Embed Size (px)
Citation preview

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
HIGH BLOOD PRESSURE
Status Report on the
NHLBI-Sponsored
CVD Prevention Guidelines
Paul A. James, M.D.
Roy J. and Lucille A. Carver College of Medicine
The University of Iowa
Iowa City IA

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Joint National Committee on
Prevention, Detection,
Evaluation, & Treatment of
High Blood Pressure (JNC)
JNC 7: 2003
JNC 6: 1997
JNC 5: 1992
JNC 4: 1988
JNC 3: 1984
JNC 2: 1980
JNC 1: 1976
Detection, Evaluation,
&Treatment of High Blood
Cholesterol
in Adults (ATP, Adult
Treatment Panel)
ATP III Update: 2004
ATP III: 2002
ATP II: 1993
ATP I: 1988
Clinical Guidelines on the
Identification, Evaluation, &
Treatment of Overweight
and Obesity in Adults
Obesity: 1998
NHLBI Adult CVD Prevention Guidelines
NHLBI-SPONSORED
ADULT CVD PREVENTION GUIDELINES

80
85
90
95
100
105
110
115
120
125
130
JNC I JNC II JNC III JNC IV JNC V JNC VI
Consider therapy
Hyper- tensive
Mild Mild Mild
Stage 1 Stage 1
Moderate Moderate Moderate
Stage 2
Severe Severe Severe Stage 3 Stage 3
Stage 2
Stage 4
High- normal
High- normal
High- normal
High- normal
Normal Normal Normal Normal
Optimal
DBP
(mm Hg)
Optimal
JNC 7
Stage 1
Stage 2
Prehyper- tension
Normal
JNC IV. Arch Intern Med. 1988;148:1023-1038.
JNC V. Arch Intern Med. 1993;153:154-183.
JNC VI. Arch Intern Med. 1997;157:2413-2446.
Chobanian AV et al. JAMA. 2003;289:2560-2572.
JNC I. JAMA. 1977;237:255-261.
JNC II. Arch Intern Med. 1980;140:1280-1285.
JNC III. Arch Intern Med. 1984;144:1045-1057.
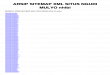
Hypertension: A Moving Target JNC Classifications: Diastolic Blood Pressure

JNC V
Optimal 110
120
130
140
150
160
170
180
190
200
210
220
JNC IV. Arch Intern Med. 1988;148:1023-1038.
JNC V. Arch Intern Med. 1993;153:154-183.
JNC VI. Arch Intern Med. 1997;157:2413-2446.
Chobanian AV et al. JAMA. 2003;289:2560-2572.
JNC I JNC II JNC III JNC IV JNC VI
Border- line
ISH
Stage 1 Stage 1
Stage 2
Stage 3
High- normal
High- normal
Normal Normal
Optimal
SBP
(mm Hg)
Normal
Border- line
ISH
Stage 4
No recommendations
for SBP in JNC I
or JNC II
JNC 7
Stage 1
Prehyper- tension
Normal
Stage 3
Stage 2
JNC I. JAMA. 1977;237:255-261.
JNC II. Arch Intern Med. 1980;140:1280-1285.
JNC III. Arch Intern Med. 1984;144:1045-1057.
Hypertension: A Moving Target JNC Classifications: Systolic Blood Pressure
Stage 2

JNC VI. Arch Intern Med. 1997;157:2413-2446.
OPTIMAL < 120 and < 80
NORMAL < 130 and < 85
STAGE 1 140-159 or 90-99
STAGE 2 160-179 or 100-109
STAGE 3 ≥ 180 or ≥ 110
NORMAL < 120 and < 80
PREHYPERTENSION 120-139 or 80-89
STAGE 1 140-159 or 90-99
STAGE 2 ≥ 160 or ≥ 100
JNC 7 (2003) JNC VI (1997)
JNC 7 Emphasized Importance of
Lower Blood Pressure
HIGH NORMAL 130-139 or 85-89
JNC 7. JAMA. 2003;289(19):2560-2572.

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Institute of Medicine Report:
Quality Chasm “In its current form, habits, and environment, American health
care is incapable of providing the public with the quality health
care it expects and deserves.”
Current: Decision making is based on training and experience.
New: Decision making is based on evidence.
Patients should receive care based on the best available
scientific knowledge. Care should not vary illogically from
clinician to clinician or from place to place.
Evidence-based Clinical Practice Guidelines can help make
this vision a reality
Institute of Medicine, Crossing the Quality Chasm: New Health System for the Twenty-first Century. Washington: National Academy Press, 2001

Evidence-Based Clinical Practice Guidelines for CVD Prevention
AHA LEVEL OF "A“ EVIDENCE IN CURRENT GUIDELINES*
*in guidelines
with level of
evidence
11.7%
26.4%
15.3%
13.5%
12.0%
22.9%
6.4%
6.1%
23.6%
0.3%
9.7%
11.0%
19.0%
4.9%
4.8%
0% 10% 20% 30%
AF
Heart failure
PAD
STEMI
Perioperative
Secondary prevention
Stable angina
SV arrhythmias
UA/NSTEMI
Valvular disease
VA/SCD
PCI
CABG
Pacemaker
Radionuclide imaging
Scientific Evidence Underlying ACC/AHA Guidelines (JAMA. 2009; 301: 831 – 841)

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Recent Evidence is changing practice
New Evidence is causing us to question aggressive
disease management strategies
Important health outcomes rather than markers of disease
are being examined.
Examples:
ACCORD (2010): Diabetics not improved with tighter control.
JATOS (2008) and Valish (2010): Hypertension: no
improvement in outcomes with Goal BP of <140 mm Hg in
elderly compared to 150 mm Hg.
Courage (2007): Stable angina: no benefit with PTCA over
medical management

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ACCORD Trial: A study that will change
our practice.
High risk patients for CVD with Type 2 DM: Average age = 62.2
years old. 1/3 had previous CV event.
Studied intensive management of diabetes, blood pressure
and lipids. Baseline: A1c = 8.3%, BP = 139/76, T.Chol = 193
mg/dl
Documented the harms of intensive (overly exuberant?)
therapy to manage risk factors for CVD.

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ACCORD Trial
Blood Pressure goal among high risk patients for CVD:
Lower is not always better. Systolic BP<140 just as good
as BP<120 for major CV events. Only stroke rate
improved but overall mortality did not.
Glycemic control with A1c of 6.5% compared to 7.5% did
not reduce major CV events but mortality increased with
more intensive treatment.
Lipid control with fenofibrate added to simvastatin did not
reduce major CV events, nonfatal MI or nonfatal stroke.

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ACCORD Trial
If we do not see benefit in high risk persons, we must question
the goals of therapy in lower risk individuals.
We need better RCT’s and we should not rely on observational
data.
There are many incentives within our current health care
system to prescribe and over treat. We must further assess the
harms.

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Adult CVD Guidelines:
NHLBI approach Advice to NHLBI from advisory groups:
Update risk factor guidelines (hypertension, cholesterol, obesity)
Develop an integrated guideline
Use an evidence-based approach including systematic reviews
The NHLBI guideline development process
Was established to assure rigor and to minimize bias
Methods being used meet many of the new IOM standards
Two recent IOM reports set new standards
“Finding What Works in Health Care” – standards for systematic
reviews
“Clinical Practice Guidelines We can Trust” – standards for developing
trustworthy CPGs

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Expertise Represented
Hypertension, primary care, cardiology, nephrology,
clinical trials, research methodology, evidence-based
medicine, epidemiology, guideline development and
implementation, nutrition/lifestyle, nursing,
pharmacology, systems of care, and informatics
Panel also includes senior scientists from NHLBI and
NIDDK with expertise in hypertension, clinical trials,
translational research, nephrology, guideline
development, and evidence-based methodology

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Disclosures
4 panel members had relationships with industry to
disclose
13 panel members had no relationships to disclose
Panel members disclose their relationships and recuse
themselves from voting on evidence statements and
recommendations relevant to their relationships
Guideline Executive Committee Policy on Disclosures: http://www.nhlbi.nih.gov/guidelines/cvd_adult/coi-rwi_policy.htm

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
How the Process Has Evolved
Strictly evidence-based
Focus only on randomized controlled trials assessing important
health outcomes (no use of intermediate/surrogate measures)
Every included study is rated for quality by two independent
reviewers using standardized tools
Evidence statements graded for quality using prespecified criteria
Separate grading for recommendations
Independent methodology team to ensure objectivity of the review
Initial set of recommendations focused on 3 key questions

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
How Were Questions Selected?
Panel Chairs and NHLBI staff developed questions based on their
expertise, brief literature review, and speaking with colleagues
These questions were sent to panel members to review, revise,
and add or delete questions
Resulted in 23 questions, which were sent to all panel members
Panel members discussed these questions on conference calls, then
independently ranked the 3-5 questions felt to be of highest priority
The five highest ranked questions discussed further and
prioritized

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Rationale for the Questions
Interest in assessing the evidence to support 140/90 mm Hg as a
treatment threshold or goal
Should the treatment threshold / goal be lower in populations with
diabetes, chronic kidney disease, coronary artery disease, stroke,
and other co-morbidities or characteristics?
Should the treatment threshold / goal be different in older adults?
Use of different treatment thresholds and goals is confusing
Is there evidence that treatment to lower BP with a particular drug
or drug class improves outcomes compared to another?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Question 1
Among adults with hypertension, does
initiating antihypertensive pharmacological
therapy at specific BP thresholds improve
health outcomes?
− When to initiate drug treatment?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Question 2
Among adults, does treatment with
antihypertensive pharmacological therapy
to a specified BP goal lead to
improvements in health outcomes?
− How low should you go?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Question 3
In adults with hypertension, do various
antihypertensive drugs or drug classes
differ in comparative benefits and harms on
specific health outcomes?
− How do you get there?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Inclusion/Exclusion Criteria
Randomized Controlled Trials
RCTs are subject to less bias and represent the gold
standard for determining efficacy and effectiveness1
Search dates: 1966 to present
Minimum one-year follow-up period
Studies with sample sizes less than 100 excluded
1 Institute of Medicine. 2011. Finding What Works In Health Care. Standards
For Systematic Reviews. Washington, DC: The National Academies Press.

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Populations Included
Adults 18 years of age and
older
Prespecified subgroups
including:
Diabetes
Chronic kidney disease
Proteinuria
Coronary artery disease
Peripheral artery disease
Previous stroke
Heart Failure
Older Adults
Men and women
Racial and ethnic groups
Smoking

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Outcomes
Overall mortality, CVD-related mortality, CKD-related mortality,
myocardial infarction, heart failure, hospitalization for heart
failure, stroke
Coronary revascularization (includes coronary artery bypass
surgery, coronary angioplasty and coronary stent placement),
peripheral revascularization (includes carotid, renal, and lower
extremity revascularization)
End stage renal disease (i.e., kidney failure resulting
in dialysis or transplant), doubling of creatinine, halving of
eGFR

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Articles Screened = 1496
Good = 8
Included = 44
Total Abstracted = 26
Excluded = 1452 (Did not meet prespecified
inclusion criteria)
Poor = 18 Fair = 18
Question 1: Among adults with hypertension, does
initiating antihypertensive pharmacological therapy at
specific BP thresholds improve health outcomes?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Articles Screened = 1978
Good = 17
Included = 92
Total Abstracted = 56
Excluded = 1886 (Did not meet prespecified
inclusion criteria)
Poor = 36 Fair = 39
Question 2: Among adults, does treatment with
antihypertensive pharmacological therapy to a specified
BP goal lead to improvements in health outcomes?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Articles Screened = 2662
Good = 15
Included = 101
Total Abstracted = 66
Excluded = 2561 (Did not meet prespecified
inclusion criteria)
Poor = 35 Fair = 51
Question 3: In adults with hypertension, do various
antihypertensive drugs or drug classes differ in comparative
benefits and harms on specific health outcomes?

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Data Abstraction and
Evidence Tables
Information from individual studies
Key data abstracted into a database
Evidence table for each study/paper: subjects, sample size, intervention, comparison, results
Evidence summaries by Critical Question
Tables and text of major elements relevant to the CQ
Graded evidence statements
Multiple ESs for each CQ
Graded recommendations based on the evidence
Multiple ESs could result in a single recommendation
27

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
NHLBI EVIDENCE QUALITY GRADING AND
RECOMMENDATION STRENGTH
Evidence Quality
High
Well-designed and conducted RCTs
Moderate
RCTs with minor limitations
Well-conducted observational studies
Low
RCTs with major limitations
Observational studies with major limitations
Recommendation Strength
A – Strong
B – Moderate
C – Weak
D – Against
E – Expert Opinion
N – No Recommendation
28

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Adult CV Guideline
Report Content Methods description
Critical Questions
With study eligibility criteria and rationale
Summary of evidence for each CQ
Summary tables and text ( e.g. “24 studies, 10 RCTs…)
Graded evidence statements (ES)
Rationale for ES based on specific studies or previous systematic reviews
Graded High, Medium, Low
Graded recommendations
Rationale for the recommendation based on the evidence
Graded A, B, C, D, E, or N
Reference citations
29

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Conclusion
The new NHLBI-sponsored adult CV guideline reports
Are strictly evidence based
Will not look like the previous guidelines
Will have more depth and rigor; will have less breadth
Will be released in 2012, one at a time as they are ready
Will subsequently be integrated
Will use evidence based strategies for Implementation
30

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Next Steps
Evidence statements and recommendations (in progress)
Draft report (in progress)
Review of the draft report by:
Other federal agencies (CDC, CMS, AHRQ, HRSA, VA, etc.)
Invited organizations and individuals
Public
Revisions based on comments received
Final report

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
THANK YOU!
For more information on the NHLBI guidelines, go to:
http://www.nhlbi.nih.gov/guidelines/index.htm

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Committee Members
Co-Chair: Suzanne Oparil, MD
Professor of Medicine and Physiology &
Biophysics, Director, Vascular Biology and
Hypertension Program, Division of
Cardiovascular Disease, Department of Medicine
University of Alabama at Birmingham School of
Medicine
Jackson T. Wright, Jr., MD, PhD
Director, Clinical Hypertension Program
Director, William T. Dahms Clinical Research
Unit, University Hospitals Case Medical Center
Professor of Medicine
Case Western Reserve University
Sandra J. Taler, MD
Associate Professor of Medicine
Division of Nephrology and Hypertension
Mayo Clinic College of Medicine
Co-Chair: Paul A. James, MD
Professor and Head, Department of Family
Medicine in the Carver College of Medicine,
Professor of Occupational and Environmental
Health in the College of Public Health, Donald J.
and Anna M. Ottilie Endowed Chair in Family
Medicine
University of Iowa
Laura Svetkey, MD, MHS
Director, Duke Hypertension Center
Director of Clinical Research at the Sarah W.
Stedman Nutrition and Metabolism Center
Professor of Medicine
Duke University
Michael L. LeFevre, MD, MSPH
Professor, Department of Family and Community
Medicine, University of Missouri

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Committee Members
Joel Handler, MD
Clinical Lead for Hypertension
Care Management Institute
Kaiser Permanente
Southern California Permanente Medical Group,
Department of Internal Medicine
Barry L. Carter, PharmD
Professor, Department of Pharmacy Practice and
Science, College of Pharmacy
Professor and Associate Head, Research
Department of Family Medicine
University of Iowa
Daniel T. Lackland, DrPH
Professor, Epidemiology and Medicine
Department of Biostatistics, Bioinformatics, and
Epidemiology
Medical University of South Carolina
Raymond R. Townsend, MD
Director, Hypertension Section
Professor of Medicine
Department of Internal Medicine−Renal
University of Pennsylvania
William C. Cushman, MD
Chief, Preventive Medicine, Veterans Affairs
Medical Center
Lead Consultant in Hypertension to VA Medical
Service
Professor, Preventive Medicine and Medicine
University of Tennessee
Thomas D. MacKenzie, MD, MSPH
Chief Quality Officer, Denver Health and Hospital
Authority
Associate Professor of Medicine
University of Colorado School of Medicine

Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Committee Members
Sidney C. Smith, Jr., MD, FACC, FAHA, FESC
Director, Center for Cardiovascular Science and
Medicine, Professor of Medicine
University of North Carolina at Chapel Hill
Olugbenga Ogedegbe, MD, MPH, MS, FAHA
Associate Professor of Medicine
Division of General Internal Medicine
Department of Medicine
New York University School of Medicine
Cheryl Dennison Himmelfarb, RN, ANP, PhD,
FAAN
Associate Professor
Department of Health Systems and Outcomes
Johns Hopkins University School of Nursing
Division of Health Sciences Informatics
Johns Hopkins University School of Medicine
Andrew S. Narva, MD (Ex-Officio)
Director, National Kidney Disease Education
Program
Division of Kidney, Urologic and Hematologic
Diseases
National Institute of Diabetes and Digestive and
Kidney Diseases
Lawrence J. Fine, MD, DrPH (Ex-Officio)
Chief, Clinical Applications and Prevention Branch
Division of Prevention and Population Science
National Heart, Lung, and Blood Institute
Eduardo Ortiz, MD, MPH (NHLBI Lead,
Ex-Officio, Non-Voting Member)
Senior Medical Officer
Division for the Application of Research
Discoveries
National Heart, Lung, and Blood Institute
National Institutes of Health