Embed Size (px)
Citation preview

www.lhsc.on.ca/bhp
Presented by:
Mike Kennedy
Prehospital Care Specialist, SWORBHP
Dr. Matt Davis
Local Medical Directive, SWORBHP
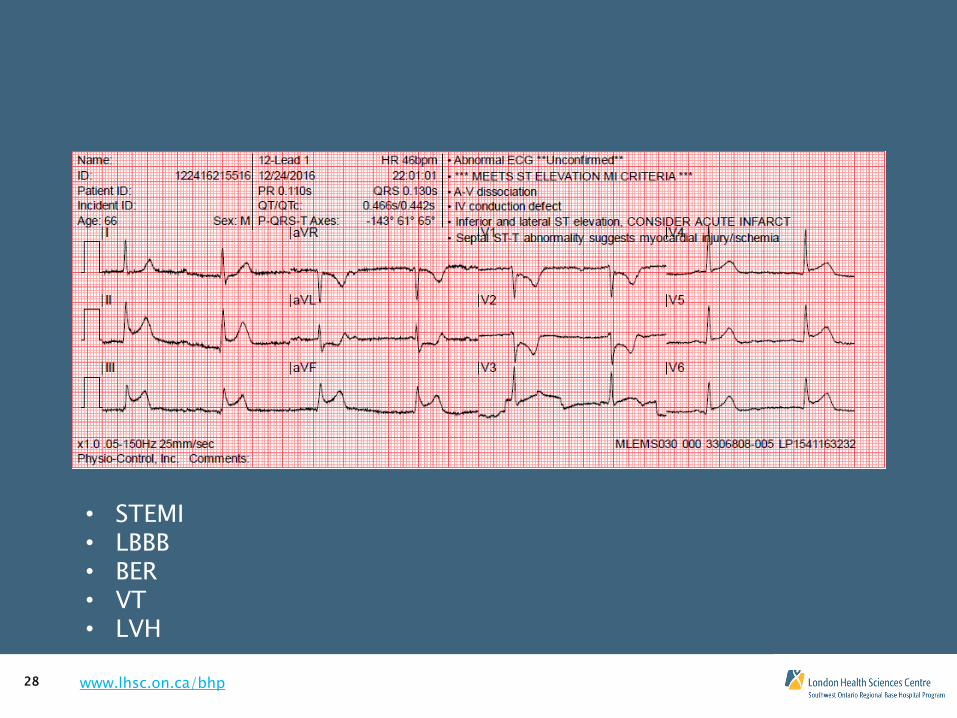
STEMI MIMICS

www.lhsc.on.ca/bhp 2
Objectives
• Recognize that ST segment elevation is a common ECG finding, but often not the result of an MI.
• Identify the most common STEMI mimics and their prevalence.
• Consider some clinical and ECG interpretation techniques for identifying STEMI mimics.
www.lhsc.on.ca/bhp 3
ST Elevation
• ST elevation (STE) can be found in patients presenting with or without chest pain.
• The challenge is, the majority of these patients are NOT experiencing an acute myocardial infarction (AMI).
• It can be challenging to identify STEMI mimics.
www.lhsc.on.ca/bhp 4
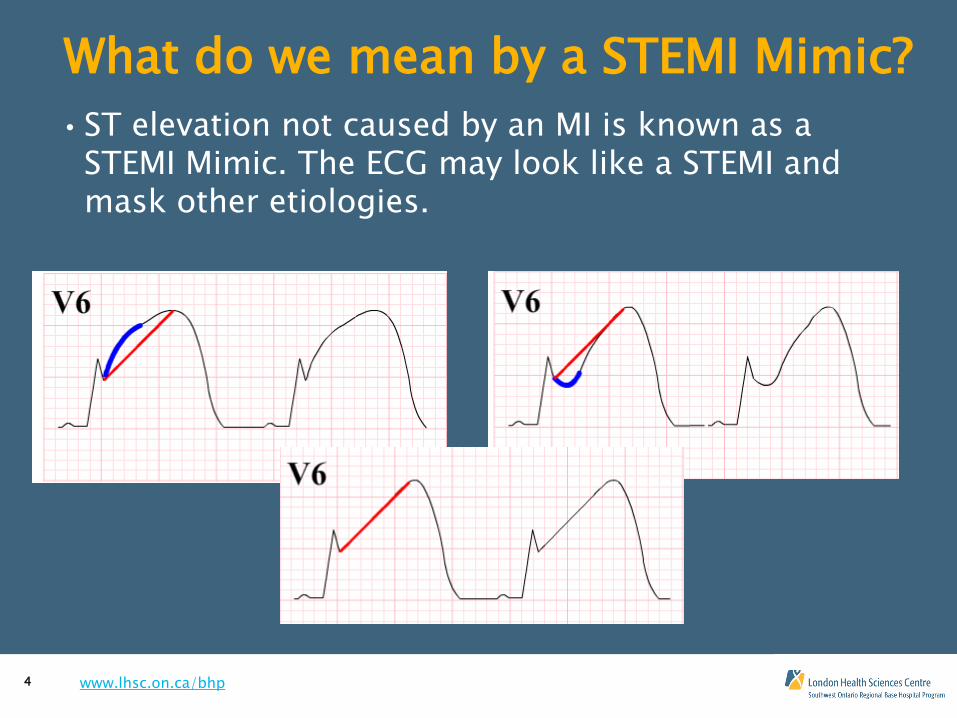
What do we mean by a STEMI Mimic?
• ST elevation not caused by an MI is known as a STEMI Mimic. The ECG may look like a STEMI and mask other etiologies.
www.lhsc.on.ca/bhp 5
Does it matter if we falsely call a MIMIC a STEMI? • Incorrectly identifying STEMI mimics as STEMIs, leads to inappropriate management of patients and use of system resources.
• Of greatest concern in our prehospital environment, is inappropriate Cath Lab Activations which negatively impact limited resources.
• The majority of false Cath Lab activations in SW Ontario are the result of unrecognized MIMICS.

www.lhsc.on.ca/bhp 6
ST Elevation & Chest Pain
• Brady et al study in 2002 evaluated most common causes of ST elevation in patients with chest pain in the ED:
1. Left Ventricular Hypertrophy – 25%
2. Left Bundle Branch Block – 15%
3. Acute Myocardial Infarction – 15%
4. Benign Early Repolarization – 12%
This study illustrates the high potential for incorrect identification of STEMIs.
www.lhsc.on.ca/bhp 7
ST Elevation & Chest Pain
• This presentation will review the 3 most common MIMICS identified on the previous slide:
LVH
LBBB
BER
• And Pericarditis (although this makes up 1% of ST elevation cases)
• Other less common causes of ST elevation and resources to aide in their review will be noted at the end of the presentation.
www.lhsc.on.ca/bhp 8
The Challenge
• No doubt this is a tough topic – many of us get fooled by MIMICS and there are no clinical signs/symptoms, history characteristics or ECG findings which are totally reliable in distinguishing STEMI vs. MIMIC
• Computer interpretation algorithms get fooled by this stuff too, that’s why clinicians must evaluate the whole picture to correctly identify a STEMI patient.
• The new Ontario provincial STEMI directive as well as the 2015 AHA guidelines indicate that paramedic interpretation should be used in addition to computer analysis to make it more likely STEMI MIMICs are identified.
www.lhsc.on.ca/bhp 9
Things To Consider
• ***Acute MI Suspected***
• Computer interpretation is very dependent on data quality, so make the effort to get good data. Artifact and unstable baseline make computer interpretation very difficult.
• Proper lead placement
• Minimize patient movement
• Skin prep if necessary

www.lhsc.on.ca/bhp 10
Basic Stats
Disease/Outcome Present Disease/Outcome Absent
Test Positive True positive False positive
Test Negative False negative True negative
Sensitivity: The ability of a test to correctly identify those with disease, in this case STEMI, without missing anyone by leaving disease undiagnosed. For example, 100 patients known to have disease are tested – 43 test positive, test has a 43% sensitivity.
Specificity: Relates to the ability of the test to correctly identify those without the disease. For example, if 100 people with no disease are tested & 98 return a negative test value, the test has 98% specificity.
Sn = TP/(TP+FN) “SnOut” Sp = TN/(FP+TN) “SpIn”

www.lhsc.on.ca/bhp 11
Basic Stats
Disease/Outcome Present Disease/ Outcome Absent
Test Positive True positive False positive
Test Negative False negative True negative
Negative Predictive Value: “Probability that an individual is not affected with the condition when a negative test result is observed” AKA % of negative test results that are truly negative
Positive Predictive Value: “Probability that an individual is affected with the condition when a positive test result is observed” AKA % of positive test results that are truly positive
NPV = TN/(TN+FN) PPV = TP/(TP + FP)
**NPV and PPV put sensitivity and specificity into context by using disease prevalence
Prev = # of occurrences/total # cases

www.lhsc.on.ca/bhp 13
Concave vs. Convex ST Segment Morphology • Useful in consideration of several MIMICS

www.lhsc.on.ca/bhp 15
Left Ventricular Hypertrophy (LVH)
• Most common cause of STE (25%) BUT LVH doesn’t always have STE.
• QRS voltage patterns are used to determine if LVH vs. STEMI

www.lhsc.on.ca/bhp 16
Left Ventricular Hypertrophy (LVH)
• Voltage Criteria: (present on the example above)
Step 1: Height of S wave in V1 & R wave in V5 or V6 >35mm - if yes, move to step 2
Step 2: R wave in aVL is > 11mm – if yes move to step 3
Step 3: Look for Strain pattern – ST depression & T wave inversion in V5 & V6
• If ALL 3 criteria are met, the patient has LVH with STE and not STEMI!
• One of these criteria in isolation of the other two does not eliminate STEMI

www.lhsc.on.ca/bhp 17
Left Bundle Branch Block (LBBB)
Diagnostic Criteria:
1. QRS Duration >120ms (in V1)
2. Broad, notched R waves in aVL, V5, V6
3. Absent Q waves in aVL, V5, V6
4. Prolonged (>60ms) R wave peak in V5, V6

www.lhsc.on.ca/bhp 18
Left Bundle Branch Block (LBBB)
• Difficulties in diagnosing AMI in patients with LBBB:
• Abnormal ST morphology & T wave polarity discordant to QRS alter the T wave and ST Segment changes usually associated with Acute Coronary Syndrome (ACS).
• Patients with BBB’s have concurrent coronary artery disease and are at higher risk of developing ischemia

www.lhsc.on.ca/bhp 19
Modified Sgarbossa Criteria
• Recognizing ACS in BBB patients can be difficult and is not currently an expectation of paramedics in Ontario, but can be aided by the Modified Sgarbossa Criteria.
• Criteria relating to appropriate ST Segment and T Wave Discordance that can aid in identifying ACS in LBBB, RBBB, LVH, RVH and paced patients.
• The expectation of paramedics in Ontario is to recognize the presence of a BBB. LBBB excludes patient’s from STEMI bypass under the provincial STEMI directive.
• Check out www.lifeinthe fastlane.com for more info on the modified sgarbossa criteria.

www.lhsc.on.ca/bhp 20
Benign Early Repolarization (BER)
• Notching or slurring at the J-point. (Fish Hook)
• Widespread concave ST elevation, most prominent in the mid- to left precordial leads (V2-5).
• Rarely in isolated limb leads.
• Prominent, slightly asymmetrical T-waves that are concordant with the QRS complexes (pointing in the same direction).
• The degree of ST elevation is modest in comparison to the T-wave amplitude (less than 25% of the T wave height in V6)

www.lhsc.on.ca/bhp 21
Benign Early Repolarization (BER)
• Common in younger adults, less common over age 50, rare over age 70.
• Be skeptical of diagnosing BER in patient > 50 with risk factors for ACS & presenting with chest pain.
.
• ST elevation is usually < 2mm in the precordial leads &< 0.5mm in the limb leads, although precordial STE may be up to 5mm in some instances.
• No reciprocal ST depression to suggest STEMI (except in aVR).
• BER changes vary with heart rate, and are more prevalent at lower heart rates.
• ST changes are relatively stable over time (no progression on serial ECG tracings).

www.lhsc.on.ca/bhp 22
Pericarditis
Clinical Manifestations
• Inflammation of the pericardium (e.g. following viral infection) produces characteristic chest pain (retrosternal, pleuritic, worse on lying flat, relieved by sitting forward), tachycardia and dyspnea.
• Widespread ST segment changes occur due to involvement of the underlying epicardium (i.e. myopericarditis).
• Occurs in multiple anatomically disparate leads. If localized to anatomically contiguous leads and/or has reciprocal changes, its STEMI not pericarditis.
• aVR – ST depression should be present in aVR. ST elevation in aVR is highly suggestive of ACS (Left Coronary Artery Occlusion).
• Clinical correlation of history, physical exam and ECG findings is key! These patient often look terrible, but again so can STEMI patients.
www.lhsc.on.ca/bhp 23
Pericarditis
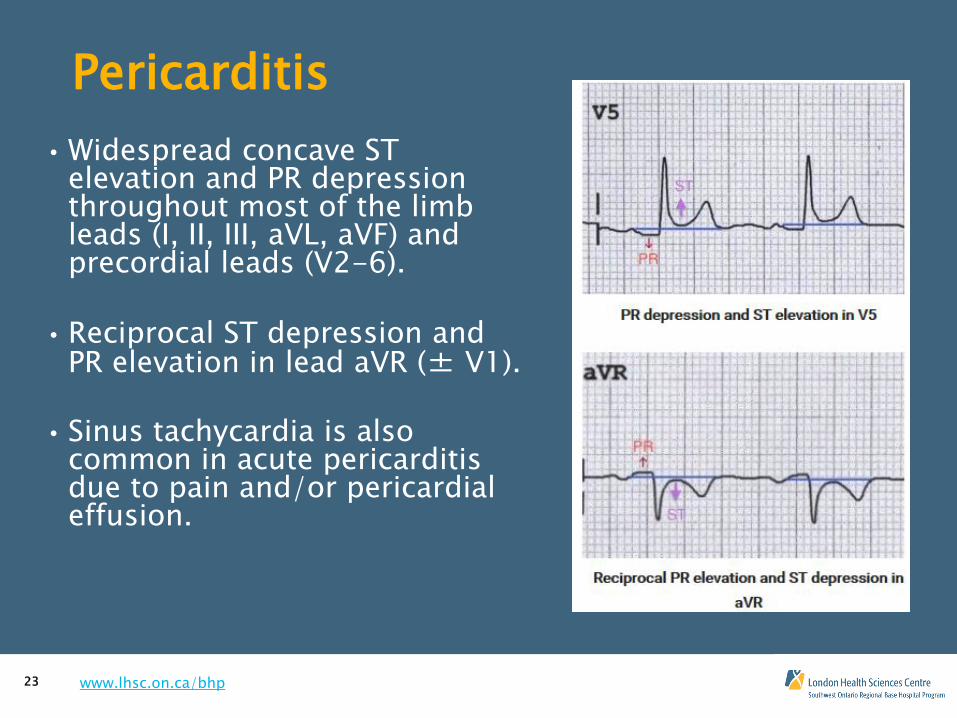
• Widespread concave ST elevation and PR depression throughout most of the limb leads (I, II, III, aVL, aVF) and precordial leads (V2-6).
• Reciprocal ST depression and PR elevation in lead aVR (± V1).
• Sinus tachycardia is also
common in acute pericarditis due to pain and/or pericardial effusion.

www.lhsc.on.ca/bhp 24
Other STEMI MIMICS • Many etiologies may cause ST elevation on ECG.
• This presentation covered the most common.
• The acronym ELEVATION may help you remember other causes
E – Electrolytes (Hyperkalemia)
L – Left Bundle Branch Block
E – Early Repolarization
V – Ventricular Hypertrophy (LVH)
A – Aneurysm (Ventricular)
T – Thailand – (Brugada Syndrome)
I – Inflammation (Pericarditis)
O – Osborne (J) Waves (Hypothermia)
N – Non-ischemic vasospasm (Prinzmetal’s angina)
• Life in the Fast Lane
• Dr. Smith’s ECG Blog
• And many other sites are great resources to learn more about these and any ECG related topics
www.lhsc.on.ca/bhp 25
Wrap Up
How do we apply all this?
• Obtain an early (ideally pre-intervention) 12 lead.
• Are there ST or T wave changes? How profound?
• Reciprocal changes?
• What does the computer interpretation say?
• Does that interpretation seem to correlate with the history, physical and chief complaint you have acquired?
• Did you take steps to ensure best possible data quality by confirming correct lead placement and minimizing movement?
• Obtain serial ECG’s to confirm or guide diagnosis.
• Communicate findings to receiving staff.
• Learn more from resources listed in this presentation.

www.lhsc.on.ca/bhp 31
References
• Ontario Base Hospital Group. Chapter 12 for 12 Lead Training – STEMI Mimics. 2008.
• Managing STEMI Mimics in the Prehospital Environment. Brandon Oto, NREMT-B
• Other references listed in the notes section of each slide.