana requires not only additional resources but additional
programmatic planning and management to ensure service for refugees and communities of
resettlement and will be an ongoing challenge for the ISDH Refugee Health Program and other
refugee stakeholders.
ISDH Refugee Health Program will continue to oversee the Refugee Health Promotion grant
to assist refugees in navigating the U.S. healthcare system and to educate refugees on health
issues they might face in the U.S.
IV. The Year Ahead
The ISDH Refugee Health Program envisions to:
continue efforts to sustain higher screening rates
continue to screen all refugees for mental health, regardless of signs and symptoms
continue to screen refugee children 0 to 12 months for inherited diseases (NBS)
continue to screen refugees for tobacco use
advocate for Indiana refugee Medicaid to cover interpretation services
screen for specific chronic diseases such as diabetes, high blood pressure and others
integrate refugees’ mental health with other chronic diseases by linking them to other
specialty care, as research shows that people with mental health suffer from chronic
diseases more than the general population
update ITARA to improve data quality and user experience
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 16/18
14
V. Glossary
Asylees: Are individuals who, on their own, travel to the United States and subsequently apply
for/receive a grant of asylum. Asylees do not enter the United States as refugees. They may enteras students, tourists, businessmen or even on undocumented status. Once in the U.S., or at a land
border or port of entry, they apply to the Department of Homeland Security (DHS) for asylum.To qualify for asylum status, the person must meet the definition of a refugee and meet an
application deadline. Asylum status permits the person to remain in the United States.
Individuals granted asylum are eligible for ORR assistance and services. (Note that asylum
applicants are not eligible for ORR assistance and services. The only exception is for certain
Cubans and Haitians (ORR, 2015).
Cuban and Haitian entrants are defined as:
A. Any individual granted parole status by the Department of Homeland Security (DHS) as a
Cuban/Haitian Entrant (Status Pending) or granted any other special status subsequently
established under the immigration laws for nationals of Cuba or Haiti, regardless of the status ofthe individual at the time assistance or services are provided, and
B. Any other national of Cuba or Haiti1. Who :(i) was paroled into the United States and has not acquired any other status under the
INA;(ii) is the subject of exclusion or deportation proceedings under the Immigration and
Nationality Act (INA); or (iii) has an application for asylum pending with DHS; and2. With respect to whom a final, non-appealable and legally enforceable order of deportation or
exclusion has not been entered [45 CFR § 401.2]. Cuban and Haitian entrants, along with Cubans
in certain other categories, are eligible to apply for adjustment of status after one year in the U.S.
Parolee: A parolee is an alien who is allowed into the U.S. even though they appear to beinadmissible to the Border and Customs Patrol Officer. Entry will only be permitted for urgent
humanitarian reasons or when the alien’s entry is determined to be for significant public benefit.
The parole is only temporary and the parolee must leave the U.S. when the condition that
allowed them entry ceases to exist.
Primary refugee: A refugee initially resettled in an Indiana jurisdiction (MDH, 2015).
Secondary refugee: A refugee originally resettled in another state in the United States before
moving to Indiana (MDH, 2015).
Special Immigrant Visa (SIV) holders: For their service to the U.S. government in Iraq andAfghanistan, Iraqi and Afghan Special Immigrants (SIVs) are granted status overseas by the U.S.
Department of State and are brought to the United States for resettlement by the U.S. Department
of State. Voluntary agencies and ORR through their programs assist with their resettlement and

8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 17/18
15
integration into the U.S. An SIV is eligible for ORR benefits and services same as a refugee and
for the same time period as a refugee, from the first day the SIV arrives in the U.S (ORR, 2015).
Victim of human trafficking (VTH):The Trafficking Victims Protection Act of 2000 (TVPA) defines “Severe Forms of Trafficking
in Persons” as:trafficking: the recruitment, harboring, transportation, provision, or obtaining of a personfor the purpose of a commercial sex act, in which a commercial sex act is induced by force, fraud
or coercion, or in which the person forced to perform such an act is under the age of 18 years; or
trafficking: the recruitment, harboring, transportation, provision, or obtaining of a person for labor or services, through the use of force, fraud or coercion for the purpose of
subjection to involuntary servitude, peonage, debt bondage or slavery (ORR, 2015).
Victim of torture:
A. “Torture” means an act committed by a person acting under the color of law specifically
intended to inflict severe physical or mental pain or suffering (other than pain or suffering
incidental to lawful sanctions) upon another person within his custody or physical control;B. “Severe mental pain or suffering” means the prolonged mental harm caused by or resultingfrom:
1) intentional infliction or threatened infliction of severe physical pain or suffering;
2) administration or application, or threatened administration or application, of mind-alteringsubstances or other procedures calculated to disrupt profoundly the senses or the personality;
3) threat of imminent death;
4) threat that another person will imminently be subjected to death, severe physical pain orsuffering, or the administration or application of mind-altering substances or other procedures
calculated to disrupt profoundly the senses or personality.
8/16/2019 State of Indiana Refugee Health Program Annual Report 2015
http://slidepdf.com/reader/full/state-of-indiana-refugee-health-program-annual-report-2015 18/18
16
VI. References
Office of Refugee Resettlement (2012). Medical Screening Protocol for Newly Arriving
Refugees. Retrieved from http://www.acf.hhs.gov/programs/orr/resource/medical-screening-protocol-for-newly-arriving-refugees
Office of Refugee Resettlement (n.d.) Emotional Wellness and Suicide Prevention. Podcastretrieved from http://www.acf.hhs.gov/programs/orr/programs/refugee-health
Office of Refugee Resettlement (2015). Refugee Fact Sheet. Retrieved from
http://www.acf.hhs.gov/programs/orr/spotlight#fact-sheets Center for Disease Control and Prevention (2014). The Difference Between Latent TB Infection
and TB Disease. Retrieved from
http://www.cdc.gov/tb/publications/factsheets/general/LTBIandActiveTB.htm Minnesota Department of Health (MDH) (2015). Refugee Health Statistics. Retrieved from
http://www.health.state.mn.us/refugee/stats/#primary
United States Citizenship and Immigration Services (2009). Memorandum. Retrieved from
http://www.uscis.gov/sites/default/files/USCIS/New%20Structure/Laws%20and%20Reg
ulations/Memoranda/2009/HIVInadmissibilityFinalHHSRule.pdf