Embed Size (px)
Citation preview
State Perspectives on Quality Performance Measures and Payment Innovation
November 16, 2016
Patrick J. RoohanDirector, Office of Quality and Patient Safety
2
New York State Department of Health
• Core mission is consistent with the triple aim:– Improve quality of care– Improve population health– Reduce costs
• Office of Quality and Patient Safety is the focal point of quality/safety initiatives for the DOH and beyond
• Lead in quality, data, HIT, evaluation and Healthcare innovation
3
Why Healthcare Reform, Why Now?
4
Why Healthcare Reform, Why Now?
$19,630
5
Why Healthcare Reform, Why Now?
$19,630• $19,630 is the cost of family health insurance coverage in NY
• Up from $12,075 in 2006, 60% increase over 9 years
• Cost sharing is going up – premium and deductibles are 10% of median income

6
Why Healthcare Reform, Why Now?
Quality Results are Mixed
7
Why Healthcare Reform, Why Now?
Quality Results are MixedGood News:• NY Ranks 14th in access to care: low % uninsured, high % accessing MDs• NY Ranks 13th in healthy living: low % smokers, low obesity rate,
low in many mortality measuresBad News:• NY Ranks 26th in avoidable hospital use and costs: high rate of avoidable hospitalizations
and ER visits• NY Ranks 28th in prevention and treatment: low rate of vaccinations,
poor hospital discharge planning, high rate of pressure sores
8
Healthcare Reform• PCMH• SHIP• SIM• APC• MACRA• MIPS• APMs• CPC+• DSRIP• VBP
How can we keep up with the “Alphabet Soup?”
All programs are well-intended – improve quality, reward quality, and control costs
9
Definitions• PCMH (Patient Centered Medical Home)
– A certification process developed by NCQA that can lead to lower costs, improved patient experience and better health outcomes.
• SHIP (State Health Improvement Plan)– A five year comprehensive plan to move NY’s health care system towards triple
aim goals: improved health, better health care, affordability
• SIM (State Innovation Model) Grant– $100 million dollar grant from CMMI towards implementing parts of the SHIP
• Specific ‘deliverables’ including a substantial movement from FFS payment to ‘value based’ payments over 5 years
• APC (Advanced Primary Care Model)– A primary care model for multi-payer engagement as part of the SIM grant.
10
Definitions
• MACRA (Medicare Access and CHIP Reauthorization Act)– Medicare’s new model that rewards value over volume, moving away from Fee-
for-service. Two tracks: MIPS and APMs
• MIPS (Merit-based Incentive Payment System)– Medicare’s new incentive program that combines quality, resource use, clinical
improvement and meaningful use of HIT
• APMs (Alternative Payment Models)– APMs are new approaches to paying for medical care through Medicare that
incentivize quality and value.
11
Definitions
• CPC+ (Comprehensive Primary Care Plus)– A national advanced primary care medical home model that aims to strengthen
primary care through a regionally-based multi-payer payment reform and care delivery transformation. Improved from the CPC program.
• DSRIP (Delivery System Redesign Investment Payment Program)– $6.4 billion dollar investment from CMS in NY Medicaid to provide more
integrated care focused on improving quality, reducing avoidable costs• Specific deliverables on quality improvement, avoidable admission reductions
• VBP (Value-Base Purchasing)– Is a strategy for linking payment to quality, not payment for volume. VBP is the
cornerstone of SIM, MACRA and DSRIP
12
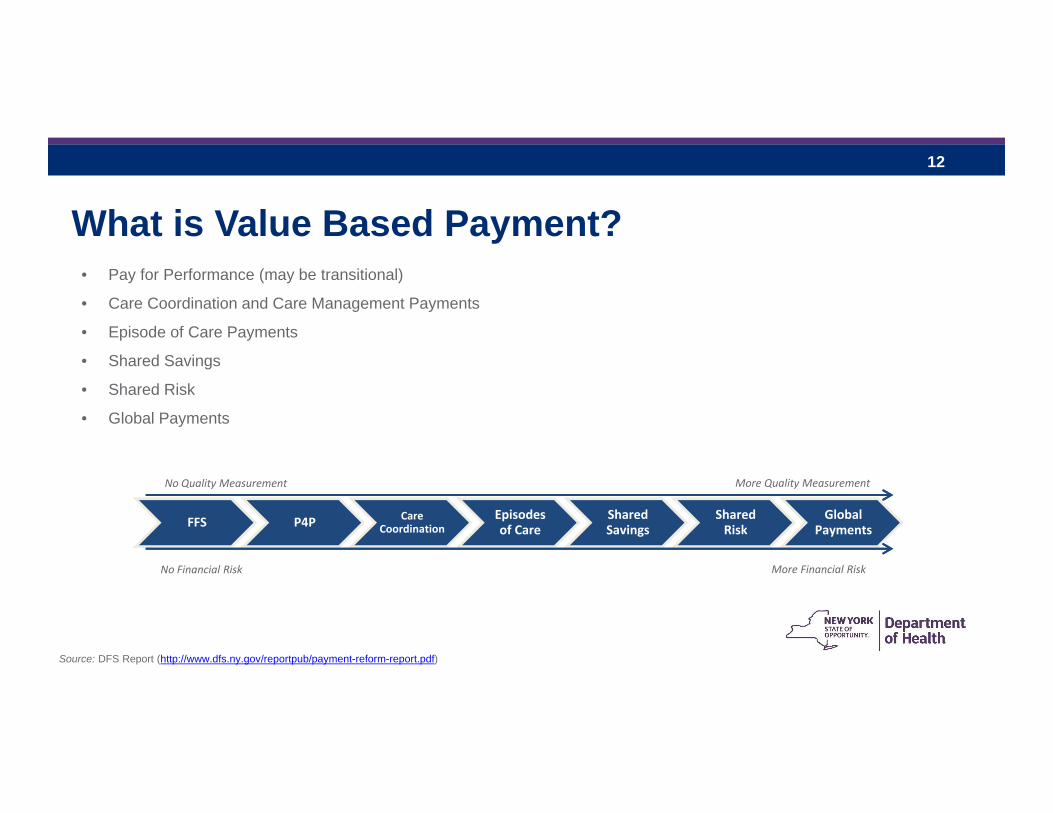
What is Value Based Payment?• Pay for Performance (may be transitional)
• Care Coordination and Care Management Payments
• Episode of Care Payments
• Shared Savings
• Shared Risk
• Global Payments
FFS P4P Care Coordination
Episodes of Care
Shared Savings
Shared Risk
Global Payments
No Quality Measurement
No Financial Risk
More Quality Measurement
More Financial Risk
Source: DFS Report (http://www.dfs.ny.gov/reportpub/payment-reform-report.pdf)
13
Health Plans and Providers are Already Engaged in Payment ReformDFS Survey (published July 2014) found:
• Variability. All major insurers had value-based payment (VBP) programs. But they are independent with inconsistent progress.
• Few Providers Impacted. Just 15% of participating providers were in VBP.• Few Consumers Impacted. Just 12% of insurers’ members were in VBP.• Most VBP Programs Still Pay on FFS Basis. Most insurers’ VBP (80%) make value-based or care
coordination payments in addition to FFS payments.• Pay-for-Performance (P4P) Predominates. Almost half of VBP are “Pay-for-Performance” models.• Some Evidence of Savings, But Most Yet to Be Measured. • Primary Care Focused. Most of VBP models involve primary care. Specialists, hospitals, non-physician
services and emergency room (ER) to a lesser degree. Lab and radiology services the least.
Source: DFS Report (http://www.dfs.ny.gov/reportpub/payment-reform-report.pdf)
14
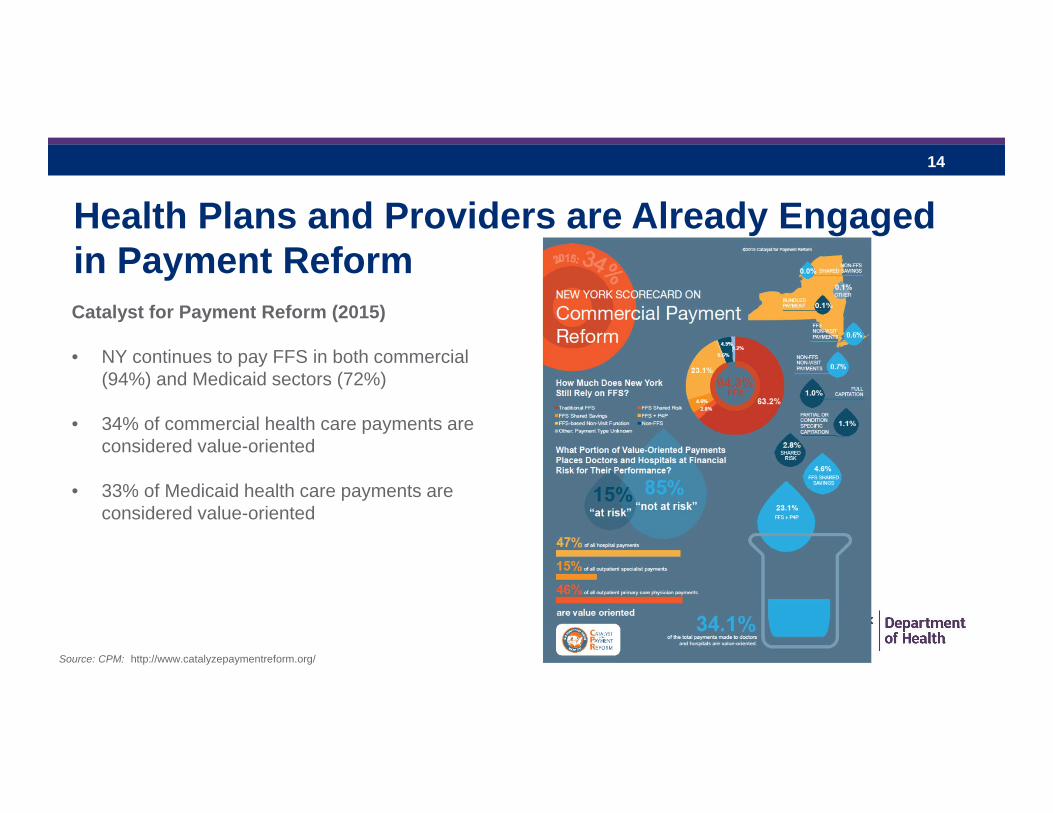
Health Plans and Providers are Already Engaged in Payment ReformCatalyst for Payment Reform (2015)
• NY continues to pay FFS in both commercial (94%) and Medicaid sectors (72%)
• 34% of commercial health care payments are considered value-oriented
• 33% of Medicaid health care payments are considered value-oriented
Source: CPM: http://www.catalyzepaymentreform.org/
15
Value Based PaymentIncreases the Importance of and
Need forQuality Measurement
RAINA JOSBERGEROFFICE OF QUALITY AND PATIENT SAFETYNEW YORK STAT DEPARTMENT OF HEALTHNOVEMBER 19, 2014
16
Health Care Reform and Value Base Payment:Need for Quality Measurement and HIT to Succeed
Health Care Reform
‐ Quality Measurement‐ Use of HIT

17
New York State Initiatives in Quality
RAINA JOSBERGEROFFICE OF QUALITY AND PATIENT SAFETYNEW YORK STATE DEPARTMENT OF HEALTHNOVEMBER 19, 2014
18
Quality Measurement
• Quality measurement of health plans (QARR)– Current: Medicaid, CHPlus, special needs plans, commercial
managed care, MLTC, qualified health plans, the Essential Plan
– Proposed: FIDA, behavioral health, HARP• DSRIP
– Significant measurement component across PPS projects
19
Quality Measurement (continued)
• Quality measurement of hospitals – Cardiac– Stroke care– HAI– Potentially Preventable Readmissions– Potentially Preventable Complications
• Long term care quality– Nursing home quality measures– Nursing home quality initiative– Home care quality measures
20
Financial Incentives for Higher Quality:
Current Medicaid Quality Incentive Programs
21
Medicaid Managed Care Quality Incentive
• Uses the QARR measurement set for the health care delivery system:
– Healthcare Effectiveness Data & Information Set (HEDIS®) measures which are developed by the National Committee for Quality Assurance (NCQA) AND
– New York State-Specific Measures
– CAHPS® – Consumer Assessment of Healthcare Providers and Systems- Satisfaction
21
22
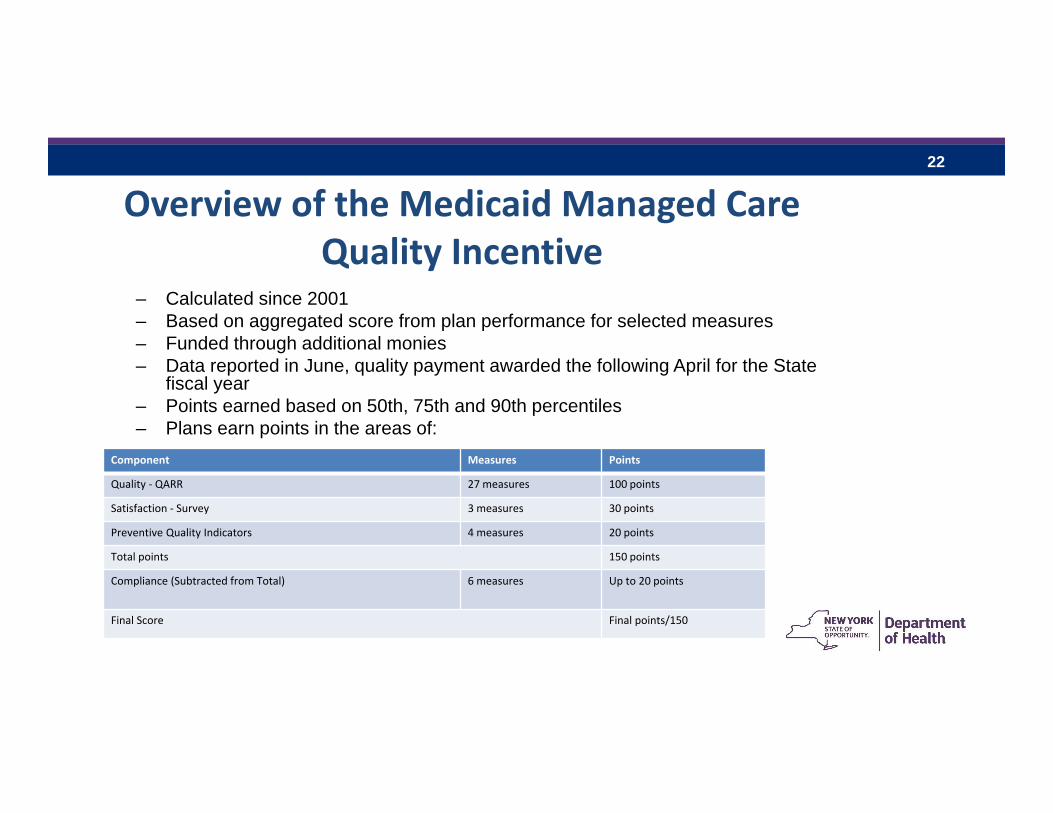
Overview of the Medicaid Managed Care Quality Incentive
– Calculated since 2001– Based on aggregated score from plan performance for selected measures– Funded through additional monies– Data reported in June, quality payment awarded the following April for the State
fiscal year– Points earned based on 50th, 75th and 90th percentiles – Plans earn points in the areas of:
Awards include financial and auto-assignment preference
Component Measures Points
Quality ‐ QARR 27 measures 100 points
Satisfaction ‐ Survey 3 measures 30 points
Preventive Quality Indicators 4 measures 20 points
Total points 150 points
Compliance (Subtracted from Total) 6 measures Up to 20 points
Final Score Final points/150
23
MMC Quality Incentive Measures
23
Quality measure examples• Avoidance of Antibiotics for Adults with Acute Bronchitis• Breast Cancer Screening• Cervical Cancer Screening
Satisfaction measure examples• Rating of Health Plan• Getting Care Needed
Preventive Quality Indicators • Two composites of select adult and pediatric PQIs/PDIs and a respiratory composite measure for adults and an asthma measure for children
Compliance• Any statement of deficiency for Plan Network, Encounter data submission,
Quality Reporting, etc.
24
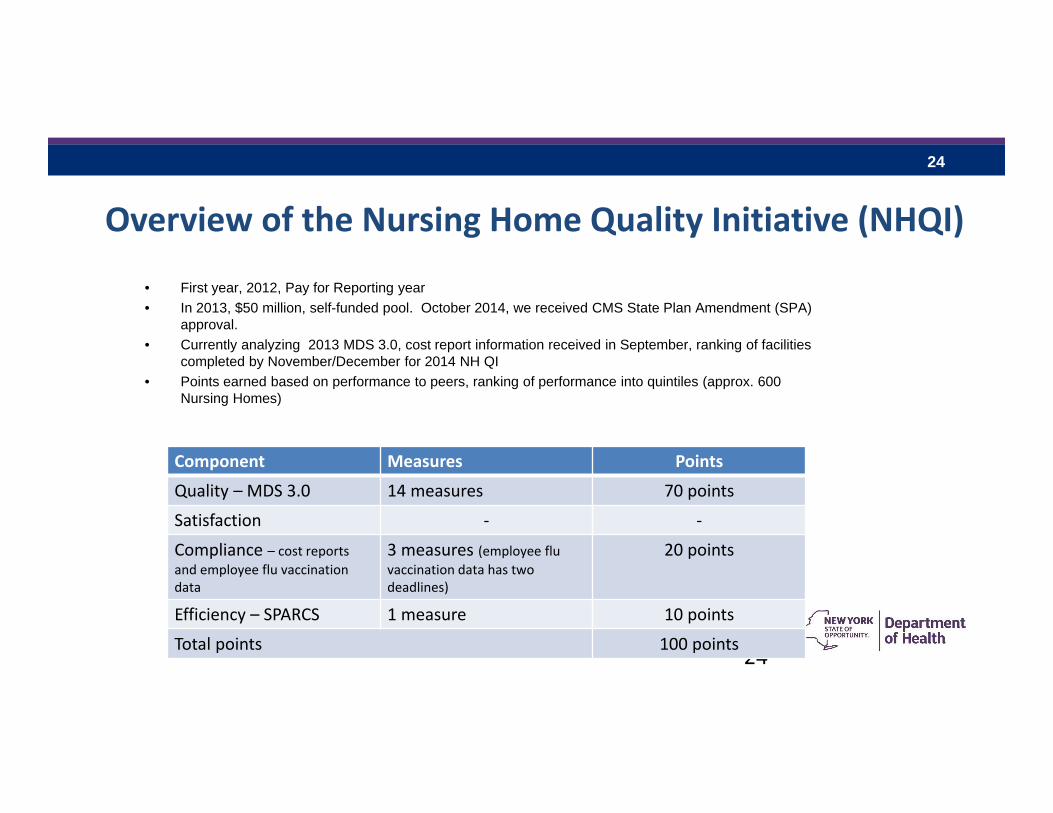
Overview of the Nursing Home Quality Initiative (NHQI)
• First year, 2012, Pay for Reporting year• In 2013, $50 million, self-funded pool. October 2014, we received CMS State Plan Amendment (SPA)
approval.• Currently analyzing 2013 MDS 3.0, cost report information received in September, ranking of facilities
completed by November/December for 2014 NH QI • Points earned based on performance to peers, ranking of performance into quintiles (approx. 600
Nursing Homes)
24
Component Measures Points
Quality – MDS 3.0 14 measures 70 points
Satisfaction ‐ ‐
Compliance – cost reports and employee flu vaccination data
3 measures (employee flu vaccination data has two deadlines)
20 points
Efficiency – SPARCS 1 measure 10 points
Total points 100 points
25
NHQI Measures
Quality examples Percent of Long Stay Residents Who Self‐Report Moderate to Severe Pain Percent of Long Stay High Risk Residents With Pressure Ulcers Percent of Long Stay Residents Whose Need for Help with Daily Activities Has Increased
Percent of Long Stay Residents with a Urinary Tract InfectionCompliance CMS’ Five‐Star Quality Rating for Health Inspections Timely submission of Nursing Home Certified Cost Reports (due 8/15/14 for non‐fiscal filers and 9/30/14 for fiscal filers)
Timely submission of Employee Flu data (due 11/15/13 and 5/1/14)Efficiency – Potentially Avoidable Hospitalizations The number of potentially avoidable hospitalizations per 10,000 long stay episode days
25
26
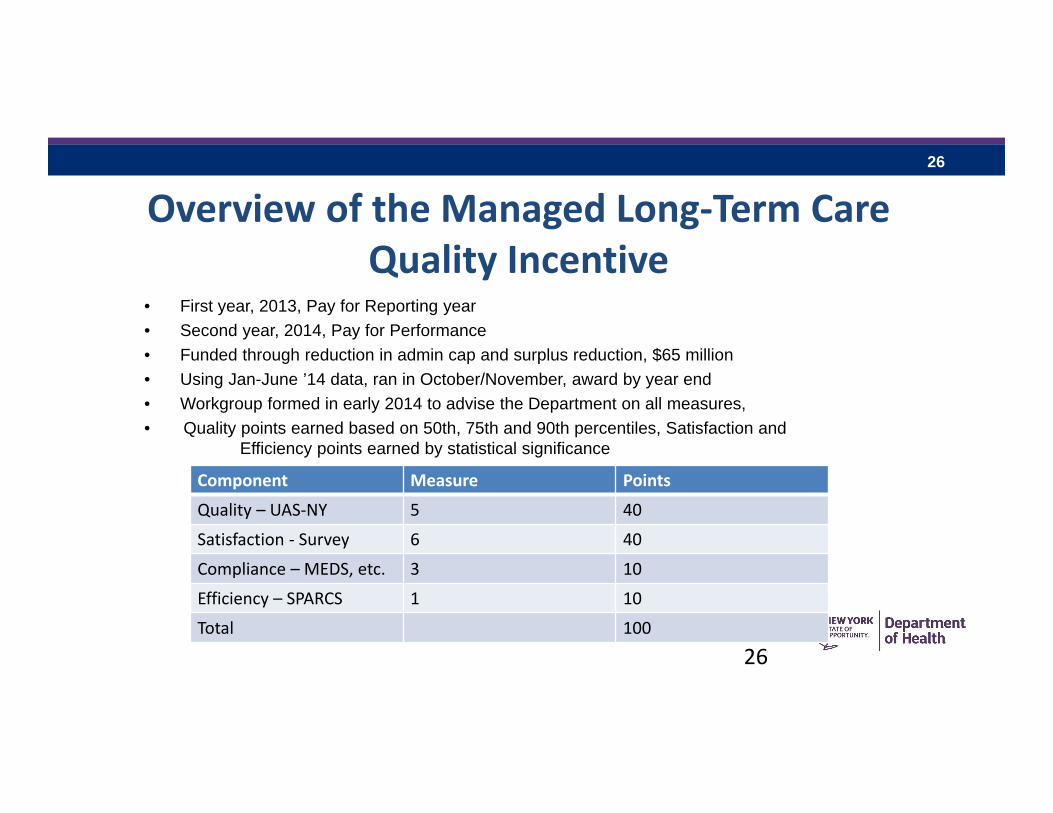
Overview of the Managed Long‐Term Care Quality Incentive
• First year, 2013, Pay for Reporting year• Second year, 2014, Pay for Performance• Funded through reduction in admin cap and surplus reduction, $65 million • Using Jan-June ’14 data, ran in October/November, award by year end• Workgroup formed in early 2014 to advise the Department on all measures, • Quality points earned based on 50th, 75th and 90th percentiles, Satisfaction and
Efficiency points earned by statistical significance
26
Component Measure Points
Quality – UAS‐NY 5 40
Satisfaction ‐ Survey 6 40
Compliance – MEDS, etc. 3 10
Efficiency – SPARCS 1 10
Total 100
27
MLTC QI MeasuresQuality examples Percentage of members who received an influenza vaccination in the last year Percentage of members who did not have falls resulting in medical intervention in the last 90 days Percentage of members who did not have an emergency room visit in the last 90 days
Satisfaction examples Percentage of members who rated their managed long‐term care plan as good or excellent Percentage of members who rated the quality of home health aide or personal care aide services within the last six months as good or excellent
Compliance examples No statement of deficiency for timeliness or completeness of Medicaid Encounter Data III submission for the measurement year
Efficiency – Potentially Avoidable Hospitalizations The number of potentially avoidable hospitalizations
27
28
FIDA Quality• January 1, 2015 start date• FIDA plans will be reporting
– Medicare Healthcare Effectiveness Data and Information Set (HEDIS)• Annual data collection by the health plans
– Health Outcome Survey (HOS)• Annual survey sponsored by the health plans
– Consumer Assessment of Healthcare Providers and Systems (CAHPS) satisfaction data• Annual survey sponsored by the health plans
– They will also be using the UAS‐NY to assess their members every six months• 1% Quality Withhold on the Medicaid/Medicare components of the capitation rate. These
withheld amounts will be repaid subject to FIDA plans’ performance.
28
29
FIDA Quality Withhold Measures
• Year 1 measure examples– Encounter data submitted accurately and completely in compliance with
contractual requirements– Customer Service – CAHPS measure– Getting appointments and care quickly – CAHPS measure
• Year 2 and 3 measure examples– Plan all‐cause readmissions – NCQA/HEDIS measure– Annual Flu vaccine – CAHPS measure– Controlling High Blood pressure – NCQA/HEDIS measure
29
30
Delivery Service Reform Incentive Payment (DSRIP)
• $6.2B from CMS to reform healthcare in NYS• Awarded in 2014• First year will be 2015, incentives to Performing Provider Systems (PPS) will be based on
milestones reached each year• Money is not guaranteed • PPS’s must choose projects from a list and must show improvement for the associated
measures to obtain the full incentive
30
Issues being AddressedIssues being Addressed
31
Managed Care Publications • Medicaid managed care quality reports:
http://www.health.ny.gov/health_care/managed_care/reports/index.htm
– Regional Consumer Guides: http://www.health.ny.gov/health_care/managed_care/reports/quality_performance_improvement.htm#link4
• Nursing home quality Initiative:http://www.health.ny.gov/health_care/medicaid/redesign/nursing_home_quality_initiative.htm
• Managed Long Term Care quality reports: http://www.health.ny.gov/health_care/managed_care/mltc/reports.htm– Regional Consumer Guides:
http://www.health.ny.gov/health_care/managed_care/mltc/consumer_guides/
31
32
Data Transparency
Open Data NY:https://health.data.ny.gov/
32
33
Current Mechanisms to Monitor Quality are not sufficient
• Current measurement activities rely on:– Claims– Chart reviews– Disease or content-based data collection
• Not timely
• Costly
• Significant provider burden 33

34
(EHR + Registry + Claims + Other)
Health IT‐enabled Quality Measurement
35
Initiatives that collect or intend to collect EHR data for use in quality measurement
To name a few of the current ones… Adirondack multi‐payer initiative
Value Based Payment initiatives APC Scorecard as part of SIM DSRIP PPS CMS MACRA with MIPS/APM
MEIPASS(Medicaid Meaningful Use) Providers must report eCQMs generated EHRs
KEY REQUIREMENT – Alignment of capability to integrate data for calculation of quality measures for various uses
36
Principles and Assumptions for Data Collection
Connect once, use multiple times Should align with, and invoke, federal standards for certified technology Ensure data can be used to calculate measures at multiple population
health levels Data collected from EHRs should be used to support multiple measures EHR derived data will provide some, but not all, data necessary to calculate
quality measures Would be used in combination with claims, registry and other data
37
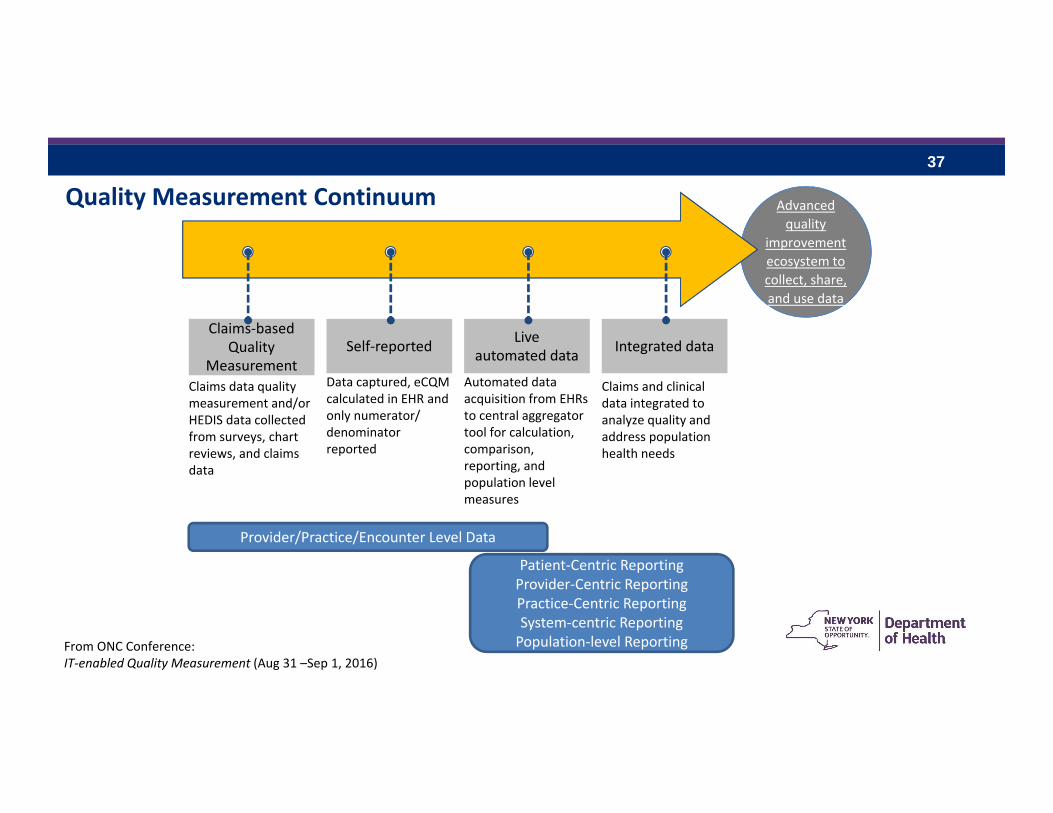
Claims‐based Quality
Measurement
and use data
Advanced quality
improvement ecosystem to collect, share, and use data
Provider/Practice/Encounter Level Data
Claims data quality measurement and/or HEDIS data collected from surveys, chart reviews, and claims data
Live automated data
Automated data acquisition from EHRs to central aggregator tool for calculation, comparison, reporting, and population level measures
Self‐reported
Data captured, eCQMcalculated in EHR and only numerator/ denominator reported
Integrated data
Claims and clinical data integrated to analyze quality and address population health needs
Patient‐Centric ReportingProvider‐Centric ReportingPractice‐Centric ReportingSystem‐centric ReportingPopulation‐level Reporting
Quality Measurement Continuum
From ONC Conference:IT‐enabled Quality Measurement (Aug 31 –Sep 1, 2016)
38
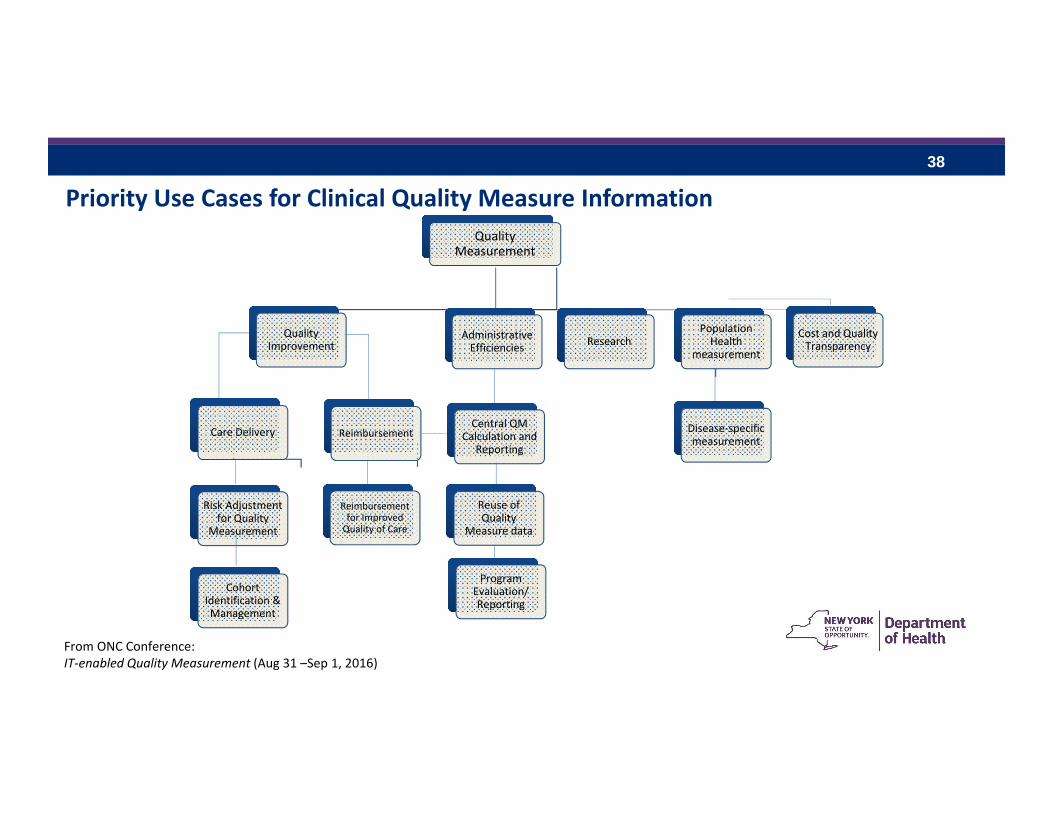
Quality Measurement
Quality Improvement
Care Delivery
Risk Adjustment for Quality
Measurement
Cohort Identification & Management
Reimbursement
Reimbursement for Improved Quality of Care
Administrative Efficiencies
Central QM Calculation and
Reporting
Reuse of Quality
Measure data
ResearchPopulation Health
measurement
Disease‐specific measurement
Cost and Quality Transparency
Priority Use Cases for Clinical Quality Measure Information
Program Evaluation/ Reporting
From ONC Conference:IT‐enabled Quality Measurement (Aug 31 –Sep 1, 2016)
39
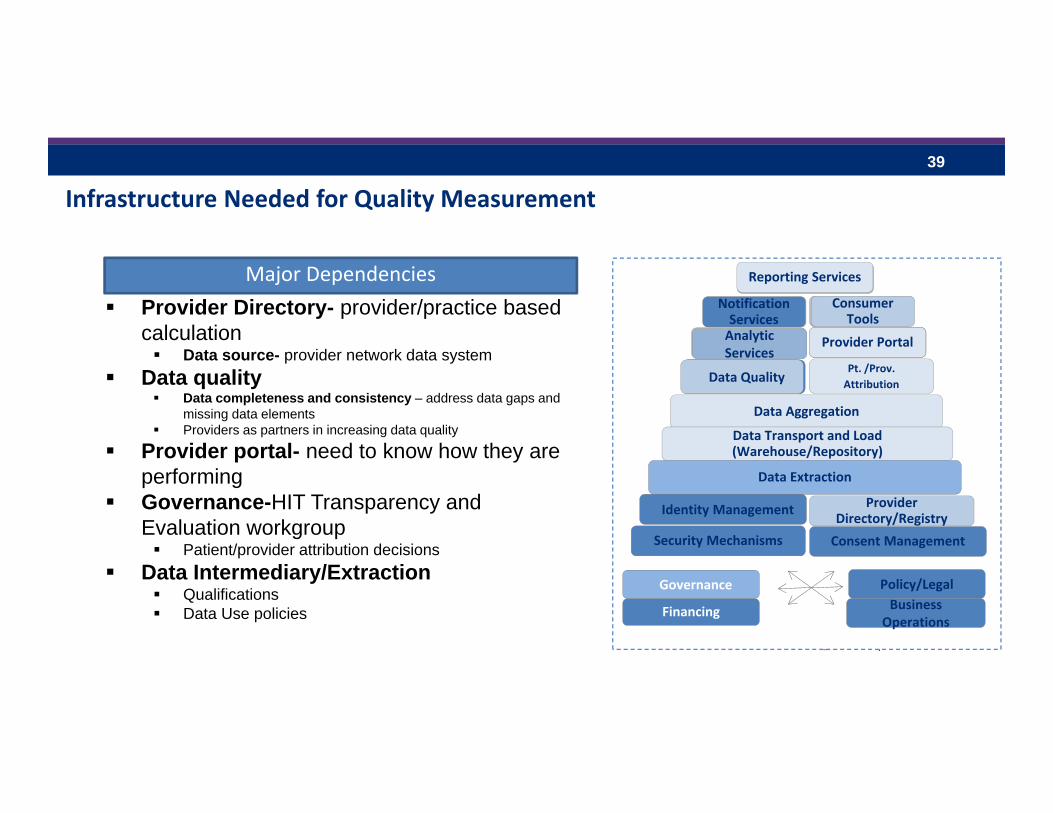
Infrastructure Needed for Quality Measurement
Provider Directory- provider/practice based calculation Data source- provider network data system
Data quality Data completeness and consistency – address data gaps and
missing data elements Providers as partners in increasing data quality
Provider portal- need to know how they are performing
Governance-HIT Transparency and Evaluation workgroup Patient/provider attribution decisions
Data Intermediary/Extraction Qualifications Data Use policies
Data Aggregation
Reporting Services
Notification Services
Consumer Tools
Analytic Services
Provider Portal
Data QualityPt. /Prov. Attribution
Data Transport and Load (Warehouse/Repository)
Data Extraction
Identity Management Provider Directory/Registry
Security Mechanisms Consent Management
Governance
Financing
Policy/LegalBusiness
Operations
Major Dependencies Reporting Services
Notification Services
Consumer Tools
Analytic Services
Provider Portal
Data Quality
40
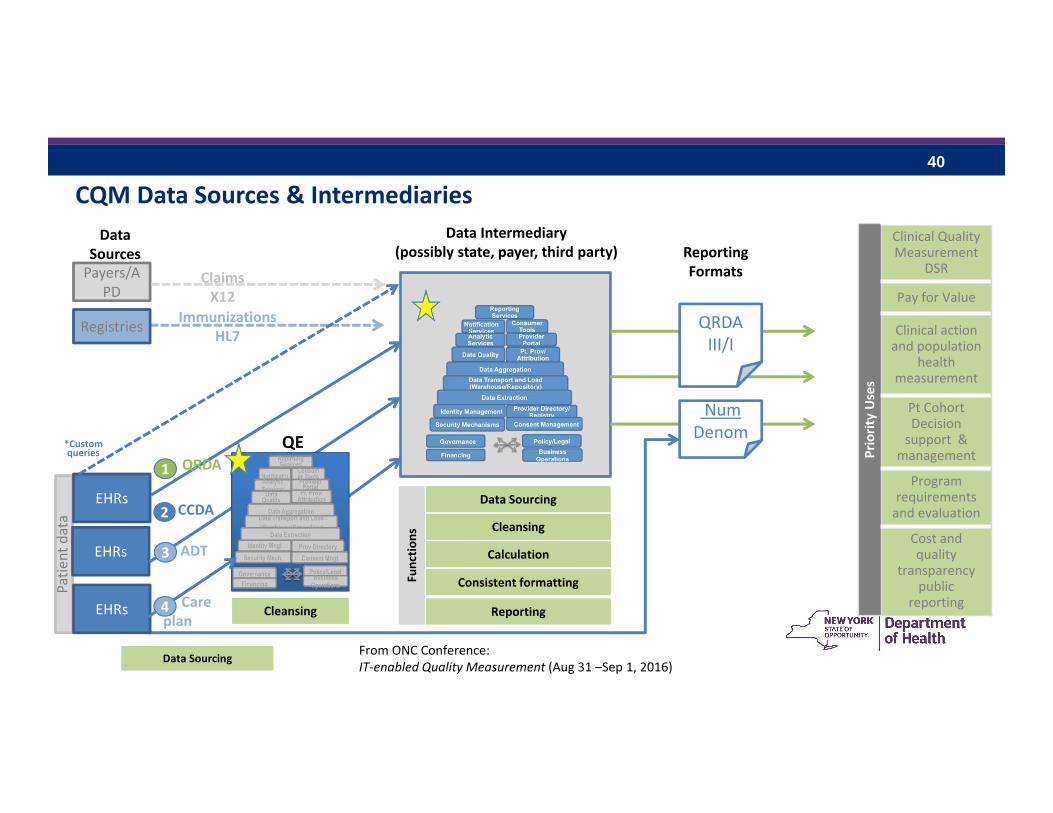
CQM Data Sources & Intermediaries
Payers/APD
Registries
Patie
nt data
Data Sources
Data Intermediary(possibly state, payer, third party)
EHRs
Data SourcingData Sourcing
PriorityUses
Clinical Quality Measurement
DSR
Pay for Value
Clinical action and population
health measurement
Pt Cohort Decision support &
management
Program requirementsand evaluation
Cost and quality
transparency public
reporting
ReportingFormats
EHRs
EHRs
CalculationCalculation
CleansingCleansing
Consistent formatting Consistent formatting
Data SourcingData Sourcing
QE
CleansingCleansing
QRDA11
CCDA22
ADT33
*Custom queries
QRDA III/I
ReportingReporting
Functio
nsFunctio
ns
Immunizations HL7
Num Denom
ClaimsX12
44 Care plan
From ONC Conference:IT‐enabled Quality Measurement (Aug 31 –Sep 1, 2016)
41
Investments in HIT:The SHIN‐NY
All Payer Database (APD)RAINA JOSBERGEROFFICE OF QUALITY AND PATIENT SAFETYNEW YORK STATE DEPARTMENT OF HEALTHNOVEMBER 19, 2014
42
SHIN‐NY
• Statewide Health Information Network for New York (SHIN‐NY) is a network that connects electronic medical records across New York State. – Within Regions through RHIOs (Regional Health Information Organizations)
– Across Regions through Statewide Patient Record Lookup
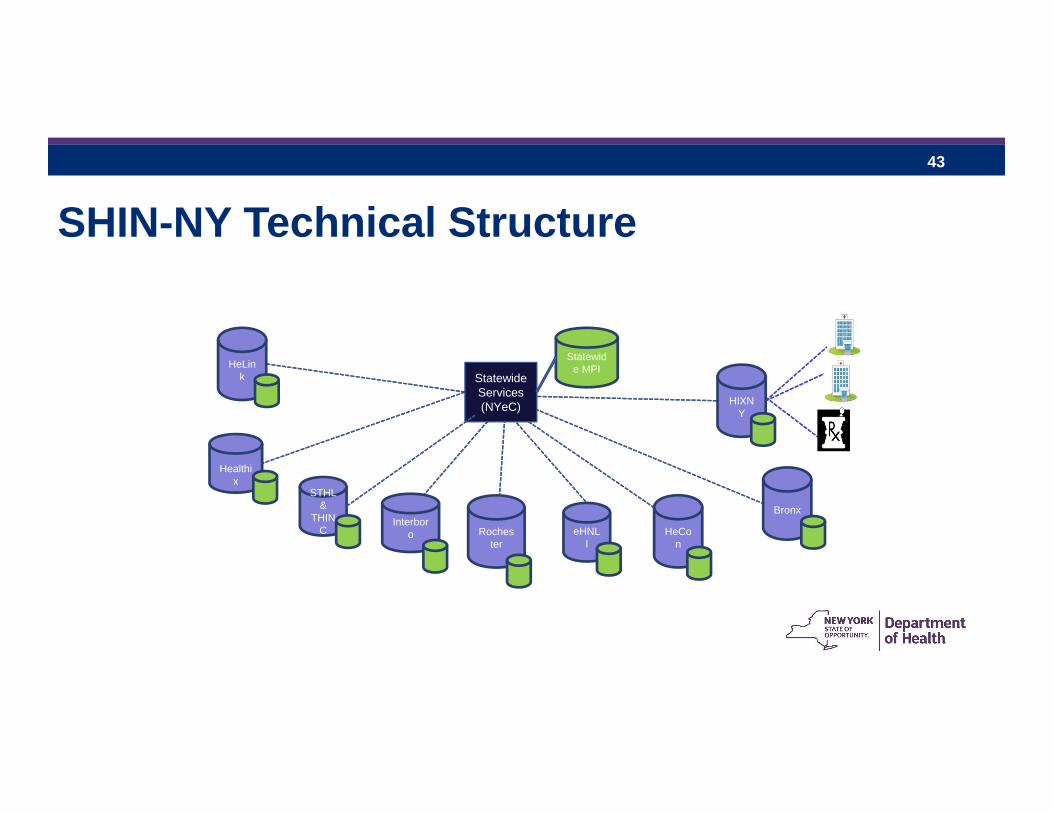
43
SHIN-NY Technical Structure
Healthix
STHL &
THINC
Interboro eHNL
I
Bronx
HIXNY
Rochester
HeCon
HeLink Statewide
Services(NYeC)
Statewide MPI
44
SHIN‐NY Core Services
• Allows a provider to see all of your medical records in his/her electronic medical record, including information from other providers and other health systems
• If your physician doesn’t have an electronic system, your records can still be accessed by him or her through an application that will include information from other doctors, hospitals and clinics
• Provides alerts (immediate notifications) if you are in the ED, you are admitted to the hospital, or you are discharged from the hospital

45
SHIN‐NY Core Services
• Consent management – approval by the patient for clinicians to view their data
• Identity management and security – system to assure access to the correct records, with proper security protocols
• Connections to public health systems
46
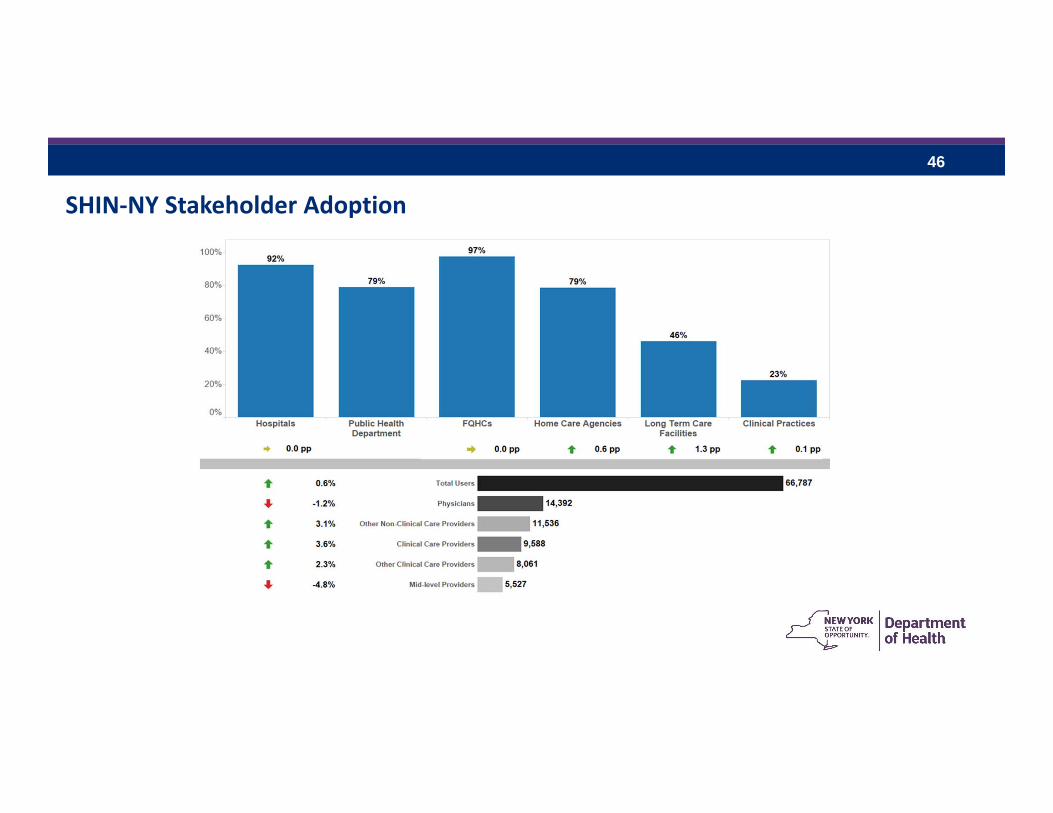
SHIN‐NY Stakeholder Adoption
47
Issues being Addressed• Consent. The SHIN‐NY Policy Committee is reviewing the current
consent model, with a report due in December• In the process of implementing cross‐QE alerts with 3 QEs, with
more to follow• Adoption• Complete data• Improving quality of the data• Using the data for quality measurement across providers, plans,
health systems
48
Expanding Long Term Care Providers’ Connections to the SHIN‐NY
• New York eHealth Collaborative administers an incentive program for Medicaid Meaningful Use Incentive program Eligible Providers to connect to the SHIN-NY
• Would expand the Data Exchange Incentive Program beyond Meaningful Use Incentive eligible providers, including long-term care, mental health, home care and others
– Allowed by CMS Medicaid Director Letter 16-003• Allow for $10,000 for those providers who connect and make data available to the SHIN-
NY• Awaiting approval from CMS
Challenges:• Dealing with non-certified systems
– Amount of data that can be made available– Security of non-certified systems- program will likely need to invoke federal HIT certification
standards related to security
49
All Payer Database (APD): What is it?The APD will be a large repository of consolidated information that will integrate health care data across all payers and all sites of care.
The APD will:• Support health care finance policy, population health and health care
system comparisons and improvements.• Serve as a key resource for consumers, providers and payers.
• The APD will begin with claims and encounter data from insurance companies.
50
APD Background
• New York State legislation enacted in the spring of 2011 (same statutory authority as SPARCS).
• Funded through Health Insurance Exchange Establishment Grants, SFY 2014‐2015 budget (HCRA funds), State Medicaid, and Federal Medicaid matching funds.
• https://www.health.ny.gov/technology/all_payer_database/
51
What is the Value of the All Payer Database
Utilization of Services Quality of Care
Cost of Care Population Health
APD
52
Who Benefits from the APD?
• State policy makers / public health• Consumers• Health insurance plans• Health care providers• Employers• Researchers
53
Progress
• APD proposed regulations out for comment– Received comments in October and in the process of reviewing
• APD Guidance Document– Under review. Policies, data reporting formats, operational
requirements
• Contract with Optum Government Solutions for data warehousing and analytic tools
54
Challenges• APD data intake solution has been delayed
– Commercial data to start in 2017
• Authority to collect self‐insured data is in question. March Supreme Court Decision, Gobeille vs. Liberty Mutual – disallowed APD reporting mandate on Self‐Insured Plans (ERISA pre‐emption ruling)
– Approximately 50% of commercially insured New Yorkers are in self‐insured products– The New York State Health Insurance Plan (NYSHIP) is self‐insured, and we are working with
the Department of Civial Service to get their participants to submit data to the APD– The court suggests that states’ APD interests might be served pursuing newly created reporting rules from
the US Depts. of Labor or Health and Human Services; the APCD National Council is coordinating a unified states’ dialogue with USDoL
55
The New York State Health Insurance Program (NYSHIP) includes both state and local government enrollees with coverage for 1.2 million
APD discussions are ongoing with Civil Service as voluntary reporting by this payer would instantly pull in a third of NY’s currently self‐insured pool (though continued growth in the self‐insured segment is expected to erode NYSHIP’s portion of the pie)
More limited dialogue on voluntary reporting has also taken place with smaller self‐insured plans in western and northern NY
Lastly, the Court suggests that states’ APD interests might be served pursuing newly created reporting rules from the US Depts. of Labor or Health and Human Services (removing federal statute pre‐emption from the equation); the APCD National Council is coordinating a unified states’ dialogue with USDoL
March Supreme Court Decision (cont.)
56
Questions?