Embed Size (px)
Citation preview
Clinical Development
ENA-713 [Rivastigmin; Exelon®]
Non-interventional Study Report
Study Code: CENA713DDE23
STATT – A non-interventional study to investigate factors associated with adherence to Exelon
® patch for the treatment of
Alzheimer’s disease
Author Dr. Beate Müller Dr. Birgit Eschweiler Dr. Klaus Hechenbichler
Document Status Final
Date of last version of the study report
04 DEC 2013
EU PAS register number
Study not registered
Property of Novartis Confidential
May not be used, divulged, published or otherwise disclosed without the consent of Novartis

Novartis Confidential Page 2 Non-interventional study report Study No. CENA713DDE23
Table of contents
1 Abstract .............................................................................................................................................. 7
2 Marketing Authorization Holder ...................................................................................................... 11
3 Investigators ..................................................................................................................................... 12
4 Ethics ................................................................................................................................................ 14
4.1 Independent ethics committee or institutional review board ............................................... 14
4.2 Patient information and consent ........................................................................................... 14
4.3 Legal and regulatory basis of the study ................................................................................ 14
5 Rationale and background ................................................................................................................ 15
6 Research question and objectives .................................................................................................... 16
7 Observational plan ........................................................................................................................... 17
7.1 Amendments and updates to the protocol ............................................................................ 17
8 Research methods ............................................................................................................................ 18
8.1 Study design ......................................................................................................................... 18
8.2 Subjects ................................................................................................................................ 18
8.3 Variables .............................................................................................................................. 19
8.4 Data sources and measurement ............................................................................................ 20
8.5 Study size ............................................................................................................................. 21
8.6 Data quality assurance .......................................................................................................... 21
8.6.1 Monitoring ........................................................................................................... 21
8.6.2 Quality control ..................................................................................................... 21
8.7 Statistical methods ............................................................................................................... 21
9 Results .............................................................................................................................................. 22
9.1 Participants ........................................................................................................................... 22
9.2 Baseline data (retrospective and 3 months after treatment initiation) .................................. 23
9.2.1 Information about patients (by caregivers and physicians) ................................. 23
9.2.2 Information about caregiver (by caregivers and physicians) ............................... 27
9.2.3 Information about patch (caregiver questionnaire) ............................................. 28
9.3 Descriptive data over time (by caregiver, 3 and 6 months) ................................................. 29
9.3.1 Application of patch and patient’s compliance ................................................... 29
9.3.2 Problems of caregiver within last 2 weeks .......................................................... 30
9.3.3 Opinion on AD .................................................................................................... 31
9.3.4 Usage of Exelon® patch ....................................................................................... 32
9.3.5 Opinion on Exelon®
patch ................................................................................... 33
9.3.6 Compliance .......................................................................................................... 35
9.3.7 Satisfaction with efficacy .................................................................................... 36

Novartis Confidential Page 3 Non-interventional study report Study No. CENA713DDE23
9.3.8 Application of the patch ...................................................................................... 37
9.4 Other analyses ...................................................................................................................... 38
9.5 Adverse events ..................................................................................................................... 38
9.5.1 Satisfaction of caregiver with tolerability ........................................................... 40
10 Discussion ........................................................................................................................................ 41
10.1 Key results ............................................................................................................................ 41
10.2 Safety conclusions ................................................................................................................ 43
11 References ........................................................................................................................................ 44
12 Appendix .......................................................................................................................................... 45
12.1 Sample study protocol including data entry forms .............................................................. 45
12.2 Table set ............................................................................................................................... 45
12.3 Signatures ............................................................................................................................. 45
Novartis Confidential Page 4 Non-interventional study report Study No. CENA713DDE23
List of tables
Table 8-1 Schedule of the STATT study ............................................................................................. 18
Table 9-1 Patient demographics and background characteristics (caregiver) ..................................... 23
Table 9-2 Clinical background (physician, retrospective information from patient’s files and
current information) ............................................................................................................ 24
Table 9-3 Prescribed patch, concomitant diseases and medication (physician, retrospective
information from patient’s files) ......................................................................................... 25
Table 9-4 Patient’s view about the disease and medication (caregiver questionnaire) ....................... 26
Table 9-5 Demographic data and medical condition of caregiver (caregiver questionnaire,
baseline visit) ...................................................................................................................... 27
Table 9-6 Caregivers physical ability to take care for the patient (physician, retrospective
information from patient’s files) ......................................................................................... 28
Table 9-7 Information on patch (caregiver questionnaire, baseline visit) ........................................... 28
Table 9-8 Extent of help with application of patch and patient’s compliance/adherence 3 and 6
months after treatment initiation (caregiver questionnaires) .............................................. 29
Table 9-9 Psychological problems caregivers experienced within 2 weeks before visits (caregiver
questionnaires, 3 and 6 months after treatment initiation) .................................................. 30
Table 9-10 Opinion on AD (3 months after treatment initiation, caregiver questionnaire) .................. 31
Table 9-11 Opinion on AD (6 months after treatment initiation, caregiver questionnaire) .................. 31
Table 9-12 Opinion about factors being the cause of AD (3 months after treatment initiation,
caregiver questionnaire) ...................................................................................................... 32
Table 9-13 Opinion about factors being the cause of AD (6 months after treatment initiation,
caregiver questionnaire) ...................................................................................................... 32
Table 9-14 Opinion on Exelon® patch (3 months after treatment initiation, caregiver questionnaire) . 33
Table 9-15 Opinion on Exelon® patch (6 months after treatment initiation, caregiver questionnaire) . 34
Table 9-16 Compliance with usage instructions (3 months after treatment initiation, caregiver
questionnaire) ...................................................................................................................... 35
Table 9-17 Compliance with usage instructions (6 months after treatment initiation, caregiver
questionnaire) ...................................................................................................................... 36
Table 9-18 Satisfaction with efficacy (3 months after treatment initiation, caregiver questionnaire) .. 36
Table 9-19 Satisfaction with efficacy (6 months after treatment initiation, caregiver questionnaire) .. 37
Table 9-20 Application of the patch (3 months after treatment initiation, caregiver questionnaire) .... 37
Table 9-21 Application of the patch (6 months after treatment initiation, caregiver questionnaire) .... 38
Table 9-22 Adverse events (patient based) ........................................................................................... 38
Table 9-23 Event-based classification of non-serious adverse drug reactions (nsADR) ...................... 39
Table 9-24 Event-based classification of serious adverse events not related (SAEnr) ......................... 39
Table 9-25 Event-based classification of serious adverse drug reactions (SADR) ............................... 40
Novartis Confidential Page 5 Non-interventional study report Study No. CENA713DDE23
List of abbreviations
AD Alzheimer’s disease
ADR adverse drug reaction
AE adverse event
AMG Arzneimittelgesetz (German Drug Law)
BAnz Bundesanzeiger (Federal Gazette)
BfArM Bundesinstitut für Arzneimittel und Medizinprodukte (Federal Institute for Drugs and
Medical Devices)
BIPQ Brief Illness Perception Questionnaire
BMQ Beliefs about Medication Questionnaire
CFR Code of Federal Regulations
CGI Clinical Global Impression
ChEI Cholinesterase-Inhibitor
CRA Clinical Research Associate
CRO Clinical Research Organisation
DMP Data Management Plan
EC European Commission
FDA Food and Drug Administration
FSA Freiwillige Selbstkontrolle für die Arzneimittelindustrie (Voluntary Self-
regulation for the Pharmaceutical Industry)
GAD Generalized Anxiety Disorder
GOÄ Gebührenordnung für Ärzte (German scale of fees for physicians)
MARS Medication Adherence Report Scale
MBOÄ Musterberufsordnung für Ärzte (Professional code of conduct)
MedDRA Medical Dictionary for Regulatory Activities
MMSE Mini–mental state examination
NICE The National Institute for Health and Clinical Excellence
NIS Non-interventional study
nsADR Non-serious adverse drug reaction
nsAEnr Non-serious adverse event not related
PEI Paul Ehrlich Institute
PHQ Patient Health Questionnaire
PT Preferred Term (MedDRA)
Novartis Confidential Page 6 Non-interventional study report Study No. CENA713DDE23
SADR Serious adverse drug reaction
SAE Serious adverse event
SAEnr Serious adverse event not related
SAP Statistical Analysis Plan
SDV Source Document Verification
SIMS Satisfaction with Information about Medicines Scale
SOC System Organ Class (MedDRA)
SOP Standard Operating Procedure
VFA Verband Forschender Arzneimittelhersteller (Association of Researching
Pharmaceutical Manufacturers)

Novartis Confidential Page 7 Non-interventional study report Study No. CENA713DDE23
1 Abstract
Title STATT – A non-interventional study to investigate factors associated with
adherence to Exelon® patch for the treatment of Alzheimer’s disease
Keywords Acetylcholinesterase inhibitors, adherence, Alzheimer’s disease, caregiver
satisfaction, rivastigmine patch, tolerability
Rationale and
background
Cholinesterase inhibitors (ChEIs) are a first-line treatment for mild-to-
moderate Alzheimer’s disease (AD). However, as in many therapeutic areas,
treatment adherence and persistence are often poor; this may be intentional or
unintentional and influenced by the ability of the patient to self-medicate,
caregiver perceptions of AD and the opinions of physicians.
Research question
and objectives
The primary objective of this study was to identify patient- and caregiver-
related sociodemographic, clinical and psychological factors associated with
adherence to rivastigmine patch.
Secondary outcomes were to identify patient- and caregiver-related factors
associated with persistence to patch therapy and caregiver satisfaction with
rivastigmine patch.
For safety evaluation, the treatment tolerability in clinical practice was
assessed by reporting of adverse events in the observation period.
No hypotheses were pre-specified, i.e. the study was of pure explorative
nature.
Study design Non-interventional study according to regulatory and legal requirements of
patients with mild-to-moderate AD, who were receiving rivastigmine patch.
Retrospective patient socio-demographic, clinical and psychosocial data at
the time of first prescription were reported by the physician 3 months after
treatment initiation. Caregivers provided cross-sectional information on
patients 3 months after treatment initiation. The completion visit was
performed 3 months later (i.e. 6 months after treatment initiation).
Setting Patients with mild-to-moderate AD, who were prescribed rivastigmine patch
by a participating physician.
Further inclusion criteria: written informed consent by the patients or by a
legally acceptable representative of the patient.
No further inclusion or exclusion criteria were specified. Patients with
contra-indications for treatment with rivastigmine as stated in the Summary
of Product Characteristics were not to be enrolled.
Subjects and study
size, including
dropouts
140-150 patients (or caregivers and corresponding physicians) were planned
to be enrolled, whereas data from 127 caregivers (reporting about 127
patients) and 18 physicians (documenting 129 patients) at baseline (3 months
after treatment initiation) and from 110 caregivers at completion visit (6
months after treatment initiation) were collected.

Novartis Confidential Page 8 Non-interventional study report Study No. CENA713DDE23
Variables and data
sources
Caregivers were asked to provide information about the patient, as well as on
their own age, physical health, mood, treatment- and disease-related beliefs
and expectations, and satisfaction with patch 3 months and 6 months post
treatment initiation.
Physicians were asked to provide retrospective information on socio-
demographic and clinical data about the patient who had been described with
Exelon® patch (from patient’s files), as well as current information (CGI,
adverse events) about the patient and patch usage 3 months post-treatment
initiation.
Results Baseline information: 50.4% of the patients with AD were female (n=64)
and the mean age was 78.2 years at the time of data recording.
Physicians’ information: majority of the patients presented with mild
(24.8%), mild to moderate (38.8%), or moderate (23.3%) AD at the time of
treatment initiation and the mean ± SD MMSE-score was 20.8 ± 3.3 points
(out of 30), corresponding to mild dementia. Three months after treatment
initiation, most physicians estimated that the CGI would be much improved
(35.7%) or a little improved (30.2%). No change was seen by 21.7% of
physicians and 7.8% physicians saw a deterioration of the AD.
High dose Exelon® patch (9.5 mg/ 24 h) was prescribed in 53.5% (n=69) and
the low dose patch in 42.6% (n=55) of patients by the physicians. Both doses
were prescribed for 5 patients (3.9%) within the 3 months since treatment
start.
Patient’s opinion: Most patients thought, that their AD was caused by their
age (76.4%, n=97). Second most common causes were thought to be genetic
endowments (26.0%, n=33) or other (26.0%, n=33). Patch application were
more favored than other types of medications (pills or liquids). Most patients
(63.0%, n=80) preferred or highly preferred patches as type of medication.
Information about caregiver: Most of the caregivers (70.9%) were female
and had a mean age of 66.4 ± 13.9 years. The majority (75.6%) never cared
for relatives before and more than half of the caregivers saw the patient most
of the time daily (59.1%). At the time of treatment initiation, the patient was
supervised by the spouse (57.4%, n=74/129), the daughter (21.7%,
n=28/129), a paid caregiver (5.4%, n=7/129), another person (3.1%,
n=4/129), or the son (3.1%, n=4/129); 8.5% of patients were supervised by
more than one person (e.g. spouse and daughter). At the time of first
treatment initiation, the ability of the caregiver to take care for the patient
was not at all restricted in 62.8% and little restricted in 17.8% of caregivers
(physician’s information).
Caregiver information over time (3 and 6 months): Most caregivers had
full responsibility (34.6%) or had to help a lot (33.9%) with the application
of the patch at baseline and no relevant changes in the extent of help was
seen 3 months later. At baseline, most of the patients were compliant with the
Exelon® patch, i.e. mostly (44.1%) or always (33.1%) supported their
caregivers when fixing the patch. In addition, the majority of the patients

Novartis Confidential Page 9 Non-interventional study report Study No. CENA713DDE23
adhered to the medication and always (55.9%) or mostly (26.8%) kept the
patch as long as necessary. Compliance and adherence data were comparable
6 months after treatment start.
Most of the caregivers had no psychological problems at all (about 57% to
63% in the four domains) or only on several days (about 20% to 24%) at
baseline. This proportion of caregivers without any significant problems
remained largely unchanged up to the completion visit.
At the first documentation, the mean score values of the “Opinion on AD”
questionnaire mostly were in the middle range of the scale (around 4.1 to
6.9), showing that patients but also caregivers were distinctly affected by the
AD, although none of the mean scores achieved extreme values. Only the
question on the duration of the disease showed that caregivers were aware of
the very long duration (mean score 8.5). At the final documentation, mean
score values were almost the same as after 3 months.
Both at 3 and 6 months after treatment start, the factors age, other factors and
genetics were ticked most often by the caregivers and thought to be the most
important factors for causing AD.
The proportion of patients who were still using the patch after treatment
initiation was 88.2% (n=112/127) at first visit (missing 7.9%) and also 88.2%
(n=97/110) at final visit (missing 4.5%). Only 5 patients (3.9%) discontinued
the Exelon® patch before baseline visit and further 5 patients (4.5%) before
final visit.
More than half of the caregivers agreed (agreed or completely agreed) with
the statements that “health would depend on the patch” (54.3%) and that the
“patch would protect the patients from feeling worse” (73.2%). Most
caregivers disagreed (disagreed or disagreed at all) with the following
statements: “worry about usage of patch” (73.2%), “patch disturbs life”
(70.9%), “concerns about addiction” (61.4%), “patch is a mystery” (52.8%),
“could not live without patch” (48.0%), and “thoughts about long-term
effects of the patch” (42.5%). At the final documentation, the level of
acceptance to the statements that caregivers had agreed with 3 months earlier
has increased slightly. Also the level of rejection with those statements
previously disagreed has increased slightly. Only with the statements “could
not live without patch” (disagreed 45.5%, 39.1% did not know) and “patient
would be very ill without the patch” (agreed 43.6%, 34.5% did not know) the
level of agreement has decreased and more caregivers ticked the “I don’t
know” boxes.
At both visits, both the caregivers and the patients were highly compliant. At
the first documentation time, most caregivers stated that she/he had never
“omitted that patch sometimes” (74.8%), “interrupted the patch for a while”
(73.2%), or “changed the fixing patch time” (64.6%). At the final
documentation time (6 months after treatment initiation), the proportion of
caregivers who have never forgotten to fix or remove the patch or who have
changed patch usage has slightly increased compared to the first
documentation. Within the last 2 weeks before the first/final documentation,
Novartis Confidential Page 10 Non-interventional study report Study No. CENA713DDE23
69.3%/70.0% of caregivers stated that there was no day of irregular use of
patch.
At the final visit, the level of satisfaction with the efficacy has increased
compared to the first documentation, with 16.4% of caregivers being very
satisfied and 64.5% satisfied with the effect on behavior and emotions,
15.5% very satisfied and 66.4% satisfied with effect on activities, and 11.8%
being very satisfied and 56.4% satisfied with the effect on memory. The
proportion of caregivers being unsatisfied has decreased compared to the first
documentation.
More than 85% of caregivers found that opening of the package, make the
patient to use it, fixing and removing of patch was easy or very easy at both
documentation timepoints.
Safety: In the observation period, 16 adverse events which occurred in 9
patients were reported. Of these, one event was considered to be a serious
adverse event not related, and another event was considered to be a serious
adverse drug reaction. This patient died during the observation period. 14
adverse events in 8 patients were reported to be related to Exelon® patch
treatment, but not serious.
Conclusions In conclusion, most caregivers and their patients adhered to the treatment
with rivastigmine (Exelon® patch) during the 6 months observation period.
The application of the patch was considered by the caregivers as easy to use,
efficacious and satisfying for both the patient and the caregiver.
Rivastigmine (Exelon® patch) proved to be a well-tolerated drug for the
treatment of patients with Alzheimer’s disease, as demonstrated by the low
incidence rate of adverse events. The nature and frequency of adverse events
occurring during the 6 months therapy were consistent with the established
safety profile of rivastigmine. The current NIS did not reveal any suspicion
of unknown risks related to the treatment with rivastigmine.
Marketing
Authorization
Holder
Novartis Pharma AG, Basel, Switzerland
Name(s) and
Affiliation(s) of
Principal
Investigator(s)
Professor Dr. med. Matthias Riepe, Ludwig Heilmeyer Straße 2, D-89312
Günzburg, Germany

Novartis Confidential Page 11 Non-interventional study report Study No. CENA713DDE23
2 Marketing Authorization Holder
Novartis Pharma AG, WSJ-790.1., CH-4002 Basel, Switzerland

Novartis Confidential Page 12 Non-interventional study report Study No. CENA713DDE23
3 Investigators
The co-ordinating investigator ("Leiter der klinischen Prüfung" [LKP] according to German Drug Law)
was:
Professor Dr. med Matthias Riepe
Ludwig Heilmeyer Straße 2
D-89312 Günzburg, Germany
Telefon: +49 8221 96-2355
A total of 18 active (by screening) study sites in Germany participated in this study. A list of the site
investigators is available by request.
The project manager was:
Dr. Beate Müller
Roonstraße 25
D-90429 Nuremberg. Germany
Phone: +49 911 273 12-046
Fax: +49 911 273 15-046
Email: [email protected]
and the Phase IV Manager NIS:
Dr. Alfons Müller
Roonstraße 25
D-90429 Nuremberg, Germany
Phone: +49 911 273 12-897
Fax: +49 911 273 15-897
Email: [email protected]
Novartis Confidential Page 13 Non-interventional study report Study No. CENA713DDE23
and the Safety Manager:
Dr. Katharina Salb
Roonstraße 25
D-90429 Nuremberg, Germany
Phone : +49 911 273 13-271
Fax : +49 911 273 12-985
Email: [email protected]
Project Implementation and Statistical Analysis was performed by:
Institut Dr. Schauerte
Kolpingring 18
D-82041 Oberhaching, Germany
Telefon: +49 89 641 804-0
Fax: +49 89 641 52 72
EMail: [email protected]

Novartis Confidential Page 14 Non-interventional study report Study No. CENA713DDE23
4 Ethics
4.1 Independent ethics committee or institutional review board
According to the joint publication of the Federal Institute for Drugs and Medical Devices (BfArM) and
the Paul Ehrlich Institute (PEI) as well as the recommendations of the VFA to improve quality and
transparency of non-interventional studies, a properly constituted Independent Ethics Committee
(Ethics Committee University Ulm) was consulted before study start.
4.2 Patient information and consent
Patients had to be provided with written information about aims and type of the study and amount of
documentation before inclusion into the study. As this was a post-marketing observational study, a
special information that exceeds the scope of the product of summary characteristics, was not necessary
in this NIS.
Eligible patients were only enrolled into the study after providing written informed consent for the
documentation of data within the NIS as well as for inspection of the patients’ medical files, or after
such consent had been provided by a legally acceptable representative of the patient. In cases where the
patient's representative gave consent, the patient had to be informed about the study to the extent
possible, given his/her understanding. The confidential nature of any patient information recorded was
maintained according to the EU Directive 95/46/EC and the national data protection law.
4.3 Legal and regulatory basis of the study
This NIS is based on Novartis internal SOPs, which are based on the following recommendations and
guidelines:
German Drug Law (§ 4 paragraph 23, third sentence (AMG))
§ 67 paragraph 6 of the German drug law (AMG)
§ 63 b of the German Drug law (AMG)
Directive 2001/83/EC of the European Parliament and of the Council
Pharmacovigilance Guidelines of Volume 9A of ‘The Rules Governing Medicinal Products in
the EU’
Recommendations of the Federal Institute for Drugs and Medical Devices (BfArM) and the
Paul-Ehrlich-Institute (PEI) on the planning, implementation and evaluation of observational
studies of 7 July 2010 (in German)
Recommendations of the Association of Research-Based Pharmaceutical Companies (VFA) to
improve further the quality and transparency of non-interventional studies of 31.01.2007 and
23.04.2007
FSA-Codex for the cooperation with specialists –Federal Gazette of 07.05.2008

Novartis Confidential Page 15 Non-interventional study report Study No. CENA713DDE23
5 Rationale and background
Cholinesterase inhibitors (ChEIs) are a first-line treatment for mild to moderate Alzheimer’s disease
(AD). However, as in many therapeutic areas, treatment adherence and persistence are often poor; this
may be intentional or unintentional and influenced by the ability of the patient to self-medicate,
caregiver perceptions of AD and the opinions of physicians.
Hence, the aim of the observational study was to evaluate factors that would help physicians to identify
those patients that might benefit from transdermal patch treatment and who are likely to adhere to the
treatment over an extended period.

Novartis Confidential Page 16 Non-interventional study report Study No. CENA713DDE23
6 Research question and objectives
The primary objective of this study was to identify patient- and caregiver-related sociodemographic,
clinical and psychological factors, associated with adherence to rivastigmine patch.
Secondary outcomes were to identify patient- and caregiver-related factors associated with persistence
to patch therapy and caregiver satisfaction with rivastigmine patch.
For safety evaluation, the treatment tolerability in clinical practice was assessed by reporting of adverse
events in the observation period and analyzed descriptively.
No hypotheses were pre-specified, i.e. the study was of pure explorative nature.
Novartis Confidential Page 17 Non-interventional study report Study No. CENA713DDE23
7 Observational plan
The study was conducted according to the original protocol, dated September 2011 (Code: 2011/31 30
57), which can be found in Section 12. Also, the sample blank CRF can be found in Section 12. The
statistical analyses performed for this study are defined in the statistical analysis plan (SAP) (see
Section 8.7).
7.1 Amendments and updates to the protocol
N/A

Novartis Confidential Page 18 Non-interventional study report Study No. CENA713DDE23
8 Research methods
8.1 Study design
This was a non-interventional study according to regulatory and legal requirements (see Section 4.3) of
patients with mild-to-moderate AD, who were receiving rivastigmine patch.
Retrospective patient socio-demographic, clinical and psychosocial data at the time of first prescription
were reported by the physician 3 months after treatment initiation: caregivers will provide cross-
sectional information on patients 3 months after treatment initiation. The completion visit was
performed 3 months later (i.e. 6 months after treatment initiation).
Table 8-1 Schedule of the STATT study
Date of contact Baseline Visit 1
(3 months after
treatment initiation)
Completion Visit
(6 months after
treatment initiation)
Inclusion/exclusion criteria x
Informed consent x
Baseline data (demographic data,
patch information, concomitant
diseases) x
Clinical data x x
Patient assessment by physician x x
Caregiver information about
patient x
Information about caregiver x x
Caregiver Satisfaction (AD
caregiver preference
questionnaire) x x
Adherence of patient (adherence
report scale) x x
Persistence of patient (persistence
scale) x x
Adverse events x x
8.2 Subjects
The study population consisted of patients with mild-to-moderate AD, who were prescribed with
rivastigmine patch by a participating physician.
Further inclusion criteria: written informed consent by the patients or by a legally acceptable
representative of the patient.
No further inclusion or exclusion criteria were specified. Patients with contra-indications for treatment
with rivastigmine as stated in the Summary of Product Characteristics were not to be enrolled.

Novartis Confidential Page 19 Non-interventional study report Study No. CENA713DDE23
The decision to include a patient into the study had to be taken after the decision on the treatment and
the prescription of the patch and had to be independent of treatment decisions.
8.3 Variables
The following baseline information was collected at visit 1 (3 months after treatment initiation):
Caregiver questionnaire:
Information about patient (sex, school attendance, age, smoking behavior, concomitant
diseases, cause of AD (patients’ view), preferred medication, extent of help with application of
patch, compliance)
Information about caregiver (sex, age, concomitant diseases, problems in the last 2 years,
frequency of patient contact, previous caregiver experience)
Opinion on AD (several aspects of AD, each rated on a 0 (no influence) to 10 (strongly
impacted) scale, quantitative analysis)
About Exelon® patch (usage, opinion on patch, compliance, number of days with irregular use,
satisfaction with efficacy, tolerability, application of patch, information on patch)
Physician questionnaire:
Retrospective information (prescribed patch, socio-demographic and clinical data about AD,
MMSE score, caregiver, drawback of caregiver’s physical ability to take care for patient,
patient’s behavior drawback for using patch)
Current information (Clinical Global Impression - CGI-score, listing of prescribed patches
including package sizes and dose)
Adverse events
The Mini-Mental State Examination (MMSE) is a brief 30-point questionnaire test that is used to
screen for cognitive impairment. Any score greater than or equal to 27 points (out of 30) indicates
normal cognition. Below this, scores can indicate severe (≤9 points), moderate (10-18 points) or mild
(19-24 points) dementia [Folstein et al 1975].
The following information was collected at visit 2 (6 months after treatment initiation):
Caregiver questionnaire:
Information about patient (extent of help with application of patch, compliance)
Information about caregiver (problems in the last 2 weeks)
Opinion on AD (quantitative analysis)
About Exelon® patch (as in visit 1)
Primary outcomes assessed compliance, persistence (self-reported (2-item measure) and physicians’
prescription data) and caregiver’s opinion and satisfaction with the Exelon® patch (self-reported;
shortened adaptation of AD Caregiver Preference Questionnaire) 3 and 6 months after the start of
treatment.

Novartis Confidential Page 20 Non-interventional study report Study No. CENA713DDE23
8.4 Data sources and measurement
Caregiver data (socio-demographic information about patient, patients’ view, experience with Exelon®
patch, information about caregiver, caregiver satisfaction) were gained from self-reported
questionnaires to be completed 3 and 6 months after treatment initiation.
Retrospective data (physician questionnaire) were obtained from the patient’s file and were transferred
at the baseline visit into the physician questionnaire. All current information was recorded directly in
the data capture form.
Safety related measurements
Adverse events that first occurred or worsened after start of study treatment had to be documented by
the physicians. Severity, outcome, and relatedness of these adverse events were listed.
Adverse events (AE) were defined as any untoward medical occurrence associated with the use of a
drug in a patient, whether or not considered to be drug related.
All adverse events had to be documented according to event type, first occurrence, duration and
severity in the enclosed CRF. In addition, it had to be documented whether the AE is considered to be
related to a drug, and if so, to which drug. The action taken due to the adverse event as well as the
event outcome also had to be documented.
Generally, a distinction is made between non-serious and serious adverse events, which have to be
reported to the Novartis Pharmacovigilance department within 24 hours of awareness. A serious
adverse event is any events which:
results in death
is life-threatening
requires inpatient hospitalization or prolongation of existing hospitalization
results in persistent or significant disability or incapacity
leads to a congenital anomaly or birth defect
is medically significant (i.e. an important medical event which significantly affects the patient,
but does not meet any of the above criteria)
Overall, adverse events are distinguished into four types based on the distinction serious/non-serious
and the causal relationship to Exelon®:
nsAEnr: non-serious adverse events not related
nsADR: non-serious adverse drug reactions (causality assured, probable, possible or not
assessable)
SAEnr: serious adverse events not related
SADR: serious adverse drug reaction (causality assured, probable, possible or not assessable)
In order to ensure the safety of every patient treated with Exelon®, every pregnancy had to be reported
to the Novartis Pharmacovigilance department within 24 hours of awareness. The pregnancy had to be
documented on a separate pregnancy form (Post Marketing Surveilance Pregnany Form) in English
language and had to be reported by the treating physician directly to the Pharmacovigilance of Novartis
Pharma GmbH.

Novartis Confidential Page 21 Non-interventional study report Study No. CENA713DDE23
8.5 Study size
Sample size calculation and power calculation was based on the primary outcome of adherence
according to self-reported data to be assessed by means of the Medication Adherence Report Scale
(MARS) score 3 months after treatment initiation. Details can be found in the original study protocol.
Based on these calculations, a sample size of at least 120 patients was calculated. A sample size of 140-
150 patients was required to compensate for drop-outs.
8.6 Data quality assurance
8.6.1 Monitoring
Source Data Verification was performed to check if all information on the CRFs was consistent with
and traceable to these source documents. Full verification of the following was required: presence of
informed consent, adherence to the inclusion/exclusion criteria, demographic data, documentation of
SAEs, concomitant diseases, concomitant medication, and the recording of data required for the
analyses of all primary and safety variables.
8.6.2 Quality control
All quality assurance procedures within the scope of the quality management system were stated in the
study specific Data Management Plan (DPM) and for each stage of the procedure specified:
Review of the CRFs for completeness and accuracy before data recording
Plausibility checks within the score of data recording
Data query form including a catalog of questions leading to queries at the study site
Implementation of an audit trail according to FDA CFR21 Part 11 Standard
Matching of CRF and database within the scope of a database audit
Protection of data integrity by documented database closing
Data Handling Report for the management of data inconsistencies relevant for data analysis that
persist after database closing. The Data Handling Report is integral part of the SAP.
The contracted CRO’s SOPs are the basis of all data management procedures.
8.7 Statistical methods
All analyses were performed by the designated CRO Institute Dr. Schauerte, Germany.
All documented data in this NIS were analyzed and reported by adequate statistical methods. No
hypotheses were pre-specified, i.e. the study was of pure explorative nature. The planned statistical
evaluation is provided in the SAP. However, due to the exploited timelines of this study and the lower
number of patients that could be included, the originally planned analysis was not performed.
All data were analyzed by descriptive statistics. Data were summarized with respect to demographic
and baseline characteristics, observations at the two visits (caregiver’s experience, opinion and
satisfaction), and safety observations and measurements. Categorical variables were summarized by
absolute and relative frequencies. Continuous variables were summarized by descriptive statistics of
the number of valid and missing observations, mean, standard deviation, minimum, median, and
maximum.
Novartis Confidential Page 22 Non-interventional study report Study No. CENA713DDE23
9 Results
9.1 Participants
The study started in October 2011. Data collection started for the first participant in January 2012. The
last participant completed the study in February 2013. Further details on administrational data can be
found in Section 12.
A total of 127 caregivers (reporting about 127 patients) and a total of 18 physicians (documenting 129
patients) in Germany completed the respective questionnaires at the baseline visit (3 months after
initiation of Exelon® patch). In addition, 110 caregiver questionnaires were completed at the
completion visit (6 months after treatment start). Thus, three different populations can be analyzed,
based on completed caregiver questionnaires at 3 months (N = 127), completed caregiver
questionnaires at 6 months (N = 110), and completed physician questionnaires at 3 months (N = 129).

Novartis Confidential Page 23 Non-interventional study report Study No. CENA713DDE23
9.2 Baseline data (retrospective and 3 months after treatment initiation)
At baseline visit, data about the patient, the disease and experience with the Exelon® patch made within
the previous 3 months was gained both from caregivers and treating physicians.
9.2.1 Information about patients (by caregivers and physicians)
Socio-demographic data and clinical background from the patient are summarized in Table 9-1 and
Table 9-2.
Table 9-1 Patient demographics and background characteristics (caregiver)
Variable N
missing Total (N=127)
Sex, n (%) 5 male 58 (45.7)
female 64 (50.4)
Age, years 9 mean (SD) 78.2 (6.8)
median (min, max) 78.5 (56-101)
School attendance, n (%) 8 not specified 37 (29.1)
6-7 years 5 (3.9)
8 years 50 (39.4)
9 years 4 (3.1)
10 years 14 (11.0)
> 10 years 9 (7.1)
Smoking, n (%) 6 Yes 9 (7.1)
No 112 (88.2)
Concomitant diseases, n (%)* 0 diabetes 36 (28.3)
anxiety disorder 8 (6.3)
cancer 18 (14.2)
heart disease 42 (33.1)
AD = Alzheimer’s disease, SD = standard deviation; *multiple responses possible out of pre-defined answers,
Source: Table Set Section 1.1, Table 1.1 to 1.5
According to caregiver’s information, half of the patients (50.4%) with AD were female (n=64) and the
mean age was 78.2 years at the time of data recording. Most patients attended school for 8 years or 10
years; no information about time of school attendance was provided for about one third (29.1%, n=37)
of patients.
The majority of patients were non-smokers (88.2%, n=112). Heart disease (33.1%, n=42) and diabetes
(28.3%, n=36) were marked most often from the four pre-defined concomitant diseases.
Demographic and clinical data were also documented by physicians, who took the information from the
patient’s files retrospectively (see Table Table 9-2).

Novartis Confidential Page 24 Non-interventional study report Study No. CENA713DDE23
Table 9-2 Clinical background (physician, retrospective information from patient’s files and current information)
Variable N missing /
not assessed Total (N=129)
Retrospective information (at the time of treatment initiation)
Age, years 0 mean (SD) 77.6 (6.6)
median (min, max) 78 (56-101)
Weight, kg 15 mean (SD) 73.2 (11.9)
median (min, max) 75 (42-99)
Severity of AD 1 beginning mild 14 (10.9)
mild 32 (24.8)
mild to moderate 50 (38.8)
moderate 30 (23.3)
ending moderate 2 (1.6)
MMSE score 60 mean (SD) 20.8 (3.3)
median (min, max) 21 (12-27)
Living 0 at home with caregiver 94 (72.9)
at home alone 21 (16.3)
nursing home 13 (10.1)
somewhere else 1 (0.8)
Current information (3 months after treatment initiation)
Estimated CGI score 5 very much improved 1 (0.8)
much improved 46 (35.7)
a little improved 39 (30.2)
no change 28 (21.7)
a little worse 9 (7.0)
much worse 1 (0.8)
AD = Alzheimer’s disease, CGI = clinical global impression, MMSE = Mini–mental state examination, SD = standard
deviation
Source: Table Set Section 3.1, Table 3.2 to 3.5, 3.8, Section 3.2, Table 3.12
According to the physicians’ information (from patients’ files), the majority of patients presented with
mild (24.8%), mild to moderate (38.8%), or moderate (23.3%) AD at the time of treatment initiation
and the mean ± SD MMSE-score was 20.8 ± 3.3 points (out of 30), corresponding to mild dementia.
Three months after treatment initiation (current information at first study visit), most physicians
estimated that the CGI would be much improved (35.7%) or a little improved (30.2%). No change was
seen by 21.7% of physicians and 10 physicians saw a deterioration of the AD.
Information about prescribed drug, concomitant diseases and other concomitant medications at the time
of treatment initiation is given in Table 9-3.

Novartis Confidential Page 25 Non-interventional study report Study No. CENA713DDE23
Table 9-3 Prescribed patch, concomitant diseases and medication (physician, retrospective information from patient’s files)
Variable N missing Total (N=129)
Retrospective information (at the time of treatment initiation)
Prescribed patch, n (%) 0 4.6 mg/24 h 55 (42.6)
9.5 mg/24 h 69 (53.5)
both 5 (3.9)
Concomitant diseases*, n (%) 0 Hypertension 50 (38.8)
Heart disease 42 (32.6)
Diabetes 35 (27.1)
Clinical depression 20 (15.5)
Cancer 17 (13.2)
Gastrointestinal
disorders 9 (7.0)
Skin disease 8 (6.2)
Anxiety disorder 6 (4.7)
Arthritis 6 (4.7)
Dysphagia 2 (1.6)
Concomitant medication, number 4 mean (SD) 3.0 (2.3)
median (min, max) 3 (0-14)
AD = Alzheimer’s disease, h = hour, SD = standard deviation; *multiple responses possible out of pre-defined answers,
Source: Table Set Section 3.1, Table 3.1, 3.6 to 3.7
At the time of treatment initiation, the high dose Exelon® patch (9.5 mg/ 24 h) was prescribed in 53.5%
(n=69) and the low dose patch in 42.6% (n=55) of patients by the physicians. Both doses were
prescribed for 5 patients (3.9%) within the 3 months since treatment start..
Most often, patients suffered from concomitant hypertension (38.8%), heart disease (32.6%), diabetes
(27.1%) and clinical depression (15.5%). The mean number of concomitant medication was 3.0 ± 2.3 at
the time of treatment initiation.
At the first study visit, physicians had prescribed a total of 414 Exelon® packages. Most often
prescribed package sizes were N3 with 90 patches (46.9%, 194/414), N1 with 30 patches (22.2%,
92/414) and N2 with 60 patches (13.8%, 57/414). Residual packages (71/414) had other sizes. Most of
these were at a dose of 9.5 mg/24 h (53.6%, 222/414) and second most at a dose of 4.6 mg/24 h
(46.1%, 191/414). The dose was not specified in one case.
Patient’s view about the disease (multiple answers possible), and the compliance/adherence to the patch
were recorded by the caregiver 3 months after treatment initiation (see

Novartis Confidential Page 26 Non-interventional study report Study No. CENA713DDE23
Table 9-4).

Novartis Confidential Page 27 Non-interventional study report Study No. CENA713DDE23
Table 9-4 Patient’s view about the disease and medication (caregiver questionnaire)
Variable N
missing Total (N=127)
AD cause (patient’s view), n (%)* 0 age 97 (76.4)
genetic endowments 33 (26.0)
nutrition 12 (9.4)
infection/virus 5 (3.9)
other 33 (26.0)
Preferred medication (patients’ view)
Pills, n (%) 14 not preferred 19 (15.0)
little preferred 21 (16.5)
moderate 48 (37.8)
preferred 22 (17.3)
highly preferred 3 (2.4)
Liquids, n (%) 14 not preferred 16 (12.6)
little preferred 19 (15.0)
moderate 48 (37.8)
preferred 22 (17.3)
highly preferred 8 (6.3)
Patches, n (%) 9 not preferred 10 (7.9)
little preferred 10 (7.9)
moderate 18 (14.2)
preferred 47 (37.0)
highly preferred 33 (26.0)
AD = Alzheimer’s disease
Source: Table Set Section 1.1, Table 1.6 to 1.7
Most patients thought, that their AD was caused by their higher age (76.4%, n=97). Second most
common causes were thought to be genetic endowments (26.0%, n=33) or other (26.0%, n=33).
Patches were more favored than other types of medications (pills or liquids). Most patients preferred or
highly preferred patches as type of medication. Patches were not preferred by 7.9% of patients
(n=10/127). Pills and liquids were moderately preferred (both 37.8%) and preferred (both 17.3%) by
most patients.

Novartis Confidential Page 28 Non-interventional study report Study No. CENA713DDE23
9.2.2 Information about caregiver (by caregivers and physicians)
Information about the caregiver provided by the caregiver was also recorded, as summarized in Table
9-5.
Table 9-5 Demographic data and medical condition of caregiver (caregiver questionnaire, baseline visit)
Variable N missing Total (N=127)
Sex, n (%) 13 male 24 (18.9)
female 90 (70.9)
Age, years 10 mean (SD) 66.4 (13.9)
median (min, max) 70 (32, 90)
Concomitant diseases affecting...,
n (%)* 0 mobility 33 (26.0)
vision 21 (16.5)
strength / stamina 16 (12.6)
usage of hands 10 (7.9)
Did you care for relatives before?
n (%) 8 yes 23 (18.1)
no 96 (75.6)
How often do you see the patient?
n (%) 10 daily (most of the time) 75 (59.1)
daily (4-7 hours) 13 (10.2)
daily (1-3 hours) 21 (16.5)
1-2 times/week 8 (6.3)
AD = Alzheimer’s disease, SD = standard deviation; *multiple responses possible out of pre-defined answers,
Source: Table Set Section 1.2, Table 1.10 to 1.12 and 1.14 to 1.15.
Most of the caregivers (70.9%, n=90/127) were female and had a mean age of 66.4 ± 13.9 years. When
asked for concomitant diseases, those affecting mobility (26.0%) and vision (16.5%) were recorded
most often by the caregivers, corresponding to their higher age. The majority (75.6%) never cared for
relatives before and more than half of the caregivers see the patient most of the time daily (59.1%).
Information about the caregiver was also provided by the physician at baseline.
At the time of treatment initiation, the patient was supervised by the spouse (57.4%, n=74/129), the
daughter (21.7%, n=28/129), a paid caregiver (5.4%, n=7/129), another person (3.1%, n=4/129), or the
son (3.1%, n=4/129). A total of 11 patients (8.5%) were supervised by more than one person (e.g.
spouse and daughter) (Source: Table Set Section 3.1, Table 3.9).
Physicians were also asked to evaluate if there were any drawbacks of the caregiver’s physical ability
to take care for the patient (see Table 9-6).

Novartis Confidential Page 29 Non-interventional study report Study No. CENA713DDE23
Table 9-6 Caregivers physical ability to take care for the patient (physician, retrospective information from patient’s files)
Drawback of caregiver's physical ability N %
Total 129 100.0
Missing 4 3.1
Not at all 81 62.8
A little 23 17.8
Medium 12 9.3
Rather 7 5.4
Very much 2 1.6
Source: Table Set Section 3.1, Table 3.10.
At the time of first treatment initiation, the ability of the caregiver to take care for the patient was not at
all restricted in 62.8% and little restricted in 17.8% of caregivers.
The majority of patients (98.4%, n=127/129) did not show any behavior that would suggest a restricted
fixing, using or removing of the patch at the time of treatment initiation (Source: Table Set Section 3.1,
Table 3.11).
9.2.3 Information about patch (caregiver questionnaire)
Caregivers were asked to evaluate the information they received with the Exelon® patch (see Table
9-7).
Table 9-7 Information on patch (caregiver questionnaire, baseline visit, n=127)
Information on
patch Missing
Not
necessary Nothing
received Too little Too much Adequate
N % N % N % N % N % N %
Reason for
patch 9 7.1 1 0.8 2 1.6 7 5.5 2 1.6 106 83.5
When to use
patch 10 7.9 1 0.8 - - 7 5.5 4 3.1 105 82.7
When to fix
patch 9 7.1 2 1.6 3 2.4 12 9.4 5 3.9 96 75.6
How to change
side 11 8.7 2 1.6 2 1.6 12 9.4 7 5.5 93 73.2
How to remove
patch 10 7.9 4 3.1 1 0.8 6 4.7 7 5.5 99 78.0
What to do in
case of AEs 9 7.1 3 2.4 3 2.4 19 15.0 2 1.6 91 71.7
Source: Table Set Section 1.4, Table 1.25.

Novartis Confidential Page 30 Non-interventional study report Study No. CENA713DDE23
Most caregivers (>70%) assessed the amount of information as adequate in all aspects. A total of
15.0% (n=19/127) found there was too little information about what to do in case of AEs. In addition,
9.4% of caregivers found it was too little information about when to fix the patch and 9.4% about how
to change side.
9.3 Descriptive data over time (by caregiver, 3 and 6 months)
9.3.1 Application of patch and patient’s compliance
Problems with the application of the patch within the last 2 weeks before questionnaire completing and
compliance / adherence of the patient were assessed 3 and 6 months after treatment initiation (see Table
9-8).
Table 9-8 Extent of help with application of patch and patient’s compliance/adherence 3 and 6 months after treatment initiation (caregiver questionnaires)
Variable 3 months 6 months
N miss Total
(N=127) N miss Total
(N=110)
Extent of help with
application of Exelon®
patch, n (%) full responsibility 12 44 (34.6) 7 39 (35.5)
help a lot 43 (33.9) 40 (36.4)
help moderately 11 (8.7) 11 (10.0)
help only a little 17 (13.4) 13 (11.8)
Compliance, n (%)
patient supports
fixing of patch never 17 3 (2.4) 11 3 (2.7)
sometimes 9 (7.1) 5 (4.5)
mostly 56 (44.1) 43 (39.1)
always 42 (33.1) 48 (43.6)
Adherence, n (%)
patient keeps patch as
long as necessary never 15 0 9 1 (0.9)
sometimes 7 (5.5) 4 (3.6)
mostly 34 (26.8) 33 (30.0)
always 71 (55.9) 63 (57.3)
Source: Table Set Section 1.1, Table 1.8 to 1.9 and Section 2.1, Table 2.1 to 2.2.
Most caregivers had full responsibility (34.6%) or had to help a lot (33.9%) with the application of the
patch at baseline and no relevant changes in the extent of help was seen 3 months later (35.5% and
36.4%, respectively).
At baseline, most of the patients were compliant with the Exelon® patch, i.e. mostly (44.1%) or always
(33.1%) supported their caregivers when fixing the patch. In addition, the majority of the patients
adhered to the medication and always (55.9%) or mostly (26.8%) kept the patch as long as necessary.
Compliance and adherence data were comparable 6 months after treatment start.

Novartis Confidential Page 31 Non-interventional study report Study No. CENA713DDE23
9.3.2 Problems of caregiver within last 2 weeks
Caregivers were also asked about any psychological problems that they experienced within the last 2
weeks before questionnaire completing (see Table 9-9).
Table 9-9 Psychological problems caregivers experienced within 2 weeks before visits (caregiver questionnaires, 3 and 6 months after treatment initiation)
Variable 3 months 6 months
n (%) N miss Total
(N=127) N miss Total
(N=110)
No interest or joy in
doing something not at all 9 75 (59.1) 8 63 (57.3)
several days 29 (22.8) 27 (24.5)
more than half of the time 10 (7.9) 9 (8.2)
almost every day 4 (3.1) 3 (2.7)
Being depressed or
hopeless not at all 9 74 (58.3) 6 62 (56.4)
several days 30 (23.6) 25 (22.7)
more than half of the time 10 (7.9) 13 (11.8)
almost every day 4 (3.1) 4 (3.6)
Being nervous,
anxious or irritable not at all 9 79 (62.2) 6 63 (57.3)
several days 26 (20.5) 32 (29.1)
more than half of the time 10 (7.9) 6 (5.5)
almost every day 3 (2.4) 3 (2.7)
No stop or control of
sorrowful thoughts not at all 9 73 (57.5) 6 67 (60.9)
several days 30 (23.6) 22 (20.0)
more than half of the time 12 (9.4) 13 (11.8)
almost every day 3 (2.4) 2 (1.8)
Source: Table Set Section 1.1, Table 1.13 and Section 2.2, Table 2.3
Most of the caregivers had no psychological problems at all (about 57% to 63% in the four domains) or
only on several days (about 20% to 24%) at baseline. This proportion of patients without any
significant problems remained largely unchanged up to the completion visit. The proportion of
caregivers with problems more than half of the time or almost every day had slightly increased during
the further 3 months of observation, though the absolute numbers of caregivers were low. For example,
being depressed or hopeless for more than half of the day were 7.9% (n=10/127) at baseline and 11.8%
(n=13/110) after further 3 months.

Novartis Confidential Page 32 Non-interventional study report Study No. CENA713DDE23
9.3.3 Opinion on AD
The caregiver’s opinion and beliefs about AD and the extent to which the patient is impacted by the
disease, each rated on a 0 (no) to 10 (strong, very much) scale, were assessed at both visits (see Table
9-10 and Table 9-11).
Table 9-10 Opinion on AD (3 months after treatment initiation, caregiver questionnaire, n=127)
Question Non-missing Mean SD
How strong does AD impact life of your patient? 118 6.2 2.2
How long will the AD last? 117 8.5 2.3
How strongly can the patient control the AD? 116 4.1 2.8
To what extent can the medication help to manage the AD? 118 6.3 2.3
How much is the patient suffering from the AD? 115 5.5 1.9
How much are you concerned by the AD? 115 6.9 2.2
How much do you understand about the AD? 118 6.0 2.5
How much is the patient emotionally affected by the AD? 118 5.6 2.4
AD = Alzheimer’s disease, SD = standard deviation
Source: Table Set Section 1.3, Table 1.16
The mean score values of the “Opinion on AD” questionnaire mostly were in the middle range of the
scale (around 4.1 to 6.9), showing that patients but also caregivers were distinctly affected by the AD,
although none of the mean scores achieved extreme values. Only the question on the duration of the
disease showed that caregivers were aware of the very long duration (mean score 8.5).
Table 9-11 Opinion on AD (6 months after treatment initiation, caregiver questionnaire, n=110)
Question Non-missing Mean SD
How strong does AD impact life of your patient? 104 6.3 2.2
How long will the AD last? 104 8.4 2.4
How strongly can the patient control the AD? 104 4.3 2.6
To what extent can the medication help to manage the AD? 104 6.4 2.2
How much is the patient suffering from the AD? 103 5.5 2.0
How much are you concerned by the AD? 104 6.9 2.1
How much do you understand about the AD? 104 6.3 2.4
How much is the patient emotionally affected by the AD? 103 5.2 2.3
AD = Alzheimer’s disease, SD = standard deviation
Source: Table Set Section 2.3, Table 2.4
The mean score values of the “Opinion on AD” questionnaire also ranged in the middle of the scale
(4.3 to 6.9), except for the question on the duration of AD (8.4). Mean score values were almost the
same as after 3 months.

Novartis Confidential Page 33 Non-interventional study report Study No. CENA713DDE23
Furthermore, caregivers were asked to select the three most important factors from a given list that may
have caused the AD. This question was asked after 3 and after 6 months of treatment initiation (Table
9-12 and Table 9-13). Originally, caregivers were to rate the most important factors on a scale of 1 to 3
(1 being the most important factor). However, many caregivers just ticked some of the factors instead.
Table 9-12 Opinion about factors being the cause of AD (3 months after treatment initiation, caregiver questionnaire, n=127)
Most
important
factors
Not ticked Ticked 1 2 3
N % N % N % N % N %
Age 18 14.2 60 47.2 32 25.2 8 6.3 9 7.1
Genetics 58 45.7 30 23.6 11 8.7 22 17.3 4 3.1
Diet 114 89.8 3 2.4 2 1.6 2 1.6 1 0.8
Infection/virus 111 87.4 8 6.3 - - - - 5 3.9
Environment 84 66.1 18 14.2 2 1.6 7 5.5 12 9.4
Other 60 47.2 26 20.5 7 5.5 14 11.0 17 13.4
Source: Table Set Section 1.3, Table 1.16
Table 9-13 Opinion about factors being the cause of AD (6 months after treatment initiation, caregiver questionnaire, n=110)
Most
important
factors
Not ticked Ticked 1 2 3
N % N % N % N % N %
Age 13 11.8 59 53.6 24 21.8 10 9.1 4 3.6
Genetics 58 52.7 22 20.0 8 7.3 14 12.7 8 7.3
Diet 104 94.5 1 0.9 - - 3 2.7 - -
Infection/virus 95 86.4 8 7.3 1 0.9 3 2.7 1 0.9
Environment 75 68.2 14 12.7 3 2.7 5 4.5 12 10.9
Other 58 52.7 24 21.8 6 5.5 6 5.5 16 14.5
Source: Table Set Section 2.3, Table 2.4
Both at 3 and 6 months after treatment start, the factors age, other factors and genetics were ticked most
often and thought to be the most important factors for causing AD. Most patients ticked age as first,
genetics as second and other factors as third most important causes. Diet and infection/virus were not
ticked by most caregivers (>80%). Also environment was not considered as important cause (not ticked
by 66.1% after 3 months and by 68.2% after 6 months). Although genetics belonged to the three most
important factors, it was not ticked by 45.7% of caregivers after 3 and 52.7% after 6 months. Taken
together, age was the predominant factor for AD.
9.3.4 Usage of Exelon® patch
The proportion of patients who were still using the patch after treatment initiation was 88.2%
(n=112/127) at first visit (missing 7.9%) and also 88.2% (n=97/110) at final visit (missing 7.3%). Only
5 patients (3.9%) discontinued the Exelon® patch before baseline visit and further 5 patients (4.5%)
before final visit (Source: Table Set Section 1.4, Table 1.17-1.18 and 2.4, Table 2.5-2.6).
Novartis Confidential Page 34 Non-interventional study report Study No. CENA713DDE23
9.3.5 Opinion on Exelon® patch
Caregivers were asked about their opinions about some statements of other persons made on the
Exelon® patch 3 and again 6 months after treatment initiation (Table 9-14 and

Novartis Confidential Page 35 Non-interventional study report Study No. CENA713DDE23
Table 9-15).
Table 9-14 Opinion on Exelon® patch (3 months after treatment initiation, caregiver questionnaire, n=127)
Opinion on
Exelon® patch
Missing I don't
agree at all I don't
agree I don't
know I agree I completely
agree
N % N % N % N % N % N %
Health depends on
patch 10 7.9 1 0.8 7 5.5 40 31.5 59 46.5 10 7.9
Worry about usage
of patch 11 8.7 60 47.2 33 26.0 9 7.1 12 9.4 2 1.6
Could not live
without patch 11 8.7 34 26.8 27 21.3 47 37.0 7 5.5 1 0.8
Thoughts about
long-term effects 11 8.7 34 26.8 20 15.7 25 19.7 35 27.6 2 1.6
Very ill without
patch 12 9.4 7 5.5 21 16.5 31 24.4 49 38.6 7 5.5
Patch is a mystery
14 11.0 50 39.4 17 13.4 29 22.8 14 11.0 3 2.4
Future health
depends on patch 11 8.7 11 8.7 7 5.5 44 34.6 49 38.6 5 3.9
Patch disturbs
life 11 8.7 67 52.8 23 18.1 20 15.7 4 3.1 2 1.6
Concerns about
addiction 11 8.7 61 48.0 17 13.4 23 18.1 15 11.8 - -
Patch protects from
feeling worse 11 8.7 1 0.8 6 4.7 16 12.6 76 59.8 17 13.4
Source: Table Set Section 1.4, Table 1.19
More than half of the caregivers agreed (agreed or completely agreed) with the statements that “health
would depend on the patch” (54.3%) and that the “patch would protect the patients from feeling worse”
(73.2%). Slightly less than half of the caregivers agreed with the statements that the patient would “be
very ill without the patch” (44.1%, 24.4% did not know) and that the patient’s “future would depend on
the patch” (42.5%, 34.6% did not know). Most caregivers disagreed (disagreed or disagreed at all) with
the following statements: “worry about usage of patch” (73.2%), “patch disturbs life” (70.9%),
“concerns about addiction” (61.4%), “patch is a mystery” (52.8%), “could not live without patch”
(48.0%, 37.0% did not know), and “thoughts about long-term effects of the patch” (42.5%).

Novartis Confidential Page 36 Non-interventional study report Study No. CENA713DDE23
Table 9-15 Opinion on Exelon® patch (6 months after treatment initiation, caregiver questionnaire, n=110)
Opinion on
Exelon® patch
Missing I don't
agree at all I don't
agree I don't
know I agree I completely
agree
N % N % N % N % N % N %
Health depends on
patch 7 6.4 1 0.9 8 7.3 31 28.2 54 49.1 9 8.2
Worry about usage
of patch 6 5.5 65 59.1 20 18.2 8 7.3 9 8.2 2 1.8
Could not live
without patch 6 5.5 21 19.1 29 26.4 43 39.1 10 9.1 1 0.9
Thoughts about
long-term effects 7 6.4 48 43.6 8 7.3 22 20.0 20 18.2 5 4.5
Very ill without
patch 6 5.5 8 7.3 10 9.1 38 34.5 42 38.2 6 5.5
Patch is a mystery
8 7.3 51 46.4 8 7.3 26 23.6 13 11.8 4 3.6
Future health
depends on patch 6 5.5 9 8.2 16 14.5 30 27.3 44 40.0 5 4.5
Patch disturbs
life 8 7.3 67 60.9 14 12.7 14 12.7 7 6.4 - -
Concerns about
addiction 7 6.4 68 61.8 10 9.1 11 10.0 14 12.7 - -
Patch protects
from feeling worse 6 5.5 4 3.6 3 2.7 11 10.0 64 58.2 22 20.0
Source: Table Set Section 2.3, Table 2.7
At final visit (6 months after treatment initiation), the level of acceptance (agreed or completely agreed)
to the statements that “health would depend on the patch” (57.3%), that the “patch would protect the
patients from feeling worse” (78.2%), and that the patient’s “future would depend on the patch”
(44.5%, 27.3% did not know) has increased slightly compared to the documentation 3 months earlier.
Also the level of rejection (disagreed or disagreed at all) has increased slightly regarding the following
statements: “worry about usage of patch” (77.3%), “patch disturbs life” (73.6%), “concerns about
addiction” (70.9%), “patch is a mystery” (53.6%), and “thoughts about long-term effects of the patch”
(50.9%). This shift of answers can be attributed to the fact that less patients ticked the “I don’t know”
box with the respective questions. Only with the statements “could not live without patch” (disagreed
45.5%, 39.1% did not know) and “patient would be very ill without the patch” (agreed 43.6%, 34.5%
did not know) the level of (dis-)agreement has decreased and more caregivers ticked the “I don’t know”
boxes.

Novartis Confidential Page 37 Non-interventional study report Study No. CENA713DDE23
9.3.6 Compliance
Caregivers were asked to what extent they deviated from the physician’s instructions or on the package
leaflet (consciously or unconsciously, see Table 9-16 and Table 9-17).
Table 9-16 Compliance with usage instructions (3 months after treatment initiation, caregiver questionnaire, n=127)
Compliance Missing Always Often Sometimes Rarely Never
N % N % N % N % N % N %
Forgotten to fix
patch 8 6.3 2 1.6 5 3.9 19 15.0 28 22.0 65 51.2
Forgotten to
remove patch 8 6.3 - - 7 5.5 17 13.4 21 16.5 74 58.3
Patch paused for
a while 9 7.1 2 1.6 5 3.9 5 3.9 13 10.2 93 73.2
Patch omitted
sometimes 9 7.1 2 1.6 2 1.6 9 7.1 10 7.9 95 74.8
Change of time
for fixing patch 8 6.3 1 0.8 8 6.3 14 11.0 14 11.0 82 64.6
Source: Table Set Section 1.4, Table 1.20
At the first documentation time, most caregivers stated that she/he had never “omitted that patch
sometimes” (74.8%), “paused the patch for a while” (73.2%), or “changed the fixing patch time”
(64.6%). A total of 58.3% of caregivers never have “forgotten to remove the patch” and 29.9%
sometimes or rarely. Similarly, 51.2% of caregivers never have “forgotten to fix the patch” and 37.0%
did so sometimes or rarely.
Within the last 2 weeks before first documentation, 69.3% of caregivers (n=88/127) stated that there
was no day of irregular use of patch, 8.7% had one day (n=11/127), 5.5% with 1-2 or 2 days (n=7/127)
and 6.3% with more than 2 days of irregular use (n=8/127). There was missing information for 13
caregivers (10.2%) (Source: Tablet Set Section 1.4, Table 1.21).

Novartis Confidential Page 38 Non-interventional study report Study No. CENA713DDE23
Table 9-17 Compliance with usage instructions (6 months after treatment initiation, caregiver questionnaire, n=110)
Compliance Missing Always Often Sometimes Rarely Never
N % N % N % N % N % N %
Forgotten to fix
patch 9 8.2 5 4.5 5 4.5 15 13.6 17 15.5 59 53.6
Forgotten to
remove patch 6 5.5 4 3.6 6 5.5 14 12.7 15 13.6 65 59.1
Patch paused for
a while 6 5.5 4 3.6 7 6.4 3 2.7 8 7.3 82 74.5
Patch omitted
sometimes 6 5.5 2 1.8 5 4.5 6 5.5 5 4.5 86 78.2
Change of time
for fixing patch 6 5.5 1 0.9 8 7.3 12 10.9 11 10.0 72 65.5
Source: Table Set Section 2.4, Table 2.8
Overall, at the final documentation time (6 months after treatment initiation), the proportion of
caregivers who have never forgotten to fix or remove the patch or who have changed patch usage has
slightly increased compared to the first documentation.
There was also a high proportion of caregivers who stated that the number of days with irregular use
was zero (70.0%). A total of 10.0% (n=11/110) had 1 day and 9.1% (n=10/110) with more than 1 day
of irregular use (Source: Tablet Set Section 2.4, Table 2.9).
9.3.7 Satisfaction with efficacy
Caregivers were asked about their satisfaction with the efficacy of the Exelon® patch at both visits (see
Table 9-18 and Table 9-19).
Table 9-18 Satisfaction with efficacy (3 months after treatment initiation, caregiver questionnaire, n=127)
Satisfaction with
efficacy Missing
Very
unsatisfied Unsatisfied Satisfied Very
satisfied
N % N % N % N % N %
Memory 10 7.9 2 1.6 31 24.4 79 62.2 5 3.9
Activities 10 7.9 - - 20 15.7 88 69.3 9 7.1
Behaviour and emotions 10 7.9 3 2.4 21 16.5 83 65.4 10 7.9
Source: Table Set Section 1.4, Table 1.22
At the first visit, the majority of caregivers was satisfied with the efficacy of the patch on the ability to
undertake activities (69.3%), on behavior and emotions (65.4%), and on memory (62.2%). Very
satisfied were 7.1%, 7.9% and 3.9%, respectively. Unsatisfied with the efficacy of the patch on
memory were 24.4% of caregivers, on behavior and emotions 16.5%, and activities 15.7%.

Novartis Confidential Page 39 Non-interventional study report Study No. CENA713DDE23
Table 9-19 Satisfaction with efficacy (6 months after treatment initiation, caregiver questionnaire, n=110)
Satisfaction with
efficacy Missing
Very
unsatisfied Unsatisfied Satisfied Very
satisfied
N % N % N % N % N %
Memory 9 8.2 1 0.9 25 22.7 62 56.4 13 11.8
Activities 7 6.4 1 0.9 12 10.9 73 66.4 17 15.5
Behaviour and emotions 7 6.4 2 1.8 12 10.9 71 64.5 18 16.4
Source: Table Set Section 2.4, Table 2.10
At the final visit, the level of satisfaction with the efficacy has increased compared to the first
documentation, with 16.4% of caregivers being very satisfied and 64.5% satisfied with the effect on
behavior and emotions, 15.5% very satisfied and 66.4% satisfied with effect on activities, and 11.8%
being very satisfied and 56.4% satisfied with the effect on memory. The proportion of caregivers being
unsatisfied has decreased compared to the first documentation.
9.3.8 Application of the patch
Caregivers were asked to evaluate the ease of application of the patch at the two visits (see Table 9-20
and Table 9-21).
Table 9-20 Application of the patch (3 months after treatment initiation, caregiver questionnaire, n=127)
Application of patch Missing Very difficult Difficult Easy Very easy
N % N % N % N % N %
Open of package 10 7.9 - - 4 3.1 58 45.7 55 43.3
Make patient to use it 9 7.1 1 0.8 5 3.9 57 44.9 55 43.3
Fix patch 9 7.1 1 0.8 3 2.4 57 44.9 57 44.9
Remove patch 9 7.1 - - 1 0.8 57 44.9 60 47.2
Source: Table Set Section 1.4, Table 1.24
At the first documentation, more than 85% of caregivers found that opening of the package, make the
patient to use it, fixing and removing of patch was easy or very easy.
Novartis Confidential Page 40 Non-interventional study report Study No. CENA713DDE23
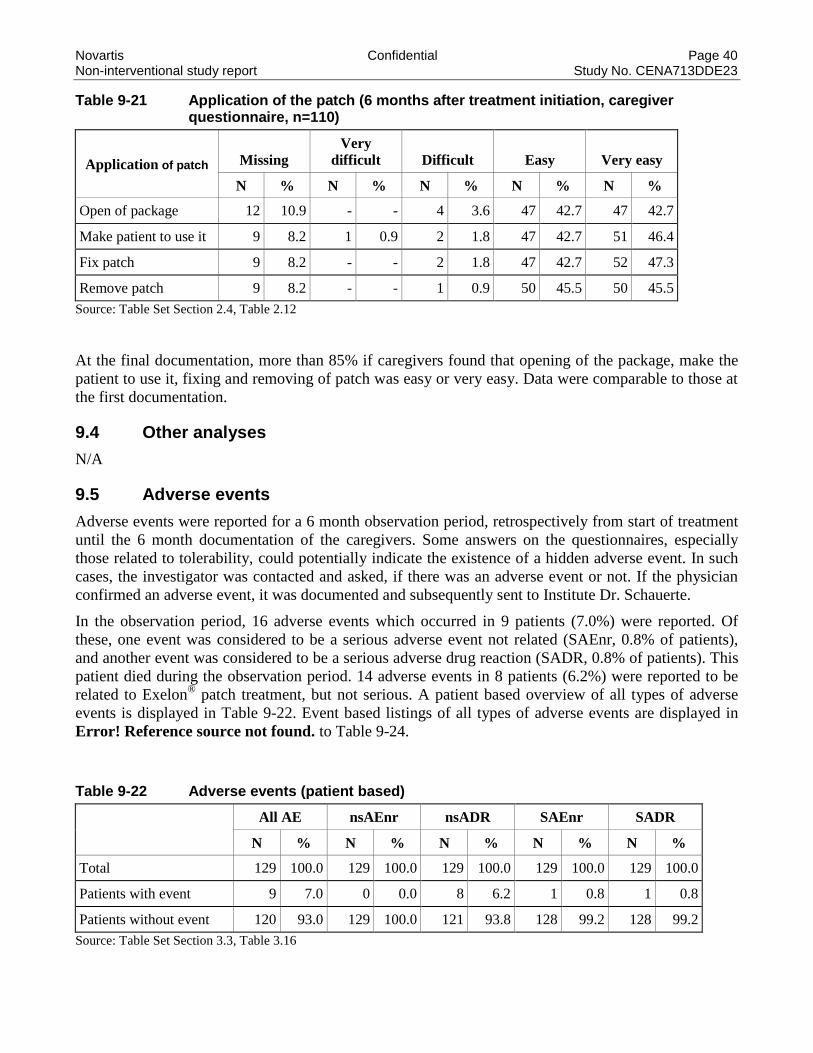
Table 9-21 Application of the patch (6 months after treatment initiation, caregiver questionnaire, n=110)
Application of patch Missing Very
difficult Difficult Easy Very easy
N % N % N % N % N %
Open of package 12 10.9 - - 4 3.6 47 42.7 47 42.7
Make patient to use it 9 8.2 1 0.9 2 1.8 47 42.7 51 46.4
Fix patch 9 8.2 - - 2 1.8 47 42.7 52 47.3
Remove patch 9 8.2 - - 1 0.9 50 45.5 50 45.5
Source: Table Set Section 2.4, Table 2.12
At the final documentation, more than 85% if caregivers found that opening of the package, make the
patient to use it, fixing and removing of patch was easy or very easy. Data were comparable to those at
the first documentation.
9.4 Other analyses
N/A
9.5 Adverse events
Adverse events were reported for a 6 month observation period, retrospectively from start of treatment
until the 6 month documentation of the caregivers. Some answers on the questionnaires, especially
those related to tolerability, could potentially indicate the existence of a hidden adverse event. In such
cases, the investigator was contacted and asked, if there was an adverse event or not. If the physician
confirmed an adverse event, it was documented and subsequently sent to Institute Dr. Schauerte.
In the observation period, 16 adverse events which occurred in 9 patients (7.0%) were reported. Of
these, one event was considered to be a serious adverse event not related (SAEnr, 0.8% of patients),
and another event was considered to be a serious adverse drug reaction (SADR, 0.8% of patients). This
patient died during the observation period. 14 adverse events in 8 patients (6.2%) were reported to be
related to Exelon® patch treatment, but not serious. A patient based overview of all types of adverse
events is displayed in Table 9-22. Event based listings of all types of adverse events are displayed in
Error! Reference source not found. to Table 9-24.
Table 9-22 Adverse events (patient based)
All AE nsAEnr nsADR SAEnr SADR
N % N % N % N % N %
Total 129 100.0 129 100.0 129 100.0 129 100.0 129 100.0
Patients with event 9 7.0 0 0.0 8 6.2 1 0.8 1 0.8
Patients without event 120 93.0 129 100.0 121 93.8 128 99.2 128 99.2
Source: Table Set Section 3.3, Table 3.16
Novartis Confidential Page 41 Non-interventional study report Study No. CENA713DDE23
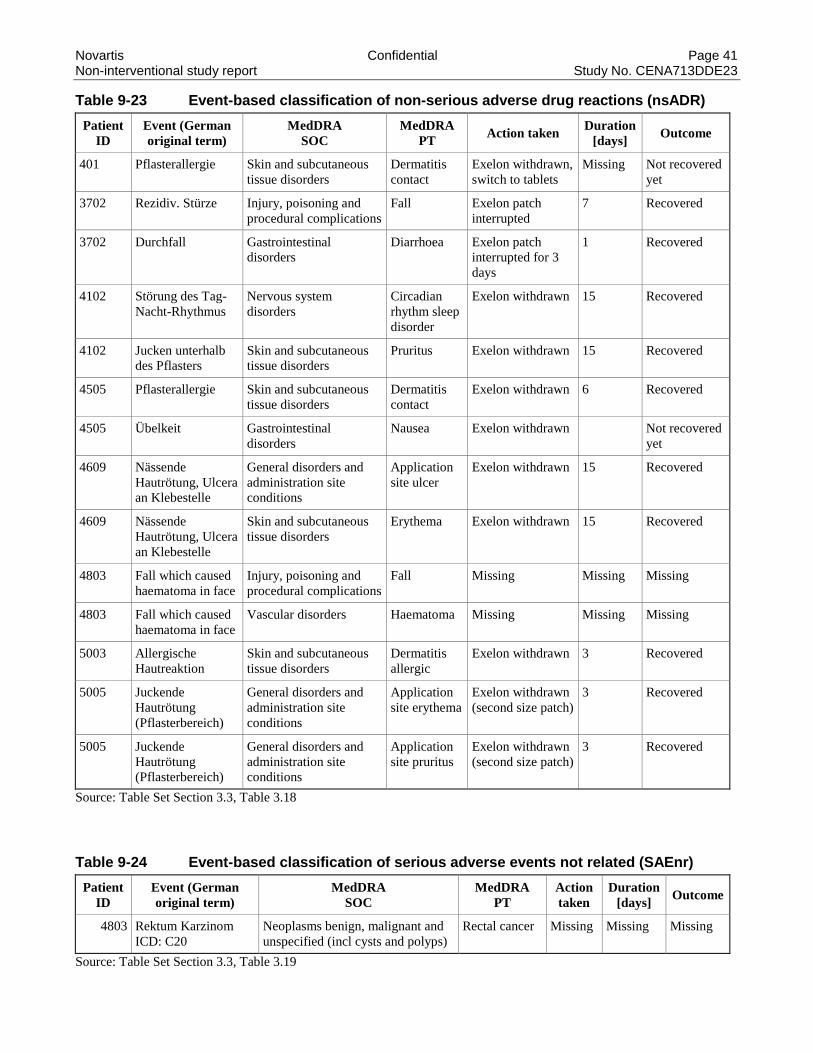
Table 9-23 Event-based classification of non-serious adverse drug reactions (nsADR)
Patient
ID
Event (German
original term)
MedDRA
SOC
MedDRA
PT Action taken
Duration
[days] Outcome
401 Pflasterallergie Skin and subcutaneous
tissue disorders
Dermatitis
contact
Exelon withdrawn,
switch to tablets
Missing Not recovered
yet
3702 Rezidiv. Stürze Injury, poisoning and
procedural complications
Fall Exelon patch
interrupted
7 Recovered
3702 Durchfall Gastrointestinal
disorders
Diarrhoea Exelon patch
interrupted for 3
days
1 Recovered
4102 Störung des Tag-
Nacht-Rhythmus
Nervous system
disorders
Circadian
rhythm sleep
disorder
Exelon withdrawn 15 Recovered
4102 Jucken unterhalb
des Pflasters
Skin and subcutaneous
tissue disorders
Pruritus Exelon withdrawn 15 Recovered
4505 Pflasterallergie Skin and subcutaneous
tissue disorders
Dermatitis
contact
Exelon withdrawn 6 Recovered
4505 Übelkeit Gastrointestinal
disorders
Nausea Exelon withdrawn Not recovered
yet
4609 Nässende
Hautrötung, Ulcera
an Klebestelle
General disorders and
administration site
conditions
Application
site ulcer
Exelon withdrawn 15 Recovered
4609 Nässende
Hautrötung, Ulcera
an Klebestelle
Skin and subcutaneous
tissue disorders
Erythema Exelon withdrawn 15 Recovered
4803 Fall which caused
haematoma in face
Injury, poisoning and
procedural complications
Fall Missing Missing Missing
4803 Fall which caused
haematoma in face
Vascular disorders Haematoma Missing Missing Missing
5003 Allergische
Hautreaktion
Skin and subcutaneous
tissue disorders
Dermatitis
allergic
Exelon withdrawn 3 Recovered
5005 Juckende
Hautrötung
(Pflasterbereich)
General disorders and
administration site
conditions
Application
site erythema
Exelon withdrawn
(second size patch)
3 Recovered
5005 Juckende
Hautrötung
(Pflasterbereich)
General disorders and
administration site
conditions
Application
site pruritus
Exelon withdrawn
(second size patch)
3 Recovered
Source: Table Set Section 3.3, Table 3.18
Table 9-24 Event-based classification of serious adverse events not related (SAEnr)
Patient
ID
Event (German
original term)
MedDRA
SOC
MedDRA
PT
Action
taken
Duration
[days] Outcome
4803 Rektum Karzinom
ICD: C20
Neoplasms benign, malignant and
unspecified (incl cysts and polyps)
Rectal cancer Missing Missing Missing
Source: Table Set Section 3.3, Table 3.19

Novartis Confidential Page 42 Non-interventional study report Study No. CENA713DDE23
Table 9-25 Event-based classification of serious adverse drug reactions (SADR)
Patient
ID
Event (German
original term)
MedDRA
SOC
MedDRA
PT
Action
taken
Duration
[days] Outcome
3102 Tod - Ursache
unbekannt
General disorders and
administration site conditions
Death Missing Missing Death
Source: Table Set Section 3.3, Table 3.20
All 14 non-serious adverse events were assessed to be related to Exelon® patch treatment (causality
probable, possible, assured, or not assessable).
Of the 14 non-serious adverse drug reactions, 5 were of mild intensity, 5 of moderate and 2 of severe
intensity (2 missings). Treatment with Exelon® patch was withdrawn due to 10 non-serious adverse
drug reactions, 2 times the treatment was interrupted (2 missings). The outcome of the non-serious
adverse drug reactions was documented as recovered for 10 events and not yet recovered for 2 events
(2 missings).
A total of 2 serious adverse events were experienced by 2 patients, for which the causality was
documented as not assessable / no causal relation. One patient died due to unknown cause. This event
(causality not assessable) was upgraded by Novartis according to conservative policy and submitted to
German health authority. Information about the outcome of the other serious event rectal cancer was
missing. For a more detailed listing of adverse events, separately for non-serious adverse drug reactions
(nsADR), serious adverse events not related (SAEnr), and serious adverse drug reactions (SADR),
please refer to the Table Set, Table 3.17 to 3.20.
9.5.1 Satisfaction of caregiver with tolerability
Caregivers were asked to assess their satisfaction with the tolerability of the patch 3 and 6 months after
treatment initiation.
At the first documentation, 47.2% of caregivers (n=60/127) assessed the tolerability of the patch as
good and 43.3% (n=55/127) as very good. Two caregivers assessed the tolerability of the patch as not
good and 2 caregivers as not good at all.
At the final documentation, satisfaction with the tolerability of the patch has increased, with 37.3% of
caregivers (n=41/110) assessing the tolerability of the patch as good and 52.7% (n=58/110) as very
good. Four caregivers (3.6%) assessed the tolerability of the patch as not good and one caregiver
(0.9%) as not good at all.

Novartis Confidential Page 43 Non-interventional study report Study No. CENA713DDE23
10 Discussion
10.1 Key results
A total of 127 caregivers (reporting about 127 patients) and a total of 18 physicians (documenting 129
patients) in Germany completed the respective questionnaires at the baseline visit (3 months after
initiation of Exelon® patch). In addition, 110 caregiver questionnaires were completed at the
completion visit (6 months after treatment start). Thus, three different populations can be analyzed,
based on completed caregiver questionnaires at 3 months (N = 127), completed caregiver
questionnaires at 6 months (N = 110), and completed physician questionnaires at 3 months (N = 129).
Baseline information: According to caregiver’s information, half of the patients (50.4%) with AD
were female (n=64) and the mean age was 78.2 years at the time of data recording. Most often, patients
suffered from concomitant hypertension (38.8%), heart disease (32.6%), diabetes (27.1%) and clinical
depression (15.5%). The mean number of concomitant medication was 3.0 ± 2.3 at the time of
treatment initiation.
According to the physicians’ information, majority of the patients presented with mild (24.8%), mild to
moderate (38.8%), or moderate (23.3%) AD at the time of treatment initiation and the mean ± SD
MMSE-score was 20.8 ± 3.3 points (out of 30), corresponding to mild dementia.
At the time of treatment initiation, the high dose Exelon® patch (9.5 mg/ 24 h) was prescribed in 53.5%
(n=69) and the low dose patch in 42.6% (n=55) of patients by the physicians. Both doses were
prescribed for 5 patients.
Three months after treatment initiation (current information at first study visit), most physicians
estimated that the CGI would be much improved (35.7%) or a little improved (30.2%). No change was
seen by 21.7% of physicians and 10 times physicians saw a deterioration of AD.
Patient’s opinion: Most patients thought that their AD was caused by their age (76.4%, n=97). Second
most common causes were thought to be genetic endowments (26.0%, n=33) or other (26.0%, n=33).
Patches were more favored than other types of medications (pills or liquids). Most patients preferred or
highly preferred patches as type of medication. Patches were not preferred by 7.9% of patients
(n=10/127). Pills and liquids were moderately preferred (both 37.8%) and preferred (both 17.3%) by
most patients.
Information about caregiver: Most of the caregivers (70.9%, n=90/127) were female and had a mean
age of 66.4 ± 13.9 years. The majority (75.6%) never cared for relatives before and more than half of
the caregivers see the patient most of the time daily (59.1%). At the time of treatment initiation, the
patient was supervised by the spouse (57.4%, n=74/129), the daughter (21.7%, n=28/129), a paid
caregiver (5.4%, n=7/129), another person (3.1%, n=4/129), or the son (3.1%, n=4/129). A total of 11
patients (8.5%) were supervised by more than one person (e.g. spouse and daughter). At the time of
first treatment initiation, the ability of the caregiver to take care for the patient was not at all restricted
in 62.8% and little restricted in 17.8% of caregivers (physician’s information).
Caregiver information over time (3 and 6 months): Most caregivers had full responsibility (34.6%)
or had to help a lot (33.9%) with the application of the patch at baseline and no relevant changes in the
extent of help was seen 3 months later (35.5% and 36.4%, respectively). At baseline, most of the
patients were compliant with the Exelon®
patch, i.e. mostly (44.1%) or always (33.1%) supported their
caregivers when fixing the patch. In addition, the majority of the patients adhered to the medication and

Novartis Confidential Page 44 Non-interventional study report Study No. CENA713DDE23
always (55.9%) or mostly (26.8%) kept the patch as long as necessary. Compliance and adherence data
were comparable 6 months after treatment start.
Most of the caregivers had no psychological problems at all (about 57% to 63% in the four domains) or
only on several days (about 20% to 24%) at baseline. This proportion of patients without any
significant problems remained largely unchanged up to the completion visit.
At the first documentation, the mean score values of the “Opinion on AD” questionnaire mostly were
in the middle range of the scale (around 4.1 to 6.9), showing that patients but also caregivers were
distinctly affected by the AD, although none of the mean scores achieved extreme values. Only the
question on the duration of the disease showed that caregivers were aware of the very long duration
(mean score 8.5). At the final documentation, mean score values were almost the same as after 3
months.
Both at 3 and 6 months after treatment start, the factors age, other factors and genetics were ticked most
often by the caregivers and thought to be the most important factors for causing AD.
The proportion of patients who were still using the patch after treatment initiation was 88.2%
(n=112/127) at first visit (missing 7.9%) and also 88.2% (n=97/110) at final visit (missing 7.3%). Only
5 patients discontinued the Exelon® patch before baseline visit and further 5 patients before final visit.
More than half of the caregivers agreed (agreed or completely agreed) with the statements that “health
would depend on the patch” (54.3%) and that the “patch would protect the patients from feeling worse”
(73.2%). Slightly less than half of the caregivers agreed with the statements that the patient would “be
very ill without the patch” (44.1%, 24.4% did not know) and that the patient’s “future would depend on
the patch” (42.5%, 34.6% did not know). Most caregivers disagreed (disagreed or disagreed at all) with
the following statements: “worry about usage of patch” (73.2%), “patch disturbs life” (70.9%),
“concerns about addiction” (61.4%), “patch is a mystery” (52.8%), “could not live without patch”
(48.0%, 37.0% did not know), and “thoughts about long-term effects of the patch” (42.5%). At final
documentation, the level of acceptance to the statements that caregivers had agreed with 3 months
earlier has increased slightly. Also the level of rejection with those statements previously disagreed has
increased slightly. Only with the statements “could not live without patch” (disagreed 45.5%, 39.1%
did not know) and “patient would be very ill without the patch” (agreed 43.6%, 34.5% did not know)
the level of (dis-)agreement has decreased and more caregivers ticked the “I don’t know” boxes.
At both visits, both the caregivers and the patients were highly compliant. At the first documentation
time, most caregivers stated that she/he had never “omitted that patch sometimes” (74.8%), “paused the
patch for a while” (73.2%), or “changed the fixing patch time” (64.6%). A total of 58.3% of caregivers
never have “forgotten to remove the patch” and 29.9% sometimes or rarely. Similarly, 51.2% of
caregivers never have “forgotten to fix the patch” and 37.0% did so sometimes or rarely. Within the
last 2 weeks before first documentation, 69.3% of caregivers (n=88/127) stated that there was no day of
irregular use of patch. At the final documentation time (6 months after treatment initiation), the
proportion of caregivers who have never forgotten to fix or remove the patch or who have changed
patch usage has slightly increased compared to the first documentation. There was also a high
proportion of caregivers who stated that the number of days with irregular use was zero (70.0%).
At the final visit, the level of satisfaction with the efficacy has increased compared to the first
documentation, with 16.4% of caregivers being very satisfied and 64.5% satisfied with the effect on
behavior and emotions, 15.5% very satisfied and 66.4% satisfied with effect on activities, and 11.8%
being very satisfied and 56.4% satisfied with the effect on memory. The proportion of caregivers being
unsatisfied has decreased compared to the first documentation.

Novartis Confidential Page 45 Non-interventional study report Study No. CENA713DDE23
More than 85% if caregivers found that opening of the package, make the patient to use it, fixing and
removing of patch was easy or very easy at both documentations.
In conclusion, most caregivers and their patients adhered to the treatment with rivastigmine (Exelon®
patch) during the 6 months observation period. The application of the patch was considered by the
caregivers as easy to use, efficacious and satisfying for both the patient and the caregiver.
10.2 Safety conclusions
In the observation period, 16 adverse events which occurred in 9 patients were reported. Of these, one
event was considered to be a serious adverse event not related, and another event was considered to be
a serious adverse drug reaction. This patient died during the observation period. 14 adverse events in 8
patients were reported to be related to Exelon® patch treatment, but not serious.
Rivastigmine (Exelon® patch) proved to be a well-tolerated drug for the treatment of patients with
Alzheimer’s disease, as demonstrated by the low incidence rate of adverse events. The nature and
frequency of adverse events occurring during the 6 months therapy were consistent with the established
safety profile of rivastigmine. The current NIS did not reveal any suspicion of unknown risks related to
the treatment with rivastigmine.

Novartis Confidential Page 46 Non-interventional study report Study No. CENA713DDE23
11 References
Folstein MF, Folstein SE, McHugh PR (1975). ""Mini-mental state". A practical method for grading
the cognitive state of patients for the clinician". Journal of Psychiatric Research 12 (3): 189–98.

Novartis Confidential Page 47 Non-interventional study report Study No. CENA713DDE23
12 Appendix
12.1 Sample study protocol including data entry forms
12.2 Table set
12.3 Signatures
I certify that this report accurately describes the conduct and the results of this clinical study.
Project Lead CRO: Caroline Schneider
Signature Date
Statistical Lead: Klaus Hechenbichler
Signature Date
I certify that this report accurately describes the conduct and the results of this clinical study.
Medical Advisor: Beate Müller
Signature Date
I have read this report and confirm to the best of my knowledge it accurately describes safety results
from the study.
Medical Safety Expert DS&E:
Katharina Salb
Signature Date
I have read this report and confirm that to the best of my knowledge it accurately describes the conduct
and results of the study.
TA Head: Alexander Fuchs
Signature Date